
Submitted:
18 July 2024
Posted:
24 July 2024
You are already at the latest version
Abstract
Background/Objectives: The global burden of metabolic dysfunction-associated steatotic liver disease (MASLD) is increasing at an alarming rate. Cardiovascular disease (CVD) is the leading cause of mortality in MASLD patients, therefore, the therapeutic interventions for MASLD should improve coronary risk factors such as obesity, diabetes and dyslipidemia, in addition to improving liver function. The evidence on effect of sodium-glucose cotransporter 2 inhibitors (SGLT2is) which have beneficial pharmacological properties for MASLD, especially the long-term effects, on the progression of MASLD in Asian population is very limited. Methods: The retrospective longitudinal study was performed by using the medical records at the National Center for Global Health and Medicine, Kohnodai Hospital, Japan. We picked up patients with type 2 diabetes who had taken SGLT2is for at least 3 years or longer between April 1, 2014 and March 31, 2018. We collected the data on metabolic parameters, including blood tests and anthropometric parameters, and compared the data before and after the initiation of SGLT2is treatment. Results: During the observation period, 324 patients had taken SGLT2is for 3 years. The 3-year-SGLT2is treatment significantly reduced body weight, hemoglobin A1c, low-density lipoprotein-cholesterol, triglyceride and non-high-density lipoprotein-cholesterol (HDL-C) and significantly increased HDL-C. Furthermore, this treatment significantly improved liver function and the markers for hepatic steatosis and hepatic fibrosis. Conclusions: Considering that the development of CVD determines the prognosis of MASLD patients, the long-term SGLT2is treatment may be an ideal therapy for MASLD patients.
Keywords:
cardiovascular disease
; hepatic fibrosis
; metabolic dysfunction-associated steatotic liver disease
; sodium-glucose cotransporter 2 inhibitors
; serum lipids
1. Introduction
Metabolic dysfunction-associated steatotic liver disease (MASLD), previously termed nonalcoholic fatty liver disease (NAFLD), is defined as the presence of hepatic steatosis in conjunction with at least one cardiometabolic risk factor (obesity, hypertension, type 2 diabetes, dyslipidemia) [1]. Approximately 1/4 of people with hepatic steatosis progress to metabolic dysfunction-associated steatohepatitis (MASH), which is characterized by hepatocellular ballooning and lobular necroinflammation, and an increased risk of fibrosis, cirrhosis, hepatic decompensation, hepatocellular carcinoma, and all-cause mortality [2]. The global burden of MASLD is increasing at an alarming rate, with global prevalence reaching up to 32.4% [3,4].
A retrospective analysis of patients with MASLD showed that cardiovascular disease (CVD) (38.3%), followed by non-liver malignancy (18.7%) and complications of liver cirrhosis (7.8%), were the three most common causes of death in MASLD patients [5], suggesting that CVD was the most crucial determinant of mortality in MASLD patients. Considering that the development of CVD determines the prognosis of MASLD patients, the therapeutic interventions for MASLD should improve coronary risk factors such as obesity, diabetes and dyslipidemia, in addition to an improving in liver function [6]. The features of metabolic syndrome are not only highly prevalent in patients with MASLD but also components of metabolic syndrome also increase the risk of developing MASLD [7]. The established conditions for developing MASLD include obesity, type 2 diabetes, hypertension and dyslipidemia such as high TG and low HDL-C levels [7]. Obesity, especially, visceral obesity is the most common and well-documented risk factor for MASLD. In the meta-analysis, the pooled odds ratio (OR) for the formation of MASLD in waist circumference and body mass index (BMI) were 2.34 (95%CI, 1.83 to 3.00) and 2.85 (95%CI, 1.60 to 5.08), respectively [8].
Sodium-glucose cotransporter 2 inhibitors (SGLT2is), are reversible inhibitor of SGLT2, leading to reduction of renal glucose reabsorption and decrease of plasma glucose, in an insulin-independent manner [9,10,11]. Such property of SGLT2is is beneficial to reduce visceral fat as well as body weight [11]. Recent meta-analysis provided evidence that SGLT2is significantly reduced visceral adipose tissue, subcutaneous adipose tissue, and ectopic liver fat, in addition to body weight, especially in young type 2 diabetic patients with MASLD and high BMI [12]. However, the evidence on effect of SGLT2is, especially the long-term effects, on the progression of MASLD in Asian population is very limited.
Here, we investigated the long-term (> 3 years) effect of SGLT2is on glucose/lipid metabolism and the markers for hepatic steatosis and hepatic fibrosis in Japanese patients with type 2 diabetes.
2. Materials and Methods
2.1. Study Population
The study protocol was approved by the Ethics Committee of the National Center for Global Health and Medicine (NCGM-S-004397), and the study was performed in accordance with the Declaration of Helsinki.
The retrospective longitudinal study was performed by using the medical records at the National Center for Global Health and Medicine, Kohnodai Hospital, Japan. We picked up patients with type 2 diabetes who had taken SGLT2is for at least 3 years or longer between April 1, 2014 and March 31, 2018. We excluded the patients who did not visit our hospital regularly.
2.2. Data Collection
We collected the data on metabolic parameters, including blood tests and anthropometric parameters, and compared the data before and after the initiation of SGLT2is treatment. Body weight, height, and blood pressure were measured according to the clinical standards. BMI was calculated by dividing body weight in kilograms by body height squared in meters. The measurements of serum hemoglobin A1c (HbA1c), total cholesterol (TC), triglyceride (TG), blood urea nitrogen (BUN), creatinine, and uric acid (UA) were performed using enzymatic assays. The hexokinase method was used for the evaluation of plasma glucose. Total protein (TP) and serum albumin were measured by the modified bromocresol green method. Total bilirubin (T-Bil) was measured by the vanadate oxidase method. A direct method was used for the measurements of serum low-density lipoprotein cholesterol (LDL-C) and high-density lipoprotein-cholesterol (HDL-C). Serum aspartate aminotransferase (AST), alanine aminotransferase (ALT) and γ-glutamyl transferase (GGT) were measured by using the Japan Society of Clinical Chemistry transferable method. The estimated glomerular filtration rate (eGFR) was calculated by age and serum creatinine based on the estimation equation for Japanese patients [13]. Non-HDL-C was calculated by subtracting HDL-C from TC. We used the hepatic steatosis index (HSI) as the marker for hepatic steatosis, and this index was calculated by using the following formula: 8 × (ALT/AST) + BMI + (2, if diabetes mellitus) + (2, if female) [14]. We used the AST-to-platelet ratio index (APRI) and fibrosis-4 (FIB-4) index as the markers for hepatic fibrosis. The APRI was calculated as follows: AST (IU/L)/Upper limit of the normal range of AST: 40 (IU/L)/Platelet count (109/L) × 100 [15]. FIB-4 index was calculated as follows: (age × AST)/(platelet counts (×109/L) × (ALT)1/2 [16,17].
2.3. Statistical Analysis
Comparisons between baseline data and the data after start of SGLT2is were analyzed by the paired t-tests. Spearman’s rank correlation coefficient was used to determine the correlations between the parameters. Missing data were excluded from analyses. All data are expressed as mean ± SD, and p < 0.05 was considered to be statistically significant. We used SPSS version 29 (IBM Corp, Armonk, NY, USA) for statistical analysis.
3. Results
3.1. Characteristics of Patients
During the observation period, 324 patients had taken SGLT2is for 3 years. Clinical and laboratory characteristics of patients studied were shown in Table 1. The mean age of the patients was 58.9±14.2 years, and the mean BMI was 28.1±5.9 kg/m2, suggesting that a relatively large number of obese patients were included in this study. The mean value of HbA1c was 8.3±1.7 %, indicating that a relatively large number of patients with poor glucose control were included. Hematological data such as hemoglobin, hematocrit and the count of platelets and the markers for renal function such as BUN, creatinine and eGFR were within normal range in most patients. UA, TP, T-Bil and albumin levels were also within normal range. The mean value of AST was the upper limit of normal range. The mean values of ALT and GGT were close to the upper limit of normal range in males and were above the normal range in females. The mean value of TG was above the upper limit of normal range.
Used SGLT2is were shown in Table 2. Six kinds of SGLT2is were used. Dapagliflozin and luseogliflozin were frequently used.
3.2. Changes in Metabolic Parameters by the 3-Year-SGLT2is Treatment
Changes in metabolic parameters by the 3-year-SGLT2is treatment were shown in Table 3. The 3-year-SGLT2is treatment significantly reduced body weight by 3.4kg. HbA1c was significantly reduced by 0.9%. TC, LDL-C, TG and non-HDL-C significantly decreased and HDL-C significantly increased. Furthermore, the 3-year-SGLT2is treatment significantly reduced AST, ALT and GGT.
3.3. Changes in the Markers for Hepatic Steatosis and Hepatic Fibrosis after the Start of SGLT2is
Changes in HSI which is the marker for hepatic steatosis, and APRI which is the maker for hepatic fibrosis after the start of SGLT2is were shown in Figure 1. The 3-year-SGLT2is treatment significantly reduced HSI, and HSI significantly decreased at one and two years after the start of SGLT2is. The 3-year-SGLT2is treatment also significantly reduced APRI, and APRI significantly decreased at one year after the start of SGLT2is.
Changes in FIB-4 index, another maker for hepatic fibrosis, after the start of SGLT2is were shown in Figure 2. The analysis using all patients showed a significant increase in FIB-4 index at 2 and 3 years after SGLT2is administration. According to FIB-4 values, patients were classified as (1) low risk for advanced hepatic fibrosis, FIB-4 < 1.3; (2) intermediate risk, FIB-4 1.3-2.66; and (3) high risk, FIB-4 ≥ 2.67 [6]. The 3-year-SGLT2is treatment significantly reduced FIB-4 index in high risk patients. In such patients, FIB-4 index significantly decreased at one year after SGLT2is administration.
3.4. Correlations between Changes in Metabolic Parameters by the 3-Year-SGLT2is Treatment
3.4.1. Correlation of Changes in Serum Lipids with Changes in Metabolic Parameters at 3 Years after the Start of SGLT2is
Correlation of changes in serum lipids with changes in metabolic parameters at 3 years after the start of SGLT2is were shown in Table 4. Change in serum TG was significantly and positively correlated with changes in HbA1c, ALT and GGT. Change in serum non-HDL-C was significantly and positively correlated with changes in HbA1c and GGT.
3.4.2. Correlation of Changes in the Markers for Hepatic Steatosis And Hepatic Fibrosis with Changes in Metabolic Parameters by the 3-Year-SGLT2is Treatment
Correlation of changes in the markers for hepatic steatosis and hepatic fibrosis with changes in metabolic parameters by the 3-year-SGLT2is treatment were shown in Table 5. The change in HSI was siginificantly and positively correlated with changes in body weight, BMI and HbA1c, and also significantly and negatively correlated with HDL-C. The change in APRI was siginificantly and positively correlated with changes in body weight, BMI and HbA1c. The change in APRI was not correlated with changes in any serum lipids.
4. Discussion
Insulin resistance observed in patients with type 2 diabetes and/or obesity enhances the expression and activity of hormone sensitive lipase (HSL) which catalyzes the hydrolysis of TG into free fatty acids (FFA) in adipose tissue [18]. Insulin resistance induces an excess TG storage within the skeletal muscle by reducing FA oxidation [19]. Serum FFA increase due to increased release from the adipose tissue and decreased FA oxidation in the skeletal muscle. An increased amount of FFA enters the liver, leading to overproduction of TG-rich lipoproteins such as very-low-density lipoprotein (VLDL). In insulin resistance, an increased FFA entry to liver, increases in components of VLDL such as apo B100 and apo CIII, and an increase in microsomal TG transfer protein (MTP) which is involved in VLDL assembly may elevate hepatic production of VLDL [20,21,22]. Insulin resistance increases expression of sterol regulatory element binding protein 1c (SREBP-1c), which induces FA synthesis [23]. FA accumulation and resulting over-production of VLDL which are induced by insulin resistance may be the features of MASLD. In short, FA accumulation and over-production of VLDL may induce inflammation and oxidative stress which develop MASLD [6].
In intravascular space, insulin resistance reduces the activity of lipoprotein lipase (LPL) which is the rate-limiting enzyme for the catabolism of TG-rich lipoproteins such as VLDL [24,25]. The formation of HDL is related to the catabolism of TG-rich lipoproteins by LPL [26]. Therefore, reduced LPL activity increases VLDL and reduces HDL. Therefore, serum high TG and low HDL-C are commonly observed in patients with type 2 diabetes, obesity and metabolic syndrome. Insulin resistance reduces LDL receptor expression [27], which can explain the increase in LDL-C in patients with type 2 diabetes and/or obesity. Niemann-Pick C1-like 1 (NPC1L1) plays a pivotal role in intestinal cholesterol absorption. Diabetes increases the expression of NPC1L1 [28], which may also contribute to an increase in TG-rich lipoproteins and LDL-C in type 2 diabetic patients.
The evidence on effects of SGLT2is on serum lipids is very limited, and we found four meta-analyses. The meta-analysis including a total of 28 randomized controlled trials (RCTs) showed that SGLT2is significantly increased serum LDL-C levels (mean difference [MD], 0.09 mmol/L; 95% confidence interval (CI), 0.03 to 0.16), p = 0.0046] and HDL-C levels (MD, 0.08 mmol/L; 95% CI, 0.06 to 0.11; p < 0.0001). Neutral effect of SGLT2is on TC (MD, 0.08 mmol/L; 95% CI, -0.08 to 0.24; p = 0.3150) and TG (MD, -0.03 mmol/L; 95% CI, -0.23, 0.16; p = 0.7382) [29]. The meta-analysis including 60 RCTs showed that SGLT2is treatment increased TC by 0.09 mmol/L (95% CI, 0.06 to 0.13), LDL-C by 0.08 mmol/L (95% CI, 0.05 to 0.10), and HDL-C by 0.06 mmol/L (95% CI, 0.05 to 0.07), while it reduced TG by 0.10 mmol/L (95% CI, 0.06 to 0.14) [30]. In Asian compared to non-Asian populations, a slightly larger increase in HDL-C and a decrease in TG were observed, but with similar results for TC and LDL-C. The meta-analysis including a total of 57 RCTs demonstrated that SGLT2is significantly increased HDL-C by 0.07 mg/dL (95% CI, 0.06 to 0.08, P < 0.00001), LDL-C by 0.11 mg/dL, (95% CI, 0.09 to 0.13 mg/dL, p < 0.00001) and TC by 0.10 mg/dL (95% CI, 0.06 to 0.15, p < 0.0001) [31]. SGLT2is significantly reduced TG by -0.10 mg/dL (95% CI, -0.13 to -0.06, p < 0.00001). The meta-analysis of 48 RCTs revealed that SGLT2is had a significant increase on TC by 0.09 mmol/L (95 % CI, 0.05 to 0.13; p < 0.0001), LDL-C by 0.10 mmol/L (95 % CI, 0.07 to 0.12; p < 0.00001), HDL-C by 0.06 mmol/L (95 % CI, 0.05 to 0.08; p < 0.00001). Additionally, SGLT2is administration showed a significant decrease in TG by -0.10 mmol/L (95 % CI, -0.13 to -0.07; p < 0.00001) [32].
Present study demonstrated that the 3-year-SGLT2is treatment significantly reduced TC and LDL-C, which completely disagreed with the results of meta-analyses. The inclusion of a relatively large number of short-term RCTs and patients of different races in such meta-analyses can explain a different result between ours and meta-analyses. Our previous study showed that SGLT2is did not show a significant effect on LDL-C and TG at 1, 2, 3, and 6 months after the start of SGLT2is [33,34], suggesting that a long-term treatment is required to evaluate the effects of SGLT2is on serum lipids. Our study showed that SGLT2is significantly increased HDL-C, which was observed in all four meta-analyses. We also showed that SGLT2is significantly reduced TG, which was observed in three of four meta-analyses.
Epidemiologic and clinical trials have shown that elevated TG and low levels of HDL-C are independent risk factors for coronary heart disease Therefore, the 2001 National Cholesterol Education Program Adult Treatment Panel III (ATP III) guidelines placed more emphasis on the importance of managing high TG and low HDL-C by identifying non-HDL-C (LDL-C + VLDL-C) [35]. An effect of SGLT2is on non-HDL-C has not been sufficiently studied, and only present study and one meta-analysis reported an effect of SGLT2is on non-HDL-C. The meta-analysis showed that SGLT2is had a significant increase in non-HDL-C by 0.09 mmol/L (95 % CI, 0.06 to 0.12; p < 0.00001) [32], which disagreed with our result that SGLT2is significantly reduced non-HDL-C. This difference may be due to the inclusion of a relatively large number of short-term RCTs and patients of different races in the meta-analysis. Most studies had shown that SGLT2is reduced TG [30,31,32], which is included in non-HDL-C. SGLT2is may reduce TG, by reducing TG-rich lipoprotein-cholesterol which is included non-HDL-C. Therefore, our result may be considered more scientifically valid.
Present study showed that SGLT2is significantly reduced LDL-C, TG and non-HDL-C, and significantly increased HDL-C. The 3-year-SGLT2is treatment significantly reduced body weight and HbA1c, suggesting that the long-term SGLT2is treatment improved insulin resistance. Such beneficial changes in serum lipids may be induced by an improvement in insulin resistance by the 3-year-SGLT2is treatment. Changes in TG and non-HDL-C were significantly and positively correlated with changes in HbA1c, supporting our hypothesis.
The evidence on effects of SGLT2is on MASLD is very limited. We previously reported that SGLT2is significantly reduced the serum levels of AST and ALT at 3 and 6 months after the start of the SGLT2is in patients with type 2 diabetes [33,34]. We found that the FIB-4 index was significantly decreased at 12 months after the start of SGLT2i treatment in a high-risk (FIB-4 ≥ 2.67) group for advanced hepatic fibrosis [36]. We also retrospectively studied 568 patients with MASLD and type 2 diabetes. At 96 weeks, the mean FIB-4 index had significantly decreased (from 1.79±1.10 to 1.56±0.75) in the SGLT2i group but not in the pioglitazone group [37]. APRI significantly decreased in both groups. The body weight of the SGLT2i-treated group decreased by 3.2 kg; however, that of the pioglitazone group increased by 1.7 kg.
Present study is the first to report the long-term effects of SGLT2is on the markers for hepatic steatosis and hepatic fibrosis. Our study showed that the 3-year-SGLT2is treatment significantly reduced HSI as the marker for hepatic steatosis and APRI as the marker for hepatic fibrosis, and a significant reduction in FIB-4 index in high-risk group was also observed. Changes in both HSI and APRI were significantly and positively correlated with changes in body weight, BMI and HbA1c, suggesting that weight loss and an improvement of insulin resistance by the 3-year-SGLT2is treatment may improve hepatic steatosis and fibrosis. Change in HSI was significantly and negatively correlated with change in HDL-C and change in GGT was significantly and positively correlated with changes in TG and non-HDL-C, suggesting that an improvement in serum lipids by SGLT2is may also favorably influence on the progression of MASLD.
SGLT2is decrease plasma glucose without an increase in insulin secretion by reducing renal glucose reabsorption, resulting in an increase in the ratio of glucagon to insulin, which activates HSL in adipose tissue [127]. FFA release from adipose tissue increases due to an increase in the hydrolysis of TG, which reduces adipose tissue size, resulting in an improvement in insulin resistance due to reduced inflammatory cytokines and increased adiponectin [128]. FFA released from adipose tissue may be promptly used by skeletal muscles and liver because SGLT2is shift the energy metabolism towards FA utilization by the alteration of the glucose–FA cycle [130]. An increase in adiponectin levels has beneficial effects on glucose and lipid metabolism by activation of adenosine monophosphate-activated protein kinase (AMPK) [94]. SGLT2is has been reported to activate AMPK and inactivate acetyl-CoA carboxylase (ACC) which regulates FA synthesis in obese mice [129]. The activation of AMPK and resulting inactivation of ACC is also associated with the improvement of MASLD. The long-term SGLT2is treatment may reduce FA accumulation in liver, which reduces inflammation and oxidative stress and results in an improvement of MASLD.
5. Conclusions
The long-term SGLT2is treatment significantly reduced atherogenic lipids such as LDL-C, TG and non-HDL-C, and increased anti-atherogenic lipoprotein, HDL. Furthermore, this treatment improved hepatic steatosis and hepatic fibrosis. Considering that the development of CVD determines the prognosis of MASLD patients, the long-term SGLT2is treatment may be an ideal therapy for MASLD patients.
Author Contributions
H. Y.; Conceptualisation, Supervision, Writing - original draft, review & editing. H. K.; Conceptualisation, Data curation. S. H.; M. H. ; H. A.; Formal analysis, Data curation. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study protocol was approved by the Ethics Committee of the National Center for Global Health and Medicine (NCGM-S-004397), and the study was performed in accordance with the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained by the opt-out approach because this study was a retrospective observational study.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
We thank the staffs of the Division of Research Support, National Center for Global Health and Medicine Kohnodai Hospital.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rinella, M.E.; Lazarus, J.V.; Ratziu, V.; Francque, S.M.; Sanyal, A.J.; Kanwal, F.; Romero, D.; Abdelmalek, M.F.; Anstee, Q.M.; Arab, J.P.; et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Hepatology. 2023, 78, 1966–1986. [Google Scholar] [CrossRef] [PubMed]
- Loomba, R.; Friedman, S.L.; Shulman, G.I. Mechanisms and disease consequences of nonalcoholic fatty liver disease. Cell. 2021, 184, 2537–2564. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.V.; Mark, H.E.; Anstee, Q.M.; Arab, J.P.; Batterham, R.L.; Castera, L.; Cortez-Pinto, H.; Crespo, J.; Cusi, K.; Dirac, M.A.; et al. Advancing the global public health agenda for NAFLD: a consensus statement. Nat. Rev. Gastroenterol. Hepatol. 2022, 19, 60–78. [Google Scholar] [CrossRef] [PubMed]
- Riazi, K.; Azhari, H.; Charette, J.H.; Underwood, F.E.; King, J.A.; Afshar, E.E.; Swain, M.G.; Congly, S.E.; Kaplan, G.G.; Shaheen, A.A. The prevalence and incidence of NAFLD worldwide: a systematic review and meta-analysis. Lancet. Gastroenterol. Hepatol. 2022, 7, 851–861. [Google Scholar] [CrossRef] [PubMed]
- Angulo, P.; Kleiner, D.E.; Dam-Larsen, S.; Adams, L.A.; Bjornsson, E.S.; Charatcharoenwitthaya, P.; Mills, P.R.; Keach, J.C.; Lafferty, H.D.; Stahler, A.; et al. Liver Fibrosis, but No Other Histologic Features, Is Associated With Long-term Outcomes of Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology. 2015, 149, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Yanai, H.; Adachi, H.; Hakoshima, M.; Iida, S.; Katsuyama, H. Metabolic-Dysfunction-Associated Steatotic Liver Disease-Its Pathophysiology, Association with Atherosclerosis and Cardiovascular Disease, and Treatments. Int. J. Mol. Sci. 2023, 24, 15473. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology. 2018, 67, 328–357. [Google Scholar] [CrossRef] [PubMed]
- Pang, Q.; Zhang, J.Y.; Song, S.D.; Qu, K.; Xu, X.S.; Liu, S.S.; Liu, C. Central obesity and nonalcoholic fatty liver disease risk after adjusting for body mass index. World. J. Gastroenterol. 2015, 21, 1650–1662. [Google Scholar] [CrossRef]
- Vallon, V.; Platt, K.A.; Cunard, R.; Schroth, J.; Whaley, J.; Thomson, S.C.; Koepsell, H.; Rieg, T. SGLT2 mediates glucose reabsorption in the early proximal tubule. J. Am. Soc. Nephrol. 2011, 22, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Jabbour, S.A.; Goldstein, B.J. Sodium glucose co-transporter 2 inhibitors: blocking renal tubular reabsorption of glucose to improve glycaemic control in patients with diabetes. Int. J. Clin. Pract. 2008, 62, 1279–1284. [Google Scholar] [CrossRef]
- Yanai, H.; Katsuyama, H.; Hamasaki, H.; Adachi, H.; Moriyama, S.; Yoshikawa, R.; Sako, A. Sodium-Glucose Cotransporter 2 Inhibitors: Possible Anti-Atherosclerotic Effects Beyond Glucose Lowering. J. Clin. Med. Res. 2016, 8, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wu, N.; Sun, C.; Jin, D.; Lu, H. Effects of SGLT-2 inhibitors on adipose tissue distribution in patients with type 2 diabetes mellitus: a systematic review and meta-analysis of randomized controlled trials. Diabetol. Metab. Syndr. 2023, 15, 113. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, S.; Imai, E.; Horio, M.; Yasuda, Y.; Tomita, K.; Nitta, K.; Yamagata, K.; Tomino, Y.; Yokoyama, H.; Hishida, A.; et al. Revised equations for estimated GFR from serum creatinine in Japan. Am. J. Kidney Dis. 2009, 53, 982–992. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Kim, D.; Kim, H.J.; Lee, C.H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.H.; Cho, S.H.; Sung, M.W.; et al. Hepatic steatosis index: A simple screening tool reflecting nonalcoholic fatty liver disease. Dig. Liver. Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.H.; Xin, Y.N.; Dong, Q.J.; Wang, Q.; Jiang, X.J.; Zhan, S.H.; Sun, Y.; Xuan, S.Y. Performance of the aspartate aminotransferase-to-platelet ratio index for the staging of hepatitis C-related fibrosis: An updated meta-analysis. Hepatology. 2011, 53, 726–736. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.; Lydecker, A.; Murray, K.; Tetri, B.N.; Contos, M.J.; Sanyal, A.J.A. Use of the Fib4 index for non-invasive evaluation of fibrosis in nonalcoholic fatty liver disease. Clin. Gastroenterol. Hepatol. 2009, 7, 1104–1112. [Google Scholar] [CrossRef] [PubMed]
- Sumida, Y.; Yoneda, M.; Hyogo, H.; Itoh, Y.; Ono, M.; Fujii, H.; Eguchi, Y.; Suzuki, Y.; Aoki, N.; Kanemasa, K. Validation of the FIB4 index in a Japanese nonalcoholic fatty liver disease population. BMC. Gastroenterol. 2012, 12, 2. [Google Scholar] [CrossRef] [PubMed]
- Sztalryd, C.; Kraemer, F.B. Regulation of hormone-sensitive lipase in streptozotocin-induced diabetic rats. Metabolism. 1995, 44, 1391–1396. [Google Scholar] [CrossRef] [PubMed]
- Kelley, D.E.; Goodpaster, B.H. Skeletal muscle triglyceride. An aspect of regional adiposity and insulin resistance. Diabetes. Care. 2001, 24, 933–941. [Google Scholar] [CrossRef]
- Fisher, E.A. The degradation of apolipoprotein B100: Multiple opportunities to regulate VLDL triglyceride production by different proteolytic pathways. Biochim. Biophys. Acta. 2012, 1821, 778–781. [Google Scholar] [CrossRef]
- Taghibiglou, C.; Carpentier, A.; Van Iderstine, S.C.; Chen, B.; Rudy, D.; Aiton, A.; Lewis, G.F.; Adeli, K. Mechanisms of hepatic very low density lipoprotein overproduction in insulin resistance. Evidence for enhanced lipoprotein assembly, reduced intracellular ApoB degradation, and increased microsomal triglyceride transfer protein in a fructose-fed hamster model. J. Biol. Chem. 2000; 275, 8416–8425. [Google Scholar]
- Chen, M.; Breslow, J.L.; Li, W.; Leff, T. Transcriptional regulation of the apoC-III gene by insulin in diabetic mice: Correlation with changes in plasma triglyceride levels. J. Lipid. Res. 1994, 35, 1918–1924. [Google Scholar] [CrossRef] [PubMed]
- Avramoglu, R.K.; Basciano, H.; Adeli, K. Lipid and lipoprotein dysregulation in insulin resistant states. Clin. Chim. Acta. 2006, 368, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Yanai, H.; Adachi, H.; Hakoshima, M.; Katsuyama, H. Atherogenic Lipoproteins for the Statin Residual Cardiovascular Disease Risk. Int. J. Mol. Sci. 2022, 23, 13499. [Google Scholar] [CrossRef] [PubMed]
- Nikkila, E.A.; Huttunen, J.K.; Ehnholm, C. Postheparin plasma lipoprotein lipase and hepatic lipase in diabetes mellitus. Relationship to plasma triglyceride metabolism. Diabetes. 1977, 26, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Nikkila, E.A.; Taskinen, M.R.; Kekki, M. Relation of plasma high-density lipoprotein cholesterol to lipoprotein-lipase activity in adipose tissue and skeletal muscle of man. Atherosclerosis. 1978, 29, 497–501. [Google Scholar] [CrossRef] [PubMed]
- Chandra, N.C. A comprehensive account of insulin and LDL receptor activity over the years: A highlight on their signaling and functional role. J. Biochem. Mol. Toxicol. 2021, 35, e22840. [Google Scholar] [CrossRef] [PubMed]
- Lally, S.; Owens, D.; Tomkin, G.H. Genes that affect cholesterol synthesis, cholesterol absorption, and chylomicron assembly: The relationship between the liver and intestine in control and streptozotosin diabetic rats. Metabolism. 2007, 56, 430–438. [Google Scholar] [CrossRef] [PubMed]
- Fan, G.; Guo, D.L.; Zuo, H. The impact of sodium-glucose Cotransporter-2 inhibitors on lipid profile: A meta-analysis of 28 randomized controlled trials. Eur. J. Pharmacol. 2023, 959, 176087. [Google Scholar] [CrossRef] [PubMed]
- Bechmann, L.E.; Emanuelsson, F.; Nordestgaard, B.G.; Benn, M. SGLT2-inhibition increases total, LDL, and HDL cholesterol and lowers triglycerides: Meta-analyses of 60 randomized trials, overall and by dose, ethnicity, and drug type. Atherosclerosis. 2024, 394, 117236. [Google Scholar] [CrossRef]
- Dar, S.; Siddiqi, A.K.; Alabduladhem, T.O.; Rashid, A.M.; Sarfraz, S.; Maniya, T.; Menezes, R.G.; Almas, T. Effects of novel glucose-lowering drugs on the lipid parameters: A systematic review and meta-analysis. Ann. Med. Surg (Lond). 2022, 77, 103633. [Google Scholar] [CrossRef]
- Sánchez-García, A.; Simental-Mendía, M.; Millán-Alanís, J.M.; Simental-Mendía, L.E. Effect of sodium-glucose co-transporter 2 inhibitors on lipid profile: A systematic review and meta-analysis of 48 randomized controlled trials. Pharmacol. Res. 2020, 160, 105068. [Google Scholar] [CrossRef]
- Katsuyama, H.; Hamasaki, H.; Adachi, H.; Moriyama, S.; Kawaguchi, A.; Sako, A.; Mishima, S.; Yanai, H. Effects of Sodium-Glucose Cotransporter 2 Inhibitors on Metabolic Parameters in Patients With Type 2 Diabetes: A Chart-Based Analysis. J. Clin. Med. Res. 2016, 8, 237–243. [Google Scholar] [CrossRef]
- Yanai, H.; Hakoshima, M.; Adachi, H.; Kawaguchi, A.; Waragai, Y.; Harigae, T.; Masui, Y.; Kakuta, K.; Hamasaki, H.; Katsuyama, H.; et al. Effects of Six Kinds of Sodium-Glucose Cotransporter 2 Inhibitors on Metabolic Parameters, and Summarized Effect and Its Correlations With Baseline Data. J. Clin. Med. Res. 2017, 9, 605–612. [Google Scholar] [CrossRef]
- Gotto, A.M. Jr. High-density lipoprotein cholesterol and triglycerides as therapeutic targets for preventing and treating coronary artery disease. Am. Heart. J. 2002, 144(6 Suppl), S33–42. [Google Scholar] [CrossRef]
- Katsuyama, H.; Hakoshima, M.; Iijima, T.; Adachi, H.; Yanai, H. Effects of Sodium-Glucose Cotransporter 2 Inhibitors on Hepatic Fibrosis in Patients With Type 2 Diabetes: A Chart-Based Analysis. J. Endocrinol. Metab. 2020, 10, 1–7. [Google Scholar] [CrossRef]
- Mino, M.; Kakazu, E.; Sano, A.; Katsuyama, H.; Hakoshima, M.; Yanai, H.; Aoki, Y.; Imamura, M.; Yamazoe, T.; Mori, T. , et al. Effects of sodium glucose cotransporter 2 inhibitors and pioglitazone on FIB-4 index in metabolic-associated fatty liver disease. Hepatol. Res. 2023; 53, 618–628. [Google Scholar]
- Obata, A.; Kubota, N.; Kubota, T.; Iwamoto, M.; Sato, H.; Sakurai, Y.; Takamoto, I.; Katsuyama, H.; Suzuki, Y.; Fukazawa, M.; et al. Tofogliflozin Improves Insulin Resistance in Skeletal Muscle and Accelerates Lipolysis in Adipose Tissue in Male Mice. Endocrinology. 2016, 157, 1029–1042. [Google Scholar] [CrossRef]
- Wang, D.; Liu, J.; Zhong, L.; Li, S.; Zhou, L.; Zhang, Q.; Li, M.; Xiao, X. The effect of sodium-glucose cotransporter 2 inhibitors on biomarkers of inflammation: A systematic review and meta-analysis of randomized controlled trials. Front. Pharmacol. 2022, 13, 1045235. [Google Scholar] [CrossRef]
- Randle, P.J.; Garland, P.B.; Hales, C.N.; Newsholme, E.A. The glucose fatty-acid cycle. Its role in insulin sensitivity and the metabolic disturbances of diabetes mellitus. Lancet. 1963, 1, 785–789. [Google Scholar] [CrossRef]
- Yanai, H.; Yoshida, H. Beneficial Effects of Adiponectin on Glucose and Lipid Metabolism and Atherosclerotic Progression: Mechanisms and Perspectives. Int. J. Mol. Sci. 2019, 20, 1190. [Google Scholar] [CrossRef]
- Xu, L.; Nagata, N.; Nagashimada, M.; Zhuge, F.; Ni, Y.; Chen, G.; Mayoux, E.; Kaneko, S.; Ota, T. SGLT2 inhibition by empagliflozin promotes fat utilization and browning and attenuates inflammation and insulin resistance by polarizing M2 macrophages in diet-induced obese mice. EBioMedicine. 2017, 20, 137–149. [Google Scholar] [CrossRef]
Figure 1.
Changes in the markers for hepatic steatosis (Hepatic steatosis index, HIS) and hepatic fibrosis (AST to platelet ratio index, APRI) after the start of SGLT2is. *p < 0.01 and **p < 0.001 vs. baseline data.
Figure 1.
Changes in the markers for hepatic steatosis (Hepatic steatosis index, HIS) and hepatic fibrosis (AST to platelet ratio index, APRI) after the start of SGLT2is. *p < 0.01 and **p < 0.001 vs. baseline data.
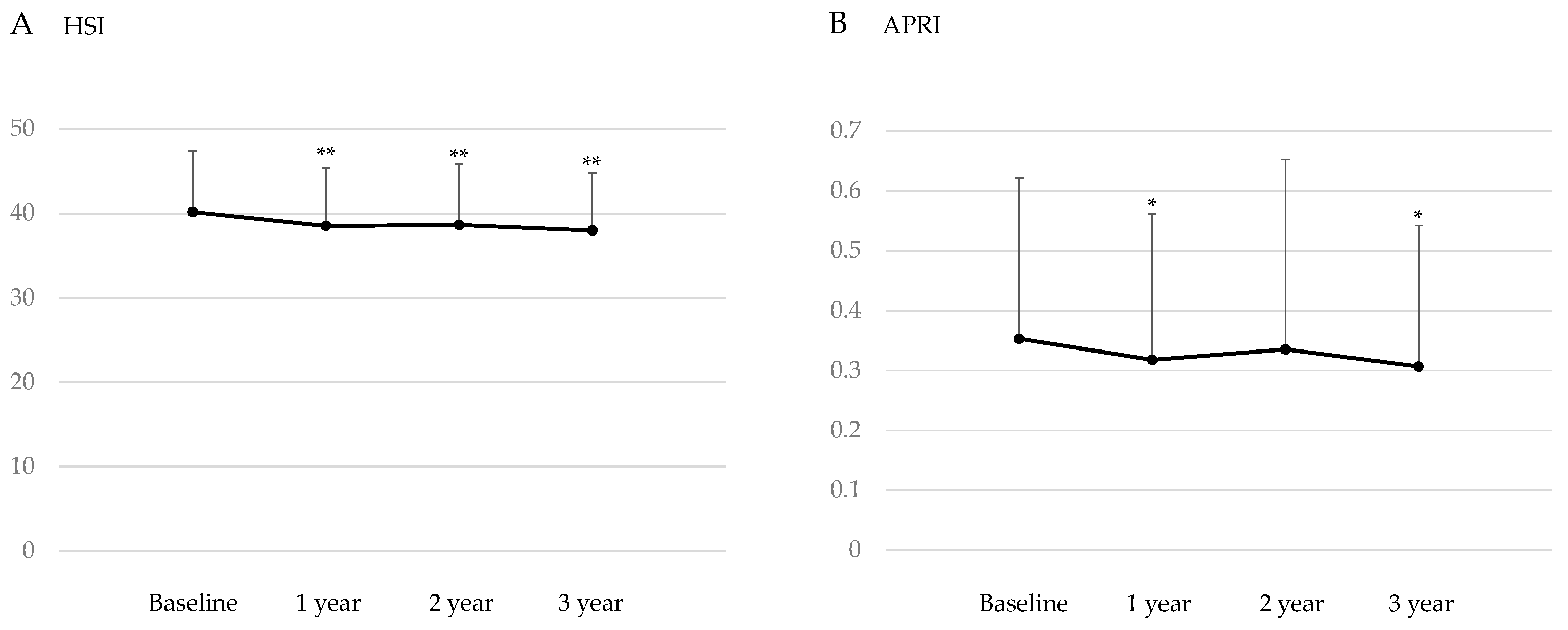
Figure 2.
Change in FIB-4 index after the start of SGLT2is in all patients (A) and in each risk group (B). Red, blue and yellow lines and circles indicate high, intermediate and low risk for advanced hepatic fibrosis, respectively. *p < 0.05 vs. baseline data.
Figure 2.
Change in FIB-4 index after the start of SGLT2is in all patients (A) and in each risk group (B). Red, blue and yellow lines and circles indicate high, intermediate and low risk for advanced hepatic fibrosis, respectively. *p < 0.05 vs. baseline data.
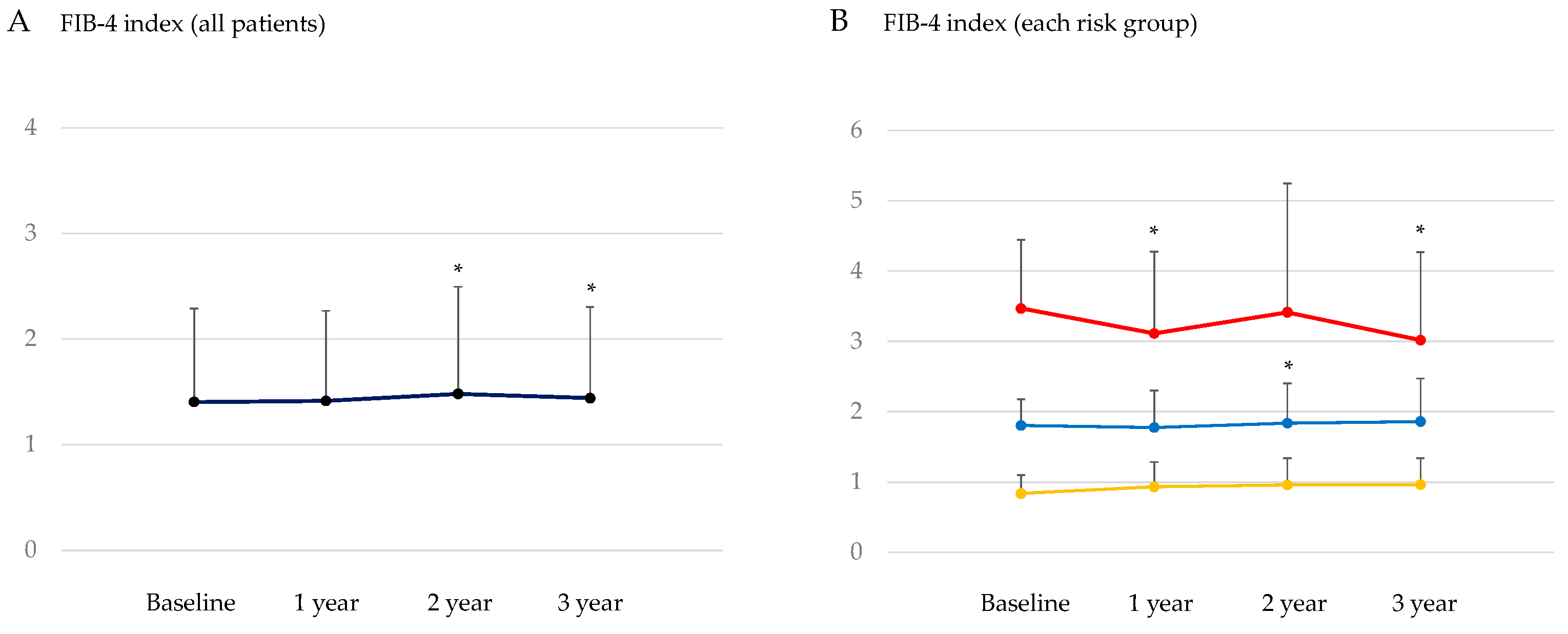

Table 1.
Clinical and laboratory characteristics of patients studied at baseline (n = 324).
| Clinical characteristics | ||
| Gender (male/female) | 188/136 58.9±14.2 163.0±10.0 74.3±18.2 28.1±5.9 133.3±17.9 76.8±12.1 |
|
| Age (years) | ||
| Body height (cm) | ||
| Body weight (kg) | ||
| Body mass index (kg/m2) | ||
| Systolic blood pressure (mmHg) | ||
| Diastolic blood pressure | ||
| Laborarory characteristics | ||
| Data at baseline | Normal range | |
| Plasma glucose (mg/dl) | 192±83 | < 110 |
| HbA1c (%) | 8.3±1.7 | 4.9~6.0 |
| Hemoglobin (g/dl) | 13.9±1.8 | Male 13.7~16.8 Female 11.6~14.8 |
| Hematocrit (%) | 41.9±5.0 | Male 40.7~50.1 Female 35.1~44.4 |
| Platelets (x 104/ml) | 24.0±7.5 | 158~348 |
| Blood urea nitrogen (mg/dl) | 16.5±6.2 | 8~20 |
| Creatinine (mg/dl) | 0.8±0.3 | Male 0.65~1.07 Female 0.46~0.79 |
| eGFR (ml/min/1.73m2) | 78±28 | 60 < |
| UA (mg/dl) | 5.5±1.4 | < 7 |
| TP (g/dl) | 7.2±0.5 | 6.6~8.1 |
| Albumin (g/dl) | 4.2±0.5 | 4.1~5.1 |
| T-Bil | 0.7±0.3 | 0.4~1.5 |
| AST (IU/l) | 30±20 | 13~30 |
| ALT (IU/l) | 38±32 | Male 10~42 Female 7~23 |
| GGT (IU/l) | 58±69 | Male 13~64 Female 9~32 |
| TC (mg/dl) | 187±40 | < 220 |
| HDL-C (mg/dl) | 50±13 | < 40 |
| LDL-C (mg/dl) | 105±32 | < 140 |
| TG (mg/dl) | 185±126 | Non-fasting value < 175 |
| Non-HDL-C (mg/dl) | 138±39 | < 170 |
Presented values indicate mean±SD. ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, gamma-glutamyl transferase; eGFR, estimated glomerular filtration rate; HDL-C, high-density lipoprotein-cholesterol; LDL-C, low-density lipoprotein-cholesterol; Non-HDL-C, non-high-density lipoprotein-cholesterol; T-Bil, total bilirubin; TC, total cholesterol; TG, triglyceride; TP, total protein; UA, uric acid.
Table 2.
Used sodium-glucose cotransporter 2 inhibitors (SGLT2is).
| Kind of SGLT2is | n (%) |
| Dapagliflozin | 98 (30%) |
| Luseogliflozin | 96 (30%) |
| Tofogliflozin | 36 (11%) |
| Ipragliflozin | 34 (10%) |
| Canagliflozin | 34 (10%) |
| Empagliflozin | 30 (9%) |
Table 3.
Changes in metabolic parameters by the 3-year-SGLT2is treatment.
| Baseline | After 3 years | p values | |
| Body weight (kg) | 74.3±18.2 | 70.9±17.6 | < 0.001 |
| Body mass index (kg/m2) | 28.1±5.9 | 26.8±5.5 | < 0.001 |
| Plasma glucose (mg/dl) | 192±83 | 162±69 | < 0.001 |
| HbA1c (%) | 8.3±1.7 | 7.4±1.2 | < 0.001 |
| TC (mg/dl) | 187±40 | 177±33 | < 0.001 |
| HDL-C (mg/dl) | 50±13 | 53±14 | < 0.001 |
| LDL-C (mg/dl) | 105±32 | 98±27 | 0.023 |
| TG (mg/dl) | 185±126 | 161±103 | 0.001 |
| Non-HDL-C (mg/dl) | 138±39 | 124±32 | < 0.001 |
| AST (IU/l) | 30±20 | 26±17 | 0.004 |
| ALT (IU/l) | 38±32 | 31±32 | 0.009 |
| GGT (IU/l) | 58±69 | 53±101 | 0.014 |
Presented values indicate mean±SD. ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, gamma-glutamyl transferase; HDL-C, high-density lipoprotein-cholesterol; LDL-C, low-density lipoprotein-cholesterol; Non-HDL-C, non-high-density lipoprotein-cholesterol; TC, total cholesterol; TG, triglyceride.
Table 4.
Correlation of changes in serum lipids with changes in metabolic parameters at 3 years after the start of SGLT2is.
Table 4.
Correlation of changes in serum lipids with changes in metabolic parameters at 3 years after the start of SGLT2is.
| Δ HDL-C | Δ LDL-C | Δ TG | Δ Non-HDL-C | |
| Δ Body weight | -0.073 | -0.099 | -0.032 | -0.029 |
| Δ BMI | -0.098 | -0.152 | -0.022 | -0.013 |
| Δ HbA1c | 0.033 | 0.033 | 0.165** | 0.151* |
| Δ AST | 0.079 | 0.079 | 0.093 | 0.025 |
| Δ ALT | -0.044 | 0.037 | 0.119* | -0.011 |
| Δ GGT | -0.021 | 0.119 | 0.285** | 0.217** |
Presented values indicate correlation coefficients. *p < 0.05, **p < 0.01. BMI, body mass index; GGT, gamma-glutamyl transferase; HDL-C, high-density lipoprotein-cholesterol; LDL-C, low-density lipoprotein-cholesterol; Non-HDL-C, non-high-density lipoprotein-cholesterol; TG, triglyceride.
Table 5.
Correlation of changes in the markers for hepatic steatosis (HIS) and hepatic fibrosis (APRI) with changes in metabolic parameters at 3 years after the start of SGLT2is.
Table 5.
Correlation of changes in the markers for hepatic steatosis (HIS) and hepatic fibrosis (APRI) with changes in metabolic parameters at 3 years after the start of SGLT2is.
| Δ HSI | Δ APRI | |
| Δ Body weight | 0.583** | 0.273** |
| Δ BMI | 0.593** | 0.258** |
| Δ HbA1c | 0.291** | 0.143* |
| Δ TG | 0.007 | 0.054 |
| Δ HDL-C | -0.228** | 0.063 |
| Δ LDL-C | -0.121 | 0.063 |
| Δ Non-HDL-C | -0.086 | -0.049 |
Presented values indicate correlation coefficients. *p < 0.05, **p < 0.01. APRI, AST to platelet relation index; BMI, body mass index; HDL-C, high-density lipoprotein-cholesterol; HIS, hepatic steatosis index; LDL-C, low-density lipoprotein-cholesterol; Non-HDL-C, non-high-density lipoprotein-cholesterol; TG, triglyceride.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



