
Submitted:
17 July 2024
Posted:
18 July 2024
You are already at the latest version
Abstract
Abstract: Background: Gender dimorphism and marital status on colorectal cancer mortality have 9 been previously documented, but the relationship between these factors and DNA mismatch repair 10 protein (MMRP) expression status is unknown. Methods: Colectomy specimens were reviewed ret- 11 rospectively for patients between 2018 to 2023 with demographics including race/ethnicity, gender, 12 marital status, faith, body mass index, pathologic staging, and MMRP expression status. Statistical 13 analyses were performed by using baseline characteristics tables and various programs in R-pack- 14 age. Results: A total 1018 colectomies were reviewed, and the tumor stages were significantly higher 15 in right colon (stage 3 and 4) than those in left colon and rectosigmoid colon (p<0.01). Marital status 16 was significantly associated with patients’ gender, age, tumor size and tumor stages (all p<0.01). 17 MMRP status were available in 775 cases, and 139 (17.9%) were MMRP deficient, and 636 (82%) 18 MMRP proficient. MMRP deficiency was significantly associated with older female patients, larger 19 tumor in size, higher tumor stages, higher histologic grade and more common in right colon (all 20 p<0.01). In addition, MMRP deficiency was statistically associated with higher percentage of di- 21 vorced and widowed patients (p<0.01). Multivariate linear regression analysis revealed persistent 22 association of MMRP deficiency with tumor size, tumor grade, tumor stage and nodal metastasis, 23 but the associations with gender and marital status no longer existed. Conclusion: The differences 24 in prevalence of CRC by gender and marital status and tumor MMRP status illustrate the im- 25 portance of these factors on tumor stages and nodal metastasis but these associations were more 26 complex with other confounding factors.
Keywords:
Colorectal Cancer
; DNA Mismatch repair enzyme
; Gender and Marital status
Introduction
Colorectal carcinoma (CRC) is one of the most common malignancies worldwide with increasing incidence due to dietary and lifestyle changes and population screening by colonoscopy in recent decades [1,2,3,4,5]. Significant age and gender differences in colorectal carcinoma regarding morbidity and mortality have been previously documented through large series of epidemiology studies [6,7,8,9]. Marital status also plays important roles in cancer mortality overall [10,11,12,13]. However, the difference between the gender and marital status and DNA mismatch repair protein expression (MMRP) is unknown. MMRP by immunohistochemistry has been validated to reflect the status of microsatellites stability (MSI) of tumors in clinical setting, and it is generally accepted that MMRP deficient tumors are MSI-high and MMRP proficient tumors are MSI-low (stable) [14]. MSI-H tumors were known to be more responsive to immune therapy (check point inhibitor therapy) through large clinical trials in clinically important tumors [15,16,17,18]. CRC is one of the earliest cancer type to adopt MSI testing (MMRP) as standard practice not only for therapeutic purpose but also for screening for Lynch syndrome, a genetic condition with susceptibility to various cancers especially in patients with family history of colon cancer [19]. MMRP testing results have been incorporated into clinical decision making for all newly diagnosed CRC patients [20].
Our previous study on relationship between endometrial carcinoma and MMRP status of tumor raised a question of mental health on MMRP gene expression manifested through standard marital status reporting in the medical records [21]. As MMRP testing by IHC was originally adopted in CRC, we sought to see if the relationship between marital status and MMRP status on endometrial carcinoma can be repeated in CRC. Our current data illustrated the importance of mental health not only on patients’ mental wellbeing, but also physically tumor gene expression, tumor staging, nodal metastasis and ultimately patient’s therapeutic planning and prognosis.
Materials and Methods
The Study Patients
The retrospective study is exempt from institutional review board approval according to section 46.101(b) of 45CFR 46, which states that research involving the study of existing pathologic and diagnostic specimens in such a manner that subjects cannot be identified is exempt from the Department of Health and Human Services Protection of Human Research Subjects. It was performed in accordance with STROBE guideline in reporting for cohort study. Colectomy specimens for neoplasia were searched in the medical record from 2018 to November 2023 and included in the study using the routine hematoxylin-eosin (H&E) stain. The clinical patients’ information including demographics was obtained from the medical records and entered in Excel spreadsheet, together with pathologic staging information including tumor type, histology, lymph node status. The data were collected in blind fashion and no randomization or preference was given in the entire dataset.
Inclusion and Exclusion Criteria
Only invasive carcinomas were included in the study and high grade dysplasia/intraepithelial (intramucosal) carcinoma were excluded. Patients with missing data (attrition) were excluded from the study.
Race/Ethnicity, Patients’ Demographics and Body Mass Index (BMI)
The patients’ racial/ethnic data were retrieved from the electronic medical record (Cerner System) according to the Center for Medicare and Medicaid Services (CMS) criteria as Asian, non-Hispanic Black, Hispanic, and non-Hispanic White. The racial/ethnic data also included “unknown”, “others”, or “declined” as one group without further information. Patients gender (sex) was retrieved from the medical record as female and male, and marital status were defined as Married, Single, Divorced/separated, and Widowed. Patients who declined to answer the marital status questions were recorded as “Other” including “decline”, “others” and “unknown”. Religious belief was recorded in binary fashion as “Yes” or “No”, and no specific religious type was used for analysis. The patients’ age and body mass index (BMI) were retrieved from the medical record, and patients’ body weights were not used for analysis.
Data Availability
The entire dataset will be available upon reasonable request for research only after the manuscript is published.
Statistical Analysis
Statistical analysis was performed by using various programs of R-Package including baseline characteristic table and multi-variant ANOVA tests. p<0.05 is considered statistically significant in all tests (http://statistics4everyone.blogspot.com/2018/01/fathers-data-visualization.html).
DNA Mismatch Repair Protein Expression (MMRP)
Immunostaining for DNA mismatch repair proteins including MLH1, MSH2, MSH6 and PMS2 was performed by using Ventana Benchmark Ultra instrument (Roche Corporation). Pathology reporting of tumors was performed as standard practice by using software of standard synoptic format from College of American Pathologists (CAP) updated and maintained by CAP.
Results
Distribution of CRC Based on Anatomic Sites and Tumor Stages
A total 1018 CRC cases from colectomy specimens were reviewed with clinical and pathologic characteristics as well as patients’ race/ethnicity, marital status, faith (religious belief), patient’s age, body mass index (BMI) and MMRP status. There were significant variations in frequencies of CRC of different anatomic sites (Figure 1). These CRC distribution results in various anatomic sites were similar to those described previously [1]. Based on the tumor size (tumor TNM staging), CRC was divided into four T-stages (Table 1). Stage 1 represented 15.3%, stage 2 14%, stage 3 48.7% and stage 4 21.9%. The tumor stages were significantly higher (stages 3 and 4) in right colon (ascending colon and cecum) than those of left colon or rectosigmoid colon p<0.01). Tumor stages were significantly positively correlated with histologic grade and lymph node metastasis (p<0.01), as expected. High tumor stages were significantly associate with lower patients’ BMI (p<0.01). There was no significant association between the race/ethnicity and gender (sex) and the tumor stages (Supplementary Table 1).
Sex and Marital Status Differences in CRC
There were 536 female patients (52.7%) and 482 male patients (47.3%) with CRC in our cohort. Statistically significantly more female patients were divorced and widowed (Table 2). There appeared more BRAF gene mutations in tumors from female patients than those from male patients (p=0.01)(Table 2). Marital status was statistically significantly associated with tumor stages, and the divorced and the widowed patients were significantly associated with higher tumor stages (stage 3 and 4) than the married patients (Table 1 and Table 3). The divorced and widowed patients were older, more females, with larger tumor size (all p<0.01, Table 1 and Table 3). Faith (religious belief) was more common in female patients (p<0.01) (Table 3).
MMRP Status in CRC
MMRP status by immunohistochemistry was available in 775 cases, and there were 139 cases (17.9%) with MMRP deficient tumors, and 636 cases (82%) with MMRP proficient tumors. There were 28 cases (3.6% of total, 20% of MMRP deficient tumors) with features consistent with Lynch syndrome, and the remaining 111 cases (80% of MMRP deficient tumor) were consistent with sporadic mutations/MLH1 gene methylations. MMRP deficiency was significantly associated with marital status (p<0.01), female gender (p<0.01), older patient age (p<0.01), tumor size (p<0.01), tumor anatomic location (p<0.01), tumor stage, tumor histologic grade and nodal metastasis (all p<0.01) (Table 4). MMRP deficient tumors were significantly larger in size, more common in right colon (ascending colon and cecum), higher histologic grade and higher tumor stages, as expected. MMRP deficient tumors were more common in divorced and widowed patients (Table 3 and table 4). After removal of probable Lynch syndrome patients from the cohort, MMRP deficiency due to sporadic mutation/MLH1 gene methylations showed similar results as described above (Table 4). The remaining 28 probable Lynch syndrome patients showed higher histologic grade, larger tumor in size and more common in the right colon, as previously described (data not shown). No significant associations between MMRP deficiency due to Lynch syndrome and marital status, gender, tumor stage and nodal metastatic stages were observed (data not shown). There was no significant difference in race/ethnicity, faith (religious belief) and BMI and MMRP status. Multivariate linear regression analysis using MMRP status revealed persistent association between MMRP deficiency and tumor size, tumor grade, tumor stage and lymph node metastasis (Figure 2). The associations between gender and marital status and MMRP status no longer existed.
Race/ethnicity was significantly associated with marital status, BMI, patients’ age, and faith (religious belief); and faith was found more common in female patients (supplementary Tables 1, 2 and 3). Approximately 10% CRC in our data were from patients younger than 50 (10.1%) (supplementary Table 3), and racial/ethnic minority groups including Asian, Black and Hispanic groups were more affected younger than the racial/ethnic White patient population (supplementary Table 3). The age-adjusted higher prevalence of CRC in male patients previously demonstrated was only showed in the age group of 60-69 in our dataset, and significantly higher prevalence of CRC was observed in female patients younger than 40 years (Supplementary Table 3).
Discussion
We have showed the clinical and pathologic characteristics of CRC in our institution from 2018 to November 2023. Despite decades of population screening by colonoscopy, the high stages CRCs (stage 3 and 4, 70.6%) in our dataset were more than doubled than those of low stage tumors (29.4%). It is difficult to determine the etiology of this variation in tumor stage of CRC, especially the overall number of low tumor stage CRCs (N=299 stage 1 and 2) was less that that of high stage CRCs (N=719). However, it is worth noting that our dataset contained invasive carcinomas only (T1 or higher), and intraepithelial carcinomas/intramucosal carcinomas (Tis) were not included in our study.
Our data also showed that there were significant gender and marital status differences in tumor sizes and tumor stages by single variate analysis, and the divorced or widowed patients were significantly more likely to have larger tumors and higher stage CRCs. Moreover, divorced or widowed patients had significantly more MMRP deficient tumors. These associations between gender/marital status and MMRP status were no longer identified by multivariate linear regression analysis, suggesting more complex multifactorial/biological process. MMRP deficiency in CRC has been extensively studied in Lynch syndrome and in predicting therapeutic efficacies using checkpoint inhibitors [22,23]. Our data showed that MMRP deficient tumors were significantly more common in right colon and transverse colon, as previously demonstrated [19], and MMRP deficiency was associated with larger tumor size, higher histologic grade, higher tumor stages, more nodal metastasis. Our data also showed that 20% of MMRP deficient tumors by IHC were Lynch syndromes, and the remaining 80% MMRP deficient tumors were sporadic due likely to MLH gene methylations [24]. MLH gene methylation is epigenetic event that can be affected by lifestyle modification. Current CRC data confirmed our previous finding that divorce or loss of life partner (widowed) exerted significant effects on MMRP gene expression, likely through methylation of MLH gene promoters [21]. It is also important to note that the relationship between divorced or widowed patients and MMRP deficiency was more significant in older female patients in CRC. These results indicated that socioemotional and psychological health of cancer patients plays an important role in tumor gene expression, tumor pathology and tumor stage, ultimately affecting the prognosis and treatment of cancer patients.
Conclusions
Socioemotional and psychological health of cancer patients is important for tumor gene expression, tumor pathology and tumor stages, ultimately affecting the prognosis and therapy of cancer patients.
Funding
No funding was received for the study.
Authorship contribution statement
PZ conceptualized the study, collected and analyzed the data, and drafted the manuscript. OB, CW, BC, JL and SS contributed to conception, data collection, critically reviewed the data and contributed to writing. AC, LK and MS contributed to data collection, data analyses and writing the manuscript. All authors read and approved the manuscript.
Financial disclosure
Authors declare no conflict of interest.
References
- Society, A.C., Colorectal Cancer Facts & Figures 2023-2025 . . 2022.
- Baidoun, F., et al., Colorectal Cancer Epidemiology: Recent Trends and Impact on Outcomes. Curr Drug Targets, 2021. 22(9): p. 998-1009.
- Arnold, M., et al., Global patterns and trends in colorectal cancer incidence and mortality. Gut, 2017. 66(4): p. 683-691. [CrossRef]
- Lu, L., et al., A global assessment of recent trends in gastrointestinal cancer and lifestyle-associated risk factors. Cancer Commun (Lond), 2021. 41(11): p. 1137-1151. [CrossRef]
- Siegel, R.L., et al., Colorectal cancer statistics, 2023. CA Cancer J Clin, 2023. 73(3): p. 233-254. [CrossRef]
- Baraibar, I., et al., Sex and gender perspectives in colorectal cancer. ESMO Open, 2023. 8(2): p. 101204. [CrossRef]
- Wong, M.C.S., et al., Differences in Incidence and Mortality Trends of Colorectal Cancer Worldwide Based on Sex, Age, and Anatomic Location. Clin Gastroenterol Hepatol, 2021. 19(5): p. 955-966.e61. [CrossRef]
- Ramai, D., et al., Gender and racial disparities in colorectal cancer incidence and mortality: a national cancer registry study. Int J Colorectal Dis, 2021. 36(8): p. 1801-1804. [CrossRef]
- van Erning, F.N., et al., Gender differences in tumor characteristics, treatment and survival of colorectal cancer: A population-based study. Cancer Epidemiol, 2023. 86: p. 102441.
- Montiel Ishino, F.A., et al., A National Study of Colorectal Cancer Survivorship Disparities: A Latent Class Analysis Using SEER (Surveillance, Epidemiology, and End Results) Registries. Front Public Health, 2021. 9: p. 628022. [CrossRef]
- Li, Q., et al., The influence of marital status on stage at diagnosis and survival of patients with colorectal cancer. Oncotarget, 2015. 6(9): p. 7339-47. [CrossRef]
- Martínez, M.E., et al., Differences in marital status and mortality by race/ethnicity and nativity among California cancer patients. Cancer, 2016. 122(10): p. 1570-8. [CrossRef]
- Wang, Y., et al., Sex differences in the association between marital status and the risk of cardiovascular, cancer, and all-cause mortality: a systematic review and meta-analysis of 7,881,040 individuals. Glob Health Res Policy, 2020. 5: p. 4. [CrossRef]
- Zito Marino, F., et al., Microsatellite Status Detection in Gastrointestinal Cancers: PCR/NGS Is Mandatory in Negative/Patchy MMR Immunohistochemistry. Cancers (Basel), 2022. 14(9). [CrossRef]
- Sargent, D.J., et al., Defective mismatch repair as a predictive marker for lack of efficacy of fluorouracil-based adjuvant therapy in colon cancer. J Clin Oncol, 2010. 28(20): p. 3219-26. [CrossRef]
- Kumarasinghe, A.P., et al., DNA mismatch repair enzyme immunohistochemistry in colorectal cancer: a comparison of biopsy and resection material. Pathology, 2010. 42(5): p. 414-20. [CrossRef]
- André, T., et al., Nivolumab plus low-dose ipilimumab in previously treated patients with microsatellite instability-high/mismatch repair-deficient metastatic colorectal cancer: 4-year follow-up from CheckMate 142. Ann Oncol, 2022. 33(10): p. 1052-1060. [CrossRef]
- André, T., et al., Pembrolizumab in Microsatellite-Instability-High Advanced Colorectal Cancer. N Engl J Med, 2020. 383(23): p. 2207-2218. [CrossRef]
- Thibodeau, S.N., G. Bren, and D. Schaid, Microsatellite instability in cancer of the proximal colon. Science, 1993. 260(5109): p. 816-9. [CrossRef]
- Amin, M.B., et al., AJCC Cancer Staging Manual. 8th ed. 2017: Springer Cham.
- Zhang, P., Mendoza, Art., Bakhtar, O., Wixom, C., Muller, S., Sadeghi, S., Clement, A., Kabakibi, L., Schwab, M., Race/ethnicity and social determinants of health in endometrial carcinomaand DNA mismatch repair protein expression status. Obstetrics & Gynecology, 2024. In review.
- Sun, B.L., Current Microsatellite Instability Testing in Management of Colorectal Cancer. Clin Colorectal Cancer, 2021. 20(1): p. e12-e20. [CrossRef]
- Sahin, I.H., et al., Immune checkpoint inhibitors for the treatment of MSI-H/MMR-D colorectal cancer and a perspective on resistance mechanisms. Br J Cancer, 2019. 121(10): p. 809-818. [CrossRef]
- Uribe, Y., et al., Intersectionality Between Epigenetics and Cancer Health Disparities Stemming from Social Determinants of Health (SDoH) Through a Gynecologic Oncology Lens: A Narrative Review. Clin Obstet Gynecol, 2023. 66(1): p. 53-62. [CrossRef]
Figure 1.
Distribution of CRC based on the anatomic sites. Left panel showed the percentage of CRC at each anatomic locations. The right panel showed distribution of CRC in right colon, transverse colon, left colon, and rectosigmoid colon. .
Figure 1.
Distribution of CRC based on the anatomic sites. Left panel showed the percentage of CRC at each anatomic locations. The right panel showed distribution of CRC in right colon, transverse colon, left colon, and rectosigmoid colon. .
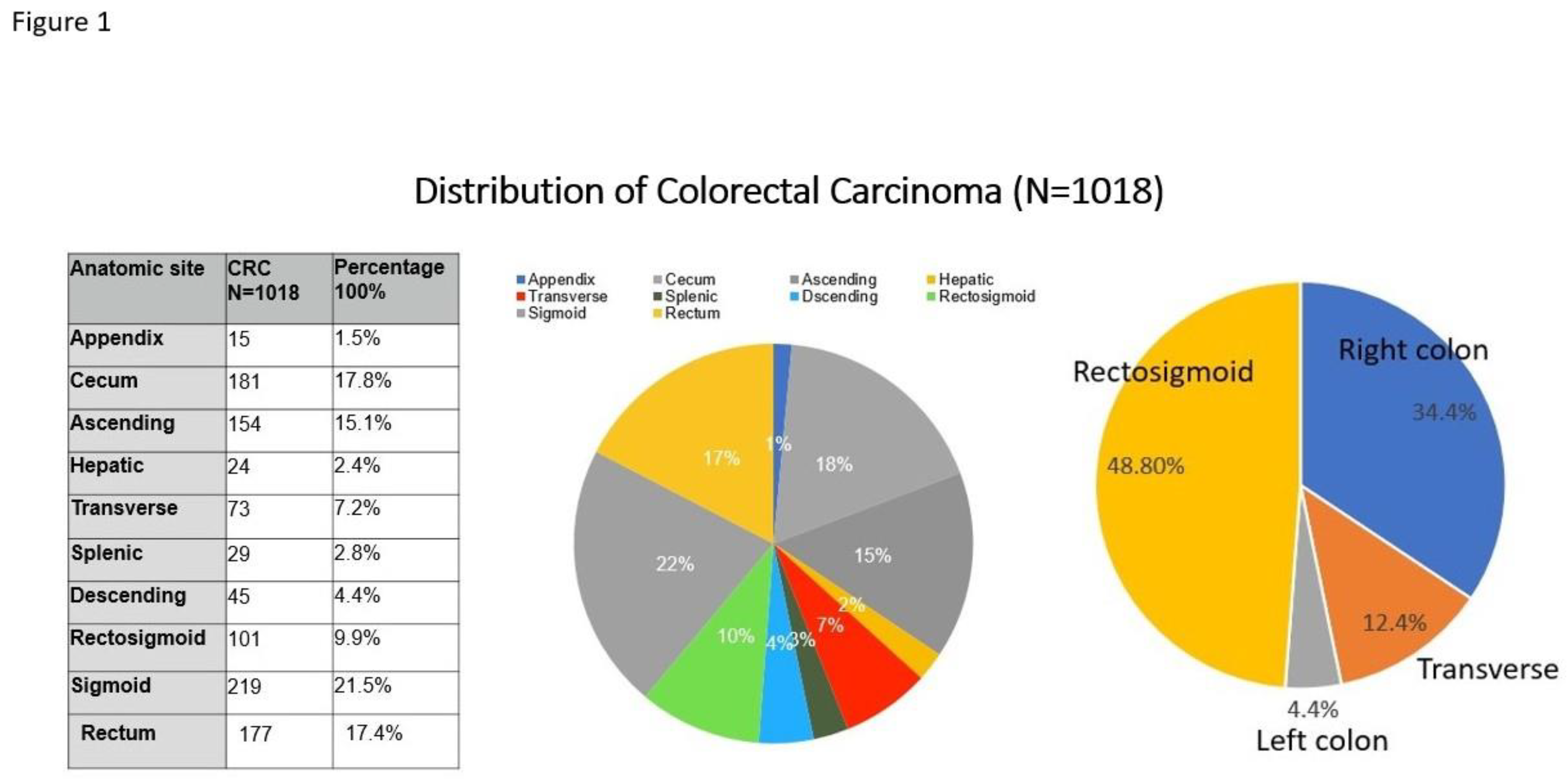
Figure 2.
Multivariate linear regression model of MMRP status in CRC patients. p<0.05 is considered statistically significant.
Figure 2.
Multivariate linear regression model of MMRP status in CRC patients. p<0.05 is considered statistically significant.
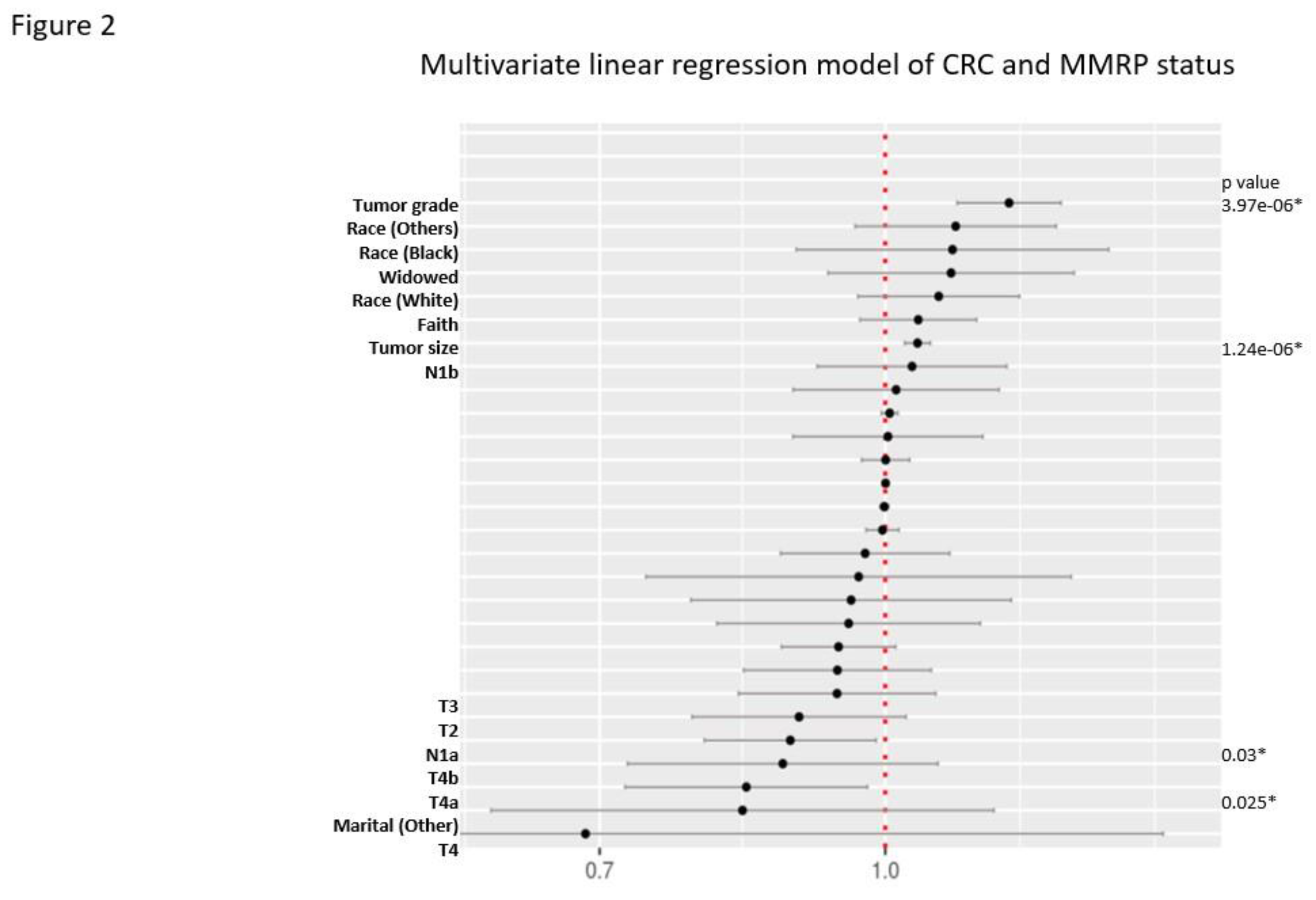

Table 1.
Tumor Stage of Colorectal Carcinoma.
| T-stage | T1 | T2 | T3 | T4 | p |
|---|---|---|---|---|---|
| (N=156)(15.3%) | (N=143)(14%) | (N=496)(48.7%) | (N=223)(21.9%) | ||
| Marital status | <0.01 | ||||
| - Divorced | 10 ( 6.4%) | 17 (11.9%) | 61 (12.3%) | 33 (14.8%) | |
| - Married | 96 (61.5%) | 81 (56.6%) | 244 (49.2%) | 103 (46.2%) | |
| - Other | 1 ( 0.6%) | 1 ( 0.7%) | 5 ( 1.0%) | 2 ( 0.9%) | |
| - Single | 41 (26.3%) | 32 (22.4%) | 103 (20.8%) | 60 (26.9%) | |
| - Widowed | 8 ( 5.1%) | 12 ( 8.4%) | 83 (16.7%) | 25 (11.2%) | |
| BMI | 26.0 [23.0;31.0] | 27.0 [23.0;30.0] | 25.0 [22.0;30.0] | 24.0 [21.0;29.0] | <0.01 |
| MMRP status | <0.01 | ||||
| - Proficient | 83 (91.2%) | 97 (89.8%) | 309 (78.0%) | 147 (81.7%) | |
| - Deficient | 8 ( 8.8%) | 11 (10.2%) | 87 (22.0%) | 33 (18.3%) | |
| Faith (religious belief) | 88 (59.9%) | 85 (60.7%) | 324 (66.8%) | 141 (64.7%) | 0.34 |
| Sex (gender) | 0.65 | ||||
| - Female | 82 (52.6%) | 69 (48.3%) | 269 (54.2%) | 116 (52.0%) | |
| - Male | 74 (47.4%) | 74 (51.7%) | 227 (45.8%) | 107 (48.0%) | |
| Patient's age (year) | 63.0 [54.5;72.0] | 65.0 [55.0;78.0] | 70.0 [60.0;81.0] | 67.0 [59.0;76.5] | <0.01 |
| Tumor size (cm) | 1.0 [ 0.5; 2.0] | 3.0 [ 1.5; 4.0] | 4.6 [ 3.3; 5.8] | 5.1 [ 3.8; 7.3] | <0.01 |
| Histologic grade | <0.01 | ||||
| - Grade 1 | 82 (52.6%) | 50 (35.0%) | 118 (23.8%) | 37 (16.6%) | |
| - Grade 2 | 70 (44.9%) | 87 (60.8%) | 332 (66.9%) | 141 (63.2%) | |
| - Grade 3 | 4 ( 2.6%) | 6 ( 4.2%) | 46 ( 9.3%) | 45 (20.2%) | |
| Lymph node number | 17.0 [12.0;21.0] | 17.0 [14.0;23.0] | 19.0 [14.0;26.0] | 18.0 [14.0;25.0] | <0.01 |
| N stage (TNM-N) | <0.01 | ||||
| - No data | 12 ( 7.7%) | 9 ( 6.3%) | 2 ( 0.4%) | 3 ( 1.3%) | |
| - No nodal metastasis | 124 (79.5%) | 100 (69.9%) | 264 (53.2%) | 55 (24.7%) | |
| - 1a | 9 ( 5.8%) | 20 (14.0%) | 70 (14.1%) | 37 (16.6%) | |
| - 1b | 6 ( 3.8%) | 6 ( 4.2%) | 69 (13.9%) | 42 (18.8%) | |
| - 1c | 1 ( 0.6%) | 0 ( 0.0%) | 14 ( 2.8%) | 7 ( 3.1%) | |
| - 2a | 1 ( 0.6%) | 5 ( 3.5%) | 43 ( 8.7%) | 36 (16.1%) | |
| - 2b | 3 ( 1.9%) | 3 ( 2.1%) | 34 ( 6.9%) | 43 (19.3%) | |
| BRAF | 1 (14.3%) | 2 (40.0%) | 26 (49.1%) | 10 (30.3%) | 0.17 |
| MLH | 2 (66.7%) | 6 (100.0%) | 32 (91.4%) | 8 (80.0%) | 0.35 |
| Lynch syndrome | 4 (50.0%) | 3 (27.3%) | 16 (18.4%) | 5 (15.2%) | 0.14 |
Table 2.
Gender Differences in Colorectal Carcinoma.
| Gender | Female | Male | Total | p |
|---|---|---|---|---|
| (N=536)(52.7%) | (N=482)(47.3%) | (N=1018) | ||
| Marital status | <0.01 | |||
| - Divorced | 72 (13.4%) | 49 (10.2%) | 121 (11.9%) | |
| - Married | 238 (44.4%) | 286 (59.3%) | 524 (51.5%) | |
| - Other | 6 ( 1.1%) | 3 ( 0.6%) | 9 ( 0.9%) | |
| - Single | 120 (22.4%) | 116 (24.1%) | 236 (23.2%) | |
| - Widowed | 100 (18.7%) | 28 ( 5.8%) | 128 (12.6%) | |
| BMI | 25.0 [22.0;30.0] | 26.0 [23.0;30.0] | 26.0 [22.0;30.0] | 0.10 |
| MMRP | <0.01 | |||
| - Proficient | 329 (78.0%) | 307 (87.0%) | 636 (82.1%) | |
| - Deficient | 93 (22.0%) | 46 (13.0%) | 139 (17.9%) | |
| Faith (religious belief) | 369 (70.3%) | 269 (57.8%) | 638 (64.4%) | <0.01 |
| Patient's age (year) | 69.0 [56.0;79.0] | 67.0 [59.0;77.0] | 68.0 [58.0;78.0] | 0.55 |
| Tumor size (cm) | 4.0 [ 2.5; 5.7] | 4.1 [ 2.2; 5.5] | 4.0 [ 2.3; 5.6] | 0.75 |
| Histologic grade | 0.06 | |||
| - Grade 1 | 138 (25.7%) | 149 (30.9%) | 287 (28.2%) | |
| - Grade 2 | 336 (62.7%) | 294 (61.0%) | 630 (61.9%) | |
| - Grade 3 | 62 (11.6%) | 39 ( 8.1%) | 101 ( 9.9%) | |
| Tumor stage (TNM-T) | 0.65 | |||
| - 1 | 82 (15.3%) | 74 (15.4%) | 156 (15.3%) | |
| - 2 | 69 (12.9%) | 74 (15.4%) | 143 (14.0%) | |
| - 3 | 269 (50.2%) | 227 (47.1%) | 496 (48.7%) | |
| - 4 | 116 (21.6%) | 107 (22.2%) | 223 (21.9%) | |
| Nodal stage (TNM-N) | 0.59 | |||
| - No data | 10 ( 1.9%) | 16 ( 3.3%) | 26 ( 2.6%) | |
| - No nodal metastasis | 282 (52.6%) | 261 (54.1%) | 543 (53.3%) | |
| - 1a | 74 (13.8%) | 62 (12.9%) | 136 (13.4%) | |
| - 1b | 70 (13.1%) | 53 (11.0%) | 123 (12.1%) | |
| - 1c | 9 ( 1.7%) | 13 ( 2.7%) | 22 ( 2.2%) | |
| - 2a | 46 ( 8.6%) | 39 ( 8.1%) | 85 ( 8.3%) | |
| - 2b | 45 ( 8.4%) | 38 ( 7.9%) | 83 ( 8.2%) | |
Table 3.
Marital Status and Colorectal carcinoma.
| Marital Status | Divorced | Married | Other | Single | Widowed | p |
|---|---|---|---|---|---|---|
| (N=121) | (N=524) | (N=9) | (N=236) | (N=128) | ||
| BMI | 25.0 [22.0;31.0] | 26.0 [22.0;30.0] | 25.0 [21.0;27.0] | 25.0 [22.0;29.5] | 25.5 [22.0;30.0] | 0.77 |
| MMRP | <0.01 | |||||
| - Proficient | 67 (76.1%) | 347 (85.9%) | 6 (75.0%) | 155 (87.1%) | 61 (62.9%) | |
| - Deficient | 21 (23.9%) | 57 (14.1%) | 2 (25.0%) | 23 (12.9%) | 36 (37.1%) | |
| Faith (religious belief) | 68 (57.6%) | 346 (67.7%) | 2 (28.6%) | 126 (54.5%) | 96 (78.0%) | <0.01 |
| Sex (gender) | <0.01 | |||||
| - Female | 72 (59.5%) | 238 (45.4%) | 6 (66.7%) | 120 (50.8%) | 100 (78.1%) | |
| - Male | 49 (40.5%) | 286 (54.6%) | 3 (33.3%) | 116 (49.2%) | 28 (21.9%) | |
| Patient's age (year) | 66.0 [59.0;75.0] | 67.0 [56.5;76.0] | 77.0 [77.0;81.0] | 64.0 [54.0;73.0] | 84.0 [76.0;90.0] | <0.01 |
| Tumor size (cm) | 4.8 [ 3.3; 6.5] | 3.9 [ 2.1; 5.4] | 5.2 [ 3.5; 5.5] | 3.5 [ 2.0; 5.1] | 4.5 [ 3.3; 6.4] | <0.01 |
| Histologic grade | 0.56 | |||||
| - Grade 1 | 31 (25.6%) | 150 (28.6%) | 1 (11.1%) | 72 (30.5%) | 33 (25.8%) | |
| - Grade 2 | 77 (63.6%) | 325 (62.0%) | 6 (66.7%) | 145 (61.4%) | 77 (60.2%) | |
| - Grade 3 | 13 (10.7%) | 49 ( 9.4%) | 2 (22.2%) | 19 ( 8.1%) | 18 (14.1%) | |
| T stage (TNM-T) | <0.01 | |||||
| - 1 | 10 ( 8.3%) | 96 (18.3%) | 1 (11.1%) | 41 (17.4%) | 8 ( 6.2%) | |
| - 2 | 17 (14.0%) | 81 (15.5%) | 1 (11.1%) | 32 (13.6%) | 12 ( 9.4%) | |
| - 3 | 61 (50.4%) | 244 (46.6%) | 5 (55.6%) | 103 (43.6%) | 83 (64.8%) | |
| - 4 | 33 (27.3%) | 103 (19.7%) | 2 (22.2%) | 60 (25.4%) | 25 (19.5%) | |
| N stage (TNM-N) | 0.64 | |||||
| - No data | 4 ( 3.3%) | 15 ( 2.9%) | 0 ( 0.0%) | 5 ( 2.1%) | 2 ( 1.6%) | |
| - No nodal metastasis | 59 (48.8%) | 290 (55.3%) | 5 (55.6%) | 117 (49.6%) | 72 (56.2%) | |
| - 1a | 19 (15.7%) | 67 (12.8%) | 1 (11.1%) | 32 (13.6%) | 17 (13.3%) | |
| - 1b | 16 (13.2%) | 58 (11.1%) | 0 ( 0.0%) | 29 (12.3%) | 20 (15.6%) | |
| - 1c | 0 ( 0.0%) | 13 ( 2.5%) | 0 ( 0.0%) | 8 ( 3.4%) | 1 ( 0.8%) | |
| - 2a | 8 ( 6.6%) | 41 ( 7.8%) | 2 (22.2%) | 25 (10.6%) | 9 ( 7.0%) | |
| - 2b | 15 (12.4%) | 40 ( 7.6%) | 1 (11.1%) | 20 ( 8.5%) | 7 ( 5.5%) | |
| BRAF mutation | 5 (41.7%) | 15 (34.9%) | 0 ( 0.0%) | 6 (28.6%) | 13 (61.9%) | 0.17 |
| MLH gene methylation | 7 (77.8%) | 15 (83.3%) | 1 (100.0%) | 9 (90.0%) | 16 (100.0%) | 0.43 |
| Lynch syndrome | 4 (19.0%) | 17 (29.8%) | 0 ( 0.0%) | 5 (21.7%) | 2 ( 5.6%) | 0.07 |
Table 4.
CRC and MMRP Status (excluding Lynch syndrome).
| MMRP status | Proficient | Deficient | Total | p |
|---|---|---|---|---|
| (N=636) | (N=111) | (N=747) | ||
| Race /ethnicity | 0.04 | |||
| - Asian | 91 (14.3%) | 6 ( 5.4%) | 97 (13.0%) | |
| - Black | 25 ( 3.9%) | 3 ( 2.7%) | 28 ( 3.7%) | |
| - Hispanic | 121 (19.0%) | 17 (15.3%) | 138 (18.5%) | |
| - Other | 90 (14.2%) | 16 (14.4%) | 106 (14.2%) | |
| - White | 309 (48.6%) | 69 (62.2%) | 378 (50.6%) | |
| Marital status | <0.01 | |||
| - Divorced | 67 (10.5%) | 17 (15.3%) | 84 (11.2%) | |
| - Married | 347 (54.6%) | 40 (36.0%) | 387 (51.8%) | |
| - Other | 6 ( 0.9%) | 2 ( 1.8%) | 8 ( 1.1%) | |
| - Single | 155 (24.4%) | 18 (16.2%) | 173 (23.2%) | |
| - Widowed | 61 ( 9.6%) | 34 (30.6%) | 95 (12.7%) | |
| BMI | 26.0 [22.0;30.0] | 25.0 [22.0;28.5] | 26.0 [22.0;30.0] | 0.43 |
| Faith (religious belief) | 388 (62.7%) | 68 (63.6%) | 456 (62.8%) | 0.95 |
| Gender (sex) | <0.01 | |||
| - Female | 329 (51.7%) | 77 (69.4%) | 406 (54.4%) | |
| - Male | 307 (48.3%) | 34 (30.6%) | 341 (45.6%) | |
| Patient age (year) | 65.5 ± 14.0 | 74.3 ± 13.2 | 67.9 ± 14.2 | <0.01 |
| Anatomic site | <0.01 | |||
| - Right colon | 182 (28.7%) | 80 (72.0%) | 262 (35.1%) | |
| - Left colon | 54 (8.4%) | 6 (5.4%) | 60 (8.0%) | |
| - Sigmoid & Rectum | 364 (57.2%) | 9 (8.1%) | 373 (49.9%) | |
| - Transverse | 36 ( 5.7%) | 16 (14.4%) | 52 ( 7.0%) | |
| Tumor size (cm) | 4.0 [ 2.5; 5.5] | 6.0 [ 4.5; 7.5] | 4.0 [ 2.3; 5.5] | <0.01 |
| Histologic grade | <0.01 | |||
| - Grade 1 | 180 (28.3%) | 17 (15.3%) | 197 (26.4%) | |
| - Grade 2 | 411 (64.6%) | 60 (54.1%) | 471 (63.1%) | |
| - Grade 3 | 45 ( 7.1%) | 34 (30.6%) | 79 (10.6%) | |
| Tumor stage (TNM-T) | <0.01 | |||
| - 1 | 83 (13.1%) | 4 ( 3.6%) | 87 (11.6%) | |
| - 2 | 97 (15.3%) | 8 ( 7.2%) | 105 (14.1%) | |
| - 3 | 309 (48.6%) | 71 (64.0%) | 380 (50.9%) | |
| - 4 | 147 (23.1%) | 28 (25.2%) | 175 (23.4%) | |
| Nodal stage (TNM-N) | 0.01 | |||
| No data | 12 ( 1.9%) | 0 ( 0.0%) | 12 ( 1.6%) | |
| N0 | 304 (47.8%) | 68 (61.3%) | 372 (49.8%) | |
| - 1a | 107 (16.8%) | 6 ( 5.4%) | 113 (15.1%) | |
| - 1b | 76 (11.9%) | 18 (16.2%) | 94 (12.6%) | |
| - 1c | 14 ( 2.2%) | 2 ( 1.8%) | 16 ( 2.1%) | |
| - 2a | 60 ( 9.4%) | 7 ( 6.3%) | 67 ( 9.0%) | |
| - 2b | 63 ( 9.9%) | 10 ( 9.0%) | 73 ( 9.8%) | |
| BRAF | 7 (14.9%) | 32 (65.3%) | 39 (40.6%) | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



