
Submitted:
20 July 2024
Posted:
22 July 2024
You are already at the latest version
Abstract
Genetic factors influence medication response (pharmacogenetics), affecting the pharmacody-namics and pharmacokinetics of many medicaments used in clinical care. The ability of medica-tions to cross the blood-brain barrier (BBB) represents a critical putative factor in the effectiveness and tolerability of various central nervous system (CNS) medications at a pharmacokinetic (dosing) level. Pharmacogenetics has the potential to personalise medicine to a greater extent than has been possible, with the potential to help reduce heuristic delays to effective tolerable pharmacotherapy. Here, we critically examine and summarise the evidence, particularly for ABCB1 polymorphisms associated with various CNS medications. These transporters appear to have a role in BBB pharmacogenetics. We identify some of the most promising variants for clinical translation while spotlighting the complexities of the involved systems and limitations of the current empirical literature.
Keywords:
pharmacogenetics
; blood-brain barrier
; drug discovery
; personalised medicine
; precision medicine
; clinical translation
1. Introduction
The blood-brain barrier (BBB) forms the primary physical defence of the central nervous system against potential toxins and pathogens. It does so by actively and passively moderating the diffusion and effusion of substances into and out of the central nervous system (CNS). A combination of tight endothelial junctions, active transporters, and adjacent pericytes and astrocytes comprise the neurovascular unit of the BBB, a complex system whose basic physiology is still being elucidated [1]. Genetic variants are known to influence medicament permeability across the BBB, though rarely consistently across a population. Specific polymorphisms are purported to interfere with BBB permeability and the drug delivery of specific CNS-acting medications and so can influence optimal medication dose based on BBB pharmacokinetics.
Medication molecules in the bloodstream encounter the endothelial BBB and, depending on the drug’s properties and whether it is a substrate for organic anion transporters (OATs) or organic cation transporters (OCTs), it may be actively transported from the bloodstream. This step is facilitated by active transport mechanisms against a concentration gradient. Numerous medications serve as substrates for organic anion or cation transport, benefiting from facilitated or expedited transport across endothelial cells at the BBB. Expressed in brain capillary endothelial cells forming the BBB, human organic anion transporting polypeptide 1A2 (OATP1A2) facilitates the uptake of various organic anions, including drugs, hormones, and toxins, from the bloodstream into the brain [2,3]. Notably, specific OATP1A2 variants, such as E184K, D185N, T259P, and D288N, have garnered clinical relevance, as highlighted in research by Wang et al. (2020[4]). Similarly, organic anion transporter 3 plays a crucial role in converting organic anions from the brain into the bloodstream. Located in the abluminal membrane of brain capillary endothelial cells, OAT3 contributes significantly to maintaining homeostasis in the central nervous system (CNS) [5]. Organic cation transporters 1 and 2 (OCT1 and OCT2) are also expressed in the BBB and brain parenchyma.
Once the drug enters the endothelial cells, it faces the tight junction barrier. Tight junction proteins (TJP), such as Claudin-5 and Occludin, restrict the paracellular movement of the drug between these cells. By sealing the intercellular gaps, TJP prevent the passive diffusion of large and hydrophilic molecules, including medications, from freely traversing between the bloodstream and brain tissue [6]. Claudin-5, the most abundant TJP in the BBB, has undergone extensive clinical investigation due to its critical role in maintaining barrier integrity. Polymorphisms in the CLDN5 gene, which encodes Claudin-5, have been scrutinised for their potential to alter BBB permeability and medication response [7]. Notably, four distinct CLDN-5 gene polymorphisms, including rs1042711, rs1042713, rs1800888, and rs1554115894, have emerged as subjects of interest in medication response research (ClinVar, [8]). However, further investigation is warranted to elucidate the precise implications of these genetic variations in clinical practice. More thoroughly investigated are the ATP binding cassette (ABC) transporters at the BBB—a family of active transporters highly expressed at the BBB and relevant to CNS medication bioavailability [1].
Active Transporters
Transport proteins, including efflux transporters like the ABCB1 gene encoding P-glycoprotein (P-gp or PGP), are embedded in the membranes of brain capillary endothelial cells. They actively pump specific molecules out of the brain and back into the bloodstream. When a drug molecule enters the endothelial cells from the bloodstream (via passive diffusion or transporters), efflux transporters like P-gp can recognise and transport the medication back into the bloodstream. This efflux mechanism helps protect the brain from potentially harmful substances and sometimes contributes to medication resistance. Genetic variations in the P-gp expression can influence the efflux transport function at the BBB, potentially affecting drug transport and permeability. ABCB1-deficent animals experience neurological and foetal drug toxicity attributed to a disruption to the area with prominent P-gp encoding genes, such as blood-brain and blood–placenta barriers [9]. Likewise, Abcb1a-/- knockout mice experiencing brain metastases exhibit successful responses to drug treatments that would typically face challenges penetrating the blood-brain barrier, such as paclitaxel. Notably, Abcb1a-/- knockout mice demonstrate brain-serum ratios for both risperidone and its active metabolite, 9-hydroxy risperidone, which are ten times higher than those observed in control mice. Furthermore, the double knockout mice, lacking both Abcb1a and Abcb1b, show brain-to-plasma ratios ranging from 1.1 to 2.6 times higher for various central nervous system medications than their wild-type counterparts [10].
Personalised and Precision Medicine
Pharmacological treatment of disease is a difficult process even for experienced clinicians following standard guidelines of gold-standard treatments, since patient factors alter drug pharmacodynamics and pharmacokinetics leading to unexpected issues with efficacy and tolerability. The rise of pharmacogenetics in medicine contributed to the emergence of personalised medicine and the more ambitious precision medicine, two innovative healthcare approaches that focus on customising medical treatments to fit each patient’s unique genetic and other individual characteristics [11]. Broadly, such approaches aim to create individualised treatment plans tailored to maximise drug responsiveness while minimising side effects without lengthy trial-and-error processes [12]. In psychiatry, treatment resistance is common. For example, 25-33% of those with schizophrenia are treatment resistant, necessitating third-line clozapine, which carries a significant burden of potentially serious side effects and mandates regular monitoring [13]. Likewise, standard targeted cancer treatments are difficult to maintain if effective, and the response reduces over time (for example, [14]). Many such responses are familial; Angst (1961)[15] first identified strong familial responses to antidepressant medications, later corroborated for lithium in bipolar disorder treatment [16] and antipsychotic response in schizophrenia [17,18]. Guided by such principles, researchers have attempted to compare pharmacogenetically-guided treatment to standardised treatment with some success, though few high-quality studies are available (see [19,20]).
2. Materials and Methods
Implicated Single Nucleotide Polymorphisms (SNPs)
To assist pharmacogenetic investigators, we have endeavoured to summarise as much of the existing clinical evidence related to pharmacogenetic factors related to BBB permeability and drug delivery. A search of the PubMed National Centre of Biotechnology Information reveals 29 human ABCB1 polymorphisms with potential drug response properties, which we list in Table 1 and subsequently describe.
3. Results
These polymorphisms in the ABCB1 gene are of interest in pharmacogenetics due to their potential to influence drug transport and response. The specific effects of each polymorphism can vary depending on the drug and the individual’s genetic background. Research continues exploring their clinical implications and relevance in optimising drug therapy for individual patients. Their proposed mechanism of action is illustrated in Figure 1.
Single Nucleotide Polymorphisms Linked to P-Glycoprotein Function
Several single nucleotide polymorphisms SNPs have been linked directly to active transporters, such as rs3842. It has been associated with improved survival rates in chronic myeloid leukemia patients treated with dasatinib [21], but not plasma concentrations of dilutegravir in HIV-positive patients [22]. Though there is some evidence that the gene is associated with efavirenz plasma concentration in Tanzanian and Ethiopian patients [23], there was no association observed in a Brazilian study of predominantly African ancestry [24]. Zaorska et al., (2021)[25] further established a link between rs1922240 and nephrotic syndrome, where the rare G allele is associated with the occurrence of childhood nephrotic syndrome, steroid dependence (for the AAC haplotype) and mesangial proliferative glomerulonephritis (wild A and AA alleles).
Similar impacts on plasma concentration and toxicity have been seen with rs1045642 although there are conflicting results. Higher methadone levels were highlighted as a potential risk factor during opioid replacement therapy by Iwersen-Bergmann et al. (2021)[26], linked to higher pain sensitivity by Zahari et al. (2017)[27] in Malay and as a protective factor for depression in a Chinese sample (Xie et al. 2015)[28]. This contrasts with a Japanese sample which demonstrated increased depression rates in carriers [29]. Though Menu et al. (2010)[30] found no impact on antidepressant therapy efficacy or tolerance, others found that a specific polymorphism of rs1045642-TT predicted lower effective doses of escitalopram and increased response from venlafaxine [31,32]. However, Kato et al. (2008)[33] suggested that carriers might have poorer responses to paroxetine, suggesting differential treatment responses based on genetic factors. Carriers are associated with higher clozapine serum concentrations with an associated body mass index increase [34], less fatigue and fewer sleep disorders in prolactin adenoma patients treated with cabergoline [35], higher rates of seizures but lower incidence of posterior reversible encephalopathy syndrome (PRES) in children with lymphatic leukemia undergoing treatment [36] and neuropsychiatric adverse reactions in oseltamivir-treated children with influenza H1N1/09 [37].
Extensive investigations have been carried out on the rs2032582 allele. Studies on a humanised mouse model with the 2677G>T mutation revealed no change in P-glycoprotein expression levels in brain capillary fractions, yet this mutation resulted in increased brain penetration of verapamil, a representative substrate of P-glycoprotein [38]. Moreover, placentas from mothers with the TT/TT genotype exhibited significantly reduced P-glycoprotein expression [39]. A correlation was also observed between the binding potential of verapamil and the dosage of T alleles [40], though two studies have found no link to donepezil efficacy in Swiss and Italian Alzheimer’s disease patients [41,42]. The allele has been associated with a higher likelihood of requiring increased methadone doses [43] and improved methadone plasma concentrations and treatment outcomes [44] in Taiwanese patients, thus influencing both the kinetics of methadone-P-glycoprotein interaction and methadone’s potency [45,46]. The need for higher doses of methadone was also reported in Han Chinese [47]. These data suggest the rs2032582 allele increases methadone potency via increasing BBB permeability, which is of considerable clinical significance given the high inter-individual variability in methadone response coupled with the significant toxicity of methadone in terms of cardiac and CNS effects, as well as potential drug-drug interactions via being a substrate for various CYP450 enzymes relevant to psychotropics (i.e. 2B6, 3A4, 2D6) [48].For antidepressants, the polymorphism significantly affects both citalopram plasma and cerebrospinal fluid concentrations [49]. The results are more conflicting for paroxetine, where it was associated with paroxetine response in a Japanese cohort [33] but not Swiss [50] or Slovakian cohorts [51].
In studies of antipsychotic medications and rs2032582, Geers et al. (2020)[52] found a protective effect against antipsychotic-induced hyperprolactinemia in a subgroup of schizophrenia patients treated with risperidone or paliperidone. Cho et al. (2010)[53] reported significantly higher pharmacokinetic parameters following levosulpiride administration, increased sleep duration was observed in Russian adolescents during episodes of psychosis [54], and Kuzman et al. (2008)[55] reported that women with schizophrenia were less prone to significant weight gain during risperidone treatment. Though Skogh et al. (2011)[56] demonstrated elevated serum and CSF olanzapine concentrations, Consoli et al. (2009)[57] noted lower clozapine concentrations, and Rafaniello et al. (2018)[58] found a lower aripiprazole concentration-to-dose ratio. Additional research has been carried out by Suzuki et al. (2014)[59]; CYP2D6-variant carriers had increased aripiprazole concentration and dose-ratios compared to non-carriers. These findings were corroborated by Belmonte et al. (2018)[60], Hattori et al. (2018)[61] and Koller et al. (2018) who identified that the variants rs1045642, rs2235048, rs1128503, rs2032582 as especially relevant[62]. on aripiprazole and by Xing et al. (2006)[63] and Yasui-Furukori et al. (2007)[64] on risperidone.
Zimprich et al. (2004)[65] reported a significant link between drug resistance and the rs2032582 allele in epilepsy patients, later confirmed by Hung et al. (2005)[66]. Though Vahab et al. (2009)[67] and Sun et al. (2016)[68] found no significant association between these genetic polymorphisms and antiepileptic drug resistance, Lovric et al. (2012)[69] observed higher lamotrigine concentrations in Croatian epilepsy patients with this polymorphism and Smolarz et al. (2017)[70] identified a significant association with drug-resistant epilepsy in the Polish population. Others separately reported associations between genetic variations and drug-resistant epilepsy in Mexican, Tunisian, Han Chinese, and Uygur populations, respectively [71,72,73,74].
Other indirect associations between BBB and drug response are observed. For example, there is a further association with increased drug response and decreased mortality in multiple myeloma patients [75] in rs2235013 carriers, increased cyclosporine levels in the months following heart transplant [76] and chemotherapy response and recurrence-free survival in late-stage lung cancer patients [77]. A similar treatment response in chemotherapy-treated stage III lung cancer has been seen for rs2235046, which is also associated with non-inflammatory Crohn’s disease in children [78] and ulcerative colitis in adults [79]. Finally, rs2235033 was not found to be associated with methotrexate response in halo-hematopoietic stem cell transplantation in paediatric patients with malignant haematological diseases [80].
SNPs Linked to Drug Transport
Examining the alleles associated with wider drug transport, Margier et al. (2019)[81] observed an association between rs868755 and increased plasma concentration of 25-hydroxycholecalciferol. Though there has been some evidence of an association between rs868755 carriers and methotrexate survival and toxicity in rheumatoid arthritis patients, this has been shown to be dependent on specific allele variants [82], and no association was found with drug resistance or sensitivity among children with refractory epilepsy [83]. Meanwhile, the rs1202168 variant is potentially related to the development of abnormal haline dispositions in mesial temporal lobe epilepsy [84] and increased risk of colorectal cancers in two predominantly Caucasian samples (German and Czech; [85]), but might be protective against colorectal cancers in German menopausal hormone replacement therapy patients [86].
Sági et al. (2021)[36] found an association between rs1128503 and higher rates of seizures and CNS relapse in children with lymphatic leukemia, particularly with the CC allele, which trends towards worse outcomes at six months compared to other variants, as reported by Cousar et al. (2013)[87]. Though investigated in several other settings, it has not been linked to methadone concentration [26], severe traumatic brain injury (TBI) recovery [87], escitalopram, venlafaxine [32] or paroxetine [33] efficacy. The ABCB1 genotypes of rs1922242 exhibited a significant association with the severity of depressive symptoms in major depressive disorder (MDD) patients who underwent continuous escitalopram treatment for 8 weeks [31]. More concerning is that women homozygous for the rs2214102 allele were found to be at a significantly increased breast cancer risk when taking combined estrogen-progestogen contraceptive pills [88]. Likewise, patients with breast cancer carrying the ancestral homozygous genotype (GG) had significantly worse progression-free survival than carriers of the non-ancestral allele [89].
A series of alleles, namely rs1211152, rs2214103, rs2235018, rs2235020 and rs2235074, have been investigated for tramadol response and some responses have been indicated, though no evidence has been provided to date. At least two genetic studies failed to detect or observe rs1211152 in their samples; one from Africa comprising Xhosa, Afrikaans, and English ancestry [90], and another from the United States [91]. Evidence from Dong et al. 2011 suggests an minor allele frequency of <2% among Mexican-American samples, whereas McMahon et al. (2010)[92] observed an MAF of around 9% in a German sample of European ancestry. By comparison, rs2235020 has been associated with improved rates of remission of MDD in a sample of Mexican Americans treated with fluoxetine [93], and rs2235074 is potentially related by haploblock to xenobiotic efflux in myeloma [94].
The rs2235035 allele has been observed as associated with increased daunorubicinol clearance in a paediatric oncology sample [95] and with atorvastatin pharmacokinetics and lipid-lowering response in a healthy Korean sample [96]. While rs3213619 has been associated with grade two neurotoxicity [97], it was not associated with survival or prognosis in adriamycin cancer patients treated with taxane-containing regimens [98]. The variant is also potentially protective against paclitaxel-induced peripheral neuropathy [99], particularly in breast cancer [100].
Louis et al. (2022)[101] have reported an associated decreased seizure occurrence after surgical resections for drug-resistant temporal epilepsy in people with rs10276036. Furthermore, Caronia et al. (2011)[102] found a strong association between the genotype and increased five-year survival rates in osteosarcoma patients treated with a combination of cisplatin, adriamycin, methotrexate, vincristine, and cyclophosphamide, suggesting that the genetic marker might have some prognostic value in cancer treatment. Similarly, Weissfeld et al. (2014)[77] reported an association between the genotype and increased survival and disease-free status at four years post-diagnosis in stage III-IV lung cancer patients treated with chemotherapy, suggesting potential implications for treatment outcomes and prognosis in lung cancer patients. However, genotype TT is strongly associated with an increased risk of nevirapine drug hypersensitivity in people with HIV infections [103,104].
Despite extensive research, most studies have not demonstrated an association between rs2032588 and psychotropic response or side effect profile. A large (n=789) naturalistic Dutch cohort study demonstrated a reduction of PGP-dependent antidepressant (citalopram, venlafaxine, paroxetine, fluvoxamine) side effects [105]. Additionally, a Jordanian cross-sectional study found an association between rs2032588 and anticonvulsant drug resistance in a cohort of 86 Jordanian men, but not women, with epilepsy [106]. Rs2032588 is much more prevalent in African populations (~18%) compared with European (~6%), and virtually absent in Asian populations [107].
SNPs Linked to Drug Response and Pharmacokinetics
Limited research appears to have been conducted for the SNPs, such as rs2888599, associated with drug response except in tramadol as carried out by the Bruce Budowle Laboratory (University of North Texas Health Science Center;[108]), though results do not appear to have been published yet. The presence of rs4148727 was not associated with an increased risk of ischaemic stroke in a South Korean sample but was associated with reduced severity [109]. Some evidence suggests that the SNP is associated with the lipid profile in type II diabetes mellitus, most strongly for apolipoprotein-A and triglycerides, with likely implications for statin management in the condition [110]. No significant association was observed for an improvement in clopidogrel efficacy compared to aspirin for stroke prevention in a large Chinese sample of high-risk patients [111]. Unfortunately, rs13237132 has no available evidence directly addressing drug response in this SNP, though despite some earlier findings, it does not appear to be associated with ovarian cancer outcomes [112], particularly when treated with taxane [113].
This is similar to rs9282564, which has had several investigations, though little corroborating findings from the clinical literature. Indirect evidence suggests that the SNP might be protective against opioid overdose ([114]). However, children undergoing tonsillectomy using intravenous morphine with GG and GA genotypes of ABCB1 polymorphism rs9282564 had higher risks of opioid-related respiratory depression, [115]). Additionally, Ray et al. (2015)[116] found an association between the SNP and a greater likelihood and faster remission of MDD with sertraline treatment. However, Sánchez-Lázaro et al. (2015)[117] reported an association between the SNP and significantly lower renal function after heart transplantation when treated with calcineurin inhibitors (tacrolimus or cyclosporine), which could be a potential risk factor for adverse outcomes in transplant patients. Burgueño-Rodríguez et al. (2023)[118] identified an association between the SNP and increased risk of neurotoxicity in paediatric acute lymphoblastic leukemia patients treated with prednisone, vincristine, L-asparaginase, daunorubicin, and methotrexate, indicating potential limitations or risks associated with this treatment regimen.
SNPs with Limited Available Information
Even less is known about the associated function of rs2235015, which has been found to be unrelated to side effects of treatment with cabergoline in patients with prolactinomas [35]. Inpatients with MDD who were homozygous GG/TT carriers had an inverse association between medication dosage and hospital stay [119]. However, no association with the polymorphism was observed for symptom severity, and this finding was corroborated in a larger naturalised cohort study of Dutch participants with depressive or anxious disorders [120]. More recent examinations suggest a negative association with depressive symptoms after at least two weeks of antidepressant treatment [121]. The mixed evidence is summarised best by the systematic review and meta-analysis by Magarbeh et al. (2023)[122], who found little robust evidence of an association in antidepressant treatment efficacy for outpatients. Otherwise, Silberbauer et al. (2022)[123] observed that the presence of the minor allele A (or AC) is associated with lower serotonin transporter occupancy than those with the major allele. Though investigated, it further appears to be unrelated to sexual dysfunction in women taking SSRIs for depression [124].
Though rs58898486 has been associated with an increased risk of MDD in Mexican-Americans, the researchers do not appear to have included the SNP in their investigation of antidepressant response [93]. Finally, there is no available evidence directly addressing drug response in rs55852620 beyond being investigated for the previously mentioned tramadol drug response.
4. Discussion
Our review has attempted to summarise a considerable body of work into the pharmacogenetics of the BBB and drug delivery in hopes of assisting future research into personalised medicine. Tailoring medicine to the individual by accounting for genetic variation in the permeability of the BBB holds a great deal of promise, particularly within oncology and psychiatry. A slim majority of the identified SNPs (15/29) have been investigated for treatment response or survival in various cancer populations, with more than a handful of clinically relevant findings. The SNP rs2032582 was linked to reduced control of acute emesis in breast cancer patients treated with granisetron [125]. Similarly, rs2214102 was associated with increased breast cancer risk and worse progression-free survival ([88,89]. In contrast, rs2235013 showed increased drug response and better progression-free survival in multiple myeloma and late-stage lung cancer patients [75,77]. Rs2235046 was associated with improved treatment response and disease-free survival in stage III lung cancer patients [77], and rs10276036 correlated with improved survival rates in osteosarcoma and lung cancer patients treated with chemotherapy [77,102]. Otherwise, rs2235035 was linked to increased daunorubicinol clearance in pediatric oncology samples [95], and rs3213619 showed associations with neurotoxicity and potential protection against peripheral neuropathy, though with no clear impact on survival in certain cancer patients ([97,98,99,100]. Finally, rs9282564 was associated with increased neurotoxicity risk in pediatric acute lymphoblastic leukemia patients [118].
Investigation into psychiatric or neurological intervention was widespread and heterogeneous, though we observed numerous clinically meaningful findings. Studies investigating the impact of ABCB1 variants on psychotropic therapy have yielded varied results. For example, Chang et al. (2015)[126] found that MDD patients with the ABCB1G2677T polymorphism exhibited differential responses to antidepressant treatment, while Kato et al. (2009)[33] observed a significant association between the G2677T/A polymorphism and paroxetine response in a Japanese cohort of major depression. Elsewhere, methadone maintenance treatment was associated with decreased risk of MDD in Chinese populations carrying rs1045642 [28]. Conversely, Shan et al. (2019)[127] found no correlation between ABCB1 polymorphisms and response to SSRIs and SNRIs in the Chinese population, and Singh et al. (2011)[32] found no evidence of association with symptom remission or medication effectiveness in MDD patients treated with escitalopram, venlafaxine, and paroxetine. Fujii et al. (2012)[29] suggested no direct association with MDD in Japanese populations, but a combination of rs1128503 and rs1045642 variants may increase susceptibility. Beyond depressive disorders and these two SNPs, considerable effort has been made to identify clinically relevant findings for varied conditions such as epilepsy and TBI, among many others. For example, evidence remains mixed but optimistic on the association between drug resistance in epilepsy patients and a haplotype comprising genetic variations (for example, C1236T, C3435T, and G2677T/A; [65,66]).
Implications and Next Steps
As the field of hepatic pharmacogenetics gains wider clinical adoption in psychiatry, we are of the considered view that the addition of ABC transporter variants has the scope to enhance dose optimisation. As many psychotropic medications are substrates for active efflux by ABC transporters such as ABCB1, the addition of such variants to phase I hepatic metabolism variants stands to enhance the accuracy of psychotropic pharmacogenetics for dose finding. Further basic and clinical studies will help pave the way to the future enhancement of psychotropic pharmacogenetics.
Author Contributions
Conceptualization, D.R.S. and A.S; methodology, investigation, writing—original draft preparation, review, and editing, All authors; visualization, R.M.L. All authors have read and agreed to the published version of the manuscript.
Funding
The authors have received no funding relevant to this review. DRS is supported by the NHRMC Medical Research Future Fund (APP1200214; 2021609).
Conflicts of Interest
AS has equity in CNSDose, an Australian DNA lab that performs pharmacogenetic analysis. All other authors declare that they have no conflicts of interest.
References
- D. Wu, Q. Chen, X. Chen, F. Han, Z. Chen and Y. Wang, Signal Transduct Target Ther, 2023, 8, 217–217.
- A. Kalliokoski and M. Niemi, Br J Pharmacol, 2009, 158, 693–705.
- Y. Zhou, J. Yuan, Z. Li, Z. Wang, D. Cheng, Y. Du, W. Li, Q. Kan and W. Zhang, Pharmacology, 2015, 95, 201–208.
- J. Wang, J. J. Wang, J. Yin, W. Li, C. Xiao, J. Han and F. Zhou, Journal of Biochemical and Molecular Toxicology, 2020, 34.
- A. R. Erdman, L. M. Mangravite, T. J. Urban, L. L. Lagpacan, R. A. Castro, M. de la Cruz, W. Chan, C. C. Huang, S. J. Johns, M. Kawamoto, D. Stryke, T. R. Taylor, E. J. Carlson, T. E. Ferrin, C. M. Brett, E. G. Burchard and K. M. Giacomini, American Journal of Physiology-Renal Physiology, 2006, 290, F905–F912.
- W. -Y. Liu, Z.-B. Wang, L.-C. Zhang, X. Wei and L. Li, CNS Neurosci Ther, 2012, 18, 609–615.
- C. Greene, N. Hanley and M. Campbell, Fluids Barriers CNS, 2019, 16, 3–3.
- N. C. f. B. Information, ClinVar, [VCV000828556.2], https://www.ncbi.nlm.nih.gov/clinvar/variation/VCV000828556.2.
- L. M. Hodges, S. M. Markova, L. W. Chinn, J. M. Gow, D. L. Kroetz, T. E. Klein and R. B. Altman, Pharmacogenetics and genomics, 2011, 21, 152–161.
- T. M. Sissung, C. E. Baum, C. T. Kirkland, R. Gao, E. R. Gardner and W. D. Figg, Mol Biotechnol, 2010, 44, 152–167.
- E. A. Ashley, Nature Reviews Genetics, 2016, 17, 507–522.
- A. M. Vicente, W. Ballensiefen and J.-I. Jönsson, J Transl Med, 2020, 18, 180–180.
- D. Siskind, V. Siskind and S. Kisely, Can J Psychiatry, 2017, 62, 772–777.
- M. Wang, R. S. Herbst and C. Boshoff, Nature Medicine, 2021, 27, 1345–1356.
- J. Angst, Psychopharmacologia, 1961, 2, 381–407.
- P. Grof, A. Duffy, P. Cavazzoni, E. Grof, J. Garnham, M. MacDougall, C. O’Donovan and M. Alda, The Journal of Clinical Psychiatry, 2002, 63, 942–947.
- M. J. Arranz and J. de Leon, Molecular Psychiatry, 2007, 12, 707–747.
- M. J. Arranz, M. Rivera and J. C. Munro, CNS Drugs, 2011, 25, 933–969.
- V. David, B. Fylan, E. Bryant, H. Smith, G. S. Sagoo and M. Rattray, Front Genet, 2021, 12, 698148–698148.
- J. O’Shea, M. Ledwidge, J. Gallagher, C. Keenan and C. Ryan, The pharmacogenomics journal, 2022, 22, 89–99.
- A. M. Madejczyk, F. Canzian, J. Góra-Tybor, D. Campa, T. Sacha, D. Link-Lenczowska, I. Florek, W. Prejzner, M. Całbecka, M. Rymko, M. Dudziński, M. J. Orzechowska and K. Jamroziak, Front Oncol, 2022, 12, 952640–952640.
- K. Tsuchiya, T. Hayashida, A. Hamada, S. Oki, S. Oka and H. Gatanaga, Pharmacogenetics and Genomics, 2017, 27, 416–419.
- E. Ngaimisi, A. Habtewold, O. Minzi, E. Makonnen, S. Mugusi, W. Amogne, G. Yimer, K.-D. Riedel, M. Janabi, G. Aderaye, F. Mugusi, L. Bertilsson, E. Aklillu and J. Burhenne, PLoS One, 2013, 8, e67946–e67946.
- A. V. C. Coelho, S. P. S. Silva, L. C. A. de Alencar, G. Stocco, S. Crovella, L. A. C. Brandão and R. L. Guimarães, The Journal of Clinical Pharmacology, 2013, 53, 1286–1293.
- K. Zaorska, P. Zawierucha, M. Świerczewska, D. Ostalska-Nowicka, J. Zachwieja and M. Nowicki, J Transl Med, 2021, 19, 130–130.
- S. Iwersen-Bergmann, S. Plattner, S. Hischke, A. Müller, H. Andresen-Streichert, H. Jungen, R. Erb and B. Beer-Sandner, Int J Legal Med, 2021, 135, 473–482.
- Z. Zahari, C. S. Lee, M. A. Ibrahim, N. Musa, M. A. Mohd Yasin, Y. Y. Lee, S. C. Tan, N. Mohamad and R. Ismail, Nursing Research, 2017, 66, 134–144.
- W. -W. Xie, L. Zhang, R.-R. Wu, Y. Yu, J.-P. Zhao and L.-H. Li, Neuropsychiatr Dis Treat, 2015, 11, 1967–1971.
- T. Fujii, M. Ota, H. Hori, D. Sasayama, K. Hattori, T. Teraishi, N. Yamamoto, M. Hashikura, M. Tatsumi, T. Higuchi and H. Kunugi, Journal of Psychiatric Research, 2012, 46, 555–559.
- P. Menu, F. Gressier, C. Verstuyft, P. Hardy, L. Becquemont and E. Corruble, Neuropsychobiology, 2010, 62, 193–197.
- K. -M. Lin, Y.-F. Chiu, I. J. Tsai, C.-H. Chen, W. W. Shen, S. C. Liu, S.-C. Lu, C.-Y. Liu, M.-C. Hsiao, H.-S. Tang, S.-I. Liu, L.-H. Chang, C.-S. Wu, H.-H. Tsou, M.-H. Tsai, C.-Y. Chen, S.-M. Wang, H.-W. Kuo, Y.-T. Hsu and Y.-L. Liu, Pharmacogenetics and Genomics, 2011, 21, 163–170.
- A. B. Singh, C. A. Bousman, C. H. Ng, K. Byron and M. Berk, Transl Psychiatry, 2012, 2, e198–e198.
- M. Kato, T. Fukuda, A. Serretti, M. Wakeno, G. Okugawa, Y. Ikenaga, Y. Hosoi, Y. Takekita, L. Mandelli, J. Azuma and T. Kinoshita, Progress in Neuro-Psychopharmacology and Biological Psychiatry, 2008, 32, 398–404.
- Piatkov, D. Caetano, Y. Assur, S. L. Lau, T. Jones, S. C. Boyages and M. McLean, Pharmgenomics Pers Med, 2017, 10, 235–242. [Google Scholar]
- A. P. Athanasoulia, C. Sievers, M. Ising, A. C. Brockhaus, A. Yassouridis, G. K. Stalla and M. Uhr, European Journal of Endocrinology, 2012, 167, 327–335.
- C. Sági, A. Gézsi, B. Egyed, Z. Jakab, N. Benedek, A. Attarbaschi, S. Köhrer, J. Sipek, L. Winkowska, M. Zaliova, S. Anastasopoulou, B. O. Wolthers, S. Ranta, C. Szalai, G. T. Kovács, Á. F. Semsei and D. J. Erdélyi, Cancers (Basel), 2021, 13, 2333.
- G. L‘Huillier, K. Ing Lorenzini, P.-A. Crisinel, M. C. Rebsamen, J. Fluss, C. M. Korff, R. P. Barbe, C.-A. Siegrist, P. Dayer, K. M. Posfay-Barbe and J. A. Desmeules, Pharmacogenomics, 2011, 12, 1493–1501.
- Y. Yamasaki, T. Moriwaki, S. Ogata, S. Ito, S. Ohtsuki, G. Minegishi, S. Abe, Y. Ohta, K. Kazuki, K. Kobayashi and Y. Kazuki, Pharmacogenetics and Genomics, 2022, 32, 288–292.
- M. Hitzl, E. Schaeffeler, B. Hocher, T. Slowinski, H. Halle, M. Eichelbaum, P. Kaufmann, P. Fritz, M. F. Fromm and M. Schwab, Pharmacogenetics, 2004, 14, 309–318.
- D. M. van Assema, M. Lubberink, P. Rizzu, J. C. van Swieten, R. C. Schuit, J. Eriksson, P. Scheltens, M. Koepp, A. A. Lammertsma and B. N. van Berckel, EJNMMI Res, 2012, 2, 57–57.
- Magliulo, M.-L. Dahl, G. Lombardi, S. Fallarini, L. M. Villa, A. Biolcati and M. G. Scordo, European Journal of Clinical Pharmacology, 2010, 67, 47–54. [Google Scholar]
- Noetzli, M. Guidi, K. Ebbing, S. Eyer, L. Wilhelm, A. Michon, V. Thomazic, I. Stancu, A.-M. Alnawaqil, C. Bula, S. Zumbach, M. Gaillard, P. Giannakopoulos, A. von Gunten, C. Csajka and C. B. Eap, Br J Clin Pharmacol, 2014, 78, 135–144. [Google Scholar]
- A. Levran, K. O’Hara, E. Peles, D. Li, S. Barral, B. Ray, L. Borg, J. Ott, M. Adelson and M. J. Kreek, Hum Mol Genet, 2008, 17, 2219–2227.
- H. -Y. Lee, J.-H. Li, Y.-L. Sheu, H.-P. Tang, W.-C. Chang, T.-C. Tang, Y.-C. Yeh, S.-Y. Wang and R.-H. Liu, Biomed Res Int, 2013, 2013, 741403–741403.
- J. Coller, D. Barratt, K. Dahlen, M. Loennechen and A. Somogyi, Clinical Pharmacology & Therapeutics, 2006, 80, 682–690.
- C. -C. Hung, M.-H. Chiou, Y.-N. Teng, Y.-W. Hsieh, C.-L. Huang and H.-Y. Lane, PLoS One, 2013, 8, e59419–e59419.
- C. -C. Hung, M.-H. Chiou, B.-H. Huang, Y.-W. Hsieh, T.-J. Hsieh, C.-L. Huang and H.-Y. Lane, Pharmacogenomics, 2011, 12, 1525–1533.
- D. Kreutzwiser and Q. A. Tawfic, CNS drugs, 2020, 34, 827–839.
- G. Nikisch, C. Eap and P. Baumann, Pharmacological Research, 2008, 58, 344–347.
- Gex-Fabry, C. B. Eap, B. Oneda, N. Gervasoni, J.-M. Aubry, G. Bondolfi and G. Bertschy, Therapeutic Drug Monitoring, 2008, 30, 474–482. [Google Scholar]
- Z. Vancova, M. Cizmarikova, J. Dragasek, S. Zofcakova, P. Kolarcik and J. Mojzis, Med Sci Monit, 2018, 24, 3136–3145.
- L. M. Geers, I. V. Pozhidaev, S. A. Ivanova, M. B. Freidin, A. F. Schmidt, D. Cohen, A. S. Boiko, D. Z. Paderina, O. Y. Fedorenko, A. V. Semke, N. A. Bokhan, B. Wilffert, J. G. W. Kosterink, D. J. Touw and A. J. M. Loonen, Br J Clin Pharmacol, 2020, 86, 1827–1835.
- H. Y. Cho, H. D. Yoo and Y. B. Lee, Neuroscience, 2010, 169, 378–387.
- D. V. Ivashchenko, S. Z. Khoang, B. V. Makhmudova, N. I. Buromskaya, P. V. Shimanov, R. V. Deitch, K. A. Akmalova, G. N. Shuev, I. V. Dorina, M. I. Nastovich, E. N. Shagovenko, E. A. Grishina, L. M. Savchenko, Y. S. Shevchenko and D. A. Sychev, Drug Metabolism and Drug Interactions, 2020, 35.
- R. Kuzman, V. Medved, N. Bozina, L. Hotujac, I. Sain and H. Bilusic, Psychiatry Research, 2008, 160, 308–315.
- E. Skogh, I. Sjödin, M. Josefsson and M.-L. Dahl, Journal of Clinical Psychopharmacology, 2011, 31, 4–9.
- G. Consoli, M. Lastella, A. Ciapparelli, M. C. Dell‘Osso, L. Ciofi, E. Guidotti, R. Danesi, L. Dell‘Osso, M. Del Tacca and A. Di Paolo, Pharmacogenomics, 2009, 10, 1267–1276.
- Rafaniello, M. Sessa, F. F. Bernardi, M. Pozzi, S. Cheli, D. Cattaneo, S. Baldelli, M. Molteni, R. Bernardini, F. Rossi, E. Clementi, C. Bravaccio, S. Radice and A. Capuano, The Pharmacogenomics Journal, 2017, 18, 422–430. [Google Scholar]
- T. Suzuki, K. Mihara, A. Nakamura, S. Kagawa, G. Nagai, K. Nemoto and T. Kondo, Therapeutic Drug Monitoring, 2014, 36, 651–655.
- Belmonte, D. Ochoa, M. Román, M. Saiz-Rodríguez, A. Wojnicz, C. I. Gómez-Sánchez, S. Martín-Vílchez and F. Abad-Santos, Basic & Clinical Pharmacology & Toxicology, 2018, 122, 596–605. [Google Scholar]
- S. Hattori, A. Suda, I. Kishida, M. Miyauchi, Y. Shiraishi, M. Fujibayashi, N. Tsujita, C. Ishii, N. Ishii, T. Moritani, M. Taguri and Y. Hirayasu, BMC Psychiatry, 2018, 18, 231–231.
- Koller, C. Belmonte, R. Lubomirov, M. Saiz-Rodríguez, P. Zubiaur, M. Román, D. Ochoa, A. Carcas, A. Wojnicz and F. Abad-Santos, Journal of Psychopharmacology, 2018, 32, 1212–1222. [Google Scholar]
- Q. Xing, R. Gao, H. Li, G. Feng, M. Xu, S. Duan, J. Meng, A. Zhang, S. Qin and L. He, Pharmacogenomics, 2006, 7, 987–993.
- Yasui-Furukori, S. Tsuchimine, M. Saito, T. Nakagami, Y. Sato and S. Kaneko, Progress in Neuro-Psychopharmacology and Biological Psychiatry, 2007, 31, 1230–1234. [Google Scholar] [CrossRef] [PubMed]
- Zimprich, R. Sunder-Plassmann, E. Stogmann, A. Gleiss, A. Dal-Bianco, A. Zimprich, S. Plumer, C. Baumgartner and C. Mannhalter, Neurology, 2004, 63, 1087–1089. [Google Scholar]
- C. -C. Hung, J. J. Tai, C.-J. Lin, M.-J. Lee and H.-H. Liou, Pharmacogenomics, 2005, 6, 411–417.
- S. A. Vahab, S. Sen, N. Ravindran, S. Mony, A. Mathew, N. Vijayan, G. Nayak, N. Bhaskaranand, M. Banerjee and K. Satyamoorthy, Drug Metabolism and Pharmacokinetics, 2009, 24, 255–260.
- Sun, B.-Q. Cao, B. Wang, S.-Q. Wu and D.-H. Jiang, Exp Ther Med, 2016, 12, 1780–1784. [Google Scholar] [CrossRef]
- M. Lovrić, N. Božina, S. Hajnšek, M. R. Kuzman, D. Sporiš, Z. Lalić, T. Božina and P. Granić, Therapeutic Drug Monitoring, 2012, 34, 518–525.
- B. Smolarz, D. Skalski, A. Rysz, A. Marchel, H. Romanowicz and M. Makowska, Acta Neurologica Belgica, 2017, 117, 849–855.
- M. Chouchi, H. Klaa, I. Ben-Youssef Turki and L. Hila, Dis Markers, 2019, 2019, 1343650–1343650.
- D. Escalante-Santiago, I. A. Feria-Romero, R. M. Ribas-Aparicio, D. Rayo-Mares, P. Fagiolino, M. Vázquez, C. Escamilla-Núñez, I. Grijalva-Otero, M. A. López-García and S. Orozco-Suárez, Front Neurol, 2014, 5, 184–184.
- Kwan, V. Wong, P. W. Ng, C. H. T. Lui, N. C. Sin, W. S. Poon, H. K. Ng, K. S. Wong and L. Baum, Pharmacogenomics, 2009, 10, 723–732. [Google Scholar]
- T. Zhao, H.-J. Li, J. Feng, H.-L. Zhang, W. Ting-Ting, L. Ma, J. Yu, W.-B. Zhao, L. Sun, L.-H. Yu and Y. Sun, Therapeutic drug monitoring, 2022, 44, 455–464.
- A. Macauda, E. Castelli, G. Buda, M. Pelosini, A. Butrym, M. Watek, M. Kruszewski, A. J. Vangsted, M. Rymko, K. Jamroziak, N. Abildgaard, E. K. Haastrup, G. Mazur, R. Ríos, A. Jurczyszyn, D. Zawirska, M. Dudziński, M. Raźny, M. Dutka, W. Tomczak, A. Suska, A. Druzd-Sitek, H. Marques, M. Petrini, M. Markiewicz, J. Martinez-Lopez, L. H. Ebbesen, E. Iskierka-Jażdżewska, J. Sainz, F. Canzian and D. Campa, British Journal of Haematology, 2018, 183, 375–384.
- A.J. de Luna, M. H. Cervera, I. S. Lázaro, L. A. Bonet, J. P. Andrés and S. A. Pellicer, 2011.
- J. L. Weissfeld, B. Diergaarde, T. Nukui, S. Buch, A. Pennathur, M. A. Socinski, J. M. Siegfried and M. Romkes, J Thorac Oncol, 2014, 9, 1264–1271.
- A. Krupoves, E. G. Seidman, D. Mack, D. Israel, K. Morgan, P. Lambrette, I. Costea, C. Deslandres, G. Grimard, L. Law, E. Levy and D. K. Amre, Inflammatory Bowel Diseases, 2009, 15, 900–908.
- A. Huebner, B. L. Browning, I. Petermann, D. Y. Han, M. Philpott, M. Barclay, R. Gearry, A. McCulloch, P. Demmers and L. R. Ferguson, Inflammatory Bowel Diseases, 2009, 15, 1784–1793.
- Ji, Y. Zhang, Y. Hu, L. Liu, S. Cao, L. Gao, B. Li, Y. Tian, L. Kong, S. Wu, J. Ling, P. Xiao, J. Lu, J. Li, Y. Yao, J. Qin and S. Hu, Blood, 2023, 142, 6960–6960. [Google Scholar]
- M. Margier, X. Collet, C. May, C. Desmarchelier, F. André, C. Lebrun, C. Defoort, A. Bluteau, P. Borel, A. Lespine and E. Reboul, The FASEB Journal, 2018, 33, 2084–2094.
- P. Moya, J. Salazar, M. J. Arranz, C. Díaz-Torné, E. del Río, J. Casademont, H. Corominas and M. Baiget, Pharmacogenomics, 2015, 17, 25–29.
- L. Gao, X. Yin, Y. Li, H. Xiao, L. Yang, H. Fan, H. Qi, J. Zhang, J. Feng and F. Zheng, Zhonghua yi xue yi Chuan xue za zhi= Zhonghua Yixue Yichuanxue Zazhi= Chinese Journal of Medical Genetics, 2019, 36, 1073–1076.
- A.Das, S. Balan, A. Mathew, V. Radhakrishnan, M. Banerjee and K. Radhakrishnan, Indian J Hum Genet, 2011, 17 Suppl 1, S41-S47.
- D. Campa, J. Sainz, B. Pardini, L. Vodickova, A. Naccarati, A. Rudolph, J. Novotny, A. Försti, S. Buch, W. von Schönfels, C. Schafmayer, H. Völzke, M. Hoffmeister, B. Frank, R. Barale, K. Hemminki, J. Hampe, J. Chang-Claude, H. Brenner, P. Vodicka and F. Canzian, PLoS One, 2012, 7, e32784–e32784.
- A. Rudolph, J. Sainz, R. Hein, M. Hoffmeister, B. Frank, A. Forsti, H. Brenner, K. Hemminki and J. Chang-Claude, Endocrine Related Cancer, 2011, 18, 371–384.
- J. m. L. Cousar, Y. P. Conley, F. A. Willyerd, A. A. Sarnaik, A. M. Puccio, P. E. Empey, P. M. Kochanek, M. J. Bell, D. O. Okonkwo and R. S. B. Clark, Neurocrit Care, 2013, 19, 192–198.
- Breast Cancer Research and Treatment, 2009, 120, 727-736.
- Vaclavikova, M. Ehrlichova, I. Hlavata, V. Pecha, R. Kozevnikovova, M. Trnkova, J. Adamek, H. Edvardsen, V. N. Kristensen, I. Gut and P. Soucek, Clinical Chemistry and Laboratory Medicine (CCLM), 2012, 50, 1999–2007. [Google Scholar]
- A. Ikediobi, B. Aouizerat, Y. Xiao, M. Gandhi, S. Gebhardt and L. Warnich, Hum Genomics, 2011, 5, 265–282.
- J. Ma, J. Divers, N. D. Palmer, B. A. Julian, A. K. Israni, D. Schladt, S. O. Pastan, K. Chattrabhuti, M. D. Gautreaux, V. Hauptfeld, R. A. Bray, A. D. Kirk, W. M. Brown, R. S. Gaston, J. Rogers, A. C. Farney, G. Orlando, R. J. Stratta, M. Guan, A. Palanisamy, A. M. Reeves-Daniel, D. W. Bowden, C. D. Langefeld, P. J. Hicks, L. Ma and B. I. Freedman, Kidney Int, 2015, 88, 584–592.
- J. McMahon, N. Akula, T. G. Schulze, P. Muglia, F. Tozzi, S. D. Detera-Wadleigh, C. J. M. Steele, R. Breuer, J. Strohmaier, J. R. Wendland, M. Mattheisen, T. W. Mühleisen, W. Maier, M. M. Nöthen, S. Cichon, A. Farmer, J. B. Vincent, F. Holsboer, M. Preisig, M. Rietschel and C. Bipolar Disorder Genome Study, Nat Genet, 2010, 42, 128–131.
- C. Dong, M. L. Wong and J. Licinio, Molecular psychiatry, 2009, 14, 1105–1118.
- A. Martino, D. Campa, G. Buda, J. Sainz, R. García-Sanz, K. Jamroziak, R. M. Reis, N. Weinhold, M. Jurado, R. Ríos, Z. Szemraj-Rogucka, H. Marques, J. Szemraj, A. Stein, R. Kumar, E. Orciuolo, F. Gemignani, S. Landi, H. Goldschmidt, M. Petrini, C. Dumontet, F. Canzian and A. M. Rossi, Leukemia, 2011, 26, 1419–1422.
- P. Thompson, H. E. Wheeler, S. M. Delaney, R. Lorier, U. Broeckel, M. Devidas, G. H. Reaman, K. Scorsone, L. Sung, M. E. Dolan and S. L. Berg, Cancer Chemother Pharmacol, 2014, 74, 831–838.
- I. Woo, S. R. Kim, W. Huh, J.-W. Ko and S.-Y. Lee, Drug Des Devel Ther, 2017, 11, 1135–1146.
- Y. Yang, J. Jia, Z. Sun, C. Liu, Z. Li, Y. Xiao, J. Yu, F. Du, Y. Shi, J. Sun, J. Shui and X. Zhang, Future Oncology, 2021, 17, 2351–2363.
- Z. Sun, X. Yang, F. Du, Y. Shi, J. Sun, J. Jia, C. Liu, Y. Xiao, J. Yu, X. Zhang and Y. Yang, The Journal of Gene Medicine, 2022, 24.
- G. K. Boora, R. Kanwar, A. A. Kulkarni, A. Abyzov, J. Sloan, K. J. Ruddy, M. S. Banck, C. L. Loprinzi and A. S. Beutler, Cancer Med, 2016, 5, 631–639.
- E. Abraham, Q. Guo, L. Dorling, J. Tyrer, S. Ingle, R. Hardy, A.-L. Vallier, L. Hiller, R. Burns, L. Jones, S. J. Bowden, J. A. Dunn, C. J. Poole, C. Caldas, P. P. D. Pharoah and H. M. Earl, Clinical Cancer Research, 2014, 20, 2466–2475.
- Louis, R. M. Busch, D. Lal, J. Hockings, O. Hogue, M. Morita-Sherman, D. Vegh, I. Najm, C. Ghosh, P. Bazeley, C. Eng, L. Jehi and D. M. Rotroff, Front Neurol, 2022, 13, 942643–942643. [Google Scholar]
- D. Caronia, A. Patiño-Garcia, A. Peréz-Martínez, G. Pita, L. T. Moreno, M. Zalacain-Díez, B. Molina, I. Colmenero, L. Sierrasesúmaga, J. Benítez and A. Gonzalez-Neira, PLoS One, 2011, 6, e26091–e26091.
- M. Dhoro, B. Ngara, G. Kadzirange, C. Nhachi and C. Masimirembwa, Current HIV Research, 2014, 11, 481–490.
- M. Dhoro, S. Zvada, B. Ngara, C. Nhachi, G. Kadzirange, P. Chonzi and C. Masimirembwa, BMC Pharmacol Toxicol, 2015, 16, 4–4.
- P. M. Bet, E. C. Verbeek, Y. Milaneschi, D. B. Straver, T. Uithuisje, M. R. Bevova, J. G. Hugtenburg, P. Heutink, B. W. Penninx and W. J. Hoogendijk, The pharmacogenomics journal, 2016, 16, 202–208.
- R. Abduljabbar, T. D. Eid, A.-M. Yousef, S. R. Mukred and M. Zawiah, Journal of Medical Biochemistry, 2023, 42, 214.
- G. P. Consortium, A. Auton, L. Brooks, R. Durbin, E. Garrison and H. Kang, Nature, 2015, 526, 68–74.
- o. N. T. H. S. Center.
- Y. -O. Kim, S.-Y. Kim, D. H. Yun and S.-W. Lee, Exp Neurobiol, 2012, 21, 164–171.
- Wu, X. Wang, H. Chen, R. Yang, H. Yu, Y. Wu and Y. Hu, Metabolites, 2022, 12, 875. [Google Scholar]
- Y. Pan, W. Chen, Y. Wang, H. Li, S. C. Johnston, T. Simon, X. Zhao, L. Liu, D. Wang, X. Meng, Y. Wang and I. Clopidogrel in High-Risk Patients With Acute Nondisabling Cerebrovascular Events, JAMA Neurol, 2019, 76, 552–560.
- L. White, R. A. Vierkant, Z. C. Fogarty, B. Charbonneau, M. S. Block, P. D. P. Pharoah, G. Chenevix-Trench, A. A. C. S. g. for, M. A. Rossing, D. W. Cramer, C. L. Pearce, J. M. Schildkraut, U. Menon, S. K. Kjaer, D. A. Levine, J. Gronwald, H. A. Culver, A. S. Whittemore, B. Y. Karlan, D. Lambrechts, N. Wentzensen, J. Kupryjanczyk, J. Chang-Claude, E. V. Bandera, E. Hogdall, F. Heitz, S. B. Kaye, P. A. Fasching, I. Campbell, M. T. Goodman, T. Pejovic, Y. Bean, G. Lurie, D. Eccles, A. Hein, M. W. Beckmann, A. B. Ekici, J. Paul, R. Brown, J. M. Flanagan, P. Harter, A. du Bois, I. Schwaab, C. K. Hogdall, L. Lundvall, S. H. Olson, I. Orlow, L. E. Paddock, A. Rudolph, U. Eilber, A. Dansonka-Mieszkowska, I. K. Rzepecka, I. Ziolkowska-Seta, L. Brinton, H. Yang, M. Garcia-Closas, E. Despierre, S. Lambrechts, I. Vergote, C. Walsh, J. Lester, W. Sieh, V. McGuire, J. H. Rothstein, A. Ziogas, J. Lubinski, C. Cybulski, J. Menkiszak, A. Jensen, S. A. Gayther, S. J. Ramus, A. Gentry-Maharaj, A. Berchuck, A. H. Wu, M. C. Pike, D. Van Denberg, K. L. Terry, A. F. Vitonis, J. A. Doherty, S. E. Johnatty, A. Defazio, H. Song, J. Tyrer, T. A. Sellers, C. M. Phelan, K. R. Kalli, J. M. Cunningham, B. L. Fridley and E. L. Goode, Cancer Epidemiol Biomarkers Prev, 2013, 22, 987–992.
- P. Peethambaram, B. L. Fridley, R. A. Vierkant, M. C. Larson, K. R. Kalli, E. A. Elliott, A. L. Oberg, K. L. White, D. N. Rider and G. L. Keeney, International journal of molecular epidemiology and genetics, 2011, 2, 185.
- D. J. Christoffersen, P. Damkier, S. Feddersen, S. Möller, J. L. Thomsen, C. Brasch-Andersen and K. Brøsen, Basic & Clinical Pharmacology & Toxicology, 2016, 119, 381–388.
- S. Sadhasivam, V. Chidambaran, X. Zhang, J. Meller, H. Esslinger, K. Zhang, L. J. Martin and J. McAuliffe, The Pharmacogenomics Journal, 2014, 15, 119–126.
- A. Ray, L. Tennakoon, J. Keller, J. E. Sarginson, H. S. Ryan, G. M. Murphy, L. C. Lazzeroni, M. H. Trivedi, J. H. Kocsis, C. DeBattista and A. F. Schatzberg, The Pharmacogenomics Journal, 2014, 15, 332–339.
- Sánchez-Lázaro, M. J. Herrero, C. Jordán-De Luna, V. Bosó, L. Almenar, L. Rojas, L. Martínez-Dolz, J. E. Megías-Vericat, L. Sendra, A. Miguel, J. L. Poveda and S. F. Aliño, Pharmacogenomics, 2015, 16, 971–979. [Google Scholar]
- G. Burgueño-Rodríguez, Y. Méndez, N. Olano, M. Schelotto, L. Castillo, A. M. Soler and J. da Luz, Front Pharmacol, 2023, 14, 1278769–1278769.
- B. Breitenstein, S. Scheuer, H. Pfister, M. Uhr, S. Lucae, F. Holsboer, M. Ising and T. M. Brückl, CNS Spectrums, 2013, 19, 165–175.
- A. L. de Klerk, I. M. Nolte, P. M. Bet, F. J. Bosker, H. Snieder, J. A. den Boer, R. Bruggeman, W. J. Hoogendijk and B. W. Penninx, The Pharmacogenomics Journal, 2012, 13, 349–353.
- M. Geers, T. Ochi, N. M. Vyalova, I. S. Losenkov, D. Z. Paderina, I. V. Pozhidaev, G. G. Simutkin, N. A. Bokhan, B. Wilffert, D. J. Touw, A. J. M. Loonen and S. A. Ivanova, Hum Psychopharmacol, 2022, 37, e2826–e2826.
- Magarbeh, C. Hassel, M. Choi, F. Islam, V. S. Marshe, C. C. Zai, R. Zuberi, R. S. Gammal, X. Men, M. Scherf-Clavel, D. Enko, B. N. Frey, R. Milev, C. N. Soares, S. V. Parikh, F. Placenza, S. C. Strother, S. Hassel, V. H. Taylor, F. Leri, P. Blier, F. Farzan, R. W. Lam, G. Turecki, J. A. Foster, S. Rotzinger, S. Kloiber, J. L. Kennedy, S. H. Kennedy, C. A. Bousman and D. J. Müller, Clinical Pharmacology & Therapeutics, 2023, 114, 88–117. [Google Scholar]
- L. R. Silberbauer, L. Rischka, C. Vraka, A. M. Hartmann, G. M. Godbersen, C. Philippe, D. Pacher, L. Nics, M. Klöbl, J. Unterholzner, T. Stimpfl, W. Wadsak, A. Hahn, M. Hacker, D. Rujescu, S. Kasper, R. Lanzenberger and G. Gryglewski, Molecular psychiatry, 2022, 27, 4502–4509.
- J. Bly, J. R. Bishop, K. L. H. Thomas and V. L. Ellingrod, J Sex Marital Ther, 2013, 39, 280–288.
- D. Tsuji, Y.-I. Kim, H. Nakamichi, T. Daimon, K. Suwa, Y. Iwabe, H. Hayashi, K. Inoue, M. Yoshida and K. Itoh, Drug Metabolism and Pharmacokinetics, 2013, 28, 299–304.
- H. H. Chang, C.-H. Chou, Y. K. Yang, I. H. Lee and P. S. Chen, Clin Psychopharmacol Neurosci, 2015, 13, 250–255.
- X. -X. Shan, Y. Qiu, W.-W. Xie, R.-R. Wu, Y. Yu, H.-S. Wu and L.-H. Li, Front Pharmacol, 2019, 10, 761–761.
Figure 1.
Mechanisms of action of ABCB1 across the luminal membrane (LM) and abluminal membrane (AM) of the blood-brain barrier using nutrient transporters (yellow and orange), peptides transporters, (purple), ABC transporters (green) ion transporters (red). The direction(s) of transport is indicated by the arrows.
Figure 1.
Mechanisms of action of ABCB1 across the luminal membrane (LM) and abluminal membrane (AM) of the blood-brain barrier using nutrient transporters (yellow and orange), peptides transporters, (purple), ABC transporters (green) ion transporters (red). The direction(s) of transport is indicated by the arrows.
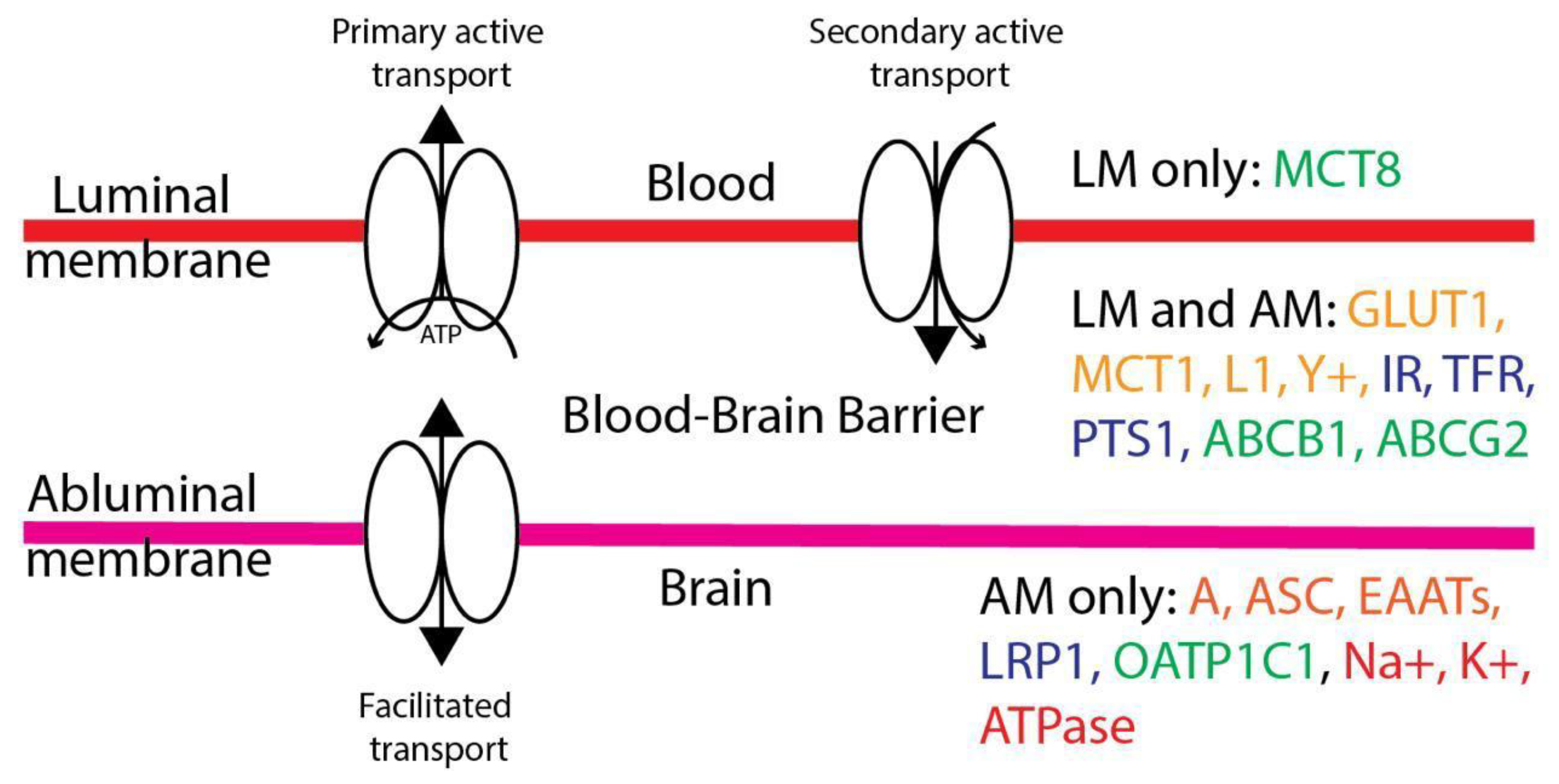

Table 1.
Clinical investigations of pharmacogenetically-informed drug-response of SNPs in the ABCB1 gene. Alternative names listed in parenthesis.
Table 1.
Clinical investigations of pharmacogenetically-informed drug-response of SNPs in the ABCB1 gene. Alternative names listed in parenthesis.
| p-glycoprotein | Drug transport | Drug response and pharmacokinetics | Limited information | |
|---|---|---|---|---|
| Rs ID | rs3842, rs1045642 (C3435T), rs1922240, rs2032582 (G2677T/A), rs2235013, rs2235033, rs2235046 | rs17064, rs868755, rs1128503, rs1202168, rs1211152, rs1922242, rs2032588, rs2214102, rs2214103, rs2235018, rs2235020, rs2235035, rs2235074, rs3213619, rs10276036 | rs2888599, rs4148727, rs9282564, rs13237132 | rs2235015 (DRD2 Taq1A), rs55852620, rs58898486 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



