Submitted:
22 July 2024
Posted:
22 July 2024
You are already at the latest version
Abstract
Background and objectives: Due to resistance and lack of treatment options, hospital-acquired Acinetobacter baumannii (A. baumannii) infections are associated with high mortality. The aim of this study was to identify the characteristics and outcomes of patients with infections caused by multidrug resistant A. baumannii in a tertiary-care teaching hospital and to determine the risk factors for in-hospital mortality. Materials and methods: A retrospective cohort study including 196 patients with A. baumannii strains isolated from different clinical specimens in the Hospital of the Lithuanian University of Health Sciences in 2016, 2017 and 2020, 2021 was conducted. Data on patients’ characteristics, comorbid diseases, treatment, length of hospital and ICU stay, outcome were collected. To determine risk factors for in-hospital mortality, logistic regression analysis was performed. Results: There were 60 (30.6%) women 136 (69.4%) men with a mean age of 61.7 ± 16.6 years (range, 52–74). More than three-fourths (76.5%, n = 150) of the patients had at least one comorbid disease. The highest number of A. baumannii strains were isolated from patients hospitalized in ICUs (43.4%, n = 85). A. baumannii strains producing three types of β-lactamases were more frequently isolated from women than men (77.8 % vs. 22.2%, p = 0.006). Infections caused by A. baumannii strains producing two types of β-lactamases were significantly more often treated with combination therapy than infections caused by strains producing one type of β-lactamase (78.9% vs. 60.0%, p = 0.019). Patients with A. baumannii strains producing two different types of β-lactamases (AmpC plus KPC, AmpC plus ESBL, or ESBL plus KPC) stayed significantly shorter at the ICU compared to patients with A. baumannii strains not producing β-lactamases (median of 9, IQR 2–18, vs. median of 26, IQR 7–38, p = 0.022). Death occurred in 58.7% (n = 115) of patients. Logistic regression analysis showed that combination therapy, length of hospital stay of < 10 days after A. baumannii infection, age of > 58 years, and absence of co-infection were independent predictors of in-hospital mortality. Conclusions: Patients with infection caused by A. baumannii strains producing two different types of β-lactamases were more frequently treated with combination therapy. Mortality of patients with multidrug resistant A. baumannii infection was high, and it was associated with patient’s age, length of hospital stay after the diagnosis of A. baumannii infection, absence of co-infection, and combination treatment.
Keywords:
Acinetobacter baumannii
; multidrug resistance
; risk factors
; mortality
; comorbidity
; hospitalization.
1. Introduction
Acinetobacter baumannii (A. baumannii) is a gram-negative, lactose non-fermenting organism, and due to its ability to survive in hospital environments, it is increasingly becoming a major pathogen of healthcare-associated infections (HAI) worldwide. With the emergence of HAI, A. baumannii has become an important cause of mortality in critically ill patients. A. baumannii is now largely regarded as one of the most troublesome pathogens and is responsible for several types of HAI including skin and soft tissue infections and invasive infections such as pneumonia, osteomyelitis, and bacteremia [1]. Moreover, A. baumannii causes community-acquired infections, although to a lesser extent [2,3]. Reports about multidrug resistant (MDR) A. baumannii are constantly increasing, especially in intensive care units (ICUs), and it is related to high attributable mortality in critically ill patients [4]. The vast majority of patients use a large number of combined broad-spectrum antimicrobial agents, which makes their immunity weaker and easier access to hospital infection [5]. MDR A. baumannii-caused infections are difficult to diagnose and treat, leading to increased mortality and prolonged hospital stays [2,3]. Many studies have linked chronic comorbid conditions, bedridden status, venous catheterization, ICU stay, infections with MDR phenotypes, concurrent fungal infection, and age to A. baumannii infection-related mortality [6,7]. Muntean et al. [8] have reported that the development of A. baumannii infection in patients admitted to the ICU, previous antibiotic therapy at admission, blood transfusion, and ulcer pressure are risk factors. Although the findings from different studies are not consistent, understanding the risk factors for MDR A. baumannii infections in patients admitted to the ICU is important to reduce the incidence and spread of such infections in the ICU. Therefore, the aim of this study was to identify the characteristics and outcomes of patients with infections caused by multidrug resistant A. baumannii in a tertiary-care teaching hospital and to determine the risk factors for in-hospital mortality.
2. Materials and Methods
2.1. Patients and Bacterial Strains
This study was carried out at a 2213-bed tertiary care teaching hospital. All hospitalized patients with a culture positive for A. baumannii during 2016, 2017, 2020, and 2021 were recruited in this study. When A. baumannii was recovered from two or more sources in the same patient, only one isolate obtained was included for analysis (in cases where susceptibility results were different, the isolate with the highest level of resistance was included). Specimens were obtained from wounds, biopsy, bronchial secretions, sputum, blood, pus, abdominal fluid, pleural fluid, urine, and cerebrospinal fluid of hospitalized patients.
All patients were older than 18 years. A retrospective data analysis was performed to evaluate patient risk factors and mortality associated with A. baumannii infection. The following data were collected for all subjects: demographic data, chronic comorbid diseases illnesses (diabetes mellitus, heart disease, renal and hepatic failure, and cancer), surgery, source of infection, laboratory and clinical data on the day of A. baumannii cultivation, hospitalization ward (ICU, medical wards, or surgical wards) at the beginning of the infection, duration of mechanical ventilation before A. baumannii infection, radiological findings (a new lung infiltrate or consolidation in chest X-ray) in the presence of A. baumannii growth in the cultures of bronchial aspirate or sputum. Sputum was accepted in cases without orotracheal intubation or tracheostomy if the culture was pure and the sample was representative of lower airways (absence of epithelial cells and ≥ 25 polymorphonuclear neutrophils per microscopic field).
Length of hospital and ICU stay before and after the development of A. baumannii infection, antimicrobial agents prescribed during hospitalization before A. baumannii infection, adjusted antibiotic therapy (when data about the susceptibility of the isolate were obtained), and cause of death were recorded.
A. baumannii detected in the culture was considered as contamination when clinical and laboratory data did not indicate any infection. The treatment of A. baumannii infection using a single antibiotic was considered monotherapy, while combination therapy was defined as the use of 2 or more antibiotics with an antimicrobial effect toward A. baumannii during the infection episode.
HAI was confirmed according to the surveillance definition of the Centers for Disease Control and Prevention/National Healthcare Safety [9]. Kaunas Regional Biomedical Research Ethics Committee approved this study (No. BE10-0016, dated December 28, 2021). The need for written consent was waived due to the retrospective nature of the study.
2.2. Antimicrobial Susceptibility Testing
Antimicrobial susceptibility testing was performed by a disk diffusion method on Müller–Hinton agar (MH II according to EUCAST, Graso Biotech Microbiology Systems, Owidz, Poland). All inoculated plates were incubated for a total of 16–20 h at 35°C ± 1°C in an ambient air incubator after inoculation with organisms and placement of disks. All the strains were tested for sensitivity to the following antibiotics: ceftazidime, cefepime, gentamicin, amikacin, ciprofloxacin, ampicillin/sulbactam, piperacillin/tazobactam, imipenem, meropenem, doxycycline, tigecycline, tetracycline, and sulfamethoxazole/trimethoprim disks (Becton Dickinson Microbiology Systems) were used. The diameter of the inhibition zone was measured in millimeters using a ruler. Inhibition zone diameters were interpreted according to the European Committee on Antimicrobial Susceptibility Testing (EUCAST) recommendations [10]. The results were interpreted according to the EUCAST breakpoints. All isolated and identified A. baumannii strains were frozen at –80°C.
Carbapenemase-producing isolates were detected phenotypically by a four-combination disk test (CDT) to determine the production of ESBL and AmpC (Abtek Biologicals, Liverpool, UK, in 2016 and 2017; Liofilchem®, Roseto degli Abruzzi, Italy, in 2021 and 2022. This work is a continuation of a previous study published in the article: Association of β-lactamase types and antimicrobial resistance in Acinetobacter baumannii [11] in the journal Medicine.
3. Results
A total of 196 isolates were collected: 60 (30.6%) from women and 136 (69.4%) from men, with a mean age of 61.7 ± 16.6 (range, 52–74) years. The mean length of hospital stay was 25.24 ± 30 (IQR, 7–34) days, and the mean length of ICU stay was 19 ± 46 (IQR, 3–20) days. The highest number of A. baumannii strains were isolated from patients hospitalized in ICU (43.4%, n = 85), followed by surgical wards (31.1%, n = 61) and medical wards (25.5%, n = 50). More than three-fourths (76.5%, n = 150) of the patients had at least one comorbid disease. Cardiac diseases accounted for 62.2% (n = 122) of all comorbid diseases; cancer, for 27.5% (n = 54); type 2 diabetes mellitus, for 18.0% (n = 35); and type 1 diabetes mellitus, for 2.1% (n = 4).
Of the 196 episodes of infection, respiratory infections caused by A. baumannii made up 66.3% (n = 130); skin and soft tissue infections plus surgical wound infections, 8.7% (n = 17); bacteremia, 6.6% (n = 13); gastrointestinal tract infections, 5.6% (n = 11); urinary tract infections, 4.1% (n = 8); and infections of other locations, 1.0% (n = 2). As much as 7.7% (n = 15) of cases were considered contamination.
Along with A. baumannii, one co-pathogen was found in 94 (47.9%) patients and two or more co-pathogens, in 102 (52.0%) patients. In cases of co-infection, Klebsiella pneumoniae and Pseudomonas aeruginosa were isolated most often with A. baumannii.
Before the diagnosis of A. baumannii infection, patients were treated with 2 antibacterial drugs on average (SD, 1; range, 0–5). Cephalosporins were the most frequently prescribed drugs (n = 147, 75.0%) followed by penicillin + BLI (n = 112, 57.1%), carbapenems (n = 76, 38.8%), antifungals (n = 33, 16.8%), and quinolones (n = 25, 12.8%). Majority of the patients (81.6%, n = 160) were subjected to mechanical ventilation lasting for 7 days on average (SD, 7; range, 1–51).
A. baumannii strains producing three types of β-lactamases were more frequently isolated from females than males (77.8% vs. 22.2%, p = 0.006). Infections caused by A. baumannii strains producing two types of β-lactamases were significantly more often treated with combination therapy than infections caused by strains producing one type of β-lactamase (78.9% vs. 60.0%, p = 0.019). No significant associations were found between the type and number of β-lactamases with patients’ characteristics such as age, cause of hospitalization mechanical ventilation, length of stay before A. baumannii infection, markers of inflammation, chronic diseases and antibiotic treatment before infection (Table 1).
Patients with A. baumannii strains producing two different types of β-lactamases (AmpC plus KPC, AmpC plus ESBL, or ESBL plus KPC) stayed significantly shorter at the ICU compared to patients with A. baumannii strains not producing β-lactamases (median of 9, IQR 2–18, vs. median of 26, IQR 7–38, p = 0.022) (Figure 1).
χ2 = 9.613, df = 3, p = 0.022 by the Kruskal-Wallis test (Dunn post hoc test for pair-wise comparison: β-lactamase non-producing strains vs. strains producing two types of β-lactamases, p = 0.016).
Error bars indicate the range of distribution; the box, the interquartile range; the horizontal line, median value; the asterisks and circles, outliers.
Despite there were no significant associations between the type of antibacterial treatment and A. baumannii strains producing different types of β-lactamases before the detection of A. baumannii infection (p > 0.05) (Table 1), possible associations were evaluated after the detection of A. baumannii infection.
Of the 196 patients with A. baumannii infection, 73 received combination therapy with colistin and BLI (37.2%), 28 received monotherapy with BL (14.3%), 16 continued empirical treatment (8.2%), 16 received combination therapy with colistin and carbapenems (8.2%), and other combinations were administered in 12 patients (6.1%). Death occurred in 34 patients (17.3%) before treatment could be administered, and 17 cases (8.7%) of A. baumannii infection were considered as colonization. Monotherapy was administered in 23.5% of patients to treat A. baumannii infection and combination therapy, in 59.2%.
Patients with infections caused by A. baumannii producing one type of β-lactamase were significantly more frequently treated with the combination of colistin and carbapenem as well as other combinations than those with infections caused by A. baumannii producing two types of β-lactamases (57.1% and 63.6% vs. 35.7% and 36.4%, p = 0.015 and p = 0.017, respectively). The combination of colistin with BLI was administered significantly more frequently to treat infections caused by A. baumannii producing two types of β-lactamases than infections caused by A. baumannii producing one type of β-lactamase (83.8% vs. 11.8%, p < 0.001). The detailed information is shown in Table 2.
Of the 196 patients diagnosed with A. baumannii infection, 58.7% (n = 115) died and 41.3% (n = 81) survived. Demographical and clinical characteristics of survivors and non-survivors are shown in Table 3. Compared to survivors, non-survivors were significantly older (55.9, SD 17.9, vs. 65.9, SD 14.2, years), were more likely to have chronic cardiovascular and respiratory diseases (49.4% vs. 71.3% and 65.4 vs. 91.3%, respectively), and were more likely to be hospitalized due to surgery (48.2% vs. 51.8%). The median length of stay in hospital after A. baumannii infection for non-survivors was 6 days (IQR, 1–21) compared to 21 days (12.5–41.5) for those who survived.
Among non-survivors, death occurred significantly more frequently in those who were treated with combination therapy than those who were treated with monotherapy (84.4% vs. 15.6%) and in those who were not co-infected with other bacteria than those who had co-infections (56.5% vs. 43.5%).
Receiver operating characteristic (ROC) curve analysis was performed to assess the ability of age and length of hospital stay after the detection of A. baumannii infection to predict in-hospital mortality in patients with drug-resistant A. baumannii. The age of > 58 years had an AUC of 0.66 (95% CI, 0.59–0.72), sensitivity of 71.3%, and specificity of 54.3% (p < 0.001) and length of hospital stay of < 10 days after the detection of A. baumannii infection had an AUC of 0.76 (95% CI, 0.70–0.82), sensitivity of 63.48%, and specificity of 80.25% (p < 0.001).
Binary logistic regression analysis was performed including the following significant variables in the univariate analysis: age, hospitalization after A. baumannii infection, combination therapy, co-infection, at least one chronic disease, hospitalization due to surgery and trauma. Several risk factors for in-hospital mortality were identified: combination therapy was associated with a 6.11-fold greater risk of in-hospital mortality (95% CI, 2.47–15.10); hospitalization of < 10 days after A. baumannii infection, with a 4.26-fold greater risk (95% CI, 1.79–10.09); age of > 58 years, with 1.06-fold greater risk (95% CI, 1.03–1.09); and no co-infection, with a 2.55-fold greater risk (95% CI, 1.15–5.65) (Table 4).
4. Discussion
A. baumannii is one of the most common opportunistic agents causing healthcare-associated infections, especially in the ICU setting [11,12]. The global estimated incidence of A. baumannii infections is approximately one million cases per year, and due to resistance and lack of treatment options, hospital-acquired A. baumannii infections are associated with high mortality, especially in critically ill patients [13,14]. This study aimed to identify the factors associated with infections caused by MDR A. baumannii, to assess the characteristics of patients and the risk factors contributing to infection-related mortality in a tertiary-care teaching hospital.
In our study, the incidence of A. baumannii infections in the ICU setting was lower than that reported in the study by Calò et al. [15] (43.4% vs. 52.5%). This difference in incidence rates may be explained by the use of infection control measures, particularly hand hygiene practices and decontamination of the hospital environment [16]. The study by Uwingabiye et al. [16] showed that patients who developed ICU-acquired A. baumannii infection had a median ICU length of 18 (IQR: 10–26) days; in our study, the median length of ICU stay was 10 (IQR, 3–20) days. Appaneal et al. [17] reported that length of stay > 10 days was higher among those with MDR A. baumannii versus non-MDR A. baumannii, suggesting that ICU-acquired A. baumannii infections are due to prolonged ICU stay. Unnecessary hospitalization days may increase the rate of hospital-acquired complications and economic burden [18]. Long stays in the ICU and the use of medical devices are necessary for the treatment of critically ill patients in modern medicine, but their presence is associated with the risk of infection. Previous studies have identified mechanical ventilation as a possible risk factor for ventilator-associated pneumonia and bacteremia [19,20]. This explains why A. baumannii isolates were most commonly found in the respiratory tract of our patients (66.3%), and this is consistent with the findings of the study by Hafiz et al. [21] who found that respiratory infections caused by A. baumannii accounted for 63% of all A. baumannii-related infections. According to the findings of other study investigating the prevalence of A. baumannii in the samples collected from different sources including blood, respiratory tract, and urine, the lower respiratory tract also represented the most common source of infection (67%) [22].
In our study, of the 196 patients, 17 (8.7%) were considered colonized, whereas infection by A. baumannii was diagnosed in 179 (91.3%) individuals. In another study, a high proportion of patients (60%) was colonized by A. baumannii [23]. Antibiotic exposure is one of the most frequently reported risk factors for MDR A. baumannii colonization or infection, and the use of carbapenems, third-generation cephalosporins, and β-lactams has been reported [24,25,26]. Antibiotic therapy facilitates the emergence of new resistant mutants or the proliferation of antibiotic-resistant A. baumannii by exerting selective pressure. In our study, monotherapy to treat A. baumannii infection was administered in 23.5% of patients and combination therapy, in 59.2%. In the study by López-Cortés et al. [27], 101 patients with sepsis caused by multidrug resistant A. baumannii were evaluated in 28 Spanish hospitals. The study reported that 67.3% of patients received monotherapy, while 32.7% received combination therapy. In the study by Park et al., 44.6% of patients with A. baumannii infections were treated with monotherapy and 55.4%, with combination therapy [28], given at a similar frequency as in our study. Combination antibiotic therapy is prescribed to treat more serious infections caused by MDR A. baumannii and polymicrobial infections [29].
In our study, in-hospital mortality was found to be 58.7%, which is comparable with mortality in other study [30]. The worldwide mortality rate among patients with A. baumannii infection ranges between 26% and 60% [30,31,32]. The higher mortality rate can be attributed to several factors including underlying medical conditions, antimicrobial resistance, and appropriateness of treatment [33]. Numerous risk factors have been investigated as potential predictors of mortality in patients infected with A. baumannii. Several studies have analyzed the risk factors for mortality among patients with A. baumannii infections, demonstrating that many comorbidities, including chronic liver, cardiovascular, and renal diseases, as well as more severe diseases, i.e. septic shock, or higher APACHE II or Pitt bacteremia scores, are associated with higher mortality rates [17,32,34,35]. Our study found that combination therapy of A. baumannii infection, hospitalization after A. baumannii infection within less than 10 days, age of > 58 years, and no co-infection were significantly associated with a greater risk of mortality. However, we did not find any significant association between the production of different types and numbers of β-lactamases and clinical outcomes of the patients.
Some limitations of this study must be acknowledged. It was a single-hospital study involving adults; in addition, A. baumannii strains were not tested in 2018, 2019, and 2020, which means that some strains may be associated with potentially higher drug resistance. For more accurate results larger multicenter studies in different countries and hospitals would be relevant. Such multicenter studies would provide a better understanding of the impact of drug-resistant A. baumannii as a causative agent for in-hospital mortality.
5. Conclusions
Patients with infection caused by A. baumannii strains producing two different types of b-lactamases were more frequently treated with combination therapy. Mortality of patients with multidrug resistant A. baumannii infection was high, and it was associated with patient’s age, length of hospital stay after the diagnosis of A. baumannii infection, absence of co-infection, and combination treatment.
Author Contributions
Conceptualization, A.V.; Data curation, K.Č.; Formal analysis, K.Č.; Methodology, K.Č and A.V.; Care, A.V.; Visualization A.V.;Writing—original draft, K.Č.;Writing—revision and editing, K.Č and A.V. All authors have read and agreed to the published version of the manuscript.
Acknowledgments
No funding was received.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Huang, H.; et al. A multi-center study on the risk factors of infection caused by multi-drug resistant Acinetobacter baumannii. BMC Infectious Diseases 2018, 18, 11. [Google Scholar] [CrossRef] [PubMed]
- Wong, D.; et al. Clinical and Pathophysiological Overview of Acinetobacter Infections: a Century of Challenges. Clin Microbiol Rev 2017, 30, 409–447. [Google Scholar] [CrossRef] [PubMed]
- Dickstein, Y.; et al. Treatment Outcomes of Colistin- and Carbapenem-resistant Acinetobacter baumannii Infections: An Exploratory Subgroup Analysis of a Randomized Clinical Trial. Clin Infect Dis 2019, 69, 769–776. [Google Scholar] [CrossRef] [PubMed]
- Diao, H.; et al. Risk factors for multidrug-resistant and extensively drug-resistant Acinetobacter baumannii infection of patients admitted in intensive care unit: a systematic review and meta-analysis. J Hosp Infect 2024, 149, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Ren, J.; et al. Risk factors and drug resistance of the MDR Acinetobacter baumannii in pneumonia patients in ICU. Open Medicine 2019, 14, 772–777. [Google Scholar] [CrossRef] [PubMed]
- Fu, Q.; Ye, H.; Liu, S. Risk factors for extensive drug-resistance and mortality in geriatric inpatients with bacteremia caused by Acinetobacter baumannii. American Journal of Infection Control 2015, 43, 857–860. [Google Scholar] [PubMed]
- Freire, M.P.; et al. Bloodstream infection caused by extensively drug-resistant Acinetobacter baumannii in cancer patients: high mortality associated with delayed treatment rather than with the degree of neutropenia. Clinical Microbiology and Infection 2016, 22, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Muntean, D.; et al. Extensively drug-resistant Acinetobacter baumannii and Proteeae association in a Romanian intensive care unit: risk factors for acquisition. Infect Drug Resist 2018, 11, 2187–2197. [Google Scholar] [CrossRef]
- Horan, T.C.; Andrus, M.; Dudeck, M.A. CDC/NHSN surveillance definition of health care–associated infection and criteria for specific types of infections in the acute care setting. American journal of infection control 2008, 36, 309–332. [Google Scholar]
- Giske, C.G.; et al. Update from the European Committee on Antimicrobial Susceptibility Testing (EUCAST). J Clin Microbiol 2022, 60, e0027621. [Google Scholar] [CrossRef]
- Černiauskienė, K.; Dambrauskienė, A.; Vitkauskienė, A. Associations between β-Lactamase Types of Acinetobacter baumannii and Antimicrobial Resistance. Medicina (Kaunas) 2023, 59. [Google Scholar]
- Gonzalez-Villoria, A.M.; Valverde-Garduno, V. Antibiotic-Resistant<i> Acinetobacter baumannii</i> Increasing Success Remains a Challenge as a Nosocomial Pathogen. Journal of Pathogens 2016, 2016, 7318075. [Google Scholar]
- Benaissa, E.; et al. Risk factors for acquiring Acinetobacter baumannii infection in the intensive care unit: experience from a Moroccan hospital. Access Microbiol 2023, 5. [Google Scholar] [CrossRef] [PubMed]
- Magill, S.S.; et al. Multistate Point-Prevalence Survey of Health Care–Associated Infections. New England Journal of Medicine 2014, 370, 1198–1208. [Google Scholar] [CrossRef] [PubMed]
- Piperaki, E.T.; et al. Carbapenem-resistant Acinetobacter baumannii: in pursuit of an effective treatment. Clinical Microbiology and Infection 2019, 25, 951–957. [Google Scholar] [CrossRef] [PubMed]
- Calò, F.; et al. Outcome of patients with carbapenem-resistant Acinetobacter baumannii infections treated with cefiderocol: A multicenter observational study. Journal of Infection and Public Health 2023, 16, 1485–1491. [Google Scholar] [CrossRef]
- Uwingabiye, J.; et al. Intensive care unit-acquired Acinetobacter baumannii infections in a Moroccan teaching hospital: epidemiology, risk factors and outcome. Germs 2017, 7, 193–205. [Google Scholar] [CrossRef] [PubMed]
- Appaneal, H.J.; et al. Treatment, clinical outcomes, and predictors of mortality among a national cohort of admitted patients with Acinetobacter baumannii infection. Antimicrobial Agents and Chemotherapy 2022, 66, e01975–21. [Google Scholar] [CrossRef]
- Arefian, H.; et al. Extra length of stay and costs because of health care-associated infections at a German university hospital. Am J Infect Control 2016, 44, 160–166. [Google Scholar] [CrossRef]
- Torres, A.; et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: Guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociación Latinoamericana del Tórax (ALAT). Eur Respir J 2017, 50. [Google Scholar]
- Papanikolopoulou, A.; et al. Ventilator-Associated Pneumonia, Multidrug-Resistant Bacteremia and Infection Control Interventions in an Intensive Care Unit: Analysis of Six-Year Time-Series Data. Antibiotics (Basel) 2022, 11. [Google Scholar] [CrossRef]
- Hafiz, T.A.; et al. A two-year retrospective study of multidrug-resistant Acinetobacter baumannii respiratory infections in critically Ill patients: Clinical and microbiological findings. Journal of Infection and Public Health 2023, 16, 313–319. [Google Scholar] [CrossRef]
- Blanco, N.; et al. Risk Factors and Outcomes Associated with Multidrug-Resistant Acinetobacter baumannii upon Intensive Care Unit Admission. Antimicrob Agents Chemother 2018, 62. [Google Scholar] [CrossRef]
- Martín-Aspas, A.; et al. Differential characteristics of Acinetobacter baumannii colonization and infection: risk factors, clinical picture, and mortality. Infection and Drug Resistance, 2018, 11, 861–872. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; et al. Risk and Prognostic Factors for Multidrug-Resistant Acinetobacter Baumannii Complex Bacteremia: A Retrospective Study in a Tertiary Hospital of West China. PLoS One 2015, 10, e0130701. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-Y.; et al. Clinical features and risk factors for development of breakthrough gram-negative bacteremia during carbapenem therapy. Antimicrobial agents and chemotherapy 2016, 60, 6673–6678. [Google Scholar] [CrossRef]
- Zhou, H.; et al. Risk factors for acquisition and mortality of multidrug-resistant Acinetobacter baumannii bacteremia: A retrospective study from a Chinese hospital. Medicine (Baltimore) 2019, 98, e14937. [Google Scholar]
- López-Cortés, L.E.; et al. Monotherapy versus combination therapy for sepsis due to multidrug-resistant Acinetobacter baumannii: analysis of a multicentre prospective cohort. J Antimicrob Chemother 2014, 69, 3119–3126. [Google Scholar]
- Park, S.Y.; et al. Survival of carbapenem-resistant Acinetobacter baumannii bacteremia: colistin monotherapy versus colistin plus meropenem. J Int Med Res 2019, 47, 5977–5985. [Google Scholar]
- Schmid, A.; et al. Monotherapy versus combination therapy for multidrug-resistant Gram-negative infections: Systematic Review and Meta-Analysis. Sci Rep 2019, 9, 15290. [Google Scholar] [CrossRef]
- Alrahmany, D.; et al. Acinetobacter baumannii Infection-Related Mortality in Hospitalized Patients: Risk Factors and Potential Targets for Clinical and Antimicrobial Stewardship Interventions. Antibiotics (Basel) 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Xiao, D.; et al. Prognosis of patients with Acinetobacter baumannii infection in the intensive care unit: A retrospective analysis. Exp Ther Med 2017, 13, 1630–1633. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.M.; et al. Risk factors for early mortality in patients with carbapenem-resistant Acinetobacter baumannii bacteraemia. J Glob Antimicrob Resist 2022, 31, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Itani, R.; et al. Acinetobacter baumannii: assessing susceptibility patterns, management practices, and mortality predictors in a tertiary teaching hospital in Lebanon. Antimicrobial Resistance & Infection Control 2023, 12, 136. [Google Scholar]
- Du, X.; et al. Predictors of mortality in patients infected with carbapenem-resistant Acinetobacter baumannii: a systematic review and meta-analysis. American journal of infection control 2019, 47, 1140–1145. [Google Scholar] [CrossRef]
- Russo, A.; et al. ISGRI-SITA (Italian Study Group on Resistant Infections of the Società Italiana Terapia Antinfettiva). Bloodstream infections caused by carbapenem-resistant Acinetobacter baumannii: Clinical features, therapy and outcome from a multicenter study. J. Infect 2019, 79, 130–138. [Google Scholar]
Figure 1.
Length of stay in the ICU by the production of β-lactamases in A. baumannii strains.
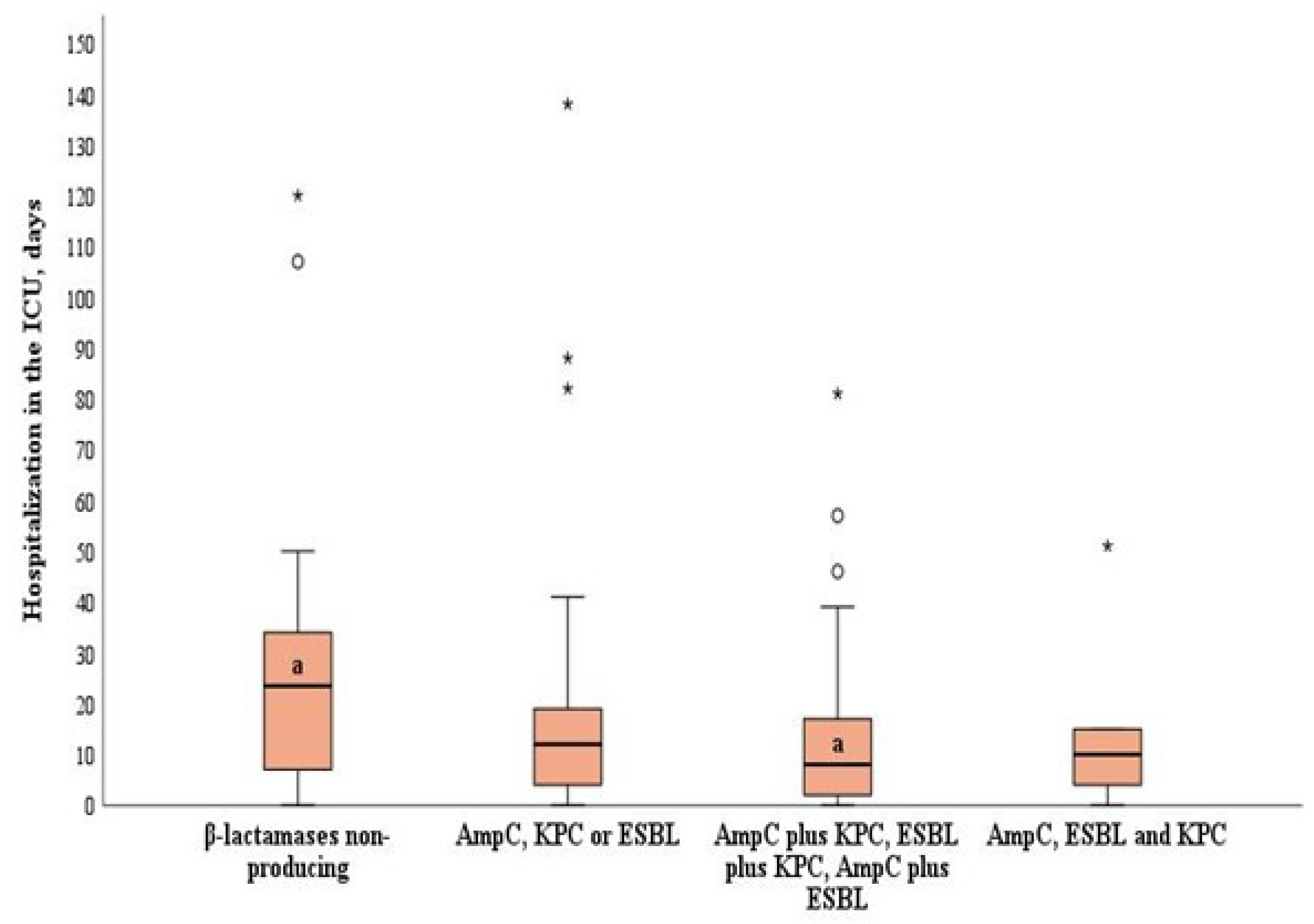

Table 1.
Comparison of demographic characteristics, admission type and underlying comorbidities and infection-related details between the pathogen A. baumannii producing different types and numbers of β-lactamases.
Table 1.
Comparison of demographic characteristics, admission type and underlying comorbidities and infection-related details between the pathogen A. baumannii producing different types and numbers of β-lactamases.
| Variable | A. baumannii strains producing different types and numbers of β-lactamases | p | ||
|---|---|---|---|---|
| One type* (n = 53) | Two different types** (n = 115) | All three types*** (n = 9) | ||
| Gender, n (%) Female |
16 (30.2) |
31 (27.0) |
7 (77.8)a |
0.006a vs. b |
| Male | 37 (69.8) | 84 (73.0) | 2 (22.2)b | |
| Age, mean (SD), years | 61.6 (17.5) | 62 (16.1) | 63.6 (16.8) | 0.949 |
| Cause of hospitalization, n (%) | ||||
| Surgery | 40 (75.5) | 83 (72.2) | 6 (66.7) | 0.825 |
| Trauma | 7 (13.2) | 7 (6.1) | 0 (0) | 0.188 |
| Comorbid disease, n (%) | 41 (77.4) | 87 (75.7) | 7 (77.8) | 0.965 |
| Antibiotic treatment before infection (class), n (%) | ||||
| Cephalosporin | 41 (77.4) | 86 (74.8) | 6 (66.7) | 0.781 |
| Penicillin + BLI | 31 (58.5) | 69 (60.0) | 4 (44.4) | 0.658 |
| Carbapenem | 22 (41.5) | 39 (33.9) | 5 (55.6) | 0.325 |
| Antifungal | 8 (15.1) | 22 (19.1) | 0 (0) | 0.308 |
| Quinolone | 9 (17.0) | 10 (8.7) | 0 (0) | 0.154 |
| Antibiotic treatment after infection, n (%) | ||||
| Monotherapy | 18 (40.0)a | 20 (21.1)b | 1 (14.3) | 0.019a vs. b |
| Combination therapy | 27 (60.0)a | 75 (78.9)b | 6 (85.7) | 0.019a vs. b |
| Length of stay before A. baumannii infection, days | 17 (10–30) | 13 (6–21) | 14 (8–33) | 0.353 |
| Length of ICU stay before A. baumannii infection, days | 6 (2–11) | 5 (2–10) | 4 (2–13) | 0.908 |
| MV duration before A. baumannii infection, days | 5 (2–10) | 4 (2–9) | 5 (2–19) | 0.497 |
| Inflammatory markers on A. baumannii infection onset | ||||
| WBC, ×109/L | 12.3 (7.3–16.2) | 11.2 (7.8–15.7) | 12.5 (4.9–16.6) | 0.988 |
| CRP, mg/L | 126.5 (76.0–250.3) | 108 (88.8–272.6) | 236.9 (86.8–295.9) | 0.294 |
Values are median (interquartile range) unless stated otherwise. *AmpC or KPC or ESBL, **AmpC Plus KPC, AmpC Plus ESBL or ESBL Plus KPC, ***AmpC, KPC and ESBL. BLI, β -lactamase inhibitors; ICU, intensive care unit; MV, mechanical ventilation; WBC, white blood cells; CRP, C-reactive protein.
Table 2.
Associations between A. baumannii strains producing different numbers and types of β-lactamases and different treatment regimens after the detection of A. baumannii infection.
Table 2.
Associations between A. baumannii strains producing different numbers and types of β-lactamases and different treatment regimens after the detection of A. baumannii infection.
| Treatment groups |
A. baumannii strains producing different types and numbers of β-lactamases | ||
|---|---|---|---|
| One type* (n = 53) | Two different types** (n = 115) | All three types*** (n = 9) |
|
| Treatment unadjusted for colonization and lethal outcome (n = 46) | 16 (34.8) | 27 (58.7) | 3 (6.7) |
| Continuation of empirical treatment (n = 15) | 3 (20.0) | 10 (66.7) | 2 (13.3) |
| Monotherapy with BLI (n = 23) | 11 (47.8) | 12 (52.2) | 0 (0.0) |
| Combination of colistin with BLI (n = 68) | 8 (11.8)a | 57 (83.8)b | 3 (4.4) |
| Combination of colistin and carbapenems (n = 14) | 8 (57.1)a | 5 (35.7)b | 1 (7.1) |
|
Other combinations#
(n = 12) |
7 (63.6)a | 4 (36.4)b | 0 (0.0) |
χ2 = 30.36, df = 10, p < 0.005. Significantly different a vs. b. *AmpC or KPC or ESBL, **AmpC Plus KPC, AmpC Plus ESBL, or ESBL Plus KPC, ***AmpC, KPC and ESBL. BLI, β-lactamase inhibitors. #Ciprofloxacin, doxycycline, or colistin + doxycycline.
Table 3.
Demographical and clinical characteristics of survivors and non-survivors.
| Variable | Survivors (n = 81) | Non-survivors (n = 115) | p |
|---|---|---|---|
| Gender, n (%) | |||
| Female | 23 (28.4) | 37 (32.2) | 0.572 |
| Male | 58 (71.6) | 78 (67.8) | |
| Age, mean (SD), years | 55.9 (17.9) | 65.9 (14.2) | <0.001 |
| Comorbid diseases, n (%) | |||
| Cardiovascular | 40 (32.8) | 82 (67.2) | 0.002 |
| Respiratory | 53 (65.4) | 105 (91.3) | <0.001 |
| Renal | 7 (8.6) | 16 (13.9) | 0.259 |
| Liver | 4 (21.1) | 15 (78.9) | 0.085 |
| Diabetes mellitus | 14 (17.3) | 25 (22.2) | 0.591 |
| Cancer | 20 (24.7) | 34 (29.6) | 0.452 |
| At least one comorbid disease | 55 (67.9) | 95 (82.6) | 0.017 |
| Cause of hospitalization, n (%) | |||
| Surgery | 68 (84.0) | 73 (63.5) | 0.002 |
| Trauma | 10 (12.3) | 5 (4.3) | 0.038 |
| Length of hospital stay before ICU, days | 10 (1 –19.7) | 10 (4–21) | 0.146 |
| Length of ICU stay before A. baumannii infection, days | 5 (1 –12) | 5 (2–10) | 0.450 |
| Length of hospital stay after A. baumannii infection, days | 21 (12.5–41.5) | 6 (1–21) | <0.001 |
| Duration of MV before A. baumannii infection, days | 3.0 (2.3–10) | 3.5 (2–9) | 0.212 |
| Duration of antibiotic treatment before A. baumannii infection, median (IQR), days | 15.0 (8–24.5) | 14.0 (8–23.0) | 0.649 |
| Antibiotic treatment after infection, n (%) | |||
| Monotherapy | 33 (40.7) | 13 (16.0) | 0.045 |
| Combination therapy | 48 (59.3) | 68 (84.0) | |
| Co-infection with other bacteria, n (%) | |||
| No | 29 (30.9) | 65 (69.1) | < 0.001 |
| Yes | 52 (51.0) | 50 (49.0) | |
| A. baumannii strains producing different types and numbers of β-lactamases, n (%) | |||
| One type* | 26 (32.1) | 27 (23.5) | 0.407 |
| Two different types** | 46 (56.8) | 69 (60.0) | |
| All three types*** | 2 (2.5) | 7 (6.1) | |
Values are median (interquartile range) unless stated otherwise. ICU, intensive care unit; MV, mechanical ventilation.
Table 4.
Risk factors for in-hospital mortality among patients with MDR A. baumannii infection.
| Risk factor | OR (95% CI) | p |
|---|---|---|
| Combination therapy | 6.11 (2.47–15.10) | < 0.001 |
| Hospitalization of < 10 days after A. baumannii infection | 4.26 (1.79–10.09) | < 0.001 |
| Age of > 58 years | 1.06 (1.03–1.09) | <0.001 |
| No co-infection | 2.55 (1.15–5.65) | 0.021 |
| At least one chronic disease | 0.621 (0.23–1.71) | 0.358 |
| Surgery | 0.68 (0.26–1.75) | 0.442 |
| Trauma | 0.37 (0.08–1.77) | 0.215 |
OR: odds ratio, CI: confidence interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



