
Submitted:
30 July 2024
Posted:
02 August 2024
You are already at the latest version
Abstract
(1) Background: Youths with multiple risks and severe disadvantages experience poorer health and educational outcomes than less disadvantaged peers. To address problems with coping and self-regulation in this group, mental skills training (MST) approaches more commonly used in sport are an emerging intervention approach. (2) Methods and Results: This narrative review synthesizes literature to explain the need for MST, how it works, and evidence to support it works by focusing on two well evaluated programmes: LifeMatters and My Strengths Training for Life™. (3) Conclusions: To support positive youth development, MST is a strengths-based, flexible and adaptable approach to help fill the shortage of available evidence-based programs for those youths facing multiple disadvantages. The findings of this review may facilitate policy makers, commissioners, program planners, and researchers in the uptake of MST or similar psychoeducational approaches in future.
Keywords:
childhood adversity
; inequalities
; mental health
; youth homelessness
; life skills
; positive youth development
; self-regulation
; solution-focused
; strengths-based
; well-being
1. Introduction
Multiple disadvantage means to live with several overlapping issues whereby one need creates another or exacerbates other needs. It is also known as having multiple and complex needs, severe multiple disadvantage, and high support needs [1,2] or by the breadth (i.e., range) and depth (i.e., severity) of need [3]. Within UK policy terms, multiple disadvantage describes a segment of the population experiencing interrelated and mutually reinforcing social harms: homelessness, current or historical offending, substance abuse, and mental illness [1]. But these needs can also include but are not limited to experiencing or witnessing violence, neglect, or abuse (e.g., domestic abuse, sexual abuse, and child sexual abuse); involvement in sex work; loss of custody of one or more children; physical ill-health; experiencing or witnessing substance misuse; living in poverty; parental instability through family breakdown or parents being in jail; and discrimination [4].
The extreme health and social inequalities faced by those with multiple disadvantage result from wider systemic problems [1,4,5], including difficulties with access to and use of health care and other support services, differences in educational attainment, and increased risk for unemployment and discrimination [6]. Young people aged 16 to 25 years old are a key group who face multiple disadvantages, particularly those experiencing homelessness. In 2022-2023, an estimated 135,800 young people in the UK sought help from their local council, a 12% increase from 2020-21 [7]. After years of austerity, changes to the UK benefits system, and further exacerbated by the Covid-19 pandemic, youth homeless services find themselves under increased pressure to meet rising demands for their services while simultaneously addressing young people’s increasingly complex support needs with fewer resources available [8,9].
Experiencing multiple disadvantage in this age group brings its own unique risks by disrupting development, impairing physical and mental health, as well as harming educational and employment attainment [6]. If these issues are not effectively addressed, inequalities may be perpetuated into adulthood and lead to lower overall quality of life. While there is growing recognition within government and the voluntary sector of the need to address multiple disadvantage and examples of psychological interventions emerging e.g., [10,11,12], gaps still remain in service provision for addressing the co-occurring needs of young people aged 16 to 24 years who are facing the most extreme forms of socio-structural disadvantage.
When designing these interventions, there is a need to better recognize and understand the impact of young people’s history of trauma and adversity. In this paper, we review research investigating the influence that exposure to adverse childhood experiences (ACEs) has on young people’s brain development, coping, and self-regulation. We explain why researchers have advocated for a strengths-based approach to improving self-regulation and outline solution-focused brief therapy (SFBT) and positive youth development (PYD) as methods to inform programme planning. We then outline how mental skills training (MST), which is an intervention approach more commonly used in sport and other performance domains, addresses the dearth of strengths-based programmes for improving self-regulation in young people. This narrative review then summarises the research related to two such programmes, LifeMatters and My Strengths Training™ for Life (MST4Life™), before discussing the strengths, limitations, implications, and future research opportunities for this area.
1.1. Adversity, Stress, and Development in Youth
A history of ACEs such as abuse, neglect, harm, and/or household dysfunction, combined with a lack of protective factors including the absence of supportive relationships, safe enviornments, and insufficient resources and support systems, can negatively impact on young people’s brain development [13]. It is now well established that structural and functional brain development occurs until around 25 years of age, contributing to many typical adolescent behaviours including greater risk taking and increased emotional reactivity [14,15]. However, exposure to ACEs can lead to prolonged activation of hypothalamic-pituitary-adrenal (HPA) axis, resulting in consistently high levels of stress hormones such as cortisol [16,17,18]. The body’s fight-or-flight response is also persistently activated, leading to increased heart rate, blood pressure, and other physiological stress markers. Collectively, this so-called toxic stress response can alter the size and neuronal architecture (e.g., neural pathways) of areas of the brain such as the amygdala, hippocampus, and prefrontal cortex [17,19,20,21]. These structural changes can also lead to functional impairments in memory and emotion regulation functioning, as well as other executive functions. Not only does this have long-term negative implications for physical and mental health, it also partly explains why so many behavioural and emotional issues occur in young people facing multiple disadvantage.
Young people can experience dysfunction of their self-regulation capacities thereby contributing to difficulties in forming and maintaining personal relationships, handling stressful situations, decision making and managing their emotions [6,20,22]. Considered to be an important protective factor, self-regulation consists of three overlapping domains of cognitive self-regulation, emotional self-regulation, and behavioural self-regulation [20]. Cognitive self-regulation includes executive functioning (e.g., mental flexibility), focused attention, and decision making. Emotional self-regulation integrates cognitive and emotional processes and involves actively managing strong and unpleasant feelings, through awareness and use of self-calming strategies. Behavioural self-regulation includes impulse control, enactment of coping strategies, conflict resolution, support seeking, and seeking and using resources to increase the chances of achieving goals [20,23,24].
Improved self-regulation helps young people’s progression towards adulthood [20] via increased education attainment and employment opportunities [25,26], and better income, financial planning and management [27]. Greater self-regulation capacity can also improve overall health and wellbeing of individuals. Indeed, a greater level of self-regulation in early or middle childhood is associated with better mental health outcomes, significantly less substance abuse, and criminal offenses in adulthood [28]. In contrast, those who experience reduced self-regulation and health and social inequalities, are more likely to engage in maladaptive coping strategies such as avoidance and withdrawal mechanisms, internalization, and substance and alcohol misuse [29,30,31].
Services supporting young people experiencing multiple disadvantages have typically offered help to meet basic needs such as food, water, housing, and crisis support. But it is also essential that these services offer opportunities for young people to develop the self-regulation skills needed for independence and overcome the negative impacts of a toxic stress response. Such interventions will help to reduce health and social inequalities by helping young people to move further along a continuum of self-regulation (see Figure 1), from lower self-regulation (e.g., lack of self-awareness, low levels of self-control, relies on others for cognitive, emotion, and/or behavioural regulation) to higher self-regulation (e.g., aware and able to effectively apply for cognitive, emotion, and/or behavioural self-regulation across a range of situations; displays a high level of self-control and organisation). Importantly, the adolescent brain is still in an ongoing period of development until around 25 years of age, with areas of the brain related to self-regulation being amongst the last to mature. Thus, there is a key opportunity for intervention prior to adulthood to improve young people’s self-regulation capacities.
1.2. Need for Strengths-Based Approaches
There have been longstanding calls for more strengths-based approaches to supporting young people who experience multiple disadvantage [32,33]. For example, young people experiencing homelessness have been found to be relunctant to engage in interventions and with support services [34]. For self-regulation interventions to be successful in supporting multiply disadvantaged young people, it is essential for these to address the underlying trauma and emotional and psychological needs in a way that is engaging and non-stigmatizing. In a deficit-based or pathology-oriented model, young people are viewed as having problems to be fixed and their risks and needs are assessed as a starting point to intervention. Programs and services are designed in response to these needs and delivered by professionals who are experts in the presenting problem(s), with young people being passive recipients of this expertise [33]. The uneven power balance in these relationships can lead young people to feeling disempowered and dependent on experts to address their problems [35].
A less stigmatising approach is to be strengths-based—involving a collaborative process between the person being supported and those supporting them. According to Rapp, et al. [36], there are six main characteristics that define strengths-based approaches: (1) it is goal-oriented; (2) it includes a systematic assessment of strengths; (3) the enviornment is seen as rich in resources; (4) there are explicit methods used to help personal and environmental strengths for goal attainment; (5) the relationship is hope-inducing; and (6) meaningful choices are provided and young people have the authority to choose. Although problems are not ignored, the starting point is what already works, identifying existing capabilities, motivations, resources and support systems, and further opportunities for improvement and growth [36]. The collaborative process is at the centre of this work, with young people playing an active role in developing and using their own strengths to achieve their goals and realise their potential [37]. Moreover, the focus of strength-based approaches is on the sharing of power and quality of relationships, with all young people viewed as having strengths and the potential for change in the context of available resources in their environments [35,38,39,40].
1.2.1. Self-Determination Theory and Basic Psychological Needs
Self-determination theory (SDT) is a key theoretical perspective that has been used to inform a principle of stengths-based approaches that all individuals have the capacity and right to affect the course of their lives [41]. Strengths based approaches are also intentionally designed to support young people’s basic psychological needs of autonomy (i.e., the degree to which people feel volitional and responsible for their own behaviour), competence (i.e., the degree to wuich people feel effective in their ongoing interactions with the social enviornment and within which experience opportunities to express their capabilities), and relatedness (i.e., the degree to which people feel a sense of belonging and connection with others within their social enviornment) [42,43,44]. According to basic psychological needs theory (BPNT; a mini theory of SDT), satisfaction of this trio of needs are considered essential for a person’s well-being as well as their adjustment, development, and flourishing. In contrast, it could be argued that deficit-based approaches are likely to frustrate or thwart these needs, which in turn is associated with problem behaviour, ill-being, and psychopathology [45].
1.2.2. Solution Focused Brief Therapy
Solution focused brief therapy (SFBT) is an example of a strengths-based approach with evidence to support its effectivenes [46] and has been applied to psychological trauma in young people to facilitate hope and well-being [47,48]. SFBT was developed by De Shazer, Berg, and colleagues as a brief, goal-oriented, and future-focused therapy based on the belief that there is always something working in people’s lives regardless of how serious or chronic the problems they face [49,50]. The focus is on “solutions talk” and “what’s right with you?” rather than “problems talk” or “what’s wrong with you”. Exceptions, the times when the problem was not present or not present to the same degree, are explored as a way to help the person to identify already exisiting solutions to their problems or challenges and other techniques such as identifying the person’s strengths and past successes and providing compliments during the solution-focused process [48]. Within community-based services, a recent meta-analysis found that SFBT is effective for a range of outcomes including depression, behavioural health (e.g., substance abuse), family functionning, and psychosocial adjustment [46].
1.2.3. Positive Youth Development
Positive youth development (PYD) also views all young people as having strengths and the potential for change but emphases the importance of the context, including the availability of resources in the young person’s environment [38,39,40]. PYD aims to promote personal development, thriving, and growth in young people by aligning strengths and resources with positive affective relationships with caring adults, challenging experiences, and skill-building opportunities. The concept of intentional self-regulation is argued to be a key process for promoting healthy, positive development by aligning adolescents’ strengths with the resources in their contexts [51,52]. By supporting young people to develop and deploy intentional self-regulation (i.e., their mental skills), it is expected that they will be able to capitalise on opportunities within their enviornment. In other words, mental skills are important assets for young people’s optimal development and will enable them to better navigate the many contextual changes that occur over adolescence [24,53]. PYD programmes for disadvantaged young people have been shown to foster positive outcomes, including educational attainment and physical and mental health, as well as reduce risk and negative outcomes, such as homelessness, drug and alcohol use, and involvement in violence [54].
1.3. Summary
Young people aged 16 to 25 are emerging adults who are still undergoing important developmental processes that will influence their future life trajectory. During this final stage of adolescent development, those with multiple disadvantages, particularly young people with a history of adversity and trauma, may experience reduced self-regulation linked to deficts in stress buffering resources. In turn, having reduced/impaired self-regulation may result in maladaptive coping (e.g., alcohol and drug use) and will likely perpetuate the many challenges young people experience through its negative impacts on cognition, emotions, and behaviours. While services are under increasing pressure to address the psychological needs resulting from trauma and adversity, such as providing young people with opportunities to develop self-regulation and other important life skills, it is not yet clear how this can be effectively done. Strengths-based approaches have been suggested as a less stigmatising and more collaborative, engaging, and psychologially needs satisfying alternative to traditional methods that focus on fixing young people’s deficits or providing help to solve their problems. This review has so far highlighted SFBT and PYD as strengths-based methods that have seperately been used to promote strengths, well-being, and/or the development of self-regulation in young people with a history of trauma. In the next section, we introduce a strengths-based intervention approach informed by sport psychology and summarise the existing evidence from two different programmes underpinned by BPNT, SFBT, and/or PYD.
2. Mental Skills Training (MST)
Mental skills training (MST) addresses the challenges in supporting young people with multiple disadvantages to develop and implement self-regulation [55]. Within sport and other performance domains, MST is a developmentally appropriate psychoeducational approach that involves the implementation of cognitive behavioural techniques to help performers to develop mental skills which enhance their learning and performance [56]. As physical differences grow smaller between competitors at elite levels, so too are the margins that make a difference between winning and losing. To gain an edge, Olympic athletes have long attested to systematic mental training as a critical component of their talent development and success [57]. Not only can MST help young people to fulfil their potential, but it can also improve their mental health and well-being. A study with dancers found that mental skills served as a protective factor for eating disorder risk [58] whereas another study with student-athlete rowers found that a 6-month MST programme led to significant improvements in mental toughness and psychological well-being [59].
MST is also a holistic approach that addresses PYD goals by equipping young people with transferable skills that can be applied to multiple life domains (e.g., school, work, relationships). That is, young people can practice and improve their mental skills in one setting (e.g., participating in sport), but then must become proficient at transferring mental skills across different contexts to more fully benefit [60]. For example, after developing a clearer understanding of MST techniques following their participation in an intervention programme, youth rugby union players aged 15 to 16 years reported being able to successfully employ mental techniques within their rugby performances as well as in other areas of their life, including school [61].
But MST is applicable for more than just athletes and has been increasingly recognised as an approach for supporting the positive development for young people, including those facing multiple disadvantages. MST appears to be suitable to those who are in the adolescent and emerging adulthood phase of development, particularly young people with a history of trauma and adversity, wherein this development has been disrupted [62]. Importantly, MST is a non-stigmatising approach because of its association with sport. Athletes do not necessarily need a problem or deficit to benefit from MST. Instead, MST is viewed just as much to uncover strengths and maximise talent as to identify weaknesses and areas for improvement via more intentional self-regulation.

Table 1.
Definitions and examples of mental skills training terminology applied to young people facing multiple disadvantages.
Table 1.
Definitions and examples of mental skills training terminology applied to young people facing multiple disadvantages.
| Term | Definition | Examples |
|---|---|---|
| Mental techniques | Cognitive or behavioural techniques used to build mental skills and qualities [63]. | Action planning Goal-setting Positive self-talk Support seeking |
| Mental skills | The capacity to intentionally self-regulate thoughts, emotions, and behaviours [63]. | Focusing attention Handling pressure Self-awareness Self-control |
| Mental qualities | Positive intrapersonal and/or interpersonal characteristics displayed by or within an individual [63]. | Intrinsic motivation Resilience Self-confidence Self-worth |
| Mental skills transfer | The application of mental skills developed in one context and then applied to a new one. | Learning positive self-talk from support worker and then using positive self-talk before a job interview. |
| Mental skills training | The systematic development, application, and implementation of mental techniques for developing mental skills to promote the mental qualities needed for well-being and optimal development [55,63]. |
LifeMatters [64] MST4Life™ [55] |
In this section, we focus on reviewing two of the most well evaluated MST programmes for young people experiencing multiple disadvantages: LifeMatters [64] and MST4Life™ [55]. But, first, we explain how MST is intended to work drawing on an updated version of Holland et al.’s conceptual process model of youth mental skills training [63].
2.1. How MST Works
Although Holland et al. [63] developed the conceptual process model of youth mental skills training for sport populations, it is applicable across a broader range of populations. We therefore refer to it henceforth as the MST process model and show its applicability to non-sport populations through the examples used (see Table 1 for terms, definitions, and examples). Underpinned by theories of self-regulation and metacognition (i.e., the awareness, directing, and monitoring of thoughts and feelings [65]), the main premise of the model is that systematic application of mental techniques will enable young people to optimally develop their mental skills, which in turn, promotes mental qualities (see Figure 2 for an updated version of the model) [63].
Mental skills are different intentional self-regulatory capabilities that young people use to actively manage their cognitive, affective, and behavioural states through the application of mental techniques. Mental techniques are self-directed, repeatable, and trainable methods employed deliberately and effortfully to regulate thoughts, feelings, and behaviours [66,67]. Finally, mental qualities are desired mental states or characteristics obtained because of this self-regulation. These can be intrapersonal qualities, such as confidence, resilience, and self-worth, or interpersonal qualities, such as being able to work in a group, give or receive social support, and develop trust and show respect in others [55]. When linked together in this way, mental techniques, skills, and qualities provide a self-directed process by which MST produces optimal outcomes for young people, including personal growth and well-being [63].
Young people need to develop a range of mental techniques that they can apply to meet the demands of a particular situation and appropriately self-regulate their thoughts, feelings, and behaviours. Let’s take the fictional example of “Lucy” to explain further. Lucy, a young person living in supported accommodation after being asked to leave her family home following months of arguing with her parents. She now needs to earn money to pay her rent but has no previous job experiences and doesn’t feel confident in her ability to come across well in an interview. A mental technique for building Lucy’s confidence is to identify her “signature” character strengths, such as by completing a strengths profile, and then determining how she can use these strengths more in her everyday life [68]. Through self-regulatory processes such as improving self-awareness and planning, Lucy may develop a more optimistic mindset, robust self-confidence, greater self-worth, as well as higher levels of motivation towards applying for a job. In support, Cooley, Quinton, Holland, Parry and Cumming [68] found young people experiencing homelessness were able to identify an average of 10 strengths (e.g., creativity, bravery, perseverance, hope) using a person-centred strengths profiling approach, and these profiles were positively associated with resilience, self-worth, and well-being. Moreover, young people who participated in the research felt that their signature strengths acted as vital protective factors within their lives.
2.2. LifeMatters
LifeMatters is a 10-session games-based life skills programme designed to teach mental skills and prosocial values in a fun, engaging, and interactive manner to adolescents and/or emerging adults who are at least 13 years of age [64,69]. It is sport psychology-informed, takes an asset building approach to PYD, incorporating both self-determination theory [70] and Lerner’s five C’s model of confidence, competence, connection, character, and caring [71]. Sessions are delivered in groups of 12 to 24 participants, with each session lasting approximately 120 minutes and a total of 20 hours of programme time. Certificates are awarded to participants and facilitators trained in the program after completion of the last session.
Sessions focus on teaching mental skills (e.g., activation control, attention and concentration, self-confidence, goal-setting, imagery, and self-talk), prosocial behaviour, team functioning, and problem-solving using group work, discussions, worksheets, and thought-provoking prosocial quotes. By incorporating physically active games, the sessions are designed so that young people can apply the material, work together, and learn from their peers to develop internal assets, personal competencies, and physical and social life skills that can be transferred to other areas of life. Small group discussions are used to encourage participants to reflect on their experiences, including any progress or hinderance to transferring/practicing the skills outside of the programme [69,72].
Aligned with positive youth development [71,73], core aspects of this culturally responsive programme include: (a) the use of trained facilitators who are positive, caring, supportive and who model prosocial behaviour and form bonds with participant; (b) facilitators as supportive mentors with whom participants can relate and trust; and (c) the use of universally understandable and applicable physically active games and psychological skills that are intended to promote skill building, agency, and contribution. An enabling environment (i.e., positive youth development climate) is intentionally created by facilitators so that participants experience a positive and supportive atmosphere that embodies respect, cultural appropriateness, and physical and psychological safety.
To date, LifeMatters has been delivered to, and evaluated with distinct youth samples in geographically and economically diverse countries (Australia, Botswana, Mexico, South Africa, and the USA) [64,72,74,75,76]. Adolescents who have taken part in this programme have reported significant improvements in areas of well-being (e.g., happiness, life satisfaction, self-concept), relatedness, and decreased social anxiety [72,74]. In a recent mixed methods evaluation, LifeMatters was delivered by trained university student facilitators to 28 South African adolescents, aged 13 to 19 years, in a low-resource setting [77]. Compared to the start of the programme, significant improvements were found in personal growth, self-efficacy, self-esteem, and PYD outcomes. It was also evident that participants experienced positive reactions (e.g., found the content enjoyable, connected with the facilitators, would repeat the programme) and learning (e.g., learned mental skills and prosocial values) from the programme. Despite challenges to implementation, such as language differences and negative associations with the use of writing tasks/surveys, the evaluation indicated that both the content and procedures of LifeMatters are relevant and appropriate for use with adolescents in low-resource settings.
Finally, because strengths-based approaches have been criticised for being poorly defined and there being gaps between what is claimed to be strengths-based vs. the reality of what is actually delivered (e.g., programmes that claim to be strengths-based but un-derpinned originate by from a deficit worldview) [35], we have mapped Life Matters to the 6 core ingredients outlined by Rapp, Saleebey and Sullivan [36]. Based on how these have been described in published literature (Table 2), LifeMatters fulfills 3/6 characteristics.
2.3. My Strengths Training for Life™ (MST4Life™)
MST4Life™ is a co-designed, young person-centred, strengths-based, and experiential psychoeducational programme for young people experiencing homelessness aged 16-24 years and living in long-term supported accommodation within the UK [55]. To ensure cultural sensitivity, it was co-designed via a community-academic partnership between a Housing Service and academic researchers [55]. Participants often have poor physical and mental health and other complex and multiple support needs (e.g., substance abuse, pregnant/young parent, involvement with the justice system). They are either not in education, employment, or training (NEET) and eligible to become EET, at risk of falling out of EET, or identified by frontline staff as someone who will potentially benefit from MST4Life™. The group-based activities of the programme are delivered in fun and interactive ways over two phases: (1) Phase 1 involves 10 weekly sessions; and (2) Phase 2 involves a 4 day/3 night trip to an outdoor adventure centre. Activities in Phase 1 are tailored to the specific groups of young people taking part and designed to become progressively more challenging. Phase 2 provides a novel environment for young people to transfer and further develop their mental skills in a novel and challenging setting that also capitalises on the wellbeing benefits associated with nature [78]. Participation in the program also counts towards an accredited life skills training award.
Based on formative work involving a narrative literature review and stakeholder consultation (i.e., 6 focus groups with 15 young people and 18 frontline staff) with the partner Housing Service, the resulting aim of MST4Life™ is to help young people experiencing homelessness to recognise, develop, apply, and transfer use of their mental skills into different contexts, including being more aware of, and better able to set effective goals and plans for achieving them, recognise and use different coping strategies, activate different forms of social support, and work effectively with others [55]. In the short-term, it is expected that young people will increase their intentional self-regulation, evident by their attendance and engagement in programme sessions, and gain intrapersonal and interpersonal mental skills. Together, these changes are predicted to contribute to improved physical, mental, and social health and wellbeing, maintaining accommodation within the service, and reducing risk behaviours. The long-term goal is to support young people to make more positive transitions into independent living (e.g., become EET and a tenant in their own rented flat) and recover from homelessness.
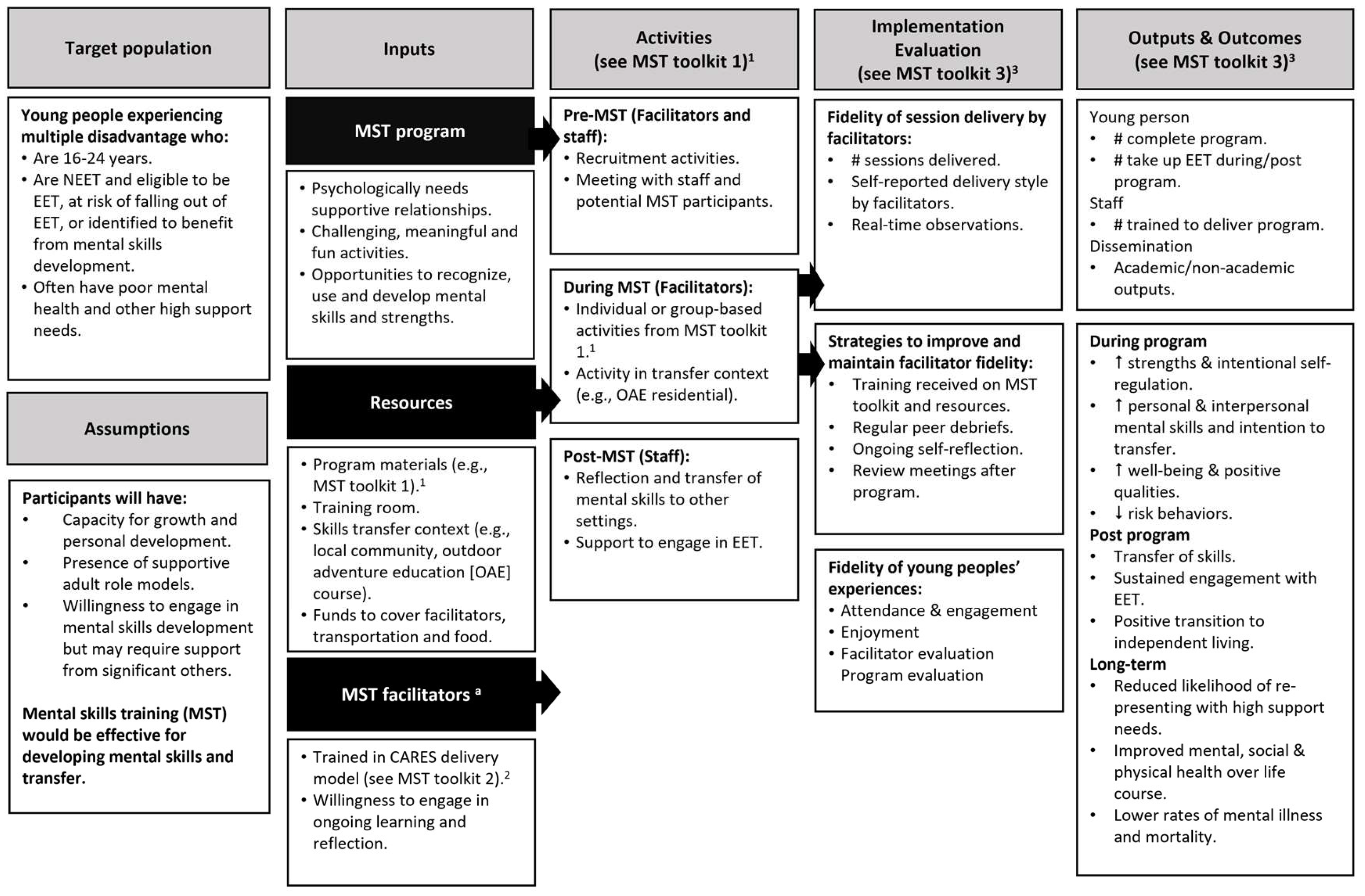
The logic model (Figure 3) and delivery plan for MST4Life™ is underpinned by BPNT [43], PYD [38], SFBT [49,50], and experiential learning approaches (e.g., Kolb’s learning cycle) [79,80]. From a PYD perspective, mental skills are viewed as important assets for optimal development that will serve as intentional self-regulation. Positive affective relationships with caring adults, challenging experiences, and skill-building opportunities are key ingredients of MST4Life™ along with intentional efforts to create a psychologically-informed environment to meet young people’s basic psychological needs for autonomy, relatedness, and competence [43]. Activities are designed to provide young people with fun and meaningful opportunities to learn, practice, and implement self regulation skills in a safe environment where mistakes can be made and there are increasing levels of challenge to ensure mastery experiences. Programme facilitators also encourage young people to notice and self-reflect on the “what, why, and how” of mental skills use to promote meta-cognition and to better manage their thoughts, feelings and behaviours within and across different contexts.
Also based on BPNT [43] and SFBT [85], programme facilitators are trained to deliver MST4Life™ using the bespoke CARES model so that they: (1) demonstrate more psychological need supportive rather than need thwarting behaviours; and (2) focus more on constructing solutions than on identifying problems in a hopeful, caring, friendly, and future-oriented way. Each letter of CARES reflects a different type of behaviour: Competence supportive (e.g., encourage young person to solve problems and make decisions for themselves), Autonomy supportive (e.g., provide meaningful choices), Relatedness and interpersonal involvement (e.g., communication of warmth, friendliness, and acceptance), Engagement through communication (e.g., ask open questions and encourage participation in activities and discussion), and Structure and group management (e.g., giving clear instructions and guidance for activities) [55,86]. In contrast, needs thwarting behaviours that are discouraged include facilitators being critical or negative towards young people, using controlling language, or interrupting the young person while they are speaking [42].
In support of its logic model, outcome evaluation during the programme found that MST4Life™ resulted in young people better recognising and using their strengths, employing both personal and interpersonal mental skills, improved well-being and other psychosocial outcomes (e.g., self-worth, resilience), and sustaining accommodation with the housing service [68,81,87,88,89,90,91]. An economic evaluation showed that improving these outcomes provides UK public sector savings from forgone tax revenues, unemployment benefits and healthcare costs leading to an estimated lifetime savings of £26m for 1,040 young people who exited homelessness in the first three years of project [91].
Process evaluations revealed that young people’s intention to transfer mental skills developed during the programme led to actual transfer of these skills post-programme [87]. Further, MST4Life™ participants also had an increased likelihood of making a positive transition from supported accommodation into independent living by 30 percentage points compared to those who received the typical support provided by the housing service [91]. Young people engaged with, enjoyed and held positive views about both the programme and the facilitators [81,87,90,92]. Fidelity assessments also showed that the programme is being delivered in the intended delivery style (i.e., CARES model), assessed via both self-reported checklists by facilitators and real-time observations of the research team [86]. Moreover, when mapping MST4Life™ to the characteristics of strengths-based approaches [36], this programme was found to incorporate all 6 (Table 2).
Table 2.
Rapp, et al. [93]’s characteristics of strengths-based approaches for LifeMatters and My Strengths Training for Life™ (MST4Life™) programmes.
Table 2.
Rapp, et al. [93]’s characteristics of strengths-based approaches for LifeMatters and My Strengths Training for Life™ (MST4Life™) programmes.
| Characteristics | LifeMatters | MST4Life™ |
|---|---|---|
|
Yes [74,75,77] | Yes [55,62] |
|
Unclear | Yes [55,62,68] |
|
Unclear | Yes [87] |
|
Yes [74] | Yes [55,94] |
|
Yes [77] | Yes [55,86,90] |
|
Unclear1 | Yes [55,90] |
1 LifeMatters is designed to meet the basic psychological need of autonomy through peer-led activities but it is unclear from the programme description as to whether participants are provided with meaningful choices [75].
3. Discussion
This narrative review examined the need for effective strengths-based interventions to improving self-regulation and other life skills in young people aged 16 to 25 facing multiple disadvantages. We contribute to the literature by summarizing research on the impact of trauma and adversity on brain development, particularly in relation to its impact on self-regulation. Recognizing that self-regulation is influenced not only by neurological processes but also by other modifiable factors, there is considerable scope to intervening during this transitional stage of development into adulthood. However, taking a deficit-based approach to this intervention may contribute to stigma and barriers to engagement [33,35].
Instead, a strengths-based approach would focus on recognising and building on young people’s already existing self-regulation capacities to better manage their thoughts, feelings, and behaviours [36]. Viewing young people facing multiple disadvantages as capable of aspirations, learning, personal growth, and demonstrating numerous strengths can foster a more empowering and positive environment. In addressing a gap for suitable strengths-based interventions, two sport psychology-informed programmes (LifeMatters, MST4Life™) have demonstrated improvements in self-regulation and overall well-being [62,76,77,81,87,88,89]. Both programmes focus on enhancing self-regulation and other life skills through an MST approach. Despite these common goals, the programmes also differ in several aspects, including their theoretical underpinnings, the extent of strengths-based components, and evaluation approaches.
LifeMatters and MST4Life™ are grounded in PYD and BPNT, with MST4Life™ also incorporating aspects of SFBT to guide the delivery style of its facilitators. PYD is a large focus of each programme, with both aiming to promote personal growth and thriving through the five C’s of confidence, competence, connection, character, and caring [77,88]. In more detail, competence is fostered through developing specific skills such as goal-setting and problem-solving. Each programme uses an experiential approach so that participants learn through engaging in activities designed to challenge them appropriately and allowing them to experience success, thereby boosting their competence. Through an enabling atmosphere informed by BPNT and the use of group activities, young people are able to build connections such as with oneself, peers, programme facilitators, and even nature such as through the outdoor adventure component of MST4Life™ [88]. Aligned with character, LifeMatters and MST4Life™ both include value-based activities that encourage participants to reflect on their values, behaviours, and goals and to show respect for oneself and others [88]. For example, LifeMatters includes prosocial messages/thoughts of the day that are sung together as a group and facilitators also encourage participants to create their own prosocial messages aligned with the prosocial values of the programme [77]. Confidence is enhanced by facilitators giving regular positive feedback and reinforcement, such as by highlighting young people’s strengths and accomplishments. Further, programme activities are designed to empower young people to set and achieve personal goals, which reinforces a sense of self-worth and confidence in their abilities [55]. Finally with regards to caring, both programmes train facilitators to be caring role models for young people. The group-based activities also afford participants the opportunity to develop leadership and teamwork skills and learn the value of being considerate towards others [88].
While both programs have used qualitative methods to provide evidence of its incorporation of the 5 Cs [88,95], LifeMatters has also incorporated the Positive Youth Development Short Form (PYD-SF) for Older Adolescents to assess the five Cs of PYD [71,96]. Improvements in character, competence, and confidence were reported after 10 sessions of LifeMatters were delivered over 5 weeks to 28 South African adolescents [77]. However, the researchers found that the forced-choice question format of the PYD-SF was unfamiliar to participants and led to errors and non-completion. The acceptability and feasibility of this type of measurement tool may therefore need further consideration before wider scale evaluation takes place in cultural settings different from that in which the questionnaire was initially developed (i.e., United States of America). Future evaluation of both programmes would benefit from empirically establishing links between the 5 Cs (as well as BPNT and SFBT) and the outcomes achieved, as well as to determine if these relationships vary according to participant characteristics. This would be important to check because recent research has shown differing relationships between the 5 Cs and risk behaviours (e.g., substance abuse, online betting) for Spanish male and female emerging adults [97]. Better understanding of these relationships would help to inform developments to, as well as the delivery and evaluation of LifeMatters and MST4Life™, as well as provide support for the theoretical underpinning and approaches used.
A further contribution of this review is in response to critique that it is not always clear how strengths-based approaches are implemented [35]. We therefore mapped both programmes to the six characteristics of strengths-based approaches outlined by Rapp, Saleebey and Sullivan [36]. LifeMatters integrates being goal orientated, encouraging the use of strengths, and building hope-inducing relationships. In addition to these characteristics present in LifeMatters, MST4Life™ also systematically assesses young people’s strengths by employing an idiographic (person-centered) tool called ‘strengths profiling,’ and promotes reflection on the use of these strengths in new ways. It also views the enviornment as a rich resource as well as providing regular opportunities for participants to make meaningful choices about the programme, such as the specific activities that are included. It is possible that LifeMatters also incorporates all six characteristics, but this has not yet been fully reported in its publications to date. What is also not yet established is the extent to which each of these core characteristics contribute to the outcomes being achieved by both programmes. In other words, are all six equally important or are some characteristics more important than others? For example, strengths-profiling is used in MST4Life™ as a structured tool that helps young people to identify and reflect on their strengths in personally meaningful ways, and this has been empirically shown to enhance resilience, self-worth, and well-being [68]. But evaluation has not yet been done to show whether increased self-awareness is a necessary precursor to encouraging young people to use their strengths. Doing so would be useful for informing future developments to LifeMatters, MST4Life™, as well as other similar strengths-based approaches aimed at improving self-regulation in young people experiencing multiple disadvantages.
While both programmes use a mixture of data sources including facilitator observations, participant reflections, as well as pre- and post-programme surveys, MST4Life™ also uses a detailed logic model to guide implementation and evaluation (Figure 3) [55,81]. Cumming, Whiting, Parry, Clarke, Holland, Cooley and Quinton [55] explained that this logic model is used for describing core elements of programme content and delivery as well as visually display how the programme is intended to work. This helps to serve as an overarching guide but is not intended to be rigid or prescriptive. Instead, the MST4Life™ logic model is iterative and fluid so it can continually meet the changing needs or circumstances of those it is intended to benefit. Evaluation of this programme is also structured by the New World Kirkpatrick model [98] to cover four different levels: reaction (i.e., participants’ responses to the programme), learning (i.e., the extent to which intended learning has been achieved), behaviour (i.e., behavioural changes from participating), and results (i.e., the impact of the programme) [81]. Although evaluation of LifeMatters and MST4Life™ have reported that participants find both these programmes to be enjoyable, Quinton, Tidmarsh, Parry and Cumming [81] showed that such positive reactions is associated with greater levels of programme engagement in MST4Life™. Moreover, greater enjoyment predicted learning outcomes (i.e., goal-setting, problem solving, time management, and emotion regulation), and this was mediated by participants’ intention to transfer the mental skills they had developed once the programme had finished. In other words, having a logic model and evaluation framework has guided researchers towards establishing the empirical support for some of the proposed mechanisms to determine whether MST4Life™ works as intended.
This narrative review is strengthened by its integration of literature across a number of research areas, enabling us to offer new ideas for how services can support young people facing multiple disadvantages. Because this is not a systematic review, we are not able to provide an evidenced-based synthesis or definitive guidelines [99]. But, as more evidence is published for these types of interventions, it would then become appropriate to conduct a systematic review and meta-analysis. Regardless, the review has implications for policy makers, commissioners, program planners, as well as researchers who are intending to develop, deliver, and/or evaluate programmes for young people facing multiple disadvantages. LifeMatters and MST4Life™ were chosen as the focus of this review because these represent two of the most evaluated strengths-based MST programmes for disadvantaged young people to date. But it does mean that we may have overlooked similar programmes that also offer insights into what works vs. doesn’t for this population. Further, there is much scope for strengthening the evidence-base by replicating and further scaling up and out both LifeMatters and MST4Life™. Although MST4Life™ has focused specifically on young people experiencing homelessness in the UK, future research could investigate its feasibility and acceptability for other multiply disadvantaged young people within the UK or in other countries, such as those with a history of ACEs, those who have been excluded from school and/or leaving care, young offenders or justice-involved youth, and NEET young people with mental health problems [55]. In contrast, LifeMatters has been delivered to disadvantaged youth in geographically and economically diverse countries such as Australia, Botswana, Mexico, South Africa, and the USA [64,72,74,75]. However, the evaluations for LifeMatters have so far been conducted with relatively small samples and lacks longer term follow-up measures to determine if post-programme changes have been maintained. Moreover, both LifeMatters and MST4Life™ have adopted non-experimental approaches and lacked control groups as compared to using standardized randomized control trials (RCTs). As pointed out by Quinton, Clarke, Parry and Cumming [89], while a RCT may mitigate placebo effect, positive outcomes due to increased contact time, or self-selection effects, non-RCT approaches offers other advantages including being able to to tailor the intervention to account for contextual characteristics or to better capitalise on local resources. In other words, researchers may need to carefully consider the trade-off between internal vs. ecological and external validity when choosing their evaluation design and to determine what would be most suitable for the context in which these programmes are being developed and delivered.
From a policy perspective, it is important to point out that while strengths-based approaches appear beneficial, services must also navigate the criticism that these approaches align too closely with neoliberal notions of self-help and individual responsibility, and overlook the structural inequalities that contribute to hardship and distress in young people [35]. For instance, young people experiencing homelessness face systemic barriers such as stigma and limited access to mental health support and affordable housing. However, strengths-based approaches can be part of larger structural actions to address these inequalities. MST4Life™, for example, is integrated within a whole-organisational approach to being a psychologically-informed environment and addressing inequalities are considered within its program design [55].
4. Conclusions
To support positive youth development, MST is a strengths-based, flexible and adaptable approach to filling the shortage of available evidence-based programs for youths facing multiple disadvantages. It appears to be a promising approach for engaging this group and improving self-regulation and well-being based on the evidence so far published for LifeMatters and MST4Life™. But further research is needed to uncover the specific mechanisms that are contributing to these and other reported outcomes. The findings of this review nevertheless point to the value of adopting a strengths-based, rather than deficits-based approach, and may facilitate policy makers, commissioners, program planners, and researchers in the development, delivery, and evaluation of MST or similar psychoeducational approaches in future.
Author Contributions
Conceptualization, J.C., M.L.Q., and G.T.; writing—original draft preparation, J.C., M.L.Q., G.T., and S.R.; writing—review and editing, J.C., M.L.Q., G.T., and S.R.; funding acquisition, J.C. and M.Q. All authors have read and agreed to the published version of the manuscript.
Funding
Financial support for this research was provided by St Basils (registered charity number: 1,080,154) and The Cook and Wolstenholme Charitable Trust (registered charity number: 1,091,984).
Institutional Review Board Statement
Not applicable for a review.
Informed Consent Statement
Not applicable for a review.
Data Availability Statement
Not applicable for a review.
Acknowledgments
We thank the staff and young people from St Basils for their ongoing contributions and support as well as staff from the University of Birmingham’s Development and Alumni Relations Office for their support in acquiring charitable funding for the research.
Conflicts of Interest
St Basils was the community partner in this research and was involved in the development and delivery of the MST4Life™ program. The funders had no role in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- Moreton, R.; Welford, J.; Collinson, B.; Greason, L.; Milner, C. Improving access to mental health services for those experiencing multiple disadvantage. Housing, Care and Support 2022. [CrossRef]
- Sandu, R.D. Defining severe and multiple disadvantage from the inside: Perspectives of young people and of their support workers. Journal of Community Psychology 2021, 49, 1470–1486. [Google Scholar] [CrossRef] [PubMed]
- Rankin, J.; Regan, S. Meeting complex needs: The future of social care; London, UK, 2004.
- Bramley, G.; Fitzpatrick, S. Hard Edges: Mapping severe and multiple disadvantage; London, UK, 2015.
- Moreton, R.; Welford, J.; Howe, P. Evaluation of Fulfilling Lives: Why we need to invest in multiple disadvantage; 2021.
- Prince, D.M.; Rocha, A.; Nurius, P.S. Multiple disadvantage and discrimination: Implications for adolescent health and education. Social Work Research 2018, 42, 169–179. [Google Scholar] [CrossRef] [PubMed]
- Centrepoint. Summary report: The youth homeless databank 2022-2023; London, UK, 2023.
- Homeless Link. We have a voice, follow our lead: Young and homeless 2020; Homeless Link: London, UK, 2020. [Google Scholar]
- Homeless Link. Young & Homeless 2018; Homeless Link: London, UK, 2018. [Google Scholar]
- Bevington, D.; Fuggle, P.; Fonagy, P. Applying attachment theory to effective practice with hard-to-reach youth: the AMBIT approach. Attachment & Human Development 2015, 17, 157–174. [Google Scholar] [CrossRef]
- Cameron, L.D.; Carroll, P.; Hamilton, W.K. Evaluation of an intervention promoting emotion regulation skills for adults with persisting distress due to adverse childhood experiences. Child Abuse & Neglect 2018, 79, 423–433. [Google Scholar] [CrossRef]
- Dowding, K.; Murphy, D.; Everitt, G.; Tickle, A. Use of one-to-one psychotherapeutic interventions for people experiencing severe and multiple disadvantages: An evaluation of two regional pilot projects. Counselling and Psychotherapy Research 2022. [Google Scholar] [CrossRef]
- Hauser, M.D. How early life adversity transforms the learning brain. Mind, Brain, and Education 2021, 15, 35–47. [Google Scholar] [CrossRef]
- Blakemore, S.-J.; Robbins, T.W. Decision-making in the adolescent brain. Nature Neuroscience 2012, 15, 1184–1191. [Google Scholar] [CrossRef] [PubMed]
- Blakemore, S.J.; Choudhury, S. Development of the adolescent brain: implications for executive function and social cognition. Journal of Child Psychology and Psychiatry 2006, 47, 296–312. [Google Scholar] [CrossRef] [PubMed]
- Brindle, R.C.; Pearson, A.; Ginty, A.T. Adverse childhood experiences (ACEs) relate to blunted cardiovascular and cortisol reactivity to acute laboratory stress: A systematic review and meta-analysis. Neuroscience & Biobehavioral Reviews 2022, 134. [Google Scholar]
- Shonkoff, J.P.; Garner, A.S.; Child, C.o.P.A.o.; Family Health, C.o.E.C. , Adoption,; Dependent Care; Developmental, S.o.; Pediatrics, B.; Siegel, B.S.; Dobbins, M.I.; Earls, M.F.; et al. The lifelong effects of early childhood adversity and toxic stress. Pediatrics 2012, 129, e232–e246. [Google Scholar] [CrossRef] [PubMed]
- Felitti, V.J. Adverse childhood experiences and adult health. Academic pediatrics 2009, 9, 131–132. [Google Scholar] [CrossRef] [PubMed]
- Hackman, D.A.; Farah, M.J.; Meaney, M.J. Socioeconomic status and the brain: mechanistic insights from human and animal research. Nature reviews. Neuroscience 2010, 11, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Murray, D.W.; Rosanbalm, K.; Christopoulos, C.; Hamoudi, A. Self-regulation and toxic stress: Foundations for understanding self-regulation from an applied developmental perspective; Office of Planning, Research and Evaluation, Administration for Children and Families, U.S. Department of Health and Human Services: Washington, DC, 2015. [Google Scholar]
- McEwen, B.S.; Gianaros, P.J. Central role of the brain in stress and adaptation: Links to socioeconomic status, health, and disease: Central links between stress and SES. Annals of the New York Academy of Sciences 2010, 1186, 190–222. [Google Scholar] [CrossRef] [PubMed]
- Willingham, D.T. Ask the cognitive scientist: Why does family wealth affect learning? American Educator 2012, 36, 33–39. [Google Scholar]
- Eldesouky, L.; Gross, J.J. Emotion regulation goals: An individual difference perspective. Social and Personality Psychology Compass 2019, 13, e12493. [Google Scholar] [CrossRef]
- Gestsdottir, S.; Lerner, R.M. Positive development in adolescence: The development and role of intentional self-regulation. Human Development 2008, 51, 202–224. [Google Scholar] [CrossRef]
- Rapp-Paglicci, L.; Stewart, C.; Rowe, W. Can a self-regulation skills and cultural arts program promote positive outcomes in mental health symptoms and academic achievement for at-risk youth? Journal of Social Service Research 2011, 37, 309–319. [Google Scholar] [CrossRef]
- Sahranavard, S.; Miri, M.R.; Salehiniya, H. The relationship between self-regulation and educational performance in students. J Educ Health Promot 2018, 7, 154. [Google Scholar] [CrossRef] [PubMed]
- Palmer, L.; Richardson, E.W.; Goetz, J.; Futris, T.G.; Gale, J.; DeMeester, K. Financial self-efficacy: mediating the association between self-regulation and financial management behaviors. Journal of Financial Counseling and Planning 2021, 32, 535–549. [Google Scholar] [CrossRef]
- Moffitt, T.E.; Arseneault, L.; Belsky, D.; Dickson, N.; Hancox, R.J.; Harrington, H.; Houts, R.; Poulton, R.; Roberts, B.W.; Ross, S. A gradient of childhood self-control predicts health, wealth, and public safety. Proceedings of the national Academy of Sciences 2011, 108, 2693–2698. [Google Scholar] [CrossRef]
- Compas, B.E.; Connor-Smith, J.K.; Saltzman, H.; Thomsen, A.H.; Wadsworth, M.E. Coping with stress during childhood and adolescence: problems, progress, and potential in theory and research. Psychological bulletin 2001, 127, 87. [Google Scholar] [CrossRef] [PubMed]
- Wadsworth, M.E. Development of maladaptive coping: A functional adaptation to chronic, uncontrollable stress. Child Development Perspectives 2015, 9, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Evans, G.W.; Kim, P. Childhood poverty and young adults’ allostatic load: The mediating role of childhood cumulative risk exposure. Psychological science 2012, 23, 979–983. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.R.; Shogren, K.A.; Wehmeyer, M.L. Supports and support needs in strengths-based models of intellectual disability. In Handbook of Research-Based Practices for Educating Students with Intellectual Disability, 1st ed.; Shogren, K.A., Ed.; Routledge: New York, NY, 2016; pp. 39–57. [Google Scholar]
- Sweeney, A.; Filson, B.; Kennedy, A.; Collinson, L.; Gillard, S. A paradigm shift: relationships in trauma-informed mental health services. BJPsych advances 2018, 24, 319–333. [Google Scholar] [CrossRef] [PubMed]
- Magwood, O.; Leki, V.Y.; Kpade, V.; Saad, A.; Alkhateeb, Q.; Gebremeskel, A.; Rehman, A.; Hannigan, T.; Pinto, N.; Sun, A.H. Common trust and personal safety issues: a systematic review on the acceptability of health and social interventions for persons with lived experience of homelessness. PloS one 2019, 14, e0226306. [Google Scholar] [CrossRef] [PubMed]
- Caiels, J.; Milne, A.; Beadle-Brown, J. Strengths-based approaches in social work and social care: Reviewing the evidence. Journal of Long Term Care 2021, 401–422. [Google Scholar] [CrossRef]
- Rapp, C.A.; Saleebey, D.; Sullivan, W.P. The future of strengths-based social work. Advances in Social Work 2006, 6, 79–90. [Google Scholar] [CrossRef]
- Morgan, A.; Ziglio, E. Revitalising the evidence base for public health: An assets model. Promotion & Education 2007, 14, 17–22. [Google Scholar]
- Lerner, R.M. The positive youth development perspective: Theoretical and empirical bases of strengths-based approach to adolescent development. In Oxford Handbook of Positive Psychology, 2nd ed.; Lopez, S.J., Snyder, C.R., Eds.; Oxford University Press: Oxford, 2009; pp. 149–163. [Google Scholar]
- Grant, J.G.; Cadell, S. Power, pathological worldviews, and the strengths perspective in social work. Families in Society 2009, 90, 425–430. [Google Scholar] [CrossRef]
- Scerra, N. Scerra, N. Strengths-based practices: An overview of the evidence. Developing Practice: The Child, Youth and Family Work Journal 2012, 43-52.
- Simmons, C.A.; Shapiro, V.B.; Accomazzo, S.; Manthey, T.J. Strengths-based social work: A meta-theory to guide social work research and practice. In Theoretical Perspectives for Direct Social Work Practice, 3rd ed.; Coady, N., Lehmann, P., Eds.; Springer: New York, NY, 2016. [Google Scholar]
- Bartholomew, K.J.; Ntoumanis, N.; Ryan, R.M.; Bosch, J.A.; Thøgersen-Ntoumani, C. Self-determination theory and diminished functioning: The role of interpersonal control and psychological need thwarting. Personality and social psychology bulletin 2011, 37, 1459–1473. [Google Scholar] [CrossRef] [PubMed]
- Deci, E.L.; Ryan, R.M. Self-determination research: Reflections and future directions. In Handbook of Self-Determination Research, Deci, E.L., Ryan, R.M., Eds.; University of Rochester Press: 2002; pp. 431–441.
- Ryan, R.M.; Deci, E.L. The darker and brighter sides of human existence: Basic psychological needs as a unifying concept. Psychological inquiry 2000, 11, 319–338. [Google Scholar] [CrossRef]
- Vansteenkiste, M.; Ryan, R.M.; Soenens, B. Basic psychological need theory: Advancements, critical themes, and future directions. Motivation and Emotion 2020, 44, 1–31. [Google Scholar] [CrossRef]
- Franklin, C.; Ding, X.; Kim, J.; Zhang, A.; Hai, A.H.; Jones, K.; Nachbaur, M.; O’Connor, A. Solution-focused brief therapy in community-based services: A meta-analysis of randomized controlled studies. Research on Social Work Practice 2024, 34, 265–277. [Google Scholar] [CrossRef]
- Coulter, S. The applicability of two strengths-based systemic psychotherapy models for young people following Type 1 Trauma. Child Care in Practice 2014, 20, 48–63. [Google Scholar] [CrossRef]
- Joubert, J.; Guse, T. A solution-focused brief therapy (SFBT) intervention model to facilitate hope and subjective well-being among trauma survivors. Journal of Contemporary Psychotherapy 2021, 51, 303–310. [Google Scholar] [CrossRef]
- Ratner, H.; George, E.; Iveson, C. Solution focused brief therapy: 100 key points and techniques; Routledge: Hove, East Sussex, 2012. [Google Scholar]
- de Shazer, S.; Dolan, Y.; Korman, H.; Trepper, T.; McCollum, E.; Kim Berg, I. More than miracles: The state of the art of solution-focused brief therapy, 2nd ed.; Routledge: New York, 2021; p. 200. [Google Scholar]
- Gestsdóttir, S.; Urban, J.B.; Bowers, E.P.; Lerner, J.V.; Lerner, R.M. Intentional self-regulation, ecological assets, and thriving in adolescence: A developmental systems model. New Directions for Child and Adolescent Development 2011, 2011, 61–76. [Google Scholar] [CrossRef] [PubMed]
- Gestsdóttir, S.; Geldhof, G.J.; Lerner, J.V.; Lerner, R.M. What drives positive youth development? Assessing intentional self-regulation as a central adolescent asset. International Journal of Developmental Science 2017, 11, 69–79. [Google Scholar] [CrossRef]
- Napolitano, C.M.; Bowers, E.P.; Gestsdóttir, S.; Chase, P.A. The development of intentional self-regulation in adolescence: Describing, explaining, and optimizing its link to positive youth development. In Advances in Child Development and Behavior, Lerner, R.M., Lerner, J.V., Benson, J.B., Eds.; JAI: 2011; Volume 41, pp. 19–38.
- Tidmarsh, G.; Thompson, J.L.; Quinton, M.L.; Cumming, J. Process evaluations of positive youth development programmes for disadvantaged young people: A systematic review. Journal of Youth Development 2022, 17, 106–140. [Google Scholar] [CrossRef]
- Cumming, J.; Whiting, R.; Parry, B.J.; Clarke, F.J.; Holland, M.J.G.; Cooley, S.J.; Quinton, M.L. The My Strengths Training for Life program: Rationale, logic model, and description of a strengths-based intervention for young people experiencing homelessness. Evaluation and Program Planning 2022, 91, 102045. [Google Scholar] [CrossRef] [PubMed]
- Vealey, R. Future directions in psychological skills training. The Sport Psychologist 1998, 2. [Google Scholar] [CrossRef]
- Orlick, T. Pursuit of Excellence, 5th ed.; Human Kinetics: Champaign, IL, 2016. [Google Scholar]
- Estanol, E.; Shepherd, C.; MacDonald, T. Mental skills as protective sttributes against eating disorder risk in dancers. Journal of Applied Sport Psychology 2013, 25, 209–222. [Google Scholar] [CrossRef]
- Golby, J.; Wood, P. The effects of psychological skills training on mental toughness and psychological well-being of student-athletes. Psychology 2016, 07, 901–913. [Google Scholar] [CrossRef]
- Danish, S.J.; Forneris, T.; Wallace, I. Sport-based life skills programming in the schools. Journal of Applied School Psychology 2005, 21, 41–62. [Google Scholar] [CrossRef]
- Sharp, L.-A.; Woodcock, C.; Holland, M.J.G.; Cumming, J.; Duda, J.L. A qualitative evaluation of the effectiveness of a mental skills training program for youth athletes. The Sport Psychologist 2013, 27, 219–232. [Google Scholar] [CrossRef]
- Cumming, J.; Clarke, F.J.; Holland, M.J.G.; Parry, B.J.; Quinton, M.L.; Cooley, S.J. A feasibility study of the My Strengths Training for Life (MST4Life) Program for young people experiencing homelessness. International Journal of Environmental Research and Public Health 2022, 19. [Google Scholar] [CrossRef] [PubMed]
- Holland, M.J.G.; Cooley, S.J.; Cumming, J. Understanding and assessing young athletes’ psychological needs. In Sport psychology for young athletes, 1st ed.; Knight, C.J., Harwood, C.G., Gould, D., Eds.; Routledge: London, 2017. [Google Scholar]
- Hanrahan, S.J. LifeMatters: Using physical activities and games to enhance the self-concept and well-being of disadvantaged youth. In Positive Psychology in Sport and Physical Activity, 1st ed.; Brady, A., Grenville-Cleave, B., Eds.; Routledge: London, 2017; Volume 7, pp. 170–181. [Google Scholar]
- Fisher, R. Thinking about thinking: Developing metacognition in children. Early Child Development and Care 1998, 141, 1–15. [Google Scholar] [CrossRef]
- Holland, M.J.; Woodcock, C.; Cumming, J.; Duda, J.L. Mental qualities and employed mental techniques of young elite team sport athletes. Journal of Clinical Sport Psychology 2010, 4, 19–38. [Google Scholar] [CrossRef]
- Vealey, R. Mental skills training in sport. In Handbook of Sport Psychology, 3 ed.; Tenenbaum, G., Eklund, R., Eds.; John Wiley and Sons: Chichester, 2007; pp. 287–309. [Google Scholar]
- Cooley, S.J.; Quinton, M.L.; Holland, M.J.G.; Parry, B.J.; Cumming, J. The experiences of homeless youth when using strengths profiling to identify their character strengths. Frontiers in Psychology 2019, 10. [Google Scholar] [CrossRef]
- Hanrahan, S.J. Using games to enhance life satisfaction and self-worth of orphans, teenagers living in poverty, and ex-gang members in Latin America. In Case studies in sport development: Contemporary stories promoting health, peace and social justice, Schinke, R.J., Lidor, R., Eds.; Fitness Information Technology: Morgantown, WV, 2013; pp. 89–101. [Google Scholar]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychol 2000, 55, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Lerner, R.M.; Lerner, J.V.; Almerigi, J.B.; Theokas, C.; Phelps, E.; Gestsdóttir, S.; Naudeau, S.; Jelicic, H.; Alberts, A.; Ma, L.; et al. Positive youth development, participation in community youth development programs, and community contributions of fifth-grade adolescents: Findings from the first wave of the 4-H study of positive youth development. The Journal of Early Adolescence 2005, 25, 17–71. [Google Scholar] [CrossRef]
- Hanrahan, S.J.; Francke Ramm, M.D.L. Improving life satisfaction, self-concept, and happiness of former gang members using games and psychological skills training. Journal of Sport for Development 2015, 3, 41–47. [Google Scholar]
- Catalano, R.F.; Skinner, M.L.; Alvarado, G.; Kapungu, C.; Reavley, N.; Patton, G.C.; Jessee, C.; Plaut, D.; Moss, C.; Bennett, K.; et al. Positive youth development programs in low- and middle-income countries: A conceptual framework and systematic review of efficacy. J Adolesc Health 2019, 65, 15–31. [Google Scholar] [CrossRef] [PubMed]
- McMahon, M.G.; Hanrahan, S.J. Life Matters: Exploring the influence of games and mental skills on relatedness and social anxiety levels in disengaged adolescent students. Journal of Applied Sport Psychology 2019, 32, 205–219. [Google Scholar] [CrossRef]
- Hanrahan, S.J.; Tshube, T. Developing Batswana coaches’ competencies through the LifeMatters programme: Teaching mental skills through games. Botswana Notes and Records 2018, 50, 189–198. [Google Scholar]
- Page, D.; Hanrahan, S.; Buckley, L. Positive youth development program for adolescents with disabilities: A pragmatic trial. International Journal of Disability, Development and Education 2024, 71, 451–467. [Google Scholar] [CrossRef]
- Page, D.T.; Hanrahan, S.; Buckley, L. Real-world trial of positive youth development program “LifeMatters” with South African adolescents in a low-resource setting. Children and Youth Services Review 2023, 146, 106818. [Google Scholar] [CrossRef]
- Mygind, L.; Kjeldsted, E.; Hartmeyer, R.; Mygind, E.; Bølling, M.; Bentsen, P. Mental, physical and social health benefits of immersive nature-experience for children and adolescents: A systematic review and quality assessment of the evidence. Health & Place 2019, 58, 102136. [Google Scholar]
- Dewey, J. Dewey, J. Experience and Education; Macmillian: New York, NY, 1963 (Original work published 1938).
- Kolb, D.A. Experiential learning: Experience as the source of learning and development.; Prentice-Hall: Englewood Cliffs, New Jersey, 1984. [Google Scholar]
- Quinton, M.L.; Tidmarsh, G.; Parry, B.J.; Cumming, J. A Kirkpatrick Model Process Evaluation of Reactions and Learning from My Strengths Training for Life™. International Journal of Environmental Research and Public Health 2022, 19. [Google Scholar] [CrossRef] [PubMed]
- Parry, B.J.; Quinton, M.; Cumming, J. Mental skills training toolkit: A resource for strengths-based development; University of Birmingham, 2020.
- Quinton, M.; Parry, B.J.; Cumming, J. Mental skills training toolkit: Ensuring psychologically informed delivery; University of Birmingham, 2020.
- Clarke, F.J.; Parry, B.J.; Quinton, M.; Cumming, J. Mental skills training commissioning and evaluation toolkit: Improving outcomes in young people experiencing homelessness; University of Birmingham, 2020.
- Lethem, J. Brief Solution Focused Therapy. Child and Adolescent Mental Health 2002, 7, 189–192. [Google Scholar] [CrossRef] [PubMed]
- Tidmarsh, G.; Whiting, R.; Thompson, J.L.; Cumming, J. Assessing the fidelity of delivery style of a mental skills training programme for young people experiencing homelessness. Evaluation and Program Planning 2022, 94, 102150. [Google Scholar] [CrossRef] [PubMed]
- Parry, B.J.; Quinton, M.L.; Holland, M.J.G.; Thompson, J.L.; Cumming, J. Improving outcomes in young people experiencing homelessness with My Strengths Training for Life (TM) (MST4Life (TM)): A qualitative realist evaluation. Children and Youth Services Review 2021, 121. [Google Scholar] [CrossRef]
- Parry, B.J.; Thompson, J.L.; Holland, M.J.G.; Cumming, J. Promoting personal growth in young people experiencing homelessness through an outdoors-based program. Journal of Youth Development 2021, 16, 157–192. [Google Scholar] [CrossRef]
- Quinton, M.L.; Clarke, F.J.; Parry, B.J.; Cumming, J. An evaluation of My Strengths Training for Life for improving resilience and well-being of young people experiencing homelessness. J Community Psychol 2021, 49, 1296–1314. [Google Scholar] [CrossRef] [PubMed]
- Tidmarsh, G.; Thompson, J.L.; Quinton, M.L.; Parry, B.J.; Cooley, S.J.; Cumming, J. A platform for youth voice in MST4Life: A vital component of process evaluations. Sport and Exercise Psychology Review 2022, 17, 73–86. [Google Scholar] [CrossRef]
- Jabbour, L.; Siu, J. Outcome and economic evaluation of the My Strengths Training for Life™ programme with St Basils; University of Birmingham: 2019.
- Cumming, J.; Clarke, F.J.; Holland, M.J.G.; Parry, B.J.; Quinton, M.L.; Cooley, S.J. A Feasibility Study of the My Strengths Training for Life™ (MST4Life™) Program for Young People Experiencing Homelessness. International Journal of Environmental Research and Public Health 2022, 19. [Google Scholar] [CrossRef] [PubMed]
- Rapp, C.A.; Saleebey, D.; Sullivan, W.P. The future of strengths-based social work. Advances in social work: Special issue on the futures of social work 2006, 6, 79–90. [Google Scholar] [CrossRef]
- Quinton, M.L.; Tidmarsh, G.; Parry, B.J.; Cumming, J. A Kirkpatrick model process evaluation of reactions and learning from my strengths training for life™. International Journal of Environmental Research and Public Health 2022, 19, 11320. [Google Scholar] [CrossRef] [PubMed]
- Page, D.T. The LifeMatters program implemented in South Africa. The University of Queensland, 2022.
- Geldhof, G.J.; Bowers, E.P.; Boyd, M.J.; Mueller, M.K.; Napolitano, C.M.; Schmid, K.L.; Lerner, J.V.; Lerner, R.M. Creation of short and very short measures of the Five Cs of Positive Youth Development. Journal of Research on Adolescence 2014, 24, 163–176. [Google Scholar] [CrossRef]
- Gomez-Baya, D.; Martin-Barrado, A.D.; Muñoz-Parralo, M.; Roh, M.; Garcia-Moro, F.J.; Mendoza-Berjano, R. The 5Cs of positive youth development and risk behaviors in a sample of spanish emerging adults: A partial mediation analysis of gender differences. European Journal of Investigation in Health, Psychology and Education 2023, 13, 2410–2427. [Google Scholar] [CrossRef] [PubMed]
- Kirkpatrick, J.; Kirkpatrick, W. An introduction to the new world Kirkpatrick model. Available online: https://www.kirkpatrickpartners.com/wp-content/uploads/2021/11/Introduction-to-The-New-World-Kirkpatrick%C2%AE-Model.pdf (accessed on 12 July 2024).
- Sukhera, J. Narrative reviews: Flexible, rigorous, and practical. Journal of Graduate Medical Education 2022, 14, 414–417. [Google Scholar] [CrossRef] [PubMed]
| 1 | Abbreviations: MST, mental skills training; MST4Life™, My Strengths Training™ for Life; ACEs, adverse childhood experiences; SFBT, solution-focused brief therapy; PYD, positive youth development; HPA, hypothalamic-pituitary-adrenal; SDT, Self-determination theory; BPNT, basic psychological needs theory; NEET, not in education, employment, or training; EET, education, employment, or training; CARES, Competence, Autonomy, Relatedness, Engagement, Structure; PYD-SF, Positive Youth Development Short Form; RCT, randomised control trial. |
Figure 1.
A continuum of self-regulation for supporting young people experiencing multiple disadvantages.
Figure 1.
A continuum of self-regulation for supporting young people experiencing multiple disadvantages.
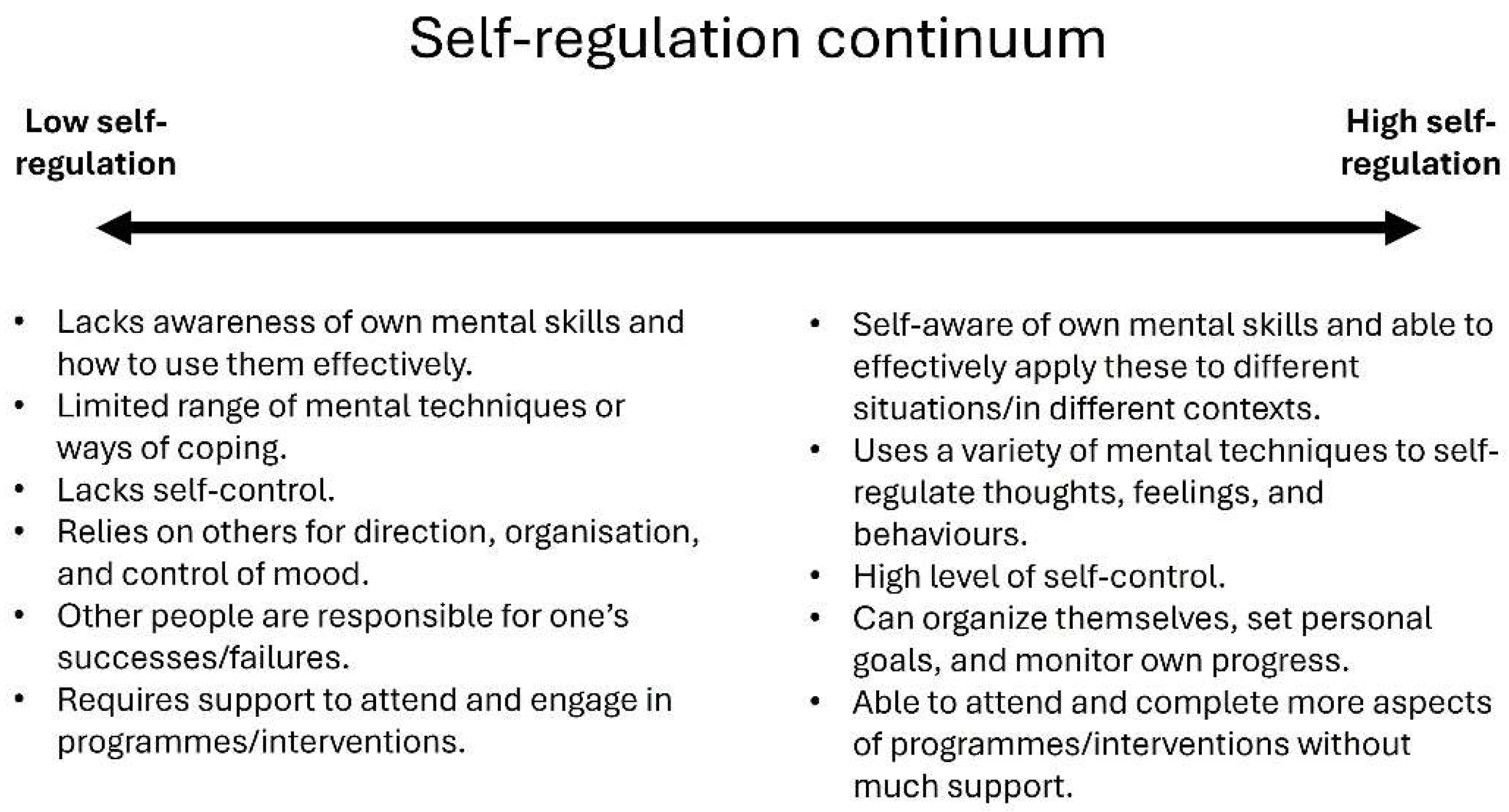
Figure 2.
Updated conceptual process model of youth mental skills training.
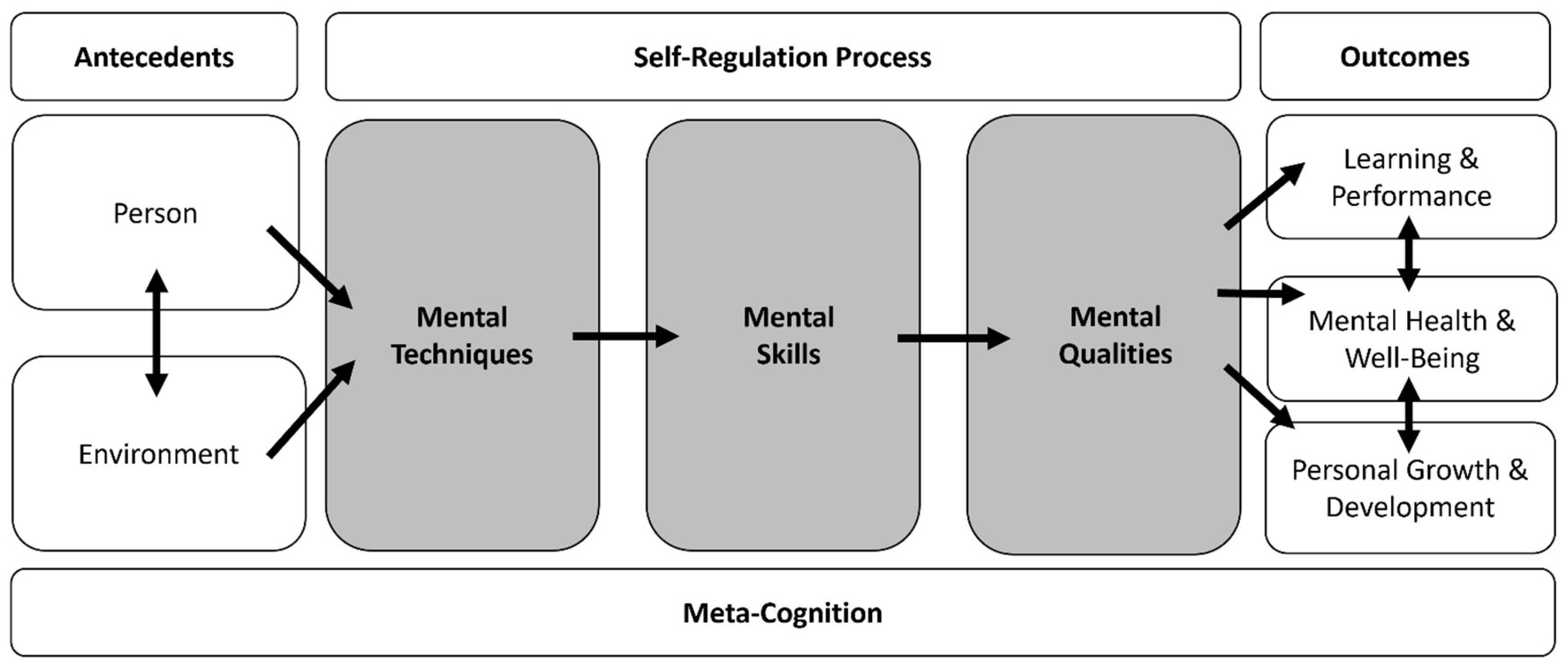
Figure 3.
Logic model of mental skills training for young people experiencing multiple disadvantage. Adapted from Quinton, et al. [81] with permission. Note. a “Staff” refers to significant others who are actively involved in the young persons’ support and development (e.g., housing service staff, support workers/progression coaches). Depending on the context, these staff may also be those acting as MST facilitators. 1MST toolkit 1 (strengths-based activities) [82]; 2MST toolkit 2—psychologically informed delivery [83], 3MST toolkit 3—strengths-based evaluation [84]. Toolkits are available to download from www.sprintproject.org.
Figure 3.
Logic model of mental skills training for young people experiencing multiple disadvantage. Adapted from Quinton, et al. [81] with permission. Note. a “Staff” refers to significant others who are actively involved in the young persons’ support and development (e.g., housing service staff, support workers/progression coaches). Depending on the context, these staff may also be those acting as MST facilitators. 1MST toolkit 1 (strengths-based activities) [82]; 2MST toolkit 2—psychologically informed delivery [83], 3MST toolkit 3—strengths-based evaluation [84]. Toolkits are available to download from www.sprintproject.org.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



