
Submitted:
25 July 2024
Posted:
26 July 2024
You are already at the latest version
Abstract
(1) Background: Alzheimer’s Disease (AD) accounts for 70% of dementia cases and with no effective pharmacological treatments, new rehabilitation methods are needed. Motor activities and transcranial direct current stimulation (tDCS) have shown promise in stabilizing and enhancing cognitive functions. Objective: We want to investigate the effects of combined motor or cognitive activity with tDCS on cognitive functions in AD patients. (2) Methods: Patients with mild or moderate AD were randomized into four groups: motor activity or cognitive activity associated with anodic or sham tDCS (MotA, MotS, CogA, CogS). They received two weeks of treatment (45 minutes, 5 days/week), with the first 15 minutes using 2mA tDCS on the dorsolateral prefrontal cortex. Cognitive assessments were conducted pre-treatment (T0), post-treatment (T1), and one week after (T2). (3) Results: Twenty patients were included. Mann-Whitney test showed significant improvements in anodic groups (MotA+CogA) in the global cognitive status (p=.042), in selective attention (p=.012), and sustained attention (p=.012) at T1, but not at T2. In addition, MotA improved in the Picture Recognition Test (p=.027) and in sustained attention (p=.047) at T2. (4) Conclusion: Combined motor or cognitive activity with anodic tDCS could slow cognitive decline in AD patients, with notable improvements in global cognitive state and attention at T1.
Keywords:
Transcranial Direct Current Stimulation
; Motor Activity
; Cognitive Stimulation Alzheimer’s disease
1. Introduction
Every three seconds somebody in the world develops dementia, with an estimation of 50 million individuals affected globally in 2019 [1]. As our global population gets older, the World Health Organization (WHO) predicts that the number of people living with dementia will increase significantly. In 2019, there were 55 million people with dementia, but by 2050, this number is projected to reach 139 million. Alzheimer's disease (AD) is known to be the most common form of dementia contributing to the 60-70% of cases (WHO, 2023), and it affects regions of the cerebral cortex, firstly the temporal and frontal lobes to then progress to the neocortex. Cognitive disabilities start as a clinical hallmark with memory problems, followed by attentive and executive difficulties, causing impairment in daily living and quality of life [2].
Since no effective pharmacological therapy is currently existent for the cure or attenuation of AD's symptoms and their progression [3], other ways to reduce its burden should be developed. The application of standard cognitive or physical treatments has been one alternative way. The efficacy of physical and cognitive training in patients with AD and Mild Cognitive Impairment (MCI), over 6 months, has been compared in a previous our study that showed the positive effects of the two treatments, demonstrating their similar effectiveness in mitigating cognitive decline [4].
In the field of neurorehabilitation, the modulation of cortical excitability and the modification of neuroplasticity have become important mechanisms on which healthcare professionals rely to improve clinical and cognitive functions [5]. Non-Invasive Brain Stimulation Techniques (NIBS) have shown great potential in this field. The primary goal of applying NIBS in neurorehabilitation is to modulate cortical excitability in a specific area that supports a specific function in order to facilitate (or suppress) the activity of that area and the interconnected areas [5,6]. NIBS aims to improve the connectivity of a brain network, which, in turn, enhances a particular behavioral or cognitive function associated with that area or network. In recent years, a specific NIBS technique, Transcranial Direct Current Stimulation (tDCS), has gained significant public interest in this context [5,7]. tDCS is a method that influences brain activity by using low, continuous electric currents (1-2 mA) applied to the scalp via electrodes for 10-30 minutes. Depending on the polarity, it can either increase the firing of brain cells and cortical excitability (anodal tDCS) or reduce cortical excitability by making the brain cells less active (cathodal tDCS). The changes in cortical excitability due to tDCS are not limited to the stimulation period and may involve mechanisms similar to those responsible for long-term changes in the brain's activation [5,7].
Studies have shown that the effects of tDCS last beyond the actual stimulation and can be strengthened through repeated sessions. In the context of neurorehabilitation, tDCS is used to improve cognitive functions by stimulating specific brain networks, however, more studies have tried to apply tDCS in patients with AD [8,9,10]. In the last years, an increased amount of research was conducted toward this direction for the advantages of the device: its portability, its non-invasive nature, safety, low price, and feasibility to be used in combination with standard therapies [11].
Studies applying tDCS to AD patients differed in their research aims: some focused on memory, mostly on word recognition [12,13,14,15,16] and working memory functions [12]; others on attention [12,13,17] or executive functions [16]; and on language [14,18,19,20].
Study protocols also varied among each other for their different methodologies, for example the targeted areas of stimulation that were: the left dorsolateral prefrontal cortex [14,17,19,21,22,23,24]; the temporoparietal areas [12,15]; the left temporal cortex and the right frontal lobe è [16], the left angular and supramarginal gyri [18], the left frontotemporal cortex [20] and the bilateral temporal lobes [13,25].
Sensitiveness in using tDCS as a rehabilitative tool has increased, but only few studies associated the tDCS as a possible treatment [14,18,22,26,27]. Using cognitive training during tDCS can greatly enhance the learning process [28]. This combination is believed to boost brain activity and strengthen specific brain regions involved in cognitive tasks, enhancing long-term brain plasticity by affecting neural networks, with the positive effects extending to similar activities [28,29] This combined approach might also help the benefits of learning last even after the treatment is over. Previous research has shown that pairing tDCS with cognitive training, specifically targeting the DLPFC, leads to improved learning and performance outcomes, particularly in terms of vigilance measures, across various neurodegenerative disorders [28,30,31,32,33]. Moreover other research è [34] highlight that combining tDCS with cognitive and/or physical training may enhance long-term potentiation (LTP)-like plasticity in the desired region beyond either treatment alone.
Therefore, this current research hypothesizes that the addition of a tDCS to cognitive or physical activities, already proven by Fonte and collaborators (2019) to be beneficial when followed by themselves, would enhance their efficacy.
The aim of the present study is to evaluate the efficacy of combining tDCS with motor or cognitive activity on cognitive functions in patients with AD.
2. Materials and Methods
A proof of concept, pilot study, single-blind randomized controlled trial (RCT) comparing the effects of motor and cognitive activity associated with tDCS on cognitive performance in AD patients. The examiner was blinded to group assignment (allocation ratio 1:1). Patients and their caregivers were informed about the experimental nature of the study and gave their written informed consent which was carried out in accordance with the Helsinki Declaration and approved by the local Ethics Committee of the University Hospital Verona, Italy (Protocol CE 2202). The study was reported in accordance with the CONSORT guidelines.
2.1. Participants
Patients with AD were recruited from Mons. Mazzali Geriatric Institute between June 2018 and May 2019. The inclusion criteria were: Mini Mental State Examination (MMSE)>15; good level of compliance; acetylcholinesterase inhibitor treatment (e.g., donepezil, rivastigmine); no modifications of medication during the last four months. Exclusion criteria were: behavioural disorders (e.g., aggressiveness); alcohol abuse; orthopedic pathology with risk of falls to the ground; respiratory pathology; severe auditory or visual deficits uncorrected; history of epileptic fits; anti-epileptic medication; metallic body implants; pacemaker; psychiatric, neurologic, systemic or metabolic disorders. After baseline evaluation, patients were allocated to one of four treatment groups according to a simple software-generated randomization scheme (www.randomization.com). The procedure for recruiting participants is summarized in Figure 1.
2.2. Treatment Procedures
Group 1 received anodal stimulation plus motor activity (MotA); Group 2 received sham stimulation plus motor activity (MotS); Group 3 received anodal stimulation plus cognitive activity (CogA); Group 4 sham stimulation plus cognitive activity (CogS).
Each group underwent 45 minutes of activity of which the first 15 minutes simultaneously with tDCS stimulation. Treatments were delivered for two weeks (45 min) for five times a week.
During the study, participants did not undergo any other physical or cognitive activities.
2.2.1. Motor Activity
A physiotherapist conducted individual motor activity, which included moderate intensity endurance and resistance training. Sessions started with 5 minutes of warm-up and ended with 5 minutes of cool-down which included active joint mobilization. Subsequently patients were subjected to endurance exercises divided in cycling on cycle ergometer walking on a platform, arm cranking on a specific ergometer with a random order.
2.2.2. Cognitive Activity
A neuropsychologist conducted individual cognitive activity, which was based upon stimulation of residual cognitive skills and in particular of memory. The stimulation was adjusted according to the severity of the cognitive decline observed. Each session began with an orientation exercise. After that, oral and paper- pencil exercises of specific cognitive functions were proposed. These exercises aimed to the natural process of reminiscence, but they also focused on the present situation, having an impact on social interaction and mood. Multisensory stimulation was introduced.
2.2.3. tDCS Procedure
The tDCS stimulation was performed using a BrainSTIM stimulator (EMS). A pair of saline-soaked electrodes were placed and secured on patients. The anode (25cm², 5x5) was positioned over the left dorsolateral prefrontal cortex (DLPFC) following the 10–20 system (F3-F7 position), and the cathode (35 cm², 7x5) was placed above the shoulder on the other side. The intensity of stimulation was set at 2mA and applied for 15 minutes at the beginning of cognitive or motor activity (45 minutes).
2.3. Evaluation Procedures
Primary and secondary outcome were measured by the same blinded examiner. Patients were evaluated before treatment (T0), immediately after treatment (T1), and one week of follow-up (T2). The cognitive assessment was carried out in one day for 1 hour. The tests used in the assessment are described below.
2.3.1. Primary Outcome
2.3.2. Secondary Outcome
Picture Recognition (PR) is a subtest of the Rivermead Behavioral Memory Test-3, an ecological memory battery resembling everyday tasks, with the aim to measure daily memory function. The examinee is shown a set of picture and then is asked to recognize them from a further set of pictures at a later time in the testing session. It has two parallel version for monitoring changes over time [37] (Range: 0-15; higher score=best performance).
Digit Span Test- Forward (DSF), used to measure span of immediate verbal recall. The examiner presents digits verbally at a rate of one per second. Examiner requires the participant to repeat the digits in the same order. The number of digits increases by one until the participant consecutively fails two trials of the same digit span length [38](higher score=best performance).
Digit Span Test- Backward (DSB), used to measure working memory. The examiner presents digits verbally and repeats the digits in reverse order. The number of digits increases by one until the participant consecutively fails two trials of the same digit span length [38] (higher score=best performance).
Phonemic Fluency Test (PFT), used to measure processing speed, language production and executive functions. Participants are given one minute to produce as many unique words as possible starting with a given letter. The participant's score in each task is given by the number of correct words [39] (higher score=best performance).
Visual Search Test (VST), to assess visual-selective attention. Three matrices are shown to the subject and the patients has to cross in 45 minutes the target stimuli between distractors [40] (Range: 0-60; higher score=best performance).
Sustained Attention to Response Test (SART): used to evaluate sustained attention and control inhibition. In the test, participants view a computer monitor on which a random series of single digits are presented at the regular rate of 1 per 1.15 seconds. The task is to press a single response key following each presentation with the exception of a nominated no-go digit, to which no response should be made. In the standard version of the test, 225 digits are presented in a continuous sequence over 4.3 minutes. The outcomes are false allarm (FA), omission (OM) and reaction times (RT) (higher score = worst performance) [41].
Neuropsychiatric Inventory (NPI) to evaluate the presence, frequency and severity of behavioral disorders [42] (Range 0-144; higher score = worst performance)
2.4. Statistical Analysis
We assessed data from all randomized patients. The Kruskall-Wallis test was used to measure the homogeneity at baseline and to compute the differences in performance between T1 and T0 (T1-T0) and between T2 and T0 (T2-T0) for all outcome measures of the four groups. The Mann-Whitney U test was used to examine the effects of tDCS comparing MotA+CogA vs. MotS+CogS. The last analysis explore the effects of CogA vs MotA groups. For these purposes, we analyzed the differences in performance between T1 and T0 (T1-T0) and between T2 and T0 (T2-T0) for all outcome measures. The alpha level for significance was set at P < 0.05. Statistical analysis was carried out using the Statistical Package for Social Science (SPSS) for Macintosh, version 26.0 (IBM SPSS Inc, Armonk, NY, USA).
3. Results
Twenty subjects (8 men and 12 women; mean age 82.4 years) presenting with AD (mean time since onset 3.3 years) were recruited from a total of 314 inpatients attending the Mons. Mazzali Geriatric Institute (Figure 1). They were randomized to the MotA group (n = 5), MotS group (n = 4), the CogA group (n = 7) or CogS group (n = 4). Patients’ demographic and clinical characteristics are reported in Table 1. Age, education and MMSE were not statistically different between the four groups. Primary and secondary outcomes measures did not significantly differ between the four groups at baseline (T0).
3.1. Primary Outcome
The Kruskall-Wallis showed no significant differences between the four groups at T1-T0 and T2-T0.
Between-groups comparisons MotA+CogA vs. MotS+CogS showed significant change in MMSE at T1-T0 (p=.042; z= -2.029). No significant difference was found at T2-T0 (p=.697; z= -.389) (see Table 2).
No significant difference in MMSE was found between MotA vs CogA groups at T1-T0 (p=.098; z= -1.653) and at T2-T0 (p=.409; z= -.825) (see Table 3).
3.2. Secondary Outcomes
The Kruskall-Wallis showed no significant differences between the four groups in all secondary outcomes at T1-T0 and at T2-T0.
Significant differences in the VST (p=.012, z= -2.515) and SART-FA (p=.012; z=-2.504) were found between MotA+CogA vs. MotS+CogS at T1-T0 but not at T2-T0 (see Table 2).
Focusing on the effects of the anodic stimulation, no significant difference was found between the MotA vs CogA at T1-T0. The same analysis showed a significant difference at T2-T0 in PR (p= .027; z= -2.212) and SART-RT (p=.047; z= -1.989) (see Table 3).
4. Discussion
At present, there is an ongoing debate in the scientific literature regarding whether tDCS exhibits clear therapeutic benefits for patients with neurodegenerative disorders. In particular, studies by Gangemi and collaborators (2021) and Yu and colleagues (2021) respectively support the effectiveness of anodal-tDCS in slowing down the progression of Alzheimer's disease in both the short and long term and as a convincing instrument in cognitive enhancement and maintenance. On the other hand, in a study by Pellicciari and Miniussi in 2018, the effectiveness of tDCS was not recorded in neurodegenerative patients.
A possible explanation for these discrepancy in outcomes would be hypothesizing in the different methodologies applied. The tDCS protocols indeed varied among each other in terms of the stimulated area and the duration of stimulation, the electrode shape and amplitude, the position of reference electrode, the on-line or off-line treatment during the stimulation with tDCS, or the use of underpowered sample sizes [7]. Finally, the assessment procedures could lead to very different results [43].
However, in literature, NIBS techniques may enhance clinical recovery by facilitating functional and structural neuronal changes, strengthening synapses, and increasing dendritic connections. tDCS can alter resting membrane potentials, either enhancing or decreasing underlying cortical excitability. Moreover, tDCS could promote rehabilitation by increasing adaptive neuroplasticity and reducing the pathological consequences in different neurological disease [34].
In literature, several studies indicate the effectiveness of DLPFC stimulation on cognitive functions [28,30,31,32], particularly in recognition memory and overall cognitive function in patients with Alzheimer's disease [17,21]. Activation of the left DLPFC, involved in various cognitive functions such as executive control and memory, plays a key role in self-initiating the use of mnemonic strategies and consolidating information for the formation of long-term memory traces (Im Jeong, 2019).
Therefore, the aim of this pilot study was to evaluate the effectiveness of tDCS as a neurorehabilitation strategy for improving clinical condition of AD. The tDCS, applied on DLPFC, was associated to a motor or cognitive activity in patients with Alzheimer’s disease.
In a study published by our team [4], indeed, it was shown that a motor intervention was equally effective as the established gold standard treatment for Alzheimer's disease, which is cognitive stimulation.
In our protocol the treatment was administered for two weeks, five times a week, each session lasting one hour. tDCS stimulation occurred during the initial 15 minutes of either the cognitive or motor stimulation, targeting the DLPFC area. To test these hypotheses, the changes in performance on various neuropsychological tests were compared across four groups: MotA, MotS, CogA, and CogS.
In the first instance, we investigated the effects of real stimulation, combining the groups that received real stimulation (MotA+CogA) and comparing them to those who received a placebo stimulation (MotS+CogS). The results show a significant improvement from T0 at T1 in global cognitive status in the real stimulation groups (MotA+CogA). This result reinforces the data present in the literature, whereby AtDCS on DLPFC area improves the performance of global cognitive status [21].
The results obtained from this study show also that anodal stimulation, combined with cognitive or motor treatment, improves performance in visual selective attention and inhibitory control (fewer false alarms in SART-FA). Therefore, the groups receiving transcranial anodal stimulation seems to have a better performance than the groups receiving sham stimulation [21].
From an analysis of the performance obtained by the groups receiving anodal stimulation (MotA vs CogA) emerge that MotA group at T2 performed significantly better in the Picture Recognition test than the CogA group. This result is partially confirmed by the study of Boggio and collaborators (2009), which reports that a stimulation of 3 sessions of AtDCS on the DLPFC (intensity of 2mA for 30 min) improves performance in tasks of recognition memory. The salient findings of Boggio’s work (2009) is that, for the first time, AtDCS has effects on recognition memory in short term (day after treatment). Similarly, the results of our study show that AtDCS combined with motor stimulation induces an improvement in recognition memory. Remains to be investigated why this intervention occurs at T2 rather than immediately at T1.
At T2, there are also significant differences between the two groups: in particular the CogA group, comparing with MotA, demonstrates a better performance in reaction time to a stimulus (TR-SART). This result contrasts with the findings of Cotelli and colleagues (2014), which indicate an improvement in performance in groups combining cognitive stimulation with AtDCS or StDCS, compared to the group receiving motor stimulation with AtDCS. Additionally, at a 12-month follow-up, Cotelli's study (2014) also reports no significant differences in the comparison between groups that received cognitive or motor stimulation with AtDCS.
From the analysis of this study don’t emerge significant results in the performance of verbal fluency for the CogA group; this result confirms the data obtained from the study of Penolazzi and collaborators (2015) in which AtDCS stimulation combined with cognitive training doesn’t elicit any improvement in the task.
Furthermore, the study's findings confirm that tDCS combined with cognitive or motor treatment doesn’t ameliorate the behavioural disorders assessed by NPI. This outcome aligns with existing literature, suggesting that tDCS alone is insufficient for inducing behavioural changes [23], even when tDCS is paired with cognitive or motor stimulation. The analysis, however, did not reveal the superiority of one intervention over the other, possibly due to the limited group size.
The results of this study indicate a superiority of the AtDCS groups over the StDCS groups, confirming findings in the existing literature [13,17,20,21]. Thus, we investigate whether the two activities associated with real stimulation, motor and cognitive rehabilitation, had the same effect, comparing the MotA group with the CogA group. It was observed that at T1, after the rehabilitation, the effects of both treatments were similar, with no clear advantage of one treatment over the other. However, at T2, it was noted that those who underwent motor treatment showed improved visual memory recognition, while those receiving cognitive treatment had faster reaction times.
The variations in results observed across different studies investigating the impact of tDCS stimulation on cognitive performance may be attributed to disparities in the specific brain regions targeted and the different tDCS protocols employed in these experiments. In our study, we coupled tDCS stimulation with daily sessions of either cognitive or motor activities, whereas other studies either featured a single tDCS session or multiple tDCS sessions on a daily basis. This study is one of the pioneering efforts to explore the beneficial effects of combining tDCS with a stimulation in Alzheimer's patients. In the past different authors have already investigated the effects of tDCS combined with cognitive stimulation [14,22,26,27], but nobody explored the effects of tDCS with a motor stimulation in these patients.
It's important to note that this study has some limitations, most notably the relatively small participant sample. Nevertheless, despite these limitations, the results clearly indicate that 10 sessions of combined tDCS treatment alongside either cognitive or motor stimulation lead to a more pronounced slowing of cognitive decline when compared to a single administration of either treatment alone.
Since tDCS is not a neurorehabilitation strategy, but it modulates brain excitability to simplify the recruitment of brain networks that have been weakened by a diminished synaptic activity [7], it should be paired with rehabilitation protocols to facilitate a more ecological improvement.
This study opens the doors to a new perspective in the neurorehabilitation field that allows us to experience tDCS as an additional tool that can amplify the effects of a stimulation, with the aim of improving the cognition of these patients. 5. Conclusions
This section is not mandatory but can be added to the manuscript if the discussion is unusually long or complex.
References
- Prince, M.; Wimo, A.; Guerchet, M.; Ali, G.-C.; Wu, Y.-T.; Prina, M. World Alzheimer Report 2015: The Global Impact of Dementia – An Analysis of Prevalence, Incidence, Cost and Trends; Alzheimer's Disease International: London, 2015; pp. 1–87. [Google Scholar]
- Weintraub, S.; Wicklund, A. H.; Salmon, D. P. The neuropsychological profile of Alzheimer disease. Cold Spring Harbor perspectives in medicine 2012, 2, a006171. [Google Scholar] [CrossRef]
- Graham, W. V.; Bonito-Oliva, A.; Sakmar, T. P. Update on Alzheimer’s Disease Therapy and Prevention Strategies. Annual review of medicine 2017, 68, 413–430. [Google Scholar] [CrossRef]
- Fonte, C.; Smania, N.; Pedrinolla, A.; Munari, D.; Gandolfi, M.; Picelli, A.; et al. Comparison between physical and cognitive treatment in patients with MCI and Alzheimer’s disease. Aging 2019, 11, 3138–3155. [Google Scholar] [CrossRef]
- Wagner, T.; Valero-Cabre, A.; Pascual-Leone, A. Noninvasive Human Brain Stimulation. Annual Review of Biomedical Engineering 2007, 9, 527–565. [Google Scholar] [CrossRef]
- Nitsche, M. A.; Paulus, W. Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. The Journal of physiology 2000, 527 Pt 3(Pt 3), 633–639. [Google Scholar] [CrossRef]
- Pellicciari, M. C.; Miniussi, C. Transcranial Direct Current Stimulation in Neurodegenerative Disorders. The journal of ECT 2018, 34, 193–202. [Google Scholar] [CrossRef]
- Chang, C.-H.; Lane, H.-Y.; Lin, C.-H. Brain Stimulation in Alzheimer’s Disease. Frontiers in psychiatry 2018, 9, 201. [Google Scholar] [CrossRef]
- Cammisuli, D. M.; Cignoni, F.; Ceravolo, R.; Bonuccelli, U.; Castelnuovo, G. Transcranial Direct Current Stimulation (tDCS) as a Useful Rehabilitation Strategy to Improve Cognition in Patients With Alzheimer’s Disease and Parkinson’s Disease: An Updated Systematic Review of Randomized Controlled Trials. Frontiers in neurology. Switzerland 2021, p 798191. [CrossRef]
- Yu, T.-W.; Lane, H.-Y.; Lin, C.-H. Novel Therapeutic Approaches for Alzheimer’s Disease: An Updated Review. International journal of molecular sciences 2021, 22. [Google Scholar] [CrossRef]
- Davis, S. E.; Smith, G. A. Transcranial Direct Current Stimulation Use in Warfighting: Benefits, Risks, and Future Prospects. Frontiers in human neuroscience 2019, 13, 114. [Google Scholar] [CrossRef]
- Ferrucci, R.; Mameli, F.; Guidi, I.; Mrakic-Sposta, S.; Vergari, M.; Marceglia, S.; et al. Transcranial direct current stimulation improves recognition memory in Alzheimer disease. Neurology 2008, 71, 493–498. [Google Scholar] [CrossRef]
- Boggio, P. S.; Ferrucci, R.; Mameli, F.; Martins, D.; Martins, O.; Vergari, M.; et al. Prolonged visual memory enhancement after direct current stimulation in Alzheimer’s disease. Brain stimulation 2012, 5, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Penolazzi, B.; Bergamaschi, S.; Pastore, M.; Villani, D.; Sartori, G.; Mondini, S. Transcranial direct current stimulation and cognitive training in the rehabilitation of Alzheimer disease: A case study. Neuropsychological rehabilitation 2015, 25, 799–817. [Google Scholar] [CrossRef] [PubMed]
- Marceglia, S.; Mrakic-Sposta, S.; Rosa, M.; Ferrucci, R.; Mameli, F.; Vergari, M.; et al. Transcranial Direct Current Stimulation Modulates Cortical Neuronal Activity in Alzheimer’s Disease. Frontiers in neuroscience 2016, 10, 134. [Google Scholar] [CrossRef] [PubMed]
- Bystad, M.; Grønli, O.; Rasmussen, I. D.; Gundersen, N.; Nordvang, L.; Wang-Iversen, H.; et al. Transcranial direct current stimulation as a memory enhancer in patients with Alzheimer’s disease: a randomized, placebo-controlled trial. Alzheimer’s research & therapy 2016, 8, 13. [Google Scholar] [CrossRef]
- Boggio, P. S.; Khoury, L. P.; Martins, D. C. S.; Martins, O. E. M. S.; de Macedo, E. C.; Fregni, F. Temporal cortex direct current stimulation enhances performance on a visual recognition memory task in Alzheimer disease. Journal of neurology, neurosurgery, and psychiatry 2009, 80, 444–447. [Google Scholar] [CrossRef] [PubMed]
- Costa, V.; Brighina, F.; Piccoli, T.; Realmuto, S.; Fierro, B. Anodal transcranial direct current stimulation over the right hemisphere improves auditory comprehension in a case of dementia. NeuroRehabilitation 2017, 41, 567–575. [Google Scholar] [CrossRef] [PubMed]
- Gangemi, A.; Fabio, R. Transcranial direct current stimulation for Alzheimer disease. Asian Journal of Gerontology and Geriatrics 2020, 15, 5–9. [Google Scholar] [CrossRef]
- Gangemi, A.; Colombo, B.; Fabio, R. A. Effects of short- and long-term neurostimulation (tDCS) on Alzheimer’s disease patients: two randomized studies. Aging clinical and experimental research 2021, 33, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Khedr, E. M.; Gamal, N. F. El; El-Fetoh, N. A.; Khalifa, H.; Ahmed, E. M.; Ali, A. M.; et al. A double-blind randomized clinical trial on the efficacy of cortical direct current stimulation for the treatment of Alzheimer’s disease. Frontiers in aging neuroscience 2014, 6, 275. [Google Scholar] [CrossRef]
- Cotelli, M.; Manenti, R.; Brambilla, M.; Petesi, M.; Rosini, S.; Ferrari, C.; et al. Anodal tDCS during face-name associations memory training in Alzheimer’s patients. Frontiers in aging neuroscience 2014, 6, 38. [Google Scholar] [CrossRef]
- Suemoto, C. K.; Apolinario, D.; Nakamura-Palacios, E. M.; Lopes, L.; Leite, R. E. P.; Sales, M. C.; et al. Effects of a non-focal plasticity protocol on apathy in moderate Alzheimer’s disease: a randomized, double-blind, sham-controlled trial. Brain stimulation 2014, 7, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Im, J. J.; Jeong, H.; Bikson, M.; Woods, A. J.; Unal, G.; Oh, J. K.; et al. Effects of 6-month at-home transcranial direct current stimulation on cognition and cerebral glucose metabolism in Alzheimer’s disease. Brain stimulation 2019, 12, 1222–1228. [Google Scholar] [CrossRef]
- Khedr, E. M.; Salama, R. H.; Abdel Hameed, M.; Abo Elfetoh, N.; Seif, P. Therapeutic Role of Transcranial Direct Current Stimulation in Alzheimer Disease Patients: Double-Blind, Placebo-Controlled Clinical Trial. Neurorehabilitation and neural repair 2019, 33, 384–394. [Google Scholar] [CrossRef]
- Andrade, S. M.; de Oliveira, E. A.; Alves, N. T.; dos Santos, A. C. G.; de Mendonça, C. T. P. L.; Sampaio, D. D. A.; et al. Neurostimulation combined with cognitive intervention in Alzheimer’s disease (NeuroAD): Study protocol of double-blind, randomized, factorial clinical trial. Frontiers in Aging Neuroscience. Frontiers Media S.A.: Switzerland 2018. [CrossRef]
- Marchi, L. Z.; Ferreira, R. G. D.; de Lima, G. N. S.; da Silva, J. A. S.; da Cruz, D. M. C.; Fernandez-Calvo, B.; et al. Multisite transcranial direct current stimulation associated with cognitive training in episodic memory and executive functions in individuals with Alzheimer’s disease: a case report. Journal of medical case reports 2021, 15, 185. [Google Scholar] [CrossRef]
- Pilloni, G.; Charvet, L. E.; Bikson, M.; Palekar, N.; Kim, M.-J. Potential of Transcranial Direct Current Stimulation in Alzheimer’s Disease: Optimizing Trials Toward Clinical Use. Journal of clinical neurology (Seoul, Korea) 2022, 18, 391–400. [Google Scholar] [CrossRef]
- Fritsch, B.; Reis, J.; Martinowich, K.; Schambra, H. M.; Ji, Y.; Cohen, L. G.; et al. Direct current stimulation promotes BDNF-dependent synaptic plasticity: potential implications for motor learning. Neuron 2010, 66, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Brunoni, A. R.; Vanderhasselt, M.-A. Working memory improvement with non-invasive brain stimulation of the dorsolateral prefrontal cortex: a systematic review and meta-analysis. Brain and cognition 2014, 86, 1–9. [Google Scholar] [CrossRef]
- Charvet, L.; Shaw, M.; Dobbs, B.; Frontario, A.; Sherman, K.; Bikson, M.; et al. Remotely Supervised Transcranial Direct Current Stimulation Increases the Benefit of At-Home Cognitive Training in Multiple Sclerosis. Neuromodulation: journal of the International Neuromodulation Society 2018, 21, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Elmasry, J.; Loo, C.; Martin, D. A systematic review of transcranial electrical stimulation combined with cognitive training. Restorative neurology and neuroscience 2015, 33, 263–278. [Google Scholar] [CrossRef]
- Gill, J.; Shah-Basak, P. P.; Hamilton, R. It’s the thought that counts: examining the task-dependent effects of transcranial direct current stimulation on executive function. Brain stimulation 2015, 8, 253–259. [Google Scholar] [CrossRef]
- Zaninotto, A. L.; El-Hagrassy, M. M.; Green, J. R.; Babo, M.; Paglioni, V. M.; Benute, G. G.; et al. Transcranial direct current stimulation (tDCS) effects on traumatic brain injury (TBI) recovery: A systematic review. Dementia & neuropsychologia 2019, 13, 172–179. [Google Scholar] [CrossRef]
- Folstein, M. F.; Folstein, S. E.; McHugh, P. R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. Journal of psychiatric research 1975, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Styliadis, C.; Kartsidis, P.; Paraskevopoulos, E.; Ioannides, A. A.; Bamidis, P. D. Neuroplastic effects of combined computerized physical and cognitive training in elderly individuals at risk for dementia: an eLORETA controlled study on resting states. Neural plasticity 2015, 2015, 172192. [Google Scholar] [CrossRef] [PubMed]
- Beschin, N.; Urbano, T.; Treccani, B. RIVERMEAD BEHAVIOURAL MEMORY TEST – THIRD EDITION (Adattamento Italiano); 2013.
- Monaco, M.; Costa, A.; Caltagirone, C.; Carlesimo, G. A. Forward and backward span for verbal and visuo-spatial data: standardization and normative data from an Italian adult population. Neurological sciences: official journal of the Italian Neurological Society and of the Italian Society of Clinical Neurophysiology 2013, 34, 749–754. [Google Scholar] [CrossRef]
- Zappalà, G.; Measso, G.; Cavarzeran, F.; Grigoletto, F.; Lebowitz, B.; Pirozzolo, F.; et al. Aging and memory: Corrections for age, sex and education for three widely used memory tests. The Italian Journal of Neurological Sciences 1995, 16, 177–184. [Google Scholar] [CrossRef]
- Spinnler, H.; Tognoni, G. italiano per lo studio neuropsicologico dell’invecchiamento, G. Standardizzazione e Taratura Italiana Di Test Neuropsicologic; Italian journal of neurological sciences: Supplementum; Masson Italia Periodici, 1987.
- Robertson, I. H.; Manly, T.; Andrade, J.; Baddeley, B. T.; Yiend, J. “Oops! ”: performance correlates of everyday attentional failures in traumatic brain injured and normal subjects. Neuropsychologia 1997, 35, 747–758. [Google Scholar] [CrossRef] [PubMed]
- Cummings, J. L.; Mega, M.; Gray, K.; Rosenberg-Thompson, S.; Carusi, D. A.; Gornbein, J. The Neuropsychiatric Inventory: comprehensive assessment of psychopathology in dementia. Neurology 1994, 44, 2308–2314. [Google Scholar] [CrossRef]
- Fonte, C.; Varalta, V.; Rocco, A.; Munari, D.; Filippetti, M.; Evangelista, E.; et al. Combined transcranial Direct Current Stimulation and robot-assisted arm training in patients with stroke: A systematic review. Restorative Neurology and Neuroscience 2021, 39, 435–446. [Google Scholar] [CrossRef]
Figure 1.
Flow diagram, Representation of the study structure. Abbreviations: MotA: Motor activity + Anodal stimulation; MotS: Motorial activity + Sham stimulation; CogA: Cognitive activity + Anodal stimulation; CogS: Cognitive activity + Sham stimulation.
Figure 1.
Flow diagram, Representation of the study structure. Abbreviations: MotA: Motor activity + Anodal stimulation; MotS: Motorial activity + Sham stimulation; CogA: Cognitive activity + Anodal stimulation; CogS: Cognitive activity + Sham stimulation.
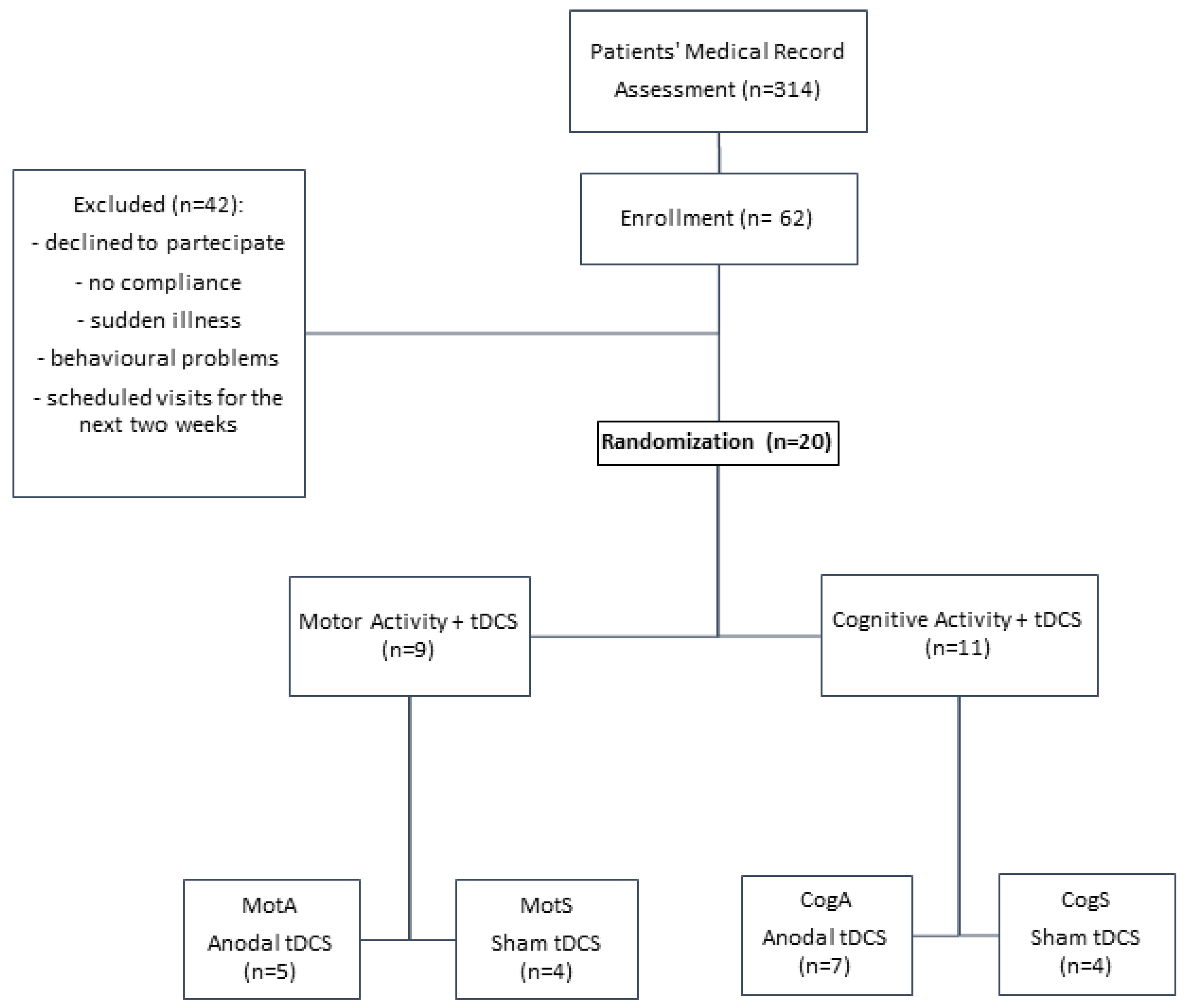

Table 1.
Demographic and clinical data. Data are given as mean ± standard deviation. Abbreviations: MotA: Motor activity + Anodal stimulation; MotS: Motorial activity + Sham stimulation; CogA: Cognitive activity + Anodal stimulation; CogS: Cognitive activity + Sham stimulation, MMSE: Mini Mental State Examination.
Table 1.
Demographic and clinical data. Data are given as mean ± standard deviation. Abbreviations: MotA: Motor activity + Anodal stimulation; MotS: Motorial activity + Sham stimulation; CogA: Cognitive activity + Anodal stimulation; CogS: Cognitive activity + Sham stimulation, MMSE: Mini Mental State Examination.
| CogA | CogS | MotA | MotS | Baseline comparison p value |
|
|---|---|---|---|---|---|
| Numbers | 7 (3♂/4♀) | 4(2♂/2♀) | 5(1♂/4♀) | 4(2♂/2♀) | |
| Age (years) | 78 ± 11 | 81 ± 5 | 85 ± 5 | 88 ± 3 | .195 |
| Education (years) | 8 ± 3 | 8 ± 3 | 8 ± 6 | 8 ± 4 | .892 |
| Time from onset (years) | 3 ± 2 | 3 ± 4 | 4 ± 4 | 4 ± 3 | .753 |
| MMSE (0-30) | 19.7 ±4.7 | 20.7 ± 6.2 | 19.6 ± 4.1 | 18 ± 3.2 | .947 |
| Pharmacological treatment | |||||
| Cholinesterase inhibitors | 4 | 1 | 4 | 2 | |
| Antipsychotics | 0 | 1 | 2 | 0 | |
| Antidepressant | 4 | 1 | 2 | 1 | |
| Benzodiazepines | 2 | 0 | 2 | 2 | |
| Hypertension medications | 4 | 3 | 3 | 1 | |
| Proton pump inhibitors | 2 | 2 | 1 | 0 | |
| Cholesterol medications | 1 | 1 | 1 | 0 | |
| Diuretics | 0 | 1 | 1 | 2 | |
| Comorbidity | |||||
| Hypertension | 4 | 2 | 1 | 1 | |
| Diabetes | 1 | 1 | 0 | 0 | |
| Hepatic steatosis | 1 | 0 | 0 | 0 | |
| Cholesterol | 1 | 1 | 1 | 0 | |
| Cardiovascular Diseases | 0 | 0 | 1 | 1 | |
| Depression | 0 | 0 | 1 | 1 |
Table 2.
Between group comparisons of MotA+CogA vs MotS+CogS. Data are given as mean ± standard deviation. Abbreviations: MotA: Motor activity + Anodal stimulation; MotS: Motorial activity + Sham stimulation; CogA: Cognitive activity + Anodal stimulation; CogS: Cognitive activity + Sham stimulation, MMSE: Mini Mental State Examination, PR: Picture Recognition, DSF: Digit Span- Forward, DSB: Digit Span- Backward, PFT: Phonemic Fluency Test, VST: Visual Search Test, SART-FA, SART-RT, SART-OM: false allarm (FA), reaction times (RT) and Omission (OM) of Sustained Attention to Response Test, NPI: Neuropsychiatric Inventory.
Table 2.
Between group comparisons of MotA+CogA vs MotS+CogS. Data are given as mean ± standard deviation. Abbreviations: MotA: Motor activity + Anodal stimulation; MotS: Motorial activity + Sham stimulation; CogA: Cognitive activity + Anodal stimulation; CogS: Cognitive activity + Sham stimulation, MMSE: Mini Mental State Examination, PR: Picture Recognition, DSF: Digit Span- Forward, DSB: Digit Span- Backward, PFT: Phonemic Fluency Test, VST: Visual Search Test, SART-FA, SART-RT, SART-OM: false allarm (FA), reaction times (RT) and Omission (OM) of Sustained Attention to Response Test, NPI: Neuropsychiatric Inventory.
| MotA+CogA | MotS+CogS | Between-group comparisons | ||||
| T1-T0 | T2-T0 | T1-T0 | T2-T0 | T1-T0 p value (Z) |
T2-T0 p value (Z) |
|
| MMSE (0-30) | 3 ± 2.17 | 1.58 ± 2.43 | -0.25 ± 3.61 | 1.12 ± 3.18 | .042 (-2.029)* | .697 (-.389) |
| PR (0-15) | 3.25 ± 3.72 | 1.58 ± 4.12 | 2.12 ± 2.23 | -0.87 ± 2.75 | .558 (-.585) | .212 (-1.247) |
| DSF | -0.16 ± 0.94 | -0.33 ± 1.07 | -0.5 ± 0.75 | -0.37 ± 0.74 | .439 (-.774) | .738 (-.335) |
| DSB | 0.33 ± 0.78 | -0.08 ± 0.67 | -0.12 ± 0.83 | -0.25 ± 1.28 | .242 (-1.169) | .537 (-.617) |
| PFT | 7.08 ± 3.34 | 3.5 ± 11.71 | 2 ± 7.54 | 2.62 ± 8.12 | .062 (-1.864) | .817 (-.232) |
| VST (0-60) | 5.58 ± 2.87 | -0.25 ± 6.55 | -0.37 ± 8.81 | 1.25 ± 5.52 | .012 (-2.515)* | .642 (-.456) |
| SART-FA | -0.7 ± 2.36 | 0.82 ± 4.64 | 6 ± 6.05 | 3.57 ± 7.59 | .012 (-2.504)* | .441 (-.771) |
| SART-RT | -43 ± 89. 01 | 5.27 ± 135.14 | 10 ± 125.41 | 57.14 ± 142.39 | .354 (-.928) | .683 (-.408) |
| SART-OM | -38.9 ± 46.17 | -32.09 ± 51.75 | -47.14 ± 67.58 | -47.28 ± 79.46 | .495 (-.683) | .618 (-.498) |
| NPI (0-144) | -4.82 ± 6.01 | -5.83 ± 6.98 | -1 ± 1.07 | -7.12 ± 7.59 | -112 (-1.591) | .846 (-.194) |
Table 3.
Between group comparisons of MotA vs CogA. Data are given as mean ± standard deviation. Abbreviations: MotA: Motor activity + Anodal stimulation; MotS: Motorial activity + Sham stimulation; CogA: Cognitive activity + Anodal stimulation; CogS: Cognitive activity + Sham stimulation, MMSE: Mini Mental State Examination, PR: Picture Recognition, DSF: Digit Span- Forward, DSB: Digit Span- Backward, PFT: Phonemic Fluency Test, VST: Visual Search Test, SART-FA, SART-RT, SART-OM: false allarm (FA), reaction times (RT) and Omission (OM) of Sustained Attention to Response Test, NPI: Neuropsychiatric Inventor.
Table 3.
Between group comparisons of MotA vs CogA. Data are given as mean ± standard deviation. Abbreviations: MotA: Motor activity + Anodal stimulation; MotS: Motorial activity + Sham stimulation; CogA: Cognitive activity + Anodal stimulation; CogS: Cognitive activity + Sham stimulation, MMSE: Mini Mental State Examination, PR: Picture Recognition, DSF: Digit Span- Forward, DSB: Digit Span- Backward, PFT: Phonemic Fluency Test, VST: Visual Search Test, SART-FA, SART-RT, SART-OM: false allarm (FA), reaction times (RT) and Omission (OM) of Sustained Attention to Response Test, NPI: Neuropsychiatric Inventor.
| MotA | CogA | Between-group comparisons | ||||
| T1-T0 | T2-T0 | T1-T0 | T2-T0 | T1-T0 p value (Z) |
T2-T0 p value (Z) |
|
| MMSE (0-30) | 4.2 ± 2.58 | 0.8 ± 2.86 | 2.14 ± 1.46 | 2.14 ± 2.11 | .098 (-1.653) | .409 (-.825) |
| PR (0-15) | 5.2 ± 4.71 | 4.8 ± 3.56 | 1.85 ± 2.26 | -0.71 ± 2.81 | .140 (-1.477) | .027 (-2.212)* |
| DSF | -0.2 ± 0.44 | -0.8 ± 0.83 | -0.14 ± 1.21 | 0 ± 1.15 | 1.0 (.000) | .265 (-1.116) |
| DSB | 0.4 ± 0.89 | 0.2 ± 0.83 | 0.28 ± 0.75 | -0.28 ± 0.48 | .927 (-.091) | .234 (-1.190) |
| PFT | 8.4 ± 2.79 | 10 ± 14.10 | 6.14 ± 3.57 | -1.14 ± 7.64 | .220 (-1.227) | .165 (-1.388) |
| VST (0-60) | 4.4 ± 2.70 | -0.8 ± 2.58 | 6.42 ± 2.87 | 0.14 ± 8.59 | .412 (-.821) | .684 (-.407) |
| SART-FA | -0.25 ± 3.30 | -0.25 ± 4.19 | -1 ± 1.78 | 1.42 ± 5.09 | .828 (-.217) | .569 (-.570) |
| SART-RT | -15.25 ± 66.44 | 115 ± 132.63 | -61.5 ± 102.89 | -57.42 ± 95.02 | .670 (-.426) | .047 (-1.989)* |
| SART-OM | -39.25 ± 19.17 | -9.75 ± 61.16 | -38.66 ± 60.13 | -44.85 ± 45.49 | .522 (-.640) | .345 (-.945) |
| NPI (0-144) | -6 ± 8.45 | -7.2 ± 9.14 | -3.83 ± 3.54 | -4.85 ± 5.55 | 1.0 (.000) | .684 (-.407) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



