
Submitted:
19 September 2024
Posted:
20 September 2024
You are already at the latest version
Abstract
Infective endocarditis (IE) results from infections by gram-positive bacteria, and, in this condition, the redox homeostasis is lost by overproduction of H2O2, leading to overstimulation of the immune system and up- regulation of the production of proinflammatory cytokines. The aim of this preliminary study of three cases with IE, was to evaluate the levels of oxidative biomarkers and of the enzymatic and non-enzymatic antioxidant systems, in subjects with IE. This is a preliminary retrospective analytical study of cases that had undergone aortic valve replacement surgery that was complicated by IE. We determined malondialdehyde (MDA), total antioxidant capacity (TAC), carbonyl groups, glutathione (GSH), thiols and the nitrate/nitrite ratio (NO3−/NO2−) in homogenized tissue of cardiac valves. We also measured the activities of GST, GPx, GR and TrxR. The super oxide dismutase (SOD) isoforms and peroxidase activities were determined using native gels. There were increases in the activities of antioxidant enzymes such as GST, SOD isoforms and peroxidases (p=0.01) and decreases in oxidative stress markers such as GSH, TAC, (p=0.01); however, MDA was increased (p=0.01). The results suggest that loss of the intricate redox homeostasis system in the aortic valve of patients with IE may favor the bacterial process and cause damage probably leading to a fatal outcome.
Keywords:
Infective endocarditis
; Oxidative stress
; Cardiac valve
; Antioxidant enzymes
; Redox homeostasis
1. Introduction
Gram-positive bacteria such as Streptococcus and Staphylococcus, are responsible for infective endocarditis (IE). These bacteria constitute 75% of the isolated microorganisms in this condition, but other species have also been found such as Escherichia coli and Pseudomonas aeruginosa among others. [1] The intracardiac site most commonly compromised is the aortic valve. The clinical characteristics present in the patients are fever, sepsis, septic shock and heart failure. The damage to the heart results from the formation of vegetations composed of fibrin and platelets [2]. Pharmacological treatment may include aminopenicillins, cephalosporins, and penicillin [3].
The gram-positive bacteria contain lipopolysaccharides (LPS) in their cell wall which are responsible for the overexpression of the host´s immune system, the induction of a cascade of proinflammation caused by cytokines and the adhesion to epithelial cells. These bacteria also have powerful toxic effects [4]. The overstimulation of the immune system is mainly due to activation of macrophages, monocytes and neutrophils and there is increased secretion of proinflammatory cytokine such as interleukins (IL)-1, -6 and -8 which can, in turn, upset the redox homeostasis in the body. This homeostasis includes the enzymatic and non-enzymatic antioxidant system [5]. The lost redox homeostasis in IE is characterized by an increase of the super oxide anion (O2–) mainly derived from NADPH oxidase and mitochondrial dysfunction. This anion contributes to increase other oxygen reactive species (ROS) such as hydrogen peroxide (H2O2) [6]. ROS may also lead to the production of hydroxyl radicals (OH–) that induce peroxidative damage to proteins, lipids, carbohydrates and nucleic acids in cardiomyocytes. This is due to the large amount of iron present in cardiomyocytes which is involved in the Fenton and Haber–Weiss reactions in presence of the OH–. In this sense, there is an association between generation of myocardial ROS and lipid peroxidation (LPO), and contractile dysfunction of the left ventricle [7]. Therefore, in this oxidative background an alteration of the antioxidant systems may be expected, but so far, the degree of participation of each particular antioxidant system remains unknown.
On the other hand, clinical management of IE, often requires of a surgical intervention or highly complex invasive procedures that are associated with several diagnostic and therapeutic dilemmas. These dilemmas are due to lack of experience of the clinicians and to the lack of published data and guidelines on the appropriate treatment [8]. Therefore, the mortality rates from this condition are high, and this constitutes a challenge in need of surveillance proposals. The existence of therapeutic guidelines for the treatment may be improve by implementing preventive and therapeutic management [9]. Therefore, the research of the role played by the deregulation of the redox homeostasis within the infectious process is relevant, regardless of the type of triggering agent of the disease, because the understanding of how redox homeostasis is compromised and its association with the process of bacterial infection could help induce a better outcome for patients. It would therefore be of importance to propose an adjuvant therapy that could contribute to re- establish the redox homeostasis. Therefore, the aim this preliminary study in three in subjects with IE, was to evaluate the levels of OS markers, the enzymatic and non-enzymatic antioxidant systems in native or prosthetic valves that required aortic valve replacement (AVR) or mitral valve. We also compare the results with those obtained from three subjects undergoing AVR without endocarditis. The results could highlight the need for future studies in a larger number of patients.
2. Materials and Methods
2.1. Recruited Patients with IE and Control Subjects
We performed a preliminary analytical retrospective review of the medical records in a list of patients diagnosed according to the modified Duke/ESC 2015 clinical criteria as patients with IE (protocol with identifier code CI-035-2024) [10]. The three selected cases with IE had been discussed by a team of expert surgeons, interventionists and clinicians who had agreed that they required a surgical or intervention by Transcatheter aortic valve implantation (TAVI) and the patients had given their informed consent for the intervention prior to surgery. Patients had also agreed that tissues could be used for microbiological and histopathological studies. In summary, the cases had had a clinically documented diagnosis which was supported by evidence, positive bacterial culture and imaging that have IE. Aortic and valve tissue were obtained during the valvuloplasty surgery due to the presence of endocarditis. Samples were obtained from the region proximal to the lesion by vegetation which could be present in different segments, and samples of each tissue were sectioned into two portions, placed in tubes under liquid nitrogen and frozen at -70 °C until studied. The control subjects were enrollment by the different disease in the surgery by AVR St. Jude with mechanical prosthesis; first case, surgery AVR; second case and mechanical AVR St. Jude; thirty cases. These patients were selected because of the valve replacement they underwent in the same way as the subjects with IE, although they are not healthy subjects and it is expected that they also present alterations in redox homeostasis, but here the difference lies in the IE present in the patients who did have the bacterial infection. Samples were obtained from the region proximal of the aortic valve replacement, the samples of each tissue were sectioned into two portions, placed in tubes under liquid nitrogen and frozen at -70 °C until studied.
2.2. Echocardiographic Study
Transesophageal echocardiography was performed using a X7-2t, transducer 2-7mHz (Phillips). All patients underwent a comprehensive study for high clinical suspicion of endocarditis under sedation.
2.3. Cardiac Valve Homogenization
The segment from the aortic valve was homogenized under liquid nitrogen after adding KH2PO4 (2 mL) 0.05 mM, pH 7.3 in presence of 20 µL antiproteases inhibitors (1 mM PMSF, 2 μM pepstatin A, 2 μM leupeptin, and 0.1% aprotinin), and the preparation was kept on ice. The Lowry method was utilized to determine the protein concentration in the homogenates [11]. All assays on biochemical variables (except for those in the native gels and western blot analysis) were made in duplicate.
2.4. Determination of the Malondialdehyde
The malondialdehyde (MDA) level was read spectrophotometrically at 532 nm. A quantity of 100 μg of homogenized tissue from the aortic valve of the cases with IE and CS were used for this determination. Methanol with BHT at 4% (100 μL) and KH2PO4 buffer pH 7.4 (1 mL) was added to the sample and then it was incubated at 37 °C for 30 min after 2-thiobarbituric acid at 0.8 M (1.5 mL) was added. It was then incubated at 90 °C for 1 h. Then, KCl at 5% (1mL) and n-butanol (4 mL) were added. The sample was shaken for 30 s, and centrifuged at 4000 rpm (2 min). The butanol phase was extracted, and the absorbance was measured [12].
2.5. Evaluation of Total Antioxidant Capacity
The total antioxidant capacity (TAC) was detected spectrophotometrically at 593 nm in 100 μg of homogenized tissue of the aortic valve of the IE and CS cases in presence of a mixture that contained C2H3O2 at 300 mM, FeCl3·6H2O at 20 mM, 2,4,6-tris-2-pyridyl-s-triazine at 10 mM, HCl at 40 mM, at pH 3.6 (1.5 mL, at ratio of 10:1:1 v/v,). The samples were incubated at 37 °C for 15 min and the absorbance was measured [13].
2.6. Carbonylation
To evaluate the carbonyl groups, 100 μg of homogenized tissue of the aortic valve were mixed with HCl 2.5 M (500 μL) and in parallel, another sample was mixed with 2,4-dinitrophenylhydrazine (500 μL) and incubated in the dark at room temperature for one hour. At the end of the incubation, C2HCl3O2 at 20% was added (500 μL) and the sample was centrifuged at 15,000× g for 5 min. The button was recovered and washed two times by adding C2H5OH/C4H8O2 (1 mL), then incubated for 10 min and centrifuged at 15,000× g for 10 min. Finally, CH6CIN3 at 6 M in KH2PO4 at 20 mM and pH 2.3 (1 mL) were added and the mixture was incubated at 37 °C for 30 min. The absorbance was read spectrophotometrically at 370 nm [12].
2.7. GSH and thiols.
For the determination of GSH, 100 μg of homogenized tissue of the aortic valve were used and this molecule was detected spectrophotometrically at 412 nm, according to Ellman’s method. The thiol groups were read spectrophotometrically at 415 nm and 50 µg of homogenized tissue of the cardiac valve of IE and CS was used according to the Erel and Neselioglu’s method [14].
2.8. NO3−/NO2− Ratio Determination.
To evaluate the NO3−/NO2− ratio, 100 μg of homogenized tissue of the aortic valve of IE and CS were previously deproteinized with 0.5 N, NaOH and 10%, ZnSO4 (100 μL). Then, 10 μL of the cytochrome c reductase (NADPH) (Sigma Aldrich Cat# 24479) were added and the sample was incubated for 30 min at 37 °C. After the incubation period, sulfanilamide 1% and N-naphthyl-ethyldiamine 0.1% (200 µL respectively) were added and the total volume was adjusted with water distilled to 1 mL. The absorbance was measured at 540 [15].
2.9. Determinations of Antioxidant Enzymes That Employ GSH
To evaluate the activities of GST, GPx, GR and TrxR, 100 μg of homogenized tissue of the aortic valve of IE and CS, were employed [12]. The GR activity was expressed as μmol of reduced GSSG/min/mg of protein, with an extinction coefficient of 6220 M−1 cm−1. The GST activity was expressed as units of GS-TNB mol/min/mg of protein, with an extinction coefficient of 14,150 M−1 cm−1. The GPx activity was expressed as nmol of NADPH oxidized/min/mg of protein, with an extinction coefficient of 6220 M−1 cm−1 at 340 nm for NADPH. The samples were incubated and monitored at 340 nm for 6 min at 37 °C. For the TrxR activity, the sample was incubated and monitored at 412 nm for 6 min at 37 °C. The TrxR activity was expressed as TNB nmol/min/mL of the serum, with an extinction coefficient of 13,600 M−1 cm−1.
2.1. Determinations of Super Oxide Dismutase Isoforms and Peroxidases Activities
The activities of super oxide dismutase (SOD) isoforms and peroxidase were determined through non-denaturing gel electrophoresis [12]. 25 µg of homogenized tissue of the cardiac valve of IE and CS were applied directly to non-denaturing 10% polyacrylamide gels. The electrophoresis was carried out at 120 volts for 4 h. For SOD isoforms activities, the gel was incubated with nitro blue tetrazolium at 2.45 mM for 20 min, then incubated with buffer of the KH2PO4 at 36 mM, EDTA at 28 mM, and riboflavin at 28 Μm pH 7.8 (20 mL) and exposed for 10 min to UV light. Purified SOD from bovine erythrocytes with a specific activity of 112 U/mg of protein (Sigma-Aldrich, St. Louis, MO, USA) was used as positive control for calculating the activity of these enzymes. For the peroxidase activity, the gel was washed with distilled water three times, for 5 min, after being incubated with 3 mg/mL 3,3,5,5-tetramethylbenzidine dissolved in CH3-OH/CH3COOH/H2O (1:1:1 v/v) with H2O2 (300 μL) total volume 20 mL, for 10 min. A quantity of 35 μL of horseradish peroxidase was loaded to a final concentration of 178.5 μg as a standard. The activities in the SOD isoforms and peroxidase gels were analyzed using densitometry with a Kodak Image® 3.5 system.
2.11. Statistical Analysis
Continuous variables are expressed as median with minimum and maximum values. Categorical variables, such as frequencies and percentages, are reported. Normality distribution was evaluated using the Shapiro-Wilk test. Non-parametric tests (Mann–Whitney) according to the Gaussian distribution, were performed to detect significant independent variables The graphical results are shown as the median, first quartile, third quartile, and half dotted line. Sigma Plot® version 15 (Systat Software Inc., SanJose, CA 95131, USA, EE. UU, North First Street, Suite 360, Jandel Corporation, San Jose, CA, USA) was used to generate the analysis and graphs. Differences were considered statistically significant when p ≤ 0.05.
3. Results
3.1. General Characteristics the Cases and Controls
Table 1 describes the general characteristics of the three patients with IE and of the control subjects. A total of three women and three men were included with an overall median age of 66 (min 43-Max 83). The demographic characteristics and admission conditions are shown. Surgical interventions were performed in two cases of IE and one underwent TAVI. The three control cases were treated by surgery. In addition, the demographic and diagnostic characteristics of patients and controls are shown in Table 2.
Table 1 General characteristics of the three patients with IE and of the control subjects.
The Figure 1 shown the echocardiographic findings cases with IE where in the case 1, is obsevate trans gastric short axis showing vegetation (yellow arrow) in relation to the sub valvular mitral apparatus. In the Case 2 left side, is showing the mitral valve endocarditis (yellow arrow), and right side is the same case, put is showing the severe mitral regurgitation. In the case 3, is showing where transesophageal short axis, in left side, and three chamber view, showing vegetation in the aortic valve (in right side, yellow arrow).
3.2. Oxidative Markers
The OS markers are shown in Figure 2. MDA was increased (p=0.01, panel A) and carbonyl groups showed a tendency to increase but without reaching a statistically significant difference (p=0.1, panel C) in the homogenized tissue of the aortic valve of the patients with IE in comparison with CS. The TAC and GSH (p=0.01, panel B and D respectively) were diminished in the patients with IE but the NO3–/NO2– ratio showed a decreasing trend. The thiol groups did not show significant changes (p=0.07, panel E and F respectively) in comparison to CS.
3.3. Activities of the Antioxidant Enzymes That Employ the Glutathione
Figure 3 shows that the GST activity in the homogenized tissue of the aortic valve was increased in IE in comparison with CS (p=0.01, panel A). However, the activities of the GPx, and TrxR only presented a tendency to increase (p=0.1, panel B and D respectively). The GR activity in IE versus CS did not show significant changes (panel C).
3.4. Peroxidases and SOD Activities
The activities of the peroxidases (p=0.04) and SOD isoforms (p=0.04 and p=0.03) were increase in the homogenized tissue of the aortic valve of the IE patients in comparison with CS (Figure 4 A and B respectively).
4. Discussion
In this paper we evaluated the levels of OS markers and the enzymatic and non-enzymatic antioxidant systems in native or prosthetic valves from patients with IE that required aortic valve replacement and in controls with AVR or mitral valve without IE. We also describe the effect of different therapeutics and compare the results with those from subjects undergoing AVR without endocarditis.
The loss of the redox homeostasis in IE is characterized by overproduction of O2– and H2O2 that results from the bacterial infection and that increases the NADPH activity in cardiomyocytes of the aortic valve. This increase, in turn, favors the activity of the enzymes that are responsible for the detoxification of these ROS such as the SOD isoforms and the family of peroxidases [6,7]. Our results show that the activity of the SOD isoforms, which have Cupper/Zinc (Cu/Zn) and manganese (Mn) in the catalytic center (SOD Cu/Zn cytosolic and SOD Mn mitochondrial respectively), and which are necessary for the dismutation processes of O2–– to H2O2 was increased in the homogenized tissue of the aortic valve of the IE patients. This result was probably due to the excess O2–– that may be provided by the over- activity of the NADPH associated to the bacterial infection. However, the activity of the SOD isoforms may favor the decrease in O2–– that, in turn, induces a high concentration of H2O2. This elevated concentration is the substrate of other enzymes such the GPx and the peroxidase families. Our results showed that the GPx activity had a tendency to decrease but without reaching statistical changes. This could be due to the small number of cases, but also to the fact that bacterial infections can decrease the activity of endogenous GPx as a mechanism for survival to perpetuate the infectious process [16]. However, the activity of peroxidases was increased in IE patients. Bacterial infections can activate eosinophil peroxidase and the myeloperoxidases in neutrophils and monocytes [17]. These enzymes that contain a hemo-group in their catalytic centers that are effective tools against bacterial infections. They utilize H2O2 to catalyze the oxidation of halides to generate hypohalous acids which is a potent oxidant that capable of oxidizing membrane lipids, proteins, RNA and DNA of microorganisms. This leads to the killing of bacteria [18]. Our results show that the activities of peroxidases were increased in the homogenized tissue of cardiac valves in patients with IE. This suggests that the peroxidase activities are increased to counteract the bacterial infection.
In addition, the increase of the H2O2 can favor the formation of OH– that oxidizes polyunsaturated fatty acid of the cell forming oxidized lipid-peroxides such as MDA, a LPO marker. Our results showed that the level of MDA was increased in the homogenized tissue of the cardiac valve in patients with IE. This increase also favors the loss of the TAC. In this sense, the concentration of GSH is depleted in bacterial infections. The reduction of GSH in the host is needed since it is an antioxidant molecule that helps fighting the increase in ROS associated with the infection process. Furthermore, throughout the infection, the bacteria can use the host's GSH for survival, replication, virulence and other processes. In fact, Streptococcus consumes it for nutritional purposes [19]. Our results show that the GSH concentration was decrease in homogenized tissue of the cardiac valve of patients with IE, reinforcing what was mentioned above. Also, the loss of GSH favors the oxidant background in the patient with IE as well as the increase of LPO and the decrease of TAC. However, the loss of GSH can also be due in part by its demand. In this sense, the activity of GST, which is an enzyme that employes GSH, forming less toxic glutathione S-conjugates, including products of LPO in the process detoxification, was increased in the homogenized tissue of the aortic valve. A possible explanation may be that it constitutes a compensatory mechanism to eliminate LPO products such as 4-hydroxy-2-nonenal and bacterial LPS. In this sense, a study in pediatric population (9-17 age) infected with Pseudomonas aeruginosa and Staphylococcus aureus that were causing chronic lung infection showed an increase of the GST [20]. Another study demonstrated that a mixture of GST-mu-class isoforms from the F. hepatica administered intraperitoneally 1 hour after a LPS injection, is capable of significantly suppressing the LPS-induced cytokine storm in a mouse model of septic shock [21]. Furthermore, the lack of significant changes in some the enzymes such as GR, TxrR, GPx and oxidative markers as thiols groups, NO3–/NO2– ratio and carbonyls groups could be due to the low number of patients with IE studied.
On the other hand, aortic stenosis is a disease that can occur in several etiologies. It is also generally found in the general population with risk factors such as age, obesity, dyslipidemia, among others. It is also widely associated with the presence of bivalve aortas and autoimmune processes. Regardless of the etiological clinical factor, once the subjects require surgery for an aortic valve replacement, the condition can be complicated by the presence of endocarditis. There are still gaps in the knowledge the mechanisms of this disease that interact with inflammation and one of them is OS. When choosing to conduct this preliminary study, we intended to determine the importance of evaluating oxidative deregulation and its importance for future clinical or cohort trials with the appropriate number of patients and sample sizes. Exploratory studies allow for the determination of whether the hypothesis deserves special attention to invest resources for long-term prospective studies when the frequency of the disease is not so high.
The cases selected in this study were carefully chosen for their clinical representativeness. In one patient, endocarditis was associated with the presence of autoimmunity. There are few reported cases of this association [22,23]. The second case did not have an autoimmune condition and there are large studies of series of patients in similar conditions; however, little information on the participation of the OS process in the mechanism of damage in the infection is studied. The reports that are available [24] have been done in animal models, or at an experimental level in vitro but not in human tissues. In the third case, aortic stenosis was performed with interventional therapy, which is most commonly indicated in older subjects with adjacent comorbidities where the surgical risk is very high [25,26].
Regarding the specific characteristics of each patient, case number one, corresponded to a 55-year-old woman with an established diagnosis of Takayasu arteritis (TA), that developed endocarditis. The culture of the aortic valve reported the presence of Staphylococcus aureus and epidermidis, (supplementary material video). Therefore, in this case, IE was fully documented. Although there are few reported cases of large vessel vasculitis, the coexistence of vasculitis and IE may exist [27]. However, there are reports that TA can be confused with IE, especially when signs and symptoms resemble the inflammatory activity or when multiple aneurysms are found [28]. This case was unfortunate, and the patient died a year after the valve replacement, since during post-surgery she was complicated with a cerebral vascular disease. Although she was treated with a timely surgical intervention, comprehensive therapeutic management could improve results in patients with similar conditions. Cases of TA are rare, and it is difficult to have large series with the coexistence of IE. However, it would be important to evaluate the use of antioxidant as an adjuvant therapy in this complex condition where inflammation persists due to the disease and can be associated with an infectious and deregulation of the OS state. In this study, all patients had a high LPO and there are no previously reported similar studies. Therefore, this is a case to highlight.
The second case with IE, was a 67-year-old woman with a bicuspid valve. Large series of patients with this condition have demonstrated that a high percentage of IE may be present in them [29]. In this case, Streptococcus viridians was found as the main pathogen, which is also one of the most frequently found bacteria. This patient has a current survival of 4 years, and in her file, we did not find complete data on the therapeutic management she had received. Nevertheless, she was in an intensive therapy area where standard management is always implemented and there was an immediate surgical resolution, (supplementary material video).
The third case corresponded to a 78-year-old man who was treated for aortic stenosis with implantation of transcatheter aortic valve (TAVI). 48 hours after this procedure, he presented endocarditis and underwent surgery. This procedure is cutting- edge and IE occurs with low frequency in the early phase, before 30 days, (supplementary material video) [2]. The patient developed IE within the first 48 hours after implantation. In most published cohorts, Enterococcus spp. has been identified as the most common pathogen, followed by Staphylococcus aureus whose incidence is relatively low, ranging between 0.1 and 3% [30,31]. However, IE post-TAVI is an early complication, and it is associated with a poor prognosis, not only in comparison with native valve endocarditis but also in comparison to surgically replacement of valve endocarditis, regarding both valve dysfunction and patient mortality [2]. The clinical profile of most TAVI candidates includes elderly patients who are at a high surgical risk due to the presence of several comorbidities at the time of the intervention [32]. This also represents a risk that can enhance common IE pathogens and the presence of other opportunistic bacteria [33]. In the case of this patient, the complication due to IE was associated with the presence of Enterobacter cloacae, Klebsiella Oxytocic. However, it also highlights the moment at which a solution was tried to be implemented both therapeutically and by surgical intervention. Furthermore, the patient was taken to a surgery called Commando with a high risk of mortality. However, the patient survived for 5 years after the reintervention by surgery and the multidisciplinary management in which he received antioxidants such as vitamin C. Although there is not a follow-up study to evaluate the effect of the antioxidant therapy, the evolution and survival achieved after the critical period, confirms the findings from a large series carried out by our group where OS was controlled through standard management and adjuvant therapy with antioxidants.
On the other hand, the control subjects that were selected for comparison with subjects with IE were intervened for aortic valve replacement and they underwent the same procedures as the subjects with IE. Although they are not healthy subjects and it is expected that they also present alterations in redox homeostasis, the difference between the groups lies in the presence of IE. It should be noted that subjects who were selected as controls and the patients with IE had different indications for aortic valve replacement and this could be a topic of discussion regarding the loss of redox homeostasis. However, the point of comparison lies in the presence and absence of the IE
5. Conclusions
The results from this series of three cases of IE in aortic valve suggest the loss of an intricate redox homeostasis system in patients with IE in the aortic valve may be favor the bacterial process, with an unfavorable result for the patient with the consequences leading to fatal outcomes. The surgical management of IE in expert hands improves these complex conditions; however, the success of the intervention must be accompanied by follow- up during the pre- and post-surgical periods aimed to reduce the metabolic conditions caused by the comorbidities in each patient. In addition to reducing the infectious and inflammatory state, the presence of OS state of deregulation requires consideration of adjuvant management with antioxidant therapy. The findings also justify future studies through clinical trials where adequate sample size is included to confirm and support this hypothesis.
Study Limitations. There are studies on IE in large series of patients, but none is focused on elucidating the participation of OS independently of the origin and comorbidities of the patient. Although the small number of cases may seem a limitation, it is not really so, since our objective was to carry out an exploratory study on this topic to determine its feasibility through prospective studies. Exploratory or preliminary studies are often recommended to previously evaluate which findings deserve attention without investing large resources.
Study Advantages. Even with a small number of cases, this is one of the few studies conducted on human valve tissue. The findings support that oxidative stress is involved in the mechanism of damage of IE as an alternative mechanism that deserves attention as a possible therapeutic treatment.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, video 1: title; Echocardiographic.
Author Contributions
Conceptualization and writing, M.E.S.; I.P.T. and E.S.C; methodology, I.P.T. and L.M.P.; Review and Medical records H.R.Z.; review and editing, V.G.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study is preliminary with a case series design where after a surgical intervention they present endocarditis. Each case had an interesting origin, one associated with autoimmunity, another with bivalve aorta and one in whom the intervention was for a more common cause. During the intervention, they are only operated after the patient agrees to be intervened and after giving informed consent. Moreover, they accept that their tissue is the subject of study and research. This protocol followed the privacy and confidentiality guidelines described in the Declaration of Helsinki of the World Medical Assembly [29,30]. All necessary measures were taken to safeguard the personal information present in the clinical records to be analyzed. The regulations of the General Health Law on Research for health in Human Beings were followed. According to article 17, Section II, this project was classified without risks. Good Clinical Practices guidelines were also followed to protect the integrity and confidentiality of the information use. [31].
Informed Consent Statement
The patients/participants gave their written informed consent to undergo surgery.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
Thanks, by the payment for the open-access publishing which was covered by the Instituto Nacional de Cardiología Ignacio Chávez.
Conflicts of Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
- Alifragki, A.; Kontogianni, A.; Protopapa, I.; Baliou, S.; Ioannou, P. Infective Endocarditis by Pasteurella Species: A Systematic Review. J. Clin. Med. 2022, 11, 50372. [Google Scholar] [CrossRef] [PubMed]
- Østergaard, L.; Lauridsen, T.K.; Iversen, K.; Bundgaard, H.; Søndergaard, L.; Ihlemann, N.; Moser, C.; Fosbøl, E. Infective endocarditis in patients who have undergone transcatheter aortic valve implantation: a review. Clin. Microbiol. Infect. 2020, 26, 999–1007. [Google Scholar] [CrossRef]
- Veve, M.P.; McCurry, E.D.; Cooksey, G.E.; Shorman, M.A. Epidemiología y resultados de la endocarditis infecciosa no relacionada con HACEK en el sureste de los Estados Unidos. PLoS. ONE. 2020, 15, e0230199. [Google Scholar]
- Vincent, L.L.; Otto, C.M. Infective Endocarditis: Update on Epidemiology, Outcomes, and Management. Curr. Cardiol. Rep. 2018, 20, 86. [Google Scholar] [CrossRef] [PubMed]
- Tsutsui, H.; Kinugawa, S.; Matsushima, S. Mitochondrial oxidative stress and dysfunction in myocardial remodelling. Cardiovasc. Res. 2009, 81, 449–456. [Google Scholar] [CrossRef]
- Ostrowski, S.; Kasielski, M.; Kordiak, J.; Zwolinska, A.; Wlodarczyk, A.; Nowak, D. Myocardial oxidative stress in patients with active infective endocarditis. Int. J. Cardiol. 2013, 167, 270–276. [Google Scholar] [CrossRef]
- Ide, T.; Tsutsui, H.; Kinugawa, S.; Suematsu, N.; Hayashidani, S.; Ichikawa, K.; Utsumi, H.; Machida, Y.; Egashira, K. Takeshita, A. Direct evidence for increased hydroxyl radicals originating from superoxide in the failing myocardium. Circ. Res. 2000, 86, 152–157. [Google Scholar] [CrossRef]
- Chen, H.; Zhan, Y.; Zhang, K.; Gao, T.; Chen, L.; Zhan, J.; Chen, Z.; Zeng, Z. The global, regional, and national burden and trends of infective endocarditis from 1990 to 2019: results from the global burden of disease study 2019. Front. Med. 2022, 9, 774224. [Google Scholar] [CrossRef]
- Borger, M.A.; Delgado, V. The 'Ten Commandments' for the 2023 European Society of Cardiology guidelines for the management of endocarditis. Eur. Heart. J. 2024, 45, 1697–1698. [Google Scholar] [CrossRef]
- Pecoraro, A.J.K.; Herbst, P.G.; Pienaar, C.; Taljaard, J.; Prozesky, H.; Janson, J.; Doubell, A.F. Modified Duke/European Society of Cardiology 2015 clinical criteria for infective endocarditis: time for an update? Open. Heart. 2022, 9, e001856. [Google Scholar] [CrossRef]
- Lowry, O.H.; Rosebrough, N.J.; Farr, A.L.; Randall, R.J. Protein measurement with the Folin phenol reagent. J. Biol. Chem. 1951, 193, 265–275. [Google Scholar] [CrossRef] [PubMed]
- Soto, M.E.; Pérez-Torres, I.; Manzano-Pech, L.; Soria-Castro, E.; Morales-Marín, A.; Ramírez-Marroquín, E.S.; Martínez-Hernández, H.; Herrera-Alarcón, V.; Guarner-Lans, V. Reduced levels of selenium and thioredoxin reductase in the thoracic aorta could contribute to aneurysm formation in patients with Marfan syndrome. Int. J. Mol. Sci. 2023, 24, 10429. [Google Scholar] [CrossRef] [PubMed]
- Chavarría, A.P.; Vázquez, R.R.V.; Cherit, J.G.D.; Bello, H.H.; Suastegui, H.C.; Moreno-Castañeda, L.; Estrada, A.G.; Hernández, F.; González-Marcos, O.; Saucedo-Orozco, H.; et al. Antioxidants and pentoxifylline as coadjuvant measures to standard therapy to improve prognosis of patients with pneumonia by COVID-19. Comput. Struct. Biotechnol. J. 2021, 19, 1379–1390. [Google Scholar] [CrossRef] [PubMed]
- Erel, O.; Neşelioğlu, S.; Tunçay, M.E.; Oğuz, E.F.; Eren, F.; Akkuş, M.S.; Güner, H.R.; Ateş, İ. A sensitive indicator for the severity of COVID-19: Thiol. Turk. J. Med. Sci. 2021, 51, 921–928. [Google Scholar] [CrossRef]
- Soto, M.E.; Manzano-Pech, L.G.; Guarner-Lans, V.; Díaz-Galindo, J.A.; Vásquez, X.; Castrejón-Tellez, V.; Gamboa, R.; Huesca, C.; Fuentevilla-Alvárez, G.; Pérez-Torres, I. Oxidant/Antioxidant Profile in the Thoracic Aneurysm of Patients with the Loeys-Dietz Syndrome. Oxid. Med. Cell Longev. 2020, 2020, 5392454. [Google Scholar] [CrossRef]
- Gutiérrez-Venegas, G.; Fernández-Rojas, B.; Rosas-Martínez, M.; Manuel Alejandro Sánchez-Carballido, M.A. Rutin prevents LTA induced oxidative changes in H9c2 cells. Prev. Nutr. Food. Sci. 2020, 25, 203–211. [Google Scholar] [CrossRef]
- Cao, Z.; Cheng, G. Recombinant myeloperoxidase as a new class of antimicrobial agents. Microbiol. Spectr. 2022, 10, e0052221. [Google Scholar] [CrossRef]
- Nauseef, W.M. Biological roles for the NOX family NADPH oxidases. J. Biol. Chem. 2008, 283, 16961–16965. [Google Scholar] [CrossRef]
- Baskerville, M.J.; Kovalyova, Y.; Mejías-Luque, R.; Gerhard, M.; Hatzios, S.K. Isotope tracing reveals bacterial catabolism of host-derived glutathione during Helicobacter pylori infection. PLoS. Pathog. 2023, 19, e1011526. [Google Scholar] [CrossRef]
- Sadowska-Bartosz, I.; Galiniak, S.; Bartosz, G.; Rachel, M. Oxidative modification of proteins in pediatric cystic fibrosis with bacterial infections. Oxid. Med. Cell. Longev. 2014, 2014, 389629. [Google Scholar] [CrossRef]
- Tisch, C.; Ernst, D.; Falke, M.; Speicher, P.; Ziaka, M. Systemic embolization due to non-bacterial thrombotic endocarditis: An autopsy case report and mini review of the literature. SAGE. Open. Med. Case. Rep. 2024, 12, 2050313X241229576. [Google Scholar] [CrossRef] [PubMed]
- Iyer, I.; Sinha, R.; Kumar, P. ; Schaf B, Berkowitz L: A 'Decrescendo' in a woman with ascending paralysis: A diagnostic challenge. Cureus. 2024, 16, e59479. [Google Scholar]
- Adedoyin, F.T.; Sridhar, B.B.M.; Rosenzweig, J.A. Impact of metal exposure on environmentally isolated Serratia marcescens' growth, oxidative-stress resistance, biofilm formation, and proliferation in eukaryotic co-culture models. Ecotoxicol. Environ. Saf. 2023, 253, 114677. [Google Scholar] [CrossRef] [PubMed]
- Ried, I.D.; Omran, H.; Potratz, M.; Rudolph, T.K.; Scholtz, S.; Bleiziffer, S.; Piper, C. Infective endocarditis after isolated aortic valve replacement: comparison between catheter-interventional and surgical valve replacement. Clin. Res. Cardiol. 2024, 113, 336–352. [Google Scholar] [CrossRef]
- Cabrucci, F.; Bacchi, B.; Codecasa, R.; Stefàno, P. Case report: Infective endocarditis after transcatheter aortic valve implantation surgically treated with sutureless prosthesis and ascending aorta replacement. Front. Cardiovasc. Med. 2023, 10, 1194304. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, E.F.; Levy, J.M.; Hong, R.; Viseskul, C.; Henshaw, C. Takayasu's arteriopathy with involvement of aortic valve and bacterial endocarditis. J. Pediatr. 1973, 83, 463–436. [Google Scholar] [CrossRef] [PubMed]
- Alcelik, A.; Karacay, S.; Hakyemez, I.N.; Akin, B.; Ozturk, S.; Savli, H. Takayasu arteritis initially mimicking infective endocarditis. Mediterr. J. Hematol. Infect. Dis. 2011, 3, e2011040. [Google Scholar] [CrossRef]
- Li, H.; Li, Y.; Jia, Z.; Ren, L.; Nappi, F.; Ma, X.; Jiang, Y.; Han, S. Postoperative follow-up of 221 patients with infective endocarditis from Gaoligong mountain area of Yunnan in China: a retrospective, single-center, observational cohort study. J. Thorac. Dis. 2024, 16, 3325–3337. [Google Scholar] [CrossRef]
- Habib, G. Infective endocarditis after transcatheter aortic valve replacement: the worst that can happen. J. Am. Heart. Assoc. 2018, 7, e010287. [Google Scholar] [CrossRef]
- Delgado, V.; Ajmone-Marsan, N.; de Waha, S.; Bonaros, K.; Brida, M.; Burri, H.; Casell, S.; Doenst, T.; Ederhy, S.; Ederhy, S.; Erb, P.A.; Foldager, D.; et al. 2023 ESC Guidelines for the management of endocarditis. Eur. Heart. J. 2023, 44, 3948–4042. [Google Scholar]
- Yumoto, T.; Ichiba, S.; Umei, N.; Morisada, S.; Tsukahara, K.; Sato, K.; Ujike, Y. Septic shock due to Aeromonas hydrophila bacteremia in a patient with alcoholic liver cirrhosis: a case report. J. Med. Case. Rep. 2014, 8, 402. [Google Scholar] [CrossRef] [PubMed]
- Brouqui P, Raoult D: Endocarditis due to rare and fastidious bacteria. Clin. Microbiol. Rev. 2001, 14, 177–207. [CrossRef] [PubMed]
- Benic, C.; Nicol, P.P.; Hannachi, S.; Gilard, M.; Didier, R.; Nasr, B. Vascular complications following transcatheter aortic valve implantation, using MANTA (Collagen Plug-Based) versus PROSTAR (Suture-Based), from a French single-center retrospective registry. J. Clin. Med. 2023, 12, 6697. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, B.; Dunn, L. The declaration of Helsinki on medical research involving human subjects: A review of seventh revision. J. Nepal. Health. Res. Counc. 2020, 7, 548–552. [Google Scholar] [CrossRef]
- Salas, M. Buenas prácticas clínicas (BPC ICH) de la conferencia internacional de armonización. https://codigof.mx/buenas-practicas-clinicas-bpc-ich-de-la-conferencia-internacional-de armonizacion, 2017, 1–61.
Figure 1.
Transesophageal echocardiographic analysis of the patient series. Panel A Case 1. Trans gastric short axis showing vegetation (yellow arrow) in relation to the sub valvular mitral apparatus. Case 2 Showing mitral valve endocarditis (yellow arrow), panel B, and with severe mitral regurgitation, panel C. Case 3. Transesophageal short axis, panel D, and three chamber view, panel E, showing vegetation in the aortic valve (yellow arrow).
Figure 1.
Transesophageal echocardiographic analysis of the patient series. Panel A Case 1. Trans gastric short axis showing vegetation (yellow arrow) in relation to the sub valvular mitral apparatus. Case 2 Showing mitral valve endocarditis (yellow arrow), panel B, and with severe mitral regurgitation, panel C. Case 3. Transesophageal short axis, panel D, and three chamber view, panel E, showing vegetation in the aortic valve (yellow arrow).
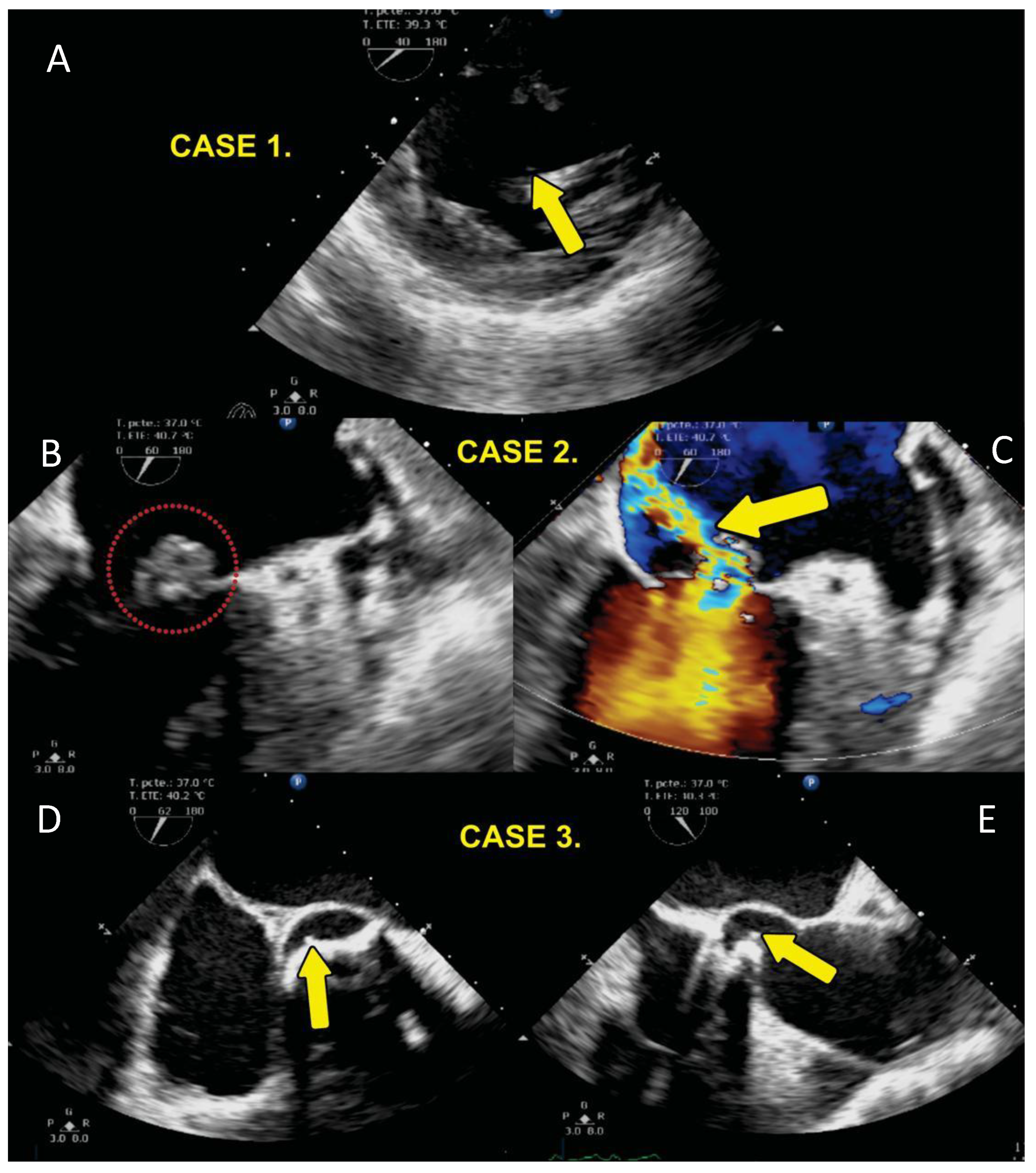
Figure 2.
Oxidative stress markers such as MDA levels (A), TAC (B), Carbonylation (C), GSH (D), thiols groups (E) and NO3–/NO2– ratio (F) in homogenized of the valve cardiac of the CS and IE. The values are expressed such as median, first quartile, third quartile, and half dotted line. The dark circles that stand out from each bar are the outliers. Abbreviations: CS= Control subjects, IE= Infective endocarditis, MDA= malondialdehyde, TAC= Total antioxidant capacity, GSH= Glutathione, NO3–/NO2– nitrate and nitrite.
Figure 2.
Oxidative stress markers such as MDA levels (A), TAC (B), Carbonylation (C), GSH (D), thiols groups (E) and NO3–/NO2– ratio (F) in homogenized of the valve cardiac of the CS and IE. The values are expressed such as median, first quartile, third quartile, and half dotted line. The dark circles that stand out from each bar are the outliers. Abbreviations: CS= Control subjects, IE= Infective endocarditis, MDA= malondialdehyde, TAC= Total antioxidant capacity, GSH= Glutathione, NO3–/NO2– nitrate and nitrite.
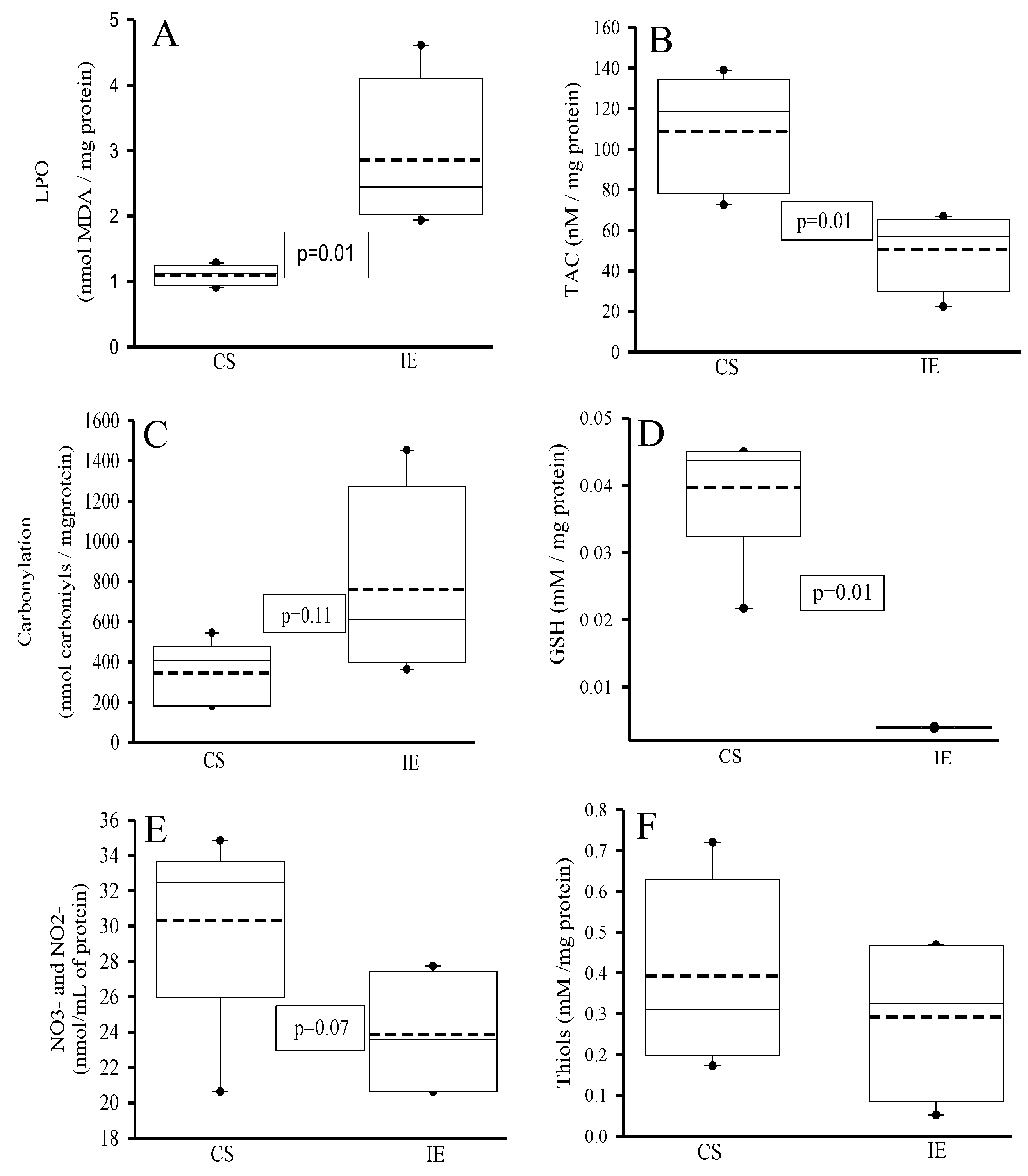
Figure 3.
Determinations of some antioxidant enzymes that employ GSH such as GST (A), GPx (B), GR (C) and TrxR (D) in homogenized tissue of the aortic valve of the CS and IE. The values are expressed such as median, first quartile, third quartile, and half dotted line. The dark circles that stand out from each bar are the outliers. Abbreviations: CS= Control subjects, IE= Infective endocarditis.
Figure 3.
Determinations of some antioxidant enzymes that employ GSH such as GST (A), GPx (B), GR (C) and TrxR (D) in homogenized tissue of the aortic valve of the CS and IE. The values are expressed such as median, first quartile, third quartile, and half dotted line. The dark circles that stand out from each bar are the outliers. Abbreviations: CS= Control subjects, IE= Infective endocarditis.
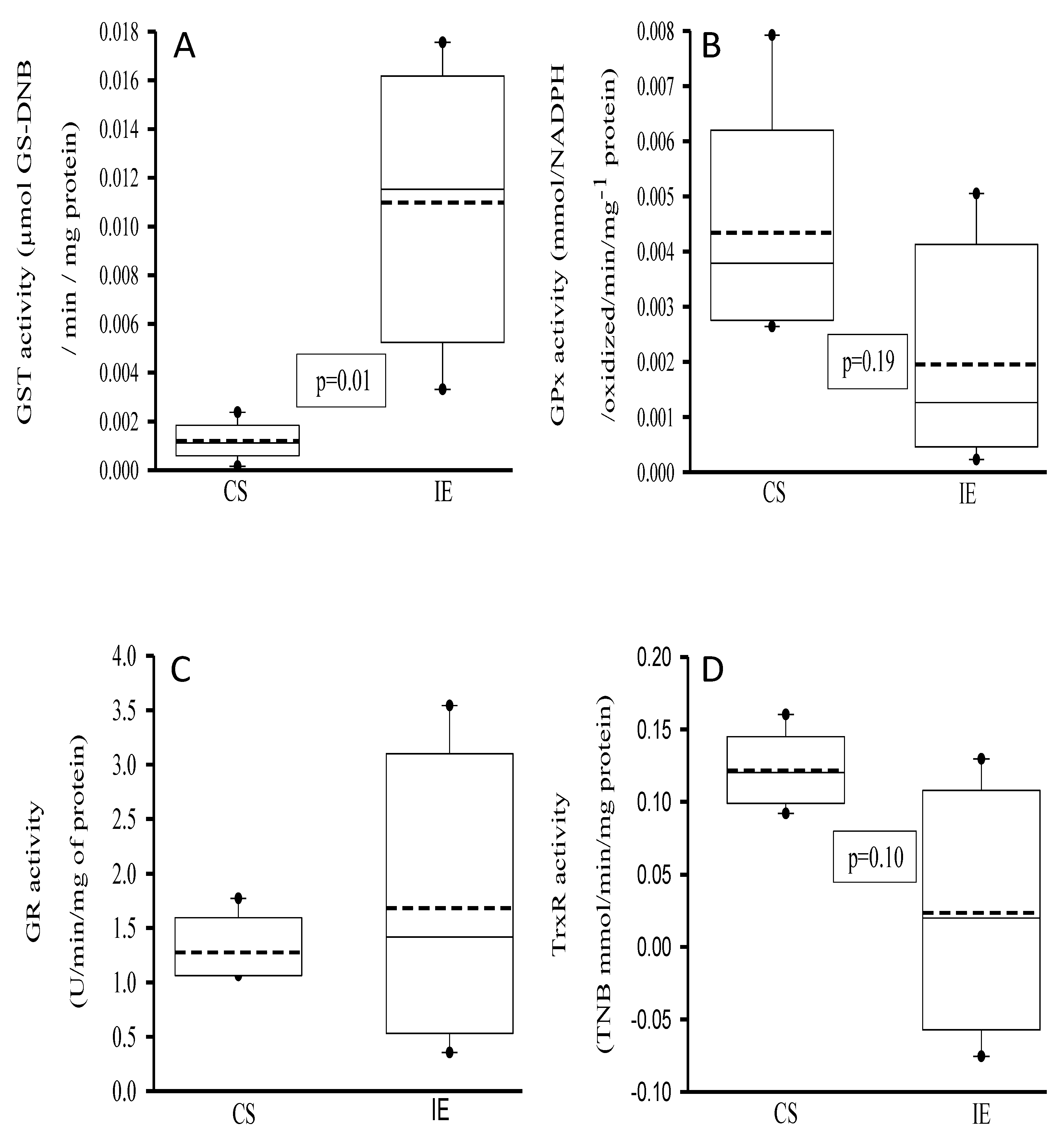
Figure 4.
Activities of Peroxidases (A) and SOD isoforms (B) in homogenized tissue of the aortic valve. The values are expressed such as median, first quartile, third quartile, and half dotted line. The dark circles that stand out from each bar are the outliers. Abbreviations: CS= Control subjects, IE= Infective endocarditis, SOD= super oxide dismutase’s.
Figure 4.
Activities of Peroxidases (A) and SOD isoforms (B) in homogenized tissue of the aortic valve. The values are expressed such as median, first quartile, third quartile, and half dotted line. The dark circles that stand out from each bar are the outliers. Abbreviations: CS= Control subjects, IE= Infective endocarditis, SOD= super oxide dismutase’s.
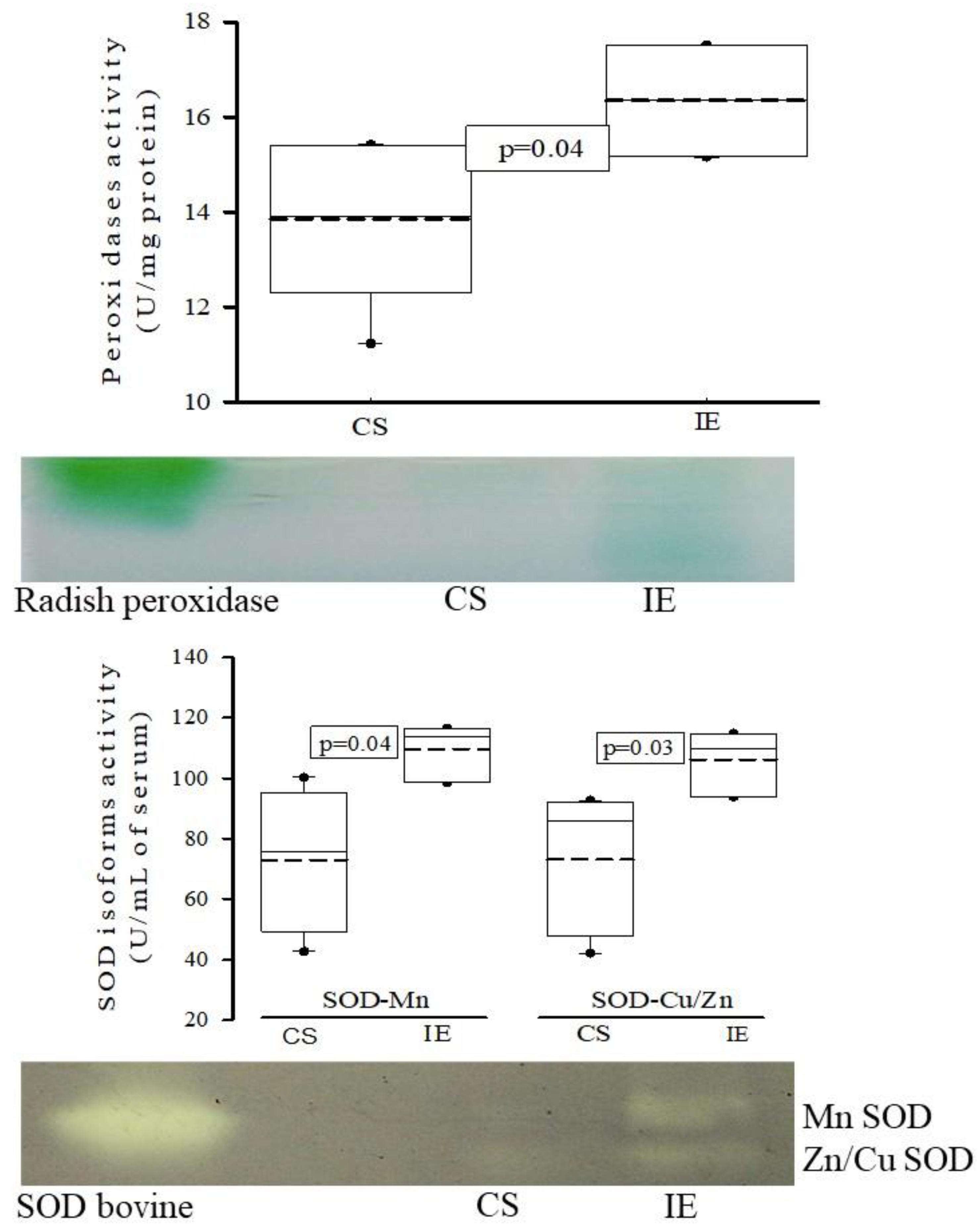

Table 1.
Demographic characteristics of the three patients with IE that required aortic valve replacement surgery and controls subjects with aortic valve damage who required aortic valve replacement and did not develop endocarditis and that were included in the study. Abbreviations: NT-Pro-BNP= Natriuretic peptide. Abbreviations: NT-Pro-BNP= Natriuretic peptide.
Table 1.
Demographic characteristics of the three patients with IE that required aortic valve replacement surgery and controls subjects with aortic valve damage who required aortic valve replacement and did not develop endocarditis and that were included in the study. Abbreviations: NT-Pro-BNP= Natriuretic peptide. Abbreviations: NT-Pro-BNP= Natriuretic peptide.
| Endocarditis | Control Subjects | |
|---|---|---|
| Age | 70 (64-83) | 65 (43-67) |
| Body Mass Index | 22 (20-25) | 29 (28-33) |
| Comorbidities | ||
| Diabetes Mellitus | 1 (33) | 1 (33) |
| Systemic Arterial Hypertension | 2 (66) | 2 (66) |
| Dyslipidemia | 1 (33) | 1 (33) |
| Smoking | 2 (66) | 2 (66) |
| Laboratories | ||
| Glucose | 119 (85-131) | 115(109-164) |
| Creatinine | 0.81 (0.7-1.5) | 1.4 (0.98-1.7) |
| Blood urea nitrogen | 30 (22-41) | 18 (15-23) |
| Uric acid | 6.7 (3.8-7) | 9.8 (5.3-10.1) |
| Natriuretic peptide NT-Pro-BNP | 7339 (1971-22494) | 200 (170-278) |
| Hemoglobin | 11.8 (11.1-14.7) | 14.4 (13.5-15.9) |
| Platelets | 172 (152-200) | 160 (91-230) |
| Leukocytes | 8.4 (5.6-16.1) | 8 (6.5-10) |
| Lymphocytes | 1.1 (1-8.7) | 2.5 (1.2-2.7) |
| Neutrophils | 6.6 (4.5-13.9) | 6.1 (3.1-7) |
| Erythrocyte sedimentation rate mm/ | 30 (27-43) | 18 (16-32) |
| C-reactive protein mg/L | 47.5 (40-200) | 2.5 (0.7-6.9) |
| Total cholesterol | 173 (138-325) | 112 (108-186) |
| High Density Lipoprotein | 53.4 (45.5-53.8) | 44 (28.5-44.5) |
| Low Density Lipoprotein | 98 (92-196) | 122 (101-125) |
| Triglycerides | 131 (130-211) | 2123 (70-221) |
| Aorta diameters | ||
| Aortic valve plane | 29 (20-38) | 26 (22-27) |
| Sinus of Valsalva | 37 (20-40) | 28 (21-58) |
| Sino tubular junction | 38 (18-40) | 27 (21-58) |
| Ascending aorta | 37 (16-39) | 30 (20-37) |
| Ejection fraction of the left ventricle | 20 (20-45) | 44 (30-65) |
Table 2.
the demographic and diagnostic characteristics of patients and controls. Abbreviations: DAoI= Double aortic injury, AVR= aortic valve replacement, AoI= Aortic insufficiency. Ao= aortic. LV= Left Ventricle. LVEF= Left ventricle ejection fraction, TAVI= Trans catheter aortic valve Implantation, MVR= mitral valve replacement, GLS= Global Strain, BAV= Atrioventricular block, PAP pulmonary arterial pressure, DM= Diabetes Mellitus, SAH= Systemic arterial Hypertension.
Table 2.
the demographic and diagnostic characteristics of patients and controls. Abbreviations: DAoI= Double aortic injury, AVR= aortic valve replacement, AoI= Aortic insufficiency. Ao= aortic. LV= Left Ventricle. LVEF= Left ventricle ejection fraction, TAVI= Trans catheter aortic valve Implantation, MVR= mitral valve replacement, GLS= Global Strain, BAV= Atrioventricular block, PAP pulmonary arterial pressure, DM= Diabetes Mellitus, SAH= Systemic arterial Hypertension.
| Case | Age | G | BMI | Diagnosis | Evolution | Death |
|---|---|---|---|---|---|---|
| 1 | 55 | F | 20 | 2009 diagnosis of Arteritis de Takayasu plus bicuspid aortic valve SAH 1999 AVR by severe AoI (Medtronic Hall). | Endocarditis in 2016. univalve prosthetic valve with pannus and abscess with tissue destruction at level of interventricular septum with bacterial growth with Staphylococcus aureus and epidermidis. Surgery AVR and implantation of, dual-chamber pacemaker, by complete BAV, she had ischemic stroke and left hemiparesis with evolution with reduced heart failure LVEF 25% died in 2017 one year after surgery. | yes |
| 2 | 67 | M | 30 | 2019 DAoI and AoI severe bicuspid aortic valve LV systolic and diastolic dysfunction LVEF 20%, smoking. | 2020 native valve endocarditis with mobile vegetation of left non-coronary valve plus ascending aortic aneurysm, Surgery AVR Medtronic Hall with bacterial growth with Streptococcus viridansj. 2024 normal functioning prosthesis, LVEF 57%. | no |
| 3 | 78 | F | 24 | DAoI and stenosis Ao, tri-valve Aortic valve. 2019 March she received intervention with Transcatheter aortic valve implantation (TAVI) Portico 25 mm plus Boston Scientific DDD Pacemaker Tachycardia Bradycardia Syndrome Comorbidities: Smoking, systemic arterial hypertension, dyslipidemia. | 2019 April she had TAVI endocarditis with vegetation in the aortic valve. Mitroaortic junction abscess plus aortitis aortic wall abscess. Valve crop Enterobacter cloacae, Klebsiella Oxytocic She was treated with aortic valve explanation surgery, ascending aorta resection. Bentall and Bo, MVR Edwards Peri mount. Mitroaortic command surgery. 2024 she is live LVEF 40%. | no |
| 4 | 60 | F | 30 | Ischemic heart disease, Tri valvular disease 2014 angioplasty in right coronary artery, 2017 aortic stenosis, AVR with mechanical prosthesis St Jude Masters HP 21, LVEF 52%. Comorbidities: Mellitus diabetes. | 2024 asymptomatic LVEF 58%. | no |
| 5 | 37 | M | 28 | 2018 Ascending aortic aneurysm aortic insufficiency, 4-cavity dilatation eccentric hypertrophy LV severe mild mitral insufficiency PAP 74 mmHg, Surgery AVR, DM, Systolic. arterial hypertension, dyslipidemia, hyperuricemia, positive smoking. LVEF 44%. | 2019 Gout, asymptomatic cardiovascular LVEF 50%, systolic dysfunction GLS 14.5. | no |
| 6 | 62 | M | 34 | Ventricular dysfunction, severe aortic and mitral insufficiency, generalized hypokinesia LVEF 30%. 2014 Surgery due to Aortic Dissection Stanford A, DeBakey 1 plus Severe tricuspid regurgitation and mechanical AVR St. Jude. SAH, Smoking. | 2017 Asymptomatic, controlled high blood pressure stopped coming since that date. | no |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



