Submitted:
10 July 2024
Posted:
24 July 2024
You are already at the latest version
Abstract
The amplified production of reactive oxygen species (ROS) or reduced oxidant protection is described as oxidative stress, which contributes to the increase in several disorders, notably obesity and neurodegenerative diseases. Flavonoids are polyphenol compounds found in a variety of foods of plant origin, such as berries, with a basic chemical structure consisting of an aromatic ring linked to a benzene ring and a pyran ring. Flavonoids have neuroprotective activity and promote synaptogenesis and neurogenesis and are also capable of inhibiting oxidative stress and neuroinflammation. Anthocyanins are water-soluble natural pigments that belong to the flavonoid class and have antioxidant and anti-inflammatory properties, helping to reduce chronic inflammation associated with various health conditions, including obesity. In addition, flavonoids and anthocyanins can modulate the expression of genes involved in lipid metabolism, promoting the oxidation of fatty acids and the reduction of lipid synthesis, contributing to the reduction of body fat accumulation. One of the most abundant flavonoids in the natural environment, quercetin, is found mainly in the form of O-glycoside derivatives and rarely as an aglycone. Quercetin has antioxidant properties, against diseases such as cancer; It also acts to combat allergic reactions, inflammatory processes, platelet disorders, obesity, hypertension and atherosclerotic and hypercholesterolemic disorders. Anthocyanins can activate intracellular signaling pathways, such as the AMPK (AMP-activated protein kinase) pathway, which has a crucial role in regulating energy metabolism and glycemic homeostasis. Activation of this pathway increases glucose uptake and fatty acid oxidation, favoring weight loss and improving insulin sensitivity. This review article aims to analyze the effects of using berries in controlling obesity and its role as a reducing factor for mild cognitive decline. A systematic review will be carried out following the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyze. We will search the following electronic databases: PubMed (Medline), Science Direct, Scopus and Web of Science.
Keywords:
berries
; obesity
; mild cognitive decline
; anthocyanins
; polyphenols
1. Introduction
Over the past few decades, the understanding of Mild Cognitive Impairment (MCI) has progressed to describe a state of cognitive functioning that lies between the cognitive decline typical of aging and dementia. This is because MCI presents with deterioration of cognitive functions that exceeds that expected for age and educational level but does not meet all essential criteria to be diagnosed as dementia [1,2]. Mild cognitive decline, unlike dementia, discreetly compromises one or more cognitive domains, without affecting the individual’s independence in their daily activities, although it may require additional effort to carry them out [3].
In addition, the prognosis for individuals with MCI is highly variable and may include recovery of typical neurological function, stability, or progression to dementia. This progression is greater in individuals with MCI compared to those without MCI in the same age group (PETERSEN et al., 2017). Thus, the subtle boundary between MCI, the cognitive slowing typical of aging and dementia constantly challenges the correct distinction and, consequently, the degree of relevance of these conditions [4].
The MCI has a wide variety of classifications, ranging from narrow definitions focused exclusively on amnesia to more comprehensive definitions that encompass other non-amnesic domains. This lack of standardized diagnostic criteria makes it difficult to accurately quantify its prevalence [5]. Progression from MCI to dementia occurs at an estimated annual rate of between 5% and 17% [4]. With global life expectancy increasing, the number of dementia cases is growing exponentially [6]. Figure 1 represents the evolutionary picture from the diagnosis of MCI progressing to cognitive deterioration and possible risk of dementia.
Several risk factors are involved in the pathogenesis of MCI, including advanced age, low educational level, physical inactivity, inadequate eating habits, excessive alcohol consumption, environmental and occupational exposure, socioeconomic status and lack of social involvement. Furthermore, there are additional risk factors associated with comorbidities, such as endocrine, metabolic, cardiovascular, neurological conditions, and psychiatric disorders. Furthermore, head injuries, inflammatory changes, use of certain medications and genetic factors such as the Apolipoprotein E (APOE) polymorphism have also been associated with an increased risk of MCI [7]. Obesity, including generalized or central obesity, or both, has been positively associated with cognitive impairment in young and middle adulthood [8].
MCI is evidenced when there is a slight cognitive impairment in relation to the previous level of performance, which may occur in one or more cognitive domains, such as learning and memory, social cognition, language, executive function, complex attention or perceptual motor. However, this cognitive deficit does not affect the individual’s independence in their daily activities, does not occur exclusively in the context of delirium and is not explained by another mental disorder. This decline happens very subtly, which makes diagnosis a challenge. Furthermore, the classification of different subtypes of MCI and their diverse clinical presentations also represents an obstacle to accurate delimitation. MCI subtypes are categorized according to the etiopathology underlying cognitive impairment, and include Alzheimer’s disease, Frontotemporal lobar degeneration, Lewy body disease, Vascular disease, Traumatic brain injury, Substance/medication use, HIV infection, Prion disease, Parkinson’s disease, Huntington’s disease, other medical condition, multiple etiologies, or unspecified. These subtypes are distinguished according to temporal evolution, the cognitive domains affected and the associated symptoms [9].
Yuan et al. demonstrated that the relationship between the prevalence of MCI and obesity is 18.5%. In addition, this same study showed that only older men (over 75 years of age), who had a high body mass index (BMI), had a higher risk of MCI compared to a normal BMI. There was no significant association between high/higher BMI and MCI in men aged between 60 and 75 years and women over 60 years [30].
Although obesity can also affect cognitive function, the underlying mechanism by which it leads to cognitive decline remains elusive. Evidence shows that obesity affects cognitive function in different ways for different people, based on age. Higher body mass index (BMI) in older people was associated with a decreased risk of dementia [31,32]. Obesity is responsible for an alarming number of deaths each year, as pointed out by the 2024 World Obesity Atlas. Of the 41 million adult deaths recorded annually, 5 million are attributed to high body mass index (BMI), of which, 4 million are related to complications such as diabetes, strokes, coronary heart disease and cancer. Tragically, most of these fatalities occur in underdeveloped and developing countries where resources are scarce. The 2024 World Obesity Atlas report also reveals a correlation between high BMI and economic development. Countries experiencing rapid economic growth often witness a significant increase in the prevalence of obesity, albeit at relatively lower levels. Furthermore, the data highlights the connection between high BMI and the global environmental crisis. Factors such as greenhouse gas emissions, uncontrolled urbanization, accumulation of plastic waste, lack of physical activity and excessive consumption of animal products contribute to the creation of unhealthy environments, fueling the cycle of obesity and its adverse ramifications [16].
According to the World Obesity Federation, obesity is recognized as a chronic, recurrent and progressive condition. The main environmental factor that drives the development of this condition is diet, together with reduced levels of physical activity. Tasty, affordable, and convenient foods have the power to activate the brain’s pleasure centers, generating feelings of gratification similar to those experienced with substances of abuse. Therefore, lack of physical activity and consumption of highly palatable foods rich in fat emerge as the main catalysts for obesity. Furthermore, other environmental factors contribute to this situation, such as reduced sleep time, exposure to endocrine disruptors, epigenetic and intergenerational effects, as well as the use of certain medications and reduced smoking. These elements enhance the effects of the main triggers of obesity, which are tasty and high-fat foods, combined with a lack of physical activity [17].
Under normal conditions, adipose tissue regulates essential biological processes through the following pathways: autocrine, paracrine and endocrine [33]. In obesity, an inflammatory process originates, known as a chronic low-grade inflammatory response of prolonged duration [34], and is the result of an increase in adipose tissue due to excessive nutrient consumption.
During this inflammatory process, there is excessive segregation of inflammatory factors known as adipokines, which are responsible for the origin of inflammation and insulin resistance, which is associated with obesity [35].
In 1987, the first adipokine, Adipsin, was described [36,38], which is actually one of the most important proteins in fat cells, but which, paradoxically, decreases in many animal models of obesity and diabetes [37]. Adipsin/complement factor D was the first adipokine described. It is responsible for maintaining adipose tissue homeostasis and increases insulin secretion in response to glucose [38]. Additionally, it controls the alternative complement pathway to catalyze the production of C3a, an insulin secretagogue [38].
2. Bioactives Compounds
There is an increase in brain functions with the use of polyphenols, directly impacting the cells and processes of the central nervous system (CNS). The effect of these polyphenolic compounds depends on their ability to cross the blood-brain barrier and remain retained in brain tissue, enabling increased neuroplasticity and improved cognition [11].
Polyphenols are bioactive compounds widely recognized for their notable antioxidant properties, notably flavonoids [12]. Polyphenols can be classified into four subclasses according to the number of inert phenolic rings, namely flavonoids, phenolic acids, stilbenes and lignans; curcuminoids are also considered polyphenols, although they do not fall into this category [53]. Curcumin has mechanisms capable of providing improvements in cognition that are still unclear and are considered only suggestive in humans. These cognitive benefits were observed after a relatively short time after supplementation (≤6 months), and the hypothesis is that, at least in part, these improvements were mediated by actions on cerebral microcirculatory function, resulting from increased endothelium-dependent vasodilation and systemic reduction of inflammation, rather than effects on the structure and function of neurons [54]. Epicatechin (EC), a flavonoid present in several food sources, such as cocoa, teas and red fruits, emerges as a component of significant interest [13,14]. Epicatechin has the potential for neurovascular protection, with the ability to regulate redox balance and oxidative stress, in addition to having positive effects on vascular and cognitive function [15].
A recent study carried out by Batista AG and collaborators (2017) demonstrated the beneficial effects of Jabuticaba peel in preventing the hyperphosphorylation of the TAU protein, consequently reducing brain inflammatory processes, in addition to significantly reducing peripheral insulin resistance [18].
The soluble dietary fiber content present in Myrciaria jaboticaba (MJP) deserves attention, as it is involved in fermentation processes by the intestinal microbiota and, therefore, relevant to promoting intestinal and systemic health. The anthocyanin class is strongly significant among the group of polyphenols and flavonoids of MJP [19]. Two important phenolic compounds were identified in MJP: cyanidin-3-O-glucoside and ellagic acid. These compounds contribute greatly to the hydrophilic antioxidant capacity of MJP [20], as they have the ability to donate their electrons or atoms and stabilize free radicals. Nonpolar compounds, such as carotenoids, are relevant for brain studies because of the lipophilicity of the blood-brain barrier [21,22]. The lipophilic fraction of the fruit skin contributes to the total antioxidant capacity, and the total concentration of carotenoids in MJP is relevant to this characteristic, in addition to its lipophilic antioxidant capacity.
Studies have found that supplementation with a purified phenolic compound protects mice against TAU phosphorylation and cognitive decline promoted by streptozotocin-induced diabetes [23] or a high-fat diet [24]. Despite this, when non-diabetic groups and thin were supplemented with the phenolic compound, such effects were not observed. In other words, phenolic compounds do not increase cognition and insulin sensitivity. They are only effective when the body suffers an insult, such as an overdose of saturated fatty acids, or other events [23,24]. A ingestão de MJP pode prevenir fosforilação da tau induzida pela dieta hiperlipídica indiretamente, pela atenuação do peso corporal/gordura e insulina periférica resistência, e diretamente modulando o sinal de insulina, inativando GSK3-. Além disso, um estudo anterior apoia a ideia de um efeito direto da ingestão de MJP na sensibilidade à insulina (via IRS-AKT-FoxO-1 no fígado) sem prevenir ganho de peso [25].
Among the bioactive compounds that make up MJP, Cyanidin-3-0-glucoside, ellagic acid and carotenes stand out, all of which are capable of crossing the blood-brain barrier and are available in the brain parenchyma [26,27]. In the brain, these compounds play a direct role in modulating neuronal receptors, kinases, transcription factors, neurotrophins, synaptic plasticity and other enzymes or proteins linked to the antioxidant and inflammatory system and insulin cascades [28]. Studies have demonstrated high activity of the antioxidant enzymes Superoxide dismutase SOD, Catalase (CAT) and Glutathione peroxidase (GPX) in the frontal lobe, indicating a reduction in oxidative stress through the activation of the antioxidant defense system18. Ingestion of jaboticaba juice can prevent the phosphorylation of TAU protein, when caused by a diet rich in fat, either indirectly, by attenuating the body weight/fat ratio and peripheral insulin resistance; or by direct mechanisms caused by modulation of the insulin signal, inactivating Glycogen Synthase Kinase (GSK-3). Insulin resistance may be critical for TAU phosphorylation, as proper insulin signaling phosphorylates the insulin receptor substrate (IRS) on the tyrosine residue, which in turn phosphorylates protein kinase B (AKT), preventing the phosphorylation of TAU by inactivation of GSK-3.
If, on the one hand, dietary components, such as fatty acids and simple sugars, harm insulin stimuli and cognitive processes, on the other hand, dietary antioxidants such as phenolic compounds and dietary fiber improve insulin sensitivity and neurogenesis [28]. The protective properties of flavonoids show enormous potential in neutralizing oxidative stress, weight gain, insulin resistance, inflammation and some aspects of cognitive deficits [21]. Phenolic compounds are found in common plant foods, and one of their most important sources is olive oil, which contains oleuropein, hydroxytyrosol and oleocanthal. Oleuropein is a glycosylated seco-iridoid with many beneficial properties; has strong antioxidant potential and protects nerve cells from neurotoxin-induced apoptosis [39].
The anti-inflammatory, antihypertensive, vasodilator, anti-obesity, anti-hypercholesterolemic and anti-atherosclerotic effects of Quercetin are known, as it is a vegetable that can be found in more than 20 types of vegetables, such as Moringa oleifera, Centella asiatica, Hypericum perforatum, among other bioflavonoids [62]. Quercetin is a positive compound that can be used in the treatment of obesity, as demonstrated in a randomized, double-blind, placebo-controlled study lasting 12 weeks, with a dose of 100 mg/day/participant, which was able to drastically reduce total body fat, especially in the percentage of fat in the arm, in addition to reducing the body mass index (BMI) of overweight or obese individuals [61].
In an in vitro experiment in Escherichia coli cell culture, Daccache et al. demonstrated that oleuropein prevented the accumulation of a mutated and rapidly aggregating TAU protein by 67% compared to the control group. For wild-type tau, the efficiency was 79%, while methylene blue, the reference tau aggregation inhibitor, was 75% effective. These results suggest that oleuropein can prevent the formation of toxic tau aggregates, probably due to the presence of aldehyde groups in the tautomeric forms of its aglycone metabolite. In the digestive tract, oleuropein is hydrolyzed into another phenolic compound, hydroxytyrosol, which is also present in olive oil and has greater bioavailability [40,41].
3. Method
A systematic review was carried out following the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses. We carried out searches in the following electronic databases: PubMed (Medline), Science Direct, Scopus and Web of Science. The keywords used in the research were: red fruits, obesity, mild cognitive decline, anthocyanins, polyphenols.
Initially, we collected 96 articles based on the keywords used, however, after using the inclusion criteria and considering the year of publication of the research, 62 scientific works remained (Figure 2).
The research was carried out in the period between April 1st and June 30th, 2024; Preference was given to publications from the last ten years. We considered as an inclusion factor publication that met the triad: bioactives-obesity-cognition. The inclusion criteria were clinical studies on humans and studies carried out on laboratory animals. Studies based on literature review were excluded. Initially, all articles of interest that met the keywords were collected; Subsequently, there was a refinement (filter) according to the inclusion criteria and the period of publication (last ten years). The studies that initially met the inclusion criteria were selected and separated.
4. Results
To strengthen the purpose of evaluating the effects of bioactive substances on cognitive processes, we created Table 1 with the compounds and their respective results, which involve biological markers, neurobehavioral assessments and/or other physiological parameters.
5. Discussion
In recent decades, greater attention has been paid to the influence of food on people’s quality of life, because of this, various dietary patterns have been suggested and instilled in the daily lives of individuals, from children to the elderly. One of the biggest villains for human health conditions are so-called ultra-processed foods. Perhaps an incorrect name, considering that ultra processing technology transforms food, without necessarily having the objective of causing harm.
A recent study suggests that the greater the consumption of ultra-processed foods, the greater the risk of damage to health, mainly cardiometabolic effects, common mental disorders and mortality. These studies justify the need to develop strategies and evaluate the effectiveness of using population and public health measures to target and reduce dietary exposure to ultra-processed foods to improve human health. These actions can be considered emergency given the bad outcomes associated with the consumption of ultra-processed foods [55].
Foods with their respective bioactive compounds have been highlighted as regulators against several chronic diseases as they have low toxicity, unlike medications that induce serious side effects. Beneficial effects of dietary anthocyanins have been described in metabolic disorders and inflammation induced by obesity. Some examples, such as red cabbage microgreens, blueberries, black currants, blackberries, cherries, black elderberries, black soybeans, chokeberries, and jabuticaba peels, contain a variety of anthocyanins, including cyanidins, delphinidins, malvidins, pelargonidins, peonidins, and petunidins, and it was observed that they can alter metabolic markers and inflammatory markers in animal and human cells [56].
We can observe a high amount of compounds capable of positively interfering in the control of obesity, resulting in benefits in people’s cognitive performance [57]. This is the big challenge, detecting what these compounds are, the concentrations necessary to reproduce the effects, as well as the ideal form for consumption, tablets, capsules, powder, chocolate bars or in the form of drinks.
But the question is how can I change the memory and behavior through a diet? What metabolic and physiological phenomena can occur to provide this improvement?
Some animal studies have demonstrated significant results regarding the beneficial effects of bioactives. All treatments carried out with jaboticaba peel in obese rats resulted in a reduction in weight gain, adiposity and improved insulin sensitivity. Twelve weeks of supplementation increased HDL cholesterol and prevented hepatic steatosis. The results suggest that jaboticaba peel acts as a functional food, being a dietary strategy to prevent or control obesity. Supplementation with jaboticaba peel can modulate important parameters of obesity and insulin metabolism [58]. Jaboticaba peel extract (PJE) showed potent antioxidant activity and a high content of bioactive compounds. Varying doses of PJE were administered, which were able to prevent weight gain, dyslipidemia, hyperglycemia, in addition to reducing COX-2 levels and improving HDL cholesterol levels in elderly and obese mice [59].
“Meta-inflammation” is a condition produced as a consequence of some issues attributed to obesity, through the occurrence of an inflammatory process characterized by the secretion of inflammatory cytokines, such as interleukin-6, C-reactive protein and tumor necrosis factor-α. Dysbiosis of the intestinal microbiome has been widely studied as the main responsible for this inflammatory process. It is believed that obesity can be combated through the use of bioactive compounds derived from foods rich in anthocyanins (cherries, red raspberries, black soybeans, blueberries, sweet cherries, strawberries and plums), which have as one of their greatest advantages, the fact that they present low toxicity and lack of serious adverse events compared to medications [60].
This review study had some limitations, highlighting the impossibility of relying solely on clinical studies (human beings) given the low number of publications with this focus. A significant part of the research is based on “in vitro” studies involving cell cultures or research involving rats and other laboratory animals. Another difficult issue to manage is obtaining tabular doses of different compounds in the most varied presentations, powders, capsules, teas, other liquids, etc. Validated tests for cognitive verification are also not uniform. Some authors use the Mini Mental State Examination (MMSE), others use memory or verbal assessment tests, among others. This non-uniformity makes it impossible to compare these compounds in the same proportion, as well as to tabulate the results.
6. Conclusions
Healthy eating is an essential factor for a good quality of life, reducing the risk of chronic diseases and increasing life expectancy. Some diets have been studied for many years, such as the Mediterranean diet, with a special relationship to reducing events such as acute myocardial infarction and stroke. Our work has shown that bioactive compounds, especially polyphenols, play a protective role in human cognition, through a significant reduction in obesity. In this bibliographic survey we were able to observe a series of substances capable of combating obesity and bringing cognitive improvements, especially for memory. We believe that combating obesity through the use of bioactives rich in polyphenols results in something beyond weight loss, resulting in better cognitive performance. Furthermore, we observed the need for a greater number of studies involving human beings, with controlled doses of the selected bioactives to better parameterize the results.
References
- Petersen, R.C. Mild Cognitive Impairment. Contin. Lifelong Learn. Neurol. 2016, 22, 404–418. [Google Scholar] [CrossRef] [PubMed]
- Eshkoor, S.A.; Mun, C.Y.; Ng, C.K.; Hamid, T.A. Mild cognitive impairment and its management in older people. Clin. Interv. Aging 2015, 10, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Hugo, J.; Ganguli, M. Dementia and Cognitive Impairment. Clin. Geriatr. Med. 2014, 30, 421–442. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C.; Lopez, O.; Armstrong, M.J.; Getchius, T.S.D.; Ganguli, M.; Gloss, D.; Gronseth, G.S.; Marson, D.; Pringsheim, T.; Day, G.S.; et al. Practice guideline update summary: Mild cognitive impairment. Neurology 2018, 90, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Jongsiriyanyong, S.; Limpawattana, P. Mild Cognitive Impairment in Clinical Practice: A Review Article. Am. J. Alzheimer's Dis. Other Dementiasr 2018, 33, 500–507. [Google Scholar] [CrossRef] [PubMed]
- Manly, J.J.; Jones, R.N.; Langa, K.M.; Ryan, L.H.; Levine, D.A.; McCammon, R.; Heeringa, S.G.; Weir, D. Estimating the Prevalence of Dementia and Mild Cognitive Impairment in the US. JAMA Neurol. 2022, 79, 1242–1249. [Google Scholar] [CrossRef] [PubMed]
- Langa, K.M.; Levine, D.A. The Diagnosis and Management of Mild Cognitive Impairment. JAMA 2014, 312, 2551–2561. [Google Scholar] [CrossRef] [PubMed]
- Hovens, I.B.; Dalenberg, J.R.; Small, D.M. A Brief Neuropsychological Battery for Measuring Cognitive Functions Associated with Obesity. Obesity (Silver Spring, Md) 2019, 27, 1988–96. [Google Scholar] [CrossRef] [PubMed]
- AMERICAN PSYCHIATRIC ASSOCIATION. Diagnostic and statistical manual of mental disorders. 5th-TR ed. [s.l.] American Psychiatric Association, 2022. Available online: https://integrada.minhabiblioteca.com.br/#/books/9786558820949/ (accessed on 6 May 2024).
- Dominguez, L.J.; Veronese, N.; Vernuccio, L.; Catanese, G.; Inzerillo, F.; Salemi, G.; Barbagallo, M. Nutrition, Physical Activity, and Other Lifestyle Factors in the Prevention of Cognitive Decline and Dementia. Nutrients 2021, 13, 4080. [Google Scholar] [CrossRef]
- Grabska-Kobyłecka, I.; Szpakowski, P.; Król, A.; Książek-Winiarek, D.; Kobyłecki, A.; Głąbiński, A.; Nowak, D. Polyphenols and Their Impact on the Prevention of Neurodegenerative Diseases and Development. Nutrients 2023, 15, 3454. [Google Scholar] [CrossRef]
- Calabrò, R.S.; De Cola, M.C.; Gervasi, G.; Portaro, S.; Naro, A.; Accorinti, M.; Manuli, A.; Marra, A.; De Luca, R.; Bramanti, P. The Efficacy of Cocoa Polyphenols in the Treatment of Mild Cognitive Impairment: A Retrospective Study. Medicina 2019, 55, 156. [Google Scholar] [CrossRef] [PubMed]
- Haskell-Ramsay, C.F.; Schmitt, J.; Actis-Goretta, L. The Impact of Epicatechin on Human Cognition: The Role of Cerebral Blood Flow. Nutrients 2018, 10, 986. [Google Scholar] [CrossRef] [PubMed]
- Tejada, S.; Sarubbo, F.; Jiménez-García, M.; Ramis, M.R.; Monserrat-Mesquida, M.; Quetglas-Llabrés, M.M.; Capó, X.; Esteban, S.; Sureda, A.; Moranta, D. Mitigating Age-Related Cognitive Decline and Oxidative Status in Rats Treated with Catechin and Polyphenon-60. Nutrients 2024, 16, 368. [Google Scholar] [CrossRef] [PubMed]
- Cheng, T.; Wang, W.; Li, Q.; Han, X.; Xing, J.; Qi, C.; Lan, X.; Wan, J.; Potts, A.; Guan, F.; et al. Cerebroprotection of flavanol (-)-epicatechin after traumatic brain injury via Nrf2-dependent and -independent pathways. Free. Radic. Biol. Med. 2015, 92, 15–28. [Google Scholar] [CrossRef] [PubMed]
- World Obesity Atlas. Obesity and its consequences. 2024. Available online: https://data.worldobesity.org/publications/WOF-Obesity-Atlas-v7.pdf (accessed on 2 June 2024).
- Bray, G.A.; Kim, K.K.; Wilding, J.P.H.; on behalf of the World Obesity Federation. Obesity: a chronic relapsing progressive disease process. A position statement of the World Obesity Federation. Obesity Reviews 2017, 18, 715–723. [Google Scholar] [CrossRef] [PubMed]
- Batista, Â.G.; Soares, E.S.; Mendonça, M.C.; da Silva, J.K.; Dionísio, A.P.; Sartori, C.R.; da Cruz-Höfling, M.A.; Marostica Junior, M.R. Jaboticaba berry peel intake prevents insulin-resistance-induced tau phosphorylation in mice. Mol Nutr Food Res. 2017, 61. [Google Scholar] [CrossRef] [PubMed]
- Dragano, N.R.V.; Marques, A.Y.C.; Cintra, D.E.C.; Solon, C.; Morari, J.; Leite-Legatti, A.V.; Velloso, L.A.; Maróstica-Júnior, M.R. Freeze-dried jaboticaba peel powder improves insulin sensitivity in high-fat-fed mice. Br. J. Nutr. 2013, 110, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Plaza, M.; Batista, Â.G.; Cazarin, C.B.B.; Sandahl, M.; Turner, C.; Östman, E.; Junior, M.R.M. Characterization of antioxidant polyphenols from Myrciaria jaboticaba peel and their effects on glucose metabolism and antioxidant status: A pilot clinical study. Food Chem. 2016, 211, 185–197. [Google Scholar] [CrossRef]
- Williams, R.J.; Spencer, J.P. Flavonoids, cognition, and dementia: Actions, mechanisms, and potential therapeutic utility for Alzheimer disease. Free. Radic. Biol. Med. 2012, 52, 35–45. [Google Scholar] [CrossRef]
- Sugiura, M.; Ogawa, K.; Yano, M. Comparison of bioavailability between β-cryptoxanthin and β-carotene and tissue distribution in its intact form in rats. Biosci. Biotechnol. Biochem. 2014, 78, 307–310. [Google Scholar] [CrossRef]
- Thomas, J.; Garg, M.L.; Smith, D.W. Dietary resveratrol supplementation normalizes gene expression in the hippocampus of streptozotocin-induced diabetic C57Bl/6 mice. J. Nutr. Biochem. 2014, 25, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Jeon, B.T.; Jeong, E.A.; Shin, H.J.; Lee, Y.; Lee, D.H.; Kim, H.J.; Kang, S.S.; Cho, G.J.; Choi, W.S.; Roh, G.S. Resveratrol Attenuates Obesity-Associated Peripheral and Central Inflammation and Improves Memory Deficit in Mice Fed a High-Fat Diet. Diabetes 2012, 61, 1444–1454. [Google Scholar] [CrossRef]
- Dragano, N.R.V.; Marques, A.Y.C.; Cintra, D.E.C.; Solon, C.; Morari, J.; Leite-Legatti, A.V.; Velloso, L.A.; Maróstica-Júnior, M.R. Freeze-dried jaboticaba peel powder improves insulin sensitivity in high-fat-fed mice. Br. J. Nutr. 2013, 110, 447–455. [Google Scholar] [CrossRef]
- Chen, T.-Y.; Kritchevsky, J.; Hargett, K.; Feller, K.; Klobusnik, R.; Song, B.J.; Cooper, B.; Jouni, Z.; Ferruzzi, M.G.; Janle, E.M. Plasma bioavailability and regional brain distribution of polyphenols from apple/grape seed and bilberry extracts in a young swine model. Mol. Nutr. Food Res. 2015, 59, 2432–2447. [Google Scholar] [CrossRef] [PubMed]
- Yan, L.; Yin, P.; Ma, C.; Liu, Y. Method Development and Validation for Pharmacokinetic and Tissue Distributions of Ellagic Acid Using Ultrahigh Performance Liquid Chromatography-Tandem Mass Spectrometry (UPLC-MS/MS). Molecules 2014, 19, 18923–18935. [Google Scholar] [CrossRef]
- Rendeiro, C.; Rhodes, J.S.; Spencer, J.P. The mechanisms of action of flavonoids in the brain: Direct versus indirect effects. Neurochem. Int. 2015, 89, 126–139. [Google Scholar] [CrossRef] [PubMed]
- Schubert, M.; Gautam, D.; Surjo, D.; Ueki, K.; Baudler, S.; Schubert, D.; Kondo, T.; Alber, J.; Galldiks, N.; Küstermann, E.; et al. Role for neuronal insulin resistance in neurodegenerative diseases. Proc. Natl. Acad. Sci. USA 2004, 101, 3100–3105. [Google Scholar] [CrossRef]
- Yuan, Y.; Li, J.; Zhang, N.; Fu, P.; Jing, Z.; Yu, C.; Zhao, D.; Hao, W.; Zhou, C. Body mass index and mild cognitive impairment among rural older adults in China: the moderating roles of gender and age. BMC Psychiatry 2021, 21, 1–11. [Google Scholar] [CrossRef]
- Hughes, T.; Borenstein, A.; Schofield, E.; Wu, Y.; Larson, E. Association between late-life body mass index and dementia: The Kame Project. Neurology 2009, 72, 1741–1746. [Google Scholar] [CrossRef]
- Atti, A.R.; Palmer, K.; Volpato, S.; Winblad, B.; De Ronchi, D.; Fratiglioni, L. Late-life body mass index and dementia incidence: Nine-year follow-up data from the Kungsholmen Project. J. Am. Geriatr. Soc. 2008, 56, 111–116. [Google Scholar] [CrossRef]
- Blancas-Flores, G.; César Almanza-Pérez, J.; Ivette López-Roa, R.; Javier Alarcón-Aguilar, F.; García-Macedo, R.; Cruz, M. Obesity as an inflammatory process. Bol. Med. Hosp. Infant. Mix. 2010, 67, 88–97. [Google Scholar]
- Fernández-Sánchez, A.; Madrigal-Santillán, E.; Bautista, M.; Esquivel-Soto, J.; Morales-González, Á.; Esquivel-Chirino, C.; Durante-Montiel, I.; Sánchez-Rivera, G.; Valadez-Vega, C.; Morales-González, J.A. Inflammation, oxidative stress, and obesity. Int J Mol Sci 2011, 12, 3117–3132. [Google Scholar] [CrossRef] [PubMed]
- Pereira, S.S.; Alvarez-Leite, J.I. Low-Grade Inflammation, Obesity, and Diabetes. Curr. Obes. Rep. 2014, 3, 422–431. [Google Scholar] [CrossRef] [PubMed]
- Cook, K.S.; Min, H.Y.; Johnson, D.; Chaplinsky, R.J.; Flier, J.S.; Hunt, C.R.; Spiegelman, B.M. Adipsin: a circulating serine protease homolog secreted by adipose tissue and sciatic nerve. Science 1987, 237, 402–405. [Google Scholar] [CrossRef] [PubMed]
- Flier, J.S.; Cook, K.S.; Usher, P.; Spiegelman, B.M. Severely impaired adiposin expression in genetics and acquired obesity. Science 1987, 237, 405–408. [Google Scholar] [CrossRef] [PubMed]
- Lo, J.C.; et al. Adipsin is an adipokine that improves beta cell function in diabetes. Cell 2014, 158, 41–53. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Sánchez, A.; Martínez-Ortega, A.J.; Remón-Ruiz, P.J.; Piñar-Gutiérrez, A.; Pereira-Cunill, J.L.; García-Luna, P.P. Therapeutic Properties and Use of Extra Virgin Olive Oil in Clinical Nutrition: A Narrative Review and Literature Update. Nutrients 2022, 14, 1440. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Morató, J.; Xicota, L.; Fitó, M.; Farré, M.; Dierssen, M.; De La Torre, R. Potential Role of Olive Oil Phenolic Compounds in the Prevention of Neurodegenerative Diseases. Molecules 2015, 20, 4655–4680. [Google Scholar] [CrossRef]
- Daccache, A.; Lion, C.; Sibille, N.; Gerard, M.; Slomianny, C.; Lippens, G.; Cotelle, P. Oleuropein and derivatives from olives as Tau aggregation inhibitors. Neurochem. Int. 2011, 58, 700–707. [Google Scholar] [CrossRef]
- da Silva Lemos, A.B.; da Fonseca, A.R.; de Souza, A.E.S.; Vivan, L.B.; Lomonaco, L.; Dias, S.T.; Salles, B.C.C.; Cerdeira, C.D.; Barros, G.B.S. Effects of the hydroalcoholic extract from the leaves and flour of the fruits of Guabiju (Myrcianthes pungens) on laboratory parameters of diabetic rats. RSD [Internet] 2021, 10, e39910817442. [Google Scholar]
- Geraldi, M.V.; Betim Cazarin, C.B.; Cristianini, M.; Vasques, A.C.J.; Geloneze, B.; Maróstica Júnior, M.R. Jabuticaba juice improves postprandial glucagon-like peptide-1 and antioxidant status in healthy adults: a randomized crossover trial. British Journal of Nutrition 2022, 128, 1545–1554. [Google Scholar] [CrossRef] [PubMed]
- Gutierres, J.M.; Carvalho, F.B.; Schetinger, M.R.; Marisco, P.; Agostinho, P.; Rodrigues, M.; Rubin, M.A.; Schmatz, R.; da Silva, C.R.; de PCognato, G.; Farias, J.G.; Signor, C.; Morsch, V.M.; Mazzanti, C.M.; Bogo, M.; Bonan, C.D.; Spanevello, R. Anthocyanins restore behavioral and biochemical changes caused by streptozotocin-induced sporadic dementia of Alzheimer’s type. Life Sci. 2014, 96, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Devore, E.E.; Kang, J.H.; Breteler, M.M.; Grodstein, F. Dietary intakes of berries and flavonoids in relation to cognitive decline. Ann. Neurol. 2012, 72, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Krikorian, R.; Shidler, M.D.; Nash, T.A.; Kalt, W.; Vinqvist-Tymchuk, M.R.; Shukitt-Hale, B.; Joseph, J.A. Blueberry Supplementation Improves Memory in Older Adults. J. Agric. Food Chem. 2010, 58, 3996–4000. [Google Scholar] [CrossRef] [PubMed]
- Small, G.W.; Siddarth, P.; Li, Z.; Miller, K.J.; Ercoli, L.; Emerson, N.D.; Martinez, J.; Wong, K.-P.; Liu, J.; Merrill, D.A.; et al. Memory and Brain Amyloid and Tau Effects of a Bioavailable Form of Curcumin in Non-Demented Adults: A Double-Blind, Placebo-Controlled 18-Month Trial. Am. J. Geriatr. Psychiatry 2018, 26, 266–277. [Google Scholar] [CrossRef] [PubMed]
- Moura, M.H.; Donado-Pestana, C.M.; Rodrigues, L.; Pessoa, E.V.; e Silva, R.R.; Festuccia, W.T.; Genovese, M.I. Long-term supplementation with phenolic compounds from jaboticaba (Plinia jaboticaba (Vell.) Berg) reduces adiposophaty and improves glucose, lipid, and energy metabolism. Food Res. Int. 2021, 143, 110302. [Google Scholar] [CrossRef]
- Ho, L.; Ferruzzi, M.G.; Janle, E.M.; Wang, J.; Gong, B.; Chen, T.-Y.; Lobo, J.; Cooper, B.; Wu, Q.L.; Talcott, S.T.; Percival, S.S.; Simon, J.E.; Pasinetti, G.M. Identification of brain-targeted bioactive dietary quercetin-3-O-glucuronide as a novel intervention for Alzheimer’s disease. The FASEB Journal 2013, 27, 769–781. [Google Scholar] [CrossRef]
- Stull, A.J.; Cash, K.C.; Champagne, C.M.; Gupta, A.K.; Boston, R.; Beyl, R.A.; Johnson, W.D.; Cefalu, W.T. Blueberries Improve Endothelial Function, but Not Blood Pressure, in Adults with Metabolic Syndrome: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Nutrients 2015, 7, 4107–4123. [Google Scholar] [CrossRef]
- Wood, E.; Hein, S.; Mesnage, R.; Fernandes, F.; Abhayaratne, N.; Xu, Y.; Zhang, Z.; Bell, L.; Williams, C.; Rodriguez-Mateos, A. Wild blueberry (poly)phenols can improve vascular function and cognitive performance in healthy older individuals: a double-blind randomized controlled trial. Am. J. Clin. Nutr. 2023, 117, 1306–1319. [Google Scholar] [CrossRef]
- Huang, F.; Marungruang, N.; Martinsson, I.; Ferrer, L.C.; Nguyen, T.D.; Gondo, T.F.; Karlsson, E.N.; Deierborg, T.; Öste, R.; Heyman-Lindén, L. A mixture of Nordic berries improves cognitive function, metabolic function and alters the gut microbiota in C57Bl/6J male mice. Front. Nutr. 2023, 10, 1257472. [Google Scholar] [CrossRef]
- Truzzi, F.; Tibaldi, C.; Zhang, Y.; Dinelli, G.; D′Amen, E. An Overview on Dietary Polyphenols and Their Biopharmaceutical Classification System (BCS). Int. J. Mol. Sci. 2021, 22, 5514. [Google Scholar] [CrossRef] [PubMed]
- Kuszewski, J.C.; Howe, P.R.C.; Wong, R.H.X. Evaluation of Cognitive Performance following Fish-Oil and Curcumin Supplementation in Middle-Aged and Older Adults with Overweight or Obesity. J. Nutr. 2020, 150, 3190–3199. [Google Scholar] [CrossRef] [PubMed]
- Lane, M.M.; Gamage, E.; Du, S.; Ashtree, D.N.; McGuinness, A.J.; Gauci, S.; et al. Ultra-processed food exposure and adverse health outcomes: umbrella review of epidemiological meta-analyses. BMJ 2024, 384, e077310. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-M.; Yoon, Y.; Yoon, H.; Park, H.-M.; Song, S.; Yeum, K.-J. Dietary Anthocyanins against Obesity and Inflammation. Nutrients 2017, 9, 1089. [Google Scholar] [CrossRef]
- de Vries, K.; Medawar, E.; Korosi, A.; Witte, A.V. The Effect of Polyphenols on Working and Episodic Memory in Non-pathological and Pathological Aging: A Systematic Review and Meta-Analysis. Front. Nutr. 2022, 8, 720756. [Google Scholar] [CrossRef]
- Lenquiste, S.A.; Lamas, C.d.A.; Marineli, R.d.S.; Moraes, A.; Borck, P.C.; Camargo, R.L.; Quitete, V.H.A.C.; Carneiro, E.M.; Junior, M.R.M. Jaboticaba peel powder and jaboticaba peel aqueous extract reduces obesity, insulin resistance and hepatic fat accumulation in rats. Food Res. Int. 2018, 120, 880–887. [Google Scholar] [CrossRef] [PubMed]
- Lamas, C.; Lenquiste, S.; Baseggio, A.; Cuquetto-Leite, L.; Kido, L.; Aguiar, A.; Erbelin, M.; Collares-Buzato, C.; Maróstica, M.; Cagnon, V. Jaboticaba extract prevents prediabetes and liver steatosis in high-fat-fed aging mice. J. Funct. Foods 2018, 47, 434–446. [Google Scholar] [CrossRef]
- Ngamsamer, C.; Sirivarasai, J.; Sutjarit, N. The Benefits of Anthocyanins against Obesity-Induced Inflammation. Biomolecules 2022, 12, 852. [Google Scholar] [CrossRef]
- Lee, J.-S.; Cha, Y.-J.; Lee, K.-H.; Yim, J.-E. Onion peel extract reduces the percentage of body fat in overweight and obese subjects: a 12-week, randomized, double-blind, placebo-controlled study. Nutrition Research Practice 2016, 10, 175–181. [Google Scholar] [CrossRef]
- Sultana, B.; Anwar, F. Flavonols (kaempeferol, quercetin, myricetin) contents of selected fruits, vegetables and medicinal plants. Food Chem. 2008, 108, 879–884. [Google Scholar] [CrossRef]
Figure 1.
Evolution from MCI to Dementia. Source: author himself.
Figure 2.
article search flow. source: the author himself.
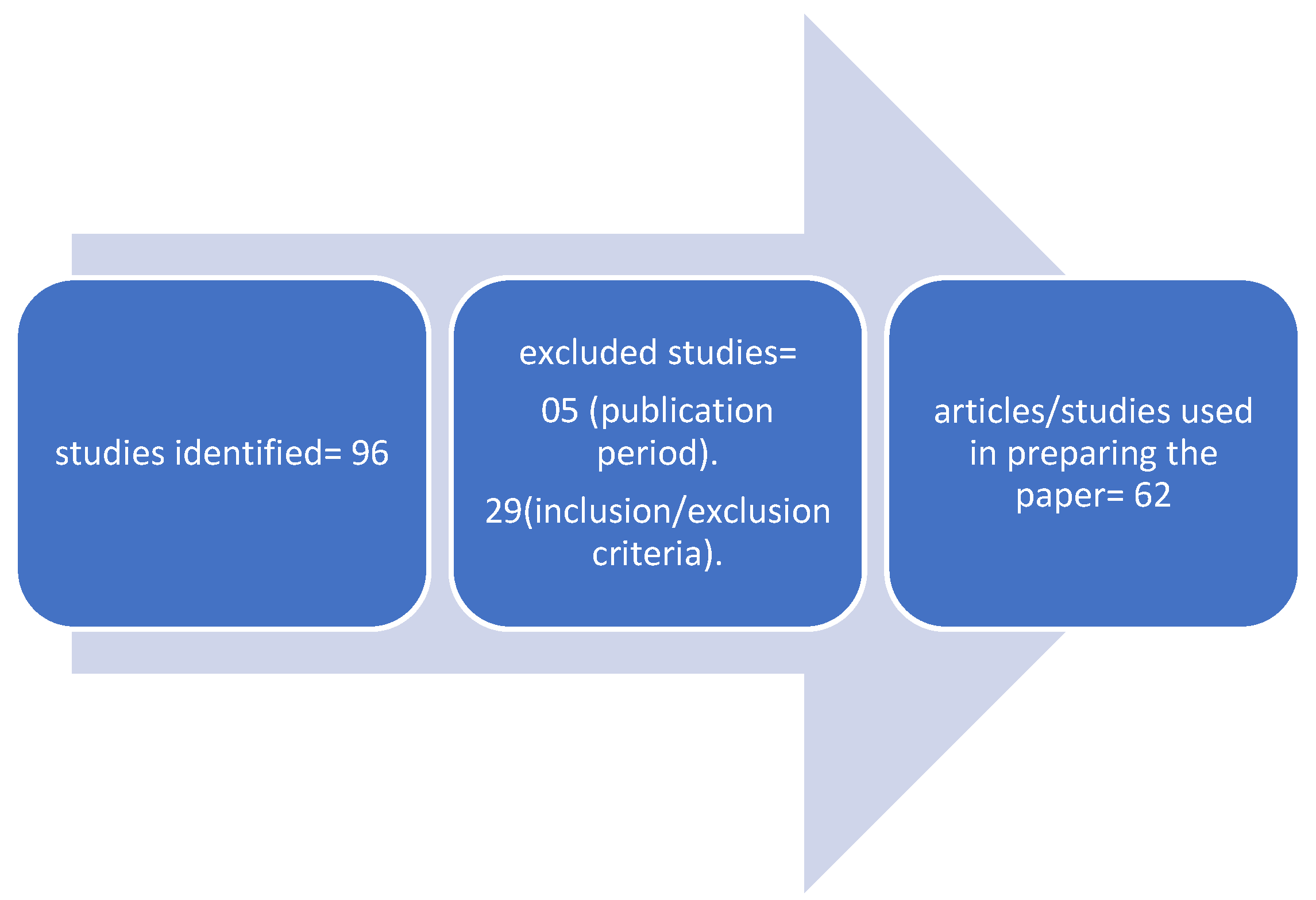

Table 1.
| Compound evaluated | Dose, time | Model used (humans, age, sex, conditions, inclusion criteria | Main results (biomarkers used) |
Reference |
|---|---|---|---|---|
| Guabiju (myrcianthes pungens) | hydroethanolic extract of Guabiju leaves at a concentration of 300 mg/Kg. The treatment was carried out for 90 days. | Wistar rats | Treatment with Guabiju leaf extract prevented the increase in liver damage, and liver function results showed significant beneficial changes in animals treated with Guabiju leaf extract, with a decrease in AST (aspartate aminotransferase) levels. This action in preventing typical complications of DM, such as liver damage, at low doses, demonstrates that this plant may have possible therapeutic activity, which must be refined with new tests and clinical trials that prove its efficacy and safety. | 42 |
| Plinia Jabuticaba | 250 ml Jabuticaba solution; 16 participants | Humans; 11 women, 5 men; healthy men and women, aged between 18 and 40, and with weight (BMI 18–25 kg/m2 ). Exclusion criteria included: age <18 years; allergy, hypersensitivity or intolerance to any food/ food ingredients; smoke; a vegetarian or vegan diet; taking a food supplement or receive any medication treatment; pregnancy or breastfeeding; diagnosis of diabetes mellitus, hypertension or reported medical history of CVD, cancer, liver, kidney, or bowel illness. |
250 ml of jaboticaba juice before a carbohydrate meal was able to improve antioxidant status and GLP-1 concentrations in healthy individuals. Compared to placebo, jaboticaba juice ingestion resulted in a GLP-1 response greater than the AUC and peaking at 60 min. Jaboticaba juice also resulted in greater antioxidant capacity. | 43 |
| Anthocyanins (extracted and purified from grape skins) | Anthocyanin10mg/KG | Male Wistar rats (3 months old) weighing 350-400 g were used in the study |
Biomarker evaluated: Acetylcholinesterase. The results demonstrated that Anthocyanin is capable of regulating ion pump activity and cholinergic neurotransmission, in addition to being capable of improving memory and acting as an anxiolytic compound in animals. | 44 |
| Blueberry, Strawberry | 145,4 a 684,1 mg/dia | 16010 participants over 70 years of age | A higher intake of blueberries and strawberries has been linked to slower rates of cognitive decline. These effect estimates were equivalent to those found in previous cohort studies, indicating that berry intake appears to delay cognitive aging by up to 2.5 years. Furthermore, in further supporting evidence, higher intakes of anthocyanidins and total flavonoids have been associated with slower rates of cognitive decline. | 45 |
| Blueberry | 734 mg/ml (phenolics); Anthocyanins 877 mg | 444 to 621 ml per day; 12 weeks 5 men, 4 women |
This preliminary study suggests, through its findings, that moderate-term blueberry supplementation may provide neurocognitive benefits with preventive potential related to neuronal mechanisms. | 46 |
| Curcumin | 40 participants without dementia, aged 51 to 84; 90 mg of Curcumin twice a day |
Human beings | Daily oral use of curcumin can improve memory and attention in adults without dementia, that is, without a neurodegenerative process. The results show that the benefits of symptoms are associated with a decrease in the accumulation of amyloid and tau proteins in brain regions that modulate mood and memory. | 47 |
| Plinia Jaboticaba | 2 groups “Food” group: 20 Control group: 46 Preparation of Phenolic Extract |
Mices | Several therapeutic properties against diet-induced obesity were demonstrated in this study. Polyphenols derived from Jabuticaba (PEJ) prevented weight gain in mice with already established obesity. Animals treated with PEJ showed a decrease in adipocyte hyperplasia and inflammation caused by adiposopathy. PEJ improved glucose metabolism by reducing FBG, glucose intolerance, insulinemia and insulin resistance, similarly, PEJ also improved lipid metabolism, decreasing plasma levels of total cholesterol and LDL-cholesterol. The study concludes that long-term PEJ supplementation can be used as an adjuvant against obesity and associated metabolic changes. | 48 |
| Quercetina-3-0-Glucoronide | Polyphenolic compounds | Cell cultures | We demonstrated that quercetin-3-O-glucuronide significantly reduced the generation of β-amyloid (Aβ) peptides by primary neuron cultures; It has also been demonstrated that quercetin-3-O-glucuronide is also capable of interfering with the initial protein-protein interaction of Aβ1–40 and Aβ1–42 that is necessary for the formation of neurotoxic oligomeric Aβ species | 49 |
| Strawberry, Blueberry | 44 men and women 45 g powder (Strawberry and Blueberry) daily for 6 weeks |
human beings | The study concludes that daily consumption of blueberries improved (increased) endothelial function over six weeks in individuals with metabolic syndrome. |
50 |
| Wild blueberry | 61 healthy older individuals aged 65-80 – 12 weeks | human beings | There is improvement in vascular and cognitive function and reduction in 24-hour ambulatory systolic blood pressure in healthy elderly people.; polyphenols may improve episodic memory processes and executive functioning in older adults at risk for cognitive decline | 51 |
| Nordic berries | 4,5 months | male mice | Supplementing with the berry mixture may have beneficial effects on spatial memory, as seen by better performance in the T-maze and Barnes maze compared to rats given the high-fat diet without fruit. It has also been observed that berry intake may help counteract high-fat diet-induced weight gain and may influence neuroinflammatory status, as suggested by increased levels of the inflammation-modifying cytokine IL-10 in mouse hippocampal extracts. supplemented with red fruits. | 52 |
source: the author himself.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



