
Submitted:
22 July 2024
Posted:
23 July 2024
You are already at the latest version
Abstract
Background: Young people with intellectual developmental disabilities have a persistent delay in the development of executive functions. Virtual reality (VR) is increasingly being used as a cognitive intervention tool, with significant effectiveness demonstrated in different types of populations. Methods: This pilot study aims to investigate the impact of a cognitive training program utilizing VR on young adults diagnosed with intellectual developmental disability (IDD). The participants (N=15) served as their own control group and were assessed three times: weeks 0, 8 and 16, with a rest period (0-8 weeks) and an intervention period (8-16 weeks). The assessments included measures of cognitive function, provided by E-Prime®. Results: Overall, an improvement in working memory and inhibitory control was found after the intervention, but not in sustained attention. Conclusions: These findings suggest that VR-based cognitive training holds promise as an effective intervention for enhancing cognitive abilities in young adults with intellectual developmental disability.
Keywords:
intellectual developmental disability
; virtual reality
; cognitive training
; serious games
; executive functions
1. Introduction
Intellectual developmental disability (IDD) is a neurodevelopmental disorder, characterized by the presence of intellectual, functional and adaptative deficits in conceptual, social, and practical domains [1]. IDD manifests itself during the developmental period and, generally, persists throughout life, with different levels of cognitive impairment severity [1,2], being often associated with other developmental disorders such as cerebral palsy, autism spectrum disorder, Down syndrome, or fragile X syndrome [3].
Difficulties in functioning can be explained by problems in concentration, processing information, memory, or self-regulation, thus, compromising their autonomy and independence in daily life [1,4,5,6,7]. Prior research suggests that individuals with intellectual developmental disability have a persistent delay in the development and a slower rate of acquisition of the executive functions [8,9]. These are higher-order cognitive mechanisms, which include working memory, processing speed, attentional control, planning, inhibitory control, solving problems that require decision-making processes for the selection of a functional response, and cognitive flexibility as a response to environmental contingencies [10,11,12,13,14,15,16,17]. It has been reported related deficits in working memory, inhibitory control and verbal fluency [18], cognitive planning [11], processing speed [9], and attention and cognitive flexibility [9,11,18,19] in individuals with intellectual developmental disability. These deficits contribute to difficulties in solving intellectual challenges crucial for daily autonomy [20]. Cognitive training seems to be crucial for addressing these issues, as it aims to improve executive functions [21,22,23]. Traditional cognitive training involves several activities [24,25], but lacks real-time feedback [23]. New technologies, such as computerized cognitive training, offer innovative interventions that are adaptable to individual performance and can provide feedback immediately after completing the activity. However, the screen-based nature of computerized cognitive training may limit ecological validity and transferability to daily life [26].
Virtual reality (VR) has gained popularity in neuroscience and as an intervention approach, proving to be effective for various deficits, especially in cognitive areas [15,21,26,27,28,29,30,31,32]. Immersive VR systems, utilizing head-mounted displays, provide interactive, embodied experiences with advantages such as non-invasiveness and real-time, controlled multisensory scenarios [26,33,34]. Immersive VR fosters a safe environment, promoting patient acceptance and calm skill practice [33,35,36]. It offers insights into brain activity, efficient performance feedback [26], and motivation through interactivity [37]. Also, immersive VR allows for the intervention to be more easily programmed, objective and progressively graded [36,38] particularly in executive functions, serving as both an intervention and assessment tool in ecologically relevant conditions [17,29,30,37]. Combining VR with serious games showed positive results in learning and skill improvement, as serious games enable goal-oriented operations within an entertaining environment [39,40].
As effective cognitive interventions for IDD should prioritize motivation, task-complexity, grading and acquisition assessment, it seems promising that greater sensory immersion might enhance cognitive processing, suggesting that virtual environments may stimulate executive functions in IDD [12]. Consistently, previous literature suggests the potential of serious games with VR as a rehabilitation tool for individuals with intellectual developmental disability [29,35]. Nonetheless, existing VR cognitive training studies predominantly focus on patients with traumatic brain injury, stroke, mild cognitive impairment, and dementia, with limited attention to individuals with ID [23,38,41]. Also, while VR interventions for physical and daily life skills are explored [36], research on executive function development in individuals with intellectual developmental disability is scarce [5,42].. Therefore, this study aims to investigate the effects of cognitive training using Immersive VR on executive functions, specifically working memory, sustained attention, and inhibitory control, in young adults with intellectual developmental disability.
2. Materials and Methods
This study employed a quasi-experimental design with a one-group temporal series structure (Figure 1). The study follow the TREND Statement Checklist for the reporting quality of nonrandomized evaluations of behavioral and public health interventions [43]. Participants served as their own control group, undergoing assessments before (two times, with an eight weeks period without any intervention in between), and after the intervention [44,45].
2.1. Participants
A convenience sampling method was used and 15 individuals attending services at the Centro de Atividades e Capacitação para a Inclusão – APACI, were selected for the study. This institution, located in Barcelos, functions as a center for activities and training for community inclusion.
Inclusion criteria were (a) young adults diagnosed with mild or moderate intellectual developmental disability, (b) aged between 18 and 35 years (c) ability to understand instructions given in Portuguese, (d) previous experience using mouse and gamepads for gaming, and (e) expressed motivation to participate in this study. Participants with (a) health conditions that could interfere with the quality of the participants’ participation (e.g., epilepsy, severe vision and hearing impairments, and motor deficits), (b) behavioral issues that could impede engagement, (c) difficulty to understand the game mechanism, and (d) concurrent similar intervention were excluded.
2.2. Instruments
A sociodemographic questionnaire was used, covering age, sex, literacy, level of IDD, and previous VR experience. Executive function variables were assessed using tests provided by E-Prime®, a software package designed for psychological experiments and cognitive science [46,47,48]. E-Prime® was operated on a computer running Windows 10, Intel® Core™ i7-6500U processor, 15-inch screen, and a USB mouse. Tests for visual-spatial working memory, sustained attention, and inhibitory control were conducted at an average distance of 50 cm from the participants’ field of vision.
The process of participant randomization is described in the flowchart prepared according to the CONSORT guidelines [49], present in Figure 2.
2.2.1. Corsi Block-Tapping Task
The Corsi Block-Tapping Task (CBTT) is a test that measures visuospatial short-term and working memory. In this test, nine squares appear on a blue screen and light up in yellow, one by one, in a variable sequence. After the stimulus presentation, participants must reproduce the sequence by clicking on each of the squares that turned yellow. The test starts with a simple sequence task that increases or decreases in complexity (varying between 2 and 8 elements) based on participants’ performance [50,51]. The test used 20 sequences. A correct answer was considered when all the numbers in the sequence were right, therefore using the number of correct answers as a performance measure. The score varies between 0 and 20 and a higher score means a better performance.
2.2.2. Simple Reaction Time Task
The Simple Reaction Time (SRT) is a test for sustained attention and processing speed [52,53]. In this test, a single star-shaped stimulus is repeatedly presented at the same location on the screen and participants must press the “1” key as quickly as possible. The time interval between stimuli varies throughout the task [48]. The test used 60 trials. A correct answer was considered when it was provided after the stimulus presentation, therefore using the number of correct answers as a performance measure. The score varies between 0 and 60 and a higher score means a better performance.
2.2.3. Stop Signal Task
The Stop Signal Task (SST) is a test designed to assess inhibitory control, involving a go signal requiring a response and a stop-signal requiring a cancellation of a response [54,55]. Participants are instructed to quickly respond to a left or right arrow presentation using, respectively, the “q” and “p” keyboard keys (go task). Periodically, stimuli appear surrounded by a red light during which participants must withhold their action of pressing any key (stop task). Feedback is provided after each attempt (Psychology Software Tools). Given the participants’ characteristics, keyboard keys were labeled to match the direction of the response arrows — the “q” key with a left arrow (<) and the “p” key with a right arrow (>). The test used 151 trials. A correct answer was considered when the response was coherent with the stimuli direction, therefore using the number of correct answers as a performance measure. The score varies between 0 and 151 and higher score means a better performance.
2.3. Procedures
This study received approval from the Ethics Committee of Escola Superior de Saúde do Politécnico do Porto (CE0109C/2022), and all procedures conformed to the principles in the Declaration of Helsinki [56]. After approval by the APACI institution, participants were selected during March 2023 and the first moment of assessment occurred. A second assessment occurred eight weeks later, without any intervention, to establish a baseline (Figure 2). Before the intervention moment, all participants underwent the benchmark session of the Enhance VR Games, receiving explanations regarding the objectives and controls. Intervention started in May 2023, took place at the APACI institution, and included 24 sessions. The third and final assessment was conducted in July 2023. Data was collected in paper format for the sociodemographic questionnaire, and digital format, through E-prime tasks, for the executive functions’ assessment. All data were coded to maintain confidentiality and will be stored for 10 years by the principal investigator [57].
To promote adherence to the intervention, when the intervention was finished, the researchers provided detailed information about the study and explained the benefits of their participation. A close follow-up was given: the schedule was provided in a timely manner according to the participant’s availability and ensuring that the session was rescheduled in case of absences, the session would be rescheduled at a time convenient for both parties [58].
2.3.1. Intervention Program: Enhance VR — Virtuleap
For cognitive training, three games available on the Enhance VR platform were used. Enhance VR is an app consisting of a library of cognitive exercises developed by Virtuleap [26]. Games were accessed through a Meta Quest 2 head-mounted display, Qualcomm snapdragon 835 processor, 4 GB RAM, 128 GB internal memory, 1400 × 1600 resolution per eye in pixels, with a refresh rate of 72 Hz, and motion controllers. The intervention protocol consisted of twenty-four 20-minute sessions, three sessions per week for eight consecutive weeks. Games were played in the same sequence — React, Memory Wall, and Whack-A-Mole — and mainly in a standing position. Sitting position was allowed if participants felt tired, but only in the Memory Wall game, as it requires less movement. The same researcher was present in all sessions. A brief overview of each game is provided next.
2.3.2. React
The React game was designed to train task switching and response inhibition skills and is based on the mechanisms of the Wisconsin Card Sorting Test [59]and the Stroop Task mechanisms [60]. The player needs to categorize approaching objects according to their shape and color, throwing them into two portals, which only accept matching objects. During the game, players need to adapt to dynamic contexts, as the portals can change their position and required objects during the levels. The difficulty increases by introducing distractor objects that must be ignored [26].
2.3.3. Memory Wall
The Memory Wall game trains short-term visuospatial memory and was inspired by the Visual Patterns Test [61]. Players need to memorize the positions of illuminated cubes that appear for three seconds, in a three-dimensional grid in their field of vision, and then reproduce the pattern. Task difficulty increases with each level, depending on the size of the grid and the number of cubes [26].
2.3.4. Whack-A-Mole
The Whack-A-Mole game focuses on sustained attention and was inspired by the Psychomotor Vigilance Test [62]. Players need to hit moles that appear at random intervals and holes before they disappear. Players need to react as quickly and accurately as possible. The difficulty increases as speed increases and multiple moles can rise simultaneously [26].
2.4. Data Analysis
Data were exported to IBM SPSS Statistics (Version 28.0) for statistical analysis ([63], considering a 0.05 significance level for all performed tests [64]. Descriptive statistics were used to characterize the sample, namely mean (x) and standard deviation (sd), for continuous or discrete variables, and frequencies (N; %) for nominal or ordinal data. The normality of variables was assessed through the Shapiro-Wilk test or the examination of data distribution using threshold criteria for skewness and kurtosis, aiming for values less than |2.0| and |9.0|, respectively [65]. One-way repeated-measures ANOVAs were employed to compare pre- and post-test conditions. Sphericity was tested using Mauchly’s test, with the Huynh-Feldt correction applied when this assumption was not met, and the epsilon was higher than 0.57. In cases where this criterion was not met, the Greenhouse-Geisser correction was utilized [65]. The Bonferroni test was used as a post-hoc measure to determine where the actual differences between the three evaluation moments are located.
3. Results
This sample had 15 participants (Table 1), aged between 22 and 34 years (mean age = 28.07 ± 3.97) and mostly males (66.70%). Participants had mild (53.30%) or moderate (46.70%) IDD level, and eight (53.30%) were illiterate. None had previous experience with VR.
Results for the CBTT, SRT, and SST in the three moments of assessment (Table 2) show that there were statistically significant differences in the scores of the working memory (pCBTT = .001) and inhibitory control (pSST = .043), suggesting that the group’s performance improved with the intervention. The attention test was not significantly different over time (pSRT = .101).
A post-hoc test for score differences between the moments of assessment (Table 3) shows that in CBTT (working memory) and SST (inhibitory control) there were no differences when comparing the first and second moments (pCBTT=1.000; pSST=1.000), but when both are compared with the moment after the intervention the differences are statistically significant in working memory (test1 vs test3 - pCBTT=.004; test2 vs test3 - pCBTT=.002) and inhibitory control (test1 vs test 3 - pSST=.010; test2 vs test3 - pSST=.039).
The analysis of the influence of IDD levels on the results of the assessment results (Table 4) show that there was a statistically significant difference between IDD levels in working memory (pCBTT =.002) and inhibitory control (pSST =.032). The interaction between IDD level and sustained attention does not have significant values.
A post-hoc test for score differences between the three moments of assessment when the level of ID is taken into account (Table 5) shows that in CBTT (working memory) and SST (inhibitory control) are no differences between the first and second moments (pCBTT=.450; pSST=.786), but the differences are statistically significant when both moments were compared with the third assessment in both levels of IDD (test1 vs test 3 - pCBTT=.002; pSST=.032; test2 vs test 3 - pCBTT=.001; pSST=.009).
4. Discussion
This study aimed to assess the effectiveness of an immersive VR cognitive training intervention, using serious games, on working memory, sustained attention, and inhibitory control in young adults with intellectual developmental disability. Overall, an improvement in working memory and inhibitory control was found, but not in sustained attention, both in the whole group and considering IDD level. Although not in all the variables, the positive result in executive functions is in line with previous studies that have used similar cognitive training interventions [35,39,42,66,67]. In fact, despite the literature being scarce, a recent systematic review about the effects of computerized task-based cognitive training programs in a game environment proved to be helpful for people with intellectual developmental disability [42]. They reported multiple studies with significant positive effects across different cognitive domains, such as visual working memory and attention, especially in adults with intellectual developmental disability [42]. Also, Giachero, Quadrini, Pisano, Calati, Rugiero, Ferrero, Pia and Marangolo [35], divided fourteen subjects in three groups according to different levels of IDD and found a greater performance in executive functions tasks — attention and short and long-term spatial memory — in all groups after the treatment, especially in the mild IDD group. Thus, using computerized cognitive training appears to be an effective strategy for improving executive functions of young people with intellectual developmental disability. Specifically, about immersive VR training in rehabilitation programs, it seems that it further provides the advantage of practicing sensory-motor, cognitive, behavioral, and adaptive functions in a safe, close-to-real-world simulation. Positive changes in working memory following the intervention were found. As there were no differences between the first and second moment (i.e., before the intervention), it is reasonable to conclude that these changes were caused by the Enhance VR games. These results are consistent with previous studies that, equally, reported working memory improvements after a computerized cognitive training program for people with intellectual developmental disability. Roording-Ragetlie, Spaltman, de Groot, Klip, Buitelaar and Slaats-Willemse [67] examined the impact of CogMed Working Memory Training on children with intellectual developmental disability in a blind randomized trial, observing improvements in working memory tasks in the group undergoing cognitive training. Another study [66] found that verbal short-term memory improved in teenagers with mild to borderline intellectual developmental disability, after a 5-week intervention, three 6-minute computerized cognitive training sessions per week. Kim and Lee [68] employed a 24-session game-based cognitive training program (30-minute sessions, biweekly, for three months) with children with intellectual developmental disability and discovered that the experimental group improved in working memory performance.
Significant improvements in inhibitory control following the intervention were found, although to a lesser extent than working memory. As far as the authors know, there is little research on inhibitory control intervention for people with intellectual developmental disability. McGlinchey, et al. [69] conducted a quasi-experimental study to investigate the influence of a cognitive training program on executive functions in people with Down syndrome who had mild to moderate intellectual developmental disability. Intervention included 20 minutes of Scientific Brain Training Pro, five days a week, for eight weeks. Post-intervention findings showed significant gains on inhibition control and working memory.
Inhibitory control was reported in the literature to have a medium to large deficit in people with intellectual developmental disability, particularly in behavioral inhibition and interference control [70], which are believed to be more deliberate types of inhibition. According to the inhibition taxonomy proposed by Nigg [71], these two subtypes of executive inhibition — defined as the “processes for intentional control or suppression of responses in the service of higher-order goals” (p. 238). In Danielsson’s study [72], inhibitory control responses were much lower in the IDD group compared to the other two groups — with identical chronological age and identical mental age. These difficulties may have to do with the fact that they had to recruit other cognitive skills linked to mental age, such as working memory (for example, keeping the rules of the task constantly updated) to carry out the task. This seems to be consistent with our own findings — where working memory and inhibitory control improved together —, and earlier research conducted by Thorell et al. [73], which suggested that these two components of executive functions are interrelated, with the functioning of one influencing the functioning of the other. Thus, working memory training may lead to gains in inhibitory tasks and vice versa, enhancing the possibility of improvement in these components. Thus, this relationship can potentially explain our findings, where these two variables improved together following the intervention program, but not sustained attention.
No significant changes were found in sustained attention between pre- and post-treatment assessment. As with inhibitory control, research on sustained attention in people with intellectual developmental disability is scarce, but our findings are consistent with a previous randomized control study that aimed to assess the efficacy of a computerized attention training program in children with intellectual developmental disability [74]. They concluded that, despite observed improvements in selective attention, none were observed regarding sustained attention.
Several studies found that people with intellectual developmental disability have a lower performance in reaction time [75-77] compared to controls with typical development, but not in visual sustained attention [76,78,79]. This means that the absence of improvement in our sample could have been influenced by the motor component of the task that was used to assess sustained attention. Indeed, it has been shown that individuals with intellectual developmental disability present longer premotor time [80], which could influence the motor component of reaction time. Vogt, et al. [81] also reported that the SRT remained unchanged following a self-selected 30-minute running exercise in individuals with intellectual developmental disability. However, several other authors have reported improvements in reaction time after programs that include physical exercise, such as the games chosen for this intervention. For example, Ringenbach, et al. [82] reported that the reaction time improved in individuals with Down syndrome after assisted cycling at 80 revolutions per minute but remained unchanged after voluntary cycling at the participant’s self-selected rate. The authors explained this result based on the difference of pace, as in the assisted cycling intervention individuals with intellectual developmental disability cycled at a rate 49.3% greater than the mean self-selected rate in the voluntary cycling intervention. Chen and Ringenbach [83] showed that 20 minutes of walking on a treadmill at a moderate intensity improved reaction time in individuals with Down syndrome. Affes, Borji, Zarrouk, Sahli and Rebai [75] suggested that low to moderate running exercises improve reaction time in people with intellectual developmental disability, and that low-intensity exercise, rather than moderate, could be more appropriate to enhance reaction time. So, this discrepancy with our results might be due to the difference of exercise intensity, which could be insufficient to produce any reaction time improvement. The design of studies with longer or more intensive interventions could change these results.
An improvement in working memory and inhibitory control independent of IDD level was found, but performance differences between IDD levels have been reported, where children [84,85,86], adolescents and adults [35,70] with mild intellectual developmental disability had fewer problems in executive functions domains than those with moderate IDD. Nonetheless, the fact that no statistically significant differences in performance were found is consistent with other studies. Giachero, Quadrini, Pisano, Calati, Rugiero, Ferrero, Pia and Marangolo [35], reported that all participants showed a better performance in a VR gardening task (twice a week for fourteen weeks), regardless of IDD level. Actually, their sample also performed better in working memory and inhibitory control after the program sessions. However, Giachero, Quadrini, Pisano, Calati, Rugiero, Ferrero, Pia and Marangolo [35] found that the three IDD groups improved equally in attention and short- and long-term spatial memory tasks, concluding that the VR videos trained not only the participants’ gardening skills but also had a significant impact on tasks requiring executive functions, attentional, and spatial skills, that were closely related to the observed procedures. Perhaps this variability in results stems from the inherent heterogeneity of IDD itself.
Using VR-based interventions targeting executive functions as working memory, sustained attention, and inhibitory control in individuals with intellectual developmental disability is not new but is not extensively explored in the literature. Only in the past decade has it re-emerged as a promising adjuvant treatment strategy for cognitive rehabilitation [87,88], so there is still interest in continuing studies that explore different approaches, populations, and results. In this study it was used an innovative platform — Enhance VR — which uses various cognitive training games, accessed through a head-mounted display. It allows for higher level of immersion and a strong sense of presence, given the simultaneous motor, visual, and proprioceptive systems integration, which is effective for enhancing motor and cognitive skills [21,89,90] in several populations. Also, other studies suggest that VR-based approaches are stimulating and allow more immediate feedback on performance, promoting more motivation and adherence to treatment [23,91].
This study has limitations worth mentioning. First, the convenience sample was small, not allowing it to be divided into experimental and control groups. However, as we used the group as its own control, it was possible to compare the first and second moments (without intervention) with the third moment (after the intervention). That given, most likely the changes seen were due to the intervention program, as it was the only change introduced during this period. An argument in favor of the program efficacy is related to the fact that the skills of people with intellectual developmental disability tend be progress slower in time when compared to typically developing people (for a longitudinal study, see [92], hence the improvement might be due to our 24-session program. On the other hand, an argument against this is that people with intellectual developmental disability tend to have less skill-based activities when compared to typically developing people ((for an observational study, see [93], hence the improvement we saw might be due simply by an added training activity. Either argument is in favor of the efficacy of this program — that we argue that could be related to its VR-based design, as discussed above, and consistently with a recent meta-analysis that reported the effectiveness of serious games on social and cognitive skills of children with intellectual developmental disability [94]. Replicating our study, or other VR-based intervention, with larger samples and a control group is recommended. Also, a follow-up assessment after the end of the intervention was not carried out. Thus, it is not possible to know whether the effects obtained immediately after the intervention were maintained in the sample subjects and, even more so, whether they were successfully applied in their daily performance, demonstrating whether there was generalization of the results acquired. Study designs that address a follow-up assessment are recommended.
5. Conclusions
VR as a therapeutic approach for individuals with intellectual developmental disability is still uncommon and requires further investigation. This study presents promising results that seem to support this intervention for improving cognitive performance. However, it should be recalled that the goal of an intervention is to transfer the new acquired skills to daily living activities and community participation, which was not covered in this experiment. IDD is characterized by multiple limitations and compromised functionality that hinders participation in the community. VR is an innovative tool that allows a virtual immersion, providing a highly customizable training context that could lead to unprecedented simulated-based interventions in a safe and controlled environment for people with intellectual developmental disability. Further large-scale studies are warranted to validate these preliminary finding and explore the long-term effects and practical implementation of VR-based interventions with clinical populations.
Author Contributions
The authors confirm contribution to the paper as follows: Conceptualization, Maria João Trigueiro, Vítor Simões-Silva and Bruno Vieira de Melo; Data curation, Maria João Trigueiro and Joana Lopes; Formal analysis, Maria João Trigueiro, Bruno Vieira de Melo and Raquel Simões de Almeida; Funding acquisition, Joana Lopes; Investigation, Joana Lopes, Vítor Simões-Silva, Bruno Vieira de Melo and Raquel Simões de Almeida; Methodology, Maria João Trigueiro, Vítor Simões-Silva and Raquel Simões de Almeida; Project administration, António Marques; Resources, António Marques; Software, Maria João Trigueiro; Supervision, António Marques; Writing – original draft, Maria João Trigueiro, Vítor Simões-Silva, Bruno Vieira de Melo and Raquel Simões de Almeida; Writing – review & editing, Joana Lopes and António Marques. All authors approved the final version of the manuscript.
Funding
This study was carried out within the scope of a broader project, called “Virtualiza-te”, which received financial support from the Instituto Nacional para a Reabilitação (INR, I.P.), based on the “Financing Program for projects by INR, I.P. for Non-Governmental Organizations of People with Disabilities”, granting the necessary resources to conduct the research.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Escola Superior de Saúde do Politécnico do Porto (CE0109C/2022 - 24/02/2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders 5th ed.; 2022.
- Schalock, R.L.; Borthwick-Duffy, S.A.; Bradley, V.J.; Buntinx, W.H.; Coulter, D.L.; Craig, E.M.; Gomez, S.C.; Lachapelle, Y.; Luckasson, R.; Reeve, A. Intellectual disability: Definition, classification, and systems of supports; ERIC: 2010.
- American Association on Intellectual and Developmental Disabilities. Definition of Intellectual Disability. Available online: https://www.operationhousecall.com/wp-content/uploads/2016/12/AAIDD_definition_of_ID-DD_2009.pdf (accessed on 23 de Abril).
- Carulla, L.S.; Reed, G.M.; Vaez-Azizi, L.M.; Cooper, S.-A.; Leal, R.M.; Bertelli, M.; Adnams, C.; Cooray, S.; Deb, S.; Dirani, L.A.; et al. Intellectual developmental disorders: towards a new name, definition and framework for “mental retardation/intellectual disability” in ICD-11. World Psychiatry 2011, 10, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Fidler, D.J.; Lanfranchi, S. Executive function and intellectual disability: innovations, methods and treatment. J Intellect Disabil Res 2022, 66, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Shree, A.; Shukla, P. Intellectual Disability: Definition, classification, causes and characteristics. Learning Community-An International Journal of Educational and Social Development 2016, 7, 9. [CrossRef]
- Srour, M.; Shevell, M. Genetics and the investigation of developmental delay/intellectual disability. Arch Dis Child 2014, 99, 386–389. [Google Scholar] [CrossRef] [PubMed]
- Cornish, K.; Cole, V.; Longhi, E.; Karmiloff-Smith, A.; Scerif, G. Mapping developmental trajectories of attention and working memory in fragile X syndrome: developmental freeze or developmental change? Dev Psychopathol 2013, 25, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Hooper, R.; Hatton, D.; Sideris, J.; Sullivan, K.; Ornstein, A.; Bailey, J. Developmental trajectories of executive functions in young males with fragile X syndrome. Res Dev Disabil 2018, 81, 73–88. [Google Scholar] [CrossRef] [PubMed]
- Bertelli, M.O.; Cooper, S.A.; Salvador-Carulla, L. Intelligence and specific cognitive functions in intellectual disability: implications for assessment and classification. Curr Opin Psychiatry 2018, 31, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Danielsson, H.; Henry, L.; Rönnberg, J.; Nilsson, L.-G. Executive functions in individuals with intellectual disability. Research in Developmental Disabilities 2010, 31, 1299–1304. [Google Scholar] [CrossRef] [PubMed]
- Zagaria, T.; Antonucci, G.; Buono, S.; Recupero, M.; Zoccolotti, P. Executive Functions and Attention Processes in Adolescents and Young Adults with Intellectual Disability. Brain Sci 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Diamond, A. Executive functions. Annu Rev Psychol 2013, 64, 135–168. [Google Scholar] [CrossRef]
- Takacs, Z.K.; Kassai, R. The efficacy of different interventions to foster children’s executive function skills: A series of meta-analyses. Psychol Bull 2019, 145, 653–697. [Google Scholar] [CrossRef]
- Brown, K.A.; Parikh, S.; Patel, D.R. Understanding basic concepts of developmental diagnosis in children. Transl Pediatr 2020, 9, S9–s22. [Google Scholar] [CrossRef]
- Fuster, J. The prefrontal cortex, 5 ed.; ELSEVIER, Ed.; Academic press: 2015.
- Lalonde, G.; Henry, M.; Drouin-Germain, A.; Nolin, P.; Beauchamp, M.H. Assessment of executive function in adolescence: A comparison of traditional and virtual reality tools. Journal of Neuroscience Methods 2013, 219, 76–82. [Google Scholar] [CrossRef]
- Menghini, D.; Addona, F.; Costanzo, F.; Vicari, S. Executive functions in individuals with Williams syndrome. J Intellect Disabil Res 2010, 54, 418–432. [Google Scholar] [CrossRef] [PubMed]
- Lanfranchi, S.; Jerman, O.; Dal Pont, E.; Alberti, A.; Vianello, R. Executive function in adolescents with Down Syndrome. J Intellect Disabil Res 2010, 54, 308–319. [Google Scholar] [CrossRef] [PubMed]
- Cortés Pascual, A.; Moyano Muñoz, N.; Quílez Robres, A. The Relationship Between Executive Functions and Academic Performance in Primary Education: Review and Meta-Analysis. Front Psychol 2019, 10, 1582. [Google Scholar] [CrossRef] [PubMed]
- Varela-Aldás, J.; Palacios-Navarro, G.; Amariglio, R.; García-Magariño, I. Head-Mounted Display-Based Application for Cognitive Training. Sensors (Basel) 2020, 20. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.; Aguirre, E.; Carter, J.; Hoare, S.; Brackley, K.; Goulden, N.; Hoare, Z.; Clarke, C.S.; Charlesworth, G.; Acton, D.; et al. Group cognitive stimulation therapy versus usual care for people with intellectual disabilities and dementia (CST-IDD) in the UK: protocol for a mixed-methods feasibility randomised controlled trial. BMJ Open 2023, 13, e072391. [Google Scholar] [CrossRef] [PubMed]
- Riva, G.; Mancuso, V.; Cavedoni, S.; Stramba-Badiale, C. Virtual reality in neurorehabilitation: a review of its effects on multiple cognitive domains. Expert Rev Med Devices 2020, 17, 1035–1061. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.; Brown, E.; Tsang, W.; Spector, A.; Aguirre, E.; Hoare, S.; Hassiotis, A. Individual cognitive stimulation therapy (iCST) for people with intellectual disability and dementia: a feasibility randomised controlled trial. Aging Ment Health 2022, 26, 698–708. [Google Scholar] [CrossRef]
- Knapp, M.; Bauer, A.; Wittenberg, R.; Comas-Herrera, A.; Cyhlarova, E.; Hu, B.; Jagger, C.; Kingston, A.; Patel, A.; Spector, A.; et al. What are the current and projected future cost and health-related quality of life implications of scaling up cognitive stimulation therapy? Int J Geriatr Psychiatry 2022, 37. [Google Scholar] [CrossRef]
- Brugada-Ramentol, V.; Bozorgzadeh, A.; Jalali, H. Enhance VR: A Multisensory Approach to Cognitive Training and Monitoring. Frontiers in Digital Health 2022, 4. [Google Scholar] [CrossRef] [PubMed]
- Ahn, N. Combined Effects of Virtual Reality and Computer Game-Based Cognitive Therapy on the Development of Visual-Motor Integration in Children with Intellectual Disabilities: A Pilot Study. Occup Ther Int 2021, 2021, 6696779. [Google Scholar] [CrossRef] [PubMed]
- Maggio, M.G.; Maresca, G.; De Luca, R.; Stagnitti, M.C.; Porcari, B.; Ferrera, M.C.; Galletti, F.; Casella, C.; Manuli, A.; Calabrò, R.S. The Growing Use of Virtual Reality in Cognitive Rehabilitation: Fact, Fake or Vision? A Scoping Review. J Natl Med Assoc 2019, 111, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Standen, P.J.; Brown, D.J. Virtual reality in the rehabilitation of people with intellectual disabilities: review. Cyberpsychol Behav 2005, 8, 272-282; discussion 283-278. [CrossRef]
- Ventura, S.; Brivio, E.; Riva, G.; Baños, R.M. Immersive Versus Non-immersive Experience: Exploring the Feasibility of Memory Assessment Through 360° Technology. Front Psychol 2019, 10, 2509. [Google Scholar] [CrossRef] [PubMed]
- Joseph, A.; Browning, M.; Jiang, S. Using Immersive Virtual Environments (IVEs) to Conduct Environmental Design Research: A Primer and Decision Framework. Herd 2020, 13, 11–25. [Google Scholar] [CrossRef] [PubMed]
- Panerai, S.; Catania, V.; Rundo, F.; Ferri, R. Remote Home-Based Virtual Training of Functional Living Skills for Adolescents and Young Adults With Intellectual Disability: Feasibility and Preliminary Results. Frontiers in Psychology 2018, 9. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Hwang, E.; Shin, H.; Gil, Y.H.; Lee, J. Top-down, bottom-up, and history-driven processing of multisensory attentional cues in intellectual disability: An experimental study in virtual reality. PLoS One 2021, 16, e0261298. [Google Scholar] [CrossRef] [PubMed]
- Tieri, G.; Morone, G.; Paolucci, S.; Iosa, M. Virtual reality in cognitive and motor rehabilitation: facts, fiction and fallacies. Expert Rev Med Devices 2018, 15, 107–117. [Google Scholar] [CrossRef]
- Giachero, A.; Quadrini, A.; Pisano, F.; Calati, M.; Rugiero, C.; Ferrero, L.; Pia, L.; Marangolo, P. Procedural Learning through Action Observation: Preliminary Evidence from Virtual Gardening Activity in Intellectual Disability. Brain Sci 2021, 11. [Google Scholar] [CrossRef]
- Nabors, L.; Monnin, J.; Jimenez, S. A Scoping Review of Studies on Virtual Reality for Individuals with Intellectual Disabilities. Advances in Neurodevelopmental Disorders 2020, 4, 344–356. [Google Scholar] [CrossRef]
- Bohil, C.J.; Alicea, B.; Biocca, F.A. Virtual reality in neuroscience research and therapy. Nat Rev Neurosci 2011, 12, 752–762. [Google Scholar] [CrossRef]
- Tao, G.; Garrett, B.; Taverner, T.; Cordingley, E.; Sun, C. Immersive virtual reality health games: a narrative review of game design. J Neuroeng Rehabil 2021, 18, 31. [Google Scholar] [CrossRef] [PubMed]
- Vacca, R.A.; Augello, A.; Gallo, L.; Caggianese, G.; Malizia, V.; La Grutta, S.; Murero, M.; Valenti, D.; Tullo, A.; Balech, B.; et al. Serious Games in the new era of digital-health interventions: A narrative review of their therapeutic applications to manage neurobehavior in neurodevelopmental disorders. Neurosci Biobehav Rev 2023, 149, 105156. [Google Scholar] [CrossRef] [PubMed]
- Boato, E.; Melo, G.; Filho, M.; Moresi, E.; Lourenço, C.; Tristão, R. The Use of Virtual and Computational Technologies in the Psychomotor and Cognitive Development of Children with Down Syndrome: A Systematic Literature Review. Int J Environ Res Public Health 2022, 19. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.Y.; Chen, I.H.; Lin, Y.J.; Chen, Y.; Hsu, W.C. Effects of Virtual Reality-Based Physical and Cognitive Training on Executive Function and Dual-Task Gait Performance in Older Adults With Mild Cognitive Impairment: A Randomized Control Trial. Front Aging Neurosci 2019, 11, 162. [Google Scholar] [CrossRef] [PubMed]
- Suárez-Iglesias, D.; Martínez-de-Quel, Ó.; Marín Moldes, J.R.; Ayán Pérez, C. Effects of Videogaming on the Physical, Mental Health, and Cognitive Function of People with Intellectual Disability: A Systematic Review of Randomized Controlled Trials. Games Health J 2021, 10, 295–313. [Google Scholar] [CrossRef]
- Des Jarlais, D.C.; Lyles, C.; Crepaz, N.; Group, T. Improving the reporting quality of nonrandomized evaluations of behavioral and public health interventions: the TREND statement. American journal of public health 2004, 94, 361–366. [Google Scholar] [CrossRef]
- Harris, A.; McGregor, J.; Perencevich, E.; Furuno, J.; Zhu, J.; Peterson, D.; Finkelstein, J. The use and interpretation of quasi-experimental studies in medical informatics. Journal of the American Medical Informatics Association 2006, 13, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Thyer, B. Quasi-experimental research designs; Oxford University Press: 2012.
- Kim, H.S.; Yeon, H.W.; Choi, M.H.; Kim, J.H.; Choi, J.S.; Park, J.Y.; Jun, J.H.; Yi, J.H.; Tack, G.R.; Chung, S.C. Development of a tactile stimulator with simultaneous visual and auditory stimulation using E-Prime software. Comput Methods Biomech Biomed Engin 2013, 16, 481–487. [Google Scholar] [CrossRef]
- Kim, J.; Gabriel, U.; Gygax, P. Testing the effectiveness of the Internet-based instrument PsyToolkit: A comparison between web-based (PsyToolkit) and lab-based (E-Prime 3.0) measurements of response choice and response time in a complex psycholinguistic task. PLoS One 2019, 14, e0221802. [CrossRef]
- Spapé, M.; Verdonschot, R.; Van Dantzig, S.; Steenbergen, H. The E-Primer: An Introduction to Creating Psychological Experiments in E-Prime; 2014.
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. Journal of Pharmacology and pharmacotherapeutics 2010, 1, 100–107. [Google Scholar] [CrossRef]
- Arce, T.; McMullen, K. The Corsi Block-Tapping Test: Evaluating methodological practices with an eye towards modern digital frameworks. Computers in Human Behavior Reports 2021, 4, 100099. [Google Scholar] [CrossRef]
- Claessen, M.H.; van der Ham, I.J.; van Zandvoort, M.J. Computerization of the standard corsi block-tapping task affects its underlying cognitive concepts: a pilot study. Appl Neuropsychol Adult 2015, 22, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Weissberg, R.; Ruff, H.A.; Lawson, K.R. The usefulness of reaction time tasks in studying attention and organization of behavior in young children. J Dev Behav Pediatr 1990, 11, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Zajdel, R.; Nowak, D. Simple and complex reaction time measurement A preliminary evaluation of new approach and diagnostic tool. Comput Biol Med 2007, 37, 1724–1730. [Google Scholar] [CrossRef] [PubMed]
- Caglayan, A.; Stumpenhorst, K.; Winter, Y. The Stop Signal Task for Measuring Behavioral Inhibition in Mice With Increased Sensitivity and High-Throughput Operation. Frontiers in Behavioral Neuroscience 2021, 15. [Google Scholar] [CrossRef] [PubMed]
- Friehs, M.A.; Dechant, M.; Vedress, S.; Frings, C.; Mandryk, R.L. Effective Gamification of the Stop-Signal Task: Two Controlled Laboratory Experiments. JMIR Serious Games 2020, 8, e17810. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. Jama 2013, 310, 2191-2194.
- Smith, G.; Morrow, H.; Ross, A. Field Trials of Health Interventions: A Toolbox; OUP Oxford © London School of Hygiene and Tropical Medicine 2015.: Oxford (UK), 2015.
- Zweben, A.; Fucito, L.M.; O’Malley, S.S. Effective strategies for maintaining research participation in clinical trials. Drug Information Journal: DIJ/Drug Information Association 2009, 43, 459-467.
- Grant, D.A.; Berg, E.A. A behavioral analysis of degree of reinforcement and ease of shifting to new responses in a Weigl-type card-sorting problem. J Exp Psychol 1948, 38, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Stroop, J.R. Studies of interference in serial verbal reactions. Journal of experimental psychology 1935, 18, 643. [Google Scholar] [CrossRef]
- Della Sala, S.; Gray, C.; Baddeley, A.; Wilson, L. Visual Patterns Test: A test of short-term visual recall. 1997.
- Dinges, D.F.; Powell, J.W. Microcomputer analyses of performance on a portable, simple visual RT task during sustained operations. Behavior Research Methods, Instruments, & Computers 1985, 17, 652-655,. [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows Armonk; IBM Corp.: NY, 2021. [Google Scholar]
- Marôco, J. Análise Estatística com o SPSS Statistics.: 7ª edição; ReportNumber, Lda: 2018.
- Gignac, G.E. How2statsbook (Online Edition 1); Author: Perth, Australia, 2019. [Google Scholar]
- Van der Molen, M.J.; Van Luit, J.E.; Van der Molen, M.W.; Klugkist, I.; Jongmans, M.J. Effectiveness of a computerised working memory training in adolescents with mild to borderline intellectual disabilities. J Intellect Disabil Res 2010, 54, 433–447. [Google Scholar] [CrossRef]
- Roording-Ragetlie, S.; Spaltman, M.; de Groot, E.; Klip, H.; Buitelaar, J.; Slaats-Willemse, D. Working memory training in children with borderline intellectual functioning and neuropsychiatric disorders: a triple-blind randomised controlled trial. Journal of Intellectual Disability Research 2022, 66, 178–194. [Google Scholar] [CrossRef]
- Kim, S.-C.; Lee, H.-s. Effect of game-based cognitive training programs on cognitive learning of children with intellectual disabilities. Applied sciences 2021, 11, 8582. [Google Scholar] [CrossRef]
- McGlinchey, E.; McCarron, M.; Holland, A.; McCallion, P. Examining the effects of computerised cognitive training on levels of executive function in adults with Down syndrome. J Intellect Disabil Res 2019, 63, 1137–1150. [Google Scholar] [CrossRef] [PubMed]
- Bexkens, A.; Ruzzano, L.; Collot d’ Escury-Koenigs, A.M.L.; Van der Molen, M.W.; Huizenga, H.M. Inhibition deficits in individuals with intellectual disability: a meta-regression analysis. Journal of Intellectual Disability Research 2014, 58, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Nigg, J.T. On inhibition/disinhibition in developmental psychopathology: views from cognitive and personality psychology and a working inhibition taxonomy. Psychological bulletin 2000, 126, 220. [Google Scholar] [CrossRef] [PubMed]
- Danielsson, H.; Henry, L.; Messer, D.; Rönnberg, J. Strengths and weaknesses in executive functioning in children with intellectual disability. Research in developmental disabilities 2012, 33, 600–607. [Google Scholar] [CrossRef] [PubMed]
- Thorell, L.B.; Lindqvist, S.; Bergman Nutley, S.; Bohlin, G.; Klingberg, T. Training and transfer effects of executive functions in preschool children. Dev Sci 2009, 12, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Kirk, H.E.; Gray, K.M.; Ellis, K.; Taffe, J.; Cornish, K.M. Computerised attention training for children with intellectual and developmental disabilities: a randomised controlled trial. J Child Psychol Psychiatry 2016, 57, 1380–1389. [Google Scholar] [CrossRef] [PubMed]
- Affes, S.; Borji, R.; Zarrouk, N.; Sahli, S.; Rebai, H. Effects of running exercises on reaction time and working memory in individuals with intellectual disability. Journal of Intellectual Disability Research 2021, 65, 99–112. [Google Scholar] [CrossRef] [PubMed]
- Costanzo, F.; Varuzza, C.; Menghini, D.; Addona, F.; Gianesini, T.; Vicari, S. Executive functions in intellectual disabilities: a comparison between Williams syndrome and Down syndrome. Research in developmental disabilities 2013, 34, 1770–1780. [Google Scholar] [CrossRef]
- Melam, G.; Buragadda, S.; Alhusaini, A.; Dhamija, P. Reaction and movement time in Down syndrome children under different visual feedback conditions. J Nov Physiother 2014, 4, 2. [Google Scholar] [CrossRef]
- Cornish, K.; Scerif, G.; Karmiloff-Smith, A. Tracing syndrome-specific trajectories of attention across the lifespan. Cortex 2007, 43, 672–685. [Google Scholar] [CrossRef] [PubMed]
- Munir, F.; Cornish, K.M.; Wilding, J. A neuropsychological profile of attention deficits in young males with fragile X syndrome. Neuropsychologia 2000, 38, 1261–1270. [Google Scholar] [CrossRef] [PubMed]
- Zafeiridis, A.; Giagazoglou, P.; Dipla, K.; Salonikidis, K.; Karra, C.; Kellis, E. Muscle fatigue during intermittent exercise in individuals with mental retardation. Research in developmental disabilities 2010, 31, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Vogt, T.; Schneider, S.; Abeln, V.; Anneken, V.; Strüder, H.K. Exercise, mood and cognitive performance in intellectual disability—A neurophysiological approach. Behavioural brain research 2012, 226, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Ringenbach, S.D.; Albert, A.R.; Chen, C.-C.; Alberts, J.L. Acute bouts of assisted cycling improves cognitive and upper extremity movement functions in adolescents with Down syndrome. Mental Retardation 2014, 52, 124–135. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.C.; Ringenbach, s. Dose–response relationship between intensity of exercise and cognitive performance in individuals with Down syndrome: a preliminary study. Journal of Intellectual Disability Research 2016, 60, 606–614. [Google Scholar] [CrossRef]
- Erostarbe-Pérez, M.; Reparaz-Abaitua, C.; Martínez-Pérez, L.; Magallón-Recalde, S. Executive functions and their relationship with intellectual capacity and age in schoolchildren with intellectual disability. Journal of Intellectual Disability Research 2022, 66, 50–67. [Google Scholar] [CrossRef]
- Memisevic, H.; Sinanovic, O. Executive function in children with intellectual disability–the effects of sex, level and aetiology of intellectual disability. Journal of intellectual disability research 2014, 58, 830–837. [Google Scholar] [CrossRef]
- Schuchardt, K.; Gebhardt, M.; Mäehler, C. Working memory functions in children with different degrees of intellectual disability. Journal of intellectual disability research 2010, 54, 346–353. [Google Scholar] [CrossRef]
- Maggio, M.G.; Maresca, G.; De Luca, R.; Stagnitti, M.C.; Porcari, B.; Ferrera, M.C.; Galletti, F.; Casella, C.; Manuli, A.; Calabrò, R.S. The growing use of virtual reality in cognitive rehabilitation: fact, fake or vision? A scoping review. Journal of the National Medical Association 2019, 111, 457–463. [Google Scholar] [CrossRef]
- De Luca, R.; Lo Buono, V.; Leo, A.; Russo, M.; Aragona, B.; Leonardi, S.; Buda, A.; Naro, A.; Calabrò, R.S. Use of virtual reality in improving poststroke neglect: Promising neuropsychological and neurophysiological findings from a case study. Applied Neuropsychology: Adult 2019, 26, 96-100.
- Knobel, S.E.; Kaufmann, B.C.; Gerber, S.M.; Cazzoli, D.; Müri, R.M.; Nyffeler, T.; Nef, T. Immersive 3D virtual reality cancellation task for visual neglect assessment: a pilot study. Frontiers in human neuroscience 2020, 14, 180. [Google Scholar] [CrossRef] [PubMed]
- Saldana, D.; Neureither, M.; Schmiesing, A.; Jahng, E.; Kysh, L.; Roll, S.C.; Liew, S.-L. Applications of head-mounted displays for virtual reality in adult physical rehabilitation: a scoping review. The American Journal of Occupational Therapy 2020, 74, 7405205060p7405205061–7405205060p7405205015. [Google Scholar] [CrossRef] [PubMed]
- Yalon-Chamovitz, S.; Weiss, P.L. Virtual reality as a leisure activity for young adults with physical and intellectual disabilities. Res Dev Disabil 2008, 29, 273–287. [Google Scholar] [CrossRef] [PubMed]
- Chadwick, O.; Cuddy, M.; Kusel, Y.; Taylor, E. Handicaps and the development of skills between childhood and early adolescence in young people with severe intellectual disabilities. Journal of Intellectual Disability Research 2005, 49, 877–888. [Google Scholar] [CrossRef]
- King, M.; Shields, N.; Imms, C.; Black, M.; Ardern, C. Participation of children with intellectual disability compared with typically developing children. Research in developmental disabilities 2013, 34, 1854–1862. [Google Scholar] [CrossRef]
- Derks, S.; Willemen, A.M.; Sterkenburg, P.S. Improving adaptive and cognitive skills of children with an intellectual disability and/or autism spectrum disorder: Meta-analysis of randomised controlled trials on the effects of serious games. International Journal of Child-Computer Interaction 2022, 33, 100488.
Figure 1.
One-group temporal series structure.

Figure 2.
CONSORT Diagram of Study Design.
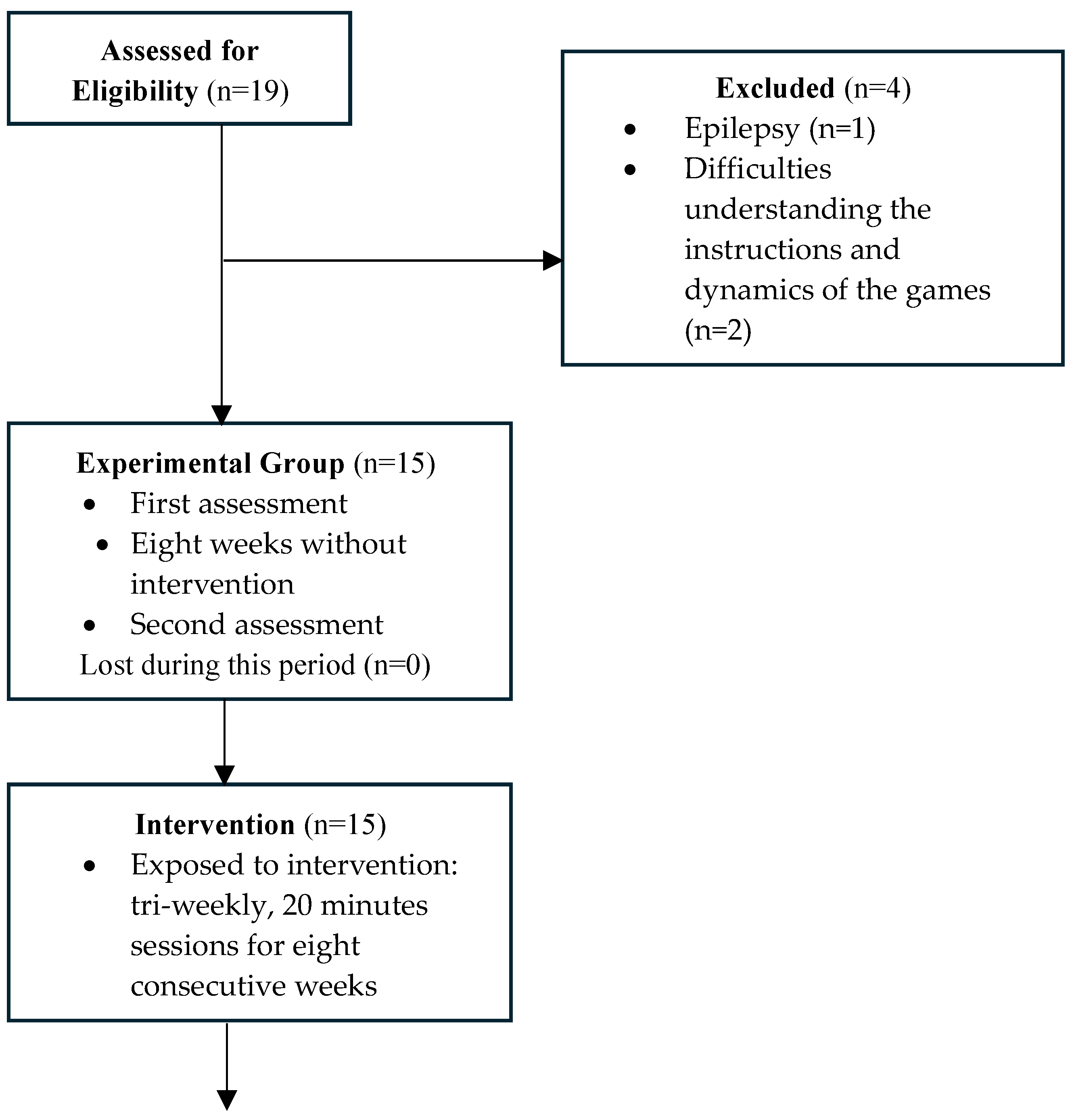
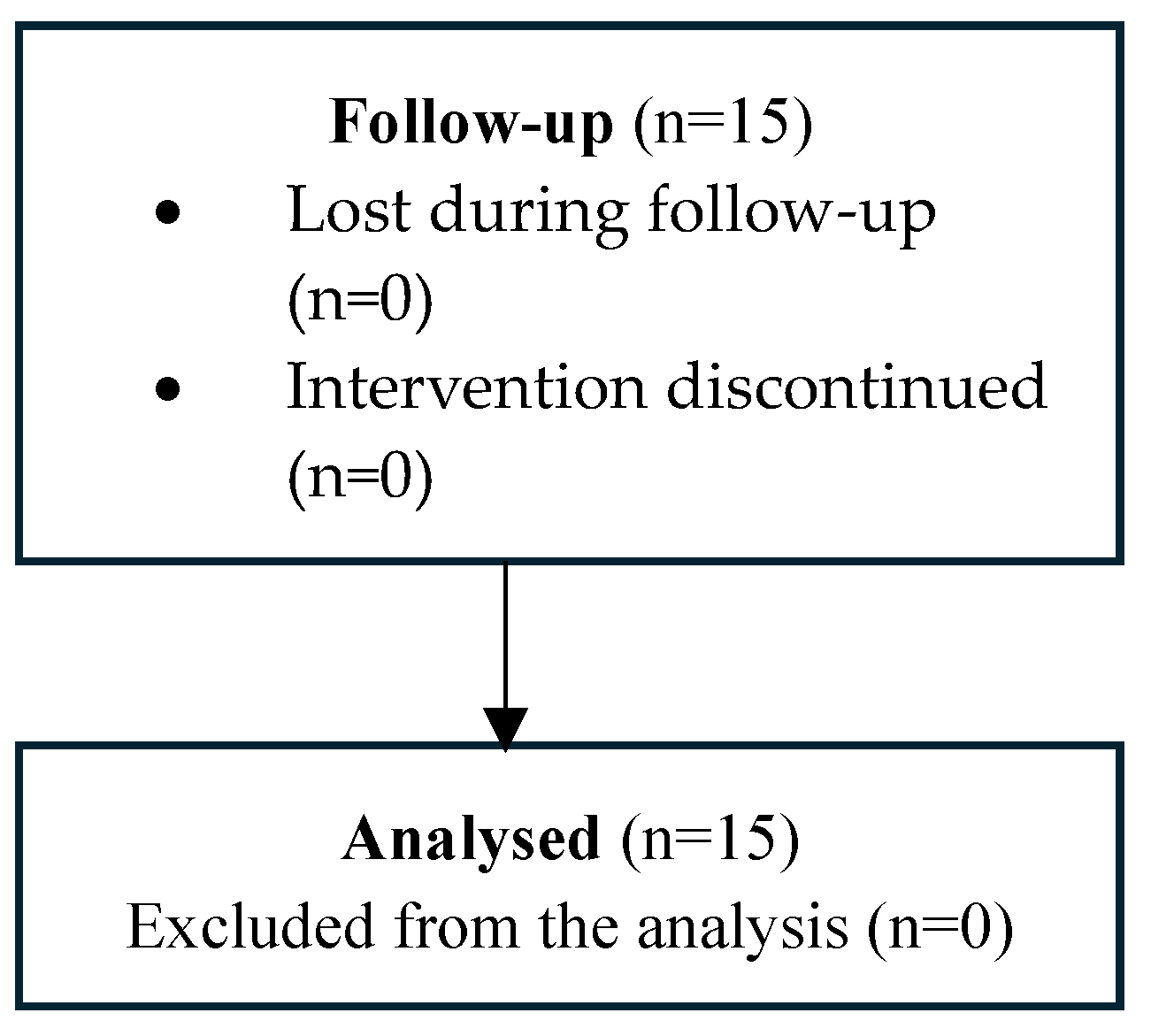

Table 1.
Sample’s sociodemographic characteristics.
| x ± SD | N (%) | ||
| Age (years) | 28.07 ± 3.97 | ||
| Gender | Male | 10 (66.70) | |
| Female | 5 (33.30) | ||
| Levels of IDD | Mild | 8 (53.30) | |
| Moderate | 7 (46.70) | ||
| Literacy | Yes | 7 (46.70) | |
| No | 8 (53.30) | ||
| Previous experience with VR | Yes | 0 (.00) | |
| No | 15 (100.00) |
IDD - Intellectual Developmental Disability; VR – Virtual Reality; x - mean; SD – standard deviation; N- Absolute frequency; % - Relative frequency.
Table 2.
Score differences in the three moments of assessment.
| test1 x ± SD | test2 x ± SD | test3 x ± SD | p-value | Power | |
| CBTT | 11.53 ± 2.03 | 11.07 ± 2.54 | 13.93 ± 1.91 | .001* | .960 |
| SRT | 55.86 ± 5.41 | 53.47 ± 11.21 | 57.73 ± 3.57 | .101 | .373 |
| SST | 90.40 ± 22.76 | 90.87 ± 23.89 | 99.53 ± 27.58 | .043* | .545 |
CBTT - Corsi Block-Tapping Task; SST - Stop Signal Task; SRT - Simple Reaction Time; x - mean; SD – standard deviation; p-value - Within-subjects p-value;*p<.05).
Table 3.
Score differences between moments of assessment.
| CBTT | SST | |||
| Mean difference | p-valuea | Mean difference | p-valuea | |
| Test1 vs. Test2 | .467 | 1.000 | -.467 | 1.000 |
| Test1 vs. Test3 | -2.400 | .004* | -9.133 | .010* |
| Test2 vs. Test3 | -2.867 | .002* | -8.667 | .039* |
CCBTT - Corsi Block-Tapping Task; SST - Stop Signal Task; *p-value - Pairwise Comparisons Bonferroni; *p-value<.05).
Table 4.
Score differences between moments of assessment.
| IDD levels | test1 | test2 | test3 | p-valuea | p-valueb | powera | powerb | |
| CBTT | Mild | 11.63±2.26 | 11.25±3.28 | 14.50±2.33 | .002* | .418 | .949 | .121 |
| Moderate | 11.43±1.90 | 10.86±1.57 | 13.29±1.11 | |||||
| SRT | Mild | 55.25±5.44 | 56.88±4.58 | 56.88±4.58 | .112 | .818 | .352 | .055 |
| Moderate | 56.57±5.71 | 57.00±3.32 | 58.71±1.80 | |||||
| SST | Mild | 99.63± 7.46 | 98.75± 8.16 | 103.38± 10.00 | .032* | .168 | .605 | .272 |
| Moderate | 79.86± 7.98 | 81.86± 8.72 | 95.14±10.69 |
- mean; ơ– standard deviation; p-valuea - Within-subjects p-value; p-valueb- Interaction p-value; powera – Within-subjects; powerb- Interaction; CCBTT - Corsi Block-Tapping Task; SST - Stop Signal Task; SRT - Simple Reaction Time; IDD – Intelectual Developmental Disability; *p-value<.05).
Table 5.
Score differences between moments of assessment considering intellectual disability level.
| Level of IDD | ||||
| CBTT | SST | |||
| Mean difference ±sd | p-valuea | Mean difference ±sd | p-valuea | |
| Test1 vs. Test2 | .47 ± .61 | .450 | .56 ± 2.03 | .786 |
| Test1 vs. Test3 | -2.37 ± .61 | .002* | 9.52 ± 3.95 | .032* |
| Test2 vs. Test3 | -2.84 ± .69 | .001* | 8.96 ± 2.93 | .009* |
CCBTT - Corsi Block-Tapping Task; SST - Stop Signal Task; IDD – Intellectual Developmental Disability; p-valuea - Pairwise Comparisons Bonferroni; *p-value<.05.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



