
Submitted:
30 July 2024
Posted:
02 August 2024
You are already at the latest version
Abstract
Venous thromboembolism (VTE) is a serious health condition and represents an important cause of morbidity and, in some cases, mortality. According to the latest estimates from the Centers for Disease Control and Prevention, 3 out of 10 people with VTE will have recurrence of clotting event within 10 years. The American Heart Association reports that VTE is more common in people over 40 years of age, and that risk doubles with each decade. The World Health Organization advises that the world’s population of people aged 60 years is going to be doubled by 2050. Deep vein thrombosis (DVT) and pulmonary embolism (PE) are the two main conditions that make up VTE. People with VTE are initially treated with anticoagulants to prevent conditions such as stroke and to reduce the recurrence of VTE. However, thrombolytic therapy is used for people with PE experiencing with low blood pressure or in severe cases of DVT. Despite the approval of direct anticoagulants in 2010, there is clear evidence that the search for new drugs that are more effective or safer than the current antithrombotic treatments continues. Thrombin plays a crucial role in regulating hemostasis and maintaining blood coagulation, and therefore serves as a major target for the treatment of hemostatic disorders such as thromboembolic syndromes, disseminated intravascular coagulation, thrombocytopenia, and acquired hemostatic disorders such as platelet dysfunction and excessive anticoagulation, among other pathologies. This review focuses on the progress in research on new anticoagulants and novel delivery systems for antithrombotic targeting to vascular embolisms.
Keywords:
thrombotic disorders
; targeted-antithrombotic approaches
; nanothrombolysis
; clot-penetrating drug
; aging
; fibrinolysis
1. Introduction
VTE is one of the most common non-malignant blood disorders in the United States (U.S.) [1] and in most countries [2], representing a serious problem for our national and global health. The clinical evidence supports the view that VTE can cause serious illness, disability, and in severe cases, death [3]. The Worcester VTE study [4] established that the annual incidence rate of VTE has risen between 1985 and 2009 and remains high. A similar trend was observed in Norway [5]. Moreover, it was shown that the incidence rates increased exponentially with age and, surprisingly, were slightly higher in women than in men. Although VTE has had much progress over the past decade, one in twelve people will be expected to experience VTE in their lifetime [6]. It is estimated that 20% of patients with VTE are at increased risk of dying, particularly within the first year after diagnosis [6,7]. The pathophysiology of VTE includes stasis, endothelial injury, and hypercoagulability, which were described by Rudolf Virchow [8]. VTE is associated with a variety of interrelated biological and functional alteration [9], but remains associated with derangements in hemostasis. VTE covers two interrelated clinical events: (1) pulmonary embolism (PE), a blockage in the lung, and (2) deep vein thrombosis (DVT), also called venous thrombosis [10].
DVT is characterized by the formation of blood clots (thrombi) in the deep veins [11,12,13], which can be categorized as acute, sub-acute, and chronic. During these periods, acute thrombi are considered to be prone to detaching from the vein, leading to a higher risk for PE. DVT is considered a multifactorial disease, indicating that many genetics and provoking factors such as immobilization and surgery affect the initiation and continuance of the disease [14]. Recently, evidence shows that plasminogen activator inhibitor-1 (PAI-1) polymorphism -675 ID, 4G/5G, factor V Leiden mutation, and prothrombin G20210A single nucleotide polymorphism (SNP) have been correlated with elevated DVT levels [15].
PE occurs when a segment of a DVT clot breaks off and blocks a pulmonary artery in the lung. This reduces blood flow in the artery, which may cause severe shortness of breath and chest pain. In the US, PE causes 60,000 to 100,000 deaths per year [16]. The 2008 European guidelines for the diagnosis and management of PE indicate that the number of new cases of this disease is approximately 0.5 to 1.0 per 1000 people [17]. There are numerous risk factors for PE [18], including family history of clots, old age, cancer, use of estrogen-containing oral contraceptives, pregnancy, and surgery. Most importantly, two out of three individuals with PE die within two hours after presentation [18].
While DVT is a severe clinical entity, it resolves spontaneously without complication. Approximately 90% of DVT cases occur in the lower limbs. About 40 to 50% of proximal DVT patients have asymptomatic PE noted with a lung scan [19], which dramatically reduces short- and long-term survival among patients. The incidence rate of isolated DVT (without PE) ranges from 45 to 117 per 100,000 people yearly [20], while PE (with or without DVT) ranges from 29 to 78 per 100,000 people yearly [21]. DVT-associated massive PE results in an estimated 300,000 deaths annually in the U.S. [22]. Given that DVT is relatively common and associated with significant morbidity and mortality, significant progress has been made in order to develop new therapies and clinical evaluations to control DVT and reduce immediate complications.
VTE coexists with numerous chronic diseases, which share risk factors such as age, obesity, metabolic syndrome, and cardiovascular diseases. Diabetes [23], cancer [24,25,26], and acquired immunodeficiency syndrome (AIDS) are the known risk factors for VTE [27]. VTE is considered to be a common medical disorder complicating pregnancy [28,29]. The aforementioned studies indicate that VTE can happen to anyone. The age-adjusted incidence of diabetes has increased sharply in recent years [30] and is projected to double by 2030 [31]. The increased risk of VTE has been reported in type 1 diabetes [32], but not with type 2 diabetes [33]. There is controversy about whether diabetes mellitus is a risk factor for VTE [34]. Increased thrombin generation [35] coupled with a higher concentration of procoagulant cell-derived circulating microparticles [36] in type 2 diabetic patients profoundly indicate a hypercoagulation state. Diabetic patients who develop VTE have an increased risk of recurrent DVT and long-term major bleeding. Diabetic nephropathy is a serious kidney-related complication of diabetes mellitus. The rate of kidney disease is increasing rapidly in the worldwide population [37]. Patients with chronic kidney disease exhibit bleeding and are prone to thrombosis. VTE event rates are doubled in the presence of chronic kidney disease. Nephrotic syndrome can cause VTE, and in patients with this syndrome, VTE is associated with elevated urine loss of antithrombin III [38], an endogenous inhibitor of coagulation, that causes the blood to clot more than normal. However, evidence shows that diabetes mellitus and diabetes complications are not risk factors for incident VTE [39]. Proteinuria is the hallmark of glomerular disease and a major risk factor for systemic cardiovascular complications. Patients with clinically active malignancy are at increased risk of VTE. Cancer-associated venous thrombosis, a common condition, is one of the leading causes of morbidity and mortality for cancer patients compared with the general population. Evidence clearly indicates that drug, sex [40], and hospitalization [41] interact with the risk of developing VTE in patients with chronic disorders. While the risk of developing VTE is highest after major surgery or injury, both immunotherapy [42] and anti-angiogenic drugs [43,44,45] are shown to cause an increased risk of VTE.
The goal of antithrombotic therapy is to reduce cardiovascular and cerebrovascular morbidity, prevent the likelihood of further VTE recurrence, help improve blood flow in the blood vessels, and prevent life-threatening events such as PE and other forms of thromboembolic events. We outline the recent advances in managing VTE and medications used to help pharmacological management, such as preventing fibrin formation, slowing down blood clots, dissolving existing blood clots, and treating thrombosis in VTE patients. We focus on the use of anticoagulants, anti–platelet agents, thrombolytic agents, and anti-fibrinolytic drugs in clinical trials. We specifically aim to highlight the potential of targeted drug delivery systems for enhancing the targeting and efficacy of new and existing anticoagulant therapy and ultimately improving patient outcomes.
2. Blood Coagulation System
Blood coagulation factors constitute a key class of proteases and cofactors that serve collectively as illustrated in (Figure 1). coagulation proteases are synthesized as inactive precursors (zymogens) in the liver and are then secreted into the blood. Upon vascular injury, the zymogens are converted to the active form by the selective enzymatic cleavage of the peptide bond(s). The blood coagulation proteases are different from each other in terms of zymogen substrate specificity, active site, and catalytic mechanism. The sequence of consecutive activation of the coagulation reaction is governed by the specificity of each protease, ions, and cofactors, whereas the degree of amplification is linked to the activation of an effector molecule downstream in the pathway. The blood coagulation pathway is divided into two phases: Phase 1 (extrinsic pathway) and Phase 2 (intrinsic pathway) (Figure 1). The extrinsic pathway includes the interaction between the transmembrane receptor tissue factor (TF) and plasma factor VII/VIIa (FVII/FVIIa) [46]. The binding of TF to FVII results in the conversion of zymogen FVII to activated factor VII (FVIIa). Evidence indicates that TF enhances FVIIa catalytic activity [47]. The TF:FVII complex is also activated by several proteases including thrombin, an effector in coagulation. The formed TF:FVIIa complex consequently activates factor IX (FIX) to activated factor IX (FIXa) and factor X (FX) to activated factor X (FXa) on the platelet surface in the presence of calcium. The intrinsic pathway includes the interaction between plasma factor XI (FXI), factor IX (FIX), and factor VIII (FVIII). Although different proteases can activate zymogen FXI to activated FXI (FXIa), thrombin and activated factor XII (FXIIa) are highly effective in mediating FXI activation. FXIa activates FIX to activated FIX (FIXa) and consequently activates factor X in the presence of activated factor VIII (FVIIIa) and calcium on the surface of a platelet. The effectors of both extrinsic and intrinsic pathways activate factor X (FX), a converging target, which integrates their function. Thus, factor Xase has emerged as a key mediator of coagulation. FXa activates factor II (prothrombin) into activated factor II (thrombin) in the presence of cofactor Va and calcium ions, the components of the common pathway. Thrombin plays a crucial role in converting factor I (fibrinogen) into fibrin, an insoluble fiber. Thrombin activates factor XIII into activated factor XIII (XIIIa), a calcium-dependent transglutaminase. FXIIIa cross-links fibrin monomers to stabilize the platelet plug and form thrombus, a blood clot.
3. Fibrinolysis
The opposite to thrombosis is fibrinolysis. Plasmin is the main protease that drives the progression of fibrinolysis. Plasmin is a molecular switch that, when activated from plasminogen by tissue plasminogen activator (tPA), urokinase-type plasminogen activator (uPA), kallikrein, XIIa, can cause the conversion of fibrin into fibrin degradation product (FDP) (Figure 2). FXII, tPA, and uPA are spatially synthesized by different cell types. FXII is synthesized by the liver. While tPA is synthesized by endothelial cells, uPA is synthesized by monocytes, macrophages, and urinary epithelial cells. Fibrinolysis is, in turn, temporally coordinated with these proteolytic processes. Plasmin activates both tPA and uPA, creating a positive feedback loop that triggers brief impetus to produce a sustained conversion of inactive plasminogen to active plasmin. This protective feedback loop prevents unnecessary accumulation of intravascular fibrin and ensures the blood has sufficient plasmin needed to remove the thrombus. Excellent reviews on the history of the discovery of fibrinolysis, current understanding of the fibrinolytic system, and the fibrinolytic system as a treatment target can also be found elsewhere [48,49].
Specific inhibitors can bind to circulating plasmin and plasminogen activators (uPA, tPA), preventing them from engaging in excessive unregulated activities and thus maintaining the integrity of the thrombus (Figure 2). Plasminogen activator inhibitor (PAI), a serpin inhibitor, inhibits both tPA and uPA [50]. Plasmin is neutralized by α2-antiplasmin, a plasma serpin. α2-antiplasmin is incapable of inhibiting plasmin when it is bound to fibrin. Plasmin is modulated by α2-macroglobin, a nonspecific protease inactivator. C1-esterase inhibitor, a physiological inhibitor of plasma kallikrein and FXIIa, also attenuates the nonspecific plasminogen activation [51,52]. Moreover, thrombin-activated fibrinolysis inhibitor (TAFI), a non-serpin inhibitor, removes C-terminal lysine and arginine residues on fibrin. This decreases the number of available plasminogen binding sites, leading to a reduction in plasmin formation and clot stabilization. The reader is referred to the following articles for more detailed information on TAFI [53,54]. Fibrinolysis is tightly regulated by the complex interplay of activating and inhibitory pathways.
4. The Physiology of Thrombosis
The procoagulant/anticoagulant balance is maintained through the interaction between platelets and vascular endothelium, and with a predominance of the active form of anticoagulant forces. Coagulation activation is tightly regulated by several endogenous anticoagulants which provide a counter mechanism to clot formation. Tissue factor pathway inhibitors (TFPI) and thrombomodulin are endothelial-associated anticoagulant proteins, while protein C, protein S, and antithrombin are circulating anticoagulant proteins. TFPI pathway inhibits early phases of the procoagulant response [55], whereas activated protein C in concert with its cofactor, protein S, degrade factors VIIIa and Va [56], the two proteins that play an important role in near the final step of the coagulation pathway. The partial deficiencies of the circulating anticoagulant proteins are causes of VTE [57], indicating that anticoagulation system is responsible for regulating hemostasis. Reader is referred to the following reviews for more detailed information [58,59,60,61] (Figure 1). Procoagulant/anticoagulant imbalance leads to the pathogenesis of stroke, ischemia, myocardial infarction, and particularly venous thromboembolism. Increasing levels of the active form of procoagulants due to reduced anticoagulants and perturbed vascular endothelium cause unchecked activation of coagulation. It has emerged that endothelial dysfunction and hemostatic derangement cause several pathophysiological disturbances of primary and secondary hemostasis, fibrinolysis, and subsequent tissue repair.
There are two broad classifications of thrombosis: arterial thrombosis and venous thrombosis, which is a major focus of this review (Figure 3). Both arterial thrombosis and venous thrombosis are similar, but there is a subtle difference between the two. Arterial thrombosis is a platelet-predominant phenomenon. Histopathologic features that have been considered specific for arterial thrombosis include fibrin, leukocytes, and an abundance of platelets, providing a white appearance [62]. Patients with arterial thrombi are at high risk for acute stroke, myocardial infarction, or peripheral arterial disease. Venous thrombosis is generally understood as a disorder in plasma coagulation, and is associated with red blood cells and fibrin-rich, presenting a red appearance “red clot” [63] (Figure 3). Venous thrombi occur in areas of reduced blood flow and stasis, leading to the accumulation of procoagulants and reduced levels of local anticoagulant pathway [64]. The severe compression of the iliac vein in pregnant women [65] patients, May-Thurner syndrome (an iliac vein compression syndrome) [66], or the combination of the two creates venous stasis that can contribute to the increased risk of VTE . On histopathology, venous clots are composed of fibrin, leukocytes, and red blood cells, and low levels of platelets compared to arterial thrombi. According to the dogma, platelets are not involved in the pathogenesis of venous thrombosis. However, recent evidence suggests that platelets play an important role in VTE pathophysiology [67], and may be involved in the initiation of DVT [68]. This suggests a need to consider the antiplatelet agents as an antithrombotic therapy for the management of DVT and VTE.
The occurrence of thrombus is determined by a physical exam, imaging tests, and the procoagulant/anticoagulant balance. Various provoking factors that cause thrombus formation disrupt the procoagulant/anticoagulant balance. These provoking factors include: (1) medical devices (vascular grafts, stents, catheters, and heart valves); (2) chronic diseases (chronic kidney disease, heart disease, uncontrolled hypertension, chronic inflammation, diabetes, cancer, old age); (3) cell perturbation (activated endothelial cells, activation of blood platelets); (4) lifestyle (being overweight or obese, smoking); and (5) medications (oral contraceptives or hormone replacement therapy).
5. Pharmacotherapy of VTE: An Update
This section provides an overview of the drugs used for the treatment of VTE. Anticoagulation therapy, thrombolytic therapy, and antiplatelet therapy are considered the standard of care for VTE treatment (Figure 4). The American Society of Hematology and the American College of Chest Physicians (ACCP) strongly recommends anticoagulation therapy. Anticoagulants as first-line medications can be used to prevent, treat, and reduce the recurrence of VTE, and help to prevent stroke in persons with atrial fibrillation [69]. Anticoagulants are a class of medications that block key serine proteases.
The conventional drugs used in the treatment of DVT are blood thinners, also called anticoagulants, that control thrombus formation. Typically, anticoagulants directly or indirectly inhibit the formation or activity of thrombin involved in maintaining the clot-forming process, although they may also contribute to other hemostatic benefits. These include: (1) heparin, an indirect thrombin inhibitor, that stops blood from forming blood clots or prevents the formation of a bigger blood clot; (2) warfarin, a vitamin K antagonist used as an oral anticoagulant, that is prescribed following the initial treatment to prevent another blood clot; (3) low molecular weight heparin (Enoxaparin, Apixaban, Betrixaban, Dabigatran, Edoxaban, and Rivaroxaban); and (4) Fondaprinux, a synthetic heparin pentasaccharide, is used to prevent VTE and treat DVT and improve survival following myocardial infarction. Indiscriminate distribution of most anticoagulants by systemic administration and lack of specificity to the DVT may contribute to an increased risk of bleeding. In addition, since most of the anticoagulants are removed via the renal system, thereby these drugs pose an increased risk for chronic kidney disease.
A combination of heparin and oral anticoagulants are commonly used for the prevention and treatment of patients with acute DVT [70]. Although highly effective, they are also associated with significant bleeding risks [71]. Therefore, accurately estimating the age and maturity of DVT is of significant importance for determining therapeutic management. However, none of the currently available risk factor tools [72] is effective enough in predicting bleeding including intracranial hemorrhage. American Society of Hematology recommendations include the following: (a) use of thrombolytic therapy for patients with PE and hemodynamic compromise to rapidly dissolve the embolic burden; (b) the target international normalized ratio (INR) should be between 2.0 to 3.0 for the majority of patients with PE [73]. A low INR range is recommended for patients with VTE receiving a vitamin K antagonist for secondary prevention; and c) use of indefinite anticoagulation for persons with recurrent unprovoked VTE or associated with chronic factors [10]. Antiplatelet agents appear to reduce recurrent VTE [74,75]. In a meta-analysis of randomized studies by the Antiplatelet Trialists’ collaboration in 1994, antiplatelet therapy was shown to reduce the risk of VTE [76]. Some patients will require combinational therapy to produce better outcomes. Many of the above medicines used to treat VTE are associated with unwanted bleeding as a side effect. Table 1 outlines the many new antithrombotic drugs that target various steps in the hemostatic system. Table 2 summarizes the recommended drug classes according to compelling indication.
6. Drugs in Development for VTE
We conducted a comprehensive search on the clinicaltrials.gov website to identify candidate drugs for VTE and related complications that had progressed through phases 1-3 of clinical trials, with their results posted within the last five years. Numerous VTE studies seek to develop new therapeutics, targeted therapeutic drugs, and technologies to improve efficacy and safety compared with traditional VTE drugs. In this section, we present important drug candidates for each target in clinical trials. These agents target coagulation factors (FXI, thrombin), modulate the endogenous inhibitors (protein C) of the blood coagulation factors, activated thrombin activatable fibrinolysis inhibitor (a regulator of fibrinolysis, or the P-selectin/PSGL-1 pathway, which has a pivotal role in both thromboinflammation and immunothrombosis (Table 3). We briefly discuss the significance of FXI and P-selectin glycoprotein ligand 1 (PSGL-1) to demonstrate how they affect thrombus formation. We also provide a summary of recent targeted therapeutic delivery methods of different nanomaterials and technologies that have shown significant promise for treating VTE and DVT.
6.1. FXI as a Novel Drug Target
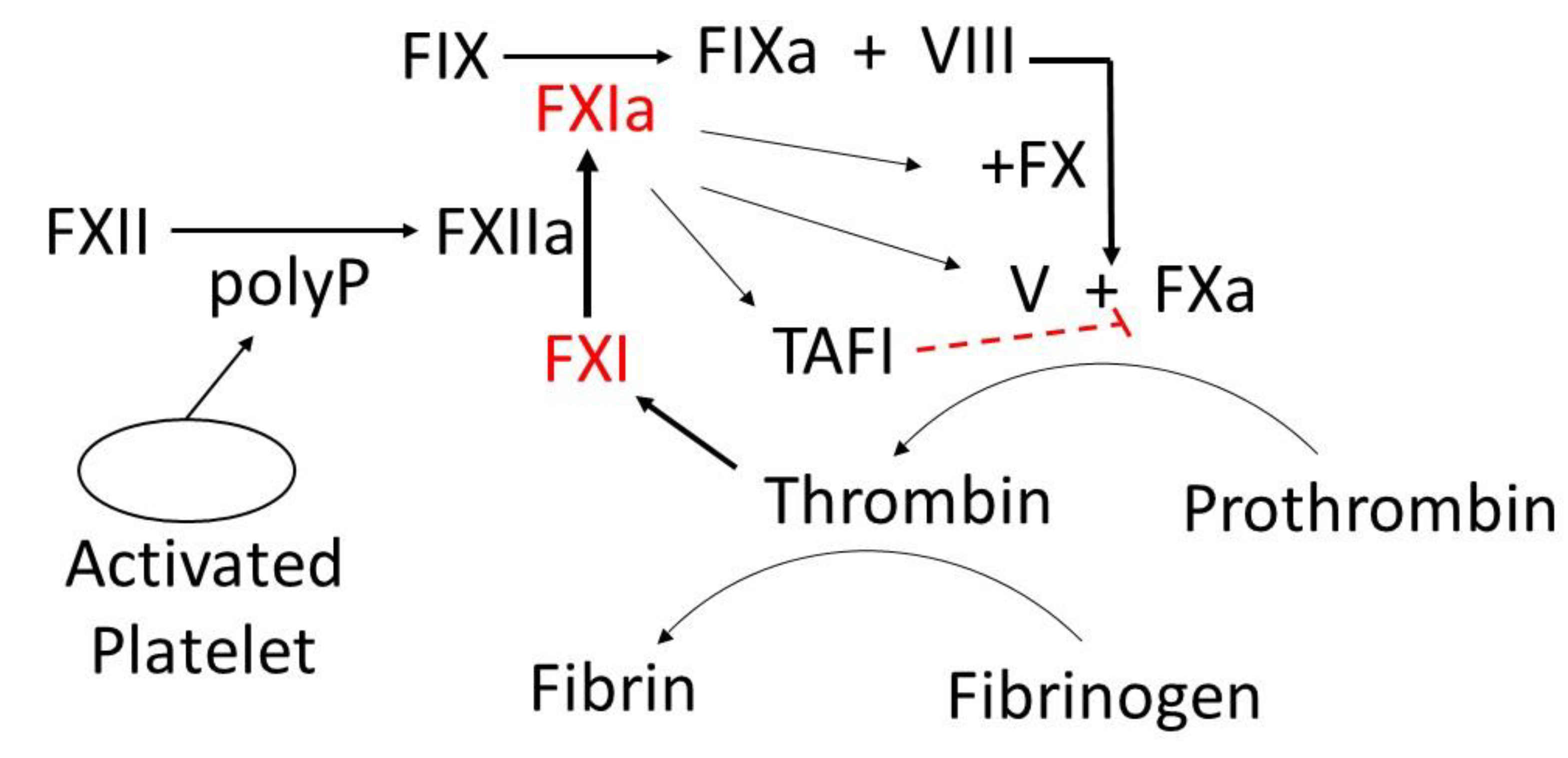
FXIa inhibitors significantly lessen subsequent or recurrent embolization [100]. Because FXI deficiency (Hemophilia C, Rosenthal Syndrome) does not manifest clinically significant bleeding disorders, one might hypothesize that FXI would be a relatively poor activator of FX. Nonetheless, this is not the case. FXI when cleaved by FXIIa (Hageman factor), forms activated factor XI (FXIa), which then activates Factor IX (FX) - mediated active FX (FXa) generation (Figure 4). FXa converts prothrombin to thrombin, a protease that converts fibrinogen to fibrin, which is responsible for trapping platelets and holding a clot in place (Figure 4). Both FXI and its substrate, Factor IX (FIX) protease, are increased in VTE [101]. FXIa/FIX complex coupled with its abundance in the blood, indicates that FXIa plays a significant role in promoting thrombus formation and that modest increases in this protease can profoundly enhance clot formation. The procoagulant property of FXIa has been studied intensively in the venous system of experimental models [102]. Patients with FXI deficiency rarely manifest hemarthroses and muscle hematomas.
When the endothelium of a blood vessel is damaged, exposing subendothelium to blood, both platelets and FXII are activated, promoting blood coagulation. Exposure of FXII to collagen leads to activation of FXII-mediated FXIa generation. Platelet-derived polyphosphate (polyP) can potentiate thrombin-feedback pathways through FXIa-mediated FIXa generation (Figure 4). Recent evidence indicates that FXIa contributes to clot formation by directly activating FX and FV [103]. The activation of FXI is also increased in the presence of thrombin[8], suggesting that thrombin circumvents the need for FXIIa to activate FXI. A positive feedback loop connected by the FXIa-mediated coagulation pathway promotes more fibrin formation (Figure 4). This positive feedback loop which enhances thrombin generation is relevant to the role of active FXI in promoting clot formation and maintaining clot stabilization. Active FXI also contributes to thrombosis through indirect activation of thrombin activatable fibrinolysis inhibitor (TAFI), which can contract fibrinolysis and pose a threat to the patient (Figure 4) [104]. An increase in FXIa-mediated activation leading to higher concentrations of active FIX, FX, thrombin [105], and TAFI can disrupt the normal equilibrium, resulting in an increased tendency to form venous thrombi. Thus, inhibition of FXIa is physiologically relevant in contexts where its concentration is elevated, such as at the site of clot formation, where thrombin is formed. Since a complete deficiency of FX in mice results in a lethal phenotype [106], inhibitors of FXIa can reduce the overconsumption of both FIX-dependent and FIX-independent FXa generation.
Figure 4.
Activation and prothrombotic activity of active Factor XI (FXIa).
Considerable progress has been made in the recent decade toward the successful development of an oral FXIa inhibitor, which could safely provide increased benefit and be used in combination with other antithrombotic for various thrombotic indications. FXIa has been successfully targeted with monoclonal antibodies, aptamers, antisense oligonucleotide inhibitors (ASOIs), natural peptides, and small synthetic molecules [107,108]. However, a few of them have reached clinical trials or market. Given the existence of several current review articles [100,108,109,110,111,112] that comprehensively cover the pharmacology and clinical efficacy of these inhibitors, we refer readers to these sources for detailed information. Phase 2 studies of different classes of FXI inhibitors are promising [113]. A recent clinical study shows that ASOIs against FXI prevent venous thrombosis in elective knee surgery. The inhibitors of FXI or FXIa are found to be effective in phase 2 studies at preventing VTE [114].
6.2. P-Selectin/PSGL-1 Pathway
Platelets have numerous adhesion proteins that are involved in platelet-platelet, platelet-endothelial, platelet-monocyte, platelet-leukocyte, and platelet-extracellular matrix (ECM) interactions. Upon activation during the course of both inflammatory and thrombogenic responses, P-selectin is released from α-granules of platelets, and from Weibel-Palade bodies of endothelial cells. P-selectin is translocated to the cell surface. P-selectin has a high affinity for PSGL-1 that is expressed on the surfaces of all leukocytes, facilitating the initial “capturing and rolling” step in the leukocyte-endothelial cell adhesion cascade [115] and adhesion in an early phase of platelet activation to limit bleeding by promoting platelet aggregation and thrombosis. Activated platelets are also capable of forming circulating aggregates with leukocytes [116] and monocytes [117] to promote systemic inflammatory responses. The inhibitors of P-selectin/PSGL-1 pathway have the potential to reduce thrombosis and inflammation (Table 3).
Excluding factor XI inhibitors, our search yielded 33 studies primarily involving modifications to existing drugs, such as variations in indications, dosage forms, dose schedules, or combinations thereof. Among these studies, we identified 4 new lead compounds. The summary of these potential new treatments is shown in (Table 3).

Table 3.
New compounds for VTE identified from recent clinical trials.
|
Conditions |
Compounds |
Mechanism of Action |
Phase |
Sponsor |
Ref. |
|---|---|---|---|---|---|
| Pulmonary embolism; thrombotic disease VTE prophylaxis with anticoagulation after total knee replacement surgery VTE Thromboembolism of vein VTE in colorectal cancer, pancreatic cancer, non-small cell lung cancer |
DS-1040b JNJ-64179375 SelK2 Isoquercetin |
Inhibits the activated form of thrombin-activatable fibrinolysis inhibitor (TAFIa). Specific exosite 1 thrombin inhibitor Targets PSGL-1 and blocks its interactions Decreases D-dimer, P-selectin, and platelet-dependent fibrin generation |
Phase1|Phase2 Phase2 Phase2 Phase2|Phase3 |
Daiichi Sankyo Janssen Research & Development, LLC Tetherex Pharmaceuticals Corporation Quercegen Pharmaceutical; National Heart, Lung, and Blood Institute (NHLBI) |
[118,119] [120,121] [122] [123] |
6.3. New Modes of Delivery for Anti-Thrombotic Drugs
While many thrombi spontaneously lyse, the fate of a thrombus depends on the persistence of increased activation of extrinsic pathway, intrinsic pathway, or reduced levels of endogenous coagulation inhibitors, such as protein C or antithrombin. Reduced levels of procoagulant proteins can lead to hemorrhage. Targeting the blood coagulation proteases therapeutically has not been an easy task due to the connectivity among them, their trypsin-like specificity, protein-protein interaction, protein-serpin interaction, protein-lipid interaction, and ions.
Although the standard anticoagulant treatment for DVT has shown remarkable progress in recent years, thrombolytic therapy has been found to be more effective in dissolving dangerous intravascular clots completely compared to anticoagulant treatment. A major advantage of thrombolytic therapy is its capability to prevent ischemic damage by improving blood flow. Like anticoagulant drugs, thrombolytic drugs have inadequate efficacy and are associated with an increased risk of hemorrhage, implying that there is room for improvement. Polymeric nanocarriers are being developed to achieve the protection and targeted delivery of thrombotic drugs. Because various functional groups can be added to nanocarrier systems that are sensitive to specific physiological environment in the circulatory system, they can be used in thrombus–targeted treatments. Nanocarrier-based delivery systems not only protect drugs from rapid degradation or excretion, but they are also capable of enhancing bioavailability and drug efficacy with respect to free drug formulations. Furthermore, nanocarrier systems exhibit robust successes in targeted delivery of antithrombotic drugs to the desired tissues and cells and enhanced intracellular delivery. In this section, we review FXI and the recent nanocarrier-based delivery systems that can offer solutions to common problems faced by several anticoagulant and thrombotic treatments. These include the following: (1) Polymers; (2) Dendrimers (3) PEGylation; (4) Liposomes; (5) Echogenic liposomes; (6) Polymeric nanoparticles; (7) Mechanically activated nanotherapeutics; (8) Fucoidan-functionalized nanocomplex; (9) Platelet-based drug delivery system; and (10) Combinational therapy.
6.3.1. Polymers
Although anticoagulant therapy remains the first line of treatment for VTE, the efficiency of treatment via optimization of more effectively delivering a therapeutic agent to a target site remains a major goal of current scientific research. Therapeutic antibodies, proteins, and nucleic acids are highly susceptible to oxidation, aggregation, degradation, and elimination. Over the past decade, the therapeutic approach of biological therapy (macromolecules or biologics) has gained momentum due to its potentially superior effects compared with small molecules. They exhibit much higher specificity than small molecule drugs. They tend to be more efficient, safer, and cause fewer unwanted side effects. Recent advances in nanomedicine (nanostructured polymers) offer new tools for delivering and maintaining therapeutic concentrations of drugs and releasing them (passively or actively) at the target site. The U.S. Food and Drug Administration (FDA) basically describes nanomedicines as products in the nanoscale range (1−100 nm) [124]. While nanomedicine with 10 nm is found in several compartments, including blood, spleen, kidney, testis, thymus, heart, lung, and brain, larger ones are detected in blood, spleen, and liver [125]. Effective and long-acting nanomedicines have shown enormous potential as therapeutics for the treatment and management of various human diseases, including pain, advanced prostate cancer, tumor-targeted delivery, Alzheimer’s disease, and Parkinson’s disease. Nanomedicine encompasses a suitable biodegradable polymer, a carrier, and an active drug or a prodrug. The drugs are generally conjugated or encapsulated by polymeric nanocarriers. A drug-polymeric nanocarrier complex is known as polymeric nanomedicine Table 4). Nanobiopolymers, products biosynthesized by living organisms, are emerging as a promising class of materials that play a vital role within the field of medicine, including controlled cancer drug delivery and gene delivery. Classification of nanomedicine platforms is based on its nanocarrier such as organic (polymer-based and lipid-based), inorganic, crystalline, or amorphous particles [126]. Organic nanomaterials (lipid-based systems) are characterized as one of the most promising innovative polymeric nanocarriers, which are now FDA-approved [127] and their respective therapeutic utility [128]. Organic nanomaterials exhibit a variety of different architectures including micelles, liposomes, dendrimers, polymersomes, hydrogels, and metal–organic compounds. Recently, organic nanomaterials have been used for the development of polymeric nanobiopolymers to attain a thrombolytic drug-loading system (Table 4). Although considerable progress has been made in the development of polymeric nanocarriers that encapsulate and deliver a controlled release of the drug to the thrombus site, the clinical translation of polymeric nanocarriers is limited.
6.3.2. PEGylation
PEGylation is a process where polyethylene glycol (PEG) chains are attached to molecules or proteins and has been used in the development of numerous therapies in the clinic. PEGylated drugs are shown to have increased circulation time [163], decreased immunogenicity [164], improved stability [165], solubility [166], bioavailability [166], and targeting and delivery [167]. However, the size of the PEG group itself can have unfavorable impacts on either the activity or pharmacokinetic behavior of the drug [168]. Other potential drawbacks of the clinical translation of PEGylated therapeutic proteins are hindered by manufacturing challenges, intracellular uptake of PEG, size enlargement, release of PEG antibodies and reduced activity of the drug [169,170].
Recently, PEGylation with various biophysiochemical properties has been designed to explore drug-targeting delivery carriers of different anti-thrombotic drugs for the treatment of DVT. PEGylation for thrombolysis is used for a wide range of drugs such as tissue plasminogen activator (tPA) [171,172], Staphylokinase(SAK) [173], urokinase (UK) [174], streptokinase (SK) (Table 3) [175]. Qi et al. [173] utilized PEG maleimide to conjugate multiple Staphylokinase (SAK) molecules, aiming to enhance their bioactivity and extend their half-life. However, the bioactive domain of SAK was unable to interact with its receptor effectively due to the steric shielding effect of PEG, which resulted in reduced bioactivity of SAK. Despite this, the conjugation improved the thermal stability of SAK molecules and did not cause detectable harm to the liver, kidney, or heart in mice. Zamanlu et al. [172] utilized PEGylation to create polymer-protein nanoparticles using poly(lactic-co-glycolic acid) (PLGA) and tPA. The study concluded that this approach may improve the biological half-life of tPA, potentially addressing clinical challenges and allowing for controlled and predictable drug release kinetics [173]. Developing improved therapies for VTE and other thrombotic conditions presents significant challenges. To enhance the effectiveness and safety of new treatments over current options, researchers must focus on two key areas. First, they need to refine PEG-conjugated thrombolytic agents to boost their activity and extend their half-life, thereby improving the relevance and translatability of preclinical models. Second, it's crucial to advance pharmacological approaches by identifying specific targets for these agents, optimizing their pharmacokinetic properties, and assessing their thrombotic action in multiple mouse models of venous thrombosis. This comprehensive approach will better capture the complexity of venous thrombosis and strengthen the foundation for translational research, ultimately leading to more effective and tolerable therapies for patients.
6.3.3. Liposomes
Liposomes are spherical vesicles with a size range of 50 to 500 nm in diameter, and are primarily made of phospholipids such as soybean phosphatidylcholine, synthetic dialkyl or trialkyl lipids [176]. During liposome preparation, cholesterol is incorporated into liposomes not only to modulate membrane permeability and fluidity [177], but also to improve the stability of the vesicle membrane in the presence of biological fluids such as blood and plasma. Liposomes containing polymers [178] and even membrane protein [179] offer multiple benefits to overcome the limitations of both the traditional drug dosage forms and conventional liposomes, the first generation of liposomes. These benefits include prolonged circulation half-life, enhanced localization of drug in the desired tissue, enhanced localization of drug in the desired tissue [180], and improved effectiveness of the encapsulated drug. Moreover, the incorporation of phospholipids-attached PEG [181] into the chemical structure of liposomes represents another approach to enhance the pharmacokinetic properties and biodistribution profiles of liposomes. Small molecules make up about 90% of all prescriptions [182]. The therapeutic effect of small hydrophilic molecules is limited by their poor pharmacokinetics and biodistribution. A recent review delves into obstacles in hydrophilic drug delivery and elucidates the design of liposomal carriers for small hydrophilic molecules that can provide solutions [183]. Hydrophobic and hydrophilic characteristics of liposomes create two distinct compartments in which drug molecules are encapsulated in the aqueous compartment of the vesicles or in the lipophilic membrane compartment. Liposomes are proven to be ideal carriers for a range of drugs as well as diagnostic and targeted drug delivery applications. FDA has approved a wide range of liposomal-based drug delivery systems for treating and preventing human diseases [184].
Liposomes loaded with various antithrombotic drugs are considered to lack proven clinical applications [185]. Currently, a number of liposome formulations are in preclinical use to deliver thrombolytic drug molecules for treating arterial thromboembolic diseases, myocardial infarction, and stroke, as well as VTE, deep vein thrombosis and pulmonary embolism (Table 3). Staphylokinase (SAK), an indirect activator of plasminogen, is a secretory enzyme produced by staphylokinase [186]. An in-depth analysis of the impact of the interaction of the SK variants with antimicrobial peptides has been explored [187]. However, the involvement of staphylokinase variants in activating plasminogen remains a dilemma. Encapsulated staphylokinase in temperature-sensitive liposomes appears to be promising [188]. Low molecular weight heparin (LMWH) in an intermediate dose outperforms other anticoagulant drugs for the prevention of VTE [189]. However, it requires systemic routes of administration (e.g., injection). Encapsulated LMWH-liposome construct exhibits a long half-life in circulation [190]. Cationic flexible liposomes demonstrate a higher entrapment efficiency of LMWH compared to neutral and anionic flexible liposome formulations [191]. Topical application of LMWH-cationic flexible liposomes deeply penetrated into the skin [191], thereby suggesting this formulation may be a compelling ally for the treatment of superficial thrombosis. Over a decade later, inhalable distearoyl-sn-glycero-3-phosphoethanolamine (DSPE) and long-circulating pegylated liposomes of LMWH are found to be effective in reducing thrombus weight, and are suggested to be a potential noninvasive approach for DVT and PE treatment [135]. However, there is no clinical evidence yet to corroborate that encapsulated HMWH-liposomes are effective therapeutics in humans.
6.3.4. Echogenic Liposome
Several targetable, drug-carrying echogenic liposome preparations have been developed following reports of multiple patient deaths due to the injection of ultrasound contrast agents [192,193]. Echogenic liposomes (ELIPs) are lipid-bilayer agents [194] that contain gas-filled monolayered microbubbles and sonosensitive vesicles. Gas vesicles are capable of scattering sound waves and, therefore, produce ultrasound contrast [195]. ELIPs are not only an ultrasound contrast agent, but also an ultrasound-activating drug delivery system [196,197]. While ELIPs were initially loaded with methotrexate (MTX), they have been loaded with a variety of therapeutic agents, such as hydrophilic and lipophilic drugs, proteins, and peptides. To learn more about echogenic liposomes, the latest progress in echogenic liposome preparations, characteristics, and applications can be found in an excellent review of drug delivery [198]. Single chain urokinase-tPA (sutPA)-loaded ELIPs specifically bind to fibrin (Table 4) [199]. Ultrasound significantly increased lytic treatment efficacy for recombinant tPA-loaded ELIPs [200]. tPA-loaded ELIPs are suitable for ultrasound-detectable local drug delivery [201]. tPA-loaded ELIPs have the potential to serve as a therapeutic antithrombotic agent in the treatment of DVT or PE [202]. Moreover, it allows a lower dosage of thrombolytic drugs to be used. Since the effectiveness of tPA-loaded ELIPs has been tested, exploring the effect of drug interactions and improving the understanding of risk factors associated with the pathogenic changes that occur in the blood vessel wall is important for developing more effective antithrombotic drugs.
6.3.5. Polymeric Nanoparticles
Polymeric nanoparticles can be used to deliver thrombolytic drugs. Several factors, including size, surface charge, and the presence or absence of a polymer coating, influence the clearance and biodistribution of nano- and microcarriers [203]. Lipid-based nanocarriers are liposomes, which were discussed earlier. Synthetic and natural polymers are employed in the design of nano- and micro-carriers for thrombolytic drugs. These polymers offer the advantage of greater resistance to mechanical stress compared to lipid-based carriers [204].
Inorganic nanocarriers used for the delivery of thrombolytic drugs are primarily represented by magnetic nanoparticles. Therapeutic agent-loaded magnetic nanoparticles drawn to the thrombus surface in response to an external magnetic field. Magnetic nanoparticles are biodegradable and participate in the iron homeostasis of the body [205,206,207,208]. Fithri et al. [147] worked on developing gold-iron oxide nanoparticles (AuIONP(+)) for thrombosis. AuIONP(+), a theranostic agent (referred to as a combination of diagnostic and therapeutic agents), in antithrombotic therapy due to the site-specific delivery of antithrombin agents to the targeted activated platelets, showed excellent antithrombotic activity. While AuIONP(+) is capable of binding to thrombi, including the exhibition of excellent properties for photoacoustic imaging of thrombus, good biocompatibility, as well as the signs of successful thrombolysis and complete thrombus elimination was not achieved [147]. However, AuIONP(+) partially restores blood flow. Zhang et al. [209] developed a novel multifunctional nanoplatform for thrombolytic therapy. This mesoporous nanoplatform has the following two key features: (1) near−infrared, alternating magnetic field and (2) urokinase plasminogen activators (uPA)−loaded Metal−Organic-Framework (MOF) derived carbon−based materials (referred to uPA@CFs). uPA@CFs exhibit near-infrared (NIR)-stimulated uPA release and heat the thrombosis at DPV via alternating magnetic field. uPA@CFs showed a high loading ability of the uPA, good NIR-stimulated uPA release, and good photothermal conversion efficiency, addressing the issue of low drug utilization rates [209].
Zhong et al. [210] worked on ultrasound-responsive phase-transitional nanoparticles for thrombolysis using Fe3O4-PLGA-PFH-CREKA nanoparticles (NPs). This well-developed phase transition agent responded effectively to low-intensity focused ultrasound (LIFU) by triggering the vaporization of liquid perfluorohexane (PFH) to achieve thrombolysis and CREKA peptide, which binds to fibrin in the thrombus, enabling targeted imaging and effective thrombolysis. LIFU-responsive photothermal (PT) thrombolysis reduced thrombus burden post-irradiation without impairing vascular tissue [210].
6.3.6. Dendrimers
Delivering accurate doses could be challenging. Precise control over the distribution of a drug in the body is a strategy to promote the accurate dose at a specific tissue site while minimizing deleterious side effects. Dendrimers, as vehicles for drug delivery systems, provide high-capacity loading and sustained release profiles. Dendrimers are highly valuable because they can address the challenges of clearance and inactivation; thereby, dendrimer-based drug delivery has attracted increasing interest for numerous reasons. Due to their site-specific delivery capability, various dendrimers and dendrimer derivatives [211] have been developed [212] and utilized for a variety of diseases [213] since their discovery in 1978 [214]. Unlike traditional polymers, dendrimers are synthetic macromolecules of nanometer dimensions. Dendrimers have attractive properties, including high solubility, low viscosity, great mixability, biodegradability, good biocompatibility, as well as high reactivity. Dendrimers have been attracting a growing interest mainly because of their characteristics, including a regularly branched tree-like structure [215], well-defined globular structures [216], the ability to attach functional groups to the chain ends of dendrimers, variable chemical composition, capability of storing [217] various carbon-rich guests with hydrophilic or hydrophobic nature via electrostatic interaction or covalent bonding, and high biological compatibility. Dendrimers are customizable nanotechnologies. The delivery of the therapeutic agents at specific sites in the body has been attained by surface modification of the terminal ends of dendrimers using numerous targeting moieties such as folic acid [218], peptides [219], monoclonal antibodies [220] and sugar groups [221]. These features allow them to be an ideal carrier for drug delivery and hold promise in increasing selectivity, reducing off-target effects, and decreasing unwanted toxicities.
Evidence indicates that amine-terminated dendrimers cause disseminated intravascular coagulation-like conditions via acting on fibrinogen in a thrombin-independent manner [156] and cationic dendrimers have been shown to activate platelets, leading to disrupted morphology [222]. Interestingly, cationic dendrimers are capable of inhibiting the extrinsic activation pathway of the coagulation system leading to prolonged prothrombin time and suppressing thrombin generation in plasma [223]. Neutral dendrimers [224] are not hemolytic and do not alter platelet morphology or their function in vitro. Dendrimers with low molecular weight [225] improve the storage time of platelets. Dendrimers have emerged as vectors for delivering clot-busting therapeutics to the target site concurrently preventing access to the nontarget site due to the availability of multiple functional groups. Tissue plasminogen activator, a clot-busting drug, is used in treating stroke. The tPA-dendrimer complex is found to have the highest clot-dissolving activity compared to that of control tPA (Table 4) [152]. Nattokinase is used for thrombolytic therapy. It has tPA activity and is capable of directly digesting fibrin via limited proteolysis. Evidence indicates that the nattokinase-dendrimer complex possesses a great thrombolysis ability both in vitro and in vivo (Table 4) [226]. Future studies are warranted to address whether the thrombolytic-neutral dendrimer complex is more effective than those of the current anticoagulants and better understand the complex pharmacology and interaction of thrombolytic-neutral dendrimer complex within preclinical models (small and large animals) and their respective biological systems including thrombus microenvironment.
6.3.7. Mechanically Activated Nanotherapeutics
Restrictions of normal blood flow are due to stenosis, thrombosis, embolism, or hemorrhage, which can lead to poor circulation. The leading causes of circulation problems are peripheral vascular disease, atherosclerosis, stroke, placental microthrombosis, and VTE. During the last decade, various types of nanoparticles have been prepared to accurately identify the thrombus and to be used for targeting various analytes such as antiplatelet and thrombolytic drugs. Herein, we highlight recent developments on stimuli-responsive nanoparticles (e.g., mechanosensitive nanoparticles), nanogels (e.g., hydrogels), and multicomponent nanoparticles (e.g., fucoidan (Fuc, a P-selectin ligand)-based core-shell nanoparticles). Our goals are: (1) to highlight the successful development of novel drug delivery systems that not only allow the drug to be localized on the thrombus to cause thrombolysis but also are characterized to reduce drug toxicity and adverse effects, and (2) to underscore how certain nanoparticles loaded with antithrombotics alone or in combination with anti-inflammatory, antioxidant and endothelial protective agents could potentially become more effective treatment for VTE and lessen the harms associated with side effects of anticoagulants and antithrombotics. Below, we focus on the update of these nanoparticles that possess high potential for the treatment of VTE. Structures, properties, and recent applications of hydrogels have been addressed before in excellent work by others [227,228].
Mechanosensitive micrometer-sized aggregates of nanoparticles function as stimuli-responsive drug carriers, designed to release their payload within blood vessels by high-fluid shear stresses at sites of vascular obstruction [159,160]. The intravenous administration of shear−activated micrometer aggregates of nanoparticles coated with tPA induces rapid clot dissolution in a mesenteric injury model [159]. It is well-established that the blood shear stress at the thrombus site is significantly greater than the force that the blood flow exerts on the vessel wall of normal arteries. A positive correlation between platelet deposition at the thrombus site and the increasing shear rate is reported [229,230,231], highlighting that the activation and aggregation of platelets are due to high shear stresses. However, characteristics of the underlying vessel, such as the stenotic length and contraction angle of stenosis appear to cause shear-dependent platelet aggregation formation [232]. Thus, thrombus formation and its complications are complex, multifactorial conditions in which both non-genetic and genetic factors are involved. Zhang et al. [233] explored the development of a novel drug delivery platform using the antiplatelet drug tirofiban (TI) and the thrombolytic drug urokinase (UK) in fucoidan (Fuc, a P-selectin ligand)−based core-shell nanoparticles (referred to UK@Fuc-TI/PPCD). P-selectin is expressed on both activated endothelial cells and activated platelets [234] under inflammation-related pathologic states [235], during thrombus development [236], and cancer progression [236]. The key features of the UK@Fuc-TI/PPCD platform are its ability to bind specifically to its target antigen, P-selectin, and its mechanosensitive capability that preferentially releases its payload under elevated shear stress. Despite its limited characterization, the use of UK@Fuc-TI/PPCD in preclinical studies as a therapeutic to dissolve blood clots looks promising. The emerging role of inflammation and ROS in metabolic disorders [237] and the interplay between inflammation and thrombosis [238] has generated increasing interest in developing an advance drug delivery system that is activated at sites of thrombus development to circumvent these problems. The focus here is on specific areas in research concerning complications of thrombosis (inflammation, reactive oxygen species (ROS) production, and endothelial perturbation) using hydrogels for therapeutic delivery. Hydrogel, the first biomaterial, is initially used to make the first soft contact lens [239]. While ordinary hydrogels exhibit the swelling-deswelling behavior in water, advanced hydrogels with tunable properties [240,241,242,243] are designed to change their properties in response to a subtle change in a tissue microenvironment. Hydrogel-based drug delivery systems are clinically offering targeted delivery and tissue repair at the site of injury, such as wound dressing [244], plastic surgery, and as tissue sealant [245]. Injectable hydrogel appears to be a promising candidate for wound healing therapy. Evidence indicates that ibuprofen−loaded heparin-modified thermosensitive hydrogel may be capable of inhibiting inflammation and improving wound healing [246]. Inflammation-responsive drug-loaded hydrogels in combination with encapsulation with vancomycin (an antibiotic)-conjugated silver nanoclusters and pH-sensitive micelles loaded with nimesulide, a nonsteroidal anti-inflammatory drug, exhibit wound healing in streptozotocin-induced diabetes in rats through antibacterial, anti-inflammatory processes [247]. Similarly, injectable hyaluronic acid hydrogel in combination with antioxidant gallic acid-grafted hyaluronic acid promotes the microglia polarization to M2 phenotype and exhibits antioxidant activity [248]. To learn more about nanotherapeutics, the reader is referred to several excellent reviews of nanoparticles and their associated challenges for therapeutic delivery [227,249,250,251,252,253]. The recent advances achieved with thrombus-targeting, inflammation-targeting, antioxidant-targeting, and endothelial-targeting nanocarriers could lay the foundation to accelerate the development of polymeric nanocarriers containing a combination of antithrombotic, antiinflammatory, antioxidant agents for the treatment of thrombosis and the clinical translation of each of these polymeric nanocarriers.
6.3.8. Platelet-Based Drug Delivery System
Platelets are the smallest anucleated cells that circulate within the blood circulatory system. They respond to both intravascular and blood vessel environmental signals. They are terminally differentiated and may have a circulatory life span of up to seven days. Platelets, or thrombocytes, serve as sentinel cells to detect vascular injury in many living species throughout the evolutionary tree. Central to their function is their ability to communicate continually with normal blood vessel endothelial cells via paracrine signaling. Excessively low levels of the paracrine signaling due to endothelial dysfunction [254] or an injury, quiescent platelets that circulate in the blood stick to the damaged tissue and transform into their active formation. The activated platelets recruit and activate more platelets to the site of vascular injury through a combination of paracrine- and autocrine-mediated signaling mechanisms via the release of platelet activators, namely thromboxane A2, adenosine diphosphate (ADP), and calcium from platelets. The activated platelets also establish a feed-forward mechanism that amplifies the coagulation cascade allowing for rapid generation of thrombin. Formed thrombin causes platelets to release the contents of their granules, undergoing morphological change, among many other functions as mentioned earlier. This state, known as ‘aggregation’ is important for a wide range of protective physiological responses, including coagulation, complement, inflammatory, and immune that are effective against a diverse variety of threats. Platelet aggregation is essential for healing to occur because they adhere to one another to form a temporary hemostatic plug, thrombus, to seal an injury, initiating the process of hemostasis. Over the last three decades, as we have learned more about how the above-mentioned physiological processes are pivotal for the progression of wound healing and tissue repair, it has become clear that there is an extensive crosstalk among them. Activation of one system influences the functional ability and activity of the other. For instance, excess platelet activation is linked to the thrombo-inflammatory process [255,256]. Elevated C3, a complement component, levels are implicated as a DVT risk factor in humans [257]. Unregulated immune and inflammatory processes can promote thrombosis [258]. Besides the coagulation system, abnormal activation of complement, immune and inflammatory systems are key players in the pathophysiology of DVT. A detailed summary of platelet adhesion, activation, and aggregation is reviewed elsewhere [259].
Not only do platelets control thrombosis but also mediate VTE, stroke, and myocardial infarction [260]. The innate roles of platelets in DVT are supported by the fact that aspirin (Table 1), an inhibitor of thromboxane A2 (a potent activator of platelets) synthesis, reduces VTE in patients undergoing orthopedic surgery [261]. Adhesion of platelets to the site of injury is mediated via the interaction between GPIbα, a platelet membrane receptor, and the von Willebrand factor (vWF) exposed on the endothelial surface [262], suggesting vWF mediates platelet activation. Evidence also shows that vWF mediates platelet aggregation through binding to GPIIb/GPIIIa, a platelet membrane glycoprotein [263,264], as described below. Evidence for a consistent role of platelet-endothelial interaction is described in the venous thrombus [258]. Elevated generation of ROS promote platelet recruitment to the developing venous thrombus, leading to thrombus growth [265]. Regardless of triggers, activation of platelets results in conformational changes (inside-out signaling) of GPIIb/IIIa, a platelet membrane protein. This conformational altered GPII/IIIa has a specific binding affinity for soluble plasma fibrinogen or other plasma molecules (vWF, fibronectin, and vitronectin) [266] with the RGD domain. The bivalent fibrinogen serves to connect two adjacent activated platelets through its specific binding site on platelets [267], allowing platelet aggregation and thrombus formation. GPIIb/IIIa has a pivotal role in the formation of platelet thrombi. The inhibitors of GPIIb/IIIa inhibit shear-induced platelet aggregation (Table 1) [268].
In view of the above studies conducted on platelet properties, significant progress in the research on biomimetic drug delivery systems has been achieved. The platelet (P) membrane is attached onto the surface of a nano-drug delivery system, poly(lactic-co-glycolic acid; PLGA), an FDA-approved polymeric core [269], to generate P-camouflaged polymeric nanoparticles (nanoplatelets), PNP [162]. Then, a site-specific conjugation technique is used that involves the conjugation of recombinant tPA (rtPA) to the activated sulfhydryl groups residing on the external surface of the platelet membrane of nanoplatelet to construct PNP-PA (Table 4). This construct aims to help target the delivery of thrombolytic drug to local thrombus sites. PNP-PA is found to have a dual benefit of possessing the major membrane adhesion-associated proteins (GPIIb/IIIa and P-selectin), thereby improving PNP-PA recruitment to the thrombus site, and the ability to achieve targeted thrombolysis. PNP-PA exhibits a low risk of bleeding complication in different animal models of thrombosis [162]. Although anticoagulants are generally used to treat DVT or PE, PNP-PA appears to be a promising agent to treat both arterial and venous thrombi.
Using a conceptually-derived strategy in a platelet-based drug delivery system, PNP-loaded lumbrokinase (LBK), a fibrinolytic enzyme, is constructed to form nanoplatelets (PNPs/LBK) to target the thrombus site [270]. Like PNP-PA, after binding of PNPs/LBK to the active platelet integrin GPIIb/IIIa and P-selectin on thrombus, LBK is released. LBK is released by phospholipase-A2-induced vesicle destabilization. Administration of PNPs/LBK has little effect on the bleeding time compared to free LBK. PNP/LBK is a promising antifibrinolytic agent, which can effectively target the thrombus site and prevent hemorrhagic episodes.
7. Future Implications and Research Opportunities
The ongoing development of antithrombotic drugs and advanced delivery systems presents significant opportunities to improve the management of VTE, a condition of increasing importance due to the rapidly aging global population. As the prevalence of chronic diseases rises among older adults, the risk of VTE and its associated complications become more pronounced, necessitating more effective and safer treatment options. Future research should focus on the identification and validation of novel targets within the coagulation cascade, particularly those that can provide a more precise modulation of thrombin activity in elderly patients with multiple comorbidities. The development of next-generation anticoagulants that offer enhanced efficacy and safety profiles compared to existing DOACs is crucial, especially for this vulnerable population. These new agents should aim to minimize bleeding risks while providing robust protection against thromboembolic events, considering the unique physiological changes and potential drug interactions in older adults. Additionally, understanding the molecular mechanisms underlying individual variability in response to antithrombotic therapy could lead to more personalized treatment approaches, optimizing therapeutic outcomes for diverse patient populations across different age groups and comorbidity profiles. This personalized approach is particularly relevant for the aging population, where tailored interventions can significantly impact quality of life and reduce the burden on healthcare systems.
Moreover, the integration of advanced drug delivery systems, such as nanoparticle-based carriers and targeted delivery mechanisms, holds promise for enhancing the specificity and bioavailability of antithrombotic agents. These technologies could enable localized drug delivery, reducing systemic exposure and associated side effects, which is especially beneficial for older patients who may be more susceptible to adverse drug reactions. Of particular interest is the development of nanothrombolytic particles, which have shown significant potential in preclinical studies for the treatment of VTE. These nanoparticles can potentially deliver thrombolytic agents directly to the site of thrombosis, enhancing efficacy while minimizing systemic side effects. However, more extensive research is needed to fully elucidate their safety profile, optimal dosing regimens, and long-term outcomes in diverse patient populations, including the elderly. Investigating the potential of combination therapies that synergistically target both platelet function and coagulation pathways may also yield significant benefits in preventing VTE recurrence and improving patient outcomes across all age groups. Furthermore, long-term clinical studies are essential to evaluate the real-world effectiveness and safety of these emerging therapies, particularly in the context of an aging population with multiple comorbidities. Collaborative efforts between academic institutions, industry, and regulatory bodies will be vital to accelerate the translation of these innovations from bench to bedside, ultimately advancing the standard of care for patients with VTE. As the global population continues to age, prioritizing research in these areas will be crucial for developing more effective, safer, and tailored antithrombotic strategies that can address the unique challenges posed by VTE in older adults and those with chronic diseases.
Author Contributions
Conceptualization, Z.S.-M.; writing—original draft preparation, Z.S.-M.; writing—review and editing, Z.S.-M., M.S., A.A. and SN; supervision, Z.S.-M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The original contributions in the study are included in the article, further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| ACCP | American College of Chest Physicians |
| ADP | Adenosine Diphosphate |
| AIDS | Acquired Immunodeficiency Syndrome |
| APTT | Activated Partial Prothrombin Time |
| ASOIs | Antisense Oligonucleotide Inhibitors |
| AuIONP+ | Gold-Iron Oxide Nanoparticles |
| C1-Inhibitor | C1-Esterase Inhibitor |
| CAD | Chronic Artery Disease |
| CKD | Chronic Kidney Disease |
| COX | Cyclooxygenase |
| CREKA | Cys-Arg-Glu-Lys-Ala |
| CRP | C-Reactive Protein |
| DIC | Disseminated Intravascular Coagulation |
| DOACs | Direct Oral Anticoagulants |
| DSPE | 1,2-Distearoyl-Sn-Glycero-3-Phosphoethanolamine |
| DVT | Deep Vein Thrombosis |
| ECM | Extracellular Matrix |
| ELIP | Echogenic Liposomes |
| FDA | U.S. Food and Drug Administration |
| FDP | Fibrin Degradation Products |
| Fibrinogen | Factor I |
| FIX | Factor IX |
| FIXa | Activated Factor IX |
| Fuc | Fucoidan |
| FVII | Factor VII |
| FVIIa | Activated Factor VII |
| FVIII | Factor VIII |
| FVIIIa | Activated Factor VIII |
| FX | Factor X |
| FXa | Activated Factor X |
| FXI | Factor XI |
| FXIa | Activated Factor XI |
| FXII | Factor XII |
| FXII | Factor XIII |
| FXIIa Hageman Factor | Activated Factor XII |
| FXIIIa | Activated Factor XIII |
| GI | Gastrointestinal |
| GP IIb/IIIa | Glycoprotein IIb/IIIa |
| HMWH | High-Molecular-Weight Heparin |
| INR | Target International Normalized Ratio |
| LBK | Lumbrokinase |
| LIFU | Low-Intensity Focused Ultrasound |
| LMWH | Low-Molecular-Weight Heparin |
| MOF | Metal-Organic-Framework |
| MTX | Methotrexate |
| NHLBI | National Heart, Lung, and Blood Institute |
| NIR | Near-Infrared |
| NPs | Nanoparticles |
| NSAIDs | Non-Steroidal Anti-Inflammatory Drugs |
| P2Y12 | Purinergic Receptor Type Y, Subtype 12 |
| PA | Plasminogen Activator |
| PAI | Plasminogen Activator Inhibitor |
| PE | Pulmonary Embolism |
| PEG | Polyethylene Glycol |
| PFH | Perfluorohexane |
| PLGA | Poly(Lactic-Co-Glycolic Acid) |
| PNP | P-camouflaged Polymeric Nanoparticles |
| polyP | Platelet-Derived Polyphosphate |
| PPACK | D-phenylalanyl-L-prolyl-L-arginyl-chloromethyl Ketone |
| PPCD | Doxorubicin-Polymer Conjugates |
| Prothrombin | Factor II |
| PSGL-1 | P-selectin Glycoprotein Ligand-1 |
| PT | Prothrombin Time |
| RGD | (Arg-Gly-Asp) Peptide |
| ROS | Reactive Oxygen Species |
| rtPA | Recombinant tPA |
| SAK | Staphylokinase |
| SCAD | Spontaneous Coronary Artery Dissection |
| SK | Streptokinase |
| SNP | Single Nucleotide Polymorphism |
| TAFI | Thrombin-Activated Fibrinolysis Inhibitor |
| TF | Tissue Factor |
| TFPI | Tissue Factor Pathway Inhibitors |
| Thrombin | Activated Factor II |
| tPA | Tissue-Type Plasminogen Activator |
| TT | Thrombin Time |
| U.S. | United States |
| UK | Urokinase |
| UK@Fuc-TI/PPCD | Urokinase (UK) in Fucoidan-Based Core-Shell Nanoparticles |
| uPA | Urokinase-Type Plasminogen Activator |
| uPA@CFs | Urokinase Plasminogen Activators (uPA)-Loaded Metal-Organic-Framework (MOF) Derived Carbon-Based Materials |
| VTE | Venous Thromboembolism |
| vWF | Von Willebrand factor |
References
- Beckman, M. G.; Hulihan, M. M.; Byams, V. R.; Oakley, M. A.; Reyes, N.; Trimble, S.; Grant, A. M. , Public health surveillance of nonmalignant blood disorders. Am J Prev Med 2014, 47, (5). 664–8. [Google Scholar] [CrossRef] [PubMed]
- Wendelboe, A. M.; Raskob, G. E. , Global Burden of Thrombosis: Epidemiologic Aspects. Circ Res 2016, 118, (9). 1340–7. [Google Scholar] [CrossRef] [PubMed]
- Beckman, M. G.; Hooper, W. C.; Critchley, S. E.; Ortel, T. L. , Venous thromboembolism: a public health concern. Am J Prev Med 2010, 38, (4 Suppl). S495–501. [Google Scholar] [CrossRef]
- Huang, W.; Goldberg, R. J.; Anderson, F. A.; Kiefe, C. I.; Spencer, F. A., Secular trends in occurrence of acute venous thromboembolism: the Worcester VTE study (1985-2009). Am J Med 2014, 127, (9), 829-39.e5.
- Naess, I. A.; Christiansen, S. C.; Romundstad, P.; Cannegieter, S. C.; Rosendaal, F. R.; Hammerstrøm, J. , Incidence and mortality of venous thrombosis: a population-based study. J Thromb Haemost 2007, 5, (4). 692–9. [Google Scholar] [CrossRef]
- Lutsey, P. L.; Zakai, N. A. , Epidemiology and prevention of venous thromboembolism. Nat Rev Cardiol 2023, 20, (4). 248–262. [Google Scholar] [CrossRef] [PubMed]
- Søgaard, K. K.; Schmidt, M.; Pedersen, L.; Horváth–Puhó, E.; Sørensen, H. T. , 30-Year Mortality After Venous Thromboembolism. Circulation 2014, 130, (10). 829–836. [Google Scholar] [CrossRef] [PubMed]
- Bagot, C. N.; Arya, R. , Virchow and his triad: a question of attribution. Br J Haematol 2008, 143, (2). 180–90. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, H. K. , Pathophysiology of venous thromboembolism. Semin Thromb Hemost 1991, 17 Suppl 3, 250–3. [Google Scholar]
- Ortel, T. L.; Neumann, I.; Ageno, W.; Beyth, R.; Clark, N. P.; Cuker, A.; Hutten, B. A.; Jaff, M. R.; Manja, V.; Schulman, S.; Thurston, C.; Vedantham, S.; Verhamme, P.; Witt, D. M.; D. Florez, I.; Izcovich, A.; Nieuwlaat, R.; Ross, S.; J. Schünemann, H.; Wiercioch, W.; Zhang, Y.; Zhang, Y. American Society of Hematology 2020 Guidelines for Management of Venous Thromboembolism: Treatment of Deep Vein Thrombosis and Pulmonary Embolism. Blood Advances 2020, 4, (19). 4693–4738. [Google Scholar] [CrossRef] [PubMed]
- Stewart, L. K.; Kline, J. A. , Metabolic syndrome increases risk of venous thromboembolism recurrence after acute deep vein thrombosis. Blood advances 2020, 4, (1). 127–135. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Ge, H.; Wang, X.; Zhang, X. , Association Between Blood Lipid Levels and Lower Extremity Deep Venous Thrombosis: A Population-Based Cohort Study. Clin Appl Thromb Hemost 2022, 28, 10760296221121282. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Feng, R.; Jiang, S.; Chang, G.; Hu, Z.; Yao, C.; Jia, B.; Wang, S.; Wang, S. , Stent patency rates and prognostic factors of endovascular intervention for iliofemoral vein occlusion in post-thrombotic syndrome. BMC Surg 2022, 22, (1). 269. [Google Scholar] [CrossRef] [PubMed]
- Cogo, A.; Bernardi, E.; Prandoni, P.; Girolami, B.; Noventa, F.; Simioni, P.; Girolami, A. , Acquired risk factors for deep-vein thrombosis in symptomatic outpatients. Arch Intern Med 1994, 154, (2). 164–8. [Google Scholar] [CrossRef]
- Hosseini, S.; Kalantar, E.; Hosseini, M. S.; Tabibian, S.; Shamsizadeh, M.; Dorgalaleh, A. , Genetic risk factors in patients with deep venous thrombosis, a retrospective case control study on Iranian population. Thromb J 2015, 13, 35. [Google Scholar] [CrossRef] [PubMed]
- Walter, K. , What Is Pulmonary Embolism? JAMA 2023, 329, (1). 104–104. [Google Scholar] [CrossRef] [PubMed]
- Torbicki, A.; Perrier, A.; Konstantinides, S.; Agnelli, G.; Galiè, N.; Pruszczyk, P.; Bengel, F.; Brady, A. J.; Ferreira, D.; Janssens, U.; Klepetko, W.; Mayer, E.; Remy-Jardin, M.; Bassand, J. P. , Guidelines on the diagnosis and management of acute pulmonary embolism: the Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC). Eur Heart J 2008, 29, (18). 2276–315. [Google Scholar]
- Bĕlohlávek, J.; Dytrych, V.; Linhart, A. , Pulmonary embolism, part I: Epidemiology, risk factors and risk stratification, pathophysiology, clinical presentation, diagnosis and nonthrombotic pulmonary embolism. Exp Clin Cardiol 2013, 18, (2). 129–38. [Google Scholar]
- Meignan, M.; Rosso, J.; Gauthier, H.; Brunengo, F.; Claudel, S.; Sagnard, L.; d'Azemar, P.; Simonneau, G.; Charbonnier, B. , Systematic lung scans reveal a high frequency of silent pulmonary embolism in patients with proximal deep venous thrombosis. Arch Intern Med 2000, 160, (2). 159–64. [Google Scholar] [CrossRef] [PubMed]
- Heit, J. A.; Spencer, F. A.; White, R. H. , The epidemiology of venous thromboembolism. J Thromb Thrombolysis 2016, 41, (1). 3–14. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, M. D.; Heit, J. A.; Mohr, D. N.; Petterson, T. M.; O'Fallon, W. M.; Melton, L. J. , 3rd, Trends in the incidence of deep vein thrombosis and pulmonary embolism: a 25-year population-based study. Arch Intern Med 1998, 158, (6). 585–93. [Google Scholar] [CrossRef] [PubMed]
- Tapson, V. F. , Acute Pulmonary Embolism. New England Journal of Medicine 2008, 358, (10). 1037–1052. [Google Scholar] [CrossRef] [PubMed]
- Piazza, G.; Goldhaber, S. Z.; Kroll, A.; Goldberg, R. J.; Emery, C.; Spencer, F. A. , Venous thromboembolism in patients with diabetes mellitus. Am J Med 2012, 125, (7). 709–16. [Google Scholar] [CrossRef] [PubMed]
- Sawaya, R. E.; Ligon, B. L. , Thromboembolic complications associated with brain tumors. J Neurooncol 1994, 22, (2). 173–81. [Google Scholar] [CrossRef]
- Vedovati, M. C.; Giustozzi, M.; Becattini, C. , Venous thromboembolism and cancer: Current and future role of direct-acting oral anticoagulants. Thromb Res 2019, 177, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Riess, H.; Beyer-Westendorf, J.; Pelzer, U.; Klamroth, R.; Linnemann, B. , Cancer-Associated Venous Thromboembolism-Diagnostic and Therapeutic Considerations: An Update Based on the Revised AWMF S2k Guideline. Hamostaseologie 2024, 44, (2). 143–149. [Google Scholar] [CrossRef] [PubMed]
- Kiser, K. L.; Badowski, M. E. , Risk factors for venous thromboembolism in patients with human immunodeficiency virus infection. Pharmacotherapy 2010, 30, (12). 1292–302. [Google Scholar] [CrossRef] [PubMed]
- Jaff, M. R. , Medical aspects of pregnancy. Cleve Clin J Med 1994, 61, (4). 263–71. [Google Scholar] [CrossRef] [PubMed]
- Raia-Barjat, T.; Edebiri, O.; Chauleur, C. , Venous Thromboembolism Risk Score and Pregnancy. Front Cardiovasc Med 2022, 9, 863612. [Google Scholar] [CrossRef] [PubMed]
- Petrauskiene, V.; Falk, M.; Waernbaum, I.; Norberg, M.; Eriksson, J. W. , The risk of venous thromboembolism is markedly elevated in patients with diabetes. Diabetologia 2005, 48, (5). 1017–21. [Google Scholar] [CrossRef]
- Wild, S.; Roglic, G.; Green, A.; Sicree, R.; King, H. , Global Prevalence of Diabetes: Estimates for the year 2000 and projections for 2030. Diabetes Care 2004, 27, (5). 1047–1053. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y. H.; Lin, Y. S.; Chen, C. H.; Tsai, K. Y.; Hung, Y. C.; Chen, H. J.; Liao, W. C.; Ho, W. C. , Type 1 diabetes is associated with an increased risk of venous thromboembolism: A retrospective population-based cohort study. PLoS One 2020, 15, (1). e0226997. [Google Scholar] [CrossRef] [PubMed]
- Hinton, W.; Nemeth, B.; de Lusignan, S.; Field, B.; Feher, M. D.; Munro, N.; Roberts, L. N.; Arya, R.; Whyte, M. B. , Effect of type 1 diabetes and type 2 diabetes on the risk of venous thromboembolism. Diabetic Medicine 2021, 38, (5). e14452. [Google Scholar] [CrossRef] [PubMed]
- Gariani, K.; Mavrakanas, T.; Combescure, C.; Perrier, A.; Marti, C. , Is diabetes mellitus a risk factor for venous thromboembolism? A systematic review and meta-analysis of case–control and cohort studies. European Journal of Internal Medicine 2016, 28, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Konieczynska, M.; Fil, K.; Bazanek, M.; Undas, A. , Prolonged duration of type 2 diabetes is associated with increased thrombin generation, prothrombotic fibrin clot phenotype and impaired fibrinolysis. Thromb Haemost 2014, 111, (04). 685–693. [Google Scholar] [CrossRef] [PubMed]
- Sabatier, F.; Darmon, P.; Hugel, B.; Combes, V.; Sanmarco, M.; Velut, J.-G.; Arnoux, D.; Charpiot, P.; Freyssinet, J.-M.; Oliver, C.; Sampol, J.; Dignat-George, F. , Type 1 And Type 2 Diabetic Patients Display Different Patterns of Cellular Microparticles. Diabetes 2002, 51, (9). 2840–2845. [Google Scholar] [CrossRef]
- Kovesdy, C. P. , Epidemiology of chronic kidney disease: an update 2022. Kidney Int Suppl (2011) 2022, 12, (1). 7–11. [Google Scholar] [CrossRef] [PubMed]
- Kauffmann, R. H.; Veltkamp, J. J.; Van Tilburg, N. H.; Van Es, L. A. , Acquired antithrombin III deficiency and thrombosis in the nephrotic syndrome. Am J Med 1978, 65, (4). 607–13. [Google Scholar] [CrossRef]
- Heit, J. A.; Leibson, C. L.; Ashrani, A. A.; Petterson, T. M.; Bailey, K. R.; Melton, L. J., Is Diabetes Mellitus an Independent Risk Factor for Venous Thromboembolism? Arteriosclerosis, Thrombosis, and Vascular Biology 2009, 29, (9), 1399-1405.
- Deischinger, C.; Dervic, E.; Nopp, S.; Kaleta, M.; Klimek, P.; Kautzky-Willer, A. , Diabetes mellitus is associated with a higher relative risk for venous thromboembolism in females than in males. Diabetes Res Clin Pract 2022, 194, 110190. [Google Scholar] [CrossRef] [PubMed]
- Tallon, E. M.; Ebekozien, O.; Sanchez, J.; Staggs, V. S.; Ferro, D.; McDonough, R.; Demeterco-Berggren, C.; Polsky, S.; Gomez, P.; Patel, N.; Prahalad, P.; Odugbesan, O.; Mathias, P.; Lee, J. M.; Smith, C.; Shyu, C. R.; Clements, M. A. , Impact of diabetes status and related factors on COVID-19-associated hospitalization: A nationwide retrospective cohort study of 116,370 adults with SARS-CoV-2 infection. Diabetes Res Clin Pract 2022, 194, 110156. [Google Scholar] [CrossRef] [PubMed]
- Roopkumar, J.; Swaidani, S.; Kim, A. S.; Thapa, B.; Gervaso, L.; Hobbs, B. P.; Wei, W.; Alban, T. J.; Funchain, P.; Kundu, S.; Sangwan, N.; Rayman, P.; Pavicic, P. G., Jr.; Diaz-Montero, C. M.; Barnard, J.; McCrae, K. R.; Khorana, A. A. , Increased Incidence of Venous Thromboembolism with Cancer Immunotherapy. Med 2021, 2, (4). 423–434. [Google Scholar] [CrossRef] [PubMed]
- Elice, F.; Rodeghiero, F.; Falanga, A.; Rickles, F. R. , Thrombosis associated with angiogenesis inhibitors. Best Pract Res Clin Haematol 2009, 22, (1). 115–28. [Google Scholar] [CrossRef] [PubMed]
- Evans, C. E.; Grover, S. P.; Humphries, J.; Saha, P.; Patel, A. P.; Patel, A. S.; Lyons, O. T.; Waltham, M.; Modarai, B.; Smith, A., Antiangiogenic Therapy Inhibits Venous Thrombus Resolution. Arteriosclerosis, Thrombosis, and Vascular Biology 2014, 34, (3), 565-570.
- Zangari, M.; Fink, L. M.; Elice, F.; Zhan, F.; Adcock, D. M.; Tricot, G. J. , Thrombotic events in patients with cancer receiving antiangiogenesis agents. J Clin Oncol 2009, 27, (29). 4865–73. [Google Scholar] [CrossRef] [PubMed]
- Mackman, N.; Tilley, R. E.; Key, N. S., Role of the Extrinsic Pathway of Blood Coagulation in Hemostasis and Thrombosis. Arteriosclerosis, Thrombosis, and Vascular Biology 2007, 27, (8), 1687-1693.
- Sorensen, A. B.; Madsen, J. J.; Svensson, L. A.; Pedersen, A. A.; Østergaard, H.; Overgaard, M. T.; Olsen, O. H.; Gandhi, P. S. , Molecular Basis of Enhanced Activity in Factor VIIa-Trypsin Variants Conveys Insights into Tissue Factor-mediated Allosteric Regulation of Factor VIIa Activity. J Biol Chem 2016, 291, (9). 4671–83. [Google Scholar] [CrossRef]
- Hvas, C. L.; Larsen, J. B., The Fibrinolytic System and Its Measurement: History, Current Uses and Future Directions for Diagnosis and Treatment. Int J Mol Sci 2023, 24, (18).
- Lin, H.; Xu, L.; Yu, S.; Hong, W.; Huang, M.; Xu, P., Therapeutics targeting the fibrinolytic system. Experimental & Molecular Medicine 2020, 52, (3), 367-379.
- Sillen, M.; Declerck, P. J., A Narrative Review on Plasminogen Activator Inhibitor-1 and Its (Patho)Physiological Role: To Target or Not to Target? Int J Mol Sci 2021, 22, (5).
- PANNELL, R.; KUNG, W.; GUREWICH, V. , C1-inhibitor prevents non-specific plasminogen activation by a prourokinase mutant without impeding fibrin-specific fibrinolysis. Journal of Thrombosis and Haemostasis 2007, 5, (5). 1047–1054. [Google Scholar] [CrossRef] [PubMed]
- Ratnoff, O. D.; Pensky, J.; Ogston, D.; Naff, G. B. , The inhibition of plasmin, plasma kallikrein, plasma permeability factor, and the C'1r subcomponent of the first component of complement by serum C'1 esterase inhibitor. J Exp Med 1969, 129, (2). 315–31. [Google Scholar] [CrossRef] [PubMed]
- Mosnier, L. O.; Bouma, B. N., Regulation of Fibrinolysis by Thrombin Activatable Fibrinolysis Inhibitor, an Unstable Carboxypeptidase B That Unites the Pathways of Coagulation and Fibrinolysis. Arteriosclerosis, Thrombosis, and Vascular Biology 2006, 26, (11), 2445-2453.
- Sillen, M.; Declerck, P. J., Thrombin Activatable Fibrinolysis Inhibitor (TAFI): An Updated Narrative Review. Int J Mol Sci 2021, 22, (7).
- Mast, A. E., Tissue Factor Pathway Inhibitor. Arteriosclerosis, Thrombosis, and Vascular Biology 2016, 36, (1), 9-14.
- Dahlbäck, B.; Villoutreix, B. O., Regulation of Blood Coagulation by the Protein C Anticoagulant Pathway. Arteriosclerosis, Thrombosis, and Vascular Biology 2005, 25, (7), 1311-1320.
- Ji, Y.; Temprano-Sagrera, G.; Holle, L. A.; Bebo, A.; Brody, J. A.; Le, N.-Q.; Kangro, K.; Brown, M. R.; Martinez-Perez, A.; Sitlani, C. M.; Suchon, P.; Kleber, M. E.; Emmert, D. B.; Bilge Ozel, A.; Dobson, D. V. A.; Tang, W.; Llobet, D.; Tracy, R. P.; Deleuze, J.-F.; Delgado, G. E.; Gögele, M.; Wiggins, K. L.; Souto, J. C.; Pankow, J. S.; Taylor, K. D.; Trégouët, D.-A.; Moissl, A. P.; Fuchsberger, C.; Rosendaal, F. R.; Morrison, A. C.; Soria, J. M.; Cushman, M.; Morange, P.-E.; März, W.; Hicks, A. A.; Desch, K. C.; Johnson, A. D.; de Vries, P. S.; CHARGE Consortium Hemostasis Working Group, I. C.; Wolberg, A. S.; Smith, N. L.; Sabater-Lleal, M., Antithrombin, Protein C, and Protein S: Genome and Transcriptome-Wide Association Studies Identify 7 Novel Loci Regulating Plasma Levels. Arteriosclerosis, Thrombosis, and Vascular Biology 2023, 43, (7), e254-e269.
- Kubier, A.; O'Brien, M. , Endogenous anticoagulants. Top Companion Anim Med 2012, 27, (2). 81–7. [Google Scholar] [CrossRef] [PubMed]
- Grover, S. P.; Mackman, N. , Anticoagulant SERPINs: Endogenous Regulators of Hemostasis and Thrombosis. Front Cardiovasc Med 2022, 9, 878199. [Google Scholar] [CrossRef] [PubMed]
- Arble, E.; Arnetz, B. B. , Anticoagulants and the Hemostatic System: A Primer for Occupational Stress Researchers. International Journal of Environmental Research and Public Health 2021, 18, (20). 10626. [Google Scholar] [CrossRef] [PubMed]
- Ahnström, J. , The potential of serpins for future treatment for haemophilia. Journal of Thrombosis and Haemostasis 2019, 17, (10). 1629–1631. [Google Scholar] [CrossRef]
- Kim, D.; Bresette, C.; Liu, Z.; Ku, D. N. , Occlusive thrombosis in arteries. APL Bioeng 2019, 3, (4). 041502. [Google Scholar] [CrossRef]
- Alkarithi, G.; Duval, C.; Shi, Y.; Macrae, F. L.; Ariëns, R. A. S. , Thrombus Structural Composition in Cardiovascular Disease. Arterioscler Thromb Vasc Biol 2021, 41, (9). 2370–2383. [Google Scholar] [CrossRef] [PubMed]
- Mackman, N. , New insights into the mechanisms of venous thrombosis. J Clin Invest 2012, 122, (7). 2331–6. [Google Scholar] [CrossRef] [PubMed]
- Cockett, F. B.; Thomas, M. L. , The iliac compression syndrome. Br J Surg 1965, 52, (10). 816–21. [Google Scholar] [CrossRef] [PubMed]
- Moudgill, N.; Hager, E.; Gonsalves, C.; Larson, R.; Lombardi, J.; DiMuzio, P. , May-Thurner syndrome: case report and review of the literature involving modern endovascular therapy. Vascular 2009, 17, (6). 330–5. [Google Scholar] [CrossRef] [PubMed]
- Heestermans, M.; Poenou, G.; Duchez, A. C.; Hamzeh-Cognasse, H.; Bertoletti, L.; Cognasse, F., Immunothrombosis and the Role of Platelets in Venous Thromboembolic Diseases. Int J Mol Sci 2022, 23, (21).
- Mereweather, L. J.; Constantinescu-Bercu, A.; Crawley, J. T. B.; Salles-Crawley, I. I. , Platelet–Neutrophil Crosstalk in Thrombosis. International Journal of Molecular Sciences 2023, 24, (2). 1266. [Google Scholar] [CrossRef]
- Wigle, P. Anticoagulation: Updated Guidelines for Outpatient Management; 2019; pp 426-434.
- Marcucci, M.; Etxeandia-Ikobaltzeta, I.; Yang, S.; Germini, F.; Gupta, S.; Agarwal, A.; Ventresca, M.; Tang, S.; Morgano, G. P.; Wang, M.; Ahmed, M. M.; Neumann, I.; Izcovich, A.; Criniti, J.; Popoff, F.; Devereaux, P. J.; Dahm, P.; Anderson, D.; Lavikainen, L. I.; Tikkinen, K. A. O.; Guyatt, G. H.; Schünemann, H. J.; Violette, P. D. , Benefits and harms of direct oral anticoagulation and low molecular weight heparin for thromboprophylaxis in patients undergoing non-cardiac surgery: systematic review and network meta-analysis of randomised trials. Bmj 2022, 376, e066785. [Google Scholar] [CrossRef] [PubMed]
- Konieczynska, M.; Kupis, R. W.; Bijak, P.; Malinowski, K. P.; Undas, A. , Acceptance of a potential major bleeding among patients with venous thromboembolism on long-term oral anticoagulation: the knowledge of the disease and therapy matters. Thrombosis research 2020, 193, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Achebe, I.; Mbachi, C.; Palacios, P.; Wang, Y.; Asotibe, J.; Ofori-Kuragu, A.; Gandhi, S. , Predictors of venous thromboembolism in hospitalized patients with inflammatory bowel disease and colon cancer: A retrospective cohort study. Thrombosis research 2020, 199, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Piazza, G.; Goldhaber, S. Z. , Acute Pulmonary Embolism. Circulation 2006, 114, (3). e42–e47. [Google Scholar]
- Flumignan, C. D.; Nakano, L. C.; Baptista-Silva, J. C.; Flumignan, R. L. , Antiplatelet agents for the treatment of deep venous thrombosis. Cochrane Database Syst Rev 2022, 7, (7). CD012369. [Google Scholar] [CrossRef] [PubMed]
- Diep, R.; Garcia, D. , Does aspirin prevent venous thromboembolism? Hematology 2020, 2020, (1). 634–641. [Google Scholar] [CrossRef] [PubMed]
- Collaborative overview of randomised trials of antiplatelet therapy--III: Reduction in venous thrombosis and pulmonary embolism by antiplatelet prophylaxis among surgical and medical patients. Antiplatelet Trialists' Collaboration. BMJ 1994, 308, (6923), 235-46.
- Landel, J. B.; Bauters, A.; Delhaye, C.; Bonello, L.; Sudre, A.; Susen, S.; Bauters, C.; Lablanche, J. M.; Lemesle, G. , Impact of initial clinical presentation on clopidogrel low response. Arch Cardiovasc Dis 2013, 106, (11). 593–600. [Google Scholar] [CrossRef] [PubMed]
- Raabe, R. D. , Ultrasound-accelerated thrombolysis in arterial and venous peripheral occlusions: fibrinogen level effects. J Vasc Interv Radiol 2010, 21, (8). 1165–72. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y. H.; Zhu, X. Y.; Fan, L. H.; Xu, H. F. , Pulmonary embolism in patients with chronic coronary syndrome masquerading as acute coronary syndrome: a case report and literature review. BMC Cardiovasc Disord 2024, 24, (1). 331. [Google Scholar] [CrossRef] [PubMed]
- Casula, M.; Casu, G.; Talanas, G.; Spano, A.; Tantry, U.; Bilotta, F.; Micheluzzi, V.; Merella, P.; Porcheddu, T.; Gorog, D. A.; Bonaca, M.; Jeong, Y. H.; Farkouh, M. E.; Kubica, J.; Isgender, M.; Gurbel, P. A.; Navarese, E. P. , Efficacy and Safety of P2Y(12) monotherapy vs standard DAPT in patients undergoing percutaneous coronary intervention: meta-analysis of randomized trials. Curr Probl Cardiol 2024, 49. (8), 102635. [Google Scholar] [CrossRef] [PubMed]
- Diabetes-Related Complications and Mortality in Patients With Atrial Fibrillation Receiving Different Oral Anticoagulants. Annals of Internal Medicine 2022, 175, (4). 490–498.
- Lip, G. Y. H.; Keshishian, A. V.; Kang, A. L.; Li, X.; Dhamane, A. D.; Luo, X.; Balachander, N.; Rosenblatt, L.; Mardekian, J.; Nadkarni, A.; Pan, X.; Di Fusco, M.; Garcia Reeves, A. B.; Yuce, H.; Deitelzweig, S. B. , Effectiveness and Safety of Oral Anticoagulants in Patients With Nonvalvular Atrial Fibrillation and Diabetes Mellitus. Mayo Clinic Proceedings 2020, 95, (5). 929–943. [Google Scholar] [CrossRef] [PubMed]
- Aursulesei, V. ; Costache, II, Anticoagulation in chronic kidney disease: from guidelines to clinical practice. Clin Cardiol 2019, 42, (8). 774–782. [Google Scholar] [CrossRef] [PubMed]
- Elenjickal, E. J.; Travlos, C. K.; Marques, P.; Mavrakanas, T. A. , Anticoagulation in Patients with Chronic Kidney Disease. American Journal of Nephrology 2023, 55, (2). 146–164. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Lim, E.; Covic, A.; Verhamme, P.; Gale, C. P.; Camm, A. J.; Goldsmith, D. , Anticoagulation in Concomitant Chronic Kidney Disease and Atrial Fibrillation. Journal of the American College of Cardiology 2019, 74, (17). 2204–2215. [Google Scholar] [CrossRef] [PubMed]
- Camm, A. J.; Sabbour, H.; Schnell, O.; Summaria, F.; Verma, A. , Managing thrombotic risk in patients with diabetes. Cardiovasc Diabetol 2022, 21, (1). 160. [Google Scholar] [CrossRef] [PubMed]
- Corken, A. L.; Ong, V.; Kore, R.; Ghanta, S. N.; Karaduta, O.; Pathak, R.; Rose, S.; Porter, C.; Jain, N. , Platelets, inflammation, and purinergic receptors in chronic kidney disease. Kidney Int 2024. [Google Scholar] [CrossRef] [PubMed]
- Delluc, A.; Lacut, K.; Rodger, M. A. , Arterial and venous thrombosis: What's the link? A narrative review. Thromb Res 2020, 191, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Ogeng'o, J. A.; Obimbo, M. M.; Olabu, B. O.; Gatonga, P. M.; Ong'era, D. , Pulmonary thromboembolism in an East African tertiary referral hospital. J Thromb Thrombolysis 2011, 32, (3). 386–91. [Google Scholar] [CrossRef]
- Simon, S. J.; Patell, R.; Zwicker, J. I.; Kazi, D. S.; Hollenbeck, B. L. , Venous Thromboembolism in Total Hip and Total Knee Arthroplasty. JAMA Netw Open 2023, 6, (12). e2345883. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.; Al-Horani, R. A., Venous Thromboembolism Prophylaxis in Major Orthopedic Surgeries and Factor XIa Inhibitors. Med Sci (Basel) 2023, 11, (3).
- Guan, Y.; Zeng, Z. , Delayed pulmonary embolism after unicompartmental knee arthroplasty: A case report. Medicine (Baltimore) 2021, 100, (1). e24230. [Google Scholar] [CrossRef] [PubMed]
- Fu, D.; Li, L.; Li, Y.; Liu, X.; Chen, H.; Wu, N.; Sun, G. , Fondaparinux sodium and low molecular weight heparin for venous thromboembolism prophylaxis in Chinese patients with major orthopedic surgery or trauma: a real-world study. BMC Surg 2022, 22. (1), 243. [Google Scholar] [CrossRef] [PubMed]
- Sharma, R.; Subedi, A. , Antithrombotic Therapy for Heart Failure in Sinus Rhythm - A Concise Review. S D Med 2024, 77, (5). 213–219. [Google Scholar]
- Lip, G. Y. H.; Banerjee, A.; Boriani, G.; Chiang, C. E.; Fargo, R.; Freedman, B.; Lane, D. A.; Ruff, C. T.; Turakhia, M.; Werring, D.; Patel, S.; Moores, L. , Antithrombotic Therapy for Atrial Fibrillation: CHEST Guideline and Expert Panel Report. Chest 2018, 154, (5). 1121–1201. [Google Scholar] [CrossRef] [PubMed]
- Ilic, I.; Radunovic, A.; Timcic, S.; Odanovic, N.; Radoicic, D.; Dukuljev, N.; Krljanac, G.; Otasevic, P.; Apostolovic, S. , Drugs for spontaneous coronary dissection: a few untrusted options. Front Cardiovasc Med 2023, 10, 1275725. [Google Scholar] [CrossRef]
- Kafi, A.; Friedman, O.; Kim, I. , Use of low-dose thrombolytics for treatment of intracardiac thrombus and massive pulmonary embolus after aborted liver transplant leads to recovery of right ventricular function and redo liver transplantation. BMJ Case Rep 2017, 2017. [Google Scholar] [CrossRef] [PubMed]
- Bertoletti, L.; Girard, P.; Elias, A.; Espitia, O.; Schmidt, J.; Couturaud, F.; Mahe, I.; Sanchez, O.; Group, I. C. W. , Recurrent venous thromboembolism in anticoagulated cancer patients: Diagnosis and treatment. Arch Cardiovasc Dis 2024, 117, (1). 84–93. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, M. L.; Nachman, P. H.; Mooberry, M. J.; Crona, D. J.; Derebail, V. K. , Recurrent venous thromboembolism in primary membranous nephropathy despite direct Xa inhibitor therapy. J Nephrol 2019, 32, (4). 669–672. [Google Scholar] [CrossRef] [PubMed]
- Xia, Y.; Hu, Y.; Tang, L., Factor XIa Inhibitors as a Novel Anticoagulation Target: Recent Clinical Research Advances. Pharmaceuticals (Basel) 2023, 16, (6).
- Plautz, W. E.; Sekhar Pilli, V. S.; Cooley, B. C.; Chattopadhyay, R.; Westmark, P. R.; Getz, T.; Paul, D.; Bergmeier, W.; Sheehan, J. P.; Majumder, R., Anticoagulant Protein S Targets the Factor IXa Heparin-Binding Exosite to Prevent Thrombosis. Arteriosclerosis, Thrombosis, and Vascular Biology 2018, 38, (4), 816-828.
- Srivastava, P.; Gailani, D. , The rebirth of the contact pathway: a new therapeutic target. Curr Opin Hematol 2020, 27, (5). 311–319. [Google Scholar] [CrossRef] [PubMed]
- Puy, C.; Rigg, R. A.; McCarty, O. J. , The hemostatic role of factor XI. Thromb Res 2016, 141, (Suppl 2). (Suppl 2), S8–s11. [Google Scholar] [CrossRef]
- Rühl, H.; Friemann, A. M.; Reda, S.; Schwarz, N.; Winterhagen, F. I.; Berens, C.; Müller, J.; Oldenburg, J.; Pötzsch, B. , Activated Factor XI is Increased in Plasma in Response to Surgical Trauma but not to Recombinant Activated FVII-Induced Thrombin Formation. J Atheroscler Thromb 2022, 29, (1). 82–98. [Google Scholar] [CrossRef] [PubMed]
- Puy, C.; Tucker, E. I.; Matafonov, A.; Cheng, Q.; Zientek, K. D.; Gailani, D.; Gruber, A.; McCarty, O. J. , Activated factor XI increases the procoagulant activity of the extrinsic pathway by inactivating tissue factor pathway inhibitor. Blood 2015, 125, (9). 1488–96. [Google Scholar] [CrossRef] [PubMed]
- Tai, S. J.; Herzog, R. W.; Margaritis, P.; Arruda, V. R.; Chu, K.; Golden, J. A.; Labosky, P. A.; High, K. A. , A viable mouse model of factor X deficiency provides evidence for maternal transfer of factor X. J Thromb Haemost 2008, 6, (2). 339–45. [Google Scholar] [CrossRef] [PubMed]
- Raskob, G. E.; Angchaisuksiri, P.; Blanco, A. N.; Buller, H.; Gallus, A.; Hunt, B. J.; Hylek, E. M.; Kakkar, A.; Konstantinides, S. V.; McCumber, M.; Ozaki, Y.; Wendelboe, A.; Weitz, J. I.; Day, I. S. C. f. W. T. , Thrombosis: a major contributor to global disease burden. Arterioscler Thromb Vasc Biol 2014, 34, (11). 2363–71. [Google Scholar] [CrossRef] [PubMed]
- Greco, A.; Laudani, C.; Spagnolo, M.; Agnello, F.; Faro, D. C.; Finocchiaro, S.; Legnazzi, M.; Mauro, M. S.; Mazzone, P. M.; Occhipinti, G.; Rochira, C.; Scalia, L.; Capodanno, D. , Pharmacology and Clinical Development of Factor XI Inhibitors. Circulation 2023, 147, (11). 897–913. [Google Scholar] [CrossRef]
- Sammut, M. A. E. , Nadir; Storey, Robert F, Factor XI and XIa inhibition: a new approach to anticoagulant therapy. The British Journal of Cardiology 2024, 31, 49–54. [Google Scholar]
- Chan, N. C.; Weitz, J. I. , New Therapeutic Targets for the Prevention and Treatment of Venous Thromboembolism With a Focus on Factor XI Inhibitors. Arterioscler Thromb Vasc Biol 2023, 43, (10). 1755–1763. [Google Scholar] [CrossRef] [PubMed]
- Weitz, J. I.; Eikelboom, J. W. , What Is the Future of Factor XI Inhibitors? Circulation 2022, 146, (25). 1899–1902. [Google Scholar] [CrossRef] [PubMed]
- Occhipinti, G.; Laudani, C.; Spagnolo, M.; Finocchiaro, S.; Mazzone, P. M.; Faro, D. C.; Mauro, M. S.; Rochira, C.; Agnello, F.; Giacoppo, D.; Ammirabile, N.; Landolina, D.; Imbesi, A.; Sangiorgio, G.; Greco, A.; Capodanno, D. , Pharmacological and clinical appraisal of factor XI inhibitor drugs. Eur Heart J Cardiovasc Pharmacother 2024, 10, (3). 245–258. [Google Scholar] [CrossRef] [PubMed]
- Presume, J.; Ferreira, J.; Ribeiras, R. , Factor XI Inhibitors: A New Horizon in Anticoagulation Therapy. Cardiol Ther 2024, 13, (1). 1–16. [Google Scholar] [CrossRef] [PubMed]
- Campello, E.; Simioni, P.; Prandoni, P.; Ferri, N., Clinical Pharmacology of Factor XI Inhibitors: New Therapeutic Approaches for Prevention of Venous and Arterial Thrombotic Disorders. J Clin Med 2022, 11, (21).
- Ludwig, R. J.; Schön, M. P.; Boehncke, W. H. , P-selectin: a common therapeutic target for cardiovascular disorders, inflammation and tumour metastasis. Expert Opin Ther Targets 2007, 11, (8). 1103–17. [Google Scholar] [CrossRef]
- Ed Rainger, G.; Chimen, M.; Harrison, M. J.; Yates, C. M.; Harrison, P.; Watson, S. P.; Lordkipanidzé, M.; Nash, G. B. , The role of platelets in the recruitment of leukocytes during vascular disease. Platelets 2015, 26, (6). 507–20. [Google Scholar] [CrossRef] [PubMed]
- Ivanov, I. I.; Apta, B. H. R.; Bonna, A. M.; Harper, M. T. , Platelet P-selectin triggers rapid surface exposure of tissue factor in monocytes. Scientific Reports 2019, 9, (1). 13397. [Google Scholar] [CrossRef] [PubMed]
- Sankyo, D., Study to Assess the Safety, Pharmacokinetics/Dynamics of DS-1040b in Subjects With Acute Submassive Pulmonary Embolism. ClinicalTrials.Gov, https://clinicaltrials.gov/study/NCT02923115: 2024.
- Zhou, J.; Kochan, J.; Yin, O.; Warren, V.; Zamora, C.; Atiee, G.; Pav, J.; Orihashi, Y.; Vashi, V.; Dishy, V. , A first-in-human study of DS-1040, an inhibitor of the activated form of thrombin-activatable fibrinolysis inhibitor, in healthy subjects. J Thromb Haemost 2017, 15, (5). 961–971. [Google Scholar] [CrossRef] [PubMed]
- Janssen Research & Development, L., A Study to Evaluate the Safety and Efficacy of Intravenous JNJ-64179375 Versus Oral Apixaban in Participants Undergoing Elective Total Knee Replacement Surgery (TEXT-TKR). Janssen Research & Development, LLC, https://clinicaltrials.gov/study/NCT03251482, 2019.
- Wilson, S. J.; Connolly, T. M.; Peters, G.; Ghosh, A.; Johnson, M.; Newby, D. E. , Exosite 1 thrombin inhibition with JNJ-64179375 inhibits thrombus formation in a human translational model of thrombosis. Cardiovasc Res 2019, 115, (3). 669–677. [Google Scholar] [CrossRef]
- Corporation, T. P., Study to Assess the Safety and Efficacy of SelK2 to Prevent Blood Clots in Patients Undergoing Total Knee Replacement. ClinicalTrials.Gov, https://clinicaltrials.gov/study/NCT03812328: 2024.
- Zwicker, J., Cancer Associated Thrombosis and Isoquercetin (CATIQ). ClinicalTrials.Gov, https://clinicaltrials.gov/study/NCT02195232: 2021.
- FDA, Considering whether an FDA-regulated product involves the application of nanotechnology. 2014, https://www.fda.gov/regulatory-information/search-fda-guidance-documents/considering-whether-fda-regulated-product-involves-application-nanotechnology.
- De Jong, W. H.; Hagens, W. I.; Krystek, P.; Burger, M. C.; Sips, A. J. A. M.; Geertsma, R. E. , Particle size-dependent organ distribution of gold nanoparticles after intravenous administration. Biomaterials 2008, 29, (12). 1912–1919. [Google Scholar] [CrossRef] [PubMed]
- Soares, S.; Sousa, J.; Pais, A.; Vitorino, C. , Nanomedicine: Principles, Properties, and Regulatory Issues. Front Chem 2018, 6, 360. [Google Scholar] [CrossRef] [PubMed]
- Shi, X.; Sun, K.; Baker Jr, J. R. , Spontaneous formation of functionalized dendrimer-stabilized gold nanoparticles. The Journal of Physical Chemistry C 2008, 112, (22). 8251–8258. [Google Scholar] [CrossRef] [PubMed]
- Patra, J. K.; Das, G.; Fraceto, L. F.; Campos, E. V. R.; Rodriguez-Torres, M. d. P.; Acosta-Torres, L. S.; Diaz-Torres, L. A.; Grillo, R.; Swamy, M. K.; Sharma, S.; Habtemariam, S.; Shin, H.-S. , Nano based drug delivery systems: recent developments and future prospects. Journal of Nanobiotechnology 2018, 16, (1). 71. [Google Scholar] [CrossRef] [PubMed]
- Meiners, K.; Hamm, P.; Gutmann, M.; Niedens, J.; Nowak-Król, A.; Pané, S.; Lühmann, T. , Site-specific PEGylation of recombinant tissue-type plasminogen activator. Eur J Pharm Biopharm 2023, 192, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Sakuragawa, N.; Shimizu, K.; Kondo, K.; Kondo, S.; Niwa, M. , Studies on the effect of PEG-modified urokinase on coagulation-fibrinolysis using beagles. Thromb Res 1986, 41, (5). 627–35. [Google Scholar] [CrossRef]
- Rajagopalan, S.; Gonias, S. L.; Pizzo, S. V. , A nonantigenic covalent streptokinase-polyethylene glycol complex with plasminogen activator function. The Journal of Clinical Investigation 1985, 75, (2). 413–419. [Google Scholar] [CrossRef] [PubMed]
- Rachmawati, H.; Damanhuri, F.; Agustian Darfiansyah, I.; Retnoningrum, D. , Pegylation of recombinant mutein streptokinase from overproduction in escherchia coli BL21 and study on the fibrinolityc activity in vitro. International Journal of Pharmacy and Pharmaceutical Sciences 2014, 6, 137–141. [Google Scholar]
- Liu, J.; Wang, Z.; He, J.; Wang, G.; Zhang, R.; Zhao, B. , Effect of site-specific PEGylation on the fibrinolytic activity, immunogenicity, and pharmacokinetics of staphylokinase. Acta Biochimica et Biophysica Sinica 2014, 46, (9). 782–791. [Google Scholar] [CrossRef] [PubMed]
- Qi, F.; Hu, C.; Yu, W.; Hu, T. , Conjugation with Eight-Arm PEG Markedly Improves the In Vitro Activity and Prolongs the Blood Circulation of Staphylokinase. Bioconjugate Chemistry 2018, 29, (2). 451–458. [Google Scholar] [CrossRef] [PubMed]
- Bai, S.; Ahsan, F. , Inhalable liposomes of low molecular weight heparin for the treatment of venous thromboembolism. J Pharm Sci 2010, 99, (11). 4554–64. [Google Scholar] [CrossRef]
- Heeremans, J. L. M.; Prevost, R.; Bekkers, M. E. A.; Los, P.; Emeis, J. J.; Kluft, C.; Crommelin, D. J. A. , Thrombolytic Treatment with Tissue-type Plasminogen Activator (t-PA) Containing Liposomes in Rabbits: a Comparison with Free t-PA. Thromb Haemost 1995, 73, (03). 488–494. [Google Scholar] [CrossRef]
- Palekar, R. U.; Myerson, J. W.; Schlesinger, P. H.; Wickline, S. A.; Pan, H., Abstract 12047: Thrombin-inhibiting Liposomes for Safe, Site-specific Inhibition of Acute Thrombosis. Circulation 2012, 126, (suppl_21), A12047-A12047.
- Palekar, R. U.; Myerson, J. W.; Schlesinger, P. H.; Sadler, J. E.; Pan, H.; Wickline, S. A. , Thrombin-Targeted Liposomes Establish a Sustained Localized Anticlotting Barrier against Acute Thrombosis. Molecular Pharmaceutics 2013, 10, (11). 4168–4175. [Google Scholar] [CrossRef] [PubMed]
- Ma, H.; Jiang, Z.; Xu, J.; Liu, J.; Guo, Z. N. , Targeted nano-delivery strategies for facilitating thrombolysis treatment in ischemic stroke. Drug Deliv 2021, 28, (1). 357–371. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Feng, X.; Jin, R.; Li, G. , Tissue plasminogen activator-based nanothrombolysis for ischemic stroke. Expert Opin Drug Deliv 2018, 15, (2). 173–184. [Google Scholar] [CrossRef] [PubMed]
- Russell, P.; Hagemeyer, C. E.; Esser, L.; Voelcker, N. H. , Theranostic nanoparticles for the management of thrombosis. Theranostics 2022, 12, (6). 2773–2800. [Google Scholar] [CrossRef] [PubMed]
- Teng, Y.; Jin, H.; Nan, D.; Li, M.; Fan, C.; Liu, Y.; Lv, P.; Cui, W.; Sun, Y.; Hao, H.; Qu, X.; Yang, Z.; Huang, Y. , In vivo evaluation of urokinase-loaded hollow nanogels for sonothrombolysis on suture embolization-induced acute ischemic stroke rat model. Bioact Mater 2018, 3, (1). 102–109. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wei, C.; Liu, M.; Yang, T.; Zhou, W.; Liu, Y.; Hong, K.; Wang, S.; Xin, H.; Ding, X. , Near-Infrared Triggered Release of uPA from Nanospheres for Localized Hyperthermia-Enhanced Thrombolysis. Advanced Functional Materials 2017, 27, (40). 1701824. [Google Scholar] [CrossRef]
- Laing, S. T.; Moody, M. R.; Kim, H.; Smulevitz, B.; Huang, S. L.; Holland, C. K.; McPherson, D. D.; Klegerman, M. E. , Thrombolytic efficacy of tissue plasminogen activator-loaded echogenic liposomes in a rabbit thrombus model. Thromb Res 2012, 130, (4). 629–35. [Google Scholar] [CrossRef] [PubMed]
- Kandadai, M. A.; Mukherjee, P.; Shekhar, H.; Shaw, G. J.; Papautsky, I.; Holland, C. K. , Microfluidic manufacture of rt-PA -loaded echogenic liposomes. Biomed Microdevices 2016, 18, (3). 48. [Google Scholar] [CrossRef] [PubMed]
- Chen, J. P.; Liu, C. H.; Hsu, H. L.; Wu, T.; Lu, Y. J.; Ma, Y. H. , Magnetically controlled release of recombinant tissue plasminogen activator from chitosan nanocomposites for targeted thrombolysis. J Mater Chem B 2016, 4, (15). 2578–2590. [Google Scholar] [CrossRef] [PubMed]
- Fithri, N. A.; Wu, Y.; Cowin, G.; Akther, F.; Tran, H. D. N.; Tse, B.; van Holthe, N. W.; Moonshi, S. S.; Peter, K.; Wang, X.; Truong, N. P.; Ta, H. T. , Gold-iron oxide nanoparticle: A unique multimodal theranostic approach for thrombosis. Applied Materials Today 2023, 31, 101750. [Google Scholar] [CrossRef]
- Tadayon, A.; Jamshidi, R.; Esmaeili, A., Targeted thrombolysis of tissue plasminogen activator and streptokinase with extracellular biosynthesis nanoparticles using optimized Streptococcus equi supernatant. Int J Pharm 2016, 501, (1-2), 300-10.
- Shaw, G. J.; Meunier, J. M.; Huang, S. L.; Lindsell, C. J.; McPherson, D. D.; Holland, C. K. , Ultrasound-enhanced thrombolysis with tPA-loaded echogenic liposomes. Thromb Res 2009, 124, (3). 306–10. [Google Scholar] [CrossRef] [PubMed]
- Hagisawa, K.; Nishioka, T.; Suzuki, R.; Maruyama, K.; Takase, B.; Ishihara, M.; Kurita, A.; Yoshimoto, N.; Nishida, Y.; Iida, K.; Luo, H.; Siegel, R. J. , Thrombus-targeted perfluorocarbon-containing liposomal bubbles for enhancement of ultrasonic thrombolysis: in vitro and in vivo study. J Thromb Haemost 2013, 11, (8). 1565–73. [Google Scholar] [CrossRef] [PubMed]
- Hassanpour, S.; Kim, H. J.; Saadati, A.; Tebon, P.; Xue, C.; van den Dolder, F. W.; Thakor, J.; Baradaran, B.; Mosafer, J.; Baghbanzadeh, A.; de Barros, N. R.; Hashemzaei, M.; Lee, K. J.; Lee, J.; Zhang, S.; Sun, W.; Cho, H. J.; Ahadian, S.; Ashammakhi, N.; Dokmeci, M. R.; Mokhtarzadeh, A.; Khademhosseini, A. , Thrombolytic Agents: Nanocarriers in Controlled Release. Small 2020, 16, (40). e2001647. [Google Scholar] [CrossRef] [PubMed]
- Paliwal, V., Creation of tPA conjugated dendrimer nanoparticles (780.4). The FASEB Journal 2014, 28, (S1), 780.4.
- Huang, M.; Lü, S.; Ji, Y.; Wang, Z.; Zhang, S.-F.; Qi, T.; Yan, J.; Li, T.; Liu, Y.; Liu, M. , A nattokinase carrier bonding with polyglutamic acid peptide dendrimer for improved thrombolysis. Polymers for Advanced Technologies 2019, 30, (9). 2353–2360. [Google Scholar] [CrossRef]
- Wu, C.; Gao, C.; Lü, S.; Xu, X.; Wen, N.; Zhang, S.; Liu, M. , Construction of polylysine dendrimer nanocomposites carrying nattokinase and their application in thrombolysis. Journal of Biomedical Materials Research Part A 2018, 106, (2). 440–449. [Google Scholar] [CrossRef] [PubMed]
- Bai, S.; Thomas, C.; Ahsan, F. , Dendrimers as a carrier for pulmonary delivery of enoxaparin, a low-molecular weight heparin. J Pharm Sci 2007, 96, (8). 2090–106. [Google Scholar] [CrossRef] [PubMed]
- Jones, C. F.; Campbell, R. A.; Brooks, A. E.; Assemi, S.; Tadjiki, S.; Thiagarajan, G.; Mulcock, C.; Weyrich, A. S.; Brooks, B. D.; Ghandehari, H.; Grainger, D. W. , Cationic PAMAM dendrimers aggressively initiate blood clot formation. ACS Nano 2012, 6, (11). 9900–10. [Google Scholar] [CrossRef] [PubMed]
- Zeibi Shirejini, S.; Carberry, J.; Alt, K.; Gregory, S. D.; Hagemeyer, C. E. , Shear-Responsive Drug Delivery Systems in Medical Devices: Focus on Thrombosis and Bleeding. Advanced Functional Materials 2023, 33, (37). 2303717. [Google Scholar] [CrossRef]
- Greineder, C. F.; Howard, M. D.; Carnemolla, R.; Cines, D. B.; Muzykantov, V. R. , Advanced drug delivery systems for antithrombotic agents. Blood 2013, 122, (9). 1565–1575. [Google Scholar] [CrossRef] [PubMed]
- Korin, N.; Kanapathipillai, M.; Matthews, B. D.; Crescente, M.; Brill, A.; Mammoto, T.; Ghosh, K.; Jurek, S.; Bencherif, S. A.; Bhatta, D.; Coskun, A. U.; Feldman, C. L.; Wagner, D. D.; Ingber, D. E. , Shear-activated nanotherapeutics for drug targeting to obstructed blood vessels. Science 2012, 337, (6095). 738–42. [Google Scholar] [CrossRef] [PubMed]
- Korin, N.; Gounis, M. J.; Wakhloo, A. K.; Ingber, D. E. , Targeted Drug Delivery to Flow-Obstructed Blood Vessels Using Mechanically Activated Nanotherapeutics. JAMA Neurology 2015, 72, (1). 119–122. [Google Scholar] [CrossRef] [PubMed]
- Marosfoi, M. G.; Korin, N.; Gounis, M. J.; Uzun, O.; Vedantham, S.; Langan, E. T.; Papa, A.-L.; Brooks, O. W.; Johnson, C.; Puri, A. S.; Bhatta, D.; Kanapathipillai, M.; Bronstein, B. R.; Chueh, J.-Y.; Ingber, D. E.; Wakhloo, A. K. , Shear-Activated Nanoparticle Aggregates Combined With Temporary Endovascular Bypass to Treat Large Vessel Occlusion. Stroke 2015, 46, (12). 3507–3513. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Zhang, Y.; Xu, J.; Liu, G.; Di, C.; Zhao, X.; Li, X.; Li, Y.; Pang, N.; Yang, C.; Li, Y.; Li, B.; Lu, Z.; Wang, M.; Dai, K.; Yan, R.; Li, S.; Nie, G. , Engineered Nanoplatelets for Targeted Delivery of Plasminogen Activators to Reverse Thrombus in Multiple Mouse Thrombosis Models. Adv Mater 2020, 32, (4). e1905145. [Google Scholar]
- Veronese, F. M.; Pasut, G. , PEGylation, successful approach to drug delivery. Drug Discov Today 2005, 10, (21). 1451–8. [Google Scholar] [CrossRef]
- Shi, D.; Beasock, D.; Fessler, A.; Szebeni, J.; Ljubimova, J. Y.; Afonin, K. A.; Dobrovolskaia, M. A. , To PEGylate or not to PEGylate: Immunological properties of nanomedicine's most popular component, polyethylene glycol and its alternatives. Adv Drug Deliv Rev 2022, 180, 114079. [Google Scholar] [CrossRef]
- Ramirez, M. L. A.; Bindini, E.; Moretti, P.; Soler Illia, G.; Amenitsch, H.; Andreozzi, P.; Ortore, M. G.; Moya, S. E. , Impact of PEGylation on the degradation and pore organization in mesoporous silica nanoparticles: A study of the inner mesoporous structure in physiologically relevant ionic conditions. Colloids Surf B Biointerfaces 2022, 219, 112797. [Google Scholar] [CrossRef] [PubMed]
- Le Devedec, F.; Strandman, S.; Hildgen, P.; Leclair, G.; Zhu, X. X. , PEGylated bile acids for use in drug delivery systems: enhanced solubility and bioavailability of itraconazole. Mol Pharm 2013, 10, (8). 3057–66. [Google Scholar]
- Gajbhiye, K. R.; Pawar, A.; Mahadik, K. R.; Gajbhiye, V. , PEGylated nanocarriers: A promising tool for targeted delivery to the brain. Colloids Surf B Biointerfaces 2020, 187, 110770. [Google Scholar] [CrossRef] [PubMed]
- McDonnell, T. C. R.; Willis, R.; Pericleous, C.; Ripoll, V. M.; Giles, I. P.; Isenberg, D. A.; Brasier, A. R.; Gonzalez, E. B.; Papalardo, E.; Romay-Penabad, Z.; Jamaluddin, M.; Ioannou, Y.; Rahman, A. , PEGylated Domain I of Beta-2-Glycoprotein I Inhibits the Binding, Coagulopathic, and Thrombogenic Properties of IgG From Patients With the Antiphospholipid Syndrome. Front Immunol 2018, 9, 2413. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Liu, M. R.; Wan, H. T. , Discussion about several potential drawbacks of PEGylated therapeutic proteins. Biol Pharm Bull 2014, 37, (3). 335–9. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Liu, M.-r.; Wan, H.-t. , Discussion about Several Potential Drawbacks of PEGylated Therapeutic Proteins. Biological and Pharmaceutical Bulletin 2014, 37, (3). 335–339. [Google Scholar] [CrossRef] [PubMed]
- Boddu, S. H. S.; Acharya, D.; Hala, V.; Jani, H.; Pande, S.; Patel, C.; Shahwan, M.; Jwala, R.; Ranch, K. M. , An Update on Strategies to Deliver Protein and Peptide Drugs to the Eye. ACS Omega 2023, 8, (39). 35470–35498. [Google Scholar] [CrossRef] [PubMed]
- Zamanlu, M.; Eskandani, M.; Barar, J.; Jaymand, M.; Pakchin, P. S.; Farhoudi, M. , Enhanced thrombolysis using tissue plasminogen activator (tPA)-loaded PEGylated PLGA nanoparticles for ischemic stroke. Journal of Drug Delivery Science and Technology 2019, 53, 101165. [Google Scholar] [CrossRef]
- Qi, F.; Hu, C.; Yu, W.; Hu, T. , Conjugation with Eight-Arm PEG Markedly Improves the In Vitro Activity and Prolongs the Blood Circulation of Staphylokinase. Bioconjug Chem 2018, 29, (2). 451–458. [Google Scholar] [CrossRef] [PubMed]
- Nan, D.; Jin, H.; Yang, D.; Yu, W.; Jia, J.; Yu, Z.; Tan, H.; Sun, Y.; Hao, H.; Qu, X.; Huang, Y. , Combination of Polyethylene Glycol-Conjugated Urokinase Nanogels and Urokinase for Acute Ischemic Stroke Therapeutic Implications. Transl Stroke Res 2021, 12, (5). 844–857. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H. X.; O'Rear, E. A. , An In Vitro Thrombolysis Study Using a Mixture of Fast-Acting and Slower Release Microspheres. Pharm Res 2016, 33, (7). 1552–63. [Google Scholar] [CrossRef] [PubMed]
- Nsairat, H.; Khater, D.; Sayed, U.; Odeh, F.; Al Bawab, A.; Alshaer, W. , Liposomes: structure, composition, types, and clinical applications. Heliyon 2022, 8, (5). e09394. [Google Scholar] [CrossRef] [PubMed]
- Kaddah, S.; Khreich, N.; Kaddah, F.; Charcosset, C.; Greige-Gerges, H. , Cholesterol modulates the liposome membrane fluidity and permeability for a hydrophilic molecule. Food and Chemical Toxicology 2018, 113, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Sriwidodo; Umar, A. K.; Wathoni, N.; Zothantluanga, J. H.; Das, S.; Luckanagul, J. A., Liposome-polymer complex for drug delivery system and vaccine stabilization. Heliyon 2022, 8, (2), e08934.
- Yao, X.; Fan, X.; Yan, N. , Cryo-EM analysis of a membrane protein embedded in the liposome. Proceedings of the National Academy of Sciences 2020, 117, (31). 18497–18503. [Google Scholar] [CrossRef] [PubMed]
- Lamichhane, N.; Udayakumar, T. S.; D'Souza, W. D.; Simone, C. B., 2nd; Raghavan, S. R.; Polf, J.; Mahmood, J., Liposomes: Clinical Applications and Potential for Image-Guided Drug Delivery. Molecules 2018, 23, (2).
- Edwards, K.; Johnsson, M.; Karlsson, G.; Silvander, M. , Effect of polyethyleneglycol-phospholipids on aggregate structure in preparations of small unilamellar liposomes. Biophys J 1997, 73, (1). 258–66. [Google Scholar] [CrossRef]
- Hopkins, A. L.; Groom, C. R. , The druggable genome. Nature reviews Drug discovery 2002, 1, (9). 727–730. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Li, X.; Zhao, C. , Strategies to Obtain Encapsulation and Controlled Release of Small Hydrophilic Molecules. Front Bioeng Biotechnol 2020, 8, 437. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Li, W.; Wang, Z.; Lu, J. , Lipid-Based Nanotechnology: Liposome. Pharmaceutics 2024, 16, (1). 34. [Google Scholar] [CrossRef] [PubMed]
- Elbayoumi, T. A.; Torchilin, V. P. , Liposomes for targeted delivery of antithrombotic drugs. Expert Opin Drug Deliv 2008, 5, (11). 1185–98. [Google Scholar] [CrossRef] [PubMed]
- Kwiecinski, J.; Peetermans, M.; Liesenborghs, L.; Na, M.; Björnsdottir, H.; Zhu, X.; Jacobsson, G.; Johansson, B. R.; Geoghegan, J. A.; Foster, T. J. , Staphylokinase control of Staphylococcus aureus biofilm formation and detachment through host plasminogen activation. The Journal of infectious diseases 2016, 213, (1). 139–148. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L. T.; Vogel, H. J. , Staphylokinase has distinct modes of interaction with antimicrobial peptides, modulating its plasminogen-activation properties. Scientific Reports 2016, 6, (1). 31817. [Google Scholar] [CrossRef] [PubMed]
- Saxena, V.; Gacchina Johnson, C.; Negussie, A. H.; Sharma, K. V.; Dreher, M. R.; Wood, B. J. , Temperature-sensitive liposome-mediated delivery of thrombolytic agents. Int J Hyperthermia 2015, 31, (1). 67–73. [Google Scholar] [CrossRef] [PubMed]
- Eck, R. J.; Elling, T.; Sutton, A. J.; Wetterslev, J.; Gluud, C.; van der Horst, I. C. C.; Gans, R. O. B.; Meijer, K.; Keus, F. , Anticoagulants for thrombosis prophylaxis in acutely ill patients admitted to hospital: systematic review and network meta-analysis. BMJ 2022, 378, e070022. [Google Scholar] [CrossRef] [PubMed]
- Kose, G. T.; Arica, M. Y.; Hasirci, V. , Low-molecular-weight heparin-conjugated liposomes with improved stability and hemocompatibility. Drug Deliv 1998, 5, (4). 257–64. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.-K.; Kim, C.-K. , Topical delivery of low-molecular-weight heparin with surface-charged flexible liposomes. Biomaterials 2006, 27, (2). 271–280. [Google Scholar] [CrossRef] [PubMed]
- Mahjoub, H.; Roméo, P.; Leung, T. K.; Burelle, D.; Cartier, R.; Basmadjian, A. J., Sudden death after intravenous administration of a perflutren contrast agent: a case of pseudocomplication? J Am Soc Echocardiogr 2009, 22, (6), 753.e5-8.
- Muskula, P. R.; Main, M. L., Safety With Echocardiographic Contrast Agents. Circulation: Cardiovascular Imaging 2017, 10, (4), e005459.
- Szijjarto, C.; Rossi, S.; Waton, G.; Krafft, M. P. , Effects of perfluorocarbon gases on the size and stability characteristics of phospholipid-coated microbubbles: Osmotic effect versus interfacial film stabilization. Langmuir 2012, 28, (2). 1182–1189. [Google Scholar] [CrossRef] [PubMed]
- Schnell, C. , Gas vesicles enable ultrasound imaging. Nature Methods 2018, 15, (3). 159–159. [Google Scholar] [CrossRef]
- Kennedy, S. R.; Lafond, M.; Haworth, K. J.; Escudero, D. S.; Ionascu, D.; Frierson, B.; Huang, S.; Klegerman, M. E.; Peng, T.; McPherson, D. D.; Genstler, C.; Holland, C. K. , Initiating and imaging cavitation from infused echo contrast agents through the EkoSonic catheter. Scientific Reports 2023, 13, (1). 6191. [Google Scholar] [CrossRef] [PubMed]
- Smith, D. A.; Vaidya, S. S.; Kopechek, J. A.; Huang, S. L.; Klegerman, M. E.; McPherson, D. D.; Holland, C. K. , Ultrasound-triggered release of recombinant tissue-type plasminogen activator from echogenic liposomes. Ultrasound Med Biol 2010, 36, (1). 145–57. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.-L. , Liposomes in ultrasonic drug and gene delivery. Advanced Drug Delivery Reviews 2008, 60, (10). 1167–1176. [Google Scholar] [CrossRef] [PubMed]
- Tiukinhoy-Laing, S. D.; Buchanan, K.; Parikh, D.; Huang, S.; Macdonald, R. C.; McPherson, D. D.; Klegerman, M. E. , Fibrin targeting of tissue plasminogen activator-loaded echogenic liposomes. Journal of Drug Targeting 2007, 15, (2). 109–114. [Google Scholar] [CrossRef]
- Shaw, G. J.; Meunier, J. M.; Huang, S.-L.; Lindsell, C. J.; McPherson, D. D.; Holland, C. K. , Ultrasound-enhanced thrombolysis with tPA-loaded echogenic liposomes. Thrombosis research 2009, 124, (3). 306–310. [Google Scholar] [CrossRef]
- Smith, D. A.; Vaidya, S.; Kopechek, J. A.; Hitchcock, K. E.; Huang, S. L.; McPherson, D. D.; Holland, C. K., Echogenic liposomes loaded with recombinant tissue-type plasminogen activator (rt-PA) for image-guided, ultrasound-triggered drug release. The Journal of the Acoustical Society of America 2007, 122, (5_Supplement), 3007-3007.
- Holland, C. K.; McPherson, D. D. , ECHOGENIC LIPSOMES FOR TARGETED DRUG DELIVERY. Proc IEEE Int Symp Biomed Imaging 2009, 2009, 755–758. [Google Scholar]
- Ricklin, D.; Hajishengallis, G.; Yang, K.; Lambris, J. D. , Complement: a key system for immune surveillance and homeostasis. Nat Immunol 2010, 11, (9). 785–97. [Google Scholar] [CrossRef] [PubMed]
- Tassa, C.; Shaw, S. Y.; Weissleder, R. , Dextran-coated iron oxide nanoparticles: a versatile platform for targeted molecular imaging, molecular diagnostics, and therapy. Acc Chem Res 2011, 44, (10). 842–52. [Google Scholar] [CrossRef] [PubMed]
- Silva, A. K.; Luciani, N.; Gazeau, F.; Aubertin, K.; Bonneau, S.; Chauvierre, C.; Letourneur, D.; Wilhelm, C. , Combining magnetic nanoparticles with cell derived microvesicles for drug loading and targeting. Nanomedicine 2015, 11, (3). 645–55. [Google Scholar] [CrossRef] [PubMed]
- de Saint Victor, M.; Crake, C.; Coussios, C. C.; Stride, E. , Properties, characteristics and applications of microbubbles for sonothrombolysis. Expert Opin Drug Deliv 2014, 11, (2). 187–209. [Google Scholar] [CrossRef] [PubMed]
- Cheng, K.; Li, T. S.; Malliaras, K.; Davis, D. R.; Zhang, Y.; Marban, E. , Magnetic targeting enhances engraftment and functional benefit of iron-labeled cardiosphere-derived cells in myocardial infarction. Circ Res 2010, 106, (10). 1570–81. [Google Scholar] [CrossRef] [PubMed]
- Fagg, W. S.; Liu, N.; Yang, M. J.; Cheng, K.; Chung, E.; Kim, J. S.; Wu, G.; Fair, J. , Magnetic Targeting of Stem Cell Derivatives Enhances Hepatic Engraftment into Structurally Normal Liver. Cell Transplant 2017, 26, (12). 1868–1877. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Liu, Y.; Zhang, T.; Wang, Q.; Huang, L.; Zhong, Z.; Lin, J.; Hu, K.; Xin, H.; Wang, X. , Targeted Thrombolytic Therapy with Metal-Organic-Framework-Derived Carbon Based Platforms with Multimodal Capabilities. ACS Appl Mater Interfaces 2021, 13, (21). 24453–24462. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Y.; Zhang, Y.; Xu, J.; Zhou, J.; Liu, J.; Ye, M.; Zhang, L.; Qiao, B.; Wang, Z. G.; Ran, H. T.; Guo, D. , Low-Intensity Focused Ultrasound-Responsive Phase-Transitional Nanoparticles for Thrombolysis without Vascular Damage: A Synergistic Nonpharmaceutical Strategy. ACS Nano 2019, 13, (3). 3387–3403. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Liu, C.; Pang, Z. , Dendrimer-Based Drug Delivery Systems for Brain Targeting. Biomolecules 2019, 9, (12). 790. [Google Scholar] [CrossRef] [PubMed]
- An, H.; Deng, X.; Wang, F.; Xu, P.; Wang, N. , Dendrimers as Nanocarriers for the Delivery of Drugs Obtained from Natural Products. Polymers 2023, 15, (10). 2292. [Google Scholar] [CrossRef] [PubMed]
- Shadrack, D. M.; Swai, H. S.; Munissi, J. J. E.; Mubofu, E. B.; Nyandoro, S. S. , Polyamidoamine Dendrimers for Enhanced Solubility of Small Molecules and Other Desirable Properties for Site Specific Delivery: Insights from Experimental and Computational Studies. Molecules 2018, 23, (6). 1419. [Google Scholar] [CrossRef] [PubMed]
- Buhleier, E.; Wehner, W., F., & Vogtle, F.,(1978).“Cascade”-and “nonskid-chain-like” syntheses of molecular cavity topologies. Synthesis, 155-158.
- Tomalia, D. A.; Baker, H.; Dewald, J.; Hall, M.; Kallos, G.; Martin, S.; Roeck, J.; Ryder, J.; Smith, P. , A New Class of Polymers: Starburst-Dendritic Macromolecules. Polymer Journal 1985, 17, (1). 117–132. [Google Scholar] [CrossRef]
- Kono, K. , Dendrimer-based bionanomaterials produced by surface modification, assembly and hybrid formation. Polymer Journal 2012, 44, (6). 531–540. [Google Scholar] [CrossRef]
- Svenson, S.; Tomalia, D. A. , Dendrimers in biomedical applications--reflections on the field. Adv Drug Deliv Rev 2005, 57, (15). 2106–29. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Kittrell, S.; Yeudall, W. A.; Yang, H. , Folic acid-decorated polyamidoamine dendrimer mediates selective uptake and high expression of genes in head and neck cancer cells. Nanomedicine (Lond) 2016, 11, (22). 2959–2973. [Google Scholar] [CrossRef] [PubMed]
- Daralnakhla, H.; Saher, O.; Zamolo, S.; Bazaz, S.; P. Bost, J.; Heitz, M.; Lundin, K. E.; EL Andaloussi, S.; Darbre, T.; Reymond, J.-L.; Zain, R.; Smith, C. I. E., Lipophilic Peptide Dendrimers for Delivery of Splice-Switching Oligonucleotides. Pharmaceutics 2021, 13, (1), 116.
- Marcinkowska, M.; Sobierajska, E.; Stanczyk, M.; Janaszewska, A.; Chworos, A.; Klajnert-Maculewicz, B., Conjugate of PAMAM Dendrimer, Doxorubicin and Monoclonal Antibody-Trastuzumab: The New Approach of a Well-Known Strategy. Polymers (Basel) 2018, 10, (2).
- Sharma, R.; Liaw, K.; Sharma, A.; Jimenez, A.; Chang, M.; Salazar, S.; Amlani, I.; Kannan, S.; Kannan, R. M. , Glycosylation of PAMAM dendrimers significantly improves tumor macrophage targeting and specificity in glioblastoma. J Control Release 2021, 337, 179–192. [Google Scholar] [CrossRef] [PubMed]
- Jones, C. F.; Campbell, R. A.; Franks, Z.; Gibson, C. C.; Thiagarajan, G.; Vieira-de-Abreu, A.; Sukavaneshvar, S.; Mohammad, S. F.; Li, D. Y.; Ghandehari, H.; Weyrich, A. S.; Brooks, B. D.; Grainger, D. W. , Cationic PAMAM dendrimers disrupt key platelet functions. Mol Pharm 2012, 9, (6). 1599–611. [Google Scholar] [CrossRef] [PubMed]
- Aisina, R.; Mukhametova, L.; Ivanova, E. , Influence cationic and anionic PAMAM dendrimers of low generation on selected hemostatic parameters in vitro. Mater Sci Eng C Mater Biol Appl 2020, 109, 110605. [Google Scholar] [CrossRef] [PubMed]
- Lo, S. T.; Stern, S.; Clogston, J. D.; Zheng, J.; Adiseshaiah, P. P.; Dobrovolskaia, M.; Lim, J.; Patri, A. K.; Sun, X.; Simanek, E. E. , Biological assessment of triazine dendrimer: toxicological profiles, solution behavior, biodistribution, drug release and efficacy in a PEGylated, paclitaxel construct. Mol Pharm 2010, 7, (4). 993–1006. [Google Scholar] [CrossRef]
- Mehrizi, T. Z.; Kafiabad, S. A.; Eshghi, P. , Effects and treatment applications of polymeric nanoparticles on improving platelets' storage time: a review of the literature from 2010 to 2020. Blood Res 2021, 56, (4). 215–228. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.-F.; Lü, S.; Gao, C.; Yang, J.; Yan, X.; Li, T.; Wen, N.; Huang, M.; Liu, M. , Multiarm-polyethylene glycol-polyglutamic acid peptide dendrimer: Design, synthesis, and dissolving thrombus. Journal of Biomedical Materials Research Part A 2018, 106, (6). 1687–1696. [Google Scholar] [CrossRef] [PubMed]
- Buwalda, S. J.; Vermonden, T.; Hennink, W. E. , Hydrogels for Therapeutic Delivery: Current Developments and Future Directions. Biomacromolecules 2017, 18, (2). 316–330. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.; Zhang, S.; Li, C.; Li, K.; Jia, X.; Wei, Q.; Qi, H.; Zhang, J. , Functionally integrating nanoparticles alleviate deep vein thrombosis in pregnancy and rescue intrauterine growth restriction. Nature Communications 2022, 13, (1). 7166. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, H. R.; Sakariassen, K. S. , Factors controlling thrombus formation on arterial lesions. Ann N Y Acad Sci 1985, 454, 162–77. [Google Scholar] [CrossRef] [PubMed]
- Sakariassen, K. S.; Joss, R.; Muggli, R.; Kuhn, H.; Tschopp, T. B.; Sage, H.; Baumgartner, H. R. , Collagen type III induced ex vivo thrombogenesis in humans. Role of platelets and leukocytes in deposition of fibrin. Arteriosclerosis 1990, 10, (2). 276–84. [Google Scholar] [CrossRef] [PubMed]
- Sakariassen, K. S.; Orning, L.; Turitto, V. T. , The impact of blood shear rate on arterial thrombus formation. Future Sci OA 2015, 1, (4). Fso30. [Google Scholar] [CrossRef] [PubMed]
- van Rooij, B. J. M.; Závodszky, G.; Hoekstra, A. G.; Ku, D. N. , Biorheology of occlusive thrombi formation under high shear: in vitro growth and shrinkage. Scientific Reports 2020, 10, (1). 18604. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Pei, Y.; Gao, L.; He, Q.; Zhang, H.; Zhu, L.; Zhang, Z.; Hou, L. , Shear force responsive and fixed-point separated system for targeted treatment of arterial thrombus. Nano Today 2021, 38, 101186. [Google Scholar] [CrossRef]
- Thomas, M. R.; Storey, R. F. , The role of platelets in inflammation. Thromb Haemost 2015, 114, (3). 449–58. [Google Scholar]
- Perkins, L. A.; Anderson, C. J.; Novelli, E. M. , Targeting P-Selectin Adhesion Molecule in Molecular Imaging: P-Selectin Expression as a Valuable Imaging Biomarker of Inflammation in Cardiovascular Disease. J Nucl Med 2019, 60, (12). 1691–1697. [Google Scholar] [CrossRef] [PubMed]
- Kappelmayer, J.; Nagy, B., Jr. , The Interaction of Selectins and PSGL-1 as a Key Component in Thrombus Formation and Cancer Progression. Biomed Res Int 2017, 2017, 6138145. [Google Scholar] [CrossRef]
- Arabshomali, A.; Bazzazzadehgan, S.; Mahdi, F.; Shariat-Madar, Z. , Potential Benefits of Antioxidant Phytochemicals in Type 2 Diabetes. Molecules 2023, 28, (20). 7209. [Google Scholar] [CrossRef] [PubMed]
- Stark, K.; Massberg, S. , Interplay between inflammation and thrombosis in cardiovascular pathology. Nat Rev Cardiol 2021, 18, (9). 666–682. [Google Scholar] [CrossRef] [PubMed]
- Wichterle, O.; Lim, D. , Hydrophilic gels for biological use. Nature 1960, 185, (4706). 117–118. [Google Scholar] [CrossRef]
- Sinawang, G.; Osaki, M.; Takashima, Y.; Yamaguchi, H.; Harada, A. , Biofunctional hydrogels based on host–guest interactions. Polymer Journal 2020, 52, (8). 839–859. [Google Scholar] [CrossRef]
- FitzSimons, T. M.; Oentoro, F.; Shanbhag, T. V.; Anslyn, E. V.; Rosales, A. M. , Preferential control of forward reaction kinetics in hydrogels crosslinked with reversible conjugate additions. Macromolecules 2020, 53, (10). 3738–3746. [Google Scholar] [CrossRef]
- Vereroudakis, E.; Bantawa, M.; Lafleur, R. P. M.; Parisi, D.; Matsumoto, N. M.; Peeters, J. W.; Del Gado, E.; Meijer, E. W.; Vlassopoulos, D. , Competitive Supramolecular Associations Mediate the Viscoelasticity of Binary Hydrogels. ACS Cent Sci 2020, 6, (8). 1401–1411. [Google Scholar] [CrossRef] [PubMed]
- Brown, A. C.; Stabenfeldt, S. E.; Ahn, B.; Hannan, R. T.; Dhada, K. S.; Herman, E. S.; Stefanelli, V.; Guzzetta, N.; Alexeev, A.; Lam, W. A.; Lyon, L. A.; Barker, T. H. , Ultrasoft microgels displaying emergent platelet-like behaviours. Nat Mater 2014, 13, (12). 1108–1114. [Google Scholar] [CrossRef]
- Ren, W.; Sands, M.; Han, X.; Tsipursky, M.; Irudayaraj, J. , Hydrogel-Based Oxygen and Drug Delivery Dressing for Improved Wound Healing. ACS Omega 2024, 9, (22). 24095–24104. [Google Scholar] [CrossRef] [PubMed]
- Clegg, J. R.; Adebowale, K.; Zhao, Z.; Mitragotri, S., Hydrogels in the clinic: An update. Bioengineering & Translational Medicine n/a, (n/a), e10680.
- Andrgie, A. T.; Darge, H. F.; Mekonnen, T. W.; Birhan, Y. S.; Hanurry, E. Y.; Chou, H. Y.; Wang, C. F.; Tsai, H. C.; Yang, J. M.; Chang, Y. H., Ibuprofen-Loaded Heparin Modified Thermosensitive Hydrogel for Inhibiting Excessive Inflammation and Promoting Wound Healing. Polymers (Basel) 2020, 12, (11).
- Wang, Y.; Wu, Y.; Long, L.; Yang, L.; Fu, D.; Hu, C.; Kong, Q.; Wang, Y., Inflammation-Responsive Drug-Loaded Hydrogels with Sequential Hemostasis, Antibacterial, and Anti-Inflammatory Behavior for Chronically Infected Diabetic Wound Treatment. ACS Applied Materials & Interfaces 2021, 13, (28), 33584-33599.
- Zhang, D.; Ren, Y.; He, Y.; Chang, R.; Guo, S.; Ma, S.; Guan, F.; Yao, M. , In situ forming and biocompatible hyaluronic acid hydrogel with reactive oxygen species-scavenging activity to improve traumatic brain injury repair by suppressing oxidative stress and neuroinflammation. Materials Today Bio 2022, 15, 100278. [Google Scholar] [CrossRef] [PubMed]
- Bae, K. H.; Wang, L.-S.; Kurisawa, M. , Injectable biodegradable hydrogels: progress and challenges. Journal of Materials Chemistry B 2013, 1, (40). 5371–5388. [Google Scholar] [CrossRef] [PubMed]
- Vermonden, T.; Censi, R.; Hennink, W. E. , Hydrogels for Protein Delivery. Chemical Reviews 2012, 112, (5). 2853–2888. [Google Scholar] [CrossRef]
- Rosenblum, D.; Joshi, N.; Tao, W.; Karp, J. M.; Peer, D. , Progress and challenges towards targeted delivery of cancer therapeutics. Nature Communications 2018, 9, (1). 1410. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Wang, X.; Xu, W.; Li, Y.; Lai, R.; Qiu, X.; Chen, X.; Chen, Z.; Mi, B.; Wu, M.; Wang, J. , Translational Challenges and Prospective Solutions in the Implementation of Biomimetic Delivery Systems. Pharmaceutics 2023, 15, (11). 2623. [Google Scholar] [CrossRef] [PubMed]
- Guan, Q.; Dou, H. , Thrombus-Targeting Polymeric Nanocarriers and Their Biomedical Applications in Thrombolytic Therapy. Front Physiol 2021, 12, 763085. [Google Scholar] [CrossRef] [PubMed]
- Ts'ao, C. H.; Spaet, T. H. , Ultramicroscopic changes in the rabbit inferior vena cava following partial constriction. Am J Pathol 1967, 51, (5). 789–813. [Google Scholar]
- Kohli, S.; Ranjan, S.; Hoffmann, J.; Kashif, M.; Daniel, E. A.; Al-Dabet, M. d. M.; Bock, F.; Nazir, S.; Huebner, H.; Mertens, P. R.; Fischer, K.-D.; Zenclussen, A. C.; Offermanns, S.; Aharon, A.; Brenner, B.; Shahzad, K.; Ruebner, M.; Isermann, B. , Maternal extracellular vesicles and platelets promote preeclampsia via inflammasome activation in trophoblasts. Blood 2016, 128, (17). 2153–2164. [Google Scholar] [CrossRef] [PubMed]
- Kohli, S.; Isermann, B. , Crosstalk between inflammation and coagulation: Focus on pregnancy related complications. Thrombosis Update 2021, 5, 100072. [Google Scholar] [CrossRef]
- Nørgaard, I.; Nielsen, S. F.; Nordestgaard, B. G. , Complement C3 and High Risk of Venous Thromboembolism: 80517 Individuals from the Copenhagen General Population Study. Clinical Chemistry 2016, 62, (3). 525–534. [Google Scholar] [CrossRef] [PubMed]
- Budnik, I.; Brill, A. , Immune Factors in Deep Vein Thrombosis Initiation. Trends Immunol 2018, 39, (8). 610–623. [Google Scholar] [CrossRef]
- Amalia, M.; Puteri, M. U.; Saputri, F. C.; Sauriasari, R.; Widyantoro, B., Platelet Glycoprotein-Ib (GPIb) May Serve as a Bridge between Type 2 Diabetes Mellitus (T2DM) and Atherosclerosis, Making It a Potential Target for Antiplatelet Agents in T2DM Patients. Life (Basel) 2023, 13, (7).
- van der Meijden, P. E. J.; Heemskerk, J. W. M. , Platelet biology and functions: new concepts and clinical perspectives. Nat Rev Cardiol 2019, 16, (3). 166–179. [Google Scholar] [CrossRef] [PubMed]
- Jameson, S. S.; Baker, P. N.; Deehan, D. J.; Port, A.; Reed, M. R. , Evidence-base for aspirin as venous thromboembolic prophylaxis following joint replacement. Bone Joint Res 2014, 3, (5). 146–9. [Google Scholar] [CrossRef] [PubMed]
- Denorme, F.; Vanhoorelbeke, K.; De Meyer, S. F. , von Willebrand Factor and Platelet Glycoprotein Ib: A Thromboinflammatory Axis in Stroke. Frontiers in Immunology 2019, 10. [Google Scholar] [CrossRef]
- Ikeda, Y.; Handa, M.; Kawano, K.; Kamata, T.; Murata, M.; Araki, Y.; Anbo, H.; Kawai, Y.; Watanabe, K.; Itagaki, I.; et al. , The role of von Willebrand factor and fibrinogen in platelet aggregation under varying shear stress. J Clin Invest 1991, 87, (4). 1234–40. [Google Scholar] [CrossRef] [PubMed]
- Goto, S.; Ikeda, Y.; Murata, M.; Handa, M.; Takahashi, E.; Yoshioka, A.; Fujimura, Y.; Fukuyama, M.; Handa, S.; Ogawa, S. , Epinephrine augments von Willebrand factor-dependent shear-induced platelet aggregation. Circulation 1992, 86, (6). 1859–63. [Google Scholar] [CrossRef] [PubMed]
- Dayal, S.; Wilson, K. M.; Motto, D. G.; Miller, F. J., Jr.; Chauhan, A. K.; Lentz, S. R. , Hydrogen peroxide promotes aging-related platelet hyperactivation and thrombosis. Circulation 2013, 127, (12). 1308–16. [Google Scholar] [CrossRef] [PubMed]
- Mousa, S. A.; Bozarth, J. M.; Naik, U. P.; Slee, A. , Platelet GPIIb/IIIa binding characteristics of small molecule RGD mimetic: distinct binding profile for Roxifiban. Br J Pharmacol 2001, 133, (3). 331–6. [Google Scholar] [CrossRef]
- Varga-Szabo, D.; Pleines, I.; Nieswandt, B., Cell Adhesion Mechanisms in Platelets. Arteriosclerosis, Thrombosis, and Vascular Biology 2008, 28, (3), 403-412.
- Goto, S.; Tamura, N.; Li, M.; Handa, M.; Ikeda, Y.; Handa, S.; Ruggeri, Z. M. , Different effects of various anti-GPIIb-IIIa agents on shear-induced platelet activation and expression of procoagulant activity. J Thromb Haemost 2003, 1, (9). 2022–30. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y. T.; Noh, Y. W.; Han, J. H.; Cai, Q. Y.; Yoon, K. H.; Chung, B. H. , Biocompatible polymer-nanoparticle-based bimodal imaging contrast agents for the labeling and tracking of dendritic cells. Small 2008, 4, (10). 1640–5. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Wang, R.; Meng, N.; Guo, H.; Wu, S.; Wang, X.; Li, J.; Wang, H.; Jiang, K.; Xie, C.; Liu, Y.; Wang, H.; Lu, W. , Platelet membrane-functionalized nanoparticles with improved targeting ability and lower hemorrhagic risk for thrombolysis therapy. Journal of Controlled Release 2020, 328, 78–86. [Google Scholar] [CrossRef]
Figure 1.
Coagulation system. It responds to vascular injury to induce blood clot formation and prevent excessive bleeding.
Figure 1.
Coagulation system. It responds to vascular injury to induce blood clot formation and prevent excessive bleeding.
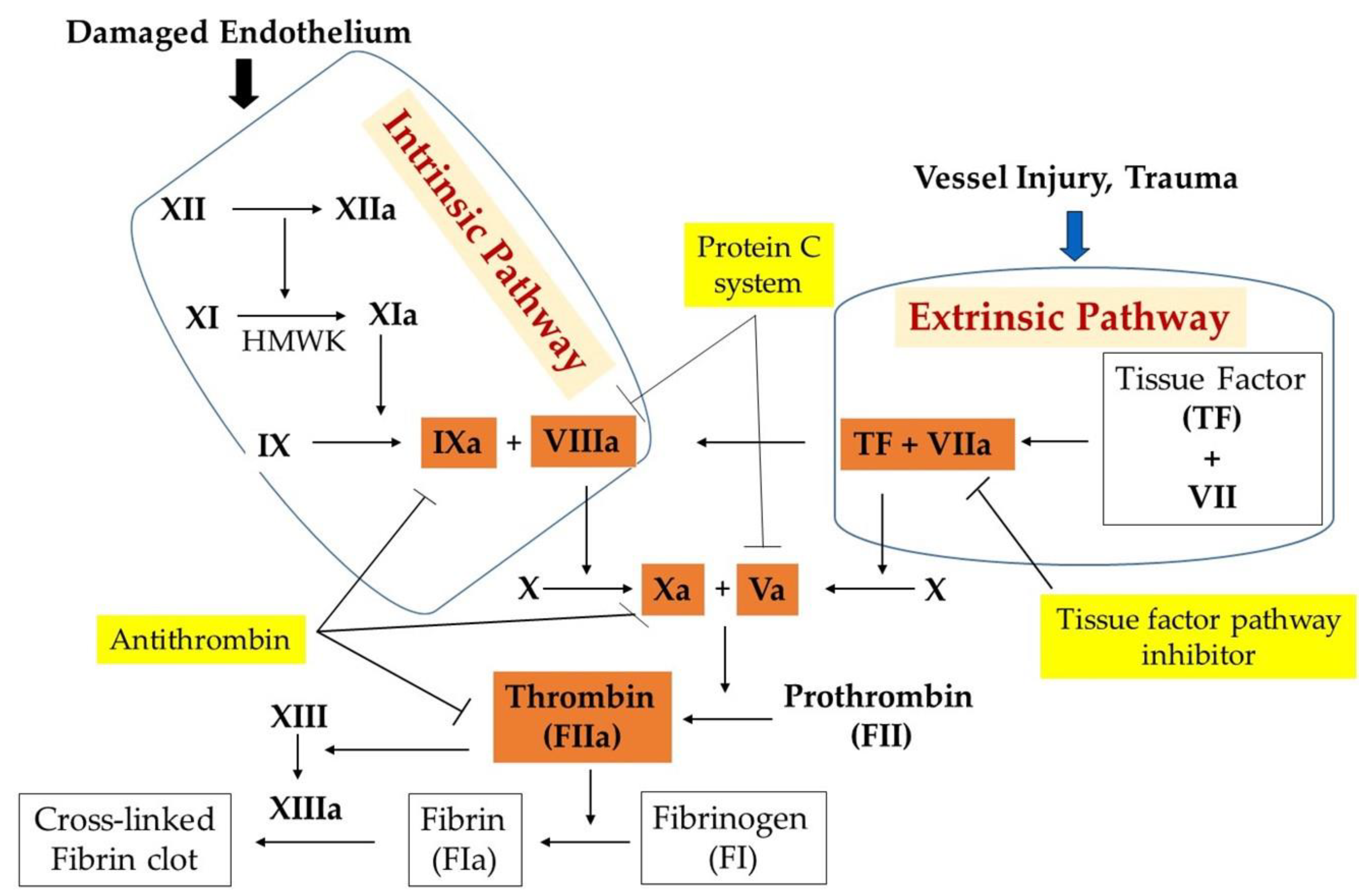
Figure 2.
Course of fibrinolytic activity and inhibition. Fibrinolysis is the process of dissolving blood clots. Tissue- or urokinase-type plasminogen activator (tPA, uPA,), kallikrein, and activated factor XII (FXIIa) can cause the transformation of plasminogen into plasmin. Formed plasmin degrades the deposited fibrin into fibrin degradation products (FDP). Plasminogen activator inhibitor -1 (PAI-1) and plasminogen activator inhibitor-2 inhibit both tPA and uPA, whereas C1- esterase inhibitor (C1-inhibitor) modulates both plasma kallikrein and FXIIa. α2-antiplasmin is a direct inhibitor of plasmin. α2-macroglobulin is a minor plasmin inhibitor. Activated thrombin-activated fibrinolysis inhibitor (TAFI) protects the fibrin clot against lysis.
Figure 2.
Course of fibrinolytic activity and inhibition. Fibrinolysis is the process of dissolving blood clots. Tissue- or urokinase-type plasminogen activator (tPA, uPA,), kallikrein, and activated factor XII (FXIIa) can cause the transformation of plasminogen into plasmin. Formed plasmin degrades the deposited fibrin into fibrin degradation products (FDP). Plasminogen activator inhibitor -1 (PAI-1) and plasminogen activator inhibitor-2 inhibit both tPA and uPA, whereas C1- esterase inhibitor (C1-inhibitor) modulates both plasma kallikrein and FXIIa. α2-antiplasmin is a direct inhibitor of plasmin. α2-macroglobulin is a minor plasmin inhibitor. Activated thrombin-activated fibrinolysis inhibitor (TAFI) protects the fibrin clot against lysis.
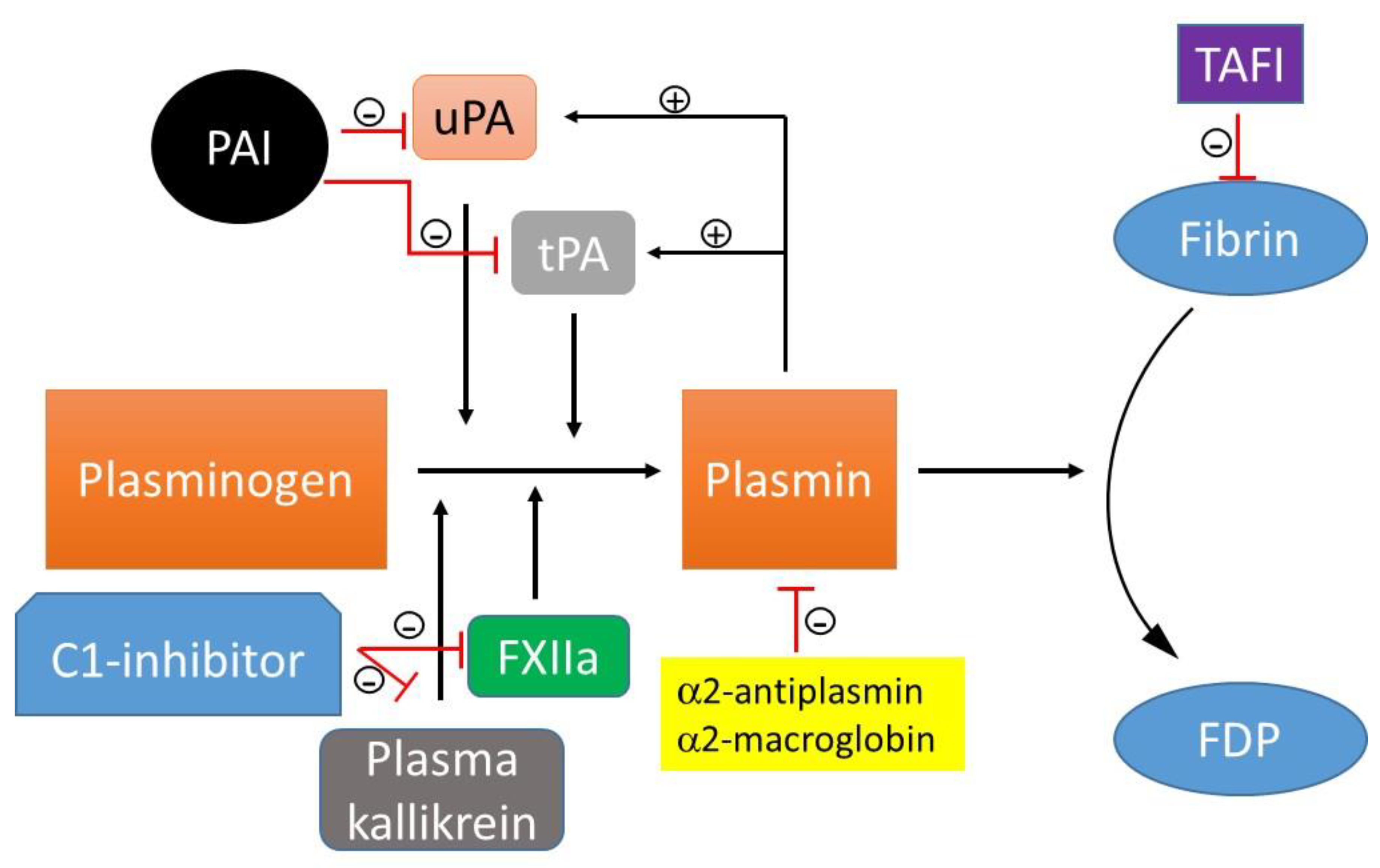
Figure 3.
The coagulation pathways and thrombosis. The bleeding time is a screening test for the arterial phase of hemostasis. Three in vitro tests are used to measure the time elapsed from activation of the intrinsic, extrinsic, and common pathways of the coagulation system. These include a) prothrombin time (PT); b) activated partial prothrombin time (APTT); and c) thrombin time (TT). Similarly, three in vitro predictive tests are used for the venous phase of hemostasis. These include: a) elevated D-dimer and CRP levels predict VTE occurrence and systemic inflammation status; b) fibrinolytic test is used to measure fibrinogen levels. Reduced fibrinolytic activity is a risk factor for venous thrombosis.; and c) thromboxane is released during thrombus formation. Increased urinary thromboxane is used to diagnose acute thromboembolic disease.
Figure 3.
The coagulation pathways and thrombosis. The bleeding time is a screening test for the arterial phase of hemostasis. Three in vitro tests are used to measure the time elapsed from activation of the intrinsic, extrinsic, and common pathways of the coagulation system. These include a) prothrombin time (PT); b) activated partial prothrombin time (APTT); and c) thrombin time (TT). Similarly, three in vitro predictive tests are used for the venous phase of hemostasis. These include: a) elevated D-dimer and CRP levels predict VTE occurrence and systemic inflammation status; b) fibrinolytic test is used to measure fibrinogen levels. Reduced fibrinolytic activity is a risk factor for venous thrombosis.; and c) thromboxane is released during thrombus formation. Increased urinary thromboxane is used to diagnose acute thromboembolic disease.
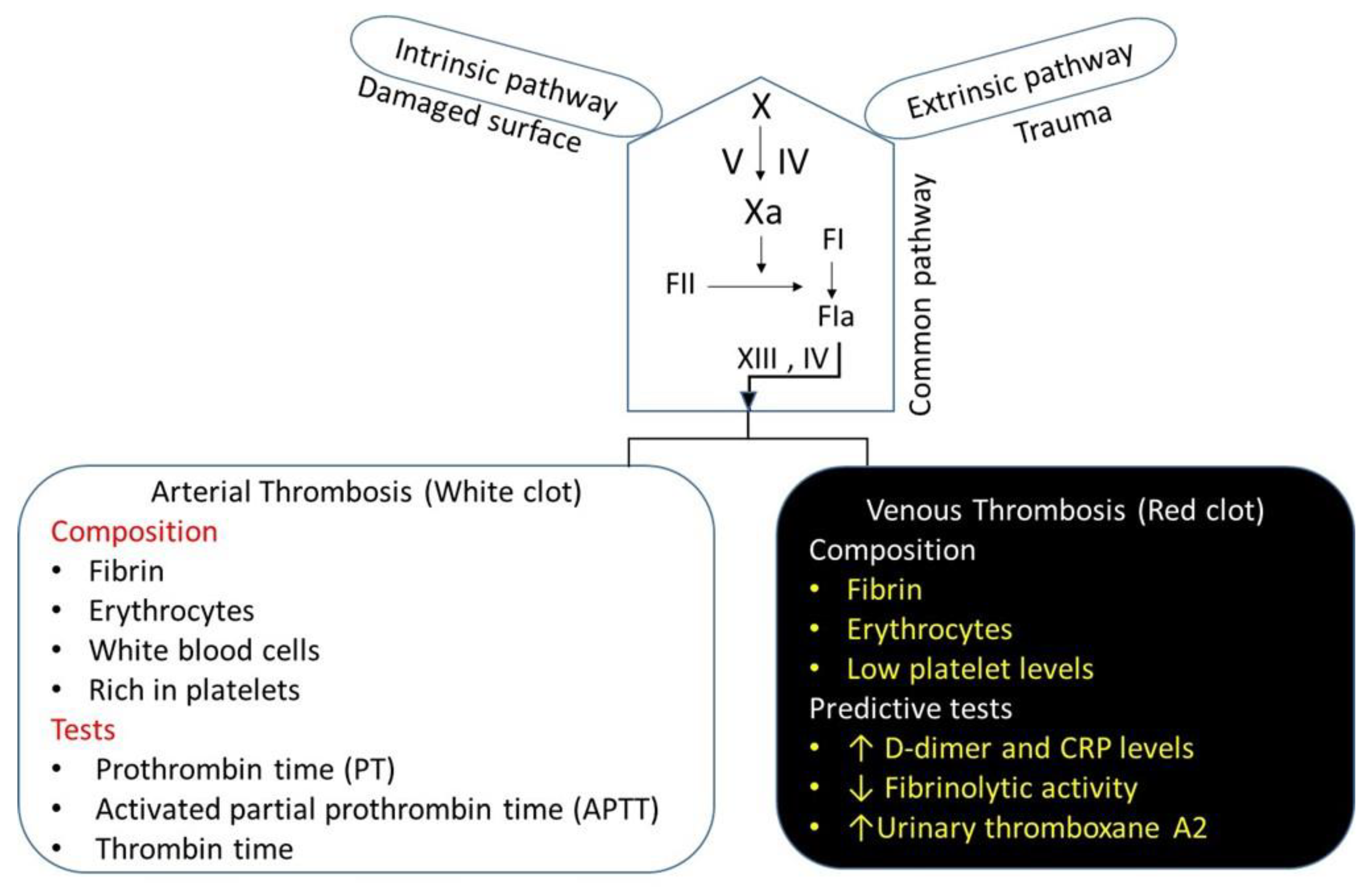
Figure 4.
The conventional treatments for VTE.
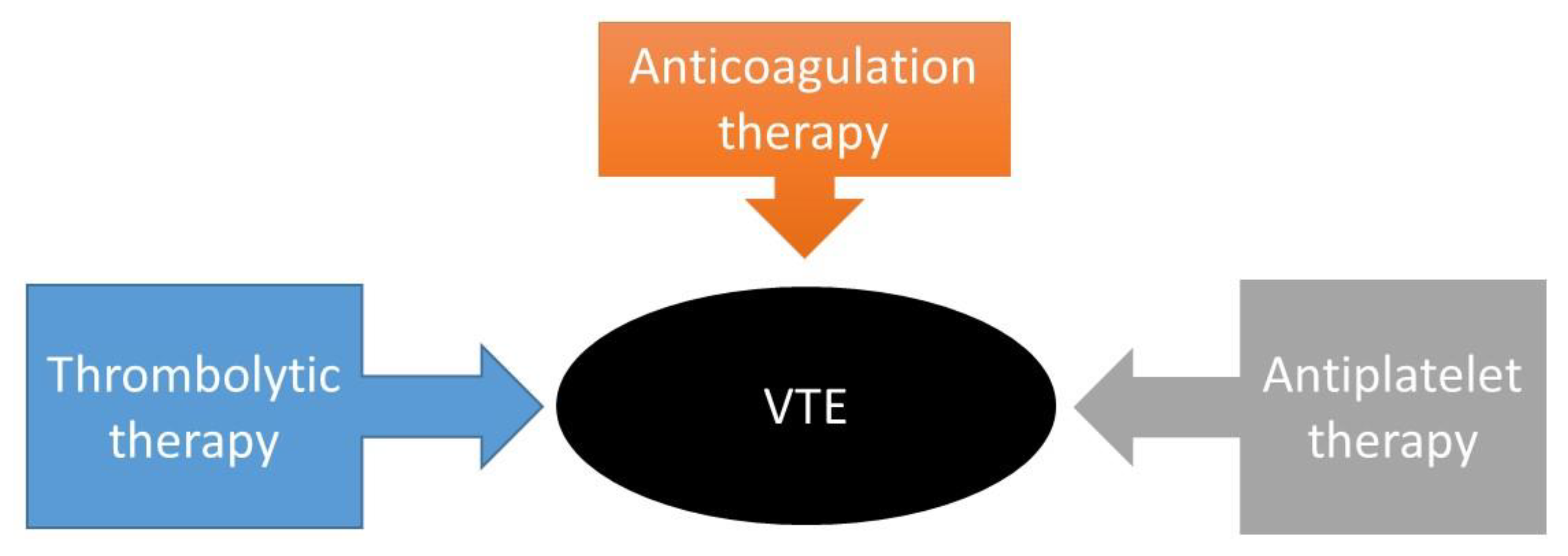
Table 1.
Selected antithrombotic drugs.
| Drug | Elimination | Risk | Comments |
|---|---|---|---|
Anticoagulants
Vitamin K antagonists
Antiplatelets
Thrombolytics
|
|
|
Approved
Approved
Approved
|
Table 2.
Compelling indications for antithrombotic drugs are based on benefits from outcome studies or clinical guidelines.
Table 2.
Compelling indications for antithrombotic drugs are based on benefits from outcome studies or clinical guidelines.
| Recommended Antithrombotic Drugs | ||||
|---|---|---|---|---|
| Compelling Indications | Anticoagulants | Antiplatelets | Thrombolytics | Ref. |
|
Coronary artery disease (CAD) CAD undergoing percutaneous coronary intervention Chronic kidney disease
Diabetes Knee replacement, orthopedic surgery Heart failure
Liver disease Recurrent VTE
|
Anticoagulants
Non–vitamin K antagonist oral anticoagulants Warfarin Rivaroxaban, Apixaban, LMWH, Fondaparinux Warfarin, oral anticoagulants Alteplase Heparins, apixaban, fondaparinux |
Antiplatelet Clopidogrel, prasugrel, or ticagrelor Purinergic receptor antagonists Aspirin Aspirin Aspirin and clopidogrel, |
Thrombolytics Thrombolytic Urokinase thrombolysis |
[77,78,79] [80] [81,82] [83] [83] [84,85] [86,87,88,89] [90,91,92,93] [94,95] [96] [97] [98,99] |
Table 4.
Characteristics of the nano-drugs and the in vitro thrombotic and fibrinolytic activity of these nano-drugs compared to their respective non-conjugated fibrinolytic activator alone.
Table 4.
Characteristics of the nano-drugs and the in vitro thrombotic and fibrinolytic activity of these nano-drugs compared to their respective non-conjugated fibrinolytic activator alone.
| Nano-Drugs | Characteristics | Outcome | Ref. |
|---|---|---|---|
PEGylation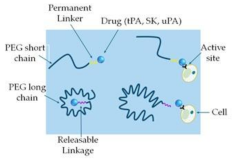
|
PEG-tPA PEG-UK PEG-SK PEG-SAK PEG-maleimide-(poly-SAK) |
Reduced proteolytic activity Slower inhibition kinetics by PAI-1 Increased fibrinolysis Resistant to plasmin cleavage Increased fibrinolysis Slightly increased fibrinolysis Increased bioactivity |
[129] [130] [131,132] [133] [134] |
Liposome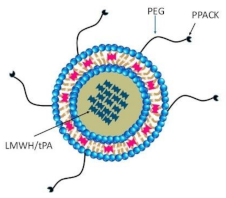
|
A circular-shaped diacyl-chain phospholipids/ phospholipid-attached PEG with cholesterol
|
Reduce thrombus weight Improve thrombolytic efficacy, reduce tPA-induced hemorrhage Prolong inhibition of thrombosis, reduced systemic side effects |
[135] [136] [137,138] |
Echogenic liposome & Polymeric nanoparticles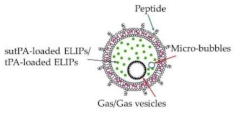 |
tPA-loaded ELIPs NIR-stimulated uPA release Magnetic nanoparticles Ultrasound-guided RDG-modified ELIPs |
Enhance thrombolytic efficiency Significant thrombolysis Prolong circulating tPA Improve thrombolytic efficacy Minimize off-target effects Similar thrombolysis, reduce the dose of tPA Complete thrombus elimination Effective thrombolysis in a rat embolism model Enhanced thrombolytic efficacy of tPA Improve recanalization rate |
[139,140,141] [142] [143] [139,144,145] [146] [146] [147] [148] [149] [150] |
Dendrimer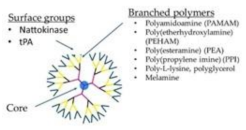
|
tPA-dendrimer complex Nattokinase-dendrimer complex LMWH-dendrimer complex Poly(amidoamine) dendrimers Poly(lysine) dendrimers |
High clot-dissolving activity Effective thrombolytic effect Prevents DVT Induce fibrinogen aggregation, contribute to the in vivo DIC, produce rapid coagulation Ideal carriers of protein drugs |
[151] [152] [153,154] [155] [156] [154] |
Mechanically activated nanotherapeutics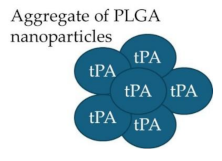
|
tPA- PLGA Shear-activated nanoparticle (tPA-SA-NP) complex tPA-loaded SA-NP and temporary endovascular bypass (TEB) |
Rapid clot dissolution Increase recanalization, reduce distal embolization |
[157,158] [159,160] [161] |
Platelet-based drug delivery system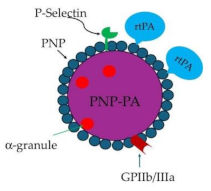
|
rtPA-PNP-PA | Thrombolysis | [162] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



