
Submitted:
29 July 2024
Posted:
30 July 2024
You are already at the latest version
Abstract
Glaucoma is one of the primary causes of blindness worldwide. Canal opening surgery, a type of minimally invasive glaucoma surgery (MIGS) applied in cases of mild to moderate glaucoma, has gained increasing popularity in recent years due to its efficacy in reducing intraocular pressure, its safety profile, the simplicity of its technique, and the reduced likelihood of compromised vision. Nevertheless, the existing body of histopathological studies remains insufficient for a comprehensive understanding of post-surgical wound healing. Consequently, debates persist among researchers regarding the mechanism through which Schlemm’s canal opening surgery reduces intraocular pressure, as well as the surgical techniques that may impact the outcomes and the factors influencing surgical success.
As the history of MIGS is relatively short and lacks sufficient systemic reviews or meta-analysis evaluating the influence of individual factors, this review was conducted to illuminate disparities in the researchers’ opinions at the current stage of research.
Keywords:
MIGS (minimally invasive glaucoma surgery)
; Schlemm’s canal opening surgery
; Trabeculotomy
; Trabeculectomy
; Canaloplasty
; Kahook dual blade
; Trabectome
; Tanito micro-hook
; surgical success
; history
1. Introduction
Ideally, glaucoma surgery must be safe and effective in reducing the intraocular pressure and maintaining the patient’s visual function. Filtering surgeries are effective in reducing IOP, however, the deterioration of post-surgical visual acuity is common [1,2], and many problems occur, such as post-surgical hypotension, bleb leaks, infection, and others. Because of these problems and the complexity of postoperative care, there has been a shift from filtering surgery to non-filtering surgeries. Canal opening surgery is a type of minimally invasive glaucoma surgery (MIGS) that has gained popularity in recent years. However, the history of MIGS is short, and controversies remain unresolved. This study provides an overview of the history and clinical controversies of canal opening surgeries.
2. History of Canal Opening Surgery
2.1. Evolution of Trabeculotomy ab Externo
As early as 1873, it was established that the trabecular meshwork is the main site of aqueous humor outflow resistance in glaucoma eyes [3]. In 1954, Barany and Scotchbrook found that the injection of testicular hyaluronidase significantly increased aqueous outflow [4].
In 1947, Barkan hypothesized that incising the trabecular meshwork, which was postulated as a primary site of outflow resistance, could reduce intraocular pressure [5]. He introduced the concept of goniotomy. This technique was a great relief for refractory congenital glaucoma patients [6]. However, at that time, the absence of appropriate surgical microscopes posed a significant challenge in accessing and incising the trabecular meshwork from inside the eye. Consequently, goniotomy was primarily indicated for congenital glaucoma, which was associated with poor outcomes after filtration surgery.
Subsequently, in England, Smith achieved success by opening Schlemm’s canal through a blunt incision in the trabecular meshwork [7]. This was accomplished by inserting a thread into Schlemm’s canal and pulling it; this technique was also reported by Burian around the same period [8].
Nine years later, Smith provided an update on his continued efforts. He said, “I have been performing Nylon filament trabeculotomy for seven years, but I’ve been holding back from writing papers in the meantime. The reason for this was that I was not sure whether the surgery was really benefiting the patient.” Subsequently, he detailed the outcomes. The outcomes of 26 cases of suture trabeculotomy and 27 cases of filtering surgery (9 irido-encleisis, 8 Scheie, 6 trephine, and 4 Stallard surgeries) were compared. The results indicated a more favorable decrease in intraocular pressure with suture trabeculotomy [9].
2.2. Trabeculotomy ab Externo: Time of Hardship
Outflow surgery was a prominent topic at that time. A comprehensive exploration of the histopathological aspects of outflow surgery took place during the 76th American Academy of Ophthalmology (AAO) meeting (Symposium: Microsurgery of the outflow channels), held in Las Vegas from September 20 to 24, 1971. The symposium presented the results of histopathological studies on trabeculectomy, sinusotomy, and trabeculotomy.
During the same symposium, it was demonstrated that aqueous outflow is a passive process and that the outflow facility (µl/min/mmHg) is enhanced by trabeculotomy. However, the opening of Schlemm’s canal in normal monkey eyes closes within 28 weeks after surgery [13], and the ability to enhance outflow diminishes over time. Grant has suggested that leaks from the flap and inadvertent cyclodialysis may lead to post-surgical hypotension [14]. Trabeculotomy ab externo was reported as a challenging procedure, which carries the risk of mis-insertion of the probe outside Schlemm’s canal [15].
Despite the AAO’s critical debate on the promotion of trabeculotomy, the publication of studies recommending trabeculotomy ab externo did not stop [16,17,18]. Dannheim subsequently reported a stable reduction in intraocular pressure for 4 years following trabeculotomy surgery [19] and reported the facilitation of aqueous outflow using tonography [20]. Mackensen noted that “Even though effects of trabeculotomy in pressure-reducing is inferior to that of fistulizing surgery, authors prefer trabeculotomy because this preserves the unaffected meshwork“ [21].
Despite the favorable clinical reports, the negative impact of the experimental studies, which demonstrated early closure of the trabecular opening after trabeculotomy and no improvement in the rate of aqueous humor outflow in monkeys, was substantial [19,22,23]. Due to these negative results, the validity of trabeculotomy ab externo as a treatment for adult-onset primary open-angle glaucoma (POAG) was questioned at that time.
2.3. Trabeculotomy ab Externo: Exploring a Way to Survive as a Treatment for Congenital Glaucoma
In a prospective study, Luntz et al. treated 19 cases of adult-onset glaucoma with a mean intraocular pressure (IOP) of 41 mmHg using trabeculotomy ab externo, achieving a success rate of 70%. In contrast, trabeculotomy in 19 cases of congenital glaucoma with a mean IOP of 34 mmHg achieved success in 18 out of 19 eyes (95%). The authors concluded that trabeculotomy was a procedure for congenital glaucoma and not for adult-onset POAG [24].
Subsequently, trabeculotomy ab externo gained recognition as a viable option for treating congenital glaucoma and infantile glaucoma. It was acknowledged as being equally effective as goniotomy, solidifying its status as a treatment for children at that time.
The disparity in efficacy between adult-onset POAG, which showed poor results, and infantile or congenital glaucoma, which exhibited positive outcomes, was attributed to the presence of rich elastic fibers in the infantile angle, which could increase the gaping of elastic tissue in the angle structure [25].
3. Historical Controversy I
3.1. Goniotomy vs. Trabeculotomy ab Externo; Which Is the Optimal Approach for Congenital Glaucoma?
As previously mentioned, trabeculotomy ab externo has gained recognition as a viable treatment for congenital glaucoma in Europe and the United States. As a next step, the debate on the comparative merits of trabeculotomy and conventional goniotomy came to a focal point.
Some of the authorities argued that congenital glaucoma patients should undergo at least one goniotomy before considering trabeculotomy [26].
McPherson compared the surgical outcomes for congenital glaucoma between trabeculotomy using a modified Harms Trabectome and goniotomy. The study concluded that the outcomes of trabeculotomy ab externo yielded superior results compared to traditional goniotomy. Additionally, the success rate of trabeculotomy was higher in congenital glaucoma cases than in adolescent glaucoma cases [27,28,29].
Rothkoff introduced a modified surgical technique which excises the deeper flap of the doubled flap and reported improved outcomes [30].
Glaucoma authorities of that era also reported that trabeculotomy was the recommended surgical approach for congenital and developmental glaucoma. Quigley and Anderson reported that trabeculotomy and goniotomy exhibited comparable performances with fewer complications in the case of childhood glaucoma. Furthermore, they documented that trabeculotomy ab externo has an advantage when dealing with cloudy cornea. Both researchers also highlighted a correlation between a child’s age and the success of the outcomes [31,32].
Subsequently, particularly in the United States, trabeculotomy gained recognition as a viable treatment option for congenital and juvenile glaucoma. At the same time, it was recognized that the outcomes deteriorated as the patient aged. This concept had widespread acceptance both within and outside the USA [33].
Before the widespread adoption of internal trabeculotomy (trabeculectomy), external trabeculotomy was frequently employed for congenital glaucoma. However, as internal trabeculotomy gained popularity, there was a shift from external to internal trabeculotomy, and it is becoming the preferred method over external trabeculotomy [34,35,36,37,38,39,40,41,42,43].
3.2. Historical Controversy II. Is Trabeculotomy ab Externo Effective for Adult POAG?
Before the introduction of the Trabectome in 2005, Lamers [18], Dannheim et al. [19], and Nagata et al. [44,45] reported the long-term success of trabeculotomy ab externo in controlling intraocular pressure in adult-onset POAG.
In the “Tuebingen Study”, Weder and others compared the surgical outcomes between trabeculotomy ab externo and goniotrephination. They concluded that trabeculotomy should be considered as an alternative operation for elderly patients with glaucoma simplex to avoid hypotonia. Their study revealed that 2/3 of 80 POAG cases were controlled without medication, and 89% achieved qualified success [46]. In 1999, Quaranta and others reported that trabeculotomy could be applied in adult-onset POAG. They compared the outcome between trabeculotomy and trabeculectomy augmented with mitomycin C in adult POAG, finding no statistically significant difference in IOP from the 6th to the 24th postoperative month between the two groups [47].
Before 2004, the clinical effectiveness of external trabeculotomy was mainly inherited in Japan, with multiple publications supporting its effectiveness in adult POAG and PEG [48,49,50,51,52,53,54,55,56,57,58]. A user-friendly probe for trabeculotomy invented by Nagata might have facilitated the widespread adoption of this technique in the country. In 2002, Tanito et al. utilized Cox multivariate analysis and reported that advanced age is a favorable prognostic factor for the successful control of IOP through trabeculotomy ab externo. Their findings also demonstrated a good post-surgical visual acuity prognosis, highlighting that elderly POAG patients with a concomitant cataract are well suited for combined phacoemulsification aspiration, implantation of an IOL, and trabeculotomy ab externo surgery [59]. At that time, the efficacy of trabeculotomy ab externo was widely accepted and was adopted as a standard treatment for mild to moderate POAG in Japan. Around 2008, trabeculotomy ab externo accounted for 38% of the total number of glaucoma surgeries performed in Japan [60].
In spite of these reports, canal opening surgery was not recognized as an effective treatment for POAG in adults globally until 2005. The shift toward canal opening surgery in the United States began to emerge in 2005. In 2005, the invention of the Trabectome® by Minckler marked the initiation of internal trabeculotomy, which was later named MIGS [25,61].
In a review article, Godfrey and others introduced canal surgeries such as the Trabectome, canaloplasty, and trabeculotomy ab externo, as effective treatments for adult glaucoma. They noted that “In other parts of the world, where canal surgery is more popular, trabeculotomy remains an option to filtering surgery for adult and juvenile glaucoma [62].”
Following the publication of this review article, it appears that many glaucoma surgeons have embraced the view that canal opening is an effective treatment for adult patients with POAG or PEG.
4. Historical Controversy II
4.1. Debate in Histological Findings after Trabeculotomy: Difference in Tissue Response between Monkeys and Humans
In an earlier study, Dannheim and colleagues investigated the post-surgical regenerative closure of Schlemm’s canal opening in monkey eyes following external trabeculotomy using a metal probe. They observed cellular regeneration in 17 healthy monkeys and noted that this regeneration was initiated between 6 and 8 weeks after the opening of the trabecular meshwork. The trabecular opening closed within 28 weeks due to the regenerated trabecular lamellae and trabecular endothelium, ultimately forming a dense scar [23]. In their study, Schlemm’s canal opening was filled with fibrous tissue, and IOP did not decrease in healthy monkey eyes. The closure of Schlemm’s canal opening in their study might have been considered a potential cause of the poor reduction in IOP.
Ito and colleagues [63] conducted an electron microscope study of the regeneration of the trabecular meshwork following trabeculotomy ab externo in 10 monkey eyes. Their research revealed that the regeneration of the trabecular meshwork begins with the regeneration of the corneo-scleral meshwork and endothelium, eventually progressing to the regeneration of the uveal meshwork. After one year, the defects were almost completely repaired by newly formed trabecular tissue, which closely resembled normal trabecular tissue. Notably, there was no direct communication between Schlemm’s canal and the anterior chamber at the one-year mark.
In contrast to the reports by Dannheim [23] and Ito [63], Hamanaka and colleagues conducted a study of histopathological changes in the trabecular meshwork (TM) and Schlemm’s canal of human eyes where trabeculotomy ab externo had been unsuccessful [64,65,66]. They reported that, in 10 out of 31 eyes, Schlemm’s canal remained open to the anterior chamber even six years after trabeculotomy ab externo [65,66]. In these cases, the inner wall of Schlemm’s canal was either covered or filled with fibrous tissue or the regenerated endothelium of Schlemm’s canal (Figure 1). This finding aligns with the histopathology observed in human eyes by d’Epiney [67], who used electron microscopy to investigate the histopathology of the angle following trabeculotomy in two human eyes with congenital glaucoma. They found that Schlemm’s canal contained abundant erythrocytes, and the inner wall of the canal exhibited an encroached endothelium. In the trabecular area, the trabecular structures were lost and were replaced by cell- and fiber-rich tissues.
These findings indicate potential differences between monkey eyes and human eyes.
Notably, the presence of an endothelial layer covering the uveal meshwork was observed in individuals who underwent laser trabeculoplasty; these findings may align with post-trabeculotomy observations [68].
It is crucial to emphasize a key distinction between monkey eyes and human eyes. In monkey eyes, Schlemm’s canal opening closes within 28 weeks, whereas this phenomenon does not occur in the human eye.
Regarding the functional aspects of the trabecular meshwork, the outflow facility after trabeculotomy did not change significantly in “normal” monkey eyes [22]. In contrast, clinical studies in humans have indicated that the reduction in IOP persisted for a long period of time [19,48,49,50,51,52,53,54,55,57,58,69].
From a clinical perspective, when eyes are examined using gonioscopy following canal opening surgery, it is common to observe a rough-surfaced, pigmented membrane-like tissue that covers the inner surface of Schlemm’s canal following internal trabeculotomy and internal trabeculectomy. Despite the formation of this membrane on the inner surface of Schlemm’s canal, delayed-onset hyphema may occur after internal trabeculotomy or trabeculectomy. This finding suggests a direct communication between the anterior chamber and collector channel [70,71,72,73,74].
The enhancement of the episcleral venous fluid wave (EVFW) in the aqueous vein serves as a sign of activated aqueous outflow following canal surgery [75].
In normal eyes, the reported number of collector channels (CCs) is approximately 80 [76]. The inferior half of the CCs drain 87% and the inferior nasal CCs drain 56% of the total outflow [77]. If the orifice of the CC becomes sealed by regenerated endothelium and/or fibrous tissues, there is a potential for an elevation in IOP (Figure 1).
Currently, we lack sufficient information regarding the degree or number of closed CCs that is crucial to impair normal aqueous outflow. In a previous report, it was suggested that only one or two active aqueous veins may be sufficient to drain enough aqueous humor from the eye [78,79]. The regeneration and fibrosis of TM tissue, along with the sealing of CCs by fibrous tissue or Schlemm’s canal endothelium, may lead to a gradual increase in post-surgical IOP [80] .
5. Evolution of Internal Trabeculotomy in Minimally Invasive Glaucoma Surgeries (MIGS)
5.1. Evolution of 360-Degree Suture Trabeculotomy
Suture trabeculotomy was first reported by Smith in 1960 [7]. With this technique, the trabecular meshwork is not excised. A nylon thread is inserted into Schlemm’s canal and pulled to open the trabecular meshwork by blunt trauma. In 1987, Lynn and Fellman gave an oral presentation on a 360-degree suture trabeculotomy. Subsequently, in 1987, Beck et al. conducted a study on the outcomes in 26 eyes of 15 patients [82]. In 2012, Chin and others reported a positive 2-year outcome of 360-degree suture trabeculotomy using a 5-0 nylon suture from outside the eye [83].
Two years later, Grover and others introduced a technique named GATT, whereby a microcatheter or suture is used for a complete 360-degree trabeculotomy from inside the eye. They identified the “trabecular shelf” as a sign of an opened Schlemm’s canal [84].
In 2014, Sato and others reported a modified technique involving the simple insertion of a nylon thread without the need for any special instruments [85].
The GATT technique encountered challenges during its initial introduction [86], and it was necessary to undergo a learning curve to acquire proficiency; however, it is now widely accepted as a viable option for treating both adult POAG and childhood glaucoma. Many reports have attested to the long-term success of GATT in effectively controlling IOP [87,88,89,90,91,92,93,94].
The histopathology of the angle after 360-degree suture trabeculotomy was reported by Hamanaka and others. In their study of 11 cases with unsuccessful IOP control, Schlemm’s canal remained open in 9 out of 11 eyes 4 years after surgery. The identified cause of failure was the fibrous proliferation and elongation of Schlemm’s canal endothelium (SCE), which was not associated with the closure of the orifice of Schlemm’s canal opening [66].
There is an ongoing debate regarding whether the outcomes of a 360-degree circumferential trabecular meshwork opening surpass those achieved with a canal opening in the range of 90-150 degrees. (See Section 3b for further details.)
5.2. Evolution of Trabectome® and Kahook Dual Blade
The Trabectome®, which was introduced by Minckler and others in 2005, stands as the pioneering device for ablating the trabecular meshwork from inside, leading to the evolution of MIGS [25,61]. They introduced a hand piece featuring a 19-gauge infusion sleeve and a 25-gauge aspiration port with a moderately sharp triangular tip. The inner wall of the trabecular meshwork was ablated in a manner similar to bipolar cautery [25]. With this technique, the conjunctiva is completely preserved, and in the case of failure, it permits subsequent filtering surgeries, such as trabeculectomy and tube shunt surgery.
As a next-generation internal trabeculectomy device, the Kahook dual blade was invented; it enabled the excision of the trabecular meshwork through the use of a dual-blade tip.
Numerous reports have documented the efficacy of Trabectome procedures [95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135,136] and Kahook dual blade (KDB) surgery [137,138,139,140,141,142,143,144,145,146,147,148,149,150,151,152,153,154,155,156,157,158,159,160,161,162,163,164,165,166,167,168] in maintaining long-term control of IOP (Figure 2).
5.3. Evolution of Internal Trabeculotomy Which Opens Trabecular Meshwork without Excising Tissue
The Tanito micro-hook (TMH Figure 3) is a device for internal trabeculotomy that pushes away the trabecular meshwork to create an opening in Schlemm’s canal. The surgical outcomes of the TMH are comparable to those achieved with the Trabectome, KDB, and trabeculotomy ab externo [128,169,170,171,172,173,174,175,176,177,178,179,180,181] and may surpass the efficacy of the iStent [182,183,184].
The T-hook (Figure 4) is a novel device designed to permit a bidirectional opening of the trabecular meshwork without injuring the outer wall tissue of Schlemm’s canal [185].
Additionally, there are other new devices that have recently been invented to push away trabecular meshwork tissues [186].
5.4. Effects of Canal Expansion (Canaloplasty) without Opening the Trabecular Meshwork
Canaloplasty facilitates aqueous outflow by expanding Schlemm’s canal, and this technique has gained widespread adoption, primarily in Europe. The fundamental mechanism underlining IOP reduction in canaloplasty may be explained by four theories, one of which is the hinge–valve theory [187]. The tension of the conduits traversing Schlemm’s canal regulates both the aqueous inflow from the anterior chamber into Schlemm’s canal and the outflow from Schlemm’s canal to the collector channel. The proposed entry site for the aqueous chamber is a funnel-shaped canal inlet, and the regulator of the aqueous outlet is a hinged collagen flap. If Schlemm’s canal expands, the tension of the conduit increases, and the hinged collagen flap is pulled, opening the outlet valve. Another theory suggests that Schlemm’s canal ruptures under high pressure, resulting in multiple defects in the inner and outer walls of Schlemm’s canal [188,189]. The third theory involves the herniation of the inner wall of Schlemm’s canal into the collector channel. In other theories, this procedure effectively reduces IOP by dilating the collapsed Schlemm’s canal, cleaning collector channel and stretching the trabecular meshwork. Even now, debate continues regarding the basic mechanism of IOP reduction following canal expansion.
The technique involves viscodilation of Schlemm’s canal, the insertion of a microcatheter (such as iTrack, etc.), and the stretching of the trabecular meshwork using a 10-0 prolene thread, facilitating aqueous outflow. Additionally, the creation of an intrascleral lake may provide an alternative drainage route into the intrascleral and suprachoroidal space [190]. Planned goniopuncture can further enhance outflow. In the case of failure following canaloplasty, trabeculotomy may be employed as the next step.
External trabeculectomy is more efficient than canaloplasty in reducing the IOP; however, the success probability using canaloplasty was not inferior to that of trabeculectomy, according to several meta-analysis studies [191,192,193].
In one report, conventional canaloplasty achieved better outcomes than the other methods [194]. There are numerous reports on the effects of canaloplasty [90,195,196,197,198,199,200,201,202,203,204,205,206,207,208,209,210,211,212,213,214,215,216,217,218,219,220,221,222,223,224,225,226,227,228,229,230,231,232,233,234,235,236,237,238,239,240,241,242,243,244,245,246,247,248,249,250,251,252,253,254,255,256]. Basically, classic canaloplasty is not considered to be canal opening surgery; however, in recent techniques using canaloplasty, Schlemm’s canal was “unroofed [246,257]”. If Schlemm’s canal is disrupted under high intracanal pressure [188,189], the difference between GATT or suture trabeculotomy and canaloplasty becomes unclear [257].
5.5. Streamline® and Hydrus®
Streamline® expands Schlemm’s canal using a viscoelastic material [258], while Hydrus, a Schlemm’s canal scaffold, combines elements of canaloplasty and iStent to dilate Schlemm’s canal and establish a connection between the anterior chamber and Schlemm’s canal [252]. Both methods are considered to be techniques that are associated with canaloplasty. These reduce IOP without significant complications.
5.6. iStent
iStent, a popular form of canal surgery, offers a low risk of complications and a mild reduction in IOP. It is a type of stenting surgery that does not open the canal. There are many review papers that compare the outcomes between iStent and canal opening MIGS [259,260,261,262,263,264]; therefore, it was not extensively reviewed in this study.
5.7. Others
Viscocanalostomy is a technique which externally modulates Schlemm’s canal. It is not included in MIGS and not commented upon in this study [265]. Recently, viscocanalostomy has been largely replaced by canaloplasty [194]. High-frequency deep sclerectomy creates an intrascleral pocket internally and facilitates the uveo-scleral pathway, but it is not included in canal opening surgery [259].
6. Clinical Controversies Regarding Internal Canal Opening Surgery
6.1. Differences between Internal Canalectomy and Canalotomy.
6.1.1. Open or Close? Does It Matter?
When Minckler and colleagues introduced the “Trabectome”, the device was designed to create permanent unroofing of the TM [25]. They believed that permanent unroofing was important for long-lasting IOP reduction, a concept that was later advanced by the Kahook dual blade (KDB) [266]. In contrast, trabeculotomy ab externo opens Schlemm’s canal through blunt trauma using a nylon filament or metal probe. This concept was succeeded by gonioscopy-assisted transluminal trabeculotomy (GATT) and internal suture trabeculotomy, which creates a “shelf” in the angle. Similarly, new devices such as the Tanito micro-hook (TMH) and the T-hook push the TM tissue away and do not excise TM, creating a double-door opening in the TM.
When post-surgical wounds were studied using anterior segment OCT, the size of the wounds was found to be greater in cases of internal trabeculectomy, such as that with the KDB, compared to internal trabeculotomy such as that with the TMH. However, no significant difference in post-surgical IOP was noted [267].
From a clinical standpoint, no discernible difference in surgical outcome was observed between the internal trabeculectomy cases, such as those involving the Trabectome and KDB, and the trabeculotomy cases, such as those involving trabeculotomy ab externo, GATT [84], the TMH [177], the T-hook [185], and 360-degree suture trabeculotomy [83,128,172,185,268,269,270,271,272].
This raises the question of whether the surgical outcomes after internal trabeculotomy differ from those after internal trabeculectomy.
However, there is still insufficient research to determine whether the long-term observations reveal distinctions between the two procedures [263,273]. The clinical findings and the histopathological studies conducted by Hamanaka and others [66] suggest that the issue regarding whether Schlemm’s canal is opened or closed may not be the critical factor; instead, the sealing of the inner surface of the canal is the issue.
On the other hand, there is a debate regarding whether the meridional extent of the canal opening affects surgical outcomes (See chap 3-2). Some believe that a larger opening is beneficial for greater IOP reduction [93,274,275,276], while others hold a contrary view.
Meta-analysis is a desirable approach for evaluating the efficacy of new surgical techniques; however, the number of randomized clinical trials in the area of MIGS is not sufficient [277]. External trabeculectomy has at least been demonstrated to have greater efficacy in reducing IOP compared to internal trabeculotomy; however, it also carries a higher risk of complications [278].
6.2. Does the Extent of Canal Opening Area Impact Surgical Outcomes?
In a clinical study, the area of active circumferential flow in Schlemm’s canal is restricted. Fellman and Grover reported that downstream episcleral vein bleaching is confined to two clock hours from the edge of the Trabectome incision. In their report, the bleaching of episcleral veins was shown to occur within 41 degrees infero-nasally and 13 degrees supero-nasally from the incisional end using the Trabectome [279]. This may explain why the effects of iStent on IOP are inferior to those of other internal trabeculotomy techniques [117,155,183,280,281,282,283]. In a meta-analysis study, the outcome of iStent was inferior to that of Hydrus [263].
Ellingsen and Morton found that the aqueous outflow facility was better when a wide area of the trabecular meshwork was opened [284]. Rosenquist and others confirmed better IOP reduction with a wider Schlemm’s canal opening in cadaver eyes [285]. Several clinical reports also suggest that a wider opening of the canal leads to better IOP reduction [89,93,274,286,287].
However, when the canal opening extends beyond 90 degrees, the effects of widening the canal opening on post-surgical intraocular pressure do not exhibit a consistent trend. Several studies indicate that there is no significant difference in the extent of IOP reduction when the canal opening exceeds 90 degrees [170,288,289,290,291,292,293]. In a hypothetical model, the decrease in outflow resistance was greater in eyes with a 4-hour incision than those with a 1-hour incision. However, the effects of expanding the incision on post-surgical IOP reached saturation point when the excision area exceeded 90 degrees [294]. In eyes where the canal opening is expanded to 360 degrees, there is no further decrease in outflow resistance [294]. The wider the canal opening, the greater the intracameral bleeding and obstruction of collector channels [295].
It has been reported that only one or two active aqueous veins are enough to drain a sufficient amount of aqueous humor to maintain normal IOP [78,79]. Thus, the survival of only a few active collector channels may be sufficient to sustain normal intraocular pressure. After the canal opening surgery, the gradual coverage of the collector channel opening due to the elongation of Schlemm’s canal endothelium, along with the proliferation of fibrous tissue, constitutes a slowly progressing phenomenon and may lead to a gradual elevation in IOP [66]. It may require a long time for the complete obstruction of 80 collector channels to occur.
If the collector channel at the site of the canal opening is intact, a localized opening may be sufficient to obtain clinical success; however, it is difficult to estimate the clinical integrity of the intra-scleral outflow before surgery.
It is still unclear whether a wide canal opening is beneficial to the restoration of the active aqueous vein or not. A prospective and long-term follow-up study is needed to address this question.
6.3. Does the Type of Glaucoma Affect Canal Opening Surgery Outcomes?
6.3.1. Steroid-Induced Glaucoma
In steroid-induced glaucoma, an abnormal extracellular matrix (ECM), consisting of abnormal collagen and dense homogenous material accumulates adjacent to the inner wall of Schlemm’s canal. These ECM characteristics are different from those observed in POAG. Clinically, Schlemm’s canal and CC are generally unaffected by steroids, and a favorable response to the canal opening surgery is expected. Many reports indicate positive outcomes following internal trabeculotomy or internal trabeculectomy [101,169,233,253,276,296,297,298,299]. Therefore, steroid-induced glaucoma may be considered a suitable candidate for the internal canal surgeries.
6.3.2. Secondary Glaucoma: Uveitic Glaucoma
When inflammatory cells obstruct the trabecular meshwork, intraocular pressure increases. In the case of prolonged inflammation, scar tissue is formed, which impairs aqueous outflow. In canal surgery, post-surgical inflammation may promote the post-surgical proliferation of fibrous tissue and induce the elongation of the SCE [169,296].
6.3.3. Pseudoexfoliation (Exfoliation) Glaucoma
In contrast to POAG, (pseudo-)exfoliation glaucoma (PEG) is characterized by higher IOP, faster visual field deterioration, poor response to medical therapy, and an increased need for surgical intervention. While some reports demonstrate positive outcomes with canal surgeries in PEG cases [17,52,55], others do not.
The reduction in IOP through canal surgery in PEG cases is significant [17,52,94,102,126,302,303], often surpassing that observed in POAG [55,304], or an equivalent outcome between PEG and POAG is shown [106,305,306]. However, it is noteworthy that pre-surgical IOP is typically higher in PEG cases, which may contribute to greater IOP reduction following canal surgery. This substantial IOP reduction in PEG cases may simply reflect the inherent nature of canal surgery, which tends to achieve higher IOP reduction in cases with high preoperative IOP. Consequently, the final IOP in PEG might remain high, potentially leading to a poor final outcome [169]. In addition to the final IOP, the fluctuation of the IOP level may affect the nerve damage. Therefore, the efficacy of canal surgery in treating PEG remains unclear.
6.4. How High Can Preoperative Intraocular Pressure Be for Indication of Canal Opening Surgery?
In many reports, the surgical reduction in IOP in canal surgery is more pronounced in eyes with higher pre-surgical IOP [169,171,180,307,308,309]. Tanito reported that (percentile IOP reduction ) = 2.1*(preoperative IOP) − 15.7 [171]. A clear correlation exists between pre-surgical IOP and the extent of IOP reduction [171]. We reported a marginal association between pre-surgical IOP and post-surgical IOP in phaco-trabeculotomy cases, reporting a regression equation: (post-surgical IOP) = 12.812+0.166*(pre-surgical IOP), P=0.0629. In this study, the critical pre-surgical IOP required to achieve 18mmHg was 31.3mmHg [308]. However, the association between pre- and post-surgical IOP was weak and may not follow a linear regression line; thus, it requires further elucidation. The upper limit of pre-surgical IOP for considering canal opening surgery has not yet been determined.
6.5. Do Pre- and Post-Surgical Eye Drops Affect Outcome?
The use of certain drugs may influence or alter the surgical outcome. A parasympathomimetic drug is employed to prevent post-surgical peripheral anterior synechia (PAS) formation, although its effects have not been comprehensively assessed [310].
The application of a vasoconstrictive agent may potentially limit intracameral bleeding [311]. The use of Rho-associated coiled-coil-containing protein kinase (ROCK) inhibitors may modulate contractile elements of the collector channel and positively impact post-surgical IOP. However, the available data are limited, and additional studies are needed to validate these findings [312,313]. The response to ROCK inhibitors may be useful in predicting the outcome of MIGS, while prolonged or multiple use of anti-glaucoma medications may adversely affect the outcome [314,315,316].
6.6. Does the Combination of Cataract Surgery Benefit Outcome of Canal Opening Surgery?
The extraction of the lens results in the retro-positioning of the iris diaphragm and increases tension on the trabecular meshwork [187]. Simple lensectomy widens the angle and intensifies the tension of the trabecular meshwork, consequently reducing the IOP [317,318,319,320]. In angle-closure glaucoma, lens extraction has a favorable impact on post-surgical IOP [124,318].
On the other hand, the results of a meta-analysis of the outcome of standalone Trabectome (39% reduction) and a combined phacoemulsification–Trabectome (27% reduction) was not conclusive [321]. Regarding POAG cases, there is ongoing debate concerning the effects of concomitant cataract surgery and canal surgery in terms of their impact on post-surgical IOP. While several studies indicate positive effects [89,302,303,309,322,323,324,325,326], conflicting findings are reported by others [84,293,327,328,329,330,331,332].
It is worth noting that combined cataract surgery negatively affects the outcome of trabeculectomy; however, this is not the case in canal surgeries [94].
6.7. How Do Post-Surgical IOP Spike and Intracameral Bleeding Affect MIGS Outcomes?
Here, we must be careful to define the difference between simple hyphema and clot formation. Surgical trauma to vascular tissue triggers the release of von Willebrand factor, initiating a cascade of events from platelet adherence and the conversion of fibrinogen to fibrin, which leads to peripheral anterior synechia (PAS) formation and the potential occlusion of the collector channel orifice [333,334]. Rao reports that the development of PAS is associated with a spike in IOP [334].
Even though the trabecular meshwork tissue is rich in tissue plasminogen activator [335] and facilitates the dissolution of a blood clot to enhance aqueous humor drainage, once a clot is formed, it may worsen tissue adhesion. Ishida and colleagues have reported a close correlation between clot formation and a subsequent elevation in post-surgical IOP [184]. Shi, Quan, and others have emphasized that a spike in IOP constitutes a risk factor for poor IOP control [336,337,338]. In other reports, clot formation is a significant risk factor for re-operation [295] and may lead to a gradual increase in post-surgical IOP [80].
6.8. Does Prior SLT (Selective Laser Trabeculoplasty) or LTP Affect MIGS Outcomes?
A modest reduction in IOP is achieved with selective laser trabeculoplasty without any significant complications. This may not affect the surgical outcome of the canal surgery [339,340], however. others report adverse effects of SLT [135,325,341]. After failed SLT, canal opening surgery is a viable candidate option to reduce IOP [342,343,344]. However, caution is necessary, as there is a report that SLT is not useful as a next step following failed canal surgery [345].
6.9. What Are the Risk Factors for the Failure of Canal Surgery?
As mentioned previously, uveitic glaucoma and pseudoexfoliation glaucoma, a history of SLT, LTP [345], and post-surgical PAS or spike are risk factors for failure. Neovascular glaucoma is contraindicated for canal surgery, except for in one report [346].
When preoperative IOP is high, the decline in IOP is large; however, the final IOP value is often high; so, preoperative high IOP is a risk factor for failure [169,309,347,348]. Regarding traumatic glaucoma, we do not have enough evidence, and it is therefore difficult to comment on. Younger age [325,349,350] was shown to be a risk for failure, except in one report [351]. This finding may contrast with the findings of older studies, in which the outcome of trabeculectomy ab externo was better in congenital glaucoma than in juvenile-onset glaucoma [31,32].
Large central corneal thickness [348,350] and myopia [352,353,354] were listed as risk factors, except in one study [355]. Male gender may affect the outcome [356]. It is noteworthy that better outcomes are reported in Hispanic people [303]. However, the Black race was associated with a higher risk of reoperation [309].
7. Conclusions
This review explores the history of canal opening surgery, the several types of procedures available, the clinical controversies surrounding them, and the risk factors associated with their failure.
External trabeculotomy, since its inception, has faced numerous challenges and has not gained global acceptance for the treatment of adult-onset POAG. It was later modified into internal trabeculotomy, which has recently become more popular. Initial experiments on normal monkey eyes indicated excessive regeneration of the trabecular meshwork, casting doubt on the efficacy of external trabeculotomy and hindering its widespread adoption in clinical practice. However, more recent studies showing mild histopathological tissue responses in humans, combined with numerous clinical success stories, have led to a shift in perspective. Currently, canal opening surgeries, classified as minimally invasive glaucoma surgery (MIGS), have gained popularity. Nevertheless, distinctions from other procedures, such as canaloplasty and stenting surgeries, have sparked significant debate. Additionally, there remains a debate concerning the surgical outcomes based on the surgical method, type of glaucoma, preoperative intraocular pressure levels, effects of concurrent cataract surgeries, impacts of postoperative anterior chamber hemorrhage, effects of treatments such as SLT, and risk factors associated with the surgery.
Future Directions
Canal opening surgery currently offers good postoperative visual acuity and effective IOP reduction, making it a promising treatment for mild to moderate glaucoma. While there are several surgical methods and devices available, they are being improved annually and should be explored to become more cost-effective and user-friendly in the future.
Author Contributions
Conceptualization EC.; Resources EC.; Writing EC.; Review and Supervision TH. EC and TH contributed equally to the preparation of this manuscript and approved the submission of this paper.
Funding
We have not received any funding from a third party.
Institutional Review Board Statement
This is a review article; thus, the ethical review and approval were waived for this study.
Informed Consent Statement
The internal review board waived the need to obtain informed consent.
Data Availability Statement
Not applicable.
Acknowledgments
This review is part of a series of studies: “Clinical Debates in Minimally Invasive Glaucoma Surgery (MIGS).” For histopathological debates, please refer to the next review, “Effect of Canal Opening Surgery on Reducing Intraocular pressure from Physio-pathological Aspect”, by Hamanaka T and Chihara E. The authors extend their profound appreciation to Dr. Murrey Johnstone for generously providing valuable insights into prior physiological and histological glaucoma research endeavors. We used chat GPT to correct grammatical errors.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Kashiwagi, K.; Kogure, S.; Mabuchi, F.; Chiba, T.; Yamamoto, T.; Kuwayama, Y.; Araie, M.; Collaborative Bleb-Related Infection, I.; Treatment Study, G. Change in visual acuity and associated risk factors after trabeculectomy with adjunctive mitomycin C. Acta Ophthalmol. 2016, 94, e561-e570. [CrossRef]
- Bindlish, R.; Condon, G.P.; Schlosser, J.D.; D’Antonio, J.; Lauer, K.B.; Lehrer, R. Efficacy and safety of mitomycin-C in primary trabeculectomy: five-year follow-up. Ophthalmology. 2002, 109, 1336-1341; discussion 1341-1332. [CrossRef]
- Leber, T. Studien ueber den flussigkeitswechsel im Auge. Graefes Arch Clin Exp Ophthalmol. 1873, 19, 87-106.
- Barany, E.H.; Scotchbrook, S. Influence of testicular hyaluronidase on the resistance to flow through the angle of the anterior chamber. Acta Physiol Scand. 1954, 30, 240-248. [CrossRef]
- Barkan, O. Goniotomy for congenital glaucoma; urgent need for early diagnosis and operation. J Am Med Assoc. 1947, 133, 526-533. [CrossRef]
- Barkan, O. GONIOTOMY FOR THE RELIEF OF CONGENITAL GLAUCOMA. Br J Ophthalmol. 1948, 32, 701-728. [CrossRef]
- SMITH, R. A new technique for opening the canal of Schlemm. Preliminary report. Br J Ophthalmol. 1960, 44, 370-373. [CrossRef]
- BURIAN, H.M. A case of Marfan’s syndrome with bilateral glaucoma. With description of a new type of operation for developmental glaucoma (trabeculotomy ab externo). Am J Ophthalmol. 1960, 50, 1187-1192. https://www.ncbi.nlm.nih.gov/pubmed/14448551.
- Smith, R. The comparison between a group of drainage operations and trabeculotomy, after a follow-up of five years. Trans Ophthalmol Soc U K (1962). 1970, 89, 511-518. https://www.ncbi.nlm.nih.gov/pubmed/5276683.
- Harms H, D.R. Trabeculotomy, Results and problems. Advances Ophthalmol. 1970, 22, 121-131.
- Harms, H.; Dannheim, R. Epicritical consideration of 300 cases of trabeculotomy ’ab externo’. Trans Ophthalmol Soc U K. 1970, 89, 491-499. https://www.ncbi.nlm.nih.gov/pubmed/5276680.
- Dannheim, R.; Harms, H. [Technic, success and mode of action of trabeculotomy]. Klin Monbl Augenheilkd. 1969, 155, 630-637. https://www.ncbi.nlm.nih.gov/pubmed/5369354.
- Dannheim, R. Symposium: microsurgery of the outflow channels. Trabeculotomy. Trans Am Acad Ophthalmol Otolaryngol. 1972, 76, 375-383. https://www.ncbi.nlm.nih.gov/pubmed/4582681.
- Grant, W.M. Symposium: microsurgery of the outflow channels. Laboratory research. Trans Am Acad Ophthalmol Otolaryngol. 1972, 76, 398-404. https://www.ncbi.nlm.nih.gov/pubmed/4200564.
- Spencer, W.H. Symposium: microsurgery of the outflow channels. Histologic evaluation of microsurgical glaucoma techniques. Trans Am Acad Ophthalmol Otolaryngol. 1972, 76, 389-397. https://www.ncbi.nlm.nih.gov/pubmed/4270305.
- Leuenberger, P.M. [Trabeculectomy and trabeculotomy (author’s transl)]. Klin Monbl Augenheilkd. 1978, 172, 555-561. https://www.ncbi.nlm.nih.gov/pubmed/651232.
- Gillies, W.E. Trabeculotomy in pseudoexfoliation of the lens capsule. Br J Ophthalmol. 1977, 61, 297-298. [CrossRef]
- Lamers, W.P. Trabeculotomy ab externo as operative treatment of glaucoma simplex. Ophthalmologica. 1972, 165, 509-512. [CrossRef]
- Dannheim, R. [The influence of healing on the long-term effect of trabeculotomy in primary open angle glaucoma (author’s transl)]. Klin Monbl Augenheilkd. 1978, 172, 27-38. https://www.ncbi.nlm.nih.gov/pubmed/628180.
- Dannheim, R.; Kubin, M. [Tonographic and tonometric aqueous humor outflow tests after trabeculotomy (author’s transl)]. Albrecht Von Graefes Arch Klin Exp Ophthalmol. 1977, 201, 277-287. [CrossRef]
- Mackensen, G.; Grehn, F. [Surgical indications in glaucoma]. Klin Monbl Augenheilkd. 1985, 187, 167-169. [CrossRef]
- Dannheim, R.; Bárány, E.H. The effect of trabeculotomy in normal eyes of rhesus and cynomolgus monkeys studied by anterior chamber perfusion. Doc Ophthalmol. 1969, 26, 90-107. [CrossRef]
- Dannheim, R.; van der Zypen, E. [Clinical, functional and electron microscopy studies on the regenerative ability of the iridocorneal angle region of primate eyes following trabeculotomy]. Albrecht Von Graefes Arch Klin Exp Ophthalmol. 1972, 184, 222-247. [CrossRef]
- Luntz, M.H.; Livingston, D.G. Trabeculotomy ab externo and trabeculectomy in congenital and adult-onset glaucoma. Am J Ophthalmol. 1977, 83, 174-179. [CrossRef]
- Minckler, D.S.; Baerveldt, G.; Alfaro, M.R.; Francis, B.A. Clinical results with the Trabectome for treatment of open-angle glaucoma. Ophthalmology. 2005, 112, 962-967. [CrossRef]
- Shaffer, R.N.; Hoskins, H.D. Montgomery lecture. Goniotomy in the treatment of isolated trabeculodysgenesis (primary congenital [infantile] developmental glaucoma). Trans Ophthalmol Soc U K (1962). 1983, 103 ( Pt 6), 581-585. https://www.ncbi.nlm.nih.gov/pubmed/6592859.
- McPherson, S.D. Results of external trabeculotomy. Am J Ophthalmol. 1973, 76, 918-920. https://www.ncbi.nlm.nih.gov/pubmed/4759851.
- McPherson, S.D.; McFarland, D. External trabeculotomy for developmental glaucoma. Ophthalmology. 1980, 87, 302-305. [CrossRef]
- McPherson, S.D.; Berry, D.P. Goniotomy vs external trabeculotomy for developmental glaucoma. Am J Ophthalmol. 1983, 95, 427-431. [CrossRef]
- Rothkoff, L.; Blumenthal, M.; Biedner, B. Trabeculotomy in late onset congenital glaucoma. Br J Ophthalmol. 1979, 63, 38-39. [CrossRef]
- Anderson, D.R. Trabeculotomy compared to goniotomy for glaucoma in children. Ophthalmology. 1983, 90, 805-806. [CrossRef]
- Quigley, H.A. Childhood glaucoma: results with trabeculotomy and study of reversible cupping. Ophthalmology. 1982, 89, 219-226. [CrossRef]
- Dascotte, J.C.; Asseman, R.; François, P.; Houliez, T.; Huron, J.C.; Castier, P.; Rouland, J.F. [Surgical treatment of congenital glaucoma. Long-term results]. J Fr Ophtalmol. 1991, 14, 229-233. https://www.ncbi.nlm.nih.gov/pubmed/1955649.
- ElSheikha, O.Z.; Abdelhakim, M.A.S.E.; Elhilali, H.M.; Kassem, R.R. Is viscotrabeculotomy superior to conventional trabeculotomy in the management of Egyptian infants with congenital glaucoma? Acta Ophthalmol. 2015, 93, e366-e371. [CrossRef]
- Temkar, S.; Gupta, S.; Sihota, R.; Sharma, R.; Angmo, D.; Pujari, A.; Dada, T. Illuminated microcatheter circumferential trabeculotomy versus combined trabeculotomy-trabeculectomy for primary congenital glaucoma: a randomized controlled trial. Am J Ophthalmol. 2015, 159, 490-497.e492. [CrossRef]
- El Sayed, Y.; Gawdat, G. Two-year results of microcatheter-assisted trabeculotomy in paediatric glaucoma: a randomized controlled study. Acta Ophthalmol. 2017, 95, e713-e719. [CrossRef]
- Shakrawal, J.; Bali, S.; Sidhu, T.; Verma, S.; Sihota, R.; Dada, T. Randomized Trial on Illuminated-Microcatheter Circumferential Trabeculotomy Versus Conventional Trabeculotomy in Congenital Glaucoma. Am J Ophthalmol. 2017, 180, 158-164. [CrossRef]
- Elwehidy, A.S.; Hagras, S.M.; Bayoumi, N.; AbdelGhafar, A.E.; Badawi, A.E. Five-year results of viscotrabeculotomy versus conventional trabeculotomy in primary congenital glaucoma: A randomized controlled study. Eur J Ophthalmol. 2021, 31, 786-795. [CrossRef]
- Elwehidy, A.S.; Bayoumi, N.H.L.; Abd Elfattah, D.; Hagras, S.M. Surgical Outcomes of Visco-Circumferential-Suture-Trabeculotomy Versus Rigid Probe Trabeculotomy in Primary Congenital Glaucoma: A 3-Year Randomized Controlled Study. J Glaucoma. 2022, 31, 48-53. [CrossRef]
- Grover, D.S.; Smith, O.; Fellman, R.L.; Godfrey, D.G.; Butler, M.R.; Montes de Oca, I.; Feuer, W.J. Gonioscopy assisted transluminal trabeculotomy: an ab interno circumferential trabeculotomy for the treatment of primary congenital glaucoma and juvenile open angle glaucoma. Br J Ophthalmol. 2015, 99, 1092-1096. [CrossRef]
- Aktas, Z.; Ozmen, M.C.; Ozdemir Zeydanli, E.; Oral, M.; Eskalen, O. Efficacy and Safety of Gonioscopy-Assisted Transluminal Trabeculotomy for Primary Congenital Glaucoma. J Glaucoma. 2023, 32, 497-500. [CrossRef]
- Harvey, M.M.; Schmitz, J.W. Use of ab interno Kahook Dual Blade trabeculectomy for treatment of primary congenital glaucoma. Eur J Ophthalmol. 2020, 30, NP16-NP20. [CrossRef]
- Elhilali, H.M.; El Sayed, Y.M.; Elhusseiny, A.M.; Gawdat, G.I. Kahook Dual Blade Ab-interno Trabeculectomy Compared With Conventional Goniotomy in the Treatment of Primary Congenital Glaucoma: 1-Year Results. J Glaucoma. 2021, 30, 526-531. [CrossRef]
- Nagata, M. Microsurgery. Trabeculotomy ab externo. Folia Ophthalmol Jpn. 1975, 26, 245-262.
- Nagata, M. Glaucoma surgery. Its indications and prognosis. Folia Ophthalmol Jpn. 1981, 32, 395-407.
- Weder, W.; Lissel, U.; Stöltzing, M. Complications and results after trabeculotomy. Dev Ophthalmol. 1987, 13, 78-84. [CrossRef]
- Quaranta, L.; Hitchings, R.A.; Quaranta, C.A. Ab-interno goniotrabeculotomy versus mitomycin C trabeculectomy for adult open-angle glaucoma: a 2-year randomized clinical trial. Ophthalmology. 1999, 106, 1357-1362. [CrossRef]
- Kubota, T.; Touguri, I.; Onizuka, N.; Matsuura, T. Phacoemulsification and intraocular lens implantation combined with trabeculotomy for open-angle glaucoma and coexisting cataract. Ophthalmologica. 2003, 217, 204-207. [CrossRef]
- Hoffmann, E.; Schwenn, O.; Karallus, M.; Krummenauer, F.; Grehn, F.; Pfeiffer, N. Long-term results of cataract surgery combined with trabeculotomy. Graefes Arch Clin Exp Ophthalmol. 2002, 240, 2-6. [CrossRef]
- Mizoguchi, T.; Kuroda, S.; Terauchi, H.; Nagata, M. Trabeculotomy combined with phacoemulsification and implantation of intraocular lens for primary open-angle glaucoma. Semin Ophthalmol. 2001, 16, 162-167. [CrossRef]
- Tanito M, O.A., Chihara E. Surgical Outcome of Combined Trabeculotomy and Cataract Surgery. J Glaucoma. 2001, 10, 302-308.
- Honjo, M.; Tanihara, H.; Inatani, M.; Honda, Y.; Ogino, N.; Ueno, S.; Negi, A.; Ichioka, H.; Mizoguchi, T.; Matsumura, M.; et al. Phacoemulsification, intraocular lens implantation, and trabeculotomy to treat pseudoexfoliation syndrome. J Cataract Refract Surg. 1998, 24, 781-786. [CrossRef]
- Saito, Y.; Oo, A.; Okamoto, S.; Kuwayama, Y.; Nakatani, H. Glaucoma triple procedure comprising trabeculotomy with a fornix-based scleral flap. Doc Ophthalmol. 1995, 89, 393-400. [CrossRef]
- Wada, Y.; Nakatsu, A.; Kondo, T. Long-term results of trabeculotomy ab externo. Ophthalmic Surg. 1994, 25, 317-320. https://www.ncbi.nlm.nih.gov/pubmed/8058264.
- Tanihara, H.; Negi, A.; Akimoto, M.; Terauchi, H.; Okudaira, A.; Kozaki, J.; Takeuchi, A.; Nagata, M. Surgical effects of trabeculotomy ab externo on adult eyes with primary open angle glaucoma and pseudoexfoliation syndrome. Arch Ophthalmol. 1993, 111, 1653-1661. [CrossRef]
- Chihara, E.; Nishida, A.; Kodo, M.; Yoshimura, N.; Matsumura, M.; Yamamoto, M.; Tsukada, T. Trabeculotomy ab externo: an alternative treatment in adult patients with primary open-angle glaucoma. Ophthalmic Surg. 1993, 24, 735-739. https://www.ncbi.nlm.nih.gov/pubmed/8290211.
- Tanihara, H.; Negi, A.; Akimoto, M.; Nagata, M. Long-term surgical results of combined trabeculotomy ab externo and cataract extraction. Ophthalmic Surg. 1995, 26, 316-324. https://www.ncbi.nlm.nih.gov/pubmed/8532283.
- Tanihara, H.; Honjo, M.; Inatani, M.; Honda, Y.; Ogino, N.; Ueno, S.; Negi, A.; Ichioka, H.; Mizoguchi, T.; Matsumura, M.; et al. Trabeculotomy combined with phacoemulsification and implantation of an intraocular lens for the treatment of primary open-angle glaucoma and coexisting cataract. Ophthalmic Surg Lasers. 1997, 28, 810-817. https://www.ncbi.nlm.nih.gov/pubmed/9336773.
- Tanito, M.; Ohira, A.; Chihara, E. Factors leading to reduced intraocular pressure after combined trabeculotomy and cataract surgery. J Glaucoma. 2002, 11, 3-9. [CrossRef]
- Chihara, E. Trends in the National Ophthalmological Healthcare Focusing on Cataract, Retina, and Glaucoma Over 15 Years in Japan. Clin Ophthalmol. 2023, 17, 3131-3148. [CrossRef]
- Minckler, D.; Baerveldt, G.; Ramirez, M.A.; Mosaed, S.; Wilson, R.; Shaarawy, T.; Zack, B.; Dustin, L.; Francis, B. Clinical results with the Trabectome, a novel surgical device for treatment of open-angle glaucoma. Trans Am Ophthalmol Soc. 2006, 104, 40-50. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1809927/pdf/1545-6110_v104_p040.pdf.
- Godfrey, D.G.; Fellman, R.L.; Neelakantan, A. Canal surgery in adult glaucomas. Curr Opin Ophthalmol. 2009, 20, 116-121. [CrossRef]
- Ito, S.; Nishikawa, M.; Tokura, T.; Yamane, A.; Yamagishi, K.; Miki, H. [Histopathological study of trabecular meshwork after trabeculotomy in monkeys]. Nippon Ganka Gakkai Zasshi. 1994, 98, 811-819. https://www.ncbi.nlm.nih.gov/pubmed/7976840.
- Amari, Y.; Hamanaka, T.; Futa, R. Pathologic investigation failure of trabeculotomy. J Glaucoma. 2015, 24, 316-322. [CrossRef]
- Tsutsui, A.; Hamanaka, T.; Manabe, K.; Kaidzu, S.; Kumasaka, T.; Tanito, M. Histologic Findings of Trabecular Meshwork and Schlemm’s Canal After Microhook Ab Interno Trabeculotomy. J Glaucoma. 2021, 30, 203-205. [CrossRef]
- Hamanaka, T.; Chin, S.; Shinmei, Y.; Sakurai, T.; Tanito, M.; Kijima, R.; Tsutsui, A.; Ueno, Y.; Ishida, N.; Ueda, T.; et al. Histological analysis of trabeculotomy - An investigation on the intraocular pressure lowering mechanism. Exp Eye Res. 2022, 219, 109079. [CrossRef]
- d’Epinay, S.L.; Remé, C. [Histopathological aspects of the surgical treatment of congenital glaucoma]. Klin Monbl Augenheilkd. 1980, 176, 566-568. [CrossRef]
- Dietlein, T.S.; Jacobi, P.C.; Lüke, C.; Krieglstein, G.K. Morphological variability of the trabecular meshwork in glaucoma patients: implications for non-perforating glaucoma surgery. Br J Ophthalmol. 2000, 84, 1354-1359. [CrossRef]
- al., C.E.e. Trabeculotomy Ab Externo: An Alternative Treatment in Adult Patients With Primary Open Angle Glaucoma. Ophthalmic Surg. 1993, 24.
- Espinoza, G.; Rodriguez-Una, I.; Pedraza-Concha, A. A Case of Bilateral Delayed-onset Hyphema Following Pupil Dilation after Gonioscopy-assisted Transluminal Trabeculotomy. J Curr Glaucoma Pract. 2020, 14, 72-75. [CrossRef]
- Ahuja, Y.; Malihi, M.; Sit, A.J. Delayed-onset symptomatic hyphema after ab interno trabeculotomy surgery. Am J Ophthalmol. 2012, 154, 476-480.e472. [CrossRef]
- Tanenbaum, R.E.; Xiao, J.; Qiu, M. Reflux hyphema from transient hypotony after Ozurdex® in eyes with prior GATT. Am J Ophthalmol Case Rep. 2023, 32, 101939. [CrossRef]
- Knape, R.M.; Smith, M.F. Anterior chamber blood reflux during trabeculectomy in an eye with previous trabectome surgery. J Glaucoma. 2010, 19, 499-500. [CrossRef]
- Tanito, M. Delayed-Onset, Recurrent Hyphema after Microhook ab interno Trabeculotomy. Case Rep Ophthalmol. 2021, 12, 57-61. [CrossRef]
- Fellman, R.L.; Feuer, W.J.; Grover, D.S. Episcleral Venous Fluid Wave Correlates with Trabectome Outcomes: Intraoperative Evaluation of the Trabecular Outflow Pathway. Ophthalmology. 2015, 122, 2385-2391.e2381. [CrossRef]
- Cha, E.D.K.; Xu, J.; Gong, L.; Gong, H. Variations in active outflow along the trabecular outflow pathway. Exp Eye Res. 2016, 146, 354-360. [CrossRef]
- Vries, d. De Zichtbare Afvoer Van Het Kammerwater.; Drukkerij Kinsbergen: Amsterdam, 1947.
- Ueda, T.; Suzumura, H.; Johnstone, M.; Uda, S.; Yoshida, K. The Correlation Between Aqueous Humor Flow and IOP Before and After Trabectome: Developing a Grading System to Quantify Flow. Ophthalmol Ther. 2018, 7, 133-143. [CrossRef]
- Stepanik, J. Measuring velocity of flow in aqueous veins. Am J Ophthalmol. 1954, 37, 918-922.
- Chihara, E.; Chihara, T. Turn Back Elevation of Once Reduced IOP After Trabeculotomy Ab Externo and Kahook Dual Blade Surgeries Combined with Cataract Surgery. Clin Ophthalmol. 2020, 14, 4359-4368. [CrossRef]
- Capitena Young, C.E.; Ammar, D.A.; Seibold, L.K.; Pantcheva, M.B.; SooHoo, J.R.; Kahook, M.Y. Histopathologic Examination of Trabecular Meshwork Changes After Trabecular Bypass Stent Implantation. J Glaucoma. 2018, 27, 606-609. [CrossRef]
- Beck, A.D.; Lynch, M.G. 360 degrees trabeculotomy for primary congenital glaucoma. Arch Ophthalmol. 1995, 113, 1200-1202. [CrossRef]
- Chin, S.; Nitta, T.; Shinmei, Y.; Aoyagi, M.; Nitta, A.; Ohno, S.; Ishida, S.; Yoshida, K. Reduction of intraocular pressure using a modified 360-degree suture trabeculotomy technique in primary and secondary open-angle glaucoma: a pilot study. J Glaucoma. 2012, 21, 401-407. [CrossRef]
- Grover, D.S.; Godfrey, D.G.; Smith, O.; Feuer, W.J.; Montes de Oca, I.; Fellman, R.L. Gonioscopy-assisted transluminal trabeculotomy, ab interno trabeculotomy: technique report and preliminary results. Ophthalmology. 2014, 121, 855-861. [CrossRef]
- Sato, T.; Hirata, A.; Mizoguchi, T. Outcomes of 360° suture trabeculotomy with deep sclerectomy combined with cataract surgery for primary open angle glaucoma and coexisting cataract. Clin Ophthalmol. 2014, 8, 1301-1310. [CrossRef]
- Verner-Cole, E.A.; Ortiz, S.; Bell, N.P.; Feldman, R.M. Subretinal suture misdirection during 360 degrees suture trabeculotomy. Am J Ophthalmol. 2006, 141, 391-392. [CrossRef]
- Sarkisian, S.R.; Mathews, B.; Ding, K.; Patel, A.; Nicek, Z. 360° ab-interno trabeculotomy in refractory primary open-angle glaucoma. Clin Ophthalmol. 2019, 13, 161-168. [CrossRef]
- Baykara, M.; Poroy, C.; Erseven, C. Surgical outcomes of combined gonioscopy-assisted transluminal trabeculotomy and cataract surgery. Indian J Ophthalmol. 2019, 67, 505-508. [CrossRef]
- Takata, M.; Ishikawa, H.; Ikeda, T.; Gomi, F. Conventional Trabeculotomy versus Gonioscopy-Assisted Transluminal Trabeculotomy: A Retrospective Cohort Study. J Clin Med. 2021, 11. [CrossRef]
- Yin, P.; Li, J.; Shi, Y.; Cao, K.; Han, Y.; Wang, H.; Liu, H.; Xin, C.; Wang, Y.; Oatts, J.; et al. Ab interno canaloplasty versus gonioscopy-assisted transluminal trabeculotomy in open-angle glaucoma: a randomised controlled trial. Br J Ophthalmol. 2023. [CrossRef]
- Liu, W.W.; Petkovsek, D.; Shalaby, W.S.; Arbabi, A.; Moster, M.R. Four-year Surgical Outcomes of Gonioscopy-assisted Transluminal Trabeculotomy in Patients with Open-Angle Glaucoma. Ophthalmol Glaucoma. 2023, 6, 387-394. [CrossRef]
- Kijima, R.; Shinmei, Y.; Chin, S.; Kanaya, R.; Shinkai, A.; Ohguchi, T.; Namba, K.; Ishida, S. Long-term Outcomes of Modified 360-Degree Suture Trabeculotomy for Uveitic Glaucoma Compared With Primary Open Angle Glaucoma. J Glaucoma. 2022, 31, 682-688. [CrossRef]
- Chen, J.; Wang, Y.E.; Quan, A.; Grajewski, A.; Hodapp, E.; Vanner, E.A.; Chang, T.C. Risk Factors for Complications and Failure after Gonioscopy-Assisted Transluminal Trabeculotomy in a Young Cohort. Ophthalmol Glaucoma. 2020, 3, 190-195. [CrossRef]
- Hepşen, İ.; Güler, E.; Yalçin, N.G.; Kumova, D.; Aktaş, Z.P. Modified 360-degree Suture Trabeculotomy for Pseudoexfoliation Glaucoma: 12-Month Results. J Glaucoma. 2016, 25, e408-412. [CrossRef]
- Maeda, M.; Watanabe, M.; Ichikawa, K. Evaluation of trabectome in open-angle glaucoma. J Glaucoma. 2013, 22, 205-208. [CrossRef]
- Ahuja, Y.; Ma Khin Pyi, S.; Malihi, M.; Hodge, D.O.; Sit, A.J. Clinical results of ab interno trabeculotomy using the trabectome for open-angle glaucoma: the Mayo Clinic series in Rochester, Minnesota. Am J Ophthalmol. 2013, 156, 927-935.e922. [CrossRef]
- Mizoguchi, T.; Nishigaki, S.; Sato, T.; Wakiyama, H.; Ogino, N. Clinical results of Trabectome surgery for open-angle glaucoma. Clin Ophthalmol. 2015, 9, 1889-1894. [CrossRef]
- Lee, J.W.Y.; Yick, D.W.F.; Tsang, S.; Yuen, C.Y.F.; Lai, J.S.M. Efficacy and Safety of Trabectome Surgery in Chinese Open-Angle Glaucoma. Medicine (Baltimore). 2016, 95, e3212. [CrossRef]
- Wecker, T.; Neuburger, M.; Bryniok, L.; Bruder, K.; Luebke, J.; Anton, A.; Jordan, J.F. Ab Interno Trabeculectomy With the Trabectome as a Valuable Therapeutic Option for Failed Filtering Blebs. J Glaucoma. 2016, 25, 758-762. [CrossRef]
- Kerr, N.M.; Wang, J.; Barton, K. Minimally invasive glaucoma surgery as primary stand-alone surgery for glaucoma. Clin Exp Ophthalmol. 2017, 45, 393-400. [CrossRef]
- Ngai, P.; Kim, G.; Chak, G.; Lin, K.; Maeda, M.; Mosaed, S. Outcome of primary trabeculotomy ab interno (Trabectome) surgery in patients with steroid-induced glaucoma. Medicine (Baltimore). 2016, 95, e5383. [CrossRef]
- Pahlitzsch, M.; Gonnermann, J.; Maier, A.B.; Bertelmann, E.; Klamann, M.K.; Erb, C. Modified goniotomy as an alternative to trabectome in primary open angle glaucoma and pseudoexfoliation glaucoma: 1 year results. Can J Ophthalmol. 2017, 52, 92-98. [CrossRef]
- Kurji, K.; Rudnisky, C.J.; Rayat, J.S.; Arora, S.; Sandhu, S.; Damji, K.F.; Dorey, M.W. Phaco-trabectome versus phaco-iStent in patients with open-angle glaucoma. Can J Ophthalmol. 2017, 52, 99-106. [CrossRef]
- Roy, P.; Loewen, R.T.; Dang, Y.; Parikh, H.A.; Bussel, I.I.; Loewen, N.A. Stratification of phaco-trabectome surgery results using a glaucoma severity index in a retrospective analysis. BMC Ophthalmol. 2017, 17, 30. [CrossRef]
- Hashemian, S.J.; Miraftabi, A.; Jafari, M.E.; Hemami, M.R. Combined cataract extraction and trabeculotomy by the internal approach for coexisting cataract and open-angle glaucoma. J Curr Ophthalmol. 2017, 29, 17-22. [CrossRef]
- Akil, H.; Chopra, V.; Huang, A.; Loewen, N.; Noguchi, J.; Francis, B.A. Clinical results of ab interno trabeculotomy using the Trabectome in patients with pigmentary glaucoma compared to primary open angle glaucoma. Clin Exp Ophthalmol. 2016, 44, 563-569. [CrossRef]
- Akil, H.; Chopra, V.; Huang, A.S.; Swamy, R.; Francis, B.A. Short-Term Clinical Results of Ab Interno Trabeculotomy Using the Trabectome with or without Cataract Surgery for Open-Angle Glaucoma Patients of High Intraocular Pressure. J Ophthalmol. 2017, 2017, 8248710. [CrossRef]
- Kostanyan, T.; Shazly, T.; Kaplowitz, K.B.; Wang, S.Z.; Kola, S.; Brown, E.N.; Loewen, N.A. Longer-term Baerveldt to Trabectome glaucoma surgery comparison using propensity score matching. Graefes Arch Clin Exp Ophthalmol. 2017, 255, 2423-2428. [CrossRef]
- Pahlitzsch, M.; Davids, A.M.; Zorn, M.; Torun, N.; Winterhalter, S.; Maier, A.B.; Klamann, M.K.; Bertelmann, E. Three-year results of ab interno trabeculectomy (Trabectome): Berlin study group. Graefes Arch Clin Exp Ophthalmol. 2018, 256, 611-619. [CrossRef]
- Esfandiari, H.; Shazly, T.A.; Waxman, S.A.; Kola, S.; Kaplowitz, K.B.; Brown, E.N.; Loewen, N.A. Similar Performance of Trabectome and Ahmed Glaucoma Devices in a Propensity Score-matched Comparison. J Glaucoma. 2018, 27, 490-495. [CrossRef]
- Dang, Y.L.; Cen, Y.J.; Hong, Y.; Huang, P.; Wang, N.L.; Wang, C.; Zhang, C.; Group, C.T.S. Safety and Efficiency of Trabectome-mediated Trabecular Meshwork Ablation for Chinese Glaucoma Patients: A Two-year, Retrospective, Multicentre Study. Chin Med J (Engl). 2018, 131, 420-425. [CrossRef]
- Dang, Y.L.; Wang, X.; Dai, W.W.; Huang, P.; Loewen, N.A.; Zhang, C.; China Trabectome Study Group, I.t.T.S.G. Two-year outcomes of ab interno trabeculectomy with the Trabectome for Chinese primary open angle glaucoma: a retrospective multicenter study. Int J Ophthalmol. 2018, 11, 945-950. [CrossRef]
- Nazarali, S.A.; Damji, K.F. Ab interno trabeculectomy with Trabectome: outcomes in African American versus Caucasian patients. Can J Ophthalmol. 2018, 53, 361-364. [CrossRef]
- Arora, S.; Maeda, M.; Francis, B.; Sit, A.J.; Mosaed, S.; Nazarali, S.; Damji, K.F. Efficacy and safety of ab interno trabeculectomy in juvenile open-angle glaucoma. Can J Ophthalmol. 2018, 53, 482-486. [CrossRef]
- Ting, J.L.M.; Rudnisky, C.J.; Damji, K.F. Prospective randomized controlled trial of phaco-trabectome versus phaco-trabeculectomy in patients with open angle glaucoma. Can J Ophthalmol. 2018, 53, 588-594. [CrossRef]
- Avar, M.; Jordan, J.F.; Neuburger, M.; Engesser, D.; Lübke, J.; Anton, A.; Wecker, T. Long-term follow-up of intraocular pressure and pressure-lowering medication in patients after ab-interno trabeculectomy with the Trabectome. Graefes Arch Clin Exp Ophthalmol. 2019, 257, 997-1003. [CrossRef]
- Esfandiari, H.; Taubenslag, K.; Shah, P.; Goyal, S.; Weiner, A.J.; Severson, M.L.; Weiner, A.; Grover, D.S.; Bussel, I.I.; Loewen, N.A. Two-year data comparison of ab interno trabeculectomy and trabecular bypass stenting using exact matching. J Cataract Refract Surg. 2019, 45, 608-614. [CrossRef]
- Bendel, R.E.; Patterson, M.T. Long-term Effectiveness of Trabectome (Ab-interno Trabeculectomy) Surgery. J Curr Glaucoma Pract. 2018, 12, 119-124. [CrossRef]
- Kasahara, M.; Shoji, N. Effectiveness and limitations of minimally invasive glaucoma surgery targeting Schlemm’s canal. Jpn J Ophthalmol. 2021, 65, 6-22. [CrossRef]
- Strzalkowska, A.; Strzalkowski, P.; Al Yousef, Y.; Grehn, F.; Hillenkamp, J.; Loewen, N.A. Exact matching of trabectome-mediated ab interno trabeculectomy to conventional trabeculectomy with mitomycin C followed for 2 years. Graefes Arch Clin Exp Ophthalmol. 2021, 259, 963-970. [CrossRef]
- Tojo, N.; Hayashi, A. The Outcomes of Trabectome Surgery in Patients with Low, Middle, and High Preoperative Intraocular Pressure. Clin Ophthalmol. 2020, 14, 4099-4108. [CrossRef]
- Wons, J.; Mihic, N.; B Pfister, I.; Anastasi, S.; Garweg, J.G.; Halberstadt, M. Effect of Preoperative Intraocular Pressure in Patients with and without Intolerance to Their IOP-Lowering Medication on the Outcome of Trabectome Surgery. Clin Ophthalmol. 2021, 15, 1851-1860. [CrossRef]
- Abtahi, M.; Rudnisky, C.J.; Nazarali, S.; Damji, K.F. Incidence of steroid response in microinvasive glaucoma surgery with trabecular microbypass stent and ab interno trabeculectomy. Can J Ophthalmol. 2022, 57, 167-174. [CrossRef]
- Wang, Y.; Liang, Z.Q.; Zhang, Y.; Hennein, L.; Han, Y.; Wu, H.J. Efficacy and safety of phacoemulsification plus goniosynechialysis and trabectome in patients with primary angle-closure glaucoma. Sci Rep. 2021, 11, 13921. [CrossRef]
- Sharma, O.; Abdulla, D.; King, A.; Chakrabarti, M.; Sharma, T. Role of minimally invasive glaucoma surgery in the management of chronic open-angle glaucoma. Sci Rep. 2021, 11, 21432. [CrossRef]
- Widder, R.A.; Hild, M.; Dietlein, T.S.; Kühnrich, P.; Rennings, C.; Szumniak, A.; Lappas, A.; Roessler, G.F. Trabectome, trabecular aspiration and phacoemulsification in a triple procedure for treating exfoliation glaucoma: A long-term follow-up. Eur J Ophthalmol. 2021, 31, 2432-2438. [CrossRef]
- Tanito, M.; Matsuo, M. trabeculotomy-related glaucoma surgeries. Taiwan J Ophthalmol. 2019, 9, 67-71. [CrossRef]
- Mori, S.; Tanito, M.; Shoji, N.; Yokoyama, Y.; Kameda, T.; Shoji, T.; Mizoue, S.; Saito, Y.; Ishida, K.; Ueda, T.; et al. Noninferiority of Microhook to Trabectome: Trabectome versus Ab Interno Microhook Trabeculotomy Comparative Study (Tram Trac Study). Ophthalmol Glaucoma. 2022, 5, 452-461. [CrossRef]
- Dubey, S.; Bansal, T.; Garg, P.; Hegde, A.; Das, R.; Rekha, P.D. Outcomes of ab-interno irrigating goniectomy with trabectome in primary and secondary glaucoma from a single center in India. Indian J Ophthalmol. 2022, 70, 3569-3574. [CrossRef]
- Fliney, G.D.; Kim, E.; Sarwana, M.; Wong, S.; Tai, T.Y.T.; Liu, J.; Sarrafpour, S.; Chadha, N.; Teng, C.C. Kahook Dual Blade versus Trabectome (KVT): Comparing Outcomes in Combination with Cataract Surgery. Clin Ophthalmol. 2023, 17, 145-154. [CrossRef]
- Un, Y.; Buyukavsar, C.; Comerter, D.; Sonmez, M.; Yildirim, Y. Long-Term Clinical Results of Trabectome Surgery in Turkish Patients with Primary Open Angle Glaucoma and Pseudoexfoliative Glaucoma. Beyoglu Eye J. 2023, 8, 14-20. [CrossRef]
- Weber, C.; Ludwig, E.; Hundertmark, S.; Brinkmann, C.K.; Petrak, M.; Holz, F.G.; Mercieca, K. Five-Year Clinical Outcomes of Inferior Quadrant Trabectome Surgery for Open Angle Glaucoma. J Glaucoma. 2023, 32, 480-488. [CrossRef]
- Kitamura, K.; Fukuda, Y.; Hasebe, Y.; Matsubara, M.; Kashiwagi, K. Mid-Term Results of Ab Interno Trabeculectomy among Japanese Glaucoma Patients. J Clin Med. 2023, 12. [CrossRef]
- Garweg, R.A.; Pfister, I.B.; Schild, C.; Halberstadt, M.; Straessle, K.; Anastasi, S.; Garweg, J.G. IOP-lowering and drug-sparing effects of trabectome surgery with or without cyclodialysis ab interno. Graefes Arch Clin Exp Ophthalmol. 2023, 261, 2917-2925. [CrossRef]
- Kono, Y.; Kasahara, M.; Hirasawa, K.; Tsujisawa, T.; Kanayama, S.; Matsumura, K.; Morita, T.; Shoji, N. Long-term clinical results of trabectome surgery in patients with open-angle glaucoma. Graefes Arch Clin Exp Ophthalmol. 2020, 258, 2467-2476. [CrossRef]
- Kono, Y.; Kasahara, M.; Sato, N.; Yokozeki, Y.; Hirasawa, K.; Shoji, N. Comparison of Short-term Visual Acuity Changes After Trabeculotomy ab Interno Using Trabectome and Trabeculectomy ab Externo. Ophthalmol Glaucoma. 2023, 6, 609-615. [CrossRef]
- Dorairaj, S.K.; Seibold, L.K.; Radcliffe, N.M.; Aref, A.A.; Jimenez-Román, J.; Lazcano-Gomez, G.S.; Darlington, J.K.; Mansouri, K.; Berdahl, J.P. 12-Month Outcomes of Goniotomy Performed Using the Kahook Dual Blade Combined with Cataract Surgery in Eyes with Medically Treated Glaucoma. Adv Ther. 2018, 35, 1460-1469. [CrossRef]
- Greenwood, M.D.; Seibold, L.K.; Radcliffe, N.M.; Dorairaj, S.K.; Aref, A.A.; Román, J.J.; Lazcano-Gomez, G.S.; Darlington, J.K.; Abdullah, S.; Jasek, M.C.; et al. Goniotomy with a single-use dual blade: Short-term results. J Cataract Refract Surg. 2017, 43, 1197-1201. [CrossRef]
- Mansoori, T. Kahook Dual Blade (KDB) in Severe and Refractory Glaucoma. J Glaucoma. 2019, 28, e89. [CrossRef]
- Le, C.; Kazaryan, S.; Hubbell, M.; Zurakowski, D.; Ayyala, R.S. Surgical Outcomes of Phacoemulsification Followed by iStent Implantation Versus Goniotomy With the Kahook Dual Blade in Patients With Mild Primary Open-angle Glaucoma With a Minimum of 12-Month Follow-up. J Glaucoma. 2019, 28, 411-414. [CrossRef]
- Salinas, L.; Chaudhary, A.; Berdahl, J.P.; Lazcano-Gomez, G.S.; Williamson, B.K.; Dorairaj, S.K.; Seibold, L.K.; Smith, S.; Aref, A.A.; Darlington, J.K.; et al. Goniotomy Using the Kahook Dual Blade in Severe and Refractory Glaucoma: 6-Month Outcomes. J Glaucoma. 2018, 27, 849-855. [CrossRef]
- Salinas, L.; Chaudhary, A.; Berdahl, J.P.; Lazcano-Gomez, G.S.; Williamson, B.K.; Dorairaj, S.K.; Seibold, L.K.; Smith, S.; Aref, A.A.; Darlington, J.K.; et al. Response: Goniotomy Using the Kahook Dual Blade in Severe and Refractory Glaucoma: 6-Month Outcomes. J Glaucoma. 2019, 28, e89. [CrossRef]
- Hirabayashi, M.T.; King, J.T.; Lee, D.; An, J.A. Outcome of phacoemulsification combined with excisional goniotomy using the Kahook Dual Blade in severe glaucoma patients at 6 months. Clin Ophthalmol. 2019, 13, 715-721. [CrossRef]
- Kornmann, H.L.; Fellman, R.L.; Feuer, W.J.; Butler, M.R.; Godfrey, D.G.; Smith, O.U.; Emanuel, M.E.; Grover, D.S. Early Results of Goniotomy with the Kahook Dual Blade, a Novel Device for the Treatment of Glaucoma. Clin Ophthalmol. 2019, 13, 2369-2376. [CrossRef]
- Barry, M.; Alahmadi, M.W.; Alahmadi, M.; AlMuzaini, A.; AlMohammadi, M. The Safety of the Kahook Dual Blade in the Surgical Treatment of Glaucoma. Cureus. 2020, 12, e6682. [CrossRef]
- Wakil, S.M.; Birnbaum, F.; Vu, D.M.; McBurney-Lin, S.; ElMallah, M.K.; Tseng, H. Efficacy and safety of a single-use dual blade goniotomy: 18-month results. J Cataract Refract Surg. 2020, 46, 1408-1415. [CrossRef]
- Berdahl, J.P.; Gallardo, M.J.; ElMallah, M.K.; Williamson, B.K.; Kahook, M.Y.; Mahootchi, A.; Rappaport, L.A.; Lazcano-Gomez, G.S.; Díaz-Robles, D.; Dorairaj, S.K. Six-Month Outcomes of Goniotomy Performed with the Kahook Dual Blade as a Stand-Alone Glaucoma Procedure. Adv Ther. 2018, 35, 2093-2102. [CrossRef]
- Dorairaj, S.K.; Kahook, M.Y.; Williamson, B.K.; Seibold, L.K.; ElMallah, M.K.; Singh, I.P. A multicenter retrospective comparison of goniotomy versus trabecular bypass device implantation in glaucoma patients undergoing cataract extraction. Clin Ophthalmol. 2018, 12, 791-797. [CrossRef]
- ElMallah, M.K.; Seibold, L.K.; Kahook, M.Y.; Williamson, B.K.; Singh, I.P.; Dorairaj, S.K.; Group, K.G.S. 12-Month Retrospective Comparison of Kahook Dual Blade Excisional Goniotomy with Istent Trabecular Bypass Device Implantation in Glaucomatous Eyes at the Time of Cataract Surgery. Adv Ther. 2019, 36, 2515-2527. [CrossRef]
- ElMallah, M.K.; Berdahl, J.P.; Williamson, B.K.; Dorairaj, S.K.; Kahook, M.Y.; Gallardo, M.J.; Mahootchi, A.; Smith, S.N.; Rappaport, L.A.; Diaz-Robles, D.; et al. Twelve-Month Outcomes of Stand-Alone Excisional Goniotomy in Mild to Severe Glaucoma. Clin Ophthalmol. 2020, 14, 1891-1897. [CrossRef]
- Porter, M.; Garza, A.; Gallardo, M. Excisional Goniotomy in Latino Patients with Open-Angle Glaucoma: Outcomes Through 24 Months. Clin Ophthalmol. 2020, 14, 3619-3625. [CrossRef]
- Laroche, D.; Nkrumah, G.; Ugoh, P.; Ng, C. Real World Outcomes of Kahook Dual Blade Goniotomy in Black and Afro-Latinx Adult Patients with Glaucoma: A 6-Month Retrospective Study. J Natl Med Assoc. 2021, 113, 230-236. [CrossRef]
- Ansari, E.; Loganathan, D. 12-month clinical outcomes of combined phacoemulsification and ab interno trabeculectomy for open-angle glaucoma in the United Kingdom. PLoS One. 2021, 16, e0252826. [CrossRef]
- Krishnamurthy, R.; Senthil, S.; Choudhari, N. Initial experience with phacoemulsification and goniotomy using the Kahook dual blade in advanced open-angle glaucoma: Six-month outcomes in Indian eyes. Indian J Ophthalmol. 2021, 69, 2484-2487. [CrossRef]
- Iwasaki, K.; Takamura, Y.; Orii, Y.; Arimura, S.; Inatani, M. Performances of glaucoma operations with Kahook Dual Blade or iStent combined with phacoemulsification in Japanese open angle glaucoma patients. Int J Ophthalmol. 2020, 13, 941-945. [CrossRef]
- Iwasaki, K.; Kakimoto, H.; Orii, Y.; Arimura, S.; Takamura, Y.; Inatani, M. Long-Term Outcomes of a Kahook Dual Blade Procedure Combined with Phacoemulsification in Japanese Patients with Open-Angle Glaucoma. J Clin Med. 2022, 11. [CrossRef]
- Ibrahim, L.F.; Pereira, A.F.R.; Terenzi, L.A.O.; Vianello, M.P.; Dorairaj, S.K.; Prata, T.S.; Kanadani, F.N. Phacoemulsification with Kahook Dual Blade goniotomy in eyes with medically treated glaucoma: analysis of surgical outcomes and success predictors. Arq Bras Oftalmol. 2021, 85, 359-363. [CrossRef]
- Ibrahim, L.F.; Silva, S.A.R.; Prata, T.S.; Kanadani, F.N. Short-term results of ab-interno trabeculotomy using Kahook Dual Blade in patients with primary congenital glaucoma. Arq Bras Oftalmol. 2021, 84, 380-382. [CrossRef]
- Bravetti, G.E.; Gillmann, K.; Salinas, L.; Berdahl, J.P.; Lazcano-Gomez, G.S.; Williamson, B.K.; Dorairaj, S.K.; Seibold, L.K.; Smith, S.; Aref, A.A.; et al. Surgical outcomes of excisional goniotomy using the kahook dual blade in severe and refractory glaucoma: 12-month results. Eye (Lond). 2023, 37, 1608-1613. [CrossRef]
- Miller, V.J.; Patnaik, J.L.; Young, C.E.C.; SooHoo, J.R.; Seibold, L.K.; Kahook, M.Y.; Ertel, M.K.; Palestine, A.G.; Pantcheva, M.B. Outcomes of Kahook Dual Blade Goniotomy for Uveitis Associated Open Angle Glaucoma or Ocular Hypertension. J Glaucoma. 2022, 31, 903-908. [CrossRef]
- Mechleb, N.; Tomey, K.; Cherfan, D.; Nemr, A.; Cherfan, G.; Dorairaj, S.; Khoueir, Z. Six months’ follow-up of combined phacoemulsification-kahook dual blade excisional goniotomy. Saudi J Ophthalmol. 2022, 36, 195-200. [CrossRef]
- Al Habash, A.; Albuainain, A. Long term outcome of combined phacoemulsification and excisional goniotomy with the Kahook Dual Blade in different subtypes of glaucoma. Sci Rep. 2021, 11, 10660. [CrossRef]
- Albuainain, A.; Al Habash, A. Three-year clinical outcomes of phacoemulsification combined with excisional goniotomy using the kahook dual blade for cataract and open-angle glaucoma in Saudi Arabia. Saudi J Ophthalmol. 2022, 36, 213-217. [CrossRef]
- Baumgarten, S.; Plange, N.; Htoon, H.M.; Lohmann, T.; Videa, A.; Koutsonas, A.; Schellhase, H.; Kuerten, D.; Walter, P.; Fuest, M. Outcomes of combined single-use dual blade goniotomy and cataract surgery. Int Ophthalmol. 2022, 42, 2685-2696. [CrossRef]
- Baumgarten, S.; Lohmann, T.; Prinz, J.; Walter, P.; Plange, N.; Fuest, M. [Ab interno trabeculotomy without/with cataract operation-An alternative treatment before or instead of trabeculectomy in patients with high intraocular pressure?]. Ophthalmologie. 2023, 120, 825-831. [CrossRef]
- Barkander, A.; Economou, M.A.; Jóhannesson, G. Outcomes of iStent Inject Versus Kahook Dual Blade Surgery in Glaucoma Patients Undergoing Cataract Surgery. J Glaucoma. 2023, 32, e121-e128. [CrossRef]
- Sakamoto, T.; Nisiwaki, H. Factors associated with 1-year outcomes and transient intraocular pressure elevation in minimally invasive glaucoma surgery using Kahook Dual Blades. Sci Rep. 2023, 13, 15206. [CrossRef]
- El Helwe, H.; Oberfeld, B.; Golsoorat Pahlaviani, F.; Falah, H.; Trzcinski, J.; Solá-Del Valle, D. Comparing Outcomes of Phacoemulsification and Endocyclophotocoagulation with Either Dual Blade Goniotomy (PEcK) or Two Trabecular Stents (ICE2). Clin Ophthalmol. 2023, 17, 2879-2888. [CrossRef]
- Tanito, M.; Sugihara, K.; Tsutsui, A.; Hara, K.; Manabe, K.; Matsuoka, Y. Midterm Results of Microhook ab Interno Trabeculotomy in Initial 560 Eyes with Glaucoma. J Clin Med. 2021, 10. [CrossRef]
- Sugihara, K.; Shimada, A.; Ichioka, S.; Harano, A.; Tanito, M. Comparison of Phaco-Tanito Microhook Trabeculotomy between Propensity-Score-Matched 120-Degree and 240-Degree Incision Groups. J Clin Med. 2023, 12. [CrossRef]
- Tanito, M.; Sugihara, K.; Tsutsui, A.; Hara, K.; Manabe, K.; Matsuoka, Y. Effects of Preoperative Intraocular Pressure Level on Surgical Results of Microhook. J Clin Med. 2021, 10. [CrossRef]
- Omoto, T.; Fujishiro, T.; Asano-Shimizu, K.; Sugimoto, K.; Sakata, R.; Murata, H.; Asaoka, R.; Honjo, M.; Aihara, M. Comparison of 12-month surgical outcomes of ab interno trabeculotomy with phacoemulsification between spatula-shaped and dual-blade microhooks. Jpn J Ophthalmol. 2021, 65, 402-408. [CrossRef]
- Sotani, N.; Kusuhara, S.; Matsumiya, W.; Okuda, M.; Mori, S.; Sotani, R.; Kim, K.W.; Nishisho, R.; Nakamura, M. Outcomes of Microhook ab Interno Trabeculotomy in Consecutive 36 Eyes with Uveitic Glaucoma. J Clin Med. 2022, 11. [CrossRef]
- Tanito, M.; Sano, I.; Ikeda, Y.; Fujihara, E. Short-term results of microhook ab interno trabeculotomy, a novel minimally invasive glaucoma surgery in Japanese eyes: initial case series. Acta Ophthalmol. 2017, 95, e354-e360. [CrossRef]
- Ishida, A.; Mochiji, M.; Manabe, K.; Matsuoka, Y.; Tanito, M. Persistent Hypotony and Annular Ciliochoroidal Detachment After Microhook Ab Interno Trabeculotomy. J Glaucoma. 2020, 29, 807-812. [CrossRef]
- Kanda, S.; Fujishiro, T.; Omoto, T.; Fujino, R.; Arai, T.; Nomoto, Y.; Aihara, M. Comparison of effectiveness and complications in trabeculotomy with phacoemulsification between ab externo and ab interno using a spatula-shaped microhook. Sci Rep. 2021, 11, 17259. [CrossRef]
- Tanito, M.; Sano, I.; Ikeda, Y.; Fujihara, E. Microhook ab interno trabeculotomy, a novel minimally invasive glaucoma surgery, in eyes with open-angle glaucoma with scleral thinning. Acta Ophthalmol. 2016, 94, e371-372. [CrossRef]
- Maheshwari, D.; Grover, D.S.; Ramakrishnan, R.; Pillai, M.R.; Chautani, D.; Kader, M.A. Early Outcomes of Combined Phacoemulsification and Ab Interno Tanito Microhook Trabeculotomy in Open-Angle Glaucoma. Ophthalmol Glaucoma. 2023. [CrossRef]
- Tanito, M.; Ikeda, Y.; Fujihara, E. Effectiveness and safety of combined cataract surgery and microhook ab interno trabeculotomy in Japanese eyes with glaucoma: report of an initial case series. Jpn J Ophthalmol. 2017, 61, 457-464. [CrossRef]
- Asaoka, R.; Nakakura, S.; Mochizuki, T.; Ishida, A.; Fujino, Y.; Ishii, K.; Obana, A.; Tanito, M.; Kiuchi, Y. Which is More Effective and Safer? Comparison of Propensity Score-Matched Microhook Ab Interno Trabeculotomy and iStent Inject. Ophthalmol Ther. 2023, 12, 2757-2768. [CrossRef]
- Omoto, T.; Fujishiro, T.; Asano-Shimizu, K.; Sugimoto, K.; Sakata, R.; Murata, H.; Asaoka, R.; Honjo, M.; Aihara, M. Comparison of the short-term effectiveness and safety profile of ab interno combined trabeculotomy using 2 types of trabecular hooks. Jpn J Ophthalmol. 2020, 64, 407-413. [CrossRef]
- Takayanagi, Y.; Ichioka, S.; Ishida, A.; Tsutsui, A.; Tanito, M. Fellow-Eye Comparison between Phaco-Microhook Ab-Interno Trabeculotomy and Phaco-iStent Trabecular Micro-Bypass Stent. J Clin Med. 2021, 10. [CrossRef]
- Harano, A.; Shimada, A.; Ichioka, S.; Sugihara, K.; Tanito, M. Fellow-Eye Comparison between Phaco-Tanito Microhook Trabeculotomy and Phaco-iStent Inject W. J Clin Med. 2023, 12. [CrossRef]
- Ishida, A.; Ichioka, S.; Takayanagi, Y.; Tsutsui, A.; Manabe, K.; Tanito, M. Comparison of Postoperative Hyphemas between Microhook Ab Interno Trabeculotomy and iStent Using a New Hyphema Scoring System. J Clin Med. 2021, 10. [CrossRef]
- Chihara, E.; Chihara, T. Development and Application of a New T-shaped Internal Trabeculotomy Hook (T-hook). Clin Ophthalmol. 2022, 16, 3919-3926. [CrossRef]
- Chan, L.; Moster, M.R.; Bicket, A.K.; Sheybani, A.; Sarkisian, S.R.; Samuelson, T.W.; Ahmed, I.I.K.; Miller-Ellis, E.; Smith, O.U.; Cui, Q.N. New Devices in Glaucoma. Ophthalmol Ther. 2023, 12, 2381-2395. [CrossRef]
- Johnstone, M.; Xin, C.; Tan, J.; Martin, E.; Wen, J.; Wang, R.K. Aqueous outflow regulation - 21st century concepts. Prog Retin Eye Res. 2021, 83, 100917. [CrossRef]
- Tamm, E.R.; Carassa, R.G.; Albert, D.M.; Gabelt, B.T.; Patel, S.; Rasmussen, C.A.; Kaufman, P.L. Viscocanalostomy in rhesus monkeys. Arch Ophthalmol. 2004, 122, 1826-1838. [CrossRef]
- Takahashi, H.; Tanito, M.; Yokoyama, M.; Park, M.; Chihara, E. Two cases of intraoperative anterior chamber angle observation using ophthalmic endoscope in viscocanalostomy. Am J Ophthalmol. 2004, 138, 1060-1063. [CrossRef]
- Byszewska, A.; Konopińska, J.; Kicińska, A.K.; Mariak, Z.; Rękas, M. Canaloplasty in the Treatment of Primary Open-Angle Glaucoma: Patient Selection and Perspectives. Clin Ophthalmol. 2019, 13, 2617-2629. [CrossRef]
- Zhang, B.; Kang, J.; Chen, X. A System Review and Meta-Analysis of Canaloplasty Outcomes in Glaucoma Treatment in Comparison with Trabeculectomy. J Ophthalmol. 2017, 2017, 2723761. [CrossRef]
- Jiang, N.; Zhao, G.Q.; Lin, J.; Hu, L.T.; Che, C.Y.; Wang, Q.; Xu, Q.; Li, C.; Zhang, J. Meta-analysis of the efficacy and safety of combined surgery in the management of eyes with coexisting cataract and open angle glaucoma. Int J Ophthalmol. 2018, 11, 279-286. [CrossRef]
- Lin, Z.J.; Xu, S.; Huang, S.Y.; Zhang, X.B.; Zhong, Y.S. Comparison of canaloplasty and trabeculectomy for open angle glaucoma: a Meta-analysis. Int J Ophthalmol. 2016, 9, 1814-1819. [CrossRef]
- Wagdy, F.M. Canaloplasty versus Viscocanalostomy in Primary Open Angle Glaucoma. Electron Physician. 2017, 9, 3665-3671. [CrossRef]
- Shingleton, B.; Tetz, M.; Korber, N. Circumferential viscodilation and tensioning of Schlemm canal (canaloplasty) with temporal clear corneal phacoemulsification cataract surgery for open-angle glaucoma and visually significant cataract: one-year results. J Cataract Refract Surg. 2008, 34, 433-440. [CrossRef]
- Tetz, M.; Koerber, N.; Shingleton, B.J.; von Wolff, K.; Bull, H.; Samuelson, T.W.; Lewis, R.A. Phacoemulsification and intraocular lens implantation before, during, or after canaloplasty in eyes with open-angle glaucoma: 3-year results. J Glaucoma. 2015, 24, 187-194. [CrossRef]
- Lewis, R.A.; von Wolff, K.; Tetz, M.; Koerber, N.; Kearney, J.R.; Shingleton, B.J.; Samuelson, T.W. Canaloplasty: Three-year results of circumferential viscodilation and tensioning of Schlemm canal using a microcatheter to treat open-angle glaucoma. J Cataract Refract Surg. 2011, 37, 682-690. [CrossRef]
- Bull, H.; von Wolff, K.; Körber, N.; Tetz, M. Three-year canaloplasty outcomes for the treatment of open-angle glaucoma: European study results. Graefes Arch Clin Exp Ophthalmol. 2011, 249, 1537-1545. [CrossRef]
- Ayyala, R.S.; Chaudhry, A.L.; Okogbaa, C.B.; Zurakowski, D. Comparison of surgical outcomes between canaloplasty and trabeculectomy at 12 months’ follow-up. Ophthalmology. 2011, 118, 2427-2433. [CrossRef]
- Schoenberg, E.D.; Chaudhry, A.L.; Chod, R.; Zurakowski, D.; Ayyala, R.S. Comparison of Surgical Outcomes Between Phacocanaloplasty and Phacotrabeculectomy at 12 Months’ Follow-up: A Longitudinal Cohort Study. J Glaucoma. 2015, 24, 543-549. [CrossRef]
- Matlach, J.; Dhillon, C.; Hain, J.; Schlunck, G.; Grehn, F.; Klink, T. Trabeculectomy versus canaloplasty (TVC study) in the treatment of patients with open-angle glaucoma: a prospective randomized clinical trial. Acta Ophthalmol. 2015, 93, 753-761. [CrossRef]
- Voykov, B.; Blumenstock, G.; Leitritz, M.A.; Dimopoulos, S.; Alnahrawy, O. Treatment efficacy and safety of canaloplasty for open-angle glaucoma after 5 years. Clin Exp Ophthalmol. 2015, 43, 768-771. [CrossRef]
- Lommatzsch, C.; Heinz, C.; Heiligenhaus, A.; Koch, J.M. Canaloplasty in patients with uveitic glaucoma: a pilot study. Graefes Arch Clin Exp Ophthalmol. 2016, 254, 1325-1330. [CrossRef]
- Xin, C.; Chen, X.; Shi, Y.; Li, M.; Wang, H.; Wang, N. One-year interim comparison of canaloplasty in primary open-angle glaucoma following failed filtering surgery with primary canaloplasty. Br J Ophthalmol. 2016, 100, 1692-1696. [CrossRef]
- Rekas, M.; Danielewska, M.E.; Byszewska, A.; Petz, K.; Wierzbowska, J.; Wierzbowski, R.; Iskander, D.R. Assessing Efficacy of Canaloplasty Using Continuous 24-Hour Monitoring of Ocular Dimensional Changes. Invest Ophthalmol Vis Sci. 2016, 57, 2533-2542. [CrossRef]
- Kuerten, D.; Plange, N.; Becker, J.; Walter, P.; Fuest, M. Evaluation of Long-term Anatomic Changes Following Canaloplasty With Anterior Segment Spectral-domain Optical Coherence Tomography and Ultrasound Biomicroscopy. J Glaucoma. 2018, 27, 87-93. [CrossRef]
- Genaidy, M.M.; Zein, H.A.; Eid, A.M. Combined phacocanaloplasty for open-angle glaucoma and cataract: 12 months results. Clin Ophthalmol. 2017, 11, 2169-2176. [CrossRef]
- Garris, W.J.; Le, C.; Zurakowski, D.; Ayyala, R.S. Comparison of surgical outcomes between canaloplasty and trabeculectomy with mitomycin C at 2-year follow-up: A longitudinal cohort study. Indian J Ophthalmol. 2018, 66, 66-70. [CrossRef]
- Rękas, M.; Byszewska, A.; Petz, K.; Wierzbowska, J.; Jünemann, A. Canaloplasty versus non-penetrating deep sclerectomy - a prospective, randomised study of the safety and efficacy of combined cataract and glaucoma surgery; 12-month follow-up. Graefes Arch Clin Exp Ophthalmol. 2015, 253, 591-599. [CrossRef]
- Byszewska, A.; Jünemann, A.; Rękas, M. Canaloplasty versus Nonpenetrating Deep Sclerectomy: 2-Year Results and Quality of Life Assessment. J Ophthalmol. 2018, 2018, 2347593. [CrossRef]
- Lewis, R.A.; von Wolff, K.; Tetz, M.; Koerber, N.; Kearney, J.R.; Shingleton, B.J.; Samuelson, T.W. Canaloplasty: circumferential viscodilation and tensioning of Schlemm canal using a flexible microcatheter for the treatment of open-angle glaucoma in adults: two-year interim clinical study results. J Cataract Refract Surg. 2009, 35, 814-824. [CrossRef]
- Davids, A.M.; Pahlitzsch, M.; Boeker, A.; Winterhalter, S.; Maier-Wenzel, A.K.; Klamann, M. Ab interno canaloplasty (ABiC)-12-month results of a new minimally invasive glaucoma surgery (MIGS). Graefes Arch Clin Exp Ophthalmol. 2019, 257, 1947-1953. [CrossRef]
- Grieshaber, M.C.; Pienaar, A.; Olivier, J.; Stegmann, R. Clinical evaluation of the aqueous outflow system in primary open-angle glaucoma for canaloplasty. Invest Ophthalmol Vis Sci. 2010, 51, 1498-1504. [CrossRef]
- Grieshaber, M.C.; Fraenkl, S.; Schoetzau, A.; Flammer, J.; Orgül, S. Circumferential viscocanalostomy and suture canal distension (canaloplasty) for whites with open-angle glaucoma. J Glaucoma. 2011, 20, 298-302. [CrossRef]
- Grieshaber, M.C.; Pienaar, A.; Olivier, J.; Stegmann, R. Canaloplasty for primary open-angle glaucoma: long-term outcome. Br J Ophthalmol. 2010, 94, 1478-1482. [CrossRef]
- Grieshaber, M.C. Stegmann Canal Expander for canaloplasty: A novel technique. Eur J Ophthalmol. 2018, 28, 472-478. [CrossRef]
- Grieshaber, M.C.; Pienaar, A.; Stegmann, R. Access to Schlemm’s canal for canaloplasty: an intra-individual comparison of two dissection techniques. Acta Ophthalmol. 2020, 98, e599-e606. [CrossRef]
- Vastardis, I.; Fili, S.; Perdikakis, G.; Gatzioufas, Z.; Kohlhaas, M. Estimation of risk-benefit ratio and comparison of post-operative efficacy results between trabeculectomy and canaloplasty. Eur J Ophthalmol. 2021, 31, 1405-1412. [CrossRef]
- Tracer, N.; Dickerson, J.E.; Radcliffe, N.M. Circumferential Viscodilation Ab Interno Combined with Phacoemulsification for Treatment of Open-Angle Glaucoma: 12-Month Outcomes. Clin Ophthalmol. 2020, 14, 1357-1364. [CrossRef]
- Hughes, T.; Traynor, M. Clinical Results of Ab Interno Canaloplasty in Patients with Open-Angle Glaucoma. Clin Ophthalmol. 2020, 14, 3641-3650. [CrossRef]
- Hirsch, L.; Cotliar, J.; Vold, S.; Selvadurai, D.; Campbell, A.; Ferreira, G.; Aminlari, A.; Cho, A.; Heersink, S.; Hochman, M.; et al. Canaloplasty and trabeculotomy ab interno with the OMNI system combined with cataract surgery in open-angle glaucoma: 12-month outcomes from the ROMEO study. J Cataract Refract Surg. 2021, 47, 907-915. [CrossRef]
- Elksne, E.; Mercieca, K.; Prokosch-Willing, V. Canaloplasty with mitomycin C after previous combined cataract surgery and Schlemm’s canal microstent implantation. Eur J Ophthalmol. 2022, 32, 712-716. [CrossRef]
- Zhang, S.; Hu, C.; Cheng, H.; Gu, J.; Samuel, K.; Lin, H.; Deng, Y.; Xie, Y.; Hu, J.; Le, R.; et al. Efficacy of bleb-independent penetrating canaloplasty in primary angle-closure glaucoma: one-year results. Acta Ophthalmol. 2022, 100, e213-e220. [CrossRef]
- Gillmann, K.; Aref, A.; Niegowski, L.J.; Baumgartner, J.M. Combined Ab interno viscocanaloplasty (ABiC) in open-angle glaucoma: 12-month outcomes. Int Ophthalmol. 2021, 41, 3295-3301. [CrossRef]
- Khaimi, M.A. Long-term medication reduction in controlled glaucoma with iTrack ab-interno canaloplasty as a standalone procedure and combined with cataract surgery. Ther Adv Ophthalmol. 2021, 13, 25158414211045751. [CrossRef]
- Łazicka-Gałecka, M.; Kamińska, A.; Gałecki, T.; Guszkowska, M.; Dziedziak, J.; Szaflik, J.; Szaflik, J.P. Canaloplasty - Efficacy and Safety in an 18-Month Follow Up Period, and Analysis of Outcomes in Primary Open Angle Glaucoma Pigmentary Glaucoma and Pseudoexfoliative Glaucoma. Semin Ophthalmol. 2022, 37, 602-610. [CrossRef]
- Gallardo, M.J. 36-Month Effectiveness of Ab-Interno Canaloplasty Standalone versus Combined with Cataract Surgery for the Treatment of Open-Angle Glaucoma. Ophthalmol Glaucoma. 2022, 5, 476-482. [CrossRef]
- Cheng, H.; Ye, W.; Zhang, S.; Xie, Y.; Gu, J.; Le, R.; Deng, Y.; Hu, C.; Zhao, Z.; Ke, Z.; et al. Clinical outcomes of penetrating canaloplasty in patients with traumatic angle recession glaucoma: a prospective interventional case series. Br J Ophthalmol. 2023, 107, 1092-1097. [CrossRef]
- Liang, Y.; Yu, Q.; Sun, H.; Sucijanti; Gu, L.; Yuan, Z. Modified suture-assisted canaloplasty in Asians with primary open-angle glaucoma: a prospective study with 12-month follow-up. BMC Ophthalmol. 2022, 22, 202. [CrossRef]
- Koerber, N.; Ondrejka, S. Four-Year Efficacy and Safety of iTrack Ab-interno Canaloplasty as a Standalone Procedure and Combined with Cataract Surgery in Open-Angle Glaucoma. Klin Monbl Augenheilkd. 2023, 240, 1394-1404. [CrossRef]
- Ondrejka, S.; Körber, N.; Dhamdhere, K. Long-term effect of canaloplasty on intraocular pressure and use of intraocular pressure-lowering medications in patients with open-angle glaucoma. J Cataract Refract Surg. 2022, 48, 1388-1393. [CrossRef]
- Bleeker, A.R.; Litchfield, W.R.; Ibach, M.J.; Greenwood, M.D.; Ristvedt, D.; Berdahl, J.P.; Terveen, D.C. Short-Term Efficacy of Combined ab Interno Canaloplasty and Trabeculotomy in Pseudophakic Eyes with Open-Angle Glaucoma. Clin Ophthalmol. 2022, 16, 2295-2303. [CrossRef]
- Hu, J.J.; Lin, H.S.; Zhang, S.D.; Ye, W.Q.; Gu, J.; Xie, Y.Q.; Tang, Y.H.; Liang, Y.B. A new bleb-independent surgery namely penetrating canaloplasty for corticosteroid-induced glaucoma: a prospective case series. Int J Ophthalmol. 2022, 15, 1077-1081. [CrossRef]
- Kicińska, A.K.; Danielewska, M.E.; Rękas, M. Safety and Efficacy of Three Variants of Canaloplasty with Phacoemulsification to Treat Open-Angle Glaucoma and Cataract: 12-Month Follow-Up. J Clin Med. 2022, 11. [CrossRef]
- Terveen, D.C.; Sarkisian, S.R.; Vold, S.D.; Selvadurai, D.; Williamson, B.K.; Ristvedt, D.G.; Bleeker, A.R.; Dhamdhere, K.; Dickerson, J.E. Canaloplasty and trabeculotomy with the OMNI. Int Ophthalmol. 2023, 43, 1647-1656. [CrossRef]
- Murphy Iii, J.T.; Terveen, D.C.; Aminlari, A.E.; Dhamdhere, K.; Dickerson, J.E.; Group, R.S. A Multicenter 12-Month Retrospective Evaluation of Canaloplasty and Trabeculotomy in Patients with Open-Angle Glaucoma: The ROMEO 2 Study. Clin Ophthalmol. 2022, 16, 3043-3052. [CrossRef]
- Xin, C.; Wang, N.; Wang, H. Intraocular Pressure Fluctuation in Primary Open-Angle Glaucoma with Canaloplasty and Microcatheter Assisted Trabeculotomy. J Clin Med. 2022, 11. [CrossRef]
- Seif, R.; Jalbout, N.D.E.; Sadaka, A.; Szigiato, A.A.; Harasymowycz, P. Size Matters: Ab Interno Canaloplasty Revision with Suture Trabeculotomy. J Curr Glaucoma Pract. 2022, 16, 152-157. [CrossRef]
- Stingl, J.V.; Wagner, F.M.; Liebezeit, S.; Baumgartner, R.; Spät, H.; Schuster, A.K.; Prokosch, V.; Grehn, F.; Hoffmann, E.M. Long-Term Efficacy and Safety of Modified Canaloplasty Versus Trabeculectomy in Open-Angle Glaucoma. Life (Basel). 2023, 13. [CrossRef]
- Xu, L.; Zhang, X.; Cao, Y.; Zhao, Y.; Gu, J.; Ye, W.; Wang, X.; Li, J.; Ren, R.; Liang, Y. Incidence and risk factors of early transient intraocular pressure elevation after canaloplasty for primary open-angle glaucoma. J Zhejiang Univ Sci B. 2023, 24, 366-370. [CrossRef]
- Williamson, B.K.; Vold, S.D.; Campbell, A.; Hirsch, L.; Selvadurai, D.; Aminlari, A.E.; Cotliar, J.; Dickerson, J.E. Canaloplasty and Trabeculotomy with the OMNI System in Patients with Open-Angle Glaucoma: Two-Year Results from the ROMEO Study. Clin Ophthalmol. 2023, 17, 1057-1066. [CrossRef]
- Patel, S.; Reiss, G. Long-Term Clinical and Safety Outcomes of Canaloplasty Performed across All Grades of Glaucoma Severity. J Ophthalmol. 2023, 2023, 5625990. [CrossRef]
- Dickinson, A.; Leidy, L.; Nusair, O.; Mihailovic, A.; Ramulu, P.; Yohannan, J.; Johnson, T.V.; Kaleem, M.; Rachapudi, S.; An, J. Short-Term Outcomes of Hydrus Microstent With and Without Additional Canaloplasty During Cataract Surgery. J Glaucoma. 2023, 32, 769-776. [CrossRef]
- Yadgarov, A.; Dentice, K.; Aljabi, Q. Real-World Outcomes of Canaloplasty and Trabeculotomy Combined with Cataract Surgery in Eyes with All Stages of Open-Angle Glaucoma. Clin Ophthalmol. 2023, 17, 2609-2617. [CrossRef]
- Voykov, B.; Szurman, P.; Dimopoulos, S.; Ziemssen, F.; Alnahrawy, O. Micro-invasive suture trabeculotomy after canaloplasty: preliminary results. Clin Exp Ophthalmol. 2015, 43, 409-414. [CrossRef]
- Seuthe, A.M.; Januschowski, K.; Szurman, P. Micro-invasive 360-degree suture trabeculotomy after successful canaloplasty – one year results. Graefes Arch Clin Exp Ophthalmol. 2016, 254, 155-159. [CrossRef]
- Xin, C.; Song, S.; Wang, N.; Wang, R.; Johnstone, M. Effects of Schlemm’s Canal Expansion: Biomechanics and MIGS Implications. Life (Basel). 2021, 11. [CrossRef]
- Gandolfi, S.A.; Ungaro, N.; Ghirardini, S.; Tardini, M.G.; Mora, P. Comparison of Surgical Outcomes between Canaloplasty and Schlemm’s Canal Scaffold at 24 Months’ Follow-Up. J Ophthalmol. 2016, 2016, 3410469. [CrossRef]
- Koerber, N.; Ondrejka, S. 6-Year Efficacy and Safety of iTrack Ab-interno Canaloplasty as a Standalone Procedure and Combined with Cataract Surgery in Primary Open-Angle and Pseudoexfoliative Glaucoma. J Glaucoma. 2023. [CrossRef]
- Kicińska, A.K.; Rękas, M. Safety and Efficacy of Three Modifications of Canaloplasty to Treat Open-Angle Glaucoma: 3-Year Outcomes. J Clin Med. 2023, 12. [CrossRef]
- Greenwood, M.D.; Yadgarov, A.; Flowers, B.E.; Sarkisian, S.R.; Ohene-Nyako, A.; Dickerson, J.E.; GROUP, G.S. 36-Month Outcomes from the Prospective GEMINI Study: Canaloplasty and Trabeculotomy Combined with Cataract Surgery for Patients with Primary Open-Angle Glaucoma. Clin Ophthalmol. 2023, 17, 3817-3824. [CrossRef]
- Creagmile, J.; Kim, W.I.; Scouarnec, C. Hydrus Microstent implantation with OMNI Surgical System Ab interno canaloplasty for the management of open-angle glaucoma in phakic patients refractory to medical therapy. Am J Ophthalmol Case Rep. 2023, 29, 101749. [CrossRef]
- Brusini, P.; Tosoni, C.; Zeppieri, M. Canaloplasty in Corticosteroid-Induced Glaucoma. Preliminary Results. J Clin Med. 2018, 7. [CrossRef]
- Brusini, P.; Papa, V. Canaloplasty in Pigmentary Glaucoma: Long-Term Outcomes and Proposal of a New Hypothesis on Its Intraocular Pressure Lowering Mechanism. J Clin Med. 2020, 9. [CrossRef]
- Brusini, P.; Papa, V.; Zeppieri, M. Canaloplasty in Pseudoexfoliation Glaucoma. Can It Still Be Considered a Good Choice? J Clin Med. 2022, 11. [CrossRef]
- Brusini, P. Canaloplasty in open-angle glaucoma surgery: a four-year follow-up. ScientificWorldJournal. 2014, 2014, 469609. [CrossRef]
- Vold, S.D.; Williamson, B.K.; Hirsch, L.; Aminlari, A.E.; Cho, A.S.; Nelson, C.; Dickerson, J.E. Canaloplasty and Trabeculotomy with the OMNI System in Pseudophakic Patients with Open-Angle Glaucoma: The ROMEO Study. Ophthalmol Glaucoma. 2021, 4, 173-181. [CrossRef]
- Lazcano-Gomez, G.; Antzoulatos, G.L.; Kahook, M.Y. Combined Phacoemulsification and STREAMLINE Surgical System Canal of Schlemm Transluminal Dilation in Eyes of Hispanic Patients with Mild to Moderate Glaucoma. Clin Ophthalmol. 2023, 17, 1911-1918. [CrossRef]
- Balas, M.; Mathew, D.J. Minimally Invasive Glaucoma Surgery: A Review of the Literature. Vision (Basel). 2023, 7. [CrossRef]
- Cantor, L.; Lindfield, D.; Ghinelli, F.; Świder, A.W.; Torelli, F.; Steeds, C.; Dickerson, J.E., Jr.; Nguyen, D.Q. Systematic Literature Review of Clinical, Economic, and Humanistic Outcomes Following Minimally Invasive Glaucoma Surgery or Selective Laser Trabeculoplasty for the Treatment of Open-Angle Glaucoma with or Without Cataract Extraction. Clin Ophthalmol. 2023, 17, 85-101. [CrossRef]
- Aref, A.A.; Parker, P.R.; Chen, M.Y. Microinvasive glaucoma surgeries: critical summary of clinical trial data with and without phacoemulsification. Curr Opin Ophthalmol. 2023, 34, 146-151. [CrossRef]
- Nichani, P.; Popovic, M.M.; Schlenker, M.B.; Park, J.; Ahmed, I.I.K. Microinvasive glaucoma surgery: A review of 3476 eyes. Surv Ophthalmol. 2021, 66, 714-742. [CrossRef]
- Bicket, A.K.; Le, J.T.; Azuara-Blanco, A.; Gazzard, G.; Wormald, R.; Bunce, C.; Hu, K.; Jayaram, H.; King, A.; Otárola, F.; et al. Minimally Invasive Glaucoma Surgical Techniques for Open-Angle Glaucoma: An Overview of Cochrane Systematic Reviews and Network Meta-analysis. JAMA Ophthalmol. 2021, 139, 983-989. [CrossRef]
- Wellik, S.R.; Dale, E.A. A review of the iStent(®) trabecular micro-bypass stent: safety and efficacy. Clin Ophthalmol. 2015, 9, 677-684. [CrossRef]
- Pullig, B.; Koerber, N.J.; Dietlein, T. Can perforations of descemet’s window (DW) improve the outcome of canaloplasty in open angle glaucoma? Graefes Arch Clin Exp Ophthalmol. 2019, 257, 1733-1740. [CrossRef]
- Seibold, L.K.; Soohoo, J.R.; Ammar, D.A.; Kahook, M.Y. Preclinical investigation of ab interno trabeculectomy using a novel dual-blade device. Am J Ophthalmol. 2013, 155, 524-529.e522. [CrossRef]
- Arimura, S.; Iwasaki, K.; Orii, Y.; Komori, R.; Takamura, Y.; Inatani, M. Randomised clinical trial for morphological changes of trabecular meshwork between Kahook dual-blade goniotomy and ab interno trabeculotomy with a microhook. Sci Rep. 2023, 13, 20783. [CrossRef]
- Hirabayashi, M.T.; Lee, D.; King, J.T.; Thomsen, S.; An, J.A. Comparison Of Surgical Outcomes Of 360° Circumferential Trabeculotomy Versus Sectoral Excisional Goniotomy With The Kahook Dual Blade At 6 Months. Clin Ophthalmol. 2019, 13, 2017-2024. [CrossRef]
- Aoki, R.; Hirooka, K.; Goda, E.; Yuasa, Y.; Okumichi, H.; Onoe, H.; Kiuchi, Y. Comparison of Surgical Outcomes Between Microhook Ab Interno Trabeculotomy and Goniotomy with the Kahook Dual Blade in Combination with Phacoemulsification: A Retrospective, Comparative Case Series. Adv Ther. 2021, 38, 329-336. [CrossRef]
- Okada, N.; Hirooka, K.; Onoe, H.; Okumichi, H.; Kiuchi, Y. Comparison of Mid-Term Outcomes between Microhook ab Interno Trabeculotomy and Goniotomy with the Kahook Dual Blade. J Clin Med. 2023, 12. [CrossRef]
- Kinoshita-Nakano, E.; Nakanishi, H.; Ohashi-Ikeda, H.; Morooka, S.; Akagi, T. Comparative outcomes of trabeculotomy ab externo versus trabecular ablation ab interno for open angle glaucoma. Jpn J Ophthalmol. 2018, 62, 201-208. [CrossRef]
- Tojo, N.; Otsuka, M.; Hayashi, A. Comparison of trabectome and microhook surgical outcomes. Int Ophthalmol. 2021, 41, 21-26. [CrossRef]
- Lavia, C.; Dallorto, L.; Maule, M.; Ceccarelli, M.; Fea, A.M. Minimally-invasive glaucoma surgeries (MIGS) for open angle glaucoma: A systematic review and meta-analysis. PLoS One. 2017, 12, e0183142. [CrossRef]
- Irie, A.; Nakashima, K.I.; Inoue, T.; Kojima, S.; Takihara, Y.; Takahashi, E. Trabeculotomy Using the Kahook Dual Blade for Exfoliation Glaucoma and Primary Open Angle Glaucoma: Comparison of Outcomes According to Incision Range. J Glaucoma. 2024, 33, 270-276. [CrossRef]
- Qiao, Y.; Tan, C.; Chen, X.; Sun, X.; Chen, J. Gonioscopy-assisted transluminal trabeculotomy versus goniotomy with Kahook dual blade in patients with uncontrolled juvenile open-angle glaucoma: a retrospective study. BMC Ophthalmol. 2021, 21, 395. [CrossRef]
- Chen, R.I.; Purgert, R.; Eisengart, J. Gonioscopy-Assisted Transluminal Trabeculotomy and Goniotomy, With or Without Concomitant Cataract Extraction, in Steroid-Induced and Uveitic Glaucoma: 24-Month Outcomes. J Glaucoma. 2023, 32, 501-510. [CrossRef]
- Gillmann, K.; Mansouri, K. Minimally Invasive Glaucoma Surgery: Where Is the Evidence? Asia Pac J Ophthalmol (Phila). 2020, 9, 203-214. [CrossRef]
- Gabai, A.; Cimarosti, R.; Battistella, C.; Isola, M.; Lanzetta, P. Efficacy and Safety of Trabeculectomy Versus Nonpenetrating Surgeries in Open-angle Glaucoma: A Meta-analysis. J Glaucoma. 2019, 28, 823-833. [CrossRef]
- Fellman, R.L.; Grover, D.S. Episcleral Venous Fluid Wave in the Living Human Eye Adjacent to Microinvasive Glaucoma Surgery (MIGS) Supports Laboratory Research: Outflow is Limited Circumferentially, Conserved Distally, and Favored Inferonasally. J Glaucoma. 2019, 28, 139-145. [CrossRef]
- Lee, D.; King, J.; Thomsen, S.; Hirabayashi, M.; An, J. Comparison Of Surgical Outcomes Between Excisional Goniotomy Using The Kahook Dual Blade And iStent Trabecular Micro-Bypass Stent In Combination With Phacoemulsification. Clin Ophthalmol. 2019, 13, 2097-2102. [CrossRef]
- Falkenberry, S.; Singh, I.P.; Crane, C.J.; Haider, M.A.; Morgan, M.G.; Grenier, C.P.; Brubaker, J.W.; Balasubramani, G.K.; Dorairaj, S. Excisional goniotomy vs trabecular microbypass stent implantation: a prospective randomized clinical trial in eyes with mild to moderate open-angle glaucoma. J Cataract Refract Surg. 2020, 46, 1165-1171. [CrossRef]
- Arnljots, T.S.; Economou, M.A. Kahook Dual Blade Goniotomy vs iStent inject: Long-Term Results in Patients with Open-Angle Glaucoma. Clin Ophthalmol. 2021, 15, 541-550. [CrossRef]
- Al Yousef, Y.; Strzalkowska, A.; Hillenkamp, J.; Rosentreter, A.; Loewen, N.A. Comparison of a second-generation trabecular bypass (iStent inject) to ab interno trabeculectomy (Trabectome) by exact matching. Graefes Arch Clin Exp Ophthalmol. 2020, 258, 2775-2780. [CrossRef]
- Ellingsen, B.A.; Grant, W.M. Trabeculotomy and sinusotomy in enucleated human eyes. Invest Ophthalmol. 1972, 11, 21-28.
- Rosenquist, R.; Epstein, D.; Melamed, S.; Johnson, M.; Grant, W.M. Outflow resistance of enucleated human eyes at two different perfusion pressures and different extents of trabeculotomy. Curr Eye Res. 1989, 8, 1233-1240. [CrossRef]
- Lee, Y.J.; Ha, A.; Kang, D.; Shim, S.R.; Jeoung, J.W.; Park, K.H.; Kim, Y.K. Comparative efficacies of 13 surgical interventions for primary congenital glaucoma in children: a network meta-analysis of randomized clinical trials. Int J Surg. 2023, 109, 953-962. [CrossRef]
- Elhusseiny, A.M.; El Sayed, Y.M.; El Sheikh, R.H.; Gawdat, G.I.; Elhilali, H.M. Circumferential Schlemm’s Canal Surgery in Adult and Pediatric Glaucoma. Curr Eye Res. 2019, 44, 1281-1290. [CrossRef]
- Kuerten, D.; Walter, P.; Baumgarten, S.; Fuest, M.; Plange, N. 12-month outcomes of ab interno excisional goniotomy combined with cataract surgery in primary open-angle glaucoma and normal tension glaucoma. Int Ophthalmol. 2023, 43, 2605-2612. [CrossRef]
- Alnahrawy, O.; Blumenstock, G.; Ziemssen, F.; Szurman, P.; Leitritz, M.A.; Dimopoulos, S.; Voykov, B. Exit strategies in canaloplasty: intraoperative conversion into 180-degree trabeculotomy or 360-degree trabeculotomy in cases of unsuccessful catheterisation of Schlemm’s canal: influence of degree of canal cleavage. Graefes Arch Clin Exp Ophthalmol. 2015, 253, 779-784. [CrossRef]
- Manabe, S.I.; Sawaguchi, S.; Hayashi, K. The effect of the extent of the incision in the Schlemm canal on the surgical outcomes of suture trabeculotomy for open-angle glaucoma. Jpn J Ophthalmol. 2017, 61, 99-104. [CrossRef]
- Asafali, F.; Rajamani, M.; Ramamurthy, C.; Chaya, C.J.; M, V. Relationship of degrees of gonioscopy assisted transluminal trabeculotomy and trabecular shelf to success using a marker suture technique. Eye (Lond). 2023, 37, 132-138. [CrossRef]
- Wecker, T.; Anton, A.; Neuburger, M.; Jordan, J.F.; van Oterendorp, C. Trabeculotomy opening size and IOP reduction after Trabectome® surgery. Graefes Arch Clin Exp Ophthalmol. 2017, 255, 1643-1650. [CrossRef]
- Zhang, Y.; Yu, P.; Sugihara, K.; Zhu, X.; Yang, X.; Li, X.; Liu, Y.; Zhang, H.; Yan, X.; Lin, F.; et al. Influence of Goniotomy Size on Treatment Safety and Efficacy for Primary Open-Angle Glaucoma: A Multicenter Study. Am J Ophthalmol. 2023, 256, 118-125. [CrossRef]
- Farrar, N.; Yan, D.B.; Johnson, M. Modeling the effects of glaucoma surgery on intraocular pressure. Exp Eye Res. 2021, 209, 108620. [CrossRef]
- Chihara, E.; Chihara, T. Consequences of clot formation and hyphema post-internal trabeculotomy for glaucoma. J Glaucoma. 2024, 33, 523-528. [CrossRef]
- Balekudaru, S.; Shah, D.; Lingam, V.; George, R.; George, A.E.; Ganesh, S.K.; Biswas, J.; Dutta Majumder, P.; Baskaran, M. A comparative analysis of surgical outcome in uveitic and non-uveitic steroid-induced glaucoma in children. Indian J Ophthalmol. 2022, 70, 4218-4225. [CrossRef]
- Dang, Y.; Kaplowitz, K.; Parikh, H.A.; Roy, P.; Loewen, R.T.; Francis, B.A.; Loewen, N.A. Steroid-induced glaucoma treated with trabecular ablation in a matched comparison with primary open-angle glaucoma. Clin Exp Ophthalmol. 2016, 44, 783-788. [CrossRef]
- Iwao, K.; Inatani, M.; Tanihara, H. Success rates of trabeculotomy for steroid-induced glaucoma: a comparative, multicenter, retrospective cohort study. Am J Ophthalmol. 2011, 151, 1047-1056.e1041. [CrossRef]
- Honjo, M.; Tanihara, H.; Inatani, M.; Honda, Y. External trabeculotomy for the treatment of steroid-induced glaucoma. J Glaucoma. 2000, 9, 483-485. [CrossRef]
- Miller, V.J.; Young, C.E.C.; SooHoo, J.R.; Seibold, L.K.; Kahook, M.Y.; Pecen, P.E.; Palestine, A.G.; Pantcheva, M.B. Efficacy of Goniotomy With Kahook Dual Blade in Patients With Uveitis-associated Ocular Hypertension. J Glaucoma. 2019, 28, 744-748. [CrossRef]
- Anton, A.; Heinzelmann, S.; Neß, T.; Lübke, J.; Neuburger, M.; Jordan, J.F.; Wecker, T. Trabeculectomy ab interno with the Trabectome® as a therapeutic option for uveitic secondary glaucoma. Graefes Arch Clin Exp Ophthalmol. 2015, 253, 1973-1978. [CrossRef]
- Tojo, N.; Abe, S.; Miyakoshi, M.; Hayashi, A. Comparison of intraocular pressure fluctuations before and after ab interno trabeculectomy in pseudoexfoliation glaucoma patients. Clin Ophthalmol. 2017, 11, 1667-1675. [CrossRef]
- Okeke, C.O.; Miller-Ellis, E.; Rojas, M. Trabectome success factors. Medicine (Baltimore). 2017, 96, e7061. [CrossRef]
- Ting, J.L.; Damji, K.F.; Stiles, M.C.; Group, T.S. Ab interno trabeculectomy: outcomes in exfoliation versus primary open-angle glaucoma. J Cataract Refract Surg. 2012, 38, 315-323. [CrossRef]
- Aktas, Z.; Ozdemir Zeydanli, E.; Uysal, B.S.; Yigiter, A. Outcomes of Prolene Gonioscopy Assisted Transluminal Trabeculotomy in Primary Open Angle Glaucoma and Pseudoexfoliation Glaucoma: A Comparative Study. J Glaucoma. 2022, 31, 751-756. [CrossRef]
- Eslami, Y.; Mohammadi, M.; Safizadeh, M.; Tabatabaei, S.M. Six-month outcomes of combined conventional needle goniotomy and phacoemulsification in eyes with early to moderate primary open-angle and pseudoexfoliation glaucoma and ocular hypertension. Indian J Ophthalmol. 2022, 70, 2030-2035. [CrossRef]
- Loewen, R.T.; Roy, P.; Parikh, H.A.; Dang, Y.; Schuman, J.S.; Loewen, N.A. Impact of a Glaucoma Severity Index on Results of Trabectome Surgery: Larger Pressure Reduction in More Severe Glaucoma. PLoS One. 2016, 11, e0151926. [CrossRef]
- Chihara, E.; Hayashi, K. Different modes of intraocular pressure reduction after three different nonfiltering surgeries and trabeculectomy. Jpn J Ophthalmol. 2011, 55, 107-114. [CrossRef]
- Yang, S.A.; Ciociola, E.C.; Mitchell, W.; Hall, N.; Lorch, A.C.; Miller, J.W.; Friedman, D.S.; Boland, M.V.; Elze, T.; Zebardast, N.; et al. Effectiveness of Microinvasive Glaucoma Surgery in the United States: Intelligent Research in Sight Registry Analysis 2013-2019. Ophthalmology. 2023, 130, 242-255. [CrossRef]
- Esfandiari, H.; Hassanpour, K.; Yaseri, M.; Loewen, N.A. Extended pharmacological miosis is superfluous after glaucoma angle surgery: A retrospective study. F1000Res. 2018, 7, 178. [CrossRef]
- Bizrah, M.; Corbett, M.C. Intracameral Phenylephrine to Arrest Intraoperative Intraocular Bleeding: A New Technique. Ophthalmol Ther. 2019, 8, 137-141. [CrossRef]
- Okuda, M.; Mori, S.; Ueda, K.; Sakamoto, M.; Kusuhara, S.; Yamada-Nakanishi, Y.; Nakamura, M. Favorable effect of ripasudil use on surgical outcomes of microhook ab interno trabeculotomy. Graefes Arch Clin Exp Ophthalmol. 2023, 261, 2603-2610. [CrossRef]
- Xu, H.; Thomas, M.T.; Lee, D.; Hirabayashi, M.T.; An, J.A. Response to netarsudil in goniotomy-treated eyes and goniotomy-naïve eyes: a pilot study. Graefes Arch Clin Exp Ophthalmol. 2022, 260, 3001-3007. [CrossRef]
- Murakami-Kojima, S.; Takahashi, E.; Eguchi-Matsumoto, M.; Saruwatari, J.; Nakashima, K.I.; Inoue, T. Risk factors for intraocular pressure elevation in a six-month period after ab interno trabeculotomy using a Kahook Dual Blade. BMC Ophthalmol. 2022, 22, 327. [CrossRef]
- Goda, E.; Hirooka, K.; Mori, K.; Kiuchi, Y. Intraocular pressure-lowering effects of Ripasudil: a potential outcome marker for Trabeculotomy. BMC Ophthalmol. 2019, 19, 243. [CrossRef]
- Okuda, M.; Mori, S.; Takano, F.; Murai, Y.; Ueda, K.; Sakamoto, M.; Kurimoto, T.; Yamada-Nakanishi, Y.; Nakamura, M. Association of the prolonged use of anti-glaucoma medications with the surgical failure of ab interno microhook trabeculotomy. Acta Ophthalmol. 2022, 100, e1209-e1215. [CrossRef]
- Richter, G.M.; Takusagawa, H.L.; Sit, A.J.; Rosdahl, J.A.; Chopra, V.; Ou, Y.; Kim, S.J.; WuDunn, D. Trabecular Procedures Combined with Cataract Surgery for Open-Angle Glaucoma: A Report by the American Academy of Ophthalmology. Ophthalmology. 2024, 131, 370-382. [CrossRef]
- Sabharwal, J.; Garg, A.K.; Ramulu, P.Y. How much does cataract surgery contribute to intraocular pressure lowering? Curr Opin Ophthalmol. 2024, 35, 147-154. [CrossRef]
- Kim, D.D.; Doyle, J.W.; Smith, M.F. Intraocular pressure reduction following phacoemulsification cataract extraction with posterior chamber lens implantation in glaucoma patients. Ophthalmic Surg Lasers. 1999, 30, 37-40.
- Hayashi, K.; Hayashi, H.; Nakao, F.; Hayashi, F. Changes in anterior chamber angle width and depth after intraocular lens implantation in eyes with glaucoma. Ophthalmology. 2000, 107, 698-703. [CrossRef]
- Kaplowitz, K.; Bussel, II; Honkanen, R.; Schuman, J.S.; Loewen, N.A. Review and meta-analysis of ab-interno trabeculectomy outcomes. Br J Ophthalmol. 2016, 100, 594-600. [CrossRef]
- Barkander, A.; Economou, M.A.; Jóhannesson, G. Kahook Dual-Blade Goniotomy with and without Phacoemulsification in Medically Uncontrolled Glaucoma. Clin Ophthalmol. 2023, 17, 1385-1394. [CrossRef]
- Pahlitzsch, M.; Gonnermann, J.; Maier, A.K.; Torun, N.; Bertelmann, E.; Joussen, A.M.; Klamann, M. [Trabeculectomy Ab Interno in Primary Open Angle Glaucoma and Exfoliative Glaucoma]. Klin Monbl Augenheilkd. 2015, 232, 1198-1207. [CrossRef]
- Nakamura, K.; Honda, R.; Soeda, S.; Nagai, N.; Takahashi, O.; Kadonosono, K.; Ozawa, Y. Factors associated with achieving intraocular pressure lower than 15 mmHg by Trabectome surgery in primary open-angle glaucoma. Sci Rep. 2021, 11, 14308. [CrossRef]
- Murata, N.; Takahashi, E.; Saruwatari, J.; Kojima, S.; Inoue, T. Outcomes and risk factors for ab interno trabeculotomy with a Kahook Dual Blade. Graefes Arch Clin Exp Ophthalmol. 2023, 261, 503-511. [CrossRef]
- Jordan, J.F.; Wecker, T.; van Oterendorp, C.; Anton, A.; Reinhard, T.; Boehringer, D.; Neuburger, M. Trabectome surgery for primary and secondary open angle glaucomas. Graefes Arch Clin Exp Ophthalmol. 2013, 251, 2753-2760. [CrossRef]
- Shinmei, Y.; Kijima, R.; Nitta, T.; Ishijima, K.; Ohguchi, T.; Chin, S.; Ishida, S. Modified 360-degree suture trabeculotomy combined with phacoemulsification and intraocular lens implantation for glaucoma and coexisting cataract. J Cataract Refract Surg. 2016, 42, 1634-1641. [CrossRef]
- Parikh, H.A.; Bussel, II; Schuman, J.S.; Brown, E.N.; Loewen, N.A. Coarsened Exact Matching of Phaco-Trabectome to Trabectome in Phakic Patients: Lack of Additional Pressure Reduction from Phacoemulsification. PLoS One. 2016, 11, e0149384. [CrossRef]
- Ahmed, S.F.; Bhatt, A.; Schmutz, M.; Mosaed, S. Trabectome outcomes across the spectrum of glaucoma disease severity. Graefes Arch Clin Exp Ophthalmol. 2018, 256, 1703-1710. [CrossRef]
- Neiweem, A.E.; Bussel, II; Schuman, J.S.; Brown, E.N.; Loewen, N.A. Glaucoma Surgery Calculator: Limited Additive Effect of Phacoemulsification on Intraocular Pressure in Ab Interno Trabeculectomy. PLoS One. 2016, 11, e0153585. [CrossRef]
- Sieck, E.G.; Epstein, R.S.; Kennedy, J.B.; SooHoo, J.R.; Pantcheva, M.B.; Patnaik, J.L.; Wagner, B.D.; Lynch, A.M.; Kahook, M.Y.; Seibold, L.K. Outcomes of Kahook Dual Blade Goniotomy with and without Phacoemulsification Cataract Extraction. Ophthalmol Glaucoma. 2018, 1, 75-81. [CrossRef]
- Dang, Y.; Roy, P.; Bussel, I.I.; Loewen, R.T.; Parikh, H.; Loewen, N.A. Combined analysis of trabectome and phaco-trabectome outcomes by glaucoma severity. F1000Res. 2016, 5, 762. [CrossRef]
- Matsuo, M.; Inomata, Y.; Kozuki, N.; Tanito, M. Characterization of Peripheral Anterior Synechiae Formation After Microhook Ab-interno Trabeculotomy Using a 360-Degree Gonio-Camera. Clin Ophthalmol. 2021, 15, 1629-1638. [CrossRef]
- Rao, A.; Khan, S.M.; Mukherjee, S. Causes of Immediate and Early IOP Spikes After Circumferential Gonioscopy-Assisted Transluminal Trabeculotomy Using ASOCT. Clin Ophthalmol. 2023, 17, 313-320. [CrossRef]
- Tripathi, B.J.; Geanon, J.D.; Tripathi, R.C. Distribution of tissue plasminogen activator in human and monkey eyes. An immunohistochemical study. Ophthalmology. 1987, 94, 1434-1438. [CrossRef]
- Quan, A.V.; Chen, J.; Wang, Y.E.; Vanner, E.A.; Grajewski, A.L.; Hodapp, E.A.; Chang, T.C. Factors Associated With Gonioscopy-Assisted Transluminal Trabeculotomy (GATT) Complications and Failure in Children. Am J Ophthalmol. 2022, 241, 168-178. [CrossRef]
- Naftali Ben Haim, L.; Yehezkeli, V.; Abergel Hollander, E.; Dar, N.; Sharon, T.; Belkin, A. Intraocular pressure spikes after gonioscopy-assisted transluminal trabeculotomy (GATT). Graefes Arch Clin Exp Ophthalmol. 2024, 262, 927-935. [CrossRef]
- Shi, Y.; Wang, H.; Oatts, J.T.; Xin, C.; Yin, P.; Zhang, L.; Tian, J.; Zhang, Y.; Cao, K.; Han, Y.; et al. A Prospective Study of Intraocular Pressure Spike and Failure After Gonioscopy-Assisted Transluminal Trabeculotomy in Juvenile Open-Angle Glaucoma: A Prospective Study of GATT in JOAG. Am J Ophthalmol. 2022, 236, 79-88. [CrossRef]
- Vold, S.D.; Dustin, L. Impact of laser trabeculoplasty on Trabectome® outcomes. Ophthalmic Surg Lasers Imaging. 2010, 41, 443-451. [CrossRef]
- Klamann, M.K.; Gonnermann, J.; Maier, A.K.; Bertelmann, E.; Joussen, A.M.; Torun, N. Influence of Selective Laser Trabeculoplasty (SLT) on combined clear cornea phacoemulsification and Trabectome outcomes. Graefes Arch Clin Exp Ophthalmol. 2014, 252, 627-631. [CrossRef]
- Mitchell, W.; Yang, S.A.; Ondeck, C.; Stewart, I.; Zhao, Y.; Roldan, A.M.; Halawa, O.; Hall, N.; Elze, T.; Miller, J.; et al. Effectiveness of angle based minimally invasive glaucoma surgery after laser trabeculoplasty: an analysis of the IRIS® Registry. Ophthalmol Glaucoma. 2024. [CrossRef]
- King, J.; Lee, D.; Thomsen, S.; Hirabayashi, M.T.; An, J. Relationship between selective laser trabeculoplasty and excisional goniotomy outcomes in glaucomatous eyes. Can J Ophthalmol. 2022, 57, 112-117. [CrossRef]
- Phillips, S.S.; Patnaik, J.L.; Capitena Young, C.E.; Ertel, M.K.; SooHoo, J.R.; Seibold, L.K.; Kahook, M.Y.; Pantcheva, M.B. Selective Laser Trabeculoplasty and Outcomes of Subsequent Phacoemulsification Combined with Kahook Dual Blade Goniotomy. Ophthalmol Ther. 2022, 11, 1883-1893. [CrossRef]
- Pahlitzsch, M.; Davids, A.M.; Winterhalter, S.; Zorn, M.; Reitemeyer, E.; Klamann, M.K.J.; Torun, N.; Bertelmann, E.; Maier, A.K. Selective Laser Trabeculoplasty Versus MIGS: Forgotten Art or First-Step Procedure in Selected Patients with Open-Angle Glaucoma. Ophthalmol Ther. 2021, 10, 509-524. [CrossRef]
- Töteberg-Harms, M.; Rhee, D.J. Selective laser trabeculoplasty following failed combined phacoemulsification cataract extraction and ab interno trabeculectomy. Am J Ophthalmol. 2013, 156, 936-940.e932. [CrossRef]
- Kanter, J.A.; Amin, P.; Komati, R.; Mackin, A.G.; Dao, D.; Shaw, L.T.; Skondra, D.; Qiu, M. Gonioscopy-assisted transluminal trabeculotomy in neovascular glaucoma: Salvaging the conventional outflow pathway. Am J Ophthalmol Case Rep. 2022, 28, 101668. [CrossRef]
- Salimi, A.; Kasner, O.; Schendel, S.; Mydlarski, M.; Kalache, D.; Vera, L.; Pintwala, R.; Harasymowycz, P. Outcomes and risk factors for Kahook Dual Blade excisional goniotomy with concomitant phacoemulsification: a multicentre Canadian study. Can J Ophthalmol. 2023. [CrossRef]
- Tojo, N.; Abe, S.; Hayashi, A. Factors That Influence of Trabectome Surgery for Glaucoma Patients. J Glaucoma. 2017, 26, 835-844. [CrossRef]
- Waldner, D.M.; Chaban, Y.; Penny, M.D.; Al-Ani, A.; Belkin, A.; Ahmed, I.I.K.; Schlenker, M.B.; Gooi, P. Segmental Suture Gonioscopy-Assisted Transluminal Trabeculotomy: Comparison of Superior Versus Inferior Hemisphere Outcomes. J Glaucoma. 2023, 32, 396-406. [CrossRef]
- Esfandiari, H.; Shah, P.; Torkian, P.; Conner, I.P.; Schuman, J.S.; Hassanpour, K.; Loewen, N.A. Five-year clinical outcomes of combined phacoemulsification and trabectome surgery at a single glaucoma center. Graefes Arch Clin Exp Ophthalmol. 2019, 257, 357-362. [CrossRef]
- Faria, B.M.; Costa, V.P.; Melillo, G.H.L.; Daga, F.B.; Scoralick, A.L.B.; Paranhos, A., Jr.; Kanadani, F.N.; Prata, T.S. Gonioscopy-Assisted Transluminal Trabeculotomy for Glaucoma: 1-Year Outcomes and Success Predictors. J Glaucoma. 2022, 31, 443-448. [CrossRef]
- Kuusniemi, A.M.; Lindbohm, N.; Allinen, P.; Koskinen, M.; Harju, M. Ab Interno Trabeculotomy: Key Prognostic Factors. J Glaucoma. 2020, 29, 211-216. [CrossRef]
- Otori, Y.; Matsuoka, T.; Kumoi, M.; Tachibana, E.; Tsujino, C.; Matsuda, S. Comparison of Surgical Outcomes Between Ab Interno Suture Trabeculotomy and Ab Externo Metal Trabeculotomy in Adult Patients with Glaucoma. Clin Ophthalmol. 2021, 15, 3213-3220. [CrossRef]
- Yoshida, T.; Nomura, T.; Yoshimoto, S.; Ohno, M.; Ito, T.; Horie, S.; Ohno-Matsui, K. Outcomes of standalone ab interno trabeculotomy in the treatment of open-angle glaucoma in eyes with high myopia. BMC Ophthalmol. 2023, 23, 261. [CrossRef]
- Tan, Q.; Li, J.; Lin, D.; Zhao, P. Risk factors of surgical failure in combined phacoemulsification and excisional goniotomy for angle-closure glaucoma. Graefes Arch Clin Exp Ophthalmol. 2023, 261, 535-543. [CrossRef]
- Olivier, M.M.G.; Smith, O.U.; Croteau-Chonka, C.C.; VanderBeek, B.L.; Maguire, M.G.; Lum, F.; Fujino, D.; Kelly, S.P.; Rich, W.L.; Miller-Ellis, E.G. Demographic and Clinical Characteristics Associated with Minimally Invasive Glaucoma Surgery Use: An Intelligent Research in Sight (IRIS®) Registry Retrospective Cohort Analysis. Ophthalmology. 2021, 128, 1292-1299. [CrossRef]
Figure 1.
A schematic drawing depicting the histopathology of human eyes following an unsuccessful trabeculotomy [66]. Surgical opening of the trabecular meshwork resulted in closure in 14 of 31 eyes (A) and remained open in 10 of 31 eyes (B) to the anterior chamber, six years (ranging from 3.4 to 22.6 years) after external trabeculotomy. These specimens were obtained during subsequent trabeculectomy after the initial trabeculotomy ab externo. In 10 eyes, in which Schlemm’s canal (SC) remained open to the anterior chamber, the inner wall of the SC was lined with extended Schlemm’s canal endothelium and/or fibrous proliferation. In 14 eyes with a closed SC, the trabecular meshwork showed sign of fibrous degeneration. Additionally, intracanalicular space might be filled with fibrous proliferation, leading to shrinkage of the SC space. In four eyes, the trabecular meshwork was covered by Schlemm’s canal endothelial cells, and in three eyes, peripheral anterior synechiae covered the trabecular meshwork. (Copyright License #5796400157661 by Exp. Eye Res. Elsevier).
Figure 1.
A schematic drawing depicting the histopathology of human eyes following an unsuccessful trabeculotomy [66]. Surgical opening of the trabecular meshwork resulted in closure in 14 of 31 eyes (A) and remained open in 10 of 31 eyes (B) to the anterior chamber, six years (ranging from 3.4 to 22.6 years) after external trabeculotomy. These specimens were obtained during subsequent trabeculectomy after the initial trabeculotomy ab externo. In 10 eyes, in which Schlemm’s canal (SC) remained open to the anterior chamber, the inner wall of the SC was lined with extended Schlemm’s canal endothelium and/or fibrous proliferation. In 14 eyes with a closed SC, the trabecular meshwork showed sign of fibrous degeneration. Additionally, intracanalicular space might be filled with fibrous proliferation, leading to shrinkage of the SC space. In four eyes, the trabecular meshwork was covered by Schlemm’s canal endothelial cells, and in three eyes, peripheral anterior synechiae covered the trabecular meshwork. (Copyright License #5796400157661 by Exp. Eye Res. Elsevier).
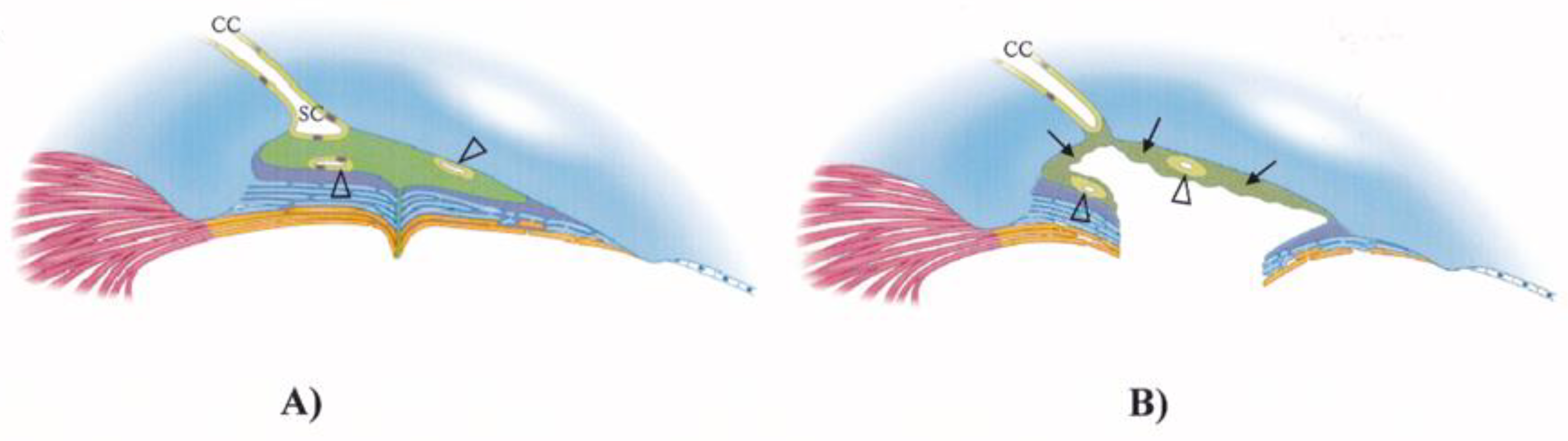
Figure 2.
Kahook dual bade is a device to excise trabecular meshwork (internal trabeculectomy) between two parallel blades near the tip. (Product of New World Medical Rancho Cucamonga CA.).
Figure 2.
Kahook dual bade is a device to excise trabecular meshwork (internal trabeculectomy) between two parallel blades near the tip. (Product of New World Medical Rancho Cucamonga CA.).
Figure 3.
Tanito micro-hook for internal trabeculotomy: A device inserted into Schlemm’s canal to push away trabecular meshwork tissue. (Product of Inami, Tokyo).
Figure 3.
Tanito micro-hook for internal trabeculotomy: A device inserted into Schlemm’s canal to push away trabecular meshwork tissue. (Product of Inami, Tokyo).

Figure 4.
Chihara T-hook for internal trabeculotomy: The T-shaped head allows bidirectional opening of the trabecular meshwork. The tip of this device is rounded and designed not to injure outer wall of Schlemm’s canal. (Product of Inami Tokyo; Handaya Tokyo; and AOI: Advanced Ophthalmic Innovations, Singapore).
Figure 4.
Chihara T-hook for internal trabeculotomy: The T-shaped head allows bidirectional opening of the trabecular meshwork. The tip of this device is rounded and designed not to injure outer wall of Schlemm’s canal. (Product of Inami Tokyo; Handaya Tokyo; and AOI: Advanced Ophthalmic Innovations, Singapore).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



