
Submitted:
22 July 2024
Posted:
22 July 2024
You are already at the latest version
Abstract
The association of alcohol intake with kidney stone disease (KSD) is not clear. We examined the National Health and Nutrition Examination Survey (NHANES) 2007-2018 and used logistic regression analyses to determine the independent association between alcohol intake and prevalent KSD. 29,684 participants were eligible for the final analysis including 2,840 prevalent stone formers (SF). Mean alcohol intake was 37.0±2.4 g/day among SF compared to 42.7±0.9 among non-SF (p=0.04). Beer [Odds ratio (OR)=0.76, 95% CI: 0.61-0.94, p=0.01] and wine (OR=0.75, 95% CI: 0.59-0.96, p=0.03) intakes were strongly associated with lower odds of prevalent KSD while liquor intake had no association. The effect from beer was dose dependent with an OR of 0.34 (95% CI: 0.20–0.57, p56g/day of beer to non-drinkers. Interestingly, the effect from wine was only significant among participants drinking moderate amount, with an OR of 0.54 (95% CI: 0.36–0.81, p=0.003) compared to non-drinkers. These effects were consistent in spline models. This study suggests that both moderate to heavy beer intake and moderate wine intake are associated with a reduced risk of KSD. Future prospective studies are needed to clarify the causal relationship.
Keywords:
Alcohol intake
; beer
; wine
; liquor
; kidney stone
Introduction
Kidney stone (KS) disease is highly prevalent and carries a significant economic burden [1]. Although adequate hydration is essential for stone prevention, types of liquid may have different modifying effects on KS risk [2,3,4].
Alcohol may increase urinary concentrations of calcium [5,6,7], phosphorus [7], and uric acid [7,8,9,10,11] thereby increasing their supersaturations. It may also increase the urinary concentration of magnesium [7,12,13,14,15], an important inhibitor of stone formation. Furthermore, it contains a fair amount of liquid and has a diuretic effect [16,17,18,19] which can reduce KS formation. The overall effect of alcohol on KS disease is unclear. In existing clinical studies, the effect of alcohol on KS disease has been inconsistent with some studies showing that it reduces the risk [20,21,22,23,24], while others showing no significant association between alcohol intake and risk of KS disease [25,26,27].
Here, we used a large US population survey database, the National Health and Nutrition Examination Survey (NHANES) from 2007 to 2018, to examine the independent association between alcohol intake and KS disease.
Methods
Study Population
NHANES is an ongoing series of cross-sectional assessments of the health and nutritional status of adults and children in the US. The survey collects demographic, socioeconomic, dietary, and health-related information, in addition to the examination and laboratory data obtained by highly trained medical personnel. A total of 59,842 participants were interviewed for NHANES from 2007 to 2018. Of these, our analysis included 29,684 participants aged 20 years or older with complete data on alcohol intake, history of KS, and the covariates of interest. (Figure 1).
Primary Exposure and Outcome
Our primary exposure was amount and type of alcohol intake using specific foods reported on the 24-hour dietary recall interviews. Individual foods and beverages with a non-zero amount of alcohol were examined and classified as beer, wine, liquor, mixed drinks, and other sources of alcohol, such as prepared alcohol containing foods. Total alcohol in grams by type was summed for each participant. Alcohol drinking status was obtained by questionnaire and categorized as never, former (no drinks in the past 12 months), and current (at least one drink in the past 12 months). Never and former drinkers who reported any alcohol on the 24-hour recall interviews were excluded. Only data from day one out of the two 24-hour recall periods was included in the present analysis.
Primary Outcome
The outcome or dependent variable of interest was prevalent KS disease. It was extracted from the interview data file. ‘Have you ever had a kidney stone?’ was the question asked during the standardized home interview. Adult participants who responded ‘yes’ to the question were considered to have a history of KS.
Covariates
Age, sex, race, history of diabetes, hypertension, thiazide use, and smoking status was obtained from the questionnaire. Body mass index (BMI) was calculated from height and weight measured during the health examination. Information on total intakes of calories, protein, and fluids (excluding alcohol) along with dietary intakes of sodium, potassium, and calcium were obtained from 24-hour dietary recall during the same day-one interview when data on the type and amount of alcohol intake was collected.
Analysis
Statistical analysis was performed with Stata MP 18 (Stata Corp, College Station TX). The complex sampling design was incorporated by applying strata, primary sampling units, and sampling weights via survey-specific procedures. Day one 24-hour recall weights were used for all analyses. Logistic regression was used to estimate unadjusted and multivariable-adjusted odds ratios (OR) and 95% confidence intervals (CI) for alcohol intake and prevalent KS disease. Alcohol intake was examined as both a categorical and a continuous predictor of KS formation. Categories were created from type of alcohol consumed and, within each type, from amounts reflecting ratios of a standard drink (14g) [28]. Alcohol intake of each type was also examined by including restricted cubic splines in the regression model [29]. Knots were specified at the 5th, 25th, 50th, 75th, and 95th percentiles of the distribution among participants drinking at least 1 gram of a specific type of alcohol. A binary indicator variable was added to the model to represent 0 to less than 1 gram of alcohol [30]. Deviations from linearity were assessed by testing coefficients for non-linear spline terms. The multivariable models included age (years), sex, race (non-Hispanic White, non-Hispanic Black, Hispanic/Latino, Non-Hispanic Other), BMI (<25, 25-<30, >30 kg/m2), diabetes (no, borderline/yes), hypertension, thiazide diuretic use, smoking (never, former, current), total dietary calories (kcal), total dietary protein (g), total fluid without alcohol contribution (g), dietary sodium (mg), potassium (mg), and calcium (mg). All p-values presented were two-tailed with p<0.05 considered statistically significant.
Results
A total of 29,684 participants were included in this analysis. 2,840 (9.7%) of these reported a history of stones. Among stone formers, 2,087 (78.1%) participants reported drinking alcohol currently, as compared to 19,985 (79.6%) participants among non-stone formers (p=0.002). Mean alcohol intake was also significantly lower with 37.0±2.4 g/day in stone formers compared to 42.7±0.91 g/day in non-stone formers (p=0.04). Stone formers tended to be older, predominantly male, Non-Hispanic White with a higher BMI compared to non-stone formers. They were also more likely to have a history of diabetes, hypertension, to use thiazides and had a history of smoking (Table 1).
Among current drinkers, 235 (43.8%) stone formers drank beer, 103 (22.5%) drank wine, and 110 (24.8%) drank liquor as compared to 2,828 (43.5%) non-stone formers who drank beer, 1,209 (23.3%) drank wine, and 1,103 (17.9%) drank liquor.
In univariate analysis of alcohol types, consumption of only beer or only wine was associated with lower odds of prevalent KS when compared to never drinkers or current drinkers who did not report alcohol by dietary recall. These associations remained after adjustment for age, sex, race, BMI, histories of hypertension, diabetes, thiazide use, cigarette smoking, dietary intakes of calorie, protein, fluid without alcohol contribution, sodium, potassium, and calcium (Table 2).
We also evaluated KS risk among current drinkers with exclusive intake of alcohol modeled as a categorical variable in tertiles or quartiles after rounding to the nearest multiple of one standard drink (14g). The multivariate-adjusted OR for stone formation among participants drinking 1-≤14g/day of beer was 1.41 (95% CI: 0.97-2.05), >14-28g/day was 0.65 (95% CI: 0.42-1.00), >28-56g/day was 0.60 (95% CI: 0.39-0.93), and >56g/day was 0.34 (95% CI: 0.20-0.57) compared to those who did not drink beer (Table 3).
Interestingly, the multivariate-adjusted OR for stone formation was 1.14 (95% CI: 0.72-1.83) among participants drinking 1-≤14g/day of wine, 0.54 (95% CI: 0.36–0.81) among those drinking >14-28g/day, and 0.85 (95% CI: 0.54–1.33) among those drinking >28g/day compared to those who did not drink wine (Table 4), showing a unique effect of moderate wine intake on KS risk.
Discussion
Alcohol has been implicated in many health problems including cardiovascular disease, liver damage, cancer and behavioral disorders. Its role in KS formation, however, remains unclear. Here, we analyzed a large cohort of US population and showed a strong protective effect from beer and wine intakes on the odds of prevalent KS. To the best of our knowledge, this is the largest population study examining specifically the role and type of alcohol intake on risk of KS formation independent of other known confounders.
KS formation occurs when stone forming elements, most commonly calcium, phosphorus, oxalate, and uric acid reach a supersaturation point followed by nucleation, aggregation, and growth. While some including citric acid and magnesium [31,32,33] inhibit KS formation, others including zinc [34,35,36,37,38] have been implicated as a promoter. Alcohol, in turn, has been shown to either directly affect the concentrations of stone forming elements or indirectly affect their promoters and inhibitors thereby potentially playing a role in KS formation. Alcohol can lead to suppressed osteoblast activity [39] and increased osteoclastic activity [40] thereby leading to bone loss and increasing urinary calcium [5,6,7] and phosphorus [7]. Together these effects seem to increase the risk of KS formation. However, alcohol also promotes urinary magnesium excretion [7,12,13,14,15,41], and increases urine output [16,17,18,19], both can be protective against stone formation. The effect of these biochemical changes in urine constituents have raised uncertainty regarding the overall effect of alcohol on KS risk.
Beer has limited alcohol content, but contains large amount of guanosine [42] which is metabolized to uric acid [43,44]. As a result, higher beer intake may lead to an increased urinary excretion of uric acid and promote KS formation [11,42,43]. While the effect of purine in beer on stone risk has not been studied exclusively, water, which accounts for 95% of content in beer [28], is known to reduce the supersaturations of stone forming elements and crystal formation [45,46]. Indeed, optimal water intake is proven to be an effective intervention for KS prevention [47,48]. We found that beer intake is strongly associated with a reduced risk of prevalent KS by as much as 24%. Our findings are consistent with what has been previously reported from other large population-based studies [3,20,24]. It should be noted that our study found a direct dose response relationship between the number of standard drinks consumed and KS risk with participants drinking moderate (>14-28g) to large (>28-56g) amount of beer every day having a progressively lowered risk of KS formation. This protective effect is likely not driven simply by the high water content in beer, as the strong association between beer and prevalent KS persisted after we adjusted for water content from beer in the sensitivity analysis (Supplemental table 1). Indeed, beer water contains a wide range of mineral and other ingredients that could influence KS risk [49].
Despite having high water content, wine has unique features that may affect KS risk. Wine consumers tend to have a higher excretion of urinary calcium [50], phosphorus [50], zinc [51], and a lower urinary excretion of magnesium [50] compared to liquor consumers and this effect remained in people consuming dealcoholized wine [50] suggesting a role of congeners in wine affecting KS risk. Even though the alcohol component has an aquaresis effect [16,17,18,19], the volume of wine consumed is usually low. Therefore, wine consumption could theoretically increase KS risk. In this study, we found a 25% reduction in KS risk among participants who drank wine. But this protection appeared to be modified by the amount of wine intake. Drinking moderate amount (14g-28g /day) of wine was associated with reduced risk of KS disease, whereas no protective effects were found among low (<14g/day) or heavy (>28g/day) drinkers suggesting a U-shaped response. Previous studies have reported a reduced risk of prevalent KS formation by 39% in men [3], and 59% in women [52] and this was confirmed by Ferraro et al [24] in a prospective study. However, Curhan et al also reported a dose related linear reduction in risk of KS in both male [3] and female [52] wine drinkers. The cause of this discrepant finding among higher wine drinkers is not clear. It might reflect the differences in study cohort and analysis methods. In addition, the studies by Curhan et al did not adjust for dietary fluid intake. Lastly, the regression analyses in this study included many other essential confounders of KS disease. Since the water content in wine can be as high as 88% [28] and there are many other unique ingredients in wine [53], it is feasible that moderate wine drinking is associated with a more favorable balance between stone promoting factors and inhibitors.
Liquor, which is a concentrated form of ethanol, leads to increased urinary calcium [5,6,7], phosphorus [7], and uric acid [54] raising possibility of harmful effect on KS formation. However, it also leads to increased urinary magnesium [7,12,13,14,15,41] and while low in volume itself when consumed, it does lead to suppression of vasopressin [55,56] which in turn results in increased urine volume suggesting a protective role in KS formation. We found that drinking any amount of liquor has no association with risk of prevalent KS disease, reflecting a well-balanced effects from KS promoters and inhibitors. Our finding is consistent with what has been reported by Goldfarb et al in a study of Vietnam Era Twin Registry [20,25]. However, Wang et al [21] in their large population study, found that drinking any amount of liquor had a reduced risk of prevalent KS. This discrepancy could be due to the differences in study cohort.
Our study has limitations. First, this is a cross-sectional study and conclusions regarding causal or temporal relationship cannot be made. Second, it is possible that stone formers who are aware about their disease increase their alcohol intake to increase fluid volume. However, such practice is generally not recommended due to the lack of solid clinical evidence and concerns of overall negative impact to health especially considering a high prevalence of hypertension among KS formers. Third, KS diagnosis was self-reported during interviews. Therefore, misclassification is possible as stone formers may have a recall bias and some may not be aware that they had a stone. Furthermore, alcohol consumers may underestimate and underreport the amount of alcohol consumed. Regardless, this should be biased toward null. Finally, we also could not evaluate the effect of alcohol intake on urinary risk profile or the type of stone since these data were not available in the NHANES.
Conclusions
Our study demonstrated that moderate to high beer and moderate wine intake is associated with a reduced prevalence of KS disease. Future prospective studies are needed to clarify the causal relationship and underlying mechanisms.
Author Contributions
Conceptualization, J.T., M.C.; Methodology, J.T., C.R.; Software, C.R.; Validation, J.T., C.R.; Data curation, C.R.; Analysis, C.R.; Writing -original draft preparation, S.S., C.R., J.T.; Writing-review and editing, J.T., M.C., C.R., S.S. CR and SS contributed equally to this study All authors have read and agreed and to the published version of the manuscript.
Funding
Brown Physicians Inc Foundation Category 3 Educational Funding on Kidney Stone Disease (PI: J Tang).
Informed Consent Statement
Patient consent was waived due to this being a database-based study.
Conflicts of Interest
Authors declare that they have no competing interests.
References
- Saigal CS, Joyce G, Timilsina AR. Direct and indirect costs of nephrolithiasis in an employed population: opportunity for disease management? Kidney Int 2005;68:1808-14.
- Borghi L, Meschi T, Amato F, Briganti A, Novarini A, Giannini A. Urinary volume, water and recurrences in idiopathic calcium nephrolithiasis: a 5-year randomized prospective study. J Urol 1996;155:839-43.
- Curhan GC, Willett WC, Rimm EB, Spiegelman D, Stampfer MJ. Prospective study of beverage use and the risk of kidney stones. Am J Epidemiol 1996;143:240-7.
- Xu C, Zhang C, Wang XL, et al. Self-Fluid Management in Prevention of Kidney Stones: A PRISMA-Compliant Systematic Review and Dose-Response Meta-Analysis of Observational Studies. Medicine (Baltimore) 2015;94:e1042.
- García-Sanchez A, Gonzalez-Calvin JL, Diez-Ruiz A, Casals JL, Gallego-Rojo F, Salvatierra D. Effect of acute alcohol ingestion on mineral metabolism and osteoblastic function. Alcohol Alcohol 1995;30:449-53.
- Perry HM, 3rd, Horowitz M, Fleming S, et al. The effects of season and alcohol intake on mineral metabolism in men. Alcohol Clin Exp Res 1999;23:214-9.
- De Marchi S, Cecchin E, Basile A, Bertotti A, Nardini R, Bartoli E. Renal tubular dysfunction in chronic alcohol abuse--effects of abstinence. N Engl J Med 1993;329:1927-34.
- Lieber CS, Jones DP, Losowsky MS, Davidson CS. Interrelation of uric acid and ethanol metabolism in man. J Clin Invest 1962;41:1863-70.
- Maclachlan MJ, Rodnan GP. Effect of food, fast and alcohol on serum uric acid and acute attacks of gout. Am J Med 1967;42:38-57.
- Faller J, Fox IH. Ethanol-induced hyperuricemia: evidence for increased urate production by activation of adenine nucleotide turnover. N Engl J Med 1982;307:1598-602.
- Gibson T, Rodgers AV, Simmonds HA, Toseland P. Beer drinking and its effect on uric acid. Br J Rheumatol 1984;23:203-9.
- McCollister RJ, Flink EB, Lewis MD. Urinary Excretion of Magnesium in Man Following the Ingestion of Ethanol. The American Journal of Clinical Nutrition 1963;12:415-20.
- Rylander R, Mégevand Y, Lasserre B, Amstutz W, Granbom S. Moderate alcohol consumption and urinary excretion of magnesium and calcium. Scand J Clin Lab Invest 2001;61:401-5.
- Barker ES, Elkinton JR, Clark JK. Studies of the renal excretion of magnesium in man. J Clin Invest 1959;38:1733-45.
- Kalbfleisch JM, Lindeman RD, Ginn HE, Smith WO. EFFECTS OF ETHANOL ADMINISTRATION ON URINARY EXCRETION OF MAGNESIUM AND OTHER ELECTROLYTES IN ALCOHOLIC AND NORMAL SUBJECTS. J Clin Invest 1963;42:1471-5.
- Eggleton, MG. The diuretic action of alcohol in man. J Physiol 1942;101:172-91.
- Strauss MB, Rosenbaum JD, Nelson WP, 3rd. The effect of alcohol on the renal excretion of water and electrolyte. J Clin Invest 1950;29:1053-8.
- Rubini ME, Kleeman CR, Lamdin E. Studies on alcohol diuresis. I. The effect of ethyl alcohol ingestion on water, electrolyte and acid-base metabolism. J Clin Invest 1955;34:439-47.
- Jones, AW. Excretion of alcohol in urine and diuresis in healthy men in relation to their age, the dose administered and the time after drinking. Forensic Sci Int 1990;45:217-24.
- Hirvonen T, Pietinen P, Virtanen M, Albanes D, Virtamo J. Nutrient intake and use of beverages and the risk of kidney stones among male smokers. Am J Epidemiol 1999;150:187-94.
- Wang H, Fan J, Yu C, et al. Consumption of Tea, Alcohol, and Fruits and Risk of Kidney Stones: A Prospective Cohort Study in 0.5 Million Chinese Adults. Nutrients 2021;13:1119.
- Krieger JN, Kronmal RA, Coxon V, Wortley P, Thompson L, Sherrard DJ. Dietary and behavioral risk factors for urolithiasis: potential implications for prevention. Am J Kidney Dis 1996;28:195-201.
- Shuster J, Finlayson B, Scheaffer RL, Sierakowski R, Zoltek J, Dzegede S. Primary liquid intake and urinary stone disease. J Chronic Dis 1985;38:907-14.
- Ferraro PM, Taylor EN, Gambaro G, Curhan GC. Soda and other beverages and the risk of kidney stones. Clin J Am Soc Nephrol 2013;8:1389-95.
- Goldfarb DS, Fischer ME, Keich Y, Goldberg J. A twin study of genetic and dietary influences on nephrolithiasis: a report from the Vietnam Era Twin (VET) Registry. Kidney Int 2005;67:1053-61.
- Liu CC, Huang SP, Wu WJ, et al. The impact of cigarette smoking, alcohol drinking and betel quid chewing on the risk of calcium urolithiasis. Ann Epidemiol 2009;19:539-45.
- Zhou Z, Huang Z, Ai G, Guo X, Zeng G, Zhu W. Association between alcohol consumption and kidney stones in American adults: 2007-2016 NHANES. Front Public Health 2023;11:1156097.
- CDC Alcohol Use-About Standard Drink Sizes. 2024. (Accessed 6/27/24, 2024, at https://www.cdc.gov/alcohol/standard-drink-sizes/index.html.
- Orsini N, Greenland S. A procedure to tabulate and plot results after flexible modeling of a quantitative covariate. Stata Journal 2011;11:1-29.
- Royston P, Sauerbrei W, Becher H. Modelling continuous exposures with a 'spike' at zero: a new procedure based on fractional polynomials. Stat Med 2010;29:1219-27.
- Grases F, Rodriguez A, Costa-Bauza A. Efficacy of Mixtures of Magnesium, Citrate and Phytate as Calcium Oxalate Crystallization Inhibitors in Urine. J Urol 2015;194:812-9.
- Lieske JC, Farell G, Deganello S. The effect of ions at the surface of calcium oxalate monohydrate crystals on cell-crystal interactions. Urol Res 2004;32:117-23.
- Shringi S, Raker CA, Tang J. Dietary Magnesium Intake and Kidney Stone: The National Health and Nutrition Examination Survey 2011-2018. R I Med J (2013) 2023;106:20-5.
- Bird ED, Thomas WC. Effect of Various Metals on Mineralization in vitro. Proceedings of the Society for Experimental Biology and Medicine 1963;112:640-3.
- Sutor, DJ. Growth studies of calcium oxalate in the presence of various ions and compounds. Br J Urol 1969;41:171-8.
- François B, Cahen R, Pascal B. Inhibitors of urinary stone formation in 40 recurrent stone formers. Br J Urol 1986;58:479-83.
- Atakan IH, Kaplan M, Seren G, Aktoz T, Gül H, Inci O. Serum, urinary and stone zinc, iron, magnesium and copper levels in idiopathic calcium oxalate stone patients. Int Urol Nephrol 2007;39:351-6.
- Tang J, McFann K, Chonchol M. Dietary Zinc Intake and Kidney Stone Formation: Evaluation of NHANES III. American Journal of Nephrology 2012;36:549-53.
- Chavassieux P, Serre CM, Vergnaud P, Delmas PD, Meunier PJ. In vitro evaluation of dose-effects of ethanol on human osteoblastic cells. Bone Miner 1993;22:95-103.
- Dai J, Lin D, Zhang J, et al. Chronic alcohol ingestion induces osteoclastogenesis and bone loss through IL-6 in mice. J Clin Invest 2000;106:887-95.
- Laitinen K, Tähtelä R, Välimäki M. The dose-dependency of alcohol-induced hypoparathyroidism, hypercalciuria, and hypermagnesuria. Bone Miner 1992;19:75-83.
- Ka T, Yamamoto T, Moriwaki Y, et al. Effect of exercise and beer on the plasma concentration and urinary excretion of purine bases. J Rheumatol 2003;30:1036-42.
- Moriwaki Y, Ka T, Takahashi S, Tsutsumi Z, Yamamoto T. Effect of Beer Ingestion on the Plasma Concentrations and Urinary Excretion of Purine Bases: One-Month Study. Nucleosides, Nucleotides & Nucleic Acids 2006;25:1083-5.
- Ka T, Moriwaki Y, Inokuchi T, et al. Effects of allopurinol on beer-induced increases in plasma concentrations and urinary excretion of purine bases (uric acid, hypoxanthine, and xanthine). Horm Metab Res 2006;38:188-92.
- Li Y, Pan J, Zhang Y, et al. Effects of small molecules water that may retard kidney stone formation. Int Urol Nephrol 2018;50:225-30.
- Ferraro PM, Baccaro R, Baroni S, et al. Effect of water composition and timing of ingestion on urinary lithogenic profile in healthy volunteers: a randomized crossover trial. J Nephrol 2021;34:875-81.
- Wang JS, Chiang HY, Chen HL, Flores M, Navas-Acien A, Kuo CC. Association of water intake and hydration status with risk of kidney stone formation based on NHANES 2009-2012 cycles. Public Health Nutr 2022;25:2403-14.
- Bao Y, Tu X, Wei Q. Water for preventing urinary stones. Cochrane Database of Systematic Reviews 2020.
- Díaz AB, Durán-Guerrero E, Lasanta C, Castro R. From the Raw Materials to the Bottled Product: Influence of the Entire Production Process on the Organoleptic Profile of Industrial Beers. Foods 2022;11.
- McDonald JT, Margen S. Wine versus ethanol in human nutrition. III. Calcium, phosphorous, and magnesium balance. Am J Clin Nutr 1979;32:823-33.
- McDonald JT, Margen S. Wine versus ethanol in human nutrition. IV. Zinc balance. Am J Clin Nutr 1980;33:1096-102.
- Curhan GC, Willett WC, Speizer FE, Stampfer MJ. Beverage use and risk for kidney stones in women. Ann Intern Med 1998;128:534-40.
- Serio F, Imbriani G, Acito M, et al. Moderate red wine intake and cardiovascular health protection: a literature review. Food Funct 2023;14:6346-62.
- Fukui S, Okada M, Rahman M, et al. Differences in the Association Between Alcoholic Beverage Type and Serum Urate Levels Using Standardized Ethanol Content. JAMA Netw Open 2023;6:e233398.
- Taivainen H, Laitinen K, Tähtelä R, Kilanmaa K, Välimäki MJ. Role of plasma vasopressin in changes of water balance accompanying acute alcohol intoxication. Alcohol Clin Exp Res 1995;19:759-62.
- Helderman JH, Vestal RE, Rowe JW, Tobin JD, Andres R, Robertson GL. The response of arginine vasopressin to intravenous ethanol and hypertonic saline in man: the impact of aging. J Gerontol 1978;33:39-47.
Figure 1.
Selection of study population.
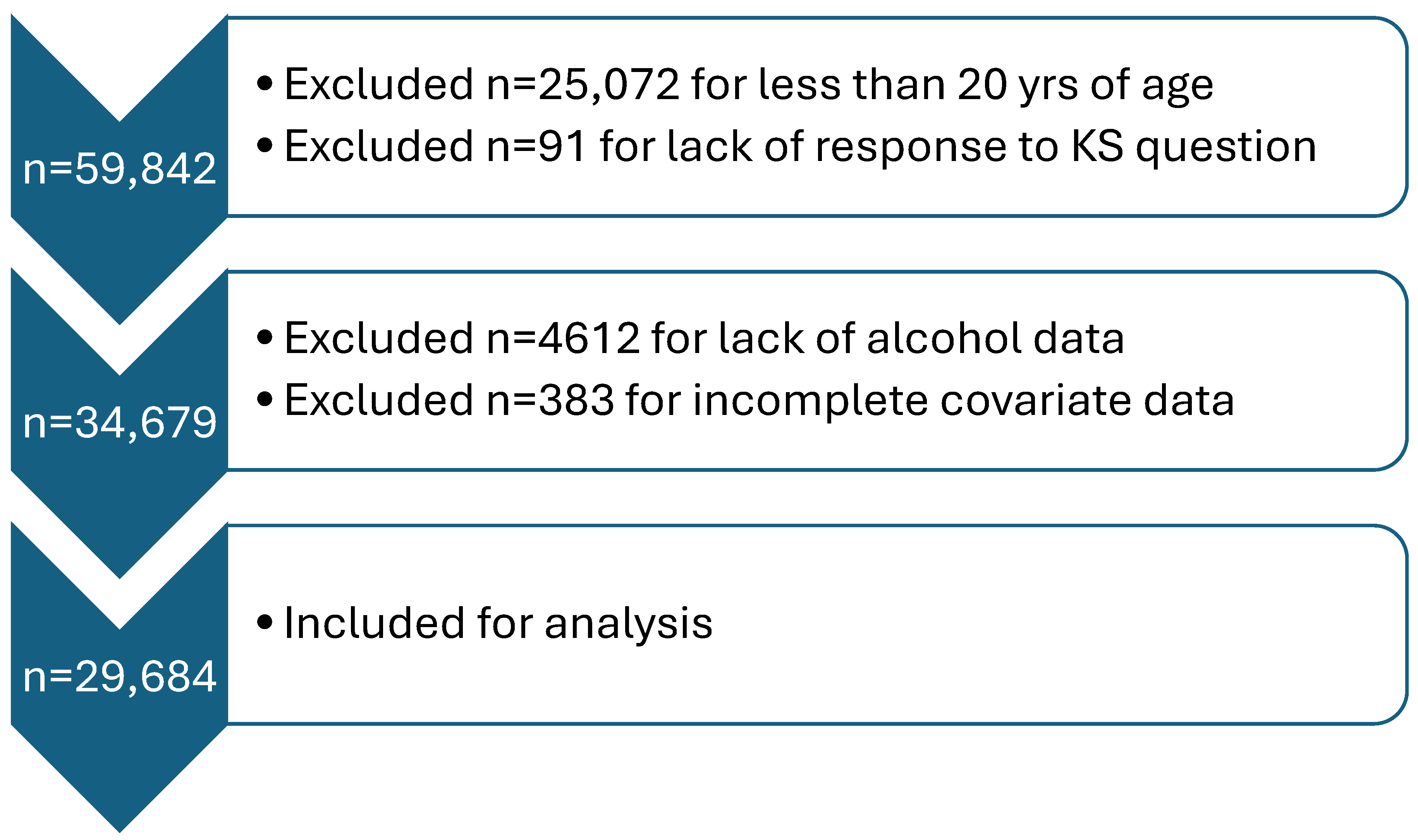
Figure 2.
Odds ratios of prevalent kidney stone by restricted cubic splines for exclusive beer intake among current drinkers. Knots at 9.4, 14.9, 28.1, 47.95, and 126.4 g of beer with a binary indicator variable for 0-<1g. P=0.02 for test of linearity. The x-axis was truncated at 224 g, omitting 27 respondents with intake >224-832 g.
Figure 2.
Odds ratios of prevalent kidney stone by restricted cubic splines for exclusive beer intake among current drinkers. Knots at 9.4, 14.9, 28.1, 47.95, and 126.4 g of beer with a binary indicator variable for 0-<1g. P=0.02 for test of linearity. The x-axis was truncated at 224 g, omitting 27 respondents with intake >224-832 g.
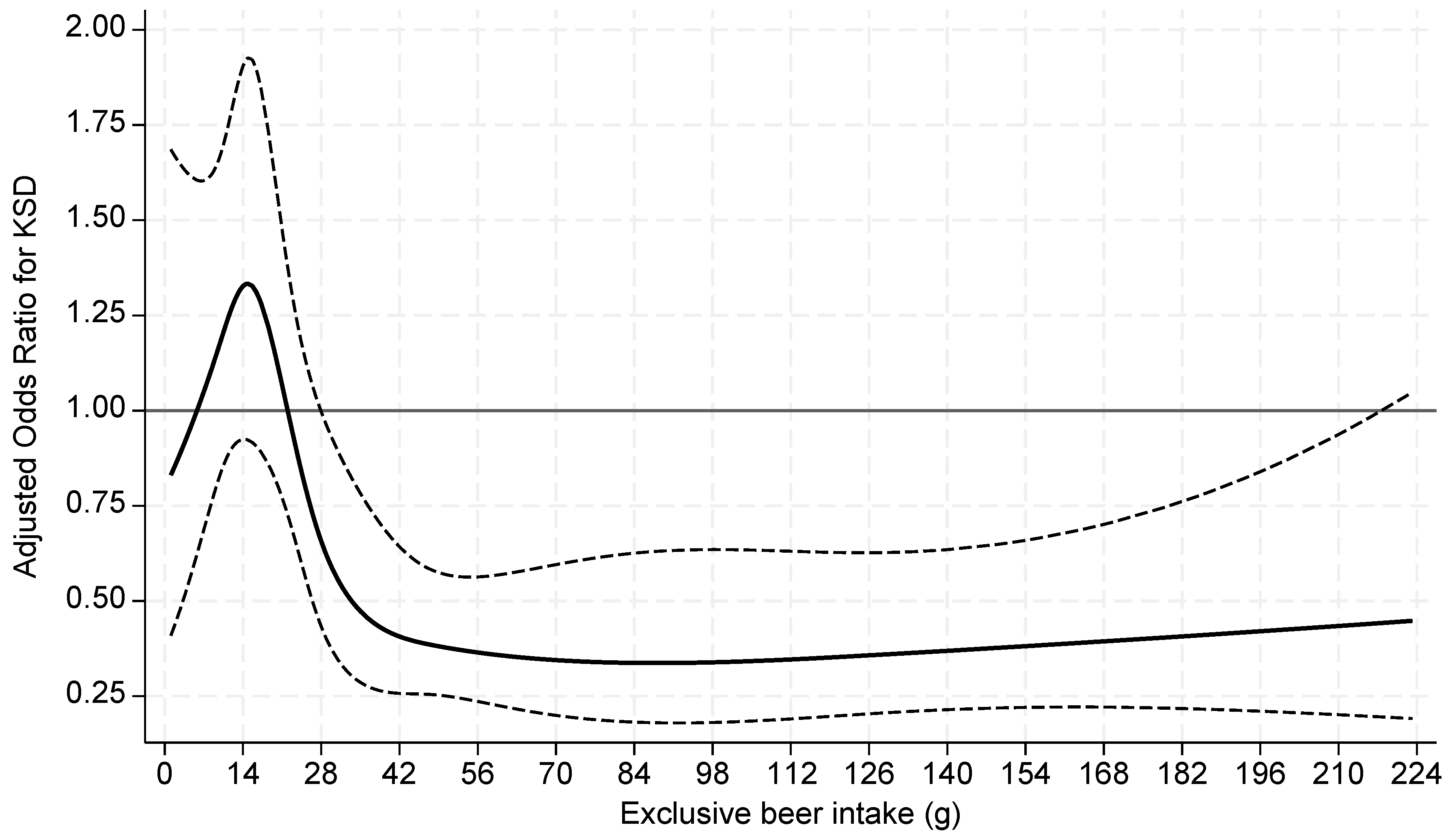
Figure 3.
Odds ratios of prevalent kidney stone by restricted cubic splines for exclusive wine intake among current drinkers. Knots at 7.2, 15.1, 21.6, 31.2, and 63.6 g of wine with a binary indicator variable for 0-<1g. P=0.04 for test of linearity. The x-axis was truncated at 98 g, omitting 14 respondents with intake >98-167 g.
Figure 3.
Odds ratios of prevalent kidney stone by restricted cubic splines for exclusive wine intake among current drinkers. Knots at 7.2, 15.1, 21.6, 31.2, and 63.6 g of wine with a binary indicator variable for 0-<1g. P=0.04 for test of linearity. The x-axis was truncated at 98 g, omitting 14 respondents with intake >98-167 g.
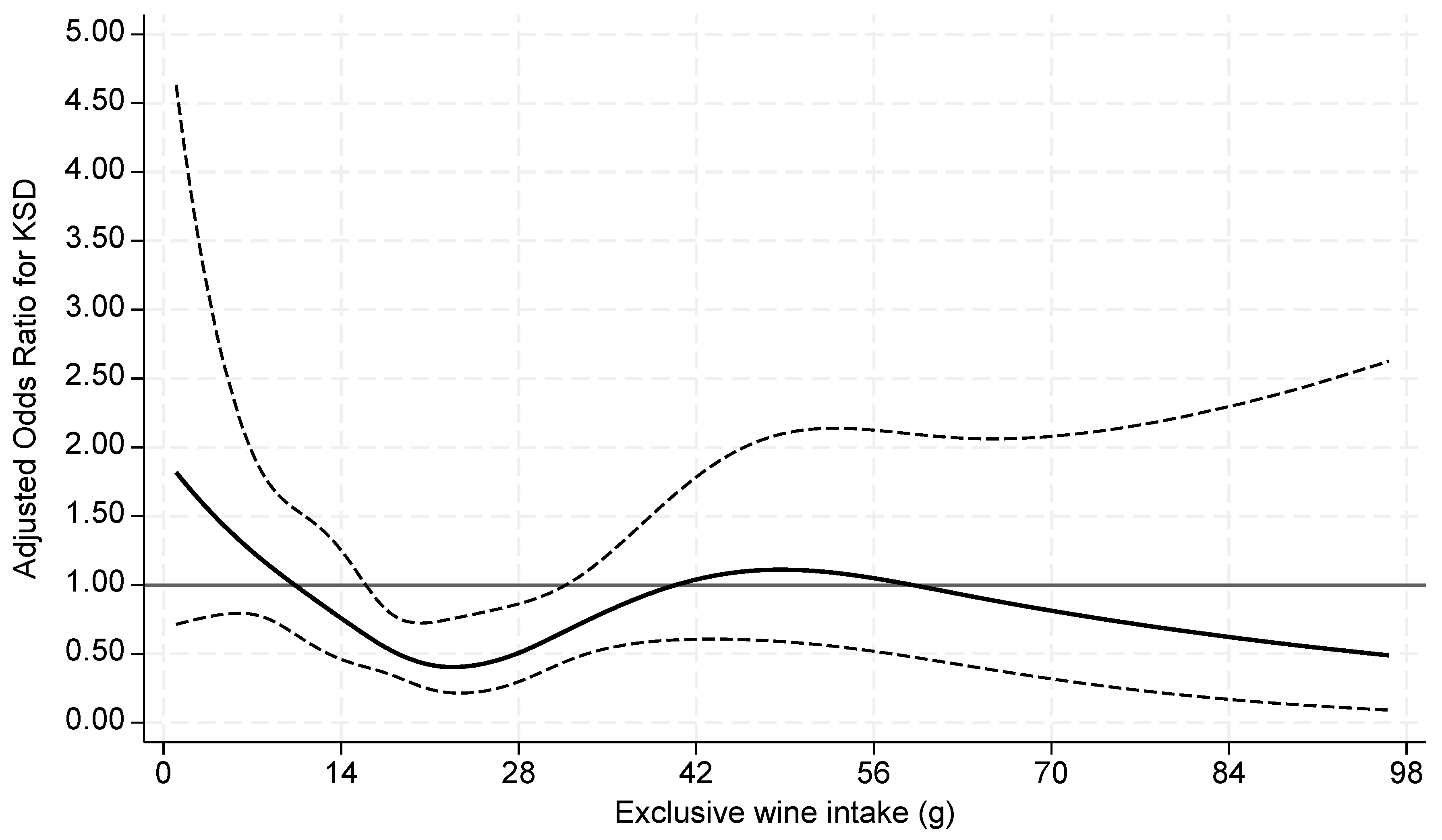
Figure 4.
Odds ratios of prevalent kidney stone for continuous liquor intake among current drinkers. P = 0.29 for test of linearity. The x-axis was truncated at 196 g, omitting 17 respondents with intake >196-404 g.
Figure 4.
Odds ratios of prevalent kidney stone for continuous liquor intake among current drinkers. P = 0.29 for test of linearity. The x-axis was truncated at 196 g, omitting 17 respondents with intake >196-404 g.
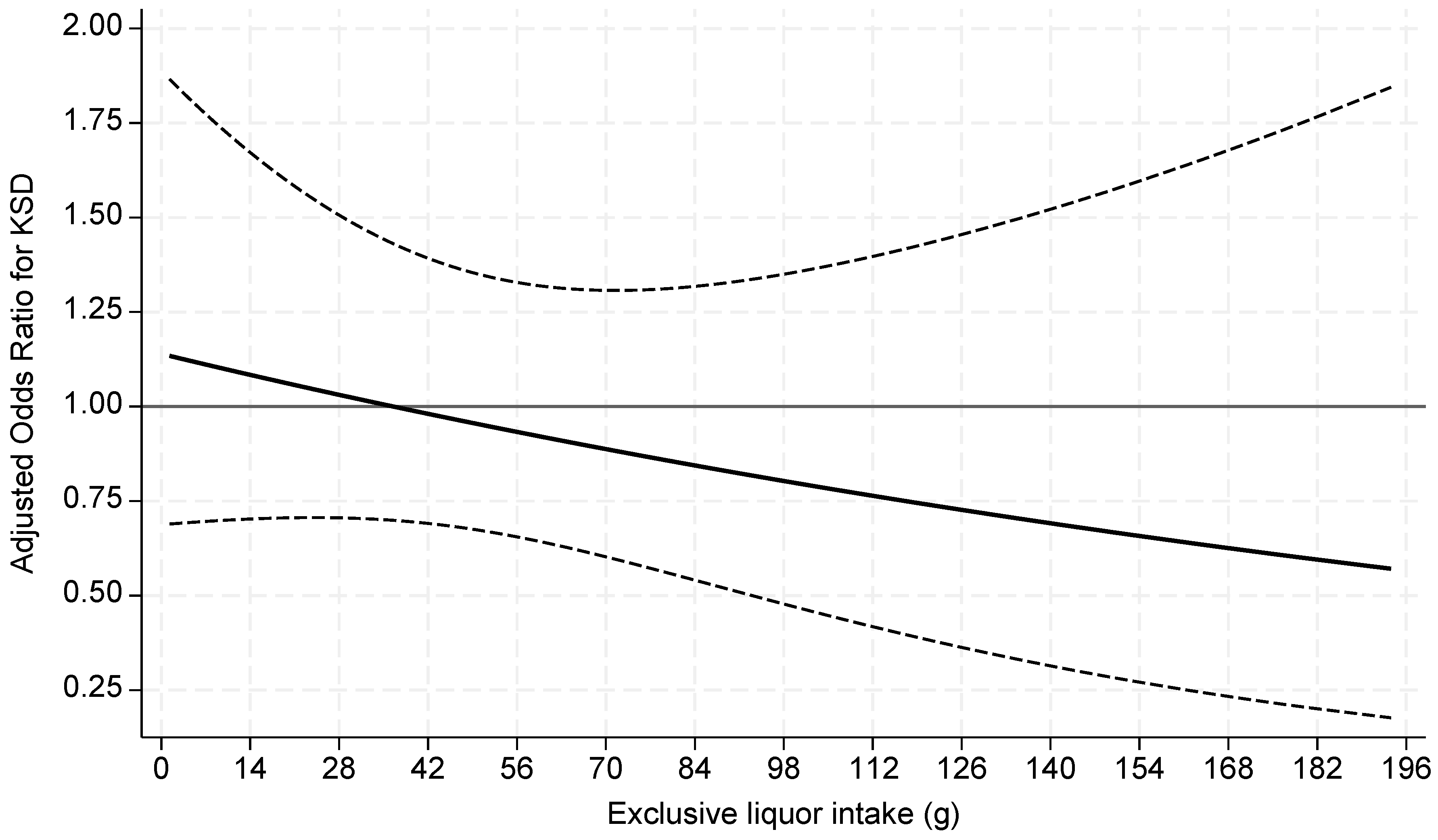

Table 1.
Baseline characteristics of study population.
| KS Former | Non-KS Former | p value | |
|---|---|---|---|
| Total n, unweighted | 9.7 (2,840) | 90.3 (26,844) | |
| Male sex | 54.6 (1,571) | 47.4 (12,865) | <0.001 |
| Age (y) | 53.7 ± 0.38 | 46.8 ± 0.26 | <0.001 |
| Race | <0.001 | ||
| Non-Hispanic White | 76.2 (1,553) | 65.3 (10,851) | |
| Non-Hispanic Black | 5.9 (376) | 11.8 (5,995) | |
| Hispanic/Latino | 11.7 (690) | 14.7 (6,844) | |
| Non-Hispanic other | 6.1 (221) | 8.2 (3,154) | |
| BMI (kg/m2) | <0.001 | ||
| <25.0 | 19.8 (542) | 30.2 (7,803) | |
| 25.0-<30.0 | 32.9 (962) | 32.8 (8,784) | |
| 30.0+ | 47.2 (1,336) | 37.0 (10,257) | |
| History of diabetes | 22.4 (736) | 10.8 (3,895) | <0.001 |
| History of hypertension | 48.7 (1,487) | 32.3 (9,841) | <0.001 |
| Thiazide diuretic use | 12.6 (377) | 7.8 (2,498) | <0.001 |
| Smoking status | <0.001 | ||
| Never | 49.8 (1,392) | 56.2 (15,104) | |
| Former | 30.6 (884) | 24.0 (6,267) | |
| Current | 19.6 (564) | 19.8 (5,473) | |
| Total calories (kcal) | 2,122.9 ± 28.7 | 2,142.9 ± 8.9 | 0.5 |
| Protein intake (g) | 80.8 ± 1.4 | 82.8 ± 0.42 | 0.16 |
| Dietary sodium (mg) | 3,534.0 ± 54.6 | 3,539 ± 15.9 | 0.93 |
| Dietary potassium (mg) | 2,644.0 ± 38.3 | 2,690.2 ± 15.5 | 0.22 |
| Dietary calcium (mg) | 934.3 ± 15.3 | 973.7 ± 6.6 | 0.02 |
| Total fluid intake, excluding alcohol (g) | 2,905.0 ± 35.4 | 2,885.9 ± 20.0 | 0.58 |
| Alcohol drinking status | 0.002 | ||
| Never | 12.3 (442) | 13.6 (4,638) | |
| Former (0 drinks in past year) | 9.7 (311) | 6.9 (2,221) | |
| Current (>0 drinks in past year) | 78.1 (2,087) | 79.6 (19,985) | |
| Type of alcohol, if any | 0.01 | ||
| Beer only | 43.8 (235) | 43.5 (2,828) | |
| Wine only | 22.5 (103) | 23.3 (1,209) | |
| Liquor only | 24.8 (110) | 17.9 (1,103) | |
| Other/combination | 8.9 (69) | 15.3 (946) |
Values are expressed as weighted means ± SE or % (unweighted n). Abbreviations: BMI = body mass index, KS = kidney stone.
Table 2.
Odds ratios of prevalent kidney stone according to type of alcohol.
| Unadjusted Model | Adjusted Model 1 | Adjusted Model 2 | Adjusted Model 3 | |||||
|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | p value | OR (95% CI) | p value | OR (95% CI) | p value | OR (95% CI) | p value | |
| Never/Currently none | REF | REF | REF | REF | ||||
| Beer only | 0.79 (0.64-0.97) | 0.02 | 0.76 (0.62-0.94) | 0.01 | 0.79 (0.64-0.97) | 0.03 | 0.76 (0.61-0.94) | 0.01 |
| Wine only | 0.75 (0.58-0.99) | 0.04 | 0.64 (0.49-0.84) | 0.001 | 0.74 (0.57-0.96) | 0.02 | 0.75 (0.59-0.96) | 0.03 |
| Liquor only | 1.08 (0.77-1.52) | 0.63 | 1.04 (0.74-1.47) | 0.82 | 1.05 (0.75-1.49) | 0.76 | 0.99 (0.69-1.42) | 0.97 |
Abbreviations: OR = odds ratio, CI = confidence interval. REF= never drinkers and current drinkers who did not report alcohol intake on day 1 recall. Model 1: adjusted for demographics. Model 2: adjusted for BMI, histories of hypertension, diabetes, thiazide use, cigarette smoking, in addition to model 1. Model 3: adjusted for dietary intakes of calorie, protein, fluid (minus alcohol contribution), sodium, potassium, and calcium in addition to model 2.
Table 3.
Odds ratios of prevalent kidney stone according to exclusive beer intake among current drinkers.
Table 3.
Odds ratios of prevalent kidney stone according to exclusive beer intake among current drinkers.
| Unadjusted Model | Adjusted Model 1 | Adjusted Model 2 | Adjusted Model 3 | |||||
|---|---|---|---|---|---|---|---|---|
| Beer | OR (95% CI) | p value | OR (95% CI) | p value | OR (95% CI) | p value | OR (95% CI) | p value |
| 0-<1g | REF | REF | REF | REF | ||||
| 1-≤ 14g | 1.46 (1.00-2.15) | 0.05 | 1.35 (0.93-1.96) | 0.11 | 1.45 (1.00-2.12) | 0.05 | 1.41 (0.97-2.05) | 0.07 |
| >14-28g | 0.67 (0.44-1.01) | 0.06 | 0.65 (0.43-0.99) | 0.04 | 0.66 (0.43-1.02) | 0.06 | 0.65 (0.42-1.00) | 0.05 |
| >28-56g | 0.60 (0.40-0.91) | 0.02 | 0.61 (0.40-0.92) | 0.02 | 0.64 (0.41-0.98) | 0.04 | 0.60 (0.39-0.93) | 0.02 |
| >56g | 0.39 (0.24-0.63) | <0.001 | 0.38 (0.24-0.62) | <0.001 | 0.38 (0.24-0.62) | <0.001 | 0.34 (0.20-0.57) | <0.001 |
Abbreviations: OR = odds ratio, CI = confidence interval. REF = No alcohol intake on day 1 recall or less than 1g of beer only. Model 1: adjusted for demographics. Model 2: adjusted for BMI, histories of hypertension, diabetes, thiazide use, cigarette smoking, in addition to model 1. Model 3: adjusted for dietary intakes of calorie, protein, fluid (minus alcohol contribution), sodium, potassium, and calcium in addition to model 2. 18,532 records included.
Table 4.
Odds ratios of prevalent kidney stone according to exclusive wine intake among current drinkers.
Table 4.
Odds ratios of prevalent kidney stone according to exclusive wine intake among current drinkers.
| Unadjusted Model | Adjusted Model 1 | Adjusted Model 2 | Adjusted Model 3 | |||||
|---|---|---|---|---|---|---|---|---|
| Wine | OR (95% CI) | p value | OR (95% CI) | p value | OR (95% CI) | p value | OR (95% CI) | p value |
| 0-<1g | REF | REF | REF | REF | ||||
| 1-≤ 14g | 0.98 (0.62-1.53) | 0.91 | 0.90 (0.56-1.44) | 0.66 | 1.10 (0.69-1.77) | 0.68 | 1.14 (0.72-1.83) | 0.57 |
| >14-28g | 0.52 (0.35-0.77) | 0.001 | 0.43 (0.29-0.64) | <0.001 | 0.53 (0.36-0.78) | 0.002 | 0.54 (0.36-0.81) | 0.003 |
| >28g | 0.86 (0.52-1.44) | 0.56 | 0.77 (0.47-1.27) | 0.31 | 0.87 (0.54-1.4) | 0.56 | 0.85 (0.54-1.33) | 0.47 |
Abbreviations: OR = odds ratio, CI = confidence interval. REF = No alcohol intake on day 1 recall or less than 1g of wine only. Model 1: adjusted for demographics. Model 2: adjusted for BMI, histories of hypertension, diabetes, thiazide use, cigarette smoking, in addition to model 1. Model 3: adjusted for dietary intakes of calories, protein, fluid (minus alcohol contribution), sodium, potassium, and calcium in addition to model 2. 16,781 records included.
Table 5.
Odds ratios of prevalent kidney stone according to exclusive liquor intake among current drinkers.
Table 5.
Odds ratios of prevalent kidney stone according to exclusive liquor intake among current drinkers.
| Unadjusted Model | Adjusted Model 1 | Adjusted Model 2 | Adjusted Model 3 | |||||
|---|---|---|---|---|---|---|---|---|
| Liquor | OR (95% CI) | p value | OR (95% CI) | p value | OR (95% CI) | p value | OR (95% CI) | p value |
| 0-<1g | REF | REF | REF | REF | ||||
| 1-≤ 28g | 1.18 (0.70-1.99) | 0.53 | 1.15 (0.67-1.96) | 0.62 | 1.20 (0.71-2.02) | 0.49 | 1.16 (0.69-1.97) | 0.58 |
| >28g | 0.97 (0.65-1.44) | 0.87 | 0.94 (0.62-1.40) | 0.75 | 0.94 (0.62-1.43) | 0.79 | 0.85 (0.56-1.30) | 0.45 |
Abbreviations: OR = odds ratio, CI = confidence interval. REF = No alcohol intake on day 1 recall or less than 1g of liquor only. Model 1: adjusted for demographics. Model 2: adjusted for BMI, histories of hypertension, diabetes, thiazide use, cigarette smoking, in addition to model 1. Model 3: adjusted for dietary intakes of calorie, protein, fluid (minus alcohol contribution), sodium, potassium, and calcium in addition to model 2. 16,682 records included.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



