
Submitted:
19 July 2024
Posted:
22 July 2024
You are already at the latest version
Abstract
The aim of the current study has been to assess externalizing problems from a gender perspective in the juvenile population. This objective has been evaluated though the Child and Adolescent Assessment System questionnaire (SENA), to measure the dimension of externalized problems. A total of 128 Spanish students took part in the survey, comprising 58 (45.3%) male and 67 (52.3%) female, aged between 12 and 16 years old (M= 13,7; Sd= 1,14). The sample was taken from three High- Schools (state and private-subsidized) in Madrid, Spain. The research for this study was conducted through a descriptive, inferential, quantitative, ex post facto design. The data analysis was performed using SPSS 27.0. The result revealed an increase in externalized problems: Attention (M= 2.65, Sd=.88), Anger Control (M= 2.27, Sd=.85) and Hyperactivity- Impulsivity (M= 2.26, Sd=.68). In addition, female students score highly in Attention Problems (F= 4.124; Sig.: .004), Hyperactivity-Impulsivity (F: 6.18; Sig.: <.001), and Anger Control (F: 2.3; Sig.: .062). This study highlights the impact and increase on students externalized mental health problems currently. It is essential to have a protective environment and promote the development of emotional intelligence, encouraging the mental health in young people. This article is part of the findings of the research project “Therapeutic Innovation Classroom for the accompaniment of teenager with Serious Mental Disorder” (Reference: 2021V/EU-UNED/02).
Keywords:
externalized disorders
; gender
; adolescent
1. Introduction
Adolescence is a critical period in their biopsychosocial development. During this stage biological, psychological and social changes are key to the development of important social and emotional skills for mental wellbeing, and it is important to have positive and protective environments. However, multiple risk factors make adolescents vulnerable to certain mental health problems, for example, leading an unhealthy lifestyle [1], technological dependency, the addictive of the Internet, video games and social networks [5], poverty and inequality or violence [9].
In the study of [6], between 15% and 30% of adolescents worldwide have a mental disorder. Among the main symptoms are depression, anxiety and behavioural disorders, with suicide being the fourth leading cause of death among young people. According to Estevez et al. [8], the suicidal attempts rate is increasing more frequently during adolescence, and this trend is increasing. By gender, girls score higher than boys on internalisation problems. Following the study [3], girls reported a higher presence of mental health problems in terms of anxiety, and symptoms of depression and stress. However, men exhibited more dissocial behaviour than women [12,13]. Regarding suicidal ideation, female group presented higher suicidal ideation rates in the early years of adolescence than the male group [5]. Findings pointed that the gender gap in mental health in adolescence is largely ubiquitous cross-culturally, with girls having worse average mental health [4]
Adolescents with mental health issues usually present disorders classified as externalizing and internalizing, with the symptoms being quite different from each other, but in both there is an emotional and behavioural problem. Externalizing factors refer to those where behavioural problems, inattention or impulsivity appear, that is, those problems that are disruptive and usually cause annoyance to third parties and produce alterations in the family, school and social environment [8]. In this article, we will focus on externalized problems, disruptive behaviours, such as hyperactivity and impulsivity, attention problems, aggressiveness, defiant behaviour, anger control problems, antisocial behaviour. The diagnosis and treatment of these behaviours can be complex due to the different biological and environmental factors involved, and comorbidity is frequent and unnoticed [10,11,12,13,14,15].
Behavioral disorders occur more frequently among young adolescents than among older adolescents. Following [9], impulsivity is a construct made up of four different factors (impulsivity, risk-taking, the ability to improvise without planning and vitality) and states that high levels of impulsivity are linked to psychiatric disorders. In addition, impulsivity is associated with poorer emotional regulation, deficits in social skills, decision-making, and problem-solving, as well as poorer stress management. Attention deficit hyperactivity disorder is neurobiologically based, characterized by the symptomatic triad of difficulty paying attention, excessive activity, and behaviours in which consequences are not considered [12]. In addition, they vary during development, modifying frequency and intensity depending on age and sex [13]. Regarding the factors of impulsivity in adolescents, it may be due to alcohol, adventures, depression that includes a range of impulse so that young people can throw without measuring the risk, imposition and immediacy in which they do it [16].
In addition, adolescents are increasingly engaging in risky behaviours at a younger age, putting their physical and mental well-being at risk. Aggressive behaviour is defined as the tendency to harm, destroy, contradict, humiliate, among other actions that lead to the affectation of the integrity of a person, oneself or an object [17,18]. Regarding the onset of aggressive behaviour, some studies point to its presence around childhood, demarcating an exacerbation towards adolescence [19,20,21], even more so when there is a history of violence within its context of development [22,23] and, with a lower academic level [24]. The problematic use of technologies indicates experiences of cyberbullying, highlighting among the most common forms insults, threats and denigrations, and as applications WhatsApp and social networks [25]. Adolescents who struggle to perceive, express, and regulate their emotions are more likely to become victims of cyberbullying [11]. According to Marco et al. [26], aggressiveness influences coping mechanisms for problem-solving and emotion management (emotional instability and empathy).
Following the DSM-5, Oppositional Defiant Disorder (ODD), is a type of childhood disruptive behaviour disorder. The main feature of ODD is a persistent pattern of angry or irritable mood, along with a susceptible attitude, defiant behaviour with challenging authority figures or norms, blaming others for their bad behaviour. Challenging behaviour tends to increase during adolescence for people with developmental disabilities [27]. In relation to the school environment, inclusion in relation to challenging behaviour is one of the most demanding challenges for teachers [28].
As for anger management problems, anger is the most primitive defense mechanism, determining its maladaptive nature is a complex phenomenon. Therefore, the concept of anger lacks clarity as to its definition, demarcation of aggression and hostility, and also its evaluation. The manifestation of anger occurs at the behavioural, verbal, and mental levels [29]. Following Yang et al. [30] studies on anger through perceived threat, high sensitivity to punishment and reward may put adolescents at risk of developing anger (comorbid) problems through increased threat and perceptions of non-reward.
Finally, consulting the ICD-10, severe Dissocial personality Disorder, characterized by aggressive behaviour towards people or animals, theft, fraud or destruction of objects, and running away from home and/or school. The prevalence of dissocial disorder, with the symptomatology of destructive or defiant behaviour, is 3.6% of adolescents aged 1014 years and 2.4% of those aged 15-19 years [31].
Therefore, it is now imperative to address adolescent mental health. From the Faculty of Education of the National Distance University, the research project “Therapeutic Innovation Classroom for the accompaniment of teenager with Serious Mental Disorder” (Reference: 2021V/EU-UNED/02) is being developed, with the aim of creating a specific classroom for therapeutic care for the permanence of students with mental disorders in the educational system. This article presents the results achieved in terms of externalized disorders from a gender perspective in adolescents.
2. Materials and Methods
Methods
A descriptive, inferential, quantitative, ex post facto design was carried out in this research.
The purpose of this study was to analyse externalising disorders from a gender perspective in the juvenile population. These include hyperactivity and impulsivity, attention problems, aggression, defiant behaviour, anger management problems and antisocial behaviour. To achieve this objective, existing differences between gender (boys and girls) was analysed in the different items through descriptive analyses, correlations, and statistical Student’s t test.
Participants
Madrid County has 3,656 High-schools, the sample has been collected in three High- Schools (state and private-subsidized) in Madrid, Spain. The sample was select through non-probabilistic sampling. A total of N = 128 subjects (male group N = 58 (45.3%) and female group N = 67 (52.3%)) took part in the survey with a range of ages between 12 and 16 years old (M = 13.7; Dt = 1.14). The students in the first year and third year of Compulsory Secondary Education [Key Stage 3 (Year 7 to Year 9); Key Stage 4 (Year 10 and Year 11)] have been selected (Table 1 and Table 2), considering that the first year of secondary education is a particularly sensitive course for emotional disturbance [27] and the third year of secondary education with the intention of having a higher age range. Finally, the socio-economic reality of the spaces in which the three institutes are located are similar in terms of socio-demographic characteristics, the absolute unemployment rate and gross income per capita [28], so we have had a homogeneous socio-economic framework.
Instrument
The questionnaire used to assess psychopathology in adolescents was the Child and Adolescent Assessment System [29] (SENA). Specifically, we have applied the SENA Secondary-School questionnaire (12-18 years old), using self-reports completed in online format. This instrument assesses through three main areas (emotional and behavioral problems, vulnerability, and protective psychological resources), through 4 scales, with differentiated blocks and with a 5-choice Likert scale response format (from Never or Almost Never to Always or Almost Always), and the scores are expressed in T-scores (M=50, Dt=10). This allows us to have a dimensional and quantitative approach that considers the problems of each subject as part of a continuum, indicating the different degrees of the continuum between normality and psychopathology. As for the scales of this self-report, they include:
- -
- Three control scales to assess possible response biases (inconsistency, negative impression, and positive impression)
- -
- Scales of emotional and behavioural problems, divided into four different blocks:
- -
- Internalized, predominantly emotional problems, such as depression, anxiety, social anxiety, somatic complaints, obsession-compulsion, and post-traumatic symptomatology.
- -
- Externalized problems, disruptive behaviours, such as hyperactivity and impulsivity, attention deficit, aggressiveness, defiant behaviour, anger management problem, antisocial behaviour.
- -
- Contextual problems (problems with family, problems with school, and problems with peers).
- -
- Specific problems (developmental delay, eating disorders, learning disabilities, schizophrenia, substance use, ...)
- -
- Vulnerability scales that evaluate a more severe problem, such as emotional regulation problems and sensation seeking.
- -
- Scales of protective psychological resources in the face of different problems, such as: self-esteem, integration and social competence and awareness of problems.
This instrument also provides information through a system of critical items that alerts the examiner to the presence of problematic aspects of relevance. And up to six global indices that summarize the scores obtained on the different scales.
The SENA questionnaire has an internal consistency using Cronbach’s alpha of 0.86 on all the scales mentioned above.
Data Collection
For data collection, permission was requested from the Center, parents and participants, following the ethical standards for the development of research with students [34]
Statistical Procedure
Statistical data analysis has been carried out using the IBM Statistical Package Program software for Social Sciences (SPSS) version 27.
3. Results
For the analysis of the results, the Externalized Problems block was analysed. The students reported levels of hyperactivity-impulsivity (29.2%), attention deficit (23.6%), and anger management problem (22.1%). The descriptive statistics of the students’ externalized problems are shown in Table 3, the students reported symptoms of attention deficit N=128 (M= 2.65, Sd=.88), anger management problem N=128 (M= 2.27, Sd=.85) and hyperactivity-impulsivity N=128 (M= 2.26, Sd=.68).
In Figure 1, the frequency of externalized problems according to gender is shown. The female group reported a higher presence of hyperactivity-impulsivity (30.2%) and anger management problem (27.4%). The male group reported a higher presence of attention Deficit (28.1%) and hyperactivity-impulsivity (28.1%).
3.1. Externalized Problem - Attention Deficit
In Figure 2, the distribution of the students’ attention deficit N=128 (M= 2.65, Sd=.88) is shown.
In the correlation analysis, attention deficit showed a significant correlation with hyperactivity and impulsivity problems (r=.711, Sig.=<.001); anger management problems (r=.480, Sig.=<.001), aggression (r=.331, Sig.=<.001), defiant behaviour (r=.418, Sig.=<.001) and antisocial behaviour (r=.307, Sig.=<.001).
In Figure 3, the distribution of attention deficit according to gender is shown. Female group reported N= 67 (M=2.79, Sd=.9) and male group N=58 (M=2.46, Sd=.75). The female group had an Md= 2.9 (Q1=2.1, Q3=3.5), with an interquartile range=1.4. The male group has an Md= 2.45 (Q1=1.8, Q3=3), with an interquartile range = 1.2.
3.2. Externalized Problem - Hyperactivity- Impulsivity
In Figure 4, the distribution of the students’ hyperactivity-impulsivity N=128 (M= 2.26, Sd=.68) is shown.
In the correlation analysis, hyperactivity-impulsivity problems showed a significant correlation with aggression (r=.368, Sig.=<.001), anger management problem (r=.545, Sig.=<.001), defiant behaviour (r=.37, Sig.=<.001) and antisocial behaviour (r=.308, sig.=<.001).
In Figure 5, the distribution of hyperactivity-impulsivity issues according to gender is shown. The female group N= 67 (M=2.47, Sd= .7) and the male group N=58 (M=2, Sd= .52). The female group had an Md= 2.5 (Q1=1.9, Q3=2.9), with an interquartile range = 1.1. The male group has an Md= 1.9 (Q1=1.6, Q3=2.2), with an interquartile range = .6.
3.3. Externalized Problem - Aggression
The distribution of externalized students’ problem aggression was analysed N=128 (M= 1.4, Sd=.45). In the correlation analysis, aggression problem showed a statistically significant correlation with anger management problem (r=.481, Sig.=<.001); defiant behaviour (r=.48, Sig.=<,001) and antisocial behaviour (r=.6, Sig.=<.001).
In Figure 6, the distribution of aggression problem according to gender is shown. The female group had N = 67 (M = 1.42, Sd = .47) and male group had N = 58 (M = 2.8, Sd = .42). The female and male groups have an Md=1.3 (Q1=1, Q3=1.6), with an interquartile range=.5.
3.4. Externalized Problem 4- Defiant Behaviour
The distribution of externalized students’ defiant behaviour problem was analysed N=128 (M= 1.63, Sd=.67). In the correlation analysis students’ problem defiant behaviour showed a statistically significant correlation with anger management problems (r=.604, Sig.= <.001) and antisocial behaviour (r=.427, Sig.= <.001).
In Figure 7, the distribution of defiant behavior according to gender is shown. The female group N= 67 (M=1.65, Sd= .73) and male group N=58 (M=1.59, Sd= .61). Female group and male group have an Md=1.3 (Q1=1, Q3=2), with an interquartile range=1.
3.5. Externalized Problem - Antisocial Behaviour
The distribution of externalized students’ antisocial behaviour was analysed N=128 (M= 1.2, Sd=.41). In the correlation analysis students’ problem antisocial behaviour has a significant correlation with anger management problems (r=.362, Sig.=<.001); and defiant behaviour (r=.427, Sig.=<.001)
In Figure 8, the distribution of antisocial behavior according to gender is shown. The female group N= 67 (M=1.23, Sd= .44) and male group N=58 (M=1.3, Sd= .38). Female group has a Md=1.1 (Q1=1, Q3=1.4) and male group has Md=1.2 (Q1=1, Q3=1.425), both with an interquartile range=.4.
3.6. Externalized Problem - Anger Management Problem
In relation to the externalized students’ problem anger management problem N=128 (M= 2.27, Sd=.84). In Figure 9, the distribution of anger management problem according to gender is shown. The female group N = 67 (M = 2.42, Sd = .84) and male group N = 58 (M = 2.06, Sd = .82). Female group has a Md=2.4 (Q1=1.8, Q3=3), with an interquartile range=1.2; and male group has Md=1.8 (Q1=1.5, Q3=2.43), with an interquartile range=.9.
4. Discussion
The results confirm that externalising problems have increased in adolescents. On one hand, our results indicate that there are statistically significant differences externalized problems according to gender. On the other hand, the need for stronger evidence warrants additional research with larger sample size that focus on larger interventions, combining contextual factors taking into account the impact of internalizing disorders to provide better support in schools.
In relation to the gender variable, there are statistically significant differences between females and males in externalizing problems. The female group reported a higher presence of attention and hyperactivity-impulsivity externalized problems. This result is consistent across the studies analyzed [36], in which a higher score predominates for women (21%) in impulsivity and emotional clarity and repair. Moreover, in the study [37], female gender stands out in the variables anguish, constancy and sensation seeking. In addition, in the study [34], learning and executive function problems were more frequent in female group with hyperactive and combined subtype. Moreover, the female group scored higher on suicidal risk. In regard to this, the literature reviewed [39], they show a greater tendency to act impulsively in women (26%) than men (15%), identifying that impulsivity is linked to depression, resulting in a higher risk of suicidal ideation.
Regarding to the hyperactivity-impulsivity variable, which is characterized by excessive mental and physical restlessness and difficulties in controlling the mind, among others, it is considered a risk factor for antisocial behaviour [41], this requires a push in emotional learning as required skill in schools.
In the present study, the main limitation was a convenience sample was used, not allowing the results to be extrapolated. In the future, should consider diverse geographical and cultural backgrounds involving high schools from different countries. Secondly, self-report measures on a Likert scale may vary in reliability depending on age, potentially affecting the accuracy of responses. In the future, should consider conducting pilot tests of the questionnaire with different age groups.
In spite of the above limitations, results showed a significant relationship in the externalizing problems, behaviour and gender, whose significance could be, verified in future explorations of the impact of these disorders in childhood and adolescence. In this way, information on the impact of these factors on behaviour could be obtained.
5. Conclusions
In conclusion, adolescence is a crucial period for the development of social and emotional habits important for mental well-being. The aim of the present study was to assess externalizing problems from a gender perspective in the adolescent’s population. This study highlights that there is an increase in adolescents’ externalized problem in hyperactivity-impulsivity, attention problems and anger management problem. Currently, it has been seen that emotional instability is positively related to unproductive coping and this to aggressiveness [37].
Therefore, it is essential to develop students’ emotional skills to promote their mental health. Emotional intelligence is the ability to interact with the world, which includes maintain interpersonal relationships, face difficult situations, solve problems, and learn to manage emotions. So, it is crucial to promote emotional programs to support students’ social emotional skills and development, strengthening their ability to recognize and manage their emotions, encourage choices regarding risk behaviors, manage difficult or adverse situations, and promote favorable environments and social networks [38]. These programmes require a multidisciplinary approach, from the family, health care, schools and community.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, F.C., E.M, and C.S.; methodology, F.C., E.M, and C.S; software, C.S and F.C; validation, E.M, C.S. and F.C.; formal analysis, E.M.; investigation, C.S.; resources, F.C.; data curation CS writing—original draft preparation, C.S.; writing—review and editing, C.S, E.M. and FC; visualization, F.C.; supervision, C.S and F.C; project administration, C.S.; funding acquisition, C.S. All authors have read and agreed to the published version of the manuscript.”.
Funding
This research is part of the UNED 2021 “Europe Research” project: “Therapeutic Innovation Classroom for the accompaniment of teenager with Serious Mental Disorder”. Reference: 2021V/EU-UNED/02. Funded by the UNED. Call for grants for the implementation of “Europe Research” projects UNED 2021.
Institutional Review Board Statement
Ethical review and approval was waived for this study because the data are exclusively part of the project “Therapeutic Innovation Classroom for the accompaniment of adolescents with Serious Mental Disorder” (Reference: 2021V/EU-UNED/02) and informed consent has been previously requested from the institutions. The data are in the custody of the Principal Investigator (PI) - UNED and have been used for this document anonymously.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Maintaining the anonymity of both educational centers and students.
Data Availability Statement
The data is in the database of the project owned by Principal Investigator (PI) - UNED.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Alaka Mani, T.L.; Sharma, M.K.; Omkar, S.N.; Nagendra, H.R. Holistic assessment of anger in adolescents–Development of a rating scale. Journal of Ayurveda and Integrative Medicine 2018, 9, 195–200. [Google Scholar] [CrossRef] [PubMed]
- David, M.; Mason, R.A.; Davis, J.L.; Gregori, E.; Lei, Q.; Lory, C.; Wang, D. School-Based Interventions Targeting Challenging Behavior of Adolescents with Developmental Disabilities: A Meta-Analysis. Journal of Developmental and Physical Disabilities 2023, 35, 17–46. [Google Scholar] [CrossRef]
- Caamaño-Navarrete, F.; Del-Cuerpo, I.; Arriagada-Hernández, C.; Alvarez, C.; Gaya, A.R.; Reuter, C.P.; Delgado-Floody, P. Association between Active Commuting and Lifestyle Parameters with Mental Health Problems in Chilean Children and Adolescent. Behav. Sci. 2024, 14, 554. [Google Scholar] [CrossRef]
- Campbell, O.L.K.; Bann, D.; Patalay, P. The gender gap in adolescent mental health: A cross-national investigation of 566,829 adolescents across 73 countries. SSM - Population Health 2021, 13, 100742. [Google Scholar] [CrossRef]
- Cuadra, A.; Veloso, C.; Vega, G.; Zepeda, A. Ideación Suicida Y relación con la Salud Mental en Adolescentes Escolarizados no Consultantes. Redalyc 2021, 46, 217–223. [Google Scholar]
- Eddy, L.S. Behavioral disorders. Journal of Continuing Education of the Spanish Society of Adolescent Medicine 2020, VIII. [Google Scholar]
- Eysenk, S.B.; Eysenk, H.J. The place of impulsiveness in a dimensional system of personality description. Br J Soc Clin Psychol 1977, 16, 57–68. [Google Scholar] [CrossRef] [PubMed]
- Estevez, E.; Emler, N.P.; Cava, M.J.; Inglés, C.J. Ajuste psicosocial en adolescentes populares agresivos y rechazados agresivos en el colegio. Psychosocial Adjustment in Aggressive Popular and Aggressive Rejected Adolescents at School. Psychosocial Intervention 2014, 23, 57–67. [Google Scholar] [CrossRef]
- Fernández, M.; Fernández Parra, A. Behavioral problems, emotional problems, and care problems in children and adolescents living in residential care. Psychology 2017, 11, 57–70. [Google Scholar]
- Gallardo-Saavedra, G.A.; Martínez-Wbaldo, M.d.C.; Padrón-García, A.L. Prevalence of ADHD in Mexican schoolchildren through screening with the Conners 3 scales. Actas Esp Psiquiatr 2019, 47, 45–53. [Google Scholar]
- Garcia, L.; Quintana, O.C.; Rey, L. Cybervictimization and life satisfaction in adolescents: Emotional intelligence as a mediating variable. Journal of Clinical Psychology with Children and Adolescents 2020, 7, 38–45. [Google Scholar]
- Kreuze, L.J.; de Jong, P.J.; Bennik, E.C.; Nauta, M.H. Anger Responses in Adolescents: Relationship with Punishment and Reward Sensitivity. Child Psychiatry and Human Development 2022, 53, 1174–1185. [Google Scholar] [CrossRef] [PubMed]
- Øen, K.; Johan Krumsvik, R. Teachers’ attitudes to inclusion regarding challenging behaviour. European Journal of Special Needs Education 2022, 37, 417–431. [Google Scholar] [CrossRef]
- Martin, J.; Hadwin, J.A. The roles of sex and gender in child and adolescent mental health. JCPP Advances 2022, 2, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Mateu, A.; Pascual, A.; Martínez, M.; Hickey, N.; Nicholls, D.; Kramer, T.; Schäfer, M. Salud mental en adolescentes víctimas y/o agresores de ciberbullying. Revista de Psicopatología y Salud Mental Del Niño y Del Adolescente 2021, 33, 43–58. [Google Scholar]
- Merchán Clavellino, A.; Martínez García, C.; Medina Mesa, Y.; Cruces Montes, S.J. Predictive model of emotional intelligence and impulsivity traits in sensation-seeking in young university students: A gender comparison. International Journal of Developmental and Educational Psychology: INFAD. Journal of Psychology 2019, 5, 291–300. [Google Scholar]
- Paredes, I.M.C.; Patiño, G.L.A. Health risk behaviors in adolescents. University and Health 2020, 22, 58–69. [Google Scholar]
- Ramírez, C.; Arcila, W. Violence, conflict and aggressiveness in the school setting. Education and Educator 2013, 16, 411–429. [Google Scholar] [CrossRef]
- Ramos Brieva, A.; Ramón y Cajal, G.-Z. Impulse Control Scale. Bank of Mental Health Instruments and Methodologies. 2002. [Google Scholar]
- Romero, E.; Gómez, F.X.A.; Villar, P.; Rodríguez, R. Indicated prevention of behavioral problems: Training of social-emotional skills in the school context. Journal of Clinical Psychology with Children and Adolescents 2019, 6, 39–47. [Google Scholar]
- Tabares, A.; Núñez, C.; Osorio, M.P.; Aguirre, A. Risk and Suicidal Ideation and its Relationship with Impulsivity and Depression in School-Age Adolescents. Ibero-American Journal of Diagnosis and Psychological Evaluation 2020, 54, 147–163. [Google Scholar]
- Vidal, A.; Matamala, M. Child and adolescent asthma and psychiatric disorders. Chilean Journal of Respiratory Diseases 2013, 29, 14–23. [Google Scholar]
- World Health Organization. Adolescent Mental Health; WHO: Geneva, 2021. [Google Scholar]
- Gámez, G.M.; Almendros, C.; Rodríguez, M.L.; Mateos, P.E. Online self-harm among Spanish adolescents: Analysis of prevalence and motivations. Journal of Clinical Psychology with Children and Adolescents 2020, 7, 9–15. [Google Scholar]
- Martinez, J. Child Development: A Review. Revista investigaciones Andina 2014, 29, 1118–1137. [Google Scholar]
- Marco, S.S.; Mayoral, A.M.; Valencia, A.F.; Roldán, D.L.; Espliego, F.A.; Delgado, L.C.; Hervás, T.G. Family Functioning in Adolescents at Risk for Suicide with Suicidal Traits. Revista de Psicología Clínica con Niños y Adolescentes 2020, 7, 50–55. [Google Scholar]
- Mestre, V.; Samper, P.; Tur-Porcar, A.M. Aggression in Adolescence. Univesrsitas Psychologica 2012, 11, 1263–1275. [Google Scholar]
- Patrón, R.; Limiñana, R.M. Victims of Family Violence: Psychological Consequences in Children of Abused Mothers. Annals of Psychology 2005, 21, 11–17. [Google Scholar]
- Hojjat, S.K.; Rezaei, M.; Namadian, G.; Hatami, S.E.; Norozi Khalili, M. Effectiveness of Emotional Intelligence Group Training on Anger in Adolescents with Substance-Abusing Fathers. Journal of Child and Adolescent Substance Abuse 2017, 26, 24–29. [Google Scholar] [CrossRef]
- Yang, J.; Li, W.; Gao, L.; Wang, X. How is Trait Anger Related to Adolescents’ Cyberbullying Perpetration? A Moderated Mediation Analysis. Journal of Interpersonal Violence 2022, 37, 9–10. [Google Scholar] [CrossRef]
- Institute of Health Metrics and Evaluation Global Health Data Exchange 2021.
- Crespo, F.; Sánchez, C. Impacto del Trastorno Mental Grave en el ámbito educativo de niños y adolescentes. Revista Complutense de Educación 2019, 30, 205–223. [Google Scholar] [CrossRef]
- Directorate-General for Territorial Coordination and Deconcentration. Informe de Progreso 2022. 2022.
- Férnandez- Pinto, I.; Santamaría, P.; Sánchez-Sánchez, F.; Carrasco-Ortiz, M.A.; del Barrio-Gándara, V. SENA: Sistema de Evaluación de Niños y Adolescentes-Manual Técnico. TEA. 2015.
- Council of International Organizations. Pautas éticas internacionales para la investigación relacionada con la salud con seres humanos. Consejo de Organizaciones Internacionales de las Ciencias Médicas (CIOMS) en colaboración con la Organización Mundial de la Salud. 2022.
- Merchán Clavellino, A.; Martínez García, C.; Medina Mesa, Y.; Cruces Montes, S.J. Modelo predictivo de la inteligencia emocional y rasgos de impulsividad en la búsqueda de sensaciones en jóvenes universitarios: Una comparación de género. International Journal of Developmental and Educational Psychology: INFAD. Revista de Psicología 2019, 5, 291–300. [Google Scholar] [CrossRef]
- Herdoiza-Arroyo, P.; Chóliz, M. Impulsividad en la Adolescencia: Utilización de una Versión Breve del Cuestionario UPPS en una Muestra de Jóvenes Latinoamericanos y Españoles. Revista Iberoamericana de Diagnóstico y Evaluación - e Avaliação Psicológica 2019, 1, 123–135. [Google Scholar] [CrossRef]
- Gallardo-Saavedra, G.A.; Martínez-Wbaldo, M.d.C.; Padrón-García, A.L. Prevalencia de TDAH en escolares mexicanos a través de un cribado con las escalas de Conners 3. Actas Esp Psiquiatr 2019, 47, 45–53. [Google Scholar] [PubMed]
- Tabares, A.; Núñez, C.; Osorio, M.P.; Aguirre, A. Riesgo e Ideación Suicida y su Relación con la Impulsividad y la Depresión en Adolescentes Escolares. Revista Iberoamericana de Diagnóstico y Evaluacion Psicologica 2020, 54, 147–163. [Google Scholar]
- Yang, J.; Li, W.; Gao, L.; Wang, X. How is Trait Anger Related to Adolescents’ Cyberbullying Perpetration? A Moderated Mediation Analysis. Journal of Interpersonal Violence 2022, 37, 9–10. [Google Scholar] [CrossRef]
- Patterson, G.R.; DeGarmo, D.S.; Knutson, N. Hyperactive and antisocial behaviors: Comorbid or two points in the same process? Development and Psychopathology 2000, 12, 91–106. [Google Scholar] [CrossRef]
Figure 1.
Distribution students’ externalised problems.
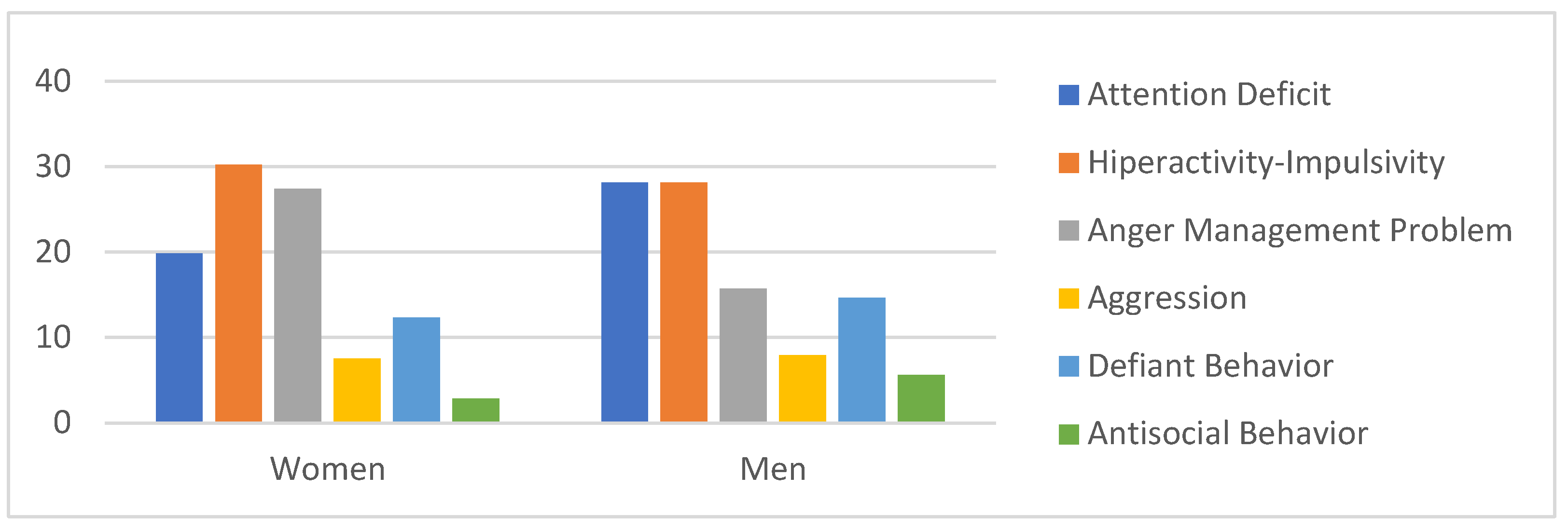
Figure 2.
Distribution students’ attention deficit.
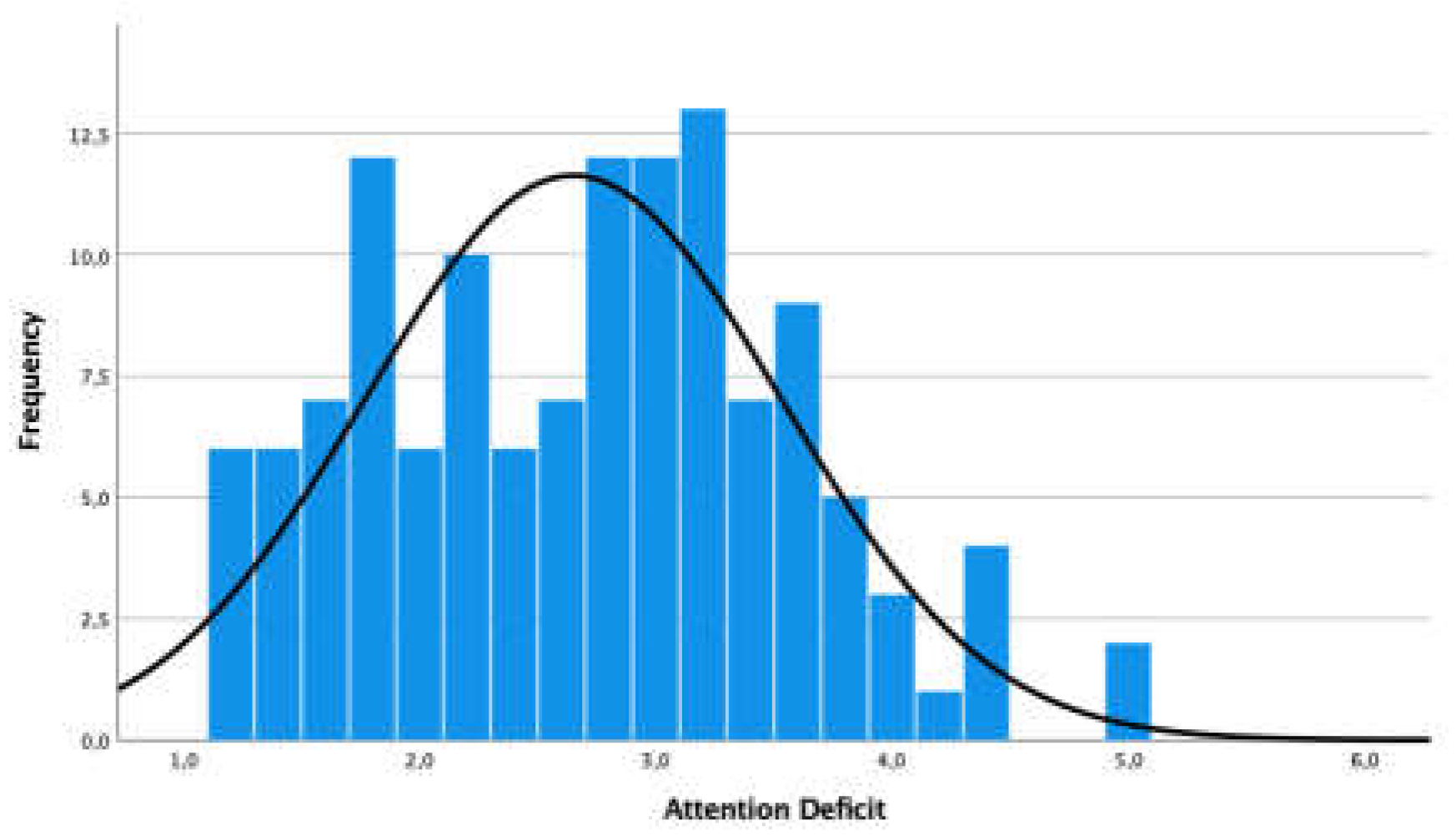
Figure 3.
Gender distribution attention deficit.
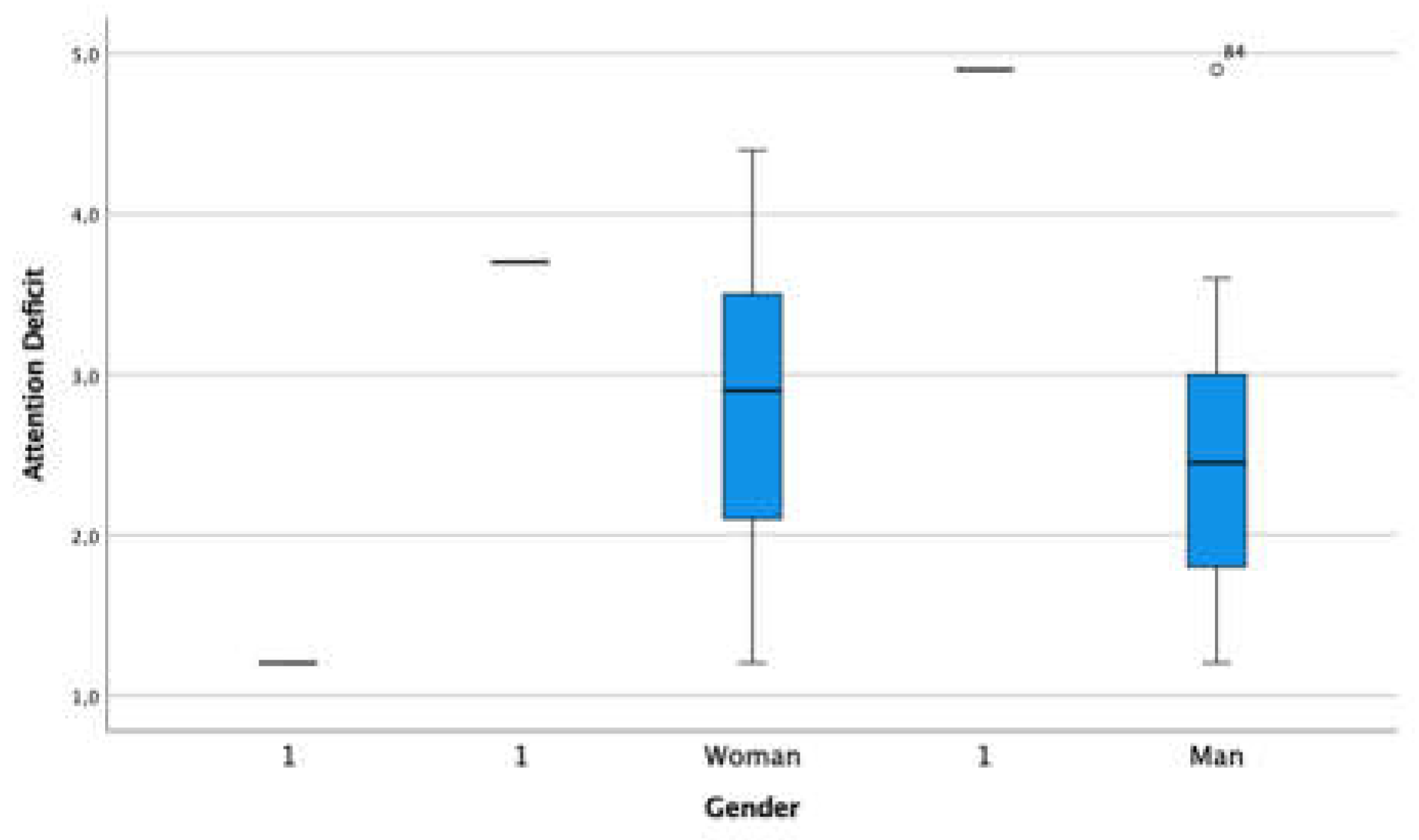
Figure 4.
Distribution student’s hyperactivity-impulsivity.
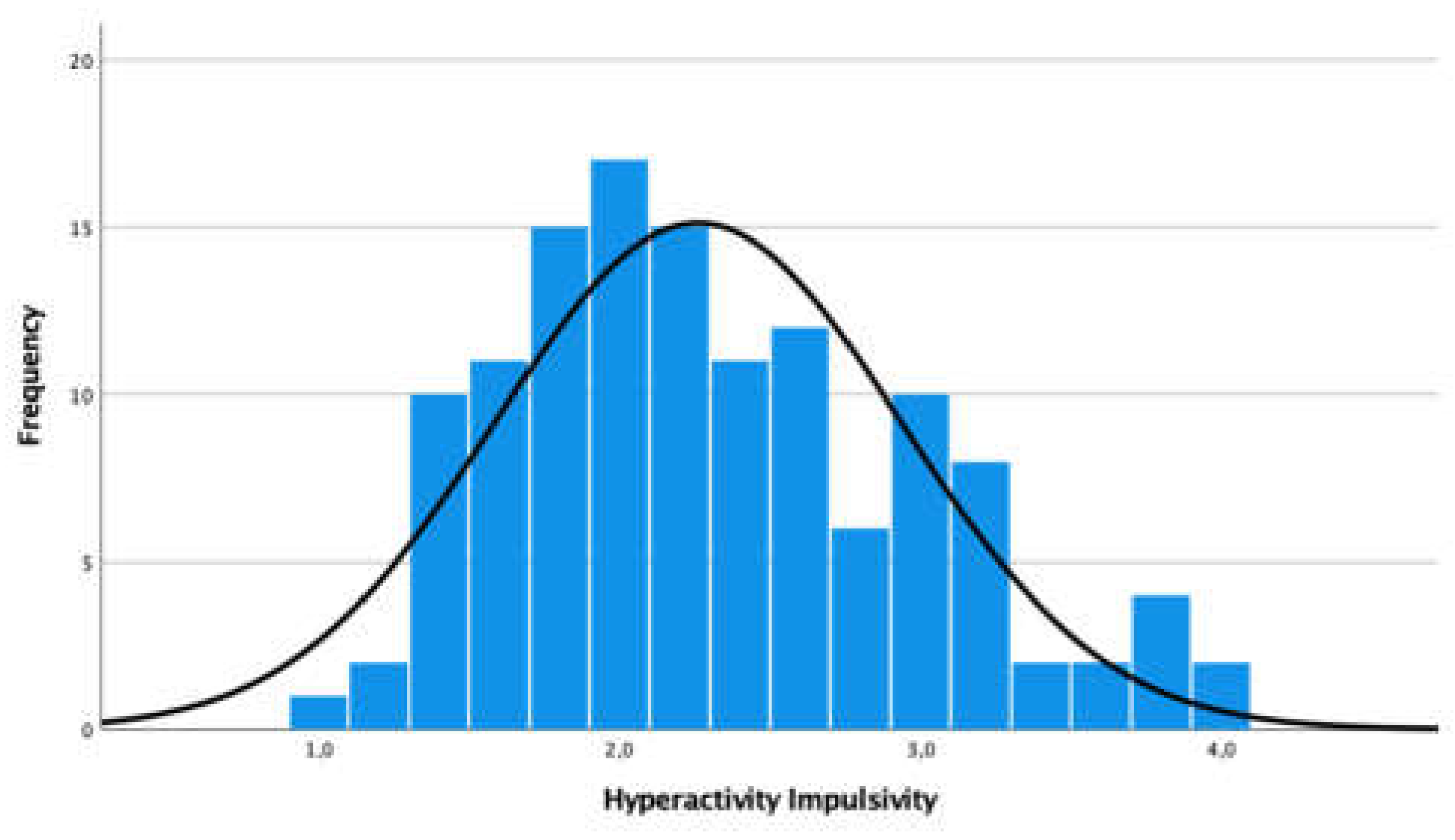
Figure 5.
Gender distribution hyperactivity impulsivity.
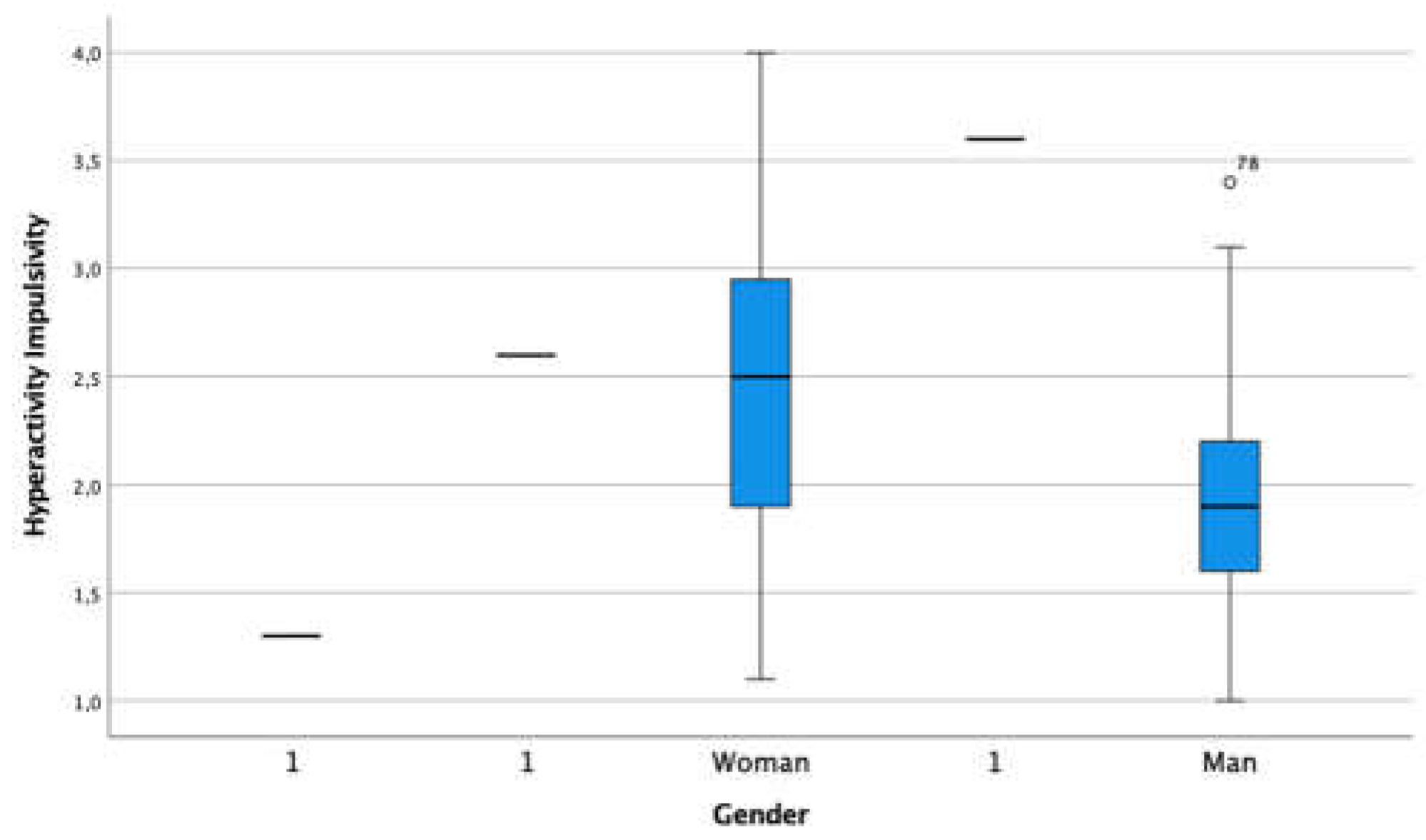
Figure 6.
Gender distribution aggression.
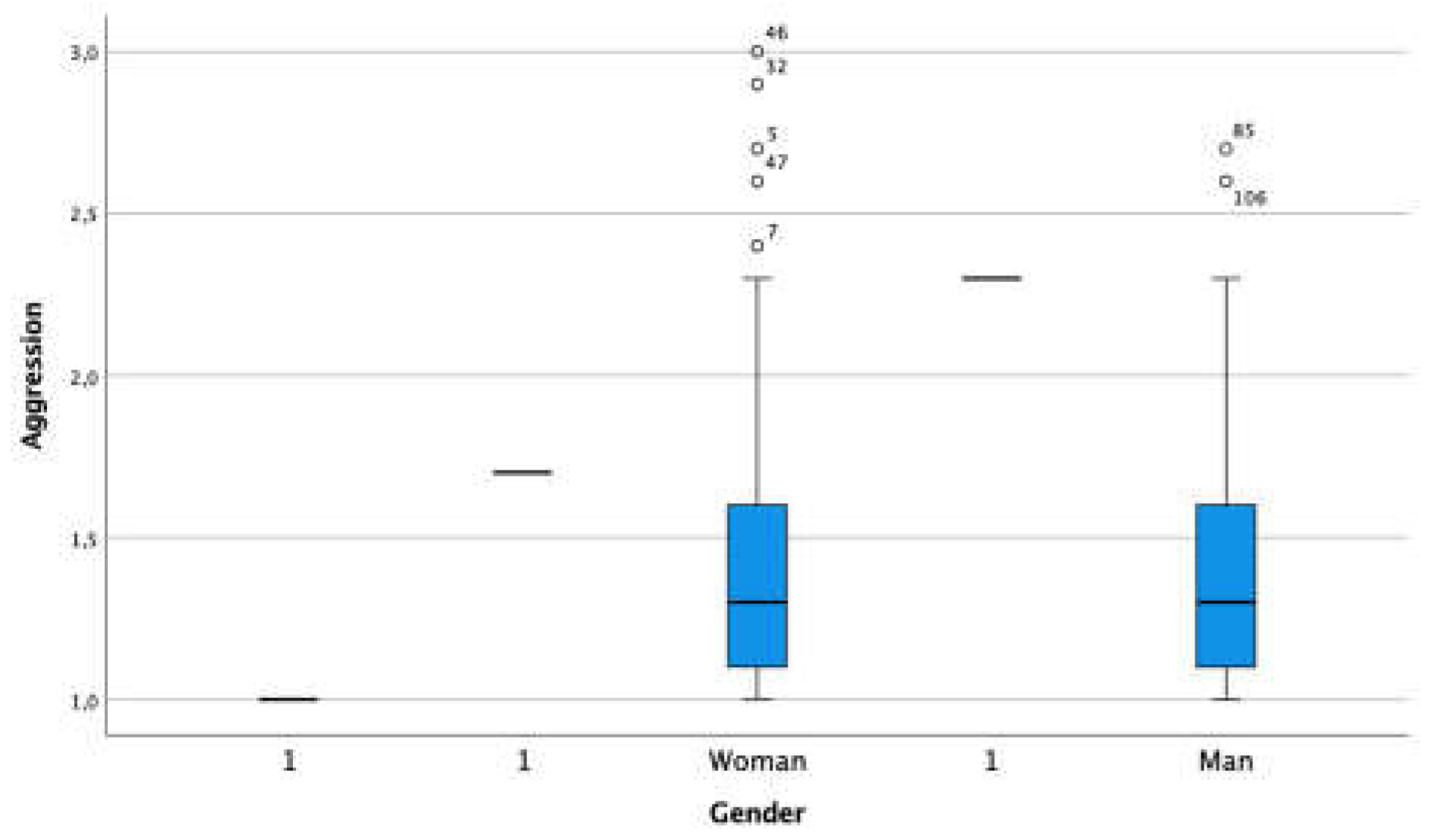
Figure 7.
Gender distribution defiant behavior.
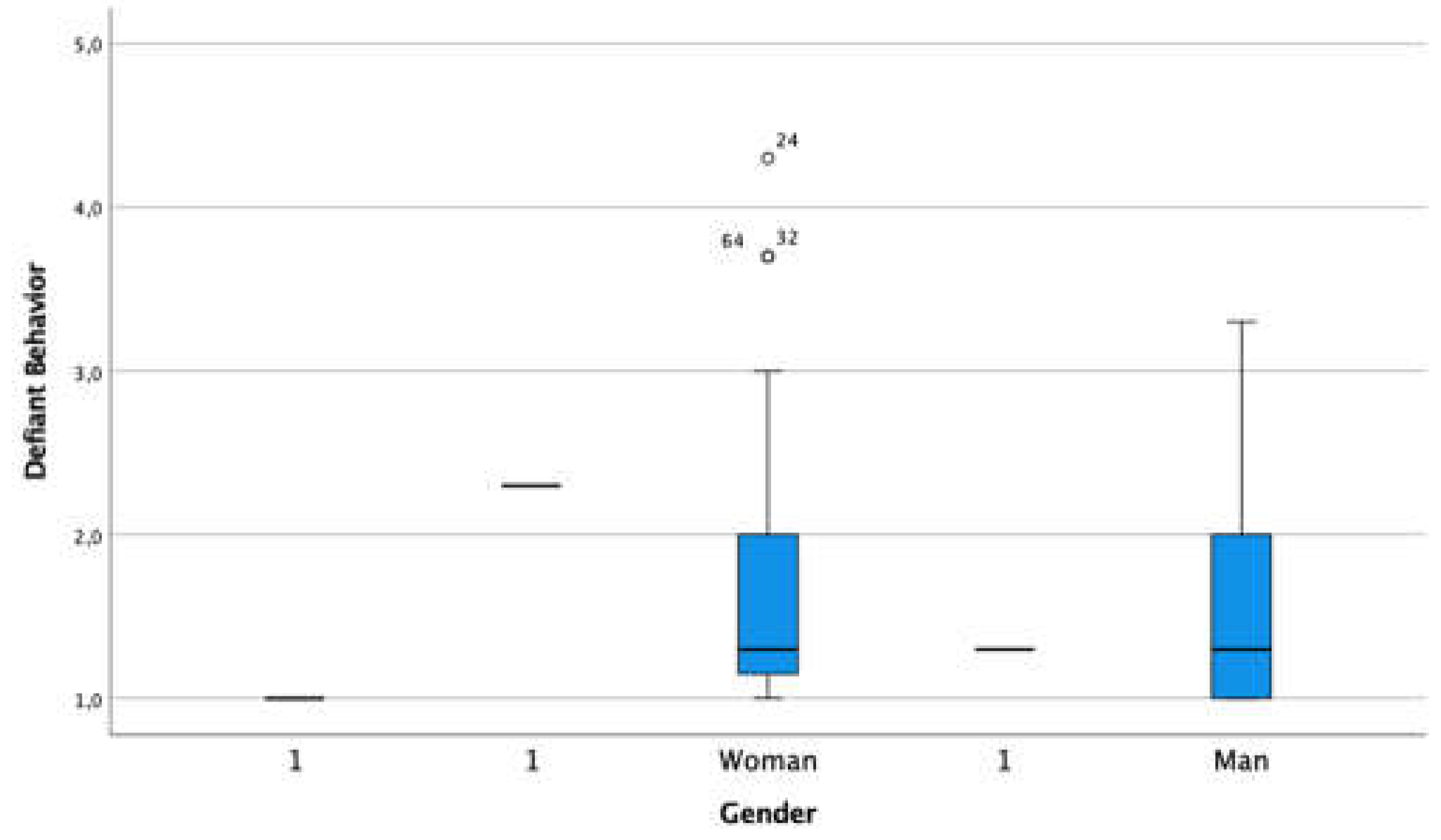
Figure 8.
Gender distribution antisocial behavior.
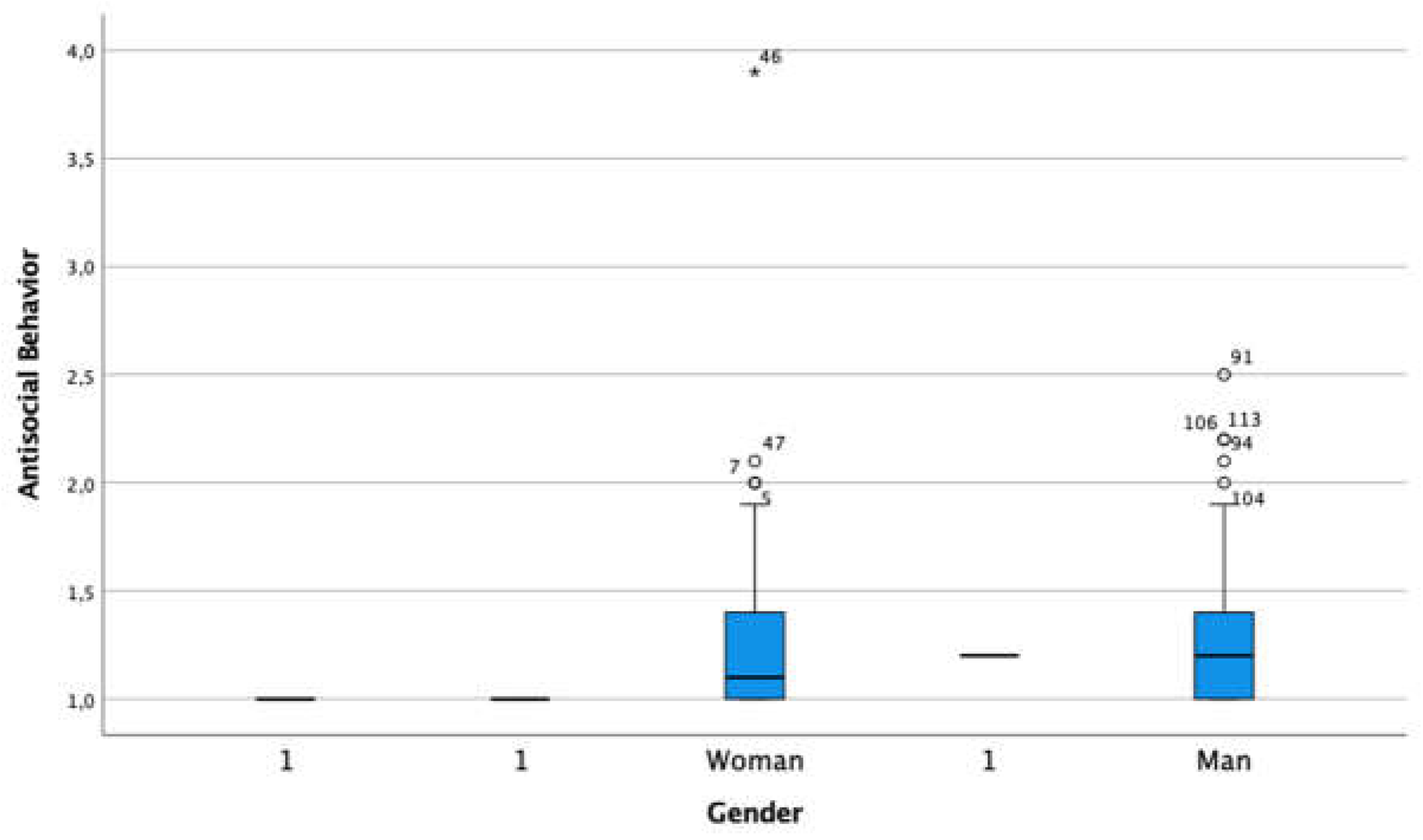
Figure 9.
Gender distribution anger management problem.
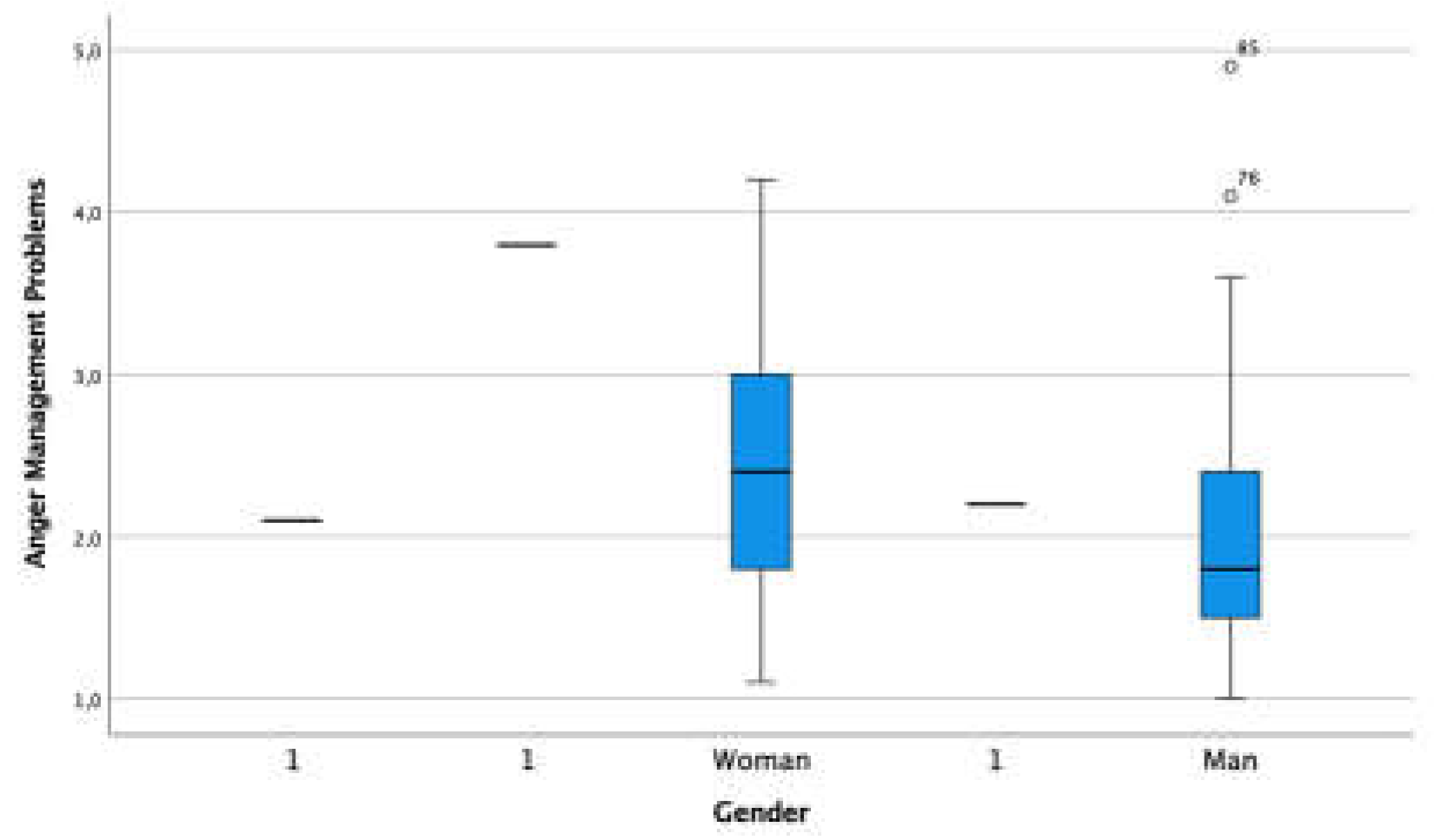

Table 1.
Sample description female group.
| Children’s Age Female Group | Frequency | Percentage | Accumulative Percentage |
| 12 | 13 | 10.2 | 10.2 |
| 13 | 21 | 16.4 | 26.6 |
| 14 | 15 | 11.7 | 38.3 |
| 15 | 17 | 13.3 | 51.6 |
| 16 | 1 | 0.8 | 52.3 |
Table 2.
Sample description male group.
| Children’s Age Male Group | Frequency | Percentage | Accumulative Percentage |
| 12 | 9 | 7 | 7 |
| 13 | 13 | 10.2 | 17.2 |
| 14 | 13 | 10.2 | 27.4 |
| 15 | 21 | 16.4 | 43.8 |
| 16 | 2 | 1.6 | 45.4 |
Table 3.
Descriptive statistics students’ externalized problems.
| N | Mean | Standard deviation | |
|---|---|---|---|
| Attention Deficit | 128 | 2.65 | .88 |
| Hyperactivity-Impulsivity | 128 | 2.26 | .68 |
| Aggression | 128 | 1.43 | .45 |
| Challenging conduct | 128 | 1.63 | .67 |
| Antisocial behavior | 128 | 1.28 | .41 |
| Anger Management Problems |
128 | 2.27 | .85 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



