Submitted:
01 August 2024
Posted:
02 August 2024
You are already at the latest version
Abstract
This study aims to evaluate tramadol’s effect during elective ovariectomy in female dogs under general anesthesia with isoflurane, premedicated with 0.025 mg/kg medetomidine IM, 0.2 mg/kg methadone IM and 2 mg/kg ketamine IM. Seventeen female dogs were divided into control (CG) and tramadol (TG) groups. Dogs in the TG also received a 4 mg/kg IV tramadol bolus one minute prior to skin incision. Heart rate (HR), systolic blood pressure, and mean blood pressure were recorded at baseline, skin incision, traction (T1) and clamping (T2) of the right ovarian pedicle, and traction and clamping of the left ovarian pedicle. Tramadol caused a 39.8% (p<0.05) and a 31.9% (p<0.05) HR increase at T1 and T2, respectively, when compared to the CG, which lasted a maximum of eight minutes. Although tramadol has a potential positive chronotropic effect, it can safely provide additional intraoperative analgesia before intense noxious stimuli, for at least seven minutes.
Keywords:
Tramadol
; Methadone
; Ovariectomy
; Analgesia
; Isoflurane
1. Introduction
Tramadol is an atypical opioid that causes activation of the mu-opioid receptors (MOR), inhibition of the norepinephrine and serotonin reuptake on the synaptic cleft, and assistance in serotonin release [1,2,3,4]. Tramadol is a very affordable and available drug (crucial characteristics in low-resource settings), and has a minor occurrence of adverse effects, compared to pure opioid agonists [3]. When tramadol is administered intravenously, it can instantly interact with the MOR, α2-adrenoreceptors and 5-HT receptors providing immediate analgesia [2,4,5,6]. It is metabolized in the liver mainly into inactive metabolites, and once it is metabolized it has a short half-life, conferring this drug an uncertain clinical effectiveness [3,7]. It is effective as an analgesic drug immediately after administration [3] and before metabolization, although its metabolites can also produce some analgesic effect [8]. Following metabolization, tramadol metabolites (mainly M1) contribute to and potentiate the analgesic effect already in place, even though not as markedly in dogs as in other species [1,9]. Although the tramadol metabolite M1 (the main metabolite responsible for tramadol’s analgesic effect) also results from tramadol metabolization in dogs, it reveals to be a minor metabolite in this species, compared to other tramadol metabolites with residual analgesic effect, which limits the analgesic effects of tramadol in dogs [6,10,11,12,13].
The enzymes responsible for tramadol metabolization are encoded by genes which are subject to polymorphisms that may compromise the metabolism of certain drugs. Nonetheless, a polymorphism is not inevitably indicative of a change in the pharmacokinetics of a drug [14]. Humans can be ultra-metabolizers, extensive-metabolizers or poor-metabolizers, which explains the ample variation in their pharmacokinetic response toward tramadol [1,15]. Dogs may endure a similar situation as some breeds have been associated with mutations leading to poor antinociceptive effects. However, additional clinical trials are necessary to confirm and generalize these findings [14,16,17]. Thus, tramadol should not be used as a single analgesic agent in dogs [2,7] and that is why tramadol is proposed as part of a multimodal analgesic approach to dogs in this study. Also, the short analgesic effect of tramadol and its associated minor side effects may be useful for intraoperative preemptive additional analgesia where intense noxious stimulation is expected [3].
Ovariectomy is a surgical procedure considered to cause moderate pain and, thus, needing adequate analgesia [18]. A multimodal pharmacological approach allows reducing drug doses and anesthetic risk, while providing excellent analgesia by targeting different noxious pathways and nociceptive receptors, and potentiating the analgesic effect [19]. The combination of different anesthetic drugs with sedative and analgesic effects, such as α2 agonists, opioids and ketamine, are among the routinely used anesthetic premedication for elective surgery [19].
The aim of this study is to evaluate the analgesic and cardiovascular effects of tramadol during noxious stimulation in female dogs submitted to ovariectomy.
2. Materials and Methods
2.1. Animals
The inclusion criteria for this study were healthy female dogs from all breeds, American Society of Anesthesiologists (ASA) physical status I-II, aged between six months to eight years old, scheduled for routine ovariectomy at the Portimão Veterinary Hospital. According to the Portuguese legislation Decree-Law nº 113/2013, which transposes to the legal order Directive Nº2010/63/EU of the European Parliament, and of the Council of 22nd September 2010 on the protection of animals used for scientific purposes, this routine clinical study is excluded from the scope of the mentioned Decree-Law ((lines b) and f) of the point 7)), meaning that ethics approval from legal entities was not required for this routine clinical study. Pet guardians were personally informed about the details of the study design, and a declaration of consent was signed before the surgery for each animal included in the study. Animals were submitted to a thorough physical exam. Blood samples were withdrawn from the cephalic vein for hemogram and biochemistry analysis, according to the routine veterinary hospital practice applied to all animals scheduled for anesthetic procedures.
2.2. Anaesthetic Protocol
Animals were randomly assigned into two distinct groups: the control group and the tramadol group. Randomisation was performed by alternately allocating each female dog to one of the study groups, when the surgical procedure was scheduled.
On surgery day, animals had a minimum food fasting period of eight hours. Water was allowed ad libitum until the pre-operative period. A 20G-24G intravenous catheter (Introcan Winged IV Catheter, B. Braun) was introduced in the left cephalic vein of each animal and connected to a fluid delivery line with an initial NaCl 0.9% (B. Braun, Germany) 2 mL/kg/hr delivery rate using an infusion pump (Cygnus Vet Infusion, Servive).
All animals in both groups were premedicated with intramuscular 0.2 mg/kg methadone (Insistor, Richter Pharma, Austria), 0.025 mg/kg medetomidine (Sedator, Dechra, Netherlands) and 2 mg/kg ketamine (Ketamidor, Richter Pharma, Austria) in the longissimus dorsi muscle. Induction of anaesthesia was performed with propofol 1% (Lipuro, Barcelona, Spain) when needed, adjusting the minimum dose to allow for tracheal intubation, followed by trichotomy and asepsis of the surgical area using diluted chlorhexidine gluconate (Clorhexidina, Zoopan, 1%) and 70% alcohol (Aga, Álcool etílico sanitário, 70%). Rescue medication with intravenous methadone 0.1 to 0.2 mg/kg would be administered if systolic blood pressure, mean blood pressure and heart rate values increased 20% or higher when compared to the previous measurement, followed by exclusion of the patient from data analysis. Animals in the tramadol group also received an intravenous 4 mg/kg bolus of tramadol (Tramadol Labesfal, Labesfal, Portugal) one minute prior to skin incision.
The ovariectomy procedures were performed by the same surgeon using a midline approach technique and, for additional postoperative analgesia, a 2 mg/kg robenacoxib (Onsior, Elanco, USA) was administered subcutaneously to all animals when suturing the abdominal wall.
2.3. Anaesthesia Monitoring and Data Collection
During the study period, heart rate (HR), expired carbon dioxide (EtCO2), peripheral oxygen saturation (SpO2), non-invasive systolic (SBP), diastolic (DBP) and mean (MBP) arterial blood pressures, body temperature (TºC) using an esophageal thermometer, respiratory rate (RR) and the isoflurane selected vaporized concentrations (Iso%) were recorded every minute. Arterial blood pressure was measured on the left hind limb at the metatarsal region using a petMAP monitor (petMAP graphic II, Ramsey Medical inc., Cardio Command, USA). The other variables were collected from the hemodynamic monitor Mindray uMEC12 (Shenzhen Mindray Bio-Medical Electronics Co., LTD, China). Animals were mechanically ventilated with a mixture of air and oxygen using a Mindray WATO EX-35 (Shenzhen Mindray Bio-Medical Electronics Co., LTD, China) mechanical ventilator and a Mindray V60 Anaesthetic Vaporizer (Shenzhen Mindray Bio-Medical Electronics Co., LTD, China). Ventilatory parameters were adjusted for each animal to maintain SpO2 values above 95% and EtCO2 values between 40-50 mmHg.
Baseline values (Bas) were recorded for all variables in animals under general anesthesia, one minute before skin incision and, in the tramadol group, before its administration. The response to surgical noxious stimuli was analyzed at skin incision (T0), traction (T1) and clamping (T2) of the right ovarian pedicle, and traction (T3) and clamping (T4) of the left ovarian pedicle.
2.4. Statistical Analysis
Data were tested for normal distribution and homogeneity of variance using the Shapiro-Wilk normality test and Levene’s test, respectively. Repeated measures analysis of variance (ANOVA) with a Greenhouse-Geisser correction and pairwise comparisons with a Bonferroni adjustment were used to compare data within groups. The Mann-Whitney test was used to compare data between groups.
Data are presented as median (interquartile range), and statistical significance is considered when p<0.05. Statistical analysis was performed using the SPSS version 28 for windows.
3. Results
A total of 17 animals were included in the study. No animal required rescue medication.
Eight female dogs were included in the control group, age 1.5 (1) years and weighing 14.7 (8.2) kg. The duration of the study period was 9 (6) min, during which HR was 59 (29) bpm, SBP was 156 (28) mmHg, DBP was 92 (25) mmHg, MBP was 116 (23) mmHg, RR was 12 (0) rpm, EtCO2 was 47 (5) mmHg, SpO2 was 97 (6) % and TºC was 37.7 (1.2) ºC.
Nine female dogs were included in the tramadol group, age 2 (4) years and weighing 8 (22.9) kg. The duration of the study period was 16 (5) min, during which HR was 77 (20) bpm, SBP was 147 (37) mmHg, DBP was 94 (18) mmHg, MBP was 108 (24) mmHg, RR was 12 (0) rpm, EtCO2 was 44 (11) mmHg, SpO2 was 96 (4) % and TºC was 37.3 (0.6) ºC.
No statistically significant differences were observed between groups in the demographic variables and duration of the study period.
Data recorded at baseline, T0, T1, T2, T3 and T4 for control and tramadol groups are presented in Table 1 and Table 2, respectively.
The time elapsed between baseline and each of the recorded times (T0, T1, T2, T3 and T4), for both the control and tramadol groups, is presented in Table 3.

Table 1.
Time elapsed between baseline and skin incision (T0), right ovarian pedicle traction (T1) and clamping (T2), left ovarian pedicle traction (T3) and clamping (T4) in the control and tramadol groups. Data are median (interquartile range).
Table 1.
Time elapsed between baseline and skin incision (T0), right ovarian pedicle traction (T1) and clamping (T2), left ovarian pedicle traction (T3) and clamping (T4) in the control and tramadol groups. Data are median (interquartile range).
| T0 min |
T1 min |
T2 min |
T3 min |
T4 min |
|
|---|---|---|---|---|---|
| Control | 1 (0) | 3 (0) | 3 (1) | 9 (1) | 9 (1) |
| Tramadol | 1 (0) | 7 (0) | 8 (1) | 16 (6) | 17 (6) |
The HR data trend during the study periods in the control group and the tramadol group are reported in Figure 1. It was observed a statistically significant difference between groups in the T1 and T2 study points.
The SBP data during the study periods in the control group and the tramadol group are reported in Figure 2. There were no statistically significant differences between groups.
4. Discussion
In our study, the intravenous administration of 4 mg/kg tramadol to female dogs under general anesthesia with methadone, medetomidine, ketamine and isoflurane caused a 39.8% (p<0.05) and 31.9% (p<0.05) increase in HR at traction (T1) and clamping (T2) of the right ovarian pedicle, respectively, when compared to the control group. This tramadol effect in HR occurred, respectively, 7 (0) and 8 (1) minutes after tramadol administration (one minute before T0), and was not accompanied by an increase in blood pressure values. In the control group, SBP showed a 9.1%, 9.1%, 11.9% and 16.1% increase at T0, T2, T3 and T4, respectively, when compared to baseline values, and near baseline values at T1. MBP showed a 1.3% and an 8.2% decrease at T0 and T1, respectively, and a 0.4%, 5.2% and 3.4% increase at T2, T3 and T4, also respectively, when compared to baseline values. It is important to notice that, despite the significant noxious stimulation associated with the presence of the surgical stimuli between baseline and clamping of the left ovarian pedicle (T4), in the tramadol group the decrease in SBP and MBP only returned to near baseline values at T3 and T4, respectively, 16 (6) minutes and 17 (6) minutes after tramadol administration, also respectively. In the presence of nociception, the increase in HR is accompanied by an increase in blood pressure [20], which indicates that nociception did not occur in the animals of the tramadol group in our study and is not the reason for the increasing in HR.
As tramadol is an interestingly pharmacological complex drug, it is important to review its main actions to better understand the discussion of the results in our study.
Tramadol exists as a racemic mixture, which means that it consists of two enantiomers, (+)-tramadol and (-)-tramadol. The positive enantiomer is more potent than the racemic mixture, but the latter has less abuse potential and fewer adverse effects [1,3,10]. Each mechanism of action is catalyzed by a different enantiomer, which means that all of them are important to provide adequate analgesia [5]. (+)-Tramadol acts mainly on the 5-HT reuptake inhibition and partially on MOR activation. (-)-Tramadol acts mostly on the NE reuptake inhibition. (+)-O-desmethyltramadol (M1) catalyzes the MOR activation, but to a much lesser extent in dogs than in humans, because it is produced in much lower amounts [3]. Thus, tramadol takes part in the antinociceptive effects of the descending inhibitory pathways in the CNS by binding to the MOR opioid receptors on the superficial layer of the dorsal horn of the spinal cord, which block the rostral transmission of the nociceptive impulses [1,4,21]. But due to the small amount of M1 produced in dogs during tramadol metabolization, its main analgesic effect comes mostly from the norepinephrine reuptake inhibition [3].
Tramadol prevents the propagation of impulses on the nerve fiber terminations [4] by increasing the neurotransmitter norepinephrine in the synaptic cleft leading to a decrease or inhibition of the pain perception [5]. The distribution of tramadol leads it to the liver, where metabolization occurs. There, mainly in the microsomes and mitochondria, it undergoes demethylation, oxidation and hepatic conjugation mediated by the Cytochrome P (CYP) 450 different enzymes, producing more than 30 metabolites. Dogs also have CYPs in the intestinal mucosa, which enhance the generation of metabolites. [5,8,9,22] When the CYP2D15 interacts with tramadol through demethylation, it produces the M1 metabolite, which is the main active metabolite in humans and in a variety of species [1,6,8,23], but not in dogs [3]. Further N-demethylation of M1 by CYP2C21 originates N,O-didesmethyltramadol (M5) which has a higher affinity than tramadol for the MOR, but, due to its high polarity, it does not penetrate the blood-brain barrier as easily as M1 [6,8,24]. The elimination of M1 takes only one to two hours, following either oral or IV administration [10,12]. This also contributes to the low utility of this metabolite in producing analgesia as a single drug [1,10,11]. The second tramadol metabolite, N-desmethyltramadol (M2), is the next metabolite to be formed mainly by CYP2B11 and CYP3A12, although CYP2C21 and CYP2D15 also participate. Both M2 and M5 are inactive in dogs, even though they are produced in higher amounts than M1 [6,8], which corroborates the fact that tramadol should not be used as a single analgesic agent in dogs [2,7].
In humans, following a single dose of 100 mg of oral tramadol the bioavailability is 70% [1], while in Beagle dogs following an oral dose of 11.2 ± 2.0 mg/kg, it is 65 ± 38 % [10]. Giorgi et al. (2010) [6] reported a bioavailability of 92 ± 9 % after IM injection of 4 mg/kg, also in Beagle dogs. Additionally, the bioavailability of tramadol in Beagle dogs after intranasal or rectal administration of a 4 mg/kg dose is 32.6 ± 20.6 % [25] and 10 ± 4 % [23], respectively. After intravenous administration in dogs, the tramadol peak plasma concentration (Cmax) will have its maximum effect shortly after administration [23]. Also, following a 4 mg/kg IM administration of tramadol the Cmax obtained was 2.5 ± 0.4 µg/mL with the corresponding time to reach Cmax (Tmax) of 20.4 ± 3 min in Beagle dogs [6]. When given orally at a dose of 11.2 ± 2 mg/kg, the tramadol Cmax was 1.4 ± 0.7 µg/mL with the corresponding Tmax of 62.4 ± 30.6 min [10]. After rectal administration of 4 mg/kg, the tramadol Cmax was 0.1 ± 0.1 µg/mL and the corresponding Tmax was 33.6 min [23]. The Cmax can be altered due to multiple factors inherent to each patient. In any route of administration, the bioavailability and the rate of absorption will have an impact on Cmax. And, if given orally, the presence of food, gastrointestinal transit time and the time of dissolution of the drug form, will also impact the Cmax [10]. Thus, the short tramadol half-life and the associated large standard deviation makes tramadol, ideally by intravenous administration, a suitable drug for short-term analgesic effect or to potentiate the preemptive analgesic multimodal approach for surgical procedures, as in our study.
Tramadol has been reported to have 15% protein binding in dogs [26,27], while in humans it is 20% [1] and it is known for having a high volume of distribution which is in accordance with its high tissue affinity [10,11,23]. Although there are mean values established for tramadol administration, it is important to state that there is considerable inter-individual and inter-species variability, due to the different absorption rates and metabolization [5,12]. In 2017, Simon & Steagall [2] claimed that for dogs, tramadol should be administered in a range of 4-6 mg/kg each six to eight hours. However, in 2019, Kukanich [28] reported that tramadol needed to be administered at doses up to 15 mg/kg each six to eight hours to reach the targeted drug concentrations needed to treat subacute to chronic pain states, which triples the daily dose reported.
In the tramadol group SBP decreased 3.7% and 15.6%, respectively 1 (0) minute (at T0) and 7 (0) minutes (at T1) after tramadol administration, and MBP decreased 7.3% and 11.6% in the same time periods, also respectively. On the other hand, in the control group SBP increased 9.1% and decreased 2.1%, respectively 1 (0) minute (at T0) and 3 (0) minutes (at T1) after baseline, and MBP decreased 1.3% and 8.2% in the same time periods, also respectively. Although the decreases in blood pressure observed in the tramadol group were not statistically significant, they should not be overlooked due to its clinical importance. A clinically relevant decrease in MBP associated with the intramuscular administration of tramadol and medetomidine was also reported by Ronagh et al., 2020 [29].
NE is a neurotransmitter released by the sympathetic nervous system that acts on the α2-adrenoreceptors producing vasoconstriction [30]. Thus, tramadol can also cause vasoconstriction and consequent hypertension due to its action in the inhibition of the NE reuptake on the synaptic cleft, contributing to the NE increased availability in the synaptic cleft [1,2,3,4]. Therefore, it would be expected a synergistic vasopressor effect between tramadol and medetomidine, an α2-adrenergic agonists drug, which would lead to a possible increase in blood pressure [30,31]. But the opposite occurred in the tramadol group in our study. This unexpected response is probably related to the tramadol influence with the serotonin action.
Tramadol also contributes to the serotonin release and to the inhibition of its reuptake on the synaptic cleft [1,2,3,4]. Both contractile and relaxant serotonin receptors were identified in blood vessels, with different balanced effects in different species and in different types of blood vessels [32]. The 5-HT3 receptor, an unusual vasculature serotonin receptor, is associated with smooth muscle relaxant effects of blood vessels, causing a vasodilation effect in some animal species [33,34,35,36,37]. Another hypothesis to explain the blood vessels smooth muscle relaxant effects of serotonin in rat’s hindquarters is via β2 adrenergic stimulation [38,39]. The decrease in arterial blood pressure observed in the tramadol group in our study may have been related with serotonin mediated relaxation of the smooth muscle of the femoral arterial wall, as reported by Philips and colleagues [40] had observed vasodilation effects of intra-arterial serotonin administration in the femoral artery in dogs anesthetized with pentobarbital. In fact, arterial blood pressure was measured on the left hind limb at the metatarsal region in the animals in our study.
In our study, MBP and SBP values were always above 60-70 mmHg and 80-90 mmHg, respectively, the minimum physiologic threshold for blood pressure values below which it is considered hypotension [20]. Also, the noxious stimuli were similar in both groups and the median SBP trend was also similar between groups. SpO2 and EtCO2 values were maintained above 95% and between 40-50 mmHg, respectively, which indicates that hypoxemia and hypercapnia also did not occur [20]. Thus, the increase in HR at T1 and T2 in the tramadol group in our study, when compared to the control group, is likely to be attributed to the reflex response to the decrease in arterial pressure observed in the tramadol group, as tramadol has a minor effect on heart rate in dogs, accordingly with the results published by Itami and colleagues [30].
Even though during the study period SBP and MBP values were above the normotensive range (80-160 mmHg and 70-120 mmHg, respectively) in some animals, both in the control and in the tramadol groups, animals cannot be considered hypertensive because they were physically examined prior to surgery, and their blood pressure values were considered normal [20,41]. Hence it can be concluded that the blood pressure values were elevated probably due to preoperative stressful conditions or due to drug administration, mainly medetomidine that causes peripheral vasoconstriction and increases the blood pressure [42,43].
When choosing to use tramadol as an intraoperative analgesic drug it is important to avoid the association with ondansetron, which can lead to a partially reversion of tramadol analgesic effects [44].
5. Conclusions
Tramadol may be useful as a short-term analgesic drug to potentiate preemptive multimodal intraoperative analgesic approach, with no clinically significant side effects, in surgical procedures where intense noxious stimulation is expected. The observed decrease in arterial pressure and the associated reflex response increase in HR because of tramadol administration may be useful in counteracting the vasopressor and bradycardic effects of α2-agonistic drugs used in anesthetic pre-medication.
Author Contributions
All authors were valuable contributors for this research. All authors have red and agreed to the published version of the manuscript.”
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study because according to the Portuguese legislation Decree-Law nº 113/2013, which transposes to the legal order Directive Nº2010/63/EU of the European Parliament, and of the Council of 22nd September 2010 on the protection of animals used for scientific purposes, this routine clinical study is excluded from the scope of the mentioned Decree-Law ((lines b) and f) of the point 7)), meaning that ethics approval from legal entities was not required for this routine clinical study. Pet guardians were personally informed about the details of the study design, and a declaration of consent was signed for each animal included in the study.
Data Availability Statement
Not applicable.
Acknowledgments
The authors would like to acknowledge Comprehensive Health Research Center (CHRC) and the Department of Veterinary Medicine, University of Évora, Évora, Portugal, and the Portimão’s Veterinary Hospital for providing the means and equipment for the realization of this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Grond, S.; Sablotzki, A. Clinical pharmacology of tramadol. Clin Pharmacokinet 2004, 43, 879–923. [Google Scholar] [CrossRef] [PubMed]
- Simon, B. T.; Steagall, P. V. The present and future of opioid analgesics in small animal practice. Journal of Veterinary Pharmacology and Therapeutics 2017, 40, 315–326. [Google Scholar] [CrossRef] [PubMed]
- Giorgi, M. Tramdol Vs Tapentadol: A new Horizon in Pain Treatment? American Journal of Animal and Veterinary Sciences 2012, 7, 7–11. [Google Scholar] [CrossRef]
- Kindu, T.; et al. Preemptive analgesic effects of tramadol for ovariohysterectomy in bitches. Journal of Veterinary Science & Technology 2018, 9. [Google Scholar] [CrossRef]
- Barbosa, J.; et al. Comparative metabolism of tramadol and tapentadol: a toxicological perspective. Drug Metabolism Reviews 2016, 48, 577–592. [Google Scholar] [CrossRef] [PubMed]
- Giorgi, M.; et al. Pharmacokinetics of tramadol and metabolites after injective administration in dogs. Polish Journal of Veterinary Sciences 2010, 13, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Giudice, E.; et al. Clinical findings in degenerative lumbosacral stenosis in ten dogs. Journal of Veterinary Behavior 2019, 33, 7–15. [Google Scholar] [CrossRef]
- Perez, T.; et al. Tramadol metabolism to o-desmethyl tramadol (M1) and N-desmethyltramadol (M2) by dog liver microsomes: species comparison and identification of responsible canine cytochrome P450s. Drug Metabolism and Disposition 2016, 44, 1963–1972. [Google Scholar] [CrossRef] [PubMed]
- Domínguez-Oliva, A.; et al. Clinical pharmacology of tramadol and tapentadol, and their therapeutic efficacy in different models of acute and chronic pain in dogs and cats. Journal of Advanced Veterinary and Animal Research 2021, 8, 404–422. [Google Scholar] [CrossRef] [PubMed]
- Kukanich, B.; Papich, M. G. Pharmacokinetics of tramadol and the metabolite O-desmethyltramadol in dogs. Journal of Veterinary Pharmacology and Therapeutics 2004, 27, 239–246. [Google Scholar] [CrossRef]
- McMillan, C.; et al. Pharmacokinetics of intravenous tramadol in dogs. The Canadian Journal of Veterinary Research 2008, 72, 325–331. [Google Scholar]
- Kukanich, B.; Kukanich, K.; Rodriguez, J. The effects of concurrent administration of cytochrome P-450 inhibitors on the pharmacokinetics of oral methadone in healthy dogs. Veterinary Anaesthesia and Analgesia 2011, 38, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Saccò, M.; et al. The relationship between blood pressure and pain. Journal of Clinical Hypertension 2013, 15, 600–605. [Google Scholar] [CrossRef]
- Van Hagen, M.; et al. Analysis of polymorphisms of canine cytochrome P450-CYP2D15. Journal of Veterinary Pharmacology and Therapeutics 2020, 43, 602–607. [Google Scholar] [CrossRef] [PubMed]
- Stamer, U. M.; et al. Impact of CYP2D6 genotype on postoperative tramadol analgesia. PAIN 2003, 105, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Martinez, S. E.; et al. Absolute quantitation of drug-metabolizing cytochrome p450 enzymes and accessory proteins in dog liver microsomes using label-free standard-free analysis reveals interbreed variability. Drug Metabolism and Disposition 2019, 47, 1314–1324. [Google Scholar] [CrossRef] [PubMed]
- Schütter, A. F.; Tünsmeyer, J; Kästner, S. B. R. Influence of tramadol on acute thermal and mechanical cutaneous nociception in dogs. Veterinary Anaesthesia and Analgesia 2017, 44, 309–316. [Google Scholar] [CrossRef] [PubMed]
- WSAVA. Guidelines for recognition, assessment and treatment of pain. Journal of Small Animal Practice 2014, 1–59.
- Pieper, K. Perioperative schmerztherapie bei hund und katzeeine Übersicht. Tierarztliche Praxis Ausgabe K: Kleintiere – Heimtiere 2016, 44, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Grubb, T.; et al. 2020 AAHA Anesthesia and Monitoring Guidelines for Dogs and Cats. Journal of the American Animal Hospital Association 2020, 56, 59–82. [Google Scholar] [CrossRef] [PubMed]
- Desmeules, J. A.; et al. Contribution of monoaminergic modulation to the analgesic effect of tramadol. British Journal of Clinical Pharmacology 1996, 41, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Perez Jimenez, t. E.; et al. Identification of canine cytochrome P-450s (CYPs) metabolizing the tramadol (+)-M1 and (+)-M2 metabolites to the tramadol (+)-M5 metabolite in dog liver microsomes. Journal of Veterinary Pharmacology and Therapeutics 2018, 41, 815–824. [Google Scholar] [CrossRef]
- Giorgi, M.; et al. Pharmacokinetics of tramadol and its major metabolites following rectal and intravenous administration in dogs. New Zealand Veterinary Journal 2009, 57, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Zhuo, H.; et al. Distribution, pharmacokinetics and primary metabolism model of tramadol in zebrafish. Molecular Medicine Reports 2016, 14, 5644–5652. [Google Scholar] [CrossRef] [PubMed]
- Di Salvo, A.; et al. Pharmacokinetics and analgesic efficacy of intranasal administration of tramadol in dogs after ovariohysterectomy. Veterinary Anaesthesia and Analgesia 2020, 47, 557–566. [Google Scholar] [CrossRef] [PubMed]
- Holford, S.; et al. Parent-metabolite pharmacokinetic models for tramadol – tests of assumptions and predictions. Journal of Pharmacology and Clinical Toxicology 2014, 2. [Google Scholar] [CrossRef]
- Vettorato, E.; et al. Pharmacokinetics and efficacy of intravenous and extradural tramadol in dogs. Veterinary Journal 2010, 183, 310–315. [Google Scholar] [CrossRef] [PubMed]
- Kukanich, B. Pain Management in Veterinary Species. In Pharmacotherapeutics for Veterinary Dispensing, 1st ed.; Mealey, K. L., Ed.; John Wiley & Sons, Inc.: New Jersey, USA, 2019; pp. 173–188. [Google Scholar]
- Ronagh, A.; et al. Comparison of sedative and some cardiopulmonary effects of intramuscular medetomidine or medetomidine–tramadol in dogs. Veterinary Anaesthesia and Analgesia 2020, 47, 381–384. [Google Scholar] [CrossRef] [PubMed]
- Itami, T.; et al. Cardiovascular effects of tramadol in dogs anesthetized with sevoflurane. Journal of Veterinary Medical Science 2011, 73, 1603–1609. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, V.; et al. Alpha-2 Agonists. Anesthesiology Clinics 2017, 35, 233–245. [Google Scholar] [CrossRef] [PubMed]
- Watts, S. W.; et al. Serotonin and blood pressure regulation. Pharmacological Reviews 2012, 64, 359–388. [Google Scholar] [CrossRef] [PubMed]
- Kemme, M. J. B.; et al. No evidence for functional involvement of 5-HT2B receptors in serotonin-induced vasodilatation in the human forearm. Journal of Cardiovascular Pharmacology 2000, 36, 699–703. [Google Scholar] [CrossRef] [PubMed]
- Bruning, T. A.; et al. No functional involvement of 5-HT receptors in nitric oxide-dependent dilation caused by serotonin in the human forearm vascular bed. Journal of Cardiovascular Pharmacology 1994, 24, 454–461. [Google Scholar] [CrossRef] [PubMed]
- Bruning, T. A.; et al. Serotonin-induced vasodilation in the human forearm is mediated by the nitric oxide pathway. Journal of Cardiovascular Pharmacology 1993, 22, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Blauw, G.; et al. Effects of 5-HT on capillary and arteriovenous anastomotic blood flow in the human hand and forearm and in the pig hind leg. Journal of Cardiovascular Pharmacology 1991, 17, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Blauw, G. J.; et al. Regional Vascular Effects of Serotonin and Ketanserin in Young, Healthy Subjects. Hypertension 1988, 11, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Calama, E.; et al. Effect of 5-hydroxytrytamine on neurogenic vasoconstriction in the isolated, autoperfused hindquarters of the rat. Clinical and Experimental Pharmacology and Physiology 2005, 32, 894–900. [Google Scholar] [CrossRef] [PubMed]
- Calama, E.; et al. 5-Hydroxytryptamine-induced vasodilator responses in the hindquarters of the anaesthetized rat, involve β2-adrenoceptors. Journal of Pharmacy and Pharmacology 2010, 55, 1371–1378. [Google Scholar] [CrossRef] [PubMed]
- Phillips, C. A.; et al. Mechanisms involved in the vasodilator action of 5-hydroxytryptamine in the dog femoral arterial circulation in vivo. European Journal of Pharmacology 1985, 113, 325–334. [Google Scholar] [CrossRef] [PubMed]
- Grimm, K. A.; et al. Lumb and Jone’s Veterinary Anesthesia and Analgesia, 5th ed.; Wiley Blackwell: Iowa, USA, 2015; p. 111. [Google Scholar]
- Giovannitti, J. A.; Thoms, S. M.; Crawford, J. J. Alpha-2 adrenergic receptor agonists: a review of current clinical applications. Anesthesia Progress 2015, 62, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, M. D. A review of the physiological effects of alpha2-agonists related to the clinical use of medetomidine in small animal practice. Canine Veterinary Journal 2003, 44, 885–897. [Google Scholar]
- De Witte, J. L.; et al. The analgesic efficacy of tramadol is impaired by concurrent administration of ondansetron. Anesthesia and Analgesia 2001, 92, 1319–1321. [Google Scholar] [CrossRef]
Figure 1.
Median values trend of heart rate in animals in the control group and in tramadol group at baseline (Bas), skin incision (T0), traction (T1) and clamping (T2) of the right ovarian pedicle, and traction (T3) and clamping (T4) of the left ovarian pedicle. *p<0.05 between groups.
Figure 1.
Median values trend of heart rate in animals in the control group and in tramadol group at baseline (Bas), skin incision (T0), traction (T1) and clamping (T2) of the right ovarian pedicle, and traction (T3) and clamping (T4) of the left ovarian pedicle. *p<0.05 between groups.
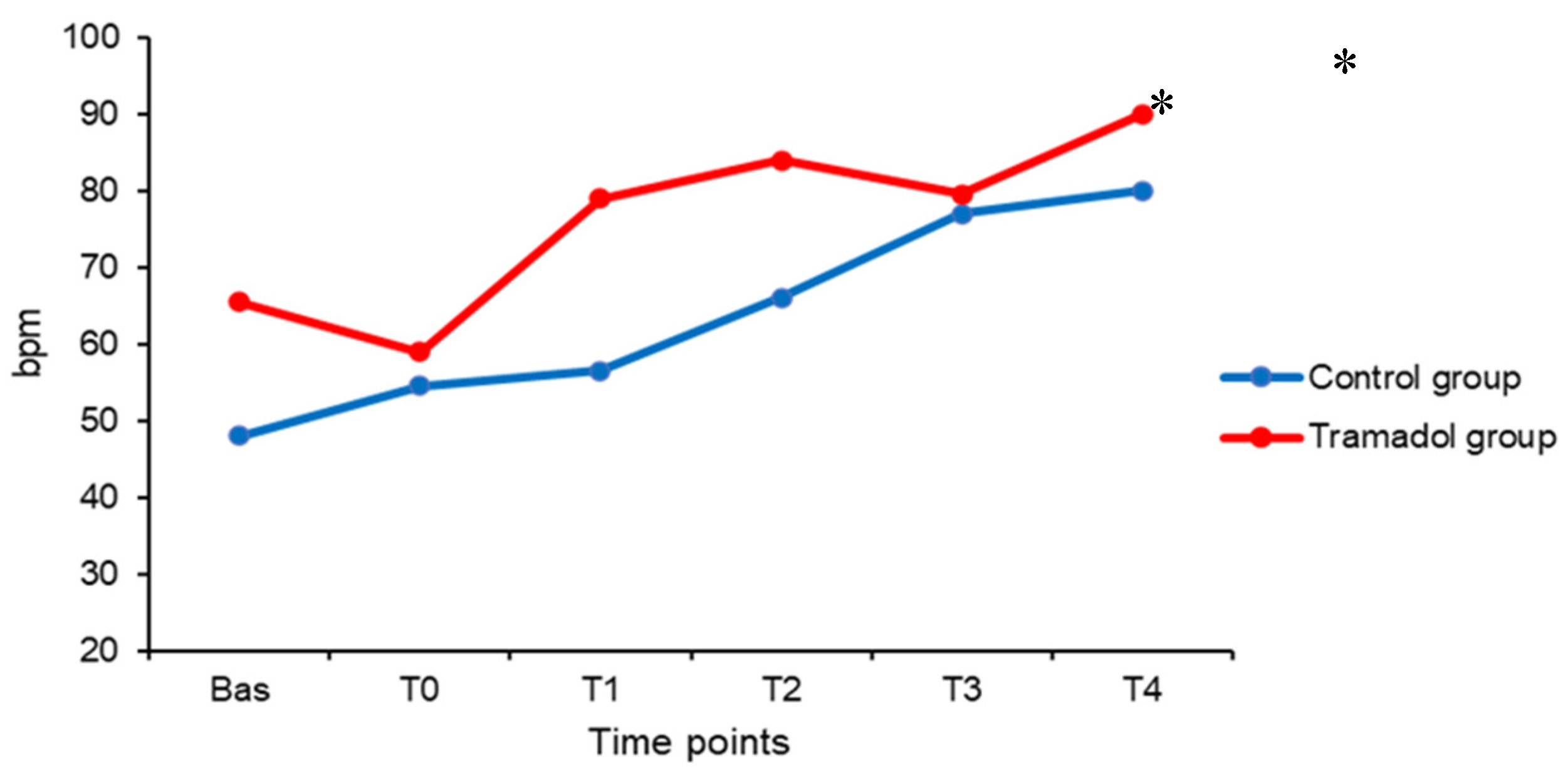
Figure 2.
Median values trend of systolic blood pressure in animals in the control group and in tramadol group at baseline (Bas), skin incision (T0), traction (T1) and clamping (T2) of the right ovarian pedicle, and traction (T3) and clamping (T4) of the left ovarian pedicle.
Figure 2.
Median values trend of systolic blood pressure in animals in the control group and in tramadol group at baseline (Bas), skin incision (T0), traction (T1) and clamping (T2) of the right ovarian pedicle, and traction (T3) and clamping (T4) of the left ovarian pedicle.
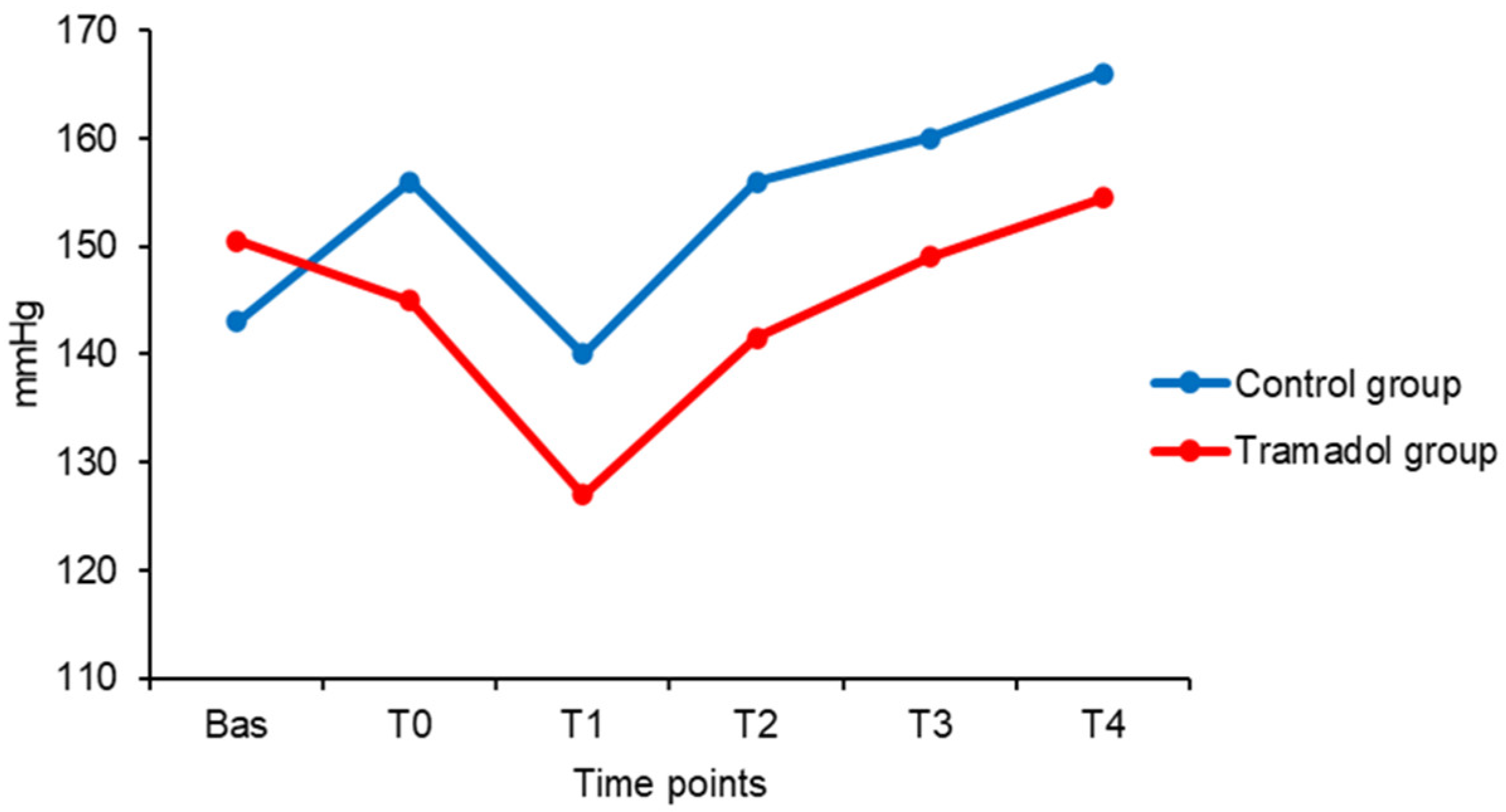
Table 1.
Heart rate (HR), systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial blood pressure (MBP), respiratory rate (RR), expired carbon dioxide pressure (EtCO2), peripheral oxygen saturation (SpO2), body temperature (TºC) and isoflurane concentration (Iso%) from animals in the control group at baseline (Bas), skin incision (T0), traction (T1) and clamping (T2) of the right ovarian pedicle, and traction (T3) and clamping (T4) of the left ovarian pedicle. Data are median (interquartile range).
Table 1.
Heart rate (HR), systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial blood pressure (MBP), respiratory rate (RR), expired carbon dioxide pressure (EtCO2), peripheral oxygen saturation (SpO2), body temperature (TºC) and isoflurane concentration (Iso%) from animals in the control group at baseline (Bas), skin incision (T0), traction (T1) and clamping (T2) of the right ovarian pedicle, and traction (T3) and clamping (T4) of the left ovarian pedicle. Data are median (interquartile range).
| HR bpm |
SBP mmHg |
DBP mmHg |
MBP mmHg |
RR rpm |
EtCO2 mmHg |
SpO2 % |
TºC ºC |
Iso% % |
|
|---|---|---|---|---|---|---|---|---|---|
| Bas | 48 (21) | 143 (39) | 89 (17) | 116 (24) | 12 (0) | 44 (8) | 99 (3) | 38 (1) | 1.5 (0) |
| T0 | 55 (17) | 156 (21) | 90 (24) | 115 (21) | 12 (0) | 47 (8) | 97 (5) | 38 (1) | 1.5 (0) |
| T1 | 57 (17) * | 140 (25) | 90 (32) | 107 (19) | 12 (0) | 48 (8) | 96 (5) | 38 (1) | 1.5 (0) |
| T2 | 66 (11) * | 156 (22) | 92 (18) | 117 (20) | 12 (0) | 46 (10) | 94 (6) | 38 (1) | 1.5 (0) |
| T3 | 77 (33) | 160 (8) | 108 (26) | 122 (25) | 12 (0) | 48 (1) | 98 (5) | 37 (1) | 1.5 (0) |
| T4 | 80 (27) | 166 (23) | 94 (17) | 120 (6) | 12 (0) | 47 (4) | 97 (4) | 37 (1) | 1.5 (0) |
No statistically significant differences were observed within the group for all variables. *p<0.05 when compared to the tramadol group.
Table 2.
Heart rate (HR), systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial blood pressure (MBP), respiratory rate (RR), expired carbon dioxide pressure (EtCO2), peripheral oxygen saturation (SpO2), body temperature (TºC) and isoflurane concentration (Iso%) from animals in the tramadol group at baseline (Bas), skin incision (T0), traction (T1) and clamping (T2) of the right ovarian pedicle, and traction (T3) and clamping (T4) of the left ovarian pedicle. Data are median (interquartile range).
Table 2.
Heart rate (HR), systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial blood pressure (MBP), respiratory rate (RR), expired carbon dioxide pressure (EtCO2), peripheral oxygen saturation (SpO2), body temperature (TºC) and isoflurane concentration (Iso%) from animals in the tramadol group at baseline (Bas), skin incision (T0), traction (T1) and clamping (T2) of the right ovarian pedicle, and traction (T3) and clamping (T4) of the left ovarian pedicle. Data are median (interquartile range).
| HR bpm |
SBP mmHg |
DBP mmHg |
MBP mmHg |
RR rpm |
EtCO2 mmHg |
SpO2 % |
TºC ºC |
Iso% % |
|
|---|---|---|---|---|---|---|---|---|---|
| Bas | 66 (22) | 151 (32) | 98 (13) | 117 (19) | 12 (0) | 44 (11) | 97 (4) | 38 (0) | 1.5 (0) |
| T0 | 59 (22) | 145 (37) | 95 (16) | 108 (31) | 12 (0) | 44 (13) | 97 (4) | 38 (0) | 1.5 (0) |
| T1 | 79 (24) | 127 (29) | 94 (24) | 103 (29) | 12 (0) | 45 (11) | 96 (4) | 37 (1) | 1.5 (0) |
| T2 | 84 (24) * | 142 (29) | 96 (17) | 110 (16) | 12 (0) | 44 (12) | 95 (6) | 37 (0) | 1.5 (0) |
| T3 | 80 (14) * | 149 (32) | 93 (20) | 108 (23) | 12 (0) | 44 (7) | 96 (2) | 37 (0) | 1.5 (1) |
| T4 | 90 (10) | 155 (36) | 92 (17) | 119 (20) | 12 (0) | 44 (7) | 96 (3) | 37 (0) | 1.5 (1) |
No statistically significant differences were observed within the group for all variables. *p<0.05 when compared to the control group.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



