
Submitted:
29 July 2024
Posted:
30 July 2024
You are already at the latest version
Abstract
Vascular impairment, muscle atrophy, and cognitive decline are important age-related conditions that have a significant impact on health. Vascular impairment directly disrupts the flow of blood, leading to the decline of muscle mass associated with aging (sarcopenia) and the decline of neuronal functions (neurodegeneration). Our inadequate understanding of the complex relationships between these conditions impedes precise diagnosis and effective treatment. This review analyzes the interrelated mechanisms that contribute to these conditions, with a specific focus on oxidative stress, chronic inflammation, and impaired nutrient delivery. The aim is to understand the common pathways involved and to suggest comprehensive therapeutic approaches. Vascular dysfunctions hinder the circulation of blood and the transportation of nutrients, resulting in sarcopenia characterized by muscle atrophy and weakness. Vascular dysfunction and sarcopenia have a negative impact on physical function and quality of life. Neurodegenerative diseases exhibit comparable pathophysiological mechanisms that affect cognitive and motor functions. Preventive and therapeutic approaches encompass lifestyle adjustments, addressing oxidative stress, inflammation, and integrated therapies that focus on improving vascular and muscular well-being. Better understanding of these links can enhance therapeutic strategies and lead to better outcomes for patients. Here, we highlight the intricate relationship among vascular dysfunction, degenerative muscle, and cognitive decline, underscoring the need for multidisciplinary approaches to treatment. Progress in this field can result in improved diagnosis, more potent therapeutic options, and enhanced preventative measures, all of which can contribute to an improved quality of life for the aging population.
Keywords:
vascular diseases
; vascular atrophy
; cognitive dysfunction
; neurodegenerative diseases
; oxidative stress
; inflammation
; aging
; insulin resistance
; nutrients
; comorbidity
1. Introduction
The growing prevalence of neurodegenerative diseases among the elderly highlights a major challenge in modern medicine. These disorders, which include Alzheimer's disease (AD), Parkinson's disease (PD), and other types of dementia, contribute significantly to cognitive and motor decline in aging populations [1,2,3]. The pathogenesis of these conditions is complex, involving a combination of genetic, environmental, and molecular factors that result in progressive neuron loss and dysfunction [4,5,6]. This neurodegenerative process is heavily influenced by age-related changes like oxidative stress, mitochondrial dysfunction, and chronic inflammation [7,8,9]. Vascular impairment, muscular atrophy, and cognitive dysfunction are intricately interconnected and form a triad [10,11,12]. Vascular diseases impair blood circulation, resulting in a lack of vital nutrients and oxygen to the brain and muscles. This can lead to serious conditions like sarcopenia and neurodegeneration. Sarcopenia, a condition marked by the decline of muscle mass and function, is worsened by inadequate vascular function, which hampers the flow of blood to the muscles and the delivery of essential nutrients. Neurodegenerative diseases such as AD and PD are both affected by vascular deficiencies, which contribute to oxidative stress, inflammation, and damage to neurons [13,14,15].
Vascular impairment refers to a condition in which blood vessels restrict or hinder the flow of blood to the upper and lower extremities. Within this particular framework, certain crucial anatomical regions, such as the brain and muscular tissues, experience a lack of oxygenated blood, resulting in potential harm or injury [16,17,18]. Cerebral small vessel disease (SVD) increases the risk of stroke, cognitive impairment, and dementia [19,20,21]. This occurs because the blood vessels in the brain experience small subcortical infarcts, lacunes, enlarged perivascular spaces, microbleeds, and atrophy [22,23,24]. These circumstances cause insufficient blood circulation in the brain, leading to inadequate perfusion. Hypertension, smoking, aging, and diabetes are factors that contribute to the occurrence of SVD [25,26,27,28].
Hypertension is a significant risk factor that contributes to cognitive decline [29,30,31]. This condition disrupts the structure and functional integrity of the blood vessels in the brain [32,33,34]. Furthermore, the depletion of calcium and impairment of contraction function, along with an augmentation in the extracellular matrix, induce significant alterations in the blood supply to specific regions of the body [35,36,37]. This exacerbates vascular reactivity, leading to dilation, tortuosity, and the formation of microaneurysms, while also diminishing the blood flow to the brain [38,39,40]. Cerebral vascular injury encompasses a range of conditions that impact the structure and function of blood vessels in the brain, thereby affecting cognitive function. Among these conditions, brain infarctions without apparent symptoms, white matter hyperintensities (WMHs), microinfarctions, and microsurgeries are highlighted [41,42,43]. Furthermore, it is essential to take into account the dysfunction of the blood-brain barrier, events with interstitial fluid drainage, alterations in cerebral blood flow, and damage to myelin [44,45,46]. Image markers such as WMHs, microsangrings, microinfarcts, cortical superficial siderosis, enlarged perivascular spaces, and large infarcts are commonly employed for the accurate diagnosis of cerebral vascular lesions [47,48,49,50] (Figure 1).
Sarcopenia is a pathological condition characterized by a significant decline in muscle strength (dynapenia), mass (quantity), and function (quality) [51,52,53]. This condition can result in a decrease in motor coordination, an increased risk of bone fractures, and difficulties in performing everyday activities. It can also lead to mortality [54,55,56,57,58]. Age-related vascular alterations, such as decreased muscle perfusion, hinder the delivery of nutrients and oxygen. Consequently, the presence of inefficient blood vessels caused by arterial stiffness and arteriolosclerosis can lead to a decrease in lean muscle mass, ultimately causing sarcopenia [17,59,60,61]. Chronic inflammatory processes, oxidative stress, insulin resistance, and impaired blood flow, all resulting from endothelial dysfunction and calcification of skeletal muscle vasculature, play a crucial role in the development of sarcopenic conditions [62,63,64]. Furthermore, as individuals age, their muscles and blood vessels become less responsive to insulin, resulting in decreased microvascular blood flow [65,66,67]. This reduction in blood flow leads to a decrease in the supply of amino acids, as insulin plays a crucial role in redirecting blood flow from non-nutritive capillaries to nutritive capillaries. Additionally, insulin activates endothelial nitric oxide in the arterioles of the pre-capillary muscle, which in turn increases the surface area of the capillary for the exchange of nutrients [61,68,69,70].
Muscle is intricately connected to nerve tissue through the process of innervation. In the sarcopenic condition, there is a particular event in which the loss of nerve supply primarily affects fast muscle fibers, which then regain nerve supply from slow-twitching motor neurons [51,71]. Consequently, the number of slow-twitch fibers increases, explaining the slow movements that are seen as people age [72,73]. When there is inadequate blood flow and therefore insufficient supply of nutrients to the muscles, along with the occurrence of neurological disorders, a reciprocal relationship is formed. This indicates that sarcopenia can worsen neurological conditions and vice versa [74,75]. As a result, the degenerative condition deteriorates, causing a decrease in nerve supply, reduced ability to regenerate, and impaired functioning of mitochondria, sarcoplasm, and calcium ions in muscle fibers [76,77,78,79]. Furthermore, sarcopenia can alter the microstructure of both the parietal grey matter and white matter, resulting in decreased brain volumes either overall or in specific regions [80,81,82]. Another contributing factor to sarcopenia is the presence of increased muscle fat infiltration (MFI). This indicates a lower quality of muscle and is linked to thinner cortical thickness in specific regions of the brain, as well as a decrease in the volume of gray matter in both the brain and cerebellum. Additionally, MFI is associated with reduced muscle strength, impaired function, and an increased risk of mortality in adults [83,84,85]. Sarcopenia encompasses not only muscular pathology but also encompasses neurological alterations [12,86]. Whether the changes in nerve supply, either due to normal bodily processes or disease, contribute to the worsening of muscle strength and physical performance in sarcopenia. The changes involve the instability of the neuromuscular junction or alterations in myofibrous calcium homeostasis. Furthermore, sarcopenia is associated with cerebral decline, and decreased physical performance, such as reduced handgrip strength, gait speed, and the chair stand test which is used to verify particularly the quadriceps muscles [87,88,89,90,91,92] [89–92].
Finally, it is crucial to consider the inseparable relationship between vascular diseases, sarcopenia, and neurodegeneration. Inadequate nutrient supply weakens arteries, leading to sarcopenia, a condition where essential alterations in the vascular body system can cause injuries in the muscular tissue. Arterial stiffness, the accumulation of fatty material and calcium in the arterial walls leading to the obstruction of blood flow, is a peripheral arterial disease that affects the blood supply to other tissues. It can also cause abdominal aortic aneurysm (AAA) and various other harmful changes in the blood vessels, which can disrupt the balance between the vascular, muscular, and cerebral environments [93]. Simultaneously, inadequate blood flow to the brain hinders the optimal growth of the nervous system, potentially resulting in neurodegenerative disorders such as AD [94,95,96,97,98].
The complex interplay of vascular disease, sarcopenia, and neurodegeneration, known as the inseparable triad, has received little attention, particularly in terms of understanding their common pathophysiological mechanisms. Vascular disorders hinder the flow of blood, leading to insufficient delivery of nutrients to both muscle and brain tissues. This exacerbates the symptoms of sarcopenia and neurodegenerative disorders such as AD and PD. While the specific impacts of these conditions are recognized, the exact biochemical and cellular processes that link them together are not completely comprehended. This review aims to fill the existing knowledge gap by investigating the role of arterial stiffness, oxidative stress, and chronic inflammation caused by vascular dysfunction in the development of muscle atrophy and cognitive decline. Additionally, it investigates the impact of sarcopenia on vascular and neurological health, exacerbating a detrimental cycle. The review seeks to clarify these mechanisms in order to emphasize the importance of integrated therapeutic strategies that focus on the triad. This approach aims to enhance the diagnosis, treatment, and prevention of age-related health issues, ultimately improving the quality of life and reducing illness and death rates among older individuals.
2. Vascular Diseases
The vascular network is an intricate arrangement comprising three distinct layers: intimate, medium, and adventitious. These layers possess various histological, biochemical, and functional attributes that are crucial for maintaining vascular balance and regulating the vascular response to stress or injury [99,100]. Additionally, they play a role in differentiating between different types of blood vessels [101]. Vascular diseases disrupt the structural integrity and functional capacity of blood vessels, leading to damage to the heart, brain, kidneys, muscles, and other organs [102,103]. The cells responsible for maintaining vascular homeostasis, which is the balance of blood vessels, are negatively affected by reactive oxygen species (ROS), chronic inflammation, alterations in blood flow, and metabolic factors such as elevated blood sugar levels, insulin, and certain types of lipids. On the other hand, compounds like polyphenols, amino acids, and omega-3 fatty acids can slow down the process of aging [104,105].
3.1. Pathophysiology and Causes of Vascular Diseases
Vascular diseases can be seen as the underlying cause of the development of ionic problems due to their promotion of a vasoconstrictor, pro-inflammatory, and pro-thrombotic environment, which leads to impaired regulation of the endothelium [106,107,108]. Thus, various anatomical regions may experience inadequate blood circulation, resulting in tissue damage and impaired growth. One possible explanation for this situation is endothelial senescence, which refers to the aging of the endothelial cells [109,110]. This aging process plays a significant role in the development of various health issues, including stroke, vascular dementia (VD), macular degeneration, obstructive sleep apnea, atherosclerosis, myocardial infarction, pulmonary hypertension, diabetes, renal failure, peripheral arterial disease, erectile dysfunction, and diabetic foot [111,112,113,114].
Cerebrovascular pathologies are strongly linked to neurological dysfunction [115,116]. Alterations in the blood-brain barrier (BBB) can contribute to or exacerbate the progression of neurodegenerative disorders [117,118]. Dysfunction in ion transport within the BBB is associated with acute brain damage and various neurological disorders, such as stroke, epilepsy, multiple sclerosis, VD, AD, and PD [119,120,121]. However, in order for this scenario to happen, certain conditions must be met. These conditions include the leakage of blood components such as fibrinogen, thrombin, albumin, and immunoglobulin G (IgG) from the cerebral capillaries, the accumulation of these components around the blood vessels, the degeneration of pericytes and endothelial cells, the breakdown of the BBB and tight junctions, and the leakage of red blood cells. All of these conditions are associated with vascular dysfunctions, which further confirms the connection between the vascular and nervous systems [122,123,124]
Coronary artery disease (CAD) is a form of vascular pathology. Atherosclerosis results in the constriction of arteries, which diminishes the circulation of blood to the brain and may as well result in transient ischemic attacks or strokes [125,126]. AAA is a vascular disease characterized by the [127,128], which can lead to a potentially fatal rupture. Although CAD and AAA are separate conditions, they both arise from the abnormal remodeling of the blood vessel walls [129,130]. The vascular middle layer undergoes a structural alteration, mainly consisting of vascular smooth muscle cells (VSMCs), which leads to the formation of lesions and diseased blood vessels. Key features comprise the absence of the intimal layer, persistent inflammation, and the degradation of elastic fibers [131,132,133].
Vascular calcification (VC) is a type of vascular disease characterized by the accumulation of calcium phosphate complexes in the walls of arteries [134]. While VC is commonly associated with the natural aging process, it has also been linked to the development of vascular diseases such as diabetes, atherosclerosis, and chronic kidney disease [135,136,137]. Nevertheless, the vascular system is intricately linked to all other systems within the body, thereby rendering the brain and muscles susceptible to potential harm arising from this vascular condition. The pathogenic process can be caused by pro-inflammatory cytokines such as interleukin (IL)-1β, IL-6, IL-8, tumor necrosis factor alpha, and transforming growth factor beta [138]. These cytokines stimulate the differentiation of VSMCs into bone-forming cells and the formation of calcifications [139]. In addition, IL-29 plays an important role in immunomodulation as other interferons, via activation of signaling pathways inducing the generation of inflammatory components. The atypical expression of IL-29 in VC-related disease hastened the process of VSMC osteogenic transformation and calcification in the presence of calcification medium (cap) by activating Janus kinase 2 (JAK2)/signal transducer and activation of transcription signaling 3 (STAT3) [140,141,142,143,144].
3.2. EffectsImpact on Blood Flow and Nutrient Delivery
Vascular dysfunction profoundly affects blood circulation and nutrient transportation through various intricate mechanisms. One key issue is the malfunction of the vascular endothelium, which impairs the synthesis of nitric oxide, an essential vasodilator responsible for regulating blood circulation and pressure. This dysfunction leads to increased vascular resistance and reduced tissue perfusion [145,146] . Chronic inflammation and oxidative stress exacerbate endothelial dysfunction, promoting the development of atherosclerosis [147,148]. Additionally, metabolic diseases like diabetes and obesity contribute to vascular impairment by inducing insulin resistance, which disrupts normal vascular function and nutrient transport [149,150]. Impaired cerebral autoregulation, often caused by metabolic and vascular disorders, reduces the brain's ability to maintain consistent blood flow, impacting cognitive function and increasing the risk of [151,152]. Sarcopenia results from decreased blood flow to the muscles, limiting oxygen and nutrient supply. These interdependent mechanisms highlight the importance of preserving vascular health to ensure adequate blood circulation and nutrient transportation, essential for preventing and managing conditions like sarcopenia and cognitive decline.
Vascular diseases also significantly impact blood flow and nutrient delivery, leading to a cascade of health problems. Atherosclerosis decreases blood flow and reduces the supply of oxygen and vital nutrients to tissues and organs. This can cause ischemia, where tissues experience a lack of blood supply, leading to pain and impaired function [153,154]. Reduced blood flow in the coronary arteries can result in angina or heart attacks, while in the peripheral arteries, it can cause peripheral artery disease (PAD), leading to pain and impaired mobility [155,156]. Hypertension, a prevalent vascular ailment, can gradually damage blood vessels, reducing their effectiveness in carrying blood and essential nutrients. This can affect the kidneys, leading to renal failure, or the brain, increasing the risk of strokes [157,158].
Moreover, diminished blood circulation caused by vascular disorders can impede wound healing and heighten susceptibility to infections, as tissues are deprived of sufficient nourishment and immune cells [159,160]. When the vascular system is compromised, the body's ability to transport white blood cells to areas of injury or infection is impaired, leading to prolonged healing times and increased vulnerability to infections. Additionally, the reduced supply of nutrients and oxygen hampers cellular repair and regeneration, exacerbating tissue damage and dysfunction [161,162]. The overall impact on the body's systems can be profound, affecting everything from physical mobility to cognitive function, underscoring the critical role of vascular health in maintaining overall well-being.
3.3. Consequences for Brain and Muscle Health
Vascular diseases have profound consequences for brain health, primarily through conditions such as stroke and VD [163,164]. When blood flow to the brain is restricted, as in the case of a stroke, brain cells are deprived of oxygen and essential nutrients, leading to cell death and potential loss of function. This can result in a range of neurological deficits, including paralysis, speech difficulties, and cognitive impairments, depending on the area of the brain affected. Chronic conditions like hypertension can also lead to small vessel disease in the brain, which is associated with cognitive decline and VD [19,165]. VD is the second most common form of dementia after AD and is characterized by problems with reasoning, planning, judgment, and memory [166,167]. These impacts not only affect the individual’s quality of life but also place a significant burden on caregivers and healthcare systems [168,169]. Furthermore, reduced cerebral blood flow can cause chronic conditions such as transient ischemic attacks (TIAs), which are temporary episodes of neurological dysfunction that increase the risk of major strokes [170,171].
The consequences of vascular diseases on muscle health are equally significant. Poor blood circulation due to conditions like PAD can lead to muscle pain, cramping, and weakness, particularly during physical activity [172,173]. This condition, known as claudication, results from inadequate oxygen delivery to the muscles, causing them to tire quickly and function less effectively [174]. Over time, the reduced blood flow can lead to muscle atrophy and loss of strength, further impairing mobility and overall physical health [175]. Additionally, the impaired delivery of nutrients and removal of metabolic waste products can exacerbate muscle fatigue and delay recovery from injuries. In severe cases, chronic insufficient blood flow can lead to critical limb ischemia, which may necessitate surgical intervention or even amputation. Poor vascular health can also result in chronic venous insufficiency, where blood pools in the veins, causing swelling, pain, and skin changes in the legs [176].
Moreover, diminished blood circulation caused by vascular disorders can impede the healing process of wounds and heighten the susceptibility to infections, as tissues are deprived of sufficient nourishment and immune cells [177,178]. When the vascular system is compromised, the body's ability to transport white blood cells to areas of injury or infection is impaired, leading to prolonged healing times and increased vulnerability to infections. Additionally, the reduced supply of nutrients and oxygen hampers cellular repair and regeneration, exacerbating tissue damage and dysfunction [179,180]. The overall impact on the body's systems can be profound, affecting everything from physical mobility to cognitive function, underscoring the critical role of vascular health in maintaining overall well-being. Vascular diseases can also contribute to the development of conditions like diabetic foot ulcers, which are difficult to heal and can lead to severe complications if not properly managed [181].
3.4. Current Treatments and Management Strategies
Presently, the management of vascular diseases involves a blend of modifications in lifestyle, pharmaceutical interventions, and surgical interventions. Implementing lifestyle changes, such as adhering to a diet that promotes heart health, regularly participating in physical activity, ceasing smoking, and effectively managing stress, are essential for preventing and controlling vascular diseases [182,183]. Pharmacological interventions encompass the administration of antihypertensive medications such as Lisinopril to regulate blood pressure, statins like Atorvastatin to reduce cholesterol levels, anticoagulants like Warfarin to prevent the formation of blood clots, and antiplatelet drugs like Aspirin to enhance blood circulation [184,185,186,187]. In more severe cases, surgical procedures such as angioplasty, stenting, and bypass surgery are employed to restore sufficient blood circulation [188,189,190]. Angioplasty involves using a balloon to open narrowed arteries, stenting involves placing a stent to keep arteries open, and bypass surgery creates a new pathway for blood to flow around blocked arteries. These treatments, often used in combination, help manage symptoms, improve quality of life, and reduce the risk of severe complications such as heart attack and stroke.
Herbal compounds have demonstrated promise as adjunctive therapies for vascular diseases [191,192,193,194]. For instance, Garlic (Allium sativum), rich in allicin, has been proven effective in lowering blood pressure and improving arterial elasticity [195]. Ginkgo biloba, for example, improves blood circulation and reduces oxidative stress thanks to its antioxidant properties [196]. In addition, Hawthorn (Crataegus species) is employed for the treatment of cardiovascular conditions by expanding blood vessels and enhancing blood circulation [197,198]. Terminalia arjuna is known for its cardioprotective properties, which help in the treatment of heart failure and ischemic conditions [199,200,201]. These herbal remedies provide a comprehensive approach, improving the effectiveness of traditional treatments while reducing adverse effects. Ongoing research and standardization are essential for the complete integration of these natural compounds into conventional medical practice, guaranteeing their safety and effectiveness.
4. Sarcopenia
Sarcopenia is a degenerative and widespread condition affecting the skeletal muscles. It is characterized by a gradual decrease in muscle mass and strength, resulting in diminished physical abilities, heightened vulnerability, increased likelihood of falling, and potentially fatal consequences [202,203,204]. This condition predominantly affects older adults and significantly impacts their quality of life and independence. Sarcopenia's pathophysiology encompasses various contributing factors. There is a rise in the apoptotic activity of myofibrils, which are the essential contractile units of muscle fibers, resulting in muscle degradation [205,206,207]. In addition, a decrease in the quantity of alpha-motor neurons, which play a crucial role in muscle contraction, also contributes to muscle weakness [208,209]. Reduced levels of anabolic hormones, such as testosterone and growth hormone, worsen muscle loss in the body due to hormonal imbalances [206,210,211]. In addition, increased concentrations of pro-inflammatory cytokines, which are molecules that transmit signals to promote inflammation, are essential in the advancement of sarcopenia [212,213,214]. The condition is primarily caused by vascular dysfunctions that hinder blood flow and nutrient delivery to muscles, resulting in energy deficiency. Understanding the various factors that contribute to sarcopenia is crucial for creating accurate diagnostic methods and effective treatment approaches to reduce its effects on the aging population [215,216].
4.1. Pathophysiology and Contributing Factors
Sarcopenia's pathophysiology encompasses a multitude of metabolic disorders. Metabolic syndrome (MetS), which is defined by the accumulation of fat in the abdominal area, high blood pressure, impaired ability to regulate blood sugar levels, and abnormal levels of lipids in the blood, plays a major role [217,218]. This syndrome induces a state of chronic inflammation characterized by continuous oxidative stress, release of inflammatory cytokines, malfunction of mitochondria, and resistance to insulin [219,220]. These factors hinder the survival of cells, resulting in the death of myocytes and the loss of muscle mass [217,221]. In addition, the malfunction of the renin-angiotensin-aldosterone system worsens sarcopenia by hindering the circulation of blood and the supply of nutrients to muscles [222,223]. Cellular senescence pathways, which involve the aging and deterioration of cells, also contribute to muscle degradation [224,225]. The reduction of growth hormone diminishes anabolic processes that are crucial for the maintenance of muscle [211,226]. High levels of myostatin, a growth factor that hinders muscle growth, also have a crucial function [227,228]. Ultimately, denervation, which refers to the deprivation of nerve supply to muscles, results in muscle atrophy and the subsequent decline in muscle function [229,230]. The combination of these factors results in a complicated interaction of metabolic disruptions and inflammatory reactions that contribute to the advancement of sarcopenia [231,232]. This emphasizes the necessity for diverse therapeutic strategies to reduce muscle loss and maintain physical function [233,234,235].
The cardiovascular system undergoes physiological changes as a result of vascular aging and prolonged exposure to risk factors, such as hypertension and hyperglycemia. These changes result in an elevation in arterial rigidity [236,237]. The arterial stiffening leads to inadequate blood supply in different parts of the body, worsening hypertension and establishing a vicious cycle of vascular decline and compromised blood circulation [238,239]. Arterial stiffness varies in different parts of the arterial tree. Central arteries, such as the aorta, may undergo distinct stiffening mechanisms compared to peripheral arteries, because of differences in their structure and function [240,241]. Consequently, this difference in rigidity can lead to different levels of damage in tissues, such as nervous and muscular tissues. Arterial stiffening hampers the transportation of oxygen and nutrients, leading to localized tissue underdevelopment or degeneration. These conditions are aggravated by chronic inflammation and oxidative stress, resulting in cellular damage and a decrease in functionality. The decrease in flexibility and functioning of blood vessels disturbs the overall balance of the body, emphasizing the significance of addressing vascular health in order to avoid systemic complications linked to aging [242,243].
Milk fat globule-EGF factor 8 protein (MFG-E8), also referred to as lactadine, is a protein found on the surface of epithelial cells that plays important roles in anti-inflammatory mechanisms and the regeneration of tissues [244]. Nevertheless, the negative consequences of this are associated with the process of arterial aging and the deterioration of neuromuscular junctions [245,246]. This protein is essential in the progression of sarcopenia, specifically due to its influence on vascular functions [247]. MFG-E8 functions as a signal provider that prompts the binding of dying cells to macrophages, serving as a crucial mediator of inflammation in a range of conditions such as cardiovascular diseases, arterial dysfunctions, sarcopenia, and the disruption of neuromuscular junctions [248,249]. As sarcopenia progresses, the expression of MFG-E8 increases, which hinders the process of mitophagy by reducing the levels of important components like Parkin, PTEN-induced kinase 1 (PINK1), and microtubule-associated proteins 1A/1B light chain 3B (LC3B)-II/I ratio. The suppression of mitophagy results in cellular harm and contributes to the deterioration and feebleness of muscles. In addition, the buildup of MFG-E8 in the walls of arteries and neuromuscular junctions worsens cardiovascular diseases and sarcopenia as people age. This emphasizes its double function in both repairing tissues and contributing to disease processes.
Furthermore, it is worth noting that specific medications can induce a decline in muscle mass and strength due to adverse drug reactions. Statins not only help prevent cardiovascular disease, but also cause a variety of skeletal muscle symptoms, ranging from muscle pain to statin-induced myopathy, with or without elevated levels. The mechanism of this condition is caused by mitochondrial dysfunction and reduced levels of coenzyme Q10, which is a result of chloride antagonism at the muscle membrane. Furthermore, they enhance the activation of programmed cell death and atrophin-1 through the attachment of a prenyl group to small guanosine triphosphate (GTP)ases belonging to the Rho family. This leads to a reduction in the size of muscle fibers, an increase in the breakdown of muscle proteins, and an upregulation of myostatin expression in the muscle. The risk of developing sarcopenia, a condition characterized by loss of skeletal muscle mass, is increased by the induction of hypoglycemia caused by diabetes control drugs. The closure of adenosine triphosphate (ATP)-sensitive potassium channels in muscle is an additional pathway that can lead to muscle atrophy through apoptosis and decrease muscle protein. Glucocorticoids ultimately hinder the function of fast contraction muscles (type II fibers), which have a high concentration of glucocorticoid receptors, as well as muscles that contain a combination of different fiber types. These substances hinder the growth of muscle proteins and promote their breakdown. Specifically, they prevent the absorption of amino acids needed for muscle protein synthesis in muscle fibers and hinder the activation of protein 1 binding of the eukaryotic translation initiation factor 4E and the ribosomal protein S6 kinase 1, which are responsible for stimulating muscle protein growth (Figure 2) [250,251,252,253].
4.2. Sarcopenic Obesity
Additionally, it is important to note the presence of sarcopenic obesity (SO) in the context of sarcopenia. SO is characterized by the simultaneous occurrence and worsening of sarcopenia as a result of increased adipose tissue [254,255]. This condition has recently been acknowledged by the European Society for Clinical Nutrition and Metabolism (ESPEN) and the European Association for the Study of Obesity (EASO) [256]. The clinical consequences of SO are considerably more severe than those observed in cases of sarcopenia or obesity occurring independently. This condition exhibits common underlying mechanisms with other diseases, including cancer, cardiovascular diseases, and kidney diseases [257,258,259]. These mechanisms include inflammation, oxidative stress, and insulin resistance, which are recognized as important factors in the development of this disease [260,261,262]. The screening for SO is conducted by assessing the concurrent presence of a high body mass index (BMI) or increased abdominal circumference, along with a change in body muscle composition [257,263,264].
Both obesity and sarcopenia are major contributors to the development of dementia [265,266]. Obesity increases the levels of pro-inflammatory cytokine IL-6 and negatively affects the ability of synapses to change and the formation of new neurons [267]. This ultimately leads to a decline in cognitive function. Increased levels of IL-6 interfere with the regular functioning of neurons and impede the formation of new neural connections, which are crucial for preserving cognitive functions [268]. In addition, myokines, such as irisin, which are released by muscles during physical activity, have a vital impact on neurological well-being [269,270]. Irisin governs the polarization of microglia, stimulates astrocytes, and adjusts insulin signaling and neuroinflammation in neurons, thus promoting brain health and cognitive functions [271,272,273]. Sarcopenic obesity worsens neurodegeneration and is associated with cardiovascular disease (CVD), cerebrovascular disease, diabetes, and depression [274,275,276]. This condition results in decreased physical activity, which further hampers muscle and cardiovascular health, all of which are crucial for sustaining cognitive function. Moreover, sarcopenic obesity diminishes the brain's neuroprotective framework, increasing the risk of neurodegenerative diseases. Hence, it is imperative to tackle both obesity and sarcopenia by implementing specific interventions, such as advocating for physical activity and controlling inflammation [277]. This is essential in order to reduce their collective influence on neurodegeneration and overall well-being, ultimately improving the quality of life for those affected [266,278,279,280].
4.4. Relationship between Vascular Disease and Sarcopenia
Sarcopenia is frequently linked to CVDs. Studies indicate that there is a higher occurrence of sarcopenia in individuals with CVDs, suggesting a direct relationship between the two conditions [281,282]. Vascular diseases exacerbate sarcopenia by obstructing blood flow and impeding the supply of nutrients to muscle tissues, resulting in muscle atrophy and weakness [283,284]. The inadequate perfusion of muscles deprives them of essential oxygen and nutrients, leading to muscle cell apoptosis and reduced regenerative capacity [285,286]. This is particularly evident in conditions such as PAD, where reduced blood flow to the limbs accelerates muscle degradation [283]. Moreover, the inflammatory mechanisms and oxidative stress linked to vascular disorders further worsen muscle breakdown [287]. Chronic inflammation, a common feature of vascular diseases, elevates levels of pro-inflammatory cytokines such as TNF-α and IL-6, which promote muscle catabolism [213]. Oxidative stress, caused by an imbalance between the production of ROS and the body's ability to detoxify these reactive intermediates, causes cellular damage and apoptosis in muscle cells [288,289]. Metabolic diseases like diabetes and obesity exacerbate these processes by causing insulin resistance [217,262,290]. Insulin resistance impairs muscle protein synthesis and increases protein degradation, further contributing to sarcopenia [291,292]. Thus, the interplay between vascular dysfunction, inflammation, oxidative stress, and metabolic disorders creates a vicious cycle that accelerates muscle deterioration.
Conversely, sarcopenia can accelerate the progression of CVDs by reducing levels of physical activity, which are crucial for preserving cardiovascular well-being [281,293]. Muscle weakness and fatigue associated with sarcopenia limit the ability to engage in regular physical exercise, leading to a sedentary lifestyle. This reduction in physical activity contributes to worsening cardiovascular risk factors, including obesity, hypertension, and dyslipidemia [294]. The connection between sarcopenia and vascular dysfunction is further affected by insulin resistance and chronic inflammation, resulting in the development of metabolic syndromes [217,295]. Insulin resistance not only affects glucose metabolism but also impacts lipid metabolism, leading to an increased risk of atherosclerosis and other cardiovascular conditions [296,297]. Therefore, it is essential to simultaneously address sarcopenia and vascular diseases through integrated therapeutic approaches that specifically focus on improving vascular health and muscle function [298]. This approach has the potential to improve overall well-being and decrease the mortality rate among elderly individuals. Early detection and comprehensive treatment strategies are crucial for managing both sarcopenia and vascular diseases [281,299]. Therapeutic interventions may include resistance training, nutritional supplementation, and pharmacological treatments aimed at reducing inflammation and oxidative stress [300,301,302]. Implementing lifestyle modifications, such as regular physical activity and a balanced diet, can also help mitigate the adverse effects of these conditions [303,304]. By addressing the interconnected pathways that contribute to both sarcopenia and vascular dysfunction, healthcare providers can enhance patient outcomes and quality of life, particularly in the aging population.
4.5. Impact on Physical Function and Quality of Life
Sarcopenia profoundly affects physical function and quality of life, particularly among the elderly [305,306]. As muscle mass diminishes, individuals experience a decrease in physical performance, which can manifest as reduced walking speed, impaired balance, and difficulty performing daily activities. This decline in physical capabilities increases the risk of falls and fractures, leading to a cycle of further inactivity and muscle deterioration. The reduction in muscle strength, a hallmark of sarcopenia, directly impacts the ability to carry out essential tasks such as climbing stairs, rising from a chair, or carrying groceries. Studies indicate that sarcopenia is significantly associated with lower physical performance, which in turn limits the ability to live independently and increases dependency on caregivers [307,308]. This loss of independence significantly impacts daily living, as older adults may struggle with personal care activities, household chores, and mobility, increasing their reliance on others and diminishing their sense of autonomy.
The decline in muscle health due to sarcopenia also has substantial implications for quality of life. Quality of life encompasses not just physical well-being, but also emotional, social, and psychological health. Sarcopenia-related impairments can lead to a sedentary lifestyle, contributing to obesity and metabolic disorders, which further degrade health status [309]. The inability to engage in social activities and hobbies due to physical limitations can result in social isolation, depression, and anxiety [310]. Additionally, the fear of falling or getting injured often prevents sarcopenic individuals from participating in physical exercise or outdoor activities, exacerbating their condition [311,312]. Research shows that health-related quality of life is significantly reduced in sarcopenic patients, with notable declines in physical functioning, vitality, and general health perception [305,313]. These psychological and social factors create a feedback loop that further diminishes the overall quality of life, as individuals may withdraw from social interactions and lose confidence in their physical abilities.
Furthermore, the economic and social burdens of sarcopenia are substantial [314,315]. Increased healthcare costs due to frequent hospitalizations, long-term care needs, and rehabilitation services place a significant financial strain on both individuals and healthcare systems. Families and caregivers also bear the emotional and physical stress of caring for sarcopenic individuals. The added responsibilities can lead to caregiver burnout, emotional distress, and reduced quality of life for the caregivers themselves. Comprehensive management strategies focusing on resistance training, nutritional interventions, and medical treatments are crucial in mitigating the impact of sarcopenia [316,317]. Early detection and targeted therapies can help maintain muscle mass and function, thereby improving physical performance and enhancing the quality of life for those affected [318]. Studies suggest that regular physical activity and strength training can help preserve muscle mass and strength, potentially delaying the onset of sarcopenia and its associated complications [319]. Ultimately, addressing sarcopenia holistically can lead to better health outcomes and reduce the societal and economic burdens associated with this condition, emphasizing the need for integrated care approaches that consider the physical, emotional, and social dimensions of health.
4.6. Strategies for Prevention and Treatment
Effective prevention and treatment strategies are crucial to mitigate the impact of sarcopenia. Among these strategies, exercise, nutrition, lifestyle modifications, and herbal compounds are paramount [320]. Exercise, particularly resistance training, plays a vital role in maintaining and enhancing muscle mass and strength. Resistance training, involving exercises that cause muscles to contract against an external resistance, is shown to be effective in combating sarcopenia [321]. This type of exercise stimulates muscle protein synthesis, improves neuromuscular function, and enhances muscle hypertrophy. Additionally, aerobic exercise complements resistance training by improving cardiovascular health and endurance, which can help maintain overall physical function [322,323].
Nutritional interventions are equally important in the prevention and management of sarcopenia [324,325]. Adequate protein intake is critical for muscle maintenance and repair. Older adults are often advised to consume higher levels of protein compared to younger individuals to counteract the anabolic resistance that occurs with aging [326]. Protein sources rich in essential amino acids, particularly leucine, are beneficial in promoting muscle protein synthesis. In addition to protein, other nutrients such as vitamin D, omega-3 fatty acids, and antioxidants play a role in muscle health. Vitamin D is crucial for muscle function, and its deficiency is linked to muscle weakness and falls [321,327]. Omega-3 fatty acids have anti-inflammatory properties that can help reduce muscle loss, while antioxidants combat oxidative stress, a factor contributing to muscle degeneration [328].
Lifestyle modifications, including maintaining a positive or neutral energy balance and reducing chronic inflammation, are essential for preventing sarcopenia [329]. Ensuring adequate caloric intake to meet energy demands without leading to obesity is crucial [330]. Obesity can exacerbate sarcopenia, creating a condition known as sarcopenic obesity, where excess fat mass further impairs physical function. Controlling inflammation through diet, physical activity, and possibly anti-inflammatory medications can help mitigate muscle breakdown. Maintaining intestinal diversity through a balanced diet that includes probiotics and prebiotics can also support overall health and muscle function [331,332].
Emerging therapeutic strategies offer additional avenues for managing sarcopenia. Research is exploring pharmaceutical interventions targeting the molecular pathways involved in muscle degradation and synthesis. For instance, myostatin inhibitors, which block a protein that inhibits muscle growth, are being investigated for their potential to enhance muscle mass and strength [227,333]. Hormone replacement therapies, particularly testosterone and growth hormone, are also under study for their anabolic effects on muscle tissue [334]. However, these treatments must be approached with caution due to potential side effects and the need for long-term safety data. Combining these pharmacological approaches with established exercise and nutritional strategies holds promise for a more comprehensive management of sarcopenia .
Additionally, herbal compounds have shown potential in the management of sarcopenia [335,336]. For example, Ginseng and Ashwagandha are known for their anti-inflammatory and muscle-strengthening properties [337,338]. Ginseng has been shown to improve muscle strength and physical performance, while Ashwagandha can enhance muscle mass and reduce muscle damage [339,340]. Curcumin, the active compound in turmeric, has strong anti-inflammatory and antioxidant properties, which can help reduce muscle degradation and improve muscle health [341]. These herbal supplements can be integrated into dietary regimens to support muscle function and mitigate the effects of sarcopenia.
In summary, the prevention and treatment of sarcopenia require a multifaceted approach that includes exercise, nutrition, lifestyle modifications, and emerging therapies, including herbal compounds. Resistance training and aerobic exercise are foundational in maintaining muscle mass and strength, while adequate protein intake and other nutrients support muscle health. Lifestyle changes to manage energy balance and inflammation are also critical. Emerging pharmaceutical treatments and herbal compounds may offer additional benefits, though they require careful consideration [342,343,344]. A holistic approach to managing sarcopenia can significantly improve the physical function and quality of life of older adults, ultimately reducing the societal and economic burdens associated with this condition.
5. Neurodegeneration
Neurodegeneration refers to pathological conditions that primarily impact neurons. It refers to a collection of neurological disorders that have distinct clinical and pathological features, and specifically impact certain subgroups of neurons in specific regions of the central nervous system (CNS). Notable examples comprise AD, PD, amyotrophic lateral sclerosis (ALS), frontotemporal dementia (FTLD), and Huntington's disease [345,346]. Furthermore, the vascular system plays a crucial role in numerous physiological processes within the human body. Problematic vascular mechanisms play a role in the development and advancement of diseases, confirming the inherent connection between vascular health and homeostasis [347,348]. Malfunctions in the vascular system can present as neurological disorders, for instance. Within this framework, it is feasible to ascertain that vascular health is intricately linked to neurodegenerative disorders. Reduced blood flow to the brain, commonly caused by conditions like high blood pressure and the buildup of fatty deposits in the arteries, can lead to a decline in cognitive function and the degeneration of nerve cells [349,350].
5.1. Pathophysiology and Risk Factors
PD is known by the loss or reduction of dopaminergic neurons in the substantia nigra (SN) and progressive and irreversible aggregation of α-Sinuclein poorly folded in multiple brain regions [351,352]. Wild protein (WT) or mutant α-Sinuclein (a-syn) accumulates in PD to form oligomers that disrupt central cell systems causing Neurodegeneration [353]. Notwithstanding, vascular parkinsonism (VP) is a Parkinsonian syndrome that can be caused by cerebrovascular disease, and this pathology represents 4% of all patients with Parkinsonism [354,355]. Patients with VP are usually older, with worse cognitive ability and pseudobulbar incontinence or paralysis. In the development of VP, vascular disorders induce disruption of the cortical connections of the basal ganglion, which may cause dysfunctions of the cortex-striate-pallid-thalamus-cortical [356] .
Regarding the relation between vascular disease and PD, both the severity and progression of cerebral SVD have been associated with incident parkinsonism [355,357]. When SVD is present in PD, it negatively affects the clinical symptoms of PD. This includes a worsening of gait, cognition, and mood and may well be associated with an additional acceleration of the already progressive course of PD [358]. Regarding the pathological mechanisms in the interaction between SVD and PD, one of the options is the structural lesions of SVD located in strategic brain regions, for example, the basal ganglia [359]. Hypoperfusion can also occur in small brain vessels [359]. The two mechanisms mentioned above cause generalized dysfunction of multiple brain pathways, including disruption of dopaminergic and nondopaminergic pathways involved in the pathophysiology of motor and non-motor symptoms in Parkinsonism. In addition, it is suspected that the permeability of the BBB is increased in SVD, and with its dysfunction astrocytes can be damaged by impairing the exchange of interstitial fluids and neuronal energy supply [360,361]. In addition, the maturation of oligodendrocyte precursor cells can also cause problems that hinder the formation and repair of myelin and energy support to axons [362]. Finally, cerebral hypoperfusion can also promote the aggregation of alpha-synuclein, leading to the pathology of PD with subsequent depletion of soluble alpha-synuclein [358,363,364].
AD is characterized by slowly progressive neurodegeneration and cognitive decline, and symptoms tend to appear many years later. Contributions to vascular cognitive impairment and decline have remarkable importance. In this scenario, cerebrovascular disease, occurs in almost all individuals with dementia, and vascular problems such as atherosclerosis, arteriolosclerosis, microinfarction, and amyloid angiopathy are prominent alongside markers of Neurodegeneration, that is, vascular pathology has become an important risk factor for AD dementia. In addition, cerebrovascular diseases contribute to neuronal loss in the pathology of AD and amyloid protein-β (Aβ) and tau related to AD [365,366].
Some nerve changes in AD include irregular activated microglia and astrocytes, elevated levels of inflammation and oxidative stress within the regions of the lesion, as well as compromised vascular functionality. Blood vessels work as transporter centers and perform various stages in the maintenance of physiological homeostasis, including helping to regulate immune responses. In this sense, vascular dysfunction, especially problems in cerebral microcirculation, can help in the pathophysiology of AD. For example, microangiopathy, rupture, and hemorrhage cause chronic hypoperfusion and reduction of cerebrospinal fluid (CSF), thus affecting normal blood circulation in the brain and neuronal function. In addition, they can assist in entering harmful substances, such as inflammatory factors in the nervous region, and impair the efflux of Aβ. Thus, the deposition of toxic proteins in the brain and subsequent neuronal damage occurs [367,368,369]. In addition, due to vascular dysfunction, individuals with AD have a higher susceptibility to hypoxia, leading to oxidative stress and resulting in various complications, including neuronal impairment and brain cell death. Therefore, the abnormal alterations in the blood vessels of AD disrupt the normal functioning of the brain and contribute to the progression of AD pathology (Figure 3) [370].
5.2. Link between Vascular Health and Neurodegeneration
Vascular health plays a crucial role in maintaining cognitive function and preventing neurodegenerative diseases. Emerging evidence suggests that cerebrovascular dysfunction is not only a contributing factor to vascular cognitive impairment but also has significant implications for primary neurodegenerative conditions such as AD, PD, and VD. Elevated blood pressure, a common vascular risk factor, has been consistently linked to age-related cognitive decline and the progression of neurodegenerative pathology underlying conditions like AD. Cerebrovascular disease can lead to cognitive impairment through multiple pathways. Chronic hypertension, for example, can cause damage to the blood-brain barrier, increase oxidative stress, and induce inflammation, all of which contribute to neuronal injury and cognitive decline. This vascular damage often precedes and accompanies the amyloid-beta plaques and tau tangles that are hallmarks of AD. Moreover, the compromised blood flow associated with vascular health issues can exacerbate neurodegeneration by depriving neurons of essential nutrients and oxygen, thereby accelerating the progression of cognitive deficits.
PD is another neurodegenerative disorder closely linked to vascular health. Vascular factors, including hypertension and diabetes, are known to exacerbate PD progression by promoting neuroinflammation and oxidative stress. These factors can further compromise the integrity of the blood-brain barrier, allowing neurotoxic substances to infiltrate the brain and accelerate neuronal damage. Consequently, improving vascular health through lifestyle modifications and medical management can have a protective effect against PD progression.
The interplay between vascular health and neurodegeneration is further illustrated by the overlapping risk factors and mechanisms underlying both conditions. Shared risk factors such as hypertension, diabetes, obesity, and smoking contribute to both vascular damage and neurodegenerative processes. Inflammation and oxidative stress, common in vascular diseases, also play significant roles in neurodegeneration. These shared pathways suggest that improving vascular health could potentially mitigate the risk of developing neurodegenerative diseases. For instance, managing blood pressure and blood sugar levels, adopting a healthy diet, and engaging in regular physical activity are strategies that can benefit both vascular and cognitive health. In addition to these risk factors, the relationship between cardiovascular risk trajectories and cognitive outcomes highlights the importance of early and sustained management of vascular health. Longitudinal studies have shown that individuals with a history of cardiovascular risk factors, such as elevated blood pressure and cholesterol levels, are more likely to experience cognitive decline and develop dementia. These findings underscore the need for proactive cardiovascular care as a means of preserving cognitive function and preventing neurodegenerative diseases. Interventions aimed at improving vascular health could delay or even prevent the onset of conditions like VD and AD, offering a dual benefit of enhancing both cardiovascular and brain health.
In summary, the link between vascular health and neurodegeneration is well-established, with vascular dysfunction contributing to the development and progression of cognitive impairment and neurodegenerative diseases. By addressing shared risk factors and implementing strategies to improve vascular health, it is possible to reduce the burden of neurodegenerative diseases and enhance overall brain health. This integrative approach highlights the importance of a holistic view in managing health, considering the interconnectedness of the body's vascular and nervous systems. Strategies such as regular exercise, a balanced diet rich in antioxidants, and effective management of cardiovascular risk factors can significantly improve vascular and cognitive health, ultimately reducing the societal and economic burdens associated with neurodegenerative diseases
5.3. Impact on Cognitive and Motor Functions
Neurodegenerative diseases have a profound impact on both cognitive and motor functions, leading to a wide range of disabilities that significantly affect the quality of life. These diseases, including AD, PD, ALS, and FTLD, result from the progressive loss of neurons in specific regions of the brain and nervous system. This neuronal loss disrupts essential neural pathways and processes, causing cognitive decline and motor impairments that often overlap and exacerbate each other. Cognitive impairments in neurodegenerative diseases are characterized by deficits in memory, executive function, language, and visuospatial skills [371,372].
In AD, the most common neurodegenerative disorder, cognitive decline begins with subtle memory lapses and progresses to severe impairments in thinking, reasoning, and the ability to perform daily activities. The accumulation of amyloid-beta plaques and tau tangles disrupts neural communication and leads to the death of neurons, particularly in the hippocampus and cortex, areas critical for memory and cognition. In PD, cognitive decline can manifest as difficulties with executive functions, such as planning and multitasking, alongside the hallmark motor symptoms of tremors, rigidity, and bradykinesia. Motor function impairments are another significant aspect of neurodegenerative diseases. In PD, the loss of dopaminergic neurons in the substantia nigra leads to motor symptoms such as tremors, muscle rigidity, bradykinesia (slowness of movement), and postural instability. These motor deficits severely limit mobility and increase the risk of falls and fractures. In ALS, the degeneration of motor neurons in the brain and spinal cord causes muscle weakness, atrophy, and eventually paralysis, affecting voluntary movements and respiratory function. FTLD and Huntington's disease also involve motor dysfunctions, although these are often overshadowed by the prominent cognitive and behavioral symptoms.
The interaction between cognitive and motor impairments in neurodegenerative diseases is complex and multifaceted. Cognitive-motor interference, where cognitive tasks negatively impact motor performance and vice versa, is a common challenge for patients. This dual-task interference can exacerbate functional limitations and increase the risk of accidents. For instance, individuals with PD may experience "freezing" episodes, where they temporarily lose the ability to move despite the intention to do so, often triggered by cognitive stressors or environmental changes. Similarly, gait disturbances in AD patients are linked to declines in cognitive function, particularly in attention and executive processing.
The co-occurrence of cognitive and motor symptoms in neurodegenerative diseases underscores the need for comprehensive management approaches that address both domains. Interventions such as cognitive rehabilitation, physical therapy, and pharmacological treatments aim to slow the progression of symptoms and improve quality of life. For example, cognitive training exercises can enhance executive function and memory, while resistance training and aerobic exercise can improve motor function and overall physical health. Pharmacological treatments, including cholinesterase inhibitors for AD and dopamine agonists for PD, provide symptomatic relief but do not halt disease progression. Emerging research into neuroprotective strategies and disease-modifying therapies offers hope for more effective treatments in the future.
5.4. Current Therapeutic Approaches
Pharmacological treatments remain a cornerstone of managing neurodegenerative diseases. In AD, cholinesterase inhibitors (e.g., donepezil and rivastigmine) and NMDA receptor antagonists (e.g., memantine) are used to alleviate cognitive symptoms by enhancing cholinergic function and modulating glutamatergic transmission. For PD, dopamine replacement therapy, primarily through levodopa combined with carbidopa, remains the gold standard, aiming to replenish dopamine levels in the brain. Additional medications, such as MAO-B inhibitors (e.g., selegiline) and dopamine agonists (e.g., pramipexole), help manage motor symptoms. ALS treatment often includes riluzole and edaravone, which are thought to reduce neuronal damage and oxidative stress, albeit with limited efficacy. Furthermore, extensive research is being conducted on novel target and drug discoveries for neurological diseases [373,374,375].
Lifestyle modifications and supportive therapies also play critical roles in the management of neurodegenerative conditions. Physical therapy and exercise are particularly beneficial in maintaining motor function and mobility in PD and ALS patients. Occupational therapy helps individuals adapt to their environment and maintain independence in daily activities. Cognitive therapies and mental exercises can aid in slowing cognitive decline in AD patients. Speech therapy is essential for addressing communication difficulties in various neurodegenerative diseases, improving the quality of life and social interaction for patients.
Emerging therapeutic approaches are exploring the potential of herbal compounds in managing neurodegenerative diseases [376]. Herbal compounds, derived from medicinal plants, offer a rich source of bioactive molecules with neuroprotective properties [377,378,379,380,381]. Curcumin, a compound found in turmeric, has garnered attention for its anti-inflammatory and antioxidant properties, which are beneficial in combating neuroinflammation and oxidative stress in AD [219,382,383]. Studies have shown that curcumin can inhibit the aggregation of amyloid-beta plaques and tau tangles, key pathological features of AD, thereby potentially slowing disease progression. Another promising herbal compound is resveratrol, found in grapes and red wine. Resveratrol is known for its ability to activate sirtuin-1 (SIRT1), a protein that promotes cellular health and longevity. In the context of neurodegeneration, resveratrol’s neuroprotective effects are linked to its capacity to reduce oxidative damage, enhance mitochondrial function, and modulate neuroinflammation [384,385,386]. Preclinical studies suggest that resveratrol can improve cognitive function and delay the progression of neurodegenerative diseases. Ginkgo biloba, an herbal extract used traditionally in Chinese medicine, is another example of a natural compound with potential neuroprotective benefits [196,387]. Ginkgo biloba extracts are rich in flavonoids and terpenoids, which have antioxidant properties. Clinical trials have indicated that Ginkgo biloba can improve cognitive function and reduce symptoms in AD patients, possibly by enhancing cerebral blood flow and reducing oxidative stress.
In summary, the current therapeutic approaches to neurodegeneration involve a combination of pharmacological treatments, lifestyle modifications, and supportive therapies. The integration of herbal compounds into these strategies offers additional benefits, leveraging their natural bioactive properties to provide neuroprotection. Curcumin, resveratrol, and Ginkgo biloba are concrete examples of herbal compounds that show promise in managing neurodegenerative diseases. Continued research and clinical trials are essential to further understand their mechanisms and optimize their use in comprehensive treatment regimens, potentially improving outcomes for patients with neurodegenerative conditions.
6. Discussion
Vascular disease, sarcopenia, and neurodegeneration are intricately linked, forming a triad of interrelated conditions that significantly impact overall health. Vascular diseases impair blood circulation, reducing the delivery of essential nutrients and oxygen to tissues such as muscles and the brain. This nutrient deficiency leads to sarcopenia, characterized by the progressive loss of muscle mass and function, resulting in frailty, falls, and decreased physical performance. The impaired blood flow also affects the brain, contributing to neurodegenerative diseases such as AD and PD. Oxidative stress, chronic inflammation, and insulin resistance are common pathophysiological mechanisms underlying these conditions. For instance, oxidative stress and inflammation caused by vascular dysfunction can damage neurons, leading to cognitive decline and motor impairments [388]. Similarly, reduced muscle perfusion exacerbates sarcopenia, while neurodegenerative processes can further impair muscular function through disrupted neural innervation. Therefore, addressing these interconnected conditions through integrated therapeutic strategies is crucial for improving the diagnosis, treatment, and prevention of age-related health issues, ultimately enhancing the quality of life for affected individuals.
Vascular disease contributes to sarcopenia and neurodegeneration through multiple interconnected mechanisms. Vascular diseases impair blood flow, reducing the delivery of oxygen and essential nutrients to muscles and the brain. This leads to muscle atrophy, a hallmark of sarcopenia, as muscles require a consistent supply of nutrients to maintain mass and function. Vascular dysfunctions, such as atherosclerosis and arterial stiffness, promote chronic inflammation and oxidative stress, exacerbating muscle degradation and contributing to sarcopenia. In the brain, reduced blood flow and nutrient supply can lead to neuronal death and impaired synaptic function, key features of neurodegenerative diseases like AD and PD. Additionally, vascular diseases can disrupt the blood-brain barrier, allowing harmful substances to enter the brain and further damage neural tissues. Insulin resistance and MetSs associated with vascular diseases also impair muscle protein synthesis and increase muscle degradation, worsening sarcopenia. The interaction among vascular dysfunction, inflammation, oxidative stress, and metabolic disturbances emphasizes the intricate connection between vascular disease, sarcopenia, and neurodegeneration. This underscores the need for integrated therapeutic strategies to alleviate these conditions and enhance patient outcomes.
Sarcopenia and neurodegenerative processes are intricately linked, forming a detrimental cycle that exacerbates both conditions. Sarcopenia, characterized by the progressive loss of muscle mass and function, leads to physical frailty and increased fall risk, which can precipitate or worsen neurodegenerative conditions such as AD and PD. The muscle loss associated with sarcopenia reduces the production of myokines, which are crucial for maintaining neuroplasticity and cognitive function. This decrease in myokines can impair brain function and accelerate neurodegeneration. Conversely, neurodegenerative diseases contribute to sarcopenia by disrupting the neural pathways responsible for muscle innervation and function. For instance, PD, which affects motor neurons, directly impairs muscle control and contributes to muscle atrophy. AD, through mechanisms such as oxidative stress and chronic inflammation, can similarly lead to muscle deterioration. Both conditions share common pathological features such as mitochondrial dysfunction, increased oxidative stress, and chronic inflammation, creating a feedback loop that worsens both muscle and cognitive health. Addressing this bidirectional relationship is crucial for developing therapeutic strategies that target both sarcopenia and neurodegeneration simultaneously to improve outcomes for affected individuals
Significant correlations between vascular disease, sarcopenia, and neurodegeneration can be identified by examining common risk factors and physiological mechanisms. Common risk factors include the natural aging process, hypertension, diabetes, and chronic inflammation. These factors contribute to the dysfunction of the endothelium, which obstructs the circulation of blood and the transportation of nutrients to both muscles and the brain, exacerbating the conditions of sarcopenia and neurodegeneration. Vascular dysfunction leads to oxidative stress and chronic inflammation, which in turn cause cellular damage in muscles and neurons. Insulin resistance, a common feature of MetS, impedes the process of muscle protein synthesis and accelerates muscle wasting, thus contributing to sarcopenia. Simultaneously, the coexistence of impaired glucose metabolism and oxidative damage plays a role in the progression of neurodegeneration, leading to a decline in cognitive functions and motor skills. The interrelated physiological mechanisms emphasize the importance of a comprehensive approach in treating these conditions, with a specific focus on integrated therapeutic strategies that aim to improve vascular health, preserve muscle mass, and protect the nervous system. Acquiring a thorough comprehension of these interconnected mechanisms is crucial for developing effective interventions that improve quality of life and reduce the incidence of illness and mortality associated with these age-related conditions.
The interrelated nature of vascular disease, sarcopenia, and neurodegeneration has profound implications for their diagnosis, treatment, and prevention. From a diagnostic perspective, having a clear understanding of the shared pathophysiological mechanisms such as chronic inflammation, oxidative stress, and insulin resistance can improve the ability to detect and differentiate these conditions at an early stage. By employing biomarkers and advanced imaging techniques, one can obtain thorough understanding of the degree of vascular damage, muscle atrophy, and neurodegenerative alterations. An essential aspect of treatment is the implementation of an integrated approach that specifically focuses on the triad. This includes pharmacological interventions like anti-inflammatory and antioxidant therapies, alongside lifestyle modifications such as exercise and nutritional strategies to improve vascular health, muscle mass, and cognitive function. Preventive measures concentrate on reducing common risk factors such as hypertension, diabetes, and sedentary lifestyles through public health campaigns that encourage physical activity, healthy eating, and regular medical check-ups. By addressing these interconnected conditions holistically, it is possible to slow their progression, reduce morbidity, and improve the overall quality of life for affected individuals
Future research should prioritize several key areas in order to better understand the triad of vascular disease, sarcopenia, and neurodegeneration. Initially, conducting research on the molecular and cellular mechanisms that underlie these interconnected conditions will offer a more profound understanding of their shared pathophysiological pathways. Oxidative stress, chronic inflammation, and insulin resistance should all be investigated as potential links between these diseases. In addition, the advancement of sophisticated biomarkers and imaging techniques can improve the early detection of diseases and provide more accurate monitoring of their progression. Longitudinal studies are crucial for comprehending the temporal connections and causal associations between vascular dysfunction, muscle atrophy, and cognitive decline. Furthermore, examining the impact of lifestyle interventions, such as engaging in physical activity and making dietary modifications, on mitigating the intensity of these conditions can offer pragmatic, non-pharmaceutical strategies for both preventing and managing them. The integration of multidisciplinary approaches encompassing neurology, cardiology, and gerontology will play a pivotal role in the development of comprehensive treatment plans. Exploring the possibilities of new therapeutic agents, such as anti-inflammatory drugs and antioxidants, has the potential to create new opportunities for treatment. The translation of these findings into effective clinical practices that enhance patient outcomes and quality of life will heavily rely on collaborative endeavors among research institutions and clinical settings [389,390,391,392,393,394,395].
5. Conclusions
This review highlights the complex interrelationships among vascular disease, sarcopenia, and neurodegeneration. These conditions share similar underlying causes, such as oxidative stress, chronic inflammation, and impaired blood flow, which collectively lead to muscle atrophy and cognitive decline. Understanding this triad is essential as it emphasizes the significance of a comprehensive approach to managing these interrelated conditions. Healthcare providers can develop holistic diagnostic, therapeutic, and preventive strategies by identifying the common risk factors and pathways involved. To effectively address these complexities, it is crucial to use integrated approaches that combine pharmacological interventions, lifestyle modifications, and advanced diagnostic techniques. For instance, resistance training and aerobic exercise are foundational in maintaining muscle mass and strength, while adequate protein intake and other nutrients support muscle health. In addition to traditional treatments, herbal compounds have shown potential benefits in managing these conditions. Curcumin, for example, is known for its anti-inflammatory and antioxidant properties, which can help reduce muscle degradation and improve muscle health. Similarly, Ginkgo biloba has been used to improve cognitive function and blood circulation, demonstrating potential neuroprotective benefits. Ultimately, enhancing our understanding of the connections among vascular health, muscle function, and cognitive performance will lead to improved patient outcomes, heightened quality of life, and decreased morbidity and mortality rates in older populations.
Author Contributions
Conceptualization, E.P.L., M.T., and S.M.B.; methodology, C.B.L., V.C.S.C., M.V.M.C., B.F.R.F.; investigation, K.Q., C.R.P.D., E.L.G., A.C.A., E.B.J; data curation, V.M.C.S.C.; writing—original draft preparation, E.P.L., M.T., S.M.B. and L.F.L.; writing—review and editing, M.T., and S.M.B.; visualization, C.B.L., A.C.A., C.R.P.D., S.M.B., E.L.G. and L.F.L.; supervision, X.X., M.T., and S.M.B.; project administration, M.T., S.M.B..; funding acquisition, M.T., and S.M.B. All authors have read and agreed to the published version of the manuscript.”
Funding
This work was supported by the HUN-REN Hungarian Research Network to M. Tanaka.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The authors attribute to Smart Servier (https://smart.servier.com/, accessed on 26 January 2024) the scientific images that were used in this article under an attribution license of public copyrights (https://creativecommons.org/licenses/by/3.0/, accessed on 26 January 2024) and under disclaimer of warranties. All Smart Servier's images were not changed in the writing of this article.
Conflicts of Interest
The authors declare no conflicts of interest.
List of abbreviations: AAA, abdominal aortic aneurysm; Aβ, amyloid protein-β; 42; AD, Alzheimer's disease; ATP, adenosine triphosphate; BBB, blood-brain barrier; CAD; coronary artery disease; CVD; cardiovascular disease; GTP, guanosine triphosphate; IL, interleukin; MetS, metabolic syndrome; MFI, muscle fat infiltration; MFG-E8, milk fat globule-EGF factor 8 protein; PAD, peripheral artery disease; PD, Parkinson's disease; ROS, reactive oxygen species; SO, sarcopenic obesity; SVD, small vessel disease; VC, vascular calcification; VSMCs, vascular smooth muscle cells; WMHs, white matter hyperintensities;
References
- Erkkinen, M.G.; Kim, M.O.; Geschwind, M.D. Clinical Neurology and Epidemiology of the Major Neurodegenerative Diseases. Cold Spring Harb Perspect Biol 2018, 10. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, M.M.; Garbarino, V.R.; Pollet, E.; Palavicini, J.P.; Kellogg, D.L., Jr.; Kraig, E.; Orr, M.E. Biological aging processes underlying cognitive decline and neurodegenerative disease. J Clin Invest 2022, 132. [Google Scholar] [CrossRef] [PubMed]
- Ricci, C. Neurodegenerative Disease: From Molecular Basis to Therapy. Int J Mol Sci 2024, 25. [Google Scholar] [CrossRef]
- Dugger, B.N.; Dickson, D.W. Pathology of Neurodegenerative Diseases. Cold Spring Harb Perspect Biol 2017, 9. [Google Scholar] [CrossRef]
- Rey, F.; Ottolenghi, S.; Zuccotti, G.V.; Samaja, M.; Carelli, S. Mitochondrial dysfunctions in neurodegenerative diseases: role in disease pathogenesis, strategies for analysis and therapeutic prospects. Neural Regen Res 2022, 17, 754–758. [Google Scholar] [CrossRef] [PubMed]
- Wilson, D.M., 3rd; Cookson, M.R.; Van Den Bosch, L.; Zetterberg, H.; Holtzman, D.M.; Dewachter, I. Hallmarks of neurodegenerative diseases. Cell 2023, 186, 693–714. [Google Scholar] [CrossRef] [PubMed]
- Bhat, A.H.; Dar, K.B.; Anees, S.; Zargar, M.A.; Masood, A.; Sofi, M.A.; Ganie, S.A. Oxidative stress, mitochondrial dysfunction and neurodegenerative diseases; a mechanistic insight. Biomed Pharmacother 2015, 74, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, G.G. Concepts and classification of neurodegenerative diseases. Handb Clin Neurol 2017, 145, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Samudra, N.; Lane-Donovan, C.; VandeVrede, L.; Boxer, A.L. Tau pathology in neurodegenerative disease: disease mechanisms and therapeutic avenues. J Clin Invest 2023, 133. [Google Scholar] [CrossRef]
- Levit, A.; Hachinski, V.; Whitehead, S.N. Neurovascular unit dysregulation, white matter disease, and executive dysfunction: the shared triad of vascular cognitive impairment and Alzheimer disease. Geroscience 2020, 42, 445–465. [Google Scholar] [CrossRef]
- Hayes, G.; Pinto, J.; Sparks, S.N.; Wang, C.; Suri, S.; Bulte, D.P. Vascular smooth muscle cell dysfunction in neurodegeneration. Front Neurosci 2022, 16, 1010164. [Google Scholar] [CrossRef]
- Arosio, B.; Calvani, R.; Ferri, E.; Coelho-Junior, H.J.; Carandina, A.; Campanelli, F.; Ghiglieri, V.; Marzetti, E.; Picca, A. Sarcopenia and Cognitive Decline in Older Adults: Targeting the Muscle-Brain Axis. Nutrients 2023, 15. [Google Scholar] [CrossRef]
- Scarian, E.; Viola, C.; Dragoni, F.; Di Gerlando, R.; Rizzo, B.; Diamanti, L.; Gagliardi, S.; Bordoni, M.; Pansarasa, O. New Insights into Oxidative Stress and Inflammatory Response in Neurodegenerative Diseases. Int J Mol Sci 2024, 25. [Google Scholar] [CrossRef]
- Olufunmilayo, E.O.; Gerke-Duncan, M.B.; Holsinger, R.M.D. Oxidative Stress and Antioxidants in Neurodegenerative Disorders. Antioxidants (Basel) 2023, 12. [Google Scholar] [CrossRef]
- Houldsworth, A. Role of oxidative stress in neurodegenerative disorders: a review of reactive oxygen species and prevention by antioxidants. Brain Commun 2024, 6, fcad356. [Google Scholar] [CrossRef]
- McGinigle, K.L. Peripheral Vascular Disease. Prim Care 2024, 51, 83–93. [Google Scholar] [CrossRef]
- Burtscher, J.; Millet, G.P.; Fresa, M.; Lanzi, S.; Mazzolai, L.; Pellegrin, M. The link between impaired oxygen supply and cognitive decline in peripheral artery disease. Prog Cardiovasc Dis, 1016. [Google Scholar] [CrossRef]
- Sweeney, M.D.; Kisler, K.; Montagne, A.; Toga, A.W.; Zlokovic, B.V. The role of brain vasculature in neurodegenerative disorders. Nat Neurosci 2018, 21, 1318–1331. [Google Scholar] [CrossRef]
- Hainsworth, A.H.; Markus, H.S.; Schneider, J.A. Cerebral Small Vessel Disease, Hypertension, and Vascular Contributions to Cognitive Impairment and Dementia. Hypertension 2024, 81, 75–86. [Google Scholar] [CrossRef]
- Hamilton, O.K.L.; Backhouse, E.V.; Janssen, E.; Jochems, A.C.C.; Maher, C.; Ritakari, T.E.; Stevenson, A.J.; Xia, L.; Deary, I.J.; Wardlaw, J.M. Cognitive impairment in sporadic cerebral small vessel disease: A systematic review and meta-analysis. Alzheimers Dement 2021, 17, 665–685. [Google Scholar] [CrossRef]
- Pala, D.; Barbosa, P.O.; Silva, C.T.; de Souza, M.O.; Freitas, F.R.; Volp, A.C.P.; Maranhão, R.C.; Freitas, R.N. Açai (Euterpe oleracea Mart.) dietary intake affects plasma lipids, apolipoproteins, cholesteryl ester transfer to high-density lipoprotein and redox metabolism: A prospective study in women. Clinical nutrition (Edinburgh, Scotland) 2018, 37, 618–623. [Google Scholar] [CrossRef]
- Pasi, M.; Cordonnier, C. Clinical Relevance of Cerebral Small Vessel Diseases. Stroke 2020, 51, 47–53. [Google Scholar] [CrossRef]
- Mena Romo, L.; Gómez-Choco, M. Neuroimaging in small vessel disease. Hipertens Riesgo Vasc 2023, 40, 25–33. [Google Scholar] [CrossRef]
- Karvelas, N.; Oh, B.; Wang, E.; Cobigo, Y.; Tsuei, T.; Fitzsimons, S.; Younes, K.; Ehrenberg, A.; Geschwind, M.D.; Schwartz, D. , et al. Enlarged perivascular spaces are associated with white matter injury, cognition and inflammation in cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy. Brain Commun 2024, 6, fcae071. [Google Scholar] [CrossRef]
- Backhouse, E.V.; Boardman, J.P.; Wardlaw, J.M. Cerebral Small Vessel Disease: Early-Life Antecedents and Long-Term Implications for the Brain, Aging, Stroke, and Dementia. Hypertension 2024, 81, 54–74. [Google Scholar] [CrossRef]
- Hoiland, R.L.; Robba, C.; Menon, D.K.; Citerio, G.; Sandroni, C.; Sekhon, M.S. Clinical targeting of the cerebral oxygen cascade to improve brain oxygenation in patients with hypoxic–ischaemic brain injury after cardiac arrest. Intensive Care Medicine 2023, 49, 1062–1078. [Google Scholar] [CrossRef]
- Lin, Z.; Lim, C.; Jiang, D.; Soldan, A.; Pettigrew, C.; Oishi, K.; Zhu, Y.; Moghekar, A.; Liu, P.; Albert, M. Longitudinal changes in brain oxygen extraction fraction (OEF) in older adults: Relationship to markers of vascular and Alzheimer's pathology. Alzheimer's & Dementia 2023, 19, 569–577. [Google Scholar]
- Mikkelsen, A.C.D.; Thomsen, K.L.; Mookerjee, R.P.; Hadjihambi, A. The role of brain inflammation and abnormal brain oxygen homeostasis in the development of hepatic encephalopathy. Metabolic Brain Disease 2023, 38, 1707–1716. [Google Scholar] [CrossRef]
- Gąsecki, D.; Kwarciany, M.; Nyka, W.; Narkiewicz, K. Hypertension, brain damage and cognitive decline. Curr Hypertens Rep 2013, 15, 547–558. [Google Scholar] [CrossRef]
- Canavan, M.; O'Donnell, M.J. Hypertension and Cognitive Impairment: A Review of Mechanisms and Key Concepts. Front Neurol 2022, 13, 821135. [Google Scholar] [CrossRef]
- Pacholko, A.; Iadecola, C. Hypertension, Neurodegeneration, and Cognitive Decline. Hypertension 2024, 81, 991–1007. [Google Scholar] [CrossRef]
- Ungvari, Z.; Toth, P.; Tarantini, S.; Prodan, C.I.; Sorond, F.; Merkely, B.; Csiszar, A. Hypertension-induced cognitive impairment: from pathophysiology to public health. Nat Rev Nephrol 2021, 17, 639–654. [Google Scholar] [CrossRef]
- Meissner, A. Hypertension and the Brain: A Risk Factor for More Than Heart Disease. Cerebrovasc Dis 2016, 42, 255–262. [Google Scholar] [CrossRef]
- Baggeroer, C.E.; Cambronero, F.E.; Savan, N.A.; Jefferson, A.L.; Santisteban, M.M. Basic Mechanisms of Brain Injury and Cognitive Decline in Hypertension. Hypertension 2024, 81, 34–44. [Google Scholar] [CrossRef]
- Totoń-Żurańska, J.; Mikolajczyk, T.P.; Saju, B.; Guzik, T.J. Vascular remodelling in cardiovascular diseases: hypertension, oxidation, and inflammation. Clin Sci (Lond) 2024, 138, 817–850. [Google Scholar] [CrossRef]
- Cai, Z.; Gong, Z.; Li, Z.; Li, L.; Kong, W. Vascular Extracellular Matrix Remodeling and Hypertension. Antioxid Redox Signal 2021, 34, 765–783. [Google Scholar] [CrossRef]
- Prado, A.F.; Batista, R.I.M.; Tanus-Santos, J.E.; Gerlach, R.F. Matrix Metalloproteinases and Arterial Hypertension: Role of Oxidative Stress and Nitric Oxide in Vascular Functional and Structural Alterations. Biomolecules 2021, 11. [Google Scholar] [CrossRef]
- Romay, M.C.; Knutsen, R.H.; Ma, F.; Mompeón, A.; Hernandez, G.E.; Salvador, J.; Mirkov, S.; Batra, A.; Sullivan, D.P.; Procissi, D. , et al. Age-related loss of Notch3 underlies brain vascular contractility deficiencies, glymphatic dysfunction, and neurodegeneration in mice. J Clin Invest 2024, 134. [Google Scholar] [CrossRef]
- Pacholko, A.; Iadecola, C. Hypertension, Neurodegeneration, and Cognitive Decline. Hypertension, 2024. [Google Scholar] [CrossRef]
- Ciurică, S.; Lopez-Sublet, M.; Loeys, B.L.; Radhouani, I.; Natarajan, N.; Vikkula, M.; Maas, A.; Adlam, D.; Persu, A. Arterial Tortuosity. Hypertension 2019, 73, 951–960. [Google Scholar] [CrossRef]
- Wardlaw, J.M.; Valdés Hernández, M.C.; Muñoz-Maniega, S. What are white matter hyperintensities made of? Relevance to vascular cognitive impairment. J Am Heart Assoc 2015, 4, 001140. [Google Scholar] [CrossRef]
- Shih, A.Y.; Blinder, P.; Tsai, P.S.; Friedman, B.; Stanley, G.; Lyden, P.D.; Kleinfeld, D. The smallest stroke: occlusion of one penetrating vessel leads to infarction and a cognitive deficit. Nat Neurosci 2013, 16, 55–63. [Google Scholar] [CrossRef]
- Wolf, G.; Lotan, A.; Lifschytz, T.; Ben-Ari, H.; Kreisel Merzel, T.; Tatarskyy, P.; Valitzky, M.; Mernick, B.; Avidan, E.; Koroukhov, N. , et al. Differentially Severe Cognitive Effects of Compromised Cerebral Blood Flow in Aged Mice: Association with Myelin Degradation and Microglia Activation. Front Aging Neurosci 2017, 9, 191. [Google Scholar] [CrossRef]
- Nakada, T.; Kwee, I.L. Fluid Dynamics Inside the Brain Barrier: Current Concept of Interstitial Flow, Glymphatic Flow, and Cerebrospinal Fluid Circulation in the Brain. Neuroscientist 2019, 25, 155–166. [Google Scholar] [CrossRef]
- Rajeev, V.; Fann, D.Y.; Dinh, Q.N.; Kim, H.A.; De Silva, T.M.; Lai, M.K.P.; Chen, C.L.; Drummond, G.R.; Sobey, C.G.; Arumugam, T.V. Pathophysiology of blood brain barrier dysfunction during chronic cerebral hypoperfusion in vascular cognitive impairment. Theranostics 2022, 12, 1639–1658. [Google Scholar] [CrossRef]
- Mierzwa, A.J.; Marion, C.M.; Sullivan, G.M.; McDaniel, D.P.; Armstrong, R.C. Components of myelin damage and repair in the progression of white matter pathology after mild traumatic brain injury. J Neuropathol Exp Neurol 2015, 74, 218–232. [Google Scholar] [CrossRef]
- Pavuluri, K.; Huston, J., 3rd; Ehman, R.L.; Manduca, A.; Jack, C.R., Jr.; Senjem, M.L.; Vemuri, P.; Murphy, M.C. Associations between vascular health, brain stiffness and global cognitive function. Brain Commun 2024, 6, fcae073. [Google Scholar] [CrossRef]
- Vints, W.A.; Kušleikienė, S.; Sheoran, S.; Valatkevičienė, K.; Gleiznienė, R.; Himmelreich, U.; Pääsuke, M.; Česnaitienė, V.J.; Levin, O.; Verbunt, J. Body fat and components of sarcopenia relate to inflammation, brain volume, and neurometabolism in older adults. Neurobiology of aging 2023, 127, 1–11. [Google Scholar] [CrossRef]
- Arosio, B.; Calvani, R.; Ferri, E.; Coelho-Junior, H.J.; Carandina, A.; Campanelli, F.; Ghiglieri, V.; Marzetti, E.; Picca, A. Sarcopenia and Cognitive Decline in Older Adults: Targeting the Muscle–Brain Axis. Nutrients 2023, 15, 1853. [Google Scholar] [CrossRef]
- Gurholt, T.P.; Borda, M.G.; Parker, N.; Fominykh, V.; Kjelkenes, R.; Linge, J.; van der Meer, D.; Sønderby, I.E.; Duque, G.; Westlye, L.T. Linking sarcopenia, brain structure and cognitive performance: a large-scale UK Biobank study. Brain Communications 2024, 6, fcae083. [Google Scholar] [CrossRef]
- Larsson, L.; Degens, H.; Li, M.; Salviati, L.; Lee, Y.I.; Thompson, W.; Kirkland, J.L.; Sandri, M. Sarcopenia: Aging-Related Loss of Muscle Mass and Function. Physiol Rev 2019, 99, 427–511. [Google Scholar] [CrossRef]
- Kara, M.; Kaymak, B.; Frontera, W.; Ata, A.M.; Ricci, V.; Ekiz, T.; Chang, K.V.; Han, D.S.; Michail, X.; Quittan, M. , et al. Diagnosing sarcopenia: Functional perspectives and a new algorithm from the ISarcoPRM. J Rehabil Med 2021, 53, jrm00209. [Google Scholar] [CrossRef]
- Wu, J.; Ding, P.; Wu, H.; Yang, P.; Guo, H.; Tian, Y.; Meng, L.; Zhao, Q. Sarcopenia: Molecular regulatory network for loss of muscle mass and function. Front Nutr 2023, 10, 1037200. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A. Sarcopenia: revised European consensus on definition and diagnosis. Age and ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Cawthon, P.M.; Orwoll, E.S.; Peters, K.E.; Ensrud, K.E.; Cauley, J.A.; Kado, D.M.; Stefanick, M.L.; Shikany, J.M.; Strotmeyer, E.S.; Glynn, N.W. Strong relation between muscle mass determined by D3-creatine dilution, physical performance, and incidence of falls and mobility limitations in a prospective cohort of older men. The Journals of Gerontology: Series A 2019, 74, 844–852. [Google Scholar] [CrossRef] [PubMed]
- Yuan, S.; Larsson, S.C. Epidemiology of sarcopenia: Prevalence, risk factors, and consequences. Metabolism 2023, 155533. [Google Scholar] [CrossRef] [PubMed]
- Barazzoni, R.; Cederholm, T.; Zanetti, M.; Cappellari, G.G. Defining and diagnosing sarcopenia: is the glass now half full? Metabolism 2023, 155558. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Gonzalez, M.C.; Prado, C.M. Sarcopenia≠ low muscle mass. European Geriatric Medicine 2023, 14, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Donato, A.J.; Machin, D.R.; Lesniewski, L.A. Mechanisms of Dysfunction in the Aging Vasculature and Role in Age-Related Disease. Circ Res 2018, 123, 825–848. [Google Scholar] [CrossRef]
- Mengozzi, A.; Pugliese, N.R.; Chiriacò, M.; Masi, S.; Virdis, A.; Taddei, S. Microvascular Ageing Links Metabolic Disease to Age-Related Disorders: The Role of Oxidative Stress and Inflammation in Promoting Microvascular Dysfunction. J Cardiovasc Pharmacol 2021, 78, S78–s87. [Google Scholar] [CrossRef]
- Damluji, A.A.; Alfaraidhy, M.; AlHajri, N.; Rohant, N.N.; Kumar, M.; Al Malouf, C.; Bahrainy, S.; Ji Kwak, M.; Batchelor, W.B.; Forman, D.E. , et al. Sarcopenia and Cardiovascular Diseases. Circulation 2023, 147, 1534–1553. [Google Scholar] [CrossRef]
- Jeon, Y.K.; Shin, M.J.; Saini, S.K.; Custodero, C.; Aggarwal, M.; Anton, S.D.; Leeuwenburgh, C.; Mankowski, R.T. Vascular dysfunction as a potential culprit of sarcopenia. Exp Gerontol 2021, 145, 111220. [Google Scholar] [CrossRef]
- El Assar, M.; Álvarez-Bustos, A.; Sosa, P.; Angulo, J.; Rodríguez-Mañas, L. Effect of Physical Activity/Exercise on Oxidative Stress and Inflammation in Muscle and Vascular Aging. Int J Mol Sci 2022, 23. [Google Scholar] [CrossRef] [PubMed]
- Purnamasari, D.; Tetrasiwi, E.N.; Kartiko, G.J.; Astrella, C.; Husam, K.; Laksmi, P.W. Sarcopenia and Chronic Complications of Type 2 Diabetes Mellitus. Rev Diabet Stud 2022, 18, 157–165. [Google Scholar] [CrossRef]
- Banks, N.F.; Rogers, E.M.; Church, D.D.; Ferrando, A.A.; Jenkins, N.D.M. The contributory role of vascular health in age-related anabolic resistance. J Cachexia Sarcopenia Muscle 2022, 13, 114–127. [Google Scholar] [CrossRef] [PubMed]
- Gallinoro, E.; Paolisso, P.; Candreva, A.; Bermpeis, K.; Fabbricatore, D.; Esposito, G.; Bertolone, D.; Fernandez Peregrina, E.; Munhoz, D.; Mileva, N. , et al. Microvascular Dysfunction in Patients With Type II Diabetes Mellitus: Invasive Assessment of Absolute Coronary Blood Flow and Microvascular Resistance Reserve. Front Cardiovasc Med 2021, 8, 765071. [Google Scholar] [CrossRef] [PubMed]
- Jahn, L.A.; Hartline, L.; Liu, Z.; Barrett, E.J. Metformin improves skeletal muscle microvascular insulin resistance in metabolic syndrome. Am J Physiol Endocrinol Metab 2022, 322, E173–e180. [Google Scholar] [CrossRef]
- Ou, Q.; Pan, D. Sarcopenia and risk of cardio-cerebrovascular disease: A two-sample Mendelian randomization study. Biosci Trends 2023, 17, 413–414. [Google Scholar] [CrossRef]
- Fang, M.; Liu, C.; Liu, Y.; Tang, G.; Li, C.; Guo, L. Association between sarcopenia with incident cardio-cerebrovascular disease: A systematic review and meta-analysis. Biosci Trends 2023, 17, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Ding, L.; Hu, H.; He, H.; Xiong, Z.; Zhu, X. Associations of Body-Roundness Index and Sarcopenia with Cardiovascular Disease among Middle-Aged and Older Adults: Findings from CHARLS. J Nutr Health Aging 2023, 27, 953–959. [Google Scholar] [CrossRef]
- Hu, C.H.; Yang, C.C.; Tu, S.J.; Huang, I.J.; Ganbat, D.; Guo, L.Y. Characteristics of the Electrophysiological Properties of Neuromuscular Motor Units and Its Adaptive Strategy Response in Lower Extremity Muscles for Seniors with Pre-Sarcopenia: A Preliminary Study. Int J Environ Res Public Health 2021, 18. [Google Scholar] [CrossRef]
- Mosole, S.; Carraro, U.; Kern, H.; Loefler, S.; Zampieri, S. Use it or lose it: tonic activity of slow motoneurons promotes their survival and preferentially increases slow fiber-type groupings in muscles of old lifelong recreational sportsmen. European journal of translational myology 2016, 26. [Google Scholar] [CrossRef]
- Barberi, L.; Scicchitano, B.M.; Musaro, A. Molecular and cellular mechanisms of muscle aging and sarcopenia and effects of electrical stimulation in seniors. European journal of translational myology 2015, 25. [Google Scholar] [CrossRef] [PubMed]
- Sui, S.X.; Williams, L.J.; Holloway-Kew, K.L.; Hyde, N.K.; Pasco, J.A. Skeletal Muscle Health and Cognitive Function: A Narrative Review. Int J Mol Sci 2020, 22. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, T.; Ulfhake, B. Sarcopenia: What Is the Origin of This Aging-Induced Disorder? Front Genet 2021, 12, 688526. [Google Scholar] [CrossRef] [PubMed]
- Coletti, C.; Acosta, G.F.; Keslacy, S.; Coletti, D. Exercise-mediated reinnervation of skeletal muscle in elderly people: An update. Eur J Transl Myol 2022, 32. [Google Scholar] [CrossRef] [PubMed]
- Mosole, S.; Rossini, K.; Kern, H.; Löfler, S.; Fruhmann, H.; Vogelauer, M.; Burggraf, S.; Grim-Stieger, M.; Cvečka, J.; Hamar, D. Reinnervation of Vastus lateralis is increased significantly in seniors (70-years old) with a lifelong history of high-level exercise (2013, revisited here in 2022). European Journal of Translational Myology 2022, 32. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, D.J.; Piasecki, M.; Atherton, P. The age-related loss of skeletal muscle mass and function: Measurement and physiology of muscle fibre atrophy and muscle fibre loss in humans. Ageing research reviews 2018, 47, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Kern, H.; Hofer, C.; Loefler, S.; Zampieri, S.; Gargiulo, P.; Baba, A.; Marcante, A.; Piccione, F.; Pond, A.; Carraro, U. Atrophy, ultra-structural disorders, severe atrophy and degeneration of denervated human muscle in SCI and Aging. Implications for their recovery by Functional Electrical Stimulation, updated 2017. Neurological research 2017, 39, 660–666. [Google Scholar] [CrossRef] [PubMed]
- Vints, W.A.J.; Kušleikienė, S.; Sheoran, S.; Valatkevičienė, K.; Gleiznienė, R.; Himmelreich, U.; Pääsuke, M.; Česnaitienė, V.J.; Levin, O.; Verbunt, J. , et al. Body fat and components of sarcopenia relate to inflammation, brain volume, and neurometabolism in older adults. Neurobiol Aging 2023, 127, 1–11. [Google Scholar] [CrossRef]
- Gurholt, T.P.; Borda, M.G.; Parker, N.; Fominykh, V.; Kjelkenes, R.; Linge, J.; van der Meer, D.; Sønderby, I.E.; Duque, G.; Westlye, L.T. , et al. Linking sarcopenia, brain structure and cognitive performance: a large-scale UK Biobank study. Brain Commun 2024, 6, fcae083. [Google Scholar] [CrossRef]
- Taubert, M.; Roggenhofer, E.; Melie-Garcia, L.; Muller, S.; Lehmann, N.; Preisig, M.; Vollenweider, P.; Marques-Vidal, P.; Lutti, A.; Kherif, F. , et al. Converging patterns of aging-associated brain volume loss and tissue microstructure differences. Neurobiol Aging 2020, 88, 108–118. [Google Scholar] [CrossRef]
- Trost, W.; Hars, M.; Fernandez, N.; Herrmann, F.; Chevalley, T.; Ferrari, S.; Gold, G.; Rizzoli, R.; Vuilleumier, P.; Trombetti, A. Functional brain changes in sarcopenia: evidence for differential central neural mechanisms in dynapenic older women. Aging Clinical and Experimental Research 2023, 35, 1015–1025. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Wu, X.; Yan, Z.; Cui, Y.; Liu, Y.; Cui, S.; Wang, Y.; Liu, T. Unveiling the muscle-brain axis: A bidirectional mendelian randomization study investigating the causal relationship between sarcopenia-related traits and brain aging. Archives of Gerontology and Geriatrics 2024, 123, 105412. [Google Scholar] [CrossRef]
- Lu, C.-f.; Liu, W.-s.; Cang, X.-m.; Sun, X.; Wang, X.-q.; Wang, C.-h.; Xu, F. The bidirectional associations between sarcopenia-related traits and cognitive performance. Scientific Reports 2024, 14, 7591. [Google Scholar] [CrossRef] [PubMed]
- Carda, S.; Cisari, C.; Invernizzi, M. Sarcopenia or muscle modifications in neurologic diseases: a lexical or patophysiological difference? Eur J Phys Rehabil Med 2013, 49, 119–130. [Google Scholar] [PubMed]
- Ardeljan, A.D.; Hurezeanu, R. Sarcopenia. 2020.
- Beeri, M.S.; Leugrans, S.E.; Delbono, O.; Bennett, D.A.; Buchman, A.S. Sarcopenia is associated with incident Alzheimer's dementia, m ild cognitive impairment, and cognitive decline. Journal of the American Geriatrics Society 2021, 69, 1826–1835. [Google Scholar] [CrossRef]
- Ladang, A.; Kovacs, S.; Lengelé, L.; Locquet, M.; Beaudart, C.; Reginster, J.-Y.; Bruyère, O.; Cavalier, E. Neurofilament-light chains (NF-L), a biomarker of neuronal damage, is increased in patients with severe sarcopenia: results of the SarcoPhAge study. Aging Clinical and Experimental Research 2023, 35, 2029–2037. [Google Scholar] [CrossRef] [PubMed]
- Pratt, J.; Pessanha, L.; Narici, M.; Boreham, C.; De Vito, G. Handgrip strength asymmetry as a new biomarker for sarcopenia and individual sarcopenia signatures. Aging Clinical and Experimental Research 2023, 35, 2563–2571. [Google Scholar] [CrossRef] [PubMed]
- Gurholt, T.; Borda, M.G.; Parker, N.; Duque, G.; Westlye, L.T.; Aarsland, D.; Andreassen, O.A. 366. Connecting Sarcopenia, Brain Structure, and Cognitive Performance: Large-Scale Evidence From the UK Biobank. Biological Psychiatry 2023, 93, S241–S242. [Google Scholar] [CrossRef]
- Arnold, W.D.; Clark, B.C. Neuromuscular junction transmission failure in aging and sarcopenia: the nexus of the neurological and muscular systems. Ageing Research Reviews 2023, 101966. [Google Scholar] [CrossRef]
- Qian, Z.; Huang, Y.; Zhang, Y.; Yang, N.; Fang, Z.; Zhang, C.; Zhang, L. Metabolic clues to aging: exploring the role of circulating metabolites in frailty, sarcopenia and vascular aging related traits and diseases. Frontiers in Genetics 2024, 15, 1353908. [Google Scholar] [CrossRef]
- Li, Y.; Hong, M.; Shi, H. Premorbid sarcopenia and functional outcome after acute stroke: a meta-analysis. Asia Pac J Clin Nutr 2023, 32, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Kopylova, V.; Boronovskiy, S.; Nartsissov, Y. Approaches to vascular network, blood flow, and metabolite distribution modeling in brain tissue. Biophysical Reviews 2023, 15, 1335–1350. [Google Scholar] [CrossRef] [PubMed]
- Wälchli, T.; Bisschop, J.; Carmeliet, P.; Zadeh, G.; Monnier, P.P.; De Bock, K.; Radovanovic, I. Shaping the brain vasculature in development and disease in the single-cell era. Nature Reviews Neuroscience 2023, 24, 271–298. [Google Scholar] [CrossRef] [PubMed]
- Tayler, H.M.; MacLachlan, R.; Güzel, Ö.; Miners, J.S.; Love, S. Elevated late-life blood pressure may maintain brain oxygenation and slow amyloid-β accumulation at the expense of cerebral vascular damage. Brain Communications 2023, 5, fcad112. [Google Scholar] [CrossRef] [PubMed]
- Seto, M.; Dumitrescu, L.; Mahoney, E.R.; Sclafani, A.M.; De Jager, P.L.; Menon, V.; Koran, M.E.; Robinson, R.A.; Ruderfer, D.M.; Cox, N.J. Multi-omic characterization of brain changes in the vascular endothelial growth factor family during aging and Alzheimer's disease. Neurobiology of aging 2023, 126, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Humphrey, J.D.; Schwartz, M.A. Vascular Mechanobiology: Homeostasis, Adaptation, and Disease. Annu Rev Biomed Eng 2021, 23, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Tomiyama, H. Vascular function: a key player in hypertension. Hypertens Res 2023, 46, 2145–2158. [Google Scholar] [CrossRef]
- Trimm, E.; Red-Horse, K. Vascular endothelial cell development and diversity. Nat Rev Cardiol 2023, 20, 197–210. [Google Scholar] [CrossRef] [PubMed]
- Simionescu, M. Implications of early structural-functional changes in the endothelium for vascular disease. Arterioscler Thromb Vasc Biol 2007, 27, 266–274. [Google Scholar] [CrossRef]
- Xu, J.; Shi, G.P. Vascular wall extracellular matrix proteins and vascular diseases. Biochim Biophys Acta 2014, 1842, 2106–2119. [Google Scholar] [CrossRef]
- Fraile-Martinez, O.; De Leon-Oliva, D.; Boaru, D.L.; De Castro-Martinez, P.; Garcia-Montero, C.; Barrena-Blázquez, S.; García-García, J.; García-Honduvilla, N.; Alvarez-Mon, M.; Lopez-Gonzalez, L. Connecting epigenetics and inflammation in vascular senescence: state of the art, biomarkers and senotherapeutics. Frontiers in Genetics 2024, 15, 1345459. [Google Scholar] [CrossRef]
- Sutton, N.R.; Malhotra, R.; St. Hilaire, C.; Aikawa, E.; Blumenthal, R.S.; Gackenbach, G.; Goyal, P.; Johnson, A.; Nigwekar, S.U.; Shanahan, C.M. Molecular mechanisms of vascular health: insights from vascular aging and calcification. Arteriosclerosis, thrombosis, and vascular biology 2023, 43, 15–29. [Google Scholar] [CrossRef]
- Cheng, J.; Wen, J.; Wang, N.; Wang, C.; Xu, Q.; Yang, Y. Ion Channels and Vascular Diseases. Arterioscler Thromb Vasc Biol 2019, 39, e146–e156. [Google Scholar] [CrossRef]
- Sacchetti, S.; Puricelli, C.; Mennuni, M.; Zanotti, V.; Giacomini, L.; Giordano, M.; Dianzani, U.; Patti, G.; Rolla, R. Research into New Molecular Mechanisms in Thrombotic Diseases Paves the Way for Innovative Therapeutic Approaches. Int J Mol Sci 2024, 25. [Google Scholar] [CrossRef]
- Rajendran, P.; Rengarajan, T.; Thangavel, J.; Nishigaki, Y.; Sakthisekaran, D.; Sethi, G.; Nishigaki, I. The vascular endothelium and human diseases. Int J Biol Sci 2013, 9, 1057–1069. [Google Scholar] [CrossRef]
- Erusalimsky, J.D. Vascular endothelial senescence: from mechanisms to pathophysiology. J Appl Physiol (1985) 2009, 106, 326–332. [Google Scholar] [CrossRef]
- Bloom, S.I.; Islam, M.T.; Lesniewski, L.A.; Donato, A.J. Mechanisms and consequences of endothelial cell senescence. Nat Rev Cardiol 2023, 20, 38–51. [Google Scholar] [CrossRef]
- Direito, R.; Barbalho, S.M.; Sepodes, B.; Figueira, M.E. Plant-Derived Bioactive Compounds: Exploring Neuroprotective, Metabolic, and Hepatoprotective Effects for Health Promotion and Disease Prevention. Pharmaceutics 2024, 16. [Google Scholar] [CrossRef]
- Han, Y.; Kim, S.Y. Endothelial senescence in vascular diseases: Current understanding and future opportunities in senotherapeutics. Experimental & Molecular Medicine 2023, 55, 1–12. [Google Scholar]
- Rahman, M.S.; Islam, R.; Bhuiyan, M.I.H. Ion transporter cascade, reactive astrogliosis and cerebrovascular diseases. Frontiers in Pharmacology 2024, 15, 1374408. [Google Scholar] [CrossRef]
- Coste, B.; Delmas, P. PIEZO Ion Channels in Cardiovascular Functions and Diseases. Circulation Research 2024, 134, 572–591. [Google Scholar] [CrossRef] [PubMed]
- Kalaria, R.N. Cerebrovascular disease and mechanisms of cognitive impairment: evidence from clinicopathological studies in humans. Stroke 2012, 43, 2526–2534. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, B.; Rypma, B.; Gratton, G.; Fabiani, M. Age-related changes in cerebrovascular health and their effects on neural function and cognition: A comprehensive review. Psychophysiology 2021, 58, e13796. [Google Scholar] [CrossRef]
- Erickson, M.A.; Dohi, K.; Banks, W.A. Neuroinflammation: a common pathway in CNS diseases as mediated at the blood-brain barrier. Neuroimmunomodulation 2012, 19, 121–130. [Google Scholar] [CrossRef]
- Lacoste, B.; Prat, A.; Freitas-Andrade, M.; Gu, C. The Blood-Brain Barrier: Composition, Properties, and Roles in Brain Health. Cold Spring Harb Perspect Biol, 2024. [Google Scholar] [CrossRef]
- Archie, S.R.; Al Shoyaib, A.; Cucullo, L. Blood-Brain Barrier Dysfunction in CNS Disorders and Putative Therapeutic Targets: An Overview. Pharmaceutics 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Kumar, D.; Jha, S.K.; Jha, N.K.; Ambasta, R.K. Ion Channels in Neurological Disorders. Adv Protein Chem Struct Biol 2016, 103, 97–136. [Google Scholar] [CrossRef]
- Song, S.; Luo, L.; Sun, B.; Sun, D. Roles of glial ion transporters in brain diseases. Glia 2020, 68, 472–494. [Google Scholar] [CrossRef]
- Liu, R.; Collier, J.M.; Abdul-Rahman, N.-H.; Capuk, O.; Zhang, Z.; Begum, G. Dysregulation of Ion Channels and Transporters and Blood-Brain Barrier Dysfunction in Alzheimer's Disease and Vascular Dementia. Aging and Disease 2024. [Google Scholar]
- Korszun-Karbowniczak, J.; Krysiak, Z.J.; Saluk, J.; Niemcewicz, M.; Zdanowski, R. The Progress in Molecular Transport and Therapeutic Development in Human Blood–Brain Barrier Models in Neurological Disorders. Cellular and Molecular Neurobiology 2024, 44, 34. [Google Scholar] [CrossRef]
- Khor, S.L.Q.; Ng, K.Y.; Koh, R.Y.; Chye, S.M. Blood-brain Barrier and Neurovascular Unit Dysfunction in Parkinson's Disease: From Clinical Insights to Pathogenic Mechanisms and Novel Therapeutic Approaches. CNS & Neurological Disorders-Drug Targets (Formerly Current Drug Targets-CNS & Neurological Disorders) 2024, 23, 315–330. [Google Scholar]
- Mendelson, S.J.; Prabhakaran, S. Diagnosis and management of transient ischemic attack and acute ischemic stroke: a review. Jama 2021, 325, 1088–1098. [Google Scholar] [CrossRef] [PubMed]
- Shao, C.; Wang, J.; Tian, J.; Tang, Y.-d. Coronary artery disease: from mechanism to clinical practice. Coronary Artery Disease: Therapeutics and Drug Discovery, 2020; 1–36. [Google Scholar]
- Weintraub, N.L. Understanding abdominal aortic aneurysm. The New England journal of medicine 2009, 361, 1114. [Google Scholar] [CrossRef] [PubMed]
- Anagnostakos, J.; Lal, B.K. Abdominal aortic aneurysms. Progress in cardiovascular diseases 2021, 65, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Amalinei, C.; Căruntu, I.-D. Etiology and pathogenesis of aortic aneurysm. Aortic Aneurysm-Recent Advances2013, 2013. [Google Scholar]
- Tao, J.; Cao, X.; Yu, B.; Qu, A. Vascular stem/progenitor cells in vessel injury and repair. Frontiers in Cardiovascular Medicine 2022, 9, 845070. [Google Scholar] [CrossRef] [PubMed]
- Paloschi, V.; Pauli, J.; Winski, G.; Wu, Z.; Li, Z.; Botti, L.; Meucci, S.; Conti, P.; Rogowitz, F.; Glukha, N. Utilization of an Artery-on-a-Chip to Unravel Novel Regulators and Therapeutic Targets in Vascular Diseases. Advanced healthcare materials 2024, 13, 2302907. [Google Scholar] [CrossRef] [PubMed]
- Qadura, M.; Syed, M.H.; Anand, S.; Bosch, J.; Connolly, S.; Aboyans, V.; Muehlhofer, E.; Yusuf, S.; Eikelboom, J. The predictive value of interarm systolic blood pressure differences in patients with vascular disease: Sub-analysis of the COMPASS trial. Atherosclerosis 2023, 372, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Sillesen, H.H. Peripheral vascular disease. Textbook of diabetes 2024, 755–767. [Google Scholar]
- Villa-Bellosta, R. Vascular calcification: key roles of phosphate and pyrophosphate. International Journal of Molecular Sciences 2021, 22, 13536. [Google Scholar] [CrossRef] [PubMed]
- Bessueille, L.; Magne, D. Inflammation: a culprit for vascular calcification in atherosclerosis and diabetes. Cellular and Molecular Life Sciences 2015, 72, 2475–2489. [Google Scholar] [CrossRef]
- Pescatore, L.A.; Gamarra, L.F.; Liberman, M. Multifaceted mechanisms of vascular calcification in aging. Arteriosclerosis, thrombosis, and vascular biology 2019, 39, 1307–1316. [Google Scholar] [CrossRef]
- Ren, S.-C.; Mao, N.; Yi, S.; Ma, X.; Zou, J.-Q.; Tang, X.; Fan, J.-M. Vascular calcification in chronic kidney disease: an update and perspective. Aging and Disease 2022, 13, 673. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Dhalla, N.S. The role of pro-Inflammatory cytokines in the pathogenesis of cardiovascular disease. International Journal of Molecular Sciences 2024, 25, 1082. [Google Scholar] [CrossRef]
- Lee, H.-Y.; Lim, S.; Park, S. Role of inflammation in arterial calcification. Korean Circulation Journal 2021, 51, 114–125. [Google Scholar] [CrossRef]
- Hao, N.; Zhou, Z.; Zhang, F.; Li, Y.; Hu, R.; Zou, J.; Zheng, R.; Wang, L.; Xu, L.; Tan, W. Interleukin-29 Accelerates Vascular Calcification via JAK2/STAT3/BMP2 Signaling. Journal of the American Heart Association 2023, 12, e027222. [Google Scholar] [CrossRef]
- Russo, M.P.; Grande-Ratti, M.F.; Burgos, M.A.; Molaro, A.A.; Bonella, M.B. Prevalence of diabetes, epidemiological characteristics and vascular complications. Archivos de cardiología de México 2023, 93, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Drumond, D.B. Avaliação da prevalência de calcificações vasculares e estimativa de risco cardiovascular baseados nos escores de Adragão e Kaupilla em transplantados renais. Universidade de São Paulo.
- Kang, J.-H.; Kawano, T.; Murata, M.; Toita, R. Vascular calcification and cellular signaling pathways as potential therapeutic targets. Life Sciences 2023, 122309. [Google Scholar] [CrossRef]
- Izzo, C.; Secondulfo, C.; Bilancio, G.; Visco, V.; Virtuoso, N.; Migliarino, S.; Ciccarelli, M.; Di Pietro, P.; La Mura, L.; Damato, A. Chronic Kidney Disease with Mineral Bone Disorder and Vascular Calcification: An Overview. Life 2024, 14, 418. [Google Scholar] [CrossRef] [PubMed]
- Tousoulis, D.; Kampoli, A.-M.; Tentolouris Nikolaos Papageorgiou, C.; Stefanadis, C. The role of nitric oxide on endothelial function. Current vascular pharmacology 2012, 10, 4–18. [Google Scholar] [CrossRef] [PubMed]
- Suvorava, T.; Metry, S.; Pick, S.; Kojda, G. Alterations in endothelial nitric oxide synthase activity and their relevance to blood pressure. Biochemical pharmacology 2022, 205, 115256. [Google Scholar] [CrossRef]
- Castellon, X.; Bogdanova, V. Chronic inflammatory diseases and endothelial dysfunction. Aging and disease 2016, 7, 81. [Google Scholar] [CrossRef]
- Higashi, Y. Roles of oxidative stress and inflammation in vascular endothelial dysfunction-related disease. Antioxidants 2022, 11, 1958. [Google Scholar] [CrossRef]
- Schulman, I.H.; Zhou, M.-S. Vascular insulin resistance: a potential link between cardiovascular and metabolic diseases. Current hypertension reports 2009, 11, 48–55. [Google Scholar] [CrossRef]
- Wu, H.; Ballantyne, C.M. Metabolic inflammation and insulin resistance in obesity. Circulation research 2020, 126, 1549–1564. [Google Scholar] [CrossRef] [PubMed]
- Claassen, J.A.; Thijssen, D.H.; Panerai, R.B.; Faraci, F.M. Regulation of cerebral blood flow in humans: physiology and clinical implications of autoregulation. Physiological reviews 2021, 101, 1487–1559. [Google Scholar] [CrossRef]
- Wang, S.; Tang, C.; Liu, Y.; Border, J.J.; Roman, R.J.; Fan, F. Impact of impaired cerebral blood flow autoregulation on cognitive impairment. Frontiers in Aging 2022, 3, 1077302. [Google Scholar] [CrossRef]
- Tohirova, J.; Shernazarov, F. Atherosclerosis: causes, symptoms, diagnosis, treatment and prevention. Science and innovation 2022, 1, 7–12. [Google Scholar]
- Alfarisi, H.A.H.; Mohamed, Z.B.H.; Ibrahim, M.B. Basic pathogenic mechanisms of atherosclerosis. Egyptian Journal of Basic and Applied Sciences 2020, 7, 116–125. [Google Scholar] [CrossRef]
- BUILDER, V. Cardiovascular Pathologies and Disorders. Mosby's Pathology for Massage Professionals-E-Book: Mosby's Pathology for Massage Professionals-E-Book, 2021; 234. [Google Scholar]
- Golledge, J. Update on the pathophysiology and medical treatment of peripheral artery disease. Nature reviews cardiology 2022, 19, 456–474. [Google Scholar] [CrossRef] [PubMed]
- Toyoda, K.; Ninomiya, T. Stroke and cerebrovascular diseases in patients with chronic kidney disease. The Lancet Neurology 2014, 13, 823–833. [Google Scholar] [CrossRef]
- Zhao, Q.; Yan, T.; Chopp, M.; Venkat, P.; Chen, J. Brain–kidney interaction: renal dysfunction following ischemic stroke. Journal of Cerebral Blood Flow & Metabolism 2020, 40, 246–262. [Google Scholar]
- Makrantonaki, E.; Wlaschek, M.; Scharffetter-Kochanek, K. Pathogenesis of wound healing disorders in the elderly. JDDG: Journal der Deutschen Dermatologischen Gesellschaft 2017, 15, 255–275. [Google Scholar] [CrossRef] [PubMed]
- Bowers, S.; Franco, E. Chronic wounds: evaluation and management. American family physician 2020, 101, 159–166. [Google Scholar] [PubMed]
- Haller, H.L.; Sander, F.; Popp, D.; Rapp, M.; Hartmann, B.; Demircan, M.; Nischwitz, S.P.; Kamolz, L.P. Oxygen, pH, lactate, and metabolism—How old knowledge and new insights might be combined for new wound treatment. Medicina 2021, 57, 1190. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Ding, B.-S. Comprehensive review of the vascular niche in regulating organ regeneration and fibrosis. Stem cells translational medicine 2022, 11, 1135–1142. [Google Scholar] [CrossRef]
- Gardener, H.; Wright, C.B.; Rundek, T.; Sacco, R.L. Brain health and shared risk factors for dementia and stroke. Nature Reviews Neurology 2015, 11, 651–657. [Google Scholar] [CrossRef]
- Bir, S.C.; Khan, M.W.; Javalkar, V.; Toledo, E.G.; Kelley, R.E. Emerging concepts in vascular dementia: a review. Journal of Stroke and Cerebrovascular Diseases 2021, 30, 105864. [Google Scholar] [CrossRef] [PubMed]
- Chojdak-Łukasiewicz, J.; Dziadkowiak, E.; Zimny, A.; Paradowski, B. Cerebral small vessel disease: A review. Advances in Clinical and Experimental Medicine 2021, 30, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.; Kalaria, R.N.; Corbett, A.; Ballard, C. Update on vascular dementia. Journal of geriatric psychiatry and neurology 2016, 29, 281–301. [Google Scholar] [CrossRef] [PubMed]
- Vasilijević, S.R.; Vuković, M.; Jerkić, L. Cognitive and language deficits in vascular dementia. Acta Medica Medianae 2021, 60. [Google Scholar] [CrossRef]
- D'Onofrio, G.; Sancarlo, D.; Addante, F.; Ciccone, F.; Cascavilla, L.; Paris, F.; Picoco, M.; Nuzzaci, C.; Elia, A.C.; Greco, A. Caregiver burden characterization in patients with Alzheimer's disease or vascular dementia. International journal of geriatric psychiatry 2015, 30, 891–899. [Google Scholar] [CrossRef]
- Xu, J.; Qiu, C. Worldwide economic costs and societal burden of dementia. Biomarkers for Preclinical Alzheimer’s Disease, 2018; 3-13. [Google Scholar]
- Béjot, Y.; Daubail, B.; Giroud, M. Epidemiology of stroke and transient ischemic attacks: Current knowledge and perspectives. Revue neurologique 2016, 172, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Lioutas, V.-A.; Ivan, C.S.; Himali, J.J.; Aparicio, H.J.; Leveille, T.; Romero, J.R.; Beiser, A.S.; Seshadri, S. Incidence of transient ischemic attack and association with long-term risk of stroke. Jama 2021, 325, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Schorr, E.N.; Peden-McAlpine, C.; Treat-Jacobson, D.; Lindquist, R. Characterization of the peripheral artery disease symptom experience. Geriatric Nursing 2015, 36, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Abola, M.T.B.; Evans, N.S.; Ratchford, E.V. Vascular disease patient information page: leg cramps. Vascular Medicine 2022, 27, 415–417. [Google Scholar] [CrossRef] [PubMed]
- Gardner, A.W.; Montgomery, P.S.; Wang, M.; Shen, B. Association between calf muscle oxygen saturation with ambulatory function and quality of life in symptomatic patients with peripheral artery disease. Journal of vascular surgery 2020, 72, 632–642. [Google Scholar] [CrossRef] [PubMed]
- Cerqueira, M.S.; Do Nascimento, J.D.S.; Maciel, D.G.; Barboza, J.A.M.; Vieira, W.H.D.B. Effects of blood flow restriction without additional exercise on strength reductions and muscular atrophy following immobilization: A systematic review. Journal of sport and health science 2020, 9, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Tibbs, D.J. Varicose veins and related disorders; Butterworth-Heinemann: 2013.
- Guo, S.a.; DiPietro, L.A. Factors affecting wound healing. Journal of dental research 2010, 89, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, H.N.; Hardman, M.J. Wound healing: cellular mechanisms and pathological outcomes. Open biology 2020, 10, 200223. [Google Scholar] [CrossRef]
- Hess, D.A.; Verma, S.; Bhatt, D.; Bakbak, E.; Terenzi, D.C.; Puar, P.; Cosentino, F. Vascular repair and regeneration in cardiometabolic diseases. European Heart Journal 2022, 43, 450–459. [Google Scholar] [CrossRef]
- Evans, C.E.; Iruela-Arispe, M.L.; Zhao, Y.-Y. Mechanisms of endothelial regeneration and vascular repair and their application to regenerative medicine. The American journal of pathology 2021, 191, 52–65. [Google Scholar] [CrossRef]
- Marco, M.; Valentina, I.; Daniele, M.; Valerio, D.R.; Andrea, P.; Roberto, G.; Laura, G.; Luigi, U. Peripheral arterial disease in persons with diabetic foot ulceration: a current comprehensive overview. Current Diabetes Reviews 2021, 17, 474–485. [Google Scholar] [CrossRef] [PubMed]
- Doughty, K.N.; Del Pilar, N.X.; Audette, A.; Katz, D.L. Lifestyle medicine and the management of cardiovascular disease. Current cardiology reports 2017, 19, 1–10. [Google Scholar] [CrossRef]
- Blumenthal, J.A.; Hinderliter, A.L.; Smith, P.J.; Mabe, S.; Watkins, L.L.; Craighead, L.; Ingle, K.; Tyson, C.; Lin, P.-H.; Kraus, W.E. Effects of lifestyle modification on patients with resistant hypertension: results of the TRIUMPH randomized clinical trial. Circulation 2021, 144, 1212–1226. [Google Scholar] [CrossRef] [PubMed]
- Sadat-Ebrahimi, S.R.; Parnianfard, N.; Vahed, N.; Babaei, H.; Ghojazadeh, M.; Tang, S.; Azarpazhooh, A. An evidence-based systematic review of the off-label uses of lisinopril. British journal of clinical pharmacology 2018, 84, 2502–2521. [Google Scholar] [CrossRef] [PubMed]
- Beltran Romero, L.M.; Vallejo-Vaz, A.J.; Muniz Grijalvo, O. Cerebrovascular disease and statins. Frontiers in Cardiovascular Medicine 2021, 8, 778740. [Google Scholar] [CrossRef] [PubMed]
- Liao, X.-Z.; Fu, Y.-H.; Ma, J.-Y.; Zhu, W.-G.; Yuan, P. Non-vitamin K antagonist oral anticoagulants versus warfarin in patients with atrial fibrillation and peripheral artery disease: a systematic review and meta-analysis. Cardiovascular Drugs and Therapy 2020, 34, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Mogul, A.; Leppien, E.E.; Laughlin, E.; Spinler, S.A. Aspirin for primary prevention of cardiovascular disease: a review of recent literature and updated guideline recommendations. Expert Opinion on Pharmacotherapy 2021, 22, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Mishima, E.; Suzuki, T.; Ito, S. Selection of patients for angioplasty for treatment of atherosclerotic renovascular disease: predicting responsive patients. American Journal of Hypertension 2020, 33, 391–401. [Google Scholar] [CrossRef] [PubMed]
- Zhao, K.; Zeng, Z.; He, Y.; Zhao, R.; Niu, J.; Sun, H.; Li, S.; Dong, J.; Jing, Z.; Zhou, J. Recent advances in targeted therapy for inflammatory vascular diseases. Journal of Controlled Release 2024, 372, 730–750. [Google Scholar] [CrossRef]
- Yu, X.; Wang, B.; Qiu, C.; He, Y.; Chen, T.; Zhu, Q.; Li, Z.; Wu, Z. A systematic review and meta-analysis of primary bypass surgery compared with bypass surgery after endovascular treatment in peripheral artery disease patients. Journal of Vascular Surgery 2023. [Google Scholar] [CrossRef]
- Minniti, G.; Laurindo, L.F.; Machado, N.M.; Duarte, L.G.; Guiguer, E.L.; Araujo, A.C.; Dias, J.A.; Lamas, C.B.; Nunes, Y.C.; Bechara, M.D. Mangifera indica L., By-Products, and Mangiferin on Cardio-Metabolic and Other Health Conditions: A Systematic Review. Life 2023, 13, 2270. [Google Scholar] [CrossRef] [PubMed]
- Nunes, Y.C.; de Oliveira Santos, G.; Machado, N.M.; Otoboni, A.M.; Laurindo, L.F.; Bishayee, A.; Fimognari, C.; Bishayee, A.; Barbalho, S.M. Peanut (Arachis hypogaea L.) seeds and by-products in metabolic syndrome and cardiovascular disorders: A systematic review of clinical studies. Phytomedicine, 2023; 155170. [Google Scholar]
- Takeda, L.N.; Laurindo, L.F.; Guiguer, E.L.; Bishayee, A.; Araújo, A.C.; Ubeda, L.C.C.; Goulart, R.d.A.; Barbalho, S.M. Psidium guajava L.: A systematic review of the multifaceted health benefits and economic importance. Food Reviews International 2023, 39, 4333–4363. [Google Scholar] [CrossRef]
- Laurindo, L.; Barbalho, S.; Araújo, A. Açaí (Euterpe oleracea Mart.) in health and disease: a critical review. Nutrients 15 (4): 989. 2023.
- Imaizumi, V.M.; Laurindo, L.F.; Manzan, B.; Guiguer, E.L.; Oshiiwa, M.; Otoboni, A.M.M.B.; Araujo, A.C.; Tofano, R.J.; Barbalho, S.M. Garlic: A systematic review of the effects on cardiovascular diseases. Critical Reviews in Food Science and Nutrition 2023, 63, 6797–6819. [Google Scholar] [CrossRef] [PubMed]
- Pagotto, G.L.d.O.; Santos, L.M.O.d.; Osman, N.; Lamas, C.B.; Laurindo, L.F.; Pomini, K.T.; Guissoni, L.M.; Lima, E.P.d.; Goulart, R.d.A.; Catharin, V.M.S. Ginkgo biloba: A Leaf of Hope in the Fight against Alzheimer’s Dementia: Clinical Trial Systematic Review. Antioxidants 2024, 13, 651. [Google Scholar] [CrossRef] [PubMed]
- Lu, M.; Zhang, L.; Pan, J.; Shi, H.; Zhang, M.; Li, C. Advances in the study of the vascular protective effects and molecular mechanisms of hawthorn (Crataegus anamesa Sarg.) extracts in cardiovascular diseases. Food & Function 2023, 14, 5870–5890. [Google Scholar]
- Cloud, A.; Vilcins, D.; McEwen, B. The effect of hawthorn (Crataegus spp.) on blood pressure: a systematic review. Advances in Integrative Medicine 2020, 7, 167–175. [Google Scholar] [CrossRef]
- Dwivedi, S.; Chopra, D. Revisiting Terminalia arjuna–an ancient cardiovascular drug. Journal of traditional and complementary medicine 2014, 4, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Thakur, S.; Kaurav, H.; Chaudhary, G. Terminalia arjuna: a potential ayurvedic cardio tonic. International Journal for Research in Applied Sciences and Biotechnology 2021, 8, 227–236. [Google Scholar] [CrossRef]
- Dutta, A.; Das, M. Terminalia arjuna and Cardiovascular Protection: A Comprehensive Overview. Ancient and Traditional Foods, Plants, Herbs and Spices used in Cardiovascular Health and Disease, 93–110.
- Trombetti, A.; Reid, K.; Hars, M.; Herrmann, F.; Pasha, E.; Phillips, E.; Fielding, R. Age-associated declines in muscle mass, strength, power, and physical performance: impact on fear of falling and quality of life. Osteoporosis international 2016, 27, 463–471. [Google Scholar] [CrossRef]
- Larsson, L.; Degens, H.; Li, M.; Salviati, L.; Lee, Y.I.; Thompson, W.; Kirkland, J.L.; Sandri, M. Sarcopenia: aging-related loss of muscle mass and function. Physiological reviews 2019, 99, 427–511. [Google Scholar] [CrossRef]
- Rodrigues, F.; Domingos, C.; Monteiro, D.; Morouço, P. A review on aging, sarcopenia, falls, and resistance training in community-dwelling older adults. International journal of environmental research and public health 2022, 19, 874. [Google Scholar] [CrossRef] [PubMed]
- Marzetti, E.; Calvani, R.; Bernabei, R.; Leeuwenburgh, C. Apoptosis in skeletal myocytes: a potential target for interventions against sarcopenia and physical frailty–a mini-review. Gerontology 2012, 58, 99–106. [Google Scholar] [CrossRef]
- Dao, T.; Green, A.E.; Kim, Y.A.; Bae, S.-J.; Ha, K.-T.; Gariani, K.; Lee, M.-r.; Menzies, K.J.; Ryu, D. Sarcopenia and muscle aging: a brief overview. Endocrinology and metabolism 2020, 35, 716–732. [Google Scholar] [CrossRef]
- Wiedmer, P.; Jung, T.; Castro, J.P.; Pomatto, L.C.; Sun, P.Y.; Davies, K.J.; Grune, T. Sarcopenia–Molecular mechanisms and open questions. Ageing research reviews 2021, 65, 101200. [Google Scholar] [CrossRef]
- Ranieri, F.; Di Lazzaro, V. The role of motor neuron drive in muscle fatigue. Neuromuscular Disorders 2012, 22, S157–S161. [Google Scholar] [CrossRef]
- Lepley, A.S.; Lepley, L.K. Mechanisms of arthrogenic muscle inhibition. Journal of sport rehabilitation 2021, 31, 707–716. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E. Hormones and sarcopenia. Current pharmaceutical design 2017, 23, 4484–4492. [Google Scholar] [CrossRef]
- Tezze, C.; Sandri, M.; Tessari, P. Anabolic resistance in the pathogenesis of sarcopenia in the elderly: role of nutrition and exercise in young and old people. Nutrients 2023, 15, 4073. [Google Scholar] [CrossRef] [PubMed]
- Pan, L.; Xie, W.; Fu, X.; Lu, W.; Jin, H.; Lai, J.; Zhang, A.; Yu, Y.; Li, Y.; Xiao, W. Inflammation and sarcopenia: a focus on circulating inflammatory cytokines. Experimental Gerontology 2021, 154, 111544. [Google Scholar] [CrossRef]
- Wang, J.; Leung, K.-S.; Chow, S.K.-H.; Cheung, W.-H. Inflammation and age-associated skeletal muscle deterioration (sarcopaenia). Journal of orthopaedic translation 2017, 10, 94–101. [Google Scholar] [CrossRef]
- Sharma, B.; Dabur, R. Role of pro-inflammatory cytokines in regulation of skeletal muscle metabolism: a systematic review. Current medicinal chemistry 2020, 27, 2161–2188. [Google Scholar] [CrossRef] [PubMed]
- Mahmoodi, M.; Shateri, Z.; Nazari, S.A.; Nouri, M.; Nasimi, N.; Sohrabi, Z.; Dabbaghmanesh, M.H. Association between oxidative balance score and sarcopenia in older adults. Scientific Reports 2024, 14, 5362. [Google Scholar] [CrossRef] [PubMed]
- Alhmly, H.F.; Fielding, R.A. A critical review of current worldwide definitions of sarcopenia. Calcified Tissue International 2024, 114, 74–81. [Google Scholar] [CrossRef]
- Nishikawa, H.; Asai, A.; Fukunishi, S.; Nishiguchi, S.; Higuchi, K. Metabolic syndrome and sarcopenia. Nutrients 2021, 13, 3519. [Google Scholar] [CrossRef] [PubMed]
- Capel, F.; Pinel, A.; Walrand, S. Accumulation of intramuscular toxic lipids, a link between fat mass accumulation and sarcopenia. OCL Oilseeds and fats crops and lipids 2019, 26, np. [Google Scholar] [CrossRef]
- de Lima, E.P.; Moretti Jr, R.C.; Torres Pomini, K.; Laurindo, L.F.; Sloan, K.P.; Sloan, L.A.; Castro, M.V.M.d.; Baldi Jr, E.; Ferraz, B.F.R.; de Souza Bastos Mazuqueli Pereira, E. Glycolipid Metabolic Disorders, Metainflammation, Oxidative Stress, and Cardiovascular Diseases: Unraveling Pathways. Biology 2024, 13, 519. [Google Scholar] [CrossRef]
- Masenga, S.K.; Kabwe, L.S.; Chakulya, M.; Kirabo, A. Mechanisms of oxidative stress in metabolic syndrome. International journal of molecular sciences 2023, 24, 7898. [Google Scholar] [CrossRef]
- Cho, H.H. Investigation of mechanisms responsible for myocyte cell death in metabolic syndrome. 2017.
- Delafontaine, P.; Yoshida, T. The renin-angiotensin system and the biology of skeletal muscle: mechanisms of muscle wasting in chronic disease states. Transactions of the American Clinical and Climatological Association 2016, 127, 245. [Google Scholar]
- Sasaki, K.-i.; Fukumoto, Y. Sarcopenia as a comorbidity of cardiovascular disease. Journal of cardiology 2022, 79, 596–604. [Google Scholar] [CrossRef]
- He, Y.; Xie, W.; Li, H.; Jin, H.; Zhang, Y.; Li, Y. Cellular senescence in sarcopenia: possible mechanisms and therapeutic potential. Frontiers in Cell and Developmental Biology 2022, 9, 793088. [Google Scholar] [CrossRef]
- Granic, A.; Suetterlin, K.; Shavlakadze, T.; Grounds, M.D.; Sayer, A.A. Hallmarks of ageing in human skeletal muscle and implications for understanding the pathophysiology of sarcopenia in women and men. Clinical Science 2023, 137, 1721–1751. [Google Scholar] [CrossRef] [PubMed]
- Priego, T.; Martín, A.; González-Hedström, D.; Granado, M.; López-Calderón, A. Role of hormones in sarcopenia. In Vitamins and hormones, Elsevier: 2021; Vol. 115, pp. 535-570.
- White, T.A.; LeBrasseur, N.K. Myostatin and sarcopenia: opportunities and challenges-a mini-review. Gerontology 2014, 60, 289–293. [Google Scholar] [CrossRef] [PubMed]
- Yasar, E.; Tek, N.A.; Tekbudak, M.Y.; Yurtdaş, G.; Gülbahar, Ö.; Uyar, G.Ö.; Ural, Z.; Çelik, Ö.M.; Erten, Y. The relationship between myostatin, inflammatory markers, and sarcopenia in patients with chronic kidney disease. Journal of Renal Nutrition 2022, 32, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Kwon, Y.N.; Yoon, S.S. Sarcopenia: neurological point of view. Journal of bone metabolism 2017, 24, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Delbono, O.; Rodrigues, A.C.Z.; Bonilla, H.J.; Messi, M.L. The emerging role of the sympathetic nervous system in skeletal muscle motor innervation and sarcopenia. Ageing research reviews 2021, 67, 101305. [Google Scholar] [CrossRef]
- Daily, J.W.; Park, S. Sarcopenia is a cause and consequence of metabolic dysregulation in aging humans: effects of gut dysbiosis, glucose dysregulation, diet and lifestyle. Cells 2022, 11, 338. [Google Scholar] [CrossRef]
- Antuña, E.; Cachán-Vega, C.; Bermejo-Millo, J.C.; Potes, Y.; Caballero, B.; Vega-Naredo, I.; Coto-Montes, A.; Garcia-Gonzalez, C. Inflammaging: implications in sarcopenia. International journal of molecular sciences 2022, 23, 15039. [Google Scholar] [CrossRef]
- Ooi, H.; Welch, C. Obstacles to the Early Diagnosis and Management of Sarcopenia: Current Perspectives. Clinical Interventions in Aging 2024, 323–332. [Google Scholar] [CrossRef]
- Qiu, C.; Yang, X.; Yu, P. Sarcopenia: Pathophysiology and Treatment Strategies. Endocrine, Metabolic & Immune Disorders-Drug Targets (Formerly Current Drug Targets-Immune, Endocrine & Metabolic Disorders) 2024, 24, 31–38. [Google Scholar]
- Hirsch, C.H.; Hategan, A. Physiology and pathology of aging. In Geriatric Psychiatry: A Case-Based Textbook, Springer: 2024; pp. 3-29.
- Rubin, J.; Nambi, V.; Chambless, L.E.; Steffes, M.W.; Juraschek, S.P.; Coresh, J.; Sharrett, A.R.; Selvin, E. Hyperglycemia and arterial stiffness: the atherosclerosis risk in the communities study. Atherosclerosis 2012, 225, 246–251. [Google Scholar] [CrossRef]
- Kim, H.-L. Arterial stiffness and hypertension. Clinical hypertension 2023, 29, 31. [Google Scholar] [CrossRef] [PubMed]
- Ikonomidis, I.; Thymis, J. The vicious circle of arterial elasticity, blood pressure, glycemia, and renal function. Hypertension Research 2023, 46, 1599–1602. [Google Scholar] [CrossRef] [PubMed]
- Laurent, S.; Agabiti-Rosei, C.; Bruno, R.M.; Rizzoni, D. Microcirculation and macrocirculation in hypertension: a dangerous cross-link? Hypertension 2022, 79, 479–490. [Google Scholar] [CrossRef] [PubMed]
- Tsuchikura, S.; Shoji, T.; Kimoto, E.; Shinohara, K.; Hatsuda, S.; Koyama, H.; Emoto, M.; Nishizawa, Y. Central versus peripheral arterial stiffness in association with coronary, cerebral and peripheral arterial disease. Atherosclerosis 2010, 211, 480–485. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.; McEniery, C.M. Central versus peripheral artery stiffening and cardiovascular risk. Arteriosclerosis, Thrombosis, and Vascular Biology 2020, 40, 1028–1033. [Google Scholar] [CrossRef] [PubMed]
- Fantin, F.; Giani, A.; Manzato, G.; Zampieri, A.; Comellato, G.; Urbani, S.; Zoico, E.; Mazzali, G.; Zamboni, M. Sarcopenia, sarcopenic obesity, and arterial stiffness among older adults. Frontiers in Cardiovascular Medicine 2024, 11. [Google Scholar] [CrossRef]
- Erkan, M.; OZCAN, S.G.G.; BEKIRCAVUSOGLU, A.F.; CATALKAYA, S. Sarcopenia is Associated with Aortic Arch Calcification on Chest X-ray in Unselected Middle-and Older-Aged Patients. 2024.
- Aziz, M.; Jacob, A.; Matsuda, A.; Wang, P. milk fat globule-EGF factor 8 expression, function and plausible signal transduction in resolving inflammation. Apoptosis 2011, 16, 1077–1086. [Google Scholar] [CrossRef] [PubMed]
- Ni, Y.-Q.; Zhan, J.-K.; Liu, Y.-S. Roles and mechanisms of MFG-E8 in vascular aging-related diseases. Ageing Research Reviews 2020, 64, 101176. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Jiang, M.; Fang, Z.T.; Chen, Z.; Li, L.; Liu, Z.; Wang, J.; Yin, X.; Wang, J.; Wu, M. Current evidence of synaptic dysfunction after stroke: Cellular and molecular mechanisms. CNS Neuroscience & Therapeutics 2024, 30, e14744. [Google Scholar]
- Danese, E.; Montagnana, M.; Lippi, G. Proteomics and frailty: a clinical overview. Expert Review of Proteomics 2018, 15, 657–664. [Google Scholar] [CrossRef]
- Tuo, Q.z.; Zhang, S.t.; Lei, P. Mechanisms of neuronal cell death in ischemic stroke and their therapeutic implications. Medicinal research reviews 2022, 42, 259–305. [Google Scholar] [CrossRef] [PubMed]
- Gunsch, G.; Paradie, E.; Townsend, K.L. Peripheral nervous system glia in support of metabolic tissue functions. Trends in Endocrinology & Metabolism, 2023. [Google Scholar]
- Kuzuya, M. Drug-related sarcopenia as a secondary sarcopenia. Geriatrics & Gerontology International 2024, 24, 195–203. [Google Scholar]
- Swidan, S. Drug-Related Sarcopenia. In Metabolic Therapies in Orthopedics, Second Edition, CRC Press: 2018; pp. 239-249.
- Matsumoto, A.; Yoshimura, Y.; Nagano, F.; Shimazu, S.; Shiraishi, A.; Kido, Y.; Bise, T. Potentially inappropriate medications are negatively associated with functional recovery in patients with sarcopenia after stroke. Aging Clinical and Experimental Research 2022, 34, 2845–2855. [Google Scholar] [CrossRef]
- Saied, S.; Prokopidis, K.; Adenaya, A.; Isanejad, M.; Sankaranarayanan, R. Is sarcopenia an associated factor of increased administration of specific medications in patients with heart failure? A systematic review and meta-analysis. Frontiers in Cardiovascular Medicine 2024, 11. [Google Scholar] [CrossRef] [PubMed]
- Zamboni, M.; Mazzali, G.; Brunelli, A.; Saatchi, T.; Urbani, S.; Giani, A.; Rossi, A.P.; Zoico, E.; Fantin, F. The role of crosstalk between adipose cells and myocytes in the pathogenesis of sarcopenic obesity in the elderly. Cells 2022, 11, 3361. [Google Scholar] [CrossRef]
- Ciudin, A.; Simó-Servat, A.; Palmas, F.; Barahona, M.J. Sarcopenic obesity: a new challenge in the clinical practice. Endocrinología, Diabetes y Nutrición (English ed.) 2020, 67, 672–681. [Google Scholar] [CrossRef]
- Benz, E.; Pinel, A.; Guillet, C.; Capel, F.; Pereira, B.; De Antonio, M.; Pouget, M.; Cruz-Jentoft, A.J.; Eglseer, D.; Topinkova, E. , et al. Sarcopenia and Sarcopenic Obesity and Mortality Among Older People. JAMA Netw Open 2024, 7, e243604. [Google Scholar] [CrossRef]
- Silveira, E.A.; da Silva Filho, R.R.; Spexoto, M.C.B.; Haghighatdoost, F.; Sarrafzadegan, N.; de Oliveira, C. The role of sarcopenic obesity in cancer and cardiovascular disease: a synthesis of the evidence on pathophysiological aspects and clinical implications. International journal of molecular sciences 2021, 22, 4339. [Google Scholar] [CrossRef]
- Evans, K.; Abdelhafiz, D.; Abdelhafiz, A.H. Sarcopenic obesity as a determinant of cardiovascular disease risk in older people: a systematic review. Postgraduate medicine 2021, 133, 831–842. [Google Scholar] [CrossRef]
- Bellafronte, N.T.; de Queirós Mattoso Ono, A.; Chiarello, P.G. Sarcopenic obesity in chronic kidney disease: challenges in diagnosis using different diagnostic criteria. Medical Principles and Practice 2021, 30, 477–486. [Google Scholar] [CrossRef]
- Lynch, G.; Murphy, C.; de Marco Castro, E.; Roche, H. Inflammation and metabolism: the role of adiposity in sarcopenic obesity. Proceedings of the Nutrition Society 2020, 79, 435–447. [Google Scholar] [CrossRef]
- Gonzalez, A.; Simon, F.; Achiardi, O.; Vilos, C.; Cabrera, D.; Cabello-Verrugio, C. The critical role of oxidative stress in sarcopenic obesity. Oxidative Medicine and Cellular Longevity 2021, 2021, 4493817. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.-h.; Choi, K.M. Sarcopenic obesity, insulin resistance, and their implications in cardiovascular and metabolic consequences. International journal of molecular sciences 2020, 21, 494. [Google Scholar] [CrossRef]
- Jurdana, M.; Cemazar, M. Sarcopenic obesity in cancer. Radiology and Oncology 2024, 58, 1–8. [Google Scholar] [CrossRef]
- Carneiro, I.P.; Mazurak, V.C.; Prado, C.M. Clinical implications of sarcopenic obesity in cancer. Current oncology reports 2016, 18, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Chou, H.-H.; Lai, T.-J.; Yen, C.-H.; Chang, P.-S.; Pan, J.-C.; Lin, P.-T. Sarcopenic obesity tendency and nutritional status is related to the risk of sarcopenia, frailty, depression and quality of life in patients with dementia. International journal of environmental research and public health 2022, 19, 2492. [Google Scholar] [CrossRef]
- Zhang, J.; Na, X.; Li, Z.; Ji, J.S.; Li, G.; Yang, H.; Yang, Y.; Tan, Y.; Zhang, J.; Xi, M. Sarcopenic obesity is part of obesity paradox in dementia development: evidence from a population-based cohort study. BMC medicine 2024, 22, 133. [Google Scholar] [CrossRef]
- Long, D.; Liu, M.; Li, H.; Song, J.; Jiang, X.; Wang, G.; Yang, X. Dysbacteriosis induces abnormal neurogenesis via LPS in a pathway requiring NF-κB/IL-6. Pharmacological Research 2021, 167, 105543. [Google Scholar] [CrossRef] [PubMed]
- Lyra e Silva, N.M.; Gonçalves, R.A.; Pascoal, T.A.; Lima-Filho, R.A.; Resende, E.d.P.F.; Vieira, E.L.; Teixeira, A.L.; de Souza, L.C.; Peny, J.A.; Fortuna, J.T. Pro-inflammatory interleukin-6 signaling links cognitive impairments and peripheral metabolic alterations in Alzheimer’s disease. Translational psychiatry 2021, 11, 251. [Google Scholar] [CrossRef]
- Mucher, P.; Batmyagmar, D.; Perkmann, T.; Repl, M.; Radakovics, A.; Ponocny-Seliger, E.; Lukas, I.; Fritzer-Szekeres, M.; Lehrner, J.; Knogler, T. Basal myokine levels are associated with quality of life and depressed mood in older adults. Psychophysiology 2021, 58, e13799. [Google Scholar] [CrossRef]
- Sadier, N.S.; El Hajjar, F.; Al Sabouri, A.A.K.; Abou-Abbas, L.; Siomava, N.; Almutary, A.G.; Tambuwala, M.M. Irisin: An unveiled bridge between physical exercise and a healthy brain. Life Sciences 2024, 339, 122393. [Google Scholar] [CrossRef] [PubMed]
- Pignataro, P.; Dicarlo, M.; Zerlotin, R.; Zecca, C.; Dell’Abate, M.T.; Buccoliero, C.; Logroscino, G.; Colucci, S.; Grano, M. FNDC5/Irisin system in neuroinflammation and neurodegenerative diseases: update and novel perspective. International Journal of Molecular Sciences 2021, 22, 1605. [Google Scholar] [CrossRef] [PubMed]
- Zheng, S.; Chen, N.; Kang, X.; Hu, Y.; Shi, S. Irisin alleviates FFA induced β-cell insulin resistance and inflammatory response through activating PI3K/AKT/FOXO1 signaling pathway. Endocrine 2022, 1–12. [Google Scholar]
- Wang, Y.; Tian, M.; Tan, J.; Pei, X.; Lu, C.; Xin, Y.; Deng, S.; Zhao, F.; Gao, Y.; Gong, Y. Irisin ameliorates neuroinflammation and neuronal apoptosis through integrin αVβ5/AMPK signaling pathway after intracerebral hemorrhage in mice. Journal of Neuroinflammation 2022, 19, 82. [Google Scholar] [CrossRef] [PubMed]
- Fang, M.; Liu, C.; Liu, Y.; Tang, G.; Li, C.; Guo, L. Association between sarcopenia with incident cardio-cerebrovascular disease: A systematic review and meta-analysis. BioScience Trends 2023, 17, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Khadra, D.; Itani, L.; Tannir, H.; Kreidieh, D.; El Masri, D.; El Ghoch, M. Association between sarcopenic obesity and higher risk of type 2 diabetes in adults: a systematic review and meta-analysis. World journal of diabetes 2019, 10, 311. [Google Scholar] [CrossRef] [PubMed]
- Pilati, I.; Slee, A.; Frost, R. Sarcopenic obesity and depression: a systematic review. The Journal of Frailty & Aging, 2022; 1–8. [Google Scholar]
- Kueck, P.J.; Morris, J.K.; Stanford, J.A. Current Perspectives: Obesity and Neurodegeneration-Links and Risks. Degenerative neurological and neuromuscular disease 2024, 111–129. [Google Scholar] [CrossRef] [PubMed]
- Jung, C.-H.; Mok, J.-O. Recent Updates on Associations among Various Obesity Metrics and Cognitive Impairment: from Body Mass Index to Sarcopenic Obesity. Journal of Obesity & Metabolic Syndrome 2022, 31, 287. [Google Scholar]
- Mastelić, T.; Višić, V.; Marasović, T.B.; Milanović, M.; Kralj, Ž.; Burilović, E.; Pernat, M.; Vukorepa, D.; Rančić, N.; Baković, M. Sarkopenija kod osoba oboljelih od demencije/Sarcopenia in Persons Suffering from Dementia.
- Booranasuksakul, U.; Macdonald, I.A.; Stephan, B.C.; Siervo, M. Body Composition, Sarcopenic Obesity, and Cognitive Function in Older Adults: Findings From the National Health and Nutrition Examination Survey (NHANES) 1999–2002 and 2011–2014. Journal of the American Nutrition Association 2024, 1–14. [Google Scholar] [CrossRef]
- Damluji, A.A.; Alfaraidhy, M.; AlHajri, N.; Rohant, N.N.; Kumar, M.; Al Malouf, C.; Bahrainy, S.; Ji Kwak, M.; Batchelor, W.B.; Forman, D.E. Sarcopenia and cardiovascular diseases. Circulation 2023, 147, 1534–1553. [Google Scholar] [CrossRef]
- He, N.; Zhang, Y.; Zhang, L.; Zhang, S.; Ye, H. Relationship between sarcopenia and cardiovascular diseases in the elderly: an overview. Frontiers in cardiovascular medicine 2021, 8, 743710. [Google Scholar] [CrossRef] [PubMed]
- Pizzimenti, M.; Meyer, A.; Charles, A.L.; Giannini, M.; Chakfé, N.; Lejay, A.; Geny, B. Sarcopenia and peripheral arterial disease: a systematic review. Journal of cachexia, sarcopenia and muscle 2020, 11, 866–886. [Google Scholar] [CrossRef] [PubMed]
- Cretoiu, S.M.; Zugravu, C.A. Nutritional considerations in preventing muscle atrophy. Muscle Atrophy 2018, 497–528. [Google Scholar]
- Muñoz-Cánoves, P.; Neves, J.; Sousa-Victor, P. Understanding muscle regenerative decline with aging: new approaches to bring back youthfulness to aged stem cells. The FEBS journal 2020, 287, 406–416. [Google Scholar] [CrossRef] [PubMed]
- Mojikon, F.D.; Kasimin, M.E.; Molujin, A.M.; Gansau, J.A.; Jawan, R. Probiotication of Nutritious Fruit and Vegetable Juices: An Alternative to Dairy-Based Probiotic Functional Products. Nutrients 2022, 14. [Google Scholar] [CrossRef]
- Kim, K.; Anderson, E.M.; Scali, S.T.; Ryan, T.E. Skeletal muscle mitochondrial dysfunction and oxidative stress in peripheral arterial disease: a unifying mechanism and therapeutic target. Antioxidants 2020, 9, 1304. [Google Scholar] [CrossRef] [PubMed]
- Damiano, S.; Muscariello, E.; La Rosa, G.; Di Maro, M.; Mondola, P.; Santillo, M. Dual role of reactive oxygen species in muscle function: can antioxidant dietary supplements counteract age-related sarcopenia? International journal of molecular sciences 2019, 20, 3815. [Google Scholar] [CrossRef] [PubMed]
- Thoma, A.; Akter-Miah, T.; Reade, R.L.; Lightfoot, A.P. Targeting reactive oxygen species (ROS) to combat the age-related loss of muscle mass and function. Biogerontology 2020, 21, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Poggiogalle, E.; Mendes, I.; Ong, B.; Prado, C.M.; Mocciaro, G.; Mazidi, M.; Lubrano, C.; Lenzi, A.; Donini, L.M.; Siervo, M. Sarcopenic obesity and insulin resistance: Application of novel body composition models. Nutrition 2020, 75, 110765. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.-j.; Zhu, C.-f. Causal relationship between insulin resistance and sarcopenia. Diabetology & metabolic syndrome 2023, 15, 46. [Google Scholar]
- Cleasby, M.E.; Jamieson, P.; Atherton, P.J. Insulin resistance and sarcopenia: mechanistic links between common co-morbidities. Journal of Endocrinology 2016. [Google Scholar] [CrossRef]
- Barbalho, S.M.; Flato, U.A.P.; Tofano, R.J.; Goulart, R.d.A.; Guiguer, E.L.; Detregiachi, C.R.P.; Buchaim, D.V.; Araújo, A.C.; Buchaim, R.L.; Reina, F.T.R. Physical exercise and myokines: relationships with sarcopenia and cardiovascular complications. International journal of molecular sciences 2020, 21, 3607. [Google Scholar] [CrossRef] [PubMed]
- Laurindo, L.F.; Camargo, F.C.; Perfeito, A.; Ciano, B.B.; Coelho, C.T.; Apolinário, G.A.; Vicentin, I.D.N.; Andreasi, J.C.; Boaro, B.L.; Tofano, R.J. Examining the Correlations between the Visceral Adiposity Index and Various Anthropometric, Biochemical, and Insulin Resistance Parameters in Brazilians: Findings from a Cross-Sectional Study. 2024.
- Lopez-Candales, A.; Burgos, P.M.H.; Hernandez-Suarez, D.F.; Harris, D. Linking chronic inflammation with cardiovascular disease: from normal aging to the metabolic syndrome. Journal of nature and science 2017, 3. [Google Scholar]
- Pansuria, M.; Xi, H.; Li, L.; Yang, X.-F.; Wang, H. Insulin resistance, metabolic stress, and atherosclerosis. Frontiers in bioscience (Scholar edition) 2012, 4, 916. [Google Scholar]
- Poznyak, A.; Grechko, A.V.; Poggio, P.; Myasoedova, V.A.; Alfieri, V.; Orekhov, A.N. The diabetes mellitus–atherosclerosis connection: The role of lipid and glucose metabolism and chronic inflammation. International journal of molecular sciences 2020, 21, 1835. [Google Scholar] [CrossRef] [PubMed]
- Silveira Rossi, J.L.; Barbalho, S.M.; Reverete de Araujo, R.; Bechara, M.D.; Sloan, K.P.; Sloan, L.A. Metabolic syndrome and cardiovascular diseases: Going beyond traditional risk factors. Diabetes/metabolism research and reviews 2022, 38, e3502. [Google Scholar] [CrossRef] [PubMed]
- Wakabayashi, H.; Sakuma, K. Comprehensive approach to sarcopenia treatment. Current clinical pharmacology 2014, 9, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, T. Selected methods of resistance training for prevention and treatment of sarcopenia. Cells 2022, 11, 1389. [Google Scholar] [CrossRef] [PubMed]
- Malafarina, V.; Uriz-Otano, F.; Iniesta, R.; Gil-Guerrero, L. Effectiveness of nutritional supplementation on muscle mass in treatment of sarcopenia in old age: a systematic review. Journal of the American Medical Directors Association 2013, 14, 10–17. [Google Scholar] [CrossRef]
- Kwak, J.Y.; Kwon, K.-S. Pharmacological interventions for treatment of sarcopenia: current status of drug development for sarcopenia. Annals of geriatric medicine and research 2019, 23, 98. [Google Scholar] [CrossRef]
- Ispoglou, T.; Wilson, O.; McCullough, D.; Aldrich, L.; Ferentinos, P.; Lyall, G.; Stavropoulos-Kalinoglou, A.; Duckworth, L.; Brown, M.A.; Sutton, L. A narrative review of non-pharmacological strategies for managing sarcopenia in older adults with cardiovascular and metabolic diseases. Biology 2023, 12, 892. [Google Scholar] [CrossRef]
- Rivera, F.B.; Escolano, B.T.; Nifas, F.M.; Choi, S.; Carado, G.P.; Lerma, E.; Vijayaraghavan, K.; Yu, M.G. Interrelationship of Sarcopenia and Cardiovascular Diseases: A review of potential mechanisms and management. Journal of the ASEAN Federation of Endocrine Societies 2024, 39, 69. [Google Scholar] [CrossRef] [PubMed]
- Fábrega-Cuadros, R.; Hita-Contreras, F.; Martínez-Amat, A.; Jiménez-García, J.D.; Achalandabaso-Ochoa, A.; Lavilla-Lerma, L.; García-Garro, P.A.; Álvarez-Salvago, F.; Aibar-Almazán, A. Associations between the severity of sarcopenia and health-related quality of life in community-dwelling middle-aged and older adults. International Journal of Environmental Research and Public Health 2021, 18, 8026. [Google Scholar] [CrossRef]
- Reis, J.M.S.; Alves, L.S.; Vogt, B.P. According to revised EWGSOP sarcopenia consensus cut-off points, low physical function is associated with nutritional status and quality of life in maintenance hemodialysis patients. Journal of Renal Nutrition 2022, 32, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Haider, S.; Luger, E.; Kapan, A.; Titze, S.; Lackinger, C.; Schindler, K.E.; Dorner, T.E. Associations between daily physical activity, handgrip strength, muscle mass, physical performance and quality of life in prefrail and frail community-dwelling older adults. Quality of Life Research 2016, 25, 3129–3138. [Google Scholar] [CrossRef]
- Swan, L.; Martin, N.; Horgan, N.F.; Warters, A.; O’Sullivan, M. Assessing Sarcopenia, Frailty, and Malnutrition in Community-Dwelling Dependant Older Adults—An Exploratory Home-Based Study of an Underserved Group in Research. International Journal of Environmental Research and Public Health 2022, 19, 16133. [Google Scholar] [CrossRef]
- Liguori, I.; Russo, G.; Aran, L.; Bulli, G.; Curcio, F.; Della-Morte, D.; Gargiulo, G.; Testa, G.; Cacciatore, F.; Bonaduce, D. Sarcopenia: assessment of disease burden and strategies to improve outcomes. Clinical interventions in aging 2018, 913–927. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Chen, C. Towards a mechanistic understanding of depression, anxiety, and their comorbidity: Perspectives from cognitive neuroscience. Frontiers Media SA: 2023; Vol. 17, p 1268156.
- Nogueira, G.; Fidelix, Y.L.; Nascimento, J.R.A.d.; Oliveira, D.V.d. Physical activity and sedentary behavior as predictors of fear of falling and risk of sarcopenia in older adults. Fisioterapia em Movimento 2023, 36, e36118. [Google Scholar] [CrossRef]
- Öztürk, G.B.; Kiliç, C.; Bozkurt, M.; Karan, M.A. Prevalence and associates of fear of falling among community-dwelling older adults. The Journal of nutrition, health and aging 2021, 25, 433–439. [Google Scholar] [CrossRef]
- Manrique-Espinoza, B.; Salinas-Rodríguez, A.; Rosas-Carrasco, O.; Gutiérrez-Robledo, L.M.; Avila-Funes, J.A. Sarcopenia is associated with physical and mental components of health-related quality of life in older adults. Journal of the American medical directors association 2017, 18, 636–e631. [Google Scholar] [CrossRef]
- Bruyère, O.; Beaudart, C.; Ethgen, O.; Reginster, J.-Y.; Locquet, M. The health economics burden of sarcopenia: a systematic review. Maturitas 2019, 119, 61–69. [Google Scholar] [CrossRef]
- Mijnarends, D.; Schols, J.; Halfens, R.; Meijers, J.; Luiking, Y.; Verlaan, S.; Evers, S. Burden-of-illness of Dutch community-dwelling older adults with sarcopenia: Health related outcomes and costs. European Geriatric Medicine 2016, 7, 276–284. [Google Scholar] [CrossRef]
- Denison, H.J.; Cooper, C.; Sayer, A.A.; Robinson, S.M. Prevention and optimal management of sarcopenia: a review of combined exercise and nutrition interventions to improve muscle outcomes in older people. Clinical interventions in aging 2015, 859–869. [Google Scholar]
- Negm, A.M.; Lee, J.; Hamidian, R.; Jones, C.A.; Khadaroo, R.G. Management of sarcopenia: a network meta-analysis of randomized controlled trials. Journal of the American Medical Directors Association 2022, 23, 707–714. [Google Scholar] [CrossRef] [PubMed]
- Xie, W.-Q.; Xiao, G.-L.; Hu, P.-W.; He, Y.-Q.; Lv, S.; Xiao, W.-F. Possible sarcopenia: early screening and intervention-narrative review. Annals of Palliative Medicine 2020, 9, 4283293–4284293. [Google Scholar] [CrossRef] [PubMed]
- Cannataro, R.; Cione, E.; Bonilla, D.A.; Cerullo, G.; Angelini, F.; D'Antona, G. Strength training in elderly: An useful tool against sarcopenia. Frontiers in sports and active living 2022, 4, 950949. [Google Scholar] [CrossRef] [PubMed]
- Barbalho, S.M.; de Alvares Goulart, R.; Minniti, G.; Bechara, M.D.; de Castro, M.V.M.; Dias, J.A.; Laurindo, L.F. Unraveling the rationale and conducting a comprehensive assessment of KD025 (Belumosudil) as a candidate drug for inhibiting adipogenic differentiation—a systematic review. Naunyn-Schmiedeberg's Archives of Pharmacology 2024, 397, 2681–2699. [Google Scholar] [CrossRef]
- Mellen, R.; Girotto, O.; Marques, E.; Laurindo, L.; Grippa, P.; Mendes, C. Insights into Pathogenesis, Nutritional and Drug Approach in Sarcopenia: A Systematic Review. Biomedicines 2023, 11, 1, 136. [Google Scholar] [CrossRef]
- Coelho-Júnior, H.J.; Calvani, R.; Picca, A.; Tosato, M.; Landi, F.; Marzetti, E. Engagement in aerobic exercise is associated with a reduced prevalence of sarcopenia and severe sarcopenia in Italian older adults. Journal of Personalized Medicine 2023, 13, 655. [Google Scholar] [CrossRef]
- Aoki, K.; Konno, M.; Honda, K.; Abe, T.; Nagata, T.; Takehara, M.; Sugasawa, T.; Takekoshi, K.; Ohmori, H. Habitual aerobic exercise diminishes the effects of sarcopenia in senescence-accelerated mice Prone8 model. Geriatrics 2020, 5, 48. [Google Scholar] [CrossRef]
- Hickson, M. Nutritional interventions in sarcopenia: a critical review. Proceedings of the Nutrition Society 2015, 74, 378–386. [Google Scholar] [CrossRef] [PubMed]
- Damanti, S.; Azzolino, D.; Roncaglione, C.; Arosio, B.; Rossi, P.; Cesari, M. Efficacy of nutritional interventions as stand-alone or synergistic treatments with exercise for the management of sarcopenia. Nutrients 2019, 11, 1991. [Google Scholar] [CrossRef] [PubMed]
- Breen, L.; Phillips, S.M. Skeletal muscle protein metabolism in the elderly: Interventions to counteract the'anabolic resistance'of ageing. Nutrition & metabolism 2011, 8, 1–11. [Google Scholar]
- Barbalho, S.M.; Sloan, L.A.; Araujo, A.C.; Laurindo, L.F.; Sloan, K.P. Vitamin D and Its Role on Inflammation, Oxidative Stress and Cardiovascular Disease. In Lipophilic Vitamins in Health and Disease, Springer: 2024; pp. 291-311.
- Lalia, A. Omega-3 fatty acids to combat sarcopenia; College of Medicine-Mayo Clinic: 2016.
- Bruyère, O.; Reginster, J.-Y.; Beaudart, C. Lifestyle approaches to prevent and retard sarcopenia: A narrative review. Maturitas 2022, 161, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Barazzoni, R.; Bischoff, S.; Boirie, Y.; Busetto, L.; Cederholm, T.; Dicker, D.; Toplak, H.; Van Gossum, A.; Yumuk, V.; Vettor, R. Sarcopenic obesity: time to meet the challenge. Obesity facts 2018, 11, 294–305. [Google Scholar] [CrossRef] [PubMed]
- Picca, A.; Fanelli, F.; Calvani, R.; Mulè, G.; Pesce, V.; Sisto, A.; Pantanelli, C.; Bernabei, R.; Landi, F.; Marzetti, E. Gut dysbiosis and muscle aging: searching for novel targets against sarcopenia. Mediators of Inflammation 2018, 2018, 7026198. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Cheung, W.H.; Li, J.; Chow, S.K.H.; Yu, J.; Wong, S.H.; Ip, M.; Sung, J.J.Y.; Wong, R.M.Y. Understanding the gut microbiota and sarcopenia: a systematic review. Journal of cachexia, sarcopenia and muscle 2021, 12, 1393–1407. [Google Scholar] [CrossRef]
- Sakuma, K.; Hamada, K.; Yamaguchi, A.; Aoi, W. Current nutritional and pharmacological approaches for attenuating sarcopenia. Cells 2023, 12, 2422. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.-T.; Wang, J.-H. The therapeutic intervention of sex steroid hormones for sarcopenia. Frontiers in Medicine 2021, 8, 739251. [Google Scholar] [CrossRef]
- German, I.J.S.; Torres, K.; Andreo, J.C.; Shindo, J.; Dallantonia, C.; Haber, L.; Detregiachi, C.R.P.; Araujo, A.; Guiguer, E.L.; Girio, R. New Trends to Treat Muscular Atrophy: Systematic Review. 2023.
- Laurindo, L.F.; Barbalho, S.M.; Marquess, A.R.; Grecco, A.I.d.S.; Goulart, R.d.A.; Tofano, R.J.; Bishayee, A. Pomegranate (Punica granatum L.) and metabolic syndrome risk factors and outcomes: A systematic review of clinical studies. Nutrients 2022, 14, 1665. [Google Scholar] [CrossRef]
- Kim, A.; Park, S.-M.; Kim, N.S.; Lee, H. Ginsenoside Rc, an Active Component of Panax ginseng, Alleviates Oxidative Stress-Induced Muscle Atrophy via Improvement of Mitochondrial Biogenesis. Antioxidants 2023, 12, 1576. [Google Scholar] [CrossRef] [PubMed]
- Rondanelli, M.; Miccono, A.; Peroni, G.; Guerriero, F.; Morazzoni, P.; Riva, A.; Guido, D.; Perna, S. A systematic review on the effects of botanicals on skeletal muscle health in order to prevent sarcopenia. Evidence-Based Complementary and Alternative Medicine 2016, 2016, 5970367. [Google Scholar] [CrossRef] [PubMed]
- Oliynyk, S.; Oh, S. Actoprotective effect of ginseng: improving mental and physical performance. Journal of ginseng research 2013, 37, 144. [Google Scholar] [CrossRef]
- Lopresti, A.L.; Smith, S.J. Ashwagandha (Withania somnifera) for the treatment and enhancement of mental and physical conditions: A systematic review of human trials. Journal of Herbal Medicine 2021, 28, 100434. [Google Scholar] [CrossRef]
- Laurindo, L.F.; de Carvalho, G.M.; de Oliveira Zanuso, B.; Figueira, M.E.; Direito, R.; de Alvares Goulart, R.; Buglio, D.S.; Barbalho, S.M. Curcumin-based nanomedicines in the treatment of inflammatory and immunomodulated diseases: An evidence-based comprehensive review. Pharmaceutics 2023, 15, 229. [Google Scholar] [CrossRef]
- Silva, I.F.d.; Bragante, W.R.; Junior, R.C.M.; Laurindo, L.F.; Guiguer, E.L.; Araújo, A.C.; Fiorini, A.M.; Nicolau, C.C.; Oshiiwa, M.; Lima, E.P.d. Effects of Smallanthus sonchifolius Flour on Metabolic Parameters: A Systematic Review. Pharmaceuticals 2024, 17, 658. [Google Scholar] [CrossRef]
- Laurindo, L.F.; Rodrigues, V.D.; Minniti, G.; de Carvalho, A.C.A.; Zutin, T.L.M.; DeLiberto, L.K.; Bishayee, A.; Barbalho, S.M. Pomegranate (Punica granatum L.) phytochemicals target the components of metabolic syndrome. The Journal of Nutritional Biochemistry, 0967. [Google Scholar]
- German, I.J.S.; Pomini, K.T.; Andreo, J.C.; Shindo, J.V.T.C.; Castro, M.V.M.d.; Detregiachi, C.R.P.; Araújo, A.C.; Guiguer, E.L.; Fornari Laurindo, L.; Bueno, P.C.d.S. New Trends to Treat Muscular Atrophy: A Systematic Review of Epicatechin. Nutrients 2024, 16, 326. [Google Scholar] [CrossRef]
- Zhang, W.; Xiao, D.; Mao, Q.; Xia, H. Role of neuroinflammation in neurodegeneration development. Signal Transduction and Targeted Therapy 2023, 8, 267. [Google Scholar] [CrossRef]
- Ciurea, A.V.; Mohan, A.G.; Covache-Busuioc, R.-A.; Costin, H.-P.; Glavan, L.-A.; Corlatescu, A.-D.; Saceleanu, V.M. Unraveling molecular and genetic insights into neurodegenerative diseases: Advances in understanding Alzheimer’s, Parkinson’s, and Huntington’s diseases and amyotrophic lateral sclerosis. International journal of molecular sciences 2023, 24, 10809. [Google Scholar] [CrossRef]
- Tanaka, M.; Tuka, B.; Vécsei, L. Navigating the Neurobiology of Migraine: From Pathways to Potential Therapies. MDPI: 2024; Vol. 13, p 1098.
- Pluvinage, J.V.; Wyss-Coray, T. Systemic factors as mediators of brain homeostasis, ageing and neurodegeneration. Nature Reviews Neuroscience 2020, 21, 93–102. [Google Scholar] [CrossRef]
- Sheikh, A.M.; Yano, S.; Tabassum, S.; Nagai, A. The Role of the Vascular System in Degenerative Diseases: Mechanisms and Implications. International Journal of Molecular Sciences 2024, 25, 2169. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, M.D.; Kisler, K.; Montagne, A.; Toga, A.W.; Zlokovic, B.V. The role of brain vasculature in neurodegenerative disorders. Nature neuroscience 2018, 21, 1318–1331. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Wang, L.; Cheng, W.; Lv, J.; Guan, X.; Guo, T.; Wu, J.; Zhang, W.; Gao, T.; Liu, X. Two distinct trajectories of clinical and neurodegeneration events in Parkinson’s disease. npj Parkinson's Disease 2023, 9, 111. [Google Scholar] [CrossRef] [PubMed]
- Bartl, M.; Dakna, M.; Schade, S.; Otte, B.; Wicke, T.; Lang, E.; Starke, M.; Ebentheuer, J.; Weber, S.; Toischer, K. Blood markers of inflammation, neurodegeneration, and cardiovascular risk in early Parkinson's disease. Movement Disorders 2023, 38, 68–81. [Google Scholar] [CrossRef] [PubMed]
- Nim, S.; O’Hara, D.M.; Corbi-Verge, C.; Perez-Riba, A.; Fujisawa, K.; Kapadia, M.; Chau, H.; Albanese, F.; Pawar, G.; De Snoo, M.L. Disrupting the α-synuclein-ESCRT interaction with a peptide inhibitor mitigates neurodegeneration in preclinical models of Parkinson’s disease. Nature Communications 2023, 14, 2150. [Google Scholar] [CrossRef] [PubMed]
- Gupta, D.; Kuruvilla, A. Vascular parkinsonism: what makes it different? Postgraduate medical journal 2011, 87, 829–836. [Google Scholar] [CrossRef] [PubMed]
- Jacob, M.A.; Cai, M.; Bergkamp, M.; Darweesh, S.K.; Gelissen, L.M.; Marques, J.; Norris, D.G.; Duering, M.; Esselink, R.A.; Tuladhar, A.M. Cerebral small vessel disease progression increases risk of incident parkinsonism. Annals of neurology 2023, 93, 1130–1141. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhang, C.; Xu, W.; Chen, J.; Tuo, J.; Wen, Y.; Huang, Z.; Zeng, R. Serum Sirtuin1 level decreases in Parkinson's disease and vascular parkinsonism: A prospective observational study. Clinical Neurology and Neurosurgery 2023, 225, 107595. [Google Scholar] [CrossRef] [PubMed]
- Oveisgharan, S.; Yu, L.; Poole, V.N.; Evia, A.M.; Barnes, L.L.; Schneider, J.A.; Arfanakis, K.; Bennett, D.A.; Buchman, A.S. Association of white matter hyperintensities with pathology and progression of parkinsonism in aging. JAMA neurology 2021, 78, 1494–1502. [Google Scholar] [CrossRef]
- Visser, A.E.; de Vries, N.M.; Richard, E.; Bloem, B.R. Tackling vascular risk factors as a possible disease modifying intervention in Parkinson’s disease. npj Parkinson's Disease 2024, 10, 50. [Google Scholar] [CrossRef]
- Camerino, I.; Ferreira, J.; Vonk, J.M.; Kessels, R.P.; de Leeuw, F.-E.; Roelofs, A.; Copland, D.; Piai, V. Systematic review and meta-analyses of word production abilities in dysfunction of the basal ganglia: Stroke, small vessel disease, Parkinson’s disease, and Huntington’s disease. Neuropsychology Review 2024, 34, 1–26. [Google Scholar] [CrossRef]
- Al-Bachari, S.; Naish, J.H.; Parker, G.J.; Emsley, H.C.; Parkes, L.M. Blood–brain barrier leakage is increased in Parkinson’s disease. Frontiers in physiology 2020, 11, 593026. [Google Scholar] [CrossRef]
- Miyazaki, I.; Asanuma, M. Neuron-astrocyte interactions in Parkinson’s disease. Cells 2020, 9, 2623. [Google Scholar] [CrossRef] [PubMed]
- Paolini Paoletti, F.; Simoni, S.; Parnetti, L.; Gaetani, L. The contribution of small vessel disease to neurodegeneration: focus on Alzheimer’s disease, Parkinson’s disease and multiple sclerosis. International journal of molecular sciences 2021, 22, 4958. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.L.; Ahn, J.H.; Chang, W.H.; Jung, W.; Kim, B.S.; Han, K.; Youn, J.; Shin, D.W. Risk of Parkinson disease in stroke patients: A nationwide cohort study in South Korea. European Journal of Neurology 2024, e16194. [Google Scholar] [CrossRef]
- Al-Kuraishy, H.M.; Jabir, M.S.; Al-Gareeb, A.I.; Albuhadily, A.K. New insight on the possible role of statins in Vascular Parkinsonism: A need for presumptive therapy. Ageing Research Reviews 2024, 102209. [Google Scholar] [CrossRef]
- Eisenmenger, L.B.; Peret, A.; Famakin, B.M.; Spahic, A.; Roberts, G.S.; Bockholt, J.H.; Johnson, K.M.; Paulsen, J.S. Vascular contributions to Alzheimer's disease. Translational Research 2023, 254, 41–53. [Google Scholar] [CrossRef] [PubMed]
- Twait, E.L.; Gerritsen, L.; Moonen, J.E.; Verberk, I.M.; Teunissen, C.E.; Visser, P.J.; van der Flier, W.M.; Geerlings, M.I.; UCC SMART Study Group, t.N.C. Plasma Markers of Alzheimer's Disease Pathology, Neuronal Injury, and Astrocytic Activation and MRI Load of Vascular Pathology and Neurodegeneration: The SMART-MR Study. Journal of the American Heart Association 2024, e032134. [Google Scholar] [CrossRef]
- Lei, T.; Yang, Z.; Li, H.; Qin, M.; Gao, H. Interactions between nanoparticles and pathological changes of vascular in Alzheimer’s disease. Advanced Drug Delivery Reviews 2024, 115219. [Google Scholar] [CrossRef]
- Toribio-Fernandez, R.; Ceron, C.; Tristão-Pereira, C.; Fernandez-Nueda, I.; Perez-Castillo, A.; Fernandez-Ferro, J.; Moro, M.A.; Ibañez, B.; Fuster, V.; Cortes-Canteli, M. Oral anticoagulants: A plausible new treatment for Alzheimer's disease? British Journal of Pharmacology 2024, 181, 760–776. [Google Scholar] [CrossRef]
- Tu, M.-C.; Huang, S.-M.; Hsu, Y.-H.; Yang, J.-J.; Lin, C.-Y.; Kuo, L.-W. Joint diffusional kurtosis magnetic resonance imaging analysis of white matter and the thalamus to identify subcortical ischemic vascular disease. Scientific Reports 2024, 14, 2570. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Xing, H.; Zhang, Z. Microvascular Perfusion Imaging in Alzheimer's Disease. Journal of Integrative Neuroscience 2024, 23, 70. [Google Scholar] [CrossRef] [PubMed]
- Battaglia, S.; Avenanti, A.; Vécsei, L.; Tanaka, M. Neural correlates and molecular mechanisms of memory and learning. MDPI: 2024; Vol. 25, p 2724.
- Liloia, D.; Zamfira, D.A.; Tanaka, M.; Manuello, J.; Crocetta, A.; Keller, R.; Cozzolino, M.; Duca, S.; Cauda, F.; Costa, T. Disentangling the role of gray matter volume and concentration in autism spectrum disorder: A meta-analytic investigation of 25 years of voxel-based morphometry research. Neuroscience & Biobehavioral Reviews.
- Martos, D.; Lőrinczi, B.; Szatmári, I.; Vécsei, L.; Tanaka, M. The Impact of C-3 Side Chain Modifications on Kynurenic Acid: A Behavioral Analysis of Its Analogs in the Motor Domain. International journal of molecular sciences 2024, 25, 3394. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Szabó, Á.; Körtési, T.; Szok, D.; Tajti, J.; Vécsei, L. From CGRP to PACAP, VIP, and beyond: unraveling the next chapters in migraine treatment. Cells 2023, 12, 2649. [Google Scholar] [CrossRef]
- Tajti, J.; Szok, D.; Csáti, A.; Szabó, Á.; Tanaka, M.; Vécsei, L. Exploring Novel Therapeutic Targets in the Common Pathogenic Factors in Migraine and Neuropathic Pain. Int J Mol Sci 2023, 24. [Google Scholar] [CrossRef]
- Fornari Laurindo, L.; Aparecido Dias, J.; Cressoni Araujo, A.; Torres Pomini, K.; Machado Galhardi, C.; Rucco Penteado Detregiachi, C.; Santos de Argollo Haber, L.; Donizeti Roque, D.; Dib Bechara, M.; Vialogo Marques de Castro, M. Immunological dimensions of neuroinflammation and microglial activation: exploring innovative immunomodulatory approaches to mitigate neuroinflammatory progression. Frontiers in Immunology 2024, 14, 1305933. [Google Scholar] [CrossRef] [PubMed]
- Valotto Neto, L.J.; Reverete de Araujo, M.; Moretti Junior, R.C.; Mendes Machado, N.; Joshi, R.K.; dos Santos Buglio, D.; Barbalho Lamas, C.; Direito, R.; Fornari Laurindo, L.; Tanaka, M. Investigating the Neuroprotective and Cognitive-Enhancing Effects of Bacopa monnieri: A Systematic Review Focused on Inflammation, Oxidative Stress, Mitochondrial Dysfunction, and Apoptosis. Antioxidants 2024, 13, 393. [Google Scholar] [CrossRef] [PubMed]
- Kalick, L.S.; Khan, H.A.; Maung, E.; Baez, Y.; Atkinson, A.N.; Wallace, C.E.; Day, F.; Delgadillo, B.E.; Mondal, A.; Watanapokasin, R.J.P.r. Mangosteen for malignancy prevention and intervention: Current evidence, molecular mechanisms, and future perspectives. 2023, 188, 106630.
- Bosso, H.; Barbalho, S.M.; de Alvares Goulart, R.; Otoboni, A. Green coffee: economic relevance and a systematic review of the effects on human health. Critical reviews in food science and nutrition 2023, 63, 394–410. [Google Scholar] [CrossRef] [PubMed]
- Barbalho, S.M.; Araújo, A.C.; Penteado Detregiachi, C.R.; Buchaim, D.V.; Guiguer É, L. The Potential Role of Medicinal Plants in Bone Regeneration. Alternative therapies in health and medicine 2019, 25, 32–39. [Google Scholar]
- Barbalho, S.M.; Bosso, H.; Salzedas-Pescinini, L.M.; de Alvares Goulart, R. Green tea: A possibility in the therapeutic approach of inflammatory bowel diseases?: Green tea and inflammatory bowel diseases. Complementary therapies in medicine 2019, 43, 148–153. [Google Scholar] [CrossRef]
- Bássoli, R.; Audi, D.; Ramalho, B.; Audi, M.; Quesada, K.; Barbalho, S. The Effects of Curcumin on Neurodegenerative Diseases: A Systematic Review. Journal of Herbal Medicine 2023, 42, 100771. [Google Scholar] [CrossRef]
- Marton, L.T.; Barbalho, S.M.; Sloan, K.P.; Sloan, L.A.; Goulart, R.d.A.; Araújo, A.C.; Bechara, M.D. Curcumin, autoimmune and inflammatory diseases: going beyond conventional therapy–a systematic review. Critical Reviews in Food Science and Nutrition 2022, 62, 2140–2157. [Google Scholar] [CrossRef] [PubMed]
- Buglio, D.S.; Marton, L.T.; Laurindo, L.F.; Guiguer, E.L.; Araújo, A.C.; Buchaim, R.L.; Goulart, R.d.A.; Rubira, C.J.; Barbalho, S.M. The role of resveratrol in mild cognitive impairment and Alzheimer's disease: a systematic review. Journal of Medicinal Food 2022, 25, 797–806. [Google Scholar] [CrossRef] [PubMed]
- Laurindo, L.F.; Direito, R.; Bueno Otoboni, A.M.; Goulart, R.A.; Quesada, K.; Barbalho, S.M.J.F.R.I. Grape processing waste: effects on inflammatory bowel disease and colorectal cancer. 2024, 40, 336-369.
- Barbalho, S.M.; Bueno Ottoboni, A.M.M.; Fiorini, A.M.R.; Guiguer, E.L.; Nicolau, C.C.T.; Goulart, R.d.A.; Flato, U.A.P.J.C.r.i.f.s. ; nutrition. Grape juice or wine: which is the best option? 2020, 60, 3876–3889. [Google Scholar] [PubMed]
- Barbalho, S.; Direito, R.; Laurindo, L.; Marton, L.; Guiguer, E.; Goulart RdA, T.R.; Carvalho, A.; Flato, U.; Capelluppi Tofano, V. Ginkgo biloba in the aging process: A narrative review. Antioxidants, 11 (3), 525. 2022.
- Jászberényi, M.; Thurzó, B.; Bagosi, Z.; Vécsei, L.; Tanaka, M. The Orexin/Hypocretin System, the Peptidergic Regulator of Vigilance, Orchestrates Adaptation to Stress. Biomedicines 2024, 12, 448. [Google Scholar] [CrossRef]
- Tanaka, M.; Vécsei, L. A Decade of Dedication: Pioneering Perspectives on Neurological Diseases and Mental Illnesses. MDPI: 2024; Vol. 12, p 1083.
- Tanaka, M.; Battaglia, S.; Giménez-Llort, L.; Chen, C.; Hepsomali, P.; Avenanti, A.; Vécsei, L. Innovation at the intersection: emerging translational research in neurology and psychiatry. MDPI: 2024; Vol. 13, p 790.
- Tanaka, M.; Vécsei, L. From Lab to Life: Exploring Cutting-Edge Models for Neurological and Psychiatric Disorders. Biomedicines 2024, 12, 613. [Google Scholar] [CrossRef] [PubMed]
- Battaglia, S.; Avenanti, A.; Vécsei, L.; Tanaka, M. Neurodegeneration in cognitive impairment and mood disorders for experimental, clinical and translational neuropsychiatry. MDPI: 2024; Vol. 12, p 574.
- Battaglia, S.; Schmidt, A.; Hassel, S.; Tanaka, M. Case reports in neuroimaging and stimulation. Frontiers Media SA: 2023; Vol. 14, p 1264669.
- Tanaka, M.; Diano, M.; Battaglia, S. Editorial: Insights into structural and functional organization of the brain: evidence from neuroimaging and non-invasive brain stimulation techniques. Front Psychiatry 2023, 14, 1225755. [Google Scholar] [CrossRef]
- Tanaka, M.; Szabó, Á.; Vécsei, L. Preclinical modeling in depression and anxiety: Current challenges and future research directions. Adv Clin Exp Med 2023, 32, 505–509. [Google Scholar] [CrossRef]
Figure 1.
Vascular impairment and cognitive dysfunction: The vascular system serves numerous functions within the human body. When it is not functioning properly, it is associated with risk factors such as hypertension, aging, and diabetes. The vascular system possesses the capacity to expand the perivascular spaces, promote microhemorrhage and atrophy, and facilitate subcortical infarctions. In this specific scenario, especially within the brain, the blood-brain barrier may undergo a decline in functionality and be impacted by disorders in the endothelial cells, as well as the presence of defensive substances such as fibrinogen, thrombin, and immunoglobulin. The outcome is a heightened susceptibility to the occurrence of stroke, cognitive decline, dementia, Alzheimer's disease (AD), and Parkinson's disease (PD).
Figure 1.
Vascular impairment and cognitive dysfunction: The vascular system serves numerous functions within the human body. When it is not functioning properly, it is associated with risk factors such as hypertension, aging, and diabetes. The vascular system possesses the capacity to expand the perivascular spaces, promote microhemorrhage and atrophy, and facilitate subcortical infarctions. In this specific scenario, especially within the brain, the blood-brain barrier may undergo a decline in functionality and be impacted by disorders in the endothelial cells, as well as the presence of defensive substances such as fibrinogen, thrombin, and immunoglobulin. The outcome is a heightened susceptibility to the occurrence of stroke, cognitive decline, dementia, Alzheimer's disease (AD), and Parkinson's disease (PD).
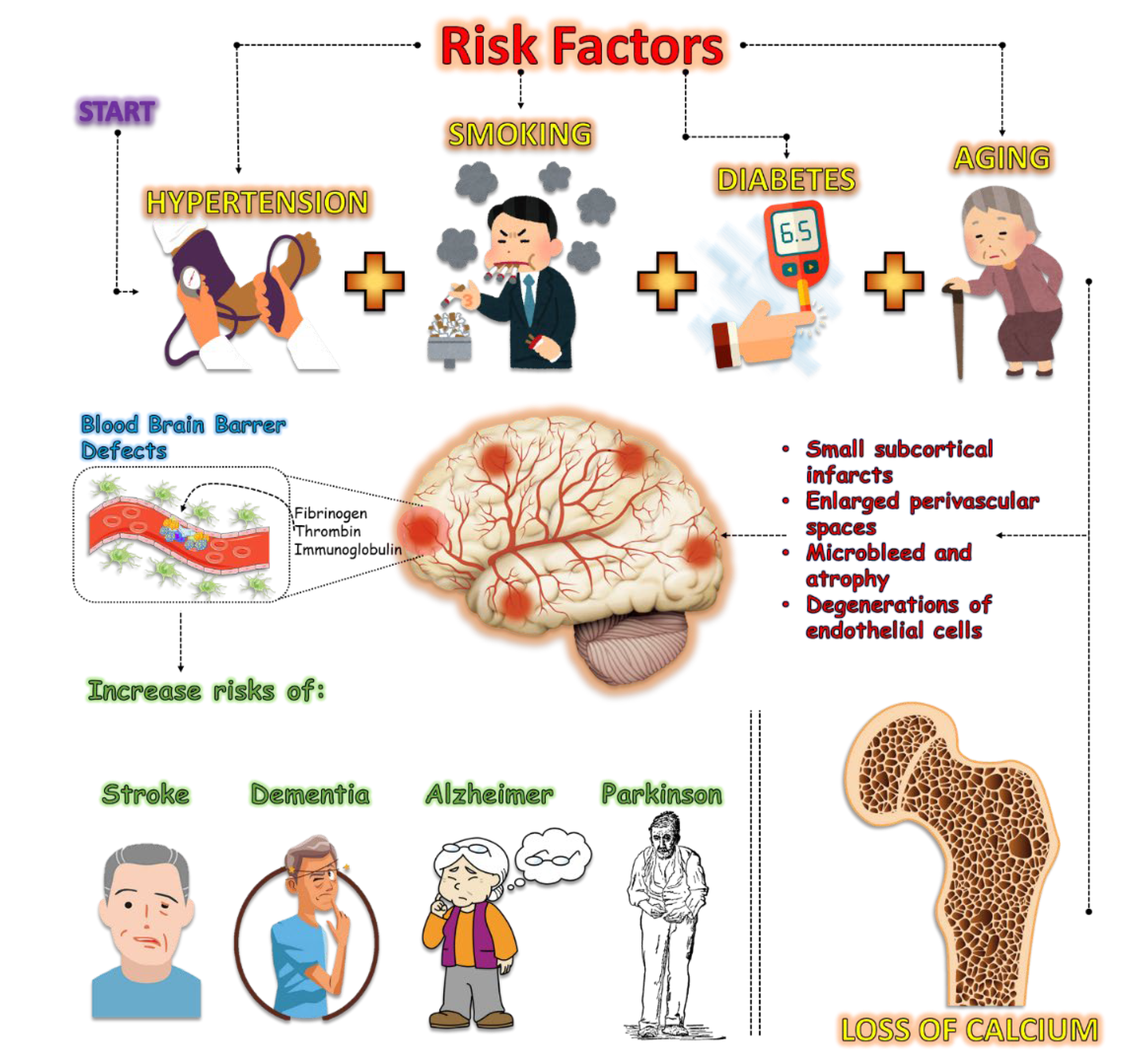
Figure 2.
Vascular problems and Neurodegeneration resulting in Sarcopenia: Vascular disorders can lead to reduced nutrition and minimal oxygen supply to cells. In this context, reactive oxygen species (ROS) are formed due to energy problems in the cell, forming pro-inflammatory cytokines such as Interleukin-6 (IL-6), Interleukin-8 (IL-8), Tumor-alpha Necrosis Factor (TNF-α) and Transforming-beta Growth Factor (TGF-β). In addition, excess interleukin-29 (IL-29) exocytosis worsens vascular problems by activation of Janus kinase 2 (JAK2) and Signal Transducer and Activation of transcription signal 3 (STAT3). This scenario, associated with impaired muscle synapses, may result in sarcopenia, quality of life and usual activities, and increasing mortality.
Figure 2.
Vascular problems and Neurodegeneration resulting in Sarcopenia: Vascular disorders can lead to reduced nutrition and minimal oxygen supply to cells. In this context, reactive oxygen species (ROS) are formed due to energy problems in the cell, forming pro-inflammatory cytokines such as Interleukin-6 (IL-6), Interleukin-8 (IL-8), Tumor-alpha Necrosis Factor (TNF-α) and Transforming-beta Growth Factor (TGF-β). In addition, excess interleukin-29 (IL-29) exocytosis worsens vascular problems by activation of Janus kinase 2 (JAK2) and Signal Transducer and Activation of transcription signal 3 (STAT3). This scenario, associated with impaired muscle synapses, may result in sarcopenia, quality of life and usual activities, and increasing mortality.
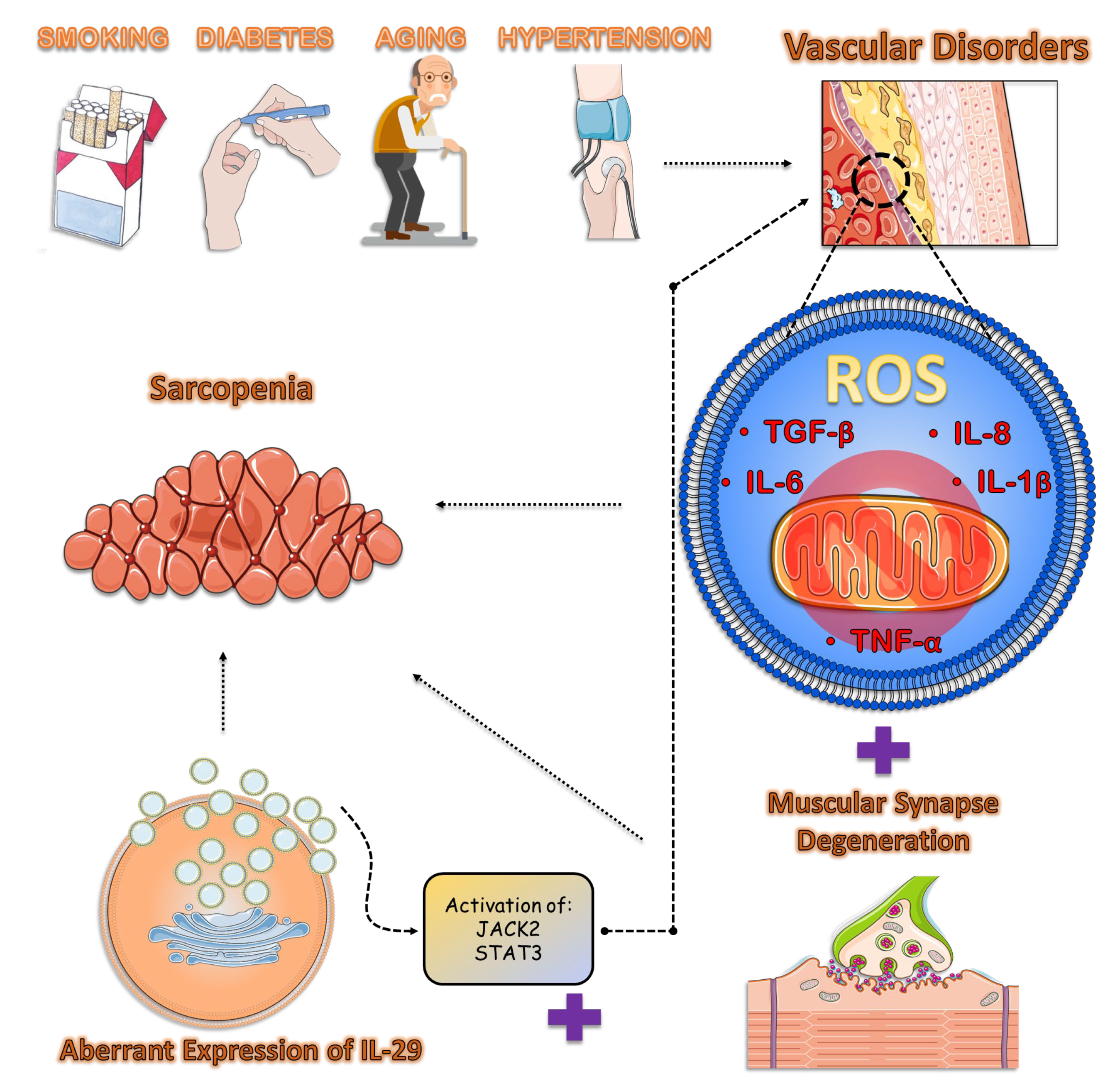
Figure 3.
Vascular problems, Neurodegeneration, and Sarcopenia: There are multiple associations between the denervation of muscle fibers, vascular disease, and sarcopenia. First, the denervation of muscle fibers impairs synapses in the muscle, decreasing neuromotor sensitivity. Through this innervation loss, oxygen species occur in the cell, which can cause mitochondrial dysfunctions, impairing the energy supply to the muscle fibers. In addition, cell dysfunction can promote aberrant expression of the MFG-E8 cell membrane protein, increasing problems of neuromuscular junctions, mitochondrial dysfunction, and problems in the vascular system. Finally, vascular problems can promote PD by reducing nutrients from the formation of substantia nigra and α-Sinucleine, and AD by reducing nutrients for the formation of Aβ protein.
Figure 3.
Vascular problems, Neurodegeneration, and Sarcopenia: There are multiple associations between the denervation of muscle fibers, vascular disease, and sarcopenia. First, the denervation of muscle fibers impairs synapses in the muscle, decreasing neuromotor sensitivity. Through this innervation loss, oxygen species occur in the cell, which can cause mitochondrial dysfunctions, impairing the energy supply to the muscle fibers. In addition, cell dysfunction can promote aberrant expression of the MFG-E8 cell membrane protein, increasing problems of neuromuscular junctions, mitochondrial dysfunction, and problems in the vascular system. Finally, vascular problems can promote PD by reducing nutrients from the formation of substantia nigra and α-Sinucleine, and AD by reducing nutrients for the formation of Aβ protein.
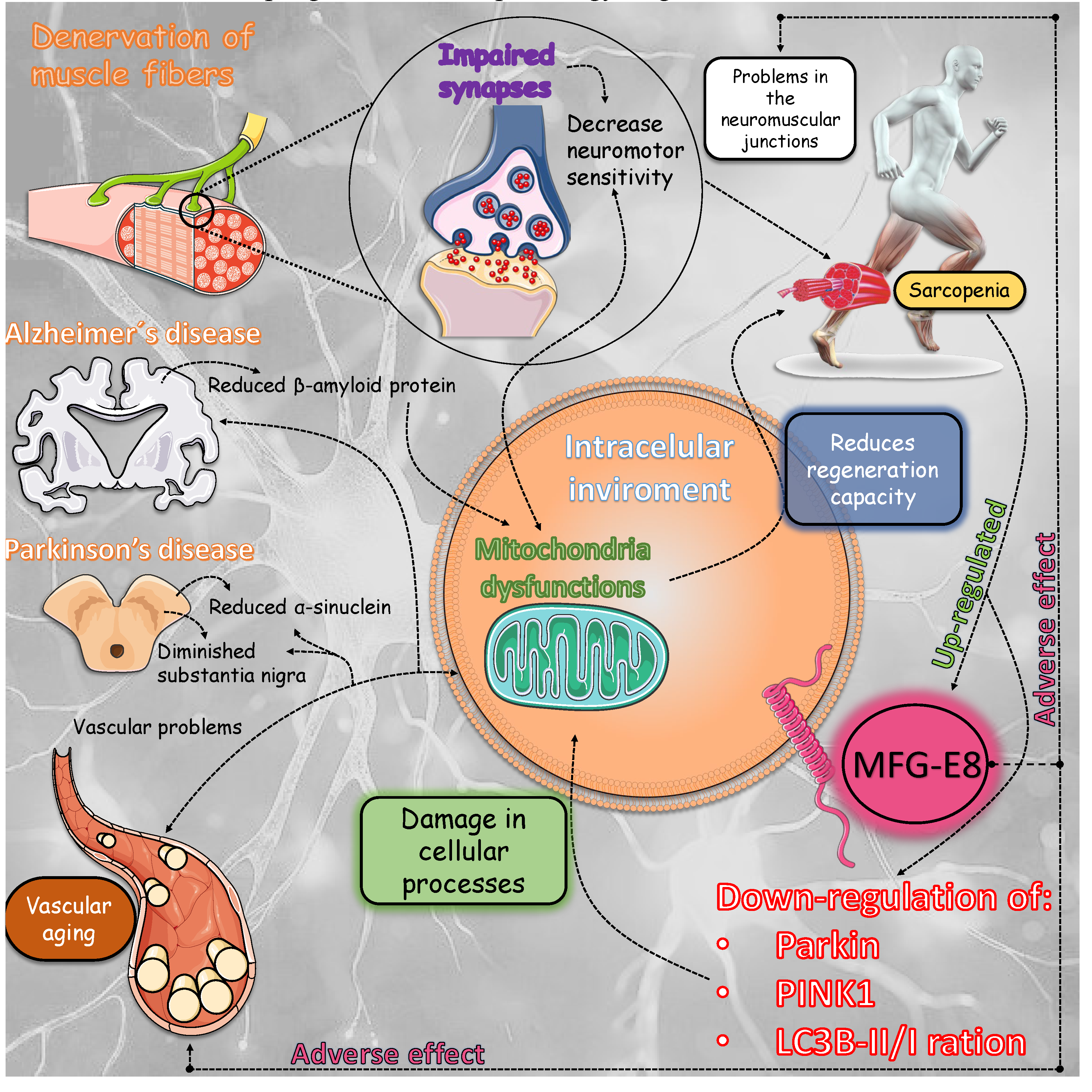
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



