Submitted:
03 August 2024
Posted:
05 August 2024
You are already at the latest version
Abstract
Background: Pleural effusion (PE) is often classified as either a transudative or an exudative process. The aim of the study was to examine the causes of pleural effusions and the short- and long-term survival in the older patients hospitalized in the acute geriatric and internal medicine wards. Methods: Patients aged ≥ 65 years, who underwent thoracentesis, were included in this retrospective study. To distinguish between exudate and transudate PE, the Light’s criteria were applied. We compared medical indices and mortality in patients with exudate PE to those with transudate effusion according two age groups (65 - 85 vs. > 85 years). Results: The rates of the main etiologies of PE were congestive heart failure (CHF), 46%, lung infections, 25%, and malignancy, 12%, of the whole study population. Lung infections accounted for 53% of the exudate PE patients, with a higher presence among the >85 group of patients. The etiology of transudate PE was primarily CHF, more common among the patients of the >85 group. In malignancy, CHF and lung infections patients, the chances of dying within one year were 80.3%, 63.2%, and 45.5%, respectively. In transudate PE patients, ten-year survival of the 65-85 group of patients was significantly higher. In the exudate PE patients, there was no difference in survival between the two age groups. Right-sided and bilateral pleural effusions were associated with worse prognosis. Conclusion: Clinicians encountering patients with PE should be aware of their heightened mortality risks, and should carefully monitor their underlying etiology and employ appropriate optimal management.
Keywords:
pleural effusion
; older adults
; congestive heart failure
; lung infections
; malignancy
; mortality
1. Introduction
Pleural effusions (PEs) are a common clinical problem in medical practice. PEs result from the accumulation of fluid in the pleural space surrounding the lungs [1]. A pleural effusion (PE) describes an excess of fluid in the pleural cavity, usually resulting from an imbalance in the normal rate of pleural fluid production or absorption, or both [2]. They develop when more fluid enters the pleural space than is removed. Potential mechanisms of pleural fluid accumulation include, among others, increased interstitial fluid in the lungs secondary to increased pulmonary capillary pressure (i.e., heart failure) or permeability (i.e., pneumonia); decreased intrapleural pressure (i.e., atelectasis); decreased plasma oncotic pressure (i.e., hypoalbuminemia); and increased pleural membrane permeability and obstructed lymphatic flow (e.g., pleural malignancy or infection) [3].
The cause of PE is often classified initially as either a transudative or an exudative process, with the former usually associated with cardiac (heart failure), renal, or hepatic dysfunction (cirrhosis), and the latter with conditions that cause an excess of inflammation, such as malignancy or infection [2,3,4]
Transudate effusion results from imbalances in hydrostatic and oncotic forces. It occurs when fluid permeates the pleural cavity via intact pulmonary vessels. In contrast, exudate effusion refers to fluid escaping into the pleural space through lesions in blood and lymph vessels due to inflammation. Exudate effusions occur when the local factors influencing the accumulation of pleural fluid are altered. Pneumonia, malignancy, and thromboembolism account for most exudative effusions in the United States [3].
Malignant PEs are known to be associated with high mortality, but there is increasing evidence that patients with non-malignant PEs also carry a high mortality rate, especially when the PEs are related to congestive heart failure (CHF) [5].
In clinical practice, exudative effusions can be separated effectively from transudative effusions using Light’s criteria. These criteria classify an effusion as exudate if one or more of the following are present: (1) the ratio of pleural fluid protein to serum protein is greater than 0.5; (2) the ratio of pleural fluid lactate dehydrogenase (LDH) to serum LDH is greater than 0.6; or (3) the pleural fluid LDH level is greater than two thirds of the upper limit of normal for serum LDH [3].
Many causes of PEs are recognized, crossing a wide variety of diseases [2]. Epidemiological data on the causes of PEs are scarce [6]. There is also little in the literature regarding mortality of patients with nonmalignant PEs [7]. We have studied the causes of PEs in two age groups of older patients hospitalized in the acute geriatric and internal medicine wards, and calculated ten-year survival of transudate vs. exudate PE.
2. Methods
2.1. Study Design, Setting and Population
We retrospectively surveyed electronic hospital health records of 700 older patients, aged ≥ 65 years old, admitted between the year 2008 and 2018 to the acute geriatric and internal medicine wards, and underwent thoracentesis. The thoracentesis was performed by using ultrasound guidance (Vscan with dual Probe, Software version 1.4, General Electric, Norway). To distinguish between exudate and transudate pleural effusion, the Light’s criteria were applied [8]. Sixty-five patients, in whom some criteria were missing were excluded. The remaining 635 patients were assigned either to exudate or transudate pleural effusion group. In each group, the patients were divided into two age groups, 65 - 85 and > 85 years old. The retrieved data included patient demographics, medical diagnoses, laboratory results and clinical outcomes. We compared mortality in the two age groups of patients (65 - 85 vs. > 85years), with exudate PE to those with transudate PE.
The study was approved by the Institutional Ethics Committee of the Kaplan Medical Center, Rehovot, Israel.
2.2. Statistical Analysis
Data were analyzed, using SPSS version 29.0 program. Categorical and nominal variables were analyzed, using Pearson’s chi-square (χ²) test. A comparison was performed between two age groups using both the chi-square test and the Fisher’s exact test. Continuous variables were presented as means ± standard deviations (SD). The normality of these variables was assessed, using the Kolmogorov-Smirnov test. In cases, in which abnormal distribution was observed, non-parametric tests were conducted. The Mann-Whitney test was used to compare the two age groups. Kaplan-Meier curves were used to describe survival of transudate and exudate pleural effusion older adults within ten years post thoracentesis. The probability of mortality within one year for the disease categories ‒ CHF, pulmonary infection, and malignancy ‒ was calculated, using the following methodology: for each category, only patients for whom the number of days from thoracentesis to the date of death was less than or equal to 365 were selected. The number of patients meeting this criterion was divided by the total number of patients in that category, and the result represents the probability of mortality. By Kaplan Meier analysis, in older adults suffering from malignancy, CHF and lung infections one-year survival post thoracentesis was calculated. P value < 0.05 was considered statistically significant.
3. Results
Selected characteristics of the 653 patients (46% females), stratified according to PE diagnosis and two age groups (65 - 85 and > 85 years), are presented in Table 1. Of the whole group of patients, 47.9% suffered from exudate PE. The mean age of the exudate PE group was 77.0 ± 5.3 in the 65 - 85 and 89.0 ± 7.00 in the > 85 group. The mean age of the transudate PE group was 77.9 ± 4.9 in the 65 - 85 and 89.6 ± 3.70 in the > 85 group. Smoking was more common in the younger group of patients in both the exudate and the transudate PE patients. In the study PE patients, the most common comorbidities were CHF, dyslipidemia, diabetes mellitus, hypertension, atrial fibrillation, and dementia. In the exudate group, except for dyslipidemia and diabetes mellitus, the percentage of the older group with the mentioned comorbidities was higher. In the transudate PE group, as in the exudate PE group, dyslipidemia and diabetes mellitus were more common in the younger group. There was no difference in the presence of the other comorbidities between the two age groups, except for dementia, which was more common in the older group. The exudate and the transudate PE patients did not differ in the laboratory tests results as well as the length of in-hospital stay and the in-hospital mortality rates.
Of the whole study population, the rates of the primary PE etiologies were CHF, lung infections and malignancy, 46%, 25% and 12%, respectively. Lung infections (including pneumonia, empyema and respiratory infections) accounted for 53% of the exudate PE patients, with a higher presence (63.4% vs. 48.1%) among the > 85 age group of patients. Malignancy played a smaller role (24.3% of the exudate PE patients), with no difference between the two age groups.
The etiology of transudate PE was primarily CHF (87.9% of the transudate PE patients), more common (91.8% vs. 84.8%) among the patients of the > 85 age group. Liver failure and renal failure much less contributed to transudate PE (4.8% of the transudate PE patients), more common (13.3% vs. 7.4%) among the 65 - 85 age group of patients (data not shown).
Patients with R-sided PE, were older (82 y vs. 80 y) than those with L-sided effusion, their in-hospital length of stay was longer (14.5 vs. 10 days), and the number of days to death was lower. In addition, their blood urea levels were higher (80 vs. 66 mg/dL) and albumin levels were lower (3.06 vs. 3.09 g/dL), Table 2.
Bilateral PE was present in 32.5%, 19.3% and 5.7% of CHF, lung infections and malignancy patients, respectively (data not shown). In comparison between unilateral vs. bilateral PE, in the latter albumin levels were lower (2.54 vs. 3.07 g/dL) and the length of stay was longer (24.6 vs. 12.7 days). The number of days to death in the bilateral PE patients was almost significantly lower than in those with the unilateral one (179.3 vs. 455.8 days), Table 3. Kaplan Meier analysis did not find difference in one-year survival between bilateral and unilateral PE (data not shown).
In malignancy, CHF and lung infections patients, the chances of dying within one year post thoracentesis were 80.3%, 63.2%, and 45.5%, respectively (Table 4).
By Kaplan Meier analysis, the impact on mortality in exudate and transudate PE, within the two age groups, is illustrated in Figure 1. In transudate PE patients, ten-year survival of the 65 - 85 age group of patients was significantly higher. In the exudate PE patients, there was no difference in survival between the two age groups. In the transudate 65 - 85 and > 85 age group of patients, the probability of survival within one year post thoracentesis was 34.6% and 21%, respectively. In the exudate PE 65 - 85 and > 85 age group of patients, there was no difference in the probability of survival within one year post thoracentesis (33.9% and 32.9%, respectively).
By Kaplan Meier analysis, in older adults suffering from malignancy, one-year survival was the lowest, followed by CHF and lung infections (Figure 2). The probability of survival within one year post thoracentesis was 19.74%, 36.81%, and 54.55% in malignancy, CHF, and lung infections patients, respectively.
4. Discussion
There are limited epidemiological data on the causes of PE [6]. Although many different diseases may cause PE, the most common causes in adults are heart failure, malignancy, pneumonia, tuberculosis, and pulmonary embolism [3]. In our study, similarly to some other studies [6,7], the most prevalent cause of PE was CHF (46%), followed by lung infections (25%), and malignancy (12%). In a non-published Spanish study in octogenarians, heart failure accounted for more than half of all PEs [9]. In CHF patients, in our study, the chances of dying within one year post thoracentesis were 63.2%. In an American study, CHF complicated by PE had 53% one-year mortality [7]. In a British study in younger patients (68 years old) with CHF, the one-year mortality rate was 50% [10].
Exudate PE is most likely to be associated with pneumonia [2]. Pneumonia is the most common etiology of exudative pleural infections, occurring in up to 9% of patients with pneumonia [7,11].
The worldwide incidence of pleural infections has been increasing. An actual increase of the disease may be due to changes in the age distribution of the population, as older age groups are becoming more prominent in many developed countries, and advanced age is associated with several diseases that may predispose to the development of pleural infections. Additionally, male sex, alcoholism, and low socioeconomic status, as well as malignancies and other common comorbidities are associated with higher risk for the development of pleural infections [11].
PE in the setting of pulmonary infection is a poor prognostic sign and is one of the major causes of pulmonary mortality and morbidity [7,12]. In lung infection patients, in our study, the chances of dying within one year post thoracentesis were 45.5%, higher than the finding in a study performed in younger older adults, in whom there was a 26% one-year mortality [7]. However, in a Finnish study of a younger group of patients, 60% of deaths occurred in patients suffering from pulmonary infection complicated by PE. Possible reason for higher mortality rate might be a high prevalence of significant comorbidities in the non-survivors [11].
Malignant PE (MPE) is the second most common exudative PE cause [8]. It is a common clinical problem that can be seen in 15% to 35% of patients diagnosed with cancer [13,14]; [14]. MPE, in our study, accounted for about 24.3% of exudate PE patients. Generally, MPE is associated with poor outcomes [7]. In our study, in malignancy pleural effusion patients, the chances of dying within one year post thoracentesis were 80.3%, similarly to the findings in American and Turkish studies 77% and 84%, respectively [7,13. In two studies, British and Estonian, in younger patients, one-year mortality rate was 70% and 61%, respectively [10,15].
To our knowledge, there is no study comparing the one- and ten-year survival of transudate and exudate PE older patients to a younger group of patients. In our study, in the transudate PE 65 - 85 and > 85 age group of patients, the probability of survival within one year post thoracentesis was 34.6% and 21%, respectively. In the exudate PE 65-85 and > 85 age group of patients, there was no difference in the probability of survival within one year post thoracentesis, 33.9% and 32.9%, respectively. Maybe, because exudate PEs include lung infections and malignancy diseases, which often have worse prognosis than transudate PEs, younger age might not be protective, as indeed described in a Finnish study of a younger group of older patients [11].
Right-sided PE was associated with older age, longer hospital stay length, lower albumin level, higher urea level, and lower survival compared to left-sided PE. To our knowledge, there is no study comparing the health condition of patients suffering from right-sided PE to those with left-sided one. Maybe right-sided effusion is more common in severely ill patients, but as it is a retrospective study, we could not identify them.
Bilateral effusions, in our study, accounted for 44% of pleural effusion patients. Bilateral pleural effusions occur in 15% of the cases in non-critically ill patients, and up to 55% of those in the intensive care population [1,7]. The etiology of bilateral PE includes, among others, CHF, liver and renal failure, and malignancy [7]. In our study, bilateral effusions were present in 32.5%, 19.3% and 5.7% of CHF, lung infections and malignancy cases, respectively. In two studies, Polish and Spanish, higher rates of patients, suffering from CHF, presented with bilateral PE, 51% and 61%, respectively [6,9].
The association between bilateral PE and mortality has been previously reported in few studies [7]. In our study, bilateral PE was almost significantly associated with higher mortality than the unilateral one. However, by Kaplan Meier analysis no significant difference was found between bilateral and unilateral PE. In the Walker et al., study, in non-malignant bilateral exudate and transudate PEs, the risk to die within one year was higher by 3.55 and by 2.78, respectively. Non-malignant bilateral exudate and transudate PEs were associated with a worse prognosis than the unilateral ones, with a 57% and 43% one-year mortality, respectively [10]. In an Israeli study, in acute pulmonary embolism patients, those with bilateral PE had a higher probability for in-hospital death in comparison with patients with unilateral PE [16]. In an American study, bilateral PE was markedly associated with high mortality and had a significantly higher risk of death.
Caregivers encountering patients with diseases complicated by PE should be aware of their heightened mortality risks and aggressive management of the underlying etiology is warranted [7].
Our study has all the disadvantages of a retrospective observational study. We did not have all the data that may have been influencing mortality, because they were not found in the patients’ electronic records. Our study strength lies in its population relatively large size. Since the study focuses on short- and long-term mortality due to diseases complicated by PE in older patients, including the oldest-old, we would like to point out that we have contributed to the medical knowledge concerning this population, whose proportion in the geriatric population is recently significantly increasing.
5. Conclusions
Older PE patients undergoing thoracentesis have high short- and long-term mortality. Although mortality rate was highest in MPE patients, mortality in non-malignant PE in older adults was considerable. Therefore, PE should be considered as a poor prognostic sign. Clinicians encountering patients with PE should be aware of their heightened mortality risks, and should carefully monitor their underlying etiology and employ appropriate optimal management.
Acknowledgments
I would like to thank Felicia Stern, PhD. RD for her assistance in the preparation and editing of this manuscript.
Contribution Statement
Data curation, G.O.; draft preparation, G.O; conceptualization, S.T.; supervision, S.T.; writing ‒ review and editing, S.T; both authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
Institutional Review Board Statement
The study was approved by the Institutional Ethics Committee of the Kaplan Medical Center, Rehovot, Israel.
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the study.
Abbreviations
|
CHF ‒ congestive heart failure PE ‒ pleural effusion PEs ‒ pleural effusions LDH ‒ lactate dehydrogenase MPE ‒ malignant pleural effusion COPD – Chronic Obstructive Pulmonary Disease CVA ‒ cerebrovascular accident CRF – chronic renal failure |
References
- Puchalski, J.T.; Argento, A.C.; Murphy, T.E.; Araujo, K.L.; Oliva, I.B.; Rubinowitz, A.N.; Pisani, M.A. Etiologies of bilateral pleural effusions. Resp. Med. 2013, 107, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Bhatnagar, R.; Maskell, N. The modern diagnosis and management of pleural effusions. BMJ 2015, 351, h4520. [Google Scholar] [CrossRef] [PubMed]
- Porcel, J.M.; Light, R.W. Diagnostic approach to pleural effusion in adults. Am. Fam. Phys. 2006, 73, 1211–1220. [Google Scholar]
- Jany, B.; Welte, T. Pleural effusion in adults—etiology, diagnosis, and treatment. Dtsch Arztebl Int. 2019, 116, 377–386. [Google Scholar] [CrossRef] [PubMed]
- Wijayaratne, T.; Yousuf, A.; Panchal, R. Cardiac related pleural effusions: a narrative review. J. Thorac. Dis. 2014, 16, 1674–1686. [Google Scholar] [CrossRef] [PubMed]
- Korczyński, P.; Górska, K.; Konopka, D.; Al-Haj, D.; Filipiak, K.J.; Krenke, R. Significance of congestive heart failure as a cause of pleural effusion: Pilot data from a large multidisciplinary teaching hospital. Cardiol. J. 2020, 27, 254–261. [Google Scholar] [CrossRef] [PubMed]
- DeBiasi, E.M.; Pisani, M.A.; Murphy, T.E.; Araujo, K.; Kookoolis, A.; Argento, A.C.; Puchalski, J. Mortality among patients with pleural effusion undergoing thoracentesis. Eur. Resp. J. 2015, 46, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Light, R.W. Pleural effusions. Med. Clin. N. Am. 2011, 95, 1055–1070. [Google Scholar] [CrossRef] [PubMed]
- Porcel, J. Pleural effusions from congestive heart failure. Sem. Respir. Crit. Care Med 2011, 31, 689–697. [Google Scholar] [CrossRef] [PubMed]
- Walker, S.P.; Morley, A.J.; Stadon, L.; De Fonseka, D.; Arnold, D.T.; Medford., A.R.L.; Maskell, N.A. Nonmalignant pleural effusions: A prospective study of 356 consecutive unselected patients. Chest 2017, 151, 1099–1105. [Google Scholar] [CrossRef] [PubMed]
- Lehtomäki, A.; Nevalainen, R.; Ukkonen, M.; Nieminen, J.; Laurikka, J.; Khan, J. Trends in the incidence, etiology, treatment, and outcomes of pleural infections in adults over a decade in a Finnish University Hospital. Scand. J. Surg. 2020, 109, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Krishna, R.; Antoine, M.H.; Rudrappa, M.. Pleural Effusion. [Updated 2023 Mar 18]. In StatPearls [Internet]. Treasure Island (FL). StatPearls Publishing, 2024. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448189/.
- Ermin, S.; Özdoğan, Y.; Batum, O.; Yılmaz, U. The role of LENT and PROMISE scores in predicting survival in malignant pleural effusion. Lung India 2022, 39, 325–330. [Google Scholar] [CrossRef] [PubMed]
- Herrera Lara, S.; Fernández-Fabrellas, E.; Juan Samper, G.; Marco Buades, J.; Andreu Lapiedra, R.; Pinilla Moreno, A.; Morales Suárez-Varela, M. Predicting malignant and paramalignant pleural effusions by combining clinical, radiological and pleural fluid analytical parameters. Lung 2017, 195, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Laisaar, T.; Palmiste, V.; Vooder, T.; Umbleja, T. Life expectancy of patients with malignant pleural effusion treated with video-assisted thoracoscopic talc pleurodesis. Interact. Cardiovasc. Thorac. Surg. 2006, 5, 307–310. [Google Scholar] [CrossRef]
- Levy, O.; Fux, D.; Bartsikhovsky, T.; Vosko, S.; Tishler, M.; Copel, L. Clinical relevance of bilateral pleural effusion in patients with acute pulmonary embolism. Inter. Med. J 2020, 50, 938–944. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Kaplan Meier Cumulative Survival Curve by exudate and transudate pleural effusions within the two age groups.
Figure 1.
Kaplan Meier Cumulative Survival Curve by exudate and transudate pleural effusions within the two age groups.
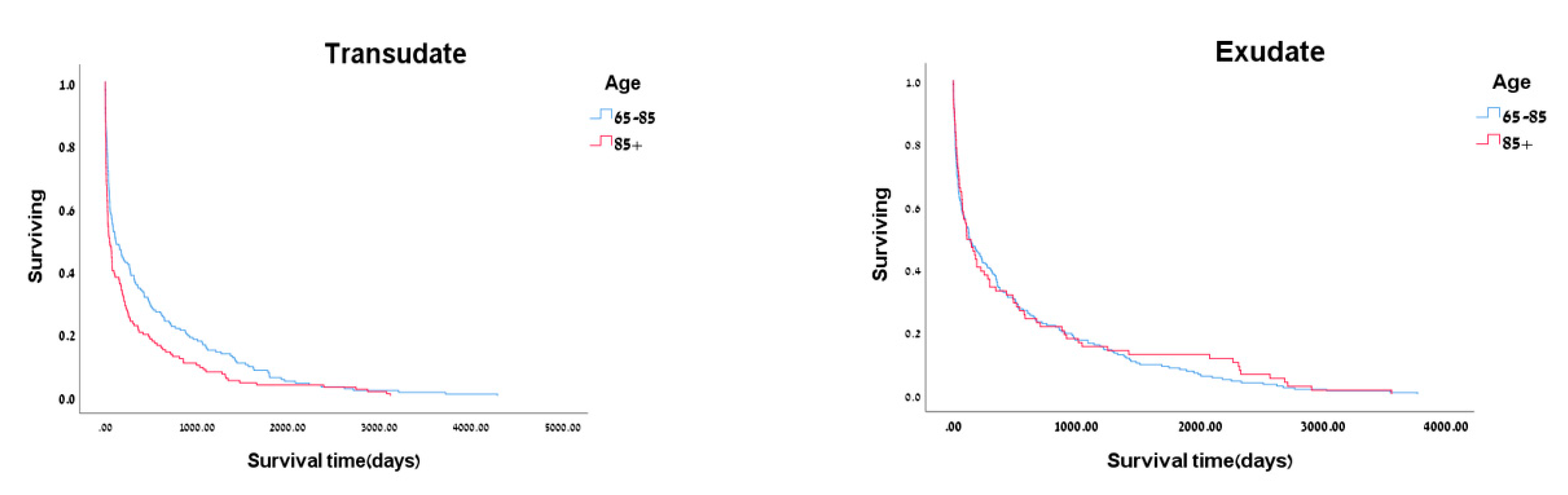
Figure 2.
Kaplan Meier cumulative one-year survival curve by malignancy, CHF and lung infections.
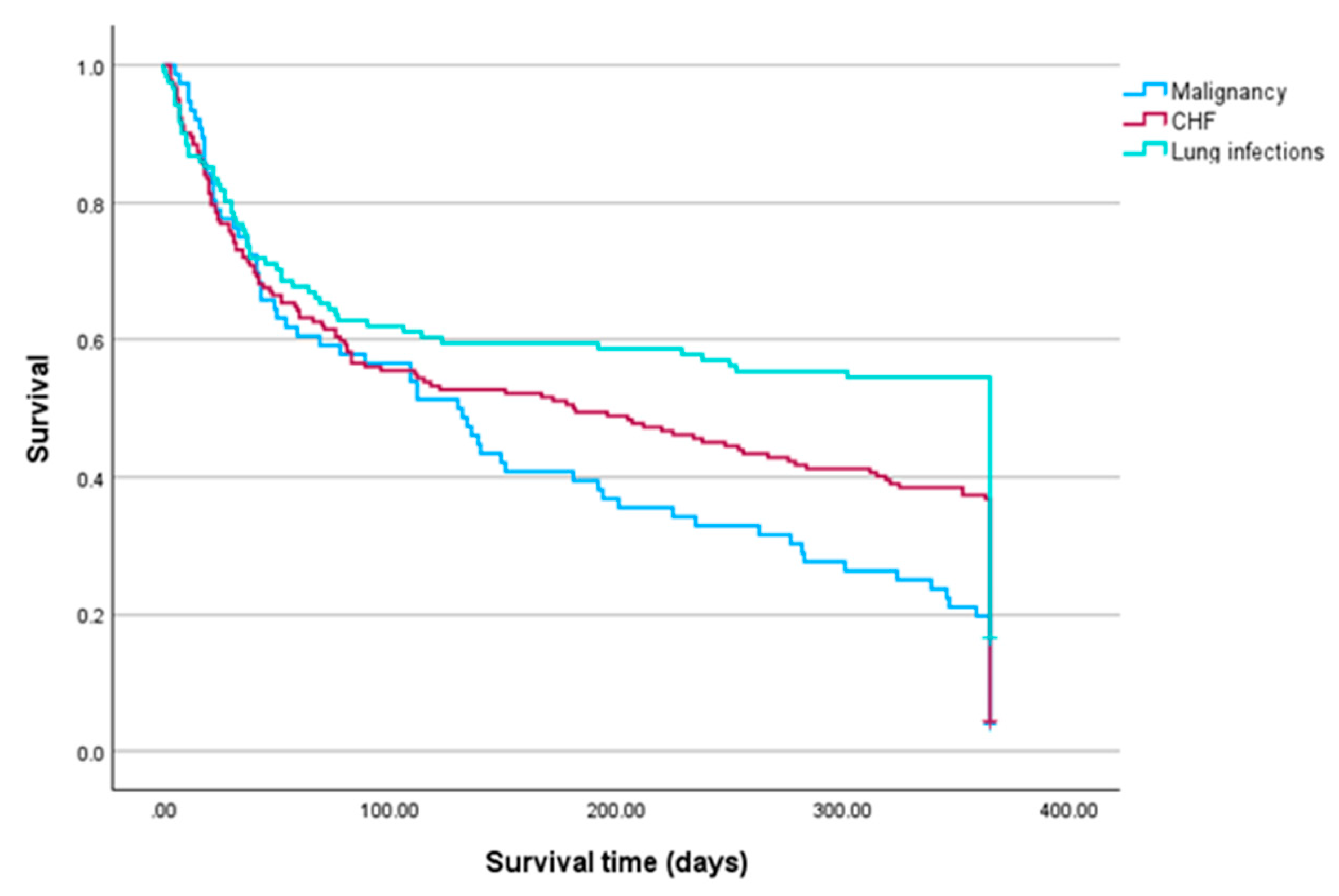

Table 1.
Univariate analysis of study selected patient characteristics by pleural effusion (N = 635).
Table 1.
Univariate analysis of study selected patient characteristics by pleural effusion (N = 635).
| Characteristic | Exudate n=304 |
p-value | Transudate n=331 |
p-value | ||
| 65-85 | >85 | 65-85 | .>85 | |||
| n=216 | n=88 | n=184 | n=147 | |||
| Age, mean ± SD | 76.13±5.52 | 88.89±10.38 | <0.001 | 77.94±4.86 | 89.59±3.72 | <0.001 |
| Female, n% | 96(44.4) | 44(50.0) | 0.378 | 94(51.1) | 68(46.3) | 0.383 |
| Smoking, n(%) | 45(20.8) | 6(6.8) | 0.003 | 25(13.6) | 9(6.1) | 0.026 |
| Length of hospital stay, mean ± SD | 10.47±12.79 | 10.48±8.91 | 0.250 | 18.56±73.11 | 11.07±10.38 | 0.811 |
| In-hospital mortality | 32(14.8) | 11(12.5) | 0.377 | 40(21.7) | 38(25.9) | 0.381 |
| Comorbidities, n(%) | ||||||
| Ischemic heart Disease | 67(31.0) | 25(28.4) | 0.653 | 64(34.8) | 58(39.5) | 0.381 |
| CHF | 33(15.3) | 26(29.5) | 0.004 | 71(38.6) | 62(42.2) | 0.508 |
| COPD | 44(20.4) | 17(19.3) | 0.835 | 39(21.2) | 35(23.8) | 0.571 |
| Dyslipidemia | 90(41.7) | 25(28.4) | 0.031 | 80(43.5) | 33(22.4) | <0.001 |
| Diabetes Mellitus | 99(45.8) | 21(23.9) | <0.001 | 93(50.5) | 46(31.3) | <0.001 |
| Hypertension | 146(67.6) | 73(83.0) | 0.007 | 139(75.5) | 117(79.6) | 0.372 |
| CVA | 40(18.5) | 12(13.6) | 0.305 | 37(20.1) | 38(25.9) | 0.215 |
| CRF | 57(26.4) | 22(25.0) | 0.802 | 60(32.6) | 45(30.6) | 0.698) |
| Atrial fibrillation | 34(15.7) | 26(29.5) | 0.006 | 66(35.9) | 64(43.5) | 0.156 |
| Dementia | 17(7.9) | 17(19.3) | 0.004 | 18(9.8) | 32(21.8) | 0.002 |
| Parkinson | 13(6.0) | 4(4.5) | 0.612 | 9(4.9) | 12(8.2) | 0.225 |
| History of carcinoma | 89(41.2) | 27(30.7) | 0.087 | 44(23.9) | 41(27.9) | 0.410 |
| Effusion side | ||||||
| Right | 77(35.6) | 34(38.6) | 0.841 | 62(33.7) | 45(30.6) | 0.794 |
| Left | 68(31.5) | 25(28.4) | 0.841 | 23(12.5) | 21(14.3) | 0.794 |
| Bilateral | 71(32.9) | 29(33.0) | 0.841 | 99(53.8) | 81(55.1) | 0.794 |
| Laboratory tests | ||||||
| Urea | 65.22±52.61 | 70.96±52.48 | 0.078 | 81.91±54.34 | 84.96±50.25 | 0.211 |
| Creatinine | 1.36±1.32 | 1.25±0.96 | 0.538 | 1.53±1.22 | 1.45±0.95 | 0.402 |
| Albumin | 3.11±0.64 | 3.04±0.54 | 0.276 | 3.05±0.60 | 3.05±0.57 | 0.885 |
| Cholesterol | 148.15±44.44 | 141.94±41.73 | 0.288 | 132.39±33.69 | 137.42±35.51 | 0.204 |
| LDH | 568.85±368.10 | 514.11±242.56 | 0.467 | 606.49±318.48 | 580.78±295.06 | 0.416 |
CHF – Congestive Heart Failure; COPD – Chronic Obstructive Pulmonary Disease; CVA – cerebrovascular accident; CRF – chronic renal failure; LDH ‒ lactate dehydrogenase.
Table 2.
Comparative Analysis of Demographic and Clinical Parameters in Patients with L-Sided vs. R-Sided pleural effusion.
Table 2.
Comparative Analysis of Demographic and Clinical Parameters in Patients with L-Sided vs. R-Sided pleural effusion.
| L-side | R-side | p-value | |
| Parameters | Mean (STD) | ||
| Age | 80.59±9.13 | 82.16±8.71 | 0.019 |
| Urea | 66.32±45.64 | 79.72±54.76 | 0.017 |
| Creatinine | 1.24±0.95 | 1.5±1.25 | 0.141 |
| Albumin | 3.09±0.56 | 3.06±0.61 | 0.001 |
| Cholesterol | 140.80±38.94 | 139.78±40.28 | 0.684 |
| LDH | 548.38±288.25 | 599.23±348.84 | 0.682 |
| Length of hospital stay | 9.83±10.36 | 14.52±49.58 | 0.001 |
| Days to death | 520.24±785.88 | 415.89±695.62 | 0.038 |
LDH ‒ lactate dehydrogenase.
Table 3.
Comparative Analysis of Demographic and Clinical Parameters in Patients with L/R-Sided vs. bilateral pleural effusion.
Table 3.
Comparative Analysis of Demographic and Clinical Parameters in Patients with L/R-Sided vs. bilateral pleural effusion.
| L/R-side | Bilateral | p-value | |
| Parameters | Mean ± SD | ||
| Age | 81.54±8.90 | 79.32±8.48 | 0.276 |
| Urea | 74.42±51.73 | 94.45±67.10 | 0.094 |
| Creatinine | 1.40±115 | 1.53±1.07 | 0.359 |
| Albumin | 3.07±0.59 | 2.54±0.75 | 0.002 |
| Cholesterol | 140.19±39.72 | 135.11±45.60 | 0.710 |
| LDH | 579.06±326.88 | 570.55±311.98 | 0.872 |
| Length of hospital stay | 12.66±39.14 | 24.60±24.77 | 0.005 |
| Days to death | 455.87±732.67 | 179.37±408.64 | 0.058 |
LDH ‒ lactate dehydrogenase.
Table 4.
The chances of dying within one year in malignancy, lung infections and CHF patients.
| Diseases | Died n(%) |
| Malignancy, n = 76 | 61(80.3) |
| Lung infections, n = 161 | 71(43.5) |
| CHF, n = 192 | 122(63.5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



