Submitted:
25 July 2024
Posted:
26 July 2024
You are already at the latest version
Abstract
Proactive deprescribing is the process of stopping a medicine before harm occurs. This study aimed to specify and validate with an international sample of healthcare professionals, a proactive deprescribing process of steps and constituent activities. We developed a proactive deprescribing process framework of steps which we populated with literature-derived activities required to be undertaken by healthcare professionals. We distributed a survey to healthcare professionals in-ternationally requesting for each activity; the frequency of its occurrence in practice and whether it was important. Extended response questions invited barriers and enablers to deprescribing. The 263 survey respondents were from 25 countries. A proactive deprescribing process was developed comprising four steps: (1) Identify a patient for potential stop of a medicine, (2) Evaluate a patient for potential stop of a medicine, (3) Stop a medicine(s), (4) After a medicine has been stopped, and 17 activities. All activities were considered important by ≥70% respondents. Nine activities re-quired healthcare professionals to undertake in direct partnership with the patient and/or care-giver, of which seven were only sometimes undertaken. Deprescribing interventions should focus on addressing the barriers and enablers of healthcare professionals undertaking the activities that require direct partnership with the patient and/or caregiver.
Keywords:
polypharmacy
; shared decision making
; behaviour change
; intervention
; deprescription
1. Introduction
Deprescribing is the process of tapering or stopping medicines to minimise unnecessary polypharmacy and improve medicines-related outcomes [1]. Deprescribing may be undertaken reactively in response to harm caused by a medicine or proactively in order to prevent a medicine causing harm in the future [2]. Reactive deprescribing requires relatively simple decision-making and is widely accepted as being routine practice [2,3,4]. Proactive deprescribing is a component of Good Prescribing Practice [5], which requires prescribers to regularly evaluate, in partnership with the patient, the ongoing suitability of the medicines that they prescribe. Routine proactive deprescribing aims to prevent harm and avoids the need to reactively deprescribe medicines.
Trials of proactive deprescribing have demonstrated that it is safe and leads to positive outcomes including a reduction in polypharmacy, falls and admissions to hospital [6,7,8]. Despite the recognised benefits and development of numerous interventions to increase healthcare professionals’ proactive deprescribing behaviour [9], it is not routine practice [2,10,11]. Whilst approximately 50% of older adults admitted to hospital are prescribed at least one medicine that should be stopped, an evaluation of 2309 older adults in the United Kingdom hospital setting found that less than 1% have a medicine proactively deprescribed [2].
There is a substantial body of research describing healthcare professionals’ barriers and enablers (determinants) to proactive deprescribing. A systematic review reported that knowledge gaps, insufficient time and perceived resistance from patients are barriers [3]. Proactive deprescribing is a complex process and for it to be undertaken safely, healthcare professionals must undertake a series of activities. Some of activities may already be routinely undertaken, for example undertaking a medication history on admission to hospital, whilst others may be more challenging and require interventions to support healthcare professionals to undertake them [12].
Avoiding redundancy when developing interventions is essential in order to minimise complexity and focus resources efficiently [13]. There is a need to identify and define the activities that healthcare professionals find most challenging when undertaking proactive deprescribing. This permits diagnosis of the barriers and enablers of these challenging activities and subsequently the development of interventions that address them.
The full breadth of activities that healthcare professionals are required to undertake proactive deprescribing are yet to be established. Numerous deprescribing processes which provide overarching steps been proposed however there is substantial heterogeneity in content and none describe the constituent activities that healthcare professionals should undertake [14]. Processes describe one or a combination of the following steps [14]: 1) Medication history 2) Identify inappropriate medicines 3) Evaluate suitability of deprescribing 4) Plan and deprescribe and 5) Monitor. Whilst these overarching steps provide a high-level indication of what should be achieved during the proactive deprescribing process, there remains a need to specify the activities within these steps that healthcare professionals should undertake. For example, specifying activities that require the healthcare professional to work in partnership with the patient and/or informal caregiver to undertake deprescribing that is borne out of shared decision-making [15]. Once the full breadth of activities has been specified, there is a need to establish which are already routinely undertaken and which require targeting by interventions.
This study aimed to specify and validate with an international sample of healthcare professionals, a proactive deprescribing process of steps and constituent activities. We also aimed to estimate the extent to which the activities are undertaken in practice and for those not routinely undertaken, to identify the determinants that require addressing by deprescribing interventions.
2. Materials and Methods
Developing a Draft Proactive Deprescribing Process of Steps and Activities
We worked with our stakeholder group (n=8) of UK-based patients and caregivers with lived experience of deprescribing and doctors, nurses and pharmacists who were independent of the research team and whose clinical role includes deprescribing.
We developed a proactive deprescribing process framework comprising the following five overarching steps derived from 10 articles [16,17,18,19,20,21,22,23,24,25] identified from an existing literature review of deprescribing processes by Reeve et al. [14]: 1) Medication history 2) Identify inappropriate medicines 3) Evaluate suitability of deprescribing 4) Plan and deprescribe and 5) Monitor. We then populated the framework with the activities required to be undertaken by healthcare professionals in order to fulfil each step. With guidance from the stakeholder group, we also indicated which activities require healthcare professionals to undertake in direct partnership with the patient or caregiver.
Two researchers (DB and PW) independently reviewed the 10 articles [16,17,18,19,20,21,22,23,24,25] from which the five overarching steps were derived and extracted descriptions of deprescribing activities required to be undertaken by healthcare professionals. We mapped activity descriptions to the relevant deprescribing step based on their relatedness. Any similar or overlapping activities were combined. We compared mapping between researchers and harmonised terminology between activities e.g., care recipient, patient, older adult was harmonised to patient. We refined the mapping and terminology by seeking feedback from the stakeholder group. This resulted in a draft process of proactive deprescribing steps and constituent activities.
Validation of the Proactive Deprescribing Process of Steps and Activities
We validated the draft process using an online survey distributed to an international audience of healthcare professionals across several health systems.
Survey Development
We produced the online survey incorporating items inviting respondents to indicate on a 5-point Likert scale from ‘never’ to ‘always’, how often they thought each deprescribing activity from the draft process was currently undertaken. Items were phrased to ask respondents to respond based on what they thought their peer group did, rather than their own behaviour, to reduce the chance of social desirability bias [26]. For each activity, we included a second item to capture the extent to which respondents felt that an activity was sufficiently important to be part of the deprescribing process. The response options were on a 3-point Likert scale of ‘not important’, ‘unsure’ and ‘important’. We included an item asking respondents to indicate whether they used any tools or guidelines to support them with identifying inappropriate medicines. Finally, we included two global items; the first inviting respondents to indicate how often they thought their peers successfully involved patients/caregivers in the process of deprescribing and the second, inviting respondents to indicate how successful they were in deprescribing on a scale of 1 (never unsuccessful) to 10 (always successful). This was followed by two extended response items inviting healthcare professionals to report any barriers and enablers to them undertaking the deprescribing activities.
We piloted and refined the survey with the stakeholder group in order to establish face validity.
Survey Distribution
Ethical approval was secured from [REDACTED] research ethics committee to undertake an international cross-sectional survey of healthcare professionals whose role includes deprescribing. An invitation to complete the survey was distributed internally via relevant organisations and networks including our social media, professional bodies and networks representing healthcare professionals. Members of these organisations were eligible if they were a doctor, nurse, pharmacist or other healthcare professional, whose role involved prescribing. The survey was hosted on Microsoft ® Forms (Appendix A) from November 2020 to April 2021. It comprised an embedded information leaflet and electronic confirmation of consent. Non-identifiable demographic information to enable us to characterise the respondent population was captured.
Sample Size Justification
The study did not aim to detect any differences between respondent groups thus no formal sample size calculation was performed. We used the convention of setting a minimum and maximum target sample size for survey responses of 100 and 1000 responses respectively [27]. Based on 50% of participants selecting the midpoint value (i.e., 5) for the global deprescribing success item, 100 responses provides a 95% confidence interval (CI) of ± 9.8%, providing acceptable precision [27,28].
Analysis
We calculated descriptive statistics using IBM SPSS version 27 to characterise the respondent population and report survey responses. For each deprescribing activity we calculated the percentage of respondents indicating that it is important. We considered an activity as important if ≥70% of respondents rated it as important [29]. We calculated the median and interquartile (IQ) frequency with which each deprescribing activity was reported to be currently undertaken and for the global item regarding successfully involved patients/caregivers in the process of deprescribing. For respondents’ personal perceived level of deprescribing success on the 10-point scale, we reported the mean and 95% CI.
We performed a content analysis on the extended response data in Microsoft® Excel, coding for barriers and enablers to deprescribing [30]. The barriers and enablers were mapped to the relevant domain of the Theoretical Domains Framework (TDF) by a research pharmacist (NB); mapping was checked by researchers experienced in using the TDF (SS and DB) [4].
3. Results
Developing a Draft Process of Proactive Deprescribing Steps and Activities
We extracted 17 activities from the 10 articles [16,17,18,19,20,21,22,23,24,25]; nine of which were deemed by our stakeholder group to require direct partnership with the patient/caregiver. Appendix B provides the data extracted from the 10 articles and the activities these underpinned. Based on feedback from our stakeholder group, we refined the deprescribing process framework by combining Step 1 (Medication history) and Step 2 (Identify inappropriate medicines) into: Identifying a patient for potential stop of a medicine. This was in recognition of stakeholders’ view that activities within these steps are often undertaken simultaneously in practice. They also recommended minor rephrasing of the other three steps.
Table 1 provides the four overarching deprescribing steps, the 17 constituent activities and the articles from which activities were derived. Appendix B provides the data underpinning the activities that we extracted from each article. Three articles contributed five activities [17,24,25], one article contributed four [20], four articles contributed two [16,18,22,23] and two articles contributed a single activity [19,21].
Validation of the Proactive Deprescribing Process of Steps and Activities
Of the 263 survey respondents, 110 (41.8%) were doctors, 85 (32.3%) pharmacists, 44 (16.7%) nurses and 24 (9.1%) were other healthcare professionals. Most doctors (87 (79.0%)) were hospital specialists and the remainder were family physicians. Europe accounted for 186 (69.9%) respondents spanning 10 countries, 26 (9.9%) respondents were from two countries in North America, five (2.0%) were from four countries in South America, six (2.4%) were from six countries in Asia, four (1.5%) were from Egypt, eight (2.4%) were from Australia and one from New Zealand.
All 17 deprescribing activities met the threshold of ≥70% respondents considering them important. Figure 1 provides the reported frequency of deprescribing activities being undertaken within respondents’ peer group. The only activity with a median score of 5 indicating that it was perceived to always happen within the peer group of respondents was ‘asking the patient/relative to disclose all medications they are taking’. Seven of the nine activities to be undertaken in direct partnership with the patient/caregiver were only ‘sometimes’ undertaken. The activity perceived to be undertaken with the lowest frequency with a lower quartile of respondents indicating that it occurs rarely was ‘asking the patient/relative about their thoughts and experiences of taking their medication’.
In step 2 of evaluating a patient for potential to stop a medicine, 160 (60.8%) respondents cited a tool or resource to help evaluate the likelihood of harm or benefit from a medicine.
The median (IQ) for the global item inviting respondents to indicate how often they thought their peers successfully involved patients/caregivers in the process of deprescribing was 3 (3, 4) indicating that they perceived the majority of their peers to only sometimes achieve this outcome.
The mean (95% CI) of 7.13 (±0.19) on the scale of 1 to 10 for perceived level of deprescribing success indicated that respondents perceived themselves successful in deprescribing in over two thirds of situations where they feel that a medicine is inappropriate and should be stopped.
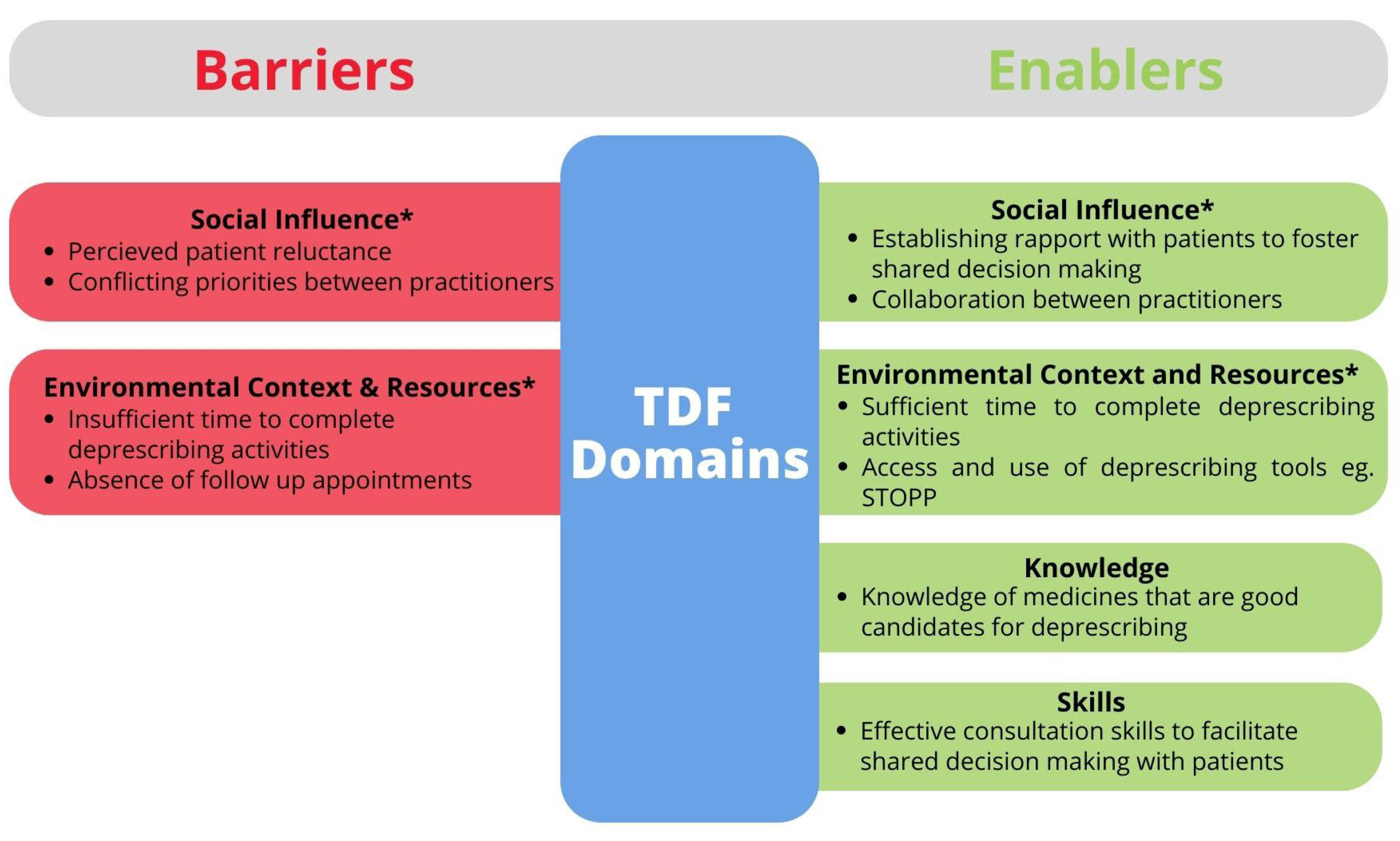
The coded barriers and enablers to deprescribing obtained from extended response data were mapped to 13 of the 14 TDF domains with only ‘Optimism’ being absent. Two enablers and four barriers were consistently reported across the data and are summarised in Figure 2. ‘Social influence’ and ‘Environmental context and resources’ appear both as barriers and enablers that require addressing. Conversely, ‘Knowledge’ and ‘Skills’ do not require addressing by interventions because respondents indicated that they already have the knowledge to identify any medicines that should be deprescribed and to safely deprescribe them. They also have the skills to navigate deprescribing consultations with patients to achieve a shared decision.
Respondents recognised that at the point of initiation, some medicines are presented to patients as ‘lifelong’. This practice contributed to the ‘Social influence’ barrier of a perception that patients were likely to be reluctant to have a medicine deprescribed that had been presented as lifelong when first prescribed.
“Patients may have been started and told they need to be on [the medicine] for life ... They may also worry that their condition will deteriorate, and this is more of a concern than potential side effects that may or may not occur.”Pharmacist
‘Social influence’ as a barrier also arose from peers with conflicting goals and priorities associated with prescribing for a given patient, particularly when this was reinforced by therapeutic area prescribing guidelines.
“Most challenging are colleagues of other specialties who in some instances are reluctant to stop some medications that are potentially harmful.”Doctor
‘Social influence’ from patients as an enabler was supported by establishing a good rapport through effective communication of deprescribing opportunities and involvement in decision making. Respondents described how the patient then became a partner, rather than someone who needed convincing that deprescribing was necessary. Similarly, adopting a collaborative approach to working with peers who may have conflicting goals was a proposed solution.
“Having a multidisciplinary team approach as well as patient engagement. Good communication between primary and secondary care is also important.”Pharmacist
The barrier related to ‘Environmental context and resources’ recognised that deprescribing is a resource intensive process, with respondents reflecting on the struggle to find sufficient time to undertake all 17 activities. Enablers proposed were dedicated time to deprescribe and strategies that make the process more efficient for example using the Screening Tool of Older Person’s Prescriptions (STOPP) criteria [31] to make the step of ‘Evaluating a patient for potential stop of a medicine’ more efficient.
“I need sufficient time, resources and ability to stop medicines successfully on a daily basis.”Pharmacist
Figure 1.
Key barriers and enablers to deprescribing within their Theoretical Domains Framework (TDF) domains. *Require addressing by interventions.
Figure 1.
Key barriers and enablers to deprescribing within their Theoretical Domains Framework (TDF) domains. *Require addressing by interventions.
This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
4. Discussion
The 17 activities that make up the four steps provide a specification validated by an international sample of healthcare professionals for the process of proactive deprescribing. Just over half of the activities were perceived to be regularly undertaken by respondents. Activities requiring direct partnership with the patient or caregiver represented all of those that were only sometimes undertaken. Proactive deprescribing interventions are required to facilitate increased delivery of these activities [15]. Interventions should comprise components that address the four barriers and two enablers to facilitate healthcare professionals to undertake these patient facing activities. Interventions should also motivate healthcare professionals to reflect on the extent to which they successfully involve patients and/or caregivers in the relevant activities.
The doctor, pharmacist and nurse study participants represented the mainstay of healthcare professional groups involved in deprescribing [3] and a range of healthcare systems spanning 25 countries. Their validation that all 17 activities are important provides content validity. Contrary to previous deprescribing processes [14], activities associated with both undertaking a medication history with evaluating whether a medicine should be stopped are combined into one step (Step 1). This was in recognition of stakeholders’ view that activities within these steps are often undertaken simultaneously in practice. This step is phrased ‘Identifying a patient for potential stop of a medicine’, reflecting the intention that the process guides service design and intervention development.
Every step of the proactive deprescribing process comprises one or more activities requiring direct partnership with the patient and/or caregiver. This aligns with the principles of shared decision making, which defines success as incorporating “what matters most” to the patient in all stages of healthcare processes [15]. It is therefore of concern that respondents thought that their peers only sometimes successfully involved patients/caregivers in the deprescribing process. In contrast, respondents felt that in the majority of cases, they had successfully deprescribed a medicine that they perceived inappropriate. Targeting interventions to support healthcare professionals to involve the patient and/or caregivers across the four deprescribing steps has the potential both to increase appropriate proactive deprescribing and enhance the patient and caregiver experience.
Several barriers to engaging with patients and caregivers provide an explanation for the vast majority of relevant activities only sometimes being undertaken in practice. Perceived patient reluctance to have a medicine deprescribed was prominent. A substantial body of literature using the revised Patient Attitudes Towards Deprescribing (rPATD) questionnaire consistently reports >90% of patients and caregivers are hypothetically willing to have a medicine deprescribed [32]. This suggests that the perceived patient reluctance expressed by respondents may be a misconception. Conversely, several large deprescribing trials report that the majority of patients in fact decline proactive deprescribing when it is proposed to them [33,34], aligning with our respondents’ perceptions. This disconnect between patients indicating high hypothetical willingness to have a medicine deprescribe in response to the rPATD and subsequently declining when it is proposed in practice may be explained by the patient orientated activities in the proactive deprescribing process developed in this study not being undertaken routinely, leading to an unsatisfactory patient experience and a subsequent unwillingness to have a medicine deprescribed.
The perception that patients are resistant to deprescribing stems from healthcare professionals failing to prime for the possibility of deprescribing [3]. For medicines prescribed by a specialist in particular, there is an ‘unspoken rule’ not intervene with their prescribing, leading to a heightened perception of patient resistance [3]. More generally, perceived resistance was explained by patients being told that medicines are “for life” when they are first prescribed. Even prescribers recognising this as problematic practice went onto self-report that they sometimes do not convey that deprescribing is a future possibility at the point of initiating a medicine. The rationale for this practice was not explored in this study, but it may be explained by the emphasis placed in influential treatment guidelines on medicines being for the ‘long-term’ [35], a recognised strategy to encourage medication adherence [36].
Lack of time is a well-recognised barrier to proactive deprescribing [3] and this study has identified that the activities that succumb are those requiring engagement with patients. These activities are the most time consuming and least flexible in terms of when they can be undertaken. Consultations are time-limited, particularly in primary care, and both patients and healthcare professionals report that they prioritise non-deprescribing activities such as history taking, diagnosis and prescribing [3,37]. Whilst other activities can be incorporated around healthcare professionals’ competing priorities, these activities can only be undertaken when the patient or a caregiver is available. Dedicated proactive deprescribing clinics are a potential solution [38]; an Australian pilot study demonstrated that a clinic for older people frequently admitted to hospital was feasible and acceptable [39]. A hospital stay or care home setting may present opportunities to undertake these activities given that patients and/or caregivers are more available than in other settings [7,37]. Conversely, although they may present other challenges such as patients being acutely unwell or lacking capacity to engage.
Consistent with the existing literature [3], this sample of healthcare professionals perceived themselves to have the required knowledge and skills to proactively deprescribe. Despite this, two-thirds reported making use of deprescribing tools, which are interventions widely used to address knowledge and skills gaps [40]. However, our findings suggest that healthcare professionals are using these tools for other purposes, potentially as a prompt and cue to deprescribe [40] or a heuristic to facilitate efficient deprescribing decisions [40,41]. Incorporation of prompts and cues into deprescribing interventions has been extensively studied. The SENATOR randomized controlled trial demonstrated that prompts and cues incorporated into electronic prescribing systems did not increase deprescribing behaviour [11,42]. Healthcare professional participants reported that prompts and cues were burdensome, disruptive and prone to alert fatigue [42]. There is significant evidence beyond the field of deprescribing asserting that tools serve as effective aids to heuristics [43,44]. There is a need for strategies to ensure that deprescribing tools are more likely to be serving as heuristics to facilitate ‘Memory attention and decision making’, which may be achieved by co-designing their implementation with the target audience [45,46,47].
After a medicine has been deprescribed, respondents report that they ‘often’ monitor patients for adverse withdrawal effects. Adherence to monitoring of clinical outcomes such as blood pressure or hospitalisation is unsurprising given that these are often requirements laid out in guidelines [35] and therefore subject to organisational auditing and benchmarking [48]. However, monitoring patients’ quality of life being only sometimes undertaken suggests that healthcare professionals are not considering patient-centred outcome measures. This may be because monitoring of these outcomes is not routine, and requires a paradigm shift towards a greater focus on quality of life and patient goals. Another explanation may be the dominance of ‘reactive’ deprescribing behaviour in current practice [2], given that clinical outcomes such as resolution of a gastric bleed upon deprescribing anticoagulants are intuitive to monitor for under these circumstances, whilst improving patient-centred outcome is not the primary aim of reactive deprescribing [49].
The international reach and representations from the primary healthcare professional groups involved in deprescribing is a strength of this study which affords confidence in the validity of the resulting deprescribing process and its constituent steps and activities. Given that recruitment was facilitated by professional networks and social media, it is impossible to establish the response rate for this study. However, it is likely that the 263 survey respondents represents a small proportion of the population who were invited to participate and thus introduces the risk of self-selection bias [50], particularly in favour of healthcare professionals who are already confident deprescribes. However, recognition that all but one patient orientated deprescribing activity are sub optimally delivered in practice affords some confidence that the findings provide an approximate reflection of real practice.
Healthcare professionals have affirmed that all 17 proposed deprescribing activities are essential and that whilst some of these are already routinely undertaken in practice, activities requiring engagement with patients are sub optimally delivered. To develop efficient interventions, developers should focus on including components targeting the eight activities requiring healthcare professionals to engage with patients. The four barriers and two enablers have been mapped to the TDF, which through its linkage to relevant behaviour change techniques [51] provides a range of theory-informed potential intervention components to support healthcare professionals to undertake the activities requiring engagement with patients. Resultant intervention will lead to a substantial change in the patient experience of deprescribing. Whilst increased engagement with patients in deprescribing is likely to be widely welcomed by patients [37], trials testing interventions should ensure that they capture the patient experience of deprescribing to inform refinement and evaluation.
Author Contributions
“Conceptualization, S.S. and D.B.; methodology, S.S. and D.B.; formal analysis, S.S., N.B. and D.B.; investigation, S.S., N.B. and D.B.; data curation, S.S., N.B. and D.B.; writing—original draft preparation, N.B.; writing—review and editing, S.S. and D.B.; visualization, S.S., N.B. and D.B.; supervision, S.S. and D.B.; project administration, N.B. All authors have read and agreed to the published version of the manuscript.”.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Faculty of Medicine and Health Sciences Research Ethics Committee, University of East Anglia, UK (protocol code 2020/21-020 27/10/2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Acknowledgments
We thank Paige Wright for supporting data collection. We thank participating healthcare professionals for their contribution to this study. We also thank the international networks who facilitated recruitment of healthcare professionals.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A
Online survey incorporating items inviting respondents to indicate on a 5-point Likert scale from ‘never’ to ‘always’, how often they thought each proactive deprescribing activity from the draft process was currently undertaken.
Appendix B
Data extracted from the 10 articles reporting deprescribing processes and the activities these underpinned.
References
- Scott IA, Hilmer SN, Reeve E, Potter K, Le Couteur D, Rigby D, et al. Reducing inappropriate polypharmacy: the process of deprescribing. JAMA Internal Medicine 2015;175:827–34.
- Scott S, Clark A, Farrow C, May H, Patel M, Twigg MJ, et al. Deprescribing admission medication at a UK teaching hospital; a report on quantity and nature of activity. International Journal of Clinical Pharmacy 2018;40:991–6. [CrossRef]
- Anderson K, Stowasser D, Freeman C, Scott I. Prescriber barriers and enablers to minimising potentially inappropriate medications in adults: a systematic review and thematic synthesis. BMJ Open 2014;4:e006544. [CrossRef]
- Scott S, Twigg MJ, Clark A, Farrow C, May H, Patel M, et al. Development of a hospital deprescribing implementation framework: a focus group study with geriatricians and pharmacists. Age and Ageing 2020;49:102–10. [CrossRef]
- General Medical Council. Good practice in prescribing and managing medicines and devices 2021.
- McDonald EG, Wu PE, Rashidi B, Wilson MG, Bortolussi-Courval É, Atique A, et al. The MedSafer study—electronic decision support for deprescribing in hospitalized older adults: a cluster randomized clinical trial. JAMA Internal Medicine 2022;182:265–73.
- Thillainadesan J, Gnjidic D, Green S, Hilmer SN. Impact of deprescribing interventions in older hospitalised patients on prescribing and clinical outcomes: a systematic review of randomised trials. Drugs & Aging 2018;35:303–19. [CrossRef]
- Thio SL, Nam J, van Driel ML, Dirven T, Blom JW. Effects of discontinuation of chronic medication in primary care: a systematic review of deprescribing trials. British Journal of General Practice 2018;68:e663–72. [CrossRef]
- Medication Without Harm 2017.
- Schuling J, Gebben H, Veehof LJG, Haaijer-Ruskamp FM. Deprescribing medication in very elderly patients with multimorbidity: the view of Dutch GPs. A qualitative study. BMC Family Practice 2012;13:1–7. [CrossRef]
- O’Mahony D, Gudmundsson A, Soiza RL, Petrovic M, Cruz-Jentoft AJ, Cherubini A, et al. Prevention of adverse drug reactions in hospitalized older patients with multi-morbidity and polypharmacy: the SENATOR* randomized controlled clinical trial. Age and Ageing 2020;49:605–14. [CrossRef]
- Scott S, Wright DJ, Bhattacharya D. The role of behavioural science in changing deprescribing practice. Br J Clin Pharmacol 2021;87:39–41. https://doi.org/10.1111/bcp.14595.
- Skivington K, Matthews L, Simpson SA, Craig P, Baird J, Blazeby JM, et al. A new framework for developing and evaluating complex interventions: update of Medical Research Council guidance. Bmj 2021;374.
- Reeve E, Shakib S, Hendrix I, Roberts MS, Wiese MD. Review of deprescribing processes and development of an evidence-based, patient-centred deprescribing process. British Journal of Clinical Pharmacology 2014;78:738–47.
- Elwyn G, Frosch D, Thomson R, Joseph-Williams N, Lloyd A, Kinnersley P, et al. Shared decision making: a model for clinical practice. Journal of General Internal Medicine 2012;27:1361–7. [CrossRef]
- Alexander GC, Sayla MA, Holmes HM, Sachs GA. Prioritizing and stopping prescription medicines. CMAJ 2006;174:1083–4. [CrossRef]
- Bain KT, Holmes HM, Beers MH, Maio V, Handler SM, Pauker SG. Discontinuing medications: a novel approach for revising the prescribing stage of the medication-use process. Journal of the American Geriatrics Society 2008;56:1946–52. [CrossRef]
- Brandt N, Stefanacci R. Discontinuation of unnecessary medications in older adults. The Consultant Pharmacist® 2011;26:845–54. [CrossRef]
- Gordon SF, Dainty C, Smith T. Why and when to withdraw drugs in the elderly and frail. Prescriber 2012;23:47–51. [CrossRef]
- Hardy JE, Hilmer SN. Deprescribing in the last year of life. Journal of Pharmacy Practice and Research 2011;41:146–51.
- Le Couteur D, Gnjidic D, McLachlan A. Deprescribing. Australian Prescriber 2011;34.
- Meeks TW, Culberson JW, Horton MS. Medications in long-term care: when less is more. Clinics in Geriatric Medicine 2011;27:171–91. [CrossRef]
- Ostini R, Hegney D, Jackson C, Tett SE. Knowing how to stop: ceasing prescribing when the medicine is no longer required. Journal of Managed Care Pharmacy 2012;18:68–72. [CrossRef]
- Scott IA, Gray LC, Martin JH, Mitchell CA. Minimizing inappropriate medications in older populations: a 10-step conceptual framework. The American Journal of Medicine 2012;125:529–37. [CrossRef]
- Woodward MC. Deprescribing: achieving better health outcomes for older people through reducing medications. Journal of Pharmacy Practice and Research 2003;33:323–8. [CrossRef]
- Gordon RA. Social desirability bias: A demonstration and technique for its reduction. Teaching of Psychology 1987;14:40–2. [CrossRef]
- Anthoine E, Moret L, Regnault A, Sébille V, Hardouin J-B. Sample size used to validate a scale: a review of publications on newly-developed patient reported outcomes measures. Health and Quality of Life Outcomes 2014;12:2. [CrossRef]
- Scott S, Clark A, Farrow C, May H, Patel M, Twigg MJ, et al. Attitudinal predictors of older peoples’ and caregivers’ desire to deprescribe in hospital. BMC Geriatrics 2019;19:1–11.
- Diamond IR, Grant RC, Feldman BM, Pencharz PB, Ling SC, Moore AM, et al. Defining consensus: a systematic review recommends methodologic criteria for reporting of Delphi studies. Journal of Clinical Epidemiology 2014;67:401–9. [CrossRef]
- Mayring P. Qualitative content analysis. A Companion to Qualitative Research 2004;1:159–76.
- O’Mahony D, O’Sullivan D, Byrne S, O’Connor MN, Ryan C, Gallagher P. STOPP/START criteria for potentially inappropriate prescribing in older people: version 2. Age and Ageing 2014;44:213–8. [CrossRef]
- Weir KR, Ailabouni NJ, Schneider CR, Hilmer SN, Reeve E. Consumer attitudes towards deprescribing: a systematic review and meta-analysis. The Journals of Gerontology: Series A 2021. [CrossRef]
- Weir K, Nickel B, Naganathan V, Bonner C, McCaffery K, Carter SM, et al. Decision-making preferences and deprescribing: perspectives of older adults and companions about their medicines. The Journals of Gerontology: Series B 2018;73:e98–107. [CrossRef]
- Martin P, Tamblyn R, Benedetti A, Ahmed S, Tannenbaum C. Effect of a pharmacist-led educational intervention on inappropriate medication prescriptions in older adults: the D-PRESCRIBE randomized clinical trial. Jama 2018;320:1889–98.
- Okeowo D, Patterson A, Boyd C, Reeve E, Gnjidic D, Todd A. Clinical practice guidelines for older people with multimorbidity and life-limiting illness: what are the implications for deprescribing? Therapeutic Advances in Drug Safety 2018;9:619–30.
- Kocurek B. Promoting medication adherence in older adults… and the rest of us. Diabetes Spectrum 2009;22:80–4. [CrossRef]
- Reeve E, To J, Hendrix I, Shakib S, Roberts MS, Wiese MD. Patient barriers to and enablers of deprescribing: a systematic review. Drugs & Aging 2013;30:793–807. [CrossRef]
- Bloomfield HE, Greer N, Linsky AM, Bolduc J, Naidl T, Vardeny O, et al. Deprescribing for community-dwelling older adults: a systematic review and meta-analysis. Journal of General Internal Medicine 2020;35:3323–32. [CrossRef]
- Mudge A, Radnedge K, Kasper K, Mullins R, Adsett J, Rofail S, et al. Effects of a pilot multidisciplinary clinic for frequent attending elderly patients on deprescribing. Australian Health Review 2015;40:86–91. [CrossRef]
- Michie S, Johnston M, Rothman AJ, de Bruin M, Kelly MP, Carey RN, et al. Developing an evidence-based online method of linking behaviour change techniques and theoretical mechanisms of action: a multiple methods study. Health Services and Delivery Research 2021;9:1–168. [CrossRef]
- Sherman SJ, Corty E. Cognitive heuristics. 1984.
- Dalton K, O’Mahony D, Cullinan S, Byrne S. Factors affecting prescriber implementation of computer-generated medication recommendations in the SENATOR trial: a qualitative study. Drugs & Aging 2020;37:703–13. [CrossRef]
- Dowding D, Merrill JA. The development of heuristics for evaluation of dashboard visualizations. Applied Clinical Informatics 2018;9:511–8. [CrossRef]
- Bekker HL. The loss of reason in patient decision aid research: do checklists damage the quality of informed choice interventions? Patient Education and Counseling 2010;78:357–64.
- Scott S, May H, Patel M, Wright DJ, Bhattacharya D. A practitioner behaviour change intervention for deprescribing in the hospital setting. Age and Ageing 2021;50:581–6. [CrossRef]
- Scott S, Atkins B, Kellar I, Taylor J, Keevil V, Alldred DP, et al. Co-design of a behaviour change intervention to equip geriatricians and pharmacists to proactively deprescribe medicines that are no longer needed or are risky to continue in hospital. Research in Social and Administrative Pharmacy 2023;19:707–16. [CrossRef]
- Grindell C, Coates E, Croot L, O’Cathain A. The use of co-production, co-design and co-creation to mobilise knowledge in the management of health conditions: a systematic review. BMC Health Services Research 2022;22:877. [CrossRef]
- Gillam SJ, Siriwardena AN, Steel N. Pay-for-performance in the United Kingdom: impact of the quality and outcomes framework—a systematic review. The Annals of Family Medicine 2012;10:461–8. [CrossRef]
- Linsky A, Zimmerman KM. Provider and system-level barriers to deprescribing: interconnected problems and solutions. Public Policy & Aging Report 2018;28:129–33. [CrossRef]
- Bradley N. Sampling for Internet Surveys. An Examination of Respondent Selection for Internet Research. Market Research Society Journal 1999;41:1–10. [CrossRef]
- Cane J, Richardson M, Johnston M, Ladha R, Michie S. From lists of behaviour change techniques (BCTs) to structured hierarchies: Comparison of two methods of developing a hierarchy of BCTs. British Journal of Health Psychology 2015;20:130–50. [CrossRef]
Figure 1.
Reported frequency of deprescribing activities within respondents’ peer group. Frequencies are reported as medians (quartiles). 1=never happens, 2=rarely happens, 3=sometimes happens, 4=often happens and 5=always happens. *Activity requires healthcare professionals to undertake in direct partnership with the patient or caregiver.
Figure 1.
Reported frequency of deprescribing activities within respondents’ peer group. Frequencies are reported as medians (quartiles). 1=never happens, 2=rarely happens, 3=sometimes happens, 4=often happens and 5=always happens. *Activity requires healthcare professionals to undertake in direct partnership with the patient or caregiver.
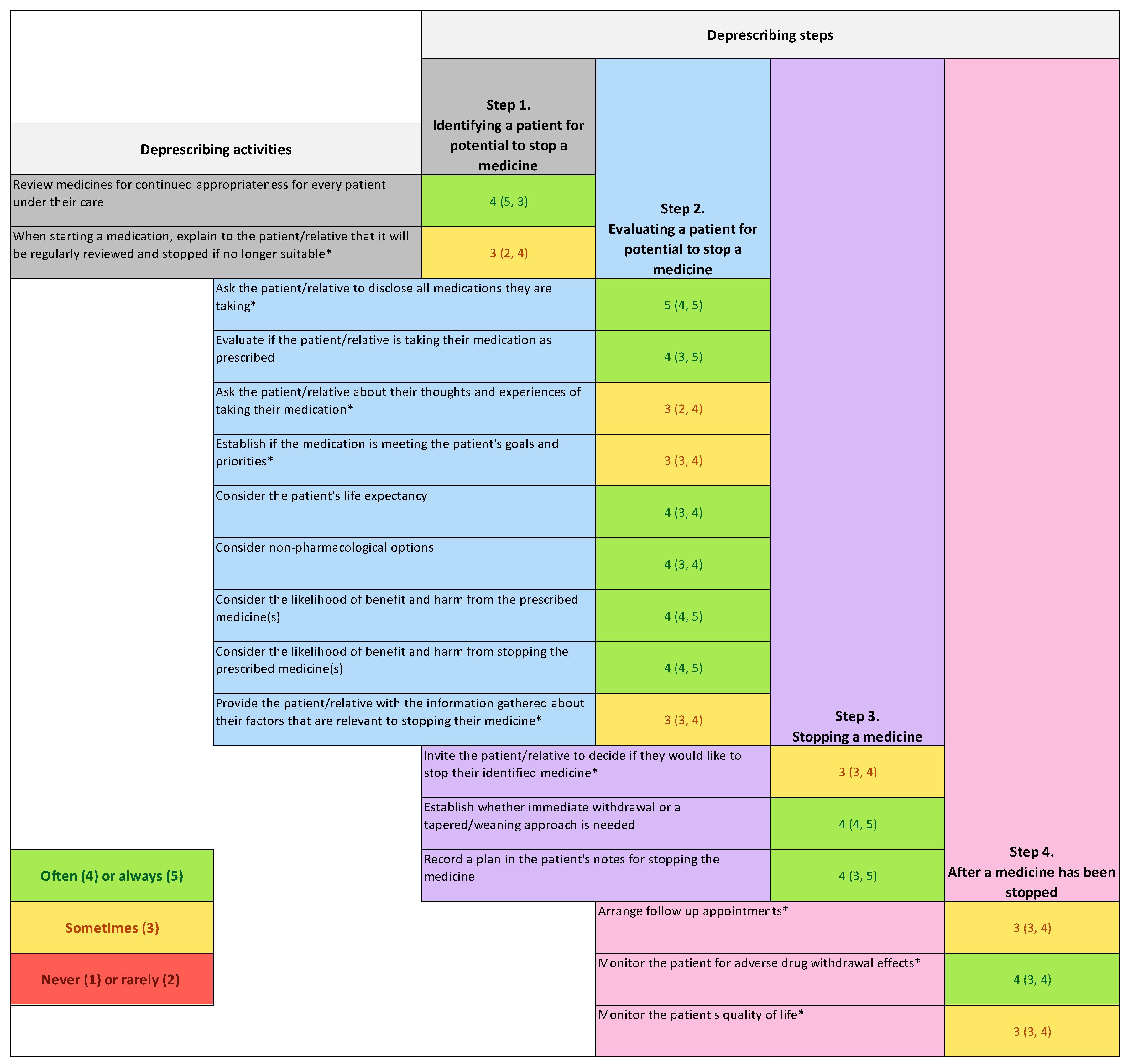

Table 1.
Draft process of proactive deprescribing steps and activities.
| Proactive deprescribing step | Activities |
| Step 1. Identify a patient for potential stop of a medicine | Review medicines for continued appropriateness for every patient under their care [17,19,22,25] When starting a medication, explain to the patient/relative that it will be reviewed regularly and stopped if no longer suitable* [21,23] |
| Step 2. Evaluate a patient for potential stop of a medicine | Ask the patient/relative to disclose all medications they are taking* [16,20,24,25] Evaluate if the patient/relative is taking their medication as prescribed [25] Ask the patient/relative about their thoughts and experiences of taking their medication* [25] Establish if the medication is meeting the patient’s goals and priorities* [20,24] Consider the patient’s life expectancy [20,24] Consider alternative non-pharmacological options [16] Consider the likelihood of benefit and harm from continuing to prescribe the medicine(s) [17,18,24] Consider the likelihood of benefit and harm from stopping the medicine(s) [17] Provide the patient/informal caregiver with the information gathered about their factors that are relevant to stopping their medicine* [25] |
| Step 3. Stop a medicine(s) | Invite the patient/informal caregiver to decide if they would like to stop their identified medicine* [22] Establish whether immediate withdrawal or a tapered or weaning approach is needed [23] Recording a plan for stopping the medicine in the patient’s notes or record [17,18] |
| Step 4. After a medicine has been stopped | Arrange follow up appointments* [20] Monitoring the patient for adverse drug withdrawal effects* [17] Monitoring the patient’s quality of life* [24] |
*Activity requires healthcare professionals to undertake in direct partnership with the patient/caregiver.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



