
Submitted:
22 July 2024
Posted:
22 July 2024
You are already at the latest version
Abstract
Conjunctival melanoma (Co-M) is an aggressive, invasive eye and eyelid cancer. Its global inci-dence of ~1 in a million is increasing at a rate ratio of ~1.4, but this rises sharply in over 65-year-olds. Although rare, Co-M has a devastating impact on the lives of those who develop it. Co-M is often misdiagnosed or overlooked leading to vision loss either from destructive effects of the tumour or side effects of therapy, facial disfigurement from radical surgery, and death from metastases. Due to its rarity, there is limited evidence for diagnosis and management; hence, there is no standardised treatment and not all cases are referred to a specialised ocular oncology centre. Recent progress in cancer immunology and genetics have revolutionised treatment of cutaneous melanoma, which share some similarities to Co-M. A better understanding of Co-M and its precursor lesions is urgently needed to lead the development of novel targeted and immuno-therapies both for local tumour control and disseminated disease. This review aims to provide a comprehensive clinical overview of the current knowledge of Co-M, its epidemiology, pathogenesis, presentation, diagnosis, management, and recent advances in novel biological therapies for personalised treatment of this disease.
Keywords:
conjunctival melanocytic intraepithelial lesions
; conjunctival melanoma
; ocular oncology
; targeted therapy
; immunotherapy
1. Introduction
Conjunctival melanoma (Co-M) is a rare, aggressive invasive ocular surface cancer, which is often misdiagnosed or overlooked and causes significant visual disabilities, poor quality of life and even death from metastases. They occur most commonly in fair-skinned populations, with the overall incidence being approximately 0.46 cases per 1,000,000 persons per year [1,2], representing around 0.25% of melanomas at all sites and 5% of all ocular melanoma. It is the second most prevalent malignancy of the conjunctiva after squamous cell carcinoma [3] originating from the basal melanocytes in the conjunctival epithelium. The majority (~70%) of Co-M cases develop from conjunctival melanocytic intraepithelial lesions (C-MIN/ PAM with atypia), while others arise from pre-existing nevi or de novo [3,4].
Previous studies have often grouped Co-M with uveal melanoma as an ocular melanoma: the latter is the most common primary intraocular malignancy in adults, arising in the choroid, ciliary body or iris; however, uveal melanoma is embryologically, biologically and clinically very different to Co-M [5,6,7,8,9]. Unlike uveal melanoma, Co-M is a mucosal melanoma with histological and functional similarities to cutaneous melanoma [10,11] with similar genetic alterations. These include UV-related driver mutations in the BRAF, NF1 and RAS genes and copy number variations [6,12,13,14,15,16,17,18,19]. BRAF and NRAS mutations are present in ~30% and ~14-25% of Co-M, respectively, with the NRAS mutant Co-M being associated with higher metastatic risk [16]. Transcriptomic studies of Co-M that have focussed on the immune tumour microenvironment have also demonstrated high PDL1-expression, and a transcriptomic subtype enriched with immune genes (immune cell-types) [12,20,21]
Clinically Co-M most often presents in the bulbar conjunctiva, near the limbus, but can affect any part of the conjunctiva and even invade the neighbouring structures in advanced cases [4,22]. Lesions vary from amelanotic to brown pigmented or even black in colour. There is no standardised treatment; however, management includes: surgical excision +/- adjuvant cryotherapy, topical chemotherapy, brachytherapy, proton beam radiotherapy or photon external beam radiation, and in advanced cases with local tissue invasion - radical orbital exenteration [18,22,23,24,25,26,27]. Postoperative complications and tumour recurrence rates are high (33-45%), warranting life-long follow-up [4,28,29,30,31]. Metastases to lymph nodes are common (~25%) but may also involve the liver, lungs and brain, with ~27% 5-year disease-specific mortality rate [32,33].
Despite recent successes with targeted and immuno-therapies in cutaneous melanoma, data on Co-M treated with similar therapies (anti-BRAF/anti-MEK/anti-PDL1) are promising but limited, stemming from single patient or small case series with inoperable or advanced disease prior to surgery [34,35,36,37,38].
This review article aims to summarise the current understanding of Co-M and explore new advancements in the knowledge of Co-M pathophysiology and its treatment developments.
2. Epidemiology and pathogenesis of Co-M
The incidence of Co-M has increased over the last 5 decades [14,39] and ranges from 0.3 to 0.8 per million per year, being highest in Northern Europe and North America. The estimated number of new cases per year is 130 in the USA and 320 in Europe [18]. Populations of Asian or African descent are less commonly affected [2,40,41,42,43]. A study in the US found that fair skinned people had the highest incidence rate of Co-M, comprising 91.2% of cases compared to 2.4% in patients of Afro-Caribbean descent [44]. However, with majority of data coming from predominantly North America or Europe, there is very limited data on other ethnic groups. Co-M mainly affects patients in their 5th or 6th decades and above; it is rare in children and there is no gender predilection [14,39,40,45,46]. The disease specific survival rate for Co-M is estimated to be 82.9% for 5 years and 69.3% for 10 years [30,40].
Although the incidence if Co-M is substantially lower than cutaneous melanoma, if incidence is adjusted to tissue surface area, the incidence is similar. A study from the USA estimated the incidence of Co-M to be 0.4 per million persons/year and the incidence of cutaneous melanoma to be at 153.5/ million persons per year [47]. The average skin area for an average human adult is 1.7m2 [48] and the conjunctiva area per eye is 17.6cm2 [49]. If the incidence of each melanoma is now calculated proportionately to the area, the incidence for cutaneous melanoma would be approximately 90 per million m2 of skin per year, and for Co-M incidence estimated at 113 per million m2 of conjunctiva per year [18]. Importantly, this puts Co-M in perspective considering the conjunctival size and although it shares similarities with skin melanoma, is hugely under researched in comparison [10].
Driver-mutations and copy-number variations in multiple chromosomes have been described in Co-M, with high-frequency mutations in NF1 (33-50%), BRAF (29-46%), and NRAS mutations (11-26%) and ATRX (25%) genes [6,12,13,14,15,16,17,50,51,52,53,54]. The latter often occurs together with an NF1 mutation [13]. NRAS mutations are associated with higher metastatic risk [13,17]. TERT promoter mutations have also been identified in up to 54% of Co-M [13,17,55,56] and even in PAM with atypia (~8%) [57]. Cisarova et al, demonstrated that the TGCA-proposed genomic classification of cutaneous melanoma (defined by the most frequently mutated genes: BRAF, NF1, RAS and triple wild-type) was also applicable to Co-M [12]. A summary of the common gene mutations is presented in Table 1.
3. Precursor lesions (C-MIL)
Approximately 70% of Co-M arise from conjunctival melanocytic intraepithelial lesions (C-MIL), also known as conjunctival melanocytic intraepithelial neoplasia (C-MIN) or primary acquired melanosis (PAM), whilst a smaller proportion develop from pre-existing nevi or de novo [3,4,61,62]. C-MIL, a precursor or preinvasive disease to Co-M, encompass a spectrum of morphological changes ranging from melanocytic hyperplasia through degrees of melanocytic atypia to melanoma in situ [63].
Both C-MIL and Co-M most frequently develop in the interpalpebral zone suggesting an association with ultraviolet (UV) radiation [45] with a number of studies revealing UV signatures (C > T transitions) [12,64,65,66]. However, both can also develop in non-sun-exposed sites but the mechanisms for this are unknown [18].
4. Clinical presentation and assessment
Co-M is often unilateral and can affect any part of the conjunctiva but commonly presents on the bulbar surface, near the limbus (Figure 1). Invasion of the cornea, eyelid, sclera or orbit may occur in advanced tumours [4]. The lesions vary in size, shape and colour. Nodular masses may be well circumscribed, while flat lesions may have irregular, ill-defined margins, especially where there is adjacent C-MIL. Colour may range from amelanotic (pinkish) to various shades of brown or even black and be patchy or mixed within the one lesion [68]. Patients may present on noticing a mass with/without pigmentation on their eye but can also have significant visual morbidities, such as: irritation/burning with redness and reflex tearing, dry eye, pain, vision disturbance, double vision or vision loss [4,69,70].
Differential diagnoses of Co-M, include benign conjunctival nevi, extraocular extension of uveal melanoma or melanocytoma (black lesions), pigmented conjunctival squamous cell carcinoma, or very rarely metastasis of cutaneous melanoma. In amelanotic lesions, differentials also include conjunctival squamous intraepithelial neoplasia, squamous cell carcinoma or lymphoma [70]. Lack of cysts (often observed in conjunctival nevi), tumour haemorrhage, large/deep tumour, tortuous feeder vessels, adherence to underlying and invasion into surrounding structures, and multifocal lesions favour melanoma over conjunctival nevus [71].
C-MIL are unilateral but most often multifocal, can involve any part of the conjunctiva (bulbar, limbal, forniceal, and palpebral, in order of decreasing frequency) (Figure 1), and may extend to the caruncle, plica and cornea. They appear as mobile, flat, irregular brown pigmented conjunctival discolorations, which may change over time [14,22,23,39,40,67]. Rarely, C-MIL can be amelanotic, making it diagnostically challenging [22,23]. Differential diagnoses of C-MIL include: benign epithelial melanosis, oculodermal melanocytosis, conjunctival nevi, Co-M, pigmented conjunctival squamous intraepithelial neoplasia [72], Addison’s disease [73], post-inflammatory hyperpigmentation, and conjunctival tattooing [74].
Imaging of all conjunctival melanocytic lesions involves regular anterior segment photo-documentation (including with eversion of eyelids), slit lamp biomicroscopy, and possibly ultrasound (to estimate tumour thickness or look for orbital involvement). There are recent developments in anterior segment optical coherence tomography [75,76] and in vivo reflectance confocal microscopy [77]. Where Co-M has locally extended into the eyelid and particularly if there is any suspicion of orbital or nasolacrimal invasion, MRI has a critical role in the assessment; diffusion and perfusion-weighted imaging can help in differentiating Co-M from other eyelid masses [78].
5. Histomorphological features
Co-M shares similar histomorphological features to those of cutaneous or other mucosal invasive melanoma [79]. The intraepithelial (radial) component can be nested, pagetoid, lentiginous, or rarely absent. It can also extend beyond the invasive component and involve adjacent structures. The invasive stromal (vertical) component can comprise nests or sheets of atypical melanocytes with cytomorphology ranging from small naevoid-type cells to highly atypical pleomorphic melanocytes with spindle or epithelioid type. Nuclei can be hyperchromatic with inconspicuous nucleoli or vesicular with prominent eosinophilic nucleoli (Figure 2). Ulceration, mitotic activity, angiotropism, satellites in transit metastases, and neurotropism may be seen. A pre-existing nevus also may be present. Melanophages and variable lymphocytic infiltrate are also often observed. Increased mitoses (> 5.5 mitoses/mm2) have been associated with nodal metastasis; ulceration and greater tumour thickness have been associated with increased mortality similar to skin melanoma [80,81].
The key histomorphological features in C-MIL are increased cellularity/hyperplasia of intraepithelial conjunctival melanocytes with increasing cytological atypia, but the basement membrane remains intact [79,82,83]. The spectrum of cytological features ranges from small melanocytes with nuclear hyperchromasia and scant cytoplasm to severely atypical large pleomorphic epithelioid cells with ample cytoplasm and prominent eosinophilic nucleoli. The range of atypical architectural patterns include linear hyperplasia of basal melanocytes to confluent lentiginous spread, intraepithelial nests, pagetoid growth, and full thickness epithelial involvement by atypical melanocytes, i.e., melanoma in situ. Nests, pagetoid spread and confluent growth extend upward from the basal epithelium, displacing squamous and/or goblet cells but there should be no evidence of invasive growth [63,79,82,83]. Epithelioid cell morphology with cytological atypia, nesting and pagetoid spread are associated with an increased risk of recurrence and progression to Co-M [23,79,82,84,85].
Terminologies more commonly used to classify these lesions include PAM with atypia and C-MIN, and the most recently validated C-MIL [83,86]. Various grading or scoring systems have been used for C-MIL [22,73,82,83,85,87,88,89]. The grading of the cytological atypia in PAM (mild, moderate, or severe), which was similar to those used in the skin and other mucosal sites [82,84], suffered from poor reproducibility between pathologists. The C-MIN scoring system was based on architectural features (i.e., horizontal, and vertical spread) and cytological atypia but can be time-consuming and complex [87].
In 2018, the 4th ‘WHO Classification of Eye Tumours’ proposed the C-MIL classification, simplifying the grading of these lesions and capturing their risk of disease progression to invasive melanoma [90]. This comprised: 1) low-grade C-MIL (corresponding to PAM with or without mild atypia or C-MIN scores 1-2; 2) high-grade C-MIL (PAM with moderate to severe atypia or C-MIN 3-5); and 3) conjunctival melanoma in-situ (PAM with severe atypia involving >75% of the epithelium or a C-MIN score >5). The system was validated in 2021 and was found that all 3 classification systems (C-MIL, C-MIN and PAM) had comparable accuracy in their ability to identify lesions with potential for recurrence [83]. In 2022, the editorial panel of the 5th edition decided to revise the classification scheme because the low-grade C-MIL in the 4th edition incorporated both non-neoplastic and neoplastic melanocytic proliferations. This led to the current system as summarised in Table 2 [63]. This was validated by a large international collaborative study and found to have substantial interobserver agreement, good reproducibility, be predictive of recurrence and invasive disease, and importantly, inform clinical treatment thresholds [86]. Photomicrographs demonstrating the C-MIL scoring grades are presented in Figure 3 [86].
All conjunctival melanocytic lesions immunohistochemically show MelanA (MART1), S100, SOX10, HMB45 (should only be present in superficial areas of nevi) and MITF (Melanocyte Inducing Transcription Factor). Nuclear expression of PRAME (Preferentially expressed Antigen in Melanoma), cyclin D1 positive and loss of p16 on immunohistochemistry can also be helpful in distinguishing Co-M from nevi or low grade C-MIL (both PRAME and cyclin D1 negative, p16 positive) [53,86,91,92,93,94]. PD-L1 may be expressed [95].
6. Treatment and prognosis
Approximately 70% of all Co-M arises from high grade C-MIL [73]; hence there is an absolute clinical need to know when to treat patients [22,23,86]. There is no standard-of-care for C-MIL or Co-M; consequently, management varies considerably between ophthalmic and specialised ocular oncology centres. This includes: surgical excision (wide local) +/- amniotic membrane allograft and +/- adjuvant cryotherapy, topical chemotherapy (mitomycin C, 5-fluorouracil or interferon alpha-2b), radiotherapy (brachytherapy, proton beam or photon external beam) or radical orbital exenteration for advanced cases with local tissue invasion [4,22,23,32,70].
Reported usefulness of sentinel lymph node biopsy (SLNB) is variable (in terms of clinical management and sensitivity of pickup) but shown to be effective for Co-M >2mm thickness and/or >10mm in diameter [99].
The postoperative complications rate (vision loss, scarring, limbal stem cell failure, ulceration/non-healing defects, etc) and risk of tumour recurrence are very high (33-61%), warranting close life-long follow-up [4,28,29,30,31,70]. Lymph node metastases are common (~25-52%; preauricular, parotid, submandibular and/or cervical nodes, depending on Co-M location) but may also involve the liver, lungs and brain (11-42%). Poor prognostic indicators/risk factors for nodal and systemic metastases, include a non-epibulbar locations, ulceration and increased tumour thickness [32,33,61,62,80,81]. The 5-year and 10-year disease-specific mortality rate is ~14-27% and 25-35%, respectively [4,30,32,33,61,62,70,100]. Similarly to the risk of metastases, tumour-related death has been associated with de novo origin, non-bulbar conjunctival location, nodular growth, multifocal lesions, and sentinel lymph node positivity [4,30,43,80,101].
The use of genetics for prognostication in Co-M is currently limited. However, as mentioned above, Co-M has genetic alterations similar to those of cutaneous melanoma, and advances in characterising Co-M genetics are offering insight into potential targeted therapies that are already in use for the treatment of cutaneous melanoma. Data on Co-M (anti-BRAF; anti-MEK; anti-PD-L1) with targeted/immunotherapies have shown promising results but are limited, with only those from small case series or single case studies in patients with inoperable disease or as first-line therapy prior surgery in advanced cases [18,34,35,38,102]. A summary of targeted therapies and immune checkpoint inhibitors are presented in Table 3 [103,104,105,106] and 4 [107,108,109], respectively. A Phase 2 clinical trial using a combination of axitinib and nivolumab in untreated advanced or metastatic mucosal melanoma (head & neck and conjunctival; NCT05384496) is underway.
7. Conclusions and future directions
Co-M is a rare, aggressive, invasive eye and eyelid cancer with increasing global incidence. Given the rarity of Co-M, international collaboration is pivotal to obtain sufficient numbers in order to progress translational research and enlist Co-M patients into clinical trials. The recent developments in cancer genetics and immunology present exciting new frontiers in better understanding of Co-M pathogenesis, and importantly provide new targets for therapy. Insight into the molecular drivers for Co-M development and its integration with clinical and histomorphological evaluation will allow earlier diagnosis, improve risk stratification and prognostication, and identify patients for specific therapies (i.e. ‘personalised/precision medicine’). This will further enable the development of clear management guidelines and enrolment into targeted therapies earlier than current practice, facilitating improved outcomes in this rare disease.
Author Contributions
Conceptualization, YK; writing – original draft preparation, KB, YK; writing – review and editing, KB, YK, RH, SEC; supervision, YK. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- E. Triay, L. Bergman, B. Nilsson, C. All-Ericsson, and S. Seregard, "Time trends in the incidence of conjunctival melanoma in Sweden," (in eng), Br J Ophthalmol, vol. 93, no. 11, pp. 1524-8, Nov 2009. [CrossRef]
- G. Virgili et al., "Incidence and Survival of Patients With Conjunctival Melanoma in Europe," (in eng), JAMA Ophthalmol, vol. 138, no. 6, pp. 601-608, Jun 01 2020. [CrossRef]
- C. Larsen et al., "A Retrospective Review of Conjunctival Melanoma Presentation, Treatment, and Outcome and an Investigation of Features Associated With BRAF Mutations," (in eng), JAMA Ophthalmol, vol. 133, no. 11, pp. 1295-303, Nov 2015. [CrossRef]
- L. Shields et al., "Conjunctival melanoma: outcomes based on tumor origin in 382 consecutive cases," (in eng), Ophthalmology, vol. 118, no. 2, pp. 389-95.e1-2, Feb 2011. [CrossRef]
- H. E. Spendlove, B. E. Damato, J. Humphreys, K. T. Barker, P. S. Hiscott, and R. S. Houlston, "BRAF mutations are detectable in conjunctival but not uveal melanomas," (in eng), Melanoma Res, vol. 14, no. 6, pp. 449-52, Dec 2004. [CrossRef]
- N. Kenawy et al., "Conjunctival melanoma copy number alterations and correlation with mutation status, tumor features, and clinical outcome," (in eng), Pigment Cell Melanoma Res, vol. 32, no. 4, pp. 564-575, Jul 2019. [CrossRef]
- S. L. Lake, F. Jmor, J. Dopierala, A. F. Taktak, S. E. Coupland, and B. E. Damato, "Multiplex ligation-dependent probe amplification of conjunctival melanoma reveals common BRAF V600E gene mutation and gene copy number changes," (in eng), Invest Ophthalmol Vis Sci, vol. 52, no. 8, pp. 5598-604, Jul 29 2011. [CrossRef]
- K. N. Smit, M. J. Jager, A. de Klein, and E. Kiliҫ, "Uveal melanoma: Towards a molecular understanding," (in eng), Prog Retin Eye Res, vol. 75, p. 100800, Mar 2020. [CrossRef]
- M. J. Jager et al., "Uveal melanoma," (in eng), Nat Rev Dis Primers, vol. 6, no. 1, p. 24, Apr 09 2020. [CrossRef]
- M. Rodrigues et al., "So Close, yet so Far: Discrepancies between Uveal and Other Melanomas. A Position Paper from UM Cure 2020," (in eng), Cancers (Basel), vol. 11, no. 7, Jul 22 2019. [CrossRef]
- L. H. Mikkelsen, A. C. Larsen, C. von Buchwald, K. T. Drzewiecki, J. U. Prause, and S. Heegaard, "Mucosal malignant melanoma - a clinical, oncological, pathological and genetic survey," (in eng), APMIS, vol. 124, no. 6, pp. 475-86, Jun 2016. [CrossRef]
- K. Cisarova et al., "Genomic and transcriptomic landscape of conjunctival melanoma," (in eng), PLoS Genet, vol. 16, no. 12, p. e1009201, Dec 2020. [CrossRef]
- S. E. Lally et al., "Mutational Landscape and Outcomes of Conjunctival Melanoma in 101 Patients," (in eng), Ophthalmology, vol. 129, no. 6, pp. 679-693, Jun 2022. [CrossRef]
- C. Larsen et al., "BRAF mutations in conjunctival melanoma: investigation of incidence, clinicopathological features, prognosis and paired premalignant lesions," (in eng), Acta Ophthalmol, vol. 94, no. 5, pp. 463-70, Aug 2016. [CrossRef]
- S. L. Scholz et al., "NF1 mutations in conjunctival melanoma," (in eng), Br J Cancer, vol. 118, no. 9, pp. 1243-1247, May 2018. [CrossRef]
- S. Gardrat et al., "Definition of Biologically Distinct Groups of Conjunctival Melanomas According to Etiological Factors and Implications for Precision Medicine," (in eng), Cancers (Basel), vol. 13, no. 15, Jul 30 2021. [CrossRef]
- N. M. van Poppelen et al., "Molecular Genetics of Conjunctival Melanoma and Prognostic Value of," (in eng), Int J Mol Sci, vol. 22, no. 11, May 28 2021. [CrossRef]
- N. J. Brouwer, R. M. Verdijk, S. Heegaard, M. Marinkovic, B. Esmaeli, and M. J. Jager, "Conjunctival melanoma: New insights in tumour genetics and immunology, leading to new therapeutic options," (in eng), Prog Retin Eye Res, vol. 86, p. 100971, Jan 2022. [CrossRef]
- M. Krauthammer et al., "Exome sequencing identifies recurrent mutations in NF1 and RASopathy genes in sun-exposed melanomas," (in eng), Nat Genet, vol. 47, no. 9, pp. 996-1002, Sep 2015. [CrossRef]
- J. Wolf et al., "Transcriptional characterization of conjunctival melanoma identifies the cellular tumor microenvironment and prognostic gene signatures," (in eng), Sci Rep, vol. 10, no. 1, p. 17022, Oct 12 2020. [CrossRef]
- L. H. Mikkelsen et al., "The molecular profile of mucosal melanoma," (in eng), Melanoma Res, vol. 30, no. 6, pp. 533-542, Dec 2020. [CrossRef]
- B. Damato and S. E. Coupland, "Conjunctival melanoma and melanosis: a reappraisal of terminology, classification and staging," (in eng), Clin Exp Ophthalmol, vol. 36, no. 8, pp. 786-95, Nov 2008. [CrossRef]
- J. A. Shields et al., "Primary acquired melanosis of the conjunctiva: risks for progression to melanoma in 311 eyes. The 2006 Lorenz E. Zimmerman lecture," (in eng), Ophthalmology, vol. 115, no. 3, pp. 511-519.e2, Mar 2008. [CrossRef]
- C. V. Miller et al., "Clinical outcome of advanced squamous cell carcinoma of the conjunctiva," (in eng), Eye (Lond), vol. 28, no. 8, pp. 962-7, Aug 2014. [CrossRef]
- N. Kenawy, A. Garrick, H. Heimann, S. E. Coupland, and B. E. Damato, "Conjunctival squamous cell neoplasia: the Liverpool Ocular Oncology Centre experience," (in eng), Graefes Arch Clin Exp Ophthalmol, vol. 253, no. 1, pp. 143-50, Jan 2015. [CrossRef]
- J. Yang and C. S. Foster, "Squamous cell carcinoma of the conjunctiva," (in eng), Int Ophthalmol Clin, vol. 37, no. 4, pp. 73-85, 1997. [CrossRef]
- Y. A. Yousef and P. T. Finger, "Squamous carcinoma and dysplasia of the conjunctiva and cornea: an analysis of 101 cases," (in eng), Ophthalmology, vol. 119, no. 2, pp. 233-40, Feb 2012. [CrossRef]
- G. K. Vora, H. Demirci, B. Marr, and P. Mruthyunjaya, "Advances in the management of conjunctival melanoma," (in eng), Surv Ophthalmol, vol. 62, no. 1, pp. 26-42, 2017. [CrossRef]
- S. Kaštelan, A. Gverović Antunica, L. Beketić Orešković, J. Salopek Rabatić, B. Kasun, and I. Bakija, "Conjunctival Melanoma - Epidemiological Trends and Features," (in eng), Pathol Oncol Res, vol. 24, no. 4, pp. 787-796, Oct 2018. [CrossRef]
- D. Paridaens, D. C. Minassian, A. C. McCartney, and J. L. Hungerford, "Prognostic factors in primary malignant melanoma of the conjunctiva: a clinicopathological study of 256 cases," (in eng), Br J Ophthalmol, vol. 78, no. 4, pp. 252-9, Apr 1994. [CrossRef]
- P. De Potter, C. L. Shields, J. A. Shields, and H. Menduke, "Clinical predictive factors for development of recurrence and metastasis in conjunctival melanoma: a review of 68 cases," (in eng), Br J Ophthalmol, vol. 77, no. 10, pp. 624-30, Oct 1993. [CrossRef]
- N. J. Brouwer, M. Marinkovic, S. G. van Duinen, J. C. Bleeker, M. J. Jager, and G. P. M. Luyten, "Treatment of conjunctival melanoma in a Dutch referral centre," (in eng), Br J Ophthalmol, vol. 102, no. 9, pp. 1277-1282, Sep 2018. [CrossRef]
- B. Esmaeli, "Patterns of regional and distant metastasis in patients with conjunctival melanoma: experience a cancer centre over four decades," vol. 11713086, no. 108, pp. 2101-5, 2001. [CrossRef]
- Sagiv et al., "Immunotherapy With Programmed Cell Death 1 Inhibitors for 5 Patients With Conjunctival Melanoma," (in eng), JAMA Ophthalmol, vol. 136, no. 11, pp. 1236-1241, Nov 01 2018. [CrossRef]
- P. T. Finger and A. C. Pavlick, "Checkpoint inhibition immunotherapy for advanced local and systemic conjunctival melanoma: a clinical case series," (in eng), J Immunother Cancer, vol. 7, no. 1, p. 83, Mar 25 2019. [CrossRef]
- E. Chang, H. Demirci, and F. Y. Demirci, "Genetic Aspects of Conjunctival Melanoma: A Review," (in eng), Genes (Basel), vol. 14, no. 9, Aug 23 2023. [CrossRef]
- B. Esmaeli and O. Sagiv, "Targeted Biological Drugs and Immune Check Point Inhibitors for Locally Advanced or Metastatic Cancers of the Conjunctiva, Eyelid, and Orbit," (in eng), Int Ophthalmol Clin, vol. 59, no. 2, pp. 13-26, 2019. [CrossRef]
- E. Rossi et al., "Dabrafenib and Trametinib in BRAF Mutant Metastatic Conjunctival Melanoma," (in eng), Front Oncol, vol. 9, p. 232, 2019. [CrossRef]
- P. Isager et al., "Uveal and conjunctival malignant melanoma in Denmark, 1943-97: incidence and validation study," (in eng), Ophthalmic Epidemiol, vol. 12, no. 4, pp. 223-32, Aug 2005. [CrossRef]
- S. Tuomaala, S. Eskelin, A. Tarkkanen, and T. Kivelä, "Population-based assessment of clinical characteristics predicting outcome of conjunctival melanoma in whites," (in eng), Invest Ophthalmol Vis Sci, vol. 43, no. 11, pp. 3399-408, Nov 2002.
- F. M. Ghazawi et al., "Incidence trends of conjunctival malignant melanoma in Canada," (in eng), Br J Ophthalmol, vol. 104, no. 1, pp. 23-25, Jan 2020. [CrossRef]
- D. N. Hu, G. Yu, S. A. McCormick, and P. T. Finger, "Population-based incidence of conjunctival melanoma in various races and ethnic groups and comparison with other melanomas," (in eng), Am J Ophthalmol, vol. 145, no. 3, pp. 418-423, Mar 2008. [CrossRef]
- C. L. Shields, J. L. Chien, T. Surakiatchanukul, K. Sioufi, S. E. Lally, and J. A. Shields, "Conjunctival Tumors: Review of Clinical Features, Risks, Biomarkers, and Outcomes--The 2017 J. Donald M. Gass Lecture," (in eng), Asia Pac J Ophthalmol (Phila), vol. 6, no. 2, pp. 109-120, 2017. [CrossRef]
- T. A. Weppelmann, K. T. Zimmerman, and V. Rashidi, "Trends in Incidence of Conjunctival Melanoma in the US," (in eng), JAMA Netw Open, vol. 5, no. 10, p. e2237229, Oct 03 2022. [CrossRef]
- G. P. Yu, D. N. Hu, S. McCormick, and P. T. Finger, "Conjunctival melanoma: is it increasing in the United States?," (in eng), Am J Ophthalmol, vol. 135, no. 6, pp. 800-6, Jun 2003. [CrossRef]
- B. W. R. Balzer, S. Cherepanoff, A. M. Joshua, M. Giblin, R. M. Conway, and A. C. Anazodo, "Conjunctival Melanoma in Childhood and Adolescence: A Systematic Review," (in eng), Ocul Oncol Pathol, vol. 5, no. 6, pp. 387-395, Oct 2019. [CrossRef]
- C. C. McLaughlin, X. C. Wu, A. Jemal, H. J. Martin, L. M. Roche, and V. W. Chen, "Incidence of noncutaneous melanomas in the U.S," (in eng), Cancer, vol. 103, no. 5, pp. 1000-7, Mar 01 2005. [CrossRef]
- M. Waugh, "Roxburgh's Common Skin Diseases," (in eng), Skinmed, vol. 20, no. 4, p. 320, 2022.
- M. A. Watsky, M. M. Jablonski, and H. F. Edelhauser, "Comparison of conjunctival and corneal surface areas in rabbit and human," (in eng), Curr Eye Res, vol. 7, no. 5, pp. 483-6, May 1988. [CrossRef]
- N. Goldenberg-Cohen et al., "T1799A BRAF mutations in conjunctival melanocytic lesions," (in eng), Invest Ophthalmol Vis Sci, vol. 46, no. 9, pp. 3027-30, Sep 2005. [CrossRef]
- J. Cao et al., "Targeting of the MAPK and AKT pathways in conjunctival melanoma shows potential synergy," (in eng), Oncotarget, vol. 8, no. 35, pp. 58021-58036, Aug 29 2017. [CrossRef]
- K. G. Griewank et al., "Conjunctival melanomas harbor BRAF and NRAS mutations and copy number changes similar to cutaneous and mucosal melanomas," (in eng), Clin Cancer Res, vol. 19, no. 12, pp. 3143-52, Jun 15 2013. [CrossRef]
- El Zaoui et al., "Conjunctival Melanoma Targeted Therapy: MAPK and PI3K/mTOR Pathways Inhibition," (in eng), Invest Ophthalmol Vis Sci, vol. 60, no. 7, pp. 2764-2772, Jun 03 2019. [CrossRef]
- H. Francis, H. E. Grossniklaus, L. A. Habib, B. Marr, D. H. Abramson, and K. J. Busam, "BRAF, NRAS, and GNAQ Mutations in Conjunctival Melanocytic Nevi," (in eng), Invest Ophthalmol Vis Sci, vol. 59, no. 1, pp. 117-121, Jan 01 2018. [CrossRef]
- van Ipenburg et al., "Prognostic value of," (in eng), Br J Ophthalmol, vol. 105, no. 10, pp. 1454-1461, Oct 2021. [CrossRef]
- G. Griewank et al., "TERT promoter mutations in ocular melanoma distinguish between conjunctival and uveal tumours," (in eng), Br J Cancer, vol. 109, no. 2, pp. 497-501, Jul 23 2013. [CrossRef]
- E. Koopmans et al., "Prevalence and implications of TERT promoter mutation in uveal and conjunctival melanoma and in benign and premalignant conjunctival melanocytic lesions," (in eng), Invest Ophthalmol Vis Sci, vol. 55, no. 9, pp. 6024-30, Aug 26 2014. [CrossRef]
- Alessandrini et al., "C-Kit SCF receptor (CD117) expression and KIT gene mutation in conjunctival pigmented lesions," (in eng), Acta Ophthalmol, vol. 91, no. 8, pp. e641-5, Dec 2013. [CrossRef]
- Beadling et al., "KIT gene mutations and copy number in melanoma subtypes," (in eng), Clin Cancer Res, vol. 14, no. 21, pp. 6821-8, Nov 01 2008. [CrossRef]
- X. Sheng et al., "Prognostic factors for conjunctival melanoma: a study in ethnic Chinese patients," (in eng), Br J Ophthalmol, vol. 99, no. 7, pp. 990-6, Jul 2015. [CrossRef]
- G. S. Missotten, S. Keijser, R. J. De Keizer, and D. De Wolff-Rouendaal, "Conjunctival melanoma in the Netherlands: a nationwide study," (in eng), Invest Ophthalmol Vis Sci, vol. 46, no. 1, pp. 75-82, Jan 2005. [CrossRef]
- C. L. Shields, S. Kaliki, S. A. Al-Dahmash, S. E. Lally, and J. A. Shields, "American Joint Committee on Cancer (AJCC) clinical classification predicts conjunctival melanoma outcomes," (in eng), Ophthalmic Plast Reconstr Surg, vol. 28, no. 5, pp. 313-23, 2012. [CrossRef]
- S. E. Coupland, T. Milman, R. M. Verdict, and N. J. Brouwer, Conjunctival Melanocytic Intraepithelial Lesions In: WHO Classification of Tumours Editorial Board. Eye tumours [Internet; beta version ahead of print] 5th ed. (WHO classification of tumours). Lyon (France): International Agency for Research on Cancer, 2023.
- H. Demirci et al., "Integrative Exome and Transcriptome Analysis of Conjunctival Melanoma and Its Potential Application for Personalized Therapy," (in eng), JAMA Ophthalmol, vol. 137, no. 12, pp. 1444-1448, Dec 01 2019. [CrossRef]
- P. A. Mundra et al., "Ultraviolet radiation drives mutations in a subset of mucosal melanomas," (in eng), Nat Commun, vol. 12, no. 1, p. 259, Jan 11 2021. [CrossRef]
- C. Rivolta et al., "UV light signature in conjunctival melanoma; not only skin should be protected from solar radiation," (in eng), J Hum Genet, vol. 61, no. 4, pp. 361-2, Apr 2016. [CrossRef]
- Y. J. Lee, C. Lee, M. K. Kim, S. I. Khwarg, and J. Y. Oh, "Conjunctival pigmented lesion: Clinicopathological analysis of 85 cases in Korean population," (in eng), Sci Rep, vol. 9, no. 1, p. 18204, Dec 03 2019. [CrossRef]
- J. Brouwer, M. Marinkovic, G. P. M. Luyten, C. L. Shields, and M. J. Jager, "Lack of tumour pigmentation in conjunctival melanoma is associated with light iris colour and worse prognosis," (in eng), Br J Ophthalmol, vol. 103, no. 3, pp. 332-337, Mar 2019. [CrossRef]
- C. L. Shields et al., "Conjunctival melanoma: risk factors for recurrence, exenteration, metastasis, and death in 150 consecutive patients," (in eng), Arch Ophthalmol, vol. 118, no. 11, pp. 1497-507, Nov 2000. [CrossRef]
- J. R. Wong, A. A. Nanji, A. Galor, and C. L. Karp, "Management of conjunctival malignant melanoma: a review and update," (in eng), Expert Rev Ophthalmol, vol. 9, no. 3, pp. 185-204, Jun 2014. [CrossRef]
- C. L. Shields et al., "Clinical Features Differentiating Benign From Malignant Conjunctival Tumors in Children," (in eng), JAMA Ophthalmol, vol. 135, no. 3, pp. 215-224, Mar 01 2017. [CrossRef]
- F. S. D. Cruz, S. F. S. D. Cruz, D. H. Ishigai, K. S. Santos, and S. Felberg, "Conjunctival tattoo: report on an emerging body modification trend," (in eng), Arq Bras Oftalmol, vol. 80, no. 6, pp. 399-400, 2017. [CrossRef]
- N. Kenawy, S. L. Lake, S. E. Coupland, and B. E. Damato, "Conjunctival melanoma and melanocytic intra-epithelial neoplasia," (in eng), Eye (Lond), vol. 27, no. 2, pp. 142-52, Feb 2013. [CrossRef]
- C. L. Shields, A. Manchandia, R. Subbiah, R. C. Eagle, and J. A. Shields, "Pigmented squamous cell carcinoma in situ of the conjunctiva in 5 cases," (in eng), Ophthalmology, vol. 115, no. 10, pp. 1673-8, Oct 2008. [CrossRef]
- E. Vizvári, Á. Skribek, N. Polgár, A. Vörös, P. Sziklai, and E. Tóth-Molnár, "Conjunctival melanocytic naevus: Diagnostic value of anterior segment optical coherence tomography and ultrasound biomicroscopy," (in eng), PLoS One, vol. 13, no. 2, p. e0192908, 2018. [CrossRef]
- N. J. Brouwer, M. Marinkovic, J. C. Bleeker, G. P. M. Luyten, and M. J. Jager, "Anterior Segment OCTA of Melanocytic Lesions of the Conjunctiva and Iris," (in eng), Am J Ophthalmol, vol. 222, pp. 137-147, Feb 2021. [CrossRef]
- E. Cinotti et al., "Handheld In Vivo Reflectance Confocal Microscopy for the Diagnosis of Eyelid Margin and Conjunctival Tumors," (in eng), JAMA Ophthalmol, vol. 135, no. 8, pp. 845-851, Aug 01 2017. [CrossRef]
- T. A. Ferreira et al., "MR and CT Imaging of the Normal Eyelid and its Application in Eyelid Tumors," (in eng), Cancers (Basel), vol. 12, no. 3, Mar 12 2020. [CrossRef]
- Zembowicz, R. V. Mandal, and P. Choopong, "Melanocytic lesions of the conjunctiva," (in eng), Arch Pathol Lab Med, vol. 134, no. 12, pp. 1785-92, Dec 2010. [CrossRef]
- Esmaeli et al., "Greater Tumor Thickness, Ulceration, and Positive Sentinel Lymph Node Are Associated With Worse Prognosis in Patients With Conjunctival Melanoma: Implications for Future AJCC Classifications," (in eng), Am J Surg Pathol, vol. 43, no. 12, pp. 1701-1710, Dec 2019. [CrossRef]
- Esmaeli et al., "Histologic features of conjunctival melanoma predictive of metastasis and death (an American Ophthalmological thesis)," (in eng), Trans Am Ophthalmol Soc, vol. 110, pp. 64-73, Dec 2012.
- R. Folberg, I. W. McLean, and L. E. Zimmerman, "Primary acquired melanosis of the conjunctiva," (in eng), Hum Pathol, vol. 16, no. 2, pp. 129-35, Feb 1985. [CrossRef]
- T. Milman et al., "Validation of the Newly Proposed World Health Organization Classification System for Conjunctival Melanocytic Intraepithelial Lesions: A Comparison with the C-MIN and PAM Classification Schemes," (in eng), Am J Ophthalmol, vol. 223, pp. 60-74, Mar 2021. [CrossRef]
- Maly, D. Epstein, K. Meir, and J. Pe'er, "Histological criteria for grading of atypia in melanocytic conjunctival lesions," (in eng), Pathology, vol. 40, no. 7, pp. 676-81, Dec 2008. [CrossRef]
- M. Sugiura, K. A. Colby, M. C. Mihm, and A. Zembowicz, "Low-risk and high-risk histologic features in conjunctival primary acquired melanosis with atypia: Clinicopathologic analysis of 29 cases," (in eng), Am J Surg Pathol, vol. 31, no. 2, pp. 185-92, Feb 2007. [CrossRef]
- H. S. Mudhar et al., "A multicenter study validates the WHO 2022 classification for conjunctival melanocytic intraepithelial lesions with clinical and prognostic relevance," (in eng), Lab Invest, p. 100281, Nov 02 2023. [CrossRef]
- B. Damato and S. E. Coupland, "Management of conjunctival melanoma," (in eng), Expert Rev Anticancer Ther, vol. 9, no. 9, pp. 1227-39, Sep 2009. [CrossRef]
- F. A. Jakobiec, "Conjunctival Primary Acquired Melanosis: Is It Time for a New Terminology?," (in eng), Am J Ophthalmol, vol. 162, pp. 3-19.e1, Feb 2016. [CrossRef]
- F. A. Jakobiec, "Clinicopathologic characteristics of premalignant and malignant melanocytic lesions of the conjunctiva," vol. 96, R. Folberg and T. Iwamato, Eds., ed. Ophthalmology 1989, 1989, pp. 147-66.
- 90. C. G. Eberhart, S. E. Coupland, R. Folberg, C. Margo, and N. Rao, Conjunctival Melanocytic Intraepithelial Neoplasia In: WHO Classification of Tumours of the Eye 4th ed. Lyon, France: International Agency for Research on Cancer, 2018.
- D. Šekoranja, G. Hawlina, and J. Pižem, "PRAME expression in melanocytic lesions of the conjunctiva," (in eng), Histopathology, vol. 79, no. 6, pp. 989-996, Dec 2021. [CrossRef]
- R. E. LeBlanc, D. M. Miller, and M. E. Zegans, "PRAME immunohistochemistry is useful in the evaluation of conjunctival melanomas, nevi, and primary acquired melanosis," (in eng), J Cutan Pathol, vol. 48, no. 12, pp. 1442-1448, Dec 2021. [CrossRef]
- H. S. Mudhar, S. S. Salvi, D. Pissaloux, and A. de La Fouchardiere, "Single Time Frame Overview of the Genetic Changes in Conjunctival Melanoma from Intraepithelial Disease to Invasive Melanoma: A Study of 4 Exenteration Specimens Illustrating the Potential Role of Cyclin D1," (in eng), Ocul Oncol Pathol, vol. 8, no. 1, pp. 52-63, Feb 2022. [CrossRef]
- H. S. Mudhar et al., "PRAME expression by immunohistochemistry and reverse transcription quantitative PCR in conjunctival melanocytic lesions-a comprehensive clinicopathologic study of 202 cases and correlation of cytogenetics with PRAME expression in challenging conjunctival melanocytic lesions," (in eng), Hum Pathol, vol. 134, pp. 1-18, Apr 2023. [CrossRef]
- S. Lassalle et al., "PD-L1 Expression in 65 Conjunctival Melanomas and Its Association with Clinical Outcome," (in eng), Int J Mol Sci, vol. 21, no. 23, Nov 30 2020. [CrossRef]
- Jain et al., "Multicenter, International Assessment of the Eighth Edition of the American Joint Committee on Cancer Cancer Staging Manual for Conjunctival Melanoma," (in eng), JAMA Ophthalmol, vol. 137, no. 8, pp. 905-911, Aug 01 2019. [CrossRef]
- S. Jia et al., "American Joint Committee on Cancer Tumor Staging System Predicts the Outcome and Metastasis Pattern in Conjunctival Melanoma," (in eng), Ophthalmology, vol. 129, no. 7, pp. 771-780, Jul 2022. [CrossRef]
- TNM Classification of Malignant Tumours, 8th ed. Oxford, UK: Wiley-Blackwell, 2017, p. 272.
- V. M. Cohen, M. Tsimpida, J. L. Hungerford, H. Jan, R. Cerio, and G. Moir, "Prospective study of sentinel lymph node biopsy for conjunctival melanoma," (in eng), Br J Ophthalmol, vol. 97, no. 12, pp. 1525-9, Dec 2013. [CrossRef]
- M. Lim, T. Tatla, D. Hersh, and J. Hungerford, "Patterns of regional head and neck lymph node metastasis in primary conjunctival malignant melanoma," (in eng), Br J Ophthalmol, vol. 90, no. 12, pp. 1468-71, Dec 2006. [CrossRef]
- G. Anastassiou, A. Heiligenhaus, N. Bechrakis, E. Bader, N. Bornfeld, and K. P. Steuhl, "Prognostic value of clinical and histopathological parameters in conjunctival melanomas: a retrospective study," (in eng), Br J Ophthalmol, vol. 86, no. 2, pp. 163-7, Feb 2002. [CrossRef]
- J. M. Grimes, N. V. Shah, F. H. Samie, R. D. Carvajal, and B. P. Marr, "Conjunctival Melanoma: Current Treatments and Future Options," (in eng), Am J Clin Dermatol, vol. 21, no. 3, pp. 371-381, Jun 2020. [CrossRef]
- M. B. Pahlitzsch, EckartMai, Christian, "Conjunctival Melanoma and BRAF Inhibitor Therapy," Journal of Clinical and Experimental Ophthalmology, vol. Volume 5, no. 1, 2014.
- J. L. Weber, K. S. Smalley, V. K. Sondak, and G. T. Gibney, "Conjunctival melanomas harbor BRAF and NRAS mutations--Letter," (in eng), Clin Cancer Res, vol. 19, no. 22, pp. 6329-30, Nov 15 2013. [CrossRef]
- Maleka, G. Åström, P. Byström, and G. J. Ullenhag, "A case report of a patient with metastatic ocular melanoma who experienced a response to treatment with the BRAF inhibitor vemurafenib," (in eng), BMC Cancer, vol. 16, p. 634, Aug 12 2016. [CrossRef]
- S. Pinto Torres, T. André, E. Gouveia, L. Costa, and M. J. Passos, "Systemic Treatment of Metastatic Conjunctival Melanoma," (in eng), Case Rep Oncol Med, vol. 2017, p. 4623964, 2017. [CrossRef]
- B. Y. Hong et al., "Immune Checkpoint Inhibitor Therapy as an Eye-Preserving Treatment for Locally Advanced Conjunctival Melanoma," (in eng), Ophthalmic Plast Reconstr Surg, vol. 37, no. 1, pp. e9-e13, 2021 Jan-Feb 01 2021. [CrossRef]
- T. Kiyohara et al., "Two cases of BRAF-mutated, bulbar conjunctival melanoma, and review of the published literature," (in eng), Clin Exp Dermatol, vol. 45, no. 2, pp. 207-211, Mar 2020. [CrossRef]
- L. J. Chaves, B. Huth, J. J. Augsburger, and Z. M. Correa, "Eye-Sparing Treatment for Diffuse Invasive Conjunctival Melanoma," (in eng), Ocul Oncol Pathol, vol. 4, no. 4, pp. 261-266, Jun 2018. [CrossRef]
Figure 1.
anterior segment photographs of C-MIL and Co-M.
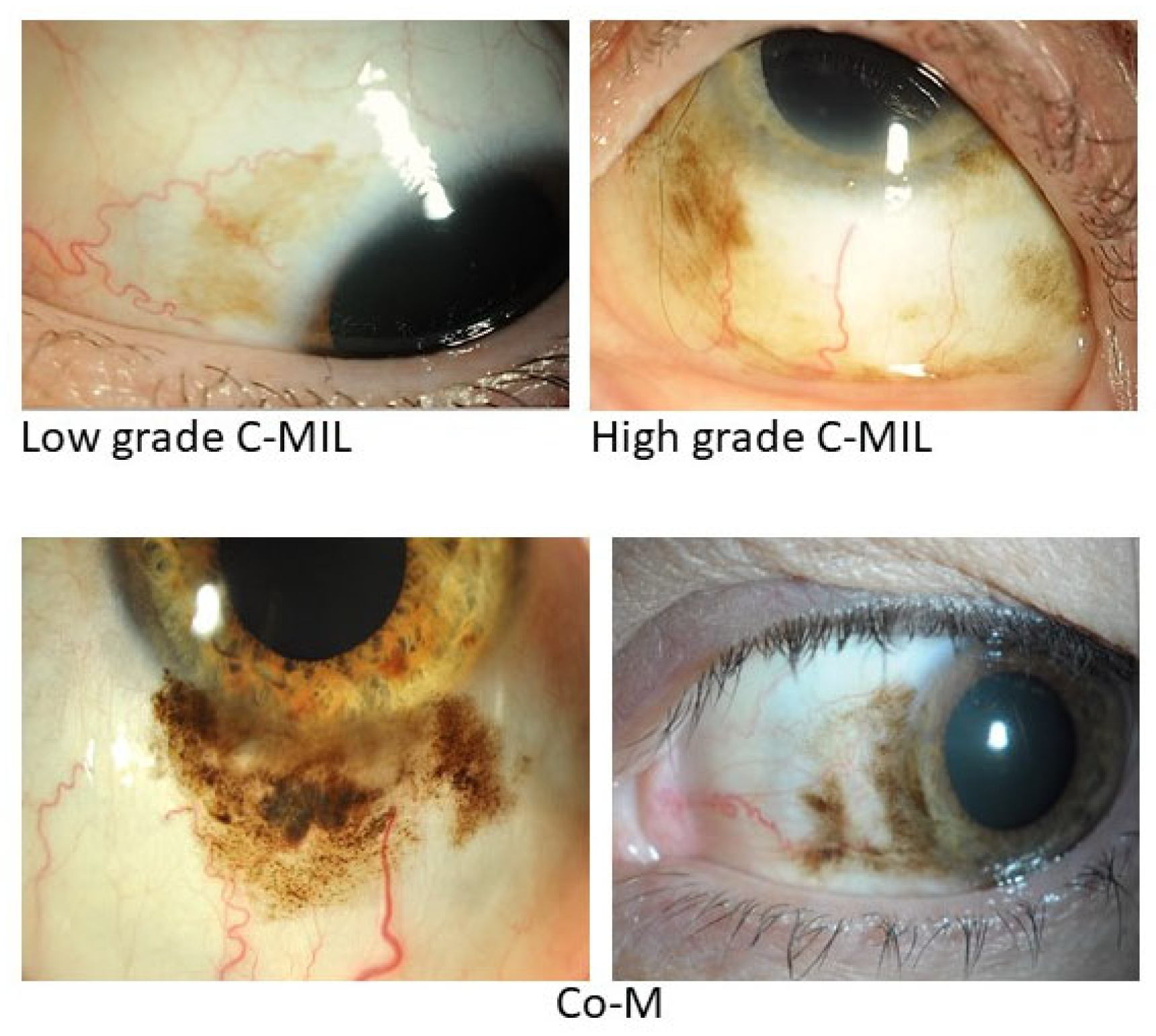
Figure 2.
Histomorphological H&E micrographs of Co-M.
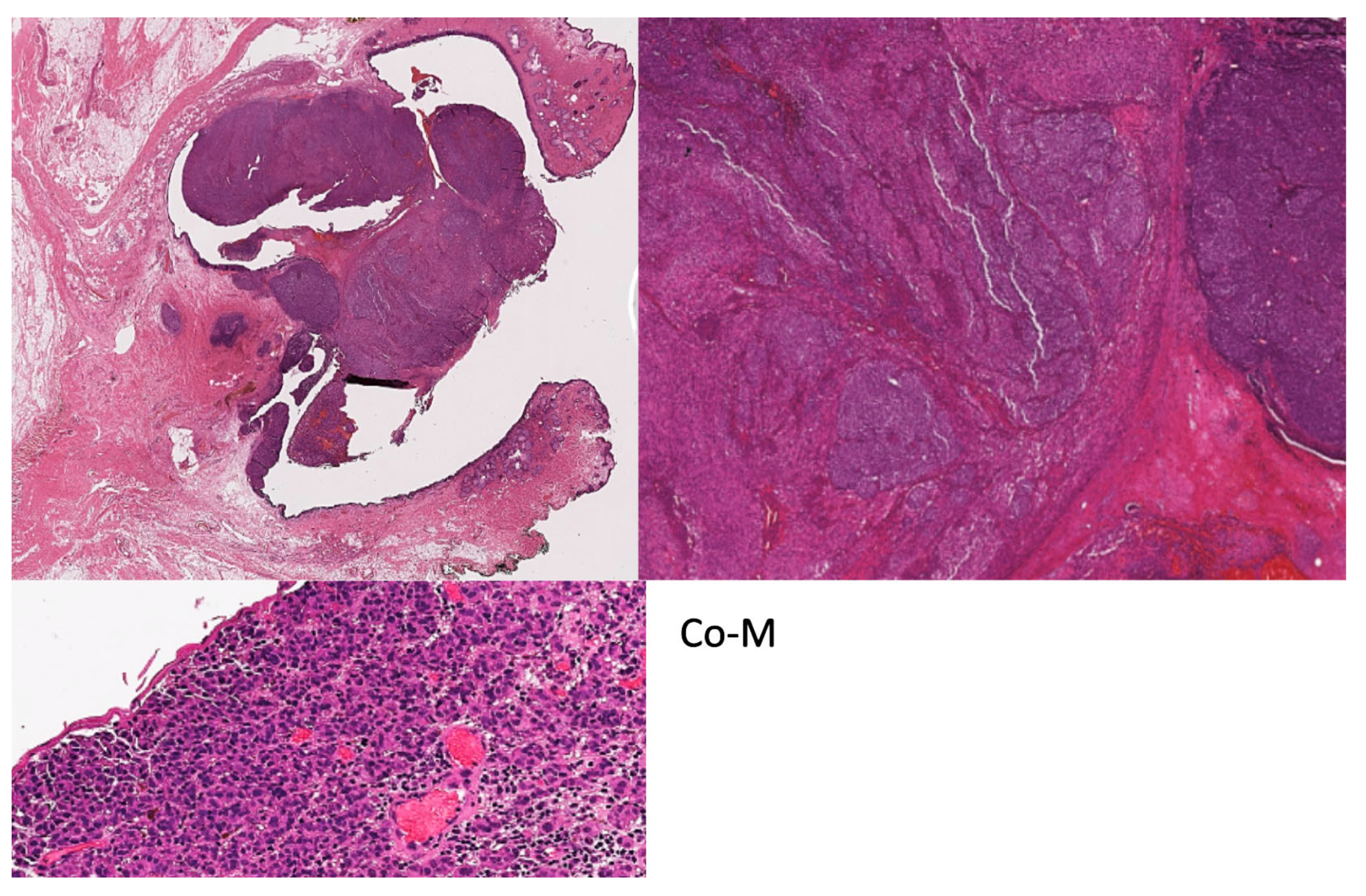
Figure 3.
Photomicrographs representing the C-MIL grading system [86].
Figure 3.
Photomicrographs representing the C-MIL grading system [86].
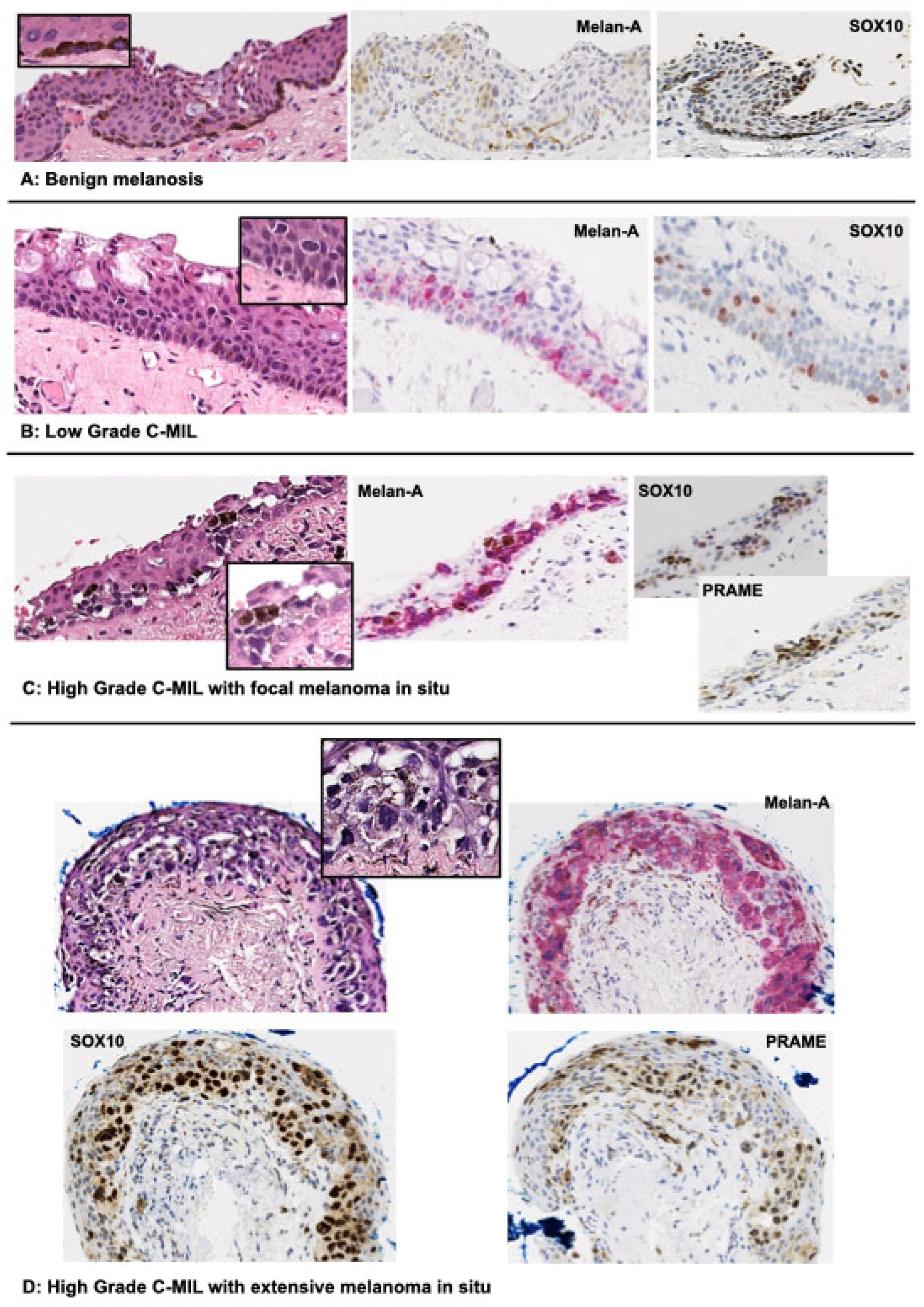

Table 1.
Common genetic mutations in conjunctival nevi, primary acquired melanosis (PAM) without atypia, PAM with atypia, and conjunctival melanoma (Co-M).
Table 1.
Common genetic mutations in conjunctival nevi, primary acquired melanosis (PAM) without atypia, PAM with atypia, and conjunctival melanoma (Co-M).
| Conjunctival nevi (%) | PAM without atypia (%) | PAM with atypia (%) | Prevalence in Co-M (%) | |
|---|---|---|---|---|
| BRAF | 14/28 (50%) (Goldenberg-Cohen et al., 2005) 13-23 (56%) (Francis et al., 2018) 7/37 (19%) (Cao et al., 2017) 9/12 (75%) (Larsen et al., 2016) 15/35 (43%) (El Zaoui et al., 2019) |
0/11 (0%) (Goldenberg-Cohen et al., 2005) 0/17 (0%) (Cao et al., 2017) |
0/4 (0%) (Goldenberg-Cohen et al., 2005) 0/13 (0%) (Cao et al., 2017) 2/8 (25%) (Larsen et al., 2016) |
4/15 (27%) (Beadling et al., 2008) 3/21 (14%) (Spendlove et al., 2004) 23/78 (29%) (Griewank, Westekemper, et al., 2013) 2/5 (40%) (Goldenberg-Cohen et al., 2005) 10/39 (26%) (Cao et al., 2017) 39/111 (35%) (Larsen et al., 2016) 4/53 (8%) (Sheng et al., 2015) 31/101 (31%) (Lally et al., 2022) 16/47 (34%) (Gardrat et al., 2021) 13/28 (46%) (van Poppelen et al., 2021) 4/14 (29%) (Cisarova et al., 2020) 23/78 (29%) (van Ipenburg et al., 2021) 11/31 (35%) (El Zaoui et al., 2019) |
| NRAS | 9/23 (39%) (Francis et al., 2018) | NA | NA | 0/11 (0%) (Beadling et al., 2008) 14/78 (18%) (Griewank, Westekemper, et al., 2013) 25/95 (26%) (Lally et al., 2022) 5/47 (11%) (Gardrat et al., 2021) 6/28 (21%) (van Poppelen et al., 2021) 1/14 (7%) (Cisarova et al., 2020) |
| KIT | 0/5 (0%) (Alessandrini et al., 2013) | NA | 1/3 (33%) (Alessandrini et al., 2013) | 1/13 (8%) (Beadling et al., 2008) 0/42 (0%) (Griewank, Westekemper, et al., 2013) 0/8 (0%) (Alessandrini et al., 2013) 6/53 (11%) (Sheng et al., 2015) 2/47 (4%) (Gardrat et al., 2021) 2/28 (7%) (van Poppelen et al., 2021) |
| TERT | 0/56 (0%) (Koopmans et al., 2014) | 0/14 (0%) (Koopmans et al., 2014) | 2/25 (8%) (Koopmans et al., 2014) | 12/38 (32%) (Griewank, Murali, et al., 2013) 16/39 (41%) (Koopmans et al., 2014) 20/47 (43%) (van Ipenburg et al., 2021) 15/24 (54%) (van Poppelen et al., 2021) 9/14 (64%) (Cisarova et al., 2020) 34/78 (43%) (van Ipenburg et al., 2021) |
| NF1 | NA | NA | NA | 21/63 (33%) (Scholz et al., 2018) 29/74 (39%) (Lally et al., 2022) 7/14 (50%) (Cisarova et al., 2020) |
Table 2.
2022 WHO classification of conjunctival melanocytic intraepithelial lesions (C-MIL) [63].
Table 2.
2022 WHO classification of conjunctival melanocytic intraepithelial lesions (C-MIL) [63].
| WHO | Acceptable alternative terminology | Increased cellularity | Histologic features | Risk of progression to invasive melanoma |
|---|---|---|---|---|
| Not applicable | Benign melanosis C-MIN (grades (0-1) PAM without atypia |
No/minimal | Conjunctival hypermelanosis (increased pigment in epithelial cells without melanocytic hyperplasia or atypia). Slight or focal melanocytic hyperplasia without atypia (parabasal melanocytes with condensed round nuclei, smaller than basal epithelial cell, inconspicuous nucleoli, and inconspicuous cytoplasm) may be seen. | None |
| Low-grade C-MIL | PAM with mild atypia C-MIN (grades 2-4) |
Yes | Predominantly basilar melanocytic proliferation with low-grade atypia (dendritic or small to moderate size polyhedral, usually non-epithelioid melanocytes with round to irregular nuclear contours, often nuclear hyperchromasia, inconspicuous nucleoli, and inconspicuous or scant cytoplasm). | Lower |
| High-grade C-MIL | PAM with moderate to severe atypia C-MIN (grade 5-10) |
Yes | More confluent basilar and significant non-basilar proliferation of melanocytes with high-grade atypia (moderate to severe), evidence of intraepithelial nested and/or pagetoid growth, and epithelioid cell cytomorphology. | Higher |
| High-grade C-MIL | Melanoma in situ | Yes | The term melanoma in situ may be used for (1) the most atypical high-grade C-MILs involving close to full thickness of the epithelium, (2) histologically obvious melanomas without documented evidence of subepithelial invasion. | Highest |
Table 3.
Reported cases of targeted therapy in Co-M.
| Study | Patient | Co-M | Primary treatment | Agent used | Dosage | Outcome | Adverse reactions |
|---|---|---|---|---|---|---|---|
| Indicated for primary CoM | |||||||
| (Pahlitzsch, 2014) | 80y, Female | BRAF mutation | Exenteration (rejected) | Vemurafenib | Successful tumour response Tumour decreased in size |
8kg weight loss Nausea vomiting, headaches |
|
| Indicated for metastatic disease | |||||||
| (Weber et al., 2013) | 45y, Male | Metastatic Co-M (nodal, subcutaneous, pulmonary, osseous) BRAF mutation v600e |
Resection | Vemurafenib | 960mg twice daily | Improvement in pain and subjective tumour regression after 1 month | Disease progression 2 months into treatment. Enlarged paraspinal mass. |
| (Maleka et al., 2016) | 53y, Female | Metastatic Co-M (orbit, parotid gland, lung, brain) BRAF mutation v600e |
Excision Cryotherapy Mitomycin eye drops Enucleation |
Vemurafenib | 960mg twice daily | Initially good response and reduction of mets, after 4 months reappearance of mets and death, | Skin rash (dose reduced to 720mg twice daily) |
| (Rossi et al., 2019) | 70y, Male | Metastatic Co-M (parotid gland and lymph node) BRAF mutation v600e |
Excisional biopsy | Dabrafenib Trametinib |
Dabrafenib (150mg twice daily) Trametinib (2mg daily) |
Reduction of lymph node metastasis activity | Fever |
| (Pinto Torres et al., 2017) | 59y, Female | Metastatic Co-M (Oropharyngeal wall) BRAF mutation v600 |
Excision | Vemurafenib | 960mg twice daily | Full symptomatic recovery after 1 month | Arthralgia, diarrhoea, skin rash (dose was reduced to 480mg twice daily) |
Table 4.
Reported cases of immune checkpoint inhibitor therapy in Co-M.
| Study | Patient | Co-M | Primary treatment | Agent used | Dosage | Outcome | Adverse reactons |
|---|---|---|---|---|---|---|---|
| Indicated for primary CoM | |||||||
| (Finger & Pavlick, 2019) | 94y, Female | Bulbar to eyelid | None (rejected exenteration) | First – Pembrolizumab Second – Pembrolizumab and ipilimumab |
Pembrolizumab – 200mg Ipilimumab – 1mg/kg |
Progression | None reported |
| (Finger & Pavlick, 2019) | 76y, Male | Recurrence. Cornea to eyelid |
Local treatments and topical interferon-alpha chemotherapy | First – ipilimumab Second – Pembrolizumab Third – Pembrolizumab and IFN-alpha |
Pembrolizumab – 2mg/kg | Ipilimumab – no response Pembrolizumab – minimal response then complete with IFN-alpha |
Ipilimumab - Adrenal insufficiency Pembrolizumab – Dermatitis |
| (Finger & Pavlick, 2019) | 84y, Female | Recurrence. Cornea to eyelid | Excision Cryotherapy Topical mitomycin Eye plaque brachytherapy |
First – Pembrolizumab Second – Pembrolizumab and ipilimumab Third – Pembrolizumab and ipilimumab and IFN-alpha |
Pembrolizumab – 200mg Ipilimumab – 1mg/kg IFN-alpha – 3 million units per eyelid |
Pembrolizumab – minimal success Pembrolizumab and ipilimumab – progression |
None reported |
| (Hong et al., 2021) | 53y, Female | Bulbar to tarsal | None | Pembrolizumab | 200mg | Complete reduction o pigment and disease free 12 months of follow up | Cutaneous pruritus |
| Indicated for metastatic disease | |||||||
| (Pinto Torres et al., 2017) | 51y, Male | Co-M recurrence with metastasis (lymph) No BRAF mutation |
Excision Lymphadenectomy |
Pembrolizumab | 2mg/kg every 3 weeks | Complete resolution of subcutaneous lesions | None noted, patient on complete remission |
| (Sagiv et al., 2018) | 68y, Female | Co-M recurrence Metastasis – lung BRAF v600e mutation |
Resection Topical mitomycin C Exenteration, sentinel lymph node biopsy |
First – Pembrolizumab Second – Ipilimumab and dacarbazine |
Pembrolizumab 2mg/kg every 3 weeks Ipilimumab – 3mg/kg Dacarbazine – 800-1000mg/m^2 |
Pembrolizumab – stable at 6 months | Ipilimumab and dacarbazine - hepatotoxicity |
| (Sagiv et al., 2018) | 58y, Female | Co-M recurrence to orbit Metastasis – lung and liver |
Multiple resections Orbital exenteration |
nivolumab | 3mg/kg every 2 weeks | Complete resolution or orbit and metastasis lesions | Elevated liver enzymes |
| (Sagiv et al., 2018) | 28y, Female | Co-M recurrence Metastasis – breast, lung and bone |
Excision Cryotherapy Topical mitomycin C |
nivolumab | 3mg/kg every 2 weeks | Complete resolution | None reported |
| (Sagiv et al., 2018) | 47y, Female | Co-M recurrence Metastasis – lung |
Excision Cryotherapy Radiotherapy Topical interferon Mitomycin C |
nivolumab | 3mg/kg every 2 weeks | Resolution of lung metastasis and free from disease 7 months after nivolumab | Diarrhoea |
| (Sagiv et al., 2018) | 74y, Male | Co-M recurrence Metastasis – lung |
Multiple excision | nivolumab | 3mg/kg every 2 weeks | Decrease in tumour size Disease free 1 month after nivolumab |
Colitis |
| (Chaves et al., 2018) | 72y, Male | Recurrent Co-M Metastasis – Lung |
Debulking and sentinel lymph node biopsy Radioactive iodine 125 |
Ipilimumab | 3mg/kg every 3 weeks | Satisfactory response to treatment and excellent local tumour control | Mild fatigue |
| (Finger & Pavlick, 2019) | 72y, Female | Epibulbar BRAF v600k Metastasis – liver, lung, bone, skin, lymph node |
Local excision and topical chemotherapy | Ipilimumab and nivolumab | Ipilimumab – 3mg/kg Nivolumab – 1mg/kg |
Resolution of subcutaneous nodules Reduction of systemic tumour burden |
Hepatotoxicity Colitis |
| (Finger & Pavlick, 2019) | 76y, Female | NRAS mutation Metastasis – lymph, skin |
Excision Cryotherapy Topical mitomycin chemotherapy |
First – ipilimumab Second – ipilimumab Third - Pembrolizumab |
Ipilimumab – 3mg/kg Pembrolizumab – 200mg |
Ipilimumab – new skin metastases and lymph metastases | None reported |
| (Kiyohara et al., 2020) | 71y, Male | Co-M recurrence BRAF v600e Metastasis – bone and liver |
Excision Cryotherapy Vemurafenib |
Nivolumab | Died 24 months after combined therapy | None reported | |
| (Hong et al., 2021) | 66y, Male | Fornix and orbit Metastasis – lung and liver |
None | Ipilimumab and nivolumab | No dose mentioned | Resolution of lesion and good response to mets | Pituitary failure |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



