
Submitted:
25 July 2024
Posted:
29 July 2024
You are already at the latest version
Abstract
Hepatocellular carcinoma (HCC) remains one of the leading causes of cancer-related mortality worldwide and a major global health burden. The treatment of HCC has experienced a paradigm shift in the last few years, following the discovery of immunotherapy. However, despite the profound success of immunotherapy in other cancer types, their response in HCC remains unsatisfactory. Some of the reasons that can explain this poor response include the immunosuppressive microenvironment of HCC, the absence of reliable biomarkers for response, and drug resistance. Previous preclinical and clinical studies have highlighted the role of combination therapy in overcoming some of these hurdles. In this article, we discuss the benefit of combining immune checkpoint inhibitors (ICIs) with stereotactic body radiation therapy (SBRT) in HCC and shed light on promising clinical trials.
Keywords:
Hepatocellular carcinoma
; combination therapy
; multidisciplinary therapy
; outcomes
; prognosis
Challenges in the Treatment of Unresectable HCC:
The therapeutic landscape of advanced hepatocellular carcinoma (HCC) has progressed rapidly in the last decade, from multi-target tyrosine kinase inhibitors (TKIs) such as sorafenib to immunotherapies including adoptive cell therapy, and targeted therapy. However, despite the major advances in our understanding of the molecular biology of cancer cells, and the rapid development in precision oncology, drug resistance remains inevitable with single-agent therapies due to intratumor heterogenicity [1,2]. Over the past years, multiple combination therapies have been developed to overcome drug resistance, improve therapeutic efficacy, and minimize drug toxicity by dose reduction. In the 1960s Sidney Farber combined actinomycin D with radiotherapy (RT) in children with Wilm’s tumor, to reduce the dose of actinomycin D required for treatment and the risk of drug toxicity [3]. Not too long after, Frei et al. combined multiple antileukemic agents to induce and maintain remission in children with acute leukemia [4]. Since then, the number of potential combination therapies has increased exponentially.
The emergence of immunotherapy has redefined the field of oncology, including HCC. Multiple treatments have been used in combination with immunotherapy for the management of unresectable HCC, which includes the combination of more than one immune-checkpoint inhibitor (ICI) such as Durvalumab plus Tremelimumab, ICIs plus vascular endothelial growth factor (VEGF) inhibitors (Atezolizumab plus Bevacizumab), ICIs plus multi-kinase inhibitors, as well as combining immunotherapy with RT [5,6].
To better estimate the prognosis of HCC, The Barcelona Clinic Liver Cancer (BCLC) staging system was developed to stratify patients, predict survival, and guide the management of HCC. It is divided into 5 stages based on liver function, performance status, and tumor burden [7]. Depending on the disease stage, multiple treatment modalities can be utilized, including surgery (liver transplantation or resection), Locoregional therapy (ablation, trans-arterial chemoembolization or radioembolization), and systemic therapy. Despite the simplicity and prognostic accuracy of the BCLC system, it has certain limitations due to treatment allocation in each stage, which may result in undertreatment [8]. A multidisciplinary approach incorporating effective tumor biomarkers might offer better stratification of HCC patients and guide them to a more personalized treatment [9].
The European Association for the Study of the Liver (EASL) provided a new concept termed “treatment stage migration” [Figure 1]; this concept was applied to patients in each BCLC group who didn’t fulfill all the criteria for treatment allocated to them and it was recommended that patients might receive the subsequent treatment for next advanced stage (left to right). Later this concept was expanded to include bi-directional migration, where patients could receive treatment assigned to an earlier stage in certain situations (right to left) [10].
Advanced HCC is characterized by significant heterogenicity in tumor burden (TB) and underlying liver dysfunction, which makes prognostic stratification and choice of treatment challenging. Several studies have evaluated TB in HCC, such as the up-to-seven, seven-eleven criteria, and metro-ticket prognostic tool [11,12,13,14,15,16]. These criteria incorporate the tumor size and number in the calculation of the TB and have proven to predict survival in HCC patients undergoing trans-arterial chemoembolization (TACE) and surgical resection.
Some studies found an association between the etiology of HCC and response to therapy; for example, HCV-positive HBV-negative HCC patients showed an improved overall survival (OS) when treated with Sorafenib compared to patients with HBV-positive HCV-negative HCC status [17]. In contrast, patients with HBV-related HCC showed improved OS vs. HCV-related HCC when treated with Lenvatinib [18]. Atezolizumab plus Bevacizumab demonstrated OS benefit vs. Sorafenib across patient subgroups according to the IMbrave150 phase III trial, except in patients with non-viral HCC (HR=1.05; 95% CI 0.68-1.63) [19]. In addition, a meta-analysis conducted to evaluate the survival benefit of immunotherapy in patients with HCC, based on three randomized clinical trials, IMbrave150, KEYNOTE-240, and CheckMate-459, and found that programmed cell death protein-1 (PD-1) and programmed cell death ligand-1 (PDL-1) inhibitors did not improve OS in patients with non-viral HCC compared to viral HCC, particularly in patients with metabolic dysfunction-associated steatotic liver disease (MASLD) vs other etiologies (median OS= 5.4 vs 11 months; P=0.023) [20].
One of major concerns in combining ICIs with other therapies is the emergence of treatment-related adverse events (TRAEs). A meta-analysis was conducted based on the analysis of 161 clinical trials, to investigate the safety of combining PD-1 and PD-L1 inhibitors with chemotherapy, targeted therapy, and RT. The incidence of grade 3 or higher adverse events was 68·3%, 47·3%, 35·9%, 12·4%, respectively [21]. 142 trials out of 161 were evaluated for TRAEs and seven trials were included in the RT group; the most common combination therapy with ICIs in this group was SBRT (n=4/7), and cancer types included solid tumors and melanoma. In the RT group, the most common all-grade adverse event was dysphagia, and the most common grade 3 or higher TRAE was lymphopenia; the incidence of grade 3 or higher TRAEs was 14.9% in the stereotactic body radiation therapy (SBRT) subgroup vs 10.8% with other radiotherapies. Nonetheless, it is worth exploring the option of combining therapies to maximize the treatment response of advanced unresectable HCC with a poor prognosis.
HCC Immune Microenvironment:
The liver is the largest solid organ in the body and comprises 4 major cell types: hepatocytes, hepatic stellate cells, Kupffer cells, and sinusoidal endothelial cells [22]. They are responsible for detoxification, coagulation, and immune response. However, chronic inflammation (e.g. chronic viral hepatitis, non-alcoholic steatohepatitis) disrupts the liver microenvironment and stimulates kupffer cells (resident liver macrophages) to secrete various cytokines and chemokines [23]. Immune suppressive cytokines such as interleukin-10 (IL-10) and transforming growth factor-beta (TGF-β) promote angiogenesis and immune evasion in HCC [24,25].
The linkage between cancer development and inflammation was first suggested by Virchow in 1863 and subsequently validated by others [26]. Several cytokines play an important role in shaping the tumor microenvironment (TME), Some cytokines induce the recruitment of tumor-associated macrophages (TAMs), and their polarization into the tumor-promoting M2-macrophage phenotype [27], which in turn recruits CD4(+)CD25(+)FoxP3(+) T-regulatory cells into the TME. Increased regulatory T-cells were found to correlate with impaired CD8(+) T-cell and HCC progression [28]. Intra-tumoral accumulation of IL-7-producing cells was also associated with angiogenesis and tumor progression [29]. In addition, activation of the TGF-β-pathway promotes fibrogenesis and immune-cell exhaustion in the TME [30]. A combination of a TGF-β-inhibitor and ICI induced a complete response in mouse models [31].
Mechanism of Action of ICIs and Biomarkers of Response: [Figure 2]
PD-1 is an immunoinhibitory transmembrane receptor expressed by T-cells and is highly expressed on tumor-specific T-cells [32]. PDL-1 is a transmembrane glycoprotein expressed by macrophages and tumor cells and acts as a ligand for PD-1. The PD-1/PDL-1 interaction promotes immune evasion of tumor cells by inhibiting the T-cells [33] and several monoclonal antibodies have been developed to block the PD-1/PDL-1 interaction in multiple cancer types [34].
Figure 2: PD-1/PDL-1 interaction
Another important inhibitory receptor expressed on T-cells is the cytotoxic T lymphocyte antigen-4 (CTLA-4), it is found in the intracellular compartment at resting state and it translocates to the cell surface upon T-cell activation [35]. T-cell activation is induced by the interaction of CD28 on the T-cell surface and B7 molecules on antigen-presenting cells.
Some of the most important biomarkers of response to ICIs in HCC include mismatch repair deficiency (dMMR), which results in the accumulation of mutations leading to microsatellite instability (MSI), this was based on the KEYNOTE-016 phase II trial, which led to the approval of pembrolizumab as tumor agnostic ICI for unresectable or metastatic dMRR/MSI-H solid tumors [36]. Recent studies have also identified programmed death-ligand-1 (PD-L1) and tumor mutational burden (TMB) as biomarkers of response to ICIs in various cancer types [37,38].
The Evolution of Immunotherapy in HCC-A Game Changer: [Figure]
In 2008 multikinase inhibitor Sorafenib became the first FDA-approved treatment for unresectable HCC based on the SHARP trial (NCT00105443) that showed a 3-month improvement in median overall survival (mOS) with 10.7 months in the sorafenib group vs 7.9 months in the placebo group (HR, 0.69; 95% CI, 0.55 to 0.87; P<0.001). Time to radiologic progression was 5.5 months in the sorafenib group vs 2.8 months in the placebo group (P<0.001) [39].
Figure 3.
Timeline of the development of FDA-approved ICIs for HCC. *First-line therapy; **Second-line therapy.
Figure 3.
Timeline of the development of FDA-approved ICIs for HCC. *First-line therapy; **Second-line therapy.
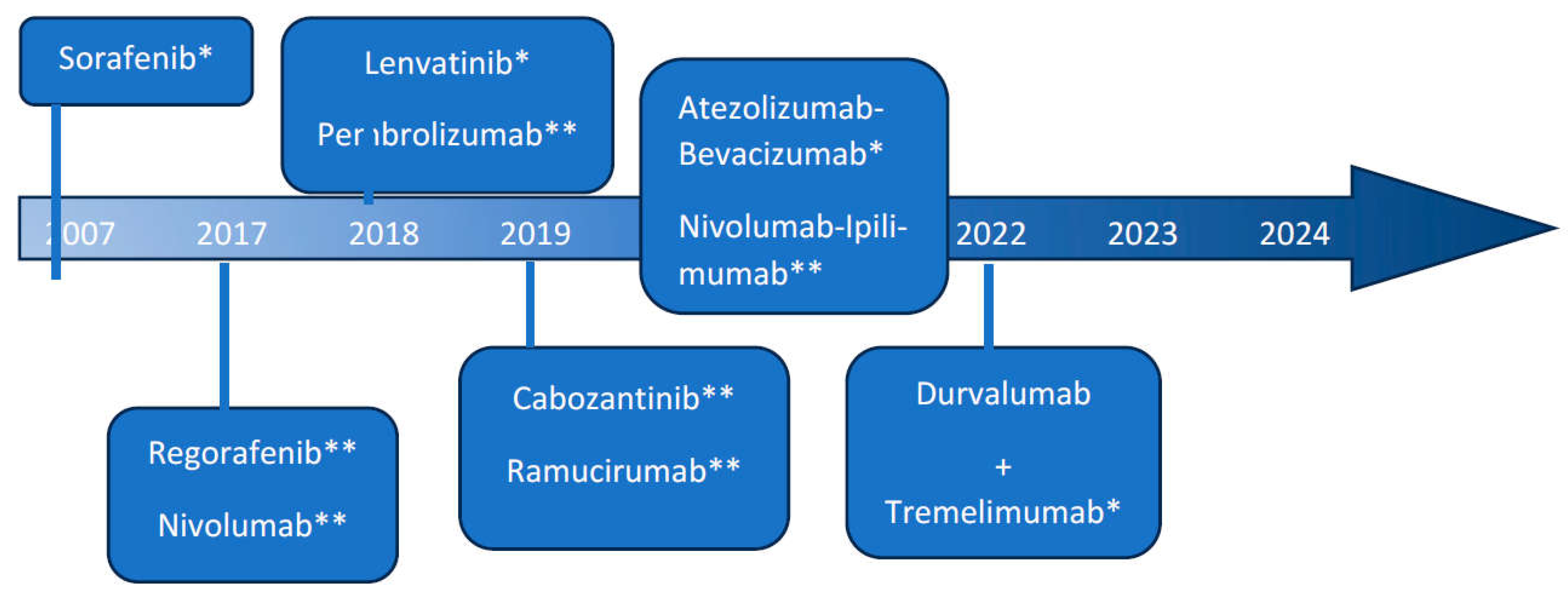
Sorafenib remained the only standard of care treatment for patients with advanced HCC, until 2017 when the FDA granted accelerated approval to Nivolumab in patients with advanced HCC previously treated with Sorafenib. Nivolumab is a monoclonal antibody that targets (PD-1) receptors. This was based on the CHECKMATE-040 trial in which patients were divided into three cohorts based on cancer etiology (HBV-infected, HCV-infected, without viral hepatitis) and received one of the following doses 0.1mg/kg (HBV-infected only), 1mg/kg, 3mg/kg, or 10mg/kg (without viral hepatitis), patients were treated until complete response, disease progression, or unacceptable toxicity. Results from this trial showed an objective response rate of 20% (95% CI 15–26) in the Nivolumab 3mg/kg dose-expansion phase and 15% (95% CI 6–28) in the dose-escalation phase, becoming the first immune checkpoint inhibitor (ICI) to be used for the treatment of advanced HCC [40]. These promising results led to the development of multiple trials that further explored the role of ICIs in the treatment of HCC, including Pembrolizumab which was evaluated in a non-randomized, open-label, phase II trial (KEYNOTE-224) and demonstrated an overall response rate of 17% (95% CI, 11 to 26) in patients with advanced HCC previously treated with Sorafenib [41]. It resulted in the FDA approval of Pembrolizumab as a second-line therapy for HCC patients who have been previously treated with Sorafenib. It was followed by a randomized, double-blind, phase III study (KEYNOTE-240) but failed to meet its prespecified statistical endpoints of improving OS and progression-free survival (PFS) [42]. Since then, multiple therapeutic modalities have been used in combination with immunotherapy, including e.g., chemotherapy, RT, and targeted therapy.
Further studies led to the development of combination therapy using Atezolizumab (anti-PD-L1) plus Bevacizumab (anti-vascular endothelial growth factor (VEGF)). This combination resulted in the improvement of OS and PFS when compared to Sorafenib as first-line treatment for unresectable HCC as demonstrated in the IMBrave150 trial; OS at 12 months was 67.2% (95% CI, 61.3 to 73.1) in the Atezolizumab-Bevacizumab group vs 54.6% (95% CI, 45.2 to 64.0) in the Sorafenib group. Median PFS was 6.8 months (95% CI, 5.7 to 8.3) vs 4.3 months (95% CI, 4.0 to 5.6) respectively [6].
The shift of immunotherapy from second-line to first-line therapy has important significance in predicting response to treatment, this is due to the disruption of the tumor microenvironment by TKIs which in turn reflects on molecular biomarkers of response [43].
Recently the infusion regimen STRIDE was evaluated in the HIMALAYA open-label, phase III trial (NCT03298451) in patients with unresectable HCC, the regimen was composed of a single dose of Tremelimumab 300mg (anti- CTLA-4), followed by Durvalumab 1500mg (anti-PDL-1) every four weeks. Subjects were randomized (1:1:1) to either the STRIDE regimen, Durvalumab only, or Sorafenib. The mOS was 16.43 months (95% CI, 14.16 to 19.58) in the STRIDE arm vs 13.77 months in the Sorafenib arm (95% CI, 12.25 to 16.13), and HR of 0.78 (96% CI, 0.65 to 0.93; P=0.0035) in favor of the STRIDE arm vs Sorafenib [5]. In October 2022, the FDA approved this combination therapy (Tremelimumab plus Durvalumab) in patients with unresectable HCC who have not received prior systemic therapy based on results from the previous trial [Table 1].
SBRT in HCC-Does It Work?
For many years HCC was considered a radioresistant tumor, due to the inability to deliver more than 30 Gy of conventional external beam radiation therapy (EBRT) to the liver without risk of radiation-induced liver damage. With the advances in the field of radiotherapy, we can now deliver optimized doses in fractionated regimens by IMRT, 3D conformal radiation therapy, proton beam therapy (PBT), or SBRT, while using computed tomography to spare normal liver tissue.
PBT induces DNA damage and cell apoptosis by generating reactive oxygen species [44]. In addition, it offers a dosimetric advantage including Bragg peak when compared to photon radiotherapy in HCC, thus allowing dose conformity and protecting organs at risk, including healthy liver parenchyma [45]. A phase II prospective trial was conducted on 76 patients with liver cirrhosis and HCC after receiving PBT and showed PFS of 36 months (95% CI 30-42 months), and a 60% 3-year PFS rate in patients within the Milan criteria [46]. This was followed by a phase III randomized clinical trial, in which 144 patients with recurrent HCC received either PBT or radiofrequency ablation (RFA) with crossover allowed, resulting in a 2-year local PFS rate of 94.8% vs. 83.9% respectively (90% CI 1.8–20; p <0.001) in the per-protocol population, and 2-year local PFS rate of 92.8% vs. 83.2% (90% CI 0.7–18.4; p <0.001) in the intension-to-treat population, meeting the non-inferiority criteria [47].
SBRT is a type of external beam radiation therapy, and it acts by delivering a precise and intense dose of radiation in fewer fractions (hypo-fractionated) while avoiding damage to normal liver tissue [48,49]. In the last few years, the role of SBRT has expanded and can be an effective tool in certain indications, for example, it can be used as a neoadjuvant locoregional therapy before liver transplant (LT) when other conventional bridge therapies such as TACE and radiofrequency ablation (RFA) are not applicable [50]. This was based on a phase II randomized trial that showed a mPFS of 17.6 months (95% CI, 6.6-28.6 months) and an ORR of 62.5% (95% CI, 54.2%-68.7%) measured by RECIST 1.1 in patients who received SBRT before deceased-donor LT [51,52]. In addition, SBRT is also used in oligometastatic disease in combination with chemotherapy and immunotherapy. Recently, a phase II study combined PD-1 antibody Sintilimab with SBRT (median dose of 54 Gy in 6 fractions) in oligometastatic (<5 metastatic lesions) HCC, and showed an overall response rate (ORR) of 96% according to the RECIST v1.1criteria [53]. The efficacy of SBRT in HCC was demonstrated in the RTOG 1112 phase III randomized clinical trial, which compared SBRT followed by Sorafenib vs Sorafenib alone in patients with HCC, median OS was 12.3 months (90% CI 10.6, 14.3) in the Sorafenib group vs 15.8 months (90% CI 11.4-19.2) in the SBRT plus Sorafenib group (HR=0.77, p=0.0554) [54].
The Rationale behind Combining SBRT and ICIs and the Evidence:
RT can induce inflammatory and immune modulatory effects in the TME. Initially, RT creates a pro-inflammatory state by releasing damage-associated molecular patterns (DAMPs) from damaged cells, activating the innate immune system (e.g., macrophages, natural killer cells, dendritic cells) and releasing pro-inflammatory cytokines [55]. This is followed by a rebound immunosuppression stage induced by the expression of (PDL-1) and TAMs that suppress T-cells and promote tumor growth [56].
Several pre-clinical studies have demonstrated the synergistic effect between SBRT and ICIs. One study showed an enhanced response of SBRT in an orthotopic murine model of HCC after delivery of three doses of anti-PD-1 antibody concurrently with 30 Gy SBRT in three fractions, and this resulted in reduced tumor growth rate and improved survival (P<0.05) [57].
An interesting phenomenon was reported in some studies following treatment with SBRT and immunotherapy, in which tumor regression was observed in lesions outside of the irradiated region, this phenomenon was termed the “abscopal effect” [58]. Several mechanisms have been postulated, including the release of tumor-associated antigens because of radiation therapy, which is then engulfed by antigen-presenting cells (e.g., dendritic cells), that in turn activates the cytotoxic T-cells and eventually attack the tumor cells outside of the irradiated region [59].
Multiple clinical trials have proven the efficacy of SBRT plus ICIs combination therapy, including a phase I trial of SBRT followed by Nivolumab plus Ipilimumab vs Nivolumab alone in advanced/unresectable HCC. Despite early closure of the study due to slow accrual, 13 patients were evaluated for the study endpoint which was dose-limiting toxicity (DLT) occurring within 6 months of SBRT and demonstrated acceptable safety with 2 (15.4%) out of 13 subjects experiencing DLTs [60].
Another study was conducted in a tertiary hospital in Hong Kong, where 226 patients with locally advanced HCC were enrolled [61]. 210 patients received TACE and 16 patients received SBRT plus immunotherapy, however, the SBRT group had a higher percentage of BCLC stage C and portal vein invasion. After propensity score matching 48 patients with TACE were compared to the 16 patients with SBRT plus immunotherapy. The SBRT dose ranged from 25 to 37.5 Gy and was given in five fractions for 1–2 weeks, followed by Nivolumab 3mg/kg every two weeks for a median of 10 cycles (range: 1-20 doses). Results showed a significant survival benefit in the SBRT plus immunotherapy group vs the TACE group, the 12-month OS was 93.8% vs 31.3% respectively and the 24-month OS was 80.4% vs 8.3%, respectively (p <0.001), the 12-month PFS was 93.3% vs 16.7% respectively, and the 24-month PFS was 77.8% vs 2.1%, respectively (p <0.001).
A single-arm study was conducted to evaluate the response rate and safety of anti-PD1 monoclonal antibody Camrelizumab plus SBRT in unresectable HCC [62]. Twenty-one patients were enrolled and received five fractions per week of palliative SBRT daily with a dose range of 30-50 Gy, 200 mg of Camrelizumab was administered intravenously from day one of SBRT and every 3 weeks. After a median follow-up period of 19.7 months, the ORR was 52.4% according to RESIST v1.1, and median PFS and OS were 5.8 (95% CI 4.2–7.4) and 14.2 months (95% CI 7.2–21.2), respectively.
As demonstrated in the IMBrave 150 phase III clinical trial Atezolizumab plus Bevacizumab resulted in better survival outcomes when compared to sorafenib in unresectable HCC and is now recommended by the FDA as first-line therapy in unresectable HCC [6], which encouraged further studies in combining ICIs with anti-angiogenic therapies. A single-arm explorative clinical trial was conducted by combining Toripalimab (PD-1 monoclonal antibody) and Anlotinib (vascular endothelial growth factor receptor inhibitor) following SBRT in unresectable HCC [63], Twenty patients were enrolled and received a total dose of 24 Gy (8 Gy*3) followed by 6 cycles of Toripalimab plus Anlotinib after last dose of SBRT, median PFS was 7.4 months (range, 1.1-27.7 months), however 70% of patients experienced TRAEs of various grades. This supports the idea that SBRT induces an adaptive immune response outside of the irradiated region. Notably, patients in this study also received a daily dose of probiotics, this suggests that the translocation of the intestinal flora plays a role in the development of HCC and that the regulation of the gut microbiome can enhance the immunologic response of ICIs [64].
Additionally, a recent retrospective study demonstrated improvement in survival outcomes when adding RT to patients with advanced HCC treated with ICIs and antiangiogenic therapy. A total of 76 patients with advanced HCC were included in the study, 33 patients received intensity-modulated radiation therapy (IMRT) or SBRT in addition to the ICIs and antiangiogenic therapy vs 43 patients only received systemic therapy and did not receive RT. The median PFS was 8.3 months (95% CI, 5.4-11.3) in the RT group vs 4.2 months (95% CI, 3.4-5.0) in the non-RT group (P < .001), and the median OS was not reached in the RT group vs 9.7 months (95% CI, 4.1-15.3) in the non-RT group (P = .002). The disease control rate (DCR) was 100% in the RT group vs 75.9% (95% CI, 56.5-89.7) in the non-RT group (P = .005) [65] [Table 2].
Current Guidelines and Future Direction:
The current NCCN guidelines recommend SBRT as an alternative to ablation and/or embolization techniques or when these therapies have failed or are contraindicated (e.g., unresectable disease or patients with local disease but poor performance status that makes them ineligible for surgery) [48,66], It is typically administered in a dose of 30-50 Gy in 3-5 fractions. However, there are no definite recommendations regarding the combination of SBRT and ICIs in HCC.
TACE is currently the first-line therapy for unresectable, large HCC with no vascular invasion [67], however, a study comparing SBRT with TACE for unresectable medium-sized (3-8 cm) HCC showed favorable disease control and OS in the SBRT group vs TACE group, with 3-year infield control of 77.5% vs 55.6% (P = .007), respectively, and a 3-year OS of 55.0% vs 13.0% (P < .001), respectively [68].
Recently, there has been growing evidence to support the use of SBRT in unresectable and oligometastatic HCC [69]. The role of SBRT in oligometastatic HCC has been suggested in multiple retrospective studies [70,71]. Further large, randomized, controlled clinical trials are needed to establish the benefit of ICIs plus SBRT in this unique subgroup, to our knowledge only one prospective phase II non-controlled trial evaluated the role of SBRT plus Sintilimab in oligometastatic HCC, 25 patients were enrolled in this study, including 24 patients with HBV and all patients had Child-Pugh class A. Even though the median OS was not reached, the OS rates at 12 and 24 months were 91.5% and 83.2%, respectively and the median PFS was 19.7 (95% CI: 16.9-NA), and the disease-control rate after treatment was 96% [72]. Notably, this study also explored the biomarkers of response to predict efficacy, lymphocyte counts and their subsets were analyzed by flow cytometry, mPFS of 19.7 months was applied as a cutoff, there was no significant difference between lymphocyte count >19.7 months vs <19.7 months at baseline, however, after three to four cycles, PFS ≥ 19.7 months was associated with higher lymphocyte counts and CD3+, CD4+, CD8+ T, and CD15+CD56+ NK cells when compared to PFS < 19.7 months. It supports the hypothesis that lymphocyte count can act as a predictor of response to SBRT in HCC, which was previously studied in non-small cell lung cancer patients [73].
Conclusion:
SBRT has significant immunomodulatory effects and can enhance the tumor response of ICIs. Several clinical trials evaluated the safety and efficacy of SBRT and demonstrated tumor response both in the irradiated region and in distant lesions. Further studies are needed to evaluate the efficacy of combining SBRT and ICIs in HCC, establish the optimal sequence of treatment, evaluate their role in oligometastatic HCC, and explore biomarkers that can help in case selection and prediction of response to treatment.
Author Contributions
Prasun K. Jalal MD made substantial contributions to the initial conception of the work, Ahmed Elhariri MD was involved in drafting the work and all other authors revised it critically for important intellectual content. All authors have given final approval of the version that was submitted for publication and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
None.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Ladd, A.D.; Duarte, S.; Sahin, I.; Zarrinpar, A. Mechanisms of drug resistance in HCC. Hepatology 2023, 79, 926–940. [Google Scholar] [CrossRef]
- Boshuizen, J.; Peeper, D.S. Rational Cancer Treatment Combinations: An Urgent Clinical Need. Mol. Cell 2020, 78, 1002–1018. [Google Scholar] [CrossRef]
- Farber, S.; D'Angio, G.; Evans, A.; Mitus, A. CLINICAL STUDIES OF ACTINOMYCIN D WITH SPECIAL REFERENCE TO WILMS' TUMOR IN CHILDREN*. Ann. New York Acad. Sci. 1960, 89, 421–424. [Google Scholar] [CrossRef] [PubMed]
- Frei, E.; Karon, M.; Levin, R.H.; Freireich, E.J.; Taylor, R.J.; Hananian, J.; Selawry, O.; Holland, J.F.; Hoogstraten, B.; Wolman, I.J.; et al. The Effectiveness of Combinations of Antileukemic Agents in Inducing and Maintaining Remission in Children with Acute Leukemia. Blood 1965, 26, 642–656. [Google Scholar] [CrossRef] [PubMed]
- Abou-Alfa, G.K.; Lau, G.; Kudo, M.; Chan, S.L.; Kelley, R.K.; Furuse, J.; Sukeepaisarnjaroen, W.; Kang, Y.-K.; Van Dao, T.; De Toni, E.N.; et al. Tremelimumab plus Durvalumab in Unresectable Hepatocellular Carcinoma. NEJM Évid. 2022, 1. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.-Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef] [PubMed]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2021, 76, 681–693. [Google Scholar] [CrossRef]
- Trevisani, F.; Vitale, A.; Kudo, M.; Kulik, L.; Park, J.-W.; Pinato, D.J.; Cillo, U. Merits and boundaries of the BCLC staging and treatment algorithm: Learning from the past to improve the future with a novel proposal. J. Hepatol. 2024, 80, 661–669. [Google Scholar] [CrossRef]
- Mehta, N.; Kotwani, P.; Norman, J.; Shui, A.; Li, P.J.; Saxena, V.; Chan, W.; Yao, F.Y. AFP-L3 and DCP are superior to AFP in predicting waitlist dropout in HCC patients: Results of a prospective study. Liver Transplant. 2023, 29, 1041–1049. [Google Scholar] [CrossRef]
- EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J Hepatol, 2018. 69(1): p. 182-236.
- Hung, Y.-W.; Lee, I.-C.; Chi, C.-T.; Lee, R.-C.; Liu, C.-A.; Chiu, N.-C.; Hwang, H.-E.; Chao, Y.; Hou, M.-C.; Huang, Y.-H. Redefining Tumor Burden in Patients with Intermediate-Stage Hepatocellular Carcinoma: The Seven-Eleven Criteria. Liver Cancer 2021, 10, 629–640. [Google Scholar] [CrossRef]
- Mazzaferro, V.M.; Llovet, J.M.; Miceli, R.; Bhoori, S.; Schiavo, M.; Mariani, L.; Camerini, T.; Roayaie, S.; Schwartz, M.E.; Grazi, G.L.; et al. Predicting survival after liver transplantation in patients with hepatocellular carcinoma beyond the Milan criteria: a retrospective, exploratory analysis. Lancet Oncol. 2009, 10, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Moris, D.; Shaw, B.I.; McElroy, L.; Barbas, A.S. Using Hepatocellular Carcinoma Tumor Burden Score to Stratify Prognosis after Liver Transplantation. Cancers 2020, 12, 3372. [Google Scholar] [CrossRef] [PubMed]
- I Tsilimigras, D.; Moris, D.; Hyer, J.M.; Bagante, F.; Sahara, K.; Moro, A.; Paredes, A.Z.; Mehta, R.; Ratti, F.; Marques, H.P.; et al. Hepatocellular carcinoma tumour burden score to stratify prognosis after resection. Br. J. Surg. 2020, 107, 854–864. [Google Scholar] [CrossRef] [PubMed]
- Vitale, A.; Lai, Q.; Farinati, F.; Bucci, L.; Giannini, E.G.; Napoli, L.; Ciccarese, F.; Rapaccini, G.L.; Di Marco, M.; Caturelli, E.; et al. Utility of Tumor Burden Score to Stratify Prognosis of Patients with Hepatocellular Cancer: Results of 4759 Cases from ITA.LI.CA Study Group. J. Gastrointest. Surg. 2018, 22, 859–871. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, K., D. Morioka, S. Conci, G.A. Margonis, Y. Sawada, A. Ruzzenente, et al., The Tumor Burden Score: A New "Metro-ticket" Prognostic Tool For Colorectal Liver Metastases Based on Tumor Size and Number of Tumors. Ann Surg, 2018. 267(1): p. 132-141.
- Jackson, R.; Psarelli, E.-E.; Berhane, S.; Khan, H.; Johnson, P. Impact of Viral Status on Survival in Patients Receiving Sorafenib for Advanced Hepatocellular Cancer: A Meta-Analysis of Randomized Phase III Trials. J. Clin. Oncol. 2017, 35, 622–628. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Wang, J.; Ding, X.; Xu, Y.; Yu, M.; Wu, H.; Deng, N.; Li, W.; Chen, J. Clinical study of lenvatinib in the treatment of hepatitis virus-related hepatocellular carcinoma and antiviral therapy. Front. Pharmacol. 2023, 13, 1032881. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.-L., S. Qin, M. Ikeda, P.R. Galle, M. Ducreux, T.-Y. Kim, et al., Updated efficacy and safety data from IMbrave150: Atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. Journal of Hepatology, 2022. 76(4): p. 862-873.
- Pfister, D.; Núñez, N.G.; Pinyol, R.; Govaere, O.; Pinter, M.; Szydlowska, M.; Gupta, R.; Qiu, M.; Deczkowska, A.; Weiner, A.; et al. NASH limits anti-tumour surveillance in immunotherapy-treated HCC. Nature 2021, 592, 450–456. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Yao, Z.; Bai, H.; Duan, J.; Wang, Z.; Wang, X.; Zhang, X.; Xu, J.; Fei, K.; Zhang, Z.; et al. Treatment-related adverse events of PD-1 and PD-L1 inhibitor-based combination therapies in clinical trials: a systematic review and meta-analysis. Lancet Oncol. 2021, 22, 1265–1274. [Google Scholar] [CrossRef]
- Ding, C.; Li, Y.; Guo, F.; Jiang, Y.; Ying, W.; Li, D.; Yang, D.; Xia, X.; Liu, W.; Zhao, Y.; et al. A Cell-type-resolved Liver Proteome. Mol. Cell. Proteom. 2016, 15, 3190–3202. [Google Scholar] [CrossRef]
- Roberts, R.A.; Ganey, P.E.; Ju, C.; Kamendulis, L.M.; Rusyn, I.; Klaunig, J.E. Role of the Kupffer Cell in Mediating Hepatic Toxicity and Carcinogenesis. Toxicol. Sci. 2006, 96, 2–15. [Google Scholar] [CrossRef]
- Chia, C.S., K. Ban, H. Ithnin, H. Singh, R. Krishnan, S. Mokhtar, et al., Expression of interleukin-18, interferon-γ and interleukin-10 in hepatocellular carcinoma. Immunology Letters, 2002. 84(3): p. 163-172.
- Chen, J.; Zaidi, S.; Rao, S.; Chen, J.-S.; Phan, L.; Farci, P.; Su, X.; Shetty, K.; White, J.; Zamboni, F.; et al. Analysis of Genomes and Transcriptomes of Hepatocellular Carcinomas Identifies Mutations and Gene Expression Changes in the Transforming Growth Factor-β Pathway. Gastroenterology 2018, 154, 195–210. [Google Scholar] [CrossRef] [PubMed]
- Balkwill, F. and A. Mantovani, Inflammation and cancer: back to Virchow? Lancet, 2001. 357(9255): p. 539-45.
- Noy, R.; Pollard, J.W. Tumor-associated macrophages: From mechanisms to therapy. Immunity 2014, 41, 49–61. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.; Xu, D.; Liu, Z.; Shi, M.; Zhao, P.; Fu, B.; Zhang, Z.; Yang, H.; Zhang, H.; Zhou, C.; et al. Increased Regulatory T Cells Correlate With CD8 T-Cell Impairment and Poor Survival in Hepatocellular Carcinoma Patients. Gastroenterology 2007, 132, 2328–2339. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.-P.; Yan, J.; Xu, J.; Pang, X.-H.; Chen, M.-S.; Li, L.; Wu, C.; Li, S.-P.; Zheng, L. Increased intratumoral IL-17-producing cells correlate with poor survival in hepatocellular carcinoma patients. J. Hepatol. 2009, 50, 980–989. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Gingold, J.A.; Su, X. Immunomodulatory TGF-β Signaling in Hepatocellular Carcinoma. Trends Mol. Med. 2019, 25, 1010–1023. [Google Scholar] [CrossRef]
- Ganesh, K.; Massagué, J. TGF-beta Inhibition and Immunotherapy: Checkmate. Immunity 2018, 48, 626–628. [Google Scholar] [CrossRef] [PubMed]
- Ahmadzadeh, M.; Johnson, L.A.; Heemskerk, B.; Wunderlich, J.R.; Dudley, M.E.; White, D.E.; Rosenberg, S.A. Tumor antigen–specific CD8 T cells infiltrating the tumor express high levels of PD-1 and are functionally impaired. Blood 2009, 114, 1537–1544. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Sun, Q.; Zhang, X. PD-1 and its ligands are important immune checkpoints in cancer. Oncotarget 2016, 8, 2171–2186. [Google Scholar] [CrossRef] [PubMed]
- Ai, L., J. Chen, H. Yan, Q. He, P. Luo, Z. Xu, et al., Research Status and Outlook of PD-1/PD-L1 Inhibitors for Cancer Therapy. Drug Des Devel Ther, 2020. 14: p. 3625-3649.
- Buchbinder, E.; Hodi, F.S. Cytotoxic T lymphocyte antigen-4 and immune checkpoint blockade. J. Clin. Investig. 2015, 125, 3377–3383. [Google Scholar] [CrossRef]
- Le, D.T.; Uram, J.N.; Wang, H.; Bartlett, B.R.; Kemberling, H.; Eyring, A.D.; Skora, A.D.; Luber, B.S.; Azad, N.S.; Laheru, D.; et al. PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N. Engl. J. Med. 2015, 372, 2509–2520. [Google Scholar] [CrossRef]
- Li, H.; van der Merwe, P.A.; Sivakumar, S. Biomarkers of response to PD-1 pathway blockade. Br. J. Cancer 2022, 126, 1663–1675. [Google Scholar] [CrossRef] [PubMed]
- Samstein, R.M.; Lee, C.-H.; Shoushtari, A.N.; Hellmann, M.D.; Shen, R.; Janjigian, Y.Y.; Barron, D.A.; Zehir, A.; Jordan, E.J.; Omuro, A.; et al. Tumor mutational load predicts survival after immunotherapy across multiple cancer types. Nat. Genet. 2019, 51, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M., S. Ricci, V. Mazzaferro, P. Hilgard, E. Gane, J.F. Blanc, et al., Sorafenib in advanced hepatocellular carcinoma. N Engl J Med, 2008. 359(4): p. 378-90.
- El-Khoueiry, A.B.; Sangro, B.; Yau, T.; Crocenzi, T.S.; Kudo, M.; Hsu, C.; Kim, T.-Y.; Choo, S.-P.; Trojan, J.; Welling, T.H., 3rd; et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): an open-label, non-comparative, phase 1/2 dose escalation and expansion trial. Lancet 2017, 389, 2492–2502. [Google Scholar] [CrossRef] [PubMed]
- Zhu, A.X.; Finn, R.S.; Edeline, J.; Cattan, S.; Ogasawara, S.; Palmer, D.; Verslype, C.; Zagonel, V.; Fartoux, L.; Vogel, A.; et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): A non-randomised, open-label phase 2 trial. Lancet Oncol. 2018, 19, 940–952. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Ryoo, B.-Y.; Merle, P.; Kudo, M.; Bouattour, M.; Lim, H.Y.; Breder, V.; Edeline, J.; Chao, Y.; Ogasawara, S.; et al. Pembrolizumab As Second-Line Therapy in Patients With Advanced Hepatocellular Carcinoma in KEYNOTE-240: A Randomized, Double-Blind, Phase III Trial. J. Clin. Oncol. 2020, 38, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Haber, P.K.; Castet, F.; Torres-Martin, M.; Andreu-Oller, C.; Puigvehí, M.; Miho, M.; Radu, P.; Dufour, J.-F.; Verslype, C.; Zimpel, C.; et al. Molecular Markers of Response to Anti-PD1 Therapy in Advanced Hepatocellular Carcinoma. Gastroenterology 2023, 164, 72–88. [Google Scholar] [CrossRef] [PubMed]
- Răileanu, M.; Straticiuc, M.; Iancu, D.-A.; Andrei, R.-F.; Radu, M.; Bacalum, M. Proton irradiation induced reactive oxygen species promote morphological and functional changes in HepG2 cells. J. Struct. Biol. 2022, 214, 107919. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Krishnan, S.; Zhang, X.; Dong, L.; Briere, T.; Crane, C.H.; Martel, M.; Gillin, M.; Mohan, R.; Beddar, S. Proton Radiotherapy for Liver Tumors: Dosimetric Advantages Over Photon Plans. Med Dosim. 2007, 33, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Bush, D.A.; Kayali, Z.; Grove, R.; Slater, J.D. The safety and efficacy of high-dose proton beam radiotherapy for hepatocellular carcinoma: a phase 2 prospective trial. Cancer 2011, 117, 3053–3059. [Google Scholar] [CrossRef]
- Kim, T.H.; Koh, Y.H.; Kim, B.H.; Kim, M.J.; Lee, J.H.; Park, B.; Park, J.-W. Proton beam radiotherapy vs. radiofrequency ablation for recurrent hepatocellular carcinoma: A randomized phase III trial. J. Hepatol. 2020, 74, 603–612. [Google Scholar] [CrossRef]
- Ohri, N., W. A. Tomé, A. Méndez Romero, M. Miften, R.K. Ten Haken, L.A. Dawson, et al., Local Control After Stereotactic Body Radiation Therapy for Liver Tumors. Int J Radiat Oncol Biol Phys, 2021. 110(1): p. 188-195.
- Kimura, T.; Fujiwara, T.; Kameoka, T.; Adachi, Y.; Kariya, S. The Current Role of Stereotactic Body Radiation Therapy (SBRT) in Hepatocellular Carcinoma (HCC). Cancers 2022, 14, 4383. [Google Scholar] [CrossRef] [PubMed]
- Kulik, L.; Heimbach, J.K.; Zaiem, F.; Almasri, J.; Prokop, L.J.; Wang, Z.; Murad, M.H.; Mohammed, K. Therapies for patients with hepatocellular carcinoma awaiting liver transplantation: A systematic review and meta-analysis. Hepatology 2017, 67, 381–400. [Google Scholar] [CrossRef]
- Kimura, T.; Fujiwara, T.; Kameoka, T.; Adachi, Y.; Kariya, S. The Current Role of Stereotactic Body Radiation Therapy (SBRT) in Hepatocellular Carcinoma (HCC). Cancers 2022, 14, 4383. [Google Scholar] [CrossRef] [PubMed]
- Lee, V.H.-F., V. Vardhanabhuti, T.C.-L. Wong, K.-O. Lam, H.C.-W. Choi, K.W.-H. Chiu, et al., Stereotactic Body Radiotherapy and Liver Transplant for Liver Cancer: A Nonrandomized Controlled Trial. JAMA Network Open, 2024. 7(6): p. e2415998-e2415998.
- Chen, Y.; Yang, P.; Du, S.; Zhou, J.; Huang, C.; Zhu, W.; Hu, Y.; Yu, Y.; Liu, T.; Zeng, Z. A phase II study of stereotactic body radiotherapy (SBRT) combined with sintilimab in patients with recurrent or oligometastatic hepatocellular carcinoma (HCC). J. Clin. Oncol. 2022, 40, 4071–4071. [Google Scholar] [CrossRef]
- Dawson, L.A.; Winter, K.A.; Knox, J.J.; Zhu, A.X.; Krishnan, S.; Guha, C.; Kachnic, L.A.; Gillin, M.; Hong, T.S.; Craig, T.; et al. NRG/RTOG 1112: Randomized phase III study of sorafenib vs. stereotactic body radiation therapy (SBRT) followed by sorafenib in hepatocellular carcinoma (HCC). J. Clin. Oncol. 2023, 41, 489–489. [Google Scholar] [CrossRef]
- Roh, J.S.; Sohn, D.H. Damage-Associated Molecular Patterns in Inflammatory Diseases. Immune Netw. 2018, 18, e27. [Google Scholar] [CrossRef] [PubMed]
- Fridman, W.H.; Pagès, F.; Sautès-Fridman, C.; Galon, J. The immune contexture in human tumours: impact on clinical outcome. Nat. Rev. Cancer 2012, 12, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Friedman, D.; Baird, J.R.; Young, K.H.; Cottam, B.; Crittenden, M.R.; Friedman, S.; Gough, M.J.; Newell, P. Programmed cell death-1 blockade enhances response to stereotactic radiation in an orthotopic murine model of hepatocellular carcinoma. Hepatol. Res. 2016, 47, 702–714. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, H. , Abscopal effect of stereotactic radiotherapy combined with anti-PD-1/PD-L1 immunotherapy: Mechanisms, clinical efficacy, and issues. Cancer Commun (Lond), 2020. 40(12): p. 649-654.
- Garelli, E.; Rittmeyer, A.; Putora, P.M.; Glatzer, M.; Dressel, R.; Andreas, S. Abscopal Effect in Lung Cancer: Three Case Reports and a Concise Review. Immunotherapy 2019, 11, 1445–1461. [Google Scholar] [CrossRef]
- Juloori, A.; Katipally, R.R.; Lemons, J.M.; Singh, A.K.; Iyer, R.; Robbins, J.R.; George, B.; Hall, W.A.; Pitroda, S.P.; Arif, F.; et al. Phase 1 Randomized Trial of Stereotactic Body Radiation Therapy Followed by Nivolumab plus Ipilimumab or Nivolumab Alone in Advanced/Unresectable Hepatocellular Carcinoma. Int. J. Radiat. Oncol. 2022, 115, 202–213. [Google Scholar] [CrossRef]
- Chiang, C.-L.; Chiu, K.W.-H.; Lee, F.A.-S.; Kong, F.-M.S.; Chan, A.C.-Y. Combined Stereotactic Body Radiotherapy and Immunotherapy Versus Transarterial Chemoembolization in Locally Advanced Hepatocellular Carcinoma: A Propensity Score Matching Analysis. Front. Oncol. 2021, 11, 798832. [Google Scholar] [CrossRef]
- Li, J.-X.; Su, T.-S.; Gong, W.-F.; Zhong, J.-H.; Yan, L.-Y.; Zhang, J.; Li, L.-Q.; He, M.-L.; Zhang, R.-J.; Du, Y.-Q.; et al. Combining stereotactic body radiotherapy with camrelizumab for unresectable hepatocellular carcinoma: a single-arm trial. Hepatol. Int. 2022, 16, 1179–1187. [Google Scholar] [CrossRef]
- Chen, Y.; Hong, H.; Fang, W.; Zhang, X.; Luo, H.; Chen, Z.; Yu, J.; Fan, W.; Chi, X.; Peng, Y. Toripalimab in combination with Anlotinib for unresectable hepatocellular carcinoma after SBRT: A prospective, single-arm, single-center clinical study. Front. Oncol. 2023, 13, 1113389. [Google Scholar] [CrossRef]
- Schwabe, R.F. and T.F. Greten, Gut microbiome in HCC - Mechanisms, diagnosis and therapy. J Hepatol, 2020. 72(2): p. 230-238.
- Ning, C., X. Zhang, Y. Wang, X. Yang, X. Yang, J. Chao, et al., Radiation Therapy With Combination Therapy of Immune Checkpoint Inhibitors and Antiangiogenic Therapy for Hepatocellular Carcinoma. International Journal of Radiation Oncology, Biology, Physics, 2024. 118(5): p. 1461-1471.
- Kwon, J.H.; Bae, S.H.; Kim, J.Y.; Choi, B.O.; Jang, H.S.; Jang, J.W.; Choi, J.Y.; Yoon, S.K.; Chung, K.W. Long-term effect of stereotactic body radiation therapy for primary hepatocellular carcinoma ineligible for local ablation therapy or surgical resection. Stereotactic radiotherapy for liver cancer. BMC Cancer 2010, 10, 475–475. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.H.; Kim, J.H.; Shim, J.H.; Ko, H.-K.; Chu, H.H.; Shin, J.H.; Yoon, H.-K.; Ko, G.-Y.; Gwon, D.I. Chemoembolization for Single Large Hepatocellular Carcinoma with Preserved Liver Function: Analysis of Factors Predicting Clinical Outcomes in a 302 Patient Cohort. Life 2021, 11, 840. [Google Scholar] [CrossRef] [PubMed]
- Shen, P.-C.; Chang, W.-C.; Lo, C.-H.; Yang, J.-F.; Lee, M.-S.; Dai, Y.-H.; Lin, C.-S.; Fan, C.-Y.; Huang, W.-Y. Comparison of Stereotactic Body Radiation Therapy and Transarterial Chemoembolization for Unresectable Medium-Sized Hepatocellular Carcinoma. Int. J. Radiat. Oncol. 2019, 105, 307–318. [Google Scholar] [CrossRef] [PubMed]
- Bujold, A.; Massey, C.A.; Kim, J.J.; Brierley, J.; Cho, C.; Wong, R.K.; Dinniwell, R.E.; Kassam, Z.; Ringash, J.; Cummings, B.; et al. Sequential Phase I and II Trials of Stereotactic Body Radiotherapy for Locally Advanced Hepatocellular Carcinoma. J. Clin. Oncol. 2013, 31, 1631–1639. [Google Scholar] [CrossRef]
- Gerum, S.; Heinz, C.; Belka, C.; Walter, F.; Paprottka, P.; De Toni, E.N.; Roeder, F. Stereotactic body radiation therapy (SBRT) in patients with hepatocellular carcinoma and oligometastatic liver disease. Radiat. Oncol. 2018, 13, 1–9. [Google Scholar] [CrossRef]
- Yao, E.; Chen, J.; Zhao, X.; Zheng, Y.; Wu, X.; Han, F.; Huang, H.; Liang, P.; Liu, J.; Wu, F.; et al. Efficacy of Stereotactic Body Radiotherapy for Recurrent or Residual Hepatocellular Carcinoma after Transcatheter Arterial Chemoembolization. BioMed Res. Int. 2018, 2018, 1–6. [Google Scholar] [CrossRef]
- Chen, Y.-X.; Yang, P.; Du, S.-S.; Zhuang, Y.; Huang, C.; Hu, Y.; Zhu, W.-C.; Yu, Y.-Y.; Liu, T.-S.; Zeng, Z.-C. Stereotactic body radiotherapy combined with sintilimab in patients with recurrent or oligometastatic hepatocellular carcinoma: A phase II clinical trial. World J. Gastroenterol. 2023, 29, 3871–3882. [Google Scholar] [CrossRef]
- Liu, C.; Hu, Q.; Xu, B.; Hu, X.; Su, H.; Li, Q.; Zhang, X.; Yue, J.; Yu, J. Peripheral memory and naïve T cells in non-small cell lung cancer patients with lung metastases undergoing stereotactic body radiotherapy: predictors of early tumor response. Cancer Cell Int. 2019, 19, 1–9. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Treatment stage migration.
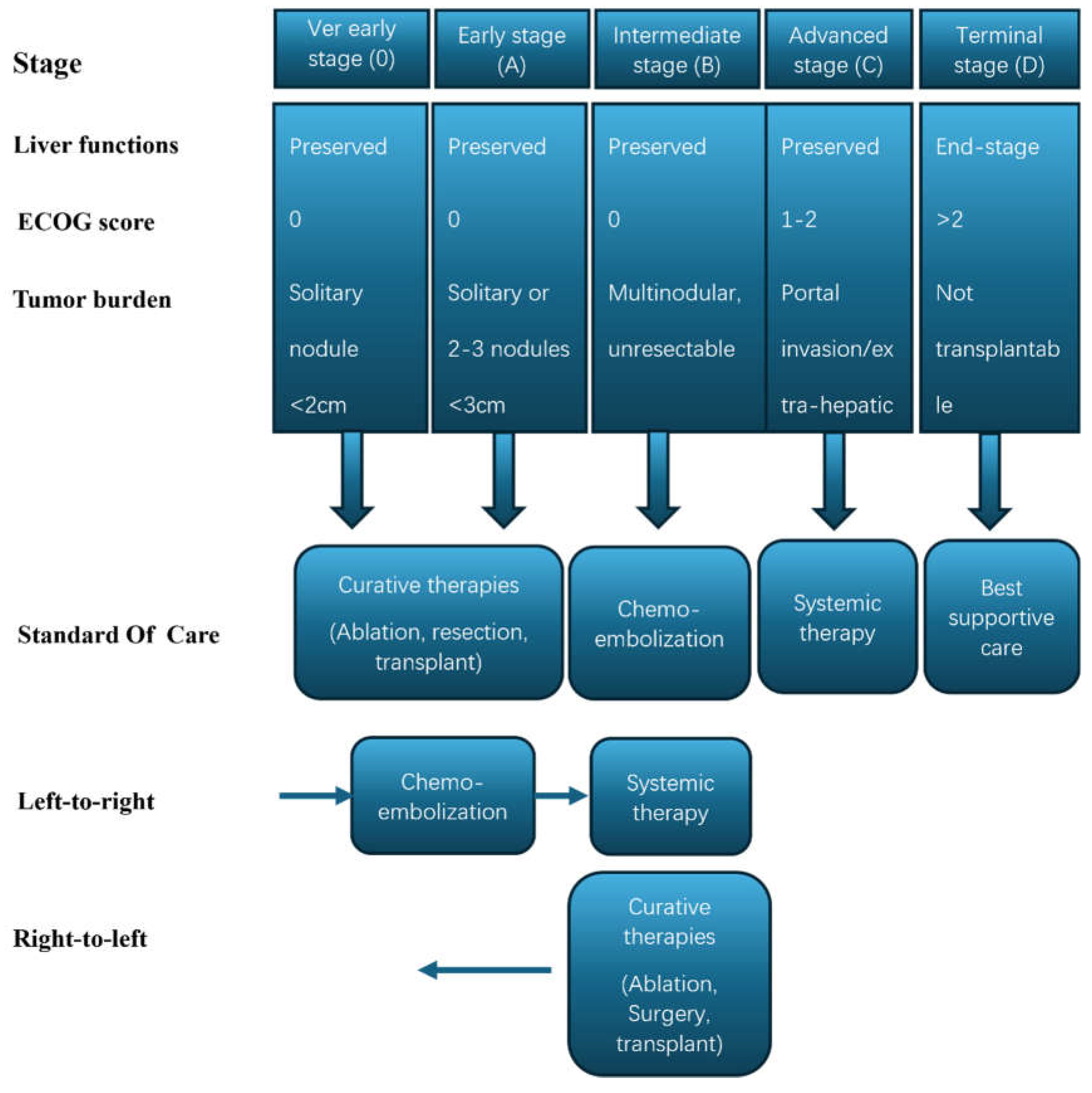
Figure 2.
MHC-1: major histocompatibility complex-1, TCR: T-cell receptor, PD-1: Programmed cell death protein-1, PDL-1: Programmed death-ligand-1.
Figure 2.
MHC-1: major histocompatibility complex-1, TCR: T-cell receptor, PD-1: Programmed cell death protein-1, PDL-1: Programmed death-ligand-1.
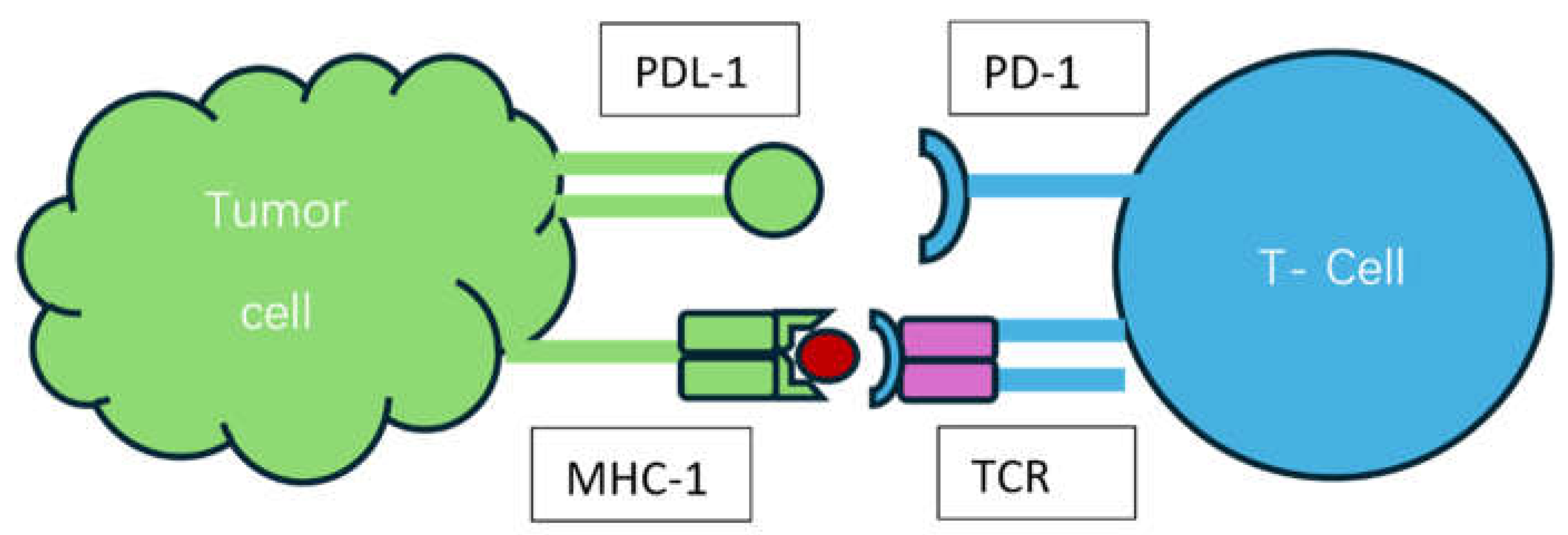

Table 1.
FDA-approved combination immunotherapies for HCC*.
| Combination therapy | Target | Indication | FDA approval date | ClinicalTrials.gov Identifier |
|---|---|---|---|---|
| Nivolumab + Ipilimumab | PD-1 + CTLA-4 | HCC who has been previously treated with sorafenib | March 10, 2020 | Cohort 4 of CHECKMATE-040 (NCT01658878) |
| Atezolizumab + Bevacizumab | PDL-1 + VEGF | unresectable or metastatic HCC who have not received prior systemic therapy | May 29, 2020 | IMbrave150 (NCT03434379) |
| Durvalumab + Tremelimumab | PDL-1 + CTLA4 | unresectable HCC | October 21, 2022 | HIMALAYA (NCT03298451) |
* Data collected from FDA.gov (Date: 22 July 2024).
Table 2.
Ongoing clinical trials combining ICIs and SBRT in HCC**.
| ICI | SBRT dose | Regimen | Study Phase | 1ry endpoint | ClinicalTrials.gov Identifier | Status |
|---|---|---|---|---|---|---|
| Atezolizumab and bevacizumab | N/A | Atezolizumab on day 1 of two study cycles (21 days/cycle) and Bevacizumab 1x weekly for 2 study cycles | I | Proportion of patients with grade 3-4 treatment-related adverse events (TRAE) | NCT04857684 | Recruiting |
| Tislelizumab | 8 Gy × 3 fractions | SBRT (day 1,3,5) and Tislelizumab (day 1, 22, 50) | I | Delay to surgery, ORR, pathologic response rate, TRAE | NCT05185531 | Active, not recruiting |
| Sintilimab | 30-54 Gy in 3-6 fractions | SBRT (1-2 weeks) then Sintilimab (200 mg every 3 weeks for up to 1 year) 4-6 weeks after completion of SBRT | I | 24 week PFS rate | NCT04167293 | Unknown |
| Durvalumab and Tremelimumab |
N/A | Sequential administration of TACE and SBRT followed by Immunotherapy | II | Downstaging for hepatectomy | NCT04988945 | Recruiting |
| Tislelizumab and regorafenib | 8 Gy × 3-5 fractions | Tislelizumab 200mg every 21 days, and regorafenib 120mg for the first 21 days of a 28-day cycle, concurrently with SBRT to all visible lesions | II | PFS | NCT05917431 | Recruiting |
| Pembrolizumab and lenvatinib | Five-fraction SBRT (week 4-week 5) | Pembrolizumab 200mg every 3 weeks and lenvatinib 12/8 mg/day for 96 weeks, plus SBRT to the portal vein thrombus and adjacent HCC | Ib/II | Safety rate, ORR |
NCT05286320 | Not yet recruiting |
| Adebrelimab and Lenvatinib | 33-48 Gy in 6 fractions over 2 weeks | SBRT followed by lenvatinib (12 mg/day) orally once daily in combination with adebrelimab 1200 mg every 3 weeks for up to 35 cycles. | II | PFS | NCT06261125 | Recruiting |
| Durvalumab and Tremelimumab | N/A | Arm I (hypofractionated RT, durvalumab) Arm II (hypofractionated RT, durvalumab, tremelimumab) |
II | ORR | NCT04430452 | Recruiting |
* Data was extracted from clinicaltrials.gov (Date: 22 July 2024).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



