
Submitted:
01 August 2024
Posted:
06 August 2024
You are already at the latest version
Abstract
This study proposes a prototype (Business Intelligence) for monitoring the continuing education of indigenous health professionals at the Secretariat of Indigenous Health (SESAI) of Brazil’s Ministry of Health (MS). The prototype builds on SESAI/MS staff knowledge and takes into account the char-acteristics and demands of the 34 Special Indigenous Health Districts (DSEIs). The prototype provides information for managing SESAI/MS continuing education in order to meet strategic goals. By im-proving the effectiveness and efficiency of the continuing education of professionals who serve Bra-zil’s indigenous population, we will be acting directly on access issues and improving the quality of life of the indigenous population.
Keywords:
Monitoring
; Business Intelligence
; Continuing Education
; Indigenous Health
1. Introduction
Staff continuing education is a permanent demand in public organizations and is fundamental for keeping healthcare professionals qualified, motivated, and well-supported, which directly impacts the health sector performance [1,2]. But continuing education can be complex and involve different demands, such as improving services, keeping up with new procedures and technologies, or simply training new personnel [3]. If health training is complex enough, then imagine the challenge of training professionals who work in indigenous healthcare, which involves different languages, cultures, rituals, and traditions, and where ancient indigenous knowledge of healthcare practices needs to be harmonized with conventional medicine practices [4,5,6].
Given these unique features and challenges, it is essential to maintain continuing education for these professionals in order to increase the effectiveness of the service provided in terms of indigenous healthcare. This requires integrating universal healthcare knowledge with indigenous customs and knowledge [7]. While improvements in indigenous peoples’ healthcare indicators have been observed in Brazil [8], many obstacles still need to be overcome, such as communication and training for healthcare professionals [9], among other aspects. Professionals need to gain qualifications and participate in continuing education activities to overcome the difficulties encountered in healthcare for indigenous peoples [10].
Previous studies point out the relevance of cultural knowledge in healthcare [11,12]. The prominence of this issue is also a reality in Brazil, considering that indigenous people possess a significant social diversity, comprising 305 ethnic groups who speak 274 languages [13]. This underscores the need for specialized healthcare training that respects indigenous peoples’ ethnic, cultural, and linguistic specificities [14,15]. Both the Federal Constitution of Brazil [16] and the 2008 United Nations Declaration [17] establish that these original peoples have the right to access all healthcare services without suffering discrimination. To achieve this, it is essential to recognize these populations’ specificities and to adapt the healthcare system to these needs [18].
Brazil has the Secretariat of Indigenous Health (SESAI), linked to the Ministry of Health (MS), which is responsible for coordinating and executing the National Healthcare Policy for Indigenous Peoples, and for managing the Indigenous Healthcare Subsystem (SasiSUS) within the Unified Health System (SUS). To address this breadth and diversity, Brazil possesses decentralized management units, i.e., 34 Special Indigenous Health Districts (DSEIs). Each of the 34 DSEIs has local and district councils formed by managers with a central role in implementing indigenous healthcare policies and services [19,20]. Brazil has approximately 1.7 million indigenous people [21], and the DSEIs collectively delivered more than 53.7 million healthcare procedures to this population between 2019 and 2022, which underscores their importance [22]. SESAI/MS has over 22,000 healthcare professionals, 52% of whom are indigenous. It is responsible for providing continuing education to healthcare professionals and for enabling healthcare services to take place in a participatory and differentiated manner, respecting these peoples’ epidemiological and sociocultural specificities [23].
Considering these specificities, indigenous healthcare management requires continuing education monitoring models that are more holistic from the planning stage. These models should consider staff training needs regarding local cultural diversity [24]. The complexity of educational processes with different cultural values becomes a management challenge, requiring the improvement of training instruments in DSEIs across Brazil [25]. To provide answers to this problem, this study proposes a prototype (Business Intelligence) for monitoring the continuing education of indigenous health professionals at the Secretariat of Indigenous Health (SESAI) of Brazil’s Ministry of Health.
This prototype is expected to establish a tool that provides indicators to manage continuing education at SESAI/MS in order to meet the strategic goals established. To that end, we resorted to previous literature that shows that using Business Intelligence (BI) techniques can be a viable solution for complex management problems, a solution that has brought beneficial results in several areas, including healthcare. The use of BI can contribute to operational efficiency, resource optimization, and management improvements [26,27] as it facilitates overcoming the challenges faced by indigenous communities. Therefore, by proposing to monitor the continuing education of healthcare professionals who serve Brazil’s indigenous population, we will be dealing directly with aspects that can reduce health inequalities, such as a greater understanding of indigenous culture, which improves indigenous healthcare [28].
2. Materials and Methods
2.1. Breadth of Business Intelligence
The prototype builds on SESAI staff knowledge and takes into account the characteristics and demands of the DSEIs, Indigenous Health Support Houses (CASAIs), and the Work Management and Health Education Division (DIGED). It was designed for application at a national level, aiming to serve the 34 districts, which are strategically divided across the Brazilian territory, taking into account the geographic distribution of indigenous communities, as highlighted in colors in Figure 1.
2.2. Participants
The activities conducted from 01.01.2024 to 12.07.2024 at the Ministry of Health’s Secretariat of Indigenous Health (SESAI/MS) were aimed at improving the monitoring of training and continuing education provided to SESAI/MS personnel. The team who created the prototype is made up of 4 researchers from a Brazilian federal university and 4 employees from the Ministry of Health. Documents relating to courses already offered to staff were also used to scale the components and metrics for creating the prototype (BI). These participants were strategically selected due to their skills, and they are directly involved in the monitoring process and continuing education.
2.3. Data Base and Process
The prototype development process used information from meetings with those responsible for the continuing education process, as well as document analysis (strategic goals, course sheets, etc.) and interviews with managers. The prototype building process consists of 3 stages: (1) goal-setting, (2) development, and (3) validation. The first stage (goal-setting) used brainstorming with SESAI/MS managers to understand the problems and receive course demands. The second stage (prototype development) was carried out to build a BI prototype. Meetings were held between the university’s research team and SESAI/MS managers to build and validate the dashboard structure, and BI usability tests were also carried out. There was considerable feedback and several adjustments at this stage. The third stage (prototype validation) involved presenting the adjusted dashboards and validating the prototype along with the DIGED managers and the CGPROJ team.
Two interviews were also conducted with the managers responsible for the prototype development process at SESAI/MS. The interviews helped to understand how BI can meet the monitoring requirements of continuing education and thus be useful in decision-making. The interviews allowed capturing problems and improvement opportunities from the interviewees. They also enabled the validation of the prototype during its building process. As a result, the interviews carried out generated important feedback, which allowed for improvements to the prototype.
3. Results and Discussion
The study developed a Business Intelligence prototype for monitoring continuing education for SESAI/MS. The prototype was designed to improve healthcare managers’ work and assist in monitoring and evaluating the continuing education of indigenous health professionals. The prototype was developed in three macro stages as presented below.
3.1. Stage 1—Goal-Setting
At this stage, brainstorming, collective meetings, and document analysis were conducted, in addition to interviews with managers, to identify the motivations for building the prototype. As a result, demand was found to arise from several aspects, such as: staff turnover, cultural diversity, lack of systematized training management, a need for qualitative information on the results achieved through the training provided, the unique characteristics of the services provided to the indigenous population, financial responsibility, among others. For illustration purposes, we transcribed some excerpts from the interviews with managers about the motivations for building the BI. The interviewees state that having a space to integrate information is important:
INTERVIEW 1: “...we already have listening time, there’s space for that already, but we don’t have a tool that guarantees that we can see where we need alignment...”,
INTERVIEW 2: “... I think that a tool that centralizes, categorizes, and standardizes can help SESAI find this direction and even standardize it...”
The interviewees also express their concern about cultural specificities, which are relevant considerations:
INTERVIEW 1: “...The indigenous population has a great uniqueness and cultural wealth. So, any and all training must take that into account.... listen to these people, because we would add much more effectiveness to our training, because they have a cultural wealth and knowledge that will add a lot to us....”
INTERVIEW 2: “...the main difference is precisely the cultural aspect in terms of understanding indigenous medicine. What we understand as traditional medicine and the practices of this medicine, care practices and indigenous medicine. So, this understanding is relevant for training management...”
Interviewees also point out aspects like skills mapping and turnover problems as relevant topics that should be better managed:
INTERVIEW 1: “...mapping the necessary skills and abilities, we need to map this and have it in one place... the matrices of skills and abilities that we’ll be able to develop...” “...turnover gets in the way and increasingly demands that we can have better training in what was received in initial training and continuing its processes through a training path...
INTERVIEW 2: “...our biggest problem is this, because we’re not following up, not monitoring, we don’t know who’s been trained, what type of training was done, what the goal was in order to understand results and impact and then see whether turnover’s a problem or not.”
Considering these motivations, and based on the concepts discussed with the SESAI management group about the form and content of a monitoring platform, this study built a monitoring prototype based on a business intelligence platform. BI was chosen in order to improve the management and allocation of resources for the training of healthcare professionals, corroborating the findings of [27].
3.2. Stage 2—Prototype Development
The prototype was developed through a process structured in two phases: 1st—Data Input, and 2nd—Dashboard processing and creation, as shown in Figure 2. In the Data Input phase, internal documents with data on the training of health professionals were analyzed, namely: 1—Course monitoring spreadsheet, 2—People registration spreadsheet, and a training evaluation response spreadsheet.
The second phase was carried out by the dedicated team and included treating and creating the dashboard. The tasks consist of treating the data, creating the dashboards, a validation process with the SESAI/MS team and, finally, sharing. The prototype presented here was developed through a process structured in two phases, as described below in Figure 2.
The dashboards allow monitoring both quantitatively (Table 1 and Figure 2) and qualitatively (Table 2 and Figure 3) and provide additional data (Figure 4 and Figure 5). This allows to monitor information about the continuing education carried out at SESAI/MS.
Since it is an interactive dashboard, users can enhance information, either by applying filters (course, goal, and modality) or by fixing the cursor on a list of courses where a window opens with detailed information (e.g., start and end date, percentage of completers, modality, total course hours, teacher, and content) (Table 2 and Figure 4).
The dashboard also allows monitoring trained students’ evaluation using scores by course, in terms of content, format, methodological approach, time, period (morning/afternoon/evening), and frequency, among other information (Figure 5).
3.3. Stage 3—Prototype Validation
Given the need to improve the evaluation of the courses offered, a module can be adopted for issuing specific periodic reports in order to monitor and evaluate course performance. At the end of the prototype construction process, validation steps were carried out with the SESAI/MS team to identify the reach, adherence and contribution of the prototype to the demands for continuing education. Initial interviews and tests indicate that the model is both usable and relevant. First, it gives continuing education managers a systemic vision by centralizing information about demands, courses already offered, people trained, and topics of interest to the indigenous population. This information is crucial for decision-making at SESAI/MS, as described by the area managers:
INTERVIEW 1: “...we use a government platform, but there’s still a quantitative issue... it’s based on the question of the aggregate population number... but from a qualitative point of view, we don’t have it,... so it’s from this perspective that we think BI can help us work on this qualitative issue...”
INTERVIEW 2: “...the tool has the potential to centralize information about training and qualification, because currently it is dispersed, both within DSEIs and internally at SESAI...”
“...I think that a tool that centralizes, categorizes, and standardizes helps SESAI to have this direction and even better standardize the entire training process that must be carried out by SESAI. No matter what we hire an institution to do, the content decision has to be made by SESAI...”
It also expands managers’ knowledge about assertiveness in training according to the indigenous population itself, where issues of culture and tradition often surpass the scientific rules dealt with in conventional medicine. For example, excerpts 3 and 4 of the interview with the SESAI/MS manager demonstrate the concern with addressing the sociocultural issues of the indigenous population:
INTERVIEW 1: ”...It’s very rich when they are involved,... They have ancient wisdom, you see there a person with philosophy and such a significant capacity for life, training can help in re-signifying traditional issues from the indigenous culture...
INTERVIEW 2: “...that the main difference is precisely the cultural issue in the sense of understanding indigenous medicine. What we understand as traditional medicine and the practices of this medicine, care practices and indigenous medicine. So, this understanding of what something is and the importance of bringing this to the indigenous population, so that it is easy to understand and, not only understand, but also execute...”
“...we are very focused sometimes on certification, on the scientific viability of a certain issue and, for them, other factors are involved. So, how to articulate one thing with another, I think this is one of the main factors...”
Finally, it is possible to observe in the interviews that BI can bring productivity gains, as it is possible to know the demands in advance, as well as monitor the results achieved. This can also contribute to the development of public policies that are suitable for the continuing education of indigenous health professionals.
INTERVIEW 1: ”... the tool allows us to have this from a qualitative point of view...
INTERVIEW 2: “...this tool can bring management to training, management in the sense of understanding this, of us being able to understand if we are achieving the result we want with training, if we are training sufficient numbers, if the issue of turnover is a problem or not, so that we can have a program, a specific policy, the characterization of this problem and have a policy specifically aimed at it...”
Therefore, the prototype (Business Intelligence) for monitoring the continuing education of indigenous health professionals, allows integrating technologies, improves operational and strategic training processes, provides a replicable model for analyzing and monitoring performance indicators, and assists in formulating public policies.
4. Conclusions
The present study proposes a prototype (Business Intelligence) for monitoring the continuing education of indigenous health professionals at the Secretariat of Indigenous Health (SESAI) of the Brazilian Ministry of Health. To achieve this proposal, we draw on previous literature that reveals that the application of Business Intelligence (BI) techniques is suitable for solving complex problems in the healthcare area [29].
The results revealed that continuing education for SESAI/MS professionals is complex and requires constant updating. This corroborates the findings of [10] when revealing that continuing education is important for health professionals to be able to provide assistance in a transcultural manner, understanding the health-disease process, but respecting the cultural diversity and customs of the indigenous population.
Practical contributions involve the use of information generated from the proposed Power BI dashboard, which allows a systemic visualization of performance indicators. This facilitates the decision-making process of managers, in addition to ensuring that continuing education and training courses are directed in a more efficient and effective way. The use of Power BI proved to be a friendly and efficient tool in identifying needs and trends linked to health, as identified in studies by [30] and [31], especially strategic ones such as training and continuing education [32].
Among the limitations, we can highlight the prototype’s application in a single sector and unique context (indigenous health). By concentrating the study on SESAI/MS, this allows us to acquire in-depth knowledge of continuing education; however, it requires caution as to the generalization of results. Future studies can apply the methodology to validate it in other sectors and contexts, which is essential for providing greater external validity to the proposed prototype (BI). The study also carried out interviews (two) with managers in the area of continuing education in indigenous health, the collected information being perceptions (self-reports). Future research can analyze the perceptions of other managers responsible for continuing education, which includes the perceptions of the professionals taking the courses (students) and those responsible for training them (teachers).
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
References
- Deriba BK, Sinke SO, Ereso BM, Badacho AS. Health professionals’ job satisfaction and associated factors at public health centers in West Ethiopia. Hum Resour Health. 30 de maio de 2017;15(1):36. [CrossRef]
- Lunkes RJ, Naranjo-Gil D, Lopez-Valeiras E. Management Control Systems and Clinical Experience of Managers in Public Hospitals. Int J Environ Res Public Health. abril de 2018;15(4):776. [CrossRef]
- Shiri R, El-Metwally A, Sallinen M, Pöyry M, Härmä M, Toppinen-Tanner S. The Role of Continuing Professional Training or Development in Maintaining Current Employment: A Systematic Review. Healthcare. janeiro de 2023;11(21):2900. [CrossRef]
- Carrie H, Mackey TK, Laird SN. Integrating traditional indigenous medicine and western biomedicine into health systems: a review of Nicaraguan health policies and miskitu health services. Int J Equity Health. 14 de dezembro de 2015;14(1):129. [CrossRef]
- Mzimela JH, Moyo I. On the Efficacy of Indigenous Knowledge Systems in Responding to the COVID-19 Pandemic: Unsettling Coloniality. Int J Environ Res Public Health. junho de 2024;21(6):731. [CrossRef]
- Parter C, Gwynn J, Wilson S, Skinner JC, Rix E, Hartz D. Putting Indigenous Cultures and Indigenous Knowledges Front and Centre to Clinical Practice: Katherine Hospital Case Example. Int J Environ Res Public Health. janeiro de 2024;21(1):3. [CrossRef]
- Quadros FAA. Análise das práticas dos(as) enfermeiros(as) indígenas das etnias Guarani, Kaiowá e Terena na perspectiva do cuidado cultural [Internet]. [s.n.]; 2016 [citado 27 de julho de 2024]. Disponível em: https://repositorio.unicamp.br/acervo/detalhe/979304.
- Wenczenovicz TJ. Saúde indígena: reflexões contemporâneas. Indians health: contemporary reflections [Internet]. 2018 [citado 29 de julho de 2024]; Disponível em: https://www.arca.fiocruz.br/handle/icict/63940.
- Sandes LFF, Freitas DA, Souza MFNS de, Leite KB de S. Atenção primária à saúde de indígenas sul-americanos: revisão integrativa da literatura. Rev Panam Salud Pública. 18 de outubro de 2018;42:e163.
- Silva EC da, Silva NCD de L e, Café LA, Almeida PMO de, Souza LN de, Silva AD da. Dificuldades vivenciadas pelos profissionais de saúde no atendimento à população indígena. Rev Eletrônica Acervo Saúde. 7 de janeiro de 2021;13(1):e5413.
- Clifford A, McCalman J, Bainbridge R, Tsey K. Interventions to improve cultural competency in health care for Indigenous peoples of Australia, New Zealand, Canada and the USA: a systematic review. Int J Qual Health Care. 1o de abril de 2015;27(2):89–98. [CrossRef]
- Truong M, Paradies Y, Priest N. Interventions to improve cultural competency in healthcare: a systematic review of reviews. BMC Health Serv Res. 3 de março de 2014;14(1):99. [CrossRef]
- Agência de Notícias—IBGE [Internet]. 2012 [citado 27 de julho de 2024]. Censo 2010: população indígena é de 896,9 mil, tem 305 etnias e fala 274 idiomas | Agência de Notícias. Disponível em: https://agenciadenoticias.ibge.gov.br/agencia-sala-de-imprensa/2013-agencia-de-noticias/releases/14262-asi-censo-2010-populacao-indigena-e-de-8969-mil-tem-305-etnias-e-fala-274-idiomas.
- Thackrah RD, Thompson SC. Refining the concept of cultural competence: building on decades of progress. Med J Aust. 2013;199(1):35–8. [CrossRef]
- Lepesteur JD. A ATENÇÃO INTEGRAL EM SAÚDE JUNTO AOS INDÍGENAS. Rev FOCO. 24 de abril de 2024;17(4):e4959–e4959.
- Constituição [Internet]. [citado 27 de julho de 2024]. Disponível em: https://www.planalto.gov.br/ccivil_03/constituicao/constituicao.htm.
- UNFPA Brasil [Internet]. 2016 [citado 29 de julho de 2024]. Declaração das Nações Unidas sobre os Direitos dos Povos Indígenas. Disponível em: https://brazil.unfpa.org/pt-br/publications/declara%C3%A7%C3%A3o-das-na%C3%A7%C3%B5es-unidas-sobre-os-direitos-dos-povos-ind%C3%ADgenas.
- Cardoso MD. Saúde e povos indígenas no Brasil: notas sobre alguns temas equívocos na política atual. Cad Saúde Pública. abril de 2014;30:860–6.
- Becker LA, Loch MR, Reis RS. Barreiras percebidas por diretores de saúde para tomada de decisão baseada em evidências. Rev Panam Salud Pública. 3 de maio de 2018;41:e147.
- Cavalcanti PC da S, Oliveira Neto AV de, Sousa MF de. Quais são os desafios para a qualificação da Atenção Básica na visão dos gestores municipais? Saúde Em Debate. junho de 2015;39:323–36.
- Agência de Notícias—IBGE [Internet]. 2023 [citado 27 de julho de 2024]. Brasil tem 1,7 milhão de indígenas e mais da metade deles vive na Amazônia Legal | Agência de Notícias. Disponível em: https://agenciadenoticias.ibge.gov.br/agencia-noticias/2012-agencia-de-noticias/noticias/37565-brasil-tem-1-7-milhao-de-indigenas-e-mais-da-metade-deles-vive-na-amazonia-legal.
- Ministério da Saúde [Internet]. [citado 27 de julho de 2024]. Saúde indígena: mais de 53,7 milhões de atendimentos foram realizados em quatro anos. Disponível em: https://www.gov.br/saude/pt-br/assuntos/noticias/2022/dezembro/saude-indigena-mais-de-53-7-milhoes-de-atendimentos-foram-realizados-em-quatro-anos.
- Ministério da Saúde [Internet]. [citado 29 de julho de 2024]. Saúde Indígena. Disponível em: https://www.gov.br/saude/pt-br/composicao/sesai/saude-indigena.
- Xu H, Yuan F, Xie T. Intelligent Study on the Opening and Selecting Course Management Model of URP System Based on Individual Preference. Em: 2020 International Symposium on Advances in Informatics, Electronics and Education (ISAIEE) [Internet]. 2020 [citado 27 de julho de 2024]. p. 1–5. Disponível em: https://ieeexplore.ieee.org/document/9403267.
- Coimbra Junior CEA, Santos RV, Escobar AL, Associação Brasileira de Pós-Graduação em Saúde Coletiva, organizadores. Epidemiologia e saúde dos povos indígenas no Brasil. Rio de Janeiro, RJ: Editora Fiocruz : ABRASCO; 2003. 257 p.
- Ramalingam S, Subramanian M, Sreevallabha Reddy A, Tarakaramu N, Ijaz Khan M, Abdullaev S, et al. Exploring business intelligence applications in the healthcare industry: A comprehensive analysis. Egypt Inform J. 1o de março de 2024;25:100438. [CrossRef]
- Trincanato E, Vagnoni E. Business intelligence and the leverage of information in healthcare organizations from a managerial perspective: a systematic literature review and research agenda. J Health Organ Manag. 1o de janeiro de 2024;38(3):305–30. [CrossRef]
- Azzopardi PS, Sawyer SM, Carlin JB, Degenhardt L, Brown N, Brown AD, et al. Health and wellbeing of Indigenous adolescents in Australia: a systematic synthesis of population data. The Lancet. 24 de fevereiro de 2018;391(10122):766–82. [CrossRef]
- Antunes FM, Gleriano JS, Dias BM, Moura AA, Gasparini LVL. Informação como apoio para tomada de decisão de gestores públicos de saúde. Rev Adm Em Saúde [Internet]. 7 de abril de 2021 [citado 27 de julho de 2024];21(82). Disponível em: https://cqh.org.br/ojs-2.4.8/index.php/ras/article/view/283.
- Ekwebene OC, Umeanowai NV, Edeh GC, Noah GU, Folasole A, Olagunju OJ, et al. The burden of diabetes in America: a data-driven analysis using power BI. Int J Res Med Sci. 30 de janeiro de 2024;12(2):392–6. [CrossRef]
- Graves SM, He L. Covid-19 Mapping with Microsoft Power BI. Terra Digit. 31 de outubro de 2020;1–5. [CrossRef]
- Leão AP da S, Gomes BRA, Cruz JCS, Silva VV da, Sena C da C, Júnior FAVO. POWER BI PARA TOMADA DE DECISÕES ESTRATÉGICAS: ANÁLISE DE INDICADORES-CHAVE DE DESEMPENHO (KPIS). Rev FOCO. 18 de julho de 2023;16(7):e2472–e2472.
Figure 1.
Map of the Special Indigenous Health Districts in Brazil. Source: SESAI (2024).
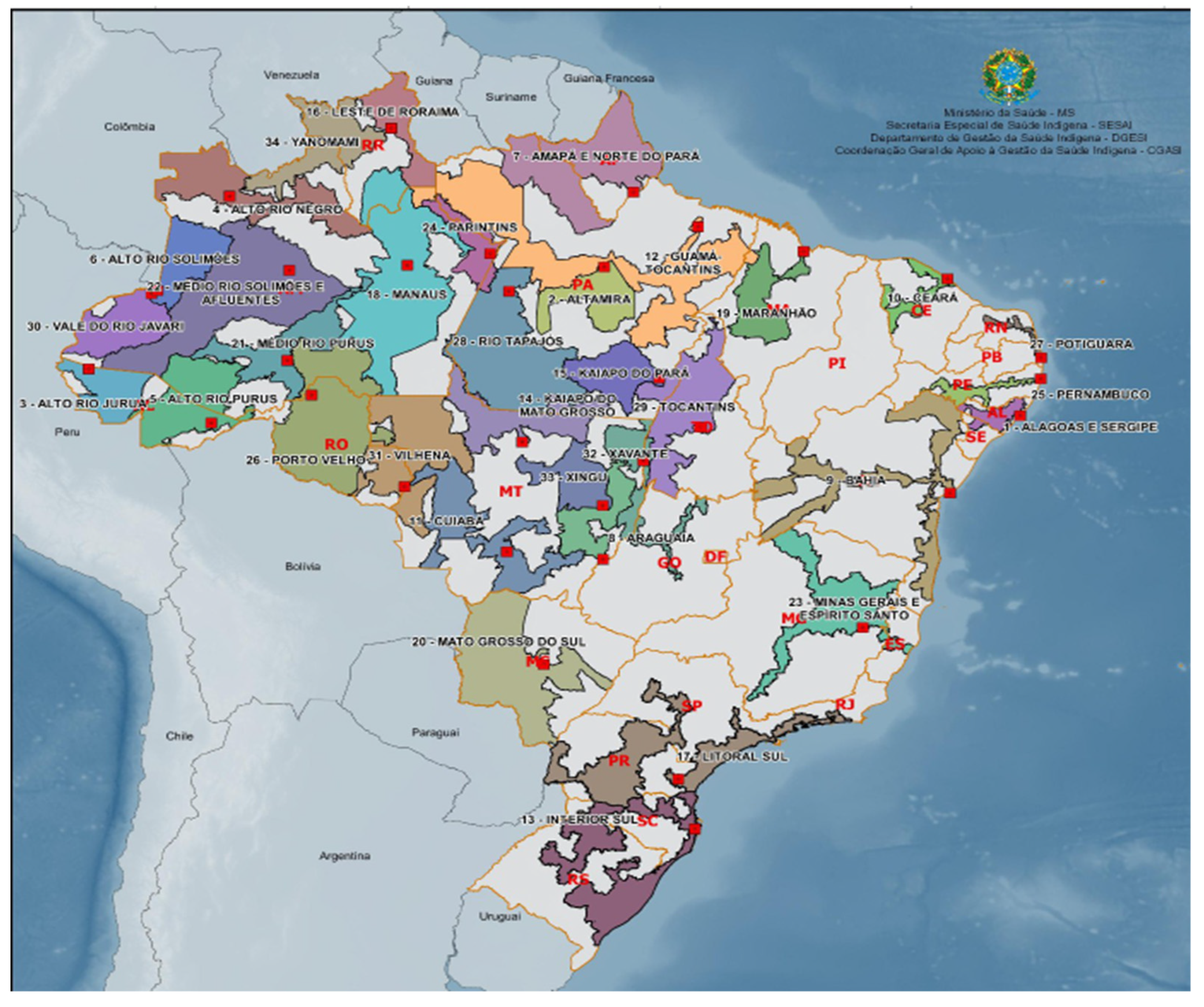
Figure 2.
Prototype development process. Source: research data.
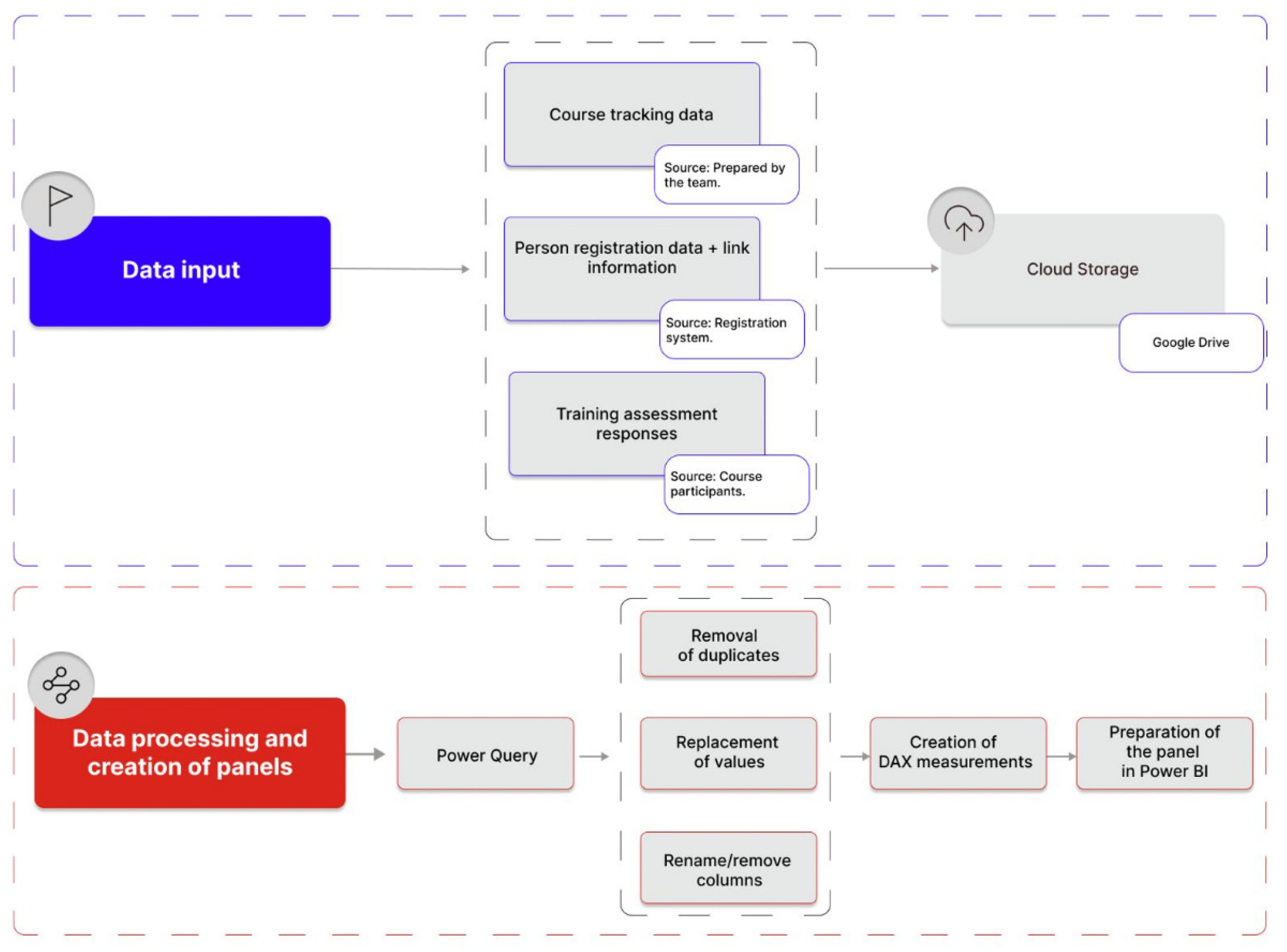
Figure 3.
Prototype of Dashboard 1 (quantitative) for controlling and monitoring continuing education.
Figure 3.
Prototype of Dashboard 1 (quantitative) for controlling and monitoring continuing education.
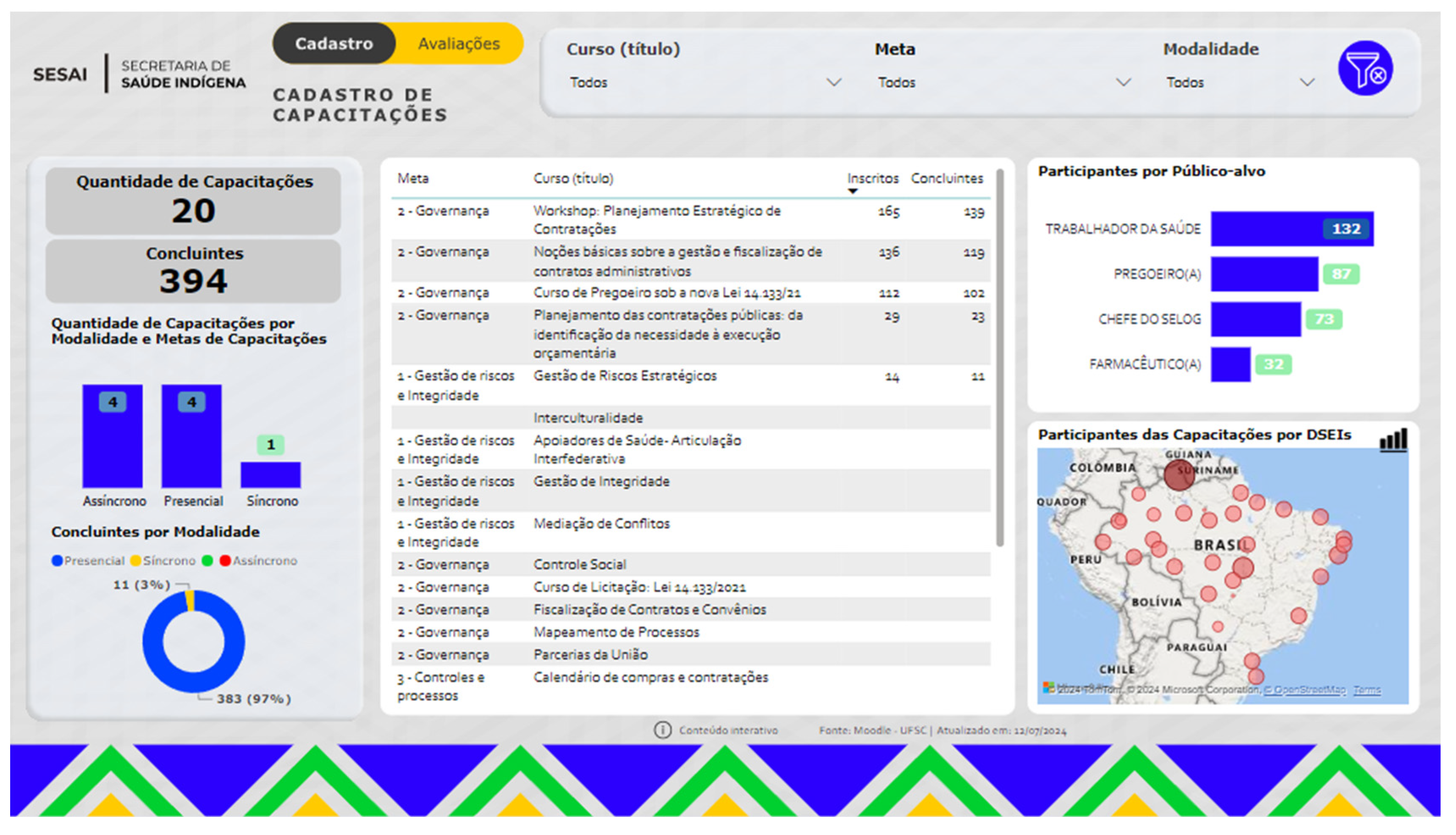
Figure 4.
Prototype of Dashboard 2 (qualitative) for controlling and monitoring continuing education.
Figure 4.
Prototype of Dashboard 2 (qualitative) for controlling and monitoring continuing education.
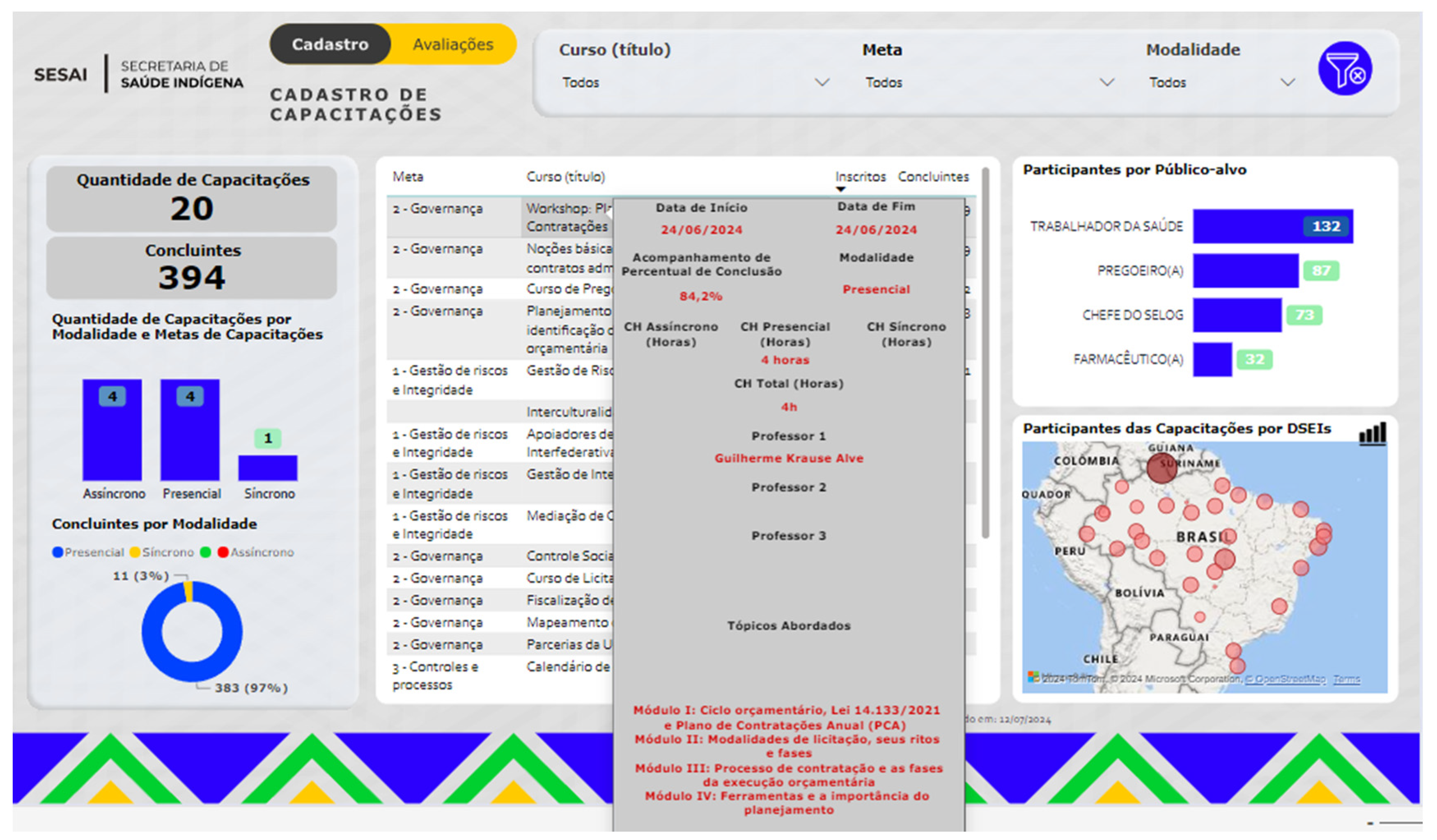
Figure 5.
Prototype of Dashboard 3 (qualitative) for controlling and monitoring continuing education.
Figure 5.
Prototype of Dashboard 3 (qualitative) for controlling and monitoring continuing education.
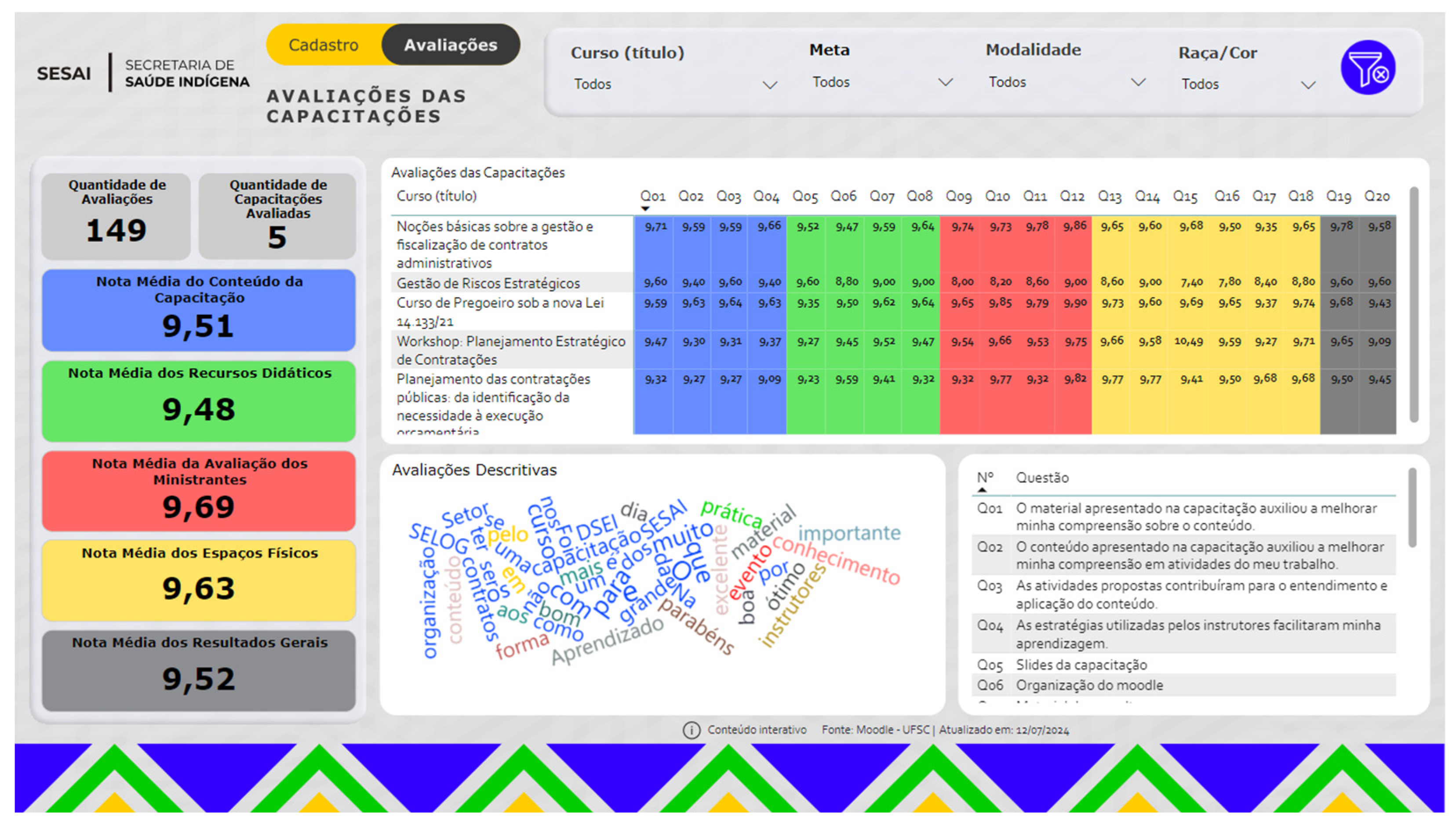

Table 1.
Dashboards structure—quantitative data.
| Dashboard 1—Quantitative | |
|---|---|
| Indicator | Usefulness/Justification |
| Training quantity | Allows quickly viewing the number of training courses executed and planned. |
| Number of completers | Allows quickly identifying the reach that the project is having and, consequently, the number of people certified. |
| Number of training courses by modality | Allows checking whether the designed strategy is being carried out (achieved). |
| Completers by modality | Shows the number of completers by course type (face-to-face, synchronous, and asynchronous courses). |
| List of courses (target, enrollees, and completers) | Allows quickly viewing the courses and topics already offered or planned, and courses that have been completed, by showing the number of enrollees and completers. |
| List of courses with interactive details (date, workload, % completion, modality, teachers and content) | The details allow understanding the course breadth (hours and content). It also shows the proportion of people who enroll and do not complete a course, allowing for timely corrective actions. |
| Participants by target audience | It allows analyzing whether only the central administration is being trained or whether the training also covers operational employees (DSEIs). Also, given the variety of activities carried out by DSEIs, this indicator shows whether all these different functions are being covered. |
| Participants in training by DSEI | Shows the level (e.g., district, region, or national) that courses are reaching. |
| Filter | Usefulness/Justification |
| Course | Allows filtering all information about a given course, such as target audience, region of the country, course modality, number of participants, completers, and content, etc. |
| Target | Allows filtering all information about a given target, such as courses linked to this goal, target audience, region of the country, course modality, number of participants, completers, and content, etc. |
| Modality | Allows filtering information by type of course (face-to-face, synchronous, and asynchronous). |
Table 2.
Dashboard structure—quantitative data.
| Dashboard 2—Qualitative | |
|---|---|
| Indicator | Usefulness/Justification |
| Number of reviews | Allows viewing whether participants are voluntarily evaluating courses in order to generate feedback. |
| Number of courses evaluated | Shows the number of training courses completed and generates a list of evaluations by course. |
| Average score for evaluations of trainers, teaching resources, content, and facility | Each average score card allows identifying the general quality of each analysis construct and evaluating the quality/excellence achieved by the course, while also identifying correction aspects if the averages are not at the expected performance. |
| Average score for general results | In the same way as the other cards, the average score of the general results aims to identify numerically (a score from 0 to 10) the quality of training. However, this card summarizes participants’ perception in relation to the other constructs evaluated. |
| List of training evaluations (course and average score by question) | This table identifies the average scores by question evaluated, thus allowing to specifically analyze which question may have pushed the average (up or down). For example, if the facility received poor ratings, it is necessary to understand whether it was due to its lighting, air conditioning, or another aspect. |
| Word cloud | The word cloud provides an idea of whether participants are bringing more positive or negative words in relation to the general perception of courses. |
| Assessment questions | Allows viewing each (qualitative) evaluation question answered by course participants. |
| Filter | Usefulness/Justification |
| Course | It allows filtering all information about course punctuality, such as the average score a course obtained and what set of words describe it. |
| Target | Allows filtering all information by course target, subdivided by targets that can be translated into themes. |
| Modality | It allows analyzing how course quality is received and perceived in relation to the modality offered (face-to-face, synchronous, and asynchronous). |
| Race/color | Allows filtering all information by the race/color of trained professionals. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



