
Submitted:
31 July 2024
Posted:
01 August 2024
You are already at the latest version
Abstract
The causes of pediatric cancers often remain unknown; however, due to the development of medicine and technology, genetic disorders may play a crucial role in the genesis of neoplasms. Over time, the number of cancer predisposition syndromes (CPS) and awareness of them are increasing, providing the possibility of cancer prevention and early detection. In this study, we presented data concerning the number and type of oncological cases and their correlation with CPS occurrence in a cohort of Central and Eastern European pediatric population. The data were collected between 2000 and 2019 at the Karol Jonscher Clinical Hospital of Poznan University of Medical Sciences, resulting in a cohort of 2,190 cases in total, of which 193 children (8.81%) were confirmed to have CPS. CPS occurred most frequently in infancy (22.90% of all children suffering from any diagnosed cancer during the first year of life, p < 0.0001), accounting for more than a quarter of all CPS cases in our cohort. CPS were least likely to be observed in patients aged 14 and 15 years (2.17% and 2.44% of children diagnosed with any of the listed cancers at the exact age, respectively, p < 0.05). Among CPS, the most common were neurofibromatosis type I (NF1), Li-Fraumeni syndrome (LFS), and Down syndrome (DS). To conclude, it is important to emphasize the need for personalized treatment for each patient affected by both CPS and subsequent cancer in order to reduce the toxicity of therapy and improve quality of life by reducing the risk of side effect.
Keywords:
cancer
; children
; cancer predisposition syndromes (CPSs)
1. Introduction
Cancers in children remain rare diseases, even though the researcher’s model estimated up to 400,000 newly diagnosed childhood neoplasms worldwide annually.[1] The exact cause of cancer diagnosis very often stays unknown, what makes it difficult to prevent in pediatric patients. In the early 70s, Knudson made a two-hit hypothesis referring to both tumor suppressor gene alleles inactivation (by mutation or epigenetic silencing) as a causative of phenotype changes.[2,3,4] Thanks to medical and technological development, the role of genetics in neoplasm pathogenesis is becoming more and more crucial, especially regarding cancer predisposition syndromes (CPSs), whose number and consciousness increase with time passing by. Depending on the data source, the incidence of CPSs is between 7 and 18% in the pediatric population suffering from neoplasms in general, up to 21% of children with central nervous system (CNS) tumors.[5,6,7,8,9,10,11,12,13] Genetic consulting and testing should be one of the routine actions during neoplasm diagnosis in the pediatric population, at least if there are prerequisites of an underlying CPS, such as young age of cancer diagnosis, phenotype features, atypical neoplasm diagnosis, positive family history or being a cancer survivor. Although several research groups have tested previously created questionnaires to facilitate the identification of relevant cancer mutations, none of these questionnaires have achieved 100% sensitivity. Unfortunately, this lack of sensitivity could contribute to missed diagnoses of CPSs.[9,14,15,16,17]
One of the most common and known CPSs is Down Syndrome (DS) – many recommendations and therapy modifications were made according to an underlying genetic disorder which are bringing benefits to affected children and their families in early cancer detection, reducing toxicity during treatment, and after all, improving survival.[18,19] These seem to be available advantages of thoroughly understanding any CPS, if only the proper effort in many medical centers will be made, especially because some of CPSs are extremely rare, but still worth detecting and getting to know them better.
In this study we present analyzed data concerning the number and type of oncological cases and their correlation with CPSs occurrence among cohort in a Central and Eastern European pediatric population. The data were collected between 2000 and 2019 in Karol Jonscher’s Clinical Hospital of Poznan University of Medical Sciences.
2. Materials and Methods
2.1. Study Population
This study represents 2,190 unselected Caucasian children from birth up to 18th year of age, hospitalized with newly diagnosed neoplasm in Karol Jonscher’s Clinical Hospital of Poznan University of Medical Sciences between 2000 and 2019. Giving the diagnosis on the day of 18th birthday or any time after the results in Poland is being taken under adult medical care in another hospital, so we do not owe any neoplasm incidence information about 18 and more years old patients from our center. Due to analyzing the retrospective latent cancer incidence data the signed permission for including the patient into our cohort study neither from legal guardians nor affected child was required. The study was approved by the Bioethics Committee of the Medical University of Poznan (Resolution No. KB-549/24).
2.2. Clinical Evaluation
The study cohort inclusion criteria required confirmed neoplasm. The cancer diagnosis led to the assigning of appropriate ICD-10 codes, from C00 to D48, and was the basis for enrolling the patient in our cohort, which first counted 3,663 patients. After detecting and removing: 1) replicated cases, 2) previously diagnosed in other regions patients, who were transferred to our hospital to continue beforehand initiated treatment (e.g. to carry out the hematopoietic stem cell transplant) and 3) children diagnosed before January 1st, 2000, the final cohort number occurred 2,190 (1,233 males and 957 females).
The cancer predisposition syndromes (CPSs) diagnosis was based on 1) phenotypic trait such as observed in e.g. Down Syndrome (DS), neurofibromatosis type 1 (NF1) or isolated hemihypertrophy (IHH), often with genetic disorder confirmation and 2) genetic testing including molecular analysis targeting mutations within a single gene, Sanger Sequencing, Whole Exome Sequencing (WES) and Next-generation Sequencing (NGS) utilizing the TriSight One Expanded Sequencing Panel by Illumina, allowing thereby to analyze 6699 genes with confirmed clinical significance, from which the oncology gene subpanel (with 125 genes included) was selected. The genetic testing was performed in Polish centers (in Lodz, Poznan, Szczecin and Warsaw), as well as abroad: in Germany, Italy, Norway, the United Kingdom and the USA.
2.3. Data Analysis
Categorical data were presented as numbers (n) and percentages (%). Univariate analyses were used to compare the distribution of studied parameters ꭓ2 test with or without Yates’ correction, depending on the number of cases. Odds ratios (ORs) and 95% confidence intervals (95% CI) were calculated for the association between the presence of CPS-related neoplasms. According to the results (OR and statistical significance) model, the best-fitting data was proposed. Statistical analyses and graphs were computed using GraphPad Prism v6 software. Differences were considered significant when p < 0.05.
3. Results
3.1. The General Characteristics of Patients
Over 20 years of retrospective follow-up 2,190 children had a new diagnosis of cancer in Karol Jonscher’s Clinical Hospital of Poznan University of Medical Sciences, a highly specialized pediatric hospital in the western region of Poland. Table 1 summarizes detailed characteristics (such as sex, size of age groups at the time of diagnosis, and a total number of exact diagnoses according to ICD-10 classification) of the children included in this study cohort. The largest group was leukemia patients (codes C91 and C92) with a total number of 692 (31.60%), the second most common group was patients with central nervous system (CNS) tumors (codes from C70 to C72) with a total number of 382 (17.44%), and the third one –lymphomas patients (from code C81 to C85) with a total number of 279 (12.74%). After adding up it gives over 61% of all newly diagnosed patients in our retrospective analysis.
3.2. Prevalence of Specific Cancers in General and According to Age
Table 2 presents the prevalence of common and rare neoplasms in children depending on age defined by ICD-10 classification. Distinguished cancers are: 1) lymphoid (C91) and 2) myeloid (C92) leukemias represented by 505 (23.06%) and 187 (8.54%) patients respectively, 3) central nervous system tumors (C70-C72) with a summed number of 382 (17.44%) children, both 4) Hodgkin (C81) and 5) non-follicular (C83) lymphomas represented by 268 (12.24%) cases in general and 144 (6.58%) vs. 124 (5.66%) patients accordingly, 6) malignances located in peripheral nerves and autonomic nervous system, i.e. neuroblastomas (C47) – 177 (8.08%) children, 7) soft tissue tumors (C49), of which rhabdomyosarcoma (RMS) was diagnosed more often, with a total number of 161 (7.35%) patients and 8) malignant neoplasm of the kidney (C64), with Wilms tumor as the most frequently diagnosed cancer in this group, and a number of 130 (5.94%) children. Mentioned diagnoses were given to 1,810 patients, which stands for over 82% of all children. The rest 380 patients were suffering from not as common neoplasms, including: endocrine glands cancers (C73-C75) with thyroid and adrenal tumors diagnosed more often and a total number of 95 (4.33%) cases, bone and articular cartilage neoplasms (C40-C41) with a summed number of 64 (2.92%) children, leukemias (besides previously mentioned) and other malignancies of lymphoid, hematopoietic and related tissue (C94-C96) represented by 61 (2.79%) patients, liver and intrahepatic bile ducts cancers (C22) with hepatoblastoma as the most frequent representant of this group and a total number of 42 (1.92%) cases, gonads neoplasms: ovary (C56) and testis (C62) with a summed number of 44 (2.01%) children including 21 (0.96%) females and 23 (1.05%) males respectively. Other cancers with a prevalence below 1% of those diagnosed in our cohort are considered as extremely rare in the pediatric population and are listed in Table 1 with an exact number of cases.
A higher prevalence of specific cancers was observed in different age groups, which is demonstrated in Table 2. Peripheral nerves and autonomic nervous system tumors (C47), soft tissue tumors (C49), kidney cancers (C64), central nervous system tumors (C70-C72), and leukemias (both C91 and C92) were diagnosed mostly during infancy and toddlerhood period. Later on in early childhood, the frequency of neoplasms classified as C47, C49, C70-C72, and C92 started to decrese, while those assigned as C64 and C91 increased up to their highest peak of prevalence in our cohort. As written above, from birth untill the end of an early childhood period, the first peak of cancer incidence in the whole children group was detected. While the frequency of neoplasms classified as C70-C72 and C91 (lymphoid leukemia) keeps decresing in pre-school and early-school age, the first of two peaks of non-follicular lymphomas (C83) incidence was detected; the second one was observed in age between 13 and 15 years old. The prevalence of Hodgkin lymphoma (C81) and myeloid leukemia (C92) started to increase noticeably in the pre-puberty and early adolescence period (up to 14 years old), leading to the incidence peak of C81 among adolescents and rather constant frequency of diagnosing C92 up the age of 17 years. In consequence, the second peak of general incidence was observed according to mentioned above, as well as some of the rarely detected in children diagnosis, which are more specific to adults: bladder cancer (C67), thyroid gland tumor (C73), bone and articular cartilage cancer (C40-C41) and testis neoplasm (C62).
To summarize, two peaks of cancer incidence in our pediatric cohort were observed: 1) in early childhood (from birth up to 5 years old) with a total number of 1,013 children (46.3%) and 2) in the adolescent period (between 15 and 17 years old) with a total number of 370 adolescents (16.9%).
3.3. Cancer Predisposition Syndromes (CPSs) Incidence According to Age
During 20 years of study follow-up cancer predisposition syndromes (CPSs) were detected in 193 out of 2,190 patients (8.81%). The neoplasm and CPSs incidence data according to age are presented in Table 3 and Figure 1.
CPSs occurred most frequently in infancy period (22.90% of all children suffering from any diagnosed cancer during the first year of life, p < 0.0001), which accounts for more than a quarter of all CPS cases in our cohort. From this group CPSs were more likely to be detected firstly among 9 months olds (equaling 41.67% of 12 cases diagnosed with neoplasm at this age, p < 0.001), secondly among newborns up to 1 month olds (25.00% with p = 0.001 and 28.57% with p < 0.01 of mentioned age groups respectively), and thirdly among 5 months olds (resulting in 26.32% of 19 patients at this age from studied cohort, however with p < 0.05). Also, during toddlerhood CPSs were still likely to occur – with frequency of 15.72% among 3 years olds (p < 0.01) and 13.74% in 2 years olds (p < 0.05) diagnosed with cancer previously. CPSs were least likely to be observed between 14- and 15-years old patients (2.17% and 2.44% of children diagnosed with any of previously listed neoplasm at exact age respectively, p < 0.05). In other age groups CPSs were diagnosed with intermediate frequency, however these results might be not enough significant (p > 0.05).
The list of CPSs that were detected in our cohort according to age are presented in Supplement Table S1. Among infants neurofibromatosis type I (NF1) occurred most frequently observed CPS resulting in 23 cases (46.94% of CPS-positive patients in that age group), especially during two first months of life giving together 11 newborns and 1 month olds (47.83% of all NF1 patients during infancy). In that short period also Down Syndrome (DS) was observed quite often, i.e. in all 3 cases detected during infancy. Other CPSs likely to be detected in the first year of life were isolated hemihypertrophy (IHH) – 6 cases after summing up and resulting to be most often diagnosed CPS among 9 months olds, Beckwith-Wiedemann Syndrome (BWS), and Li-Fraumeni Syndrome (LFS), 5 cases each, of which BWS was prevailing among 5 months olds. In toddlerhood, from 2 to 3 years olds NF1 again occurred to be most frequently diagnosed (15 patients after summing up), but also mentioned LFS and DS, resulting in 10 and 7 cases among pointed two years of life respectively. Other detected CPSs were BWS and IHH, 5 cases each. To be more specific, in 3 years olds also constitutional mismatch repair deficiency syndrome (CMMRDS) was detected, which wasn’t observed at any other age, and hemophagocytic lymphohistiocytosis (HLH) – in 2 and 2 cases respectively. Among 14- and 15-years old patients, so in less likely to be diagnosed with CPS-related cancer group, NF1 was detected in 3 cases after summing up, HLH in 14 years old child and multiple endocrine neoplasia syndrome (MEN) in 15 years old child, resulting in CPS 5 cases during these two years of life.
3.4. Observed Age Ranges for the Highest Risk of CPS-Related Cancer Development in Children
We devided our cohort into four age ranges, which were taken under statistical analysis. The designated age limits constituted the model best suited to the study population.
Children between 11 and 18 years had the lowest risk of developing CPS-associated neoplasm (above 17% vs 35% non-CPS related cancers) (Table 4). In relation to this subgroup, the highest risk for diagnosis of CPS-related cancers was between 0 and 1 month olds (7.52-fold), then from 2 up to 12 months olds (5.81-fold), and between 1 and 11 years olds (2.08-fold).
3.5. Neoplasms Diagnosed in CPS-Positive Patients
In supplement Table S2 data about diagnosed cancers among 193 CPS-positive patients are included, according to ICD-10 classification. From all detected cancer predisposition syndromes (CPS) neurofibromatosis type I (NF1) prevailed in general (83 patients), but also in patients diagnossed with malignancies of peripheral nerves and autonomic nervous system (C47), central nervous system (CNS) tumors (C71-C72), and malignant neoplasms of other connective and soft tissues (C49). The second most common CPS occurred Li-Fraumeni Syndrome (LFS) resulting in 34 cases, of whom the largest group was patients suffering from C71, C47, and malignant neoplasms of liver and intrahepatic bile ducts (C22). Also 2 cases of multiple cancers in LFS-positive patients were observed, both with the same neoplasms diagnosed (rhabdomyosarcoma and myeloid leukemia). The third worth mentioning CPS is Down Syndrome with 19 cases, all affected by leukemias, both lymphoid (C91) and myeloid (C92). What is interesting, all of diagnosed with isolated hemihypertrophy (IHH) patients had confirmed a malignant neoplasm of kidney (C64). Beckwith-Wiedemann Syndrome (BWS) was detected in 10 cases, of whom 7 patients were diagnosed with C64. Other observed CPSs occurred less often and are listed in supplement Table S2.
4. Discussion
To our knowledge, it is the first study summarizing cancer predisposition syndromes (CPSs) incidence based on childhood neoplasms prevalence among Central and Eastern European population with 20 years of data collection. In our cohort of 2,190 cancer-positive pediatric patients, 193 of them (8.81%) were diagnosed with an underlying cancer predisposition syndrome (CPS). Most of current researchers assume CPS prevalence to oscillate between 7 and 18% in pediatric population in general, beyond children with central nervous system (CNS) tumors, in whom the percentage reaches even 21%.[5,6,7,8,9,10,11,12,13] We believe that CPSs appeared in our population during several previous decades at least as often as nowadays. However, their detecting possibilities were limited. What is more – during the 20 years of our study follow-up, the availability of genetic testing was changing for the better;[20,21,22,23,24] however, it remains underfunded in Poland, and in consequence, is out of reach for less affluent families or financing by public hospitals. In this regard, several confirmed CPSs seems to be underestimated. Probably also the cancer incidence in our cohort is down sided due to domestic or abroad medical tourism, depending on permanent residence, finance possibilities, and other causes.[25,26] And so these aspects remain the study limitations worth mentioning before further considerations.
As stated before, we observed two peaks of cancer incidence among studied population, what corresponds with other researches.[27,28] The first one (demonstrated during first five years of life) may be correlated with a high prevalence of blastomas caused by malignance process in precursor cells (like neuroblastoma, Wilms tumor, medulloblastoma, hepatoblastoma, retinoblastoma), known as a group of early childhood tumors, which become unspecific among older children. The second incidence peak, in the adolescent period, according to biological completion of the ripening process and, in consequence, similarity rather to adults than to children, can be explained by a growing number of lymphomas in general, myeloid leukemias, thyroid cancers, testis neoplasms, and bladder malignances, which are observed more frequently in the mature population.[29,30]
What is worth mentioning, the number of childhood cancer survivors among adolescents and adults is increasing with time passing by due to earlier detection and still improving treatment strategies.[31,32] In consequence, more people may be suffering from side-effects related to previous neoplasm diagnosis, as well as to used therapy, and a number of them will be the greater the longer time from cancer diagnosis is going to pass.[33,34,35,36,37] One of the worst late complications seems to remain secondary malignancy, with particularly higher risk among CPS-positive patients.[38,39,40,41] However, to be mindful about health consequences and treatment responsibilities related to CPSs, the patient need to have genetic guidance and to be diagnosed with any molecular disorder first.
In our cohort, conducting diagnostic tests for CPSs was considered in case of rare and unspecific cancer occurrence, phenotypic features, recurrence or multiplied neoplasm detection, and burdened family history. Genetic counseling was often carried out after the diagnosis of neoplasm, while early detection seems to be crucial for effective preventive medical care with tailoring any needed (especially neoplasm) treatment to the underlying mutation. Probably conducting the diagnosis of CPS should be considered more often than verified algorithms propose so far.[9,14,15,16,17,42,43] Especially due to the developing branch of genomic screening leading to explanation of a CPS-related neoplasm detection.[12,18,24,39,44] For that reasons we, and other researchers groups, highlight the necessity of personalized treatment in any affected by both CPS and subsequent neoplasm patient to reduce therapy toxicity and improve the quality of one’s life by decreasing the risk of side effects.[45,46,47] Appropriate guidelines are being published for last few years, and so we recommend to follow.[19,48,49,50,51,52,53]
5. Conclusions
A higher prevalence of CPSs in infancy and toddlerhood period may be associated with inherited genetic disorders and according to Knudson’s two-hits theory, the development of neoplasm can occur right after the second mutation (i.e. second hit) with the first being associated with the presence of CPS. Although Knudson’s theory cannot explain the molecular basis of every inherited neoplasm in children, it remains a key starting point for advancements in genomic research.[54]
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table 1: Detected cancer predisposition syndromes (CPSs) in 193 patients according to age at time of neoplasm diagnosis. Table 2: Detected cancer predisposition syndromes (CPSs) in 193 patients according to diagnosed neoplasm defined by ICD-10 classification.
Author Contributions
Conceptualization G.T-K., E.S., P.S.-S., D.J.-L.; methodology, G.T-K., E.S., D.J.-L.; software, G.T-K., E.S., D.J.-L.; validation, G.T-K., E.S., P.S.-S., D.J.-L.; formal analysis, G.T-K., E.S., P.S.-S., D.J.-L.; investigation, G.T-K., D.J.-L.; resources, G.T-K., E.S., P.S.-S., D.J.-L.; data curation, G.T-K., E.S., D.J.-L. writing—original draft preparation, G.T-K., E.S., D.J.-L. ; writing—review and editing, G.T-K., E.S., P.S.-S., D.J.-L.; visualization, G.T-K., E.S.; supervision, E.S., D.J.-L.; project administration, G.T-K., E.S., P.S.-S., D.J.-L.; funding acquisition, G.T-K., E.S., P.S.-S., D.J.-L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Bioethics Committee at Poznan University of Medical Sciences (KB- 549/24).
Data Availability Statement
All data are presented in manuscript and supplementary information.
Acknowledgments
Not relevant.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Ward, Z.J.; Yeh, J.M.; Bhakta, N.; Frazier, A.L.; Atun, R. Estimating the total incidence of global childhood cancer: a simulation-based analysis. The Lancet Oncology 2019, 20, 483–493. [Google Scholar] [CrossRef] [PubMed]
- Knudson, A.G. Mutation and cancer: statistical study of retinoblastoma. Proc Natl Acad Sci U S A 1971, 68, 820–823. [Google Scholar] [CrossRef] [PubMed]
- Chernoff, J. The two-hit theory hits 50. Mol Biol Cell 2021, 32, rt1. [Google Scholar] [CrossRef] [PubMed]
- Hino, O.; Kobayashi, T. Mourning Dr. Alfred G. Knudson: the two-hit hypothesis, tumor suppressor genes, and the tuberous sclerosis complex. Cancer Sci 2017, 108, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Newman, S.; Nakitandwe, J.; Kesserwan, C.A.; Azzato, E.M.; Wheeler, D.A.; Rusch, M.; Shurtleff, S.; Hedges, D.J.; Hamilton, K.V.; Foy, S.G.; et al. Genomes for Kids: The Scope of Pathogenic Mutations in Pediatric Cancer Revealed by Comprehensive DNA and RNA Sequencing. Cancer Discov 2021, 11, 3008–3027. [Google Scholar] [CrossRef] [PubMed]
- Gröbner, S.N.; Worst, B.C.; Weischenfeldt, J.; Buchhalter, I.; Kleinheinz, K.; Rudneva, V.A.; Johann, P.D.; Balasubramanian, G.P.; Segura-Wang, M.; Brabetz, S.; et al. The landscape of genomic alterations across childhood cancers. Nature 2018, 555, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Kratz, C.P.; Jongmans, M.C.; Cavé, H.; Wimmer, K.; Behjati, S.; Guerrini-Rousseau, L.; Milde, T.; Pajtler, K.W.; Golmard, L.; Gauthier-Villars, M.; et al. Predisposition to cancer in children and adolescents. Lancet Child Adolesc Health 2021, 5, 142–154. [Google Scholar] [CrossRef] [PubMed]
- Fiala, E.M.; Jayakumaran, G.; Mauguen, A.; Kennedy, J.A.; Bouvier, N.; Kemel, Y.; Fleischut, M.H.; Maio, A.; Salo-Mullen, E.E.; Sheehan, M.; et al. Prospective pan-cancer germline testing using MSK-IMPACT informs clinical translation in 751 patients with pediatric solid tumors. Nat Cancer 2021, 2, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Rossini, L.; Durante, C.; Bresolin, S.; Opocher, E.; Marzollo, A.; Biffi, A. Diagnostic Strategies and Algorithms for Investigating Cancer Predisposition Syndromes in Children Presenting with Malignancy. Cancers (Basel) 2022, 14, 3741. [Google Scholar] [CrossRef] [PubMed]
- Wilson, C.L.; Wang, Z.; Liu, Q.; Ehrhardt, M.J.; Mostafavi, R.; Easton, J.; Mulder, H.; Hedges, D.J.; Wang, S.; Rusch, M.; et al. Estimated number of adult survivors of childhood cancer in United States with cancer-predisposing germline variants. Pediatr Blood Cancer 2020, 67, e28047. [Google Scholar] [CrossRef] [PubMed]
- Bakhuizen, J.J.; Hopman, S.M.J.; Bosscha, M.I.; Dommering, C.J.; van den Heuvel-Eibrink, M.M.; Hol, J.A.; Kester, L.A.; Koudijs, M.J.; Langenberg, K.P.S.; Loeffen, J.L.C.; et al. Assessment of Cancer Predisposition Syndromes in a National Cohort of Children With a Neoplasm. JAMA Netw Open 2023, 6, e2254157. [Google Scholar] [CrossRef] [PubMed]
- Hansford, J.R.; Das, A.; McGee, R.B.; Nakano, Y.; Brzezinski, J.; Scollon, S.R.; Rednam, S.P.; Schienda, J.; Michaeli, O.; Kim, S.Y.; et al. Update on Cancer Predisposition Syndromes and Surveillance Guidelines for Childhood Brain Tumors. Clin Cancer Res 2024, 30, 2342–2350. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Walsh, M.F.; Wu, G.; Edmonson, M.N.; Gruber, T.A.; Easton, J.; Hedges, D.; Ma, X.; Zhou, X.; Yergeau, D.A.; et al. Germline Mutations in Predisposition Genes in Pediatric Cancer. N Engl J Med 2015, 373, 2336–2346. [Google Scholar] [CrossRef] [PubMed]
- Jongmans, M.C.J.; Loeffen, J.L.C.M.; Waanders, E.; Hoogerbrugge, P.M.; Ligtenberg, M.J.L.; Kuiper, R.P.; Hoogerbrugge, N. Recognition of genetic predisposition in pediatric cancer patients: An easy-to-use selection tool. Eur J Med Genet 2016, 59, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Diets, I.J.; Waanders, E.; Ligtenberg, M.J.; van Bladel, D.A.G.; Kamping, E.J.; Hoogerbrugge, P.M.; Hopman, S.; Olderode-Berends, M.J.; Gerkes, E.H.; Koolen, D.A.; et al. High Yield of Pathogenic Germline Mutations Causative or Likely Causative of the Cancer Phenotype in Selected Children with Cancer. Clin Cancer Res 2018, 24, 1594–1603. [Google Scholar] [CrossRef] [PubMed]
- Byrjalsen, A.; Hansen, T.V.O.; Stoltze, U.K.; Mehrjouy, M.M.; Barnkob, N.M.; Hjalgrim, L.L.; Mathiasen, R.; Lautrup, C.K.; Gregersen, P.A.; Hasle, H.; et al. Nationwide germline whole genome sequencing of 198 consecutive pediatric cancer patients reveals a high incidence of cancer prone syndromes. PLoS Genet 2020, 16, e1009231. [Google Scholar] [CrossRef] [PubMed]
- Wagener, R.; Taeubner, J.; Walter, C.; Yasin, L.; Alzoubi, D.; Bartenhagen, C.; Attarbaschi, A.; Classen, C.-F.; Kontny, U.; Hauer, J.; et al. Comprehensive germline-genomic and clinical profiling in 160 unselected children and adolescents with cancer. Eur J Hum Genet 2021, 29, 1301–1311. [Google Scholar] [CrossRef] [PubMed]
- Shahani, S.A.; Marcotte, E.L. Landscape of germline cancer predisposition mutations testing and management in pediatrics: Implications for research and clinical care. Front Pediatr 2022, 10, 1011873. [Google Scholar] [CrossRef] [PubMed]
- Baruchel, A.; Bourquin, J.-P.; Crispino, J.; Cuartero, S.; Hasle, H.; Hitzler, J.; Klusmann, J.-H.; Izraeli, S.; Lane, A.A.; Malinge, S.; et al. Down syndrome and leukemia: from basic mechanisms to clinical advances. Haematologica 2023, 108, 2570–2581. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, H.; Fujita, M. Whole genome sequencing analysis for cancer genomics and precision medicine. Cancer Sci 2018, 109, 513–522. [Google Scholar] [CrossRef] [PubMed]
- Sabour, L.; Sabour, M.; Ghorbian, S. Clinical Applications of Next-Generation Sequencing in Cancer Diagnosis. Pathol Oncol Res 2017, 23, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, R.; Krishnan, Y. The chemistry of next-generation sequencing. Nat Biotechnol 2023, 41, 1709–1715. [Google Scholar] [CrossRef] [PubMed]
- Sąsiadek, M.M.; Łaczmańska, I.; Maciejczyk, A.; Matkowski, R.; Gil, J. Genetyka i onkologia (część 1.). Podstawy medycyny personalizowanej w onkologii opartej na badaniach genetycznych. Biuletyn Polskiego Towarzystwa Onkologicznego Nowotwory 2020, 5, 193–199. [Google Scholar]
- Garutti, M.; Foffano, L.; Mazzeo, R.; Michelotti, A.; Da Ros, L.; Viel, A.; Miolo, G.; Zambelli, A.; Puglisi, F. Hereditary Cancer Syndromes: A Comprehensive Review with a Visual Tool. Genes (Basel) 2023, 14, 1025. [Google Scholar] [CrossRef] [PubMed]
- Zhong, L.; Deng, B.; Morrison, A.M.; Coca-Stefaniak, J.A.; Yang, L. Medical, Health and Wellness Tourism Research-A Review of the Literature (1970-2020) and Research Agenda. Int J Environ Res Public Health 2021, 18, 10875. [Google Scholar] [CrossRef] [PubMed]
- Birchley, G.; Linney, M.; Turner, S.W.; Wilkinson, D. Clinical ethics: medical tourism in children. Arch Dis Child 2021, 106, 1143–1144. [Google Scholar] [CrossRef] [PubMed]
- Lupo, P.J.; Spector, L.G. Cancer Progress and Priorities: Childhood Cancer. Cancer Epidemiol Biomarkers Prev 2020, 29, 1081–1094. [Google Scholar] [CrossRef] [PubMed]
- Mullen, C.J.R.; Barr, R.D.; Franco, E.L. Timeliness of diagnosis and treatment: the challenge of childhood cancers. Br J Cancer 2021, 125, 1612–1620. [Google Scholar] [CrossRef] [PubMed]
- Urszula Wojciechowska; Klaudia Barańska; Irmina Michałek; Paweł Olasek; Marta Miklewska; Joanna A. Didkowska Nowotwory złośliwe w Polsce w 2020 roku. Cancer in Poland in 2020; Krajowy Rejestr Nowotworów. Polish National Cancer Registry: Warszawa, 2022; pp. 1–100.
- Miller, K.D.; Fidler-Benaoudia, M.; Keegan, T.H.; Hipp, H.S.; Jemal, A.; Siegel, R.L. Cancer statistics for adolescents and young adults, 2020. CA Cancer J Clin 2020, 70, 443–459. [Google Scholar] [CrossRef] [PubMed]
- Becker, C.; Graf, N.; Grabow, D.; Creutzig, U.; Reinhardt, D.; Weyer-Elberich, V.; Spix, C.; Kaatsch, P. Early deaths from childhood cancer in Germany 1980-2016. Cancer Epidemiol 2020, 65, 101669. [Google Scholar] [CrossRef] [PubMed]
- Robison, L.L.; Hudson, M.M. Survivors of childhood and adolescent cancer: life-long risks and responsibilities. Nat Rev Cancer 2014, 14, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Keikhaei, B.; Bahadoram, M.; Keikha, A.; Bahadoram, S.; Hassanzadeh, S.; Mahmoudian-Sani, M.-R. Late side effects of cancer treatment in childhood cancer survivors. J Oncol Pharm Pract 2023, 29, 885–892. [Google Scholar] [CrossRef] [PubMed]
- Sylvest, R.; Vassard, D.; Schmidt, L.; Schmiegelow, K.; Macklon, K.T.; Forman, J.L.; Pinborg, A. Parenthood among men diagnosed with cancer in childhood and early adulthood: trends over time in a Danish national cohort. Hum Reprod 2021, 36, 2576–2586. [Google Scholar] [CrossRef] [PubMed]
- Camilli, M.; Skinner, R.; Iannaccone, G.; La Vecchia, G.; Montone, R.A.; Lanza, G.A.; Natale, L.; Crea, F.; Cameli, M.; Del Buono, M.G.; et al. Cardiac Imaging in Childhood Cancer Survivors: A State-of-the-Art Review. Curr Probl Cardiol 2023, 48, 101544. [Google Scholar] [CrossRef] [PubMed]
- Kok, W.E. Too often and too early: the risk of cardiac ischaemia in adult survivors of childhood cancer. Heart 2021, 107, 6–7. [Google Scholar] [CrossRef] [PubMed]
- Landier, W.; Skinner, R.; Wallace, W.H.; Hjorth, L.; Mulder, R.L.; Wong, F.L.; Yasui, Y.; Bhakta, N.; Constine, L.S.; Bhatia, S.; et al. Surveillance for Late Effects in Childhood Cancer Survivors. J Clin Oncol 2018, 36, 2216–2222. [Google Scholar] [CrossRef] [PubMed]
- Cesen Mazic, M.; Reulen, R.C.; Jazbec, J.; Zadravec Zaletel, L. Trends in treatment of childhood cancer and subsequent primary neoplasm risk. Radiol Oncol 2022, 56, 552. [Google Scholar] [CrossRef] [PubMed]
- Zahnreich, S.; Schmidberger, H. Childhood Cancer: Occurrence, Treatment and Risk of Second Primary Malignancies. Cancers (Basel) 2021, 13, 2607. [Google Scholar] [CrossRef] [PubMed]
- Tanjak, P.; Suktitipat, B.; Vorasan, N.; Juengwiwattanakitti, P.; Thiengtrong, B.; Songjang, C.; Therasakvichya, S.; Laiteerapong, S.; Chinswangwatanakul, V. Risks and cancer associations of metachronous and synchronous multiple primary cancers: a 25-year retrospective study. BMC Cancer 2021, 21, 1045. [Google Scholar] [CrossRef] [PubMed]
- Vogt, A.; Schmid, S.; Heinimann, K.; Frick, H.; Herrmann, C.; Cerny, T.; Omlin, A. Multiple primary tumours: challenges and approaches, a review. ESMO Open 2017, 2, e000172. [Google Scholar] [CrossRef] [PubMed]
- Linga, B.G.; Mohammed, S.G.A.A.; Farrell, T.; Rifai, H.A.; Al-Dewik, N.; Qoronfleh, M.W. Genomic Newborn Screening for Pediatric Cancer Predisposition Syndromes: A Holistic Approach. Cancers (Basel) 2024, 16, 2017. [Google Scholar] [CrossRef] [PubMed]
- Beigh, M.; Vagher, J.; Codden, R.; Maese, L.D.; Cook, S.; Gammon, A. Newborn Screening for Li-Fraumeni Syndrome: Patient Perspectives. Res Sq 2024, rs.3.rs-4351728. [CrossRef]
- Comitani, F.; Nash, J.O.; Cohen-Gogo, S.; Chang, A.I.; Wen, T.T.; Maheshwari, A.; Goyal, B.; Tio, E.S.; Tabatabaei, K.; Mayoh, C.; et al. Diagnostic classification of childhood cancer using multiscale transcriptomics. Nat Med 2023, 29, 656–666. [Google Scholar] [CrossRef]
- Ripperger, T.; Bielack, S.S.; Borkhardt, A.; Brecht, I.B.; Burkhardt, B.; Calaminus, G.; Debatin, K.-M.; Deubzer, H.; Dirksen, U.; Eckert, C.; et al. Childhood cancer predisposition syndromes-A concise review and recommendations by the Cancer Predisposition Working Group of the Society for Pediatric Oncology and Hematology. Am J Med Genet A 2017, 173, 1017–1037. [Google Scholar] [CrossRef] [PubMed]
- Helms, L.; Guimera, A.E.; Janeway, K.A.; Bailey, K.M. Innovations in Cancer Treatment of Children. Pediatrics 2023, 152, e2023061539. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, G.T.; Chen, Y.; Yasui, Y.; Leisenring, W.; Gibson, T.M.; Mertens, A.C.; Stovall, M.; Oeffinger, K.C.; Bhatia, S.; Krull, K.R.; et al. Reduction in Late Mortality among 5-Year Survivors of Childhood Cancer. N Engl J Med 2016, 374, 833–842. [Google Scholar] [CrossRef] [PubMed]
- Knoblauch, A.L.; Blaß, B.-I.; Steiert, C.; Neidert, N.; Puzik, A.; Neumann-Haefelin, E.; Ganner, A.; Kotsis, F.; Schäfer, T.; Neumann, H.P.H.; et al. Screening and surveillance recommendations for central nervous system hemangioblastomas in pediatric patients with Von Hippel-Lindau disease. J Neurooncol 2024, 168, 537–545. [Google Scholar] [CrossRef] [PubMed]
- Vagher, J.; Mehrhoff, C.J.; Florou, V.; Maese, L.D. Genetic Predisposition to Sarcoma: What Should Clinicians Know? Curr Treat Options Oncol 2024, 25, 769–783. [Google Scholar] [CrossRef] [PubMed]
- Kamihara, J.; Bourdeaut, F.; Foulkes, W.D.; Molenaar, J.J.; Mossé, Y.P.; Nakagawara, A.; Parareda, A.; Scollon, S.R.; Schneider, K.W.; Skalet, A.H.; et al. Retinoblastoma and Neuroblastoma Predisposition and Surveillance. Clin Cancer Res 2017, 23, e98–e106. [Google Scholar] [CrossRef] [PubMed]
- Radtke, H.B.; Berger, A.; Skelton, T.; Goetsch Weisman, A. Neurofibromatosis Type 1 (NF1): Addressing the Transition from Pediatric to Adult Care. Pediatric Health Med Ther 2023, 14, 19–32. [Google Scholar] [CrossRef] [PubMed]
- Kumamoto, T.; Yamazaki, F.; Nakano, Y.; Tamura, C.; Tashiro, S.; Hattori, H.; Nakagawara, A.; Tsunematsu, Y. Medical guidelines for Li-Fraumeni syndrome 2019, version 1.1. Int J Clin Oncol 2021, 26, 2161–2178. [Google Scholar] [CrossRef] [PubMed]
- Brioude, F.; Kalish, J.M.; Mussa, A.; Foster, A.C.; Bliek, J.; Ferrero, G.B.; Boonen, S.E.; Cole, T.; Baker, R.; Bertoletti, M.; et al. Expert consensus document: Clinical and molecular diagnosis, screening and management of Beckwith-Wiedemann syndrome: an international consensus statement. Nat Rev Endocrinol 2018, 14, 229–249. [Google Scholar] [CrossRef] [PubMed]
- Brodeur, G.M.; Nichols, K.E.; Plon, S.E.; Schiffman, J.D.; Malkin, D. Pediatric Cancer Predisposition and Surveillance: An Overview, and a Tribute to Alfred G. Knudson Jr. Clin Cancer Res 2017, 23, e1–e5. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Identification of 193 cancer predisposition syndromes (CPSs) in a regional Caucasian unselected cohort of 2,190 children with a neoplasm from a Central and Eastern European population a) in infants (from birth up to 1 year old), b) in whole studied cohort.
Figure 1.
Identification of 193 cancer predisposition syndromes (CPSs) in a regional Caucasian unselected cohort of 2,190 children with a neoplasm from a Central and Eastern European population a) in infants (from birth up to 1 year old), b) in whole studied cohort.
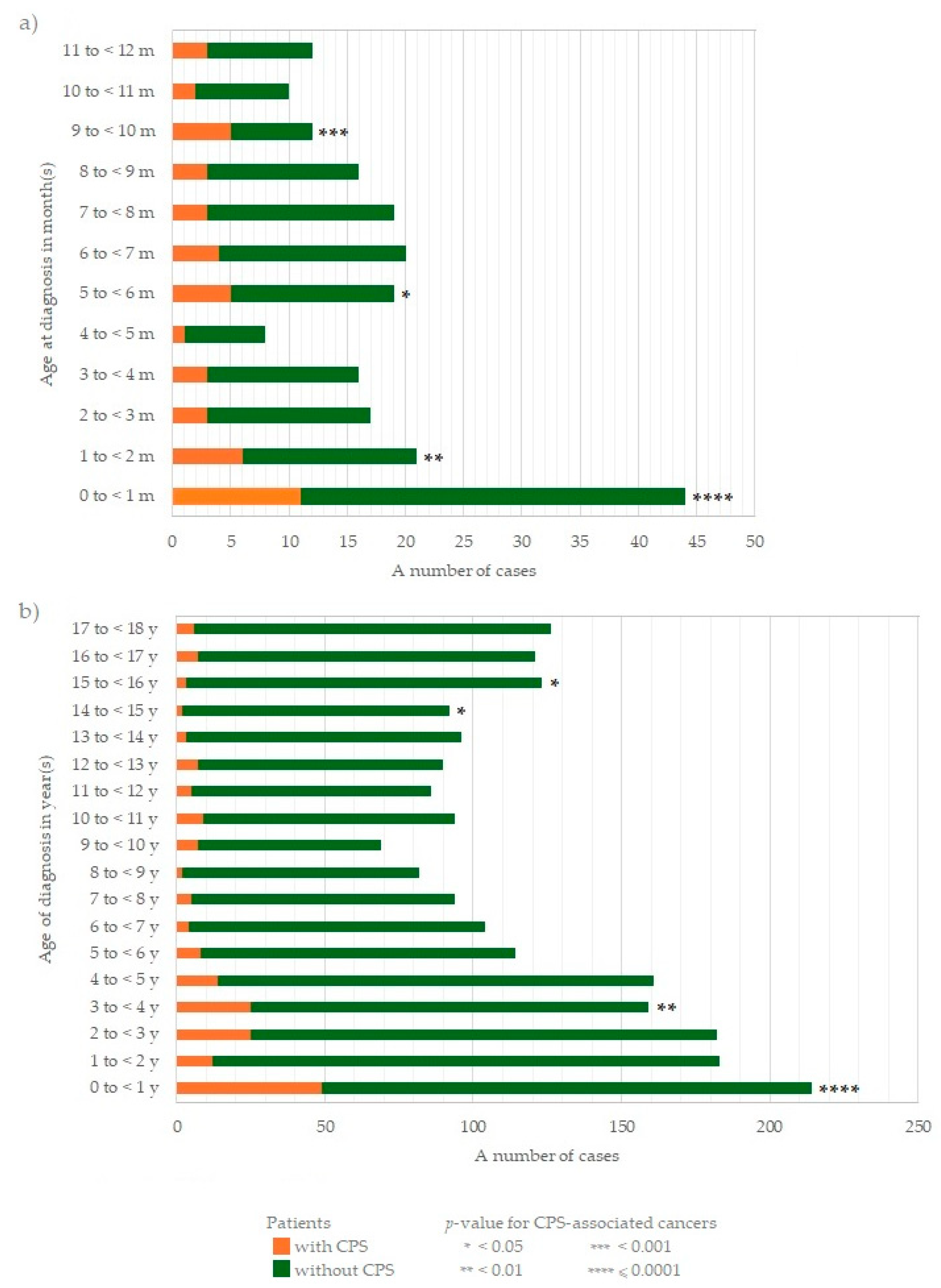

Table 1.
The general characteristics of the studied patient cohort include sex, size of age groups at the time of diagnosis, and a total number of exact diagnoses according to ICD-10 classification.
Table 1.
The general characteristics of the studied patient cohort include sex, size of age groups at the time of diagnosis, and a total number of exact diagnoses according to ICD-10 classification.
| Characteristic | No. (%) | |
| Sex | ||
| Male | 1,233 (56.30) | |
| Female | 957 (43.70) | |
| Age at diagnosis of neoplasm, years old [y] | ||
| 0 to < 5 y | 899 (41.05) | |
| 5 to < 10 y | 463 (21.14) | |
| 10 to < 15 y | 458 (20.91) | |
| 15 to < 18 y | 370 (16.89) | |
| Diagnosis | ||
| ICD-10 | Mayor diagnosis | |
| C11 | Malignant neoplasm of nasopharynx | 4 (0.18) |
| C22 | Malignant neoplasm of liver and intrahepatic bile ducts | 42 (1.92) |
| C30 | Malignant neoplasm of the nasal cavity and middle ear | 2 (0.09) |
| C37 | Malignant neoplasm of thymus | 1 (0.05) |
| C38 | Malignant neoplasm of the heart, mediastinum and pleura | 7 (0.32) |
| C39 | Malignant neoplasm of other and ill-defined sites in the respiratory system and intrathoracic organs | 1 (0.05) |
| C40 | Malignant neoplasm of bone and articular cartilage of limbs | 37 (1.69) |
| C41 | Malignant neoplasm of bone and articular cartilage of other and unspecified sites | 27 (1.23) |
| C43 | Malignant melanoma of the skin | 1 (0.05) |
| C47 | Malignant neoplasm of peripheral nerves and autonomic nervous system | 177 (8.08) |
| C48 | Malignant neoplasm of retro-peritoneum and peritoneum | 4 (0.18) |
| C49 | Malignant neoplasm of other connective and soft tissue | 161 (7.35) |
| C56 | Malignant neoplasm of ovary | 21 (0.96) |
| C62 | Malignant neoplasm of testis | 23 (1.05) |
| C64 | Malignant neoplasm of kidney, except renal pelvis | 130 (5.94) |
| C67 | Malignant neoplasm of bladder | 4 (0.18) |
| C68 | Malignant neoplasm of other and unspecified urinary organs | 1 (0.05) |
| C69 | Malignant neoplasm of the eye and adnexa | 12 (0.55) |
| C70 | Malignant neoplasm of meninges | 5 (0.23) |
| C71 | Malignant neoplasm of the brain | 357 (16.30) |
| C72 | Malignant neoplasm of the spinal cord, cranial nerves and other parts of the central nervous system | 20 (0.91) |
| C73 | Malignant neoplasm of the thyroid gland | 73 (3.33) |
| C74 | Malignant neoplasm of the adrenal gland | 17 (0.78) |
| C75 | Malignant neoplasm of other endocrine glands and related structures | 5 (0.23) |
| C76 | Malignant neoplasm of other and ill-defined sites | 13 (0.59) |
| C79 | Secondary malignant neoplasm of other and unspecified sites | 3 (0.14) |
| C80 | Malignant neoplasm, without specification of the site | 1 (0.05) |
| C81 | Hodgkin lymphoma | 144 (6.58) |
| C83 | Non-follicular lymphoma | 124 (5.66) |
| C84 | Mature T/NK-cell lymphomas | 1 (0.05) |
| C85 | Other and unspecified types of non-Hodgkin lymphoma | 10 (0.46) |
| C88 | Malignant immunoproliferative diseases | 9 (0.41) |
| C91 | Lymphoid leukemia | 505 (23.06) |
| C92 | Myeloid leukemia | 187 (8.54) |
| C94 | Other leukemias of specified cell type | 10 (0.46) |
| C95 | Leukemia of unspecified cell type | 2 (0.09) |
| C96 | Other and unspecified malignant neoplasms of lymphoid, hematopoietic and related tissue | 49 (2.24) |
Table 2.
The prevalence of common and rare neoplasms in children, depending on age, is defined by ICD-10 classification (described in Table 1), presented by numbers and percentages given in brackets. The percentages of specific cancer incidence according to age are related in columns.
Table 2.
The prevalence of common and rare neoplasms in children, depending on age, is defined by ICD-10 classification (described in Table 1), presented by numbers and percentages given in brackets. The percentages of specific cancer incidence according to age are related in columns.
| Age [y] | C47 N=177 |
C49 N=161 |
C64 N=130 |
C70-72 N=382 |
C81 N=144 |
C83 N=124 |
C91 N=505 |
C92 N=187 |
Other N=380 |
Total N=2,190 | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 to < 1 | 64 (36.2) | 31 (19.3) | 17 (13.1) | 34 (8.9) | 1 (0.7) | 3 (2.4) | 13 (2.6) | 9 (4.8) | 42 (11.1) | 214 (9.8) | |||
| 1 to < 2 | 32 (18.1) | 16 (9.9) | 14 (10.8) | 29 (7.6) | 0 (0.0) | 5 (4.0) | 30 (5.9) | 18 (9.6) | 39 (10.3) | 183 (8.4) | |||
| 2 to < 3 | 20 (11.3) | 17 (10.6) | 15 (11.5) | 34 (8.9) | 0 (0.0) | 5 (4.0) | 60 (11.9) | 12 (6.4) | 19 (5.0) | 182 (8.3) | |||
| 3 to < 4 | 11 (6.2) | 13 (8.1) | 23 (17.7) | 30 (7.9) | 3 (2.1) | 4 (3.2) | 55 (10.9) | 9 (4.8) | 11 (2.9) | 159 (7.3) | |||
| 4 to < 5 | 10 (5.6) | 12 (7.5) | 22 (16.9) | 26 (6.8) | 2 (1.4) | 5 (4.0) | 59 (11.7) | 9 (4.8) | 16 (4.2) | 161 (7.4) | |||
| 5 to < 6 | 10 (5.6) | 4 (2.5) | 13 (10.0) | 21 (5.5) | 0 (0.0) | 7 (5.6) | 42 (8.3) | 7 (3.7) | 10 (2.6) | 114 (5.2) | |||
| 6 to < 7 | 7 (4.0) | 6 (3.7) | 3 (2.3) | 23 (6.0) | 5 (3.5) | 11 (8.9) | 31 (6.1) | 5 (2.7) | 13 (3.4) | 104 (4.7) | |||
| 7 to < 8 | 4 (2.3) | 1 (0.6) | 5 (3.8) | 23 (6.0) | 2 (1.4) | 8 (6.5) | 29 (5.7) | 10 (5.3) | 12 (3.2) | 94 (4.3) | |||
| 8 to < 9 | 2 (1.1) | 5 (3.1) | 4 (3.1) | 19 (5.0) | 4 (2.8) | 7 (5.6) | 26 (5.1) | 5 (2.7) | 10 (2.6) | 82 (3.7) | |||
| 9 to < 10 | 2 (1.1) | 3 (1.9) | 2 (1.5) | 13 (3.4) | 5 (3.5) | 6 (4.8) | 23 (4.6) | 3 (1.6) | 12 (3.2) | 69 (3.2) | |||
| 10 to < 11 | 3 (1.7) | 4 (2.5) | 2 (1.5) | 17 (4.5) | 7 (4.9) | 9 (7.3) | 24 (4.8) | 13 (7.0) | 15 (3.9) | 94 (4.3) | |||
| 11 to < 12 | 3 (1.7) | 6 (3.7) | 0 (0.0) | 15 (3.9) | 11 (7.6) | 5 (4.0) | 12 (2.4) | 16 (8.6) | 18 (4.7) | 86 (3.9) | |||
| 12 to < 13 | 2 (1.1) | 4 (2.5) | 1 (0.8) | 15 (3.9) | 12 (8.3) | 6 (4.8) | 19 (3.8) | 10 (5.3) | 21 (5.5) | 90 (4.1) | |||
| 13 to < 14 | 0 (0.0) | 9 (5.6) | 0 (0.0) | 12 (3.1) | 11 (7.6) | 12 (9.7) | 23 (4.6) | 14 (7.5) | 15 (3.9) | 96 (4.4) | |||
| 14 to < 15 | 2 (1.1) | 5 (3.1) | 1 (0.8) | 13 (3.4) | 10 (6.9) | 7 (5.6) | 14 (2.8) | 13 (7.0) | 27 (7.1) | 92 (4.2) | |||
| 15 to < 16 | 1 (0.6) | 8 (5.0) | 1 (0.8) | 19 (5.0) | 26 (18.1) | 13 (10.5) | 18 (3.6) | 10 (5.3) | 27 (7.1) | 123 (5.6) | |||
| 16 to < 17 | 3 (1.7) | 6 (3.7) | 6 (4.6) | 17 (4.5) | 21 (14.6) | 6 (4.8) | 11 (2.2) | 13 (7.0) | 38 (10.0) | 121 (5.5) | |||
| 17 to < 18 | 1 (0.6) | 11 (6.8) | 1 (0.8) | 22 (5.8) | 24 (16.7) | 5 (4.0) | 16 (3.2) | 11 (5.9) | 35 (9.2) | 126 (5.8) | |||
| Legend | < 5.0% | 5.0-9.9% | 10.0-14.9% | 15.0-19.9% | ≥ 20.0% | ||||||||
Table 3.
The incidence of neoplasm in children according to age at diagnosis and the presence of cancer predisposition syndromes (CPSs).
Table 3.
The incidence of neoplasm in children according to age at diagnosis and the presence of cancer predisposition syndromes (CPSs).
| Age, year(s)/month(s) old [y/m] |
CPS presence | Statistical analysis | |||
| No N=1,997 n (%) |
Yes N=193 n (%) |
OR |
95% CI |
p |
|
| 0 to < 1 y | 165 (8.3) | 49 (25.4) | 3.78 | 2.63 - 5.42 | < 0.0001 |
| 0 to < 1 m | 33 (1.7) | 11 (5.7) | 3.60 | 1.79 - 7.24 | 0.0001 |
| 1 to < 2 m | 15 (0.8) | 6 (3.1) | 4.24 | 1.63 - 11.1 | 0.0048 |
| 2 to < 3 m | 14 (0.7) | 3 (1.6) | 2.24 | 0.64 - 7.85 | 0.1839 |
| 3 to < 4 m | 13 (0.7) | 3 (1.6) | 2.41 | 0.68 - 8.53 | 0.1613 |
| 4 to < 5 m | 7 (0.4) | 1 (0.5) | 1.48 | 0.18 - 12.1 | 0.5225 |
| 5 to < 6 m | 14 (0.7) | 5 (2.6) | 3.77 | 1.34 - 10.6 | 0.0216 |
| 6 to < 7 m | 16 (0.8) | 4 (2.1) | 2.62 | 0.87 - 7.92 | 0.0926 |
| 7 to < 8 m | 16 (0.8) | 3 (1.6) | 1.95 | 0.56 - 6.77 | 0.2313 |
| 8 to < 9 m | 13 (0.7) | 3 (1.6) | 2.41 | 0.68 - 8.53 | 0.1613 |
| 9 to < 10 m | 7 (0.4) | 5 (2.6) | 7.56 | 2.38 - 24.1 | 0.0004 |
| 10 to < 11 m | 8 (0.4) | 2 (1.0) | 2.60 | 0.55 - 12.4 | 0.4891 |
| 11 to < 12 m | 9 (0.5) | 3 (1.6) | 3.49 | 0.94 - 13.0 | 0.1408 |
| 1 to < 2 y | 171 (8.6) | 12 (6.2) | 0.71 | 0.39 - 1.30 | 0.2609 |
| 2 to < 3 y | 157 (7.9) | 25 (13.0) | 1.74 | 1.11 - 2.74 | 0.0144 |
| 3 to < 4 y | 134 (6.7) | 25 (13.0) | 2.07 | 1.31 - 3.26 | 0.0014 |
| 4 to < 5 y | 147 (7.4) | 14 (7.3) | 1.04 | 0.59 - 1.85 | 0.8848 |
| 5 to < 6 y | 106 (5.3) | 8 (4.1) | 0.77 | 0.37 - 1.61 | 0.5997 |
| 6 to < 7 y | 100 (5.0) | 4 (2.1) | 0.77 | 0.37 - 1.61 | 0.5997 |
| 7 to < 8 y | 89 (4.5) | 5 (2.6) | 0.57 | 0.23 - 1.42 | 0.3005 |
| 8 to < 9 y | 80 (4.0) | 2 (1.0) | 0.25 | 0.06 - 1.03 | 0.0606 |
| 9 to < 10 y | 62 (3.1) | 7 (3.6) | 1.17 | 0.53 - 2.60 | 0.8565 |
| 10 to < 11 y | 85 (4.3) | 9 (4.7) | 1.10 | 0.55 - 2.23 | 0.9334 |
| 11 to < 12 y | 81 (4.1) | 5 (2.6) | 0.64 | 0.26 - 1.60 | 0.4472 |
| 12 to < 13 y | 83 (4.2) | 7 (3.6) | 0.87 | 0.40 - 1.90 | 0.8698 |
| 13 to < 14 y | 93 (4.7) | 3 (1.6) | 0.32 | 0.10 - 1.03 | 0.0678 |
| 14 to < 15 y | 90 (4.5) | 2 (1.0) | 0.22 | 0.05 - 0.91 | 0.0351 |
| 15 to < 16 y | 120 (6.0) | 3 (1.6) | 0.25 | 0.08 - 0.78 | 0.0163 |
| 16 to < 17 y | 114 (5.7) | 7 (3.6) | 0.62 | 0.29 - 1.35 | 0.2966 |
| 17 to < 18 y | 120 (6.0) | 6 (3.1) | 0.51 | 0.22 - 1.17 | 0.1420 |
Table 4.
Age ranges relevant to the incidence of CPS-associated neoplasm in children.
| Age, year(s)/month(s) old [y/m] |
CPS presence | Statistical analysis | |||
| No N = 1997 n (%) |
Yes N = 193 n (%) |
OR |
95% CI |
p |
|
| 11 to < 18 y | 701 (35.1) | 33 (17.1) | 1.00 | reference | |
| 1 to < 11 y | 1131 (56.6) | 111 (57.5) | 2.08 | 1.40 – 3.11 | 0.0002 |
| 2 to < 12 m | 117 (5.9) | 32 (16.6) | 5.81 | 3.44 – 9.81 | < 0.0001 |
| 0 to < 2 m | 48 (2.4) | 17 (8.8) | 7.52 | 3.91 – 14.5 | < 0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



