
Submitted:
29 July 2024
Posted:
29 July 2024
You are already at the latest version
Abstract
Background: Liver failure profoundly affects the immune system, leading to dysregulation of innate and adaptive immune responses.
Body: This review explores the intricate relationship between liver function and immune homeostasis. The role of the liver as a central hub in immune response initiation is elucidated, emphasizing its involvement in hepatic inflammation induction and subsequent systemic inflammation. Cytokines, chemokines, growth factors, and lipid mediators orchestrate these immune processes, serving as both prognostic biomarkers and potential therapeutic targets in liver failure-associated immune dysregulation. Furthermore, the review delves into the mechanisms underlying immunosuppression in liver failure, encompassing alterations in innate immune cell functions such as neutrophils, macrophages, and natural killer cells (NK cells), as well as perturbations in adaptive immune responses mediated by B and T cells.
Conclusion: Understanding the immunological consequences of liver failure is crucial for developing targeted therapeutic interventions and improving patient outcomes in liver disease management.
Keywords:
Liver Cirrhosis
; Chronic Liver Failure
; Immune Response
; Cytokines
; Chemokines
; Immunosuppression
; Innate And Adaptive Immune Response
1. Introduction
Liver disease remains a prominent issue in the contemporary world. It is the eleventh-leading cause of death worldwide, accounting for over two million deaths annually. Among them, liver cancer is responsible for 1/3 to nearly 1/2 of them. Liver cirrhosis is the final manifestation of hepatic fibrosis caused by chronic inflammation. It results in replacing the healthy liver parenchyma with fibrotic tissue, formation of regenerative nodules, and alterations in vascular architecture. As recent studies show, those changes are, to a certain extent, reversible. Cirrhosis is associated with gastrointestinal system dysregulation, leading to impaired gut function and dysbiosis [1].
Nevertheless, the consequences of cirrhosis are local and systemic, affecting most organs and the immune system. The immune response is attenuated, inevitably resulting in immune deficiency. However, as the ability to combat pathological threats declines, the amount of pro-inflammatory cytokines causing systemic inflammation rises [2].
Acute chronic liver failure (ACLF) is a term used to describe a unique syndrome observed in patients with acutely decompensated chronic liver disease. Its occurrence relates to multiorgan dysfunction and unfavorable short-term survival [3]. There is no single recognized definition of ACLF. Significant associations and societies involved in the research of liver diseases have coined their criteria [4]. It leads to missed diagnoses and problems with incorporating proper treatment. However, most researchers agree that it is a severe form of decompensated liver cirrhosis and is associated with a systemic inflammatory response. ACLF is frequently precipitated by some intrahepatic conditions (alcoholic hepatitis, HBV reactivation), extrahepatic conditions (bacterial infection, gastrointestinal bleeding), or both [5]. The predominant precipitating factor exhibits local and definitional variability, although alcohol consumption emerges as the foremost cause.
The liver plays a crucial role in the proper functioning of the immune system. The proteins produced by the liver and the immune cells are essential to maintaining an appropriate response to foreign- and self-antigens. It is well known that liver failure might lead to both hyper- and hyporesponsiveness of the immune system. However, in this review, we would like to discuss the immune consequences of cirrhosis and ACLF and describe the most recent possible clinical markers and therapeutic targets.
2. Role of the Liver in Immune Response
The liver plays a highly significant role in the proper functioning of the immune system, being responsible for cytokine and acute phase reactant production. The hepatic artery supplies the liver with blood; however, it provides only a minor part of oxygen and nutrients to the organ. Most of the blood entering the liver comes from the portal vein. The blood flowing in it is rich in nutrients from the intestines; however, portal blood also contains pathogens and microbe-derived molecules that have passed through the intestinal epithelium [6]. Thus, the liver must develop immune tolerance in the face of harmless substances, while providing immunosurveillance and neutralizing pathogens and the harmful molecules they secrete. This immune system surveillance is facilitated by multiple cell lines unique to the liver and a distinct proportion of residual lymphocytes.
Kupffer cells (KC) are the most abundant macrophage population residing in the liver. They are immobilized in sinusoidal lumens, constantly investigating the flowing blood in search of threatening pathogens [7]. However, the cells are not only involved in bacterial endocytosis but their role in regulating the number of neutrophils has also been documented. Liver sinusoidal endothelial cells (LSEC) contribute with KCs and intrahepatic myeloid cells in the regulation of T lymphocytes. T cells remain suppressed in normal circumstances, avoiding the excess inflammatory response. This state is achieved by constantly producing anti-inflammatory cytokines such as Il-10, low MHC II content on antigen-presenting cells, and low levels of costimulatory molecules [8].
The liver is home to most of the Invariant killer T cells (iNKT) that respond to lipid antigens from both the external and internal environment. They do not require costimulation from other cells and can solely rely on TCR interaction with antigens [9].
3. The Initiation of Hepatic Inflammation
Pathogen-associated molecular patterns (PAMPs) and danger-associated molecular patterns (DAMPs) are substances from microorganisms and damaged cells. They are recognized by pattern recognition receptors (PRRs), e.g., toll-like receptors (TLRs) or NOD-like receptors (NLRs). In cirrhosis, gut membrane permeability significantly increases, allowing for increased bacterial transcytosis. Due to bacterial overgrowth and dysbiosis, the influx of PAMPs into the intestines' lymphoid tissue is increased. In addition, microbes permeate blood vessels entering the systemic circulation, triggering low-grade inflammation. Furthermore, DAMPs are constantly released from the damaged hepatocytes, intensifying systemic inflammation [10].
4. Systemic Inflammation
In the course of liver disease, there is both an intense systemic inflammatory response and immunosuppression (Figure 1). It has been shown that the systemic inflammatory response is the most crucial cause leading to sudden deterioration in patients who already have chronic liver disease. In the initial stage of ACFL development, pathogens strongly stimulate the immune system and consequent activation, recruitment, and differentiation of effector immune cells. Macrophages play a vital role at this stage. Their population can be divided into M1 macrophages, which participate in antigen presentation and secrete mainly pro-inflammatory cytokines and reactive oxygen species, and M2 macrophages, which secrete mainly anti-inflammatory cytokines [11]. M1 and M2 macrophages will be activated in the early stages of ACLF development. Activation of macrophages (Kupffer cells) present in the liver leads to the recruitment of innate effector cells and liver damage. Circulating monocytes in the blood will also play an important role, as they will infiltrate the liver. As a result of their proliferation, local liver damage can occur, which will induce the secretion of pro-inflammatory cytokines. The expression of progressive inflammation is the increasing secretion of inflammatory mediators, which we can divide into protein mediators (such as cytokines, chemokines, or growth factors) and lipid mediators [12]. Numerous studies have shown that the secretion of inflammatory mediators is directly related to patients' clinical status and mortality [13]. Moreover, some of these mediators may become therapeutic targets in the future.
Figure 1.
During liver disease, the immune system's function becomes severely impaired, leading to hyperresponsiveness.
Figure 1.
During liver disease, the immune system's function becomes severely impaired, leading to hyperresponsiveness.
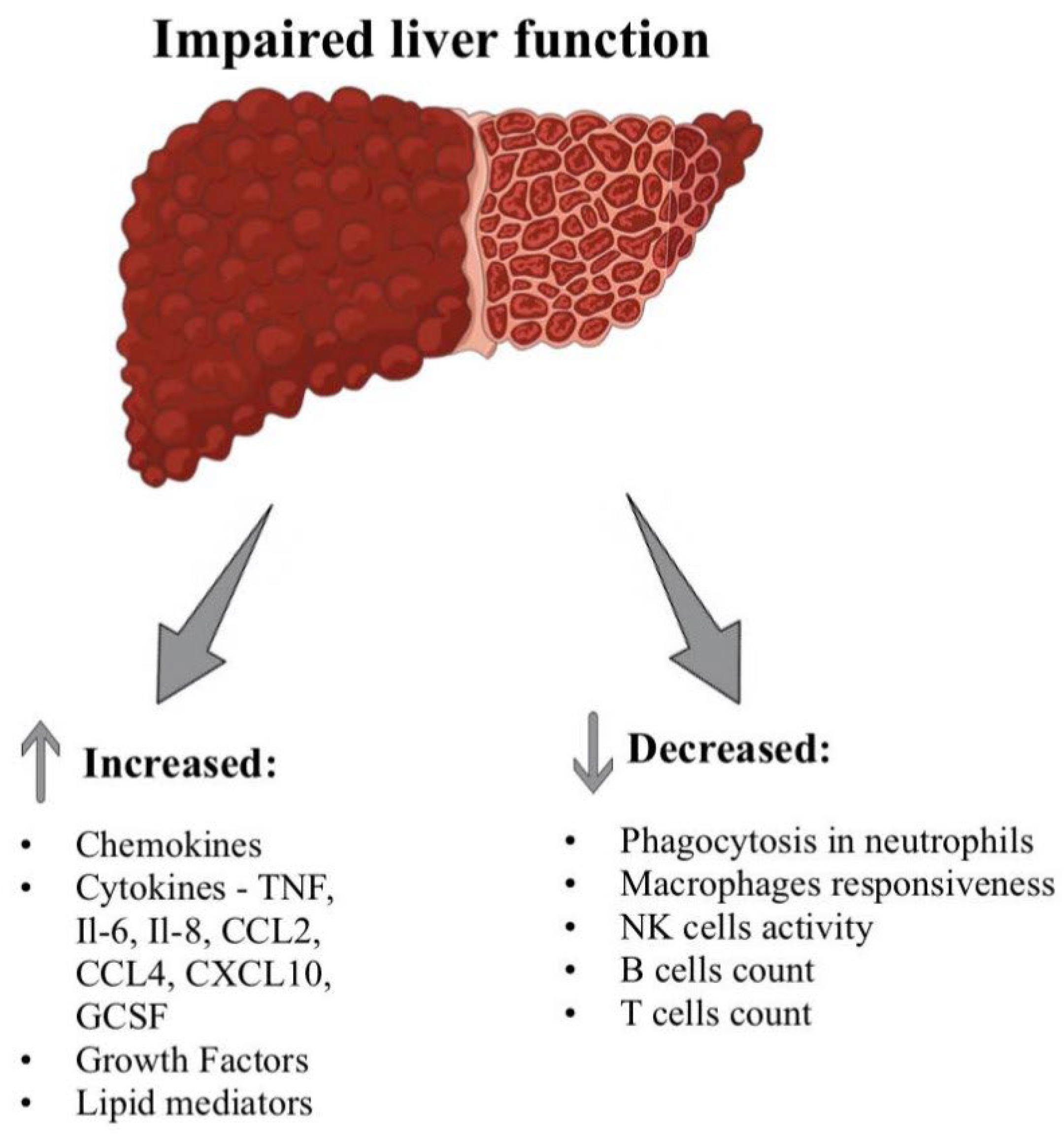

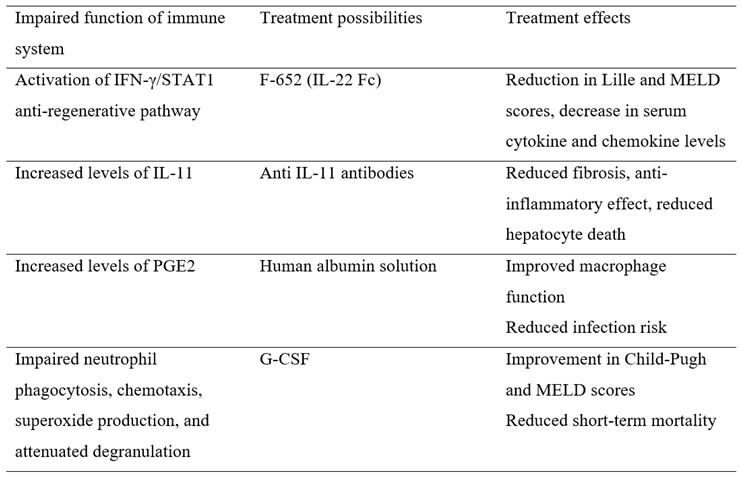
Table 1.
Treatment possibilities address various immunological dysfunctions.
5. Mediators of Inflammation
5.1. Cytokines
Cytokines are proteins that are critical mediators of inflammation. They are responsible for regulating and determining the nature of the immune response. Depending on which combinations of cytokines are produced depends on whether an immune response develops and whether it is cytotoxic, humoral, cellular, or allergic. Once released from immune cells, they bind to specific receptors and initiate a signaling cascade, developing an immune response [14,15]. Cytokines can be divided into pro-inflammatory cytokines, which include TNF-α, IL-1β, and IL-6, and anti-inflammatory cytokines, which include IL-10 and IL-4. Both anti-inflammatory and pro-inflammatory cytokines are involved in developing liver conditions, such as decompensated cirrhosis and ACLF [12]. IL-1β and TNF-α, produced in response to infection and tissue damage, stimulate TLR4 and thereby lead to the induction of IL-6 secretion. This pleiotropic cytokine is an important stimulator of acute-phase protein secretion [16]. A study using a mouse model combined with an ethanol-feeding model showed that the acute inflammatory response associated with IL-6 can lead to a transition from stable chronic inflammation to progressive liver damage [17].
Moreover, the TNF-α signaling pathway may contribute to the induction of hepatocyte apoptosis in ACLF. Moreover, despite the elevation of IL-10 levels, a marked imbalance in favor of pro-inflammatory cytokines was still observed [18]. Baseline levels of inflammatory markers measured in the plasma of patients on admission were slightly elevated in compensated cirrhosis, significantly increased in uncompensated cirrhosis, and were highest in ACLF patients who had "full-blown" systemic inflammation. Compared to controls, patients with uncompensated cirrhosis had elevated levels of inflammatory and anti-inflammatory cytokines, including IL-6, IL-7, IL-8, IL-10, IL-12, and TNF-α. However, patients who developed ACLF showed an opposite pattern of cytokines and decreased levels of IL-7, IL-10, IL-12, TNF-α, MCP-1, and IFN-γ while maintaining levels of IL-6 and IL-8 [19]. Another group also observed an increase in most types of cytokines and chemokines in patients with acute uncompensated cirrhosis, with a significant increase in cytokines in patients with ACLF relative to patients without ACLF involving only those involved in the innate immune response. The secretion of inflammatory mediators in ACLF is so massive that we can use the phrase "cytokine storm" in its context. The secretion of numerous cytokines, similar to that in ACLF, occurs during sepsis and every form of COVID-19 infection [20,21].
5.1.1. Cytokines as Prognostic Biomarkers
Cytokine levels correlate with clinical status and patient mortality, making cytokines good candidates to be prognostic biomarkers. A study of 412 patients with hepatitis B virus-related acute-on-chronic liver failure (HBV-ACLF) showed a positive correlation between high serum IL-6 levels and prognosis. In a retrospective analysis, the predictive value of IL-6 levels on 90-day mortality in patients with ACLF was similar to that of MELD (Model of End-Stage Liver Disease) or Meld-Na. It was higher than CRP and serum leukocyte levels [22]. Moreover, IL-6 has recently been shown to be an independent risk factor for death after 28, 90, and 180 days in patients with liver failure [23]. Moreover, the predictive value of serum IL-6 concentration in the development of overt hepatic encephalopathy within 180 days was higher than the efficacy of MELD, especially for patients who had not previously developed overt hepatic encephalopathy [24]. In contrast, a study of patients with esophageal variceal bleeding showed an association between the incidence of infection and death in these patients and levels of high mobility protein group 1 (HMG1) and IL-6. Also, patients with clinically significant portal hypertension (≥ 10 mmHg) had elevated serum levels of IL-6 and IL-18. More recently, IL-6, IL-22, interferon-α2, soluble TNF receptor 1, lipocalin-2, and α-fetoprotein have been linked to mortality within 28 days in patients with severe alcoholic hepatitis, and IL-6, IL-13, and endotoxin levels to mortality within 90 days. Moreover, a parameter composed of IL-13 levels and age was better at predicting 90-day mortality in patients with AH than MELD [25]. Low levels of stem cell factor (SCF), low levels of basic fibroblast growth factor (bFGF), and high levels of IL-13 have also been shown to correlate with an increased risk of ACLF [26].
5.1.2. Cytokines as Potential Therapeutic Targets
Due to the high mortality rate among patients who develop ACFL and the lack of effective therapy, new therapies, including those based on interference with cytokine signaling, are being sought all the time. Based on a model of severe liver impairment, impaired liver regeneration processes have been shown to result from a shift in activation of the IL-6/STAT3 pro-regenerative pathway to the IFN-γ/STAT1 anti-regenerative pathway, which in turn was related to the inability of Kupffer cells to produce IL-6. Therapy with IL-22Fc reversed this switch in mice and may have therapeutic potential in humans in the future as well [27,28]. Recently, a phase II study was conducted evaluating the therapeutic potential of F-652, a type of IL-22Fc, in the treatment of patients with alcohol-associated hepatitis. F-652 has been shown to improve patients' prognosis, as demonstrated by a reduction in Lille and MELD scores and a decrease in serum cytokine and chemokine levels [29]. Manipulating the signaling of other cytokines, such as IL-6 and IL-11, may also be an important therapeutic option for treating ACLF in the future. However, for now, there are many obstacles in the way. For example, IL-11 has also been shown to have pro-inflammatory and anti-regenerative effects [30,31]. It has been observed that therapy with antibodies that block IL-11 signaling leads to reduced fibrosis, has anti-inflammatory effects, and reduces hepatocyte death in mice with diet-induced steatohepatitis [32] (Figure 2). The use of anti-IL11 therapy is being considered in many diseases, including the treatment of acute and chronic kidney disease [33].
5.2. Chemokines
Chemokines (chemotactic cytokines) are a family of small and soluble proteins that act as signaling molecules and function by binding to G-Protein Coupled Receptors (GPCRs) on the cell surface [34]. They play a crucial role in immune system homeostasis and participate in developing immune and inflammatory responses by stimulating leukocyte migration [35]. Due to differences in the number and position of the N-terminal cysteine residues, chemokines can be divided into 4 subfamilies: the CXC group, the CX3C group (CX3CL1 or fractalkine), the (X)C group, and the CC group [36]. The increased secretion of chemokines such as CXCL10, CCL2, CCL4, and IL-8 have been observed in both cirrhosis decompensation and ACFL [18,19]. IL-8 is secreted by hepatocytes, stellate cells, and Kupffer cells, among others, and its levels are associated with the prognosis of patients with ACLF [37]. The gene encoding IL-8 is activated in response to IL-1 and TNFα due to the synergistic action of NF-κB in combination with AP-1 or C/EBP [38]. Recently, it has also been suggested that high levels of IL-1β in the serum of ACLF patients may promote IL-8 expression in human umbilical cord mesenchymal stem cells (hUC-MSCs) via the NF-κB signaling pathway, thereby reducing the therapeutic effect of hUC-MSCs on ACLF [39]. It has also been reported that IL-8 can induce the conversion of mature hepatocytes toward a cholangiocyte phenotype [40]. Retrospective analysis showed that IL-8 may be an independent predictor of 28-day mortality in ACLF-HBV patients but not mortality at 90 and 180 days [41]. More recently, CXCL2, IL-8, total bilirubin, and age were isolated as independent risk factors for poor prognosis in HBV-ACLF patients, and an immunological prognostic model was developed based on them, which had a higher prognostic value than Chronic Liver Failure Consortium (CLIF-C) ACLF, MELD and MELD-Na [42]. In another study, HBV-ACLF patients had statistically significantly higher serum CXCL1 levels compared to healthy subjects, patients with chronic HBV infection, and patients with HBV-compensated cirrhosis [43]. Studies using a mouse model of ACLF have shown that CXCL1 is involved in the mobilization of ACLF neutrophils, and its knockdown leads to reduced neutrophil infiltration, the release of fewer reactive oxygen species, and inhibition of hepatocyte apoptosis, resulting in reduced liver damage and inflammation [44]. Further studies are needed to determine whether CXCL1 can become a prognostic marker and therapeutic target [43]. Elevated IL-8, CXCL9, and CXCL10 levels were associated with shorter survival of cirrhotic patients undergoing transjugular intrahepatic portal-systemic shunt (TIPS). Moreover, CXCL10 has also been linked to the incidence and mortality of ACLF [45,46,47]. Miao Huang et al. recently identified C-C motif chemokine ligand 5 (CCL5) as an essential factor leading to reduced liver regenerative capacity. CCL5 induced the transition of macrophages into a pro-inflammatory phenotype via the forkhead box O (FoxO) 3a pathway, which led to reduced hepatocyte growth factor (HGF) production. CCL5 may be a promising therapeutic target for the treatment of posthepatectomy liver failure (PHLF) [48].
5.3. Growth Factors
In addition to cytokines and chemokines, granulocyte-macrophage colony-stimulating factor (GM-CSF) and granulocyte colony-stimulating factor (G-CSF) were abundant in the serum of ACLF patients [18]. They are crucial for differentiating and activating monocytes and neutrophils [49]. In the liver, they induce progenitor cell proliferation [50]. In the case of ACLF, it was reported that G-CSF administration was associated with improved patient survival, which was most likely related to restoration of immune function and reduced risk of infection [51]. Based on ACLF models, it has been shown that the use of G-CSF and a TLR4 inhibitor leads to the inhibition of inflammation, promotes liver regeneration, and may reduce mortality in ACLF [52]. The transforming growth factor β1/interleukin-31 (TGF-β1/IL-31) pathway has also been shown to correlate with the degree of liver damage and the worse prognosis of patients with ACLF [53]. High fibroblast growth factor 21 (FGF21) levels were observed in cirrhotic patients admitted to the intensive care unit. Moreover, it was higher in patients with ACLF but did not correlate with the severity of the course of ACLF [54].
5.4. Lipid Mediators
Lipid mediators are biologically active lipids that mainly affect numerous cellular processes by binding to G-protein-coupled receptors [55]. In the course of liver diseases, there is an imbalance in the secretion of lipid mediators, including a disruption between pro-inflammatory and anti-inflammatory mediators [56]. Analyzing the plasma of 200 patients with decompensated cirrhosis with or without ACFL for as many as 100 lipid mediators, 16 lipid mediators associated with the patient's condition were identified. Moreover, levels of Leukotriene E4 (LTE4) and 12-Hydroxyheptadecatrienoic acid (12-HHT) distinguished patients with ACLF from those without ACLF. In addition, LTE4 levels were associated with inflammatory markers, non-apoptotic cell death, and short-term patient mortality [57]. LTE4, like other leukotrienes, is a known mediator of the inflammatory response [58]. Moreover, analysis of albumin-associated lipid mediators showed that patients with acute uncompensated cirrhosis at risk of disease progression to ACFL have low levels of anti-inflammatory lipid mediators. Prostaglandin (PG) E2 was absent from the albumin of patients with acute uncompensated cirrhosis, suggesting that it is mainly present in this group of patients in a form separated from albumin [59]. We were also able to link the survival of patients with ACLF to changes in the profile of levels of pro-secretory lipid mediators [60]. Previous studies have also reported that PGE2 is associated with immune deficits in patients with acute decompensated cirrhosis, although the literature data on the subject are divergent [57,61]. PGE2 levels were higher in HBV-ACLF patients than in healthy controls and patients with stable viral hepatitis. Moreover, it was shown that increased serum PGE2 levels were associated with a higher risk of infection in patients with ACLF [62]. Moreover, reduced prostaglandin E receptor 2 (EP2) expression on CD8+ T cells was observed in HBV-ACLF patients. Altered PGE2-EP2 was associated with excessive inflammation and stimulation of cells of the acquired immune system in response to LPS and Escherichia coli infection [63]. Albumin infusions have also been shown to promote the reversal of immune dysfunction by binding and inactivating PGE2 [64]. Besides, increased PGE2 levels in patients with acute uncompensated cirrhosis who received albumin may be associated with a higher risk of inflammation during the first few days after hospitalization [60]. On the other hand, based on a mouse model, it was also shown that PGE2 secreted by MSCs showed therapeutic potential in treating acute liver failure. PGE2 blocked TGF-β-activated kinase 1 and activated the NLRP3 inflammasome in liver macrophages, reducing cytokine secretion. In addition, PGE2, through the STAT6 and mTOR pathway, induced the transition of macrophages to an anti-inflammatory (M2) form, contributing to reducing hepatocyte death and inflammation [65].
6. Immunosuppression
Liver failure leads to systemic inflammation and strongly affects immune responsiveness. Due to immune dysfunction, innate immune paralysis, disturbance in immune tolerance, and decreased innate and adaptive responses occur. Consequently, those patients develop immunosuppression, which might lead to opportunistic infections and lowered response to vaccinations. In this paper, we discussed changes in immune cell counts and cellular pathway pathologies.
6.1. Innate Immune Response
6.1.1. Neutrophils
The liver plays a crucial role in the innate immune response; thus, liver failure might significantly impact its responsiveness. It is well known since the 1970s that cirrhosis impairs neutrophil phagocytosis, chemotaxis, superoxide production, and attenuated degranulation responses [66,67,68,69]
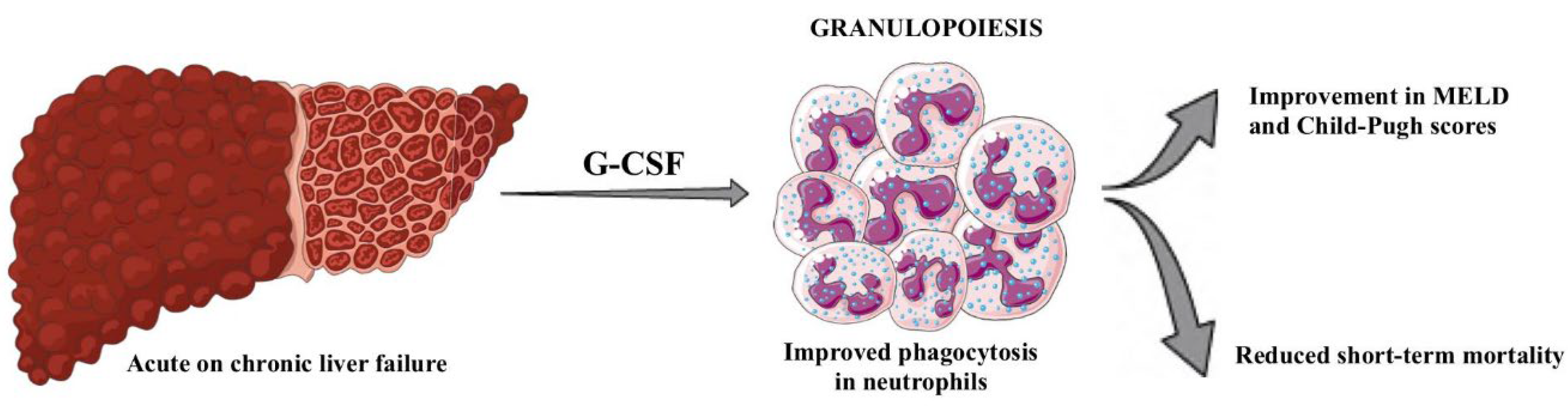
More importantly, correlations have been found between neutrophils in patients with ACLF and increased mortality [70]. There has also been a study comparing neutrophils from patients with cirrhosis to healthy controls, which has shown decreased expression of a neutrophil adhesion receptor CD62L and reduced transendothelial migration [71]. Exposure to G-CSF is proven not only to significantly improve phagocytic and bactericidal function in neutrophils from acute liver failure patients ex vivo but also might reduce short-term mortality in patients with ACLF [71,72,73]. Furthermore, metanalysis from 2023 carried out by Konstantis et al. has shown that the administration of G-CSF might lead to improvements in overall survival and liver function and prognosis, as evidenced by the improvement in the MELD score [74] (Figure 3). On the contrary, another study suggests that there are no clear conclusions regarding the usefulness of G-CSF in ACLF. However, survival benefits were observed in Asian patients [75].
6.1.2. Macrophages
It is crucial to note that as cirrhosis or ACLF progresses, immune responses become attenuated and are accompanied by macrophage hyporesponsiveness. There is evidence that the cyclooxygenase (COX)-derived eicosanoid prostaglandin E2 (PGE2) correlates with cirrhosis-associated immunosuppression. Elevated circulating concentrations of PGE2 were found in the plasma of patients with acute decompensation of cirrhosis [76]. Albumin, which reduces PGE2 bioavailability, was decreased in the serum of patients with acute decompensation and appears to have a role in modulating PGE2-mediated immune dysfunction. In vivo, administration of human albumin solution to these patients significantly improved the plasma-induced impairment of macrophage pro-inflammatory cytokine production in vitro. Consequently, it creates a therapeutic option - human albumin solution infusions may be used to reduce circulating PGE2 levels and thus reduce the risk of infection in patients with acutely decompensated cirrhosis [76,77,78].
What is more, several studies have reported increased expression of the inhibitory MERTK (Mer receptor tyrosine kinase), which regulates M2 macrophage polarization via the JAK1/STAT6 signaling pathway) by circulating monocytes from patients with ACLF, as compared with patients with stable cirrhosis and healthy controls [79]. Furthermore, upregulation of MERTK weakens the antigen presentation function and reduces the secretion of inflammatory cytokines [80]. Recently, a study on mice with ACLF detected changes in MERTK, JAK1/STAT6, inflammatory cytokines, and macrophage polarization markers in vitro and in vivo. Furthermore, treatment with mesenchymal stem cells improved liver function and 48-h survival of ACLF mice but also alleviated inflammatory injury by promoting M2 macrophage polarization and elevated MERKT expression levels in macrophages [81].
6.1.3. Natural Killer Cells (NK Cells)
Constituting as much as half of the resident lymphocyte population in a healthy liver, natural killer cells exhibit a significantly higher abundance than peripheral blood. Natural killer (NK) cells have cytotoxic and antitumor properties, enabling them to neutralize pathogens and impair the development of neoplasms [82]. Weiss et al. observed in their study a reduced proportion of memory lymphocytes and NK cells in the immune cell profile of patients with ACLF. The selective depletion of these cells emerged as a significant factor contributing to systemic immunosuppression [83]. In patients with cirrhosis, NK cell lytic activity is reduced by elevated levels of TGF-β in advanced liver disease in mouse models [84]. Another critical factor might be suppression of NKG2D, an inhibitory receptor on the NK cell, which is the likely mechanism by which their cytotoxic activity is reduced in chronic liver disease [85].
A different study has shown a possible role of NK cells in HBV-ACLF. Increased counts of CXCL-10 and NK cells were found in the liver, and excessive production of CXCL-10 in the peripheral blood contributed to the apoptosis of NK cells in vitro, as the influence of CXCL-10 and NK cells on each other might mediate the unbalanced distribution of NK cells. Moreover, the decrease in NK cells was associated with the level of HBV DNA and disease severity and had good prognostic performance in predicting the outcome of patients with HBV-ACLF through AUROC analysis [86].
6.2. Adaptive Immune Response
Acute-on-chronic liver failure (ACLF) occurs in patients who have an acute decompensation of cirrhosis, consequently leading to organ failures and an increased risk of in-hospital mortality. ACLF is connected with systemic inflammation, elevated blood leukocyte counts, increased plasma levels of C-reactive protein, and increased concentrations of cytokines and chemokines [87]. The white blood cell count is a component of the ACLF scoring system developed by the Chronic Liver Failure Consortium, providing an accurate prediction of early mortality in ACLF patients [88]. It has been proposed that in ACLF, peripheral leukocytosis is enriched with effector immune cells with a high potential for inducing tissue damage [89].
6.2.1. B Cells
Cirrhosis affects the innate immune response and causes dysregulation of the adaptive immune response. Studies have proven decreased numbers of B cells, including the CD5+ subset, among patients with alcoholic liver disease [90]. Weiss E. et al. conducted a study using results of clinical complete blood count measurements and microarray (genomewide) analysis of blood RNA expression in HS and 3 groups of patients with cirrhosis, comprising AC, AD, and ACLF. The key results showed that patients with ACLF had leukocytosis fueled by increased populations of neutrophils (that had unique phenotype) and macrophages M0-like monocytes, and as expected, which will be described later in this paper, decreased lymphocyte count related to a depletion in memory lymphocytes (of the B-cell, CD4 T-cell lineages), CD8 T cells and NK cells [83].
Another study demonstrated loss of CD27+ memory B cells, impaired function, impaired IgG production, and reduced allostimulatory capabilities. Hiroyoshi D. et al. have found out, that among patients with chronic hepatitis C, only those that have progressed to cirrhosis display a loss of CD27+ memory B-cells with associated functional abnormalities, such as impaired activation, impaired TNFβ and IgG production and impaired allostimulatory capacity. However, overall immunoglobulin levels are elevated in cirrhotics due to increased levels of pathogen-specific immunoglobulins such as antibodies against Saccharomyces cerevisiae (ASCA) and against Galα1–3Galβ1–3GlcNAc (alpha-Gal) [91]. This study has shown that cirrhosis is associated with profound reductions of CD27+IgM+ B-cells, a subset of memory B-cells thought to be generated in response to T-independent antigens [92]. Dysfunctional B-cell activation in cirrhosis resulting from hepatitis C infection associated with the disappearance of CD27-positive B-cell population.
Furthermore, another study has proven that alcoholics admitted for acute alcoholic liver disease (ALD) had decreased CD5+ count. In addition to the loss of CD5+ B cells, there was a reduction in the percentage of B cells which were CD5−CD45RAhi. This subset appears phenotypically similar to the IgM-producing CD5−CD45RAlo subset and thus may be enriched for autoantibody-producing cells [93].
Liver cirrhosis might also influence the efficacy of the hepatitis B vaccination, as shown in numerous studies. Hassnine A. et al. carried out a retrospective observational clinical study on 500 individuals (400 chronic HCV patients and 100 healthy controls), who were divided into 5 groups: A (control group), B (cirrhotic patient not receiving treatment), C (chronic hepatitis patients receiving treatment), D (cirrhotic patients receiving treatment), and E (HCC patients receiving treatment). HCV infection and its complications, such as cirrhosis, are one of the main risk factors for vaccine hypo-responsiveness, as they found a significantly lower response to HBV vaccination in HCV-infected individuals, with an overall response rate of 80% and on multivariate analyses that included age, gender, cirrhosis, alcohol abuse, and Diabetes Mellitus (DM), only patients with liver cirrhosis were less likely to be reactive [94]. Another study from 2020 retrospectively evaluated all patients with chronic HCV infection at Hennepin County Medical Center in Minneapolis, Minnesota, between 2002 and 2018. They have noticed a significantly lower response to HBV vaccination in HCV-infected individuals, with an overall response rate of 79% and a response rate of 50% when the cohort of those who received 3 or more vaccine doses was assessed, compared to the response rate 90–98% among the healthy population [95].
6.2.2. T Cells
The activity of T cell populations during liver disease is influenced by various factors, including the extent of gut translocation of microbes, the activation of antigen-presenting cells (APCs), and the proliferative capacity of T lymphocytes, which tends to decrease with the progression of cirrhosis [96].
A recent study involving ACLF patients revealed a significant increase in mononuclear myeloid-derived suppressor cells. This expansion reduced T cell proliferation and heightened vulnerability to bacterial infections [97].
Furthermore, an increase in T regulatory cells might be connected with poorer short-term survival in ACLF patients with hepatitis B, which might be used as a therapeutic target in the long term. The restoration of a balanced TReg to Th17 ratio seems crucial for improved outcomes, and as a consequence, it likely signifies a proper return to immune homeostasis [98].
One of the most recent studies indicates lower expression of HLA-DR, CD86, and CD54 on monocyte-derived dendritic cells in ACLF patients compared to chronic hepatitis B patients and healthy controls. This may relate to higher levels of procalcitonin (PCT), lower levels of albumin, and decreased prothrombin activity. These patients' T cells also showed lower Ki-67 and interferon-gamma (IFN-γ) production [99].
7. Conclusions
It is well known that the liver plays a crucial role in the proper functioning of the immune system, as it creates immune tolerance and neutralizes pathogens and their metabolites. The development of liver conditions, including decompensated cirrhosis and ACLF, involves both anti-inflammatory and pro-inflammatory cytokines. Moreover, ACLF patients exhibit a predominance of pro-inflammatory cytokines, including TNFα and IL-6, along with chemokines, such as IL-8, MCP-1, IP-10, and MIP-1β. The extensive secretion of inflammatory mediators in ACLF is often called a "cytokine storm." Moreover, cytokines might be used as prognostic markers and potential therapeutic targets.
Regarding the studies, Il-6 is an independent risk factor for death after 28, 90, and 180 days in patients with liver failure [23]. A recent phase II study investigated the therapeutic efficacy of F-652, an IL-22Fc variant, in patients with alcohol-associated hepatitis. While exploring the manipulation of signaling pathways involving other cytokines like IL-6 and IL-11 holds promise as potential therapeutic avenues for future ACLF, further research is essential [100].
As versatile signaling molecules, chemokines significantly influence immune responses and inflammatory processes by regulating leukocyte migration through interaction with G-Protein Coupled Receptors. CXCL2, IL-8, total bilirubin, and age can be independent prognostic factors in HBV-ACLF patients.
Another potential therapeutic method is exposure to the G-CSF, which has been shown to improve overall survival and liver function, as evidenced by the improvement in the MELD score [74]. Macrophages also become impaired in the ACLF patients.
Immunosuppression is a significant clinical problem in patients with liver failure. The increased CXCL-10 levels promote NK cell apoptosis, which contributes to systemic immunosuppression, and the IgG production and costimulatory functions of CD27 memory B cells are impaired in cirrhosis. In addition, the increase in regulatory T cells is probably linked to worse outcomes in HBV patients. On the other hand, reduced T cell proliferation evoked by myeloid-derived suppressor cells causes patients to be more prone to develop life-threatening infections. This paper discussed the most critical aspects of the immune system in liver failure. However, further research is still needed, as liver diseases are a significant problem in society, and studies over possible markers and therapeutic targets might improve the mortality rate and quality of life of those patients.
List of abbreviations:
ACLF – Acute chronic liver failure
ALD – alcoholic liver disease
APCs – antigen-presenting cells
bFGF – basic fibroblast growth factor
CCL5 – C-C motif chemokine ligand 5
CLIF-C – Chronic Liver Failure Consortium
COX – cyclooxygenase
DAMPs – danger-associated molecular patterns
EP2 – prostaglandin E receptor 2
FGF21 – fibroblast growth factor 21
FoxO – forkhead box O
G-CSF – granulocyte colony-stimulating factor
GM-CSF – granulocyte-macrophage colony-stimulating factor
GPCRs – G-Protein Coupled Receptors
HBV-ACLF – hepatitis B virus-related acute-on-chronic liver failure
HMG1 – high mobility protein group 1
IFN-γ – interferon-gamma
iNKT – Invariant killer T cells
KC – Kupffer cells
LTE4 – Leukotriene E 4
LSEC – Liver sinusoidal endothelial cells
MELD – Model of End-Stage Liver Disease
MERTK – Mer receptor tyrosine kinase
NK – Natural killer
NLRs – NOD-like receptors
PAMPs – Pathogen-associated molecular patterns
PG – Prostaglandin
PGE2 – derived eicosanoid prostaglandin E2
PHLF – posthepatectomy liver failure
PRRs – pattern recognition receptors
SCF – stem cell factor
TLRs – toll-like receptors
TIPS – transjugular intrahepatic portal-systemic shunt
TGF-β1/IL-31 – transforming growth factor β1/interleukin-31
12-HHT – 12-Hydroxyheptadecatrienoic acid
Author Contributions
Conceptualization, N.R.; investigation, A.D., B.W. and J.M.; writing—original draft preparation, A.D., B.W. and J.M.; writing—review and editing, N.R., J.K. and A.S.; visualization, A.D., B.W. and J.M.; supervision, N.R.; project administration, A.S.; funding acquisition, N.R. All authors have read and agreed to the published version of the manuscript.
Funding
The Students’ Research Group of Cancer Cell Biology of the Department of Molecular and Cell Biology of the Wroclaw Medical University, SKN No. 148, and the Subsidy from the Department of Molecular and Cell Biology SUBZ.D260.24.076.
Institutional Review Board Statement
Not Applicable
Informed Consent Statement
Not Applicable
Data Availability Statement
No new data were created or analyzed in this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kalaitzakis, E. Gastrointestinal dysfunction in liver cirrhosis. World J. Gastroenterol. 2014, 20, 14686–95. [Google Scholar] [CrossRef] [PubMed]
- Noor, M.T.; Manoria, P. Immune Dysfunction in Cirrhosis. J. Clin. Transl. Hepatol. 2017, XX, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Hernaez, R.; Kramer, J.R.; Liu, Y.; Tansel, A.; Natarajan, Y.; Hussain, K.B.; Ginès, P.; Solà, E.; Moreau, R.; Gerbes, A.; et al. Prevalence and short-term mortality of acute-on-chronic liver failure: A national cohort study from the USA. J. Hepatol. 2018, 70, 639–647. [Google Scholar] [CrossRef] [PubMed]
- Leão, G.S.; Lunardi, F.L.; Picon, R.V.; Tovo, C.V.; de Mattos, A.A. Acute-on-chronic liver failure: A comparison of three different diagnostic criteria. Ann. Hepatol. 2019, 18, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Sarin, S.K.; Choudhury, A. Acute-on-chronic liver failure: terminology, mechanisms and management. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 131–149. [Google Scholar] [CrossRef] [PubMed]
- Brandl, K.; Kumar, V.; Eckmann, L. MINI-REVIEW Microbiome and Host Interactions Gut-liver axis at the frontier of host-microbial interactions. Am J Physiol Gastrointest Liver Physiol 2017. [Google Scholar] [CrossRef] [PubMed]
- Bilzer, M.; Roggel, F.; Gerbes, A.L. Role of Kupffer cells in host defense and liver disease. Liver Int. 2006, 26, 1175–1186. [Google Scholar] [CrossRef] [PubMed]
- Sana, G.; Lombard, C.; Vosters, O.; Jazouli, N.; Andre, F.; Stephenne, X.; Smets, F.; Najimi, M.; Sokal, E.M. Adult Human Hepatocytes Promote CD4+ T-Cell Hyporesponsiveness Via Interleukin-10-Producing Allogeneic Dendritic Cells. Cell Transplant. 2014, 23, 1127–1142. [Google Scholar] [CrossRef] [PubMed]
- Gu, X.; Chu, Q.; Ma, X.; Wang, J.; Chen, C.; Guan, J.; Ren, Y.; Wu, S.; Zhu, H. New insights into iNKT cells and their roles in liver diseases. Front. Immunol. 2022, 13, 1035950. [Google Scholar] [CrossRef]
- Martin-Mateos, R.; Alvarez-Mon, M.; Albillos, A. Dysfunctional Immune Response in Acute-on-Chronic Liver Failure: It Takes Two to Tango. Front. Immunol. 2019, 10, 973. [Google Scholar] [CrossRef]
- Yunna, C.; Mengru, H.; Lei, W.; Weidong, C. Macrophage M1/M2 polarization. Eur. J. Pharmacol. 2020, 877, 173090. [Google Scholar] [CrossRef] [PubMed]
- Clària, J.; Arroyo, V.; Moreau, R. Roles of systemic inflammatory and metabolic responses in the pathophysiology of acute-on-chronic liver failure. JHEP Rep. 2023, 5, 100807. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Hu, J.; Gou, C.; Jin, H.; Zhang, C.; Liu, Y.; Wang, Y.; Wang, X. Serum Interleukins as Potential Prognostic Biomarkers in HBV-Related Acute-on-Chronic Liver Failure. Mediat. Inflamm. 2022, 2022, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Dinarello, C.A.; Molgora, M.; Garlanda, C. Interleukin-1 and Related Cytokines in the Regulation of Inflammation and Immunity. Immunity 2019, 50, 778–795. [Google Scholar] [CrossRef] [PubMed]
- Clària, J.; Arroyo, V.; Moreau, R. The Acute-on-Chronic Liver Failure Syndrome, or When the Innate Immune System Goes Astray. J. Immunol. 2016, 197, 3755–3761. [Google Scholar] [CrossRef] [PubMed]
- Hirano, T. IL-6 in inflammation, autoimmunity and cancer. Int. Immunol. 2020, 33, 127–148. [Google Scholar] [CrossRef] [PubMed]
- Karatayli, E.; Hall, R.A.; Weber, S.N.; Dooley, S.; Lammert, F. Effect of alcohol on the interleukin 6-mediated inflammatory response in a new mouse model of acute-on-chronic liver injury. Biochim. et Biophys. Acta (BBA) - Mol. Basis Dis. 2018, 1865, 298–307. [Google Scholar] [CrossRef]
- Clària, J.; Stauber, R.E.; Coenraad, M.J.; Moreau, R.; Jalan, R.; Pavesi, M.; Amorós. ; Titos, E.; Alcaraz-Quiles, J.; Oettl, K.; et al. Systemic inflammation in decompensated cirrhosis: Characterization and role in acute-on-chronic liver failure. Hepatology 2016, 64, 1249–1264. [Google Scholar] [CrossRef]
- Dirchwolf, M.; Podhorzer, A.; Marino, M.; Shulman, C.; Cartier, M.; Zunino, M.; Paz, S.; Muñoz, A.; Bocassi, A.; Gimenez, J.; et al. Immune dysfunction in cirrhosis: Distinct cytokines phenotypes according to cirrhosis severity. Cytokine 2015, 77, 14–25. [Google Scholar] [CrossRef]
- Zanza, C.; Romenskaya, T.; Manetti, A.C.; Franceschi, F.; La Russa, R.; Bertozzi, G.; Maiese, A.; Savioli, G.; Volonnino, G.; Longhitano, Y. Cytokine Storm in COVID-19: Immunopathogenesis and Therapy. Medicina 2022, 58, 144. [Google Scholar] [CrossRef]
- Cron, R.Q.; Goyal, G.; Chatham, W.W. Cytokine Storm Syndrome. Annu. Rev. Med. 2023, 74, 321–337. [Google Scholar] [CrossRef]
- Remmler, J.; Schneider, C.; Treuner-Kaueroff, T.; Bartels, M.; Seehofer, D.; Scholz, M.; Berg, T.; Kaiser, T. Increased Level of Interleukin 6 Associates With Increased 90-Day and 1-Year Mortality in Patients With End-Stage Liver Disease. Clin. Gastroenterol. Hepatol. 2018, 16, 730–737. [Google Scholar] [CrossRef] [PubMed]
- Xiao, N.; Liu, L.; Zhang, Y.; Nie, Y.; Zhu, X. A practical nomogram based on serum interleukin-6 for the prognosis of liver failure. Front. Med. 2022, 9, 1035699. [Google Scholar] [CrossRef]
- Labenz, C.; Toenges, G.; Huber, Y.; Nagel, M.; Marquardt, J.U.; Schattenberg, J.M.; Galle, P.R.; Labenz, J.; Wörns, M. Raised serum Interleukin-6 identifies patients with liver cirrhosis at high risk for overt hepatic encephalopathy. Aliment. Pharmacol. Ther. 2019, 50, 1112–1119. [Google Scholar] [CrossRef]
- Tornai, D.; Mitchell, M.; McClain, C.J.; Dasarathy, S.; McCullough, A.; Radaeva, S.; Kroll-Desrosiers, A.; Lee, J.; Barton, B.; Szabo, G. A novel score of IL-13 and age predicts 90-day mortality in severe alcohol-associated hepatitis: A multicenter plasma biomarker analysis. Hepatol. Commun. 2023, 7. [Google Scholar] [CrossRef]
- Wang, S.; Zhu, H.; Pan, L.; Zhang, M.; Wan, X.; Xu, H.; Hua, R.; Zhu, M.; Gao, P. Systemic inflammatory regulators and risk of acute-on-chronic liver failure: A bidirectional mendelian-randomization study. Front. Cell Dev. Biol. 2023, 11, 1125233. [Google Scholar] [CrossRef]
- Xiang, X.; Feng, D.; Hwang, S.; Ren, T.; Wang, X.; Trojnar, E.; Matyas, C.; Mo, R.; Shang, D.; He, Y.; et al. Interleukin-22 ameliorates acute-on-chronic liver failure by reprogramming impaired regeneration pathways in mice. J. Hepatol. 2019, 72, 736–745. [Google Scholar] [CrossRef]
- Hwang, S.; Hicks, A.; Hoo, C.Z.; Kwon, Y.S.; Cho, Y.E.; Moore, J.; Gao, B. Novel treatment of acute and acute-on-chronic liver failure: Interleukin-22. Liver Int. 2023. [Google Scholar] [CrossRef] [PubMed]
- Arab, J.P.; Sehrawat, T.S.; Simonetto, D.A.; Verma, V.K.; Feng, D.; Tang, T.; Dreyer, K.; Yan, X.; Daley, W.L.; Sanyal, A.; et al. An Open-Label, Dose-Escalation Study to Assess the Safety and Efficacy of IL-22 Agonist F-652 in Patients With Alcohol-associated Hepatitis. Hepatology 2020, 72, 441–453. [Google Scholar] [CrossRef]
- Cook, S.A. The Pathobiology of Interleukin 11 in Mammalian Disease is Likely Explained by its Essential Evolutionary Role for Fin Regeneration. J. Cardiovasc. Transl. Res. 2023, 16, 755–757. [Google Scholar] [CrossRef]
- Ng, B.; Xie, C.; Su, L.; Kuthubudeen, F.F.; Kwek, X.-Y.; Yeong, D.; Pua, C.J.; Cook, S.A.; Lim, W.-W. IL11 (Interleukin-11) Causes Emphysematous Lung Disease in a Mouse Model of Marfan Syndrome. Arter. Thromb. Vasc. Biol. 2023, 43, 739–754. [Google Scholar] [CrossRef] [PubMed]
- Widjaja, A.A.; Singh, B.K.; Adami, E.; Viswanathan, S.; Dong, J.; D’agostino, G.A.; Ng, B.; Lim, W.W.; Tan, J.; Paleja, B.S.; et al. Inhibiting Interleukin 11 Signaling Reduces Hepatocyte Death and Liver Fibrosis, Inflammation, and Steatosis in Mouse Models of Nonalcoholic Steatohepatitis. Gastroenterology 2019, 157, 777–792. [Google Scholar] [CrossRef]
- Widjaja, A.A.; Viswanathan, S.; Shekeran, S.G.; Adami, E.; Lim, W.-W.; Chothani, S.; Tan, J.; Goh, J.W.T.; Chen, H.M.; Lim, S.Y.; et al. Targeting endogenous kidney regeneration using anti-IL11 therapy in acute and chronic models of kidney disease. Nat. Commun. 2022, 13, 1–18. [Google Scholar] [CrossRef]
- Gustavsson, M. New insights into the structure and function of chemokine receptor:chemokine complexes from an experimental perspective. J. Leukoc. Biol. 2020, 107, 1115–1122. [Google Scholar] [CrossRef] [PubMed]
- Hughes, C.E.; Nibbs, R.J.B. A guide to chemokines and their receptors. FEBS J. 2018, 285, 2944–2971. [Google Scholar] [CrossRef]
- Lei, W.; Jia, L.; Wang, Z.; Liang, Z.; Zhao, A.; Liu, Y.; Tian, Y.; Zhao, L.; Chen, Y.; Shi, G.; et al. CC chemokines family in fibrosis and aging: From mechanisms to therapy. Ageing Res. Rev. 2023, 87, 101900. [Google Scholar] [CrossRef]
- Khanam, A.; Trehanpati, N.; Riese, P.; Rastogi, A.; Guzman, C.A.; Sarin, S.K. Blockade of Neutrophil’s Chemokine Receptors CXCR1/2 Abrogate Liver Damage in Acute-on-Chronic Liver Failure. Front. Immunol. 2017, 8, 464. [Google Scholar] [CrossRef]
- Matsushima, K.; Yang, D.; Oppenheim, J.J. Interleukin-8: An evolving chemokine. Cytokine 2022, 153, 155828. [Google Scholar] [CrossRef]
- Wang, Y.-H.; Wang, M.-L.; Tao, Y.-C.; Wu, D.-B.; Chen, E.-Q.; Tang, H. The high level of IL-1β in the serum of ACLF patients induces increased IL-8 expression in hUC-MSCs and reduces the efficacy of hUC-MSCs in liver failure. Stem Cell Res. Ther. 2023, 14, 1–13. [Google Scholar] [CrossRef]
- Sasaki, T.; Suzuki, Y.; Kakisaka, K.; Wang, T.; Ishida, K.; Suzuki, A.; Abe, H.; Sugai, T.; Takikawa, Y. IL-8 induces transdifferentiation of mature hepatocytes toward the cholangiocyte phenotype. FEBS Open Bio 2019, 9, 2105–2116. [Google Scholar] [CrossRef]
- Liu, L.; Chen, P.; Xiao, N.; Liu, Q.; Zhu, X. Interleukin-8 predicts short-term mortality in acute-on-chronic liver failure patients with hepatitis B-related-related cirrhosis background. Ann. Med. 2023, 55, 2287708. [Google Scholar] [CrossRef]
- Zhu, B.; Gao, F.; Li, Y.; Shi, K.; Hou, Y.; Chen, J.; Zhang, Q.; Wang, X. Serum cytokine and chemokine profiles and disease prognosis in hepatitis B virus-related acute-on-chronic liver failure. Front. Immunol. 2023, 14. [Google Scholar] [CrossRef]
- Xiao, L.; Tang, S.; Zhang, L.; Ma, S.; Zhao, Y.; Zhang, F.; Xie, Z.; Li, L. Serum CXCL1 Is a Prognostic Factor for Patients With Hepatitis B Virus–Related Acute-On-Chronic Liver Failure. Front. Med. 2021, 8. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.; Zhang, J.; Zhang, L.; Zhao, Y.; Xiao, L.; Zhang, F.; Li, Q.; Yang, Y.; Liu, Q.; Xu, J.; et al. Knockdown of CXCL1 improves ACLF by reducing neutrophil recruitment to attenuate ROS production and hepatocyte apoptosis. Hepatol. Commun. 2023, 7. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Wang, X.; Yang, T.; Yan, Y.; Xiang, T.; Yang, L.; Luo, X. High Interleukin-8 Levels Associated With Decreased Survival in Patients With Cirrhosis Following Transjugular Intrahepatic Portosystemic Shunt. Front. Med. 2022, 9, 829245. [Google Scholar] [CrossRef] [PubMed]
- Berres, M.-L.; Asmacher, S.; Lehmann, J.; Jansen, C.; Görtzen, J.; Klein, S.; Meyer, C.; Strunk, H.M.; Fimmers, R.; Tacke, F.; et al. CXCL9 is a prognostic marker in patients with liver cirrhosis receiving transjugular intrahepatic portosystemic shunt. J. Hepatol. 2014, 62, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, J.M.; Claus, K.; Jansen, C.; Pohlmann, A.; Schierwagen, R.; Meyer, C.; Thomas, D.; Manekeller, S.; Claria, J.; Strassburg, C.P.; et al. Circulating CXCL10 in cirrhotic portal hypertension might reflect systemic inflammation and predict ACLF and mortality. Liver Int. 2018, 38, 875–884. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.; Jiao, J.; Cai, H.; Zhang, Y.; Xia, Y.; Lin, J.; Shang, Z.; Qian, Y.; Wang, F.; Wu, H.; et al. C-C motif chemokine ligand 5 confines liver regeneration by down-regulating reparative macrophage-derived hepatocyte growth factor in a forkhead box O 3a–dependent manner. Hepatology 2022, 76, 1706–1722. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, H.M.; Pitts, K.; Wang, T.; Lee, E.; Buchbinder, E.; Dougan, M.; Armstrong, D.G.; Paine, R.; Ragsdale, C.E.; Boyd, T.; et al. Recombinant GM-CSF for diseases of GM-CSF insufficiency: Correcting dysfunctional mononuclear phagocyte disorders. Front. Immunol. 2023, 13, 1069444. [Google Scholar] [CrossRef]
- Lu, W.-Y.; Bird, T.G.; Boulter, L.; Tsuchiya, A.; Cole, A.M.; Hay, T.; Guest, R.V.; Wojtacha, D.; Man, T.Y.; Mackinnon, A.; et al. Hepatic progenitor cells of biliary origin with liver repopulation capacity. Nat. Cell Biol. 2015, 17, 971–983. [Google Scholar] [CrossRef]
- Simonetto, D.A.; Shah, V.H.; Kamath, P.S. Improving survival in ACLF: growing evidence for use of G-CSF. Hepatol. Int. 2017, 11, 473–475. [Google Scholar] [CrossRef] [PubMed]
- Engelmann, C.; Habtesion, A.; Hassan, M.; Kerbert, A.J.; Hammerich, L.; Novelli, S.; Fidaleo, M.; Philips, A.; Davies, N.; Ferreira-Gonzalez, S.; et al. Combination of G-CSF and a TLR4 inhibitor reduce inflammation and promote regeneration in a mouse model of ACLF. J. Hepatol. 2022, 77, 1325–1338. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Guo, R.; Ming, D.; Deng, Y.; Su, M.; Lin, C.; Li, J.; Lin, Z.; Su, Z. The Transforming Growth Factor β1/Interleukin-31 Pathway Is Upregulated in Patients with Hepatitis B Virus-Related Acute-on-Chronic Liver Failure and Is Associated with Disease Severity and Survival. Clin. Vaccine Immunol. 2015, 22, 484–492. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Margáin, A.; Pohlmann, A.; Ryan, P.; Schierwagen, R.; Chi-Cervera, L.A.; Jansen, C.; Mendez-Guerrero, O.; Flores-García, N.C.; Lehmann, J.; Torre, A.; et al. Fibroblast growth factor 21 is an early predictor of acute-on-chronic liver failure in critically ill patients with cirrhosis. Liver Transplant. 2018, 24, 595–605. [Google Scholar] [CrossRef] [PubMed]
- Narumiya, S.; Yokomizo, T.; Aoki, J. Lipid Mediators in Inflammation. In Inflammation - From Molecular and Cellular Mechanisms to the Clinic, Wiley-VCH Verlag GmbH & Co. KGaA: Weinheim, Germany, 2017. [CrossRef]
- Artru, F.; McPhail, M.J.W.; Triantafyllou, E.; Trovato, F.M. Lipids in Liver Failure Syndromes: A Focus on Eicosanoids, Specialized Pro-Resolving Lipid Mediators and Lysophospholipids. Front. Immunol. 2022, 13, 867261. [Google Scholar] [CrossRef] [PubMed]
- López-Vicario, C.; Checa, A.; Urdangarin, A.; Aguilar, F.; Alcaraz-Quiles, J.; Caraceni, P.; Amorós, A.; Pavesi, M.; Gómez-Cabrero, D.; Trebicka, J.; et al. Targeted lipidomics reveals extensive changes in circulating lipid mediators in patients with acutely decompensated cirrhosis. J. Hepatol. 2020, 73, 817–828. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, F.; Yokomizo, T. The leukotriene receptors as therapeutic targets of inflammatory diseases. Int. Immunol. 2019, 31, 607–615. [Google Scholar] [CrossRef]
- Casulleras, M.; Flores-Costa, R.; Duran-Güell, M.; Zhang, I.W.; López-Vicario, C.; Curto, A.; Fernández, J.; Arroyo, V.; Clària, J. Albumin Lipidomics Reveals Meaningful Compositional Changes in Advanced Cirrhosis and Its Potential to Promote Inflammation Resolution. Hepatol. Commun. 2022, 6, 1443–1456. [Google Scholar] [CrossRef] [PubMed]
- Becares, N.; Härmälä, S.; China, L.; Colas, R.A.; Maini, A.A.; Bennet, K.; Skene, S.S.; Shabir, Z.; Dalli, J.; O’brien, A. Immune Regulatory Mediators in Plasma from Patients With Acute Decompensation Are Associated With 3-Month Mortality. Clin. Gastroenterol. Hepatol. 2020, 18, 1207. [Google Scholar] [CrossRef]
- O'Brien, A.J.; Fullerton, J.N.; A Massey, K.; Auld, G.; Sewell, G.; James, S.; Newson, J.; Karra, E.; Winstanley, A.; Alazawi, W.; et al. Immunosuppression in acutely decompensated cirrhosis is mediated by prostaglandin E2. Nat. Med. 2014, 20, 518–523. [Google Scholar] [CrossRef]
- Huang, X.-P.; Wang, Y.; Chen, L.; Sun, W.; Huang, Y.; Xu, Y.; Feng, T.-T.; Luo, E.-P.; Qin, A.-L.; Zhao, W.-F.; et al. Elevated serum prostaglandin E2 predicts the risk of infection in hepatitis B virus-related acute-on-chronic liver failure patients. Asian Pac. J. Trop. Med. 2017, 10, 916–920. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, C.; Qi, J.; Wu, F.; Guan, J.; Chen, Z.; Zhu, H. Altered PGE2-EP2 is associated with an excessive immune response in HBV-related acute-on-chronic liver failure. J. Transl. Med. 2019, 17, 1–14. [Google Scholar] [CrossRef]
- China, L.; Maini, A.; Skene, S.S.; Shabir, Z.; Sylvestre, Y.; Colas, R.A.; Ly, L.; Salles, N.B.; Belloti, V.; Dalli, J.; et al. Albumin Counteracts Immune-Suppressive Effects of Lipid Mediators in Patients With Advanced Liver Disease. Clin. Gastroenterol. Hepatol. 2017, 16, 738–747. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Liu, Y.; Ding, H.; Shi, X.; Ren, H. Mesenchymal stem cell-secreted prostaglandin E2 ameliorates acute liver failure via attenuation of cell death and regulation of macrophage polarization. Stem Cell Res. Ther. 2021, 12, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Campbell, A.; Dronfield, M.; Toghill, P.; Reeves, W. Neutrophil function in chronic liver disease. Clin Exp Immunol. 1981, 45, 81–89. [Google Scholar] [PubMed]
- Tritto, G.; Bechlis, Z.; Stadlbauer, V.; Davies, N.; Francés, R.; Shah, N.; Mookerjee, R.P.; Such, J.; Jalan, R. Evidence of neutrophil functional defect despite inflammation in stable cirrhosis. J. Hepatol. 2011, 55, 574–581. [Google Scholar] [CrossRef]
- DeMeo, A.N.; Andersen, B.R.; English, D.K.; Peterson, J. Defective Chemotaxis Associated with a Serum Inhibitor in Cirrhotic Patients. Journal of Laboratory and Clinical Medicine 1971, 286, 735–740. [Google Scholar] [CrossRef]
- Van Epps, D.E.; Strickland, R.G.; Williams, R.C. Inhibitors of leukocyte chemotaxis in alcoholic liver disease. Am. J. Med. 1975, 59, 200–207. [Google Scholar] [CrossRef]
- Mookerjee, R.P.; Stadlbauer, V.; Lidder, S.; Wright, G.A.; Hodges, S.J.; Davies, N.A.; Jalan, R. Neutrophil dysfunction in alcoholic hepatitis superimposed on cirrhosis is reversible and predicts the outcome. Hepatology 2007, 46, 831–840. [Google Scholar] [CrossRef]
- Fiuza, C.; Salcedo, M.; Clemente, G.; Tellado, J.M. Granulocyte Colony-Stimulating Factor Improves Deficient In Vitro Neutrophil Transendothelial Migration in Patients with Advanced Liver Disease. Clin. Vaccine Immunol. 2002, 9, 433–9. [Google Scholar] [CrossRef]
- Kedarisetty, C.K.; Anand, L.; Bhardwaj, A.; Bhadoria, A.S.; Kumar, G.; Vyas, A.K.; David, P.; Trehanpati, N.; Rastogi, A.; Bihari, C.; et al. Combination of Granulocyte Colony-Stimulating Factor and Erythropoietin Improves Outcomes of Patients With Decompensated Cirrhosis. Gastroenterology 2015, 148, 1362–1370. [Google Scholar] [CrossRef]
- Rolando, N.; Wade, J.; Davalos, M.; Wendon, J.; Philpott-Howard, J.; Williams, R. The Systemic Inflammatory Response Syndrome in Acute Liver Failure. Hepatology 2000, 32, 734–739. [Google Scholar] [CrossRef] [PubMed]
- Konstantis, G.; Tsaousi, G.; Pourzitaki, C.; Kitsikidou, E.; Magouliotis, D.E.; Wiener, S.; Zeller, A.C.; Willuweit, K.; Schmidt, H.H.; Rashidi-Alavijeh, J. Efficacy of Granulocyte Colony-Stimulating Factor in Acute on Chronic Liver Failure: A Systematic Review and Survival Meta-Analysis. J. Clin. Med. 2023, 12, 6541. [Google Scholar] [CrossRef]
- Hou, X.; Li, Y.; Yuan, H.; Cai, J.; Liu, R.; Li, J.; Zhu, C. Therapeutic Effect and Safety of Granulocyte Colony-Stimulating Factor Therapy for Acute-On-Chronic Liver Failure: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front. Med. 2021, 8. [Google Scholar] [CrossRef]
- O'Brien, A.J.; Fullerton, J.N.; A Massey, K.; Auld, G.; Sewell, G.; James, S.; Newson, J.; Karra, E.; Winstanley, A.; Alazawi, W.; et al. Immunosuppression in acutely decompensated cirrhosis is mediated by prostaglandin E2. Nat. Med. 2014, 20, 518–523. [Google Scholar] [CrossRef]
- Choe, W.H.; Baik, S.K. Prostaglandin E2-mediated immunosuppression and the role of albumin as its modulator. Hepatology 2015, 61, 1080–1082. [Google Scholar] [CrossRef] [PubMed]
- Arroyo, V.; Moreau, R. Tying up PGE2 with albumin to relieve immunosuppression in cirrhosis. Nat. Med. 2014, 20, 467–469. [Google Scholar] [CrossRef] [PubMed]
- Bernsmeier, C.; Pop, O.T.; Singanayagam, A.; Triantafyllou, E.; Patel, V.C.; Weston, C.J.; Curbishley, S.; Sadiq, F.; Vergis, N.; Khamri, W.; et al. Patients With Acute-on-Chronic Liver Failure Have Increased Numbers of Regulatory Immune Cells Expressing the Receptor Tyrosine Kinase MERTK. Gastroenterology 2015, 148, 603–615. [Google Scholar] [CrossRef] [PubMed]
- Kou, K.; Sun, X.; Tian, G.; Zhi, Y.; Fan, Z.; Lv, G. The Mechanisms of Systemic Inflammatory and Immunosuppressive Acute-on-Chronic Liver Failure and Application Prospect of Single-Cell Sequencing. J. Immunol. Res. 2022, 2022, 1–18. [Google Scholar] [CrossRef]
- Li, Z.-H.; Chen, J.-F.; Zhang, J.; Lei, Z.-Y.; Wu, L.-L.; Meng, S.-B.; Wang, J.-L.; Xiong, J.; Lin, D.-N.; Wang, J.-Y.; et al. Mesenchymal Stem Cells Promote Polarization of M2 Macrophages in Mice with Acute-On-Chronic Liver Failure via Mertk/JAK1/STAT6 Signaling. STEM CELLS 2023, 41, 1171–1184. [Google Scholar] [CrossRef]
- Lian, Z.X.; Li, L. The Liver as a Lymphoid Organ. In Liver Immunology: Principles and Practice; 2020. [CrossRef]
- Weiss, E.; de la Grange, P.; Defaye, M.; Lozano, J.J.; Aguilar, F.; Hegde, P.; Jolly, A.; Moga, L.; Sukriti, S.; Agarwal, B.; et al. Characterization of Blood Immune Cells in Patients With Decompensated Cirrhosis Including ACLF. Front. Immunol. 2021, 11, 619039. [Google Scholar] [CrossRef] [PubMed]
- Jeong, W.-I.; Park, O.; Suh, Y.-G.; Byun, J.-S.; Park, S.-Y.; Choi, E.; Kim, J.-K.; Ko, H.; Wang, H.; Miller, A.M.; et al. Suppression of innate immunity (natural killer cell/interferon-γ) in the advanced stages of liver fibrosis in mice. Hepatology 2011, 53, 1342–1351. [Google Scholar] [CrossRef] [PubMed]
- Radaeva, S.; Sun, R.; Jaruga, B.; Nguyen, V.T.; Tian, Z.; Gao, B. Natural Killer Cells Ameliorate Liver Fibrosis by Killing Activated Stellate Cells in NKG2D-Dependent and Tumor Necrosis Factor–Related Apoptosis-Inducing Ligand–Dependent Manners. Gastroenterology 2006, 130, 435–452. [Google Scholar] [CrossRef] [PubMed]
- Li, H.-J.; Yang, N.; Mu, X.; Tang, L.; Wang, S.-S.; Zhou, C.-B.; Yuan, J.-H.; Wang, H.-Y.; Yu, Y.-Y.; Li, J.; et al. Reduction of natural killer cells is associated with poor outcomes in patients with hepatitis B virus-related acute-on-chronic liver failure. Hepatol. Int. 2022, 16, 1398–1411. [Google Scholar] [CrossRef] [PubMed]
- Br, V.K.; Sarin, S.K. Acute-on-chronic liver failure: Terminology, mechanisms and management. Clin. Mol. Hepatol. 2023, 29, 670–689. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.; He, S.; Zheng, Y.; Wang, L. The value of NLR versus MLR in the short-term prognostic assessment of HBV-related acute-on-chronic liver failure. Int. Immunopharmacol. 2023, 121, 110489. [Google Scholar] [CrossRef] [PubMed]
- Clària, J.; Stauber, R.E.; Coenraad, M.J.; Moreau, R.; Jalan, R.; Pavesi, M.; Amorós. ; Titos, E.; Alcaraz-Quiles, J.; Oettl, K.; et al. Systemic inflammation in decompensated cirrhosis: Characterization and role in acute-on-chronic liver failure. Hepatology 2016, 64, 1249–1264. [Google Scholar] [CrossRef] [PubMed]
- Hensley, M.K.; Deng, J.C. Acute on Chronic Liver Failure and Immune Dysfunction: A Mimic of Sepsis. Semin. Respir. Crit. Care Med. 2018, 39, 588–597. [Google Scholar] [CrossRef] [PubMed]
- Mehta, A.S.; Long, R.E.; Comunale, M.A.; Wang, M.; Rodemich, L.; Krakover, J.; Philip, R.; Marrero, J.A.; Dwek, R.A.; Block, T.M. Increased Levels of Galactose-Deficient Anti-Gal Immunoglobulin G in the Sera of Hepatitis C Virus-Infected Individuals with Fibrosis and Cirrhosis. J. Virol. 2008, 82, 1259–1270. [Google Scholar] [CrossRef]
- Tangye, S.G.; Good, K.L. Human IgM+CD27+ B Cells: Memory B Cells or “Memory” B Cells? J. Immunol. 2007, 179, 13–19. [Google Scholar] [CrossRef]
- Cook, R.T.; Waldschmidt, T.J.; Cook, B.L.; Labrecque, D.R.; Mclatchie, K. Loss of the CD5+ and CD45RAhi B cell subsets in alcoholics. Clin. Exp. Immunol. 1996, 103, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Hassnine, A.A.; Saber, M.A.; Fouad, Y.M.; Sarhan, H.; Elsayed, M.M.; Zaki, Z.M.; Abdelraheem, E.M.; Abdelhalim, S.M.; Elsayed, A.M. Clinical study on the efficacy of hepatitis B vaccination in hepatitis C virus related chronic liver diseases in Egypt. Virus Res. 2023, 323, 198953. [Google Scholar] [CrossRef]
- Ashhab, A.A.; Rodin, H.; Campos, M.; Abu-Sulb, A.; Hall, J.A.; Powell, J.; Debes, J.D. Response to hepatitis B virus vaccination in individuals with chronic hepatitis C virus infection. PLOS ONE 2020, 15, e0237398. [Google Scholar] [CrossRef] [PubMed]
- Morishima, C.; Di Bisceglie, A.M.; Rothman, A.L.; Bonkovsky, H.L.; Lindsay, K.L.; Lee, W.M.; Koziel, M.J.; Fontana, R.J.; Kim, H.; Wright, E.C.; et al. Antigen-specific T lymphocyte proliferation decreases over time in advanced chronic hepatitis C. J. Viral Hepat. 2012, 19, 404–413. [Google Scholar] [CrossRef]
- Bernsmeier, C.; Triantafyllou, E.; Brenig, R.; Lebosse, F.J.; Singanayagam, A.; Patel, V.C.; Pop, O.T.; Khamri, W.; Nathwani, R.; Tidswell, R.; et al. CD14+ CD15− HLA-DR− myeloid-derived suppressor cells impair antimicrobial responses in patients with acute-on-chronic liver failure. Gut 2017, 67, 1155–1167. [Google Scholar] [CrossRef] [PubMed]
- Shen, C.; Yan, W.-Z.; Zhao, C.-Y.; Che, H.-H.; Liu, X.-Y.; Liu, Z.-Z.; Wang, Y.-D.; Wang, W.; Li, M.; Gao, J. Increased CD4+CD25+ regulatory T cells correlate with poor short-term outcomes in hepatitis B virus-related acute-on-chronic liver failure patients. J. Microbiol. Immunol. Infect. 2015, 48, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Shi, H.; Zhang, L.; Shi, H.; Miao, X.; Chen, L.; Chen, Y.; Ma, Y. Comparative analysis of monocyte-derived dendritic cell phenotype and T cell stimulatory function in patients with acute-on-chronic liver failure with different clinical parameters. Front. Immunol. 2023, 14, 1290445. [Google Scholar] [CrossRef]
- Widjaja, A.A.; Chothani, S.P.; Cook, S.A. Different roles of interleukin 6 and interleukin 11 in the liver: implications for therapy. Hum. Vaccines Immunother. 2020, 16, 2357–2362. [Google Scholar] [CrossRef]
Figure 2.
Anti-Il-11 antibodies reduce fibrosis and hepatocyte death and have anti-inflammatory properties.
Figure 2.
Anti-Il-11 antibodies reduce fibrosis and hepatocyte death and have anti-inflammatory properties.
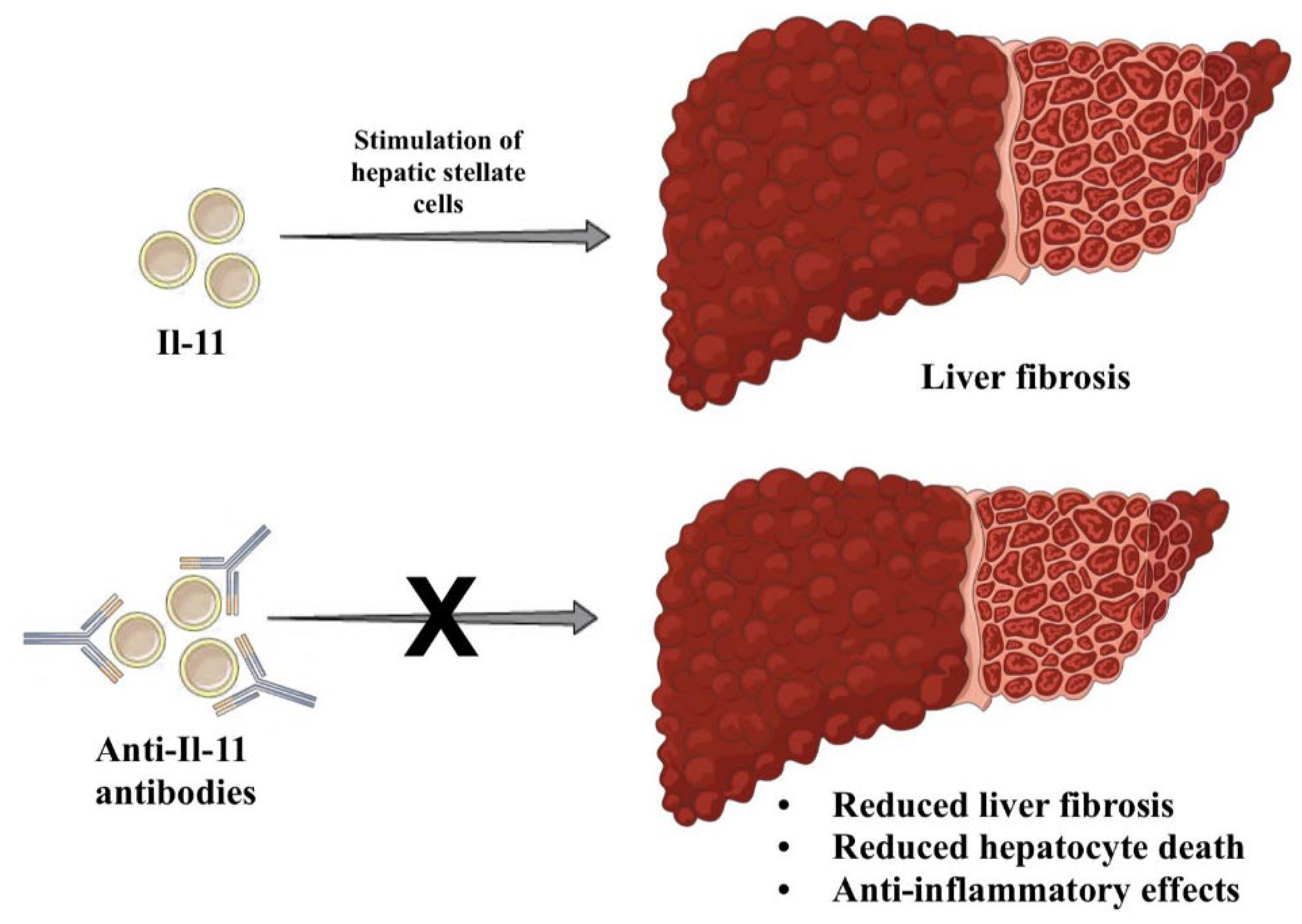
Figure 3.
The figure presents the role of the G-CSF in granulopoiesis and its effect on the clinical course of liver failure.
Figure 3.
The figure presents the role of the G-CSF in granulopoiesis and its effect on the clinical course of liver failure.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



