
Submitted:
17 July 2024
Posted:
17 July 2024
You are already at the latest version
Abstract
Background/Objectives: Encouraging results reported of Platelet-Rich Plasma (PRP) treatment for knee osteoarthritis (KOA). The present retrospective study reports the efficacy and safety of a high dose of neutrophile and red blood cell-depleted PRP to treat 212 patients with KOA. Methods: 212 consecutive patients diagnosed with Kellgren-Lawrence (KL) grading 1-3 KOA chronic knee pain for at least 1 year were treated with 3 injections at 15-day intervals with a high dose of neutrophil-depleted PRP (4 billion platelets). Clinical outcomes were retrospectively recorded as a percentage of responders at 3,6, and 12-month follow-up, following the OMERACT-OARSI criteria. Pain through VAS score and WOMAC score have also been recorded. Results: 4ml of PRP containing 4X109 platelets were obtained by single spin centrifugation and injected intra-articular into each patient with no pre-activation. The overall responder rate of patients responding to OMERACT-OARSI criteria at 3,6,12 months was 68.9%, 72,7% and 70,6%. There was a significant improvement in VAS and WOMAC scores at 3-, 6- and 12-month follow-up compared to the pre-treatment value (p< 0.01). The lowest VAS score was observed at 6 months overall and in all three-grade KL groups. KL2 groups showed the best results regarding pain reduction and WOMAC score at 6 months (p< 0.01). Conclusions: a high dose of neutrophil-depleted PRP is an effective treatment for KL1-3 KOA. It provides symptomatic relief, can potentially reduce disease progression, and has sustained effects for up to 12 months.
Keywords:
High dose PRP
; Knee Osteoarthritis
; neutrophil- depleted
; Leukocyte Poor PRP
1. Introduction
Osteoarthritis (OA) is a cartilage degenerative pathology associated with both structural and functional changes in the joint, affecting more than 500 million people worldwide, with an impressive increase in cases due to the aging of the population [1]. Osteoarthritis doesn’t simply result from regular wear and tear but arises from a multifaceted interaction of genetic, biomechanical, and inflammatory elements [2]. The gradual breakdown of cartilage, changes in subchondral bone density, and the initiation of synovial inflammation all play roles in the development of knee osteoarthritis. This complex of changes is mediated by an interplay of proinflammatory and anti-inflammatory cytokines, chemokines, growth factors, and adipokines, such as leptin [2]. Another interesting aspect of the disease progression are the epigenetic variations able to regulate genetic expression through DNA methylation, histone modifications, and mRNA [2]. In the last 10 years, extensive research has tried to develop non-surgical treatment options to postpone or possibly even replace extensive surgeries such as total knee arthroplasty [3].
Platelet Rich Plasma (PRP) has been used for various indications for more than 30 years, suggesting a promising autologous treatment in regenerative medicine [4,5]. Recently, the European Society of Sports Traumatology, Knee Surgery and Arthroscopy (ESSKA) consensus indicated PRP as a valid treatment option for Knee OA (KOA), based on a growing body of evidence in the existing literature [6]. PRP therapy is the most frequently used autologous Orthobiologic therapy for KOA because it is minimally invasive, repeatable, and safe [6]. Due to chronic inflammation correlated with OA, positive outcomes after PRP treatment are believed to be primarily related to the anti-inflammatory effects of PRP [7,8,9]. PRP has a dual effect on articular cartilage injuries. Firstly, it inhibits NFκB signaling, thus reducing inflammation. Secondly, it promotes chondrocyte secretion of anabolic factors such as TGF-β1, IL-4, IL-10, and IL-13, which stimulate extracellular matrix synthesis and cartilage repair[5,10,11]. It is well known that growth factors secreted by platelets alfa-granules play an essential role in tissue regeneration. In 1987, Sprugel et al. [12] provided in vivo evidence that PDGF, bFGF, and TGF beta induce granulation tissue. The responses that were observed after 10 days were found to represent a secondary process that is primarily mediated through the recruitment of effector immune cells, macrophages and limphocytes, which are drawn into the tissue by each growth factor [12]. Therefore, the effects observed were not directly caused by the factors themselves. Moreover, platelets release chemokines, and cytokines such as platelet factor 4 (PF4), P-Selectins (integrin activators), and RANTES which are responsible for recruiting and activating other immune cells [5]. Additionally, PRP releases Tissue Inhibitors Metallo Proteases (TIMP), which inhibit the increased expression of MMP-1 and MMP-3 induced by inflammatory factors, thereby decreasing extracellular matrix degradation and improving the condition of articular cartilage injury [13]. This data is in accordance with clinical outcomes, which indicates that Leukocyte-Poor PRP (LP-PRP) may be superior to Leukocyte-Rich PRP (LP-PRP) to treat KOA [14,15,16]. Furthermore, it’s widely recognized that the PRP composition ought to have minimal or absent red blood cells (RBCs) to prevent the harmful impact of hemolysis and eryptosis on musculoskeletal tissues [17] . In addition, the analgesic effect of LP-PRP seems to be greater than that of LR-PRP, as shown in a recent meta-analysis on 24 RCTs comprising 1344 patients with knee OA[18]. Moreover, data indicate that multiple injections can outperform a single injection at 1 year follow up [6]. More importantly, the effectiveness of PRP seems to be strongly related to a platelet dose higher than 3.5 × 109 platelets, while a lower platelet dose around 1.5 × 109 platelets showed negative results [11]. In keeping, in our center we treated KOA patients with High Dose Platelets PRP, Leukocyte Poor-PRP (LP-PRP), containing mainly mononuclear cells as the residual WBC population, with no red contamination, able to reach a clinical dose of 4 ×109 platelets in a single spin procedure. Therefore, we performed the present retrospective study to confirm the safety and efficacy of this high platelet dose, neutrophil depleted, autologous PRP for knee OA.
2. Materials and Methods
2.1. Patients
212 consecutive patients, for a total of 636 infiltrative PRP procedures, for chronic symptomatic knee osteoarthritis were treated in our center between 2021 and 2023.
The clinical protocol after PRP quality validation was approved by the Transfusional Center, according to the current regulation of non-transfusional blood component (DM 1.8.2019) with the approval number protocol n.859. For this study the electronic clinical records of this cohort patients were reviewed retrospectively. The study was approved by the ethics committee of our hospital.
All patients treated presented knee osteoarthritis based on Kellgren–Lawrence (KL) grades 1-3 and presented chronic knee pain for at least 1 year despite other known conservative treatments (oral non-steroidal anti-inflammatory drugs, HA or corticosteroid injections). A standing anteroposterior and lateral radiograph was obtained to evaluate the grade of KOA using the Kellgren–Lawrence (KL) classification system.
Each patient was assessed with X-ray, and a complete blood count before PRP treatment was performed.
Inclusion criteria for patients eligible for the protocol included:
- Age: > 18 years
- Hgb: > 12 g/dl
- PLT (minimum value): ≥120,000/µl
- WBC < 10,000/mm3
- No corticosteroid therapies for more than one month
- No NSAIDs for at least one week
Exclusion criteria included sepsis, bacteremia, fever, infectious diseases, immunodeficiency syndromes, hematological diseases, patients on anticoagulant or antiplatelet therapy, severe heart diseases, hemodynamic instability, pregnancy, alcohol abuse and drug use. Patients diagnosed with tricompartmental OA KL grade 4, rheumatoid arthritis, or concomitant severe hip OA, previously treated with a high tibial osteotomy or cartilage transplantation procedure, were not included. We also excluded infections, necrosis, osteomyelitis and inflammation at the inoculation site. Written informed consent was obtained from all patients.
Clinical outcome was evaluated recording the visual analogue scale (VAS) score (0 = no pain to 10 = worst possible pain [19]. Functional levels of the patients were assessed by WOMAC which is considered a reliable and valid method for the assessment of patients with knee OA [20] prior to the first injection and at 3-, 6- and 12-months follow-up.
The clinical outcome follows up of 31 patients was not completed, therefore we collected complete 12-month follow-up data on 212 patients (Figure 1).
To compare efficacy to a previous study on knee OA patients treated with PRP produced by the same device, we also recorded the OMERACT- OARSI score, which is based on a combination of absolute and relative changes in pain, function, and patient global assessment. As in the previous study of Saita et al. [21] patients were classified as responders if one of the following two criteria was fulfilled: (1) high improvement in pain: ≥50% improvement + absolute change of ≥20 in pain; or (2) improvement in at least two of the following: ≥20% improvement + absolute change of ≥10 in pain, ≥20% improvement + absolute change of ≥10 in function, or ≥20% improvement + absolute change of ≥10 in the patient global assessment of disease activity. Clinical outcome was assessed at the initiation of treatment and at 3, 6 and 12 months after the third PRP injection.
2.2. PRP Preparation and Protocol
The PRP production protocol, and the quality of the produced PRP were certified by the Transfusional Center (approval number protocol 859). The PRP preparation was obtained by a single spin centrifugation of whole blood using two Tropocells PRP 11ml Vacutainer tubes (Estar Medical, Israel). This PRP tube contains a separator gel and a buffered pH 7.2 dextrose solution anticoagulant. A total of 22 mL of whole blood was drawn, and 2 mL of PRP was obtained from each tube after PPP was discarded, according to the manufacturer’s instructions. In brief, 22 mL of whole blood was withdrawn into two Tropocells PRP tubes. Next, the tubes were centrifuged for 10 minutes at 1500g. After discarding the supernatant platelet-poor plasma (PPP), 20X gentle mixing was performed to optimize the platelet harvesting from the surface of the separation gel, 2.0 mL of PRP from each tube was recovered and pooled together to obtain a final dose of 4ml of PRP. PRP was immediately injected. PRP was not pre-activated with CaCl2 or Ca/Gluconate, with the aim of having an in vivo activation by the patient’s collagen, in the attempt to release growth factors in the intra-articular space and not before. A blood count and a PRP platelets count were performed to establish the platelet dose.
PRP Injection was performed with the patient placed in the supine position, knees in full extension, with aseptic technique. PRP was injected into the suprapatellar bursa via the lateral suprapatellar approach using a 21-gauge needle. The superior lateral aspect of the patella was palpated, and the needle was inserted 1 cm above and 1 cm laterally. The needle was tilted beneath the patella at a 45-degree angle. If joint fluid could be aspirated, it was removed before injecting the PRP. In our protocol, LP-PRP was injected three times, one every 15 days. After PRP treatment, patients were allowed to bear weight, and local ice application was recommended for 20 minutes, 4-6 times a day, for the initial 48-72 hours to reduce possible discomfort if needed. Activities of the knee were not recommended for 48-72 hours.
2.3. Statistical Analyses
To test the efficacy of PRP therapy, the Fisher’s exact test was performed to compare the results at the baseline and follow-up end points. Fisher’s exact test was performed to compare each KL grade and thus confirm whether the efficacy of PRP therapy was dependent upon the severity of KOA Statistical analysis was performed by an independent statistician using the SPSS software (SPSS 17.0, SPSS, Chicago, USA).
Within groups, the data between the baseline and the follow-up times (3,6,12 months) were compared using the student t test and paired or Wilcoxon signed-rank tests as applicable. The data at the various follow-up points were analyzed using repeated-measures analysis of variance followed by post hoc tests. P < .05 was considered statistically significant for all tests. All p-values were two-sided, and p-values of <0.05 were considered statistically significant.
3. Results
3.1. Patient Characteristics
Table 1 shows the patients’ demographics.
3.2. Biological Characteristics of Injected PRP
Complete blood count before and after were performed on 60 consecutive patients (20 patients for each group KL1, KL2, KL3). The baseline platelet count ranged from 179 to 305 ×103 platelet/µl, mean 225 ± 37×103/µl) corresponding to a total of 4.7 X109 platelets in the drawn blood (4.7± 0.79 X109).
From 20 ml of blood were obtained 4ml of PRP (2ml of PRP from each tube) containing an average platelets concentration of 960+/-108 x103/µl platelets, corresponding to an average platelet dose of 4 X109 (range 3,82 -4.24X109, mean value 3.9+/-0.2). The platelet concentration did not differ across the three KL grade patients’ groups (PRP KL1 937+/- 16, KL2 896+/- 33, KL3 989+/- 25). The obtained platelet recovery rate was 82%, and the platelet concentration fold was 4X. Regarding leukocytes content, the PRP obtained is a LP-PRP, with a depletion of neutrophils, and a residual white blood cells (WBC) concentration of 3 +/- 0.22 X103/µl, mostly represented by mononuclear cell (85%). RBCs concentration <0.05 X106/µl indicating that the separator gel was able to remove RBCs and reverse the initial composition of blood (95% of RBCs). The separation obtained with the gel was stable, no red cell contamination was observed during mixing for inversion to resuspend platelets in PRP.
According to DEPA classification is BBB a high dose platelet (B: high dose of injected platelets, from 3 to 5 billion platelets, B: efficiency platelets recovery rate 70-90%, B pure PRP percentage of platelets in the PRP compared with RBC and leucocytes is from 70% to 90%)[22].According to the PAW classification system the obtained PRP is classified as P3-Bβ PRP (P3; Platelet concentration from 750,000-1,250,000 platelets/mL, no exogen activator, B Leukocyte concentration below baseline level, β Neutrophil concentration below baseline level [23].
Biological characteristics of the obtained PRP are reported in Table 2.
3.3. Clinical Outcome after PRP According to the OMERCAT-OARSI, VAS and WOMAC Score
The clinical outcome was recorded 3,6 to 12 months after PRP therapy. The overall responder rate of patients responding to the OMERACT-OARSI criteria at 3,6,12 months was respectively 71,2%, 73,6% and 69,3%. The highest responder rates were recorded for KL grade 2 at 6 month (76,3%) and 12 months (71,4%). Results are reported in Table 4 and Figure 2.
There was a significant improvement in VAS score at 3-, 6- and 12-months follow-up compared to the pre-treatment value (p< 0.01), as reported in Table 5. The lowest VAS score was observed at 6 months, both overall and in all three grade KL groups.
At 12 month the VAS score was higher than at 6 months, even if it was still significatively lower than at the basal level, suggesting that the analgesic effect of PRP started to vanish. KL2 groups showed the best result regarding pain reduction at 6-month FU.
A similar trend was observed for the WOMAC total score: there was a significant improvement at 6- and 12-month follow-up, compared to the pre-treatment value (p< 0.01).
The best clinical WOMAC total score were recorded at 6-month overall and in all three KL groups. The best clinically significant outcome was observed in all groups at 6 months.
All three KL groups showed patients with mild transient adverse events like pain andstiffness. No adverse effects were observed in any patients.
4. Discussion
PRP has received significant attention lately as a potential Disease Modifying OA Drug (DMOAD) therapy for symptomatic knee osteoarthritis [6,24,25].
The PRP used in this study is classified as P3-Bβ PRP according to the PAW classification system [23], while according to the DEPA classification is BBB a high dose platelet [22].
Our retrospective study on 212 patients demonstrated that a dose of 4 billion platelets (3.9+/- 0.2) in 4 ml volume of neutrophil poor-PRP improves functional outcomes and reduces pain in patients with grade 1-3 KL KOA. Moreover, we observed in our cohort of patients an overall Responder Rate based on OMERACT-OARSI responder criteria, of 71,2 %, 73,6% and 69,3% respectively at 3,6,12 months. The most beneficial effects in terms of the number of responder patients, and clinical outcome reach their peak after 6 months of the injections and are reduced later at 12 months, even though the outcome remains better compared to the pre-treatment baseline level. Our data are in line with those observed in a prospective clinical study on 517 patients with grade KL2 and KL3 KOA treated with LP-PRP produced by the same PRP device, where 4 to 5 mL of LP-PRP was injected three times every 4 weeks, resulting in a 75.2% responder rate in KL2 and 66.5 % in KL3 after 12 months [21]. Saita et al. [21] also treated KL4 grade which showed a significantly lower responder rate (50.9%) than KL2 and KL3 patients. In this study, a multivariate logistic regression analysis showed that the higher grade of knee osteoarthritis is a significative predictor of a negative clinical outcome, showing that the relative risk for non-responders in severe KL4 KOA was 2.1 (95% CI, 1.5–3.0) at 6 months and 2.3 (1.6–3.2) at 12 months when compared with KL2 and KL3 grade KOA. Based on this data, we decided to exclude KL4 patients, and treat KL1 KOA patients instead, which showed a high rate of responders at 6 and 12 months, 76,4% and 71,2% respectively.
Our results in terms of clinical outcome measured as VAS and WOMAC score are in line with earlier studies, although comparison is rather difficult because of huge differences in PRP platelet concentrations and dose, leukocytes, and red blood cell contents [6,26,27,28]. Despite all these challenges and confounding factors, a recent meta-analysis of 35 RCT demonstrated best overall outcome in patients treated with PRP as compared to control, HA or steroids at 3, 6, 12 months follow up intervals, as observed in our study [26]. More interesting is to compare our real-world data to RCTs trials data on KOA treated with a comparable PRP in terms of leukodepletion and platelet dose. Patel et al. [25] RCT trial compared the efficacy of two different single-injection LP-PRP platelet doses in patients diagnosed with KL1 and KL2 KOA: 4 mL of PRP standard dose containing 2.8 billion/platelet (2.82 X109) billion and 8 ml of PRP containing 5.5 billion platelets (5.65 X109). The leucocyte-poor PRP used was 3.5 times concentrated, with an average platelet concentration of 706.74 X103/µl in the standard dose group and 681.44 X103/µl in the high dose group [25]. [25]. Patients with early knee OA had significantly better improvement in pain and function when treated with an 8 mL injection of PRP containing a high platelet dose of 5.5 billion compared with a 4 mL injection of PRP containing a lower dose of 2.8 billion platelets [25].
Recently, this data was confirmed in a systematic review by Berrigan et al[29]. This analysis showed that 28 studies, with a mean platelet dose of 5.5 +/- 0.4 billion platelets, had statistically significant positive outcomes at 6 months vs control, whereas 3 studies with a low mean platelet dose of 2.3 +/-0.4 showed no difference versus control (P < .01) [29].These data strongly suggest that clinical outcomes from PRP implants for KOA could be related to a higher platelet dose. These data also strongly support the idea that concentration alone does not correspond to dosage, and it can be misleading [10,30]. A proper concentration calculation should consider the baseline platelet concentration (which varies among patients), the volume of blood collected, and the final volume of the PRP product. Dosage should be standardized, referring to the absolute number of platelets and any other components of PRP delivered per injection, as is the case with any other therapeutic drug, leading to the new concept of a minimal effective platelet dose PRP. Our data supports the efficacy of a neutrophil poor PRP containing 4 billion platelet doses, comparable to the 5 billion doses used by Patel et al[25]. In fact, Patel et al [25] noted a different trend in the results between the two dose groups: a continuously improving trend in outcome scores from 3-month to 6-month follow-up in the 5.5 billion platelet dose group while in the 2.5 billion platelets, the best scores were measured at 3-month with deterioration at 6 months, albeit still better than the baseline. Our retrospective trial observed the same trend in all three KL grades groups.
Interestingly, an optimal platelets dose superior to 3,5 billion was supported for the first time, by Everts et al[31]. The effectiveness of different dose PRP was studied in a variety of soft tissue studies, including tendinopathies, hamstring pathologies, meniscus lesions, and plantar fasciitis, relating for the first time the clinical outcome to the platelet doses [31]. Studies with less than 2 × 109 dose platelets injected, showed a negative result, while studies where dose exceeded 3.5 × 109 platelets generally reported more positive results [31]. In keeping with the RESTORE randomized trial, patients with symptomatic KL2 and KL3 KOA treated with PRP intra-articular injection of 1.6×109 platelets (325 X103/µl, 5 ml PRP), compared with saline placebo, showed no significant difference in symptoms or joint structure at 12 months [32]. Moreover, a recent study suggests a 10 billion platelet dose for a sustained therapeutic effect in KOA with a significant improvement of IKDC and WOMAC scores at one year follow-up [24]. For these reasons, we are evaluating switching from our actual LP-PRP protocol based on 2 PRP tubes drawing 10 ml of blood each, which ensures 4 billion platelets are injected, to 2 PRP tubes drawing 20 ml of blood with the same separator gel to harvest 8 billion platelet doses. An alternative strategy could be to repeat PRP treatment with 4 billion platelets after 12 months.
An explanation for the correlation between high dose platelets or high concentration folds (3-5X) and pain reduction, could be the high concentrations of serotonin released by platelet dense granules [5]. PRP can reduce pain in patients treated for lateral epicondylitis and knee OA, as observed in a systematic review and meta-analysis [33].
In addition to the high platelet dose, regarding the biological profile, the PRP used in this study is neutrophil-depleted, red cells depleted, with a physiological concentration of mononuclear cells and non-activated (Tab.2).
Regarding the presence of red blood cells, data indicates clearly that it is essential to reduce or eliminate the content of RBCs in PRP formulations to avoid the damaging effects of hemolysis and eryptosis on musculoskeletal tissues [17].Therefore the PRP formulation of these biologics should contain minimal to no RBCs [34]
The effect of leukocyte concentration in PRP preparation is highly debated [35]. Studies have shown that leucocytes in PRP can damage cartilage, whereas leukocyte-poor PRP promotes chondrogenesis in vivo and better functional outcomes [15,36,37,38] . Neutrophils can cause harmful effects, such as the release of inflammatory cytokines and matrix metalloproteinases (MMPs) that promote pro-inflammatory and catabolic effects [39]. Positive outcomes after PRP treatment for OA are believed to be primarily related to the anti-inflammatory effects of PRP [7,8]. Moreover, the risk of local adverse reactions appeared to be increased after LR-PRP compared with LP-PRP injection [40]. A recent meta-analysis suggests that leukocyte-poor PRP may be a superior line of treatment for knee OA over leukocyte-rich PRP[41]. Data are in accordance with the indications from another meta-analysis, which suggest that the analgesic effect of LP-PRP was greater than that of LR-PRP [42]. On the other hand, not all the leukocytes are the same: neutrophils are inflammatory cells, triggering post-PRP treatment flares, while monocytes and macrophage phenotypes are regenerative cells that support various mechanisms of action in tissue regeneration [5] [43,44]. Based on extensive in vitro and in vivo data on peripheral blood mononuclear cells (PBMNC), autologous preparations containing monocytes and lymphocytes are key players in tissue regeneration [45,46,47,48,49,50,51]. PBMNC showed enhanced cartilage repair, increased cell migration, and an immunomodulation effect both in animals and humans [52,53,54,55]. Interestingly, preliminary positive results in OA treatment by PBMNC autologous implants were observed[56,57,58,59,60] Moreover, PBMNC, together with a high dose of platelets, may recruit other immune cells [51]. It was well described that platelets in PRP should contribute to chemotactic cell migration and stimulate immunomodulatory activities[5] as observed for the first time by Sprugel, which indicates that PDGF, bFGF, and TGF beta induce granulation tissue through a secondary process mediated by macrophages and lymphocytes rather than a direct effect of the factors themselves [12]. To maximize this effect, GF release should be slow and last over time, especially considering the very short life of GFs (from minutes to hours) [61]. It is also demonstrated that when pure PRP is given to tissue, it activates slowly upon encountering type I collagen in the absence of this preactivation[62] . Moreover, studies have shown that the proliferation of mesenchymal stem cells is increased five-fold by inactive pH 7 buffered PRP [63]. More importantly, in a different study, it was shown that inactivated PRP enhanced the development of cartilage and bone both in vivo and in vitro, while activated PRP reduced chondrogenesis and osteogenesis [64] . Regarding safety, we did no observe any minor or major complications in our patient’s cohort. Our real-world data showed that inactivated, pH 7 buffered neutrophil and RBCs-depleted high dose PRP a positive outcome at 6 and 12 months in KL1-2-3 grade KOA patients, with no adverse effects.
5. Conclusions
Despite the major limitation of our study, which is the absence of a control group, this real-world data showed that a high dose of neutrophils and RBC-depleted PBMNC at physiological levels and inactivated PRP is an effective treatment for KL1-KL3 KOA, showing an overall responder rate of 70%. It provides symptomatic relief, has the potential to reduce disease progression, and has sustained effects for up to 12 months. Moreover, this study supports evidence that a clinically effective PRP contains 4 billion platelets, suggesting that the dose is the most critical parameter for sustained therapeutic effect. However, further studies are mandatory to evaluate if higher doses (8–10 billion) are more beneficial. Moreover, the complete absence of adverse events and side effects from using an autologous product uncontaminated by populations that can generate local inflammation should not be overlooked. This treatment can therefore be recommended for patients with KOA of varying degrees and can also be repeated over time. Furthermore, it remains a viable alternative for patients who do not respond to other conservative treatments or for patients who cannot or do not wish to undergo surgery.
Author Contributions
Conceptualization, ADM. and GM.; methodology, ADM, MB and RP.; software, ADM; validation.; writing—original draft preparation, ADM, MB and RP; writing—review and editing, ADM and GM.; visualization, ADM; supervision, GM. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Gemelli Hospital a (protocol code 859) for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
For this study the electronic clinical records of this cohort patients were reviewed retrospectively. The data are not publicly available due to protection of patients’ privacy.
Acknowledgments
The authors are grateful to Dr. Laura Rehak, for the basic science rationale and references.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 354 Diseases and Injuries for 195 Countries and Territories, 1990-2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [CrossRef]
- Primorac, D.; Molnar, V.; Rod, E.; Jeleč, Ž.; Čukelj, F.; Matišić, V.; Vrdoljak, T.; Hudetz, D.; Hajsok, H.; Borić, I. Knee Osteoarthritis: A Review of Pathogenesis and State-Of-The-Art Non-Operative Therapeutic Considerations. Genes (Basel) 2020, 11, 1–35. [CrossRef]
- Gangadharan, S.B.; Satapathy, S.; Dixit, T.; C, Dr.S.; Ravindran, S.; Parida, P.K. Platelet-Rich Plasma Treatment for Knee Osteoarthritis: A Systematic Investigation. Multidisciplinary Reviews 2024, 6, 2023ss015. [CrossRef]
- Everts, P.A.; van Erp, A.; DeSimone, A.; Cohen, D.S.; Gardner, R.D. Platelet Rich Plasma in Orthopedic Surgical Medicine. Platelets 2021, 32, 163–174. [CrossRef]
- Everts, P.; Onishi, K.; Jayaram, P.; Lana, J.F.; Mautner, K. Platelet-Rich Plasma: New Performance Understandings and Therapeutic Considerations in 2020. Int J Mol Sci 2020, 21, 1–36. [CrossRef]
- Laver, L.; Filardo, G.; Sanchez, M.; Magalon, J.; Tischer, T.; Abat, F.; Bastos, R.; Cugat, R.; Iosifidis, M.; Kocaoglu, B.; et al. The Use of Injectable Orthobiologics for Knee Osteoarthritis: A European ESSKA-ORBIT Consensus. Part 1—Blood-derived Products (Platelet-rich Plasma). Knee Surgery, Sports Traumatology, Arthroscopy 2024. [CrossRef]
- Zahir, H.; Dehghani, B.; Yuan, X.; Chinenov, Y.; Kim, C.; Burge, A.; Bandhari, R.; Nemirov, D.; Fava, P.; Moley, P.; et al. In Vitro Responses to Platelet-Rich-Plasma Are Associated with Variable Clinical Outcomes in Patients with Knee Osteoarthritis. Scientific Reports 2021 11:1 2021, 11, 1–13. [CrossRef]
- Gato-Calvo, L.; Magalhaes, J.; Ruiz-Romero, C.; Blanco, F.J.; Burguera, E.F. Platelet-Rich Plasma in Osteoarthritis Treatment: Review of Current Evidence. Ther Adv Chronic Dis 2019, 10, 1–18. [CrossRef]
- Andia, I.; Maffulli, N. Platelet-Rich Plasma for Managing Pain and Inflammation in Osteoarthritis. Nat Rev Rheumatol 2013, 9, 721–730. [CrossRef]
- Everts, P.A.; Mazzola, T.; Mautner, K.; Randelli, P.S.; Podesta, L. Modifying Orthobiological PRP Therapies Are Imperative for the Advancement of Treatment Outcomes in Musculoskeletal Pathologies. Biomedicines 2022, 10. [CrossRef]
- Everts, P.A.; Lana, J.F.; Onishi, K.; Buford, D.; Peng, J.; Mahmood, A.; Fonseca, L.F.; van Zundert, A.; Podesta, L. Angiogenesis and Tissue Repair Depend on Platelet Dosing and Bioformulation Strategies Following Orthobiological Platelet-Rich Plasma Procedures: A Narrative Review. Biomedicines 2023, 11. [CrossRef]
- Sprugel, K.H.; Mcpherson, J.M.; Clowes, A.W.; Ross, R. Effects of Growth Factors in Vivo I. Cell Ingrowth Into Porous Subcutaneous Chambers; 1987; Vol. 129;
- Liang, Y.; Li, J.; Wang, Y.; He, J.; Chen, L.; Chu, J.; Wu, H. Platelet Rich Plasma in the Repair of Articular Cartilage Injury: A Narrative Review. Cartilage 2022, 13. [CrossRef]
- Gupta, A.; Jeyaraman, M.; Potty, A.G. Leukocyte-Rich vs. Leukocyte-Poor Platelet-Rich Plasma for the Treatment of Knee Osteoarthritis. Biomedicines 2023, 11.
- Di Martino, A.; Boffa, A.; Andriolo, L.; Romandini, I.; Altamura, S.A.; Cenacchi, A.; Roverini, V.; Zaffagnini, S.; Filardo, G. Leukocyte-Rich versus Leukocyte-Poor Platelet-Rich Plasma for the Treatment of Knee Osteoarthritis: A Double-Blind Randomized Trial. Am J Sports Med 2022, 50, 609–617. [CrossRef]
- Zhou, Y.; Li, H.; Cao, S.; Han, Y.; Shao, J.; Fu, Q.; Wang, B.; Wu, J.; Xiang, D.; Liu, Z.; et al. Clinical Efficacy of Intra-Articular Injection with P-PRP Versus That of L-PRP in Treating Knee Cartilage Lesion: A Randomized Controlled Trial. Orthop Surg 2023, 15, 740–749. [CrossRef]
- Everts, P.A.; Malanga, G.A.; Paul, R. V.; Rothenberg, J.B.; Stephens, N.; Mautner, K.R. Assessing Clinical Implications and Perspectives of the Pathophysiological Effects of Erythrocytes and Plasma Free Hemoglobin in Autologous Biologics for Use in Musculoskeletal Regenerative Medicine Therapies. A Review. Regen Ther 2019, 11, 56. [CrossRef]
- Xiong, Y.; Gong, C.; Peng, X.; Liu, X.; Su, X.; Tao, X.; Li, Y.; Wen, Y.; Li, W. Efficacy and Safety of Platelet-Rich Plasma Injections for the Treatment of Osteoarthritis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front Med (Lausanne) 2023, 10. [CrossRef]
- Carlsson, A.M. Assessment of Chronic Pain. I. Aspects of the Reliability and Validity of the Visual Analogue Scale. Pain 1983, 16, 87–101. [CrossRef]
- Pham, T.; van der Heijde, D.; Altman, R.D.; Anderson, J.J.; Bellamy, N.; Hochberg, M.; Simon, L.; Strand, V.; Woodworth, T.; Dougados, M. OMERACT-OARSI Initiative: Osteoarthritis Research Society International Set of Responder Criteria for Osteoarthritis Clinical Trials Revisited. Osteoarthritis Cartilage 2004, 12, 389–399. [CrossRef]
- Saita, Y.; Kobayashi, Y.; Nishio, H.; Wakayama, T.; Fukusato, S.; Uchino, S.; Momoi, Y.; Ikeda, H.; Kaneko, K. Predictors of Effectiveness of Platelet-Rich Plasma Therapy for Knee Osteoarthritis: A Retrospective Cohort Study. J Clin Med 2021, 10. [CrossRef]
- Magalon, J.; Chateau, A.L.; Bertrand, B.; Louis, M.L.; Silvestre, A.; Giraudo, L.; Veran, J.; Sabatier, F. DEPA Classification: A Proposal for Standardising PRP Use and a Retrospective Application of Available Devices. BMJ Open Sport Exerc Med 2016, 2. [CrossRef]
- Delong, J.M.; Russell, R.P.; Mazzocca, A.D. Platelet-Rich Plasma: The PAW Classification System. Arthroscopy - Journal of Arthroscopic and Related Surgery 2012, 28, 998–1009. [CrossRef]
- Bansal, H.; Leon, J.; Pont, J.L.; Wilson, D.A.; Bansal, A.; Agarwal, D.; Preoteasa, I. Platelet-Rich Plasma (PRP) in Osteoarthritis (OA) Knee: Correct Dose Critical for Long Term Clinical Efficacy. Sci Rep 2021, 11. [CrossRef]
- Patel, S.; Gahlaut, S.; Thami, T.; Chouhan, D.K.; Jain, A.; Dhillon, M.S. Comparison of Conventional Dose Versus Superdose Platelet-Rich Plasma for Knee Osteoarthritis: A Prospective, Triple-Blind, Randomized Clinical Trial. Orthop J Sports Med 2024, 12. [CrossRef]
- Qiao, X.; Yan, L.; Feng, Y.; Li, X.; Zhang, K.; Lv, Z.; Xu, C.; Zhao, S.; Liu, F.; Yang, X.; et al. Efficacy and Safety of Corticosteroids, Hyaluronic Acid, and PRP and Combination Therapy for Knee Osteoarthritis: A Systematic Review and Network Meta-Analysis. BMC Musculoskelet Disord 2023, 24. [CrossRef]
- Ivander, G.; Anggono, Y. A Comparison of Intra-Articular Hyaluronic Acid and Platelet-Rich Plasma for Knee Osteoarthritis: A Systematic Review. Orthop Rev (Pavia) 2024, 16. [CrossRef]
- Migliorini, F.; Driessen, A.; Quack, V.; Sippel, N.; Cooper, B.; Mansy, Y. El; Tingart, M.; Eschweiler, J. Comparison between Intra-Articular Infiltrations of Placebo, Steroids, Hyaluronic and PRP for Knee Osteoarthritis: A Bayesian Network Meta-Analysis. Arch Orthop Trauma Surg 2021, 141, 1473–1490. [CrossRef]
- Berrigan, W.A.; Bailowitz, Z.; Park, A.; Reddy, A.; Liu, R.; Lansdown, D. A Higher Platelet Dose May Yield Better Clinical Outcomes for PRP in the Treatment of Knee Osteoarthritis: A Systematic Review. Arthroscopy 2024. [CrossRef]
- Prost, D.; Bardot, T.; Baud, A.; Calvo, A.; Aumont, S.; Collado, H.; Borne, J.; Rajon, O.; Ponsot, A.; Malaterre, A.; et al. Long Term Improvement of Knee Osteoarthritis after Injection of Single High/Very High Volume of Very Pure PRP: A Retrospective Analysis of Patients Optimally Managed in Dedicated Centers. Regen Ther 2024, 25, 203–212. [CrossRef]
- Everts, P.A.; Lana, J.F.; Onishi, K.; Buford, D.; Peng, J.; Mahmood, A.; Fonseca, L.F.; van Zundert, A.; Podesta, L. Angiogenesis and Tissue Repair Depend on Platelet Dosing and Bioformulation Strategies Following Orthobiological Platelet-Rich Plasma Procedures: A Narrative Review. Biomedicines 2023, 11. [CrossRef]
- Bennell, K.L.; Paterson, K.L.; Metcalf, B.R.; Duong, V.; Eyles, J.; Kasza, J.; Wang, Y.; Cicuttini, F.; Buchbinder, R.; Forbes, A.; et al. Effect of Intra-Articular Platelet-Rich Plasma vs Placebo Injection on Pain and Medial Tibial Cartilage Volume in Patients With Knee Osteoarthritis: The RESTORE Randomized Clinical Trial. JAMA 2021, 326, 2021–2030. [CrossRef]
- Johal, H.; Khan, M.; Yung, S. hang P.; Dhillon, M.S.; Fu, F.H.; Bedi, A.; Bhandari, M. Impact of Platelet-Rich Plasma Use on Pain in Orthopaedic Surgery: A Systematic Review and Meta-Analysis. Sports Health 2019, 11, 355–366. [CrossRef]
- Gupta, A.; Maffulli, N.; Jain, V.K. Red Blood Cells in Platelet-Rich Plasma: Avoid If at All Possible. Biomedicines 2023, 11. [CrossRef]
- Gupta, A.; Jeyaraman, M.; Potty, A.G. Leukocyte-Rich vs. Leukocyte-Poor Platelet-Rich Plasma for the Treatment of Knee Osteoarthritis. Biomedicines 2023, 11. [CrossRef]
- Xu, Z.; Yin, W.; Zhang, Y.; Qi, X.; Chen, Y.; Xie, X.; Zhang, C. Comparative Evaluation of Leukocyte-and Platelet-Rich Plasma and Pure Platelet-Rich Plasma for Cartilage Regeneration. Sci Rep 2017, 7. [CrossRef]
- Peng, Y.; Guanglan, W.; Jia, S.; Zheng, C. Leukocyte-Rich and Leukocyte-Poor Platelet-Rich Plasma in Rotator Cuff Repair: A Meta-Analysis. Int J Sports Med 2022, 0. [CrossRef]
- Lana, J.F.; Huber, S.C.; Purita, J.; Tambeli, C.H.; Santos, G.S.; Paulus, C.; Annichino-Bizzacchi, J.M. Leukocyte-Rich PRP versus Leukocyte-Poor PRP - The Role of Monocyte/Macrophage Function in the Healing Cascade. J Clin Orthop Trauma 2019, 10, S7–S12. [CrossRef]
- Fedorova, N. V.; Ksenofontov, A.L.; Serebryakova, M. V.; Stadnichuk, V.I.; Gaponova, T. V.; Baratova, L.A.; Sud’ina, G.F.; Galkina, S.I. Neutrophils Release Metalloproteinases during Adhesion in the Presence of Insulin, but Cathepsin G in the Presence of Glucagon. Mediators Inflamm 2018, 2018. [CrossRef]
- Kim, J.H.; Park, Y.B.; Ha, C.W.; Roh, Y.J.; Park, J.G. Adverse Reactions and Clinical Outcomes for Leukocyte-Poor Versus Leukocyte-Rich Platelet-Rich Plasma in Knee Osteoarthritis: A Systematic Review and Meta-Analysis. Orthop J Sports Med 2021, 9. [CrossRef]
- Belk, J.W.; Kraeutler, M.J.; Houck, D.A.; Goodrich, J.A.; Dragoo, J.L.; McCarty, E.C. Platelet-Rich Plasma Versus Hyaluronic Acid for Knee Osteoarthritis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. American Journal of Sports Medicine 2021, 49, 249–260. [CrossRef]
- Xiong, Y.; Gong, C.; Peng, X.; Liu, X.; Su, X.; Tao, X.; Li, Y.; Wen, Y.; Li, W. Efficacy and Safety of Platelet-Rich Plasma Injections for the Treatment of Osteoarthritis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front Med (Lausanne) 2023, 10, 1204144. [CrossRef]
- Ogle, M.E.; Segar, C.E.; Sridhar, S.; Botchwey, E.A.; Coulter, W.H. Monocytes and Macrophages in Tissue Repair: Implications for Immunoregenerative Biomaterial Design. Exp Biol Med 2016, 241, 1084–1097. [CrossRef]
- Wynn, T.A.; Vannella, K.M. Macrophages in Tissue Repair, Regeneration, and Fibrosis. Immunity 2016, 44, 450–462. [CrossRef]
- Caballero-Sánchez, N.; Alonso-Alonso, S.; Nagy, L. Regenerative Inflammation: When Immune Cells Help to Re-Build Tissues. FEBS J 2024, 291, 1597–1614. [CrossRef]
- Groppa, E.; Colliva, A.; Vuerich, R.; Kocijan, T.; Zacchigna, S. Immune Cell Therapies to Improve Regeneration and Revascularization of Non-Healing Wounds. Int J Mol Sci 2020, 21, 1–22. [CrossRef]
- Forbes, S.J.; Rosenthal, N. Preparing the Ground for Tissue Regeneration: From Mechanism to Therapy. Nat Med 2014, 20, 857–869. [CrossRef]
- Julier, Z.; Park, A.J.; Briquez, P.S.; Martino, M.M.; Julier, Z.; Park, A.J.; Briquez, P.S.; Martino, M.M. Promoting Tissue Regeneration by Modulating the Immune System. Acta Biomater 2017, 53, 13–28. [CrossRef]
- Chisari, Em.; Rehak, L.; Khan, W.S.; Maffulli, N. The Role of the Immune System in Tendon Healing: A Systematic Review. Br Med Bull 2020, 133, 49–54. [CrossRef]
- Chisari, E.; Rehak, L.; Khan, W.S.; Maffulli, N. Tendon Healing in Presence of Chronic Low-Level Inflammation: A Systematic Review. Br Med Bull 2019, 132, 97–116. [CrossRef]
- Rehak, L.; Giurato, L.; Meloni, M.; Panunzi, A.; Manti, G.M.; Uccioli, L. The Immune-Centric Revolution in the Diabetic Foot: Monocytes and Lymphocytes Role in Wound Healing and Tissue Regeneration—A Narrative Review. J Clin Med 2022, 11.
- Hopper, N.M.; Wardale, J.; Rushton, N. Mononuclear Cells Enhance Cell Migration out of Human Articular Cartilage. J Tissue Eng Regen Med 2012, 6.
- Hopper, N.; Wardale, J.; Brooks, R.; Power, J.; Rushton, N. Peripheral Blood Mononuclear Cells Enhance Cartilage Repair in in Vivo Osteochondral Defect Model. 2015, 1–16. [CrossRef]
- Hopper, N.; Wardale, J.; Howard, D.; Brooks, R.; Rushton, N.; Henson, F. Peripheral Blood Derived Mononuclear Cells Enhance the Migration and Chondrogenic Differentiation of Multipotent Mesenchymal Stromal Cells. Stem Cells Int 2015, 2015. [CrossRef]
- Yuan, Z.; Jiang, D.; Yang, M.; Tao, J.; Hu, X.; Yang, X.; Zeng, Y. Emerging Roles of Macrophage Polarization in Osteoarthritis: Mechanisms and Therapeutic Strategies. Orthop Surg 2024, 16, 532–550. [CrossRef]
- Zhu, Y.; Fu, W. Peripheral Blood-Derived Stem Cells for the Treatment of Cartilage Injuries: A Systematic Review. Front Bioeng Biotechnol 2022, 10, 956614. [CrossRef]
- Abdine, N.M.; Moustafa, K.A.; Bakery, R.H.E.; Sarhan, N.E.; Salah, E.F. Effect of Intra-Articular Injection of Peripheral Blood Mononuclear Cells Versus Platelet-Rich Plasma on Restoration of Collagen Fibers of the Articular Cartilage in a Rat Model of Knee Osteoarthritis. Egyptian Journal of Histology 2023, 46, 1861–1869. [CrossRef]
- Bohaud, C.; Contreras-Lopez, R.; De La Cruz, J.; Terraza-Aguirre, C.; Wei, M.; Djouad, F.; Jorgensen, C. Pro-Regenerative Dialogue Between Macrophages and Mesenchymal Stem/Stromal Cells in Osteoarthritis. Front Cell Dev Biol 2021, 9, 2367. [CrossRef]
- Kanda, K.; Asawa, Y.; Inaki, R.; Fujihara, Y.; Hoshi, K.; Hikita, A. Requirement of Direct Contact between Chondrocytes and Macrophages for the Maturation of Regenerative Cartilage. Scientific Reports 2022 11:1 2021, 11, 1–17. [CrossRef]
- Li, M.; Yin, H.; Yan, Z.; Li, H.; Wu, J.; Wang, Y.; Wei, F.; Tian, G.; Ning, C.; Li, H.; et al. The Immune Microenvironment in Cartilage Injury and Repair. Acta Biomater 2022, 140, 23–42. [CrossRef]
- Roh, Y.H.; Kim, W.; Park, K.U.; Oh, J.H. Cytokine-Release Kinetics of Platelet-Rich Plasma According to Various Activation Protocols. Bone Joint Res 2016, 5, 37. [CrossRef]
- Mishra, A.; Woodall, J.; Vieira, A. Treatment of Tendon and Muscle Using Platelet-Rich Plasma. Clin Sports Med 2009, 28, 113–125. [CrossRef]
- Mishra, A.; Tummala, P.; King, A.; Lee, B.; Kraus, M.; Tse, V.; Jacobs, C.R. Buffered Platelet-Rich Plasma Enhances Mesenchymal Stem Cell Proliferation and Chondrogenic Differentiation. Tissue Eng Part C Methods 2009, 15, 431–435. [CrossRef]
- Han, B.; Woodell-May, J.; Ponticiello, M.; Yang, Z.; Nimni, M. The Effect of Thrombin Activation of Platelet-Rich Plasma on Demineralized Bone Matrix Osteoinductivity. J Bone Joint Surg Am 2009, 91, 1459–1470. [CrossRef]
Figure 1.
1 Flowchart of the retrospective cohort data collection.
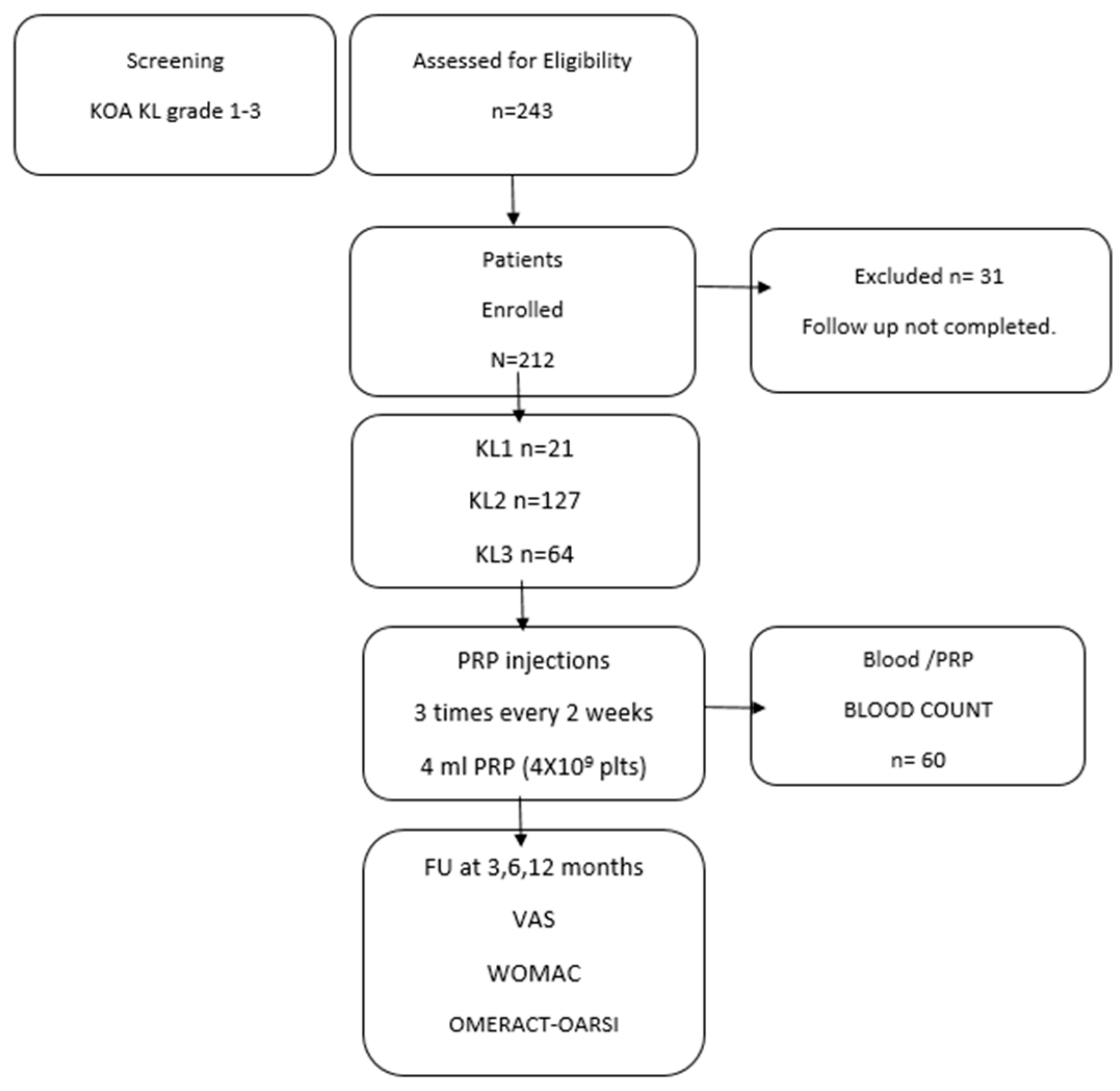
Figure 2.
Responder Rate (OMERACT-OARSI).
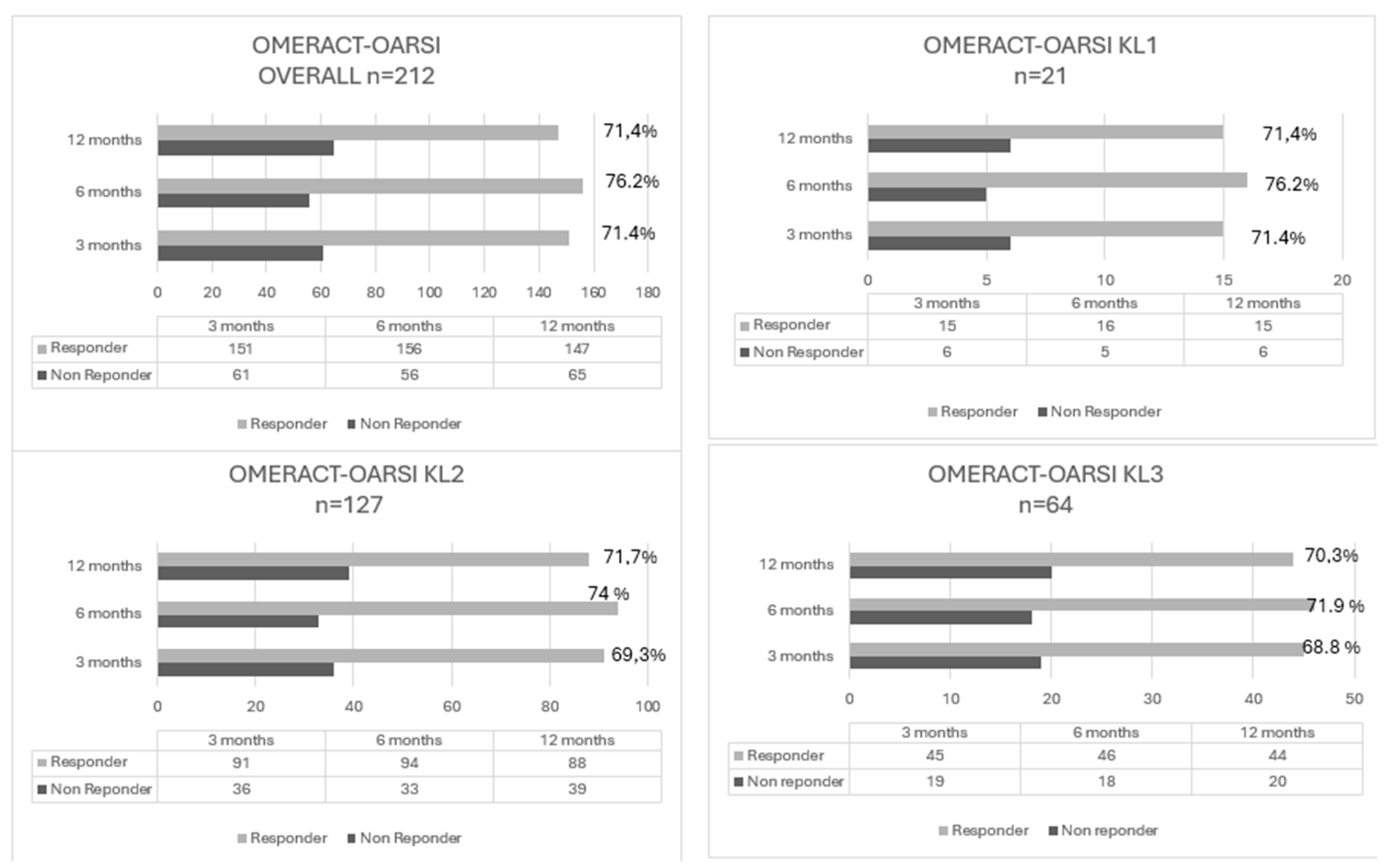

Table 1.
Patient Characteristics.
| n=212 | |
|---|---|
|
Age (mean +/- SD) Range (years) |
56.09 +/- 9.23 19-89 |
|
Gender Male n (%) Female n (%) |
42% 58% |
|
BMI (kg/m2) Range BMI |
25.3 +/-4.1 23-28.3 |
| Side | |
| Left /Right Knee (%) | 44%/56% |
| KL Grade | |
| Grade 1 n (%) | 21 out 212 (9,9 %) |
| Grade 2 n (%) | 127 out 212 (59,9 %) |
| Grade 3 n (%) | 64 out 212 (30,2 %) |
| Basal Platelets (X103/µl) | 225+/- 37 |
| VAS score | 6.49 +/- 1.15 |
| WOMAC score | 41.98 +/- 6.8 |
KL, Kellgren–Lawrence; PRP, platelet-rich plasma.
Table 2.
Biological characteristics of injected PRP (n=60).
| Blood | PRP | |
|---|---|---|
| Blood Volume /PRP volume* | 20 ml | 4.1 +/- 0.3 |
| Platelet Conc. (103/µl) | 235+/- 37 | 960+/- 108 |
| Platelet dose (Billions 109) | 4.7 +/-0.79 | 3.9+/- 0.2 |
| WBC (103/µl) | 10.3 +/- 2.3 | 3 +/- 0.22 |
| Granulocyte (103/µl) | 7.5 +/- 0.89 | 0.5 +/- 0.05 |
| Limphocytes (103/µl) | 2.7+/- 1.6 | 2.1+/- 0.8 |
| Monocytes (103/µl) | 0.78+/- 1.8 | 0.42+/- 0.49 |
| PB-MNC (103/µl) | 3.56 +/- 1.2 | 2.38 +/- 0.98 |
| RBC (106/µl) | 5.40+/- 2.9 | 0.053 +/- 0.01 |
| Platelets conc fold | 4 X | |
| Platelet Recovery Rate% | 82,1 +/- 0,4 | |
| % Mononuclear cells/WBC | 80 % |
*n=60 (n=20 for each KL group). Two TropoCells PRP tubes for each patient were used for a total of 20ml blood withdrawal and 4ml of PRP injected.
Table 4.
Responder Rate OMERACT-OARSI responder criteria at 3,6,12 months.
| Non-Responder | Responder | Patients | Responder Rate | |
|---|---|---|---|---|
| Overall | ||||
| 3 months | 61 | 151 | n=212 | 71,2% |
| 6 months | 56 | 156 | n=212 | 73,6 % |
| 12 months | 66 | 147 | n=212 | 69,3, % |
| KL Grade 1 | ||||
| 3 months | 6 | 15 | n= 21 | 71,4% |
| 6 months | 5 | 16 | n= 21 | 76,2% |
| 12 months | 6 | 15 | n= 21 | 71,4% |
| KL Grade 2 | ||||
| 3 months | 36 | 91 | n= 127 | 71,7 % |
| 6 months | 33 | 94 | n= 127 | 74,0% |
| 12 months | 39 | 88 | n= 127 | 69,3% |
| KL Grade 3 | ||||
| 3 months | 19 | 45 | n=64 | 70,3% |
| 6 months | 18 | 46 | n=64 | 71,9% |
| 12 months | 20 | 44 | n=64 | 68,8% |
*Two TropoCells PRP 11 ml tubes for each patient, 4ml PRP injected.
Table 5.
Clinical outcome VAS, WOMAC at 3,6,12 months.
| Basal- Pretreatment | 3m | 6m | 12m | |
|---|---|---|---|---|
| VAS pain | ||||
| Overall | 6.49 +/- 1.15 | 4.3 +/- 1.8* | 2.69 +/- 0.98* | 3.79 +/- 0.78* |
| KL1 | 6.02 +/- 1.09 | 4.66 +/- 1.23* | 2.81 +/- 0.6* | 3.81+/- 0.3* |
| KL2 | 6.41 +/- 0.65 | 4.15+/- 0.98* | 2.6+/- 0.53* | 3.65+/- 0.89* |
| KL3 | 6.58+/- 1.09 | 4.99+/- 1.2* | 2.4+/- 0.99* | 3.48+/- 1.1* |
| WOMAC | ||||
| Overall | 41.98 +/- 6.8 | 36.55+/- 13.5* | 34.9 +/- 11.8* | 39.3 +/- 8,05 |
| KL1 | 40.65 +/- 11.9 | 36.99 +/- 9.5* | 35.8 +/- 12.3* | 38.2 +/- 9,99 |
| KL2 | 41.65 +/- 9.5 | 35.05 +/- 9.99* | 34.1 +/- 14.0* | 38.1 +/- 8,67 |
| KL3 | 40.65 +/- 3.9 | 36.18 +/- 4.89* | 35.8 +/- 9.06* | 40.13 +/- 12.04 |
Data are reported as mean ± SD. VAS, visual analog scale; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index. *Significant differences between groups for that time point (P < .001; Wilcoxon signed-rank test).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



