
Submitted:
01 August 2024
Posted:
02 August 2024
You are already at the latest version
Abstract
Breast cancer (BC) is the leading cause of cancer-related mortality among women, and hormone receptor (HR)-positive subtype makes up majority of all cases. The standard-of-care (SOC) in HR+/HER2- metastatic BC (MBC) is endocrine therapy (ET) plus a CDK4/6 inhibitor (CDK4/6i). ESR1 mutations could impair clinical efficacy of the ETs. Similarly, PIK3CA mutations may serve as a negative prognostic marker. Furthermore, MBC is challenging to treat despite new drug approvals. Our patient received multiple lines of ET ± CDK4/6i and chemotherapy but persistently progressed after each or stopped the treatment due to adverse events. Here we showed for the first time that all-oral combination of elacestrant plus alpelisib was feasible, tolerable and clinically active in an ESR1 and PIK3CA co-mutated and heavily pretreated patient. We achieved a remarkable response in the metastatic lesions with minor toxicity issues. This case highlights the importance of utilizing up-to-date therapeutic agents and reactive decision-making during personalized cancer treatment.
Keywords:
HR+/HER2- metastatic breast cancer
; HR-positive
; Selective estrogen receptor degrader (SERD)
; Elacestrant
; Alpelisib
; Precision oncology
; Cancer genomics
Introduction
Breast cancer (BC) is the most commonly diagnosed cancer type in the US and worldwide according to estimates by ACS [1] and GLOBOCAN [2], respectively. HR-positive patients constitute 75-80% of all BC cases. The standard-of-care (SOC) in the HR+/HER2- metastatic patients is endocrine therapy (ET) in combination with CDK4/6 inhibitors [3,4]. However, targeted treatment options after progression on the SOC is quite limited, and their sequencing for the optimum response is not clearly defined [5,6].
ESR1 mutations can lead to acquired resistance to ETs, but especially prevalent after progression on prior aromatase inhibitor (AI) treatment, even more prevalent after AI plus CDK4/6i and in the metastatic setting (de novo: 3.9% vs. up to 55% posttreatment) [7,8,9,10]. As these mutations could be also associated with worse survival, new treatment strategies need to be explored. Recent approval of elacestrant, an orally available selective estrogen receptor degrader (SERD), for ER+/HER2-, ESR1-mutated advanced or metastatic breast cancer (A/MBC) patients exemplifies the success of such a strategy. PIK3CA is also frequently altered and is an actionable target in breast cancer. Although some studies discovered PIK3CA mutation as a negative prognostic marker following the SOC, PI3K-alpha specific inhibitor alpelisib together with fulvestrant was not approved in the first line but following progression on or after an endocrine-based regimen in HR+/HER2-, PIK3CA-mutated, A/MBC patients. These alterations could limit the efficacy of endocrine and targeted therapies. However, there are currently no data (ongoing, NCT05563220) regarding the safety and clinical activity for combination of elacestrant and inhibitors against PI3K/AKT/mTOR pathway and/or CDK4/6 in the ER-positive, ESR1 and PIK3CA co-mutated BC patients.
Here, to our knowledge, we report the first case of safety and efficacy of all-oral elacestrant and alpelisib combination in a heavily pretreated, ESR1 and PIK3CA co-mutated HR+/HER2- MBC patient. There was a partial response following this combination with minor adverse events.
Results
Case Presentation
The patient presented here is a 43-year-old Caucasian female diagnosed with MBC (cT2N3M1, stage IV) in January 2018. The PET/CT revealed a 28-mm mass in the left breast as well as FDG uptake in multiple lymph nodes (LN – right supraclavicular and right lower paratracheal, precarinal and subcarinal) and mediastinal metastasis (proven by biopsy examination – see below). The patient had no history of chronic disease or continuous drug use (only oral contraceptive for 1-year), and no known allergies. She is a light-smoker (10 packs/year) but a non-drinker. Although the patient’s cousin was also newly diagnosed with breast cancer, there were no germline BRCA mutations.
The breast Tru-Cut biopsy was ER+ (70%), PR+ (20%) and HER2- (1+) with a Ki-67 proliferation index (KPI) of 15%. The mediastinal LN biopsy was compatible with breast cancer metastasis. Accordingly, she received neoadjuvant chemotherapy (NACT) consisting of dose-dense doxorubicin/cyclophosphamide (AC – 4 cycles, doxorubicin 60 mg/m2 and cyclophosphamide 600 mg/m2 every 2 weeks) followed by weekly paclitaxel (T – 12 cycles, 80 mg/m2) from February to July 2018 (Figure 1). Although there was a metabolic and pathologic complete response in August 2018 by PET/CT, breast-conserving surgery (lumpectomy) showed a 15-mm mass with histological grade 3 and diffuse DCIS (no invasive component) in September 2018. The patient was treated with adjuvant tamoxifen (20 mg/day, plus leuprorelin acetate (LA)/q3M) from September 2018 to January 2021. Due to increased CA 15-3 levels, a PET/CT was requested in January 2021, revealing disease progression in the mediastinal lymph nodes and new bone metastases. She was administered letrozole (2.5 mg/day) plus palbociclib (125 mg/day, 3 weeks on/1 week off – plus LA and zoledronic acid) from January to November 2021. A partial response was observed in the mediastinal LNs and bone lesions by PET/CT in April 2021 (RECIST v1.1 [11]). However, progressive disease was observed in the bone lesions, and 3 new liver lesions in segment 5 emerged in November 2021, all of which was treated via liver radiofrequency ablation (RFA). Later, the treatment was changed to capecitabine (1,250 mg/m2 twice daily) plus docetaxel (75 mg/m2 on day 1). This regimen was stopped due to hand-foot syndrome caused by capecitabine in January 2022, and it was switched to gemcitabine (1,200 mg/m2 on day 1 and 8 every 3 weeks) plus paclitaxel (75 mg/m2 on day 1, January – July 2022). The PET/CT in March 2022 showed regression in the bone lesions, and the liver foci disappeared (potentially due to the RFA). The patient experienced grade 1 neuropathy, probably caused by paclitaxel. Accordingly, the treatment was changed to single-agent gemcitabine.
The patient was offered a comprehensive genomic profiling (CGP) test (OncoDEEP – April 2023, liver Tru-Cut biopsy – ER 10%, PR 60% and HER2-negative, CGP #1 in Figure 1), which detected ESR1 Y537S, PIK3CA E545K and CCND1 amplification with a TMB of 14.95 muts/Mb, MSS and HRD-positive status. The test also reported the following IHC findings: AR 1%, HER2 0%, CD8 10%, and negative PD-L1 status (CPS: 0). The pathology examination confirmed HR-positive, HER2-negative breast cancer with extensive metastasis to liver. The patient received ET plus alpelisib (300 mg/day, April – May 2023) at an external clinic but experienced hyperglycemia (blood sugar >300 mg/dL) that led to treatment discontinuation. She was later treated with carboplatin plus paclitaxel for 2 cycles (May – July 2023).
She was later admitted to our clinic for a second opinion, and we recommended a CGP test to design a patient-tailored treatment plan. We also requested a PET/CT (July 2023) to comprehend the current status of the disease. We first utilized a liquid biopsy to account for tumor heterogeneity of the extensive metastasis (FoundationOne®Liquid CDx – July 2023, CGP #2 in Figure 1) and observed the following alterations: ESR1 Y537S, PIK3CA E545K, FGFR2-TACC2 rearrangement, MAP3K1 Q1261*, SETD2 S470*, TP53 H193R, and equivocal amplifications of CCND1, MDM2, MYC, EMSY, FGF19, FGF3, and FGF4. The tumor fraction was elevated, blood tumor mutational burden (bTMB) was 9 muts/Mb, and MSI-H was not detected. We decided to use elacestrant plus alpelisib considering ESR1 and PIK3CA mutations. While waiting for response from the off-label drug committee for the combination and access to elacestrant, we initially started with fulvestrant plus alpelisib (150 mg/day), complemented by ketogenic diet. The patient tolerated the treatment without any blood sugar elevation but experienced grade 1 diarrhea, nausea and asthenia. We also offered a Tempus CGP test (August 2023, CGP #3 in Figure 1) due to the presence of an FGFR2 rearrangement at DNA level, as Tempus could assess the presence of rearrangements/fusions at both DNA and RNA level. RNA-based analysis is currently considered the gold standard for such alterations. While some alterations were missing in this test using liver biopsy, it reported many of the same alterations: ESR1 Y537S, PIK3CA E545K, MAP3K1 Q1261*, TP53 H193R as well as copy number gains in CCND1, EMSY, FGF3 and FGF4. The tTMB was 4.2 muts/Mb with an MSS and negative PD-L1 status (TPS <1%, CPS <1). This test additionally reported overexpression of ERBB3 and PGR, and a homologous recombination deficiency (HRD) score of 26.1%, where the cut-off to define HRD is 21% in breast cancer. The biomarkers and alterations reported by each test were compared in Figure 1b. The co-occurrence pattern of ESR1 and PIK3CA alterations were shown in a metastatic breast cancer cohort (INSERM, cBioPortal, Figure 1c).
As our patient received multiple lines of chemotherapy and hormonal therapy including short-term fulvestrant and due to the presence of ESR1 Y537S and PIK3CA E545K mutations, we recommended and switched to elacestrant (345 mg/day) plus alpelisib (100 mg/day, increased to 150 mg/day with a ketogenic diet) combination. The treatment was well-tolerated with grade 1 asthenia, highlighting that alpelisib retreatment after hyperglycemia could be managed by dose reduction and ketogenic diet (increasing tolerability and efficacy). The PET/CT (October 2023 vs. July 2023) revealed a partial response in the metastatic lesions and improved clinical status (Figure 2, a vs. c and b vs. d). Unfortunately, performance status deterioration and disease progression (time-to-progression: ~5.5 months) by ultrasound examination were reported at the external clinic in January 2024. We added lenvatinib to the treatment to target FGF/R alterations but the patient succumbed to death after 3 months (April 2024).
Written informed consent was obtained from the patient for both treatment and publication of her anonymized data in this scientific publication. We also submitted an off-label drug use application to the Ministry of Health and received approval.
Discussion
BC, as the most diagnosed cancer, is a global health problem with a 5-year survival rate less than 30% in the distant metastatic cases [12]. The first-line treatment in the HR+/HER2- MBC without visceral metastasis and without germline BRCA1/2 mutation is endocrine therapy (a nonsteroidal AI or fulvestrant) plus a CDK4/6 inhibitor [3,4]. However, de novo or especially acquired resistance to hormone therapy is observed in many patients, rendering current approaches ineffective. Some resistance mechanisms include acquisition of ESR1 mutations, loss of ER and high cyclin E1 expression, dysregulation in ER co-regulatory proteins, amplifications in MYC and FGFR1 as well as TP53 mutations [13,14,15,16].
ESR1 mutations are frequently detected in metastatic tumors as compared to the primary tumors [17]. Many of these mutations are activating and can drive ligand-independent ER activity but may differentially affect the response to endocrine therapies (Y537S vs. D538G, E380Q, S463P) [18]. They are mostly found after aromatase inhibitor treatment (or AI plus CDK4/6i), and are associated with worse patient outcomes [9,19]. Unlike AIs, some clinical studies showed that fulvestrant-based treatment could be efficacious in the ESR1-mutant patients similar to the ESR1 WT patients [7]. However, ESR1 Y537S mutation was found to be statistically enriched in the posttreatment (fulvestrant plus palbociclib) samples through the genomic landscape and clonal evolution analysis in the PALOMA-3 trial [20]. Similarly, patients harboring baseline Y537S mutation had a shorter progression-free survival (PFS – 1.8 vs. 3.5 months) than those WT for this residue following fulvestrant treatment (cohort A) in the plasmaMATCH phase 2 trial [21]. One strategy to overcome the resistance could be chemotherapy and fulvestrant combination; however, a study demonstrated that the combination was synergistic in the Y537S-mutant models but dependent on p53 activity [22]. Considering the previous failures with multiple lines of chemotherapy and the patient’s TP53 mutation, this approach was not prioritized in our case. Moreover, PIK3CA mutations or activation have been previously associated with resistance to chemotherapy in many cancer types [23,24,25]. As next generation of anti-estrogen therapies active against ESR1 mutations have been developed, they could form the backbone for the treatment of the endocrine-refractory patients. Following the phase III EMERALD trial, elacestrant has received regulatory approval as monotherapy for postmenopausal women or adult men with ER+/HER2-, ESR1-mutated advanced or metastatic breast cancer with disease progression following at least one line of endocrine therapy [26]. Patients with concurrent ESR1 and TP53 mutations (8.61 vs. 1.87 months), or ESR1 mutations with liver and/or lung metastases (7.26 vs. 1.87 months) exhibited remarkably longer PFS upon elacestrant vs. placebo [27]. There are also ELAINE 2 phase II trial [28] (with abemaciclib) and a case report (monotherapy) [29] showing the clinical efficacy of lasofoxifene (LAS), a nonsteroidal selective estrogen receptor modulator (SERM), in a similar group of patients after disease progression on prior therapies. Lastly, early results from a randomized phase II trial (SERENA-2) demonstrated improved and promising clinical outcomes with a next-generation oral SERD, camizestrant versus fulvestrant in postmenopausal women with advanced ER+/HER2˗ breast cancer with disease recurrence or progression after ≤1 endocrine therapy and a baseline ESR1 mutation, including Y537S [30,31]. Since our patient did not obtain clinical benefit from the ET-containing regimens and potential resistance to fulvestrant through Y537S mutation, we switched to elacestrant to enhance therapeutic efficacy.
PIK3CA is the most commonly mutated gene in TCGA PanCancer Atlas [32] and METABRIC breast cancer cohorts [33]. A meta-analysis in advanced HR+, HER2- breast cancer patients not receiving PI3K-targeted drugs revealed that PIK3CA mutation was a negative prognostic factor for both progression-free and overall survival (OS) [34]. For example, PFS was shorter in patients concomitant ESR1 and PIK3CA mutations compared to all ESR1-mutated patients (5.45 vs. 8.61 months) although elacestrant still led to significantly higher PFS compared to placebo (5.45 vs. 1.94 months) [27]. In line, LAS plus abemaciclib yielded a 73% CBR and 12.9 months PFS in the ESR1-mutant patients whereas they were 63% and 7.8 months in the ESR1 and PIK3CA co-mutant patients [35]. Just 5 hotspot mutations cover approximately 75% of all PIK3CA mutations in breast cancer, where E545K accounts for more than 15% [36]. These alterations could be currently targeted by alpelisib, capivasertib or mTOR inhibitor, everolimus [37,38]. While alpelisib with fulvestrant is indicated for postmenopausal women and men with HR+/HER2-, PIK3CA-mutated, advanced or metastatic breast cancer as following progression on or after an endocrine-based regimen, the everolimus with exemestane is for patients with metastatic HR-positive breast cancer who progressed on nonsteroidal aromatase inhibitor (NSAI) therapy [39]. Prior exposure to CDK4/6 inhibitors did not lead to differential survival outcomes with this combination. More recently, pan-AKT inhibitor capivasertib in combination with fulvestrant has been approved in HR+/HER2- locally advanced or metastatic breast cancer harboring one or more AKT1, PIK3CA, or PTEN alterations following the positive results from the phase 3 CAPItello-291 trial [38]. However, the currently available data regarding the tolerability and efficacy of elacestrant with these agents is limited even though there are ongoing early-phase clinical trials (NCT05563220 and NCT05386108, n=3 for elacestrant 300 mg/day plus alpelisib 250 mg/day) evaluating the combinations of elacestrant with alpelisib, capivasertib, everolimus or CDK4/6 inhibitors [40]. Here our precision oncology center, for the first time, showed that elacestrant and alpelisib at doses selected through molecular tumor board discussions was well-tolerated with minor toxicities such as grade 1 asthenia. The ketogenic diet was reported to potentially improve tolerability and efficacy of PI3K inhibitors. Similarly, prophylactic metformin could diminish incidence and severity of hyperglycemia [41]. Overall, we achieved a partial response in the liver and bone metastatic lesions upon combinatorial treatment (Figure 2).
Gene fusions are strong oncogenic drivers that can drive tumorigenesis, cancer progression and therapeutic failure. However, FGFR2-TACC2 rearrangement reported in the FoundationOne Liquid CDx was later predicted to be “not in-frame” upon additional information request from the test provider. It was a result of chromosome 10 duplication fragment with breakpoints at chr10:123241583 and chr10:123788371 [5′- FGFR2 (x1-17) -3′:3′- TACC2 (x2-1) -5′]. Consistently, Tempus test from the liver biopsy did not report any FGFR2-TACC2 rearrangement although the alteration was detected at DNA level, it was absent at RNA level. Besides, out-of-frame fusions are often assumed to be inactivating mutations and labeled as passenger mutations [42,43,44]. Considering that RNA-based approach is the gold standard for the detection of structural variants, we initially did not include any FGFR inhibitor in the combination therapy. Similarly, the specimen harbors CCND1 and FGF amplifications (albeit equivocal in the F1 Liquid CDx) that can undermine therapeutic benefit. Pan-FGFR inhibitors such as pemigatinib have limited activity against these amplifications [45]. Multikinase FGFR inhibitors, unlike specific FGFR inhibitors, have also activity against other receptor tyrosine kinases (RTKs), such as VEGFR, which could be upregulated due to the presence of the TP53 mutation [46,47]. For example, lenvatinib in combination with palbociclib was highly active (50% PR) in the FGF/FGFR and accompanying alterations [48]. Therefore, these alterations should be monitored carefully during the course of treatment.
Overall, HR+/HER2- MBC is a challenging clinical entity to treat, especially after the failure of the SOC and in the heavily pretreated patients. Fortunately, we demonstrated for the first time that all-oral combination of elacestrant plus alpelisib with dose modifications and ketogenic diet was feasible and clinically active in an ESR1 and PIK3CA co-mutated patient. This case underlines the importance of utilizing up-to-date therapeutic agents and reactive decision-making (such as addition of lenvatinib) during personalized cancer treatment. It is also important to note that we should strive to make precision oncology the standard-of-care, not the currently organ-based therapeutic approaches. The timely evaluation and approval of such off-label drug combinations by health authorities could speed up paradigm shift towards precision oncology.
Data Availability Statement
All the data generated for the study are available in this article or from the corresponding author upon request.
Acknowledgements
We are grateful to our patient who made this study possible, and all the members of the medical oncology team involved in the treatment and care process.
Conflicts of Interest
The authors declare that they have no conflict of interest.
References
- Siegel RL, Miller KD, Wagle NS, et al.: Cancer statistics, 2023. CA Cancer J Clin 73:17-48, 2023.
- Sung H, Ferlay J, Siegel RL, et al.: Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 71:209-249, 2021. [CrossRef]
- Al Sukhun S, Temin S, Barrios CH, et al.: Systemic Treatment of Patients With Metastatic Breast Cancer: ASCO Resource-Stratified Guideline. JCO Glob Oncol 10:e2300285, 2024.
- D’Amico P, Cristofanilli M: Standard of Care in Hormone Receptor-Positive Metastatic Breast Cancer: Can We Improve the Current Regimens or Develop Better Selection Tools? JCO Oncol Pract 18:331-334, 2022.
- Ma J, Chan JJ, Toh CH, et al.: Emerging systemic therapy options beyond CDK4/6 inhibitors for hormone receptor-positive HER2-negative advanced breast cancer. NPJ Breast Cancer 9:74, 2023.
- Mittal A, Molto Valiente C, Tamimi F, et al.: Filling the Gap after CDK4/6 Inhibitors: Novel Endocrine and Biologic Treatment Options for Metastatic Hormone Receptor Positive Breast Cancer. Cancers (Basel) 15, 2023.
- Turner NC, Swift C, Kilburn L, et al.: ESR1 Mutations and Overall Survival on Fulvestrant versus Exemestane in Advanced Hormone Receptor-Positive Breast Cancer: A Combined Analysis of the Phase III SoFEA and EFECT Trials. Clin Cancer Res 26:5172-5177, 2020.
- Brett JO, Spring LM, Bardia A, et al.: ESR1 mutation as an emerging clinical biomarker in metastatic hormone receptor-positive breast cancer. Breast Cancer Res 23:85, 2021.
- Chaudhary N, Chibly AM, Collier A, et al.: CDK4/6i-treated HR+/HER2- breast cancer tumors show higher ESR1 mutation prevalence and more altered genomic landscape. NPJ Breast Cancer 10:15, 2024.
- Zundelevich A, Dadiani M, Kahana-Edwin S, et al.: ESR1 mutations are frequent in newly diagnosed metastatic and loco-regional recurrence of endocrine-treated breast cancer and carry worse prognosis. Breast Cancer Res 22:16, 2020.
- Eisenhauer EA, Therasse P, Bogaerts J, et al.: New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). European journal of cancer 45:228-247, 2009. [CrossRef]
- Yang SX, Hewitt SM, Yu J: Locoregional tumor burden and risk of mortality in metastatic breast cancer. NPJ Precis Oncol 6:22, 2022.
- McAndrew NP, Finn RS: Clinical Review on the Management of Hormone Receptor-Positive Metastatic Breast Cancer. JCO Oncol Pract 18:319-327, 2022. [CrossRef]
- Belachew EB, Sewasew DT: Molecular Mechanisms of Endocrine Resistance in Estrogen-Positive Breast Cancer. Front Endocrinol (Lausanne) 12:599586, 2021.
- O’Leary B, Cutts RJ, Huang X, et al.: Circulating Tumor DNA Markers for Early Progression on Fulvestrant With or Without Palbociclib in ER+ Advanced Breast Cancer. J Natl Cancer Inst 113:309-317, 2021.
- Turner NC, Liu Y, Zhu Z, et al.: Cyclin E1 Expression and Palbociclib Efficacy in Previously Treated Hormone Receptor-Positive Metastatic Breast Cancer. J Clin Oncol 37:1169-1178, 2019.
- Herzog SK, Fuqua SAW: ESR1 mutations and therapeutic resistance in metastatic breast cancer: progress and remaining challenges. Br J Cancer 126:174-186, 2022.
- Toy W, Weir H, Razavi P, et al.: Activating ESR1 Mutations Differentially Affect the Efficacy of ER Antagonists. Cancer Discov 7:277-287, 2017.
- Chandarlapaty S, Chen D, He W, et al.: Prevalence of ESR1 Mutations in Cell-Free DNA and Outcomes in Metastatic Breast Cancer: A Secondary Analysis of the BOLERO-2 Clinical Trial. JAMA Oncol 2:1310-1315, 2016.
- O’Leary B, Cutts RJ, Liu Y, et al.: The Genetic Landscape and Clonal Evolution of Breast Cancer Resistance to Palbociclib plus Fulvestrant in the PALOMA-3 Trial. Cancer Discov 8:1390-1403, 2018.
- Kingston B, Pearson A, Herrera-Abreu MT, et al.: ESR1 F404 mutations and acquired resistance to fulvestrant in the plasmaMATCH study. Journal of Clinical Oncology 40, 2022.
- Ma W, Hermida-Prado F, Guarducci C, et al.: Combination of fulvestrant and chemotherapy in ESR1 Y537S mutant breast cancer cells and potential synergy mechanism related to p53 wildtype. Journal of Clinical Oncology 38, 2020.
- Dong M, Shan B, Han X, et al.: Baseline Mutations and Up-Regulation of PI3K-AKT Pathway Serve as Potential Indicators of Lack of Response to Neoadjuvant Chemotherapy in Stage II/III Breast Cancer. Front Oncol 11:784985, 2021.
- Pergialiotis V, Nikolaou C, Haidopoulos D, et al.: PIK3CA Mutations and Their Impact on Survival Outcomes of Patients with Cervical Cancer: A Systematic Review. Acta Cytol 64:547-555, 2020.
- Wang Q, Shi YL, Zhou K, et al.: PIK3CA mutations confer resistance to first-line chemotherapy in colorectal cancer. Cell Death Dis 9:739, 2018.
- Bidard FC, Kaklamani VG, Neven P, et al.: Elacestrant (oral selective estrogen receptor degrader) Versus Standard Endocrine Therapy for Estrogen Receptor-Positive, Human Epidermal Growth Factor Receptor 2-Negative Advanced Breast Cancer: Results From the Randomized Phase III EMERALD Trial. J Clin Oncol 40:3246-3256, 2022.
- Bardia A, O’Shaughnessy J, Bidard FC, et al.: Abstract PS17-02: Elacestrant vs standard-of-care in ER+/HER2- advanced or metastatic breast cancer (mBC) with ESR1 mutation: key biomarkers and clinical subgroup analyses from the phase 3 EMERALD trial. Cancer Res 84, 2024.
- Damodaran S, O’Sullivan CC, Elkhanany A, et al.: Open-label, phase II, multicenter study of lasofoxifene plus abemaciclib for treating women with metastatic ER+/HER2- breast cancer and an ESR1 mutation after disease progression on prior therapies: ELAINE 2. Ann Oncol 34:1131-1140, 2023.
- Gal-Yam EN, Levanon K: Lasofoxifene Monotherapy Induces Durable Complete Remission in a Patient with Estrogen Receptor-Positive, Metastatic Breast Cancer with an ESR1 Mutation. JCO Precis Oncol 7:e2300097, 2023.
- Wong NZH, Yap DWT, Ong RJM, et al.: Efficacy of Oral SERDs in the treatment of ER+, HER2 - metastatic breast cancer, a stratified analysis of the ESR1 wild type and mutant subgroups. Ann Oncol, 2023.
- Oliveira M, Pominchuk D, Hamilton EP, et al.: Clinical activity of camizestrant, a next-generation SERD, versus fulvestrant in patients with a detectable ESR1 mutation: Exploratory analysis of the SERENA-2 phase 2 trial. Journal of Clinical Oncology 41.
- Berger AC, Korkut A, Kanchi RS, et al.: A Comprehensive Pan-Cancer Molecular Study of Gynecologic and Breast Cancers. Cancer Cell 33:690-705 e9, 2018. [CrossRef]
- Pereira B, Chin SF, Rueda OM, et al.: The somatic mutation profiles of 2,433 breast cancers refines their genomic and transcriptomic landscapes. Nat Commun 7:11479, 2016.
- Fillbrunn M, Signorovitch J, Andre F, et al.: PIK3CA mutation status, progression and survival in advanced HR + /HER2- breast cancer: a meta-analysis of published clinical trials. BMC Cancer 22:1002, 2022.
- Damodaran S, Cristofanilli M, Goetz M, et al.: Abstract PO2-14-09: Baseline genomic alterations and the activity of lasofoxifene (LAS) plus abemaciclib (Abema) in patients with ER+/HER2-metastatic breast cancer (mBC): the ELAINE 2 study. Cancer Research 84:PO2-14-09-PO2-14-09, 2024.
- Martinez-Saez O, Chic N, Pascual T, et al.: Frequency and spectrum of PIK3CA somatic mutations in breast cancer. Breast Cancer Res 22:45, 2020.
- Vernieri C, Corti F, Nichetti F, et al.: Everolimus versus alpelisib in advanced hormone receptor-positive HER2-negative breast cancer: targeting different nodes of the PI3K/AKT/mTORC1 pathway with different clinical implications. Breast Cancer Res 22:33, 2020.
- Turner NC, Oliveira M, Howell SJ, et al.: Capivasertib in Hormone Receptor-Positive Advanced Breast Cancer. N Engl J Med 388:2058-2070, 2023.
- Baselga J, Campone M, Piccart M, et al.: Everolimus in postmenopausal hormone-receptor-positive advanced breast cancer. N Engl J Med 366:520-9, 2012.
- Varella L, Cristofanilli M: Evaluating Elacestrant in the Management of ER-Positive, HER2-Negative Advanced Breast Cancer: Evidence to Date. Onco Targets Ther 16:189-196, 2023.
- Llombart-Cussac A, Pérez-Garcia JM, Borrego MR, et al.: Preventing alpelisib-related hyperglycaemia in HR+/HER2−/PIK3CA-mutated advanced breast cancer using metformin (METALLICA): a multicentre, open-label, single-arm, phase 2 trial. Eclinicalmedicine 71, 2024.
- Howarth KD, Mirza T, Cooke SL, et al.: NRG1 fusions in breast cancer. Breast Cancer Res 23:3, 2021.
- Liu J, Tokheim C, Lee JD, et al.: Genetic fusions favor tumorigenesis through degron loss in oncogenes. Nat Commun 12:6704, 2021.
- An S, Koh HH, Chang ES, et al.: Unearthing novel fusions as therapeutic targets in solid tumors using targeted RNA sequencing. Front Oncol 12:892918, 2022.
- Subbiah V, Iannotti NO, Gutierrez M, et al.: FIGHT-101, a first-in-human study of potent and selective FGFR 1-3 inhibitor pemigatinib in pan-cancer patients with FGF/FGFR alterations and advanced malignancies. Ann Oncol 33:522-533, 2022.
- Wheler JJ, Janku F, Naing A, et al.: TP53 Alterations Correlate with Response to VEGF/VEGFR Inhibitors: Implications for Targeted Therapeutics. Mol Cancer Ther 15:2475-2485, 2016.
- Li AM, Boichard A, Kurzrock R: Mutated TP53 is a marker of increased VEGF expression: analysis of 7,525 pan-cancer tissues. Cancer Biol Ther 21:95-100, 2020.
- Uehara Y, Ikeda S, Kim KH, et al.: Targeting the FGF/FGFR axis and its co-alteration allies. ESMO Open 7:100647, 2022.
Figure 1.
Timeline of disease status and treatment response as well as comparison of the comprehensive genomic profiling results. a) A 43-year-old female was diagnosed with metastatic breast cancer in 2018. She received multiple lines of chemotherapy or endocrine therapy-containing regimens from 2018 to 2024. Although partial responses had been achieved with some of these treatments, the disease eventually progressed or the treatment was halted due to toxicity issues. From July-August 2023, our team have followed a precision oncology approach through comprehensive genomic profiling, and achieved a partial response with an all-oral combination of elacestrant plus alpelisib as well as ketogenic diet. b) Comparison of the biomarkers and alterations detected and reported by 3 different CGP tests. c) Co-occurrence pattern of ESR1 and PIK3CA alterations in a metastatic breast cancer patient cohort (INSERM, cBioPortal).
Figure 1.
Timeline of disease status and treatment response as well as comparison of the comprehensive genomic profiling results. a) A 43-year-old female was diagnosed with metastatic breast cancer in 2018. She received multiple lines of chemotherapy or endocrine therapy-containing regimens from 2018 to 2024. Although partial responses had been achieved with some of these treatments, the disease eventually progressed or the treatment was halted due to toxicity issues. From July-August 2023, our team have followed a precision oncology approach through comprehensive genomic profiling, and achieved a partial response with an all-oral combination of elacestrant plus alpelisib as well as ketogenic diet. b) Comparison of the biomarkers and alterations detected and reported by 3 different CGP tests. c) Co-occurrence pattern of ESR1 and PIK3CA alterations in a metastatic breast cancer patient cohort (INSERM, cBioPortal).
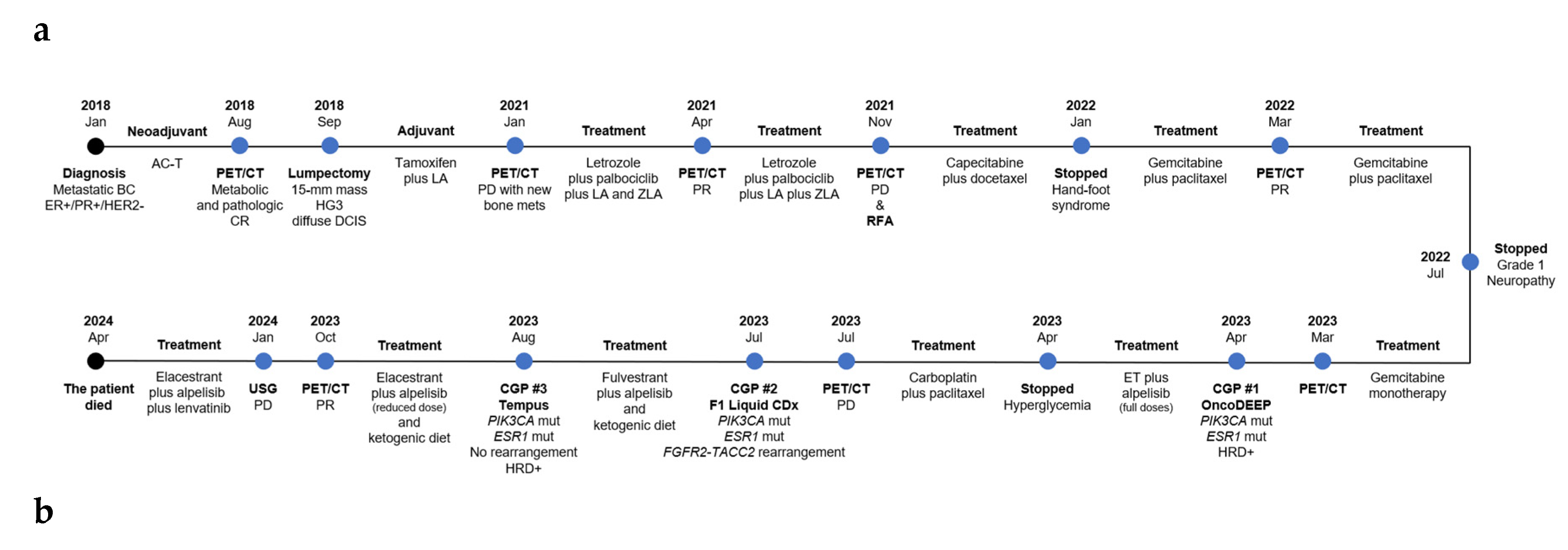
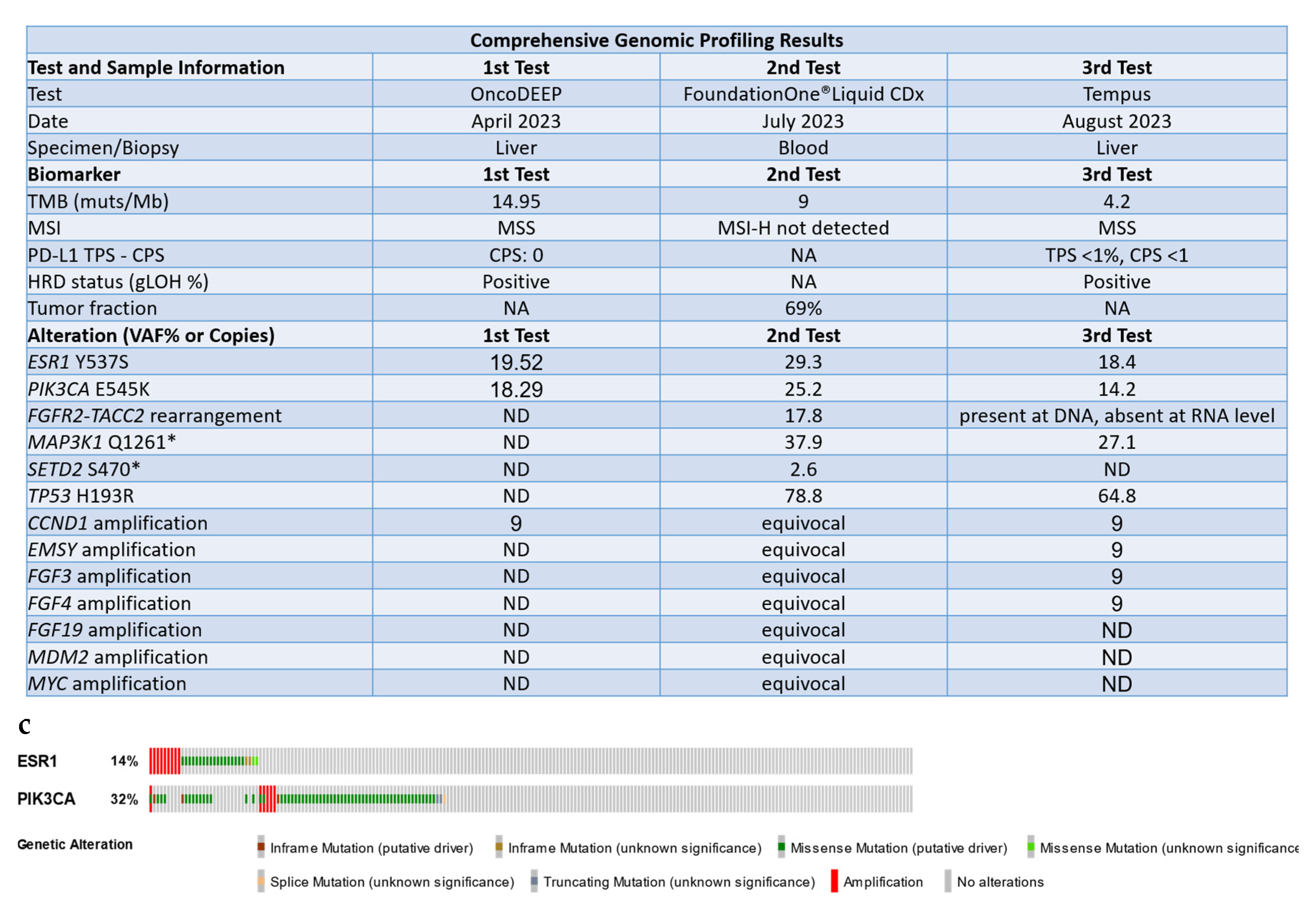
Figure 2.
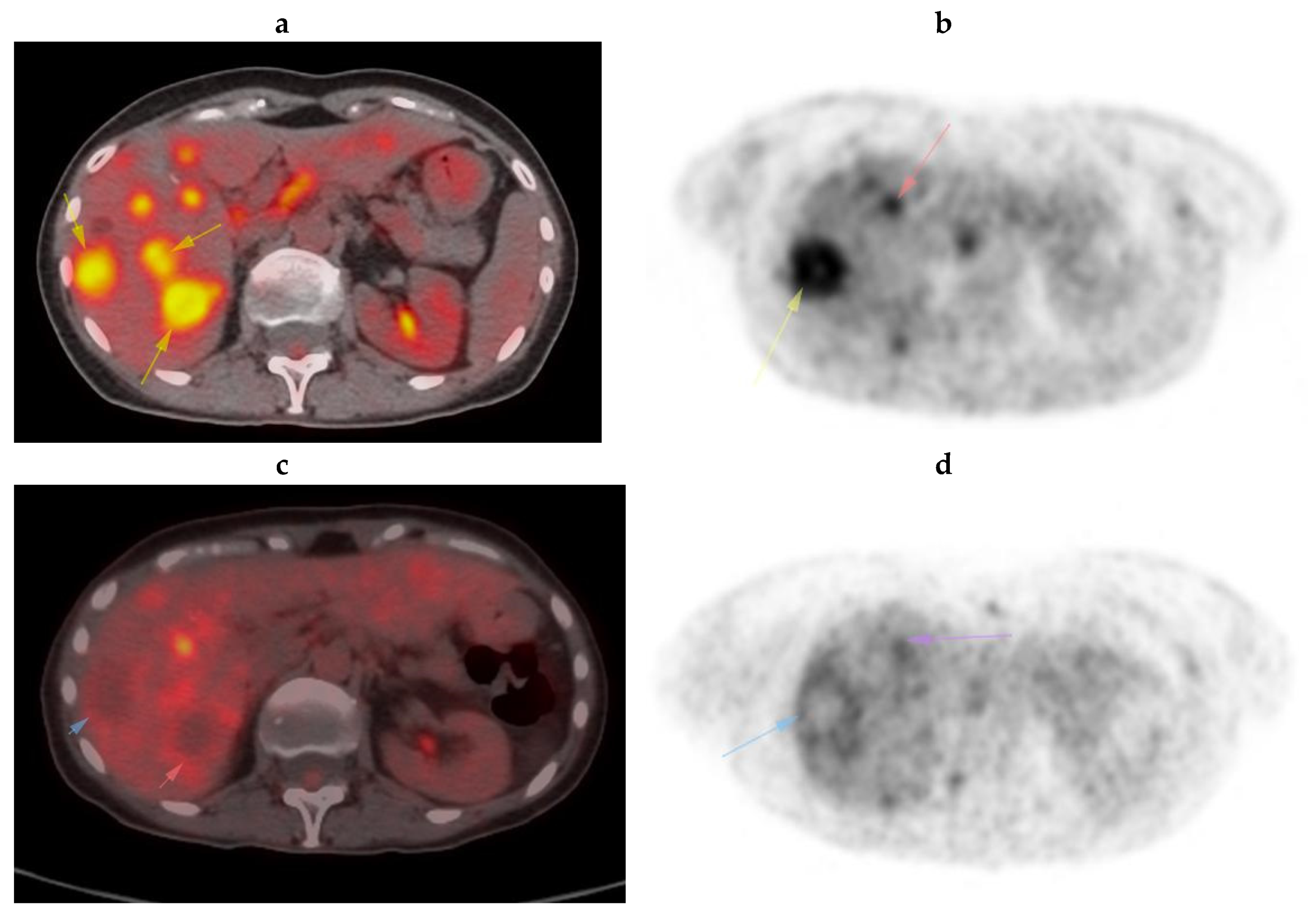
A partial response was observed in the metastatic lesions upon elacestrant plus alpelisib combination. a) July 2023 pet shows lesions in the liver parenchyma at the level of segments 5 and 6 with prominent FDG uptake, consistent with metastasis (arrows – see a vs. c). b) July 2023 PET shows lesions in the liver parenchyma in segments 8 and 4 with prominent FDG uptake, consistent with metastasis (arrows – see b vs. d). c) 3 months later, a significant decrease in the FDG uptake of the lesions was observed, and only peripheral mild FDG uptake is present (arrows). d) PET examination performed 3 months later shows only peripheral mild FDG uptake (arrows).
Figure 2.
A partial response was observed in the metastatic lesions upon elacestrant plus alpelisib combination. a) July 2023 pet shows lesions in the liver parenchyma at the level of segments 5 and 6 with prominent FDG uptake, consistent with metastasis (arrows – see a vs. c). b) July 2023 PET shows lesions in the liver parenchyma in segments 8 and 4 with prominent FDG uptake, consistent with metastasis (arrows – see b vs. d). c) 3 months later, a significant decrease in the FDG uptake of the lesions was observed, and only peripheral mild FDG uptake is present (arrows). d) PET examination performed 3 months later shows only peripheral mild FDG uptake (arrows).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



