
Submitted:
30 July 2024
Posted:
02 August 2024
You are already at the latest version
Abstract
Climbing is an Olympic discipline in full development and multidisciplinary in nature, in which the influence of body composition and nutritional status on performance has not yet been clarified despite the quest for low weight in anti-gravity disciplines such as climbing. The present study aimed to do a nutritional (3-day dietary diaries) and body composition (ISAK profile) assessment of sport climbing athletes of different genders and sport levels. The mean age of the forty-six Spanish climbers (22 men and 24 women) was 30 years (SD: 9) with 7.66 years of experience (SD: 6.63). The mean somatotype of the athletes was classified as balanced mesomorph. Negative correlations were observed between fat mass variables and climbing level (p<0.01), and positive correlations with forearm circumference (p<0.05). Mean energy availability (EA) was 33.01 kcal-kg FFM1-d1 (SD: 9.02), with 55.6% of athletes in suboptimal EA status and 35.6% in low energy availability (LEA) status. Carbohydrate and protein intakes were below recommendations in 57.8% and 31.1% of athletes, respectively. There were deficient intakes of all micronutrients except phosphorus in males. These findings suggest that climbing athletes are at high risk of developing low energy availability states and concomitant problems. Optimal nutritional monitoring may be advisable in this type of athlete to try to reduce the risk of LEA.
Keywords:
nutrition assessment
; sport climbing
; bouldering
; rock climbing
; low energy availability
; dietary intake
; relative energy deficiency in sport
1. Introduction
Sport climbing is a relatively young discipline and highly diverse in its practice given the wide variety of environments or permutations of routes, among many others, where categorisation at the individual level is particularly complex [1]. Since the first World Championships held in Germany in 1991, sport climbing has experienced a growing competitive development, even becoming part of the official programme of the Tokyo Summer Olympic Games in 2020 with three disciplines of differential character such as Speed, Lead and Bouldering (the latter two called difficulty disciplines) [2]; becoming a sport with a huge increase in the number of events and practitioners at international level with more than 20 million people around the world being practitioners of some of its disciplines [2,3].
In sport climbing, participants are required to conquer climbing routes, either on natural rock or artificial walls, in real-time competitions, encompassing both indoor and outdoor environments [2]. In lead climbing for example, typical ascent times range from 2-7 minutes and oxygen consumption (VO2) averages around 20-25 ml-kg1-min1 during this period [4]. This activity is characterised by a predominant contribution of the aerobic and alactic anaerobic systems with an important role of the economy of effort. [5].
Despite its competitive nature, the factors that influence climbing performance do not seem to be well understood to date, suggesting that it is a multifactorial sport discipline where performance seems to be influenced by numerous factors [3,6,7,8]. Although trainable variables can also explain the majority of sport climbing performance, the body composition and anthropometric characteristics of the sport climbing athlete can make the difference between victory and defeat when the equality between competitors is at its highest [9,10,11,12].
Climbing athletes, irrespective of gender and climbing level, maintain relatively low body fat levels and weights [9,11]. These anthropometric differences between climbing athletes and the general population [12] may increase the risk of low energy availability (LEA) in this group compared to non-climbers [13,14].
A prolonged state of LEA could cause adverse physiological and psychological outcomes, as well as potential unfavourable effects on the health and athletic performance of these athletes [15], conceptualised in what we know today as the Female Athlete Triad, Male Athlete Triad and Relative Energy Deficiency in Sport (RED-S) models [16]. Recent international consensuses have even gone into the nature of this problem in search of establishing primary, secondary and tertiary prevention plans for RED in athletes [17,18].
Therefore, given the negative influence of nutritional inadequacy on the sporting performance of these athletes, coupled with the specific additional demands of sport climbing athletes during a training and/or competition phase [19]; adequate nutritional control in these athletes could be an additional influencing factor for their sporting performance and make a difference in trying to achieve a successful and satisfying climb [13,20].
However, knowledge about body composition and its relationship with the nutritional status of Spanish climbers is still quite diffuse, despite the potential effects that these aspects could have on the sporting performance and health of these athletes. Therefore, this study sought to evaluate body composition and nutritional status in Spanish climbing athletes.
2. Materials and Methods
2.1. Design
A descriptive, observational and cross-sectional study design was used, where an anthropometric and body composition assessment of the subjects was performed, and dietary diaries were completed [21].
All these tests were conducted in person at the GekoAventura (Valladolid, Spain) and Sputnik Climbing (Las Rozas, Madrid, Spain) climbing walls during a period of time between March 2023 and February 2024.
Participants were recruited during the months of March to 2023 at Sputnik team camps at the Sputnik Climbing centre (Las Rozas, Madrid, Spain) and the GekoAventura climbing gym (Valladolid, Spain), through poster appeals and publications on different social networks informing about the purpose and requirements of the study, while also providing private forms for enrolment in the study. We looked for athletes who practice sport climbing in any modality and conditions, on a regular basis (weekly climbing practice), aged between 16-50 years, with no pathologies or use of drugs that could interfere with the study, and a minimum of 1 years’ experience as inclusion criteria. Pregnant athletes were also excluded from the study.
Data collection was carried out during a single visit per subject, with the subject being shown the corresponding instructions to enable them to complete the dietary records. They were provided with the contact details of two researchers (AMF and AAA) for the submission of the dietary records.
2.2. Ethical Issues
This study complied with the principles of the European Code of Conduct for Research Integrity [22] and followed the steps of the EU General Data Protection Regulation 2016/679 (GDPR) [23]. This was approved by the Ethics Committee of the University of Granada (3340/CEIH/2023).
Prior to the start of the study, all participants and/or their legal guardians were required to complete an informed consent form regarding the use and protection of the data to be included in the study.
2.3. Sport Characteristics
Participants were surveyed according to the recommended standards of the IRCRA (International Rock Climbing Research Association) position statement to improve the comparability of the study [24]. Therefore they answered a series of questions on predominant discipline, percentages of time spent in the last 3/12 months in each discipline and indoor/outdoor climbing, weekly "net" climbing hours in the last 3 and 12 months, years of experience, and participation/presence in national competitions. In addition, the highest consolidated degree of climbing difficulty (wall or surface successfully climbed repeatedly) by each of the participants in the last month was subjectively reported according to the International Rock Climbing Research Association reporting scale (24) to facilitate a common approach to the data.
2.4. Body Composition
Body weight were taken with a Tanita BC-545N electronic scale (Japan). These measurements were taken on an empty stomach, first thing in the morning with the subjects undressed.
For height, a SECA (Germany) wall-mounted tape measuring tape with a range of 220 centimetres and 1 millimetre division was used, as well as an anthropometric box 50 centimetres high and 40 centimetres wide to measure sitting height. Both measurements were taken during the course of an inspiration with the subjects positioned in the Frankfort plane, and the height of the anthropometric box was then subtracted from the seated height. Similarly, the arm span was taken at the end of an inspiration with the subject resting the dactylion point of the right hand on the end (corner) of a wall and marking the dactylion point of the left hand with a marker pen on the wall itself, trying to reach the maximum distance between the two points [25].
The rest of the anthropometric data were taken with a Harpenden plicometer (UK, accuracy 0.2 mm and range 0-80mm) for the measurement of skinfolds (tríceps, subscapular, bíceps, iliac crest, supraspinale, abdominal, thigh, calf), Slide sliding caliper (resolution 1mm and measurement range 1-20cm) for the measurement of bone diameters (humerus, bi-styloid and femur), Cercorf segmometer (Brazil, accuracy 0.5 mm and measuring range 3 m) for hand length measurement (midstylion-dactylion), and a Cescorf tape measure (Brazil, accuracy 1 mm, range 2 m) for girths measurement (arm relaxed, arm flexed, forearm, thigh middle and calf) and parallel to the ground for wingspan.
Anthropometric assessment of body composition was performed using the International Society for the Advancement of Kineanthropometry (ISAK) restricted profile by an ISAK level 2 certified practitioner [25,26]. Two measurements were taken for each measurement, with the mean value reported if the technical error of measurement was <5%. If the technical error of measurement was >5%, a third measurement was taken reporting the median of the 3 values.
The sum of 6 skinfolds (tríceps, subscapular, suprascapular, supraspinale, abdominal, thigh, calf) and 8 skinfolds (tríceps, subscapular, bíceps, iliac crest, supraspinale, abdominal, thigh, calf) were estimated for their application in sports nutrition and association with the individual adiposity index of each athlete [27,28].
Given its applicability and relationship with Dual Energy X-ray Absorptiometry, the Slaughter-Lohman and Poortmans formulas were used to estimate the weight in kilograms of fat mass and muscle mass respectively in participants aged 8-18 years [29], and the Durnin and Womersley (fat mass in kg) and Lee (muscle mass in kg) formulas for the rest of the participants [30,31]. Rocha's formula was used to estimate bone mass for all participants [32].
Fat mass percentage values were calculated using Poortmans and Durnin and Womersley values due to their good agreement with DXA observed in previous studies in sport climbing athletes [30,33].
Once the anthropometric measurements were collected, the different components of the somatotype were calculated from the method of Health and Carter [34] using the following equations previously used in previous work with climbers [35]:
Endomorphy: −0.7182 + 0.1451(x) − 0.00068(x2) + 0.0000014(x3) in which x is the sum of the triceps, subscapular, and supraspinale folds, multiplied by (70.18/height in cm).
Mesomorphy: (0.858 × H) + (0.601 × F) + (0.188 × B) + (0.161 × P) − (0.131 × E) + 4.5, where H is the biepicondilar breadth of the humerus, F is the bicondilar breadth of the femur, B is the flexed arm circumference, P is the perimeter of the calf, and E is height.
Ectomorphy: for this parameter, there are three formulas based on the weight index, which were the result of the formula WI = Height a√Weight
If WI ≥40.75, the formula was 0.732 × WI − 28.58;
If WI <40.75 but >38.25, the formula was 0.463 × WI − 17.63;
If WI ≤38.25, the given value was 0.1.
2.5. Nutritional or Dietary Assessment
Athletes were subjected to prospective measurements (dietary diary) of dietary intake as a gold standard for an adequate nutritional or dietary assessment of the athlete [36].
2.5.1. Dietary Diary and Adjustment to Requirements
Participants were instructed by two expert members of the research team (AM-F and AA-A) to complete a food diary or dietary record. They were asked to record all meals and fluids eaten during 3 days of training, including the time and place of meals eaten, as well as the ingredients, amounts of ingredients and recipes used. Participants were also asked to record whether or not they used any supplements during those days, as well as the format and dosage of the supplements used.
Subsequently, the records were analysed using the nutritional software based on cloud computing technology DietoPro.com [37]. The estimated energy intakes of the athletes were compared with the estimates made in the previous section to calculate energy availability. On the one hand, the macronutrient intakes (carbohydrates, proteins and fats) of the athletes in the sample were compared with the nutritional recommendations proposed by recent review articles for rock climbing athletes, using as reference ranges of 3-7 g CHO/kg per day and an intake of 20-35% of the total energy content from fat [13,14]. Reference protein intakes were adjusted according to the predominant discipline of the athlete, using as reference values of 1.4-2 g/kg BM in boulderers and 1.2-1.8 g/kg BM for other climbing athletes [14]. Moreover, the estimated average intakes of vitamins (thiamine, riboflavin, niacin, folic acid, vitamins B6, B12, C, A, D and E) and minerals (Ca, Fe, P, K, Mg, Zn, I, Se) for each participant were compared with the Dietary Reference Intakes (DRI) for the Spanish population established by the Spanish Federation of Nutrition, Food and Dietetics Societies (FESNAD) in 2010 [38].
2.5.2. Estimation of Energy Availability
To assess the energy availability (EA) of each athlete, exercise energy expenditure (EEE) was calculated from the "net" climbing time (time per week spent climbing surfaces of any type) declared in the sports characteristics questionnaire and its conversion to kilocalories using the metabolic equivalent of the task (MET) corresponding to the values for climbing included in the Compendium of Physical Activities [39,40]. For the calculation of fat-free mass (FFM), the subject's body weight was subtracted from the values obtained for FM from the Slaughter-Lohman and Durnin and Womersley formulae based on the anthropometric analysis of each athlete.
The EA in relation to the fat-free mass of the sample was finally estimated from the values of EEE, energy intake and FFM of each athlete using the following formula [41,42]:
EA=(EI-EEE)/FFM
2.6. Statistical Analysis
Sample size calculation was performed using the G* POWER software (Heinrich-Heine-Universität Düsseldorf, Germany) [45] with an alpha of 0.05, an effect size of 0.70 and a statistical power of 0.95, and to establish statistical differences between conditions a minimum of 46 participants was required.
Statistical analysis was carried out using SPSS Statistics software (version 27, IBM, USA). Means, standard deviations, frequencies and percentages were used for basic description. Normality was calculated using the Shapiro-Wilk test. Homogeneity of variances was estimated using Levene's test. For comparison of independent group distributions, the independent samples t-test was used for normally distributed data. The non-parametric Mann-Whitney test was used when the normality of the distribution was not respected [46,47]. Pearson's correlation coefficient (R) was used to correlate those variables with a normal distribution. Spearman's correlation coefficient was used when the normality of the distribution was not respected. Correlation values (R) were set at <0.2: weak correlation, 0.2-0.8: medium correlation and >0.8: strong correlation [21]. The magnitude of the difference in effect size was obtained with Cohen's d index, which was interpreted as null (0-0.19), small (0.20-0.49), medium (0.50-0.7) and large (≥0.80) [48]. The level of statistical significance for all tests was set at 95%.
3. Results
This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
3.1. Sample Characteristics
The demographic data and sporting characteristics of the participants are shown in Table 1. Forty-six climbers (22 men and 24 women; 7.66 years (SD: 6.63) of experience) from Spain, aged between 17 and 50 years (mean age 30 years (SD: 9)) participated in the present study. According to the IRCRA classification, a total of 14 participants (7 males and 7 females) were classified as intermediate (level 2), 18 (8 males and 10 females) as advanced (level 3), 11 (6 males and 5 females) as elite (level 4), and 3 (1 male and 2 females) as higher elite (level 5), although the latter were integrated inside "elite" athletes´group. Fifty percent reported bouldering as the predominant discipline, while 2.2% and 47.8% reported speed and lead respectively. Of the 46 subjects, 11 (6 males and 5 females) reported current or past participation in state or international championships, while the remaining 35 did not report having participated in any events.
Statistically significant differences with large effect sizes were only observed for weight (p<0.01, d = 2.487, CI = 1.703-3.256), height (p<0.01, d = 2.284, CI = 1.527-3.026) and BMI (p<0.01, d = 1.409, CI = 0.754-2.051) between the two genders.
3.2. Body Composition
The values of the different body composition variables according to the different classifications or climbing levels are shown in Table 2. The somatotype of the male climbers was classified with values typical of an ecto-mesomorphic somatotype (endomorphy: 2.17 (SD:0.90); mesomorphy: 5.95 (SD: 0.77); ectomorphy: 2.81 (SD: 0.84)), while that of the female athletes fell within a balanced mesomorphic somatotype (endomorphy: 2.82 (SD: 0.57); mesomorphy: 4.04 (SD: 0.85); ectomorphy: 3.14 (SD: 0.86)); classifying the total somatotype of the sample as balanced mesomorphic (endomorphy: 2.51 (SD: 0.81); mesomorphy: 4.95 (SD: 1.26); ectomorphy: 2.98 (SD: 0.86)). The mean somatotype values for the different groups of athletes are represented in Figure 1.
Statistically highly significant (p<0.01) medium negative correlations were observed between all variables related to the athlete's body fat and the IRCRA score. Medium correlations between endomorphy (r= -0.589), ∑6 (r= -0.573), ∑8 (r= -0.616), % Fat mass (r= -0.497) and fat mass in kilogrames (r= -0.590) with respect to the athlete's IRCRA score.
Statistically significant (p<0.05) moderate positive correlations were also observed between the IRCRA score of the sample with respect to the values of ectomorphy (r= 0.308) and forearm girth (r= 0.342). No significant correlations were found between the remaining body composition variables and the IRCRA score of the sample.
3.3. Dietary Intake
Despite instructions and insistence given to each participant, one female intermediate athlete (IRCRA scale: 14) did not declare her dietary intake from the 3-day dietary diary, so only the dietary data provided by the remaining 45 athletes are included.
3.3.1. Energy Intake and Energy Availability
The results of the estimated EI and energy expenditure estimates of the participants are shown in Table 3. The mean intake of the sample of climbers was 1803.70 kcal-day1 (SD: 554.18), with a mean EA of 33.01 kcal-kg FFM1-d1 (SD: 9.02). Of the 45 subjects, only 8.9% (13.6% and 4.3% of males and females respectively) had an EA > 45 kcal-kg FFM1-d1. Some 55.6% of the athletes (54.5% and 56.5% of males and females, respectively) had suboptimal EA values of between 30-45 kcal-kg FFM1-d1; while 35.6% (31.8% and 39.1% of males and females, respectively) of the 45 athletes were classified as LEA (<30 kcal-kg FFM1-d1).
Although statistically significant sex differences with a strong effect size were observed in the total daily energy intake (p<0.01, d = 1.747, CI = 1.049-2.430), no statistically significant differences were observed between men and women in the EEE as well as in the energy intake and energy availability of athletes when these values were expressed in relation to fat-free mass.
Statistically significant (p<0.05) medium correlations were also observed between daily energy intake (kcal/day) and the endomorph (r= -0.346) and mesomorph (r= 0.406) somatotypes (Table 6).
3.3.2. Macronutrient Intake
The results of macronutrient intake are shown in Table 3. Regarding CHOs intake, 57.8% of the athletes (50% male and 65.2% female) reported intakes below the minimum value of 3 g-kg BM1 recommended for these athletes, while the remaining 42.2% were within the recommendations of 3-7 g CHOs-kg BM1 per day.
Regarding protein intake, most of the 45 athletes (51.1% of the total, 50% and 52.2% men and women respectively) reported intakes in relation to body mass within the recommended values for each discipline (1.4-2 g-kg BM1 in boulderers and 1.2-1.8 g-kg BM1 for the rest); while 31.1% (22.7% men and 39.1% women) and 17.8% (27.3% men and 8.7% women) presented intakes below and above these recommendations respectively.
In terms of fat intake, no climber reported fat intakes below 20% of total energy intake, with 82.2% of athletes (77.3% male and 87% female) reporting an energy intake from fat intake greater than 35% of total energy intake.
Statistically significant differences were observed between males and females with a strong effect size for total daily intake of carbohydrate (p<0.01, d = 1.245, CI = 0.599-1.880), protein (p<0.01, d = 1.788, CI = 1.085-2.880) and fat (p<0.01; d = 1.485; CI = 0.815-2.141), but no such differences were observed when expressed in relation to the athlete's body mass or as a percentage contribution to total energy intake. Statistically significant gender differences in another parameter were only observed when protein intake was related to athlete body mass (p<0.05).
Moderate significant correlations (p<0.05) were found between carbohydrate intake and the mesomorph component of the athletes (r= 0.371); as well as in the endomorph and mesomorph somatotypes for protein intakes (r= -0.451 and r= 0.380 for endomorph and mesomorph respectively) and fat (r= -0.303 and r= 0.382 for endomorph and mesomorph respectively) (Table 6).
3.3.3. Micronutrient Intake
The results of the intake of the different micronutrients are shown in Table 4 and Table 5. Within the vitamins, the variables with the highest prevalence of subjects with intakes below the Spanish RDA were: vitamin E with 66.7% of the athletes (59.1% of men and 73.9% of women), folic acid with 53.3% (59.1% men and 47.8% women), thiamine with 42.2% (31.8% men and 52.2% women), vitamin D with 42.2% (36.4% men and 47.8% women), riboflavin with 40% (36.4% men and 43.5% women) and vitamin A with 35.6% (40.9% men and 30.4% women). Others such as vitamin B6 (20%), vitamin C (17.8%), niacin (15.6%) and vitamin B12 (6.7%) showed the lowest prevalence values of climbers with deficient vitamin intakes.
On the other hand, regarding mineral intake, of the 45 athletes: 88.9% (81.8% of men and 95.7% of women), 64.4% (40.9% men and 87% women), 57.8% (50% men and 65.2% women), 51.1% (40.9% men and 60.9% women) and 51.1% (27.3% men and 73.9% women) reported intakes of iodine, potassium, calcium, magnesium and selenium respectively, below the recommended daily intakes for the Spanish population. While 48.9% (27.3% men and 69.6% women), 46.7% (9.1% men and 82.6% women) and 44.4% (45.5% men and 43.5% women) of climbers reported deficient intakes of sodium, iron and zinc respectively. Only 13% of female athletes reported phosphorus intakes below the RDA, with 100% of male athletes having adequate intakes of this mineral.
Statistically significant differences were observed in daily intakes of thiamine (p=0.011, d = 0.560, CI = -0.040-1.153), vitamin B6 (p=0.046, d = 0.613, CI = 0.011-1.208), phosphorus (p<0.01, d = 1.273, CI = 0.623-1.910), potassium (p<0.01, η2 = 1.113, CI = 0.478-1.910), magnesium (p=0.013; d = 0.775; CI = 0.163-1.377), iron (p=0.031; d = 0.568; CI = -0.0332-1.162), zinc (p<0.01; d = 0.117; CI = -0.468-0.702), iodine (p=0.011; d = 0.533; CI = -0.065-1.125) and selenium (p<0.01; d = 1.244; CI = 0.597-1.878) between male and female athletes.
Statistically significant correlations (p<0.05) were observed between daily niacin intake and IRCRA score (r= -0.420); endomorphy values and daily intakes of thiamine (r= -0.298), niacin (r= -0.297), phosphorus (r= -0.300), zinc (r= -0.313), iodine (r= -0.410) and selenium (r= -0.348); and between mesomorphy values and intakes of phosphorus (r= 0.321), potassium (r= 0.339), zinc (r= 0.333) and selenium (r= 0.441) (Table 6).

Table 6.
Correlations between dietary variables, somatotype and ability and experience sport´s level.
Table 6.
Correlations between dietary variables, somatotype and ability and experience sport´s level.
| IRCRA score | Experience (years) | Endomorphy | Mesomorphy | Ectomorphy | |
|---|---|---|---|---|---|
| R | R | R | R | R | |
| Energy intake (kcal/day) | 0,90* | 0,033* | -0,346# | 0,406# | 0,018# |
| EA (kcal·kg· FFM−1·d−1) | -0,245* | -0,170* | 0,061# | -0,136# | 0,256# |
| Carbohydrate (g/day) | -0,038* | -0,044* | -0,199* | 0,371* | -0,039* |
| Fat (g/day) | 0,185* | 0,118* | -0,303# | 0,382# | 0,044# |
| Protein (g/day) | 0,236* | -0,021* | -0,451# | 0,380# | 0,090# |
| Thiamin (mg/day) | 0,113* | 0,076* | -0,298* | 0,229* | 0,066* |
| Riboflavin (mg/day) | 0,120* | -0,126* | -0,241* | 0,187* | 0,093* |
| Niacin (mg/day) | 0,420* | 0,124* | -0,297* | 0,027* | 0,189* |
| Vitamin B6 (mg/day) | 0,179* | -0,049* | -0,213# | 0,132# | 0,128# |
| Folic acid (µg/day) | 0,090* | -0,107* | -0,022* | -0,005* | 0,165* |
| Vitamin B12 (µg/day) | 0,058* | -0,064* | -0,141* | 0,206* | -0,027* |
| Vitamin C (mg/day) | -0,041* | -0,198* | 0,041* | -0,045* | 0,093* |
| Vitamin A (µg/day) | 0,023* | 0,067* | 0,161* | -0,112* | 0,015* |
| Vitamin D (µg/day) | 0,042* | -0,026* | 0,107* | 0,127* | -0,133* |
| Vitamin E (mg/day) | 0,093* | 0,183* | -0,087* | 0,167* | 0,075* |
| Calcium (mg/day) | -0,093* | -0,129* | 0,014# | 0,141# | 0,054# |
| Phosphorus (mg/day) | 0,119* | -0,078* | -0,300# | 0,321# | 0,039# |
| Potassium (mg/day) | 0,118* | 0,009* | -0,258* | 0,339* | -0,014* |
| Magnesium (mg/day) | -0,051* | -0,096* | -0,041* | 0,219* | 0,024* |
| Iron (mg/day) | 0,062* | -0,050* | -0,251* | 0,217* | 0,038* |
| Zinc (mg/day) | 0,173* | -0,107* | -0,313* | 0,333* | 0,066* |
| Iodine (µg/day) | 0,207* | 0,076* | -0,410* | 0,185* | 0,182* |
| Selenium (µg/day) | 0,071* | -0,050* | -0,348* | 0,441* | -0,151* |
#Pearson´s R; *Spearman's R; bolding letter: <0,05; bolding and italic letter: <0,01.
3.3.4. Supplement Use
37.8% of participants (40.9% of males and 34.8% of females) reported taking some type of supplement during the study period. The most commonly used supplements were protein powder (n=7) and creatine (n=7). Vitamin B12 supplementation was the third most used supplement by climbers (n=5), followed by vitamin C and vitamin B6 (n=3). Other reported supplements (n≤2) were vitamin D, iron, riboflavin, omega-3, magnesium, essential amino acids, collagen, inositol, caffeine, folic acid, vitamin E, zinc and calcium.
Athletes supplemented with protein (p<0.01, d = 1.183, CI = 0.333-2.020), vitamin D (p=0.018, d = 8.707, CI = 6.369-11.005), riboflavin (p=0.024; d = 2.513; CI = 0.987 -4.014), vitamin B6 (p<0.01; d= 1.688; CI = 0.455 -2.904), vitamin B12 (p<0.01; d = 4,634; CI = 3.273-5.969), iron (p=0.024; d = 2.805; CI = 1.255-4.327) and magnesium (p<=0.024; d = 2.529; CI = 1.001-4.030) showed significantly different intakes of the respective nutrients with strong effect sizes relative to those athletes not taking such supplements.4. Discussion
This is, to date and to the knowledge of this research group, the first study to assess energy availability in Spanish climbing athletes.
Body composition.
In the present study, significant negative correlations stand out in all those parameters linked to the fat component of the athlete in relation to his or her level of ability. These observations are totally coherent with the results of other review works on climbers that show how body fat content tends to decrease when comparing elite climbing athletes with those less advanced [12]. Even authors such as Watts et al. [49] in one of the pioneering international competitions of modern sport climbing previously showed how body fat and body mass values differ in elite sport climbing athletes compared to other athletic groups or controls. Therefore, this tendency to a reduced body fat level in these athletes should not be surprising, and may be associated with other determinants of sport performance in this sport such as finger strength or upper body power, which have not been performed in the present study [10,50,51].
Regarding the fat percentage of the athletes, other authors observed different %FM values in climbing athletes such as figures of 12.3% (SD: 3.2) in Chilean male athletes of different levels [33]; as well as values of 13.60% (SD: 8.0) and 9.16% (SD: 3.0) for female and male elite climbers respectively, and 21.77% (SD: 0.9) and 10.7% (SD: 4.0) for female and male recreational climbers respectively [35]. The values shown by the athletes in the present study are somewhat higher than those reflected by these authors in Chilean and Spanish athletes respectively, with mean values of 14.06% (SD: 4.29) and 22.01% (SD: 3.29) for male and female athletes in this sample. These data are somewhat more similar to those expressed by Gibson-Smith et al. [21] in English athletes, with lower fat content and 8-skinfolds sum in men, but higher in women than the values obtained in the present study. It should be noted that the percentage values interpreted above were calculated using the Durnin and Womersley formula, an aspect that should be considered with caution when comparing these values with others obtained in a different way.
It may be prudent to further consider the Durnin and Womersley equation for %FM when DXA is not available [33].
The athletes of this study show a mesomorphic component greater than those obtained by Novoa-Virgnau et al. [35]. Also, it is observed how despite presenting very similar mean values of endomorphy and ectomorphy in both men and women, elite athletes show lower mean values of mesomorphy than those in the present study. However, as highlighted above, it is the endomorphic component that seems to show a significant influence on sport climbing success, while the other anthropometric components may not have a clear influence in determining success in this type of sporting discipline [52].
Finally, previous studies have similarly shown that higher climbing skills are associated with larger forearm girth [53]. Given the link of this anthropometric variable with maximal grip strength [54] and the interest in the sport climbing athlete in improved strength and recovery of the finger flexor muscles (53), the present study again highlights the importance of considering forearm girth in determining athletic performance in the sport of climbing [55].
Energy intake.
The values of EA are somewhat higher than those observed in previous studies in climbers [42,56], but still reflect worrying data on the prevalence of sport climbing athletes in suboptimal EA and LEA status. In contrast to the work of Simič et al. [56], where no athlete reached the target values of 45 kcal-kg FFM1-d1, in the present study only 8.9% of athletes reached these target values; while athletes in the LEA range showed mean values intermediate between those obtained in Irish [44] and Slovenian [56] athletes. Nevertheless, it would be important to test these data cautiously considering the possible limitations derived from the application of tools such as metabolic equivalents (METs) when estimating the energy availability of athletes [57].
In relation to energy intake, the values obtained are curiously similar to the intakes reported in previous studies for male climbers (37.2 kcal-kg FFM1-d1 (SD: 9.0)), although with notably lower intakes in female athletes (45.6 7.0 kcal-kg FFM1-d1 (SD: 7.0)) [21]. Even, the mean values of the sample (36.82 kcal-kg FFM1-d1 (SD: 8.44)) are similar to the mean intakes of Scottish climbing athletes [58]; with mean daily intakes similar to those observed by Chmielewska et al. [42] in Polish climbers, although somewhat lower than those observed by Monedero et al. [44] in Irish athletes.
This again highlights the concern of a deficient energy status in sport climbing athletes [13], especially because of its effects on the athletes' health status and sport performance [59]. Analysing the energy intake of these athletes and its link to variables related to health and performance of these athletes could be of interest.
Macronutrient intake.
In line with much of the available literature on sport climbing athletes [44,56,58], the majority of the athletes in the present study show a deficient carbohydrate intake with respect to the specific recommendations for the sport of climbing. Furthermore, the average carbohydrate intake of the Spanish athletes included in the study is clearly lower than the values previously referenced in previous studies on climbers, despite also showing intakes below the recommendations [21,42,44,56,58,60]. Deficient carbohydrate intakes could lead to a reduction in body glycogen levels and accelerate the onset of fatigue and the deterioration of sports performance in these athletes [61,62].
Similarly, and in accordance with much of the literature [21,44,56,60], fat intake in relation to total energy intake was shown to be above the recommendations of 35% in a large proportion of the climbing athletes in the present study. Considering also the effects of low-carbohydrate and high-fat diets on exercise economy [63] and the importance of this factor in the performance of climbing athletes [5], it would seem an interesting feat to try to seek increases in caloric intake from an increase in carbohydrate intake in this population group, especially in those climbers who perform outdoor climbing in prolonged or successive sessions where lactate levels may be increased [64].
In relation to protein intake, the intakes reported by Spanish climbers do not differ greatly from the values reflected in other studies with climbers [21,44,58], although Simič et al. [56] and Chmielewska et al. [42] showed protein intakes in relation to BM lower than these findings. Nevertheless, considering the deficient energy intakes, the prevalence of athletes below protein recommendations and the high frequency of isometric contractions performed during climbing [13,65], it may be prudent to monitor the intake of this macronutrient in climbing athletes for the adequacy of body mass and grip strength [66,67].
Micronutrient intake.
A large proportion of the athletes in the present study showed deficient intakes of most of the vitamins and minerals evaluated. As in previous studies, Spanish athletes showed intakes below the recommendations for iron, calcium, magnesium, potassium, zinc, iodine and vitamins D, E, B1, B3, B6, B12 and C [21,42,44,56,60]. However, these data should be interpreted with caution, given the need for longer dietary recording time in order to estimate individual intake more accurately [68,69]. Similarly, the use of population-based reference values such as RDAs may favour the inference of possible nutritional deficiencies and aggravate the magnitude of the findings [70].
Nevertheless, these data underscore the need for continuous and more prolonged monitoring of the intake of different micronutrients to advocate for adequate intake of vitamins and minerals to ensure proper physiological functions. Biochemical testing could also be a useful tool to understand the nutritional status of different micronutrients in these at-risk population groups, especially considering those groups at higher risk and micronutrients that may compromise athletic performance in these sports disciplines such as iron, vitamin D, calcium, B vitamins, magnesium and zinc [13,14]. Even complementing an assessment of body composition with a biochemical analysis of those micronutrients in which it may be interrelated can be an interesting aspect during the nutritional monitoring process of these athletes [71].
Therefore, these aspects may be especially relevant in climbing athletes, where low energy intake and inadequate intake of macronutrients may be predisposing factors for different micronutrient deficiencies [59,72].
Supplement use.
37.8% of the athletes reported using one or more supplements, somewhat lower than previously reported supplement use in climbing athletes [73]. Similar to previous observations in Polish [42] and English [21] climbing athletes, protein powder supplements were the most commonly used by athletes in the present study. Similarly, the use of supplements such as different vitamins (vitamin C, D), minerals (calcium, iron, magnesium), amino acid mixtures, collagen, omega 3, caffeine or creatine, previously reported in work with climbers [21,42,74,75], was also reported.
However, although several supplements could be beneficial due to their mechanism of action and the nature of the sport of sport climbing, it can be deduced that climbing athletes do not show dietary habits in accordance with their sport. Therefore, improving the nutritional status of climbers by adapting dietary habits to the specific requirements of their sporting discipline could be the priority nutritional strategy as opposed to the indiscriminate use of dietary supplements, as is the case in other Olympic disciplines [76,77,78]. However, in situations of diagnosed deficiencies, athletes following restrictive dietary patterns or where there is a potential effect on the athlete's sporting performance, the safe, effective and necessary use of certain nutritional supplements may be of interest [20,73,79,80,81,82].
Limitations.
To the knowledge of the present research group, this is one of the first studies to establish a relationship between nutritional intakes and energy availability in sport climbing athletes with their respective anthropometric and body variables. These findings may encourage the development of future research that considers the implications of nutrition on sport performance and health in this population group. In addition, the inclusion in the present study of previously validated nutritional and body assessment methods facilitates the comparability of the results with those obtained in external research.
However, this study is not without limitations.
The main limiting factor of the present study is the bias arising from the use of self-reported tools, questionnaires or records, and there may be a risk of underestimation of the intakes and counts obtained [83]. Also, the short duration of dietary diaries may be a limiting aspect in accurately estimating nutritional intakes at the individual level, especially of micronutrients [68,69]. Biochemical assessment of sport climbing athletes could be an interesting addition to future research.
Finally, the variability and method-specific biases present in measurement techniques such as anthropometry could be an added bias when analysing and interpreting the different data obtained [84,85]. The use of validated reference methods may be advisable for body composition assessments in climbing athletes in future studies.
4. Conclusions
Climbing athletes of different skill levels are at risk of developing low energy availability and related problems due to inadequate nutritional and energy intake in relation to the demands of the sport discipline.
A tendency towards a reduced endotraining component could be an added risk factor in these athletes for the development of deficient energy states resulting from limited carbohydrate intakes.
Future research should delve deeper into the bio-health and performance consequences to which this type of nutritional deficiency may predispose this population. Adequate nutritional monitoring and assessment by qualified professionals are recommended in this group of athletes, as well as the application of guidelines or practical tools that encourage a higher energy intake in those athletes most at risk.
Author Contributions
The study was designed by AM-F, JC-P and MM-A; data were collected and analysed by AM-F, AA-A, AT-I and JC-P; data interpretation and manuscript preparation were undertaken by AM-F, JC-P, JA-L and MM-A. All authors reviewed and approved the final manuscript.
Funding
The funding sponsors had no role in the design of the study, in the collection, analyses, or interpretation of the data; in the writing of the manuscript, or in the decision to publish the results. This study was funded by the High Council for Sports (CSD), Spanish Ministry of Culture and Sport, through the NESA NETWORK “Spanish Network of Sports Care at Altitude (RADA)” Ref. 19/UPB/23. This work was carried out thanks to the support of the University of Granada (Own Research Plan—P. 10) for research stays granted to MM-A at the University of Murcia under the responsibility and supervision of JA-L.
Informed Consent Statement
All of these volunteers signed their informed consent to participation in the study, which was approved by the Ethics Committee of the University of Granada (3340/CEIH/2023).
Data Availability Statement
There are restrictions on the availability of data for this trial, due to the signed consent agreements around data sharing, which only allow access to external re-searchers for studies following the project’s purposes. Requestors wishing to access the trial data used in this study can make a request to mariscal@ugr.es.
Acknowledgments
The authors thank Geko Aventura Climbing Center and Sputnik Research Proyect for their support. This paper will be part of Agustin Mora-Fernandez's doctoral thesis. Being completed as part of the “Nutrition and Food Sciences Program” at the University of Granada. Spain.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Jones G, Schöffl V, Johnson MI. Incidence, Diagnosis, and Management of Injury in Sport Climbing and Bouldering: A Critical Review. Current Sports Medicine Reports. 2018 Nov;17(11):396.
- Batuev M, Robinson L. Organizational evolution and the Olympic Games: the case of sport climbing. Sport in Society. 2019 Oct 3;22(10):1674–90.
- Sanchez X, Torregrossa M, Woodman T, Jones G, Llewellyn DJ. Identification of Parameters That Predict Sport Climbing Performance. Frontiers in Psychology. 2019;10. Available from: https://www.frontiersin.org/articles/10.3389/fpsyg.2019.01294.
- Watts, PB. Physiology of difficult rock climbing. Eur J Appl Physiol. 2004 Apr 1;91(4):361–72.
- Bertuzzi RC de M, Franchini E, Kokubun E, Kiss MAPDM. Energy system contributions in indoor rock climbing. Eur J Appl Physiol. 2007 Oct 1;101(3):293–300.
- España-Romero V, Ortega Porcel FB, Artero EG, Jiménez-Pavón D, Gutiérrez Sainz Á, Castillo Garzón MJ, et al. Climbing time to exhaustion is a determinant of climbing performance in high-level sport climbers. Eur J Appl Physiol. 2009 Nov 1;107(5):517–25.
- Wall CB, Starek JE, Fleck SJ, Byrnes WC. Prediction of indoor climbing performance in women rock climbers. The Journal of Strength & Conditioning Research. 2004 Feb;18(1):77.
- Sanchez X, Boschker MSJ, Llewellyn DJ. Pre-performance psychological states and performance in an elite climbing competition. Scandinavian Journal of Medicine & Science in Sports. 2010;20(2):356–63.
- Mermier CM, Janot JM, Parker DL, Swan JG. Physiological and anthropometric determinants of sport climbing performance. British Journal of Sports Medicine. 2000 Oct 1;34(5):359–65.
- Giles D, Barnes K, Taylor N, Chidley C, Chidley J, Mitchell J, et al. Anthropometry and performance characteristics of recreational advanced to elite female rock climbers. Journal of Sports Sciences. 2021 Jan 2;39(1):48–56.
- Laffaye G, Levernier G, Collin JM. Determinant factors in climbing ability: Influence of strength, anthropometry, and neuromuscular fatigue. Scandinavian Journal of Medicine & Science in Sports. 2016;26(10):1151–9.
- Ginszt M, Saito M, Zięba E, Majcher P, Kikuchi N. Body Composition, Anthropometric Parameters, and Strength-Endurance Characteristics of Sport Climbers: A Systematic Review. The Journal of Strength & Conditioning Research. 2023 Jun;37(6):1339.
- Michael MK, Witard OC, Joubert L. Physiological demands and nutritional considerations for Olympic-style competitive rock climbing. Taiar R, editor. Cogent Medicine. 2019 Jan 1;6(1):1667199.
- Leslie-Wujastyk M, Gibson-Smith E. Nutritional Considerations for Female Rock Climbers. J of SCI IN SPORT AND EXERCISE. 2024 Jan 29. Available from. [CrossRef]
- Logue DM, Madigan SM, Melin A, Delahunt E, Heinen M, Donnell SJM, et al. Low Energy Availability in Athletes 2020: An Updated Narrative Review of Prevalence, Risk, Within-Day Energy Balance, Knowledge, and Impact on Sports Performance. Nutrients. 2020 Mar;12(3):835.
- De Souza MJ, Strock NCA, Ricker EA, Koltun KJ, Barrack M, Joy E, et al. The Path Towards Progress: A Critical Review to Advance the Science of the Female and Male Athlete Triad and Relative Energy Deficiency in Sport. Sports Med. 2022 Jan 1;52(1):13–23.
- Burke LM, Ackerman KE, Heikura IA, Hackney AC, Stellingwerff T. Mapping the complexities of Relative Energy Deficiency in Sport (REDs): development of a physiological model by a subgroup of the International Olympic Committee (IOC) Consensus on REDs. Br J Sports Med. 2023 Sep 1;57(17):1098–108.
- Torstveit MK, Ackerman KE, Constantini N, Holtzman B, Koehler K, Mountjoy ML, et al. Primary, secondary and tertiary prevention of Relative Energy Deficiency in Sport (REDs): a narrative review by a subgroup of the IOC consensus on REDs. Br J Sports Med. 2023 Sep 1;57(17):1119–26.
- Callender NA, Hayes TN, Labrador NB. Cardiorespiratory demands of competitive rock climbing. Appl Physiol Nutr Metab. 2021 Feb;46(2):161–8.
- Beck KL, von Hurst PR, O’Brien WJ, Badenhorst CE. Micronutrients and athletic performance: A review. Food and Chemical Toxicology. 2021 Dec 1;158:112618.
- Gibson-Smith E, Storey R, Ranchordas M. Dietary Intake, Body Composition and Iron Status in Experienced and Elite Climbers. Frontiers in Nutrition. 2020;7. Available from: https://www.frontiersin.org/articles/10.3389/fnut.2020.00122.
- ALL European Academies. The European Code of Conduct for Research Integrity. 2022.
- Reglamento (UE) 2016/679 del Parlamento Europeo y del Consejo, de 27 de abril de 2016, relativo a la protección de las personas físicas en lo que respecta al tratamiento de datos personales y a la libre circulación de estos datos y por el que se deroga la Directiva 95/46/CE. OJ L Apr 27, 2016. Available from: http://data.europa.eu/eli/reg/2016/679/oj/spa.
- Draper N, Giles D, Schöffl V, Konstantin Fuss F, Watts P, Wolf P, et al. Comparative grading scales, statistical analyses, climber descriptors and ability grouping: International Rock Climbing Research Association position statement. Sports Technology. 2015 Oct 2;8(3–4):88–94.
- Norton K, Eston R. Kinanthropometry and Exercise Physiology. Routledge; 2018. 579 p.
- Norton KI. Estándares para la evaluación de la antropometría. In: Kinantropometría y fisiología del ejercicio. Available from: https://www.taylorfrancis.com/chapters/edit/10.4324/9781315385662-4/standards-anthropometry-assessment-kevin-norton.
- Cabañas M, Esparza F. Compendio de cineantropometría. Madrid: CTO. 2009;2:496 p.
- Lohman, TG. Skinfolds and Body Density and Their Relation to Body Fatness: A Review. Human Biology. 1981;53(2):181–225.
- Curilem Gatica, C. Evaluación de la composición corporal en niños y adolescentes: directrices y recomendaciones. Nutr Hosp. 2016 Jun 30;33(3). Available from: http://revista.nutricionhospitalaria.net/index.php/nh/article/view/285 30.
- Silveira EA, Barbosa LS, Rodrigues APS, Noll M, De Oliveira C. Body fat percentage assessment by skinfold equation, bioimpedance and densitometry in older adults. Archives of Public Health. 2020 Jul 18;78(1):65.
- González-Mendoza RG, Gaytán-González A, Jiménez-Alvarado JA, Villegas-Balcázar M, Jáuregui-Ulloa EE, Torres-Naranjo F, et al. Accuracy of Anthropometric Equations to Estimate DXA-Derived Skeletal Muscle Mass in Professional Male Soccer Players. Journal of Sports Medicine. 2019 Jan 1;2019:e4387636.
- Torres-Unda J, Zarrazquin I, Gil J, Ruiz F, Irazusta A, Kortajarena M, et al. Anthropometric, physiological and maturational characteristics in selected elite and non-elite male adolescent basketball players. J Sports Sci. 2013;31(2):196–203. Available from. [CrossRef]
- Téllez MJA, Carrasco F, Romero VE, Inostroza J, Bustamante A, Altamirano IS. A comparison of body composition assessment methods in climbers: Which is better? PLOS ONE. 2019 Nov 20;14(11):e0224291.
- Carter JEL. The heath-carter anthropometric somatotype. CD-Rom. 2002.
- Novoa-Vignau MF, Salas-Fraire O, Salas-Longoria K, Hernández-Suárez G, Menchaca-Pérez M. A comparison of anthropometric characteristics and somatotypes in a group of elite climbers, recreational climbers and non-climbers. Medicina Universitaria. 2017 Apr 1;19(75):69–73.
- Burke, LM. Dietary assessment methods for the athlete: pros and cons of different methods. 2015;28(150).
- Sebastià, N. Dietopro.com: una nueva herramienta de gestión dietoterapéutica. Nutrición Hospitalaria. 2014 Sep 1;(3):678–85.
- Federación Española de Sociedades de Nutrición A y D (FESNAD). Ingestas dietéticas de referencia (IDR) para la población española. Act Diet. 2010;14:196–7.
- Ainsworth BE, Haskell WL, Herrmann SD, Meckes N, Bassett Jr DR, Tudor-Locke C, et al. 2011 Compendium of Physical Activities: a second update of codes and MET values. Medicine & science in sports & exercise. 2011;43(8):1575–81.
- Ainsworth B, Whitt-Glover M, IRWIN M, Swartz A, Strath S, O’BRIEN W, et al. Compendium of Physical Activities: an Update of Activity Codes and MET Intensities. Medicine and science in sports and exercise. 2000 Oct 1;32:S498-504.
- Loucks, AB. Energy Balance and Energy Availability. In: The Encyclopaedia of Sports Medicine. John Wiley & Sons, Ltd; 2013; p. 72–87. Available from: https://onlinelibrary.wiley.com/doi/abs/10.1002/9781118692318.ch5.
- Chmielewska A, Regulska-Ilow B. The Evaluation of Energy Availability and Dietary Nutrient Intake of Sport Climbers at Different Climbing Levels. International Journal of Environmental Research and Public Health. 2023 Jan;20(6):5176.
- Melin AK, Heikura IA, Tenforde A, Mountjoy M. Energy Availability in Athletics: Health, Performance, and Physique. International Journal of Sport Nutrition and Exercise Metabolism. 2019 Mar 1;29(2):152–64.
- Monedero J, Duff C, Egan B. Dietary Intakes and the Risk of Low Energy Availability in Male and Female Advanced and Elite Rock Climbers. The Journal of Strength & Conditioning Research. 2023 Mar;37(3):e8.
- Faul F, Erdfelder E, Lang AG, Buchnr A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods. 2007;39:175–91.
- MacFarland TW, Yates JM. Mann–Whitney U test. Introduction to Nonparametric Statistics for the Biological Sciences Using R. Cham: Springer International Publishing. 2016;103–32. Available from: https://link.springer.com/chapter/10.1007/978-3-319-30634-6_4.
- Sainani, KL. Dealing with non-normal data. Pm&r. 2012;4(12):1001-1005.
- Cohen, J. Methods in psychology. A power primer. Psychological Bulletin. 1992;112(1):155–9.
- Watts PB, Martin DT, Durtschi S. Anthropometric profiles of elite male and female competitive sport rock climbers. Journal of Sports Sciences. 1993 Apr 1;11(2):113–7.
- Saul D, Steinmetz G, Lehmann W, Schilling AF. Determinants for success in climbing: A systematic review. Journal of Exercise Science & Fitness. 2019 Sep 1;17(3):91–100.
- Grant S, Hasler T, Davies C, Aitchison TC, Wilson J, Whittaker A. A comparison of the anthropometric, strength, endurance and flexibility characteristics of female elite and recreational climbers and non-climbers. Journal of Sports Sciences. 2001 Jan 1;19(7):499–505.
- Puletic M, Stankovic D. The influence of somatotype components on success in sport climbing. Facta Universitatis, Series: Physical Education and Sport. 2014 Oct 16;(0):105–11.
- Son S, Seo Y, Son J, Yun S, Lee DT. Comparison of finger flexion strength and muscular recovery of male lead sport climbers across climbing classes. Physical Therapy in Sport. 2024 Jan 1;65:122–9.
- Anakwe R, Huntley J, Mceachan J. Grip Strength and Forearm Circumference in a Healthy Population. J Hand Surg Eur Vol. 2007 Apr 1;32(2):203–9.
- Arazi H, Rashidlamir A, Abolhasani MZ, Hosaini SA. Profiling and predicting performance of indoor rock climbers. Rev bras cineantropom desempenho hum. 2018 Feb;20:82–94.
- Simič V, Jevšnik Š, Mohorko N. Low energy availability and carbohydrate intake in competitive adolescent sport climbers. Kinesiology. 2022 Dec 31;54(2):268–77.
- Byrne NM, Hills AP, Hunter GR, Weinsier RL, Schutz Y. Metabolic equivalent: one size does not fit all. Journal of Applied Physiology. 2005 Sep;99(3):1112–9.
- Michael MK, Joubert L, Witard OC. Assessment of Dietary Intake and Eating Attitudes in Recreational and Competitive Adolescent Rock Climbers: A Pilot Study. Frontiers in Nutrition. 2019;6. Available from: https://www.frontiersin.org/articles/10.3389/fnut.2019.00064.
- Mathisen TF, Ackland T, Burke LM, Constantini N, Haudum J, Macnaughton LS, et al. Best practice recommendations for body composition considerations in sport to reduce health and performance risks: a critical review, original survey and expert opinion by a subgroup of the IOC consensus on Relative Energy Deficiency in Sport (REDs). Br J Sports Med. 2023 Sep 1;57(17):1148–60.
- Úbeda Martín N, Carvacho CL, García González Á. Energy and nutritional inadequacies in a group of recreational adult Spanish climbers. Archivos de medicina del deporte: revista de la Federación Española de Medicina del Deporte y de la Confederación Iberoamericana de Medicina del Deporte. 2021;38(204 (Julio / Agosto)):237–44.
- Widrick JJ, Costill DL, Fink WJ, Hickey MS, McConell GK, Tanaka H. Carbohydrate feedings and exercise performance: effect of initial muscle glycogen concentration. Journal of Applied Physiology. 1993 Jun;74(6):2998–3005.
- Hawley JA, Schabort EJ, Noakes TD, Dennis SC. Carbohydrate-Loading and Exercise Performance. Sports Med. 1997 Aug 1;24(2):73–81.
- Burke LM, Ross ML, Garvican-Lewis LA, Welvaert M, Heikura IA, Forbes SG, et al. Low carbohydrate, high fat diet impairs exercise economy and negates the performance benefit from intensified training in elite race walkers. The Journal of Physiology. 2017;595(9):2785–807.
- Booth J, Marino F, Hill C, Gwinn T. Energy cost of sport rock climbing in elite performers. British Journal of Sports Medicine. 1999 Feb 1;33(1):14–8.
- Burd NA, Tang JE, Moore DR, Phillips SM. Exercise training and protein metabolism: influences of contraction, protein intake, and sex-based differences. Journal of Applied Physiology. 2009 May;106(5):1692–701.
- Nunes EA, Colenso-Semple L, McKellar SR, Yau T, Ali MU, Fitzpatrick-Lewis D, et al. Systematic review and meta-analysis of protein intake to support muscle mass and function in healthy adults. Journal of Cachexia, Sarcopenia and Muscle. 2022;13(2):795–810.
- Lemon PWR, Proctor DN. Protein Intake and Athletic Performance. Sports Medicine. 1991 Nov 1;12(5):313–25.
- Larson-Meyer DE, Woolf K, Burke L. Assessment of nutrient status in athletes and the need for supplementation. Int J Sport Nutr Exerc Metab. 2018;28(2):139–58. Available from: https://journals.humankinetics.com/view/journals/ijsnem/28/2/article-p139.xml.
- Basiotis PP, Welsh SO, Cronin FJ, Kelsay JL, Mertz W. Number of days of food intake records required to estimate individual and group nutrient intakes with defined confidence. J Nutr. 1987;117(9):1638–41. Available from: http://academic.oup.com/jn/article-pdf/117/9/1638/23998106/jn1170091638.pdf.
- Devaney BL, Barr SI. DRI, EAR, RDA, AI, UL: Making sense of this alphabet soup. Nutr Today. 2002;37(6):226. Available from: https://journals.lww.com/nutritiontodayonline/fulltext/2002/11000/dri,_ear,_rda,_ai,_ul__making_sense_of_this.3.aspx?casa_token=Y89Y2-oAY8oAAAAA:sEK88-YU9934yRD44ibOSTc_qJDYs9Y7_mn2Fo6V5VQ0cXDmJr9s0W5JR0-pSqRccR9-1Mttn2tC13WZEi7XBNTi3wC4s9FF-u28ig&casa_token=hQ5BAnR0EakAAAAA:5Os56XMR_CqVKdRiKitaGmCRkQ8OVsiliFRbjF1XDqkG9-VcrMrQiMrVXwog-HWJIk3snNM5N8lvaAS57WGDYSwn7S6X4Bnn4BGi3g.
- Mora-Fernandez A, Rojas JP, Gimenez-Blasi N, Conde-Pipó J, Latorre JA, Mariscal-Arcas M. Relationship of vitamin D status with biomarkers of muscle damage and body composition in Spanish elite female football players: A cross-sectional study. Appl Sci (Basel). 2024;14(14):6349. Available from: https://www.mdpi.com/2076-3417/14/14/6349.
- Jordan SL, Albracht-Schulte K, Robert-McComb JJ. Micronutrient deficiency in athletes and inefficiency of supplementation: Is low energy availability a culprit? PharmaNutrition. 2020 Dec 1;14:100229.
- Okoren L, Magkos F. Physiological Characteristics, Dietary Intake, and Supplement Use in Sport Climbing. Curr Nutr Rep. 2023 Dec 1;12(4):788–96.
- People G, Parker, Anthony R, Craddock J. Rock climbers’ self-reported dietary practices and supplement use in the context of supporting climbing performance. JSES. 2021;5(2). Available from: https://protect-eu.mimecast.com/s/iE5nCzBp2uM1XrLi4OjJyi?domain=jses.net.
- Sas-Nowosielski K, Wycislik J. Energy and macronutrient intake of advanced Polish sport climbers. Journal of Physical Education and Sport. 2019;19(Suppl. 3):829–32.
- Mora-Fernandez A, Lopez-Moro A, Chirosa-Rios LJ, Mariscal-Arcas M. A systematic review of the effects of nutrient intake in handball players on exercise performance. Appl Sci (Basel). 2022;12(23):12378. Available from: https://www.mdpi.com/2076-3417/12/23/12378.
- Jiménez-Casquet MJ, Conde-Pipó J, Valenzuela-Barranco I, Rienda-Contreras R, Olea-Serrano F, Bouzas C, et al. Nutrition status of female winter sports athletes. Nutrients. 2023;15(20):4472. Available from: https://www.mdpi.com/2072-6643/15/20/4472.
- Jiménez-Casquet MJ, Conde-Pipo J, Valenzuela-Barranco I, Rienda-Contreras R, Olea-Serrano F, Monserrat-Mesquida M, et al. Cross-sectional study of the anthropometric profile and nutrient status of elite female ice hockey players: Differences by play position. Nutrients. 2024;16(4):471. Available from: https://www.mdpi.com/2072-6643/16/4/471.
- Celorrio San Miguel AM, Roche E, Herranz-López M, Celorrio San Miguel M, Mielgo-Ayuso J, Fernández-Lázaro D. Impact of melatonin supplementation on Sports Performance and circulating biomarkers in Highly Trained Athletes: A systematic review of randomized controlled trials. Nutrients. 2024;16(7):1011. Available from: https://www.mdpi.com/2072-6643/16/7/1011.
- Kostrakiewicz-Gierałt, K.Plant-based proteins, peptides and amino acids in food products dedicated for sportspeople—A narrative review of the literature. Nutrients. 2024;16(11):1706. Available from: https://www.mdpi.com/2072-6643/16/11/1706.
- Fernández-Lázaro D, Arribalzaga S, Gutiérrez-Abejón E, Azarbayjani MA, Mielgo-Ayuso J, Roche E. Omega-3 fatty acid supplementation on post-exercise inflammation, muscle damage, oxidative response, and sports performance in physically healthy adults—A systematic review of randomized controlled trials. Nutrients. 2024;16(13):2044. Available from: https://www.mdpi.com/2072-6643/16/13/2044.
- Macuh M, Kojić N, Knap B. The effects of nitrate supplementation on performance as a function of habitual dietary intake of nitrates: A randomized controlled trial of elite football players. Nutrients. 2023;15(17):3721. Available from: https://www.mdpi.com/2072-6643/15/17/3721.
- Bingham, SA. Limitations of the Various Methods for Collecting Dietary Intake Data. Annals of Nutrition and Metabolism. 2008 Nov 19;35(3):117–27.
- Gorstein J, Sullivan K, Yip R, de Onís M, Trowbridge F, Fajans P, et al. Issues in the assessment of nutritional status using anthropometry. Bull World Health Organ. 1994;72(2):273–83.
- Mulasi U, Kuchnia AJ, Cole AJ, Earthman CP. Bioimpedance at the Bedside: Current Applications, Limitations, and Opportunities. Nut in Clin Prac. 2015 Apr;30(2):180–93.
Figure 1.
Mean somatotype values for the different groups of athletes.
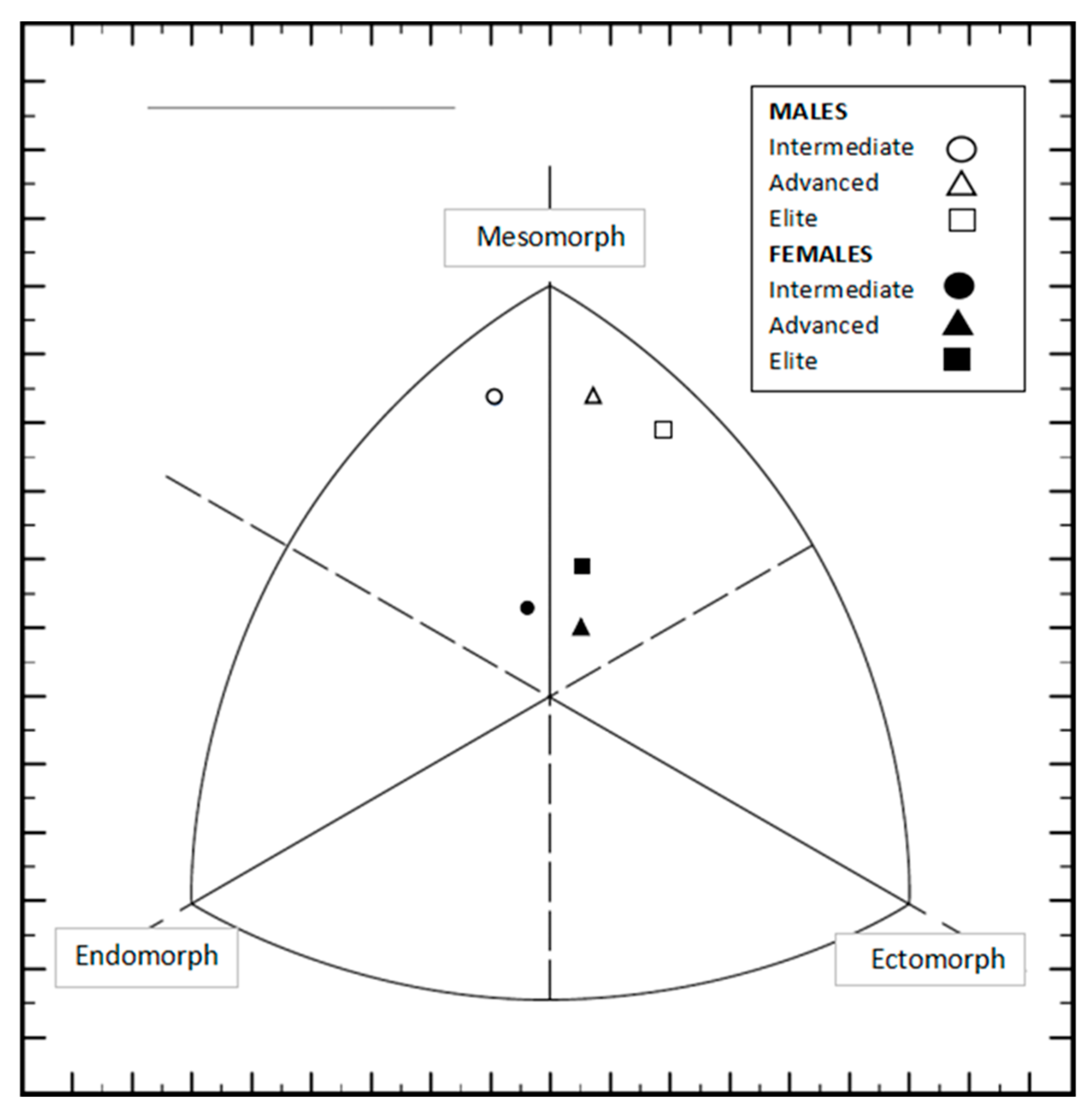
Table 1.
Demographic and sporting characteristics of participants.
| Total (n=46) | Males (n=22) | Females (n=24) |
P ♂ vs ♀ |
Effect Size** | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | d | IC (95%) | |||
| Age (years) | 30 | 9 | 32 | 10 | 28 | 8 | 0,190# | 0,393 | (-0,194 - 0,975) | |
| Weight (kg) | 59,56 | 10,12 | 67,78 | 7,77 | 52,03 | 4,65 | <0,01* | 2,487 | (1,703 - 3,256) | |
| Height (cm) | 167,73 | 8,62 | 174,49 | 6,89 | 161,53 | 4,27 | <0,01# | 2,284 | (1,527- 3,026) | |
| BMI (kg/m^2) | 21,02 | 1,96 | 22,20 | 1,71 | 19,93 | 1,52 | <0,01# | 1,409 | (0,754 – 2,051) | |
| IRCRA score | 19,07 | 4,72 | 20,00 | 4,61 | 18,21 | 4,75 | 0,189* | 0,383 | (-0,203 – 0,965) | |
| Experience (years) | 7,66 | 6,63 | 8,57 | 7,17 | 6,83 | 6,13 | 0,460* | 0,261 | (-0,321 – 0,841) | |
| Volume of climbing per week (hours) | 2,71 | 1,69 | 2,70 | 1,73 | 2,73 | 1,70 | 0,921* | -0,018 | (-0,596 – 0,561) | |
| Time spent climbing in the last 3 months (%) | Boulder | 53,91 | 28,26 | 55,68 | 30,37 | 52,29 | 26,74 | 0,689# | 0,119 | (-0,461 – 0,697) |
| Speed | 1,54 | 10,32 | 3,18 | 14,92 | 0,04 | 0,20 | 0,926* | 0,305 | (-0,279 – 0,885) | |
| Lead | 44,54 | 28,29 | 41,14 | 30,12 | 47,67 | 26,77 | 0,440# | -0,230 | (-0,809 – 0,352) | |
| Time spent climbing in the last 12 months (%) | Boulder | 53,80 | 25,41 | 53,64 | 30,01 | 53,96 | 21,01 | 0,966# | -0,013 | (-0,591 – 0,566) |
| Speed | 0,89 | 5,90 | 1,82 | 8,53 | 0,04 | 0,20 | 0,926* | 0,301 | (-0,282 – 0,882) | |
| Lead | 42,48 | 24,57 | 40,00 | 28,45 | 44,75 | 20,75 | 0,519# | -0,192 | (-0,771 – 0,389) | |
| Time spent climbing in the last 3 months (%) | Inside | 71,52 | 23,71 | 74,09 | 21,02 | 69,17 | 26,15 | 0,594* | 0,207 | (-0,375 – 0,785) |
| Outside | 28,48 | 23,71 | 25,91 | 21,02 | 30,83 | 26,15 | 0,594* | -0,207 | (-0,785 – 0,375) | |
| Time spent climbing in the last 12 months (%) | Inside | 67,61 | 23,45 | 66,36 | 24,36 | 68,75 | 23,04 | 0,894* | -0,101 | (-0,679 – 0,479) |
| Outside | 30,22 | 21,60 | 29,09 | 20,39 | 31,25 | 23,04 | 0,722* | -0,099 | (-0,677 – 0,480) | |
SD: Standard Deviation; *Mann–Whitney U test; **Cohen’s d index; # independent samples t-test.
Table 2.
Variables related to body composition and correlations with IRCRA scale.
| Males (n=22) | Females (n=24) | IRCRA scale | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Intermediate (level 2) (n=7) |
Advanced (level 3) (n=8) |
Elite & High Elite (levels 4 & 5) (n=7) |
Intermediate (level 2) (n=7) |
Advanced (level 3) (n=10) |
Elite & High Elite (levels 4 & 5) (n=7) |
||||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | R* | |
| Weight (kg) | 69,77 | 5,62 | 66,35 | 5,74 | 67,41 | 11,56 | 54,94 | 5,40 | 51,12 | 3,33 | 50,40 | 4,78 | 0,012 |
| Height (cm) | 172,69 | 3,21 | 173,50 | 5,01 | 177,43 | 10,55 | 162,09 | 6,74 | 162,32 | 2,39 | 159,86 | 3,34 | 0,188 |
| BMI (kg/m2) | 23,38 | 1,50 | 22,03 | 1,51 | 21,22 | 1,58 | 20,91 | 1,52 | 19,40 | 1,18 | 19,72 | 1,69 | -0,159 |
| Sitting height (cm) | 88,01 | 3,53 | 91,10 | 2,46 | 92,66 | 7,44 | 86,39 | 2,56 | 85,84 | 2,65 | 84,93 | 1,21 | 0,172 |
| Arm span (cm) | 176,71 | 6,99 | 177,55 | 5,84 | 182,21 | 10,35 | 164,33 | 6,83 | 162,92 | 3,41 | 163,74 | 5,57 | 0,147 |
| ∑6 skinfolds (mm) | 61,52 | 16,41 | 47,25 | 12,22 | 34,92 | 3,05 | 66,31 | 6,10 | 64,09 | 8,62 | 58,70 | 12,65 | -0,573 |
| ∑8 skinfolds (mm) | 79,54 | 21,53 | 58,91 | 15,70 | 44,19 | 3,68 | 80,16 | 8,07 | 77,08 | 10,17 | 69,28 | 15,34 | -0,616 |
| Arm relaxed girth (cm) | 30,83 | 1,32 | 29,89 | 1,86 | 28,56 | 2,49 | 24,89 | 1,91 | 25,30 | 1,15 | 25,09 | 1,48 | -0,018 |
| Arm flexed girth (cm) | 33,32 | 1,17 | 32,92 | 1,78 | 32,30 | 3,43 | 25,98 | 1,76 | 26,58 | 1,24 | 27,16 | 1,41 | 0,204 |
| Forearm girth (cm) | 26,91 | 3,77 | 27,84 | 1,50 | 27,70 | 1,97 | 22,84 | ,57 | 23,08 | 1,14 | 23,42 | ,72 | 0,342 |
| Thigh middle girth (cm) | 50,12 | 2,24 | 48,16 | 2,77 | 47,06 | 3,74 | 47,26 | 2,55 | 43,68 | 2,72 | 44,34 | 3,11 | -0,150 |
| Calf girth (cm) | 36,40 | 2,10 | 36,18 | 1,53 | 35,78 | 2,47 | 34,06 | 1,57 | 32,76 | 2,36 | 32,83 | 1,34 | 0,002 |
| hand length (cm) | 18,54 | 0,92 | 18,39 | 0,57 | 18,57 | 1,24 | 16,34 | 0,86 | 17,07 | 0,56 | 16,81 | 0,68 | 0,183 |
| Humerus breadth (cm) | 7,61 | 0,20 | 7,57 | 0,38 | 7,67 | 0,34 | 6,13 | 0,37 | 6,43 | 0,27 | 6,43 | 0,37 | 0,247 |
| Bi-styloid breadth (cm) | 5,89 | 0,38 | 5,85 | 0,26 | 6,11 | 0,44 | 5,07 | 0,14 | 5,21 | 0,20 | 5,20 | 0,16 | 0,281 |
| Femur breadth (cm) | 9,83 | 0,26 | 9,95 | 0,39 | 10,17 | 0,53 | 8,97 | 0,24 | 8,84 | 0,29 | 8,77 | 0,35 | 0,164 |
| Fat Mass (kg) | 12,18 | 2,86 | 9,66 | 2,94 | 6,92 | 1,91 | 12,75 | 2,29 | 11,66 | 1,42 | 10,00 | 2,52 | -0,590 |
| Bone Mass (kg) | 11,94 | 0,66 | 12,09 | 0,93 | 13,14 | 1,88 | 9,21 | 0,73 | 9,30 | 0,43 | 9,04 | 0,43 | 0,191 |
| Muscle Mass (kg) | 31,18 | 2,54 | 30,70 | 2,51 | 30,37 | 5,33 | 20,57 | 1,33 | 20,19 | 1,84 | 20,10 | 1,52 | 0,163 |
| % Fat Mass | 17,35 | 3,47 | 14,52 | 4,05 | 10,25 | 1,88 | 23,09 | 2,43 | 22,81 | 2,46 | 19,77 | 4,26 | -0,497 |
| Endomorphy | 2,99 | 1,01 | 2,08 | 0,57 | 1,46 | 0,19 | 2,99 | 0,38 | 2,89 | 0,49 | 2,55 | 0,79 | -0,589 |
| Mesomorphy | 6,19 | 0,70 | 6,04 | 0,94 | 5,61 | 0,58 | 3,87 | 1,20 | 3,94 | 0,70 | 4,35 | 0,66 | 0,143 |
| Ectomorphy | 2,16 | 0,67 | 2,82 | 0,85 | 3,46 | 0,43 | 2,66 | 0,95 | 3,46 | 0,66 | 3,14 | 0,92 | 0,308 |
SD: Standard Deviation; *Spearman's R; bolding letter: <0,05; bolding + italic letter: <0,01 .
Table 3.
Energy requirements, EA and macronutrient intake.
| Total (n=45) | Males (n=22) | Females (n=23) |
P ♂ vs ♀ |
Effect Size** | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | d | IC (95%) | |||
| Energy requirements | ||||||||||
| EEE (kcal/day) | 184,33 | 126,64 | 211,72 | 152,29 | 159,21 | 93,95 | 0,235* | 0,419 | (-0,168 – 1,002) | |
| Energy Intake | ||||||||||
| Total kcal/day | 1803,70 | 554,18 | 2176,98 | 505,10 | 1446,64 | 313,17 | <0,01# | 1,747 | (1,049 – 2,430) | |
| Total kcal·kg· FFM−1·d−1 | 36,82 | 8,44 | 37,60 | 8,23 | 36,07 | 8,76 | 0,551 | 0,179 | (-0,407 – 0,764) | |
| Energy Availability (kcal·kg· FFM−1·d−1) | 33,01 | 9,02 | 34,06 | 8,63 | 32,01 | 9,45 | 0,451# | 0,227 | (-0,361 – 0,812) | |
| Carbohydrate Intake | ||||||||||
| Total g/day | 172,01 | 71,07 | 210,60 | 73,75 | 135,09 | 44,66 | <0,01* | 1,245 | (0,599 – 1,880) | |
| g/kg·day | 2,87 | 1,02 | 3,12 | 1,07 | 2,63 | 0,92 | 0,105# | 0,493 | (-0,103 – 1,084) | |
| % Total Energy Intake | 37,31 | 7,07 | 38,04 | 6,93 | 36,62 | 7,28 | 0,504# | 0,201 | (-0,386 – 0,786) | |
| Protein Intake | ||||||||||
| Total g/day | 93,89 | 31,06 | 115,08 | 27,29 | 73,62 | 18,43 | <0,01# | 1,788 | (1,085 – 2,476) | |
| g/kg·day | 1,57 | ,43 | 1,71 | 0,44 | 1,43 | 0,38 | 0,021* | 0,703 | (0,096 – 1,302) | |
| % Total Energy Intake | 21,11 | 4,05 | 21,50 | 3,89 | 20,73 | 4,25 | 0,527# | 0,190 | (-0,397 – 0,775) | |
| Fat Intake | ||||||||||
| Total g/day | 80,84 | 25,49 | 96,42 | 24,58 | 65,93 | 15,73 | <0,01# | 1,485 | (0,815 – 2,141) | |
| % Total Energy Intake | Total | 40,77 | 6,10 | 40,14 | 5,94 | 41,38 | 6,31 | 0,504# | -0,201 | (-0,786 – 0,386) |
| Saturated Fatty Acids | 10,65 | 2,27 | 10,52 | 1,97 | 10,77 | 2,56 | 0,714# | -0,110 | (-0,694 – 0,476) | |
| Monounsaturated Fatty Acids | 16,95 | 4,11 | 17,52 | 4,43 | 16,40 | 3,80 | 0,366# | 0,273 | (-0,316 – 0,858) | |
| Polyunsaturated Fatty Acids | 7,36 | 2,92 | 7,26 | 2,53 | 7,46 | 3,31 | 0,964* | -0,066 | (-0,650 – 0,519) | |
SD: Standard Deviation; * Mann–Whitney U test; **Cohen’s d index; # independent samples t-test.
Table 4.
Intake of vitamins and adjustment to Spanish RDAs.
| Total (n=45) | Males (n=22) | Females (n=23) |
p ♂ vs ♀ |
Effect Size** | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | d | IC (95%) | |||
| Thiamine | Total mg/day | 1,35 | 0,62 | 1,53 | 0,51 | 1,19 | 0,69 | 0,011* | 0,560 | (-0,040-1,153) |
| % RDA | 122,94 | 56,76 | 127,23 | 42,16 | 118,83 | 68,63 | 0,153* | 0,147 | (-0,439-0,718) | |
| Riboflavin | Total mg/day | 1,85 | 1,11 | 2,05 | 1,14 | 1,65 | 1,07 | 0,054* | 0,365 | (-0,227-0,952) |
| % RDA | 129,82 | 78,25 | 129,34 | 71,26 | 130,27 | 86,00 | 0,555* | -0,012 | (-0,596-0,573) | |
| Niacin | Total mg/day | 75,32 | 124,32 | 33,89 | 15,02 | 114,95 | 165,34 | 0,256* | -0,683 | (-1,281--0,077) |
| % RDA | 513,90 | 895,30 | 192,78 | 83,26 | 821,06 | 1181,00 | 0,683* | -0,742 | (-1,343--0,133) | |
| Vitamin B6 | Total mg/day | 2,13 | 0,89 | 2,40 | 0,78 | 1,88 | 0,93 | 0,046# | 0,613 | (0,011-1,208) |
| % RDA | 157,19 | 63,77 | 161,49 | 51,63 | 153,09 | 74,51 | 0,664# | 0,131 | (-0,455-0,715) | |
| Folic acid | Total µg/day | 321,96 | 143,32 | 333,22 | 129,91 | 311,19 | 157,24 | 0,525* | 0,152 | (-0,434-0,737) |
| % RDA | 107,32 | 47,77 | 111,07 | 43,30 | 103,73 | 52,41 | 0,525* | 0,152 | (-0,434-0,737) | |
| Vitamin B12 | Total µg/day | 27,39 | 72,29 | 20,49 | 60,13 | 34,00 | 83,10 | 0,200* | -0,186 | (-0,770-0,401) |
| % RDA | 1369,51 | 3614,28 | 1024,25 | 3006,56 | 1699,76 | 4155,03 | 0,200* | -0,186 | (-0,770-0,401) | |
| Vitamin C | Total mg/day | 168,44 | 188,04 | 146,13 | 101,18 | 189,77 | 244,89 | 0,856* | -0,231 | (-0,816-0,357) |
| % RDA | 280,73 | 313,40 | 243,55 | 168,63 | 316,29 | 408,16 | 0,856* | -0,231 | (-0,816-0,357) | |
| Vitamin A | Total µg/day | 874,42 | 570,67 | 868,02 | 714,27 | 880,55 | 405,28 | 0,329* | -0,022 | (-0,606-0,563) |
| % RDA | 135,03 | 86,30 | 122,77 | 102,56 | 146,76 | 67,55 | 0,073* | -0,277 | (-0,863-0,312) | |
| Vitamin D | Total µg/day | 10,33 | 18,88 | 12,78 | 24,87 | 7,99 | 10,52 | 0,555* | 0,253 | (-0,335-0,838) |
| % RDA | 206,69 | 377,52 | 255,67 | 497,32 | 159,84 | 210,40 | 0,555* | 0,253 | (-0,335-0,838) | |
| Vitamin E | Total mg/day | 19,28 | 38,85 | 15,23 | 6,06 | 23,16 | 54,32 | 0,107* | -0,203 | (-0,788-0,384) |
| % RDA | 128,54 | 258,97 | 101,52 | 40,39 | 154,39 | 362,15 | 0,107* | -0,203 | (-0,788-0,384) | |
SD: Standard Deviation; * Mann–Whitney U test; **Cohen’s d index; # independent samples t-test.
Table 5.
Mineral intake and adjustment to Spanish RDA.
| Total (n=45) | Males (n=22) | Females (n=23) |
p ♂ vs♀ |
Effect Size** | ||||||
| Mean | SD | Mean | SD | Mean | SD | d | IC (95%) | |||
| Calcium | Total mg/day | 866,88 | 355,37 | 949,10 | 371,21 | 788,24 | 328,35 | 0,131# | 0,460 | (-0,135 – 1,050) |
| % RDA | 96,25 | 39,61 | 105,46 | 41,25 | 87,45 | 36,71 | 0,129# | 0,462 | (-0,133 – 1,052) | |
| Phosphorus | Total mg/day | 1226,44 | 413,06 | 1454,23 | 392,27 | 1008,55 | 304,69 | <0,01# | 1,273 | (0,623 – 1,910) |
| % RDA | 171,41 | 59,57 | 204,66 | 58,01 | 139,60 | 41,50 | <0,01# | 1,295 | (0,644 – 1,934) | |
| Potassium | Total mg/day | 2897,10 | 1198,47 | 3496,63 | 1253,12 | 2323,63 | 818,83 | <0,01* | 1,113 | (0,478 – 1,738) |
| % RDA | 93,45 | 38,66 | 112,79 | 40,42 | 74,96 | 26,41 | <0,01* | 1,113 | (0,478 – 1,738) | |
| Magnesium | Total mg/day | 349,70 | 171,95 | 413,72 | 192,97 | 288,46 | 124,79 | 0,013* | 0,775 | (0,163 – 1,377) |
| % RDA | 106,93 | 49,40 | 118,21 | 55,13 | 96,15 | 41,60 | 0,188* | 0,453 | (-0,142 – 1,043) | |
| Iron | Total mg/day | 14,60 | 6,15 | 16,33 | 5,36 | 12,94 | 6,51 | 0,031* | 0,568 | (-0,032 – 1,162) |
| % RDA | 126,12 | 73,12 | 177,91 | 62,23 | 76,57 | 41,80 | <0,01* | 1,920 | (1,202 – 2,623) | |
| Zinc | Total mg/day | 10,41 | 9,36 | 10,98 | 3,02 | 9,87 | 12,88 | <0,01* | 0,117 | (-0,468 – 0,702) |
| % RDA | 125,89 | 132,84 | 113,55 | 32,39 | 137,69 | 184,37 | 0,296* | -0,180 | (-0,765 – 0,406) | |
| Iodine | Total µg/day | 97,41 | 114,14 | 127,76 | 151,42 | 68,38 | 48,66 | 0,011* | 0,533 | (-0,065 – 1,125) |
| % RDA | 64,94 | 76,09 | 85,17 | 100,95 | 45,59 | 32,44 | 0,011* | 0,533 | (-0,065 – 1,125) | |
| Selenium | Total µg/day | 61,47 | 41,33 | 83,90 | 47,71 | 40,02 | 16,12 | <0,01* | 1,244 | (0,597 – 1,878) |
| % RDA | 114,03 | 74,52 | 154,16 | 86,23 | 75,64 | 29,30 | <0,01* | 1,231 | (0,585 – 1,864) | |
SD: Standard Deviation; * Mann–Whitney U test; **Cohen’s d index; # independent samples t-test.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



