
Submitted:
29 July 2024
Posted:
30 July 2024
You are already at the latest version
Abstract
Anthrax is a severe acute zoonotic disease of herbivores caused by Gram-positive, anaerobic, spore-forming bacteria. It is transmitted via direct contact with sick farm animals or those who have died of Anthrax. This study intends to present a cutaneous form of Anthrax in a 36-year-old woman suffered from a painless ulcer on her thumb five days after handling a head of sheep. The lesion started as a small papule that developed as a painless vesicular blister on the dorsal exterior surface of the right thumb. However, upon clinical investigation, the patient showed an absence of fever, lethargy, and pain. Swabs were collected and examined according to conventional microbiological tests. Direct smear revealed a Gram-positive bacilli that showed spore formation resembling B. anthracis. Nutrient agar, 5% sheep blood agar, and PLET agar were streaked by the swab. Other swabs were inoculated into the peptone water. All cultured media were inoculated at 37 oC for 24 hours. The morphology of growing colonies was examined, while the biochemical tests were done to identify the isolated bacteria, including a motility test and antibiotic sensitivity. The results of this study approved the existence of Bacillus anthracis by microbiological analyses. Accordingly, cutaneous form of anthrax was diagnosed, and specific systematic and local treatments were provided for the patient. In conclusion, this study confirmed the diagnosis of cutaneous Anthrax, a highly contagious disease that needed early detection and more attention and awareness should be taken when handling animal products.
Keywords:
Anaerobic
; Anthrax
; Bacillus anthracis
; bacilli
; cutaneous
1. Introduction
Anthrax is a serious infectious disease. Worldwide, every year, approximately 2,000 cutaneous anthrax cases are reported [1]. Human anthrax is very rare but causes a serious human disease. Primarily, it is an animal disease that causes high mortality in livestock. Damaged skin, inhalation, and digestion are common routes to enter Bacillus anthracis, the causative agent [2,3]. The genus of Bacillus encloses many spore-forming bacteria. It includes pathogenic and valuable bacteria such as the Bacillus species, which are used to prepare antibiotics like B. subtilis. Additionally, G. stearothermopilus is used as an indicator of sterilization procedure [4,5]. However, the most well-known, historically important pathogenic partner is Bacillus anthracis, the first microorganism seen under the light microscope and the first Bacillus isolated by Koch in 1876 as a pure culture. It was also the first microorganism utilized to formulate attenuated vaccines. Nonetheless, Bacillus anthracis became a famous name after its use as a bio-terrorism weapon [6,7].
Anthrax skin forms commonly emerge in nearly 95% of cases [8]. This form is ordinarily associated with occupational exposure to the sick or products of dead animals. Bacillus anthracis, the causative agent, may affect any exposed skin area, like the foot, hand, face, neck, arm, and head. It is worth mentioning that the pathogen can enter via injured skin and is associated with an incubation period extended from 1 week to 12 days. The cutaneous form of anthrax is a primary painless pruritic skin papule that usually appears 3 to 5 days after contact with infected animals. The papule broadens after one to two days and develops an ulcer, usually 1-3 cm in diameter, with a rounded and regular boundary. After the next few days, the ulcer was enclosed by a blister. Following necrosis and drying of the ulcer, the characteristic black depressed eschar lesion develops. However, without secondary infection, the lesion is not purulent. After one to two weeks, the eschar lesion is divided and falls off leading to develop a scar-like lesion in most cases. However, if the head or neck lesion is severe, edema develops around it and compromises the respiratory system [9,10,11]. Regional lymphadenopathy was reported, accompanied by systemic manifestations such as headache, fever, and malaise. The percentage of death occurs is about 20% of untreated patients, while it is only 1% of treated patients with antibiotics [11,12]. A review of the literature revealed scarce publications regarding cutaneous anthrax in Iraq. Consequently, this study intends to present a case report of cutaneous anthrax in a 36-year-old female, including a description of the lesions, isolation of the causative agents, and the treatment follow-up.
2. Case Report Narrative
A 36-year-old woman suffered from a painless ulcer on her thumb 5 days after handling a head of sheep. The lesion started as a small papule and developed into a vesicular blister on the dorsal exterior surface of the right thumb without any pain (Figure 1).
No fever and phlegm were recognized on the patient during clinical examination, accompanied by painless lesions. Conventional bacteriological methods were used to investigate Bacillus anthracis. These included lack of hemolysis and motility, growing on selective media, capsule staining, and susceptibility to penicillin. The swabs were collected from the lesion, and a direct smear was done and stained with Gram stain. Direct smear revealed a Gram-positive bacilli that formed spores (Figure 2).
Then, the swabs were streaked on nutrient agar, 5% sheep blood agar supplied by selective elements, including Sulfamethoxazole. Trimethoprim, Polymyxin B, Cycloheximide, and Polymyxin-lysozyme -EDTA/Thallous acetate agar ( PLET). Then, the swabs were dipped into peptone water. All cultured media were incubated for 18-24 hours at 37 o C. The isolated bacteria were investigated based on the colonies' morphology and conventional biochemical tests. Additionally, a motility test and antibiotic sensitivity were also performed. The growing colonies on blood agar (Figure 3) were white creamy, non-hemolytic, 2-4 mm in diameter with a slightly moist nonglossy appearance. While on PLET agar the colonies appeared small, white, domed, and circular.
These microbiological analyses demonstrated the isolation of Bacillus anthracis isolates from the lesion. Accordingly, the diagnosis of cutaneous Anthrax was made, and specific systematic antibiotic (ciprofloxacin) and local treatments were prescribed for the patient (Figure 4).
3. Discussion
Bacillus anthracis's endospores are the cause of the classical form of anthrax. It is a disease mainly of herbivores and livestock [13]. Anthrax causative agent was reported as endemic in various countries from different continents like Africa, Asia, and southern & central Europe. It is Gram-positive, aerobic, and spore-forming bacteria [14]. Human infection is gained via ingestion, inhalation, or handle the products of infected livestock and animal dead from anthrax. However, people can get an infection when they eat the vegetative form of the infected meat. Human anthrax is divided into four clinical forms according to the entrance of the pathogen: inhalation or respiratory, skin or cutaneous, oro-pharyngeal, and gastrointestinal. The toxin of anthrax and Poly-D-glutamic acid capsule are the principal virulence factors in the pathogenicity of anthrax. Moreover, pXO1 and pXO2 are the specific virulence plasmids that carry the coded genes for these factors. However, man is somewhat resistant to anthrax [5]. Cutaneous anthrax has been reported repeatedly by veterinarians, butchers, and other experts who come in contact with animals. In this case report, a patient presented with a thumb lesion that started as a papule 4-5 days after handling a head of sheep. This lesion presentation is compatible with previously reported cases [9,10,11,12]. They mentioned that the ordinary sites are the neck, face, and hand, which are the exposed skin areas [14]. In the current case study, the source of infection was a sheep, which might be infected with anthrax. The spores might gain entrance via a breach in the patient's skin and lead to the distinguishing lesion. Moreover, 2-5 days later, the patient surrounded the lesion with erythema and edema. Then, a vesicle filled with fluid developed, and the fluid became black due to hemorrhage. Afterward, ulceration and eschar developed with localized lymphadenopathy. In the beginning, the case was diagnosed as an ordinary ulcer, but unresponsive to treatment led to sending the patient for a bacteriological culture that approved the presence of Gram-positive, spore-forming bacilli compatible with morphological and biochemical features of Bacillus anthracis. This skin presentation of the disease agrees with 37 reported cases in northern Iraq in 2008 and was considered the first reported outbreak in Iraq, according to the minister of health in the Kurdistan region. They also said that all 37 patients suffered from the cutaneous form which is not as severe as the lung or other internal organs more serious anthrax forms [16].
In Iraq, anthrax has been reported in livestock since 1980 [17,18], which led the Agriculture Ministry/ General Veterinary Directory to introduce the annual anthrax vaccination program. However, periodic outbreaks of anthrax in livestock or humans were reported. Zhao et al. [17] mentioned an average annual percentage change (47.5%) for anthrax. Despite anthrax control procedures in Iraq, sporadic cases of the disease remain a health problem. These results are compatible with previously reported studies which showed that cutaneous form has reached up to 95% of anthrax infections worldwide [15,19,20,21]. Anthrax is considered a crucial, deadly, contagious zoonotic disease that can rapidly spread from animal to human beings or from animal to animal. [22,23,24]. Bacillus anthracis is a vital microorganism that received attention in Iraq because Iraq was accused of using this microorganism as a potential agent of bioterrorism in the former regime.
4. Conclusions
Cutaneous anthrax is reported in this study despite the paucity of the occurrence of the disease. Anthrax is an endemic overwhelming disease for humans and livestock. Therefore, the authorities from various ministries should validate new and rapid diagnostic methods and report these cases. Attention must be paid to using the precautionary procedure to control the spreading of the disease in livestock, forcing the livestock owners to vaccinate their animals and raise awareness among the population while handling animal products, especially meat.
Author Contributions
Conceptualization, AKA and AJK; methodology, AKA, MAJ, and AHA; software, AKA, MAJ, and FAJ; validation, AKA, AHA and AJK.; formal analysis, AKA, MAJ, and FAJ; investigation, AKA, AJK, MAJ, and FAJ; resources, AKA, AJK, and MAJ; data curation, AKA, AHA, and AJK; writing—original draft preparation, AKA; writing—review and editing, AKA, AJK, and AHA; visualization, AKA, AHA, and AJK; supervision, AKA; project administration, AKA and FAJ; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee at College of Veterinary Medicine, University of Al-Muthanna (protocol code 1813 in 6 Feb 2024).
Informed Consent Statement
Written and signed informed consent has been obtained from the Patient to publish this paper.
Acknowledgments
The authors would like to thank the workers in the Al-Muthanna Hospital laboratory for their efforts in microbiological investigations. This study is self-supported; no funding has been received from any authorities. There is no conflict of interest related to the publication of this manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Leonard, T.E.; Siratan, E.; Hartiadi, L.Y.; Crystalia, A.A. Insights into antimicrobial peptides in fighting anthrax: A review. Drug Dev Res 2021, 82, 754–66. [Google Scholar] [CrossRef] [PubMed]
- Hanna, P.C.; Ireland, J.A. Understanding Bacillus anthracis pathogenesis. Trends Microbiol 1999, 7, 180–2. [Google Scholar] [CrossRef] [PubMed]
- Zakowska, D.; Bartoszcze, M.; Niemcewicz, M.; Bielawska-DrózdKocik, A.; Kocik, J. New aspects of the infection mechanisms of B. anthracis. Ann Agric Environ Med 2012, 19, 613–8. [Google Scholar] [PubMed]
- Logan, N.A. Bacillus anthracis, Bacillus cereus and other aerobic endospore forming bacteria. In book: Topley and Wilsons Microbiology and microbiological infections 2005, 10th ed vol 2. London: Arnold. [CrossRef]
- Turnbull, P.C.B. Guidelines for the Surveillance and Control of Anthrax in Humans and Animals. 3rd ed. World Health Organization. https://iris.who. 1066. [Google Scholar]
- Brook, I. The prophylaxis and treatment of anthrax. Int J Antimicrob Agents 2002, 20, 320–5. [Google Scholar] [CrossRef] [PubMed]
- Kolbe, A.; Yuen, M.G.; Doyle, B.K. A case of human cutaneous anthrax. Med J Aust 2006, 185, 281–2. [Google Scholar] [CrossRef] [PubMed]
- Karbalaei, Z.B.M.; Ghavidel, M.; Farsiani, H.; Ghazvini, K. Cutaneous anthrax in the northeast of Iran: A case report and review of the literature. Rev Clini Med 2018, 5, 26–8. [Google Scholar] [CrossRef]
- Ray, T.K.; Hutin, Y.J.; Murhekar, M.V. Cutaneous anthrax, West Bengal, India, 2007. Emerg Infect Dis. 2009, 15, 497–9. [Google Scholar] [CrossRef] [PubMed]
- Rao, G.R.R.; Padmaja, J.; Lalitha, M.K.; Rao, P.V.K.; Gopal, K.V.T.; Kumar, H.K.Y.; Mohanraj, P. An outbreak of cutaneous anthrax in a non-endemic district – Vishakapatnam in Andhra Pradesh. Indian J Dermatol Venereol Leprol 2005, 71, 102–5. [Google Scholar] [CrossRef] [PubMed]
- Kisaakye, E.; Ario, A.R.; Bainomugisha, K.; Cossaboom, C.M.; Lowe, D.; Bulage, L.; Kadobera, D.; Sekamatte, M.; Lubwama, B.; Tumusiime, D. , Tusiime, P., Downing, R., Buule, J., Lutwama, J., Salzer, J.S., Matkovic, E.; Ritter, J.; Gary, J.; Zhu, B.P. Outbreak of Anthrax Associated with Handling and Eating Meat from a Cow, Uganda, 2018. Emerg Infect Dis 2020, 26, 2799–2806. [Google Scholar] [CrossRef] [PubMed]
- Thappa, D.M.; Dave, S.; Karthikeyan, K.; Gupta Shelly. JIPMER. An outbreak of human anthrax: a report of 15 cases of Cutaneous anthrax. Indian J dermatol 2000, 45, 186–91. [Google Scholar]
- Procop, G.W.; Church, D.L. ; Hall,, G.S.; Janda, W.M.; Koneman, E.W.; Schreckenberger P.; Woods, J.L. Aerobic and facultative Gram-positive bacilli. Koneman’s Color Atlas and Textbook of Diagnostic Microbiology. 7th ed. Wolters Kluwer Health, Philadelphia, 2017. 775-783.
- Guastalegname, M.; Rondinone, V.; Lucifora, G.; et al. An Outbreak of Human Systemic Anthrax, including One Case of Anthrax Meningitis, Occurred in Calabria Region (Italy): A Description of a Successful One Health Approach. Life 2022, 12, 909. [Google Scholar] [CrossRef] [PubMed]
- Tuncali, D.; Akbuga, U.B.; Aslan, G. Ankara Education and Research Hospital, Department of Plastic Reconstructive and Anaesthetic Surgery, Cebeci, Ankara, Turkey. Indian J Plastic Surg 2004, 37, 131–3. [Google Scholar]
- Thirty seven human anthrax cases in northern Iraq outbreak. Available online: https://reliefweb.int/report/iraq/37-human-anthrax-cases-northern-iraq-outbreak (accessed on 3 March 2024).
- Zhao, Y.; Lafta, R.; Hagopian, A.; Flaxman, A.D. The epidemiology of 32 selected communicable diseases in Iraq, 2004-2016. Int J Infect Dis 2019, 89, 102–9. [Google Scholar] [CrossRef] [PubMed]
- Amiri, B.; Ghaderi, E.; Mohamadi, P.; Shirzadi, S.; Afrasiabian, S.; Salimi Zand, H.; Karimi, A.; Goodarzi, E.; Khazaei, Z.; Moayed, L. Geographical distribution of Anthrax using Geographic Information System (GIS) during 2010-2015 in Iran. Med J Islam Repub Iran. 2021, 17, 35–277. [Google Scholar] [CrossRef] [PubMed]
- Hanna, P.C.; Ireland, J.A. Understanding Bacillus anthracis pathogenesis. Trends Microbiol 1999, 7, 180–2. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, A.; Khan, S.U.; Hasnat, M.A.; et al. Anthrax outbreaks in Bangladesh, 2009-2010. Am J Trop Med Hyg 2012, 86, 703–10. [Google Scholar] [CrossRef] [PubMed]
- Kibar, O.M. Suspected cutaneous anthrax in rural areas. J Infect Dev Ctries 2019, 13, 118–22. [Google Scholar] [CrossRef] [PubMed]
- Jernigan, D.B.; Raghunathan, P.L.; Bell, B.P.; Brechner, R.; Bresnitz, E.A.; Butler, J.C.; Cetron, M.; Cohen, M.; Doyle, T.; Fischer, M.; Greene, C.; Griffith, K.S.; Guarner, J.; Hadler, J.L.; Hayslett, J.A.; Meyer, R.; Petersen, L.R.; Phillips, m M. ; Pinner, R.; Popovic, T. National Anthrax Epidemiologic Investigation Team. Investigation of bioterrorism-related anthrax, United States, 2001: epidemiologic findings. Emerg Infec Dis 2002, 8, 1019–1028. [Google Scholar] [CrossRef] [PubMed]
- Inglesby, T.V.; Henderson, D.A.; Bartlett, J.G.; Ascher, M.S.; Eitzen, E.; Friedlander, A.M.; Hauer, J.; McDade, J.; Osterholm, M.T.; O'Toole, T.; Parker, G.; Perl, T.M.; Russell, P.K.; Tonat, K. Anthrax as a biological weapon: medical and public health management. Working Group on Civilian Biodefense. JAMA 1999, 281, 1735–1745. [Google Scholar] [CrossRef] [PubMed]
- Kamal, S.M.; Rashid, A.K.; Bakar, M.A.; Ahad, M.A. Anthrax: an update. Asian Pac J Trop Biomed 2011, 1, 496–501. [Google Scholar] [CrossRef]
Figure 1.
shows the vesicle formation on the lesion.

Figure 2.
Direct smear shows Gram-positive bacilli isolated from swabs collected from the lesion.

Figure 3.
Blood agar shows white creamy, non-hemolytic, 2-4 mm in diameter with slightly moist non-glossy colonies.
Figure 3.
Blood agar shows white creamy, non-hemolytic, 2-4 mm in diameter with slightly moist non-glossy colonies.
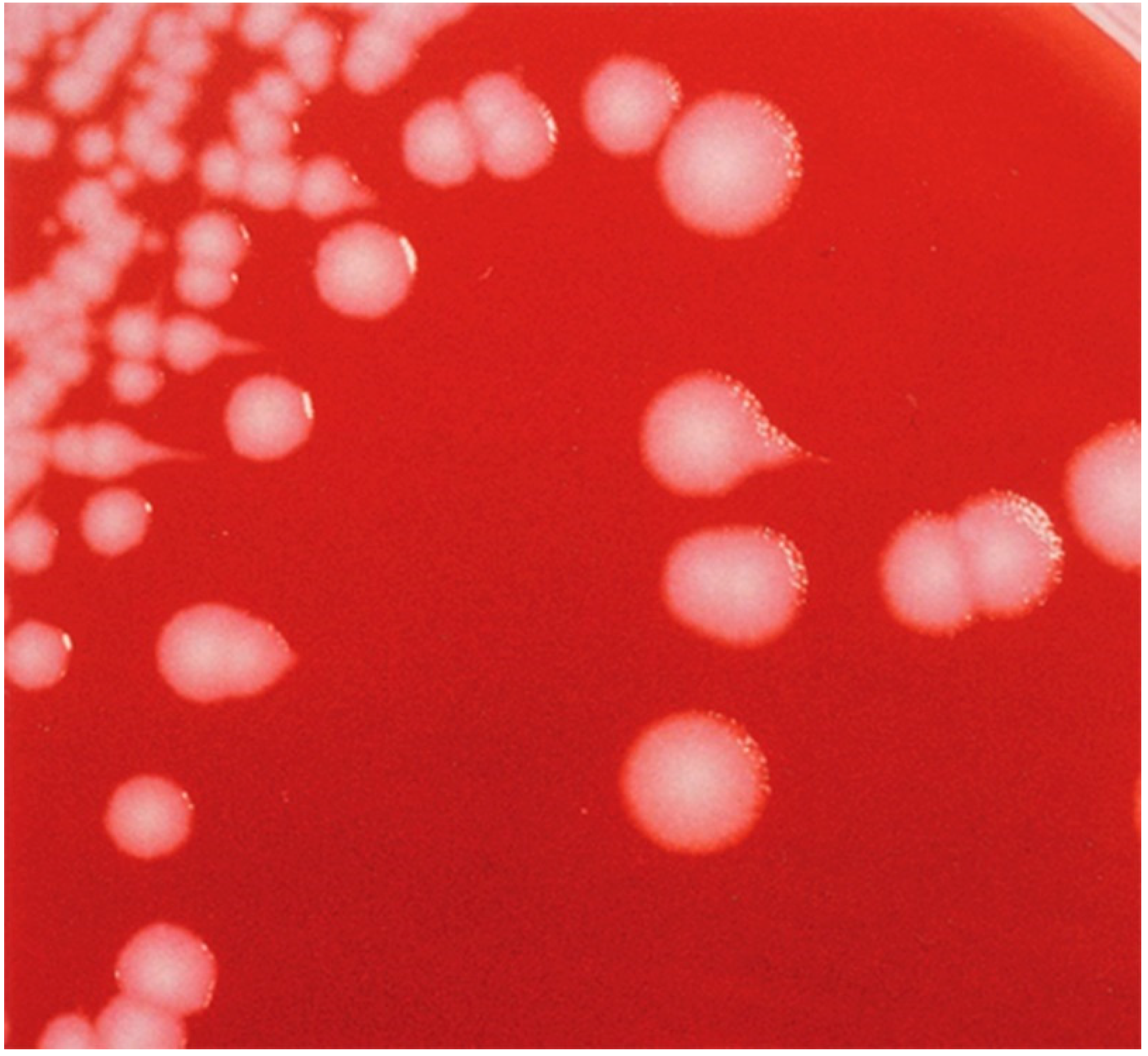
Figure 4.
The scar formation on the lesion after treatment.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



