
Submitted:
29 July 2024
Posted:
30 July 2024
You are already at the latest version
Abstract
The Chinese community is one of the main minorities in Colombia, and although China has made advances in public health, it faces a growing burden of cardiovascular diseases. This study focuses on evaluating cardiovascular risk factors in Chinese immigrants in Barranquilla, Colombia, due to the lack of specific data on this population. Methods: A cross-sectional study was conducted with 67 Chinese immigrants over 18 years of age residing in Barranquilla. Sociodemographic, anthropometric, clinical, and biochemical data were collected through structured interviews and medical record reviews. Cardiovascular risk was estimated using the 10-year ASCVD (Atherosclerotic Cardiovascular Disease) formula from the ACC/AHA. Statistical tests were employed to assess significant differences and relationships between variables. Results: The sample included 54% women with an average age of 53 years. 75% were over 45 years old, with the main occupations being trade (43%) and homemaking (40%). 54% had social security. Significant differences were observed in systolic blood pressure and the prevalence of smoking and alcoholism between men and women. Women had higher levels of HDL and lower creatinine, while men had higher levels of hemoglobin and creatinine. Cardiovascular risk was high in 9% of cases, moderate in 39%, and low in 52%. Conclusions: Chinese immigrants in Barranquilla present a significant prevalence of cardiovascular risk factors influenced by their socioeconomic situation and barriers to accessing healthcare. Interventions should focus on improving access to healthcare services and promoting healthy lifestyles for this vulnerable community.
Keywords:
Cardiovascular
; Chinese
; Immigrants
; Lifestyles
; Caribbean Region Colombian
1. Introduction
According to the International Organization for Migration (IOM), there are currently more than 107 million Chinese immigrants living abroad, and if their descendants are included, the number increases to around 60 million. In Colombia, the community from China is considered the largest Asian community according to the 2018 National Population and Housing Census conducted by the National Administrative Department of Statistics (DANE) [1].
In recent decades, China has made significant progress in public health but also faces challenges such as an aging population and a growing burden of non-communicable diseases. The prevalence of cardiovascular risk factors such as smoking, obesity, and diabetes has increased due to rapid socioeconomic and lifestyle changes. However, little is known about these risk factors in the global Chinese immigrant population, making their control difficult [2,3].
Chinese immigrants in countries such as the United States and Canada face significant challenges in accessing healthcare due to language, cultural, and economic barriers [4,5,6]. In Colombia, there is little information about the health of Chinese immigrants, generating particular interest in studying their sociodemographic, health, and lifestyle characteristics, as well as their cardiovascular risk [7].
Cardiovascular risk factors and disease are topics of interest for public health and medical research. In China, cardiovascular disease is the leading cause of death. Factors such as hypertension, smoking, and diabetes have a high prevalence in the Chinese population, and these risk factors also affect Chinese immigrants who may adopt less healthy lifestyles in host countries [5,8].
In Canada, a higher incidence of diabetes was found among Chinese immigrants compared to the local population [9]. In Madrid, high prevalence of smoking, hypertension, diabetes, dyslipidemia, and overweight was reported in the Chinese immigrant population. Chinese immigrants may face additional obstacles to accessing healthcare due to language, cultural, and financial barriers, highlighting the need for specific studies on their health in Colombia [10,11].
Given the lack of information on the Chinese immigrant population in Barranquilla (CO), whose demographic presence is quite significant, this study aims to describe their sociodemographic and health characteristics and evaluate their cardiovascular risk to improve understanding and healthcare for this community in the region.
2. Materials and Methods
2.1. Subjects
The study population included 67 Chinese immigrant patients residing in Barranquilla, Colombia. Subjects were selected from a non-probabilistic sample in health brigades and sociodemographic information campaigns. Subjects included had to be born in China, be over 18 years of age, and have resided in Barranquilla for at least one year. Those with severe medical conditions that prevented their participation were excluded. Sociodemographic and clinical data were collected through structured interviews and medical record reviews, ensuring informed consent from all participants.
2.2. Variables
The variables of interest in this study were divided into several categories. Sociodemographic variables (age, sex, occupation, educational level, and social security system). Anthropometric and clinical variables (BMI, SBP, DBP, family history, comorbidities, and risk behaviors). Biochemical variables (glucose, hemoglobin (Hb), lipid profile, and renal function). Cardiovascular risk was estimated using the 10-year ASCVD (Atherosclerotic Cardiovascular Disease) formula from the ACC/AHA, categorized as low, moderate, and high risk. These variables were analyzed to identify their relationship with cardiovascular risk, also considering lifestyle factors and barriers to accessing the healthcare system.
2.3. Statistical Methods
The Kolmogorov-Smirnov test was used to assess data normality. Quantitative variables were presented as medians and interquartile ranges or mean and standard deviation according to normality. Absolute and relative frequencies were used to describe categorical variables. The Wilcox Sum rank test was used to evaluate medians obtained between male and female patients. The Fisher's exact test was used to analyze categorical variables. The relationship between cardiovascular risk by ASCVD ACC/AHA score (low risk, moderate risk, and high risk), lifestyle, and barriers to accessing the healthcare system was explored through multiple correspondence analysis. A p-value < 0.05 was considered statistically significant. R-CRAN software version 4.3.2 was used for statistical analysis.
3. Results
A total of 67 Chinese immigrant patients were included. Most were female (54%) with an average age of 53±13 years. 75% of the patients were over 45 years old. Regarding occupation, most were engaged in trade (43%) and homemaking (40%). Up to 55% of the patients had completed secondary education. Of the total patients, 35 (54%) had social security, of which 32 (91%) were affiliated with the contributory system and 3 (9%) with the subsidized system.

Table 1.
Sociodemographic Characteristics of Chinese Immigrant Patients.
| Characteristic | n = 67 ¹ |
|---|---|
| Age | 53 ± 13 |
| Gender | |
| Female | 36 (54%) |
| Male | 31 (46%) |
| Occupation | |
| Merchant | 29 (43%) |
| Homemaker | 27 (40%) |
| Self-employed | 5 (7.5%) |
| Education | |
| Primary | 9 (13%) |
| Secondary | 37 (55%) |
| High School | 15 (22%) |
| Technical | 4 (6.0%) |
| Technological | 1 (1.5%) |
| University | 1 (1.5%) |
| Social Security | 35 (54%) |
| Regime | |
| Contributory | 32 (48%) |
| Subsidized | 3 (4.5%) |
¹ Mean ± SD; n (%).
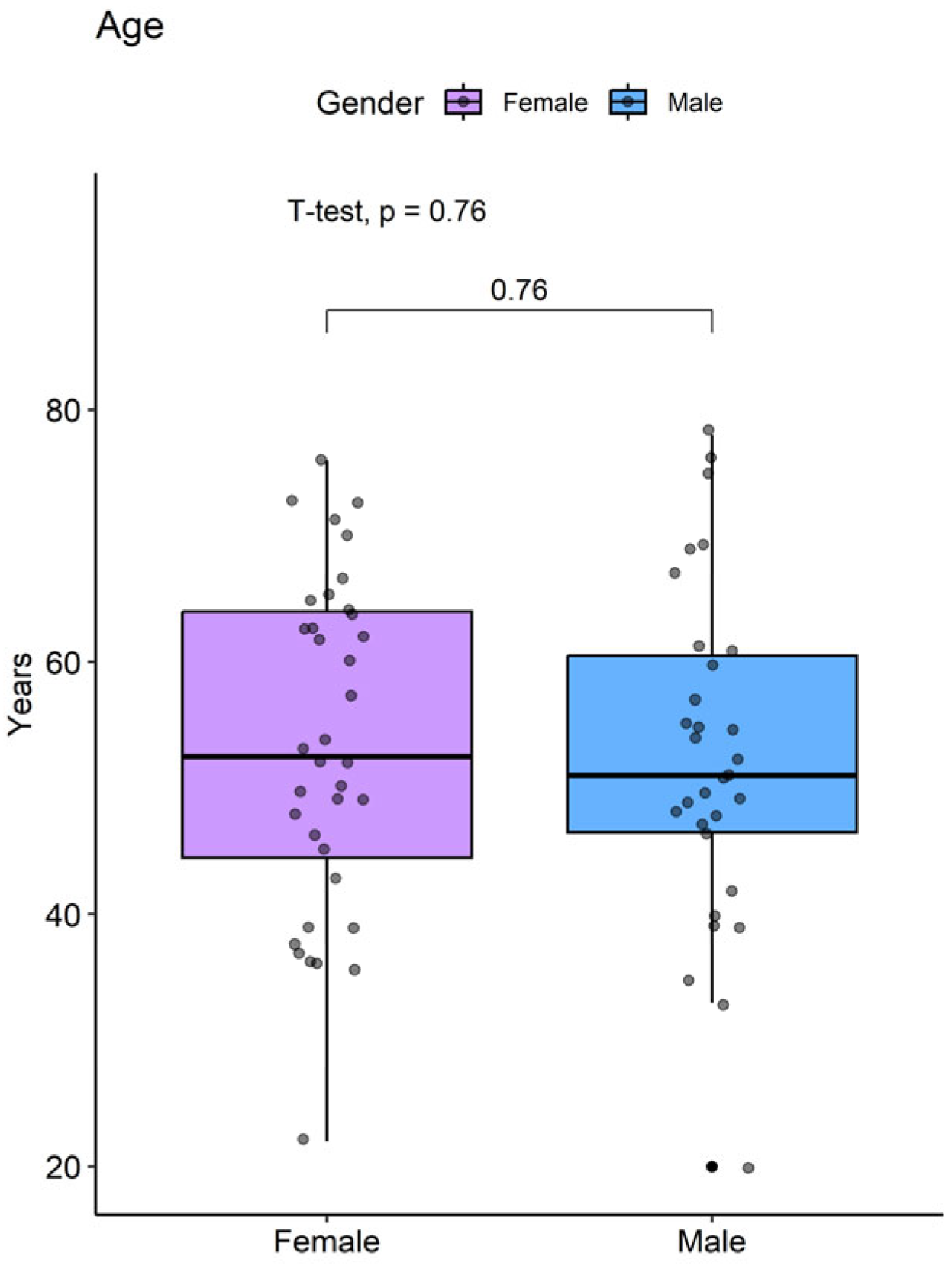
There were no significant differences in the ages of the patients between males (52.6 ± 13.2 years) and females (53.5 ± 13.1 years) (p=0.73).
Figure 1.
Age Distribution Between Males and Females
3.1. Anthropometric Parameters and Pathological Background
Table 2 summarizes the comparison of anthropometric parameters and pathological background (family, comorbidities, surgical) between male and female patients. BMI and nutritional status were similar between both groups (p>0.05). Dyslipidemia was the most frequent comorbidity (12%), followed by arterial hypertension (6%). No statistical differences were observed in DBP, prevalence of comorbidities, or surgical history studied (all p>0.05) (Table 2).
A significant difference was observed in Systolic Blood Pressure (SBP); female patients (125 IQR: 90 180 mmHg) reported a higher median SBP compared to males (120 IQR: 90 160 mmHg) (p = 0.0302) (Figure 2). Additionally, significant differences were identified in the prevalence of smoking (52% vs 0%) (p<0.001) and alcoholism (35% vs 3%) (p < 0.0013), being more prevalent in males (Table 2).
3.2. Biochemical Profile
In the analysis of the biochemical profile of Chinese immigrant patients, a statistically significant difference was observed in hemoglobin (Hb) levels. Female patients reported a median of 13.1 g/dl (IQR:11-15), while males obtained a median of 15.4 g/dl (IQR: 12.1-18.2) (p < 0.001) (Table 3).
Regarding the lipid profile, the median HDL was significantly higher in female patients with a value of 53 mg/dl (IQR: 28-95) compared to male patients with a median of 44 mg/dl (IQR: 29-88) (p = 0.020). In the evaluation of renal function, male patients obtained significantly higher medians in serum creatinine (0.9 IQR: 0.6-1.3 vs. 0.7 IQR: 0.5-1.2 mg/dl), blood urea nitrogen (17 IQR: 10-26 vs. 15.5 IQR: 7-21 mg/dl), and urea (36 IQR: 21-56 vs. 33 IQR: 15-45 mg/dl) compared to female patients (all p < 0.05). No significant differences were observed in the medians of glucose, platelets (PLQ), total cholesterol (CLT), triglycerides (TGL), low-density lipoprotein (LDL), or glomerular filtration rate (GFR) between the groups (all p > 0.05) (Figure 3).
3.3. ASCVD ACC/AHA Cardiovascular Risk Profile and Renal Function
The 10-year ASCVD (Atherosclerotic Cardiovascular Disease) risk of the ACC/AHA (American College of Cardiology/American Heart Association) was estimated and related to renal function parameters (Table 4). It was observed that 6 (9%) patients had high ASCVD risk (≥20%), 26 (39%) moderate risk (5-19.9%), and 35 (52%) low risk (<5%) (Table 4).
Significant differences were observed in the ages of the stratified ASCVD risk groups, with median ages of 48 years (IQR: 20-67) in the low-risk group, 61 years (IQR: 35-73) in the moderate-risk group, and 76 years (IQR: 67-78) in the high-risk group (p<0.001). Regarding sex, male patients had significantly higher proportions of high risk (67% vs 33%) and moderate risk (62% vs 38%) compared to females (p=0.04).
When analyzing renal function, it was observed that patients with high ASCVD risk had a significantly lower median GFR (ml/min/m²) (78 IQR: 47-99) compared to patients with moderate risk (94 IQR: 61-146) and low risk (100 IQR: 71-147) (p=0.02). Patients with low risk reported a significantly lower median BUN compared to patients with moderate risk (15 IQR:7-22 vs. 17 IQR: 10-26 p=0.01) (Figure 4).
In this study, 18/67 (27%) patients presented hematuria, and 7/67 (10%) reported proteinuria in urine tests. No statistical differences were observed when comparing the prevalence of hematuria and proteinuria according to cardiovascular risk stratification (Table 4).
3.4. Lifestyle and ASCVD ACC/AHA Cardiovascular Risk Profile
In this study, a multiple correspondence analysis was performed to explore the relationship between 10-year cardiovascular risk stratified by ASCVD ACC/AHA formula as low, moderate, and high risk, and lifestyles (fruit/vegetable consumption, physical activity, and fluid intake). According to the Cos2 parameter (square of the cosine), the variables best represented in the analysis dimensions are physical activity, no daily fruit consumption, and fluid intake when possible. It was observed that patients with high 10-year ASCVD risk tended to engage in physical activity (>30 min/day), and a relationship was observed between fluid intake when possible and no daily fruit consumption (Figure 5).
3.5. Medical Care Opportunity and ASCVD ACC/AHA Cardiovascular Risk Profile**
In most patients (58%), the last medical visit was more than 2 years ago, and 64% attended only when necessary. Regarding the difficulty of care, 13/67 (19%) considered it very difficult, and 23/67 (34%) reported it as difficult. Most patients reported that language (90%) was the main barrier to medical care.
In the multiple correspondence analysis, the variables best represented by Cos2 were difficulty in care (very difficult, difficult, and not difficult) and barriers to care (language, lack of knowledge). It was observed that patients with high ASCVD risk tended to face barriers to medical care due to language, with last medical visits over 2 years, while patients with low ASCVD risk tended to attend only when necessary to private health entities (Figure 6).
4. Discussion
The study population included 67 Chinese immigrant patients residing in Barranquilla, Colombia. The sample was predominantly female (54%) with an average age of 53 years, which is consistent with previous studies showing a higher proportion of women in immigrant communities. Most participants were engaged in trade (43%) or homemaking (40%), and more than half (55%) had completed secondary education. Social security was present in 54% of cases, with a predominance of the contributory system [7,12].
These results reflect a situation of socioeconomic vulnerability, especially in terms of education and access to social security [13]. The prevalence of informal occupations such as trade and homemaking may negatively influence access to healthcare services and the adoption of healthy lifestyles. Informal occupations, which often do not provide stable income or employment benefits such as health insurance, can limit individuals' ability to finance their medical care, leaving them more exposed to unmet health risks [14].
Furthermore, the lack of higher education limits employment opportunities and can lead to lower incomes, which in turn can restrict access to healthy foods, safe living environments, and the ability to participate in regular physical activities. Education has been shown to be a critical determinant of health, as it influences knowledge about healthy living habits, the use of preventive services, and adherence to medical treatments [15,16].
Access to the healthcare system is crucial for managing chronic diseases and preventing severe complications. Lack of coverage or inadequate coverage can lead to delays in diagnosis and treatment, worsening health outcomes. The combination of these socioeconomic factors creates an environment where Chinese immigrants may face significant difficulties in maintaining good health. Job insecurity and lack of social security can also increase stress and anxiety, known risk factors for cardiovascular and other chronic diseases [17].
The situation of socioeconomic vulnerability, particularly in terms of education and formal access to the social security system, as well as the prevalence of informal occupations within the commercial sector or exclusive homemaking in the case of women, may negatively influence access to healthcare services and the adoption of healthy lifestyles. Poor socioeconomic conditions have been shown to lead to lower quality of life and higher health risks in migrant populations, with a relationship found between low educational levels and higher rates of chronic diseases due to lack of access to health systems and preventive services [18,19].
The high prevalence of dyslipidemia and arterial hypertension highlights the need for interventions aimed at preventing and managing these risk factors. Dyslipidemia, characterized by abnormal blood lipid levels, is an important risk factor for the development of cardiovascular diseases, especially in immigrant populations that may experience changes in diet and lifestyle. Studies have found that Chinese immigrants in various countries have a high prevalence of dyslipidemia due to the adoption of Western diets rich in saturated fats and refined carbohydrates [15].
Arterial hypertension, identified in 6% of patients, is another critical condition requiring attention. Uncontrolled hypertension can lead to severe complications such as cardiovascular disease, kidney failure, and strokes [20,21]. The significant difference in SBP between men and women could be related to hormonal factors, differences in stress management, or variations in access to and adherence to medical treatments. Previous studies have shown that postmenopausal women may have higher SBP due to decreased estrogen, increasing cardiovascular risk [22,23].
The higher prevalence of smoking and alcoholism in men is also a concerning finding, as these negative health habits are well-established risk factors for a variety of chronic diseases, including cardiovascular diseases, cancer, and liver diseases [24,25,26]. The high prevalence of smoking and alcoholism among Chinese immigrant men may be influenced by cultural, social, and economic factors. Studies have observed that smoking and alcohol consumption rates were significantly higher among Asian immigrant men due to social pressure and the lack of culturally appropriate intervention programs [27].
Early intervention and education on healthy habits are fundamental to reducing cardiovascular risk. Interventions should include tobacco and alcohol cessation programs, education on the risks associated with these habits, and the development of community support strategies. Interventions should begin as soon as possible after immigration, focusing on nutritional education, promoting physical activity, and managing stress to prevent the development of dyslipidemia and hypertension [28,29].
Women presented lower levels of hemoglobin, indicating potential nutritional factors. However, women, especially premenopausal, typically have lower hemoglobin levels due to blood loss during menstruation [30]. Additionally, differences in dietary intake and iron absorption may contribute to these lower levels. In China, women have been observed to have a higher prevalence of anemia compared to men, associated with diet and socioeconomic status [31,32].
Higher HDL levels in women are consistent with literature showing that women generally tend to have higher HDL levels than men, possibly due to the protective effects of estrogen. Elevated HDL in women is an important protective factor against cardiovascular disease, which is particularly relevant in assessing cardiovascular risk in immigrant populations [33,34].
Men showed higher levels of creatinine, GFR, blood urea nitrogen, and urea. These parameters are indicators of renal function and protein metabolism. Higher muscle mass in men generally leads to higher creatinine levels. Regarding GFR, studies have shown that men tend to have a higher glomerular filtration rate but are also more susceptible to a reduction in this rate with age and the presence of chronic diseases such as hypertension and diabetes [35]. Moreover, Chinese men tend to consume more protein, resulting in higher levels of these markers. Additionally, risk factors such as hypertension and diabetes, which are prevalent in Chinese populations, can contribute to renal dysfunction [36].
The cardiovascular risk estimated using the ASCVD ACC/AHA formula showed that 9% of patients had high risk, 39% moderate risk, and 52% low risk. Significant differences in ages and gender between risk groups indicate that men, especially older men, are more frequent in the high-risk group [37].
These findings show that Chinese men have a higher risk of cardiovascular disease than women, particularly as they age [38]. The prevalence of risk factors such as smoking, hypertension, and dyslipidemia is higher in men, contributing to their higher cardiovascular risk. Furthermore, lifestyle changes after migration, such as adopting less healthy diets and reducing physical activity, can exacerbate these risks [39].
The correspondence found between high ASCVD risk and lack of physical activity (>30 min/day), as well as fluid and fruit consumption patterns, indicated possible lack of regular access to healthy foods. This suggests that although these patients try to maintain an adequate level of physical activity, they may face barriers in their daily diet due to limited availability of healthy foods or economic restrictions. Regular physical activity is an essential component in reducing cardiovascular risk, but its effectiveness may be compromised if not complemented by a balanced diet rich in fruits and vegetables [40,41].
Moreover, most patients reported significant difficulties in accessing medical care, primarily due to language barriers. This language barrier can affect patients' ability to communicate effectively with healthcare professionals, understand medical instructions, and adhere to prescribed treatments [42]. The last medical visit over two years ago in most cases reflects a worrying disconnection with the healthcare system, which can lead to suboptimal management of chronic diseases and an increase in health complications.
Language barriers have been demonstrated to be one of the main reasons immigrants do not seek or delay medical care. Studies have reported that language barriers can lead to lower treatment adherence, inadequate understanding of medical instructions, and consequently poorer prognosis in chronic diseases. These barriers can also result in inappropriate use of emergency services instead of regular visits to primary care doctors, contributing to fragmented care and worse health outcomes [43].
5. Conclusions
The findings reflect a marked socioeconomic vulnerability, especially in terms of education and access to social security. The prevalence of informal occupations such as trade and homemaking limits access to healthcare services and contributes to the adoption of less healthy lifestyles. The lack of higher education restricts employment opportunities, leading to lower incomes and hindering access to healthy foods and regular physical activities. This socioeconomic vulnerability is closely linked to higher health risks and lower quality of life, highlighting the need for specific interventions to improve the socioeconomic conditions of this population.
Difficulties in communicating with healthcare professionals, understanding medical instructions, and adhering to prescribed treatments contribute to suboptimal management of chronic diseases and an increase in health complications. The disconnection with the healthcare system reflected in the lack of regular medical visits exacerbates these problems and leads to worse health outcomes. Improving this situation requires a multidimensional approach that considers both socioeconomic determinants and clinical risk factors and barriers to accessing healthcare. Implementing specific and culturally sensitive intervention strategies can significantly reduce health risks and promote better overall well-being in this community.
Author Contributions
Conceptualization, L.T.K., K.C.M., A.C.B., A.C.-B. and H.J.G.-T.; methodology, H.J.G.-T. AND A.D.V.; validation, L.T.K. and K.C.M.; formal analysis, H.J.G.-T. AND A.D.V.; data curation, A.C.B. and A.C.-B.; writing—original draft preparation, L.T.K., K.C.M., A.C.B., A.C.-B., A.D.V. and H.J.G.-T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding and is part of the final research of the Internal Medicine residency program of the Universidad Simón Bolívar (BAQ, CO) of the Lin Tan Kuang and Kevin Castro Márquez.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of the Clínica de la Costa (BAQ, CO) on May 16, 2023 and Institutional Review Board of the Universidad Simón Bolívar, code 640 – 012/2023 INV on 23 April 2023.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
All data underlying the results are available as part of this article.
Acknowledgments
We would like to express our gratitude to the Internal Medicine residency program of the Universidad Simón Bolívar (BAQ, CO), for providing us with the opportunity to train in this beautiful branch of medicine.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Valbuena Ramírez, G.; Castellanos Caballero, E.; Cristancho Fajardo, C. East Asian Inmigration to Colombia: Chinese, Japanese, and South Korean Residents According to the 2018 National Population and Housing Census of Colombia, Universidad Externado de Colombia, 2021.
- Guerrero-Pinedo, F.; Ochoa-Zárate, L.; Salazar, C.J.; Carrillo-Gómez, D.C.; Paulo, M.; Flórez-Elvira, L.J.; Velasquez-Noreña, J.G. Association of Traditional Cardiovascular Risk Factors in Adults Younger than 55 Years with Coronary Heart Disease. Case-Control Study. SAGE open Med. 2020, 8, 2050312120932703. [Google Scholar] [CrossRef]
- Li, X.; Wu, C.; Lu, J.; Chen, B.; Li, Y.; Yang, Y.; Hu, S.; Li, J. Cardiovascular Risk Factors in China: A Nationwide Population-Based Cohort Study. Lancet. Public Heal. 2020, 5, e672–e681. [Google Scholar] [CrossRef] [PubMed]
- Zhu, A.L.; Le, A.D.; Li, Y.; Palaniappan, L.P.; Srinivasan, M.; Shah, N.S.; Wong, S.S.; Valero-Elizondo, J.; Elfassy, T.; Yang, E. Social Determinants of Cardiovascular Risk Factors Among Asian American Subgroups. J. Am. Heart Assoc. 2024, 13, e032509. [Google Scholar] [CrossRef] [PubMed]
- Clough, J.; Lee, S.; Chae, D.H. Barriers to Health Care among Asian Immigrants in the United States: A Traditional Review. J. Health Care Poor Underserved 2013, 24, 384–403. [Google Scholar] [CrossRef] [PubMed]
- Lai, D.W.L.; Chau, S.B.Y. Predictors of Health Service Barriers for Older Chinese Immigrants in Canada. Health Soc. Work 2007, 32, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Gomez, D.A.; Diaz, L.M. Chinese Organizations in Colombia. Migr. y Desarro. 2016, 14, 75–110. [Google Scholar] [CrossRef]
- Wang, Z.-W. Status of Cardiovascular Disease in China. J. Geriatr. Cardiol. 2023, 20, 397–398. [Google Scholar] [CrossRef] [PubMed]
- Sebastian, S.A.; Avanthika, C.; Jhaveri, S.; Carrera, K.G.; Camacho L, G.P.; Balasubramanian, R. The Risk of Cardiovascular Disease Among Immigrants in Canada. Cureus 2022, 14, e22300. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Alvarez, E.; Lanborena, N.; Borrell, L.N. Cardiovascular Disease Risk Factors in Spain: A Comparison of Native and Immigrant Populations. PLoS One 2020, 15, e0242740. [Google Scholar] [CrossRef]
- Sebastian, S.A.; Sethi, Y.; Padda, I.; Johal, G. Ethnic Disparities in the Burden of Cardiovascular Disease Among Immigrants in Canada. Curr. Probl. Cardiol. 2024, 49, 102059. [Google Scholar] [CrossRef]
- García, J.L. China En Barranquilla. Memorias 2016, I–V. [Google Scholar] [CrossRef]
- Badanta, B.; Vega-Escaño, J.; Barrientos-Trigo, S.; Tarriño-Concejero, L.; García-Carpintero Muñoz, M.Á.; González-Cano-Caballero, M.; Barbero-Radío, A.; De-Pedro-Jimenez, D.; Lucchetti, G.; de Diego-Cordero, R. Acculturation, Health Behaviors, and Social Relations among Chinese Immigrants Living in Spain. Int. J. Environ. Res. Public Health 2021, 18. [Google Scholar] [CrossRef]
- Mazza, J.; Myers, M.; Orozco, M. Chinese Migration to Latin America and the Caribbean. 2016 Inter-American Dialogue 2016, 13. [Google Scholar]
- Gong, Z.; Zhao, D. Cardiovascular Diseases and Risk Factors among Chinese Immigrants. Intern. Emerg. Med. 2016, 11, 307–318. [Google Scholar] [CrossRef] [PubMed]
- Koirala, B.; Turkson-Ocran, R.; Baptiste, D.; Koirala, B.; Francis, L.; Davidson, P.; Himmelfarb, C.D.; Commodore-Mensah, Y. Heterogeneity of Cardiovascular Disease Risk Factors Among Asian Immigrants: Insights From the 2010 to 2018 National Health Interview Survey. J. Am. Heart Assoc. 2021, 10. [Google Scholar] [CrossRef]
- Diaz, J.; Taboada, I.; Abreu, A.; Vargas, L.; Polanco, Y.; Zorrilla, A.; Beatty, N. Evaluating Rural Health Disparities in Colombia: Identifying Barriers and Strategies to Advancing Refugee Health. Int. J. Environ. Res. Public Health 2023, 20, 6948. [Google Scholar] [CrossRef] [PubMed]
- Roncancio, D.J.; Cutter, S.L.; Nardocci, A.C. Social Vulnerability in Colombia. Int. J. Disaster Risk Reduct. 2020, 50, 101872. [Google Scholar] [CrossRef]
- Bustamante-matoma, H. Local Perspectives and Analysis of the Impact of Chinese Migration in Colombia. 2024, 15–41.
- Burnier, M.; Damianaki, A. Hypertension as Cardiovascular Risk Factor in Chronic Kidney Disease. Circ. Res. 2023, 132, 1050–1063. [Google Scholar] [CrossRef]
- Cipolla, M.J.; Liebeskind, D.S.; Chan, S.-L. The Importance of Comorbidities in Ischemic Stroke: Impact of Hypertension on the Cerebral Circulation. J. Cereb. Blood Flow Metab. 2018, 38, 2129–2149. [Google Scholar] [CrossRef]
- Jain, A.; Kumar, S.; Acharya, S.; Kabra, R.; Sawant, R. Assessment of Blood Pressure Variability in Postmenopausal Women. Cureus 2022, 14, e29471. [Google Scholar] [CrossRef]
- Migneco, A.; Ojetti, V.; Covino, M.; Mettimano, M.; Montebelli, M.R.; Leone, A.; Specchia, L.; Gasbarrini, A.; Savi, L. Increased Blood Pressure Variability in Menopause. Eur. Rev. Med. Pharmacol. Sci. 2008, 12, 89–95. [Google Scholar]
- Mukamal, K.J. The Effects of Smoking and Drinking on Cardiovascular Disease and Risk Factors. Alcohol Res. Health 2006, 29, 199–202. [Google Scholar]
- Rosoff, D.B.; Davey Smith, G.; Mehta, N.; Clarke, T.-K.; Lohoff, F.W. Evaluating the Relationship between Alcohol Consumption, Tobacco Use, and Cardiovascular Disease: A Multivariable Mendelian Randomization Study. PLoS Med. 2020, 17, e1003410. [Google Scholar] [CrossRef]
- Pelucchi, C.; Gallus, S.; Garavello, W.; Bosetti, C.; La Vecchia, C. Cancer Risk Associated with Alcohol and Tobacco Use: Focus on Upper Aero-Digestive Tract and Liver. Alcohol Res. Health 2006, 29, 193–198. [Google Scholar]
- White, M.; Harland, J.O.; Bhopal, R.S.; Unwin, N.; Alberti, K.G. Smoking and Alcohol Consumption in a UK Chinese Population. Public Health 2001, 115, 62–69. [Google Scholar] [CrossRef]
- Li, X.X.; Zhao, Y.; Huang, L.X.; Xu, H.X.; Liu, X.Y.; Yang, J.J.; Zhang, P.J.; Zhang, Y.H. Effects of Smoking and Alcohol Consumption on Lipid Profile in Male Adults in Northwest Rural China. Public Health 2018, 157, 7–13. [Google Scholar] [CrossRef]
- Nagao, T.; Nogawa, K.; Sakata, K.; Morimoto, H.; Morita, K.; Watanabe, Y.; Suwazono, Y. Effects of Alcohol Consumption and Smoking on the Onset of Hypertension in a Long-Term Longitudinal Study in a Male Workers’ Cohort. Int. J. Environ. Res. Public Health 2021, 18. [Google Scholar] [CrossRef]
- Todd, T.; Caroe, T. Newly Diagnosed Iron Deficiency Anaemia in a Premenopausal Woman. BMJ 2007, 334, 259. [Google Scholar] [CrossRef]
- Kalasuramath, S.; S, V.C.; Kumar, M.; Ginnavaram, V.; Deshpande, D. V Impact of Anemia, Iron Deficiency on Physical and Cardio Respiratory Fitness among Young Working Women in India. Artic. Indian J. Basic Appl. Med. Res. 2015, 408–415. [Google Scholar]
- Liao, Q.; Chinese Children, P.W. & P.W.I.D.E.S.G. [Prevalence of Iron Deficiency in Pregnant and Premenopausal Women in China: A Nationwide Epidemiological Survey]. Zhonghua Xue Ye Xue Za Zhi 2004, 25, 653–657. [Google Scholar]
- Yang, W.; Xiao, J.; Yang, Z.; Ji, L.; Jia, W.; Weng, J.; Lu, J.; Shan, Z.; Liu, J.; Tian, H.; et al. Serum Lipids and Lipoproteins in Chinese Men and Women. Circulation 2012, 125, 2212–2221. [Google Scholar] [CrossRef]
- Zhang, C.; Zhuang, Y.; Qiang, H.; Liu, X.; Xu, R.; Wu, Y. Relationship between Endogenous Estrogen Concentrations and Serum Cholesteryl Ester Transfer Protein Concentrations in Chinese Women. Clin. Chim. Acta 2001, 314, 77–83. [Google Scholar] [CrossRef]
- Noronha, I.L.; Santa-Catharina, G.P.; Andrade, L.; Coelho, V.A.; Jacob-Filho, W.; Elias, R.M. Glomerular Filtration in the Aging Population. Front. Med. 2022, 9, 769329. [Google Scholar] [CrossRef]
- Wei, H.; Yan, Y.; Gong, J.; Dong, J. Prevalence of Kidney Damage in Chinese Elderly: A Large-Scale Population-Based Study. BMC Nephrol. 2019, 20, 341. [Google Scholar] [CrossRef]
- Rodgers, J.L.; Jones, J.; Bolleddu, S.I.; Vanthenapalli, S.; Rodgers, L.E.; Shah, K.; Karia, K.; Panguluri, S.K. Cardiovascular Risks Associated with Gender and Aging. J. Cardiovasc. Dev. Dis. 2019, 6. [Google Scholar] [CrossRef]
- Ma, L.-Y.; Chen, W.-W.; Gao, R.-L.; Liu, L.-S.; Zhu, M.-L.; Wang, Y.-J.; Wu, Z.-S.; Li, H.-J.; Gu, D.-F.; Yang, Y.-J.; et al. China Cardiovascular Diseases Report 2018: An Updated Summary. J. Geriatr. Cardiol. 2020, 17, 1–8. [Google Scholar]
- Li, C.; Carolino, E.; Sousa, J. Dietary Acculturation and Food Habit Changes among Chinese Immigrants in Portugal. Nutrients 2023, 15. [Google Scholar] [CrossRef]
- Mora, S.; Cook, N.; Buring, J.E.; Ridker, P.M.; Lee, I.-M. Physical Activity and Reduced Risk of Cardiovascular Events: Potential Mediating Mechanisms. Circulation 2007, 116, 2110–2118. [Google Scholar] [CrossRef]
- Alissa, E.M.; Ferns, G.A. Dietary Fruits and Vegetables and Cardiovascular Diseases Risk. Crit. Rev. Food Sci. Nutr. 2017, 57, 1950–1962. [Google Scholar] [CrossRef]
- Noe-Bustamante, L.; Mora, L.; Ruiz, N.G. In Their Own Words: Asian Immigrants’ Experiences Navigating Language Barriers in the United States. Pew Res. Cent. 2022. [Google Scholar]
- Aparício, S.L.; Duarte, I.; Castro, L.; Nunes, R. Equity in the Access of Chinese Immigrants to Healthcare Services in Portugal. Int. J. Environ. Res. Public Health 2023, 20. [Google Scholar] [CrossRef]
Figure 2.
Comparison of BMI and Systolic Blood Pressure Between Males and Females
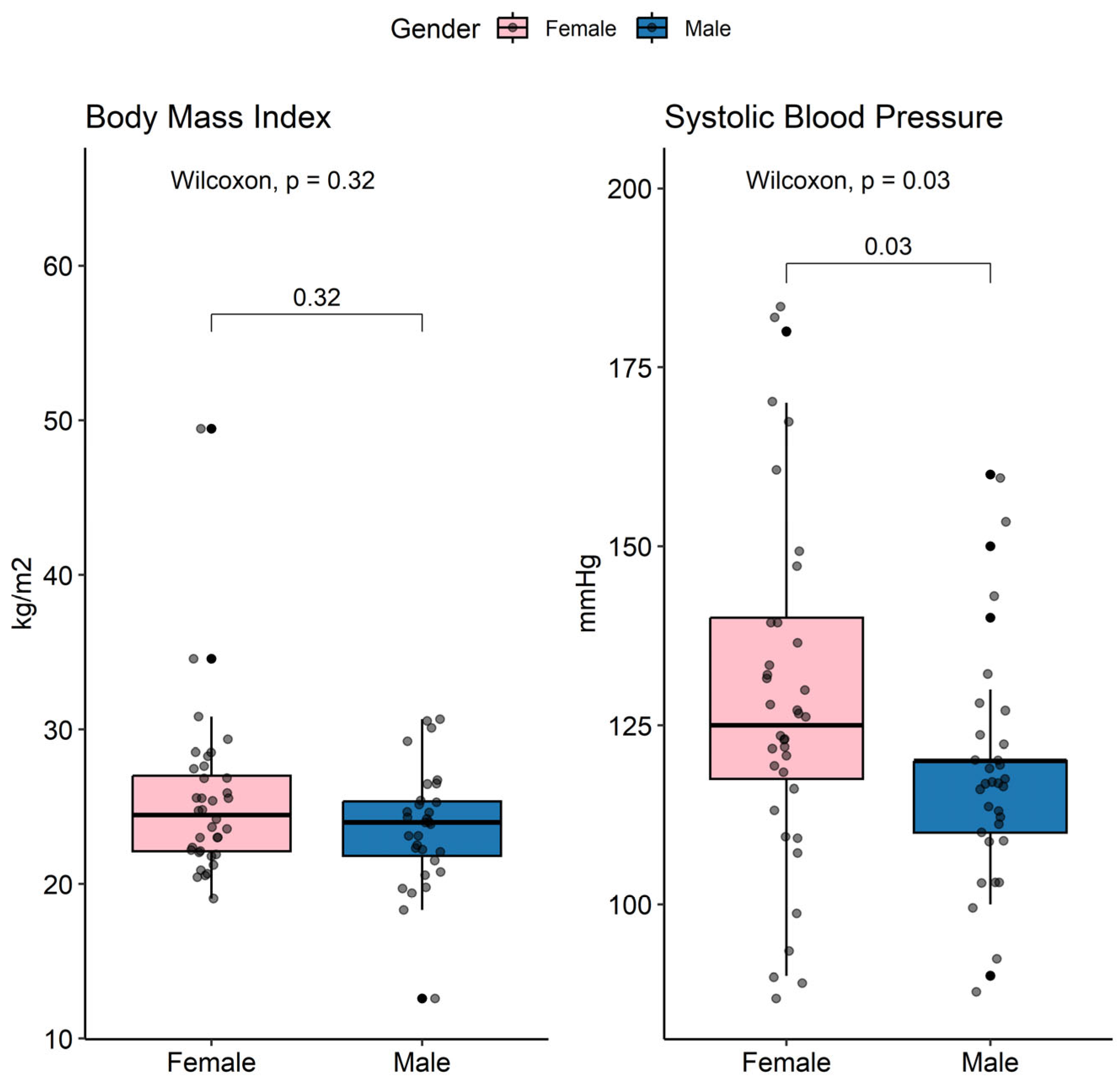
Figure 3.
Comparison of Lipid Profile and Renal Function Parameters Between Males and Females
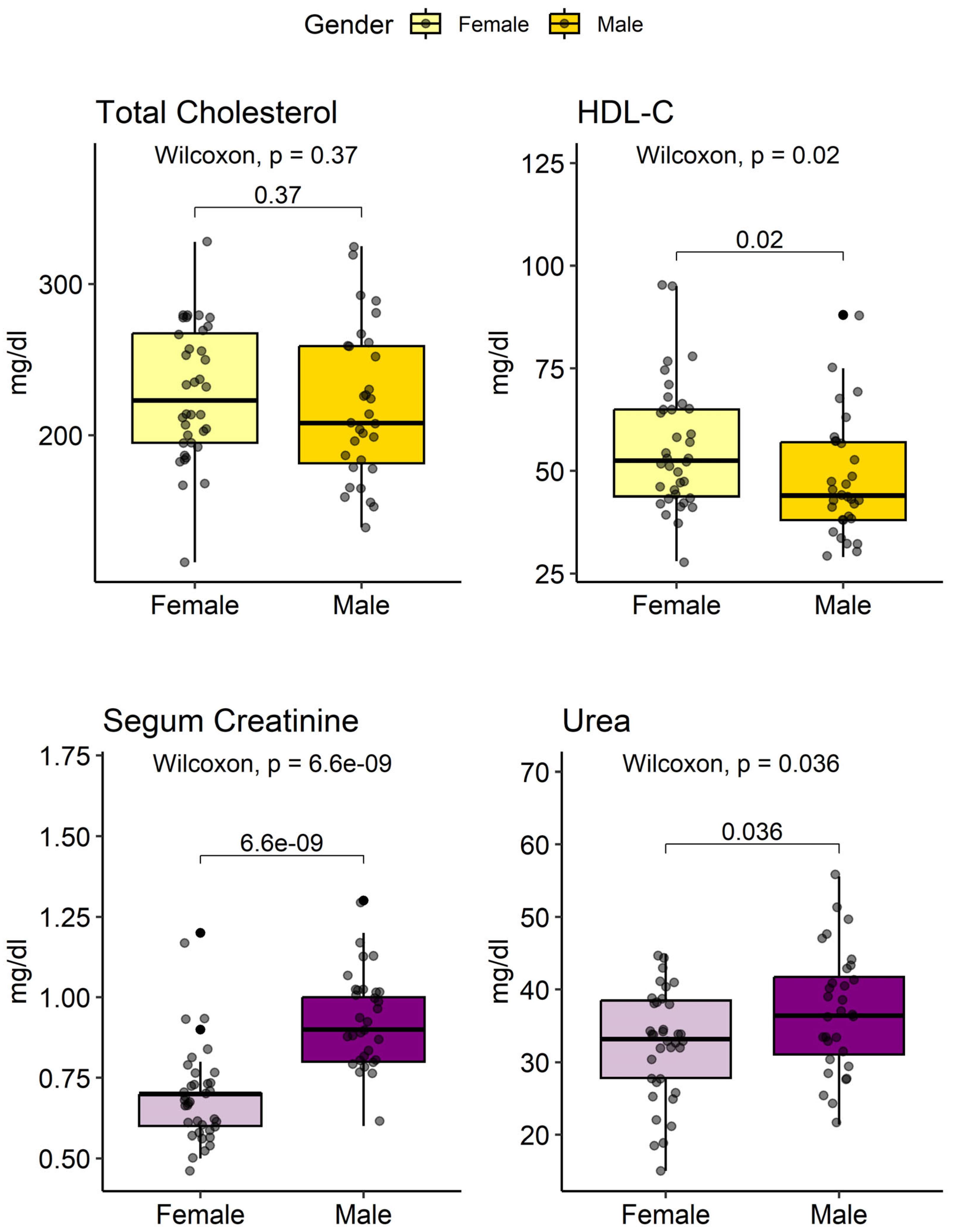
Figure 4.
Comparison of Glomerular Filtration Rate and Blood Urea Nitrogen Levels by ASCVD ACC/AHA Risk Stratification
Figure 4.
Comparison of Glomerular Filtration Rate and Blood Urea Nitrogen Levels by ASCVD ACC/AHA Risk Stratification
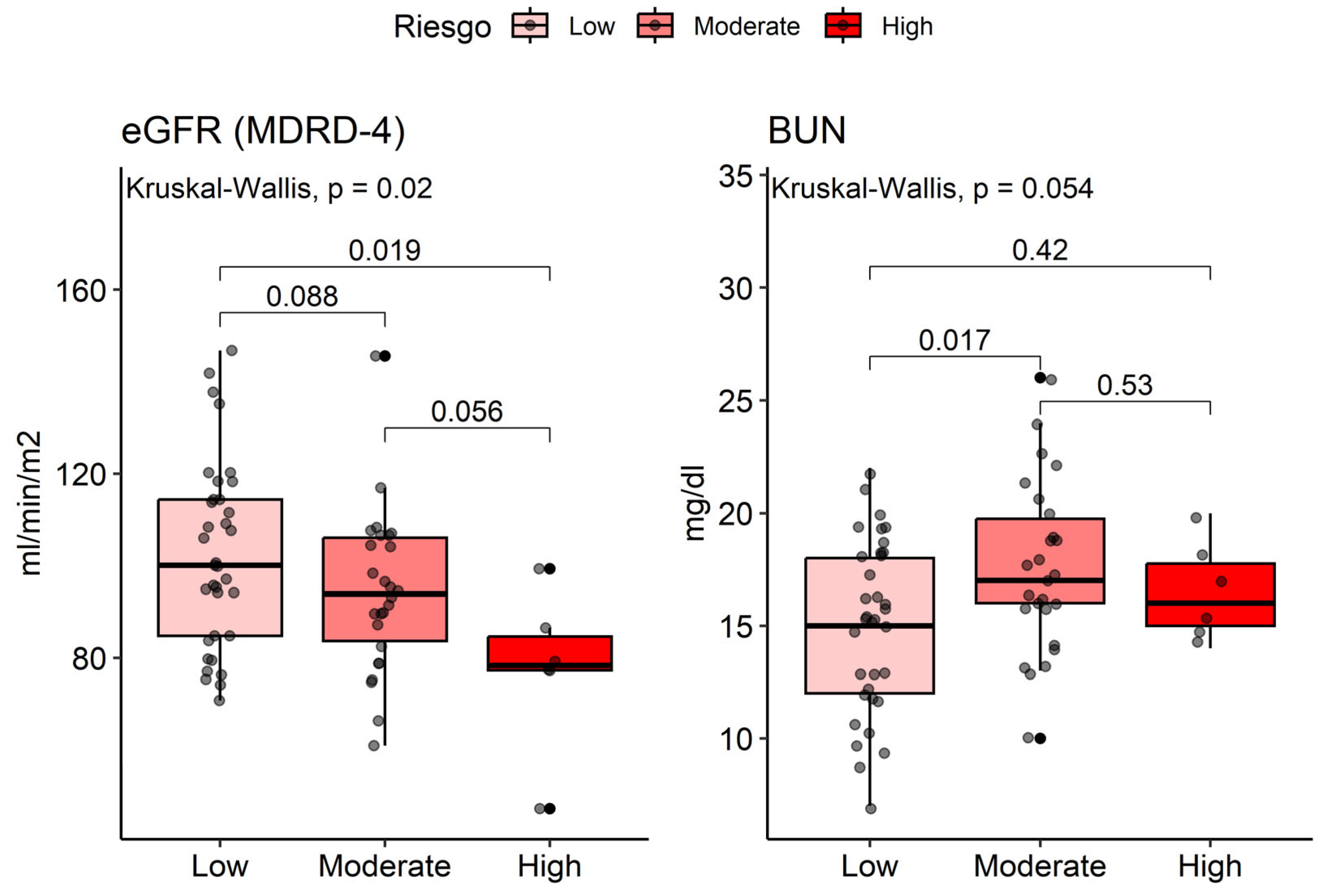
Figure 5.
Multiple Correspondence Analysis Between ASCVD Risk and Lifestyles
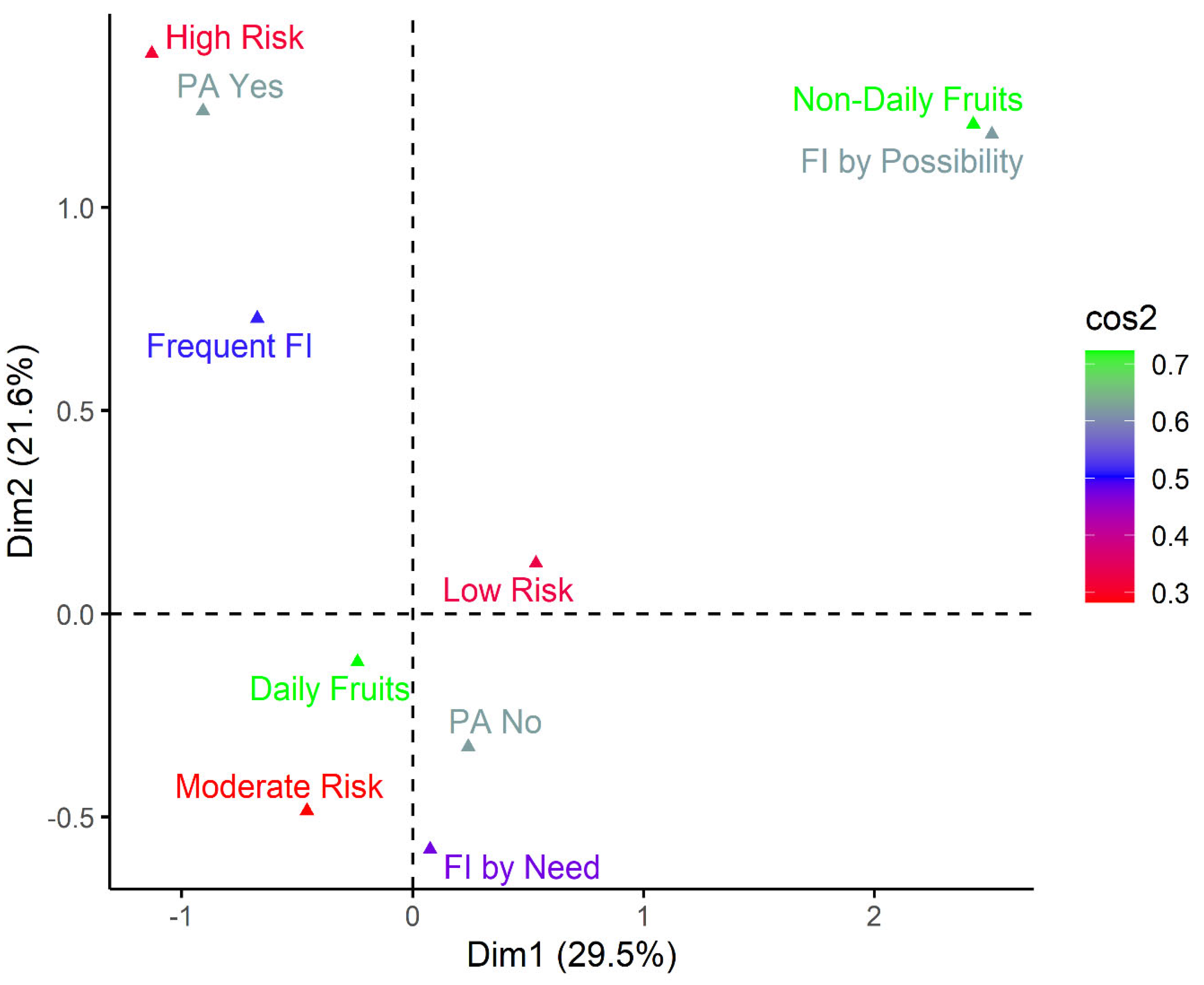
Figure 6.
Multiple Correspondence Analysis Between ASCVD Risk and Medical Care Opportunities
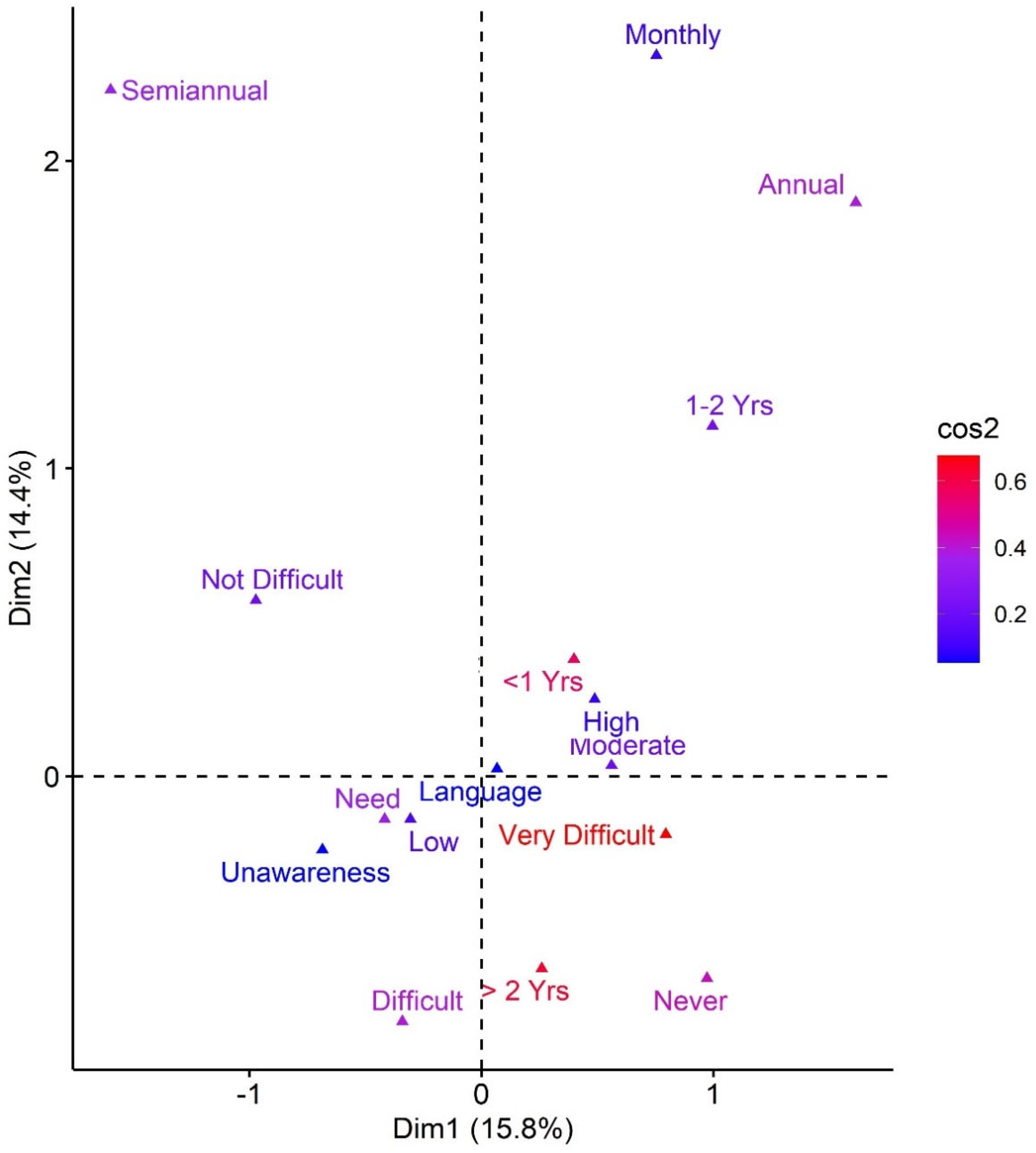
Table 2.
Anthropometric Parameters and Pathological Background in Chinese Immigrant Patients
| Characteristic | Female (n=36) ¹ |
Male (n=31) ¹ |
p-value |
|---|---|---|---|
| Anthropometric | |||
| BMI | 24.5 (19.1, 49.5) | 24.0 (12.6, 30.7) | 0.3 ² |
| BMI Status | 0.5 ³ | ||
| Normal | 18 (50%) | 19 (61%) | |
| Overweight | 15 (42%) | 9 (29%) | |
| Obesity | 3 (8.3%) | 3 (9.7%) | |
| SBP | 125 (90, 180) | 120 (90, 160) | 0.030 ² |
| DBP | 80 (60, 100) | 70 (60, 90) | 0.3 ² |
| Family History | |||
| Family HTN | 11 (33%) | 5 (17%) | 0.2 ³ |
| Family DM2 | 3 (9.7%) | 2 (6.9%) | >0.9 ³ |
| Comorbidities | |||
| Smoking | 0 (0%) | 16 (52%) | <0.001 ³ |
| Alcoholism | 1 (2.8%) | 11 (35%) | <0.001 ³ |
| HTN | 2 (5.6%) | 2 (6.5%) | >0.9 ³ |
| CAD | 0 (0%) | 1 (3.2%) | 0.5 ³ |
| AMI | 0 (0%) | 1 (3.2%) | 0.5 ³ |
| DM2 | 2 (5.6%) | 1 (3.2%) | >0.9 ³ |
| Dyslipidemia | 5 (14%) | 3 (9.7%) | 0.7 ³ |
| OSAHS | 1 (2.8%) | 0 (0%) | >0.9 ³ |
| COPD | 0 (0%) | 1 (3.2%) | 0.5 ³ |
| Lithiasis | 1 (2.8%) | 1 (3.2%) | >0.9 ³ |
| Neoplasia | 1 (2.8%) | 0 (0%) | >0.9 ³ |
| COVID-19 | 2 (5.6%) | 2 (6.5%) | >0.9 ³ |
| Surgical History | |||
| PCI | 0 (0%) | 1 (3.2%) | 0.5 ³ |
| Orthopedic Surgery | 2 (5.6%) | 1 (3.2%) | >0.9 ³ |
BMI: Body Mass Index; SBP: Systolic Blood Pressure; DBP: Diastolic Blood Pressure; HTN: Hypertension; CAD: Coronary Artery Disease; AMI: Acute Myocardial Infarction; DM2: Type 2 Diabetes Mellitus; COPD: Chronic Obstructive Pulmonary Disease; OSAHS: Obstructive Sleep Apnea Hypopnea Syndrome; PCI: Percutaneous Coronary Intervention; ¹Median (Range); n (%); ²Wilcoxon rank sum test; ³Fisher’s exact test.
Table 3.
Biochemical Profile in Chinese Immigrant Patients
| Profile | Parameter | Female (n=36) ¹ |
Male (n=31) ¹ |
p-value |
|---|---|---|---|---|
| Hemogram | Glucose | 90 (65, 333) | 91 (71, 337) | 0.2 ² |
| Hb (g/dl) | 13.1 (11, 15) | 15.4 (12.1, 18.2) | <0.001 ² | |
| WBC (×10³/µL) | 7,4 (4,7, 11,3) | 7,7 (4,9, 13) | 0.8 ² | |
| Platelets (×10³/µL) | 266 (160, 387) | 254 (135, 452) | 0.3 ² | |
| Lipid Profile | TC (mg/dL) | 223 (116, 328) | 208 (139, 325) | 0.4 ² |
| HDL-C (mg/dL) | 53 (28, 95) | 44 (29, 88) | 0.02 ² | |
| TG (mg/dL) | 133 (44, 491) | 127 (51, 805) | 0.6 ² | |
| LDL-C (mg/dL) | 142 (53, 237) | 134 (66, 216) | 0.5 ² | |
|
Renal unction |
Cr (mg/dL) | 0.7 (0.5, 1.2) | 0.9 (0.6, 1.3) | <0.001 ² |
| eGFR (mL/min/1.73m2) | 96 (47, 147) | 93 (61, 146) | 0.2 ² | |
| BUN (mg/dL) | 15.5 (7, 21) | 17 (10, 26) | 0.036 ² | |
| Urea (mg/dL) | 33 (15, 45) | 36 (21, 56) | 0.036 ² |
Hb: Hemoglobin; WBC: White Blood Cells; TC: Total Cholesterol; HDL-C: High-Density Lipoprotein Cholesterol; LDL-C: Low-Density Lipoprotein Cholesterol; TG: Triglycerides; Cr: Creatinine; eGFR: Estimated Glomerular Filtration Rate (MDRD-4); BUN: Blood Urea Nitrogen; ¹ Median (Range); ² Wilcoxon rank sum test
Table 4.
Cardiovascular Risk Profile by ASCVD ACC/AHA Formula and Renal Function in Chinese Patients
Table 4.
Cardiovascular Risk Profile by ASCVD ACC/AHA Formula and Renal Function in Chinese Patients
| Characteristic | ASCVD Risk | p-value | ||
|---|---|---|---|---|
| Low (n=35) ¹ |
Moderate (n=26) ¹ |
Alto (n=6) ¹ |
||
| Age | 48 (20, 67) | 61 (35, 73) | 76 (67, 78) | <0.001 ² |
| Gender | 0.040 ³ | |||
| Female | 24 (69%) | 10 (38%) | 2 (33%) | |
| Male | 11 (31%) | 16 (62%) | 4 (67%) | |
| Renal Function | ||||
| Cr (mg/dL) | 0.7 (0.5, 1.1) | 0.8 (0.6, 1.3) | 1.0 (0.7, 1.2) | 0.04 ² |
| eGFR (mL/min/1.73m2) | 100 (71, 147) | 94 (61, 146) | 78 (47, 99) | 0.02 ² |
| BUN (mg/dL) | 15 (7, 22) | 17 (10, 26) | 16 (14, 20) | 0.054 ² |
| Urea (mg/dL) | 32 (15, 47) | 36 (21, 56) | 34 (30, 43) | 0.06 ² |
| Urinalysis | ||||
| Proteinuria | 0 (0%) | 5 (14%) | 2 (7.7%) | 0.8 ³ |
| Hematuria | 0 (0%) | 10 (29%) | 8 (31%) | 0.4 ³ |
| ASCVD Score Risk (%) | 1 (1, 5) | 9 (5, 18) | 30 (20, 37) | <0.001 ² |
Cr: Creatinine, eGFR: Estimated Glomerular Filtration Rate (MDRD-4), BUN: Blood Urea Nitrogen. ASCVD: Atherosclerotic Cardiovascular Disease; ¹ Mean ± SD; n (%); ² Kruskal-Wallis rank sum test; ³ Fisher’s exact test
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



