
Submitted:
25 July 2024
Posted:
26 July 2024
You are already at the latest version
Abstract
The emergence of antimicrobial resistance (AMR) Candida auris presents a formidable global health challenge, causing severe healthcare-associated infections with high mortality rates. Its ability to colonize surfaces and resist standard disinfectants undermines traditional hygiene practices, prompting an urgent need for novel strategies. Ultraviolet C (UVC) light offers a promising approach due to its rapid and broad-spectrum germicidal efficacy. This review comprehensively examines the current knowledge of UVC LED technology in combating C. auris, highlighting its effectiveness, limitations, and potential applications in healthcare hygiene. UVC light has potent activity against C. auris, including multidrug-resistant (MDR) strains. UVC can reduce C. auris on contaminated surfaces, aiding in transmission prevention. This review explores implementation strategies, including mobile UVC systems for targeted disinfection of high-risk areas and equipment, integration into air handling units (AHUs) to continuously disinfect recirculating air, and incorporation into water treatment systems. Current limitations in our understanding of UVC safety and effectiveness necessitate further research to optimize application protocols and ensure treatment safety while maintaining efficacy against C. auris. Integrating UVC disinfection technology into infection control programs holds promise for strengthening hygiene practices that will curb the global spread of C. auris and improve patient outcomes.
Keywords:
Antimicrobial resistance
; Candida auris
; Global Spread
; High Mortality Rates
; Hospital Infections
; Superbug
; UVC Light
; Hospital Waste Management
1. Introduction
Antimicrobial Resistance
Antimicrobial resistance (AMR) poses a significant threat to global health and economic development, with emerging pathogens like Candida auris (C. auris) sparking particular concern. AMR is characterized by microorganisms (bacteria, viruses, fungi, and parasites) resisting the effects of antimicrobial medications that they were once susceptible to, rendering them ineffective [1,2,3,4]. This phenomenon significantly threatens human health with rising attributable morbidity, mortality, and healthcare costs [5,6]. In recent years, the emergence of multidrug-resistant (MDR) pathogens, which are resistant to multiple classes of drugs, has intensified the danger of microbial spread and infection [7]. In response to the global public health threat due to AMR, the World Health Organization (WHO) convened a global tripartite in partnership with the Food and Agriculture Organization of the United Nations (FAO) and the World Organization for Animal Health (WOAH) to monitor and evaluate global progress on AMR [8,9]. The spread of AMR and fungal diseases is further complicated by the rapid rise in healthcare-associated infections (HAIs), which now constitute the most common adverse patient events [10]. Other contributing challenges include the non-uniform surveillance and monitoring systems for AMR across geopolitical locations, cross-sector and multi-industry siloes, non-uniform policies, and resource disparities to build and maintain the infrastructure needed to sufficiently address AMR [8].
Candida auris
Candida auris is a member of the candida genus, which colonizes the skin more than other mucosal surfaces like the gastrointestinal system, leading to potential person-to-person transmission [11]. C. auris has been in the media spotlight due to frequent infections with poor prognosis among compromised hosts and its persistent antifungal resistance compared to other Candida species. While cases of C. auris have been on the rise since the first accurately identified case in Japan in 2009, there has been a rapid spike in global cases recently [12]. Media attention to the active outbreaks across the United States (Washington, Nevada, Illinois, and New York) in early 2024 has raised alarm bells for healthcare and public health officials [13,14,15,16,17,18]. Some savvy social media users have even dubbed the emerging crisis the “Candida auris fungus 2024 pandemic” [19]. C. auris is currently the only fungal pathogen identified by the Centers for Disease Control and Prevention (CDC) as an urgent threat by the Mycotic Diseases Branch [20,21].
While most reports suggest that C. auris infections are not a threat to healthy individuals, vulnerable populations and healthcare facilities are at high risk for adverse outcomes. Nosocomial infections, also called hospital-acquired infections or healthcare-associated infections (HAIs), are associated with the worst outcomes for C. auris clinical infection, with expert consensus advising that C. auris-associated candidemia (Candida-related blood infections) and subsequent sepsis could contribute to crude mortality rates as high as 72% in hospitals and residential healthcare facilities [10,22]. Despite the remarkably high mortality rate, there are very few effective drugs against C. auris due to the growing AMR and (well-meaning) misuse of antibiotics and antifungals [23]. C. auris is also an opportunistic fungus with frequent outbreaks overlapping with other pathogenic spreads, such as COVID-19. A recent retrospective chart review at one of NYC’s largest hospitals found that C. auris incidence tripled during the COVID-19 pandemic [18].
Despite recent attention, including media coverage, public health advisories, and even heightened scholarly work on C. auris (annual publication and citation growth rate of nearly 38%), implementing robust prevention and disinfection practices to reduce the overall burden of C. auris presents substantial challenges [24]. Poor surveillance and non-uniform screening practices contribute to the continued spread [15,25]. However, once C. auris is colonized (presence of fungus on the skin, but without any clinical infection), there are no specific interventions that reduce or eliminate colonization [26]. While a few medications have an efficacious impact on C. auris, early detection and treatment are imperative for optimal outcomes. Early treatment is often prohibitive without standardized and uniform screening and surveillance [23].
Environmental Disinfection
Considering the challenges of identifying and treating C. auris colonization and infection, primary prevention through environmental disinfection may be the most promising method for reducing nosocomial spread. However, effective environmental disinfection also faces substantial challenges in implementation [26]. Infection control strategies span from environmental disinfection of contaminated areas (water, air, and surface) to appropriate waste management strategies. Current environmental infection control procedures focus almost entirely on manual cleaning and chemical disinfection [26]; however, this is not 100% effective against C. auris and leaves substantial room for nosocomial spread. Current waste management strategies emphasize segregation, transport, and disposal procedures but often fail to properly disinfect and sanitize waste contaminated with highly pathogenic microbes such as C. auris.
UVC LED Technology
The resilient and antimicrobial-resistant nature of C. auris poses significant challenges to adequate disinfection protocols in healthcare settings. No-touch disinfection is a critical disinfection modality for the management of C. auris outbreaks and the reduction of the global candidemia burden. No-touch disinfection includes Ultraviolet C light emitting diodes (UVC LED) disinfection or vaporized hydrogen peroxide systems used for terminal cleaning and disinfection procedures [27]. UVC technology is a validated disinfection modality for water, air, and surface applications, and the UVC spectrum (200 – 280 nm) offers enhanced germicidal disinfection when used in conjunction with common chemical cleaning agents [28,29,30,31,32,33,34,35]. UVC LED technology can inactivate microbes and pathogens because the intracellular structures, like DNA/RNA and proteins, are susceptible to the specific density of UVC photons that are emitted in a controlled environment, causing critical genomic damage that mainly occurs through a disruption in the adenine-to-thymine bond, resulting in a pyrimidine dimer between the adenines. Damage to the cell structures prevents the microbes from replicating and limits survival times substantially [30,31,36,37,38]. Despite genetic damage to pathogenic cells, UVC is considered safe for human cells and DNA/RNA up to a specific energy exposure (though shielding may be necessary for direct human exposure) [39,40,41]. Tailored UVC wavelengths, time, and other parameters of the disinfection mechanism vary by microbe or pathogen, environmental application (i.e., water, air, and surface), and specific conditions of the contaminated element. The most common UVC wavelength used for healthcare disinfection is 253.7 nm emitted by low-pressure mercury lamps, as this is absorbed by microbial cell structures, allowing for targeted DNA/RNA damage.
Waste Management
Effective waste management is a critical component of controlling the spread of C. auris in healthcare facilities. Implementing robust waste management practices alongside proper patient care protocols is crucial to protect healthcare workers and patients from this emerging fungal threat. Healthcare wastes are generated within healthcare facilities, research centers, and laboratories related to medical procedures, with considerable potential for microbial contamination and transmission. It is estimated that between 75% and 90% of all healthcare waste is generalized and non-hazardous, with the remaining 10% to 25% considered hazardous and may cause environmental or health risks [42]. Hazardous waste covers a wide range of materials, including pathological waste, sharps waste, chemical waste, pharmaceutical waste, cytotoxic waste, radioactive waste, and infectious waste [43]. Improper waste management practices can facilitate the spread of C. auris through contact with contaminated waste by healthcare workers, and environmental contamination in healthcare facilities [44].
Infectious waste may contain pathogens (including fungi like C. auris) capable of causing disease in susceptible hosts and may include waste contaminated with blood or body fluids, cultures, and stocks of infectious agents from laboratory work, and waste from infected patients in isolation wards [42]. Microorganisms in a reservoir (such as an inanimate object) may exit the reservoir via a suitable mode of transmission (such as through droplets or contact) and gain entry to infect the susceptible host [45]. This transmission pathway further explains how C. auris can easily spread throughout and beyond healthcare facilities. High-income countries, on average, generate 0.5 kg of hazardous waste per hospital bed per day, while low-income countries generate 0.2 kg per hospital bed per day [43]. Despite the importance of safe and adequate healthcare waste management, 2019 data showed that one in three healthcare facilities globally does not safely manage healthcare waste [46].
Traditionally, waste management relies on methods like chemical disinfection or incineration. While effective, these methods have drawbacks: chemicals can pose environmental and health risks, and incineration can contribute to air pollution [47]. UVC LEDs offer a promising alternative for waste management, providing a safe and environmentally friendly disinfection method. UVC LEDs can be adapted for various waste streams, including healthcare waste, food waste, and wastewater, offering a broader application than some traditional methods.
While UVC LEDs offer a compelling alternative for waste management, there are still challenges to overcome for widespread adoption:
- a.
- Safety Concerns: UVC light can cause damage to skin and eyes upon direct exposure. Implementing proper safeguards, like protective equipment, engineering controls (enclosed systems), and training for workers is essential.
- b.
- Limited Penetration Depth: UVC light has limited ability to penetrate through materials. This means that for effective disinfection, waste needs to be spread out in a thin layer or the UVC source needs to be strategically placed to ensure all areas are exposed.
- c.
- Efficacy for Complex Waste Streams: The effectiveness of UVC LEDs may vary depending on the type of waste and the presence of organic matter that can shield microorganisms from the UVC light. Further research is needed to optimize UVC LED application for different waste compositions.
- d.
- Long-Term Performance and Maintenance: The long-term effectiveness of UVC LEDs can be impacted by factors like aging and dust accumulation. Regular maintenance and monitoring of UVC LED systems are crucial to ensure consistent disinfection performance.
- e.
- Regulatory Landscape: Regulations governing the use of UVC LEDs for waste disinfection may vary by region. Staying updated on relevant regulations and obtaining necessary approvals is essential.
Enhanced Infection Prevention and Control
UVC LEDs may be a feasible and scalable method for environmental disinfection with technical applications in water, air, surface, and waste disinfection [48,49,50,51,52,53,54,55,56,57]. This review provides a comprehensive analysis and critical discussion of the relevant literature on the global public health threat and economic disruption relative to the rapid spread of C. auris, the feasibility of applying UVC LED disinfection technology to environmental services and waste management strategies in healthcare facilities, and the challenges to implementing robust infection prevention protocols and surveillance systems. We offer recommendations for scalable and affordable UVC LED-enhanced disinfection protocols and briefly discuss future research and development in the field.
2. Relevant Literature
Due to the cross-industry content, literature was obtained through reputable research databases (e.g., PubMed, Web of Science, and Dimensions) that index high-quality journals from a broad range of fields, including the physical sciences (e.g., mycology, biochemistry, biology, engineering, and physics) and applied sciences (e.g., public health, healthcare management, medicine, and economics). Search terms included (but not limited to) “Candida auris,” “C. auris,” “antimicrobial resistance,” “nosocomial spread,” “C. auris surveillance,” “UVC disinfection,” “healthcare facility disinfection,” and “global fungal disease burden.” Additional literature was identified by carefully reviewing appropriate articles’ citations and relevant conference presentations. Our review critically examines the evidence base for the feasibility of UVC LED disinfection and waste management of C. auris.
2.1. Global disease Threat of C. auris
Fungal diseases account for a significant global burden of morbidity and mortality. Fungal infections (including skin, nails, and hair) are estimated to impact approximately one billion people, with associated mortality rates accounting for over 1.5 million deaths annually [58]. Nearly all forms of yeast are from the Candida genus, though many are not responsible for infection or have only superficial infection capacity [59]. Ringworm, nail fungus, yeast infections (e.g., vaginal candidiasis), and thrush (e.g., oral Candida infections) are among the most common fungal infections [60]. Candidiasis is an infection caused specifically by a Candida species and can present in many infection sites; however, there are over 200 specific species [61]. The annual incidence of oral and esophageal candidiasis is estimated to be approximately 3.3 million, with the global burden of recurrent vulvovaginal candidiasis being approximately 134 million each year. Invasive candidiasis is unlike oral and vaginal candidiasis because it infects the bloodstream, brain, heart, eyes, bones, and other internal parts of the body. The annual incidence of invasive candidiasis (from any form of Candida spp.) is estimated to be approximately 750,000 [58]. Candidemia, a common healthcare-associated infection, is a specific and dangerous blood infection caused by Candida isolates with adverse outcomes [62].
C. auris is a particularly resilient branch of the Candida species that rapidly develop multi-drug resistance with morphisms specific to regional development or genetic clade [63]. To date, C. auris has been reported in over 47 countries worldwide, representing all continents except Antarctica [64]. C. auris strains have been categorized into different genomic clades: I (southern Asia), II (eastern Asia), III (Africa), IV (South America), and V (Iran), each with independent emergence, which is visualized in Figure 1. C. auris clades are revealed by genome analysis, PCR amplification of genetic loci, or mass spectrometry [65]. Despite the first isolation in 2009 (ear canal), retrospective sample testing revealed the presence of C. auris as far back as 1996 in South Korea [12]. More than 740 isolates of C. auris have now been identified [23,63,66,67,68,69,70,71,72,73,74]. Multidrug-resistant and pan-drug-resistant C. auris isolates are increasingly detected worldwide [75,76].
The rising ambient air temperatures (i.e., emerging climate change), combined with changes in avian migration patterns, farm activities, and increased urban dwellers, have created an environment that supports thermotolerant fungi like C. auris [67,77]. Since first being identified in Japan, C. auris has become a globally transmitted pathogenic infection that often leads to invasive candidemia and invasive candidiasis of the heart and central nervous system [78,79]. In 2016, the Centers for Disease Control and Prevention (CDC) identified the first reported case of a patient in the United States with C. auris, discovered via a misidentified isolate collected in 2013 [80]. C. auris has been identified in several infection sites and bodily fluids, including blood, urine, bile, ear canal, nares, axilla, skin, and, in rare instances, the oral, esophageal, and gut mucosa [63].
C. auris has gained notoriety due to its increasing resistance to common antifungal agents and the possibility that it may be the first fungal disease related to emerging climate change [67,77]. Many C. auris strains have a high minimum inhibitory concentration (MIC) towards antifungal drug classes and common disinfectants, contributing to the challenge of decolonization and the treatment of infections [51,63]. Its pathogenicity has been associated with virulent traits like the production of proteases, lipases, mannosyltransferases, oligopeptides, siderophore-based iron transporters, and biofilm formation. These virulent traits assist C. auris in invading, colonizing, and acquiring nutrients from the host [11]. Further, C. auris has the capability of transforming into a persistent yeast capable of surviving under unfavorable conditions [11,61,81,82].
Once C. auris colonizes and progresses to invasive candidiasis or candidemia, several molecular mechanisms can evade the action of antifungals, leading to resistance to agents like amphotericin B and the Azole and Echinocandins classes of drugs. Azole (e.g., fluconazole) resistance is associated with the overexpression of drug efflux pumps belonging to ATP Binding Cassette (ABC) and Major Facilitator Superfamily (MFS) transporters and encoding alterations of the ergosterol synthesis pathway (overexpression of ERG11, and point mutations in ERG11, Y132F or K143R). The Echinocandin resistance in C. auris is shown to be attributable to mutations of FKS1, a gene that codes the enzyme responsible for the key fungal cell wall component, β(1,3)D-glucan. Single nucleotide polymorphisms in genes related to the ergosterol synthesis pathway leading to altered sterol composition and potential amino acids substitution in the FUR1 gene (i.e., F211I) have been linked to C. auris resistance to polyenes (e.g., amphotericin B) and nucleoside analogs (e.g., flucytosine) respectively [61,83,84,85,86,87,88]. In addition to the multidrug resistance, C. auris can survive on surfaces, including human skin, for extended periods, contributing to high mortality rates (30-60%) in healthcare settings [63,64,89,90]. Difficulties in pathogen identification and disinfection have also led to increased transmission and delayed infection management [11,61,81,82].
While antifungals may be used to treat invasive candidiasis due to C. auris, multidrug-resistant and pan-drug-resistant isolates are rapidly being identified across the globe [78]. The near-simultaneous emergence of multi-drug resistant C. auris on multiple continents, as well as the associated high mortality rate, make C. auris a significant global threat [91]. The changing climate trending towards warmer global temperatures is not enough to fully explain the rapid ability to develop resistance to antifungals [67]. More concerning is that many MDR C. auris outbreaks have no direct epidemiological links, indicating they are developing new resistance in each cluster [92]. In 2022, the World Health Organization listed C. auris on the ‘WHO fungal priority pathogens list’ in the critical priority group, urging global action on three priority areas: (1) surveillance, (2) research & development and innovation, and (3) public health interventions [78]. In 2018, the CDC made C. auris a nationally notifiable infectious disease [93].
The global incidence rate of C. auris infections cannot currently be established due to a lack of uniform surveillance systems, few epidemiological outbreak studies, and limited diagnostic capability [78]. Conventional laboratories often misidentify C. auris as one of several similar isolates, such as other Candida species like C. haemulonii, C. famata, and C. sake, as well as Rhodotorula glutinis, R. mucilaginosa, and Saccharomyces species [25,94]. While accurate incidence rates are challenging to estimate, individual studies and health systems across the globe have evaluated incidence through outbreak investigations. Studies across Asia, Europe, the Middle East, Africa, Australia, and the Americas have examined colonization, progression to IC and candidemia, and specific antimicrobial resistance [12,79,91,95,96,97,98,99,100,101]. Du et al. (2020) estimate that there are over 400,000 candidemias (bloodstream infections) each year across all species, with a global mortality rate higher than 40%; however, other studies have estimated mortality rates up to 60% [102].
In the United States, the CDC reported 1,747 confirmed clinical cases across 26 states and DC, with 95% of cases occurring in population-dense states (i.e., New York, Illinois, New Jersey, California, and Florida) by the end of 2020 [80]. This rapid escalation continued in the US, with over 3200 active cases accumulated between 2019 – 2021, which rose from a 45% case increase in 2019 to a 95% case increase in 2021, with a three-fold increase in AMR cases [103]. Following this trend, the CDC reported 2,377 clinical cases and 5,754 screening cases of C. auris in 2022 [20]. These rates are widely thought to be under-reported due to a lack of robust surveillance systems and non-uniform screening protocols [15].
While incidence rates may be underreported or unreliable, disease burden has been tracked more frequently. The median length of hospital stay for adult patients identified with C. auris candidemia was 46-68 days (70-140 days for pediatric patients) (WHO, 2022). Researchers and hospital investigation teams more frequently report mortality rates; however, rates related to IC and candidemia vary significantly across the globe as noted in Table 1. Since the emergence of C. auris, mortality rates reported for candidemia have been quite high, nearing 50% of diagnosed infections [63]. Further complicating accurate surveillance and monitoring is that misidentification of Candida species also extends to mortality reporting errors. Mortality rates are often reported only for candidemia or IC, without species attribution [104].
2.1.1. Vulnerable Populations
While invasive candidiasis and other infections from C. auris are not thought to pose a significant threat to healthy people even if colonization occurs, vulnerable populations are often unprotected and unable to successfully clear the infection without intensive therapies [110]. Invasive candidiasis and candidemia are nosocomial infections that can disproportionately impact the critically ill, immunocompromised, elderly, and patients with extensive comorbidities or a history of frequent antimicrobial therapy [12,23,63,78,111]. Patients with indwelling medical devices (e.g., central venous catheters), patients using parenteral nutrition, patients on mechanical ventilation, and hospital admissions longer than 10-15 days are among the most at risk for adverse outcomes [78]. Underlying respiratory and/or cardiovascular illness, vascular surgery, prior antifungal exposures, and low APACHE II score (ICU-based severity-of-disease classification system) are considered significant risk factors associated with C. auris candidemia and poor prognosis [63,112]. Nosocomial outbreaks of invasive candidiasis (C. auris-specific) in intensive care (ICU) settings are common, especially where colonization on non-human hosts has been previously identified [94]. In an analysis of 27 ICUs in India, where 1,400 candidemia cases were reported, over 5% were attributed to C. auris [112]. Rudramurthy et al. (2017) also found that patients with C. auris candidemia had longer ICU admissions prior to diagnosis than other microbial infections, indicating that nosocomial spread contributed to fungal outbreaks in India [78]. It is estimated that unless substantial actions to address AMR infections are taken, nearly 10 million people will die annually by 2050 [113,114].
Annually, over 2 million children die globally before their first month of life [115,116], with infection as one of the top three most prevalent causes (along with prematurity-related complications and intrapartum-related complications) [116,117]. Candida species are responsible for the greatest number of neonatal invasive fungal infections [117]. The most common Candida species affecting pediatric populations are C. albicans, C. parapsilosis, C. glabrata, and C. krusei [118]; however, C. auris is now impacting pediatric populations as well. In a prospective cohort study of hospitalized infants (<60 days postnatal age with sepsis) in Low and Middle-Income Countries (LMICs) at 19 hospitals across 11 countries, researchers found C. auris to be the third most commonly reported pathogen [3,4,117,118,119]. In South Africa, C. auris was among the 5th most common Candida species responsible for candidemia [120]. In India, of 273 neonates from three hospitals with neonatal invasive candidiasis (NIC) cases, investigators isolated C. auris in 2.2% of the cases, highlighting the vulnerability and susceptibility of infants in LMICs [121].
The crude mortality rate associated with NIC varies significantly, unsurprisingly, with higher rates disproportionately impacting LMICs compared to high-income countries (HIC) (8.9%-75% in LMIC and 12%-37% in HIC) [117]. Risk factors for neonates developing NIC or candidemia include preterm birth, older infants and children with ICU stays, post-surgical stays, underlying malignancies, malnourishment or requiring parenteral nutrition, post-solid organ transplantation, an underlying renal disease requiring hemodialysis, central venous catheter placement, and requiring respiratory support [118,119]. A case study in Italy found that an extremely low birth weight preterm neonate born via vaginal delivery from a C. auris colonized mother was colonized within only a few hours after birth [122]. Though limited by the ability to clearly determine if the colonization route was the birth canal or the ICU environment, this case does highlight the heightened risk for already vulnerable infants to C. auris [122].
2.1.2. Economic Impact
AMR is a significant and global threat to public health and the successful clinical management of microorganisms [2,6]. Economic simulations run by the World Bank suggest that by 2050, with an optimistic (i.e., low) AMR impact, the annual global gross domestic product (GDP) could fall by approximately 1.1%, with GDP shortfalls exceeding $1 trillion annually after 2030. Less optimistic simulations (i.e., high AMR impact) predicted a 3.8% decline in annual GDP by 2050, with an annual shortfall of $3.4 trillion by 2030 [123]. The predicted impact of AMR is likely to disproportionately impact low-income countries and increase the rate of poverty [123]. The total economic burden of fungal diseases and AMR in the US is thought to be dramatically underestimated [59,124]. The financial burden can be estimated as a total burden or pared down to direct costs, loss of productivity costs, premature death costs, costs per patient, and costs per hospitalization. In the absence of a standard reporting mechanism, economic burden is not always consistent across reports. Table 2 provides an overview of the estimated global economic burden for all AMR diseases, fungal diseases, and candidiasis/candidemia specifically.
2.2. Public Health Pandemonium – AMR and Nosocomial Spread of C. auris
2.2.1. Public Health Prevention
Global public health initiatives often fall into three categories: primary, secondary, and tertiary prevention methods. Tertiary (treating infections before spread) and secondary prevention (screening for colonization and early infection of common pathogens) are common protocols for addressing AMR; however, the most effective form of public health prevention is primary prevention (stopping transmission of the pathogen before colonization). The WHO Tripartite Global Action Plan Objective Three (GAPO 3) is specifically aimed at primary prevention by reducing infection through adequate sanitation, hygiene, and infection prevention measures [8]. GAPO 3 urges participating countries to develop or implement robust action plans for infection prevention and control through enhanced waste management and improved WASH conditions (water, sanitation, and hygiene), among other priorities.
Multidrug-resistant C. auris is increasingly becoming a challenge for successful clinical intervention [127]. AMR is closely linked to misguided and clinically ineffective prescribing practices of antibiotics and the increased presence of antibiotics in food sources such as farm-raised meats [128]. Global estimates suggest that AMR and MDR infections are directly responsible for over 1.2 million deaths and are a contributory factor in nearly 5 million deaths each year, with a concerning annual upward trend [78]. Even more concerning is the burden of AMR-related deaths falls heaviest on resource-limited settings. AMR and basic antifungal stewardship programs, often absent or insufficient in resource-limited regions, are critical in addressing this global health threat [78]. Guided by the similar principles of standard antibiotic stewardship programs that suggest effective diagnostic tools and encourage empirical antibiotic use, antifungal stewardship aims to protect the effectiveness of antifungal therapy in the future [127]. Antifungal stewardship programs must be tailored to the specific resources and capacity of each healthcare institution and health system. Key elements common in all antifungal stewardship programs include guidelines for diagnostic tests to inform therapy initiation and withdrawal, specialist consultation, identification of provider knowledge gaps and coinciding education, and implementation of prescribing restrictions when specialized infectious disease support is available [129]. In many healthcare institutions, especially in developing countries, the resources, capacity, and specialized health workforce required to create and operationalize effective antifungal programs may be limited. Lack of access to diagnostic tests and delayed results, and unavailability of C. auris low-resistance antifungal (e.g., echinocandins, which have limited availability in many countries despite designation as a WHO essential medicine) make effective antifungal stewardship challenging in many resource-limited health systems [78,127].
The lack of accurate screening and non-uniform testing protocols significantly contributes to the rising spread of AMR pathogens. Detecting C. auris is particularly challenging due to the over 700 isolates and limited laboratory testing capabilities [23]. Labs often misidentify C. auris as another Candida species due to common multiplex testing mediums that lack the sensitivity and accuracy to detect specific strains of C. auris. Hospitals, healthcare facilities, and clinical labs have no standard testing protocols or procedures with tests ranging from differential or selective media, mass spectrometry, and real-time PCR (polymerase chain reaction) tests. Each test varies in sensitivity and accuracy, as well as the associated need for precision in implementation, sensitivity to tester variation, and cost for scaled testing [130]. Rapid and accurate testing for C. auris colonization on surfaces, in water, and in human hosts is critical. In addition to identifying the C. auris colonization or infection, labs need the capacity and standardized protocol to complete pathogen genomic analysis and antimicrobial resistance testing to determine the best action for remediation. Enhanced screening protocols play a significant part in outbreak investigations and rapid remediation, particularly in reducing nosocomial spread [130].
Effective infection prevention control measures to prevent the transmission of C. auris must include strategies that consider demonstrated transmission pathways, including isolation of patients and contacts, wearing personal protective equipment, routine screening of patients, skin decontamination, environmental cleaning, and terminal decontamination [100,102,131]. Source control of C. auris should include disinfection of commonly identified surfaces where C. auris is colonized (mattress, bed rail, bedside tables, ventilators), aseptic removal of intravascular catheters, and adequate drainage and disposal of biological material. Biswal et al. noted that C. auris could be reduced by the most common hospital chemical disinfectants if adhering to the proper concentrations and contact time; however, these protocols are challenging to meet in understaffed and under-resourced ICUs [132].Terminal cleaning with UV-C light to reduce infection of nosocomial pathogens may be effective at preventing transmission of Candida auris but may need to be a supplement to standard disinfection strategies [133,134].
2.3. Current Healthcare Environmental Infection Control Standard Procedures
The global spread of C. auris has been attributed to the easy transmission through direct or indirect contact on high-touch surfaces, air, and wastewater, the ability to survive outside of a human host, and the ability to sustain long periods of desiccation, biofilm formation, and high thermal tolerance [21,41,63,89,121,135,136,137,138,139]. Not only is C. auris highly resilient to hostile environments, but studies suggest that it is also adaptive to environmental stress, creating near-impossible parameters for disinfection [63]. In India, ICU patients who were not colonized with C. auris at the time of admission were later colonized during their stay [132]. After a C. auris outbreak at a London hospital, researchers found that C. auris was not isolated from any patient prior to their admission to the ICU [100]. Once the patient’s skin is colonized, transmission can proceed via skin-to-skin contact with individuals beyond the healthcare setting [140]. Appropriate infection control protocols include identifying C. auris colonization and infections and genomic analysis to assess for AMR. However, a critical factor in infection management is adequate and scalable disinfection [104]. Given the broad range of colonization sites, disinfection and environmental health facility management is critical for water, air, and surface. Due to the cross-sector siloes, the protocols for point-of-service (e.g., patient and bed-specific cleaning in rapid rooming flips) disinfection across applications, larger healthcare facility environmental health management, and waste management are often ineffective and inefficient.
According to several pathogenic surveillance agencies (i.e., CDC, European Centre of Disease Prevention and Control, Pan American Health Organization, World Health Organization, Public Health England, and Centre for Opportunistic, Tropical and Hospital Infections in South Africa), infection prevention and control of C. auris in healthcare settings includes proper hand hygiene, transmission-based precautions (i.e., patient and room precautions to limit exposure), cleaning and disinfection, uniform screening and surveillance practices, and enhanced communication [26,104,111]. These generic and nonspecific disinfection procedures all lack the specificity for C. auris. This strategic gap in environmental C. auris mitigation to prevent nosocomial spread is apparent [39]. Each component of the infection prevention protocol is critical; however, this review focuses specifically on disinfection as a primary prevention method. Environmental disinfection and cleaning (hand hygiene products are included here; however, policies and methods of hand washing are not) in patient care and high-traffic environments is challenging and covers patient and room turnover, daily cleaning practices, mobile and high-touch equipment disinfection (e.g., blood pressure cuffs, glucometers, stethoscopes, crash carts, etc.) [26]. Standard protocols are limited by the required complex procedures to reach efficacy, availability of disinfecting agents, and end-user education. Another significant limitation is the non-standardized use of “no-touch” disinfection, such as UVC LED technology. Reliance on standard contact and air precautions for patient care of colonized individuals is not a sustainable or widely effective method. Enhanced disinfection and waste management is necessary for a robust infection prevention and control policy.
2.3.1. Water
C. auris can survive and spread through wastewater as well. A recent study in Nevada positively detected the dangerous fungus in nearly 80% of effluent samples with over 90% positivity rates near healthcare facilities [141]. Testing and surveillance of wastewater, particularly in effluent sewer sheds near healthcare facilities, can help identify and track potential outbreaks and trigger early warning alarms for public health action. Lower-resourced regions and LMICs without proper water infrastructure may also reuse wastewater after only superficial disinfection. If water treatment and disinfection strategies in these areas do not fully inactivate C. auris, public health could be compromised by transmission of the pathogen through daily WASH activities. The documented capability to produce biofilms can complicate wastewater system testing and surveillance and require more nuanced disinfection of water supplies [41,141]. The most common methods of water decontamination are chemicals (i.e., chlorination and ozonation). However, these methods generate persistent residual carcinogenic by-products (such as chlorine or bromate) [142,143,144]. Furthermore, these methods have led to new resistant microorganisms and affected the organoleptic properties of water [143,144]. No specific healthcare setting infection prevention and control protocols were found, including an absence of water testing protocols for C. auris isolates as a function of outbreak surveillance.
2.3.2. Air
Airborne transmitted pathogenic infections, which occur via droplets or aerosol, are also a common concern [145,146,147]. Coughing, sneezing, and even talking may lead to pathogen transmission, which became a critical concern during the COVID-19 pandemic. Researchers have also found a positive relationship between decontamination effectiveness and airflow conditions [148]. In poorly ventilated environments, indoor air has lower convection, leading to the environmental accumulation of pathogens and increasing the likelihood of infection [149]. C. auris can spread through contamination of air handling units (AHUs) [150]. Fungal colonies can be transmitted via aerosolized particulates with both active and passive air samples. In Tehran, air samples tested positive for the presence of fungi (C. auris was not included in the testing protocol), indicating low air quality and the need for enhanced filtration and air purification [151]. However, the lack of discriminant air particulate testing and non-uniform air sampling renders the rate of aerosolized C. auris transmission unknown. Public Health England’s efforts to address C. auris include a targeted effort to understand the transmission pathways via the aerosolized spread, particularly in healthcare settings; however, data from this ongoing study has yet to be reported [152]. No standard air purification protocols or procedures for monitoring and disinfecting air handling systems for C. auris were found.
2.3.3. Surface
C. auris can survive on surfaces for more than three weeks (wet or dry surfaces), with colony growth (up to 1 log increase) possible on wet wood surfaces [41,104,153]. Among the surfaces from which C. auris has been isolated in healthcare facilities include mattresses, bedside tables, bed rails, chairs, windowsills, ventilators, thermometers, pulse oximeters, IV poles, and ECG leads [21,26,63,100,132,154]. C. auris colonization and survival can also spread to sinks, bathrooms, cleaning buckets, computers, phones, and doors with relative ease [67]. In fact, an outbreak in Brazil during the height of the COVID-19 pandemic (March 2020) and increased infection prevention and control awareness was traced back to colonized axillary thermometers reused across patients without sufficient disinfection [154].
In surface applications, the current chemical disinfection protocols range widely by site and sector and are impacted by the MICs associated with C. auris isolates. Common disinfection wipes containing quaternary ammonium compounds (QACs) used for high-touch surfaces or in floor detergent mixtures are ineffective on the fungal strain, allowing transfer and spread of C. auris colonies to other areas [104,155]. Only a few hospital-grade disinfectants are certified by the Environmental Protection Agency (EPA) to kill C. auris (List P), and no registered products have been developed specifically for C. auris [104,156]. Three of the most common hospital disinfectants (QACs, Iodine-based, and chlorine-based) have only minimal effectiveness unless strict protocols are followed, including follow-up with ethanol-based gel sanitizers after wet-to-dry cleaning. Disinfectants without sporicidal claims were not able to inactivate C. auris [155].
While chlorine-based products were considered the most effective for superficial disinfection, strict cleaning protocols must be followed [26,39,51,104,133,157]. Even slight deviation from the established protocol diminishes effectiveness tremendously, and use in patient care areas is limited due to the caustic chemical properties and respiratory irritation [104,157]. All high-touch items and multi-use equipment, personal protective equipment, and employee items require disinfection after every use; however, when these standards are not followed, nosocomial spread increases [158]. Chemical-based cleaning agents also require accurate concentrations tailored to the specific surface for cleaning and cannot be used across varying surfaces with efficacy [12]. In environments where strict adherence to complex cleaning protocols requires nuanced chemical concentrations and specific wet and dry times before effectiveness, the window for error widens. Despite adherence to standard infection prevention and control procedures, a significant, high-mortality C. auris outbreak was identified in a European tertiary care hospital [159]. Healthcare facilities facing growing patient boarding challenges, rapid turnover of fatigued and burned-out staff, and continual cost cuts can lead to seemingly innocuous shortcuts in environmental disinfection procedures. However, even small deviations amplify the nosocomial spread of C. auris and contribute to AMR in patients who become colonized in healthcare facilities. Switching to single-patient-use materials is recommended where feasible [111]; however, this is costly and not always practical in lower-resourced facilities where the reuse of even single-use equipment is common. Healthcare facilities overburdened with patients and have limited human and resource capacity often use less than ideal infection control procedures, leading to C. auris outbreaks [67,158].
Further complicating surface colonization and resistance to disinfection is the proclivity for biofilm formation. Biofilms can form around the exterior of fungal (and other microbial) colonies on plastics, steel, poly-cotton, and other high-touch surfaces, including on dampness-prone skin niches (e.g., sweat in axillary regions) [41,160]. Biofilms may promote multi-drug resistance as the film protects C. auris from hostile environments, including dehydration and common germicides [41,98,104]. In healthcare settings, biofilm development contributes to the overall nosocomial spread and pathogenicity, particularly among medical equipment, including those with direct internal mucosal exposures (e.g., urinary and intravenous catheter tubing) [41,63,161]. When biofilm formation is present, common hospital-grade disinfectants are even less effective. Ledwoch and Maillard (2018) tested 12 commercial wipes and hypochlorite disinfectants on C. auris biofilms on stainless steel. They found that over 50% failed to decrease survival or transferability, and up to 75% failed even to delay regrowth [162].
For skin colonization, common chlorhexidine-based soaps are not widely effective through standard hand washing procedures, which may be due to biofilm formation [104,134]. Additional steps using alcohol-based sanitizers are needed to reach maximal disinfection from the skin [104]. When using alcohol-based sanitizers, at least one minute of wet contact time is necessary to achieve disinfection; however, the standard hand sanitation time for healthcare professionals is often under 15 seconds [163]. Even using optimal conditions, chlorohexidine (0.5%-4.0%) and other common alcohol disinfectants often achieve less than a 3-log10 reduction. There are no efficacy studies that demonstrate inactivation of C. auris colonization on skin with only 15 seconds of contact time [163]. No matter what chemical agent is used for disinfection, terminal cleaning should be completed at least twice daily in addition to per-patient disinfection practices [12], which adds another layer of time and capacity complexity to the infection prevention protocols.
Other less common disinfecting agents have been used with varying effectiveness. Farnesol, which is a quorum-sensing molecule, has been used to inhibit biofilm formation, similar to its properties in C. albicans, and has the capacity to reduce the expression of multi-drug resistance genes [164]. Ozone disinfection units have also been used for beds and linens with some success; however, they require long exposure times [51].
2.3.4. Waste Management
Regulated medical waste (RMW) or healthcare waste is not governed by a single regulating body, and therefore, waste management protocols vary widely by facility and region. Over time, common medical waste management strategies have included incineration, steam, microwave irradiation, mechanical, chemical, and pyrolysis [165,166]; however, disinfection and sterilization of healthcare waste have now become more common [167]. Disinfection of surgical waste is paramount for disrupting and preventing the spread of infectious diseases, such as pathogenic MDR microbes. Disease outbreaks across several countries and facilities have been traced back to an organizational failure to comply with established guidelines for medical waste [167]. Standard disinfection of medical waste using chemical disinfectants has serious challenges, including hazardous operating conditions and limited germicidal efficacy. Without proper disinfection of infectious waste, transmission across healthcare facilities and among waste workers and communities is likely [168]. Another notable challenge in LMICs is that increased diagnostic testing has generated a rise in healthcare waste that was not accounted for during implementation planning. Many of the facilities and even governments of LMICs were not prepared to be held accountable for adequate waste management strategies, strongly calling for strategies that required lower resources, costs, and technical expertise [169].
Fundamental principles for the appropriate management of hazardous waste to safeguard public health and environmental protection have been established through several international agreements, including [170]:
- The Basel Convention on the Control of Transboundary Movements of Hazardous Waste and Their Disposal minimizes the generation of hazardous wastes, the treatment of waste close to where it was generated, and the transboundary movement of hazardous waste.
- The Bamako Convention is a treaty with well over a dozen signatories that bans the importation of hazardous wastes into Africa.
- Polluter Pays Principle - the producer of waste is legally and financially liable for disposing of waste in a manner safe for people and the environment.
- Precautionary Principle - When risk is uncertain, it must be regarded as significant.
- Proximity Principle - Hazardous waste must be treated and disposed of as close as possible to where it was produced.
As improved healthcare access and technological advancements have grown exponentially, the need for enhanced waste management has also risen. Infectious disease outbreaks have driven the need for field testing of medical waste to identify and disrupt pathogen spread. Field indicators have been used in West African nations (Liberia & Guinea) to improve the efficacy of chlorine-based disinfection against Ebola, while modern technology (e.g., genome sequencing of contaminants for targeted disinfection) continues to be applied for contemporary standards [171]. Some facilities in Uganda and India have even designed smart waste bins to assist in the proper segregation and disinfection of infectious waste [172,173].
Incomplete disinfection and variation in medical waste management procedures can significantly contribute to the spread of infectious diseases. Within the context of national healthcare systems, active governmental intervention can help establish and operationalize a successful and sustainable healthcare waste management system [42]. Components of the development of effective and safe healthcare waste management systems must include 1) healthcare waste management planning at the national level and at healthcare facilities, 2) waste minimization, reuse, and recycling protocols, 3) waste segregation, 4) safe storage, and transport, and 5) treatment and effective disposal of waste [42]. While these strategies are not specific to the disinfection of C. auris, a broad application of microbial disinfection of healthcare waste should be applied to serve in multi-layered protection procedures.
2.4. UVC LED Disinfection of C. auris in Healthcare Settings
UVC technology is rapidly advancing, as are the many use cases, with many potential opportunities in healthcare settings. The evidence confirms that UVC can inactivate up to 99.99% of microbial pathogens, including highly resilient C. auris. Conventional UVC disinfection uses low-pressure mercury lamps emitting light at the wavelength of 253.7 nm; however, the energy dose required to kill or inactivate resilient pathogens (e.g., C. auris) often rises quickly beyond the safe exposure levels for humans [40]. The recent emergence of UVC light-emitting diodes (LEDs) as an alternative to mercury lamps is a significant advancement. UVC LEDs can potentially provide as good or better disinfection as traditional mercury lamps but have other advantages beyond efficacy ratings [174]. Conventional mercury lamps (254 nm peak wavelength) can have high energy demands, short lifespans, cumbersome sizes, and pose potential human exposure hazards [31,175]. UVC LEDs can emit light at multiple wavelengths between 250 – 280 nm and have lower energy and voltage requirements, smaller sizes, and optics that can be tailored to microbial disinfection [31,176,177].
C. auris is susceptible to UVC inactivation; however, longer exposure times and higher doses of UVC energy are required when compared to other common Candida species (C. auris k-values 0.108 to 0.176 cm2/mJ vs. C. albicans k-values 0.239 and 0.292 cm2/mJ). In general, lower k-values were found for isolates expressing AMR properties, indicating a higher dose of UVC is necessary for the inactivation of AMR C. auris [53]. Studies have determined the optimal wavelength dose for inactivating C. auris. As shown in Table 3, Mariita et al. (2022) found that a peak wavelength sensitivity of 267–270 nm offered higher disinfection performance against multidrug-resistant C. auris. Giese and Darby (2000) also noted that wavelength sensitivities of 267 and 270 nm showed a similar effect, with the fastest inactivation rate at the average log reduction value (LRV) of 0.13 LRV/mJ−1/cm2. A linear regression analysis revealed a significant association between all arrays and their disinfection efficacy at 5, 10, 20, and 40 mJ/cm−2 while emphasizing the effectiveness of UVC emission wavelengths of 267–270 nm [54].
The applications for UVC disinfection in healthcare settings are broad. UVC LED technology can be effectively and easily integrated into protocols for water, air, surface, and waste disinfection. In fact, a systematic review of UVC germicidal inactivation found that UVC had a potent effect on microorganisms, including those with AMR, when used as an adjunct to manual chemical cleaning procedures [179]. UVC disinfection in water and water distribution systems at healthcare sites can ensure that pathogens, like C. auris, are not recycled within closed systems and can prevent transmission to water treatment facilities where wide distribution would be possible. UVC LED water reactors at treatment facilities can prevent the transmission of pathogens to community and household water sources. In air applications, UVC LED technology can be applied to air handling units and circulated air systems to enhance the purification of recirculated air. Pathogens can colonize inside air ducts, become dislodged, and then spread through circulated air and deposited on surfaces where skin contact can escalate. UVC disinfection of in-duct systems will purify and disinfect forced air, while in-room units will disinfect the circulating air between two UV sources. In surface application, mobile UVC units may provide terminal cleaning enhancements for all surfaces (particularly high-touch surfaces). Mobile units may be autonomous robots or personnel-monitored units but can disinfect manually pre-cleaned areas with a high degree of efficacy.
2.4.1. Water
UVC LED technology is a proven method for disinfecting water and wastewater, which are primary transmission sources of many gastrointestinal pathogens. Several studies have demonstrated the efficacy of UVC LED technology at inactivating microbial pathogens in water and wastewater, though few studies have specifically evaluated C. auris due to its rapid transmission via surface contact first [35,141,144,180,181,182,183,184,185,186,187,188].
Research has discovered that UVC technology has applications in disinfecting drinking water [181,182,189], rainwater disinfection [190], and food processing water management [191]. UVC LED technology in water reactors can inactivate biofilm-bound Pseudomonas aeruginosa (265nm at UV dose 8 mJ/cm2) to a 1.3 ± 0.2 log inactivation or LRV [180], pathogenic bacteria Aeromonas salmonicida and Escherichia coli (265nm at UV dose 24 mJ/cm2 and 28 mJ/cm2) to a 4.5 log reduction [35], Giardia sp. and Cryptosporidium sp. [183], and a wide range of other pathogenic microbes [33,34,143,192]. UVC LED disinfection also reduces the use of harmful chemicals and any associated risks while demonstrating efficacy at eliminating microorganisms, pharmaceuticals, and personal care product residue [193].
In addition to the disinfection of water for consumption or daily use and solid waste management, UVC may also effectively disinfect wastewater, particularly in and around healthcare facilities. Researchers isolated C. auris from wastewater, demonstrating an epidemiologic link to healthcare facilities within that wastewater treatment plant’s sewer shed in Southern Nevada, further highlighting the importance of scalable and sustainable pathogen disinfection [194]. Researchers have specifically found effective UVC disinfection for wastewater reuse [142,195,196] and sewage decontamination [197]. While chlorine-based disinfection has traditionally been used to disinfect wastewater, concerns about the impact have resulted in UVC disinfection as an alternative [42]. UVC LED water reactors are effective at eliminating microorganisms in water and wastewater using peak wavelengths between 260-270 nm, with synergistic inactivation at 260|280 nm for E. coli [28,48]. Human norovirus can be effectively inactivated in wastewater by UVC LED water reactors and scaled tertiary wastewater treatment facilities, which can integrate UVC LED Driven Advanced Oxidation Processes (AOP) to decontaminate and disinfect wastewater simultaneously [184,185]. Combined UVC LED and AOP disinfection of wastewater has also been effective at reducing medical contaminants. The combined UVC LED + H2O2 wastewater treatment system showed efficacy and efficiency for smaller-scale water treatment facilities [198].
The effectiveness of UVC-based water disinfection depends on several important operating parameters. More opaque liquids reduce UV treatment effectiveness at different levels [182,199]. Whereas water circulation and exposure time improve water decontamination effectiveness [200]. Interestingly, water volume causes a dubious effect on UVC treatment, with insignificant to slightly better performance in lower volumes [189,200]. Continuous or pulsed UVC light application provides comparable results [143]. Depending on the intended final use of the treated water, the protocols must reach different decontamination targets. For drinking water, the treatment should disinfect the surface with at least a 4-log reduction [182]. The reuse of wastewater, excreta, and greywater, on the other hand, requires at least a 3-log reduction for water disinfection [182]. Combined UV wavelengths or combining UV treatments with other methods may also have additive effects. Several studies have demonstrated that combining UV wavelengths [144,187,195,201,202] and multi-method treatment applications [142,196,203] have demonstrated synergistic effects that have improved the disinfection or decontamination process. Combining UVA and UVC [144,187,202] or UVB and UVC [186], UVC with other light sources such as excimer lamps [203], or UVC with chemical oxidants [196] all lead to synergistic effects.
A systematic review of the literature found that all examined studies achieved some level of decontamination or disinfection. Most studies achieved biological reductions of less than 3 log [144,181,186,187,201,202,204], and three studies achieved sterilization levels up to 5-6 log reduction [182,191,199]. These results give users confidence in applying UVC for its decontamination capabilities in the water. While UVC light can inactivate microbial pathogens, some pathogens can recover from the UVC decontamination effect. These microorganisms use dark repair and photoreactivation processes to recover from the UVC impact [146,186,195,205].
2.4.2. Air
UVC LED disinfection is effective at inactivating aerosolized viruses, bacteria, and fungi [145,146,147]. There is variation in how UVC technology is used to purify air of microbial contaminants, ranging from sanitizing the air circulating between UVC sources to disinfecting the surfaces of air handling units, filters, and fans to prevent re-circulation of spores [40,206,207,208]. Some studies of UVC LED air treatment have demonstrated disinfection of some, but not all, biological indicators [145,146,147], and one study achieved sterilization in part of its biological targets [148].
Forced air handling systems can incorporate UVC disinfection technology into traditional filters and interior surfaces of the fans and system (in-duct systems) to further purify the air that is dispersed into the environment. While C. auris is not part of the standard air pathogen testing array, adding UV disinfection to filters increases the log reduction of many harmful pathogens, including C. albicans [208]. The log reduction of airborne pathogens is dependent on the highly variable UV dose and standard operating parameters of each in-duct UV disinfection product [209]. Air purification systems with combined HEPA + UV disinfection technology have been found effective at sanitizing rooms up to 12 m2 in area [206]. Stand-alone UV recirculation units (or unitary UV systems) are another common application of UV air disinfection that works similarly to in-duct systems but are more compact and operate at variable air flows. These units draw air from the floor or near other high-concentration areas and then redistribute the cleaned air at breathing height [208]. A 2-log reduction of Candida spores was achieved in a 2-point circulating air sanitation cycle; however, when combining surface and air UVC disinfection in a single room, the required dose is unknown [40]. Mobile air disinfection units have shown effectiveness at eliminating C. auris from recycled air in healthcare settings using combination systems that disperse ozone into a room before sanitizing the recombinant air with UVC light [40]. The Khan-Mariita Equivalent Ventilation Model (KM Model) supplements standard mechanical ventilation with UVC air treatment, accounting for many of the previously noted variables (e.g., room size, occupancy, existing ventilation, and targeted air changes per hour) [207]. In healthcare settings (as with many other environments), it is challenging to circulate only fresh air. Therefore, recirculation of potentially contaminated air is necessary. Utilization of the enhanced KM model that integrates UVC disinfection into standard mechanical ventilation allows for increased energy efficiency, net carbon-zero requirements, and decreased dependency on outside air injection. Broad application of the principle of UVC disinfection of C. auris on surface and circulated air shines a spotlight on the potential for building systems to integrate the KM Model as a standard ventilation system, in addition to other disinfection protocols [207].
Muramoto et al. (2021) developed an air purifier that combines UVA/UVC LEDs, a HEPA filter, a honeycomb ceramics filter, and a pre-filter. In this system, the LEDs are responsible for treating the surface of the HEPA filter to decontaminate any microorganisms trapped in it, leading to the faster elimination of floating influenza viruses [210]. Researchers are also particularly interested in demonstrating how compact systems that are easy to implement in different settings are applicable to UVC LED disinfection [146,147,148,211]. Nicolau et al. (2022b) found that UVC possessed higher decontamination efficacy than ozone and was capable of achieving synergistic effects when combined with other methods.
2.4.3. Surface
Researchers have also determined UVC decontamination effectiveness on different materials, including various hard surfaces (e.g., carpet or laminate) [212], food contact surfaces [213], and recreational ball types [214]. In addition to the decontamination effectiveness, Wood et al. (2021) evaluated the relative humidity impact on the decontamination effectiveness and compared conventional UVC sources with LEDs. Trivellin et al. (2021) found that UVC light did not cause any visual changes or material degradation following disinfection. A synergistic effect from the combination of UVC treatment with mild temperatures (60 ◦C) was also found [145].
UVC disinfection is also specifically effective at inactivating C. auris on hard surfaces, which is common in healthcare settings [49,51,52,53,55,56,57,215]. The use of UVC technology as an adjuvant disinfection modality for C. auris may be an advantageous environmental mitigation strategy [26]. While there is no standard log reduction requirement for C. auris, at least a 3-log10 reduction (99.9% reduction) is suggested to most likely be clinically effective [57]. A review of several UVC exposure parameters and devices found that UVC was clinically effective against C. auris when using proper conditions [56]. In lab testing, a mobile UVC tower equipped with high-performance bulbs at the 254 nm wavelength used for a continuous 7-minute exposure period in a patient-room-sized test chamber demonstrated 99.97% inactivation of C. auris [52]. Other lab settings have found UVC technology to be an effective approach to inactivating C. auris as well [49,50,51,55]. Maslo et al. (2019) saw a 99.6% reduction after a 10-minute pulsed-xenon UV light exposure cycle at a 2-meter distance from their mobile UV device and 100% elimination after more than 15 minutes of exposure. Chatterjee et al. (2020) reported a 0.8 to 1.19 log reduction of C. auris when exposed for 30 minutes. However, despite the increased exposure time, isolates from clade III were not susceptible to inactivation in their lab testing [49]. In 2020, an experimental test at the University of Siena found a 4.43 log reduction of C. auris after 15 minutes of exposure to a novel UVC chip [50]. In a modification of the American Society for Testing and Materials (ASTM), six relatively low-cost (<$15,000 per unit) UVC devices (3 room decontamination devices and 3 UVC box devices) were tested against the suggested clinically effective 3-log10 reduction of C. auris. Three of the tested units (one room decontamination and two enclosed boxes) met all criteria for effective decontamination [216]. In a lab test, UVC exposure (267 – 270 nm) prevented C. auris biofilm growth on stainless steel and plastic and significantly reduced formation on poly-cotton fabrics [54]. The field studies branch of the Respiratory Health Division at NIOSH) found UV disinfection of C. auris was 99.9% effective but required significantly higher UV energy dose than other Candida species (C. auris 103–192 mJ/cm2 vs. C. albicans 78-80 mJ/cm2) [217].
Some studies have reported that C. auris is resistant to UVC treatment [218]; however, this seems to be a misnomer. More recent research has determined specific UVC parameters necessary for inactivation, aligning with the fungus’ propensity to respond differently to other common disinfectants and antimicrobial therapies due in part to the higher MIC and rapidly developing AMR [219]. While UVC inactivation efficacy is reduced when used outside of the recommended parameters, proper use as an adjuvant to other disinfection protocols is advantageous [51]. Time and exposure parameters, such as irradiance and fluence rate, in addition to clade and strain-specific parameters, are critical variables when determining the most efficacious disinfection protocol. Findings seem to suggest that efficacy is inversely proportional to the distance from the UVC source [219]; however, some studies achieved inactivation at shorter distances, although later experienced regrowth [39]. The UV-360 Room Sanitiser (UltraViolet Devices, Inc. Valencia, CA), using four vertical UV lamps (254 nm) in a 360-degree motion sensor cycle, produced maximal inactivation after 30-minute exposure cycles; however, they noted that Japan/Korean strains were most susceptible compared to Venezuela, Spain, and India strains [219]. Whole room decontamination devices are capable of a 4.57 log reduction in C. auris when in the direct line of sight but had slightly reduced efficacy (3.96) when only achieving indirect exposure [57].
2.4.4. Waste Management
Disinfection or reduction of disease-causing microorganisms in medical waste to minimize disease transmission is imperative (WHO, 2014). Since completely destroying all microorganisms is challenging, sterilizing medical and surgical instruments is generally expressed as a 6 log10 reduction (a 99.9999% reduction) or greater of a specified microorganism [42]. In addition to thermal, chemical, biological, and mechanical waste-treatment technologies already discussed, UV has also been identified as an effective synergistic waste-treatment modality. Smart waste bins may include UV light for additive disinfection of the interior walls and air circulating inside closed waste units, rendering waste safer to transport within and outside of healthcare facilities [172]. Other UV waste management strategies include disinfection of waste prior to disposal, such as with mobile boxes designed to disinfect used N-95 masks during the COVID-19 pandemic [220]. Novel applications for small, mobile waste bins with integrated UVC LED disinfection are also emerging to address contamination before large-scale storage [221]. While UV has been used to destroy airborne and surface pathogens as a supplement to other technologies, it may be limited in its ability to penetrate closed waste bags. The effectiveness of UVC is likely to depend on the processes and protocols in place, allowing a direct line of sight to the discarded waste [42].
2.4.5. UVC LED Disinfection Critical Factors
Effective UVC LED disinfection of C. auris and other AMR pathogens relies on several critical factors across applications. Pathogen inactivation in water applications is highly dependent on the turbidity of the water and UV transmittance (or wavelength). Air temperature and humidity are critical factors in UV disinfection of AHUs. Air velocity inside units is also an important factor, as higher velocities result in cooled air. Many critical factors impact surface UV disinfection, including the material, topography, and reflectiveness of the material to be treated. The critical factors associated with surface disinfection are also important considerations in air applications, as the interior surfaces of AHUs are necessary. UVC disinfection in waste management is beholden to many of these critical factors depending on the specific waste and container to be treated
2.5. Case Studies of UV-C in Reducing C. auris
2.5.1. Water
No clinical case studies were available that examined the specific efficacy of UVC LED disinfection of C. auris in healthcare facilities’ water or wastewater. However, despite this lack of specific attention, several case studies demonstrate pan-microorganism reduction efficacy in water treatment facilities worldwide. The implementation of several point-of-use UVC LED water reactors (alongside chlorination systems) in the United States has demonstrated viral and bacterial inactivation efficacy using peak wavelengths ranging from 272 to 285 nm, depending on the unit and additive methods [222,223]. Due to the small size of UVC LED water reactors and affordable implementation, smaller villages in LMICs can also implement water disinfection infrastructure. There have been reportable success stories from across India and Thailand [224,225,226]. Sundar & Kanmani implemented a portable UVC water reactor at handpumps in a small village in South India, achieving a 2-log reduction of bacterial contaminants. Other portable UVC LED water reactors with multi-pass geometry were implemented throughout India with the effective elimination of test-selected E. coli [225]. Both of these implementations were considered cost-effective and efficient due to the relatively affordable price, small size, low-to-zero energy requirements, and practical operation guides [225,226]. In Thailand, the UVC LED wastewater reactor was implemented in conjunction with pre-treatment sand and settler filters. The UVC LED disinfection was effective at inactivating coliforms found in the wastewater [224]. When combined with adsorbent additives (e.g., agricultural waste), solar-powered UVC LED water reactors are effective at reducing microbial load in community wastewater, proving advantageous for public health protection [227]. In addition, two commercial-grade UVC LED water treatment systems have produced high-grade water purification in their large-scale implementations. In Singapore, the NEWater Initiative utilizes UVC LED to disinfect the entire country’s water system. The Orange County Water District’s Groundwater Replenishment System uses UVC LED disinfection of wastewater to prevent runoff into the Pacific Ocean [193].
2.5.2. Air
The mobile (remote, smart app-controlled) OZY AIR+Light combination air purification system disperses 60 g/h of ozone into a room for a preset time. Then, UVC sanitizers provide a flux of 80 m3/h, and the air is exposed to UVC LEDs before it is cycled back to the room [40]. In a clinical trial across Italian hospitals, the OZY AIR+Light system achieved a greater than 99% reduction in C. auris spores in each of three cycles of disinfection in medium- to high-risk patient areas. In the United States, UVC air purification units (15 W of high output UVC energy at 253.7 nm wavelength with a MERV 5 filter prior to UV light treatment) were installed in 16 special care unit rooms, hallways, and biohazard rooms of a long-term acute care hospital. After installation and continuous run time (81 days), there was a 42% reduction in airborne bacteria and a significant reduction in clinical HAIs, including common pathogens with contact spread. While the air sampling did not test for C. auris specifically in this study, efficacy against other AMR fungal spores shows promise for the extension of UVC air disinfection to C. auris [228]. In a similar study (not tailored to C. auris), HAIs were dramatically reduced after the clinical installation of in-room VidaShield (American Green Technology) continuous air purification units in the long-term ventilation unit of a hospital [229].
2.5.3. Surface
Clinical pilot testing designed to mimic common surfaces in a hospital setting (i.e., steel, plastic, glass) also found UVC technology to be effective at disinfecting after 10 minutes of exposure; however, effectiveness was statistically different across all three surfaces. While this pilot study was conducted in a clinical environment, only four patient rooms with random swab testing were used in the experiment at a time without any known outbreaks [32]. The Tru-D (Lumalier, Memphis, TN) UVC room disinfection device was clinically tested in an acute-care tertiary hospital in Chapel Hill, North Carolina. Room decontamination achieved a 4.45 log10 reduction (direct line of sight) of C. auris after a 17-19 minute cycle on the bacterial setting [57]. After standard chemical cleaning agents were completed, a larger academic medical center pilot tested a UVC disinfection robot (UVD robot, Clean Room Solutions) in two hospital outpatient clinics. The autonomous robot substantially reduced C. auris growth on surfaces compared to standard cleaning and disinfection practices. The clinical study confirmed previous in vitro tests that suggested longer exposure times are needed as the resiliency of the microbe increases [230]. Clinical studies of ICU terminal disinfection have demonstrated that UVC is considerably more effective (96.75% reduction) than aerosolized hydrogen peroxide (50.71% reduction) at no-touch reduction of C. auris on surfaces already manually cleaned [231]. A large systematic review evaluated the efficacy of 12 commercial UVC applications in adjunct disinfection across the United States, Canada, and South Africa. Among the 12 clinical studies, each found UVC surface disinfection to be effective at substantially reducing microbial load. In addition, several studies noted that the UVC disinfection protocol was easy to implement and recommended adoption for future adjuvant cleaning procedures [179].
2.5.3. Waste Management
No clinical case studies were identified examining the efficacy of UVC LED disinfection of healthcare and medical waste. While many studies previously discussed demonstrated lab-tested effectiveness, additional research is needed to report on the real-world implementation of this strategy.
3. Discussion
3.1. Benefits, Feasibility, & Challenges of Implementing UVC Disinfection in Healthcare Settings
Based on substantial lab testing and clinical case studies, UVC LED technology is a feasible and beneficial disinfection modality for healthcare environments. While this technology is promising, implementation and clinical efficacy measures present important challenges. Given the need for continued research on the standardization of disinfection conditions for C. auris, UVC LED disinfection across water, air, and surface can be used in a combination protocol and as an adjuvant sanitation procedure.
3.1.1. Challenges
Implementation of UVC LED disinfection is not without challenges. Across surface applications, the most predominant challenge is the requirement for specific conditions and parameters to reach the required clinical log reduction unique to C. auris [30,39,52,54,163,206]. Another notable challenge is that different isolates and clades have varying susceptibility to UVC light and require specific parameters tailored to the unique strain present [163]. The operational time required within an empty room for disinfection may be unachievable in busy healthcare facilities [30,52,232]. Operating limitations resulting in diminished efficacy are also possible, including shadows, changes in topography and surface, barriers to direct line of sight, physical contamination, and lack of standardization [233]. Specialized units (e.g., mobile disinfection devices and robots) also required trained personnel (e.g., microbiologists and technical engineers) to operate and troubleshoot errors in real-time and test the device’s sensitivity to the identified isolates [52,230,233]. Additionally, while UVC is considered safer than UVA and UVB, there are still risks for human exposure. There are unknown health and safety risks associated with frequent UVC disinfection exposure, and the standard shielding parameters are not yet fully understood [54,233].
While UVC LED devices are relatively low-cost or cost-effective, upfront purchase prices may be a barrier to low-resourced facilities [206]. Cost is particularly prohibitive if multiple units are required to meet protocol standards and efficient disinfection across a larger facility [52]. Compared to alternative disinfection, UVC devices are more costly than current standard procedures (e.g., air purification without UVC and manual cleaning-only protocols) [234]. Successful implementation of UVC disinfection is predicated on the availability of electricity, which can be a challenge in LMICs. A multiagency report found that close to 1 billion people in LMICs are served by healthcare facilities without a reliable electricity supply or no electricity at all [235]. It is estimated that 1 in 4 health facilities in sub-Saharan Africa have no electricity and that 2 in 3 healthcare facilities in LMICs lack access to reliable energy [236]. In air applications, air purification units equipped with HEPA filters + UVC LEDs (along with all other types of air purification with and without UVC) have been noted to sanitize a smaller than declared space, making it challenging for healthcare administrators to purchase and implement air purification units adequately sized for full disinfection of a desired area [234].
Patient and operator safety is another significant concern. While UVC is safer than other subtypes of UV light (i.e., UVA and UVB are more highly carcinogenic) and meets global requirements to phase out mercury lamps due to the harmful health and environmental impact, there are still safety risks that are not fully understood. When used outside of the intended purpose or straying from the suggested parameters for use, DNA damage, skin damage, and other adverse bodily effects are possible. Direct exposure to higher UVC wavelengths may also cause photocarcinogenic, mutagenic, or cytotoxic damage to human cells. While the adverse effect of direct UVC light exposure is not well researched, caution is needed when operating these devices [179]. Shielding is likely necessary for any direct UVC source; however, the wavelength, energy threshold, and other baseline parameters are not yet known [54].
3.1.2. Benefits
Despite these challenges, the benefits of enhanced no-touch UVC disinfection procedures are substantial. Given the limited efficacy of chemical agents in reducing colonization, the tremendous barriers to implementing strict disinfection procedures in overburdened healthcare settings, and the rapidly rising AMR and vast spread of C. auris, there is a significant need for supplementary disinfection modalities. While time to disinfect is noted as a challenge, many emerging commercial systems offer rapid disinfection as compared to traditional procedures. UVC LED arrays intended to disrupt and eliminate biofilm formation can achieve >99.99% microbial reduction without any optimization in under 40 seconds, compared to the traditional 60-second wet contact time required for various chemical disinfectants [54]. Many other commercial units report effective pathogen reduction in under 10 minutes [237].
Implementation of adjunct UVC LED disinfection across water, air, surface, and waste applications provides multi-layer protection against dangerous and costly C. auris spread. While there are costs associated with any UVC device (air, surface, or water), the upfront price is considerably less than the accrued costs of outbreaks (direct and indirect costs). The addition of UVC disinfection in healthcare settings can substantially reduce the global incidence and mortality rates related to C. auris, disrupting the current escalation of AMR candidemia and IC. As international resource mobilization for LMICs progresses, implementation of UV-C disinfection as a supplement disinfection modality is likely to become feasible despite current challenges. The United Nations Development Programme’s ‘Solar for Health’ initiative, which has equipped over 1,000 health centers with solar PV systems across 15 countries, including 11 in sub-Saharan Africa, provides strong infrastructure support that could equip LMICs in integrating UVC LED disinfection across water, air, surface, and waste applications. [236].
Quality of life benefits for patients who contract C. auris while admitted for other primary conditions are tremendous, but the costs associated with HAIs are skyrocketing. It is also important to note that the Medicare non-payment policy holds the healthcare facilities responsible for all HAI-associated costs due to a failure to prevent infections [238]; however, this is not consistent across all payers [239]. Facing rising healthcare costs and dwindling payer reimbursements, healthcare facilities should prioritize patient safety and infection prevention. UVC LED water, air, and surface disinfection is a simple, cost-effective method with proven efficacy at reducing C. auris and decreasing clinical candidemia.
3.2. Recommendations for the use of UVC Disinfection in Healthcare Settings to Reduce Transmission of C. auris
Since no specific chemical cleaning agents or germicides are designed to target C. auris, supplemental disinfection protocols are critical in reducing the transmission of C. auris. UVC LED technology across water, air, and surface applications and enhanced waste management protocols can bolster insufficient infection control procedures. The relatively low cost of UVC LED technology and broad use applications position it as an option for immediate adoption in healthcare settings. It is our recommendation to implement a multi-layered, enhanced UVC LED disinfection protocol, as illustrated in Figure 2, as an adjunct to any current infection prevention and control procedures. UVC LED water reactors for disinfection of water and wastewater have the highest impact, while air and surface applications follow close behind. UVC water disinfection has the potential to impact the greatest population with the fewest units and associated costs. UVC air disinfection for air handling systems has a similar impact ratio, reaching many people with only one unit; however, circulating air disinfection systems would need to be placed in discrete areas and would require additional units and cost. UVC LED surface disinfection is the most challenging to implement and is limited to single-room use. While disinfection is highly effective, it offers the lowest impact ratio when used only during terminal cleaning. UVC LED disinfection of waste has a more limited direct impact in healthcare facilities; however, the trickle-down effect may be substantial. Effective disinfection of healthcare waste can prevent community transmission of HAIs and limit the pathogenic spread of fungi like C. auris. If patient safety and infection control budgets allow for the implementation of UVC LED disinfection measures in each application, this would be considered the gold standard for infection prevention and control.
In the absence of an unlimited budget, careful consideration of the healthcare facility’s specific needs, the existing infrastructure, and the institutional capacity for implementation should be considered. The following recommendations outline considerations for scaled implementation, standard operating procedures, and policy revisions for any UVC disinfection applications in healthcare facilities.
- 1.
- Determine the UVC application (i.e., water, air, surface, and/or waste) needed and how it will be integrated into the current infection prevention and control infrastructure.
- 2.
- Ensure the UVC LED device meets all regional, national, and international disinfection standards.
- a.
- Ensure all regulations put forth by the CDC or other regulating bodies are followed. We suggest using UVC LED disinfection as an adjunct to currently accepted chemical disinfection until nationally and internationally recognized regulations are amended to consider UVC LED technology a first-line defense for the disinfection of C. auris.
- 3.
- Research all available devices with a cross-tabulated list of specific needs. Then, find the device that most closely aligns with the facility’s size and disinfection challenges.
- a.
- Consider the necessary operating parameters and associated critical factors across application areas that are necessary for effective disinfection.
- b.
- Assess the time and space requirements for effective disinfection in contrast to the available time and space for implementation.
- c.
- If the budget allows layer UVC LED disinfection technology (e.g., water, air, surface, and waste; however, given C. auris’s primary transmission route, a minimum of surface disinfection devices are strongly suggested.
- 4.
- Consider the human capacity and technical expertise required to implement and operate each type of device.
- a.
- Determine if the current infection prevention team will be sufficiently trained to augment disinfection with UVC LED or if new training or staff will be required.
- i.
- Any new training or personnel requirement should be factored into the budget assessment for the device.
- 5.
- Ensure the UVC LED technology adopted meets all required industry disinfection standards specific to the application.
- a.
- b.
- c.
- Water - NSF/ ANSI 55 Class A certification [244]
- 6.
- Establish robust evaluation protocols
- a.
- Accurate data collection and disease surveillance are necessary to determine the efficacy of C. auris inactivation and reduce colony spread.
- 7.
- Develop and implement routine maintenance schedules for all UVC LED systems to ensure their proper function and efficacy in disinfection.
- 8.
- Educate all healthcare system staff and administrators on the new infection prevention and control protocols, device safety, and disinfection procedures.
- 9.
- Write all policies and procedures in language the entire staff can understand and operationalize.
- 10.
- Establish a routine schedule for the evaluation of emerging UVC LED technology applications and device updates or upgrades.
4. Future Directions, in the Collection, Analyses, or Interpretation of Data, in the Writing of the Manuscript,
Emerging UVC LED technology development in C. auris disinfection has been rapid and critical to advancing human health and well-being. Across applications, additional research is needed to support the standardization of UVC LED disinfection in healthcare facilities as an adjuvant modality or as a first-line prevention and control mechanism. In addition to further exploring the efficacy of UVC LED disinfection across water, air, surface, and waste applications, studies should also focus on the best practices for C. auris disinfection parameters and conditions, including wavelength, energy requirements, time of exposure, distance from the UVC source, direct vs. indirect exposures, manual disinfection requirements, and frequency of use. Beyond further evaluation of clinical and operational efficacy and efficiency, additional research is needed on UVC LED systems’ power, lifetime, reliability, optimal substrate material, and the size of LEDs inside devices [245]. Standardization and certification of these operational parameters by a centralized regulating body should be a future goal for researchers and policymakers. Adoption of standard UVC LED disinfection procedures as part of a certified infection prevention and control program should also be addressed at the health system or facility level.
5. Conclusions
This article emphasizes the urgent need for surveillance, infection control, and global collaboration to combat the formidable fungal superbug, C. auris. Traditional cleaning and disinfection methods are inefficient and often ineffective, particularly when not performed in optimal conditions. UVC LED technology has demonstrated efficacy in inactivating C. auris and other healthcare-associated pathogens across many applications, including water, air, surface, and wastewater. UVC LED disinfection may also be more efficient and cost-effective than certain traditional methods. It is important to consider the UVC disinfection operating parameters and other critical factors necessary for effective treatment across each application. Despite the critical factors that must be met, UVC disinfection can also be used synergistically with current cleaning and infection control standards to increase efficacy in reducing the transmission of AMR superbugs.
*Note - All economic and financial estimates are indicated in US dollars. Any global economic impact reports have been converted to US dollars from the primary source for this review.
Appendices
None
Supplementary Materials
None
Author Contributions
Conceptualization, Richard Mariita and Jamie Reedy; methodology, Richard Mariita and Jamie Reedy; resources, Richard Mariita Jamie Reedy, Theekshana Fernando, Silas Awuor, Eric Omwenga; writing—original draft preparation, Jamie Reedy, Theekshana Fernando, and Silas Awuor; writing—review and editing, Richard Mariita, Jamie Reedy, Theekshana Fernando, Silas Awuor, Eric Omwenga, & Tatiana Koutchma; visualization, Richard Mariita and Jamie Reedy.; supervision, Richard Mariita; project administration, Jamie Reedy. All authors have read and agreed to the published version of the manuscript.”
Funding
This research received no external funding
Informed consent statement
Not Applicable
Data Availability statement
Not Applicable
Acknowledgments
We would like to acknowledge Britt Hafner for his work on visual elements.
Conflicts of Interest
All authors declare no conflicts of interest except Richard Mariita. Richard Mariita consults for Crystal IS, an Asahi Kasei Company that manufactures UVC-LEDs. Crystal IS had no role in the design of the review; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Centers for Disease Control and Prevention Air: Environmental Guidelines. Available online: https://www.cdc.gov/infectioncontrol/guidelines/environmental/appendix/air.html (accessed on 6 March 2024).
- Founou, R.C.; Founou, L.L.; Essack, S.Y. Clinical and Economic Impact of Antibiotic Resistance in Developing Countries: A Systematic Review and Meta-Analysis. PLOS ONE 2017, 12, e0189621. [Google Scholar] [CrossRef] [PubMed]
- Prestinaci, F.; Pezzotti, P.; Pantosti, A. Antimicrobial Resistance: A Global Multifaceted Phenomenon. Pathog Glob Health 2015, 109, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Salam, Md.A.; Al-Amin, Md.Y.; Salam, M.T.; Pawar, J.S.; Akhter, N.; Rabaan, A.A.; Alqumber, M.A.A. Antimicrobial Resistance: A Growing Serious Threat for Global Public Health. Healthcare (Basel) 2023, 11, 1946. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.J.L.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Aguilar, G.R.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global Burden of Bacterial Antimicrobial Resistance in 2019: A Systematic Analysis. The Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef] [PubMed]
- Dadgostar, P. Antimicrobial Resistance: Implications and Costs. Infect Drug Resist 2019, 12, 3903–3910. [Google Scholar] [CrossRef] [PubMed]
- Gajic, I.; Jovicevic, M.; Popadic, V.; Trudic, A.; Kabic, J.; Kekic, D.; Ilic, A.; Klasnja, S.; Hadnadjev, M.; Popadic, D.J.; et al. The Emergence of Multi-Drug-Resistant Bacteria Causing Healthcare-Associated Infections in COVID-19 Patients: A Retrospective Multi-Centre Study. Journal of Hospital Infection 2023, 137, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Tripartite Monitoring Global Progress on Antimicrobial Resistance; WHO, FAO, OIE: Rome, Italy, 2018; ISBN 978-92-5-130800-4.
- US Department of Agriculture NVAP Reference Guide - WOAH and International Standards. Available online: https://www.aphis.usda.gov/nvap/reference-guide/emergency-management/woah (accessed on 2 July 2024).
- Sikora, A.; Zahra, F. Nosocomial Infections. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2024. [Google Scholar]
- Bravo Ruiz, G.; Lorenz, A. What Do We Know about the Biology of the Emerging Fungal Pathogen of Humans Candida Auris? Microbiological Research 2021, 242, 126621. [Google Scholar] [CrossRef] [PubMed]
- Thatchanamoorthy, N.; Rukumani Devi, V.; Chandramathi, S.; Tay, S.T. Candida Auris: A Mini Review on Epidemiology in Healthcare Facilities in Asia. Journal of Fungi 2022, 8, 1126. [Google Scholar] [CrossRef] [PubMed]
- Business Today Desk Deadly Fungus, Candida Auris, Emerges in US: All You Need to Know. Business Today 2024.
- Haas, G. Hospital Infections from ‘Superbug’ Hit New High in January; Sunrise Hospital Cases up Again. KLAS: Local News, 2024. [Google Scholar]
- Putka, S. Candida Auris: What to Know About the Fungal Infection Spreading Across the U.S. MedPage Today Special Reports 2024.
- Sisson, P. Kaiser Working to Contain Spread of Fungal Infection at Zion Medical Center. San Diego Union-Tribune, 2024.
- Spokane Regional Health District Candida Auris Advisory for Healthcare Providers - Feb 1 2024; Washington, 2024.
- Dall, C. New York Hospital Reports Spike in Candida Auris during COVID-19. CIDRAP 2024.
- TikTok Candida Auris Fungus 2024 Pandemic. Available online: https://www.tiktok.com/discover/candida-auris-fungus-2024-pandemic (accessed on 15 March 2024).
- Centers for Disease Control and Prevention, National Center for Emerging and Zoonotic Infectious Diseases (NCEZID), Division of Foodborne, Waterborne, and Environmental Diseases (DFWED) Tracking Candida Auris. Available online: https://www.cdc.gov/fungal/candida-auris/tracking-c-auris.html (accessed on 15 March 2024).
- Irfan, H.; Ahmed, A.; Hafeez, H.; Tatsadjieu, N.L.S. Multidrug-Resistant Candida Auris Outbreak: A New Challenge for the United States. IJS Global Health 2023, 6, e0223. [Google Scholar] [CrossRef]
- Cortegiani, A.; Misseri, G.; Fasciana, T.; Giammanco, A.; Giarratano, A.; Chowdhary, A. Epidemiology, Clinical Characteristics, Resistance, and Treatment of Infections by Candida Auris. Journal of Intensive Care 2018, 6, 69. [Google Scholar] [CrossRef] [PubMed]
- Osei Sekyere, J. Candida Auris: A Systematic Review and Meta-analysis of Current Updates on an Emerging Multidrug-resistant Pathogen. Microbiologyopen 2018, 7, e00578. [Google Scholar] [CrossRef] [PubMed]
- Ettadili, H.; Vural, C. Current Global Status of Candida Auris an Emerging Multidrug-Resistant Fungal Pathogen: Bibliometric Analysis and Network Visualization. Braz J Microbiol 2024, 55, 391–402. [Google Scholar] [CrossRef] [PubMed]
- Caceres, D.H.; Forsberg, K.; Welsh, R.M.; Sexton, D.J.; Lockhart, S.R.; Jackson, B.R.; Chiller, T. Candida Auris: A Review of Recommendations for Detection and Control in Healthcare Settings. Journal of Fungi 2019, 5, 111. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention Infection Prevention and Control for Candida Auris. Available online: https://www.cdc.gov/fungal/candida-auris/c-auris-infection-control.html (accessed on 15 March 2024).
- Weber, D.J.; Rutala, W.A.; Anderson, D.J.; Sickbert-Bennett, E.E. ....úNo Touch..Ñ Methods for Health Care Room Disinfection: Focus on Clinical Trials. American Journal of Infection Control 2023, 51, A134–A143. [Google Scholar] [CrossRef] [PubMed]
- Beck, S.E.; Ryu, H.; Boczek, L.A.; Cashdollar, J.L.; Jeanis, K.M.; Rosenblum, J.S.; Lawal, O.R.; Linden, K.G. Evaluating UV-C LED Disinfection Performance and Investigating Potential Dual-Wavelength Synergy. Water Res 2017, 109, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Dai, T.; Vrahas, M.S.; Murray, C.K.; Hamblin, M.R. Ultraviolet C Irradiation: An Alternative Antimicrobial Approach to Localized Infections? Expert Rev Anti Infect Ther 2012, 10, 185–195. [Google Scholar] [CrossRef]
- Raeiszadeh, M.; Adeli, B. A Critical Review on Ultraviolet Disinfection Systems against COVID-19 Outbreak: Applicability, Validation, and Safety Considerations. ACS Photonics 2020, 7, 2941–2951. [Google Scholar] [CrossRef]
- Reedy, J.M.; Pousty, D.; Waliaula, B.W.; Maniga, J.; Mamane, H.; Mariita, R.M. Enhancing Quality of Life, Public Health, and Economic Development in the Global South through Waterborne Disease Prevention with Ultraviolet C Light-Emitting Diode Technology. GHES 2024, 0. [Google Scholar] [CrossRef]
- Różańska, A.; Walkowicz, M.; Bulanda, M.; Kasperski, T.; Synowiec, E.; Osuch, P.; Chmielarczyk, A. Evaluation of the Efficacy of UV-C Radiation in Eliminating Microorganisms of Special Epidemiological Importance from Touch Surfaces under Laboratory Conditions and in the Hospital Environment. Healthcare 2023, 11, 3096. [Google Scholar] [CrossRef] [PubMed]
- Shen, L.; Griffith, T.M.; Nyangaresi, P.O.; Qin, Y.; Pang, X.; Chen, G.; Li, M.; Lu, Y.; Zhang, B. Efficacy of UVC-LED in Water Disinfection on Bacillus Species with Consideration of Antibiotic Resistance Issue. Journal of Hazardous Materials 2020, 386, 121968. [Google Scholar] [CrossRef]
- Song, K.; Mohseni, M.; Taghipour, F. Mechanisms Investigation on Bacterial Inactivation through Combinations of UV Wavelengths. Water Research 2019, 163, 114875. [Google Scholar] [CrossRef]
- Zhang, W.; Huang, R.; Zhang, T.; Wang, B.; Li, N.; Sun, Y.; Ma, H.; Zhang, Q.; Zhang, J.; Liu, Y. Study on the Inactivation and Reactivation Mechanism of Pathogenic Bacteria in Aquaculture by UVC-LED. Frontiers in Marine Science 2023, 10. [Google Scholar] [CrossRef]
- Chatterley, C.; Linden, K. Demonstration and Evaluation of Germicidal UV-LEDs for Point-of-Use Water Disinfection. J Water Health 2010, 8, 479–486. [Google Scholar] [CrossRef]
- Choi, K.-H.; Kumar, A.; Schweizer, H.P. A 10-Min Method for Preparation of Highly Electrocompetent Pseudomonas Aeruginosa Cells: Application for DNA Fragment Transfer between Chromosomes and Plasmid Transformation. J Microbiol Methods 2006, 64, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Cai, M.; Wang, L.; Niu, F.; Yang, D.; Zhang, G. Evaluation Survey of Microbial Disinfection Methods in UV-LED Water Treatment Systems. Sci Total Environ 2019, 659, 1415–1427. [Google Scholar] [CrossRef]
- Bandara, N.; Samaranayake, L. Emerging Strategies for Environmental Decontamination of the Nosocomial Fungal Pathogen Candida Auris. J Med Microbiol 2022, 71. [Google Scholar] [CrossRef]
- Sottani, C.; Barraza, G.F.; Frigerio, F.; Corica, G.; Cuna, F.S.R. della; Cottica, D.; Grignani, E. Effectiveness of a Combined UV-C and Ozone Treatment in Reducing Healthcare-Associated Infections in Hospital Facilities. Journal of Hospital Infection 2023, 139, 207–216. [Google Scholar] [CrossRef]
- Mariita, R.M.; Davis, J.H.; Lottridge, M.M.; Randive, R.V. Shining Light on Multi-Drug Resistant Candida Auris: Ultraviolet-C Disinfection, Wavelength Sensitivity, and Prevention of Biofilm Formation of an Emerging Yeast Pathogen. MicrobiologyOpen 2022, 11, e1261. [Google Scholar] [CrossRef]
- Prüss, A.; Emmanuel, J.; Stringer, R.; Pieper, U.; Townend, W.; Wilburn, S.; Chantier, Y. ; World Health Organization Safe Management of Wastes from Health-Care Activities / Edited by A. Prüss …[et Al]; 2nd ed.; World Health Organization: Geneva, 2014; ISBN 978-92-4-154856-4. [Google Scholar]
- World Health Organization Health-Care Waste. Available online: https://www.who.int/news-room/fact-sheets/detail/health-care-waste (accessed on 19 March 2024).
- Sansom, S.E.; Gussin, G.M.; Schoeny, M.; Singh, R.D.; Adil, H.; Bell, P.; Benson, E.C.; Bittencourt, C.E.; Black, S.; Del Mar Villanueva Guzman, M.; et al. Rapid Environmental Contamination With Candida Auris and Multidrug-Resistant Bacterial Pathogens Near Colonized Patients. Clinical Infectious Diseases 2024, 78, 1276–1284. [Google Scholar] [CrossRef] [PubMed]
- The National Institute for Occupational Safety and Health (NIOSH) Chain of Infection Components. Available online: https://www.cdc.gov/niosh/learning/safetyculturehc/module-2/3.html (accessed on 19 March 2024).
- World Health Organization Global Analysis of Healthcare Waste in the Context of COVID-19: Status, Impacts and Recommendations; Geneva, Switzerland, 2022; ISBN 978-92-4-003961-2.
- Marsh, J. Hazardous Waste Incineration: A Closer Look at Environmental Solutions. Available online: https://environment.co/hazardous-waste-incineration-closer-look-at-environmental-solutions/ (accessed on 5 July 2024).
- Beck, S.E. Wavelength-Specific Effects of Ultraviolet Light on Microorganisms and Viruses for Improving Water. Disinfection. Dissertation, University of Colorado Boulder: Boulder, Colorado, 2015. [Google Scholar]
- Chatterjee, P.; Choi, H.; Ochoa, B.; Garmon, G.; Coppin, J.D.; Allton, Y.; Lukey, J.; Williams, M.D.; Navarathna, D.; Jinadatha, C. Clade-Specific Variation in Susceptibility of Candida Auris to Broad-Spectrum Ultraviolet C Light (UV-C). Infect Control Hosp Epidemiol 2020, 41, 1384–1387. [Google Scholar] [CrossRef]
- Frongillo, E.; Amodeo, D.; Nante, N.; Cevenini, G.; Messina, G. A Novel Technology for Disinfecting Surfaces Infested with Candida Auris: The UVC Chip. European Journal of Public Health 2022, 32, ckac131–251. [Google Scholar] [CrossRef]
- Fu, L.; Le, T.; Liu, Z.; Wang, L.; Guo, H.; Yang, J.; Chen, Q.; Hu, J. Different Efficacies of Common Disinfection Methods against Candida Auris and Other Candida Species. J Infect Public Health 2020, 13, 730–736. [Google Scholar] [CrossRef] [PubMed]
- Koutras, C.; Wade, R.L. Ultraviolet-C Mediated Inactivation of Candida Auris, a Rapid Emerging Health Threat. American Journal of Infection Control 2024, 52, 133–135. [Google Scholar] [CrossRef]
- Lemons, A.R.; McClelland, T.; Martin, S.B.; Lindsley, W.G.; Green, B.J. Susceptibility of Candida Auris to Ultraviolet Germicidal Irradiation (UVGI) Correlates with Drug Resistance to Common Antifungal Agents. American Journal of Infection Control 2019, 47, S18. [Google Scholar] [CrossRef]
- Mariita, R.M.; Davis, J.H.; Lottridge, M.M.; Randive, R.V. Shining Light on Multi-drug Resistant Candida Auris: Ultraviolet-C Disinfection, Wavelength Sensitivity, and Prevention of Biofilm Formation of an Emerging Yeast Pathogen. Microbiologyopen 2022, 11, e1261. [Google Scholar] [CrossRef]
- Maslo, C.; du Plooy, M.; Coetzee, J. The Efficacy of Pulsed-Xenon Ultraviolet Light Technology on Candida Auris. BMC Infect Dis 2019, 19, 540. [Google Scholar] [CrossRef]
- Omardien, S.; Teska, P. Skin and Hard Surface Disinfection against Candida Auris – What We Know Today. Front. Med. 2024, 11. [Google Scholar] [CrossRef]
- Rutala, W.A.; Kanamori, H.; Gergen, M.F.; Sickbert-Bennett, E.E.; Weber, D.J. Inactivation of Candida Auris and Candida Albicans by Ultraviolet-C. Infect Control Hosp Epidemiol 2022, 43, 1495–1497. [Google Scholar] [CrossRef]
- Bongomin, F.; Gago, S.; Oladele, R.O.; Denning, D.W. Global and Multi-National Prevalence of Fungal Diseases—Estimate Precision. Journal of Fungi 2017, 3, 57. [Google Scholar] [CrossRef]
- Kumar, S.; Kumar, A.; Roudbary, M.; Mohammadi, R.; Černáková, L.; Rodrigues, C.F. Overview on the Infections Related to Rare Candida Species. Pathogens 2022, 11, 963. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention Types of Fungal Diseases. Available online: https://www.cdc.gov/fungal/diseases/index.html (accessed on 15 March 2024).
- Sanyaolu, A.; Okorie, C.; Marinkovic, A.; Abbasi, A.F.; Prakash, S.; Mangat, J.; Hosein, Z.; Haider, N.; Chan, J. Candida Auris: An Overview of the Emerging Drug-Resistant Fungal Infection. Infect Chemother 2022, 54, 236–246. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention Invasive Candidiasis. Available online: https://www.cdc.gov/fungal/diseases/candidiasis/invasive/index.html (accessed on 15 March 2024).
- Du, H.; Bing, J.; Hu, T.; Ennis, C.L.; Nobile, C.J.; Huang, G. Candida Auris: Epidemiology, Biology, Antifungal Resistance, and Virulence. PLOS Pathogens 2020, 16, e1008921. [Google Scholar] [CrossRef] [PubMed]
- Sikora, A.; Hashmi, M.F.; Zahra, F. Candida Auris. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2024. [Google Scholar]
- Chow, N.A.; Muñoz, J.F.; Gade, L.; Berkow, E.L.; Li, X.; Welsh, R.M.; Forsberg, K.; Lockhart, S.R.; Adam, R.; Alanio, A.; et al. Tracing the Evolutionary History and Global Expansion of Candida Auris Using Population Genomic Analyses. mBio 2020, 11, 10–1128. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, P.A.; Rivera, S.M.; Escandon, P.; Caceres, D.H.; Chow, N.; Stuckey, M.J.; Díaz, J.; Gomez, A.; Vélez, N.; Espinosa-Bode, A.; et al. Hospital-Associated Multicenter Outbreak of Emerging Fungus Candida Auris, Colombia, 2016. Emerg Infect Dis 2019, 25, 1339–1346. [Google Scholar] [CrossRef] [PubMed]
- Chakrabarti, A.; Sood, P. On the Emergence, Spread and Resistance of Candida Auris: Host, Pathogen and Environmental Tipping Points. J Med Microbiol 2021, 70, 001318. [Google Scholar] [CrossRef] [PubMed]
- Chowdhary, A.; Sharma, C.; Duggal, S.; Agarwal, K.; Prakash, A.; Singh, P.K.; Jain, S.; Kathuria, S.; Randhawa, H.S.; Hagen, F.; et al. New Clonal Strain of Candida Auris, Delhi, India. Emerging Infectious Diseases journal 2013, 19. [Google Scholar] [CrossRef]
- Govender, N.P.; Magobo, R.E.; Mpembe, R.; Mhlanga, M.; Matlapeng, P.; Corcoran, C.; Govind, C.; Lowman, W.; Senekal, M.; Thomas, J. Candida Auris in South Africa, 2012–2016. Emerg Infect Dis 2018, 24, 2036–2040. [Google Scholar] [CrossRef]
- Lone, S.A.; Ahmad, A. Candida Auris-the Growing Menace to Global Health. Mycoses 2019, 62, 620–637. [Google Scholar] [CrossRef] [PubMed]
- Nelson, R. Emergence of Resistant Candida Auris. The Lancet Microbe 2023, 4, e396. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, J.; Abdolrasouli, A.; Farrer, R.A.; Cuomo, C.A.; Aanensen, D.M.; Armstrong-James, D.; Fisher, M.C.; Schelenz, S. Genomic Epidemiology of the UK Outbreak of the Emerging Human Fungal Pathogen Candida Auris. Emerg Microbes Infect 2018, 7, 43. [Google Scholar] [CrossRef]
- Shariq, A.; Rasheed, Z.; Alghsham, R.S.; Abdulmonem, W.A. Candida Auris: An Emerging Fungus That Presents a Serious Global Health Threat. Int J Health Sci (Qassim) 2023, 17, 1–2. [Google Scholar] [PubMed]
- van Schalkwyk, E.; Mpembe, R.S.; Thomas, J.; Shuping, L.; Ismail, H.; Lowman, W.; Karstaedt, A.S.; Chibabhai, V.; Wadula, J.; Avenant, T.; et al. Epidemiologic Shift in Candidemia Driven by Candida Auris, South Africa, 2016–20171. Emerg Infect Dis 2019, 25, 1698–1707. [Google Scholar] [CrossRef]
- Chow, N.A.; Gade, L.; Tsay, S.V.; Forsberg, K.; Greenko, J.A.; Southwick, K.L.; Barrett, P.M.; Kerins, J.L.; Lockhart, S.R.; Chiller, T.M.; et al. Multiple Introductions and Subsequent Transmission of Multidrug-Resistant Candida Auris in the USA: A Molecular Epidemiological Survey. The Lancet Infectious Diseases 2018, 18, 1377–1384. [Google Scholar] [CrossRef] [PubMed]
- Mishra, S.K.; Yasir, M.; Willcox, M. Candida Auris: An Emerging Antimicrobial-Resistant Organism with the Highest Level of Concern. The Lancet Microbe 2023, 4, e482–e483. [Google Scholar] [CrossRef] [PubMed]
- Casadevall, A.; Kontoyiannis, D.P.; Robert, V. On the Emergence of Candida Auris: Climate Change, Azoles, Swamps, and Birds. mBio 2019, 10, e01397–19. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization WHO Fungal Priority Pathogens List to Guide Research, Development and Public Health Action; Geneva, 2022.
- Satoh, K.; Makimura, K.; Hasumi, Y.; Nishiyama, Y.; Uchida, K.; Yamaguchi, H. Candida Auris Sp. Nov., a Novel Ascomycetous Yeast Isolated from the External Ear Canal of an Inpatient in a Japanese Hospital. Microbiol Immunol 2009, 53, 41–44. [Google Scholar] [CrossRef]
- Lindquist, S. epiTrends. July 2021 .
- Fasciana, T.; Cortegiani, A.; Ippolito, M.; Giarratano, A.; Di Quattro, O.; Lipari, D.; Graceffa, D.; Giammanco, A. Candida Auris: An Overview of How to Screen, Detect, Test and Control This Emerging Pathogen. Antibiotics (Basel) 2020, 9, 778. [Google Scholar] [CrossRef] [PubMed]
- Spivak, E.S.; Hanson, K.E. Candida Auris: An Emerging Fungal Pathogen. J Clin Microbiol 2018, 56, e01588–17. [Google Scholar] [CrossRef] [PubMed]
- Bandara, N.; Samaranayake, L. Emerging and Future Strategies in the Management of Recalcitrant Candida Auris. Medical Mycology 2022, 60, myac008. [Google Scholar] [CrossRef]
- Escandón, P.; Chow, N.A.; Caceres, D.H.; Gade, L.; Berkow, E.L.; Armstrong, P.; Rivera, S.; Misas, E.; Duarte, C.; Moulton-Meissner, H.; et al. Molecular Epidemiology of Candida Auris in Colombia Reveals a Highly Related, Countrywide Colonization With Regional Patterns in Amphotericin B Resistance. Clin Infect Dis 2019, 68, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Rybak, J.M.; Doorley, L.A.; Nishimoto, A.T.; Barker, K.S.; Palmer, G.E.; Rogers, P.D. Abrogation of Triazole Resistance upon Deletion of CDR1 in a Clinical Isolate of Candida Auris. Antimicrob Agents Chemother 2019, 63, e00057-19. [Google Scholar] [CrossRef]
- Chowdhary, A.; Prakash, A.; Sharma, C.; Kordalewska, M.; Kumar, A.; Sarma, S.; Tarai, B.; Singh, A.; Upadhyaya, G.; Upadhyay, S.; et al. A Multicentre Study of Antifungal Susceptibility Patterns among 350 Candida Auris Isolates (2009-17) in India: Role of the ERG11 and FKS1 Genes in Azole and Echinocandin Resistance. J Antimicrob Chemother 2018, 73, 891–899. [Google Scholar] [CrossRef]
- Healey, K.R.; Kordalewska, M.; Jiménez Ortigosa, C.; Singh, A.; Berrío, I.; Chowdhary, A.; Perlin, D.S. Limited ERG11 Mutations Identified in Isolates of Candida Auris Directly Contribute to Reduced Azole Susceptibility. Antimicrob Agents Chemother 2018, 62, e01427-18. [Google Scholar] [CrossRef] [PubMed]
- Rybak, J.M.; Sharma, C.; Doorley, L.A.; Barker, K.S.; Palmer, G.E.; Rogers, P.D. Delineation of the Direct Contribution of Candida Auris ERG11 Mutations to Clinical Triazole Resistance. Microbiol Spectr 2021, 9, e01585-21. [Google Scholar] [CrossRef]
- Egger, N.B.; Kainz, K.; Schulze, A.; Bauer, M.A.; Madeo, F.; Carmona-Gutierrez, D. The Rise of Candida Auris: From Unique Traits to Co-Infection Potential. Microb Cell 2022, 9, 141–144. [Google Scholar] [CrossRef]
- Montoya, M.C.; Moye-Rowley, W.S.; Krysan, D.J. Candida Auris: The Canary in the Mine of Antifungal Drug Resistance. ACS Infect. Dis. 2019, 5, 1487–1492. [Google Scholar] [CrossRef]
- Lockhart, S.R.; Etienne, K.A.; Vallabhaneni, S.; Farooqi, J.; Chowdhary, A.; Govender, N.P.; Colombo, A.L.; Calvo, B.; Cuomo, C.A.; Desjardins, C.A.; et al. Simultaneous Emergence of Multidrug-Resistant Candida Auris on 3 Continents Confirmed by Whole-Genome Sequencing and Epidemiological Analyses. Clinical Infectious Diseases 2017, 64, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Lyman, M.; Forsberg, K.; Reuben, J.; Dang, T.; Free, R.; Seagle, E.E.; Sexton, D.J.; Soda, E.; Jones, H.; Hawkins, D.; et al. Notes from the Field: Transmission of Pan-Resistant and Echinocandin-Resistant Candida Auris in Health Care Facilities ― Texas and the District of Columbia, January–April 2021. MMWR Morb Mortal Wkly Rep 2021, 70, 1022–1023. [Google Scholar] [CrossRef] [PubMed]
- Kainer, M.A.; Kemble, S.; Black, S.; Blog, D.; Lutterloh, E.; Quinn, M.; VonBank, B.; Barrett, P.; Greeley, R.; Kratz, M.; et al. Standardized Case Definition for Candida Auris Clinical and Colonization/Screening Cases and National Notification of C. Auris Case, Clinical 2018.
- Gonzalez-Lara, M.F.; Ostrosky-Zeichner, L. Invasive Candidiasis. Semin Respir Crit Care Med 2020, 41, 003–012. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.; Khan, Z.; Al-Sweih, N.; Alfouzan, W.; Joseph, L. Candida Auris in Various Hospitals across Kuwait and Their Susceptibility and Molecular Basis of Resistance to Antifungal Drugs. Mycoses 2020, 63, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Araúz, A.B.; Caceres, D.H.; Santiago, E.; Armstrong, P.; Arosemena, S.; Ramos, C.; Espinosa-Bode, A.; Borace, J.; Hayer, L.; Cedeño, I.; et al. Isolation of Candida Auris from 9 Patients in Central America: Importance of Accurate Diagnosis and Susceptibility Testing. Mycoses 2018, 61, 44–47. [Google Scholar] [CrossRef] [PubMed]
- Calvo, B.; Melo, A.S.A.; Perozo-Mena, A.; Hernandez, M.; Francisco, E.C.; Hagen, F.; Meis, J.F.; Colombo, A.L. First Report of Candida Auris in America: Clinical and Microbiological Aspects of 18 Episodes of Candidemia. J Infect 2016, 73, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Chybowska, A.D.; Childers, D.S.; Farrer, R.A. Nine Things Genomics Can Tell Us About Candida Auris. Front Genet 2020, 11, 351. [Google Scholar] [CrossRef] [PubMed]
- Kohlenberg, A.; Monnet, D.L.; Plachouras, D.; Group, C. auris survey collaborative Increasing Number of Cases and Outbreaks Caused by Candida Auris in the EU/EEA, 2020 to 2021. Eurosurveillance 2022, 27, 2200846. [Google Scholar] [CrossRef]
- Schelenz, S.; Hagen, F.; Rhodes, J.L.; Abdolrasouli, A.; Chowdhary, A.; Hall, A.; Ryan, L.; Shackleton, J.; Trimlett, R.; Meis, J.F.; et al. First Hospital Outbreak of the Globally Emerging Candida Auris in a European Hospital. Antimicrobial Resistance & Infection Control 2016, 5, 35. [Google Scholar] [CrossRef]
- Zhu, Y.; O’Brien, B.; Leach, L.; Clarke, A.; Bates, M.; Adams, E.; Ostrowsky, B.; Quinn, M.; Dufort, E.; Southwick, K.; et al. Laboratory Analysis of an Outbreak of Candida Auris in New York from 2016 to 2018: Impact and Lessons Learned. J Clin Microbiol 2020, 58, e01503–19. [Google Scholar] [CrossRef]
- Chowdhary, A.; Sharma, C.; Meis, J.F. Candida Auris: A Rapidly Emerging Cause of Hospital-Acquired Multidrug-Resistant Fungal Infections Globally. PLOS Pathogens 2017, 13, e1006290. [Google Scholar] [CrossRef] [PubMed]
- Lyman, M.; Forsberg, K.; Sexton, D.J.; Chow, N.A.; Lockhart, S.R.; Jackson, B.R.; Chiller, T. Worsening Spread of Candida Auris in the United States, 2019 to 2021. Ann Intern Med 2023, 176, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Ku, T.S.N.; Walraven, C.J.; Lee, S.A. Candida Auris: Disinfectants and Implications for Infection Control. Front Microbiol 2018, 9, 726. [Google Scholar] [CrossRef] [PubMed]
- Farooqi, J.Q.; Jabeen, K.; Saeed, N.; Iqbal, N.; Malik, B.; Lockhart, S.R.; Zafar, A.; Brandt, M.E.; Hasan, R. Invasive Candidiasis in Pakistan: Clinical Characteristics, Species Distribution and Antifungal Susceptibility. J Med Microbiol 2013, 62, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Pfaller, M.A.; Diekema, D.J. Epidemiology of Invasive Candidiasis: A Persistent Public Health Problem. Clin Microbiol Rev 2007, 20, 133–163. [Google Scholar] [CrossRef] [PubMed]
- Smidt, M.C.F.; Meiring, S.; Mpembe, R.; Kularatane, R.; Govender, N. Factors Associated with Mortality among Patients with Candidaemia in South Africa, 2012. International Journal of Infectious Diseases 2014, 21, 288. [Google Scholar] [CrossRef]
- Doi, A.M.; Pignatari, A.C.C.; Edmond, M.B.; Marra, A.R.; Camargo, L.F.A.; Siqueira, R.A.; da Mota, V.P.; Colombo, A.L. Epidemiology and Microbiologic Characterization of Nosocomial Candidemia from a Brazilian National Surveillance Program. PLoS One 2016, 11, e0146909. [Google Scholar] [CrossRef] [PubMed]
- Taori, S.K.; Khonyongwa, K.; Hayden, I.; Athukorala, G.D.A.; Letters, A.; Fife, A.; Desai, N.; Borman, A.M. Candida Auris Outbreak: Mortality, Interventions and Cost of Sustaining Control. J Infect 2019, 79, 601–611. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention About Candida Auris (C. Auris) Available online:. Available online: https://www.cdc.gov/fungal/candida-auris/candida-auris-qanda.html (accessed on 15 March 2024).
- Ahmad, S.; Asadzadeh, M. Strategies to Prevent Transmission of Candida Auris in Healthcare Settings. Curr Fungal Infect Rep 2023, 17, 36–48. [Google Scholar] [CrossRef]
- Rudramurthy, S.M.; Chakrabarti, A.; Paul, R.A.; Sood, P.; Kaur, H.; Capoor, M.R.; Kindo, A.J.; Marak, R.S.K.; Arora, A.; Sardana, R.; et al. Candida Auris Candidaemia in Indian ICUs: Analysis of Risk Factors. Journal of Antimicrobial Chemotherapy 2017, 72, 1794–1801. [Google Scholar] [CrossRef]
- Chokshi, A.; Sifri, Z.; Cennimo, D.; Horng, H. Global Contributors to Antibiotic Resistance. J Glob Infect Dis 2019, 11, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Laxminarayan, R.; Duse, A.; Wattal, C.; Zaidi, A.K.M.; Wertheim, H.F.L.; Sumpradit, N.; Vlieghe, E.; Hara, G.L.; Gould, I.M.; Goossens, H.; et al. Antibiotic Resistance-the Need for Global Solutions. Lancet Infect Dis 2013, 13, 1057–1098. [Google Scholar] [CrossRef] [PubMed]
- UNICEF Neonatal Mortality. Available online: https://data.unicef.org/topic/child-survival/neonatal-mortality/ (accessed on 15 March 2024).
- World Health Organization Newborns: Improving Survival and Well-Being. Available online: https://www.who.int/news-room/fact-sheets/detail/newborns-reducing-mortality (accessed on 15 March 2024).
- Cook, A.; Ferreras-Antolin, L.; Adhisivam, B.; Ballot, D.; Berkley, J.A.; Bernaschi, P.; Carvalheiro, C.G.; Chaikittisuk, N.; Chen, Y.; Chibabhai, V.; et al. Neonatal Invasive Candidiasis in Low- and Middle-Income Countries: Data from the NeoOBS Study. Medical Mycology 2023, 61, myad010. [Google Scholar] [CrossRef] [PubMed]
- Warris, A. Candida Auris, What Do Paediatricians Need to Know? Archives of Disease in Childhood 2018, 103, 891–894. [Google Scholar] [CrossRef] [PubMed]
- Berrio, I.; Caceres, D.H.; Coronell R, W.; Salcedo, S.; Mora, L.; Marin, A.; Varón, C.; Lockhart, S.R.; Escandón, P.; Berkow, E.L.; et al. Bloodstream Infections With Candida Auris Among Children in Colombia: Clinical Characteristics and Outcomes of 34 Cases. Journal of the Pediatric Infectious Diseases Society 2021, 10, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Shuping, L.; Mpembe, R.; Mhlanga, M.; Naicker, S.D.; Maphanga, T.G.; Tsotetsi, E.; Wadula, J.; Velaphi, S.; Nakwa, F.; Chibabhai, V.; et al. Epidemiology of Culture-Confirmed Candidemia Among Hospitalized Children in South Africa, 2012–2017. The Pediatric Infectious Disease Journal 2021, 40, 730. [Google Scholar] [CrossRef]
- Chakrabarti, A.; Sood, P.; Rudramurthy, S.M.; Chen, S.; Jillwin, J.; Iyer, R.; Sharma, A.; Harish, B.N.; Roy, I.; Kindo, A.J.; et al. Characteristics, Outcome and Risk Factors for Mortality of Paediatric Patients with ICU-Acquired Candidemia in India: A Multicentre Prospective Study. Mycoses 2020, 63, 1149–1163. [Google Scholar] [CrossRef]
- Mesini, A.; Saffioti, C.; Mariani, M.; Florio, A.; Medici, C.; Moscatelli, A.; Castagnola, E. First Case of Candida Auris Colonization in a Preterm, Extremely Low-Birth-Weight Newborn after Vaginal Delivery. Journal of Fungi 2021, 7, 649. [Google Scholar] [CrossRef] [PubMed]
- Jonas, O.; Irwin, A.; Berthe, F.C.J.; Le Gall, F.G.; Marquez, P.V. Drug-Resistant Infections : A Threat to Our Economic Future (Vol. 2) : Final Report (English); HNP/Agriculture Global Antimicrobial Resistance Initiative; World Bank Group: Washington D.C, 2017. [Google Scholar]
- Benedict, K.; Whitham, H.K.; Jackson, B.R. Economic Burden of Fungal Diseases in the United States. Open Forum Infectious Diseases 2022, 9, ofac097. [Google Scholar] [CrossRef]
- Benedict, K.; Jackson, B.R.; Chiller, T.; Beer, K.D. Estimation of Direct Healthcare Costs of Fungal Diseases in the United States. Clin Infect Dis 2019, 68, 1791–1797. [Google Scholar] [CrossRef]
- Wan Ismail, W.N.A.; Jasmi, N.; Khan, T.M.; Hong, Y.H.; Neoh, C.F. The Economic Burden of Candidemia and Invasive Candidiasis: A Systematic Review. Value in Health Regional Issues 2020, 21, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Perlin, D.S.; Rautemaa-Richardson, R.; Alastruey-Izquierdo, A. The Global Problem of Antifungal Resistance: Prevalence, Mechanisms, and Management. The Lancet Infectious Diseases 2017, 17, e383–e392. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Repository, S.; Basu, S. Antibiotic Resistance: A Threat to Global Health | Perils of Growing Antibiotic Resistance in Today’s World. 2020. [CrossRef]
- Muñoz, P.; Valerio, M.; Vena, A.; Bouza, E. Antifungal Stewardship in Daily Practice and Health Economic Implications. Mycoses 2015, 58, 14–25. [Google Scholar] [CrossRef] [PubMed]
- Dennis, E.K.; Chaturvedi, S.; Chaturvedi, V. So Many Diagnostic Tests, So Little Time: Review and Preview of Candida Auris Testing in Clinical and Public Health Laboratories. Frontiers in Microbiology 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Chowdhary, A.; Voss, A.; Meis, J.F. Multidrug-Resistant Candida Auris: ‘New Kid on the Block’ in Hospital-Associated Infections? Journal of Hospital Infection 2016, 94, 209–212. [Google Scholar] [CrossRef] [PubMed]
- Biswal, M.; Rudramurthy, S.M.; Jain, N.; Shamanth, A.S.; Sharma, D.; Jain, K.; Yaddanapudi, L.N.; Chakrabarti, A. Controlling a Possible Outbreak of Candida Auris Infection: Lessons Learnt from Multiple Interventions. Journal of Hospital Infection 2017, 97, 363–370. [Google Scholar] [CrossRef]
- Anderson, D.J.; Chen, L.F.; Weber, D.J.; Moehring, R.W.; Lewis, S.S.; Triplett, P.F.; Blocker, M.; Becherer, P.; Schwab, J.C.; Knelson, L.P.; et al. Enhanced Terminal Room Disinfection and Acquisition and Infection Caused by Multidrug-Resistant Organisms and Clostridium Difficile (the Benefits of Enhanced Terminal Room Disinfection Study): A Cluster-Randomised, Multicentre, Crossover Study. The Lancet 2017, 389, 805–814. [Google Scholar] [CrossRef] [PubMed]
- Sherry, L.; Ramage, G.; Kean, R.; Borman, A.; Johnson, E.M.; Richardson, M.D.; Rautemaa-Richardson, R. Biofilm-Forming Capability of Highly Virulent, Multidrug-Resistant Candida Auris. Emerg Infect Dis 2017, 23, 328–331. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.; Alfouzan, W. Candida Auris: Epidemiology, Diagnosis, Pathogenesis, Antifungal Susceptibility, and Infection Control Measures to Combat the Spread of Infections in Healthcare Facilities. Microorganisms 2021, 9, 807. [Google Scholar] [CrossRef]
- Černáková, L.; Roudbary, M.; Brás, S.; Tafaj, S.; Rodrigues, C.F. Candida Auris: A Quick Review on Identification, Current Treatments, and Challenges. International Journal of Molecular Sciences 2021, 22, 4470. [Google Scholar] [CrossRef]
- Kumar, J.; Eilertson, B.; Cadnum, J.L.; Whitlow, C.S.; Jencson, A.L.; Safdar, N.; Krein, S.L.; Tanner, W.D.; Mayer, J.; Samore, M.H.; et al. Environmental Contamination with Candida Species in Multiple Hospitals Including a Tertiary Care Hospital with a Candida Auris Outbreak. Pathog Immun 2019, 4, 260–270. [Google Scholar] [CrossRef] [PubMed]
- Vallabhaneni, S. Investigation of the First Seven Reported Cases of Candida Auris, a Globally Emerging Invasive, Multidrug-Resistant Fungus — United States, May 2013–August 2016. MMWR Morb Mortal Wkly Rep 2016, 65. [Google Scholar] [CrossRef] [PubMed]
- Vila, T.; Sultan, A.S.; Montelongo-Jauregui, D.; Jabra-Rizk, M.A. Candida Auris: A Fungus with Identity Crisis. Pathog Dis 2020, 78, ftaa034. [Google Scholar] [CrossRef] [PubMed]
- Cristina, M.L.; Spagnolo, A.M.; Sartini, M.; Carbone, A.; Oliva, M.; Schinca, E.; Boni, S.; Pontali, E. An Overview on Candida Auris in Healthcare Settings. Journal of Fungi 2023, 9. [Google Scholar] [CrossRef]
- Barber, C.; Crank, K.; Papp, K.; Innes, G.K.; Schmitz, B.W.; Chavez, J.; Rossi, A.; Gerrity, D. Community-Scale Wastewater Surveillance of Candida Auris during an Ongoing Outbreak in Southern Nevada. Environ. Sci. Technol. 2023, 57, 1755–1763. [Google Scholar] [CrossRef]
- Miralles-Cuevas, S.; De la Obra, I.; Gualda-Alonso, E.; Soriano-Molina, P.; Casas López, J.L.; Sánchez Pérez, J.A. Simultaneous Disinfection and Organic Microcontaminant Removal by UVC-LED-Driven Advanced Oxidation Processes. Water 2021, 13, 1507. [Google Scholar] [CrossRef]
- Nyangaresi, P.O.; Qin, Y.; Chen, G.; Zhang, B.; Lu, Y.; Shen, L. Comparison of the Performance of Pulsed and Continuous UVC-LED Irradiation in the Inactivation of Bacteria. Water Research 2019, 157, 218–227. [Google Scholar] [CrossRef] [PubMed]
- Song, K.; Taghipour, F.; Mohseni, M. Microorganisms Inactivation by Wavelength Combinations of Ultraviolet Light-Emitting Diodes (UV-LEDs). Science of The Total Environment 2019, 665, 1103–1110. [Google Scholar] [CrossRef]
- Kim, D.-K.; Kang, D.-H. UVC LED Irradiation Effectively Inactivates Aerosolized Viruses, Bacteria, and Fungi in a Chamber-Type Air Disinfection System. Applied and Environmental Microbiology 2018, 84, e00944–18. [Google Scholar] [CrossRef]
- Lai, A.C.K.; Nunayon, S.S. A New UVC-LED System for Disinfection of Pathogens Generated by Toilet Flushing. Indoor Air 2021, 31, 324–334. [Google Scholar] [CrossRef]
- Nunayon, S.S.; Zhang, H.H.; Lai, A.C.K. A Novel Upper-Room UVC-LED Irradiation System for Disinfection of Indoor Bioaerosols under Different Operating and Airflow Conditions. Journal of Hazardous Materials 2020, 396, 122715. [Google Scholar] [CrossRef] [PubMed]
- Nunayon, S.S.; Zhang, H.; Lai, A.C.K. Comparison of Disinfection Performance of UVC-LED and Conventional Upper-Room UVGI Systems. Indoor Air 2020, 30, 180–191. [Google Scholar] [CrossRef] [PubMed]
- Umar, M.; Anglès d’Auriac, M.; Wennberg, A.C. Application of UV-LEDs for Antibiotic Resistance Genes Inactivation – Efficiency Monitoring with qPCR and Transformation. Journal of Environmental Chemical Engineering 2021, 9, 105260. [Google Scholar] [CrossRef]
- Didik, T.; Yau, A.P.-Y.; Cheung, H.L.; Lee, S.-Y.; Chan, N.-H.; Wah, Y.-T.; Luk, H.K.-H.; Choi, G.K.-Y.; Cheng, N.H.-Y.; Tse, H.; et al. Long-Range Air Dispersion of Candida Auris in a Cardiothoracic Unit Outbreak in Hong Kong. J Hosp Infect 2023, 142, 105–114. [Google Scholar] [CrossRef]
- Ghajari, A.; Lotfali, E.; Azari, M.; Fateh, R.; Kalantary, S. Fungal Airborne Contamination as a Serious Threat for Respiratory Infection in the Hematology Ward. Tanaffos 2015, 14, 257–261. [Google Scholar] [PubMed]
- Brown, C.S.; Guy, R. National Public Health Response to Candida Auris in England. J Fungi (Basel) 2019, 5, 93. [Google Scholar] [CrossRef] [PubMed]
- Dire, O.; Ahmad, A.; Duze, S.; Patel, M. Survival of Candida Auris on Environmental Surface Materials and Low-Level Resistance to Disinfectant. Journal of Hospital Infection 2023, 137, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Nobrega de Almeida, J.; Brandão, I.B.; Francisco, E.C.; de Almeida, S.L.R.; de Oliveira Dias, P.; Pereira, F.M.; Santos Ferreira, F.; de Andrade, T.S.; de Miranda Costa, M.M.; de Souza Jordão, R.T.; et al. Axillary Digital Thermometers Uplifted a Multidrug-susceptible Candida Auris Outbreak among COVID-19 Patients in Brazil. Mycoses 2021, 64, 1062–1072. [Google Scholar] [CrossRef] [PubMed]
- Rutala, W.A.; Bolomey, A.C.; Cadnum, J.L.; Donskey, C.J. Inactivation and/or Physical Removal of Candida Auris from Floors by Detergent Cleaner, Disinfectants, Microfiber, and Ultraviolet C Light (UV-C). Infection Control & Hospital Epidemiology, 2023; 1–3. [Google Scholar] [CrossRef]
- US EPA, O. EPA’s Registered Antimicrobial Products Effective Against Candida Auris [List P]. Available online: https://www.epa.gov/pesticide-registration/epas-registered-antimicrobial-products-effective-against-candida-auris-list (accessed on 6 March 2024).
- Goulart, M.A.; El Itani, R.; Buchanan, S.R.; Brown, D.S.; Hays, A.K.; King, W.B.; Luciani, D.L.; Neilsen, C.D.; Verdecia, J.L. Identification and Infection Control Response to Candida Auris at an Academic Level I Trauma Center. American Journal of Infection Control 2024, 52, 371–373. [Google Scholar] [CrossRef]
- Prestel, C.; Anderson, E.; Forsberg, K.; Lyman, M.; de Perio, M.A.; Kuhar, D.; Edwards, K.; Rivera, M.; Shugart, A.; Walters, M.; et al. Candida Auris Outbreak in a COVID-19 Specialty Care Unit — Florida, July–August 2020. MMWR Morb Mortal Wkly Rep 2021, 70, 56–57. [Google Scholar] [CrossRef]
- Ruiz-Gaitán, A.; Moret, A.M.; Tasias-Pitarch, M.; Aleixandre-López, A.I.; Martínez-Morel, H.; Calabuig, E.; Salavert-Lletí, M.; Ramírez, P.; López-Hontangas, J.L.; Hagen, F.; et al. An Outbreak Due to Candida Auris with Prolonged Colonisation and Candidaemia in a Tertiary Care European Hospital. Mycoses 2018, 61, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Horton, M.V.; Johnson, C.J.; Kernien, J.F.; Patel, T.D.; Lam, B.C.; Cheong, J.Z.A.; Meudt, J.J.; Shanmuganayagam, D.; Kalan, L.R.; Nett, J.E. Candida Auris Forms High-Burden Biofilms in Skin Niche Conditions and on Porcine Skin. mSphere 2020, 5, e00910–19. [Google Scholar] [CrossRef] [PubMed]
- Horton, M.V.; Nett, J.E. Candida Auris Infection and Biofilm Formation: Going beyond the Surface. Curr Clin Microbiol Rep 2020, 7, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Ledwoch, K.; Maillard, J.-Y. Candida Auris Dry Surface Biofilm (DSB) for Disinfectant Efficacy Testing. Materials (Basel) 2018, 12, 18. [Google Scholar] [CrossRef] [PubMed]
- Weber, D.J.; Rutala, W.A.; Sickbert-Bennett, E. Emerging Infectious Diseases, Focus on Infection Prevention, Environmental Survival and Germicide Susceptibility: SARS-CoV-2, Mpox, and Candida Auris. American Journal of Infection Control 2023, 51, A22–A34. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, V.; Ahmad, A. Abrogation of Pathogenic Attributes in Drug Resistant Candida Auris Strains by Farnesol. PLoS One 2020, 15, e0233102. [Google Scholar] [CrossRef] [PubMed]
- Salkin, I.F.; Krisiunas, E.; Turnberg, W.L. Medical and Infectious Waste Management. Journal of the American Biological Safety Association 2000, 5, 54–69. [Google Scholar] [CrossRef]
- World Health Organization Overview of Technologies for the Treatment of Infectious and Sharp Waste from Health Care Facilities; World Health Organization: Geneva, 2019; ISBN 978-92-4-151622-8.
- Rutala, W.A.; Weber, D.J. Disinfection, Sterilization, and Control of Hospital Waste. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, 2015; 3294–3309.e4. [Google Scholar] [CrossRef]
- Aziz, H.A.; Omar, F.M.; Halim, H.A.; Hung, Y.-T. Health-Care Waste Management. In Solid Waste Engineering and Management: Volume 3; Wang, L.K., Wang, M.-H.S., Hung, Y.-T., Eds.; Springer International Publishing: Cham, 2022; pp. 163–229. ISBN 978-3-030-96989-9. [Google Scholar]
- Street, A.; Vernooij, E.; Rogers, M.H. Diagnostic Waste: Whose Responsibility? Global Health 2022, 18, 30. [Google Scholar] [CrossRef] [PubMed]
- International Committee of the Red Cross Medical Waste Management; Geneva, Switzerland, 2015;
- Sater, M.; Farrell, T.; Pangestu, F.; Herriott, I.; Anahtar, M.; Kwon, D.; Shenoy, E.; Hooper, D.; Huntley, M. Democratizing Sequencing for Infection Control: A Scalable, Automated Pipeline for WGS Analysis for Outbreak Detection. Infection Control & Hospital Epidemiology 2020, 41, s442–s443. [Google Scholar] [CrossRef]
- Roselin, A.; Prasath, A.; Krishna, R.; Mohanarathinam, A. Clinical Waste Storage System with Contamination Prevention Mechanism Using UV and Arduino Microcontroller. In Proceedings of the 2023 International Conference on Inventive Computation Technologies (ICICT); April 2023; pp. 1585–1591. [Google Scholar]
- Okethwengu, H.; Amisiri, B.; Ogwang, E. A TECHNICAL REPORT ON THE DESIGN AND CONSTRUCTION OF A SMART WASTE BIN FOR MEDICAL WASTE MANAGEMENT. SJ Engineering Africa 2024, 1, 21–21. [Google Scholar] [CrossRef]
- Nicolau, T.; Gomes Filho, N.; Padrão, J.; Zille, A. A Comprehensive Analysis of the UVC LEDs’ Applications and Decontamination Capability. Materials (Basel) 2022, 15, 2854. [Google Scholar] [CrossRef] [PubMed]
- Matafonova, G.; Batoev, V. Recent Advances in Application of UV Light-Emitting Diodes for Degrading Organic Pollutants in Water through Advanced Oxidation Processes: A Review. Water Res 2018, 132, 177–189. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.Z.; Craik, S.A.; Bolton, J.R. Comparison of the Action Spectra and Relative DNA Absorbance Spectra of Microorganisms: Information Important for the Determination of Germicidal Fluence (UV Dose) in an Ultraviolet Disinfection of Water. Water Res 2009, 43, 5087–5096. [Google Scholar] [CrossRef] [PubMed]
- Lawal, O.; Cosman, J.; Pagan, J. UVSolutions. 2018,.
- Giese, N.; Darby, J. Sensitivity of Microorganisms to Different Wavelengths of UV Light: Implications on Modeling of Medium Pressure UV Systems. Water Research 2000, 34, 4007–4013. [Google Scholar] [CrossRef]
- Ramos, C.C.R.; Roque, J.L.A.; Sarmiento, D.B.; Suarez, L.E.G.; Sunio, J.T.P.; Tabungar, K.I.B.; Tengco, G.S.C.; Rio, P.C.; Hilario, A.L. Use of Ultraviolet-C in Environmental Sterilization in Hospitals: A Systematic Review on Efficacy and Safety. Int J Health Sci (Qassim) 2020, 14, 52–65. [Google Scholar] [PubMed]
- Gora, S.L.; Rauch, K.D.; Ontiveros, C.C.; Stoddart, A.K.; Gagnon, G.A. Inactivation of Biofilm-Bound Pseudomonas Aeruginosa Bacteria Using UVC Light Emitting Diodes (UVC LEDs). Water Research 2019, 151, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Gross, A.; Stangl, F.; Hoenes, K.; Sift, M.; Hessling, M. Improved Drinking Water Disinfection with UVC-LEDs for Escherichia Coli and Bacillus Subtilis Utilizing Quartz Tubes as Light Guide. Water 2015, 7, 4605–4621. [Google Scholar] [CrossRef]
- Kim, D.-K.; Kim, S.-J.; Kang, D.-H. Inactivation Modeling of Human Enteric Virus Surrogates, MS2, Qβ, and ΦX174, in Water Using UVC-LEDs, a Novel Disinfecting System. Food Research International 2017, 91, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Lee, U.; Jang, E.-S.; Lee, S.; Kim, H.-J.; Kang, C.-W.; Cho, M.; Lee, J. Near Dissolved Organic Matter Microfiltration (NDOM MF) Coupled with UVC LED Disinfection to Maximize the Efficiency of Water Treatment for the Removal of Giardia and Cryptosporidium. Water Research 2023, 233, 119731. [Google Scholar] [CrossRef]
- Mariita, R.M.; Davis, J.H.; Randive, R.V. Illuminating Human Norovirus: A Perspective on Disinfection of Water and Surfaces Using UVC, Norovirus Model Organisms, and Radiation Safety Considerations. Pathogens 2022, 11, 226. [Google Scholar] [CrossRef]
- Miralles-Cuevas, S.; De la Obra, I.; Gualda-Alonso, E.; Soriano-Molina, P.; Casas López, J.L.; Sánchez Pérez, J.A. Simultaneous Disinfection and Organic Microcontaminant Removal by UVC-LED-Driven Advanced Oxidation Processes. Water (20734441) 2021, 13, 1507. [Google Scholar] [CrossRef]
- Nyangaresi, P.O.; Qin, Y.; Chen, G.; Zhang, B.; Lu, Y.; Shen, L. Effects of Single and Combined UV-LEDs on Inactivation and Subsequent Reactivation of E. Coli in Water Disinfection. Water Research 2018, 147, 331–341. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Chu, X.N.; He, M.; Liu, X.C.; Hu, J.Y. Impact of UVA Pre-Radiation on UVC Disinfection Performance: Inactivation, Repair and Mechanism Study. Water Research 2018, 141, 279–288. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Acosta, N.; Bautista, M.A.; McCalder, J.; Himann, J.; Pogosian, S.; Hubert, C.R.J.; Parkins, M.D.; Achari, G. Quantitative Evaluation of Municipal Wastewater Disinfection by 280 Nm UVC LED. Water 2023, 15, NA. [Google Scholar] [CrossRef]
- Mariita, R.M.; Blumenstein, S.A.; Beckert, C.M.; Gombas, T.; Randive, R.V. Disinfection Performance of a Drinking Water Bottle System With a UV Subtype C LED Cap Against Waterborne Pathogens and Heterotrophic Contaminants. Front Microbiol 2021, 12, 719578. [Google Scholar] [CrossRef] [PubMed]
- Sundar, K.P.; Kanmani, S. Design and Evaluation of Zero-Energy UVC-LED Reactor Fitted with Hand Pump System for Disinfection. AQUA - Water Infrastructure, Ecosystems and Society 2020, 70, 77–88. [Google Scholar] [CrossRef]
- Vitzilaiou, E.; Kuria, A.M.; Siegumfeldt, H.; Rasmussen, M.A.; Knøchel, S. The Impact of Bacterial Cell Aggregation on UV Inactivation Kinetics. Water Research 2021, 204, 117593. [Google Scholar] [CrossRef] [PubMed]
- Nyangaresi, P.O.; Zhang, B.; Shen, L.; Nyangaresi, P.O.; Zhang, B.; Shen, L. Effects of UV-LED Irradiation on E. Coli in Water Disinfection. In E. Coli Infections - Importance of Early Diagnosis and Efficient Treatment; IntechOpen, 2020 ISBN 978-1-83962-524-4.
- Faretra, G. The Power of UV Treatment for Wastewater. Wastewater Digest 2023.
- Rossi, A.; Chavez, J.; Iverson, T.; Hergert, J.; Oakeson, K.; LaCross, N.; Njoku, C.; Gorzalski, A.; Gerrity, D. Candida Auris Discovery through Community Wastewater Surveillance during Healthcare Outbreak, Nevada, USA, 2022. Emerging Infectious Diseases journal 2023, 29. [Google Scholar] [CrossRef]
- Shen, L.; Griffith, T.M.; Nyangaresi, P.O.; Qin, Y.; Pang, X.; Chen, G.; Li, M.; Lu, Y.; Zhang, B. Efficacy of UVC-LED in Water Disinfection on Bacillus Species with Consideration of Antibiotic Resistance Issue. Journal of Hazardous Materials 2020, 386, 121968. [Google Scholar] [CrossRef]
- Yadav, M.; Gole, V.L.; Sharma, J.; Yadav, R.K. Biologically Treated Industrial Wastewater Disinfection Using Synergy of US, LED-UVS, and Oxidants. Chemical Engineering and Processing - Process Intensification 2021, 169, 108646. [Google Scholar] [CrossRef]
- Sowndarya, S.; Kanmani, S.; Amal Raj, S. Disinfection of Biologically Treated Sewage Using AlGaN-Based Ultraviolet-C Light-Emitting Diodes in a Novel Reactor System. DWT 2021, 212, 71–77. [Google Scholar] [CrossRef]
- Leong, D.; Chen, H.-B.; Wang, G.-S. Application of UVC-LED/H2O2 in Wastewater Treatments: Treatment Efficacy on Disinfection Byproduct Precursors and Micropollutants. Sustain Environ Res 2023, 33, 33. [Google Scholar] [CrossRef]
- Kim, S.-S.; Shin, M.; Kang, J.-W.; Kim, D.-K.; Kang, D.-H. Application of the 222 nm Krypton-Chlorine Excilamp and 280 nm UVC Light-Emitting Diode for the Inactivation of Listeria Monocytogenes and Salmonella Typhimurium in Water with Various Turbidities. LWT 2020, 117, 108458. [Google Scholar] [CrossRef]
- Park, S.-K.; Jo, D.-M.; Kang, M.-G.; Khan, F.; Hong, S.D.; Kim, C.Y.; Kim, Y.-M.; Ryu, U.-C. Bactericidal Effect of Ultraviolet C Light-Emitting Diodes: Optimization of Efficacy toward Foodborne Pathogens in Water. Journal of Photochemistry and Photobiology B: Biology 2021, 222, 112277. [Google Scholar] [CrossRef] [PubMed]
- Betzalel, Y.; Gerchman, Y.; Cohen-Yaniv, V.; Mamane, H. Multiwell Plates for Obtaining a Rapid Microbial Dose-Response Curve in UV-LED Systems. Journal of Photochemistry and Photobiology B: Biology 2020, 207, 111865. [Google Scholar] [CrossRef] [PubMed]
- Song, K.; Mohseni, M.; Taghipour, F. Mechanisms Investigation on Bacterial Inactivation through Combinations of UV Wavelengths. Water Research 2019, 163, 114875. [Google Scholar] [CrossRef] [PubMed]
- Shin, M.; Kim, S.-S.; Kang, D.-H. Combined Treatment with a 222-Nm Krypton-Chlorine Excilamp and a 280-Nm LED-UVC for Inactivation of Salmonella Typhimurium and Listeria Monocytogenes. LWT 2020, 131, 109715. [Google Scholar] [CrossRef]
- Gora, S.L.; Rauch, K.D.; Ontiveros, C.C.; Stoddart, A.K.; Gagnon, G.A. Inactivation of Biofilm-Bound Pseudomonas Aeruginosa Bacteria Using UVC Light Emitting Diodes (UVC LEDs). Water Research 2019, 151, 193–202. [Google Scholar] [CrossRef]
- Schreier, W.J.; Kubon, J.; Regner, N.; Haiser, K.; Schrader, T.E.; Zinth, W.; Clivio, P.; Gilch, P. Thymine Dimerization in DNA Model Systems: Cyclobutane Photolesion Is Predominantly Formed via the Singlet Channel. J. Am. Chem. Soc. 2009, 131, 5038–5039. [Google Scholar] [CrossRef]
- Gullotto, C.; Dragoni, L.; Amodeo, D.; Cevenini, G.; Nante, N.; Messina, G. Air Purifiers, Comparison between Real and Declared Surface for Use: Fake It or Make It? European Journal of Public Health 2022, 32, ckac131–249. [Google Scholar] [CrossRef]
- Kahn, K.; Mariita, R.M. Quantifying the Impact of Ultraviolet Subtype C in Reducing Airborne Pathogen Transmission and Improving Energy Efficiency in Healthy Buildings: A Kahn–Mariita Equivalent Ventilation Model. Front. Built Environ. 2021, 7. [Google Scholar] [CrossRef]
- Kowalski, W. Airstream Disinfection. In Ultraviolet Germicidal Irradiation Handbook: UVGI for Air and Surface Disinfection; Kowalski, W., Ed.; Springer: Berlin, Heidelberg, 2009; pp. 177–209. ISBN 978-3-642-01999-9. [Google Scholar]
- Kowalski, W. Ultraviolet Germicidal Irradiation Handbook: UVGI for Air and Surface Disinfection; Springer Berlin Heidelberg: Berlin, Heidelberg, 2009; ISBN 978-3-642-01998-2. [Google Scholar]
- Muramoto, Y.; Kimura, M.; Kondo, A. Verification of Inactivation Effect of Deep-Ultraviolet LEDs on Bacteria and Viruses, and Consideration of Effective Irradiation Methods - IOPscience. Japanese Journal of Applied Physics 2021, 60. [Google Scholar] [CrossRef]
- Nicolau, T.; Gomes Filho, N.; Padrão, J.; Zille, A. A Comprehensive Analysis of the UVC LEDs’ Applications and Decontamination Capability. Materials 2022, 15, 2854. [Google Scholar] [CrossRef] [PubMed]
- Wood, J.P.; Archer, J.; Calfee, M.W.; Serre, S.; Mickelsen, L.; Mikelonis, A.; Oudejans, L.; Hu, M.; Hurst, S.; Rastogi, V.K. Inactivation of Bacillus Anthracis and Bacillus Atrophaeus Spores on Different Surfaces with Ultraviolet Light Produced with a Low-pressure Mercury Vapor Lamp or Light Emitting Diodes. Journal of Applied Microbiology 2021, 131, 2257–2269. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Kang, D.-H. Effect of Surface Characteristics on the Bactericidal Efficacy of UVC LEDs. Food Control 2020, 108, 106869. [Google Scholar] [CrossRef]
- Trivellin, N.; Buffolo, M.; Onelia, F.; Pizzolato, A.; Barbato, M.; Orlandi, V.T.; Del Vecchio, C.; Dughiero, F.; Zanoni, E.; Meneghesso, G.; et al. Inactivating SARS-CoV-2 Using 275 Nm UV-C LEDs through a Spherical Irradiation Box: Design, Characterization and Validation. Materials 2021, 14, 2315. [Google Scholar] [CrossRef] [PubMed]
- Rutala, W.A.; Weber, D.J. Are Room Decontamination Units Needed to Prevent Transmission of Environmental Pathogens? Infection Control & Hospital Epidemiology 2011, 32, 743–747. [Google Scholar] [CrossRef]
- Pearlmutter, B.S.; Haq, M.F.; Cadnum, J.L.; Jencson, A.L.; Carlisle, M.; Donskey, C.J. Efficacy of Relatively Low-Cost Ultraviolet-C Light Devices against Candida Auris. Infection Control & Hospital Epidemiology 2022, 43, 747–751. [Google Scholar] [CrossRef]
- Lemons, A.R.; McClelland, T.L.; Martin, S.B.; Lindsley, W.G.; Green, B.J. Inactivation of the Multi-Drug-Resistant Pathogen Candida Auris Using Ultraviolet Germicidal Irradiation. Journal of Hospital Infection 2020, 105, 495–501. [Google Scholar] [CrossRef]
- Cadnum, J.L.; Shaikh, A.A.; Piedrahita, C.T.; Jencson, A.L.; Larkin, E.L.; Ghannoum, M.A.; Donskey, C.J. Relative Resistance of the Emerging Fungal Pathogen Candida Auris and Other Candida Species to Killing by Ultraviolet Light. Infect Control Hosp Epidemiol 2018, 39, 94–96. [Google Scholar] [CrossRef] [PubMed]
- de Groot, T.; Chowdhary, A.; Meis, J.F.; Voss, A. Killing of Candida Auris by UV-C: Importance of Exposure Time and Distance. Mycoses 2019, 62, 408–412. [Google Scholar] [CrossRef] [PubMed]
- Karidis, A. Waste Management Pros Build UV Sanitizer for Health Providers. Waste 360 2020.
- Manda, V.; Balachandran, S.; Danaboina; Roopak; Batchu, S. R.S.; Raj, S.; Kumar, janagam; Govindu, S.; Mahesh, D.; Houji, R.; et al. UV Sterilizing Dustbin. International Journal for Modern Trends in Science and Technology 2021, 7, 71–75. [Google Scholar]
- Hull, N.M.; Herold, W.H.; Linden, K.G. UV LED Water Disinfection: Validation and Small System Demonstration Study. AWWA Water Science 2019, 1, e1148. [Google Scholar] [CrossRef]
- Wu, J.; Cao, M.; Tong, D.; Finkelstein, Z.; Hoek, E.M.V. A Critical Review of Point-of-Use Drinking Water Treatment in the United States. npj Clean Water 2021, 4, 1–25. [Google Scholar] [CrossRef]
- Nguyen, T.M.H.; Suwan, P.; Koottatep, T.; Beck, S.E. Application of a Novel, Continuous-Feeding Ultraviolet Light Emitting Diode (UV-LED) System to Disinfect Domestic Wastewater for Discharge or Agricultural Reuse. Water Res 2019, 153, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Pramanik, P.; Das, S.; Adhikary, A.; Chaudhuri, C.R.; Bhattacharyya, A. Design and Implementation of Water Purification System Based on Deep Ultraviolet Light Emitting Diodes and a Multi-Pass Geometry Reactor. Journal of Water and Health 2020, 18, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Sundar, K.P.; Kanmani, S. Design and Evaluation of Zero-Energy UVC-LED Reactor Fitted with Hand Pump System for Disinfection. AQUA - Water Infrastructure, Ecosystems and Society 2020, 70, 77–88. [Google Scholar] [CrossRef]
- Mkilima, T.; Sabitov, Y.; Shakhmov, Z.; Abilmazhenov, T.; Tlegenov, A.; Jumabayev, A.; Turashev, A.; Kaliyeva, Z.; Utepbergenova, L. Exploring the Potential of Biofunctionalized Agricultural Waste Adsorbents Integrated with UV-LED Disinfection for Enhanced Wastewater Treatment. Case Studies in Chemical and Environmental Engineering 2024, 9, 100691. [Google Scholar] [CrossRef]
- Ethington, T.; Newsome, S.; Waugh, J.; Lee, L.D. Cleaning the Air with Ultraviolet Germicidal Irradiation Lessened Contact Infections in a Long-Term Acute Care Hospital. American Journal of Infection Control 2018, 46, 482–486. [Google Scholar] [CrossRef] [PubMed]
- Kane, D.W.; Finley, C.; Brown, D. UV-C Light and Infection Rate in a Long Term Care Ventilator Unit: Canadian Journal of Infection Control / Revue Canadienne de Prévention Des Infections. CAN J INFECT CONTROL 2018, 33, 44–48. [Google Scholar]
- Astrid, F.; Beata, Z.; Van den Nest Miriam; Julia, E. ; Elisabeth, P.; Magda, D.-E. The Use of a UV-C Disinfection Robot in the Routine Cleaning Process: A Field Study in an Academic Hospital. Antimicrobial Resistance & Infection Control 2021, 10, 84. [Google Scholar] [CrossRef]
- Kelly, S.; Schnugh, D.; Thomas, T. Effectiveness of Ultraviolet-C vs Aerosolized Hydrogen Peroxide in ICU Terminal Disinfection. Journal of Hospital Infection 2022, 121, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Anderson, D.J.; Knelson, L.P.; Moehring, R.W.; Lewis, S.S.; Weber, D.J.; Chen, L.F.; Triplett, P.F.; Blocker, M.; Cooney, R.M.; Schwab, J.C.; et al. Implementation Lessons Learned From the Benefits of Enhanced Terminal Room (BETR) Disinfection Study: Process and Perceptions of Enhanced Disinfection with Ultraviolet Disinfection Devices. Infection Control & Hospital Epidemiology 2018, 39, 157–163. [Google Scholar] [CrossRef]
- Demeersseman, N.; Saegeman, V.; Cossey, V.; Devriese, H.; Schuermans, A. Shedding a Light on Ultraviolet-C Technologies in the Hospital Environment. Journal of Hospital Infection 2023, 132, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Gullotto, C.; Sparacino, M.; Amodeo, A.; Cevenini, G.; Nante, N.; Messina, G. Which One to Choose? A Cost-Effectiveness Analysis between Different Technologies of Air Purifiers. European Journal of Public Health 2022, 32, ckac131–250. [Google Scholar] [CrossRef]
- A: Health Organization Energizing Health, 2023.
- United Nations Development Programme Solar for Health. Available online: https://www.undp.org/energy/our-flagship-initiatives/solar-for-health (accessed on 21 March 2024).
- R-Zero How UV-C Light Can Help Combat the Spread of Candida Auris. R-Zero, 2023.
- Peasah, S.; McKay, N.; Harman, J.; Al-Amin, M.; Cook, R. Medicare Non-Payment of Hospital-Acquired Infections: Infection Rates Three Years Post Implementation. MMRR 2013, 3, E1–E16. [Google Scholar] [CrossRef] [PubMed]
- Cohen, C.C.; Liu, J.; Cohen, B.; Larson, E.L.; Glied, S. Financial Incentives to Reduce Hospital-Acquired Infections Under Alternative Payment Arrangements. Infect Control Hosp Epidemiol 2018, 39, 509–515. [Google Scholar] [CrossRef]
- Insero, B. How to Calculate Cleaning Times. ISSA 2022.
- 2024.
- ASHRAE ASHRAE Standards and Guidelines. Available online: https://www.ashrae.org/technical-resources/ashrae-standards-and-guidelines (accessed on 21 March 2024).
- International Organization for Standardization ISO 15858:2016(En), UV-C Devices — Safety Information — Permissible Human Exposure 2016.
- NSF International NSF/ANSI 55-2022 - Ultraviolet Microbiological Water Treatment Systems 2022.
- Zollner, C.J.; DenBaars, S.P.; Speck, J.S.; Nakamura, S. Germicidal Ultraviolet LEDs: A Review of Applications and Semiconductor Technologies. Semicond. Sci. Technol. 2021, 36, 123001. [Google Scholar] [CrossRef]
Figure 1.
The global distribution of Candida auris is categorized into four clades based on phylogenetic analysis and geographic origin. Reprinted from [65].
Figure 1.
The global distribution of Candida auris is categorized into four clades based on phylogenetic analysis and geographic origin. Reprinted from [65].
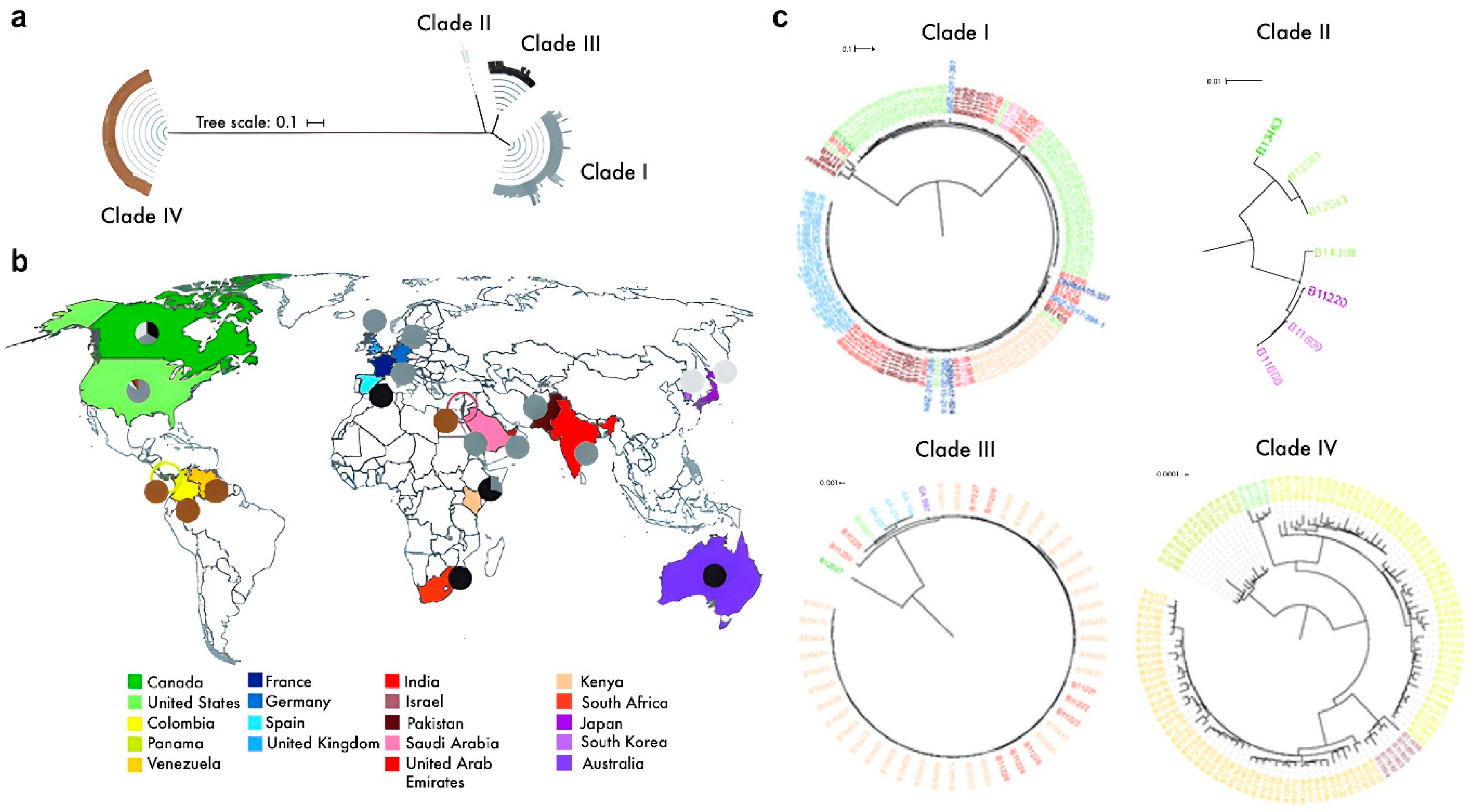
Figure 2.
Illustration of potential multi-layered UVC LED protocol for enhanced infection prevention and control in a healthcare environment. UVC LED disinfection is not suggested to replace standard or regulated infection prevention protocols. (Image created using icons designed by Freepik).
Figure 2.
Illustration of potential multi-layered UVC LED protocol for enhanced infection prevention and control in a healthcare environment. UVC LED disinfection is not suggested to replace standard or regulated infection prevention protocols. (Image created using icons designed by Freepik).
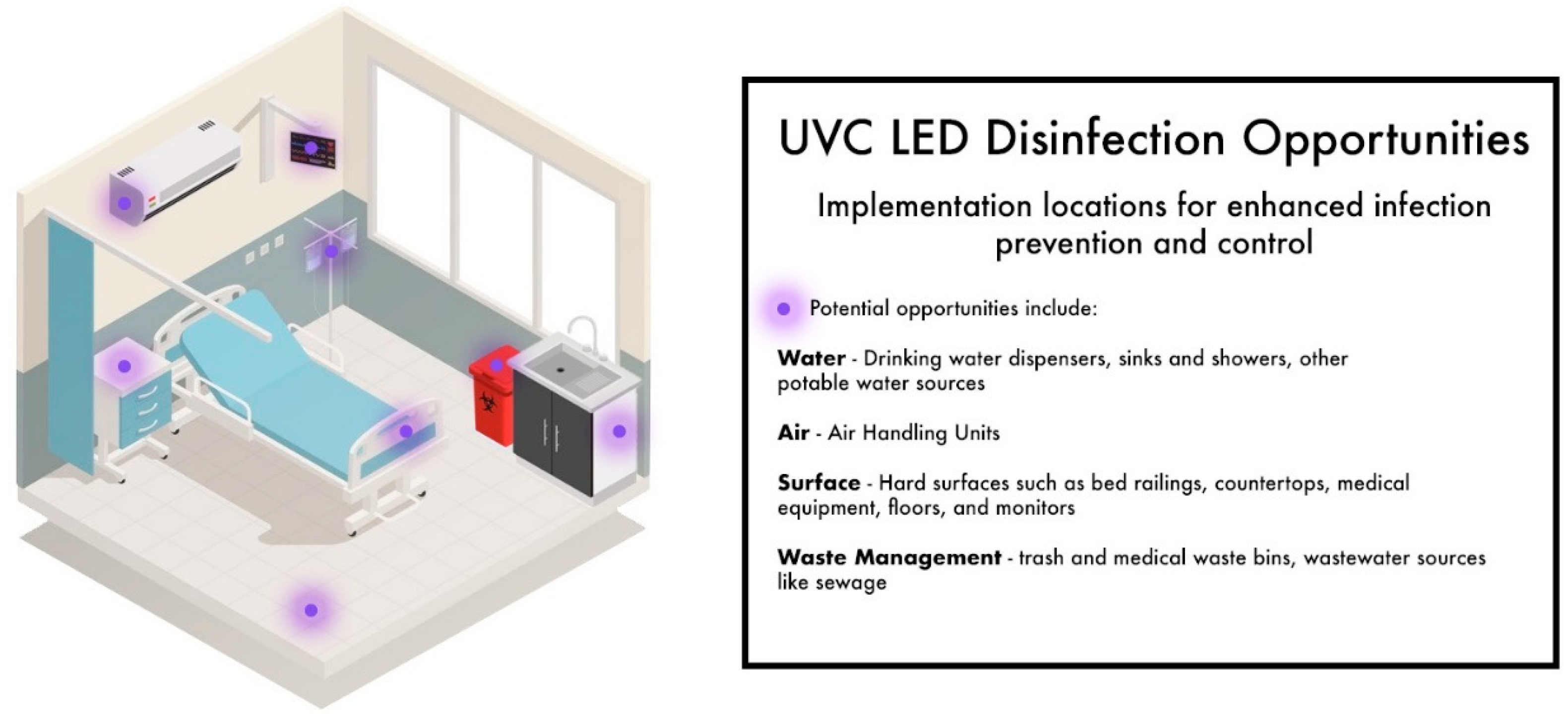

Table 1.
Global Mortality Estimates – Global Crude Mortality Rates Attributable to Candidemia .
| Country | Mortality Rate (estimated) | Date | Citation |
|---|---|---|---|
| Pakistan | 52% | 2009 | (Farooqi et al., 2013) [105] |
| India | 50%* | 2009-2011 | (Chowdhary et al., 2013) [68] |
| 44% | (Pfaller & Diekema, 2007) [106] | ||
| South Africa | 46% | 2012 | (Smidt et al., 2014) [107] |
| Panama | 78%* | 2017 | (Araúz et al., 2018) [96] |
| Venezuela | 28%* | 2012 – 2013 | (Calvo et al., 2016) [97] |
| Brazil | 72% | 2007 – 2010 | (Doi et al., 2016) [108] |
| Columbia | 43% | 2015 – 2016 | (Armstrong et al., 2019) [66] |
| England (3 London hospitals) | 14.5%* | 2015 – 2018 | (Taori et al., 2019) [109] |
| India, US, UK (combined systematic review) | 30%* | _____ | (Osei Sekyere, 2018) [23] |
*Rate attributed specifically to C. auris.
Table 2.
Global Economic Burden of Fungal Disease and Antimicrobial Resistance.
| Economic Burden | Cost Estimate ($USD)* | Cost Type | Source | Citation |
|---|---|---|---|---|
| AMR disease burden | ||||
| Europe | $9.77 billion | Total burden | (Prestinaci et al., 2015) [3] | |
| United States | $55 billion | Total Burden | CDC | (Dadgostar, 2019) [6] |
| $20 billion | Direct healthcare costs | |||
| $35 billion | Loss of productivity | |||
| Fungal Disease Burden | ||||
| $11.5 billion | Total burden | CDC | (Benedict et al., 2019, 2022; Kumar et al., 2022) [59,124,125] | |
| $7.5 billion | Direct healthcare costs | |||
| $870 million | Loss of productivity | |||
| $3.2 billion | Premature death | |||
| Candidiasis & Candidemia Burden | ||||
| Noninvasive Candidiasis | $2.5 billion | Total Cost Burden | CDC | (Benedict et al., 2019, 2022) [124,125] |
| Invasive Candidiasis | $1.7 billion | Total Cost Burden | ||
| $1.2 billion | Direct medical costs | |||
| $75 million | Loss of productivity | |||
| $450 million | Premature death | |||
| Western Developed Countries | Range: $48,487 - $157,574 | Cost per patient | Systematic Review | (Wan Ismail et al., 2020) [126] |
| Western Developed Countries | Range: $10,216 -$37,715 | Cost per hospitalization | Systematic Review | |
| London Outbreak | $1.2 million | At time of outbreak | Institutional Report | (Taori et al., 2019) [109] |
| $73,000 per month | Year to year post-outbreak | |||
*All economic estimates are indicated in US dollars. Any global economic impact reports have been converted to US dollars from the primary source for this review.
Table 3.
UVC efficacy in inactivating C. auris is found with 267 and 270 nm peak wavelengths, and log reduction value (LRV) 3 (99.9% reduction) is obtained.
Table 3.
UVC efficacy in inactivating C. auris is found with 267 and 270 nm peak wavelengths, and log reduction value (LRV) 3 (99.9% reduction) is obtained.
| Peak wavelength (nm) | Time (s) | Dose (mJ/cm−2) | Controls (CFU ml−1 ) | UVC treated (CFU ml−1 ) | Log Reduction Value (LRV) | % Reduction | Susceptibility constant (k) (cm2 mJ) | References |
|---|---|---|---|---|---|---|---|---|
| 252 | 5 10 20 40 |
5 10 20 40 |
8.60E + 05 8.60E + 05 8.60E + 05 8.60E + 05 |
3.67E + 05 2.43E + 05 7.67E + 04 9.33E + 02 |
0.37 0.55 1.05 2.96 |
57.336 71.744 91.081 99.892 |
0.0691 | (Mariita et al., 2022) [54] |
| 261 | 5 10 20 40 |
5 10 20 40 |
8.60E + 05 8.60E + 05 8.60E + 05 8.60E + 05 |
5.47E + 05 2.03E + 05 5.50E + 04 5.21E + 03 |
0.20 0.63 1.20 2.22 |
36.617 76.477 93.627 99.396 |
0.0565 | (Giese & Darby, 2000) [178] |
| 267 | 5 10 20 40 |
5 10 20 40 |
6.40E + 05 6.40E + 05 6.40E + 05 6.40E + 05 |
2.50E + 05 4.33E + 04 2.33E + 02 1.00E + 01 |
0.41 1.17 3.44 4.81 |
60.938 93.234 99.964 99.998 |
0.1294 | (Mariita et al., 2022) [54] |
| 270 | 5 10 20 40 |
5 10 20 40 |
9.53E + 05 9.53E + 05 9.53E + 05 9.53E + 05 |
3.33E + 05 6.33E + 04 3.33E + 02 2.33E + 01 |
0.46 1.18 3.46 4.61 |
65.058 93.358 99.965 99.998 |
0.126 | (Giese & Darby, 2000) [178] |
| 273 | 5 10 20 40 |
5 10 20 40 |
8.00E + 05 8.00E + 05 8.00E + 05 8.00E + 05 |
3.27E + 05 1.07E + 05 2.03E + 03 3.67E + 01 |
0.39 0.88 2.59 4.34 |
59.125 86.625 99.746 99.995 |
0.111 | (Mariita et al., 2022) [54] |
| 280 | 5 10 20 40 |
5 10 20 40 |
4.07E + 05 4.07E + 05 4.07E + 05 4.07E + 05 |
2.07E + 05 1.70E + 05 2.87E + 04 4.00E + 01 |
0.29 0.38 1.16 4.01 |
49.140 58.537 93.000 99.990 |
0.0889 | (Mariita et al., 2022) [54] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



