
Submitted:
30 July 2024
Posted:
31 July 2024
You are already at the latest version
Abstract
Cannabidiol (CBD), a non-psychotropic main component of the Cannabis plant, is approved as a drug in the European Union (EU) under the name “Epidyolex”. However, the approval process as a food ingredient under the Novel Food Regulation was paused by the European Food Safety Authority (EFSA) due to a lack of safety data. Nevertheless, there is a growing, unregulated market in which CBD is advertised with various health claims and different dosage instructions. Of particular concern is its toxic effect on the liver and possible reproductive toxicity in humans. Studies suitable for calculating a benchmark dose were identified from the available data. Animal studies yielded a Benchmark Dose Lower Confidence Limit (BMDL) of 43 mg/kg bw/day, which translates into a safe human dose of approximately 15 mg/day. Only a Lowest Observed Adverse Effect Level (LOAEL) of 4.3 mg/kg bw/day could be identified from the human data. This updated risk assessment confirmed the Health-based Guidance Value (HBGV) of 10 mg/day based on human LOAEL. Despite existing data gaps, preliminary regulation appears advisable as the current form of the gray CBD market is unacceptable from the standpoint of consumer safety and protection.
Keywords:
cannabidiol
; novel food
; health-based guidance value
; benchmark dose
; risk assessment
1. Introduction
Cannabidiol (CBD) (Figure 1) is one of the main components of the Cannabis plant (Figure 2) alongside tetrahydrocannabinol (THC). Unlike THC, CBD has no psychotropic effect, but products are claimed to have various nutritional and health benefits.
Due to its strong lipophilic character, CBD has a low oral bioavailability [1]. When dissolved in fat or together with a high-fat meal, bioavailability can be significantly increased [1,2]. In addition, chronic consumption can cause the substance to accumulate in fatty tissue and thus lead to long exposure windows [1,3].
As a multi-target drug, CBD interacts with various receptors throughout the body. In addition to the cannabinoid receptors CB1 and CB2, the substance also acts on receptors of various ligand-gated ion channels (e.g. glycine and GABA receptors such as GABAA) as well as agonistically on the PPARγ receptors and TRPV receptors such as TRPV1, and has a modulating effect on various G-protein-coupled receptors (e.g. adenosine and serotonin receptors, GPR55) [4]. Through its modulating effect on GABAergic neurotransmission, for example, it can affect the excitability of the central nervous system even in people with defective GABAA receptors, making it an interesting candidate for the treatment of neurological disorders [5].
CBD is subject to high first-pass metabolism (Figure 2) by CYP450 enzymes (especially CYP2C19, CYP3A4) and UGT enzymes (UGT1A9, UGT2B7) [2]. Of the large number of metabolites, the main ones are 7-hydroxy cannabidiol (7-OH-CBD), 7-carboxy cannabidiol (7-COOH-CBD), 6-hydroxy cannabidiol (6-OH-CBD) and 4-hydroxy cannabidiol (4-OH-CBD), with 7-OH-CBD being the primary active metabolite [6,7] with a pharmacological activity similar to that of CBD [8]. The conversion of CBD to 7-OH-CBD is mainly catalyzed by CYP2C19 [6,7,8], although CYP2C9 is also thought to play a role [6,8]. The ratio of concentrations of CBD and 7-OH-CBD shifts towards CBD with prolonged use of CBD [2,9]. The active metabolite is further oxidized to the inactive 7-COOH-CBD by CYP2C19, CYP2D6 [6] and CYP3A4 [6,8]. CBD is also converted by CYP2C19 and CYP3A4 to the minor metabolites 6-OH-CBD and 4-OH-CBD [7]. Levels of 7-COOH-CBD increase after several weeks of CBD use and can still be detected in plasma several weeks after the last dose of CBD [9]. In women, the concentration of 7-COOH-CBD is higher than in men, which may be due to the higher proportion of fat tissue in women [8,9]. There appears to be little difference between the different metabolic phenotypes [2,9]. This may be partly due to the fact that CBD and its metabolites reversibly inhibit CYP enzymes. CBD can inhibit CYP2C19 and CYP3A isoforms and 7-OH-CBD can inhibit CYP2C9 and CYP2D6 [10].The effects of the metabolites are not yet fully understood and are still being studied.
Under the trade name “Epidyolex” in the EU and “Epidiolex” in the USA, a prescription CBD medicinal product has been approved as an orphan drug for the treatment of rare epilepsy syndromes, namely Lennox-Gastaut syndrome and Dravet syndrome, in children aged two years and older. Subsequently, another indication was added for the treatment of tuberous sclerosis [2].
In contrast to the well-defined legal framework for medicinal products, the regulatory landscape for CBD as a food supplement in the EU is markedly different. Since the consumption of CBD as a pure substance or in the form of CBD-rich hemp extracts has not been proven before 15 May 1997, the substance is categorized as novel in the European Commission's Novel Food Catalogue [11] and requires pre-market approval under the Novel Food Regulation (Regulation (EU) 2015/2283) [12]. In the European Food Safety Authority (EFSA) statement from 2022, various data gaps were identified, which is why authorization has not yet been granted [13]. Supplements containing CBD are therefore not legal marketable in the EU. In the United States, CBD from industrial hemp with a maximum THC content of 0.3% was legalized at the federal level by the Agriculture Improvement Act of 2018 (also known as the Farm Bill). The FDA (Food and Drug Administration), on the other hand, has only approved one CBD product, the drug Epidiolex. According to the FDA, the use of CBD in food and dietary supplements is illegal because it is a pharmacologically active ingredient in the approved drug Epidiolex, and as such is excluded from being a dietary supplement [14].
Of particular concern when it comes to foods containing CBD is the liver toxicity at higher doses [15] and possible reprotoxic effects [16,17]. In contrast to pharmaceuticals, there is no compromise between efficacy and the potential for adverse effects in the context of foods. Foods must not be injurious to health [18].
Despite these restrictions, the European and American markets are flooded with CBD products. These are most commonly offered in the form of oils, but also as capsules, gummy bears, or in chocolates. The aim of the study was an update of the risk assessment of CBD in the light of new study results published since the authors last evaluation in 2023 [19].
2. Materials and Methods
Since this paper is about CBD as a food, this research was limited to orally administered CBD alone. To focus on the effects of CBD, studies where CBD was taken with THC or other co-medications were excluded.
2.1. Market and Consumers
To gain a comprehensive understanding of the current state of the CBD market with principal focus on the European and American markets, a search was conducted on PubMed and Google Scholar using the terms “cannabidiol” and keywords such as “market”, “advertising”, and “label accuracy”. In order to understand the motivation of consumers, a search was conducted for surveys that provided relevant information about the reason for consumption and the use of cannabidiol. Relevant articles were searched for citations from which further information was obtained. To get an impression of the amount of CBD consumed, a search for “CBD dosage” was made on Google on 2 December 2023 and the various websites for recommended dosages were reviewed.
2.2. Risks
To gain insight into the toxicity of CBD, a search was conducted on PubMed and Google Scholar for the terms “cannabidiol safety” and “cannabidiol toxicity”. Meta-reviews and the most recent findings were given particular attention, with a focus on liver toxicity and reproductive toxicity.
2.3. Health-Based-Guidance-Value (HBGV)
In order to support a regulatory evaluation of CBD as a novel food, a Health-Based Guidance Value (HBGV) for CBD was calculated based on the results of the most recent studies not included in [19]. To achieve this, it is necessary to identify a Benchmark Dose or a No-Observed-Adverse-Effect Level (NOAEL) as a suitable reference point (RP). If this is not possible, a Lowest-Observed-Adverse-Effect Level (LOAEL) may be used as an alternative. The EFSA recommends, if possible, to use the Benchmark Dose approach instead of the NOAEL approach as RP for risk assessments [20].
For a BMD to be calculated from existing studies, the following criteria must be met [21]: the observed effects must be stated as mean values with associated deviation, the measured biological effect must be in a dose-response relationship to the substance used and the number of animals tested per group should also be stated. In addition to the control group, at least three different dose groups, expressed in mg/kg bw/day, should have been tested without concomitant medication or THC.
The benchmark dose approach was based on the US Environmental Protection Agency (EPA) Benchmark Dose online tool and its Technical Guidance Manual [22]. The default settings of the program with a confidence level of 0.95 were used. The online tool calculated various statistical models and indicated whether these models were viable. The most appropriate model was selected based on the lowest Akaike information criterion (AIC). This is a method for comparing different models. The lowest AIC value means that the amount of information lost in this model is lower than in the other models, and therefore it is the most informative model.
To identify suitable human studies, "Clinical Trial" and "Randomized Controlled Trial" as the article type was selected in PubMed (as of 22/05/2024) and a search for the term "cannabidiol safety" was conducted. A total of 121 results were obtained, and studies that did not match the specified criteria were discarded. Seven studies had to be excluded because CBD was only used topically. In 43 of the discarded studies, other concomitant cannabinoids, mainly THC, were tested in addition to CBD. Another six studies included concomitant medications. 51 studies were not eligible because there were no adequate dose groups and often only one or two different doses were tested. In addition, four further studies lacked a comparison with a placebo and could also not be used. One study was duplicated and one study each was eliminated for the reasons that it was only a study design, a study on a cell-based model or had nothing to do with CBD. Two studies were eliminated because they were reviews.
Four studies remained in the end [23,24,25,26]. Three of the studies [23,24,25] were single-dose studies without dosage by weight (mg/day instead of mg/kg bw/day). However, no serious adverse effects were found in these studies. The final study [26] was conducted on children aged 4-10 years and adverse effects were not clearly related to dose-response. It is regrettable that a BMD cannot yet be calculated on the basis of human studies. For the time being, the NOAEL approach must therefore be used. The NOAEL or LOAEL for liver toxicity in humans was derived from a meta-study and the HBGV was calculated using the uncertainty factors (UF) recommended by EFSA [27]. In order to calculate a BMD for the liver toxicity in animals, a search of PubMed and Google Scholar was conducted for animal studies that met the aforementioned criteria.
3. Results
3.1. Market and Consumers
Cannabidiol is becoming increasingly popular and the market is growing, with sales in Europe predicted to reach 3.47 billion EUR by 2024 [28].
Various surveys from Germany [29], UK and Ireland [30], and the USA [31,32] and Canada [32] have looked at the number of users, reasons for use and public perception of CBD. CBD appears to be most popular in the USA, where 26% of respondents [32] stated that they had used CBD, compared to 11% in Germany [29]. However, there is also some time in between the studies (2022 USA, 2020 Germany), and the number of consumers in Germany may have increased in the meantime. The most prevalent method of oral administration of CBD is in the form of oils, tinctures, and edibles [29,31,33], and the internet, including social media, seems to be a popular source of information [31,34,35].
One study searched the social media platform Twitter (now X.com) for information on CBD and came across many health-related statements [36]. If cannabidiol is marketed as a food in the EU, the substance is subject to the Health Claims Regulation (EC) No. 1924/2006, which prohibits such claims for food and food supplements.
Another study examined the use of CBD on Pinterest, a social media platform with a visual search engine [37]. CBD is mostly presented positively here, health-related statements are also made and almost none of the so-called pins contain information on any adverse effects. Many of them link to CBD online stores, followed by personal blog posts or other social media. Only around 1% link to medical websites or pharmaceutical companies. This discrepancy between the high volume of information generated by CBD retailers and the lack of evidence-based information on this social media platform is also reflected in surveys on the perception and risk assessment of the population. Over 50% of respondents rated CBD as a low-risk substance [29] that is “good” or “very good” for health [29,32], and many respondents also saw no problem in taking CBD together with prescription drugs [31]. Moreover, efficacy claims are frequently based on personal experience reports [31,37], rather than medical evidence.
Most commonly, consumers appear to use CBD to relieve pain [29,30,31,32,35,38] and to improve sleep [29,31,32,33,38] or mental health. The latter refers on the one hand to a stress-reducing [29,33,38] and relaxing effect of CBD [29,33], on the other hand it also refers to serious psychological problems such as depression [31,32,35] and anxiety [30,31,32,38]. Sometimes the prescribed medication is reduced or omitted in favor of CBD [31,38].
In addition to the illegality of health claims, the unregulated market presents another challenge. A significant number of studies have demonstrated that the CBD concentration in the product frequently does not align with the information displayed on the label [39,40,41,42]. In the best-case scenario, overlabeling may mislead consumers; in the worst case, underlabeling can result in overdosing and the development of adverse effects. One study [39] found that underlabeling occurred mainly with high-dose CBD oils. Drinks were more likely to be affected by underlabeling, in some cases only traces of the substance below the limit of quantification were detected, possibly due to the poor water solubility of the substance. One study from Germany [43] looked at 22 CBD oils and 4 oils of other phytocannabinoids. The actual concentration of cannabinoids was on average 21% higher than what was claimed on the packaging. In 7 samples, even 2 drops of oil contained a higher concentration of THC than the EFSA's acute reference dose of 1 µg/kg body weight.
Since many people obtain their information from the Internet, dosing information recommended on the web is summarized in Table 1.
Of the 26 first search hits, 24 were online stores for CBD, one was the website of a newspaper and one was the website of a job exchange for doctors. Here the wide range of dosages is of note, which are often divided into low, medium and high doses. Here too, prohibited health claims can be found for specific doses. There is also frequent advice to increase the dosage slowly, starting with a low dose, until the desired effect is achieved. However, there is currently no proof of efficacy for CBD in many indications. Consequently, there is a risk that in the case of diseases for which CBD has insufficient efficacy, consumers will continue to increase their doses in the hope of achieving a positive effect at some point.
The studies by Kaufmann et al. provide insight into the dosages actually used by long-term consumers, as all participants had already consumed CBD for at least 30 days (most often more than 12 months) before the start of the study and were able to determine their own dosage and dosage form freely. The average dosage in the studies was just over 50 mg with standard deviation (SD) of approximately 40 mg [38,44,45], with a range of 8-390 mg/day [38,44] and 2.5-390 mg/day [22] respectively.
3.2. Health Risks
This section examines the potential health risks associated with the consumption of CBD, with a particular focus on its use as a dietary supplement or in food products. Adverse effects of the prescription drug Epidiolex (dose range 10-25 mg/kg bw/day) include gastrointestinal discomfort, infections, loss of appetite, drowsiness and lethargy, seizure, cough, elevated liver enzymes and rash [2].
In vitro and in vivo studies show a positive influence of CBD on various liver diseases, as it probably protects the liver from oxidative stress and probably has an effect on lipid metabolism and cell apoptosis of the liver [46]. This positive influence has not yet been confirmed in clinical studies on humans, where CBD was found to increase liver enzymes. This is of particular concern when consuming CBD as a dietary supplement, as these changes in blood parameters, unlike the other adverse effects, may not be noticed by the consumer for a long time unless blood is regularly tested by a doctor.
The liver toxicity of CBD was investigated in a meta-analysis by Lo et al. [15]. CBD can increase liver values up to a drug-induced liver injury (DILI), whereby the CBD-associated DILI is comparable to other liver-toxic compounds such as statins and fluoroquinolones, and it occurred in both children and adults, including healthy adults. DILI was not studied at doses below 300 mg/day. The association of increased liver enzymes and DILI is specifically significant at CBD doses of >1000 mg/day or ≥20 mg/kg bw/day and concomitant use of valproic acid, a drug from the anticonvulsant group, which is also used for treating epilepsy. In most cases, the increase in liver enzymes is reversible after discontinuation of CBD, sometimes the values even normalize spontaneously despite maintaining the therapy [15].
Two studies by Kaufmann et al. examined the impact of long-term oral consumption of CBD on liver health. The studies excluded people with known liver disease, liver dysfunction, CBD allergy and people taking certain medications, supplements or foods known to affect the liver. 1475 people enrolled, of which 839 [45] or 1061 [44] people completed the study. As already mentioned in section 3.1, the study participants were able to choose the dose and dosage form themselves and the daily dose ranged from 2.5 mg to 390 mg [44,45]. It is noticeable that the smallest amounts were taken by people who used nano-formulations, the largest by people who chose CBD as an additive or as a capsule/pill dosage form. In both studies, almost 10% of the study participants showed an increase in the liver enzyme aspartate transaminase (ALT) in the final blood test and around 4% showed an increase in the liver enzyme alanine transaminase (AST). Elevated ALT > 3x upper limit of normal (ULN) occurred in 3 [45] and 4 [44] individuals, respectively, and were associated with underlying diseases. The authors state that there was no connection between the selected dose and the ALT elevation rather than demographic, physical and medical conditions. These results were compared with the incidence of elevated liver enzymes in the general population measured by the National Health and Nutrition Examination Survey (NHANES) from 1999-2002, and because of similar values, Kaufmann et al. claimed that CBD was not harmful to the liver at these doses. Given the absence of comparison groups and the unavailability of blood values prior to long-term CBD consumption, the authors believe that it is not currently possible to make a definitive statement regarding the impact of CBD on the test subjects' livers. A comparison with the general population is not tenable due to the exclusion criteria from the study and the time difference of at least 10 years. Furthermore, it is not entirely clear why 222 more subjects were included in one study. Caputi also criticized the study design [47]: On the one hand, observational studies may be inadequate to address the issue at hand; on the other hand, the majority of the study participants are women, who are less prone to liver problems. Furthermore, only subjects who had already consumed CBD over a longer period of time were admitted to the study, which meant that individuals who did not tolerate the substance well were excluded from the outset.
It is assumed that cannabidiol has a toxic effect on reproduction in animals, but comprehensive studies on humans are lacking. A review by Carvalho et al. [16] deals with the effect of CBD, which has an impact on the reproductive system of male animals both at the genetic level and through enzyme induction and competition with other substrates for certain enzymes. Receptors and enzymes of the endocannabinoid system are thought to play a role in the hypothalamic-pituitary-gonadal axis and thus influence the production of sex hormones. Studies both in vivo and in vitro have shown that CBD can have a stimulating or inhibitory effect on CYP enzymes (such as inhibition of CYP3A4 which is responsible for the metabolism of testosterone [6]) that control the breakdown of sex steroids. A biphasic effect of CBD has been shown in rodents: at low doses it indirectly increases the concentration of endocannabinoids, which have an inhibitory effect on copulation, while at high doses it can have a stimulatory effect on sexual behavior by blocking endocannabinoid enzymes and activating TRPV1 receptors. The substance presumably has an influence on testosterone and androgen concentrations, as well as a gonadotoxic effect on spermatogenesis. CBD consumption by the mother shortly before birth can induce long-term changes in the reproductive endocrine functions of the male offspring in rodents. Unfortunately, due to the study designs of the animal experiments, no statement on the reversibility of the dysregulation of the reproductive system is possible.
A study by Sarrafpour et al. [48] investigated the use of CBD during pregnancy in humans. The use of CBD for morning sickness seems to be popular. The problem with this is the poor study situation. The high lipophilicity of CBD, which makes the substance potentially placental, could be problematic. The cannabinoid system plays a role in all stages of pregnancy, from conception to birth, so effects on the newborn and the pregnant woman cannot be ruled out. It also has an anti-angiogenic effect on the endothelial cells of the human umbilical vein and can therefore lead to pregnancy complications. CBD's ability to modulate the immune system by influencing cytokine levels and apoptosis could also be a cause for concern. This could interfere with the development of the fetus' immune system. Studies in an ex vivo model [49,50] have also shown that CBD can alter the function of two efflux transporters: the breast cancer resistance protein (BCRP) and the P-glycoprotein (P-gp), which can be inhibited by CBD and thus make the placental barrier more permeable to xenobiotics, which can ultimately harm the fetus.
3.3. Health-Based-Guidance-Value (HBGV)
The results of the benchmark dose modeling are presented in Table 2. The BMDL of 43 mg/kg per day was the most appropriate and was therefore chosen as a reference point (RP). In order to calculate an HBGV using the BMDL of the animal studies as RP, it is necessary to apply an interspecies default factor of 10 and a human intraspecies default factor of 10 in order to extrapolate from animal studies on rats to the effect on humans and to extrapolate the differences between each human. Furthermore, a default factor of 2 is used to extrapolate from subchronic to chronic consumption [51].
An HBGV of 0.21 mg/kg bw/day can be calculated from the animal study using the BMDL. This would correspond to a low-risk daily intake of approximately 15 mg (Table 3). However, as this value is not based on human studies, it is more conservative to use human studies to define an appropriate reference point for the HBGV, even if this precludes the use of a BMDL for the time being.
A LOAEL of 300 mg/day can be derived from the meta-study by Lo et al. [15]. This is the lowest dose tested in humans at which DILI occurred. This value was derived from a subacute 28-day study by Crippa et al. [55] on 59 healthy adults in which liver enzymes increased in four individuals at this dose (150 mg twice a day). The EFSA also confirms this value as LOAEL [13]. Consequently, when extrapolating from a LOAEL to a NOAEL, an additional UF must be included [27], which needs to be decided on a case-by-case basis as there is no standard value. Therefore, the UF of 3 used by the EFSA for THC, a structurally similar compound, was applied [56].
The EFSA is unable to provide default values for extrapolation from subacute studies to chronic intake. It should be noted that the human studies conducted over longer periods do not indicate the specific point in time at which the liver values of the test subjects were elevated. In most cases, however, the increases were detected in the fourth week [15]. Given these uncertainties and the evidence that these liver problems may be reversible by cessation of use, it is proposed that the extra UF may be excluded at this point. Instead, warnings might be placed on the package to limit daily consumption to two weeks without medical supervision.
The 300 mg dose can be converted to the kg body weight of a 70 kg individual, resulting in an approximate dose of 4.29 mg/kg bw/day. This results in a HBGV of 0.14 mg/kg bw/day (equivalent to approximately 10 mg per day) for a temporary use of 2 weeks (Table 3).
Previously, Lachenmeier et al. [19] have calculated a BMDL of 20 mg/kg bw/day based on a rat study, GWTX1412 [57], published by the FDA as part of the Epidiolex approval. This BMDL is judged to be of higher quality because the study included more animals per group, used purified CBD as the test compound, and was conducted over a longer period of 26 weeks. The endpoint used was centrilobular hypertrophy of the liver. The HBGV calculated by Lachenmeier et al. is close to the candidate HBGV calculated in this study at 0.20 mg/kg/day or 14 mg/day.
The results of the animal studies appear to indicate that a value of 10 mg/day may be the most appropriate for HBGV. This value was derived from human studies and represents the lowest dose, which is indicative of a favorable safety profile. Taking CBD above this HBGV is not recommended and may be associated with risks.
4. Discussion
Human studies are preferable to animal studies. Unfortunately, the use of a LOAEL entails considerable uncertainties. However, animal studies appear to support this value, as evidenced by the results from this study or by previous studies [19]. Based on an average daily consumption of 50 mg ± 40 mg [45], the majority of consumers exceed the HBGV of 10 mg. In one recent study of CBD products on the German market, an average of 2-7 drops of CBD oil per day was found to exceed the HBGV while the manufacturer's dosage recommendation was 1-20 drops per day [43]. Furthermore, doses above the LOAEL are sometimes suggested on the internet. In light of these findings, it is imperative that the risk management takes prompt action to regulate the market and protect consumers.
As mentioned above, Lachenmeier et al. [19] calculated an HBGV for CBD in food. They also derived the same HBGV from the study by Crippa et al. [55]. Their study also included the GWTX1412 [57] animal study mentioned above. However, no extra UF was used to extrapolate from subchronic to chronic study duration. If an UF of 2 was included, a more conservative limit of 0.10 mg/kg/day or 7 mg/day would be obtained. However, this value is also close to the HBGV calculated in this study.
Similarly, Henderson et al. [58] calculated an ADI (acceptable daily intake) for the general population using human studies. Also based on the study by Crippa et al. [55], a NOAEL of 300 mg/day was selected as the RP or, in this case, POD (point of departure). As this value is a LOAEL and not a NOAEL, the UF for extrapolation from LOAEL to NOAEL is consequently missing in the calculation. They only use a UF of 3 for inter-human variability. The rationale behind the deviation from the standard default value of 10 and the omission of the pharmacodynamic difference between individuals is unclear. Pharmacodynamics may vary due to differences in receptor density, hence the importance of gradual dose titration during therapy [1,59]. Pharmacokinetics may vary depending on genetics, weight, the time of administration (fasting or with food), the vehicle, and other factors [1]. They also have an upper intake level (UL) for the consumption of CBD only by healthy adults who do not want to have children and are not pregnant or breastfeeding. The NOAEL chosen was 1000 mg/day, as reported in the study by Lo et al. [15]. As this is the dosage that is strongly associated with an increase in liver values, this value is not suitable for a risk assessment of CBD in food and the resulting UL of 1.42 mg/kg/day is not safe.
The Swiss Federal Office for Food Safety and Veterinary Medicine (BLV) has issued a statement recommending that a daily oral dose of 12 mg should not be exceeded due to the liver damaging effects of CBD [60]. This value was derived from a human study published in a document from GW Pharmaceuticals, the pharmaceutical company that manufactures Epidiolex. This 2019 document [61] mentions that Epidiolex's approval studies showed DILI at 5 mg/kg/day. The BLV calculated the maximum daily dose of 12 mg using a UF of 10 for inter-human variability and 3 to reflect that effects occurred at the lowest dose tested. This is consistent with the HBGV of this study.
In the United Kingdom, the COT (Committee on Toxicity) of the FSA (Food Standards Agency) has initially set an upper daily intake of 70 mg CBD [62]. The CBD dose of ≤ 1 mg/kg was chosen for this value, as inhibitory interactions with some medications occurred at this dose. They then calculated this for a person with a standard weight of 70 kg. Based on new data, the COT more recently adjusted this value and set a provisional ADI of 0.15 mg/kg bw/day or 10 mg/day for a 70 kg person for pure CBD [63]. This value was calculated on the basis of three unpublished 90-day rodent studies submitted by the applicants for novel food authorization, but unfortunately not available to the public. The NOAEL (72, 50 and 25 mg/kg bw/day) was taken as the POD based on adverse effects on the liver from these three studies. Supported by the results of human studies, an average ADI of 10 mg/day was calculated from the ADIs (17, 12 and 5.6 mg per person) of these studies. All the recommended maximum daily doses that have been discussed are summarized in Table 4.
Although there are not many human studies in the low-dose range, the existing human studies [15,61] seem sufficient to assess the risk of CBD for liver effects, even at low doses, especially since the human data are supported by animal studies. However, much more research is needed to assess the potential risk of harm to fertility. The endocannabinoid system plays an important role in all stages of pregnancy, from conception to birth, so effects on the newborn and the pregnant woman cannot be ruled out. It should therefore not be taken during pregnancy and breastfeeding for safety reasons. Men who wish to have children should also consider whether they should take CBD. It would make sense to print the following warnings on CBD products to increase safety "For adults only", "CBD should not be used during pregnancy, breastfeeding or when planning to have children", "Do not exceed 10 mg per day for a maximum of 2 weeks at a time", and "If you have existing liver problems or are taking medication, you must consult a qualified healthcare professional before use".
Another challenge is bioavailability, which can vary considerably depending on the fasting state and vehicle. One study has demonstrated that the selection of a vehicle oil for CBD can influence its bioavailability, not to mention CBD as a nano-formulation [64]. A lot of research is currently underway in this area with the aim of increasing bioavailability. The introduction of new formulations into the market may necessitate a corresponding adjustment to the HBGV.
Another significant source of uncertainty is the presence of other cannabinoids in full-spectrum hemp extracts, which are frequently found alongside CBD. These have been the subject of even less research than CBD, making it currently impossible to assess their exact effects and adverse effects.
Food supplements are not medicinal products and therefore different risk assessments apply here. There is nothing wrong with the nutritional use of CBD to improve general well-being; anything beyond this is a prohibited health- or disease-related claim. The use of CBD for medical purposes should be reserved for CBD products that are approved as medicinal products. These can also be dosed higher than the HBGV after a precise risk-benefit assessment. It is now important to educate consumers with evidence-based information and to combat the huge amount of (sometimes false) information provided by those who make money from CBD marketing.
5. Conclusions
After a thorough evaluation of the latest study results on liver toxicity, animal and human studies seem to be consistent in their results, so that an HBGV of 10 mg/day for CBD in food seems justified. Due to possible reprotoxic effects, this value excludes pregnant and lactating women and people trying to conceive for safety reasons, who should be warned by safety information on the products. In addition, consumption for more than two weeks at a time should be avoided. Nevertheless, further studies in the low-dose range are necessary, especially on reproductive toxicity.
Supplementary Materials
The following supporting information can be downloaded at: www.mdpi.com/xxx/s1, MS Word files with reports generated by the BDMS software for the three studies as summarized in Table 2).
Author Contributions
Conceptualization, D.W.L.; validation, E.W.; formal analysis, E.W.; investigation, E.W.; resources, D.W.L. and H.F.; data curation, E.W.; writing—original draft preparation, E.W.; writing—review and editing, D.W.L., C.S., S.G.W. and H.F.; visualization, E.W.; supervision, D.W.L. and H.F.; project administration, D.W.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Publicly available datasets were analyzed in this article. New derivative data presented in this article are available in the Supplementary Materials.
Acknowledgments
This manuscript was published as part of the Postgraduate Study Program “Toxicology and Environmental Protection” at the University of Leipzig, Germany.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A

Table A1.
CBD online dosing recommendations.
| Website | Low dosage (micro dosage) |
Medium dosage (standard dosage) |
High dosage (macro dosage) |
Recommended dosage or Maximum dosage |
|---|---|---|---|---|
| Algeacare.com | - | - | - | 20-40 mg/day, increase by 5 mg every week until the desired effect is achieved |
| Hanfgeflüster.de | - | - | - | 20-50 mg, increase until the desired effect is achieved |
| Cbd-vital.de | 1-20 mg/day (stress, sleep problems, balance) |
10-100 mg/day (severe problems) |
50-800 mg/day (very severe problems) |
- |
| Canatura.com (page on dosage according to symptoms) | 0.2 mg/kg/day = 14 mg/day 2 (general health, nausea, migraine) |
0.6 mg/kg/day = 42 mg/day 2 (nausea, chronic pain, sleep disorder, anxiety, migraine) |
1.2 mg/kg/day = 84 mg/day 2 (chronic pain, sleep disorder, anxiety, epilepsy, cancer) |
10-150 mg/day, adjust dosage individually |
| Canatura.com (page on dosage according to body weight) |
14 mg/day 2 | 49 mg/day 2 | 91 mg/day 2 | - |
| Sueddeutsche.de | - | - | - | Start with 7.5 mg/day, slowly increase until the desired effect is achieved |
| Alpinols.de |
14 mg/day 2 | 49 mg/day 2 | 70 mg/day 2 | - |
| Cbd-deal24.de |
0.5-25 mg/day | 10-100 mg/day | 50-800 mg/day | - |
| Benetui.de | 14 mg/day 2 | 49 mg/day 2 | 91 mg/day 2 |
pain: 2.5-20 mg; anxiety/stress: 5-30 mg; sleep disorder: 40-160 mg; epilepsy: 200-300 mg |
| 321cbd.com | 0.25 mg/kg/day = 17.5 mg/day 2 (mild sleep disorders) |
0.5 mg/kg/day = 35 mg/day 2 (moderate sleep disorders) |
- | Usual dosage: 25 mg/day |
| Biobloom-cbd.de | - | - | - | Dosage according to individual comfort dose |
| Naturecan.de | - | - | - | Start with 20 mg/day, increase gradually |
| Praktischarzt.de | 0.5-20 mg/day (sleep disorder, stress, imbalance, malaise, nausea, mild pain, mild mental problems) |
20-100 mg/day (depression, arthritis, MS, medium pain, medium mental problems) |
400 mg/day (epilepsy, cancer, tumor, severe pain, severe mental problems) |
Start with 2-5 mg/day, individual increase according to well-being |
| Vaay.com | - | - | - | 20-100 mg/day, adjust dosage individually; start with 5 mg for 3 days, increase dosage to 10 mg for 3 days, continue with 15 mg |
| Cbd360.de | 2-20 mg/day (mild pain, mild stress, metabolic disorders, nausea, inflammation) Day 1-15: increase slowly from 0.02 mg/kg/day (= 1.4 mg/day 2) to 0.2 mg/kg/day (= 14 mg/day 2) |
20-80 mg/day (medium pain, medium stress, inflammation, autoimmune disease, anxiety disorder, lyme disease, depression, arthritis, MS, autism, weight loss) Day 16-30: If needed increase slowly from 0.3 mg/kg/day (=21 mg/day 2) to 1 mg/kg/day (=70 mg/day 2) |
80-800 mg/day (severe pain, epilepsy, cancer, liver problems) Day 31-45: If needed increase slowly from 1.5 mg/kg/day (= 105 mg/day 2) to 4 mg/kg/day (= 280 mg/day 2) |
- |
| Cbd-und-mehr.at | - | - | - | Start with low dosage and increase individually; first week: two drops of a 10% oil once a day; second week: two drops of a 10% oil twice a day; third week: two drops of a 15% oil three times a day |
| Marryjane.de | 14 mg/day 2 | 49 mg/day 2 | 91 mg/day 2 | pain: 2.5-20 mg/day anxiety: 33-49 mg/day intestinal diseases: 10 mg/day psychosis: 600 mg/day |
| Cbdwelt.de | - | - | - | ususal dosage: 20-100 mg/day Start low and increase slowly until the desired effect is achieved |
| Tomhemps.com | 1 mg/4.5 kg/day = 15.6 mg/day 2 |
3 mg/4.5 kg/day = 46.7 mg/day 2 | 6 mg/4.5 kg/day = 93.3 mg/day 2 | - |
| Cannalin.de | - | - | - | 70-100 mg, start with 5 mg and increase by 5mg every second day |
| Dutchnaturalhealing.com | - | - | - | 50-70 mg, start with 10-20mg |
| Cbdsfinest.de | 0.5-20 mg/day (headache, sleep disorders, mood swings, nausea, stress, metabolic disorder) |
10-100 mg/day (pain, inflammation, anxiety, depression, MS, IBS, arthritis, autism, fibromyalgia) |
50-800 mg/day (epilepsy, cancer, liver problems) |
- |
| Hanfgeflüster.de | - | - | - | 20-50 mg/day, individual adjustment every 2 weeks |
| Cannatrust.eu | 15 mg/day 2 | 45 mg/day 2 | 90 mg/day 2 | - |
| Magu-cbd.com | - | - | - | 20-40 mg/day |
| Pharma-hemp.com | - | - | - | Start with 0.5 mg/kg/day = 35 mg/day 2 |
1 Dosage recommendations online often refer to a low, medium and high dose range and slow dose adjustment is often recommended. Dosages are often mentioned with supposedly suitable indications. 2 Refers to a person weighing 70 kg.
References
- Lucas, C.J.; Galettis, P.; Schneider, J. The Pharmacokinetics and the Pharmacodynamics of Cannabinoids. Br. J. Clin. Pharmacol. 2018, 84, 2477–2482. [Google Scholar] [CrossRef] [PubMed]
- Epidyolex | European Medicines Agency. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/epidyolex (accessed on 2 April 2024).
- Millar, S.A.; Stone, N.L.; Yates, A.S.; O’Sullivan, S.E. A Systematic Review on the Pharmacokinetics of Cannabidiol in Humans. Front. Pharmacol. 2018, 9, 1365. [Google Scholar] [CrossRef]
- Castillo-Arellano, J.; Canseco-Alba, A.; Cutler, S.J.; León, F. The Polypharmacological Effects of Cannabidiol. Molecules 2023, 28, 3271. [Google Scholar] [CrossRef] [PubMed]
- Ruffolo, G.; Gaeta, A.; Cannata, B.; Pinzaglia, C.; Aronica, E.; Morano, A.; Cifelli, P.; Palma, E. GABAergic Neurotransmission in Human Tissues Is Modulated by Cannabidiol. Life 2022, 12, 2042. [Google Scholar] [CrossRef] [PubMed]
- Beers, J.L.; Fu, D.; Jackson, K.D. Cytochrome P450–Catalyzed Metabolism of Cannabidiol to the Active Metabolite 7-Hydroxy-Cannabidiol. Drug Metab. Dispos. 2021, 49, 882–891. [Google Scholar] [CrossRef]
- Jiang, R.; Yamaori, S.; Takeda, S.; Yamamoto, I.; Watanabe, K. Identification of Cytochrome P450 Enzymes Responsible for Metabolism of Cannabidiol by Human Liver Microsomes. Life Sci. 2011, 89, 165–170. [Google Scholar] [CrossRef]
- Zhang, Q.; Melchert, P.W.; Markowitz, J.S. Pharmacokinetic Variability of Oral Cannabidiol and Its Major Metabolites after Short-Term High-Dose Exposure in Healthy Subjects. Med. Cannabis Cannabinoids 2024, 7, 1–9. [Google Scholar] [CrossRef]
- Batinic, A.; Sutlovic, D.; Kuret, S.; Burcul, F.; Kalajzic, N.; Matana, A.; Dujic, G.; Vrdoljak, J.; Kumric, M.; Bozic, J.; et al. Differences in Plasma Cannabidiol Concentrations in Women and Men: A Randomized, Placebo-Controlled, Crossover Study. Int. J. Mol. Sci. 2023, 24, 10273. [Google Scholar] [CrossRef]
- Bansal, S.; Paine, M.F.; Unadkat, J.D. Comprehensive Predictions of Cytochrome P450 (P450)-Mediated In Vivo Cannabinoid-Drug Interactions Based on Reversible and Time-Dependent P450 Inhibition in Human Liver Microsomes. Drug Metab. Dispos. 2022, 50, 351–360. [Google Scholar] [CrossRef]
- Food and Feed Information Portal Database | FIP. Available online: https://ec.europa.eu/food/food-feed-portal/screen/novel-food-catalogue/search (accessed on 30 April 2024).
- European Parliament and the Council of European Union. Regulation (EU) No 2015/2283 of the European Parliament and of the Council of on Novel Foods. 25 November.
- EFSA Panel on Nutrition, Novel Foods and Food Allergens (NDA); Turck, D.; Bohn, T.; Castenmiller, J.; De Henauw, S.; Hirsch-Ernst, K.I.; Maciuk, A.; Mangelsdorf, I.; McArdle, H.J.; Naska, A.; et al. Statement on Safety of Cannabidiol as a Novel Food: Data Gaps and Uncertainties. EFSA J. Eur. Food Saf. Auth. 2022, 20, e07322. [Google Scholar] [CrossRef]
- Commissioner, O. of the FDA Regulation of Cannabis and Cannabis-Derived Products, Including Cannabidiol (CBD). FDA 2024. [Google Scholar]
- Lo, L.A.; Christiansen, A.; Eadie, L.; Strickland, J.C.; Kim, D.D.; Boivin, M.; Barr, A.M.; MacCallum, C.A. Cannabidiol-Associated Hepatotoxicity: A Systematic Review and Meta-Analysis. J. Intern. Med. 2023, 293, 724–752. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, R.K.; Andersen, M.L.; Mazaro-Costa, R. The Effects of Cannabidiol on Male Reproductive System: A Literature Review. J. Appl. Toxicol. 2020, 40, 132–150. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, R.K.; Rocha, T.L.; Fernandes, F.H.; Gonçalves, B.B.; Souza, M.R.; Araújo, A.A.; Barbosa, C.C.; Silva, D.M.; Campos, H.M.; Tomazett, M.V.; et al. Decreasing Sperm Quality in Mice Subjected to Chronic Cannabidiol Exposure: New Insights of Cannabidiol-Mediated Male Reproductive Toxicity. Chem. Biol. Interact. 2022, 351, 109743. [Google Scholar] [CrossRef] [PubMed]
- European Parliament an the Council of the European Union Regulation (EC) No 178/2002 of the European Parliament and of the Council of 28 January 2002 Laying down the General Principles and Requirements of Food Law, Establishing the European Food Safety Authority and Laying down Procedures in Matters of Food Safety. 2002.
- Lachenmeier, D.W.; Sproll, C.; Walch, S.G. Does Cannabidiol (CBD) in Food Supplements Pose a Serious Health Risk? Consequences of the European Food Safety Authority (EFSA) Clock Stop Regarding Novel Food Authorisation. Psychoactives 2023, 2, 66–75. [Google Scholar] [CrossRef]
- Committee, E.S.; More, S.J.; Bampidis, V.; Benford, D.; Bragard, C.; Halldorsson, T.I.; Hernández-Jerez, A.F.; Bennekou, S.H.; Koutsoumanis, K.; Lambré, C.; et al. Guidance on the Use of the Benchmark Dose Approach in Risk Assessment. EFSA J. 2022, 20, e07584. [Google Scholar] [CrossRef]
- Davis, J.A.; Gift, J.S.; Zhao, Q.J. Introduction to Benchmark Dose Methods and U.S. EPA’s Benchmark Dose Software (BMDS) Version 2.1.1. Toxicol. Appl. Pharmacol. 2011, 254, 181–191. [Google Scholar] [CrossRef] [PubMed]
- US EPA, O. Benchmark Dose Technical Guidance. Available online: https://www.epa.gov/risk/benchmark-dose-technical-guidance (accessed on 21 May 2024).
- Arout, C.A.; Haney, M.; Herrmann, E.S.; Bedi, G.; Cooper, Z.D. A Placebo-Controlled Investigation of the Analgesic Effects, Abuse Liability, Safety and Tolerability of a Range of Oral Cannabidiol Doses in Healthy Humans. Br. J. Clin. Pharmacol. 2022, 88, 347–355. [Google Scholar] [CrossRef] [PubMed]
- McCartney, D.; Kevin, R.C.; Suraev, A.S.; Sahinovic, A.; Doohan, P.T.; Bedoya-Pérez, M.A.; Grunstein, R.R.; Hoyos, C.M.; McGregor, I.S. How Long Does a Single Oral Dose of Cannabidiol Persist in Plasma? Findings from Three Clinical Trials. Drug Test. Anal. 2023, 15, 334–344. [Google Scholar] [CrossRef]
- Schoedel, K.A.; Szeto, I.; Setnik, B.; Sellers, E.M.; Levy-Cooperman, N.; Mills, C.; Etges, T.; Sommerville, K. Abuse Potential Assessment of Cannabidiol (CBD) in Recreational Polydrug Users: A Randomized, Double-Blind, Controlled Trial. Epilepsy Behav. EB 2018, 88, 162–171. [Google Scholar] [CrossRef]
- Devinsky, O.; Patel, A.D.; Thiele, E.A.; Wong, M.H.; Appleton, R.; Harden, C.L.; Greenwood, S.; Morrison, G.; Sommerville, K. Randomized, Dose-Ranging Safety Trial of Cannabidiol in Dravet Syndrome. Neurology 2018, 90, e1204–e1211. [Google Scholar] [CrossRef] [PubMed]
- Committee, E.S. Guidance on Selected Default Values to Be Used by the EFSA Scientific Committee, Scientific Panels and Units in the Absence of Actual Measured Data. EFSA J. 2012, 10, 2579. [Google Scholar] [CrossRef]
- Sales of CBD in Europe 2022-2026 Forecast. Available online: https://www.statista.com/statistics/1306959/forecast-cbd-sales-europe/ (accessed on 26 January 2024).
- Geppert, J.; Lietzow, J.; Hessel-Pras, S.; Kirsch, F.; Schäfer, B.; Sachse, B. Usage and Health Perception of Cannabidiol-Containing Products among the Population in Germany: A Descriptive Study Conducted in 2020 and 2021. BMC Public Health 2023, 23, 2318. [Google Scholar] [CrossRef] [PubMed]
- Bhamra, S.K.; Desai, A.; Imani-Berendjestanki, P.; Horgan, M. The Emerging Role of Cannabidiol (CBD) Products; a Survey Exploring the Public’s Use and Perceptions of CBD. Phytother. Res. PTR 2021, 35, 5734–5740. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, C.; Moeller, K.E.; McGuire, M.; Melton, B.L. Consumer Perception, Knowledge, and Uses of Cannabidiol. Ment. Health Clin. 2023, 13, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Goodman, S.; Wadsworth, E.; Schauer, G.; Hammond, D. Use and Perceptions of Cannabidiol Products in Canada and in the United States. Cannabis Cannabinoid Res. 2022, 7, 355–364. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, M.; Merten, J.W.; Gordon, B.T.; Hamadi, H. CBD (Cannabidiol) Product Attitudes, Knowledge, and Use Among Young Adults. Subst. Use Misuse 2020, 55, 1138–1145. [Google Scholar] [CrossRef] [PubMed]
- Mathur, K.; Vuppalanchi, V.; Gelow, K.; Vuppalanchi, R.; Lammert, C. Cannabidiol (CBD) Consumption and Perceived Impact on Extrahepatic Symptoms in Patients with Autoimmune Hepatitis. Dig. Dis. Sci. 2020, 65, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Corroon, J.; Phillips, J.A. A Cross-Sectional Study of Cannabidiol Users. Cannabis Cannabinoid Res. 2018, 3, 152–161. [Google Scholar] [CrossRef]
- Soleymanpour, M.; Saderholm, S.; Kavuluru, R. Therapeutic Claims in Cannabidiol (CBD) Marketing Messages on Twitter. Proc. IEEE Int. Conf. Bioinforma. Biomed. 2021, 2021, 3083–3088. [Google Scholar] [CrossRef]
- Merten, J.W.; Gordon, B.T.; King, J.L.; Pappas, C. Cannabidiol (CBD): Perspectives from Pinterest. Subst. Use Misuse 2020, 55, 2213–2220. [Google Scholar] [CrossRef]
- Kaufmann, R.; Bozer, A.H.; Jotte, A.K.; Aqua, K. Long-Term, Self-Dosing CBD Users: Indications, Dosage, and Self-Perceptions on General Health/Symptoms and Drug Use. Med. Cannabis Cannabinoids 2023, 6, 77–88. [Google Scholar] [CrossRef] [PubMed]
- Melchert, D.; Schaare, F.; Winterhalter, P.; Beuerle, T. CBD Products: Labeling Accuracy of an Obscure Niche Market. Food Control 2024, 160, 110375. [Google Scholar] [CrossRef]
- Bonn-Miller, M.O.; Loflin, M.J.E.; Thomas, B.F.; Marcu, J.P.; Hyke, T.; Vandrey, R. Labeling Accuracy of Cannabidiol Extracts Sold Online. JAMA 2017, 318, 1708–1709. [Google Scholar] [CrossRef]
- Johnson, E.; Kilgore, M.; Babalonis, S. Label Accuracy of Unregulated Cannabidiol (CBD) Products: Measured Concentration vs. Label Claim. J. Cannabis Res. 2022, 4, 28. [Google Scholar] [CrossRef] [PubMed]
- Vandrey, R.; Raber, J.C.; Raber, M.E.; Douglass, B.; Miller, C.; Bonn-Miller, M.O. Cannabinoid Dose and Label Accuracy in Edible Medical Cannabis Products. JAMA 2015, 313, 2491–2493. [Google Scholar] [CrossRef]
- Lindekamp, N.; Weigel, S.; Sachse, B.; Schäfer, B.; Rohn, S.; Triesch, N. Comprehensive Analysis of 19 Cannabinoids in Commercial CBD Oils: Concentrations, Profiles, and Safety Implications. J. Consum. Prot. Food Saf. 2024. [Google Scholar] [CrossRef]
- Kaufmann, R.; Harris Bozer, A.; Jotte, A.R.K.; Aqua, K. The Effects of Long-Term Self-Dosing of Cannabidiol on Drowsiness, Testosterone Levels, and Liver Function. Med. Cannabis Cannabinoids 2023, 6, 32–40. [Google Scholar] [CrossRef]
- Kaufmann, R.; Aqua, K.; Lombardo, J.; Lee, M. Observed Impact of Long-Term Consumption of Oral Cannabidiol on Liver Function in Healthy Adults. Cannabis Cannabinoid Res. 2023, 8, 148–154. [Google Scholar] [CrossRef]
- Chen, S.; Kim, J.-K. The Role of Cannabidiol in Liver Disease: A Systemic Review. Int. J. Mol. Sci. 2024, 25, 2370. [Google Scholar] [CrossRef]
- Caputi, T.L. Re: “Observed Impact of Long-Term Consumption of Oral Cannabidiol on Liver Function in Healthy Adults” and a Recent Announcement of a New Cannabidiol Safety Study. Cannabis Cannabinoid Res. 2022, 7, 896–897. [Google Scholar] [CrossRef] [PubMed]
- Sarrafpour, S.; Urits, I.; Powell, J.; Nguyen, D.; Callan, J.; Orhurhu, V.; Simopoulos, T.; Viswanath, O.; Kaye, A.D.; Kaye, R.J.; et al. Considerations and Implications of Cannabidiol Use During Pregnancy. Curr. Pain Headache Rep. 2020, 24, 38. [Google Scholar] [CrossRef] [PubMed]
- Feinshtein, V.; Erez, O.; Ben-Zvi, Z.; Erez, N.; Eshkoli, T.; Sheizaf, B.; Sheiner, E.; Huleihel, M.; Holcberg, G. Cannabidiol Changes P-Gp and BCRP Expression in Trophoblast Cell Lines. PeerJ 2013, 1, e153. [Google Scholar] [CrossRef] [PubMed]
- Feinshtein, V.; Erez, O.; Ben-Zvi, Z.; Eshkoli, T.; Sheizaf, B.; Sheiner, E.; Holcberg, G. Cannabidiol Enhances Xenobiotic Permeability through the Human Placental Barrier by Direct Inhibition of Breast Cancer Resistance Protein: An Ex Vivo Study. Am. J. Obstet. Gynecol. 2013, 209, 573–e1. [Google Scholar] [CrossRef] [PubMed]
- Guth, S.; Roth, A.; Engeli, B.; Lachenmeier, D.W.; Cartus, A.T.; Hüser, S.; Baum, M.; Diel, P.; Eisenbrand, G.; Hengstler, J.G.; et al. Comparison of Points of Departure between Subchronic and Chronic Toxicity Studies on Food Additives, Food Contaminants and Natural Food Constituents. Food Chem. Toxicol. Int. J. Publ. Br. Ind. Biol. Res. Assoc. 2020, 146, 111784. [Google Scholar] [CrossRef] [PubMed]
- Henderson, R.G.; Lefever, T.W.; Heintz, M.M.; Trexler, K.R.; Borghoff, S.J.; Bonn-Miller, M.O. Oral Toxicity Evaluation of Cannabidiol. Food Chem. Toxicol. 2023, 176, 113778. [Google Scholar] [CrossRef] [PubMed]
- Tallon, M.J.; Child, R. Subchronic Oral Toxicity Assessment of a Cannabis Extract. Regul. Toxicol. Pharmacol. 2023, 144, 105496. [Google Scholar] [CrossRef]
- Dziwenka, M.; Dolan, L.C.; Rao, M. Safety of Elixinol Hemp Extract: In Vitro Genetic Toxicity and Subchronic Toxicity in Rats. J. Toxicol. 2023, 2023, 5982883. [Google Scholar] [CrossRef] [PubMed]
- Crippa, J.A.S.; Zuardi, A.W.; Guimarães, F.S.; Campos, A.C.; de Lima Osório, F.; Loureiro, S.R.; dos Santos, R.G.; Souza, J.D.S.; Ushirohira, J.M.; Pacheco, J.C.; et al. Efficacy and Safety of Cannabidiol Plus Standard Care vs Standard Care Alone for the Treatment of Emotional Exhaustion and Burnout Among Frontline Health Care Workers During the COVID-19 Pandemic: A Randomized Clinical Trial. JAMA Netw. Open 2021, 4, e2120603. [Google Scholar] [CrossRef]
- Arcella, D.; Cascio, C.; Mackay, K. Acute Human Exposure Assessment to Tetrahydrocannabinol (Δ9-THC). EFSA J. 2020, 18, e05953. [Google Scholar] [CrossRef]
- FDA. Drug Approval Package: Epidiolex (Cannabidiol). Company: GW Research Ltd. Application Number: 210365 Orig 1. FDA Application Review Files. Pharmacology Review(s). 2018. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2018/210365Orig1s000PharmR.pdf.
- Henderson, R.G.; Vincent, M.; Rivera, B.N.; Bonn-Miller, M.O.; Doepker, C. Cannabidiol Safety Considerations: Development of a Potential Acceptable Daily Intake Value and Recommended Upper Intake Limits for Dietary Supplement Use. Regul. Toxicol. Pharmacol. 2023, 144, 105482. [Google Scholar] [CrossRef] [PubMed]
- Grotenhermen, F. Pharmacokinetics and Pharmacodynamics of Cannabinoids. Clin. Pharmacokinet. 2003, 42, 327–360. [Google Scholar] [CrossRef] [PubMed]
- BLV (Bundesamt für Lebensmittelsicherheit und Veterinärwesen) Briefing Letter Cannabidiol (CBD) in Lebensmitteln und Lebereffekte. Available online: https://www.blv.admin.ch/blv/de/home/lebensmittel-und-ernaehrung/rechts-und-vollzugsgrundlagen/bewilligung-und-meldung/bewilligung/cannabis-cannabidiol.html (accessed on 11 June 2024).
- GW Pharmaceuticals Submission on Scientific Data and Information about Products Containing Cannabis or Cannabis-Derived Compounds (FDA-2019-N-1482-4257 Attachment 1) Available online: https://downloads.regulations.gov/FDA-2019-N-1482-4257/attachment_1.pdf.
- Committee on Toxicity Updated Position Paper on the Potential Risk of CBD in CBD Food Products Available online: https://cot.food.gov.uk/sites/default/files/2021-08/CBD%20Position%20Paper%20updated%20July%202021.pdf.
- Joint Position Paper from ACNFP & COT on Establishing Provisional ADI for Pure Form CBD in Foods | Advisory Committee on Novel Foods and Processes. Available online: https://acnfp.food.gov.uk/JointpositionpaperfromACNFP%26COTonestablishingprovisionalADIforpureformCBDinfoods (accessed on 17 June 2024).
- O’Sullivan, S.E.; Jensen, S.S.; Kolli, A.R.; Nikolajsen, G.N.; Bruun, H.Z.; Hoeng, J. Strategies to Improve Cannabidiol Bioavailability and Drug Delivery. Pharmaceuticals 2024, 17, 244. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Figure 1. Structural formula of Cannabidiol
Figure 2.
Cannabis sativa plant (own photography by H.F.)

Figure 3.
CBD and its main metabolites (phase 1 metabolism in the liver).
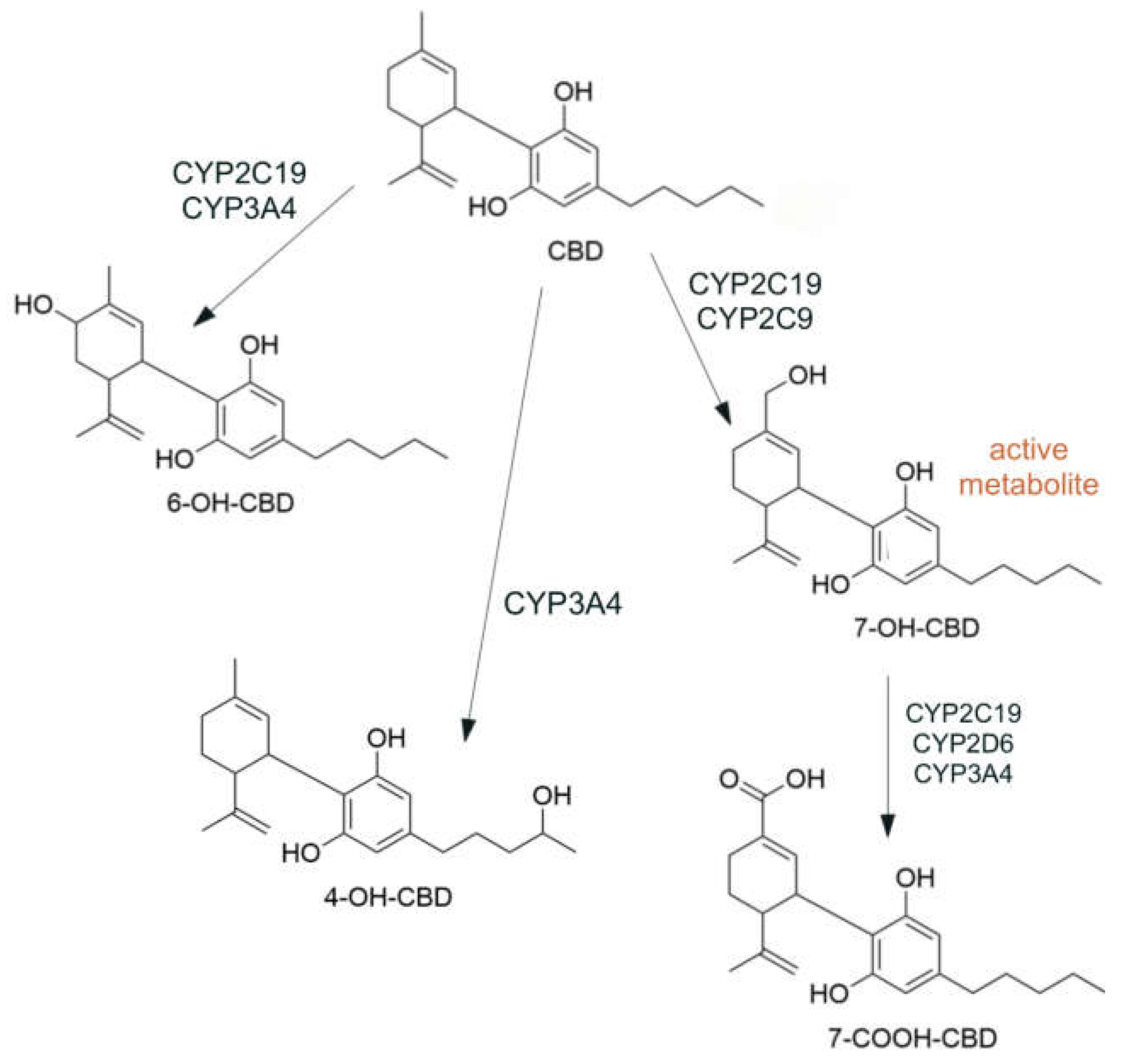
Table 1.
CBD online dosing recommendations (full data in Appendix Table A1).
| Dosage 1 | Number of investigated websites (n= 26) | Dosage mean value (and range) [mg/day] |
|---|---|---|
| Low dosage (micro dosage) |
13 | 15 (0.5 – 25) |
| Medium dosage (standard dosage) |
13 | 47 (10 – 100) |
| High dosage (macro dosage) |
12 | 227 (50 – 800) |
| Other dosage information | 10 | 62 (2.5 – 300) |
| Medicinal indication statements 2 | 8 | - |
1 Dosage recommendations online often refer to a low, medium and high dose range and titration to effective dose is often recommended. 2 Dosages are often mentioned with supposedly suitable indications.
Table 2.
Benchmark Dose Modeling for Cannabidiol in animal experiments.
| Study, Tested Substance |
Species, Sex1 |
Study design, CBD Doses 2 | Endpoint | BMDL | BMD | p-Value | Model 3 |
|---|---|---|---|---|---|---|---|
| Henderson et al. [52] CBD-isolate |
Rats, female | 90 day oral toxicity study 0, 50, 80, 120, 140 mg/kg bw/day |
liver weight | 43 mg/kg bw/day | 64 mg/kg bw/day | 0.242 | Power |
| Tallon and Child [53] Hemp extract (6.27% CBD) |
Rats, female | 90 day oral toxicity study 0, 30, 115.13, 230.25, 460.5 mg/kg bw/day |
liver weight | (80 mg/kg bw/day) 3 |
(94 mg/kg bw/day) 3 | 0.948 | Linear |
| Dziwenka et al. [54] Elixinol Hemp Extract (around 65% CBD) |
Rats, male | 90 day oral toxicity study 0, 18.95, 33.16, 56.84 mg/kg bw/day |
liver weight | (30 mg/kg bw/day)4 | (41 mg/kg bw/day)4 | 0.644 | Exponential 3 |
1 The more sensitive sex was selected. 2 Dosages were adjusted to the pure CBD content stated in the study, if necessary. 3 Recommended model results (lowest Akaike Information Criterion (AIC)) selected with BMDS online webapp. 4Not a pure CBD test substance, therefore a general statement is not possible.
Table 3.
Candidates for a health-based guidance value from animal and human studies.
| Human study | Animal study | |
|---|---|---|
| Study | Crippa et al. [55] | Henderson et al. [52] |
| Reference Point (RP) | LOAEL of 300 mg/day (= 4.29 mg/kg bw/day) |
BMDL of 43 mg/kg bw/day |
| Uncertainty factor (UF) | 30 1 | 200 2 |
| HBGV | 0.14 mg/kg bw/day (10 mg/day) |
0.21 mg/kg bw/day (15 mg/day) |
110 for intraspecies variability x 3 for extrapolation from LOAEL to NOAEL. 210 for interspecies variability x 10 for intraspecies variability x 2 for extrapolation from subchronic to chronic.
Table 4.
Summary of health-based guidance values for oral cannabidiol intake.
| Study | Health-based guidance value/ acceptable daily intake |
Rationale |
|---|---|---|
| COT FSA [62] (2021) | 70 mg/day | 1 mg/kg bw/day for inhibitory interactions in humans |
| BLV [60] (2021) | 12 mg/day | 5 mg/kg bw/day for DILI in humans |
| Lachenmeier et al. [19] (2023) | 10 mg/day | 300 mg/day for DILI in humans |
| Henderson et al. [58] (2023) | 30 mg/day | 300 mg/day for DILI in humans |
| COT FSA [63] (2023) | 10 mg/day | 72, 50 and 25 mg/kg bw/day for adverse liver effects in rodents |
| This study | 10 mg/day | 300 mg/day for DILI in humans |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



