
Submitted:
26 July 2024
Posted:
29 July 2024
You are already at the latest version
Abstract
Age diversity in the workplace is a growing challenge. This study aimed to assess work ability among Family and Community Nurses (FCNs) in a large Local Health Authority (LHA) in Tuscany, Italy. The Work Ability Index (WAI) was administered to 178 FCNs, along with demographic and occupational data. Results showed a significant negative correlation between chronological age and WAI, indicating decreasing work ability with age. Moreover, work setting, educational attainment, and health conditions influenced work ability. Nurses working in home settings and those with higher educational levels reported better work ability. A high prevalence of health conditions, particularly musculoskeletal disorders, was observed. These findings highlight the need for targeted interventions to support FCNs' work ability and address age-related challenges. This study provides a foundation for developing strategies to optimize the nursing workforce and ensure high-quality care delivery.
Keywords:
work ability
; work ability index
; diversity management
; family and community nurses
1. Introduction
The workforce today is a diverse mosaic, reflecting variations in culture, gender, disability, immigration status, and more. This diversity is evident and must be acknowledged by management as a critical factor in organizational success. It mirrors the global market, immigration trends, and the increasing presence of women in the workforce [1]. Thus, effective management must prioritize diversity, creating an inclusive environment where every individual feels valued and empowered to contribute their best.
1.1. Diversity Management (DM)
Diversity management (DM) has been defined as “an approach to human resource management aimed at creating an inclusive work environment capable of fostering the expression of individual potential and using it as a strategic lever for achieving organizational objectives” [2]. This definition underscores the strategic importance of inclusivity in the workplace. Indeed, by focusing on inclusivity, DM can allow organizations to leverage the unique strengths and perspectives of each employee. Understanding who makes up a "community" of workers, the pathologies they are affected by, their level of education and competence, chronological and professional age [3], gender, and work ability at a given time, is important for identifying the best organizational strategy, how to best place and manage staff within the corporate context to derive the maximum benefit. Dimensions of diversity have been grouped into two main categories [4]: (i) primary diversity (age, gender, ethnicity, religion, etc.) which are inherent traits of an individual and cannot be changed, and (ii) secondary diversity (educational and professional background, experience and role within the organization, income, geographic location, etc.) which are acquired elements and thus can be modified over time. Additionally, there are organizational differences to consider, which are characteristics of a person linked to their position and hierarchical level within the work context [5]. At European Union level, the Action Plan 2023-2024 on the Diversity and inclusion in the workplace [6] has been released, underlying the importance of the subject and detailing all the managerial actions that must be addressed towards diversity, defining DM as "the active and conscious development of a far-sighted managerial process, oriented towards the acceptance of differences and the strategic and communicative use of certain differences and similarities as potential for the organization, a process that creates added value for the enterprise." In Italy, the development of DM policies is closely linked to changes in the labour market. Like other international contexts, the Italian landscape is increasingly characterized by a strong growth in workforce diversification [7]. The main trends through which the process of change manifests itself are at least three. The first concerns the increased presence of women in the labour market. The second is the increasingly widespread presence of immigrant workers in the work system. Italy is, in fact, a country that welcomes significant flows of foreign population, and this exponentially increases the proportion of non-Italian personnel in workplaces, mostly in the sectors of industry and services. The third aspect concerns the progressive increase in life expectancy which determines the coexistence of people of different ages within organizations, with aspirations and perspectives related to their own age. Alongside these profound changes in the composition of the workforce and in the occupational structure of the Italian context, another element that has made it possible to pay greater attention to the issue of DM is surely the reform regarding the mandatory placement of disabled persons, initiated through various legislative interventions from the late 1990s, which has contributed to promoting greater involvement of people with disabilities in the Italian labour market [8]. The term disability is defined by the World Health Organization as "any limitation or loss (resulting from an impairment) of ability to perform an activity in the manner or within the range considered normal for a human being. Disability reflects impairment at the level of the person and as such, encompasses disturbances at the level of the individual. Disability refers to functional capabilities manifested through acts and behaviours that by consensus constitute essential aspects of daily life" [9]. Recent ISTAT (Istituto Nazionale di Statistica) data show that there are 3,150,000 people with disabilities in Italy; among those aged 15-64 years, only 32% are employed (less than half a million people) [10]. Based on a 2020 survey conducted by IREF (Istituto di ricerche educative e formative), 40% of disabled resources of working age hold a university degree, but their level of employment often does not match their qualifications, resulting in an issue of overqualification. Another concerning statistic is the number of unemployed individuals: one-third of employed individuals with disabilities have stopped working [11]. In this social and economic challenge, multicultural competencies appear more necessary than ever for the success of diversity inclusion and acceptance policies. These competencies are identified [12] in three main categories: (i) multicultural mindset, which involves the ability to embrace diverse thinking and behaviour styles and includes aspects such as: new thinking, welcoming strangers, acceptance, tolerance towards change, confrontation, diversity, flexible judgment, ability to avoid stereotypes, (ii) multicultural communication competencies, involving the ability to conduct communication through perceptiveness (ensuring each interlocutor understands the conveyed meaning), listening orientation, transparency, and (iii) multicultural leadership capabilities, through: influence (adapting to the communication style of the interlocutor) and finding synergistic solutions. An empirical analysis on diversity management conducted in 2015 [13] showed that DM is associated with higher levels of inclusion, which in turn increases engagement and dedication among both non-native and native employees within public sector organizations. As a matter of fact, through appropriate valorisation of differences, "not only can profit margins increase through innovation and efficiency savings, but individuals employed in work organizations, both private and public, will also benefit, resulting in increased job satisfaction levels and employee loyalty" [14].
1.2. Age Diversity and the Work Ability Concept
Life extension allows an increasing number of older workers to remain in the workforce, often becoming subject to discrimination from younger colleagues or management who perceive them as less productive, less dynamic, or less suited to modern technologies [15]. However, it is important to emphasize that age is not necessarily synonymous with a decline in work capacity; rather, it represents added value in terms of experience, maturity, and emotional stability [16]. The concept of Age Diversity (AD) aims to valorise these characteristics by promoting an inclusive work environment that fosters interaction and collaboration across different generations. The concept of Work Ability (WA), proposed by the Finnish Association of Occupational Health [17], is the result of a balance between supply and demand of resources between the individual and the organization." Firms tend to consider older workers as less "convenient" as a result of seniority-related wages, unreadiness for change and innovation, higher complexity in training, health problems, and less availability for required mobility [18]. Another important concept is that of "organizational age": it not only refers to the duration of the relationship between the worker and the organization but also to occupational age (i.e., the career stage in which the individual find themselves). There are various interventions that management can undertake to protect against age discrimination; crucially, mapping the company’s workforce and identifying existing competencies for optimal utilization are essential, and this work addresses this specific need. It is essential to quantify people’s work ability at any given time to understand how best to manage it. The tool we used is the Work Ability Index (WAI) [19], that can provide insights into both the individual’s WA and their health status.
1.3. The Work Ability Index (WAI)
The issue of age management has been the subject of study since the 1980s in Scandinavian countries, which were among the first to recognize its dimensions. Finland played a pioneering role in this regard, with Ilmarinen’s groundbreaking studies questioning how job content and demands influence individuals’ perception of their ability to perform their work and, crucially, how this perception varies over time based on these variables. According to Ilmarinen, WA is based on the balance between individual resources and job demands [20]. The starting point was the demographic challenge as it presented itself in Finland in the early 1980s. Due to the baby boomer generations born between 1943 and 1960, predictions of a high proportion of older workers in the labour force were not difficult to make. To explore this issue, Ilmarinen created and validated the construct of WA, conceptually defined as "the measure of a worker’s ability to perform their work now and in the foreseeable future, in relation to the demands of their job and their mental and physical resources" [21]. WA is influenced by individual health conditions, functional capacities [22,23], knowledge, professional competence, satisfactory environmental and relational working conditions, attitudes, and motivations [24]. This concept is dynamic and changes throughout everyone’s working life, with age being one of the primary factors influencing this perception [25]. To quantify this construct, the WAI has been developed, structured into seven dimensions. This index assesses work ability in relation to job demands, diagnosed illnesses, and absences taken [26]. It is calculated based on responses to a series of questions that consider both the physical and mental demands of the job, as well as the worker’s health status and resources. How the worker evaluates their own work capacity is crucial as it significantly affects their approach to the workplace. A longitudinal study on aging municipal workers in Helsinki [27], the WAI was able to predict the incidence of work disability among 50-year-old workers. Alan Walker, one of Europe’s leading experts in AM, defines good practices as interventions aimed at "combatting age barriers, directly or indirectly, promoting age diversity, and providing a work environment where every individual can develop their potential without being disadvantaged because of their age. In one of his works [28] , Walker highlights the importance of AM strategies to promote initiatives supporting the retention and reintegration of older workers, as employers can no longer rely on a sufficient presence of young workers and must increasingly address the ageing of their existing human resources [29]. Walker also distinguishes between reactive and preventive interventions. Reactive interventions address cases where ageing of the workforce has already become problematic for the organization in terms of skills and costs. On the other hand, preventive interventions systematically embrace the entire organizational culture to prevent the issue from arising in the first place. It is for this reason that this work has been undertaken, to implement proactive interventions. By focusing on proactive strategies, the aim is to foster an organizational culture that not only supports the continuous development of all employees but also mitigates potential issues before they become problematic. This approach is intended to ensure a more inclusive, skilled, and adaptable workforce, ultimately benefiting both the employees and the organization.
2. Materials and Methods
The WAI was used to assess the work ability of Family and Community Nurses (FNCs) in the largest Local Health Authority (LHA) of Tuscany, to evaluate an individual’s capacity to perform their work tasks, considering the demands of their job, their health status, and their mental resources. Among all nurses, FNCs were selected because they play a crucial role in providing comprehensive, continuous, and coordinated care to individuals and families within the community. Their work is integral to promoting health, preventing illness, and managing chronic conditions in a way that is culturally sensitive and tailored to the specific needs of the community. The COVID-19 pandemic has further highlighted the necessity of reducing hospital admissions to alleviate the burden on healthcare systems. FNCs are essential in this context as they can effectively manage and monitor patients in the community, reducing the need for hospital visits. The primary endpoint consists in evaluating the degree of work ability among FCNs within the territorial nursing care of the LHA. The secondary endpoint consists in identifying any changes in work ability in relation to chronological age, gender, nationality, professional age, work setting, type of professional training, job demands, and existing pathologies. We aim to conduct this assessment on a regular basis over time and eventually expand it to include all nurses working within the LHA. This intervention aims to assess the work ability of the nurses by capturing their self-reported perceptions regarding their current work ability compared to the best period of their life, the demands of their job, diagnosed illnesses, impairment due to illnesses, absenteeism due to illness, their own prognosis of work ability for the next two years, and their mental resources. The survey will provide insights into how these demographic and occupational variables influence the nurses’ work ability and will help identify factors that may impact their ability to balance personal and professional life effectively.
The WAI consists of the following items:
- Current work ability compared to the best time of life (0-10 points);
- Work ability in relation to job demands (2-10 points);
- Number of current diagnosed diseases (1-7 points);
- Reduction in work ability due to diseases estimated by the individual (1-6 points);
- Absences due to illness in the last 12 months (1-5 points);
- Perception of own work ability in the next two years (1, 4, 7 points);
- Mental resources (1-4 points).
The index can range from 7 to 49. Based on it, different levels of work ability and goals to pursue are defined according to the following table:

Table 1.
Range of WAI.
| Score | Work Ability | Aim |
|---|---|---|
| 7-27 | Poor | Restore work capacity |
| 28-36 | Mediocre | Improve work capacity |
| 37-43 | Good | Support work capacity |
| 44-49 | Excellent | Maintain work capacity |
Alongside the questionnaire, additional questions were included in the census sample regarding variables such as gender, age, nationality, professional age, specific workplace location within the LHA, work setting (outpatient services, community work setting, or both), professional training (regional school -nursing schools before the transition to University system-, three-year bachelor’s degree, master’s degree in nursing, first and second level master’s degree, Ph.D.). The questionnaire was electronically administered in accordance with the GDPR (General Data Protection Regulation) 2016/679, the main European legislation on the protection of personal data. FNCs were informed that participation was voluntary, and that non-participation or withdrawal would not result in prejudice or harm to them. Within the database, data were collected anonymously. The total sample consisted of 178 full-time FCNs, and their answers were analysed using descriptive and inferential statistical tools, which allowed us not only to obtain a detailed picture of the characteristics of the FCNs personnel, but also to correlate the WAI with different variables of interest. Data analysis was performed using IBM SPSS Statistics for Windows, Version 29.0. and WAI associations with gender, chronological and professional age, work setting, and educational attainment were explored.
3. Results
Out of 481 FCNs working in the LHA, the 37% responded, determining a sample of 178 FCNs. In Table 2, the overall chronological age is represented: the sample’s age ranges from 25 to 63 years, with a mean age of 46.7 and a SD of 10,42.
Detailed percentages for each age group within the study sample are provided based on age ranges and gender composition are provided in Table 3:
The sample consists of 82.02% women and 17.98% men. Compared to the total, only 4 people are not of Italian nationality. As depicted in Table 4, the 62.36% of nurses have been working for more than 20 years, 17.42% for 11-20 years, and 20.22% for less than 11 years.
Next table (Table 5) provides details on sample’s professional training and work setting: the 38.20% of the sample attended the regional school, 15.17% hold a bachelor’s degree, and 24.16% hold a bachelor’s degree in nursing. Among these, 6 nurses have a master’s degree, 18.45% have a master’s degree, the rest in obtained a Ph.D.
Most of the sample (54,49%) works in home setting, the 11,24% works entirely in the outpatient setting, while 34.27% carry out their work in both outpatient and home settings.
"Poor" WA (1.69%), "mediocre" (24.16%), "good" (51.12%), and "excellent" WA (23.03%) are the overall results, which are also differentiated by gender. Overall, 74.15% of the sample falls within perceived WA scores of good or excellent level, while 25.85% fall within a mediocre or poor level. Women exhibit better perceived WA compared to men; in fact, 76.03% of women fall within scores of good or excellent level, whereas men in the same category constitute 65.63%. Conversely, 23.97% of women have a mediocre or poor level of perceived WA, compared to 34.38% of men.
Analysis of the individual items that constitute the WAI, as reported in Table 7, overall and divided per gender. The mean and SD of the score for each item were calculated according to variations in chronological age and professional age. Additionally, the mean and SD of the score for each item were calculated according to variations in chronological age and divided by gender. The same was done for professional age. These results were included solely as measures reported in the comments related to the analysis of each individual item.
The type of commitment required for the job: the 2,25% of the sample declared that the commitment required is predominantly physical, the 14,61% declared it as predominantly mental, and the 83,15% declared that the nature of the commitment required is both physical and mental.
The average scores of the various items do not differ significantly between women and men.
1. Current work capacity compared to the best period of your life. Maximum work capacity has a value of 10. Respondents are called to give a score on their current work capacity. The overall mean is 7,67 and women self-assessed a 7,71 compared to 7,5 men’s mean value. This item shows a peak in the chronological age range of 36-45, and then decreases again. Regarding professional age, decreases are observed in the ranges of 6-10 and more than 20 years. There are no substantial differences between the two genders for both categories (chronological age and professional age).
2. Work capacity in relation to job demands: respondents were asked to estimate from very good and very poor (on a 5 points Likert scale). This item shows a progressive decrease of work capacities in relation to job demands with professional age, and this decrease is also observed with chronological age, particularly from the age of 46. An opposite trend is observed between the two genders for both categories (chronological age and professional age).
3. Number of current illnesses diagnosed by a physician. The broad categories to which respondents have responded include outcomes of injuries following accidents, musculoskeletal disorders, cardiovascular diseases, respiratory diseases, mental disorders, digestive diseases, genitourinary diseases, skin diseases, tumours, endocrine and metabolic diseases, blood disorders, birth defects. A more substantial difference exists regarding the number of currently diagnosed diseases, with women having a mean of 5.32 and men having a mean of 4.25. The peak occurs in the chronological age range of 36-45 years, followed by a progressive decrease. The trend also declines regarding professional age, after 20 years of work. As additional information, here are the percentage values related to health conditions: 38.76% of the entire sample states not to have any pathology, 36.86% have a medical diagnosis for pathologies, and 24.38% report having pathologies but without a medical diagnosis. Considering the group of subjects with medical diagnoses, the most reported pathologies are musculoskeletal disorders (21.12%), followed by cardiovascular diseases (8.76%), endocrine or metabolic diseases (7.97%), genitourinary diseases (7.57%), mental disorders (7.17%), and gastrointestinal diseases (6.77%), as reported in Figure 1.
4. Estimate of reduced work capacity due to illness. Respondents were asked how much their current work was hindered by their health conditions. Both chronological and professional trends decrease over time, for both genders.
5. Absences due to illness in the last year. Respondents were required to indicate how many full days of work have they been absent from work due to health issues (illness, treatments, visits, diagnostic exams) choosing from: none, less than 10 days, 10 to 24 days, 25 to 99 days, 100 to 365 days. This item peaks in the chronological age range of 36-45 and then decreases again, while regarding professional age, the curve notably declines in the 11-20 range. The trend is opposite for the two genders: women decrease over time, while men increase.
6. Assessment of work capacity over the next 2 years. Considering their current health conditions, respondents were required to indicate if they felt unlikely, or not sure, or fairly sure to perform their current job in the next 2 years. The peak of “fairly sure” forecast shows two peaks in the chronological age ranges of 36-46 and in professional age within the 11-20 interval, followed by a decrease in both cases. No substantial differences are highlighted between the two genders.
7. Personal resources. Respondents were asked to self-assess their ability to perform your usual daily activities satisfactorily recently (often, quite often, sometimes, rather rarely, never). There is a decrease with advancing chronological age and a progressive decline with increasing professional age. The curves in both genders are very similar in both categories.
After describing the data statistically in their general form, the interrelation between the WAI and chronological age was analysed. Using the Pearson correlation coefficient (ρ), a negative correlation (p < 0.05) between the WAI and participants’ age is highlighted, as reported in Table 8.
This indicates that as the variable of chronological age increases, lower scores are observed in relation to work ability, thus indicating a perceived lower work capacity by the individual. This means that younger nurses exhibit a higher work ability index compared to older nurses. A linear regression analysis relating the dependent variable WAI (y) to the explanatory variable chronological age (x) was performed. As depicted in Figure 2, shows a result which is consistent with the Pearson analysis, consisting of a line with a coefficient β of -0.22 and a constant B of 44.49.
In addition, another factor we have focused on is professional age, calculating both WAI’s mean and SD for each range of years of professional experience, as shown in Table 9:
The mean WAI index decreases with increasing professional age of the subjects involved. As shown in Table 10, 56.70% of those who work solely in home settings report having good work ability, while 21.65% consider it mediocre. There doesn’t appear to be a significant difference in the percentages of "good" and "mediocre" work ability among those who work in ambulatory settings.
WAI’s mean and SD were calculated for the different settings, and the WAI indicates (in descending order) an average work ability index of 39.89 with a SD of 4.42 for home setting, 39.42 with a SD of 5.46 for both settings combined, and 37.45 with a SD of 6.54 for outpatient settings.
Regarding the educational attainment (Table 11), a mediocre work ability is mostly indicated by those who attended the regional school, obtained a bachelor’s degree, or attended post-basic studies; however, most of these individuals still fall into the "good" category. For the majority of those who obtained a bachelor’s degree, a good to excellent work ability is reported, as shown in Table 11.
From the table below (Table 12), it can be observed that the WAI results indicate an average work ability index of 40.16 with a SD of 4.70 for individuals who report having no diagnosed pathologies, and 35.17 with a SD of 5.31 for those with diagnosed pathologies.
Additionally, the mean and SD scores were calculated for each item based on educational attainment. FNCs who attended regional school or obtained a bachelor’s degree show significantly lower current work ability compared to those with different educational backgrounds (such as a bachelor’s degree or post-basic training).
4. Discussion
These findings are not generalizable and provide a snapshot of the surveyed population. Following this logic, they become invaluable for local management, enabling them to design tailored improvement actions and policies that precisely address the needs of this specific group of individuals. This targeted approach allows for more effective and relevant interventions, enhancing the overall well-being and productivity of the workforce within the local context. A truly concerning finding is the one related to health conditions: a significant 61.24% of participants report having one or more than one, with a majority having received a medical diagnosis. Musculoskeletal disorders are the most reported conditions, particularly among female nurses, accounting for 21.12% of the reported diagnoses. Age-related differences in health conditions are also evident. Higher prevalence rates of health conditions are observed in the age groups 46-55 and 56-63. Correspondingly, the WAI results indicate a mediocre average work ability index for nurses with diagnosed conditions compared to those without any reported health issues. These findings emphasize the importance of addressing age-specific health challenges in the nursing workforce. Professional experience further influences health outcomes. The average score for the questionnaire item regarding the current number of diagnosed illnesses significantly decreases for nurses with over 20 years of experience compared to other professional age groups. This suggests that long-term professional experience may be associated with better health management or reporting. A notable influence of the work setting on mental health conditions such as depression and burnout was observed. Nurses working in outpatient settings exhibit nearly double the percentage of mental health issues compared to those working exclusively in home settings. This raises important questions about whether these mental health conditions are influenced by the outpatient work environment itself or if nurses with pre-existing conditions are more likely to choose outpatient work. Further research is warranted to explore this relationship. This highlights the need for targeted interventions to improve work conditions in outpatient settings. Interestingly, there are no significant gender differences in WA. However, educational attainment does seem to play a role, with individuals who attended Regional School, obtained a bachelor’s degree, or pursued post-basic studies reporting mediocre work ability. This suggests that educational background may influence perceptions of work ability and highlights the need for educational support and ongoing professional development. In addressing these findings, job crafting emerges as a crucial strategy. By aligning the worker’s capabilities and preferences with their role, job crafting encourages proactive behaviours that enhance job satisfaction and coherence with individual skills and preferences [30]. This approach allows organizations to effectively position each employee within the organizational context, maximizing their potential benefits and supporting overall occupational health and well-being.
5. Conclusion
If properly managed, diversity can empower individuals, allowing each to express their potential and have a positive impact on organizational outcomes [31]. Highlighting issues of aging or AD and measuring them, disability diversity, gender, and cultural diversity in a complex work context composed of workers differing in age, gender, education level, health status, and work ability, as well as the work setting and job demands, provides a snapshot of the organization. As Ilmarinen and colleagues underline [12,20], the management’s objective should be to promote WA during the aging of their personnel, aiming for improved work quality and production, high quality of life and well-being for the personnel, and a meaningful and active transition from work for both the individual and the organization [32]. Relying on their experience, in addition to making the WAI a managerial tool to be regularly used, we should also capitalize on factors that they recognize to have the greatest impact on WA levels, namely the characteristic of job demands and environmental factors, followed by organizational characteristics and the work community, professional skills, and lifestyle. These are some of the organizational and managerial recommendations we can draw from their studies and the evidence they have produced: (i) the strongest predictor of high WA levels is the use of knowledge as a tool for work, along with improvements in working conditions and job tasks. Conversely, factors such as uncomfortable postures, a stressful work environment, a cold work climate, and outdated tools are strongly associated with low levels of the WAI, (ii) valuing experience in terms of independence is the most significant promoter of WA, (iii) continuous training and the opportunity for career development and influencing work methods are positively correlated with high levels of the WAI, (iv) engaging in physical exercise during leisure time shows positive correlations with high levels of WA, (v) supportive work environments are of paramount importance for professional development. A widespread adoption of good practices in age management will assist organizations in adapting to the inevitable ageing of their workforce, enhancing competitiveness and productivity among an ageing active population, improving employment opportunities for mature workers, extending working lives, and promoting equal opportunities among workers of different age groups. This study has the limit of being monocentric, and it has the limitation of being aimed only at a portion of the staff. To overcome the limitations of the study, it would be desirable to replicate the same protocol in other healthcare facilities and/or in different regions to evaluate whether various organizational conditions within companies influence WA.
Author Contributions
Conceptualization, C.D.M. and C.B.; methodology, C.D.M. and C.B.; software, C.D.M.; validation, C.B., M.A., D.A. and P.Z.; formal analysis, C.D.M.; investigation, C.D.M.; data curation, C.B. and C.D.M.; writing—original draft preparation, C.B.; writing—review and editing, C.B.; supervision, C.B., M.A., D.A., P.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and European GDPR 2016/679.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to due to the corporate ownership, writer, of the data. They may however be requested from the corresponding author upon reasonable request.
Guidelines and Standards Statement
This organizational study adheres to the Standards for Reporting Qualitative Research (SRQR) guidelines to ensure the quality and transparency of the reported study.
Public Involvement Statement
No public involvement in any aspect of this research.
Use of Artificial Intelligence
AI or AI-assisted tools were not used in drafting any aspect of this manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- M. Y. Byrd and C. L. Scott, “Diversity in the workforce: Current issues and emerging trends,” 2024.
- M. C. Barabino, B. Jacobs, and M. A. Maggio, “Il diversity management,” Svilupp. Organ., vol. 184, pp. 19–31, 2001.
- J. Lyons, “Chronological age, professional age, and eminence in psychology.,” Am. Psychol., vol. 23, no. 5, p. 371, 1968. [CrossRef]
- S. M. Byrd, “Workforce America!: Managing Employee Diversity as a Vital,” People Strateg., vol. 15, no. 3, p. 98, 1992.
- S. E. Jackson and M. N. Ruderman, “Diversity in Work Teams, Washington,” DC Am. Psychol. Assoc., 1996.
- European Commission, “Action Plan 2023-2024 - Fact Sheet on the Diversity and inclusion in the workplace,” 2023.
- ISTAT, “Rapporto annuale 2024 sul mercato del lavoro e retribuzioni,” 2024.
- F. Malzani, “Dal collocamento mirato al diversity management. Il lavoro dei disabili tra obbligo e inclusione nella prospettiva di genere,” Riv. del Dirit. della Sicur. Soc., vol. 19, no. 4, pp. 717–740, 2019. [CrossRef]
- W. H. Organization, “Disability, including prevention, management and rehabilitation,” Geneva, Switz. Author, 2005.
- ISTAT, “Disabilità in cifre,” 2024.
- L. Proietti and G. Zucca, “La qualità del lavoro per le persone con disabilità,” Ist. di Ric. Educ. e Form. IREF, 2020.
- D. Trickey, “Diversity management competencies and the development challenge: special competencies, skills and attitudes needed to ‘manage through cultures,’” Divers. Manag. e Soc. Multicult., vol. 35, no. 2, pp. 220–232, 2004.
- T. Ashikali and S. Groeneveld, “Diversity management for all? An empirical analysis of diversity management outcomes across groups,” Pers. Rev., vol. 44, no. 5, pp. 757–780, 2015. [CrossRef]
- K. Monks, “The business impact of equality and diversity: The international evidence,” -4266, 2007.
- T. Rabl, “Age, discrimination, and achievement motives: A study of German employees,” Pers. Rev., vol. 39, no. 4, pp. 448–467, 2010. [CrossRef]
- L. L. Carstensen et al., “Emotional experience improves with age: evidence based on over 10 years of experience sampling.,” Psychol. Aging, vol. 26, no. 1, p. 21, 2011. [CrossRef]
- L. Kokkinen and A. Konu, “Work ability of employees in changing social services and health care organizations in Finland,” Int. J. Occup. Med. Environ. Health, vol. 25, pp. 151–165, 2012. [CrossRef]
- G. Costa and M. Gianecchini, Risorse umane. Persone, relazioni e valore. McGraw-Hill, 2019.
- K. Tuomi, J. Ilmarinen, A. Jahkola, L. Katajarinne, and A. Tulkki, “Work Ability Index (WAI),” Helsinki Finnish Inst. Occup. Heal., 1998.
- J. Ilmarinen, Ageing workers in the European Union: status and promotion of work ability, employability and employment. Finnish Institute of Occupational Health, 1999.
- J. Ilmarinen, “Work ability—a comprehensive concept for occupational health research and prevention,” Scand. J. Work. Environ. Health, vol. 35, no. 1, pp. 1–5, 2009. [CrossRef]
- G. Pezzagno and G. Brunetti, “Work capacity, residual capacity and work tolerance times. A proposed measuring method,” G. Ital. Med. Lav., vol. 13, no. 1–6, pp. 35–50, 1991.
- P. Capodaglio, E. M. Capodaglio, G. Bazzini, M. Imbriani, and G. Ferrari, “Physical workload demands: the combined use of 2 evaluation programs,” G. Ital. Med. Lav., vol. 15, no. 5–6, pp. 117–126, 1993.
- J. E. Ilmarinen, “Aging workers,” Occup. Environ. Med., vol. 58, no. 8, p. 546, 2001. [CrossRef]
- D. Camerino et al., “Low-perceived work ability, ageing and intention to leave nursing: a comparison among 10 European countries,” J. Adv. Nurs., vol. 56, no. 5, pp. 542–552, 2006. [CrossRef]
- J. Ilmarinen, “The work ability index (WAI),” Occup. Med. (Chic. Ill)., vol. 57, no. 2, p. 160, 2007. [CrossRef]
- K. Tuomi, J. Ilmarinen, R. Martikainen, L. Aalto, and M. Klockars, “Aging, work, life-style and work ability among Finnish municipal workers in 1981—1992,” Scand. J. Work. Environ. Health, pp. 58–65, 1997.
- Walker, “Managing an ageing workforce: A guide to good practice,” 2012.
- G. Naegele and A. Walker, “A guide to good practice in age management,” 2006.
- G. R. Slemp and D. A. Vella-Brodrick, “Optimising employee mental health: The relationship between intrinsic need satisfaction, job crafting, and employee well-being,” J. Happiness Stud., vol. 15, pp. 957–977, 2014. [CrossRef]
- R. R. Thomas Jr, “From affirmative action to affirming diversity.,” Harv. Bus. Rev., vol. 68, no. 2, pp. 107–117, 1990.
- K. Tuomi, P. Huuhtanen, E. Nykyri, and J. Ilmarinen, “Promotion of work ability, the quality of work and retirement,” Occup. Med. (Chic. Ill)., vol. 51, no. 5, pp. 318–324, 2001. [CrossRef]
Figure 1.
Number of diagnosed pathologies by chronological age range.
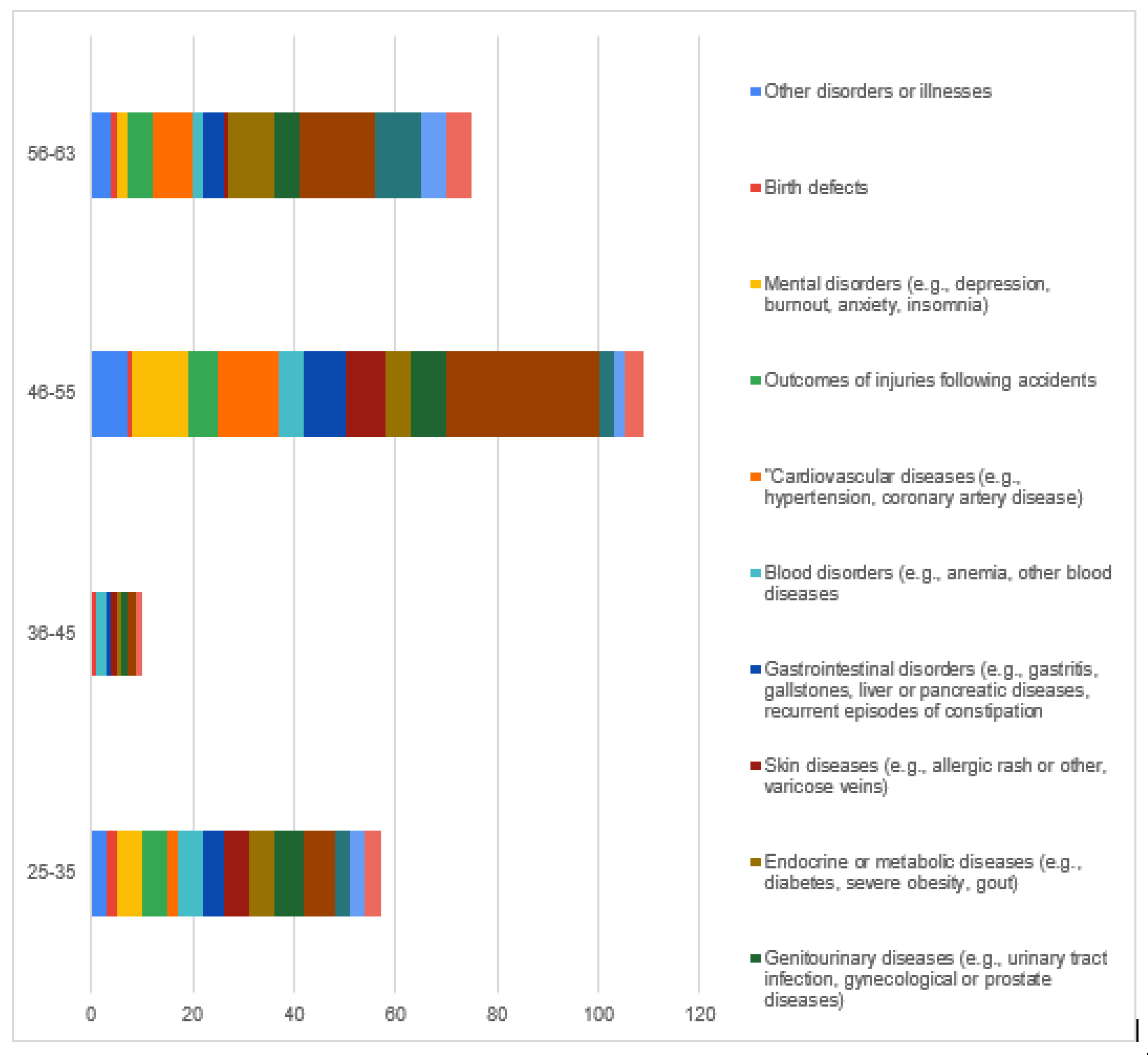
Figure 2.
Linear regression WAI/Chronological age.
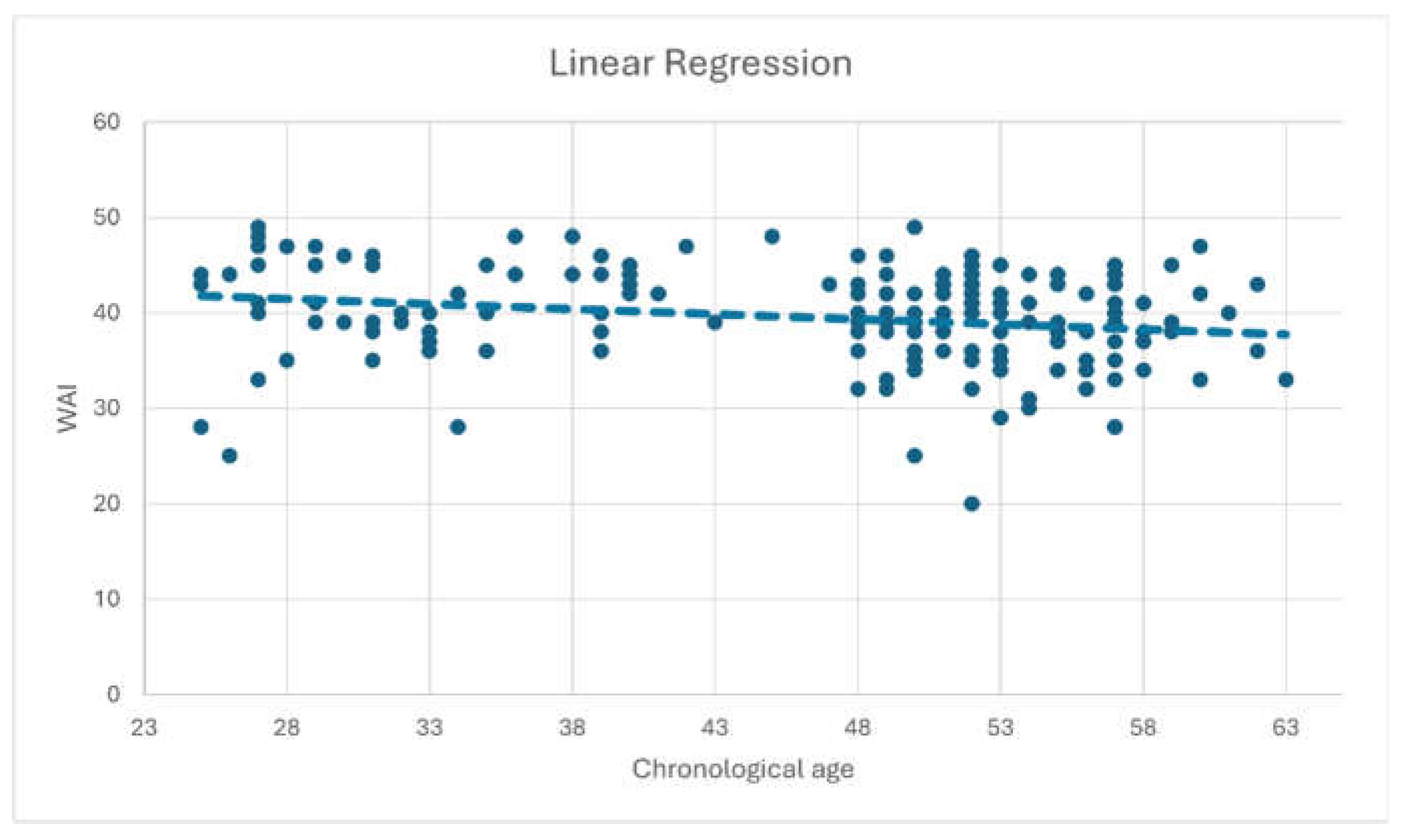
Table 2.
Overall descriptive analysis of the sample.
| Chronological Age, Overall | |
|---|---|
| Min | 25 |
| Max | 63 |
| Mean | 46,7 |
| SD | 10,42 |
Table 3.
Percentages divided by age groups.
| Chronological Age Groups and Gender | ||
|---|---|---|
| Women | Men | |
| 25-35 yrs. | 20,55% | 28,13% |
| 36-45 yrs. | 8,22% | 18,75% |
| 46-55 yrs. | 53,42% | 28,13% |
| 56-63 yrs. | 17,81% | 25,00% |
| Women | Men | |
| Gender | 82,02% | 17,08% |
Table 4.
Details on nationality and professional age.
| Nationality | |
| Italian | 97,75% |
| EU | 1,69% |
| Extra EU | 0,56% |
| Professional age | |
| 1-5 yrs. | 10,67% |
| 6-10 yrs. | 9,55% |
| 11-20 yrs. | 17,42% |
| >20 yrs. | 62,36% |
Table 5.
Details on professional training and work setting.
| Professional training | |
| Regional school | 38,20% |
| Bachelor’s Degree | 15,17% |
| Bachelor’s degree in nursing | 24,16% |
| Master’s Degree, I or II level | 18,45% |
| Ph.D. | 4,02% |
| Work setting | |
| Outpatient | 11,24% |
| Home setting | 54,49% |
| Both | 34,27% |
Table 6.
WAI results of the investigated sample.
| WAI Sample’s Results | ||||
|---|---|---|---|---|
| WAI Score | Work Ability | Overall N% | Women | Men |
| 7-27 | poor | 1,69% | 1,37% | 3,13% |
| 28-36 | mediocre | 24,16% | 22,60% | 31,25% |
| 37-43 | good | 51,12% | 52,74% | 43,75% |
| 44-49 | excellent | 23,03% | 23,29% | 21,88% |
| Mean WAI | 39,46 | |||
| SD | 5,13 | |||
Table 7.
WAI results divided by item, overall and gender.
| WAI Items | ||||||
|---|---|---|---|---|---|---|
| Women | Men | |||||
| Items | Mean Overall | SD Overall | Mean | SD | Mean | SD |
| Current work ability compared to the best time of life | 7,67 | 1,48 | 7,71 | 1,42 | 7,5 | 1,75 |
| Work ability in relation to job demands | 7,91 | 1,24 | 7,88 | 1,26 | 8,03 | 1,17 |
| Number of current diagnosed diseases | 5,12 | 1,79 | 5,32 | 1,71 | 4,25 | 1,90 |
| Reduction in work ability due to diseases estimated by the individual | 5,12 | 0,98 | 5,14 | 1,01 | 5,06 | 0,84 |
| Absences due to illness in the last 12 months | 4,07 | 0,93 | 4,06 | 0,94 | 4,15 | 0,88 |
| Perception of own work ability in the next two years | 6,30 | 1,41 | 6,30 | 1,41 | 6,34 | 1,47 |
| Mental resources | 3,20 | 0,64 | 3,20 | 0,63 | 3,18 | 0,69 |
Table 8.
Covariance and Pearson correlation coefficient calculated on the sample.
| Mean WAI | 39,46 |
| DS WAI | 5,13 |
| Mean chronological age | 46,74 |
| SD chronological age | 10,42 |
| Covariance | -11,61 |
| Pearson correlation coefficient | -0,2 |
| p-value | 0,05 |
Table 9.
WAI Mean and Standard Deviation divided by professional age ranges.
| Professional Age | Mean WAI | SD WAI | Title 1 | Title 2 | Title 3 |
|---|---|---|---|---|---|
| 1-5 yrs. | 42 | 6,02 | entry 1 | data | data |
| 6-10 yrs. | 40,52 | 5,16 | |||
| 11-20 yrs. | 40,58 | 4,91 | |||
| >20 yrs. | 38,54 | 4,85 |
Table 10.
WAI divided by workplace setting.
| Work Setting | WAI | |||
|---|---|---|---|---|
| Excellent | Good | Mediocre | Poor | |
| Outpatient | 25% | 30% | 35% | 10% |
| Home setting | 21,65% | 56,70% | 21,65% | 0% |
| Both | 24,59% | 49,18% | 24,59% | 1,64% |
Table 11.
WAI with respect to educational qualification.
| WAI | ||||
|---|---|---|---|---|
| Excellent | Good | Mediocre | Poor | |
| Regional school | 14,71% | 57,35% | 25,00% | 2,94% |
| Bachelor’s degree | 11,11% | 51,85% | 37,04% | 0,00% |
| Bachelor’s degree in nursing | 37,21% | 46,51% | 13,95% | 2,33% |
| Post-base studies | 30,00% | 45,00% | 25,00% | 0,00% |
Table 12.
Average WAI difference with a significance level of 5% between those who reported having no medical conditions and those with doctor-diagnosed conditions.
Table 12.
Average WAI difference with a significance level of 5% between those who reported having no medical conditions and those with doctor-diagnosed conditions.
| Mean WAI | SD | P-Value | |
|---|---|---|---|
| No | 40,16 | 4,70 | <0.05 |
| Yes, diagnosed | 35,17 | 5,31 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



