
Submitted:
23 July 2024
Posted:
23 July 2024
You are already at the latest version
Abstract
Background: Resistant hypertension (HTN) is associated with high risk of cardiovascular complications. Our study aimed to assess prevalence, characteristics and treatment of patients with resistant HTN; Methods: We screened 4340 consecutive cardiovascular patients and identified 3762 with HTN. Of them 128 fulfilled criteria for resistant HTN and were included in our study. We matched these patients to 128 hypertensive patients with controlled HTN; Results: Resistant HTN patients were 3.4% of all hypertensives. Most of these patients (67.2%) were at high or very high cardiovascular risk compared to controlled HTN patients (40.6%), p<0001. Resistant HTN patients had more frequently concomitant chronic kidney disease (CKD) (60.9%), overweight/obesity (52.3%), dyslipidemias (35.2%), smoking (27.3%) and diabetes (21.9%) compared to controlled HTN patients (37.5%, 29.7%, 28.1%, 14.1% and 7.8% respectively), p<0.001. Regression analysis showed strongest association of resistant HTN with CKD (OR 6.64), stage III HTN (OR 3.07) and obesity/overweight (OR 2.60). In contrast, single-pill combinations (SPCs) were associated with lower likelihood of uncontrolled HTN (OR 0.58); Conclusions: Resistant HTN represented a small proportion of all hypertensives in our study, but it was characterized by high/very high cardiovascular risk. Optimized therapy including increased usage of SPCs could improve blood pressure control and long-term prognosis of these patients.
Keywords:
resistant
; hypertension
; treatment
; control
; cardiovascular
; risk
1. Introduction
Arterial hypertension (HTN) is defined as a sustained increase of the systolic blood pressure (SBP) ≥140 and/or diastolic blood pressure (DBP) ≥90 mmHg on repeated office measurements and when necessary – confirmed by 24-hour ambulatory blood pressure (BP) measurement and/or multiple home BP measurements [1,2,3]. Nowadays, HTN is a controllable disease for most patients [1,2]. Modern therapeutic strategies based on single-pill combinations, including different pharmacological classes could achieve target BP values in as many as 60% of patients on double combinations and 90-95% of those on triple combinations [2]. Yet, some hypertensives remain uncontrolled, irrespective of the therapeutic approach: many of these cases are referred as patients with “Resistant HTN” [1,2,3]. According to most guidelines HTN is considered “true resistant” if treatment with optimal or best tolerated doses of ≥3 drugs, including a thiazide/thiazide-like diuretic, a blocker of renin-angiotensin-aldosterone system (RAAS) and a calcium channel blocker (CCB) plus appropriate lifestyle measures fail to lower office BP to <140/90 mmHg [1,2,3,4]. After applying these criteria, resistant HTN prevalence is estimated to be 5-10% of the entire hypertensive population in most countries according to data from clinical studies and registries (up to 19% according to some publications) [1,2,3,5]. However, true prevalence of resistant HTN is difficult to be estimated because of its dependence on a large number of factors: clinical settings (general population, tertiary referral center, clinical trials), classes and optimal doses of the antihypertensive drugs used, exclusion or retention of patients not adhering to treatment, methods of BP measurement, definition of the target BP value representing BP control, etc. [2,3,5]. Exclusion of secondary HTN hypertension and confirmation of good adherence to therapy are also required to define true resistant HTN and exclude pseudo-resistant HTN [1,2,3,4] .
Resistant hypertension can be very common among patients some concomitant diseases and risk factors (RF) such as a chronic kidney disease (CKD), type 2 diabetes mellitus (DM), obesity, obstructive sleep apnea (OSA), high sodium intake, sedentary lifestyle, excessive alcohol consumption, older age, etc. [2,3,5].
Regarding the pathophysiology of resistant HTN, it is probably involving an interplay between multiple neurohumoral factors such as increased sympathetic activity and increased levels of aldosterone, endothelin-1, vasopressin, etc. [2,3,5,6,7,8,9,10,11]. These factors contribute to increased peripheral vascular resistance, retention of sodium and volume overload, increased arterial stiffness, all of them leading to cardio-renal damage [3,5,8,9,11].
Patients with resistant HTN are considered by many to be at higher risk for development of subclinical and clinically manifested hypertension-mediated organ damage (HMOD) such as left ventricular hypertrophy, atherosclerotic vascular disease, atrial fibrillation, heart failure, ischemic and hemorrhagic stroke, CKD (including end-stage renal failure) and premature cardiovascular death [2,5,12]. According to some clinical studies many of these patients have a 10-year risk for fatal or non-fatal cardiovascular event >20% at the time of diagnosis [2,3,4].
Unsolved issues regarding true prevalence of resistant HTN, clinical characteristics of this heterogeneous group of hypertensive patients and therapeutic challenges many clinicians face, gave us grounds to conduct our clinical study trying to find an answer to at least part of these questions related to resistant HTN.
2. Materials and Methods
We conducted an observational, retrospective, non-interventional study in which as a first step we screened consecutively 4340 patients for HTN. Screening included patients hospitalized at our clinic for different cardiovascular pathologies/diagnoses for the period 01 July 2018 – 27 March 2024. We found HTN in 3762 (86.7%) of all patients. At the next step, applying criteria recommended by 2018 Europeans Society of Cardiology (ESC)/European Society of Hypertension (ESH) Guidelines and 2023 ESH Guidelines for the management of arterial hypertension were screened the hypertensive population for resistant HTN [1,2].
Inclusion criteria for our study were: 1. Age ≥18 years; 2. Established diagnosis “Arterial hypertension” according to 2018 ESC/ESH Guidelines or/and 2023 ESH Guidelines for diagnosis and treatment of this disease; 3. Maintenance of SBP ≥140 and/or diastolic BP ≥90 mmHg after ≥1 month of treatment with optimal or best tolerated doses of 3 or more drugs, including a thiazide/thiazide-like diuretic, an RAAS blocker – either an inhibitor of the angiotensin converting enzyme (ACEi) or an angiotensin II receptor blocker (ARB) and a calcium channel blocker (CCB); 4. Uncontrolled HTN was confirmed by 24-h Holter-BP monitoring; 5. Good adherence (≥80% of the treatment period) to the prescribed treatment; 6. Patient’s agreement and signed informed consent at hospital admission to participate in all planned physical, instrumental and laboratory investigations.
Exclusion criteria were the following ones: 1. Patients with HTN at target BP values, achieved by ≤3 antihypertensive drugs; 2. Patients with uncontrolled HTN by ≥3 drugs, but not in optimal doses or not including ACEi/ARB + CCB + thiazide/thiazide-like diuretic or the treatment period is <1 month; 3. Established diagnosis “Secondary HTN”; 4. Suspected/confirmed pseudo-resistant HTN; 5. Patient’s clinical condition or/and concomitant factors/diseases made the planned instrumental investigations not feasible.
After applying the aforementioned criteria we identified 128 patients with resistant HTN: they represented 2.9% of all cardiovascular patients (n = 4340) we screened and 3.4% of the hypertensive population (n = 3762) in our study. Of patients with resistant HTN 63 (49.2%) were males and 65 (50.8%) - females, p = 0.860. The median age was 58.0 years with interquartile range (IQR) 46.0-69.0 years.
At the third step, we matched resistant HTN patients in a “case-control” manner of analysis to 128 consecutive hypertensive patients from the general hypertensive population in our study who had achieved control on HTN. These patients had to fulfil the following inclusion criteria: 1. Office SBP 130-139 mmHg for patients aged ≥65 years and 120-129 mm Hg for those aged <65 years; 2. Office DBP 70-80 mm Hg; 3. Mean 24-h Holter-monitoring values <130 mm Hg for SBP and <80 mm Hg for DBP; 4. Mean daytime Holter-monitoring SBP <135 mm Hg and <85 mm Hg for DBP; 5. Mean nighttime Holter-monitoring SBP <120 mm Hg for SBP and <70 mm Hg for DBP; 6. Control of HTN was achieved by ≤3 antihypertensive drugs (with a free or a single-pill combination if >1 drug used) from different classes at standard or maximal doses taken for at least 4 weeks; 7. Patient’s agreement and signed informed consent at hospital admission to participate in all planned physical, instrumental and laboratory investigations.
The control group was matched to the resistant HTN group only for achieved control of HTN. Figure 1 summarizes the participant’s inclusion process in our study.
The study was conducted in accordance with the ethical standards, laid down in the 1964 Declaration of Helsinki and its later amendments, guidelines for good clinical practices, and local regulations. Approval by a local ethics committee was not necessary for this type of clinical studies/scientific research (observational, retrospective, non-interventional) in our country. All participants had signed an informed consent at their hospital admission that they agree to be examined and treated according the diagnostic and treatment plan proposed by the clinician/hospital team in charge and the results could be used anonymously for scientific purposes. The study was registered at https://www.clinicaltrials.gov/ on 7th of February, 2024 with reference number KPVB0001RH.
Patients’ information was collected in a structured questionnaire form including demographic characteristics, medical history (complaints, cardiovascular risk factors and comorbidities, treatment, etc.), clinical, instrumental and laboratory findings of interest. We gathered the necessary data directly from the medical documentation of patient’s hospitalization and other documents if available. Instrumental investigations included electrocardiography (ECG), transthoracic echocardiography, 24-h Holter BP monitoring, routine laboratory parameters. Contrast computed tomography (CT) imaging of the kidneys with renovasography was conducted to all patients with resistant HTN and to patients with controlled HTN whose kidney echography plus duplex Doppler-sonography showed abnormal findings. Additional investigations had been performed, if necessary.
Patient’s cardiovascular risk was calculated according to the 2021 ESC Guidelines on cardiovascular prevention and 2023 ESH Guidelines for the management of arterial hypertension [2,12].
Statistical Analysis
The statistical analysis was performed by SPSS statistical package, version 19.0 (SPSS Inc, Chicago, IL). The data were summarized by frequencies and percentages for categorical variables and by minimal, maximal, mean values and standard deviation for continuous ones with normal distribution or a median and 25th -75th percentiles IQR for continuous variables with skewed distributions. The normality of distribution of continuous data was assessed by Shapiro-Wilk test. For comparison of categorical variables we used independent χ2-test, Fisher’s exact test and Gamma-test for categorical ordinal variables. Analysis of variance (ANOVA) was used for comparison of parametric data, Mann-Whitney U test and Kruskal-Wallis H test – for nonparametric data. The correlation between the variables was assessed by Pearson or Spearman correlation method depending on data distribution. Association between the independent (concomitant conditions/factors/diseases) and dependent variables (resistant/controlled HTN) was determined by logistic regression analysis with the strength of each variable demonstrated by the odds ratio (OR). All results were considered to be statistically significant at p-value <0.05.
3. Results
3.1. Patient’s Demographic and Clinical Characteristics
Table 1 presents demographic characteristics, concomitant risk factors and diseases, and the cardiovascular risk of the participants in our study. Both genders were almost equally represented not only in the general study population, but also in the two groups that were compared (resistant/controlled HTN). Patients with resistant HTN were younger with а median age of 5 years compared to controlled HTN. As visible from Table 1 both groups had comparable duration of elevated BP, however patients with resistant-to-treatment HTN were more frequently with moderate and severe HTN (SPB ≥160 and/or DBP ≥ 100 mm Hg). Subclinical and clinically manifested HMOD were also more common among patients with resistant HTN indicating advanced stage of hypertension. Risk factors and concomitant diseases that were more prevalent among resistant HTN patients were active smoking, overweight/obesity, type 2 diabetes DM and chronic CKD. Ischemic heart disease had borderline statistical significance and other RF and concomitant diseases had comparable prevalence among both groups.
Among patients with CKD in the study population, 54 (42.2%) with resistant and 14 (10.9%) with controlled HTN had a renovascular disease, 15 (11.7%) with resistant and 8 (6.3%) with controlled HTN – a renal parenchymal disease and 10 (7.8%) with resistant, and 3 (2.3%) with controlled HTN – both renovascular and renal parenchymal disease, p <0.001.
3.2. Laboratory and Instrumental Investigations
Table 2 shows some basic laboratory parameters that were investigated in patients from our study. Patients with resistant HTN had higher levels of fasting blood glucose and creatinine, and lower estimated glomerular filtration rate (eGFR), calculated according to the equation recommended by the 2021 Guidelines of CKD Epidemiology Collaboration Group (CKD-EPI) compared to patients with controlled HTN [13]. For all other laboratory parameters both groups were comparable.
Figure 2 shows CKD stage based on eGRF, calculated according to 2021 CKD-EPI equation. Patients with resistant HTN had more advanced CKD compared to patients with controlled HTN, but for both groups kidney dysfunction was moderate to severe (IIIb stage) at worst: there were not patients from either group with severe (IV stage) and terminal (V stage) CKD.
Table 3 shows office BP values, 24-h Holter-BP monitoring values and office-measured heart rate (HR) of the study population. Patients with resistant HTN had significantly higher BP values both from office and Holter-BP measurements compared to patients with controlled HTN. We found no statistically significant difference between the two groups for HR.
Figure 3 shows the circadian BP dipping status of the study population, assessed by 24-h Holter-BP monitoring. According to our results non-dipping and reverse dipping state were significantly more common among patients with resistant HTN.
3.3. Risk Profile of the Study Population
Figure 4 demonstrates the cardiovascular risk of the participants in our study. The risk was calculated according to the algorithms, proposed by the 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice and 2023 ESH Guidelines for the management of arterial hypertension. According to the results significant percentage of all hypertensive patients participating in our study (~54%) were at high and very high cardiovascular risk: >67% of patients with resistant and >40% of those with controlled HTN, p<0.001.
3.4. Treatment of the Study Population
Table 4 shows the antihypertensive classes of drugs, used by our patients prior to re-evaluation of their therapeutic approach. Calcium channel blockers, mostly dihydropyridine -type (DHP-CCB), diuretics (mostly thiazide/thiazide-like) and ARBs were most frequently prescribed classes in patients with resistant HTN. The same classes were most preferred for patients with controlled HTN too, but prescription rates were significantly lower compared to resistant HTN. Prescription of second-line antihypertensive drugs - mineralocorticoid receptor antagonists (MRA), α1-receptor blockers and centrally acting agents was higher in patients with resistant HTN.
Most frequently prescribed representatives of each antihypertensive class were the following ones:
- Perindopril in 34 (43.6%) of 78 patients on ACEi: 15 (44.1%) of 34 patients with resistant HTN and 19 (43.2%) of 44 patients with controlled HTN, p = 0.637;
- Valsartan in 87 (59.2%) of 147 patients on ARB: 54 (65.9%) of 82 patients with resistant HTN and 33 (50.8%) of 65 patients with controlled HTN, p = 0.072;
- Amlodipine in 80 (44.2%) of 181 patients on CCB: 37 (34.6%) of 107 patients with resistant HTN and 43 (58.1%) of 74 patients with controlled HTN, p < 0.001.
- Hydrochlorothiazide in 90 (49.7%) of 181 patients on diuretics: 45 (42.5%) of 106 patients with resistant HTN and 45 (58.4%) of 77 patients with controlled HTN, p = 0.001;
- Bisoprolol in 82 (65.6%) of 125 patients on beta-blockers: 50 (65.8%) of 76 patients with resistant HTN and 32 (65.3%) of 49 patients with controlled HTN, p = 0.537;
- Spironolactone in 23 (85.2%) of 27 patients on MRAs: 17 (80.9%) of 21 patients with resistant HTN and 6 (100.0%) of 6 patients with controlled HTN, p = 0.006
- Doxazosin in 11 (64.7%) of 17 patients on α1-receptor blockers: 10 (66.7%) of 15 patients with resistant HTN and 1 (50.0%) of 2 patients with controlled HTN, p = 0.012;
- Moxonidine in 52 (88.1%) of 59 patients on centrally acting agents: 40 (85.1%) of 47 patients with resistant HTN and 12 (100.0%) of 12 patients with controlled HTN, p <0.001.
Regarding the number of antihypertensive classes participants in our study had been prescribed, the median was 3 (IQR 2-4): 3 (IQR 3-4.5) in patients with resistant HTN and 2 (IQR 2-3) in patients with controlled HTN, p <0.001.
The median of the number of antihypertensive tablets patients from our study took daily was 3 (IQR 1-5): 4 (IQR 3-6) in patients with resistant HTN and 1.5 (IQR 1-3) in patients with controlled HTN, p <0.001.
The median of all tablets the patients from our study took (for HTN and concomitant diseases) was 4 (IQR 2-8): 6 (IQR 4-10) in patients with resistant HTN and 2 (IQR 1-4.5) in patients with controlled HTN, p <0.001. There was not statistically significant difference between males and females regarding the median of the number of antihypertensive classes, number of antihypertensive tablets and the number of all tablets taken daily.
Single-pill combinations including 2 to 3 antihypertensive classes were used by 145 (56.6%): 64 (50.0%) of patients with resistant HTN and 81 (63.3%) of patients with controlled HTN, p = 0.002. Figure 5 shows the percentage of patients with resistant versus controlled HTN treated with double SPCs and a triple SPCs.
We analyzed also the prescription rate of some other classes of drugs, frequently used by HTN patients for concomitant diseases/conditions:
- Oral anticoagulants – in 34 (13.3%) of 256 patients (mostly direct oral anticoagulants - 33 of 256, 12.9%): 21 (16.4%) of patients with resistant and 13 (10.2%) with controlled HTN, p = 0.250;
- Antiplatelet drugs – in 20 (7.9%) of 256 patients: 12 (9.4%) with resistant HTN and 8 (6.3%) with controlled HTN, p = 0.381;
- Lipid-lowering drugs – in 68 (26.6%) of 256 patients (mostly a statin - 61 of 256, 23.8%): 41 (32.0%) with resistant and 27 (21.1%) with controlled HTN, p = 0.045;
- Sodium-glucose cotransporter-2 (SGLT2) inhibitors – in 17 (6.6%) of 256 patients: 8 (6.2%) of patients with resistant and 9 (7.0%) with controlled HTN, p = 0.761.
The therapeutic decision for patients with resistant HTN in our study was optimization of the pharmacological treatment in 110 (85.9%) of 128, of them 58 (92.1%) males and 52 (80.0%) females. Interventional treatment was indicated to 18 (14.1%) of 128: 5 (7.9%) males and 13 (20.0%) females, p = 0.011. It included renal artery revascularization because of a significant stenosis in 10 (7.8%) and renal denervation in 8 (6.3) of 128 resistant HTN patients in whom further pharmacological optimization was not possible for any reason.
3.5. Impact of Concomitant Risk Factors/Diseases and Drug Treatment on HTN Control
Table 5 shows the variables (demographic factors, concomitant clinical conditions/diseases, treatment) with strongest association with resistant HTN in our study. We found significant positive association of resistant HTN with CKD, advanced stage of HTN, obesity/overweight, concomitant IHD and type 2 DM, and active smoking, while gender, age, dyslipidemia, cerebrovascular disease, PAD, AF, HF and other analyzed factors did not exert significant influence on the odds ratio for resistant HTN. Treatment with single-pill combinations and certain classes of drugs were associated with higher likelihood for controlled HTN.
4. Discussion
In our study patients with resistant HTN were 3.4% of all hypertensive patients – prevalence that is slightly lower, but generally comparable to published data by other authors [2,14,15]. According to the 2018 ESC/ESH and 2023 ESH Guidelines patients with true resistant HTN are ~5% of all patients with high BP [1,2]. The percentage of resistant HTN patients in our study and other studies on this topic may not seem so significant at first glance, but having in mind the number of all hypertensive patients worldwide – approximately 1.28 billion adults aged 30–79 years, it means >43 million people with HTN resistant to treatment, constantly exposed to high and very high cardiovascular risk.
What is important to be discussed is that the definition of resistant HTN adopted by many guidelines is based on maintenance of office BP values ≥140/90 mmHg after appropriate lifestyle measures have been taken by the patients and they are treated with optimal or best tolerated doses of at least three drugs (a thiazide/thiazide-like diuretic, a RAAS blocker and a CCB) [1,2,4,5]. However, the proposed cut-off BP values are discrepant to the target BP values which are <130/80 mm Hg for many hypertensive patients [1,2,12]. For this reason, some authors suggest lower office BP values (<130/80 mmHg) for the definition of resistant HTN or values dependent on the target BP for the corresponding HTN population, which we completely agree with [6,16,17,18]. 2017 American Heart Association/American College of Cardiology taskforce defined resistant hypertension as uncontrolled BP ≥130/80 mm Hg while on optimal doses of at least three antihypertensives with one being a diuretic [18]. This amendment of the criteria for resistant HTN may increase considerably percentage of patients with true resistant HTN [3,6,16,18]. On the other hand, prevalence will be lower if patients with normal out-of-office BP values are excluded from statistics: data from meta-analyses show that the percentage of patients that could be removed for this reason may vary from 14% to 37% [3,6,18].
When discussing our results, we actually prefer to talk about “resistant HTN” instead of “true resistant HTN”, although we have practically applied ESC/ESH criteria for the latter [1,2]. To our opinion, this approach is more applicable for studies conducted in real clinical settings and also more important from clinical point of view. Definition of true resistant HTN requires exclusion of secondary (symptomatic) HTN due to a concomitant disease/condition [1,2,4]. As seen from our results the majority of our patients with uncontrolled HTN have concomitant conditions/diseases, whose influence on BP cannot be ruled out, i.e. patients with HTN uncontrolled by ≥3 drugs who do not have any concomitant conditions, that may interfere with BP control are just a few. And even for them it is impossible to perform all possible laboratory and instrumental investigations that exist to completely exclude a symptomatic component of HTN (secondary HTN). As recommended by most guidelines on HTN, laboratory and instrumental investigations for detection of secondary HTN are justified only in the presence certain clinical features and/or pathological findings from routine investigations [1,2,4,18]. The problem is that absence of characteristic symptoms and signs of a secondary HTN does not exclude secondary HTN at all [2,3,15,16].
In our study CKD was the strongest predictor of resistant HTN: ~60% of patients with resistant HTN had CKD and chronic kidney dysfunction increased ~6.6-fold the odds ratio for difficult-to-control HTN. According to other authors ~60-80% of patients with a kidney disease have high BP and CKD increases 2-3 the likelihood for resistant HTN [2,3,5,19]. It is important to mention, that kidneys diseases are a very heterogeneous group of pathologies, not all of them related to BP elevation and progression to CKD [3,5,13,19]. In addition, many hypertensive patients have high BP preceding development of CKD for years as the scenario was for many of our CKD patients (data from the medical documentation) [3,5,20]. Occurrence of CKD frequently deteriorates BP control, sometimes to the level of resistant HTN, but according to us it does not classify these patients as cases of secondary HTN [2,3,5,18]. For this reason, we regarded patients with CKD and uncontrolled HTN in our study as “resistant HTN patients”, but not “secondary HTN patients”, which should exclude many of them from the analysis.
Other factors in our patient’s population strongly associated with resistant HTN were overweight/obesity, insulin resistance/type 2 diabetes, increasing the odds ratio for uncontrolled HTN ~2.6, 2.1 and 1.9-fold respectively. According to other authors diabetes increases the likelihood for resistant HTN ~ 2-fold and obesity - 2 to 4.5-fold [3,5,21,22,23]. For smoking most publications we found mentioned only that it more common among patients with resistant HTN, but no details about the level of association was presented [2,18,22,24] . These concomitant pathologies must be taken into consideration, when planning therapeutic strategy because they are very common among patients with high BP. Interestingly, despite there is strong evidence that obesity and smoking are involved in BP elevation, these conditions/diseases are usually not regarded as etiologies for “secondary HTN” in contrast to kidney diseases [1,2,3,4].
Other conditions strongly associated in our study with development of resistant HTN were IHD, stage II and stage III HTN. In the study of Smith et al. 38% of patients with coronary artery disease had resistant HTN [25]. In addition, these patients had much worse cardiovascular outcomes compared to patients with IHD with controlled HTN [25]. According to us, the very IHD and drugs used for it are unlikely to cause directly resistance to HTN treatment. The link between these 2 diseases is probably increased activity of renin-angiotensin-aldosterone and sympathetic nervous system, causing vasoconstriction, increased arterial resistance, endothelial damage and vascular remodeling [6,9,10,11,26,27]. These processes are involved not only in the mechanisms of development of HTN, but also in coronary atherosclerosis, clinically manifested with IHD [9,11,20,26]. Some of the discussed mechanisms are probably responsible also for the changed circadian BP rhythm and impaired dipping state [5,28,29]. In our study pathological deviations in BP dipping state were significantly more common among patients with resistant (in ~53%) versus controlled HTN (~12%). Other authors (Ingabire et al.) have found a non-dipping pattern of BP in up to 78% of their patients with uncontrolled HTN [30]. High prevalence of non-dipping and reverse dipping we found among our population with resistant HTN is important for 2 main reasons: 1. These conditions are recognized risk factors for major adverse cardiac events; 2. They require careful elaboration of antihypertensive strategy (choice of antihypertensive classes, preference of drugs with high through-to-peak ratio, regiment for drug intake, etc.).
Regarding higher prevalence of HMOD (II and III stage of HTN) in resistant HTN and strong association between these conditions we found in our study, it is logical and could be explained by the harmful effect of high BP on the heart and arteries (cardiovascular remodeling), the kidneys, brain and the eyes - target organs for high BP [3,5].
We did not find statistically significant sex difference between resistant and controlled HTN patients (percentage of males and females patients was comparable within the very groups too). Most of the other publications we came upon during literature search showed similar prevalence of resistant HTN among males and females, however there were a few in which resistant HTN was more prevalent among males [14,28,31,32,33]. Our patients with resistant HTN were younger compared to patients with controlled HTN, although we expected the opposite. Aging of vessels with loss of elastic fibers is resulting in stiffening of the arterial wall which is considered one of the main pathogenic mechanisms for development of high BP (particularly for the SBP) [5,20,28]. Correlation and regression analyses we conducted did not show statistically significant association of resistant HTN with age. Aging matters for increased incidence of HTN, but other factors/mechanisms probably have more important role for resistance of HTN to treatment. Most of the other publications we found showed increased incidence and prevalence of resistant to treatment HTN with aging, however these studies were mostly outpatient [14,22,28,32,34]. We admit that some important factors for HTN control (such as patient’s adherence to therapy, concomitant medications, physician’s inertia to treatment optimization, etc.) could be expressed at different level in in-hospital and outpatient conditions.
Regarding treatment, we found that the majority of our patients were on guidelines-recommended first-line treatment: ~88% were on a RAAS inhibitor (ARB in 57.4% and ACEi in 30.5%), ~71% on CCB and ~72% on a diuretic (~1/2 of them on a thiazide/thiazide-like diuretic). Our results differ to some extent from the results of one of the largest clinical studies that have been recently published in the same field - the HYPEDIA study [35]. It evaluated the implementation of the 2018 European guidelines for treating hypertension in 3122 patients (mean age 64 ± 12.5 years) and showed that ARBs were used in 69%, CCBs in 47%, ACEi in 19%, diuretics in 39% and beta-blockers 19% [36]. In our study we included patients from tertiary medical care which may be associated with the difference in the therapeutic approach to patients [2,17,28,35].
Our subgroup analysis showed that percentage of patients with resistant HTN on ARB, CCB and diuretics was significantly higher compared to controlled HTN, but it could be explained by the necessity of more drugs from different classes to achieve BP control: the median of number of tablets used by patients with uncontrolled HTN was the median was 3 (IQR 3-4.5) compared to 2 (IQR 2-3) in patients with controlled HTN, p <0.001. ACEi were more prescribed to patients with controlled HTN, but difference with resistant HTN group was not statistically significant. We did not find objective results from other studies performed in real clinical settings about the prescription rate of different antihypertensive classes to patient with resistant HTN which we could compare to our data.
What was also important from our results was the less usage of SPCs by patients with resistant HTN (~57%) compared to those with controlled HTN. It could be at least partially related to insufficient HTN control in the first group according to us. Free combinations are characterized by worse compliance and persistence to therapy (particularly in chronic diseases) which could compromise the effect of any drug [36,37,38]. On the other hand, SPCs improve significantly adherence and the rate of achieving target BP values [2,36,37]. According to 2023 ESH Guidelines on HTN double combinations are expected to achieve sufficient BP control in ~60%, and triple SPC – in ~90% of all hypertensive patients [2]. Our results showed that patients treated with SPCs had 42% lower odds for resistant HTN compared to patients on free combinations after statistical adjustment for other influencing factors. We did not find clinical data from other studies showing exact numbers by which SPCs reduce the risk/OR for development of HTN or/and improve control of BP in patients with resistant HTN compared to free combinations, however most publications on this topic agree that SPCs improve significantly BP control.
The therapeutic approach to the majority of our patients (~86%) was optimization of the drug treatment. Detailed analysis of our data outlined the following possibilities to achieve better BP control in resistant HTN:
1. Increased prescription rate of SPCs: a guidelines-based double SPC as initial therapy;
2. Early addition of a third component to the SPC (a triple SPC) if target BP has not been achieved within 2-4 weeks: therapeutic inertia should be avoided.
3. Drugs in the combination should be at standard doses that could be increased in a step-wise approach to maximal doses, particularly the thiazide/thiazide like diuretics, RAAS inhibitors and CCBs;
4. Long-acting representatives of each classes with highest trough-to-peak ratio should be used;
5. If a combination with an ACEi in optimal doses and duration of treatment fails to achieve target BP values within a reasonable period of time or if it has stopped working, the ACEi should be replaced by an ARB. Development of tachyphylaxis with ACEi is not uncommon (up to 30% according to some data) [39]. Results from the largest clinical trial comparing an ARB (telmisartan) to ACEi (ramipril) – ONTARGET also supports switch from an ACEi to an ARB in patients with insufficient BP control from the first class, particularly in high-risk patients [40].
6. In patients who have not achieved BP target values by a triple combination with a RAAS inhibitor, CCB and a thiazide/thiazide-like diuretic at standard/maximally tolerated doses within 4 weeks of treatment, a second-line drug must be added to therapy: preferably a MRA or a beta-blocker (preferably bisoprolol) or an α-1 receptor blocker (preferably doxazosin) or a centrally acting agent or a combination of them in lower or standard doses. Thiazide/thiazide-like diuretics could be switched to a loop diuretic (preferably torasemide), particularly if eGFR is <45 ml/min/1.73m2. Current ESC/ESH Guidelines on HTN recommend a MRA (spironolactone or eplerenone) to be added to the therapy of patients who have not achieved BP control by first-line drugs [1,2]. These recommendations came after results from PATHWAY-2 clinical trial were published [27]. They showed that the average reduction in home SBP was greater with spironolactone compared with placebo (-8.70 mm Hg), doxazosin (-4.03 mm Hg), and bisoprolol (-4.48 mm Hg) [27]. In our study only ~16% of resistant HTN had been prescribed a MRA. Oher therapeutic options recommended by the current guidelines - α1-receptor blockers, beta-blockers, centrally acting agents were also underrepresented in the therapy of our patients with resistant HTN. In contrast to PATHWAY-2 our results showed that α1-receptor blockers (most of our patients were on doxazosin) were associated with lower likelihood for resistant HTN compared to MRAs (spironolactone or eplerenone).
7. Renal denervation or novel device-based therapies (carotid baroreceptor stimulation, cardiac neuromodulation therapy, iliac arteriovenous anastomosis, etc.) remain an option for patients with true resistant HTN who have not achieved target BP by the strategies discussed above [2].
8. In all patients with HTN efforts should be made at individual and public levels to increase awareness about the importance of strict adherence to therapy and regular home BP measurements. Any deterioration of BP control, if sustained and not due to obvious temporary causes should urge patients to attend their treating physicians.
In our study >50% of hypertensives were at high or very high cardiovascular risk, particularly patients with resistant HTN (~67%). Epidemiological data published by other authors show variable level cardiovascular risk, dependent on the analyzed hypertensive populations and the concomitant RF/diseases [2,5,14,28]. However, most authors agree that patients with resistant HTN should be regarded as patients at high or very high cardiovascular risk [2,15,28,32]. This should be observed in the holistic therapeutic approach necessitating sufficient control of all concomitant factors/diseases (obesity/overweight, dyslipidemia, DM/IGT, smoking, etc.) [2,3,4,12]. After all, reduction of BP should not be an end in itself, but a part of the global therapeutic strategy, aiming to lower the total cardiovascular risk [2,4,12].
Study Limitations
1. Number of patients included in our study does not allow extrapolation of our results over the entire population of patients with resistant HTN; 2. We analyzed prevalence and influence of some of the most common, but not all factors/diseases that could be associated with development of resistant HTN; 3. Results and analysis represent just a momentary “snapshot” of the situation because we conducted a retrospective, cross-sectional study - the results after treatment optimization were not available for analysis.
5. Conclusions
Patients with resistant HTN represented a relatively small proportion of all hypertensives in our study, but they were characterized by high or very high cardiovascular risk. Factors with strongest association with resistant HTN were CKD, Stage II and III HTN, obesity/overweight, IHD, Type 2 DM and active smoking, whereas treatment with SPCs, α-1 receptor blockers, centrally acting agents and MRA were associated with lower likelihood for uncontrolled BP. The therapeutic strategy to patients with resistant HTN should be holistic, aiming to achieve control not only of HTN but also of all concomitant RF/diseases because the ultimate goal is reduction of the total cardiovascular risk.
Author Contributions
Conceptualization, S.N.; Methodology, S.N., E.M. and N.R.; Validation, S.N. and N.R.; Formal analysis, S.N. and E.M.; Investigation, S.N. and N.R.; Resources, S.N. and E.M.; Data curation, S.N. and N.R; Writing—original draft preparation – S.N.; Writing— S.N., E.M. and N.R.; Visualization, S.N. and E.M; Supervision, N.R.; Project administration, S.N.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. Approval by an Institutional Review Board or Ethics Committee is not required in Bulgaria for this type of research (observational, retrospective, non-interventional study). Our study was registered at https://www.clinicaltrials.gov/ on 7th of February, 2024 with reference number KPVB0001RH.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data supporting reported results is available and can be provided by Stefan Naydenov, MD, PhD; email: snaydenov@gmail.com.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D. L.; Coca, A.; De Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the Management of Arterial Hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Cardiology and the European Society of Hypertension. Journal of Hypertension 2018, 36, 1953–2041. [Google Scholar] [CrossRef] [PubMed]
- Mancia, G.; Kreutz, R.; Brunström, M.; Burnier, M.; Grassi, G.; Januszewicz, A.; Muiesan, M. L.; Tsioufis, K.; Agabiti-Rosei, E.; Algharably, E. A. E.; et al. 2023 ESH Guidelines for the Management of Arterial Hypertension The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension: Endorsed by the International Society of Hypertension (ISH) and the European Renal Association (ERA). Journal of Hypertension 2023, 41, 1874–2071. [Google Scholar] [CrossRef] [PubMed]
- Parasher, A.; Jhamb, R. Resistant Hypertension: A Review. Int J Adv Med 2021, 8(9), 1433. [Google Scholar] [CrossRef]
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N. A.; Poulter, N. R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G. S.; Tomaszewski, M.; et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension 2020, 75, 1334–1357. [Google Scholar] [CrossRef] [PubMed]
- Hypertension, Third edition. ; Nadar, S., Lip, G. Y. H., Eds.; Oxford cardiology library; Oxford University Press: Oxford, United Kingdom ; New York, NY, 2023. [Google Scholar]
- Matanes, F.; Khan, M. B.; Siddiqui, M.; Dudenbostel, T.; Calhoun, D.; Oparil, S. An Update on Refractory Hypertension. Curr Hypertens Rep 2022, 24, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Mendes, M.; Dubourg, J.; Blanchard, A.; Bergerot, D.; Courand, P.-Y.; Forni, V.; Frank, M.; Bobrie, G.; Menard, J.; Azizi, M. Copeptin Is Increased in Resistant Hypertension. Journal of Hypertension 2016, 34, 2458–2464. [Google Scholar] [CrossRef] [PubMed]
- Calhoun, D. A. Hyperaldosteronism as a Common Cause of Resistant Hypertension. Annu. Rev. Med. 2013, 64, 233–247. [Google Scholar] [CrossRef] [PubMed]
- Grassi, G.; Seravalle, G.; Brambilla, G.; Pini, C.; Alimento, M.; Facchetti, R.; Spaziani, D.; Cuspidi, C.; Mancia, G. Marked Sympathetic Activation and Baroreflex Dysfunction in True Resistant Hypertension. International Journal of Cardiology 2014, 177, 1020–1025. [Google Scholar] [CrossRef] [PubMed]
- Velasco, A.; Siddiqui, M.; Kreps, E.; Kolakalapudi, P.; Dudenbostel, T.; Arora, G.; Judd, E. K.; Prabhu, S. D.; Lloyd, S. G.; Oparil, S.; Calhoun, D. A. Refractory Hypertension Is Not Attributable to Intravascular Fluid Retention as Determined by Intracardiac Volumes. Hypertension 2018, 72, 343–349. [Google Scholar] [CrossRef]
- Dudenbostel, T.; Acelajado, M. C.; Pisoni, R.; Li, P.; Oparil, S.; Calhoun, D. A. Refractory Hypertension: Evidence of Heightened Sympathetic Activity as a Cause of Antihypertensive Treatment Failure. Hypertension 2015, 66, 126–133. [Google Scholar] [CrossRef]
- Visseren, F. L. J.; Mach, F.; Smulders, Y. M.; Carballo, D.; Koskinas, K. C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on Cardiovascular Disease Prevention in Clinical Practice. European Heart Journal 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Charles, K.; Lewis, M. J.; Montgomery, E.; Reid, M. The 2021 Chronic Kidney Disease Epidemiology Collaboration Race-Free Estimated Glomerular Filtration Rate Equations in Kidney Disease: Leading the Way in Ending Disparities. Health Equity 2024, 8, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Noubiap, J. J.; Nansseu, J. R.; Nyaga, U. F.; Sime, P. S.; Francis, I.; Bigna, J. J. Global Prevalence of Resistant Hypertension: A Meta-Analysis of Data from 3.2 Million Patients. Heart 2019, 105, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Sinnott, S.-J.; Smeeth, L.; Williamson, E.; Douglas, I. J. Trends for Prevalence and Incidence of Resistant Hypertension: Population Based Cohort Study in the UK 1995-2015. BMJ 2017, j3984. [Google Scholar] [CrossRef] [PubMed]
- Koracevic, G.; Micic, S.; Stojanovic, M.; Zdravkovic, M. A Need for Improvement in the Definition of Resistant Arterial Hypertension. Medicina 2023, 59(4), 803. [Google Scholar] [CrossRef] [PubMed]
- Banga, S.; Mungee, S.; Patel, A. R.; Singh, S.; Kizhakekuttu, T. J. Management of Resistant Hypertension Based on Recommendations from Different Guidelines and the Systolic Blood Pressure Intervention Trial. Cureus 2019. [Google Scholar] [CrossRef] [PubMed]
- Carey, R. M.; Calhoun, D. A.; Bakris, G. L.; Brook, R. D.; Daugherty, S. L.; Dennison-Himmelfarb, C. R.; Egan, B. M.; Flack, J. M.; Gidding, S. S.; Judd, E.; et al. Resistant Hypertension: Detection, Evaluation, and Management: A Scientific Statement From the American Heart Association. Hypertension 2018, 72(5). [Google Scholar] [CrossRef]
- Georgianos, P. I.; Agarwal, R. Hypertension in Chronic Kidney Disease (CKD): Diagnosis, Classification, and Therapeutic Targets. American Journal of Hypertension 2021, 34, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Frąk, W.; Wojtasińska, A.; Lisińska, W.; Młynarska, E.; Franczyk, B.; Rysz, J. Pathophysiology of Cardiovascular Diseases: New Insights into Molecular Mechanisms of Atherosclerosis, Arterial Hypertension, and Coronary Artery Disease. Biomedicines 2022, 10(8), 1938. [Google Scholar] [CrossRef]
- Weitzman, D.; Chodick, G.; Shalev, V.; Grossman, C.; Grossman, E. Prevalence and Factors Associated With Resistant Hypertension in a Large Health Maintenance Organization in Israel. Hypertension 2014, 64, 501–507. [Google Scholar] [CrossRef]
- Mahapatra, R.; Kaliyappan, A.; Chinnakali, P.; Hanumanthappa, N.; Govindarajalou, R.; Bammigatti, C. Prevalence and Risk Factors for Resistant Hypertension: Cross-Sectional Study From a Tertiary Care Referral Hospital in South India. Cureus 2021. [Google Scholar] [CrossRef] [PubMed]
- Ciobanu, D. M.; Kilfiger, H.; Apan, B.; Roman, G.; Veresiu, I. A. RESISTANT HYPERTENSION IN TYPE 2 DIABETES: PREVALENCE AND PATIENT CHARACTERISTICS. Medicine and Pharmacy Reports 2015, 88, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Mohammad, A.; Abujbara, M.; Alshraideh, J.; Jaddou, H.; Ajlouni, K. The Prevalence of Resistant Hypertension Among Type 2 Diabetic Patients Attending the National Center for Diabetes, Endocrinology, and Genetics. J Endocrinol Metab 2017, 7, 153–158. [Google Scholar] [CrossRef]
- Smith, S. M.; Gong, Y.; Handberg, E.; Messerli, F. H.; Bakris, G. L.; Ahmed, A.; Bavry, A. A.; Pepine, C. J.; Cooper-DeHoff, R. M. Predictors and Outcomes of Resistant Hypertension among Patients with Coronary Artery Disease and Hypertension. Journal of Hypertension 2014, 32, 635–643. [Google Scholar] [CrossRef] [PubMed]
- Cai, A.; Calhoun, D. A. Resistant Hypertension: An Update of Experimental and Clinical Findings. Hypertension 2017, 70, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; MacDonald, T. M.; Morant, S.; Webb, D. J.; Sever, P.; McInnes, G.; Ford, I.; Cruickshank, J. K.; Caulfield, M. J.; Salsbury, J.; et al. Spironolactone versus Placebo, Bisoprolol, and Doxazosin to Determine the Optimal Treatment for Drug-Resistant Hypertension (PATHWAY-2): A Randomised, Double-Blind, Crossover Trial. The Lancet 2015, 386, 2059–2068. [Google Scholar] [CrossRef] [PubMed]
- Smith, S. M.; Gurka, M. J.; Winterstein, A. G.; Pepine, C. J.; Cooper-DeHoff, R. M. Incidence, Prevalence, and Predictors of Treatment-resistant Hypertension with Intensive Blood Pressure Lowering. J of Clinical Hypertension 2019, 21, 825–834. [Google Scholar] [CrossRef] [PubMed]
- Bendzala, M.; Kruzliak, P.; Gaspar, L.; Soucek, M.; Mrdovic, I.; Sabaka, P.; Dukat, A.; Gasparova, I.; Malan, L.; Takazawa, K. Prognostic Significance of Dipping in Older Hypertensive Patients. Blood Pressure 2015, 24, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Ingabire, P. M.; Ojji, D. B.; Rayner, B.; Ogola, E.; Damasceno, A.; Jones, E.; Dzudie, A.; Ogah, O. S.; Poulter, N.; Sani, M. U.; et al. High Prevalence of Non-Dipping Patterns among Black Africans with Uncontrolled Hypertension: A Secondary Analysis of the CREOLE Trial. BMC Cardiovasc Disord 2021, 21, 254. [Google Scholar] [CrossRef]
- Joo, H. J.; Yum, Y.; Kim, Y. H.; Son, J.-W.; Kim, S. H.; Choi, S.; Han, S.; Shin, M.-S.; Jeong, J.-O.; Kim, E. J.; Working Group on Hypertension Complication. Gender Difference of Blood Pressure Control Rate and Clinical Prognosis in Patients With Resistant Hypertension: Real-World Observation Study. J Korean Med Sci 2023, 38, e124. [Google Scholar] [CrossRef]
- Daugherty, S. L.; Powers, J. D.; Magid, D. J.; Tavel, H. M.; Masoudi, F. A.; Margolis, K. L.; O’Connor, P. J.; Selby, J. V.; Ho, P. M. Incidence and Prognosis of Resistant Hypertension in Hypertensive Patients. Circulation 2012, 125, 1635–1642. [Google Scholar] [CrossRef] [PubMed]
- Mosca, L.; Barrett-Connor, E.; Kass Wenger, N. Sex/Gender Differences in Cardiovascular Disease Prevention: What a Difference a Decade Makes. Circulation 2011, 124, 2145–2154. [Google Scholar] [CrossRef]
- Brant, L. C. C.; Passaglia, L. G.; Pinto-Filho, M. M.; De Castilho, F. M.; Ribeiro, A. L. P.; Nascimento, B. R. The Burden of Resistant Hypertension Across the World. Curr Hypertens Rep 2022, 24, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Kollias, A.; Foukarakis, E.; Karakousis, K.; The HYPEDIA Study Group; Adamopoulos, E. ; Afaras, G.; Aggelopoulos, G.; Alexandropoulos, T.; Alexiadis, S.; Alexoudis, A. et al.; Implementation of the 2018 ESC/ESH Guidelines for the Management of Hypertension in Primary Care: The HYPEDIA Study. J Hum Hypertens 2022, 37, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, A.; Drame, K.; Geutjens, S.; Airaksinen, M. Does the Polypill Improve Patient Adherence Compared to Its Individual Formulations? A Systematic Review. Pharmaceutics 2020, 12, 190. [Google Scholar] [CrossRef] [PubMed]
- Tsioufis, K.; Kreutz, R.; Sykara, G.; Van Vugt, J.; Hassan, T. Impact of Single-Pill Combination Therapy on Adherence, Blood Pressure Control, and Clinical Outcomes: A Rapid Evidence Assessment of Recent Literature. Journal of Hypertension 2020, 38, 1016–1028. [Google Scholar] [CrossRef] [PubMed]
- Corrao, G.; Parodi, A.; Zambon, A.; Heiman, F.; Filippi, A.; Cricelli, C.; Merlino, L.; Mancia, G. Reduced Discontinuation of Antihypertensive Treatment by Two-Drug Combination as First Step. Evidence from Daily Life Practice. Journal of Hypertension 2010, 28, 1584–1590. [Google Scholar] [CrossRef] [PubMed]
- Izzo Jr, J. L.; Weir, M. R. Angiotensin-Converting Enzyme Inhibitors: Angiotensin-Converting Enzyme Inhibitors. The Journal of Clinical Hypertension 2011, 13, 667–675. [Google Scholar] [CrossRef]
- Telmisartan, Ramipril, or Both in Patients at High Risk for Vascular Events. N Engl J Med 2008, 358, 1547–1559. [CrossRef]
Figure 1.
Screening and selection of participants for our study; ESC - European society of cardiology; ESH – Europeans Society of Hypertension; HTN – arterial hypertension.
Figure 1.
Screening and selection of participants for our study; ESC - European society of cardiology; ESH – Europeans Society of Hypertension; HTN – arterial hypertension.
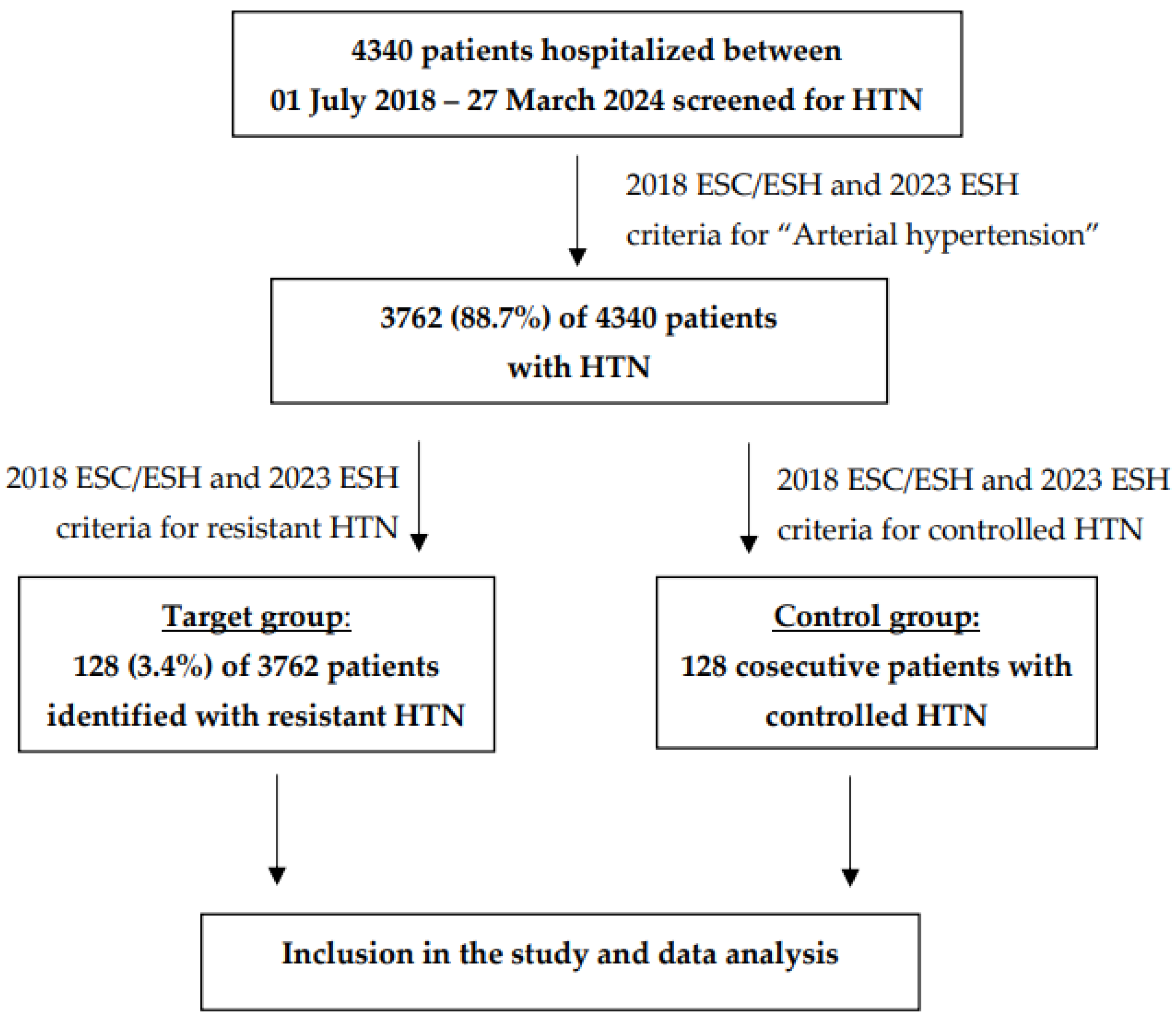
Figure 2.
CKD stage of patients with resistant and controlled HTN according to the equation recommended by the 2021 Guidelines of CKD Epidemiology Collaboration Group [13].
Figure 2.
CKD stage of patients with resistant and controlled HTN according to the equation recommended by the 2021 Guidelines of CKD Epidemiology Collaboration Group [13].
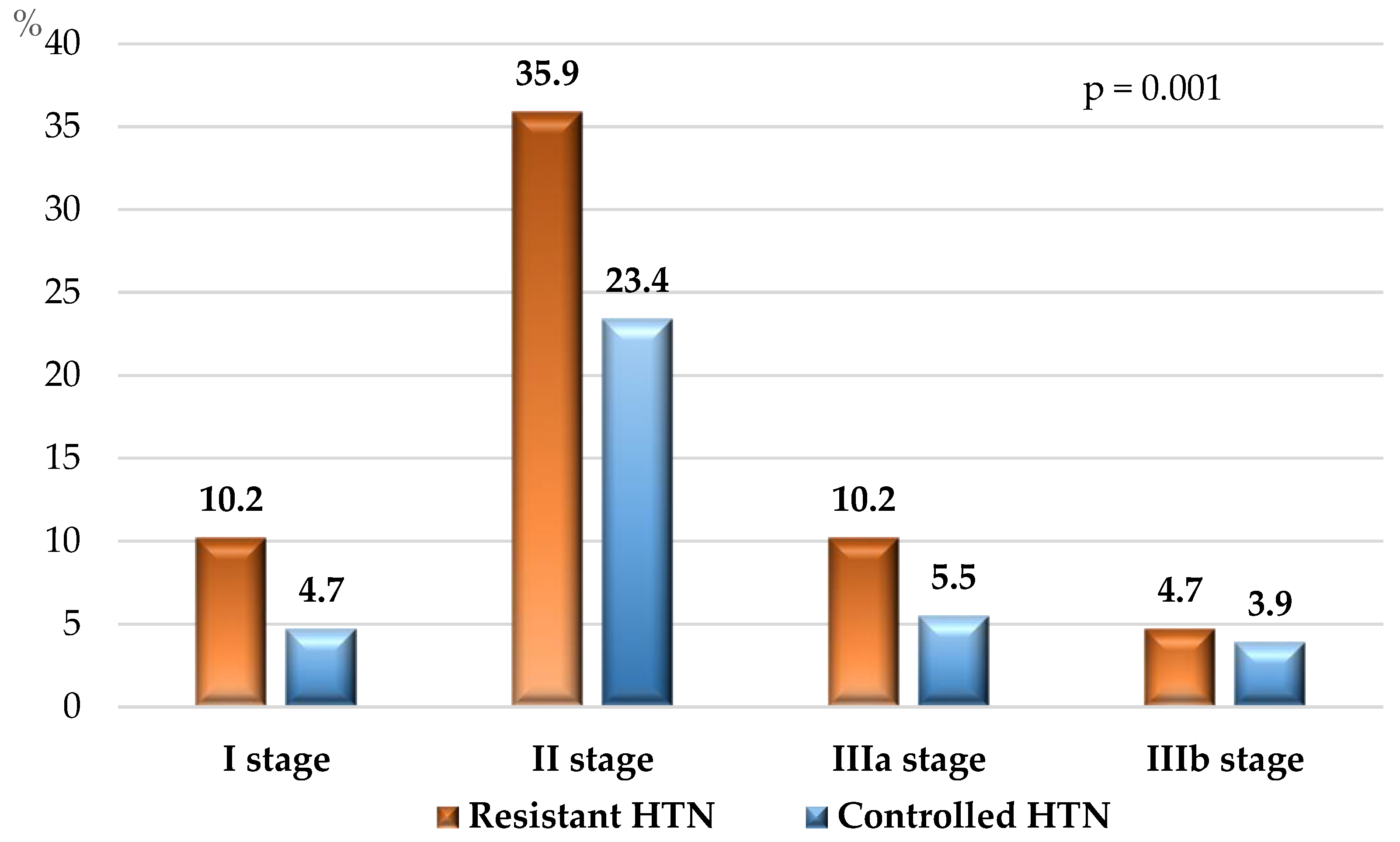
Figure 3.
Dipping state of patients with resistant and controlled HTN. Normal dipping state – 10-20% decrease of the nighttime SBP and DBP to the daytime values; Non-dipping – 1-9% decrease of nighttime SBP and/or DBP compared to the daytime values; Reverse dipping – nighttime SBP and/or DBP increase compared to the daytime values;.
Figure 3.
Dipping state of patients with resistant and controlled HTN. Normal dipping state – 10-20% decrease of the nighttime SBP and DBP to the daytime values; Non-dipping – 1-9% decrease of nighttime SBP and/or DBP compared to the daytime values; Reverse dipping – nighttime SBP and/or DBP increase compared to the daytime values;.
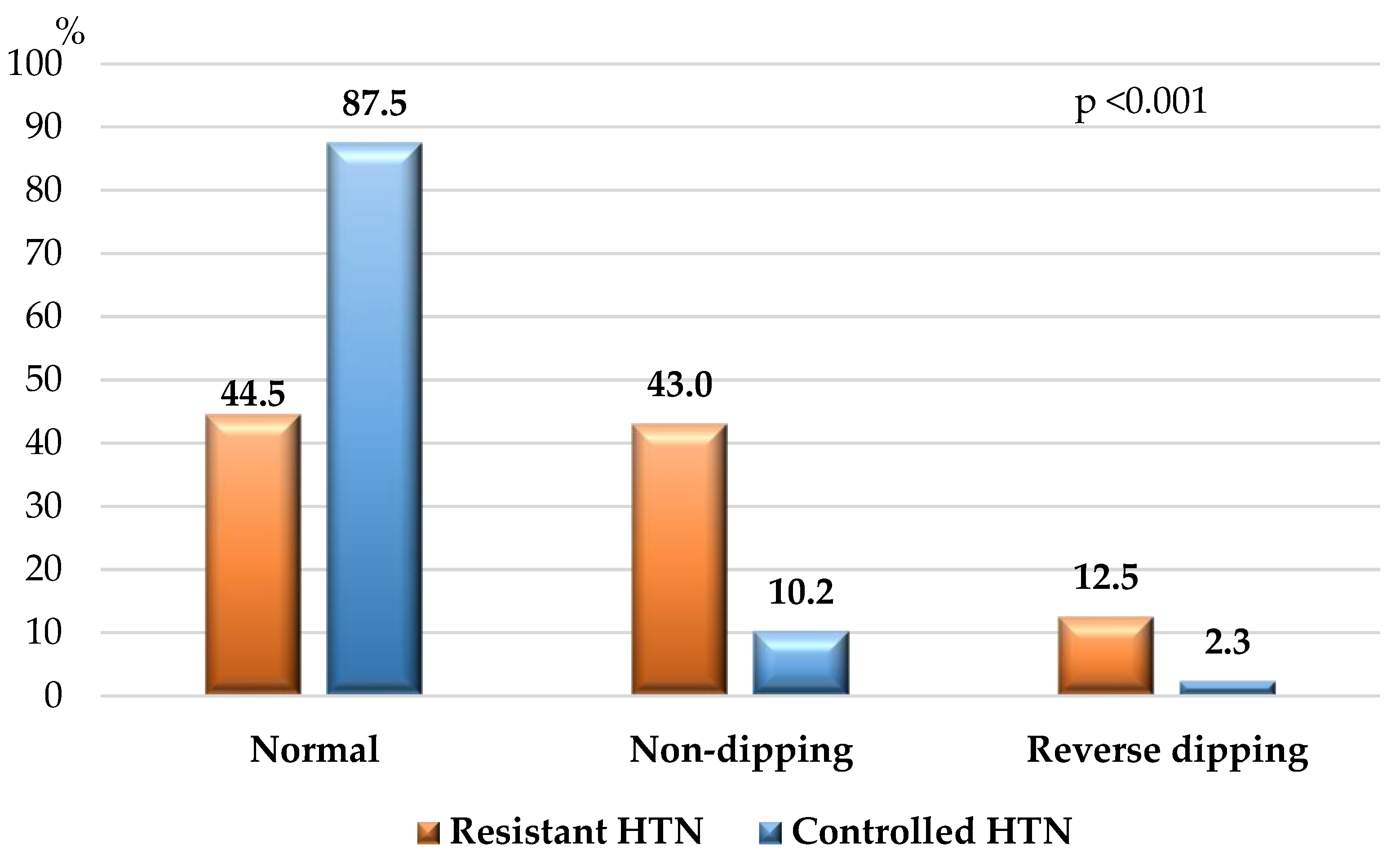
Figure 4.
Cardiovascular risk of the study population. HTN – arterial hypertension.
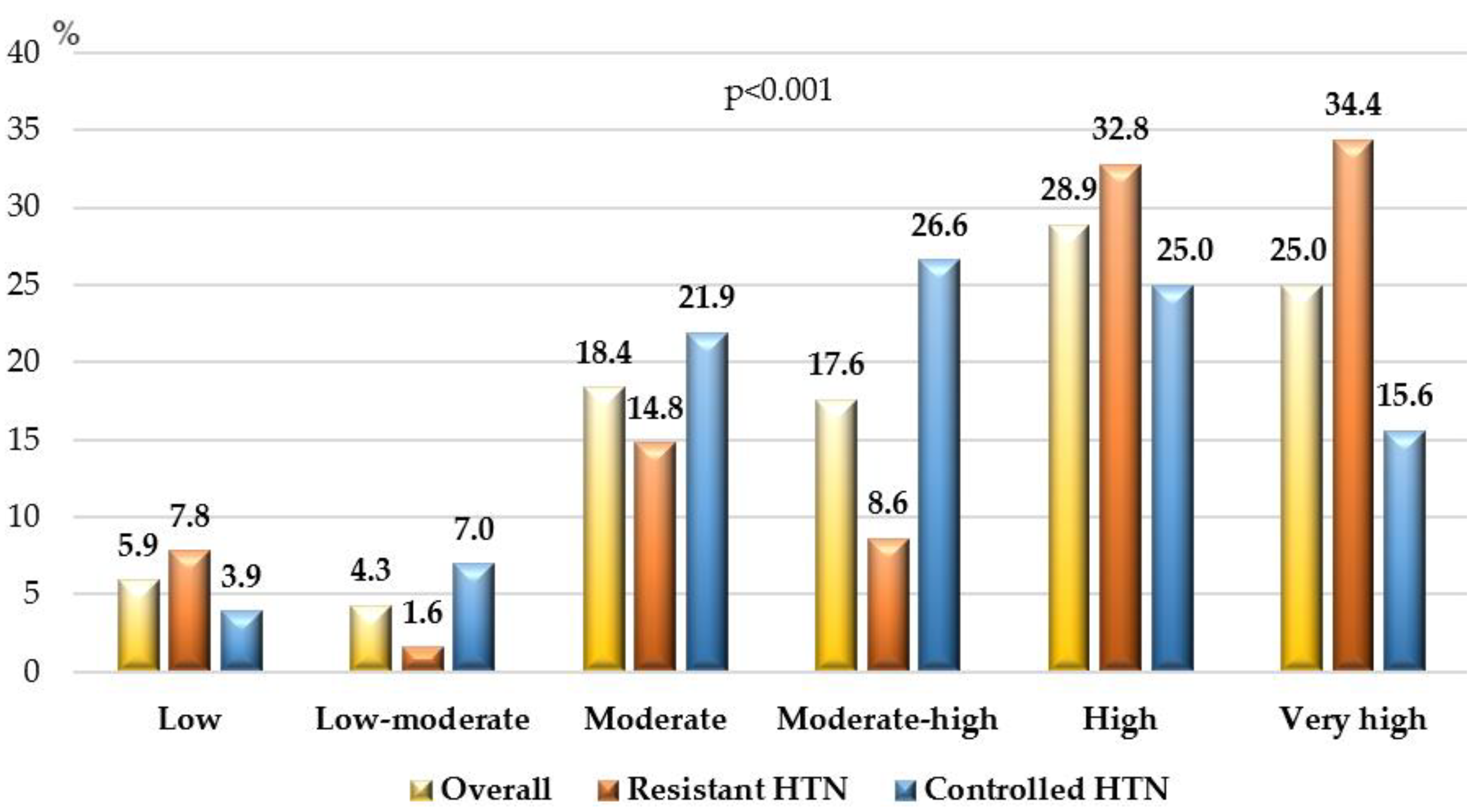
Figure 5.
Treatment with double and triple single-pill combinations. HTN – arterial hypertension; SPC – single-pill combination.
Figure 5.
Treatment with double and triple single-pill combinations. HTN – arterial hypertension; SPC – single-pill combination.
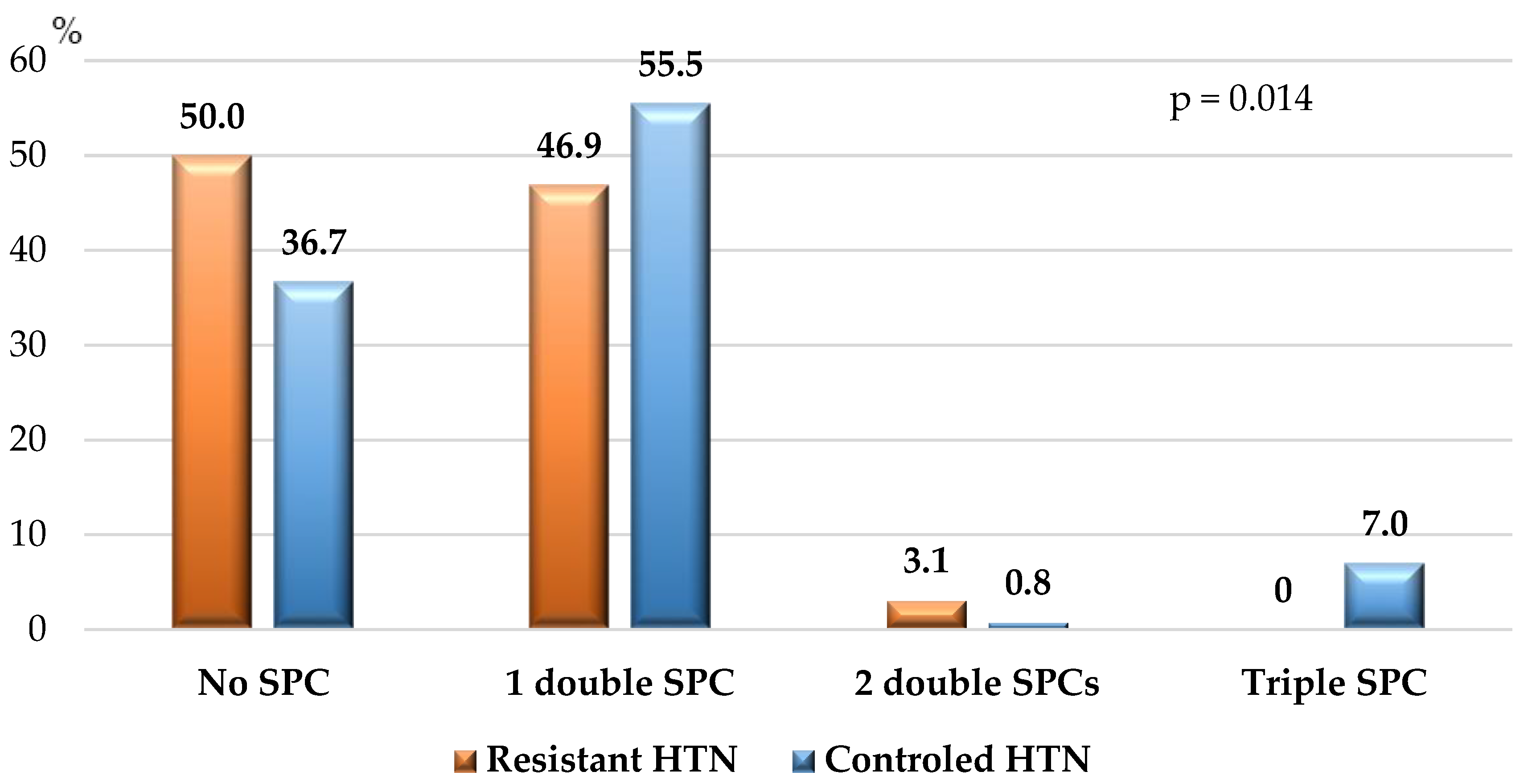

Table 1.
Patient’s characteristics at inclusion in the study.
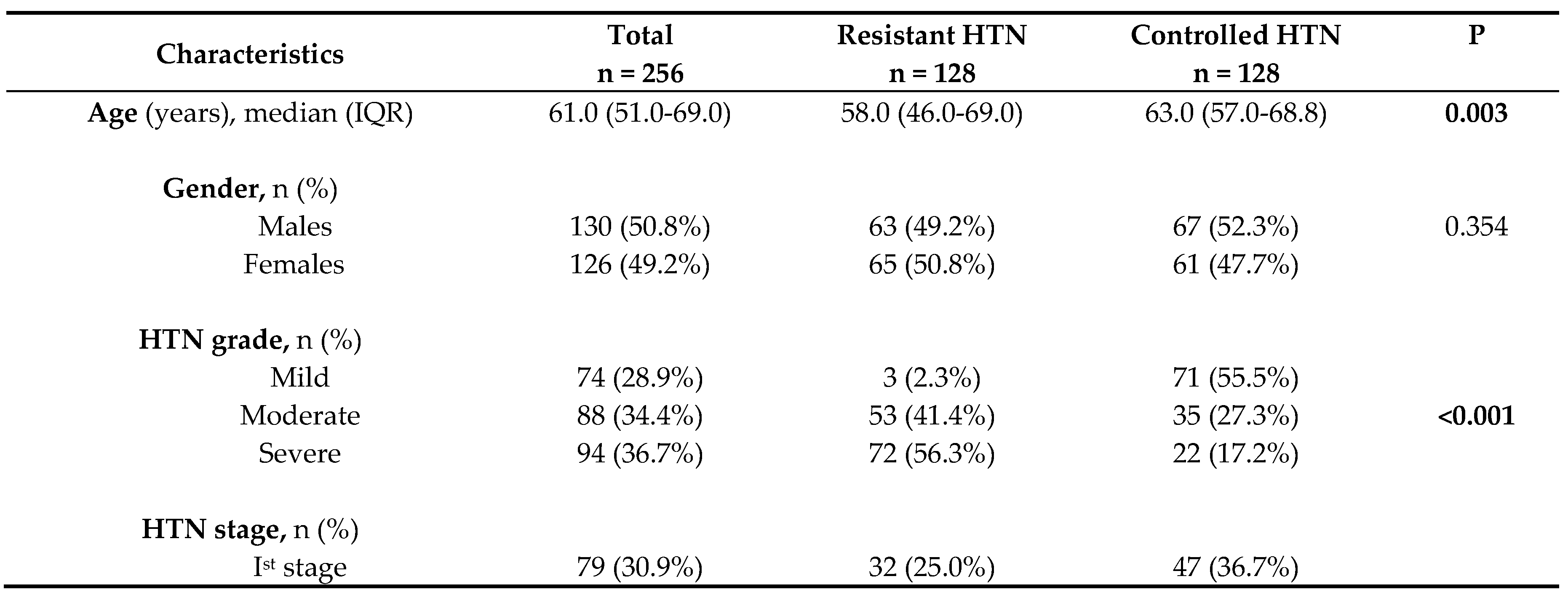
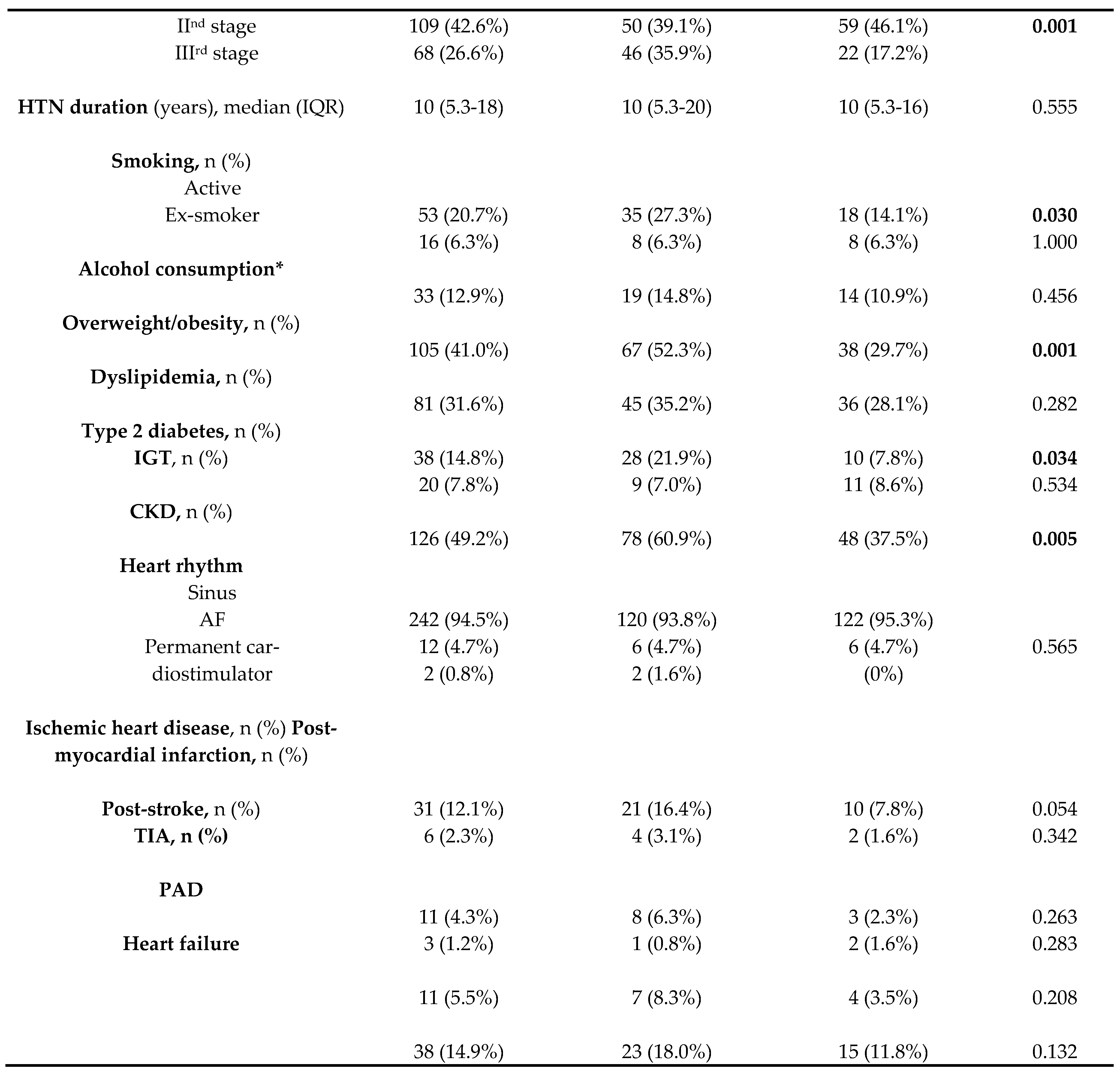
AF – atrial fibrillation; CKD – chronic kidney disease; HTN – arterial hypertension; IGT – impaired glucose tolerance; IQR – interquartile range; Mild HTN - SBP 140-159 and/or DBP 90-99 mmHg; Moderate HTN - SBP 160-179 and/or DBP 100-109 mmHg; Severe HTN - SBP ≥180 and/or DBP ≥180 mmHg; PAD – peripheral arterial disease; TIA – transitory ischemic attack; * ≥14 units per week for males and ≥8 units per unit for females (1 unit = 25 ml of standard alcohol drink with 40.0% alcohol content or 125 ml of wine with 12.0% alcohol content or 250 ml beer with 5.0% alcohol content), p – p-value for statistical significance.
Table 2.
Basic laboratory parameters of the study population.
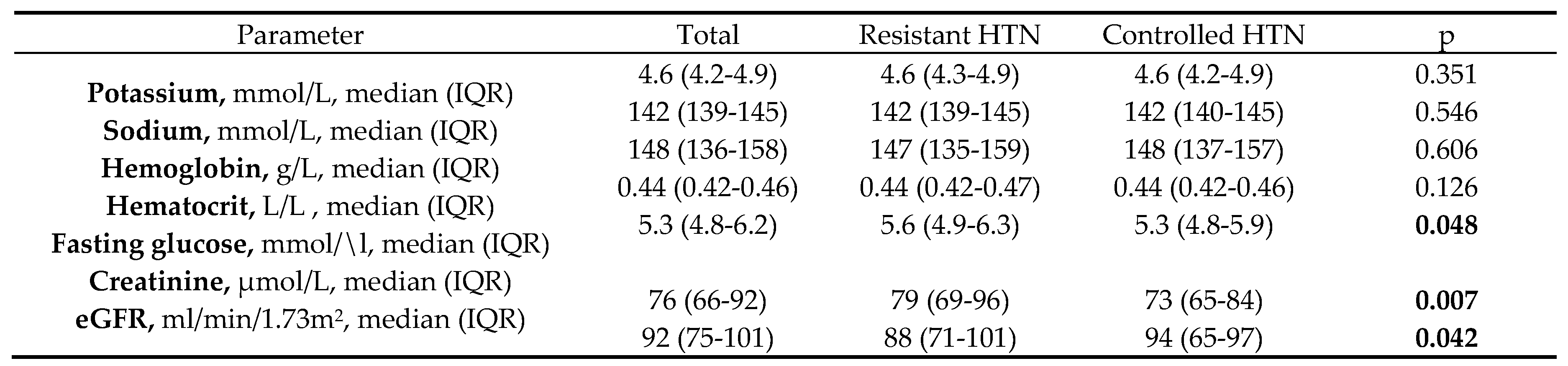
eGFR – estimated glomerular filtration rate (according to the equation recommended by the 2021 Guidelines of CKD Epidemiology Collaboration Group) [13]; IQR – interquartile range .
Table 3.
Office BP measurement, 24-h Holter-BP monitoring and office HR measurement.
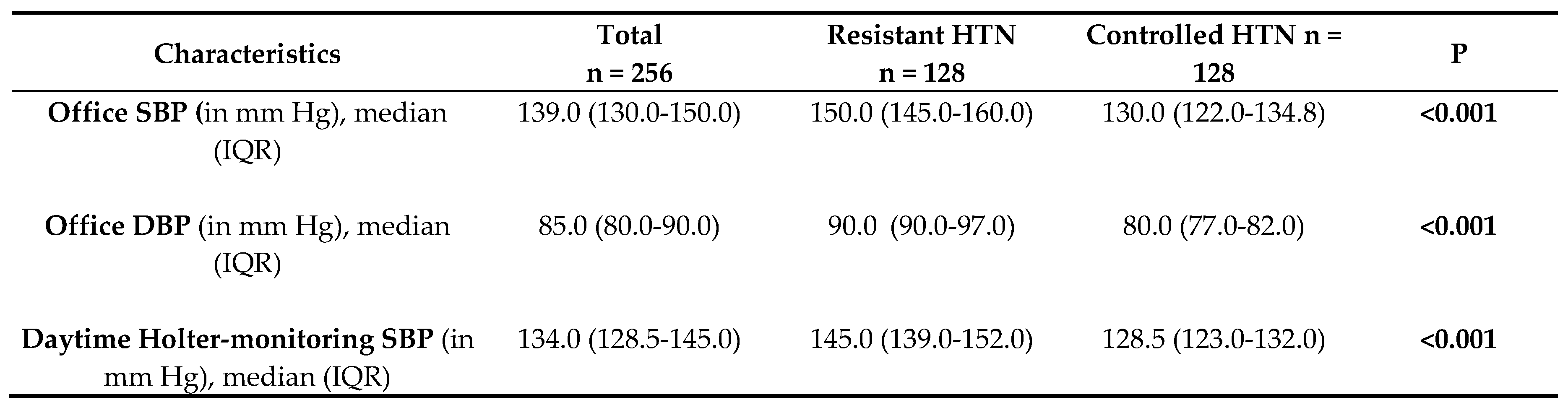
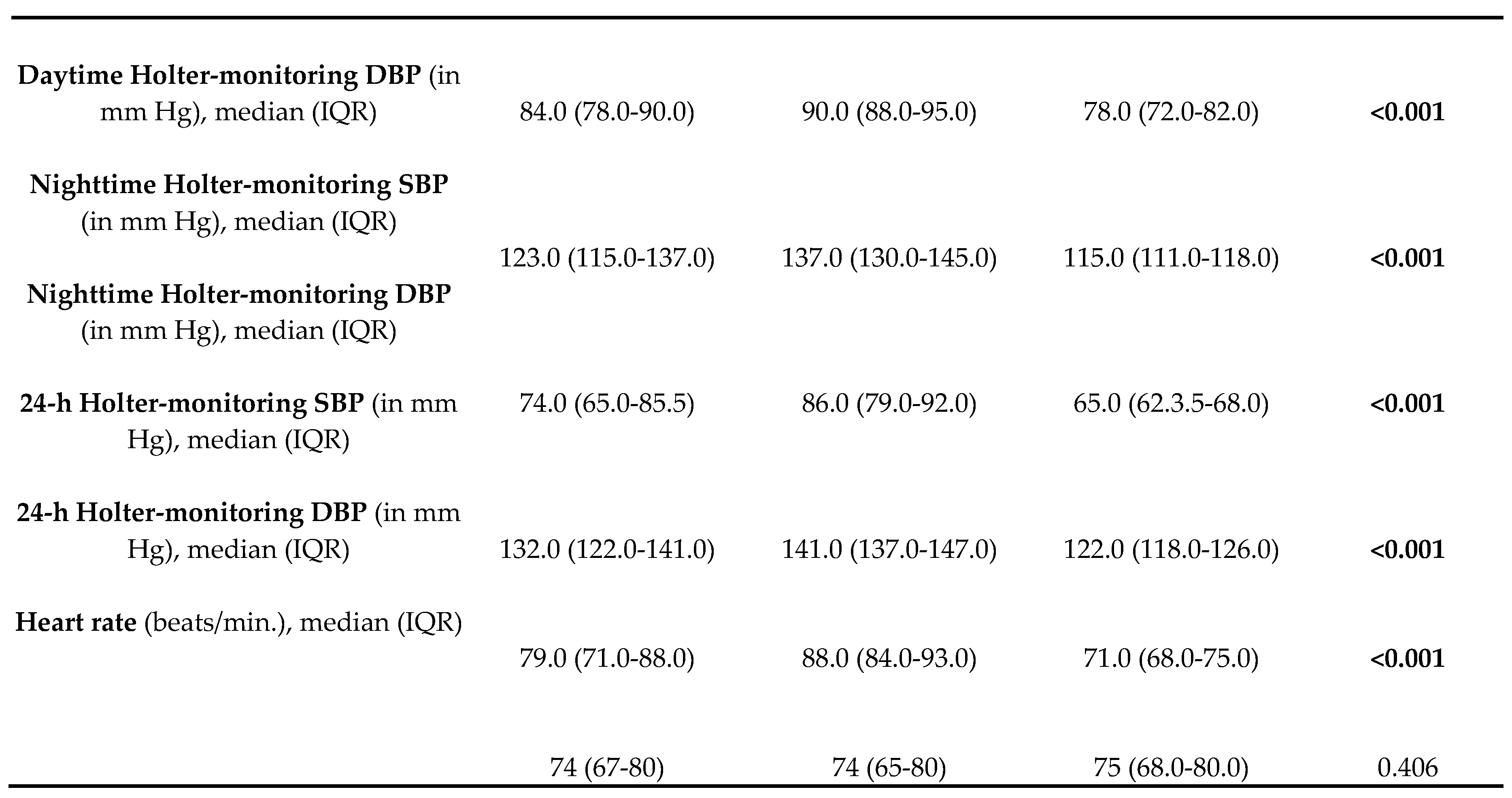
DBP – diastolic blood pressure; HR – heart rate; IQR – interquartile range; SBP – systolic blood pressure.
Table 4.
Antihypertensive classes used by the patients, included in our study.
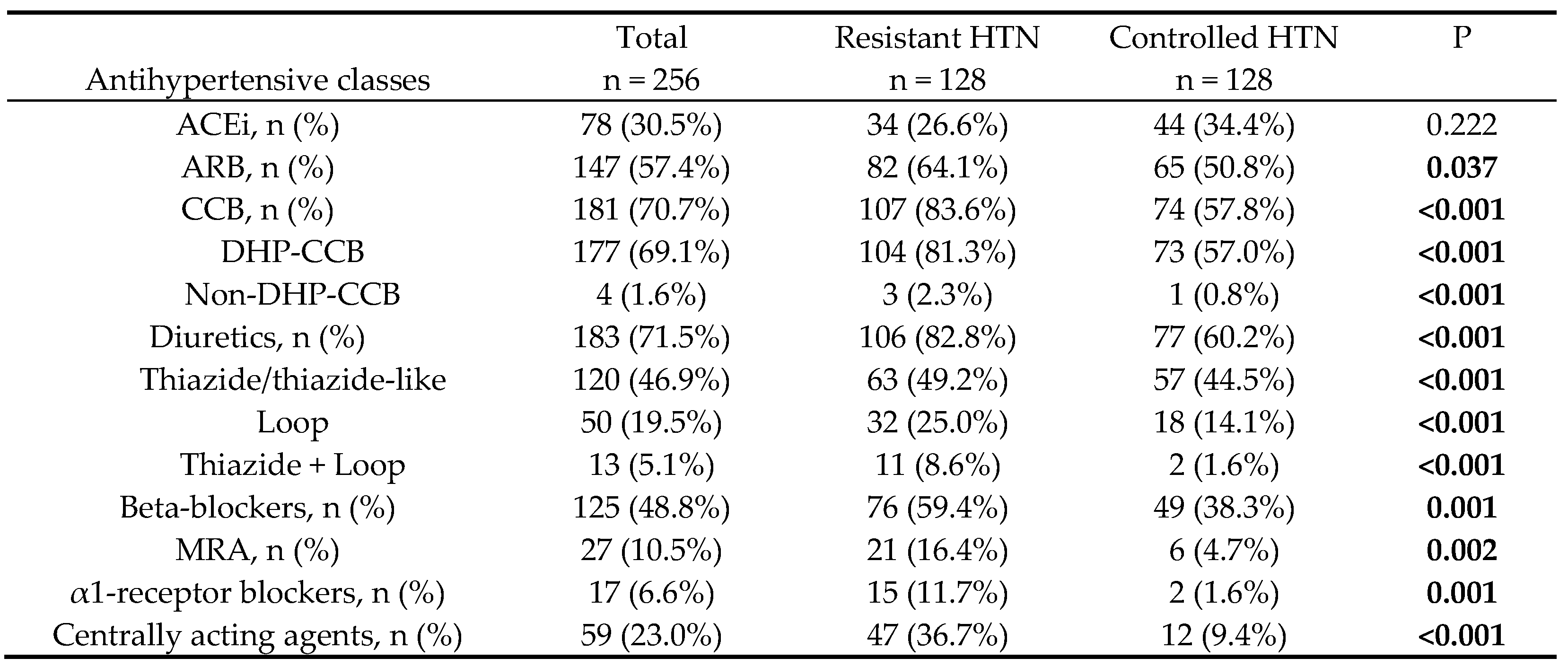
ACEi – Angiotensin- converting enzyme inhibitors; ARB – angiotensin II receptor blockers; CCB - Calcium channel blockers; DHP-CCB – dihydropyridine calcium channel blocker; HTN – arterial hypertension; MRA - mineralocorticoid receptor antagonists; Non-DHP-CCB – non-dihydropyridine calcium channel blocker; p – p-value for statistical significance.
Table 5.
Association of different factors with resistant HTN.
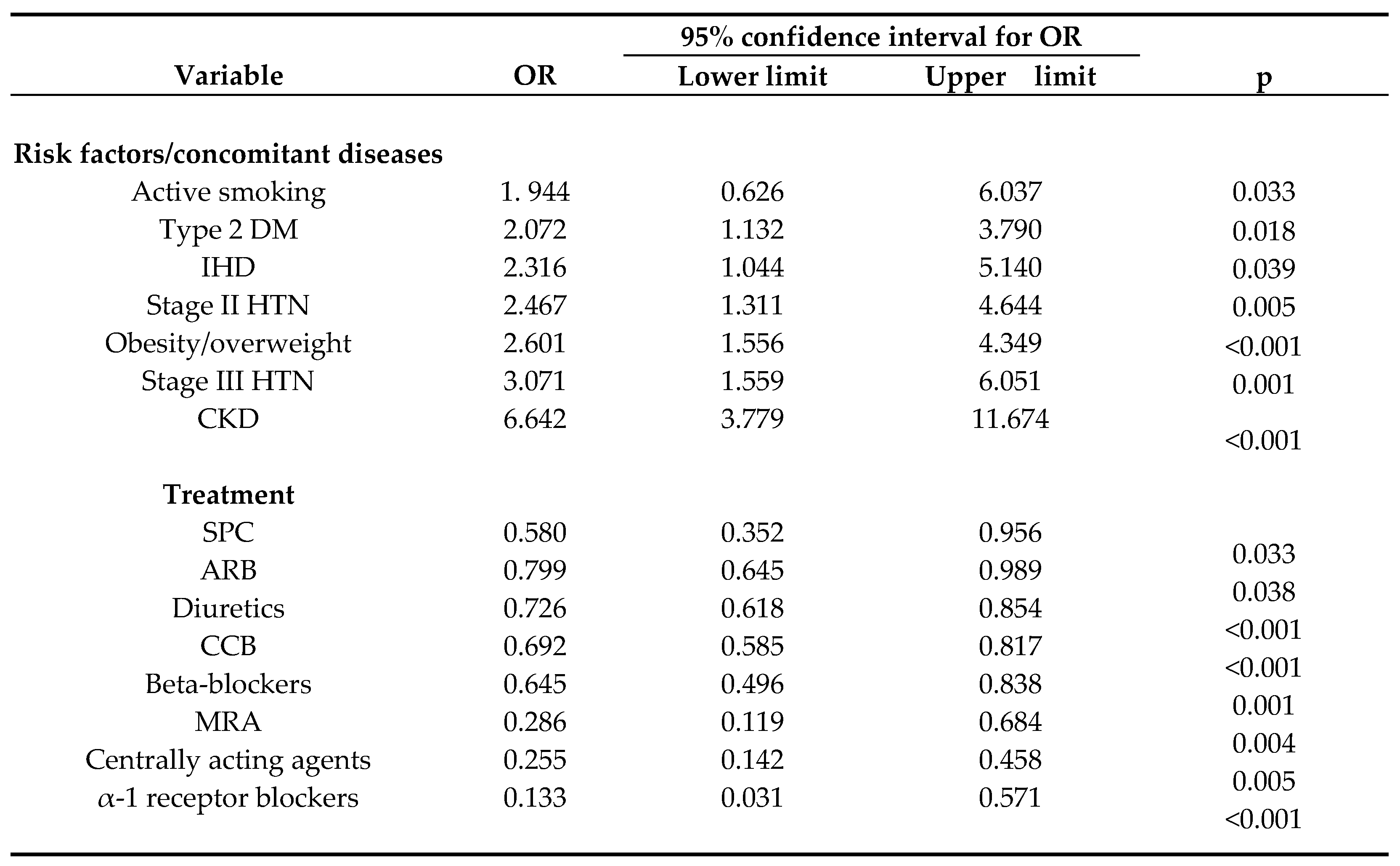
Logistic regression analysis was used to assess the association of various variables with resistant HTN. Prior independent χ2-test was applied to identify categorical variables with statistically significant relationship with resistant HTN. These variables were entered into the univariate logistic regression model; ARB – angiotensin II receptor blocker; CCB – calcium channel blockers; CI – confidence interval; CKD – chronic kidney disease; DM – diabetes mellitus; IHD – ischemic heart disease; MRA – mineralocorticoid receptor antagonist; HTN – arterial hypertension; OR – odds ratio; p – level of significance; SPC – single-pill combination.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



