
Submitted:
02 August 2024
Posted:
06 August 2024
You are already at the latest version
Abstract
Introduction
Pedestrian road injuries are a significant public health issue in Georgia, Syria, and Tajikistan. This study investigates the trends in mortality, Years of Life Lost (YLLs), and incidence rates of pedestrian road injuries from 1990 to 2021, with a focus on sex-specific differences, using age-standardized data from the Global Burden of Disease (GBD) database.
Methods
The data for this analysis were obtained from the GBD database, emphasizing age-standardized rates of mortality, YLLs, and incidence of pedestrian-related road injuries in Georgia, Syria, and Tajikistan. The population was divided into male and female cohorts for comparison. Statistical methods included descriptive statistics, independent samples t-tests, and effect size calculations to evaluate the differences between sexes. Temporal trends were analyzed to observe changes over the study period.
Results
Mortality
The analysis revealed that males had a significantly higher mean mortality rate (7.18, SD = 2.94) compared to females (2.26, SD = 0.78). The independent samples t-test confirmed a significant difference (t(62) = 9.141, p < 0.001). The effect sizes were substantial, with Cohen's d at 2.285, Hedges' g at 2.257, and Glass's Δ at 6.281. Over time, the mortality rates exhibited peaks in the early 1990s and mid-2000s, with a general decline afterward. Males consistently showed higher mortality rates than females throughout the period.
YLLs (Years of Life Lost)
For YLLs, males had a significantly higher mean rate (332.59, SD = 132.31) compared to females (103.35, SD = 32.57), with the t-test indicating a significant difference (t(62) = 9.515, p < 0.001). Effect sizes supported the significance of this difference, with Cohen's d at 2.379, Hedges' g at 2.350, and Glass's Δ at 7.308. The YLL rates showed notable peaks in the early 1990s and mid-2000s, followed by a decline, with males maintaining higher rates than females.
Incidence
Regarding incidence, males had a higher mean rate (235.90, SD = 36.09) compared to females (89.53, SD = 15.29). The t-test results (t(62) = 21.125, p < 0.001) and effect sizes (Cohen's d = 5.281, Hedges' g = 5.217, and Glass's Δ = 9.574) confirmed a significant difference between the sexes. Incidence rates demonstrated a significant decline from 1990 to 2000, followed by fluctuations, with males consistently experiencing higher rates than females.
Conclusion
This study underscores significant sex differences in mortality, YLLs, and incidence rates due to pedestrian road injuries in Georgia from 1990 to 2021, with males consistently showing higher rates. These findings emphasize the need for targeted interventions to address the specific vulnerabilities of male pedestrians in Georgia. The data and analysis were facilitated through collaboration with the Global Burden of Disease Study, whose contributions were invaluable.
Keywords:
pedestrian road injuries
; georgia
; tajikistan
; mortality rates
; years of life lost
; incidence
; sex differences
; global burden of disease
1. Introduction
Road-related injuries (RTIs) account for a substantial global burden of disease—resulting in 1.19 million deaths yearly [1]. Despite the significant economic and societal toll posed by RTIs across the world, existing research has primarily focused on epidemiologic investigations of high-income countries while neglecting low- and middle-income countries that have undergone significant transition towards urbanization and motorization [2]. Though many middle and low-income countries have quickly embraced motorization, their infrastructure fails to keep pace resulting in poorly maintained roads, insufficient pedestrian walkways, and inadequate traffic systems, all contributing to heightened orthopedic injury risks. These issues hold especially true for low-income countries that have previously had war destroy much of the infrastructure, such as Syria. As this discrepancy continues to widen, our study aims to uncover the current epidemiologic trends of pedestrian RTIs to identify areas for reform disease prevention initiatives and advocate for health promotion. More specifically, we are exploring how the burden of disease changes over time, comparing these three major low-income countries with a combined population of 35.796 million as of 2022. Finally, we are exploring the Human Development Index (Tables S1–S6) and determining whether differences between the countries in HDI—and over time—is related to the incidence, deaths, and years of life lost. Crucially, we posit that improved HDI correlates with more substantial infrastructure, both in trauma and orthopedics care, and with safety and prevention guidelines upstream of the operating room that improve road safety for pedestrians. Indeed, more regional economic productivity can afford citizens newer vehicles with improved safety features like traffic lights, side rails on elevated roads, and pothole filling crews to help cars stay on the roads and improve the safety of pedestrians.
Existing literature on RTIs in these countries have primarily focused on specific populations without comprehensively examining trends over time. The TEPHINET assessment of 2014 pedestrian-related injuries focused exclusively on three major urban cities in Georgia: Tbilisi, Batumi, and Rustavi [3]. Though valuable, this urban-centric inquiry overlooks significant rural disparities in road infrastructure [4], inadequate pedestrian crosswalks [5] or roadway lighting [6], and adverse socioeconomic determinants of health [7] that can result in the evidenced increase in fatal RTIs in rural regions of Georgia compared to its urban capital [8]. More crucially, rural neighborhoods suffer from limited access to orthopedic emergency services thereby contributing to exacerbated risks to mortality in affected pedestrians [9].
Insights from the 2014 Georgia National Reproductive Age Mortality Survey further detail the gravity of RTIs with 85.9% of all RTIs resulting in death at the scene of the collision [10] However, this survey notably only examined road traffic fatalities in women of reproductive age—raising the question of how sex-specific differences may affect outcomes of pedestrian RTIs in Georgia.
More concerningly, very little is reported in the literature regarding Syrian population-based estimates of different injuries, let alone regarding Syrian road injuries [11,12]. This ongoing problem has resulted in substantial obstacles in nuanced public health planning and prevents the ability to effectively promote health and prevent disease in the Syrian population.
The limited scope of current Georgian and Syrian RTI-related research has ultimately prevented a holistic understanding of the evolving dynamics and persistent challenges associated with road safety on orthopedic health across diverse demographic groups nationwide. To address this gap, our study conducted a comprehensive analysis using the Global Burden of Disease database, uniquely analyzing longitudinal, sex-specific trends of pedestrian RTIs in mortality rates, years of life lost (YLLs), and incidence rates over time. This approach aims to shape interventions and policies tailored to the regional needs of Georgia and Syria, and further explore differences in pedestrian-related health outcomes stemming from their variations in Human Development Index (HDI), gross national income (GNI) per capita, and gender inequality, despite their geographic proximity.
2. Materials and Methods
Our epidemiological study utilized the 2021 Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) database from the University of Washington’s Institute for Health Metrics and Evaluation—unique for its comprehensive investigation of 371 diseases and injuries across 204 countries and territories from 1980 to 2021 [13]. Our primary measures of interest using the GBD database were our age-standardized rates of mortality, YLLs, and incidence of pedestrian RTIs in the Republic of Georgia and Syria over time, capturing both temporal and demographic trends. Moreover, trends in Georgia and Syria’s HDI and Gender Inequality Index were analyzed to determine regional socioeconomic impacts on pedestrian RTI health outcomes (see Tables S1–S8). To investigate sex-specific trends in pedestrian RTIs, our population was split into male and female cohorts.
Statistical analysis of the GBD database involved descriptive statistics to elucidate overarching trends in pedestrian injury-related age-adjusted mortality, YLLs, and incidence across male and female cohorts in Georgia across time. Calculations included measures of central tendency (mean) and dispersion (standard deviation (SD) and standard error mean (SEM)).
Further analysis was performed with independent samples t-tests to determine if observed sex-specific differences were indeed statistically significant or a cause of random sampling variability. Prior to t-test analysis, Levene’s Test for Equality of Variances was employed to assess whether the samples to be compared were derived from a population with equal variance. Independent samples t-tests for Equality of Means were then utilized to determine a significant sex-specific difference when equal variances are assumed and when equal variances are not assumed. Key statistical measures included t-values, degrees of freedom (df), one-sided and two sided p-values, mean differences, standard error of the difference (SED), and 95% confidence interval (CI).
Effect size calculations were also calculated to quantify the strength of sex-specific differences found by our t-tests independent of sample size. Effect size calculations included Cohen’s d (using the pooled standard deviation), Hedges’ g (using the pooled standard deviation and a correction factor), and Glass’s Δ (using the sample standard deviation of the control group)—essential to determining the practical significance of our observed findings beyond mere statistical significance. All effect size calculations were accompanied by standard error estimates and 95% CI.
Temporal trends analysis identified fluctuations in pedestrian road injury-related mortality rates and YLLs over the course of the study period, 1980 to 2021, and in incidence from 1990 to 2021—attributed to delayed GBD incidence data collection. By analyzing this, we recognized patterns crucial to comprehending the changing landscape of pedestrian RTIs and were able to identify potential factors that may have contributed to increases, decreases, and stagnations in pedestrian injuries to better inform targeted public health interventions.
By utilizing these statistical methods, we were allowed a comprehensive framework for uncovering disparities and trends in pedestrian road injuries across sexes to ultimately guide evidence-based interventions and policy decisions.
3. Results
3.1. Mortality
Descriptive statistics revealed increased mean pedestrian mortality in males compared to females in both Georgia (males: 7.17925238; females: 2.25876444; Table 1) and Syria (males: 7.75097855, females: 2.72985709; Table 2). Levene’s test substantiated differences between male and female mortality in Georgia (F = 43.570, p < 0.001; Table 3) and Syria (F = 33.713, p < 0.001; Table 4).
Independent samples t-test, assuming equal variances, revealed sex-specific differences in pedestrian mortality in Georgia (t(62 ) = 9.141, p < 0.001; Table 3) and Syria (t(62) = 15.458, p < 0.001; Table 4). Without assuming equal variances, sex-specific differences persisted in Georgia (t(35.372) = 9.141, p < 0.001) and Syria (t(35.372) = 15.458, p < 0.001). Georgian effect sizes included Cohen’s d = 2.285, Hedges’ g = 2.257, and Glass’s Δ = 6.281 (Table 5); in Syria, Cohen’s d = 3.865, Hedges’ g = 3.818, and Glass’s Δ = 8.533 (Table 6).
In Georgia, pedestrian mortality (deaths per 100,000 people) peaked in 1990 followed by a decline until 1999 and consistent increase—peaking in 2013 (Figure 1). In Syria, pedestrian mortality depicted consistent declines (Figure 2). Male and female age-standardized mortality followed similar patterns with males displaying consistently higher mortality throughout 1980–2021.
3.2. Years of Life Lost
Mean pedestrian RTI YLLs were also elevated in males compared to females in Georgia (males: 332.549925; females: 103.354992; Table 7) and Syria (males: 335.050333; females: 119.304384; Table 8). Levene’s test substantiated these differences in Georgia (F = 40.967, p < 0.001; Table 9) and Syria (F = 24.742, p < 0.001; Table 10)
Independent samples t-test, assuming equal variances, noted sex-specific differences in pedestrian RTI YLLs in Georgia (t(62) = 9.515, p < 0.001; Table 9) and Syria (t(62) = 12.355, p < 0.001; Table 10). Without assuming equal variances, sex-specific differences persisted in Georgia (t(34.742) = 9.515, p < 0.001) and Syria (t(40.522) = 12.355, p < 0.001). Georgian effect sizes included Cohen’s d = 2.379, Hedges’ g = 2.350, and Glass’s Δ = 7.038 (Table 10); in Syria, Cohen’s d = 3.089, Hedges’ g = 3.051, and Glass’s Δ = 5.923 (Table 11).
Pedestrian RTI-related YLLs per 100,000 people in Georgia possessed notable peaks in 1990 and 2013 followed by decreasing rates. Contrastingly, Syrian YLLs depict consistent and sharp declines. Male and female age-standardized pedestrian RTI-related YLLs modeled similar patterns with males consistently higher throughout 1990-2021 (Figure 3 and Figure 4).
3.3. Incidence
Males suffered elevated mean pedestrian RTI incidence in Georgia (males: 235.900751, females: 89.5330378; Table 12) and Syria (males: 179.094635, females: 83.6737342; Table 13). Levene’s test confirmed sex-specific significance in Georgia (F = 38.517, p < 0.001; Table 14) and Syria (F = 15.440, p < 0.001; Table 15).
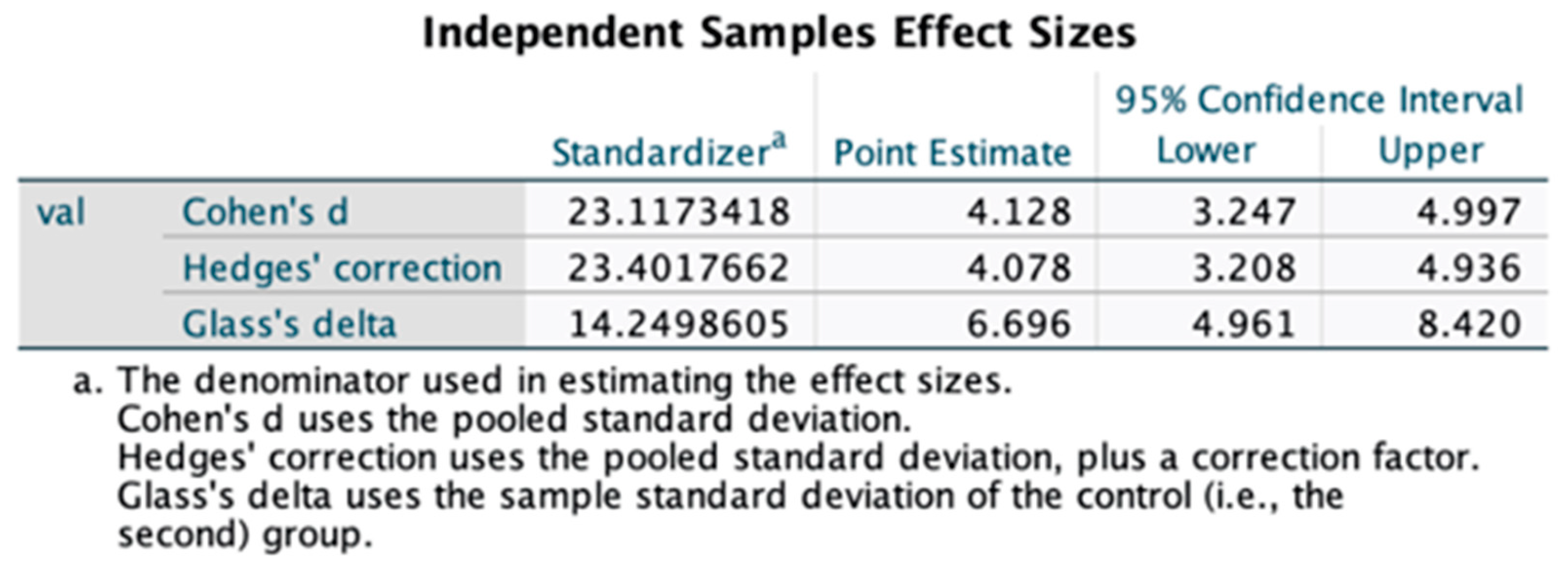
Independent samples t-test, assuming equal variances, further revealed sex-specific differences in pedestrian RTI incidence in Georgia (t(62) = 21.125, p < 0.001; Table 14) and Syria (t(62) = 16.511, p < 0.001; Table 15). Without assuming equal variances, sex-specific differences persisted in Georgia (t(41.780) = 21.125, p < 0.001) and Syria (t(44.783) = 12.355, p < 0.001). Georgian effect sizes included Cohen’s d = 5.281, Hedges’ g = 5.217, and Glass’s Δ = 9.574 (Table 16); in Syria, Cohen’s d = 4.128, Hedges’ g = 4.078, and Glass’s Δ = 6.696 (Table 17).
Georgian pedestrian RTI incidence (cases per 100,000 people) decreased from 1990-2000 and peaked in 2015—where it remained until 2021. Syrian incidence consistently decreased until 2010 by which it remained constant. Male and female age-standardized pedestrian RTI incidence followed similar trends with males at consistently higher rates throughout 1990-2021 (Figure 5 and Figure 6).
3.4. HDI and Gender Inequality
In 2022, Georgia’s HDI (0.814) was ranked 60th with a GNI per capita at $15,952 (2017 PPP), positive GNI-HDI disparity of 19, and improved HDI rank by 4 from 2015-2022. Georgia’s gender inequality index (0.283) ranks 69th with 98.2% and 98.7% of females and males aged 25+ receiving some secondary education, respectively. Labor force participation was 55.5% for females and 73.5% for males aged 15+. Georgian expected and mean years of schooling were 16.7 and 12.7 years, respectively.
2022 Syrian HDI (0.557) was ranked 157th with a GNI per capita at $3,594 (2017 PPP), negative GNI-HDI disparity of -2, and decreased HDI rank by 1 from 2015-2022. Syria’s gender inequality index (0.487) ranks 123rd with 24.1% and 32% of females and males aged 25+ receiving secondary education, respectively, and 14.4% and 68.9% of females and males aged 15+ in the labor force, respectively. Syrian expected and mean years of schooling were 7.4 and 5.7 years, respectively.
For correlation analysis of HDI and its relationship with mortality, YLLs, incidence, and DALYs due to pedestrian road injuries, a Shapiro-Wilk's test was initially performed to determine normality. If normality was assumed, Pearson's correlation analysis was conducted; otherwise, Spearman's rank correlation was used. In Georgia, significant positive correlations were found between HDI and mortality (r = 0.435, p < 0.001), YLLs (r = 0.333, p = 0.006), incidence (r = 0.371, p = 0.002), and DALYs (r = 0.345, p = 0.005). In contrast, Syria demonstrated significant negative correlations between HDI and mortality (r = -0.532, p = 0.002), YLLs (r = -0.392, p = 0.026), incidence (r = -0.486, p = 0.005), and DALYs (r = -0.406, p = 0.021). Tajikistan showed no significant correlations between HDI and the studied outcomes (p > 0.05 for all). These findings highlight the complex relationship between socioeconomic development, as measured by HDI, and pedestrian road injury outcomes, indicating that higher HDI is associated with better outcomes in Georgia but worse outcomes in Syria, potentially due to differences in infrastructure and healthcare systems.
4. Discussion
4.1. Juxtaposed Neighbors: Comparing Georgia and Syria
When comparing the geographically proximate countries, Georgian mortality and YLLs are lower than that of Syria. This finding may be influenced by Georgia’s higher HDI reflecting enhanced longevity, healthcare access, and quality of living [14]. Furthermore, the substantially higher GNI in Georgia likely contributed to the reduced pedestrian mortality and YLLs as opposed to its substantially higher incidence when compared to Syria due to its associated with enhanced pedestrian safety infrastructure such as speed bumps and signaled crosswalks [15,16] Contrary to previous research associating higher educational attainment with decreased pedestrian RTI incidence due to decreased likelihood for employment in occupations increasing exposure to roadway hazards [17], Georgian pedestrian RTI incidence is more than 30% increase compared to Syria—which may be a cause of Georgia’s stark GNI-HDI disparity of 19. Such a vast difference in GNI and HDI ranking suggests that despite possessing relatively high income levels, Georgia’s human development has not advanced as expected, thus suggesting potential areas of improvement in healthcare access, standard of living, and education.
Most notably, Syrian effect sizes for Cohen’s d and Hedges’ g were consistently higher than that of Georgia for mortality, YLLs, and incidence. These larger effect sizes are likely a reflection of the poor gender inequality in Syria—ranking at 123 compared to Georgia’s ranking at 69. Due to exacerbated gender inequality, Syrian males enter the workforce nearly five times more than females due to cultural and societal norms restricting female employment. As such, men are at increased risk of pedestrian RTIs from having to travel to work whereas females are more likely to stay home to tend to housework and childcare [18] Despite their geographic proximity, Georgian and Syrian disparities in HDI, GNI, and gender inequality likely influences the substantial differences in their pedestrian RTI health outcomes, emphasizing the need for targeted regional interventions to address each country’s unique challenges effectively.
4.2. Understanding Georgian Men’s Higher Incidence of Pedestrian RTIs
Examination of mortality, YLLs, and incidence of pedestrian RTIs in Georgia and Syria reveals staggering sex-linked differences throughout 1980-2021—all nearly 2-3 times greater than their female counterparts. Notably, the Georgian and Syrian effect sizes for Cohen’s d and Hedges’g are all larger when analyzing incidence compared to mortality and YLLs. This finding signifies that while there is a drastically higher number of male pedestrian injuries, disparities in mortality and YLLs are less pronounced when compared to females.
The markedly increased Georgian and Syrian male pedestrian injury incidence can be explained by behavioral and physiological sex-related differences placing men at worsened risk for injury. Existing literature describes behavioral sex differences including male-specific delayed start up times to begin walking once they have decided to do so and a heightened tendency to cross the street despite narrower time frames remaining to safely cross—ultimately resulting in higher rates of risky and unsafe pedestrian street crossing behaviors compared to their female counterparts [19]. Furthermore, studies indicate significantly higher predisposition for thrill seeking [20], aggression [21], and general risk acceptance [2]1, manifesting in reduced compliance with crosswalk timing rules [22]. On the contrary, females tend to exhibit more cautious behavior due to perceptions of heightened probability and severity of risks from road related injuries [23,24,25] and diminished enjoyment expected from performing risky behaviors [24].
Beyond behavioral sex differences, male-specific physiological factors have also explained increased pedestrian RTI risk. When performing sit-to-stand measures to determine sensorimotor, balance, and psychological capacities, males uniquely exhibited slower sit-to-stand scores with older age—a strong indicator of decreased mobility and an inability to accurately discern one’s crossing speed [19] Consequently, future interventions should pursue behavioral and physiological approaches to increase awareness of the importance of crosswalk traffic light adherence, dangers of risky pedestrian behaviors, and decline in male mobility with age resulting in inaccurate judgments of crossing speeds.
4.3. Sex-Specific Disparities in Orthopedic Trauma Outcomes from Pedestrian Road Injuries
Though significantly increased in males, the smaller diverse effect sizes for Georgian mortality and YLLs compared to incidence suggests that while males experience more pedestrian RTIs, injury severity may not be as profound in males compared to females.
While little is known regarding quantitative pedestrian severity differences across sexes, research has described sex-linked differences in trauma health outcomes including significantly longer casualty ward stays for females compared to males [26]. Women have also demonstrated significantly worse functional outcomes, well-being scores, and depression across all follow-up time points—6, 12, and 18 months after the initial traumatic event [27].
As described in orthopedic studies conducted on pedestrian vs. motor vehicle accident-related trauma, craniocerebral injuries are the leading type of injury, occurring in 57.1% of all cases [28] These injuries encompass a spectrum of traumatic brain injuries that have notable sex-related differences in health outcomes. For instance, menstrual-related hormonal fluctuations have been found to influence the severity and recovery trajectory of traumatic brain injuries due to variations in neuroinflammatory responses and potential disparities in symptom presentation and reporting—explaining the worsened severity of female pedestrian RTIs. As such, future studies should investigate sex-specific differences in pedestrian trauma outcomes to better tailor clinical decision making and design sex-specific prevention programs to reduce the severity of female pedestrian injuries.
4.4. Implications of Temporal Trends in Pedestrian Road Injuries
For mortality, YLLs, and incidence, Georgian temporal trends reveal notable peaks in the early 1990s and early 2010s, with a subsequent decline in mortality and YLLs and a constant incidence rate. The early 1990s peak can potentially be explained by significant socioeconomic changes in the 1980s from the “second economy” of the Georgia by which the most common consumer purchase was the motorcar [29]. This rapid motorization outpaced their now outdated road infrastructure designed with inadequate safety provisions and struggles to accommodate the unsafe mountainous Georgian topography [30].
Because of the rapidly rising incidence and mortality from pedestrian RTIs, road safety quickly became of national priority thereby spurring the introduction of the 2008 National Traffic Safety Strategy [31], 2010 National Road Safety Action Plan [32], and, most notably, the 2016 Georgia’s National Road Safety Strategy [33]. Implementation of these road safety initiatives involved multi-sectoral collaboration to enforce driving speed management, more efficient emergency medical response, and deterring dangerous risk seeking behaviors through increased police enforcement and public safety announcements.
Along with improved road safety, as part of the Georgian National Healthcare Strategy, the 2013 Universal Healthcare program was introduced thereby decreasing socioeconomic disparities caused by financial barriers to healthcare access for the previously uninsured [34]. Strategic initiatives encompassed a push for improved access to medical facilities and more comprehensive insurance coverage [35].
Most notably, the lack of change in incidence after 2015 as opposed to the steady decline in mortality and YLLs during this same period suggests that though the annual amount of pedestrian RTIs remain consistent, the subsequent health outcomes substantially improved. This disparity underscores the particularly significant role of improved healthcare in supporting the safety and health promotion pedestrians. As the leading cause for spinal and orthopedic injuries worldwide [36], road-related injuries underscore the pivotal role of orthopedic surgeons in the management of pedestrian RTI patients to facilitate early mobilization, prevent long-term disability, and restore quality of life.
Though significant strides have been made in healthcare access, a persistent issue remains with the average ratio of physicians to nurses in Georgia less than 0.8 since 2014 [37], nearly a third of the average ratio in the WHO European region. Even with improved insurance coverage and medical facilities, efforts to address the ongoing nursing shortage, particularly in orthopedic nursing, remains pivotal to ensuring effective healthcare delivery for pedestrian RTI patients.
Despite consistent declines in pedestrian RTI mortality, YLLs, and incidence over time, little is described regarding specific Syrian changes or interventions that have contributed to these improvements. Finally, the correlation analysis between HDI and pedestrian road injury outcomes reveals significant insights into the socioeconomic factors influencing health disparities in Georgia, Syria, and Tajikistan. In Georgia, positive correlations between HDI and mortality, YLLs, incidence, and DALYs suggest that as HDI increases, so do the rates of pedestrian road injuries, potentially indicating a disparity between economic development and effective public health interventions. Conversely, Syria's negative correlations highlight that higher HDI is associated with lower injury rates, suggesting that improvements in socioeconomic conditions contribute to better health outcomes. Tajikistan, with no significant correlations, reflects the need for further investigation into other influencing factors. These findings emphasize the importance of tailored public health strategies that consider the unique socioeconomic contexts of each country. Efforts to improve infrastructure, healthcare access, and targeted interventions are crucial in mitigating the burden of pedestrian road injuries, particularly in countries like Georgia where economic growth has not translated into proportional health benefits.
To further improve the mortality and YLLs of pedestrian RTIs, concerted efforts must be made towards increasing healthcare access and quality, with particular emphasis on mitigating the orthopedic nursing shortage in the Republic of Georgia. By integrating comprehensive healthcare initiatives alongside sex-specific approaches to decrease incidence of pedestrian RTIs, the Georgian healthcare system can effectively promote the health of their citizens.
5. Conclusion
Our findings shed light on drastic sex-specific differences in pedestrian road injuries in the Georgia and Syria from 1980-2021—with nearly 2-3 times higher mortality, YLLs, and incidence rates in males compared to females. Longitudinal temporal trends highlight the effectiveness of road safety initiatives and healthcare reform programs. To effectively dismantle these health disparities, our message remains clear—addressing the orthopedic nursing shortage and implementing sex-specific, tailored road safety interventions are paramount. Future studies should rigorously develop and evaluate these interventions and explore trends in other socio-demographic variables critical in influencing pedestrian road injuries.
Author Contributions
Conceptualization, Cameron John Sabet; Methodology, Cameron John Sabet, Phillip C. McKegg, Muhammad Mustafa, Dang Nguyen and Le Huu Nhat Minh; Software, Cameron John Sabet, Phillip C. McKegg and Amber Park; Formal analysis, Cameron John Sabet and Amber Park; Investigation, Cameron John Sabet; Data curation, Phillip C. McKegg; Writing – original draft, Cameron John Sabet and Britney Shaw; Writing – review & editing, Cameron John Sabet, Britney Shaw, Sai Kurapati and Dang Nguyen; Visualization, Cameron John Sabet and Sai Kurapati; Supervision, Le Huu Nhat Minh. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data available in a publicly accessible repository.
Conflicts of Interest
The authors declare no conflict of interest.
References
- CDC. Global Road Safety. Transportation Safety. Published June 7, 2024. Accessed July 9, 2024. https://www.cdc.gov/transportation-safety/global/index.html.
- Tavakkoli M, Torkashvand-Khah Z, Fink G, et al. Evidence From the Decade of Action for Road Safety: A Systematic Review of the Effectiveness of Interventions in Low and Middle-Income Countries. Public Health Rev. 2022;43:1604499. Published 2022 Feb 21. [CrossRef]
- Chachava T, Mebonia N, Merabishvili Z, Tongren JE, Chikovani N. Assessment of the Surveillance and Causal Factors of the Pedestrian’s Injuries in Georgia | TEPHINET. Published 2016. Accessed July 9, 2024. https://www.tephinet.org/learning/fead/assessment-surveillance-and-causal-factors-pedestrians-injuries-georgia.
- Ai Q, Zhang J, Ye Y. Strategies to enhance the level of service and safety of rural roads: A case study. PLoS One. 2024;19(3):e0300525. Published 2024 Mar 14. [CrossRef]
- Abou-Senna H, Radwan E, Mohamed A. Investigating the correlation between sidewalks and pedestrian safety. Accid Anal Prev. 2022;166:106548. [CrossRef]
- Li Q, Wang Z, Kolla RDTN, et al. Modeling effects of roadway lighting photometric criteria on nighttime pedestrian crashes on roadway segments. J Safety Res. 2023;86:253-261. [CrossRef]
- Saeednejad M, Sadeghian F, Fayaz M, et al. Association of Social Determinants of Health and Road Traffic Deaths: A Systematic Review. Bull Emerg Trauma. 2020;8(4):211-217. [CrossRef]
- Chkhaberidze N, Burkadze E, Axobadze K, et al. Epidemiological characteristics of injury in Georgia: A one-year retrospective study. Injury. 2022;53(6):1911-1919. [CrossRef]
- Wu VS, Schmidt JE, Jella TK, et al. Rural Communities in the United States Face Persistent Disparities in Access to Orthopaedic Surgical Care. Iowa Orthop J. 2023;43(1):15-21.
- Lomia N, Berdzuli N, Sharashidze N, et al. Socio-Demographic Determinants of Road Traffic Fatalities in Women of Reproductive Age in the Republic of Georgia: Evidence from the National Reproductive Age Mortality Study (2014). Int J Womens Health. 2020;12:527-537. Published 2020 Jul 13. [CrossRef]
- Maziak W, Ward KD, Rastam S. Injuries in Aleppo, Syria; first population-based estimates and characterization of predominant types. BMC Public Health. 2006;6:63. Published 2006 Mar 13. [CrossRef]
- Soori H, Khorasani-Zavareh D. Road traffic injuries measures in the Eastern Mediterranean Region: findings from the Global Status Report on Road Safety - 2015. J Inj Violence Res. 2019;11(2):149-158. [CrossRef]
- Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2021 (GBD 2021). Seattle, United States: Institute for Health Metrics and Evaluation (IHME), 2024.
- Bilbao-Ubillos J. Another Approach to Measuring Human Development: The Composite Dynamic Human Development Index. Social Indicators Research: An International and Interdisciplinary Journal for Quality-of-Life Measurement. 2013;111(2):473-484.
- Eid HO, Abu-Zidan FM. Pedestrian injuries-related deaths: a global evaluation. World J Surg. 2015;39(3):776-781. [CrossRef]
- Yasin YJ, Grivna M, Abu-Zidan FM. Reduction of pedestrian death rates: a missed global target. World J Emerg Surg. 2020;15(1):35. Published 2020 May 19. [CrossRef]
- Lascala EA, Gerber D, Gruenewald PJ. Demographic and environmental correlates of pedestrian injury collisions: a spatial analysis. Accid Anal Prev. 2000;32(5):651-658. [CrossRef]
- Yücel A, Utas C, Luchsinger G, Kavlak IV, Kristjansdottir IB, Freizer S. Needs Assessment of Syrian Women and Girls Under Temporary Protection Status in Turkey. Published online 2018. Accessed July 17, 2024. https://eca.unwomen.org/en/digital-library/publications/2018/08/needs-assessment-of-syrian-women-and-girls-under-temporary-protection-status-in-turkey.
- Holland C, Hill R. Gender differences in factors predicting unsafe crossing decisions in adult pedestrians across the lifespan: a simulation study. Accid Anal Prev. 2010;42(4):1097-1106. [CrossRef]
- Cross CP, Cyrenne DL, Brown GR. Sex differences in sensation-seeking: a meta-analysis. Sci Rep. 2013;3:2486. [CrossRef]
- Turner C, McClure R. Age and gender differences in risk-taking behaviour as an explanation for high incidence of motor vehicle crashes as a driver in young males. Inj Control Saf Promot. 2003;10(3):123-130. [CrossRef]
- Tom A, Granié MA. Gender differences in pedestrian rule compliance and visual search at signalized and unsignalized crossroads. Accid Anal Prev. 2011;43(5):1794-1801. [CrossRef]
- Holland C, Hill R. The effect of age, gender and driver status on pedestrians' intentions to cross the road in risky situations. Accid Anal Prev. 2007;39(2):224-237. [CrossRef]
- Harris CR, Jenkins M, Glaser D. Gender differences in risk assessment: Why do women take fewer risks than men? Judgment and Decision Making. 2006;1(1):48-63. [CrossRef]
- Wang H, Schwebel DC, Tan D, Shi L, Miao L. Gender differences in children's pedestrian behaviors: Developmental effects. J Safety Res. 2018;67:127-133. [CrossRef]
- Joestl J, Lang NW, Kleiner A, Platzer P, Aldrian S. The Importance of Sex Differences on Outcome after Major Trauma: Clinical Outcome in Women Versus Men. J Clin Med. 2019;8(8):1263. Published 2019 Aug 20. [CrossRef]
- Holbrook TL, Hoyt DB, Anderson JP. The importance of gender on outcome after major trauma: functional and psychologic outcomes in women versus men. J Trauma. 2001;50(2):270-273. [CrossRef]
- Samona J, Colen R. Orthopedic Considerations in the Pedestrian versus Motor Vehicle Accident Polytrauma Patient. Case Rep Orthop. 2012;2012:149847. [CrossRef]
- O’Hearn D. The Consumer Second Economy: Size and Effects. Soviet Studies. 1980;32(2):218-234.
- Breen J. Road safety management capacity review: Georgia. Global Road Safety Facility (GRSF), World Bank. 2013.
- Ministry of Economic Development of Georgia. Georgian National Traffic Safety Strategy. Tbilisi, Georgia; 2008.
- Ministry of Regional Development and Infrastructure of Georgia. National Road Safety Action Plan. Tbilisi, Georgia; 2010.
- Ministry of Economy and Sustainable Development of Georgia. Georgia's National Road Safety Strategy 2016. United Nations Economic Commission for Europe. 2016. https://unece.org/DAM/trans/doc/2018/UNDA/Georgia_s_National_Road_Safety_Strategy_2016.pdf.
- Verulava T, Jorbenadze R, Barkalaia T. INTRODUCTION OF UNIVERSAL HEALTH PROGRAM IN GEORGIA: PROBLEMS AND PERSPECTIVES. Georgian Med News. 2017;(262):116-120.
- Ministry of Labour, Health and Social Affairs of Georgia. National Health Care Strategy 2011-2015: Access to Quality Health Care. Tbilisi, Georgia; 2011. https://faolex.fao.org/docs/pdf/geo212908.pdf.
- Algahtany MA. Association between orthopedic fractures and traumatic spinal injury due to road traffic accidents. Eur Rev Med Pharmacol Sci. 2021;25(24):7878-7886. [CrossRef]
- “Every young nurse wants to leave this country” – Natalia Chikovani talks about challenges of nursing in Georgia. World Health Organization. Published 2021. Accessed July 11, 2024. https://www.who.int/europe/news-room/feature-stories/item/every-young-nurse-wants-to-leave-this-country-natalia-chikovani-talks-about-challenges-of-nursing-in-georgia.
Figure 1.
Age-standardized pedestrian road injury-related mortality. Temporal trends for males (purple), females (orange), and both sexes (green) in the Republic of Georgia.
Figure 1.
Age-standardized pedestrian road injury-related mortality. Temporal trends for males (purple), females (orange), and both sexes (green) in the Republic of Georgia.
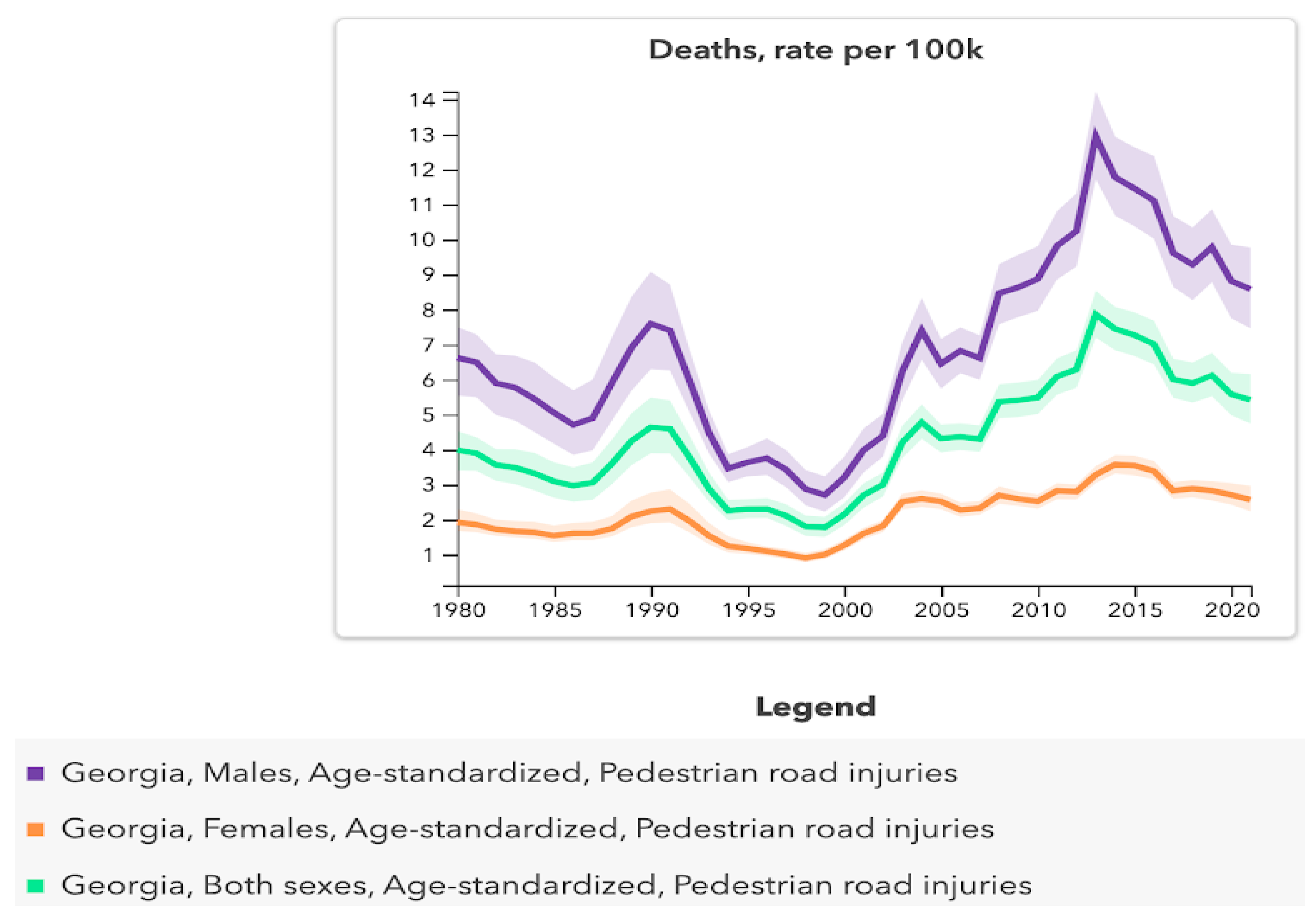
Figure 2.
Age-standardized pedestrian road injury-related mortality. Temporal trends for males (purple), females (orange), and both sexes (green) in the Syrian Arab Republic.
Figure 2.
Age-standardized pedestrian road injury-related mortality. Temporal trends for males (purple), females (orange), and both sexes (green) in the Syrian Arab Republic.
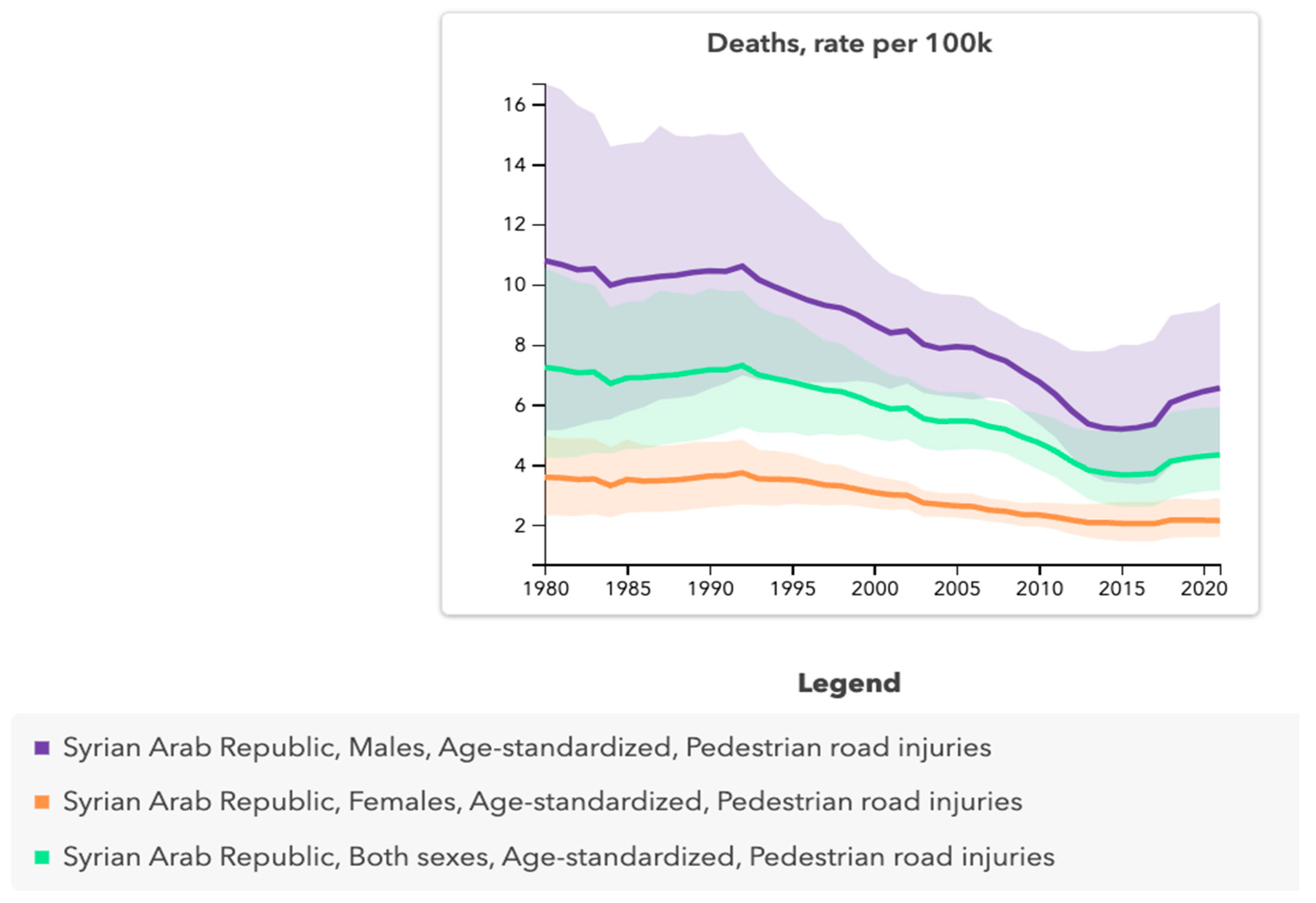
Figure 3.
Age-standardized pedestrian road injury-related years of life lost. Temporal trends for males (purple), females (orange), and both sexes (green) in the Republic of Georgia.
Figure 3.
Age-standardized pedestrian road injury-related years of life lost. Temporal trends for males (purple), females (orange), and both sexes (green) in the Republic of Georgia.
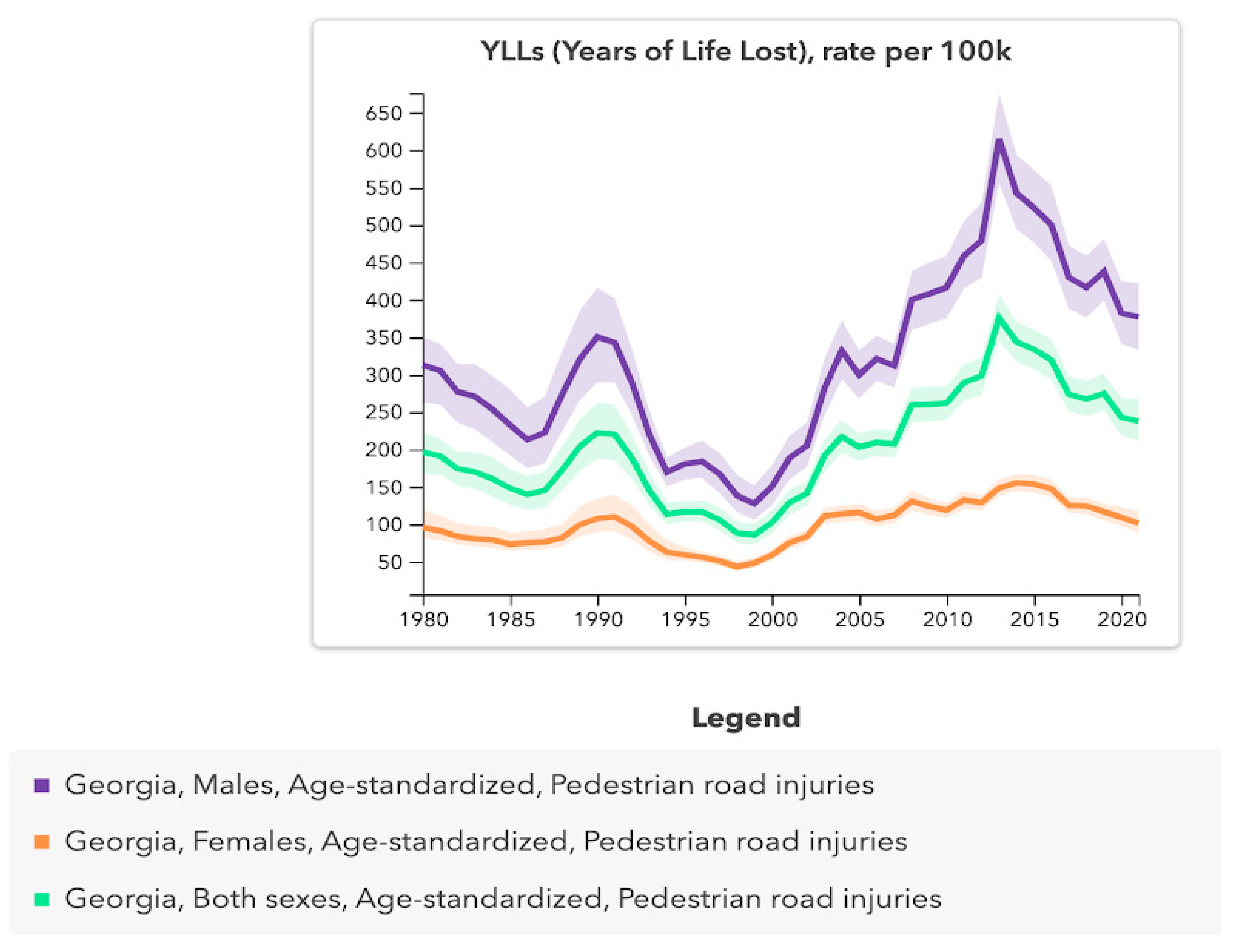
Figure 4.
Age-standardized pedestrian road injury-related years of life lost. Temporal trends for males (purple), females (orange), and both sexes (green) in the Syrian Arab Republic.
Figure 4.
Age-standardized pedestrian road injury-related years of life lost. Temporal trends for males (purple), females (orange), and both sexes (green) in the Syrian Arab Republic.
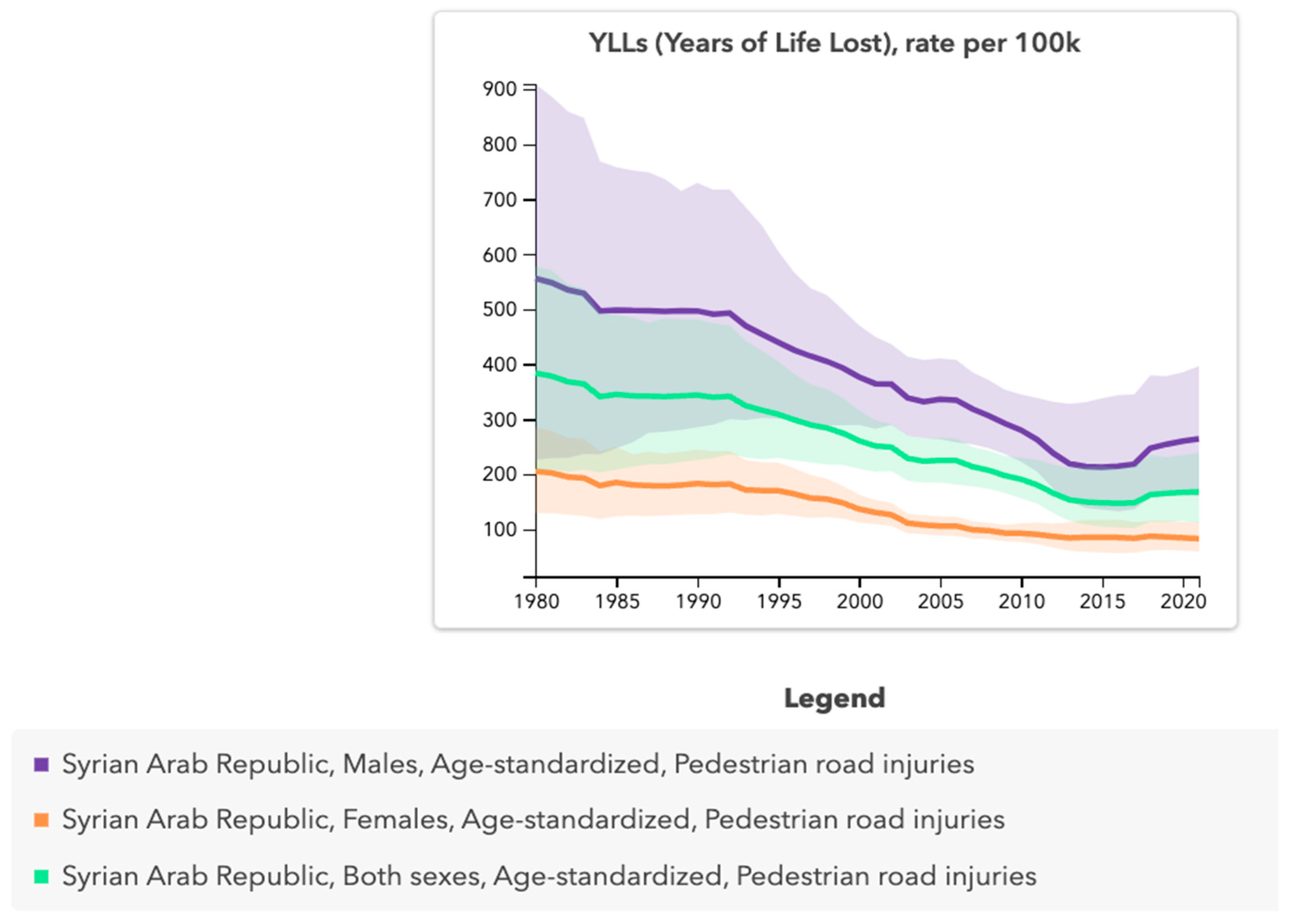
Figure 5.
Age-standardized pedestrian road injury-related incidence. Temporal trends for males (purple), females (orange), and both sexes (green) in the Republic of Georgia.
Figure 5.
Age-standardized pedestrian road injury-related incidence. Temporal trends for males (purple), females (orange), and both sexes (green) in the Republic of Georgia.
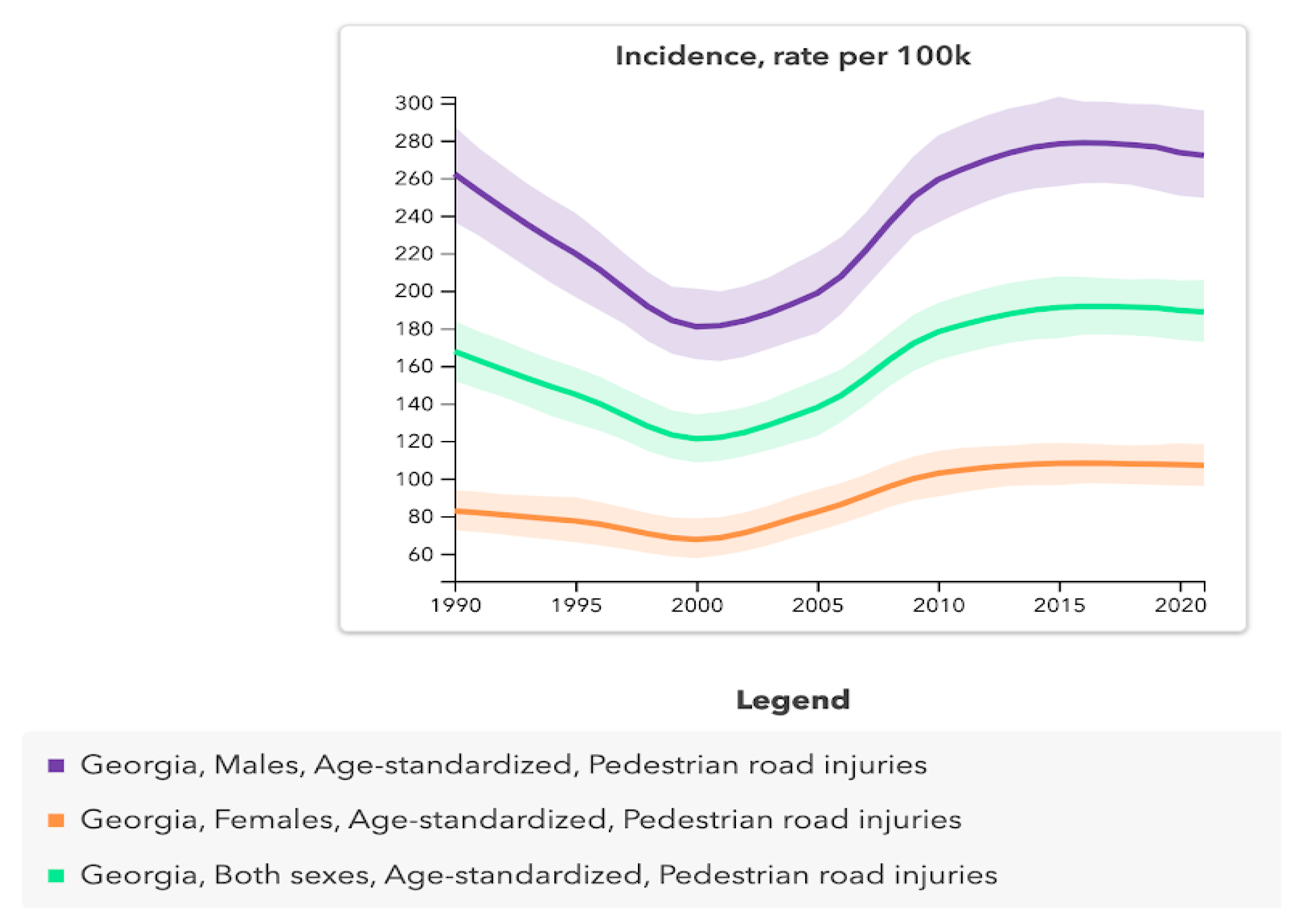
Figure 6.
Age-standardized pedestrian road injury-related incidence. Temporal trends for males (purple), females (orange), and both sexes (green) in the Syrian Arab Republic.
Figure 6.
Age-standardized pedestrian road injury-related incidence. Temporal trends for males (purple), females (orange), and both sexes (green) in the Syrian Arab Republic.
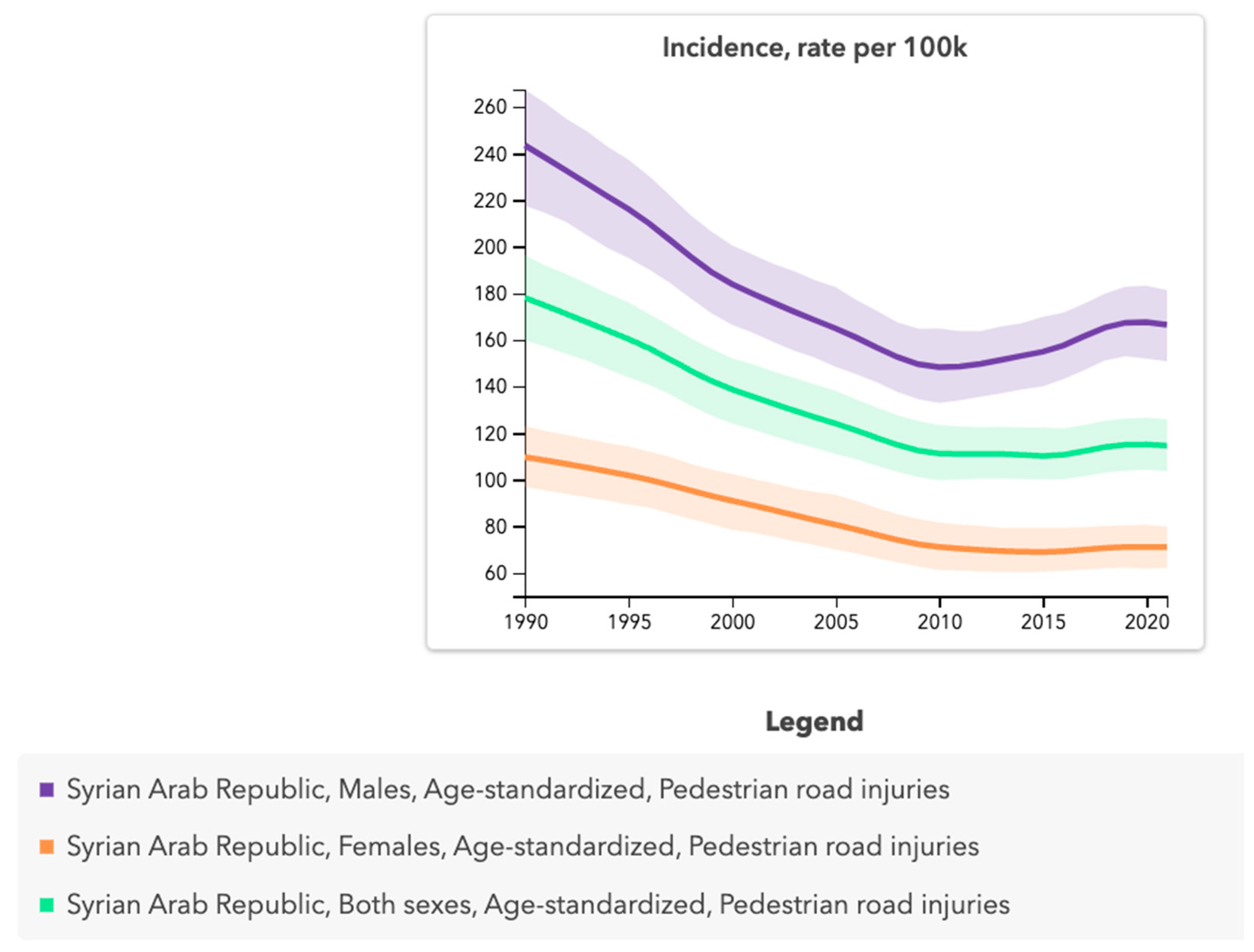

Table 1.
Descriptive statistics analysis for age-standardized pedestrian road injury-related mortality for males compared to females in the Republic of Georgia, 1980–2021.
Table 1.
Descriptive statistics analysis for age-standardized pedestrian road injury-related mortality for males compared to females in the Republic of Georgia, 1980–2021.
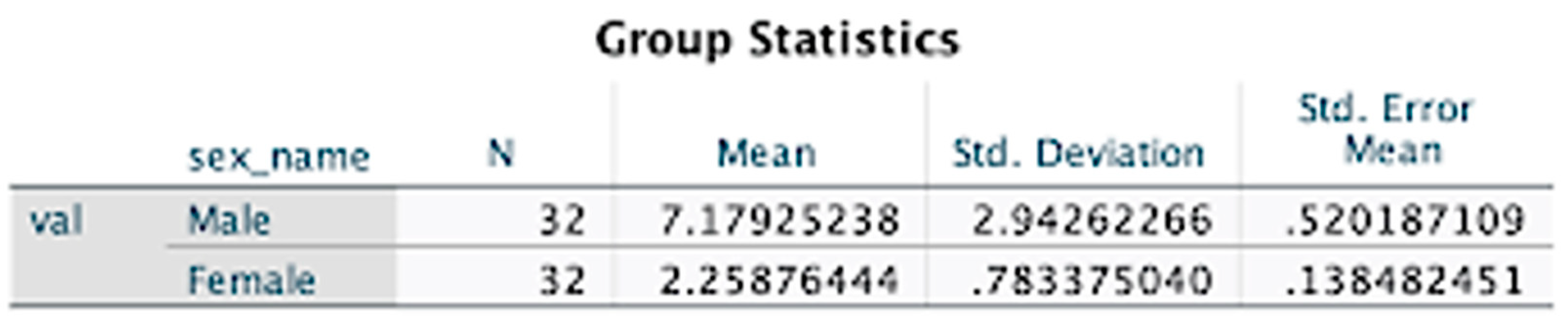
Table 2.
Descriptive statistics analysis for age-standardized pedestrian road injury-related mortality for males compared to females in the Syrian Arab Republic, 1980–2021.
Table 2.
Descriptive statistics analysis for age-standardized pedestrian road injury-related mortality for males compared to females in the Syrian Arab Republic, 1980–2021.

Table 3.
Descriptive independent samples test results for age-standardized pedestrian road injury-related mortality for males compared to females in the Republic of Georgia, 1980–2021.
Table 3.
Descriptive independent samples test results for age-standardized pedestrian road injury-related mortality for males compared to females in the Republic of Georgia, 1980–2021.

Table 4.
Descriptive independent samples test results for age-standardized pedestrian road injury-related mortality for males compared to females in the Syrian Arab Republic, 1980–2021.
Table 4.
Descriptive independent samples test results for age-standardized pedestrian road injury-related mortality for males compared to females in the Syrian Arab Republic, 1980–2021.

Table 5.
Descriptive independent samples effect sizes for age-standardized pedestrian road injury-related mortality for males compared to females in the Republic of Georgia, 1980–2021.
Table 5.
Descriptive independent samples effect sizes for age-standardized pedestrian road injury-related mortality for males compared to females in the Republic of Georgia, 1980–2021.
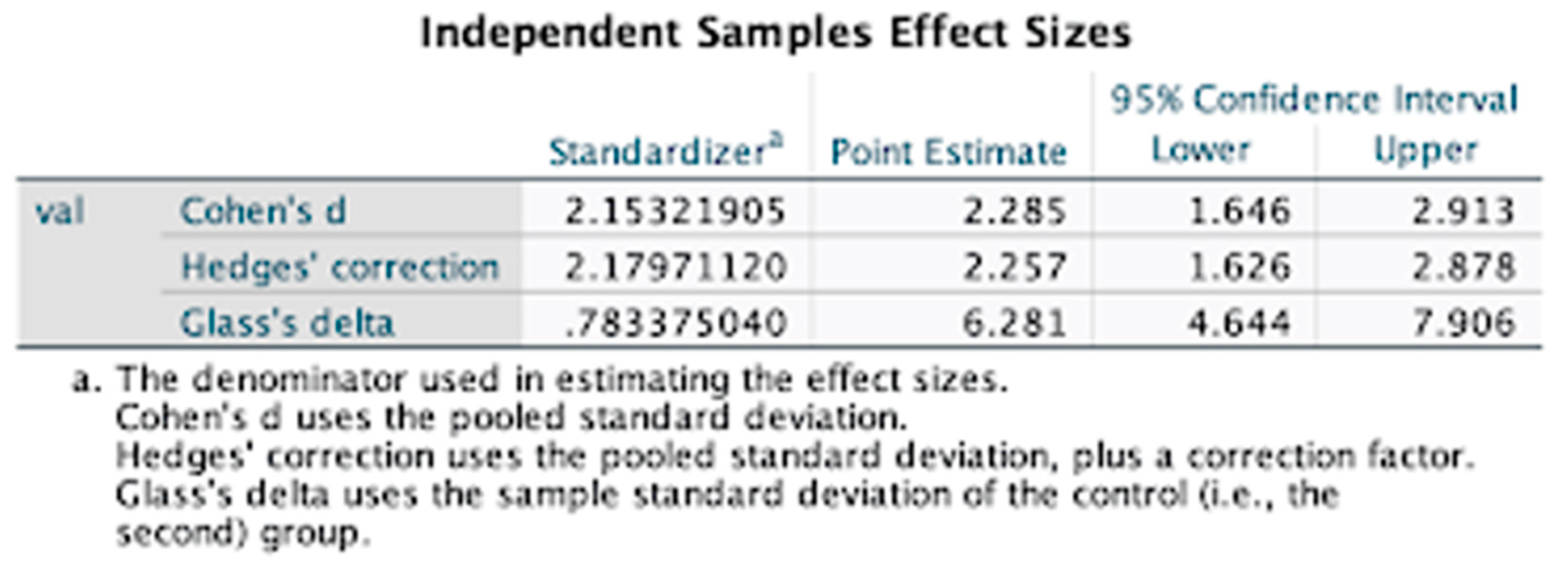
Table 6.
Descriptive independent samples effect sizes for age-standardized pedestrian road injury-related mortality for males compared to females in the Syrian Arab Republic, 1980–2021.
Table 6.
Descriptive independent samples effect sizes for age-standardized pedestrian road injury-related mortality for males compared to females in the Syrian Arab Republic, 1980–2021.
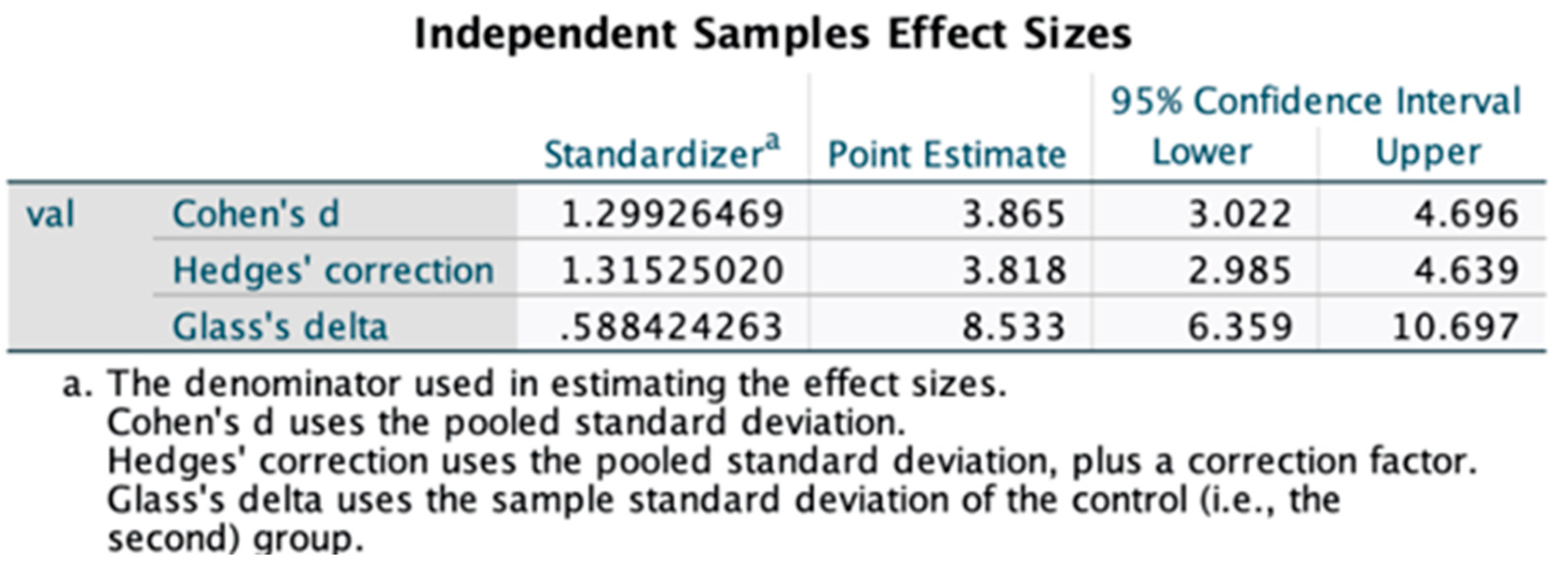
Table 7.
Descriptive statistics analysis for age-standardized pedestrian road injury-related years of life lost for males compared to females in the Republic of Georgia, 1980–2021.
Table 7.
Descriptive statistics analysis for age-standardized pedestrian road injury-related years of life lost for males compared to females in the Republic of Georgia, 1980–2021.
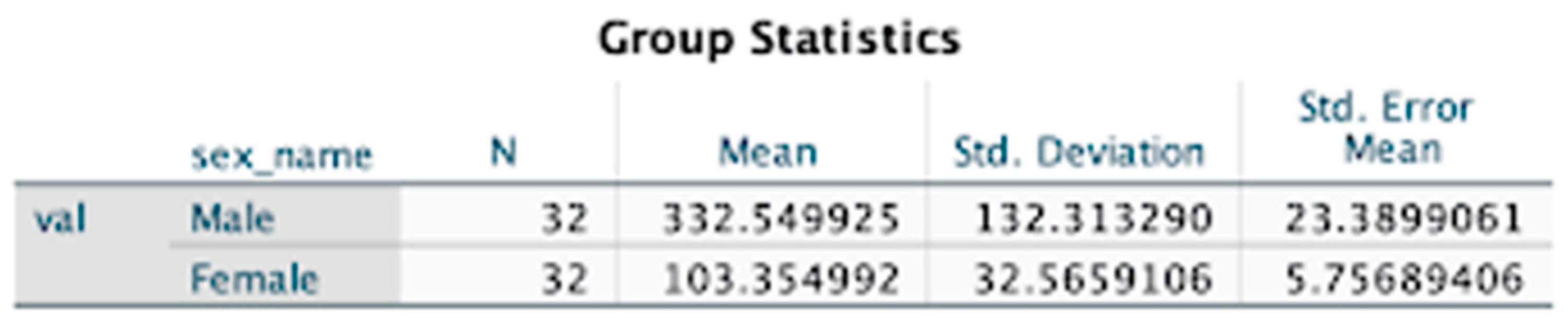
Table 8.
Descriptive statistics analysis for age-standardized pedestrian road injury-related years of life lost for males compared to females in the Syrian Arab Republic, 1980–2021.
Table 8.
Descriptive statistics analysis for age-standardized pedestrian road injury-related years of life lost for males compared to females in the Syrian Arab Republic, 1980–2021.
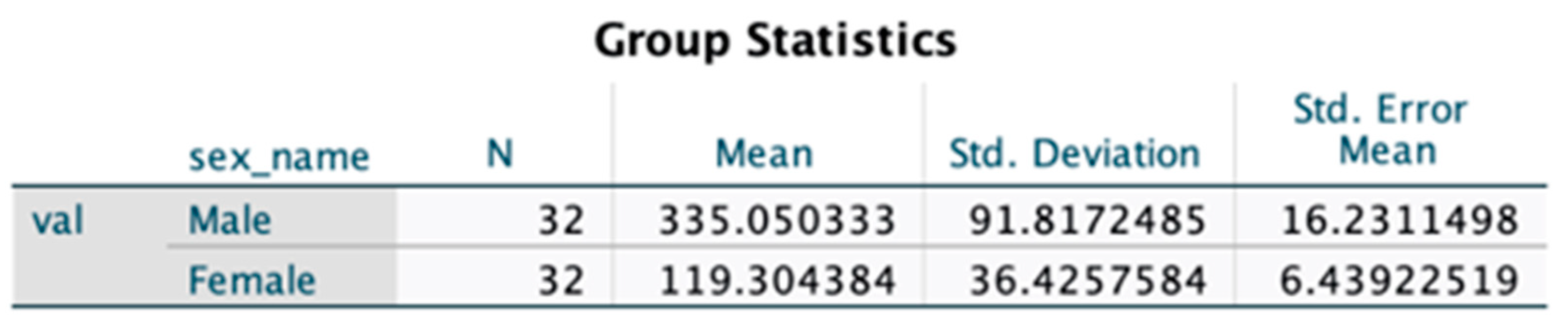
Table 9.
Descriptive independent samples test results for age-standardized pedestrian road injury-related years of life lost for males compared to females in the Republic of Georgia, 1980–2021.
Table 9.
Descriptive independent samples test results for age-standardized pedestrian road injury-related years of life lost for males compared to females in the Republic of Georgia, 1980–2021.

Table 10.
Descriptive independent samples test results for age-standardized pedestrian road injury-related years of life lost for males compared to females in the Syrian Arab Republic, 1980–2021.
Table 10.
Descriptive independent samples test results for age-standardized pedestrian road injury-related years of life lost for males compared to females in the Syrian Arab Republic, 1980–2021.

Table 10.
Descriptive samples effect sizes for age-standardized pedestrian road injury-related years of life lost for males compared to females in the Republic of Georgia, 1980–2021.
Table 10.
Descriptive samples effect sizes for age-standardized pedestrian road injury-related years of life lost for males compared to females in the Republic of Georgia, 1980–2021.
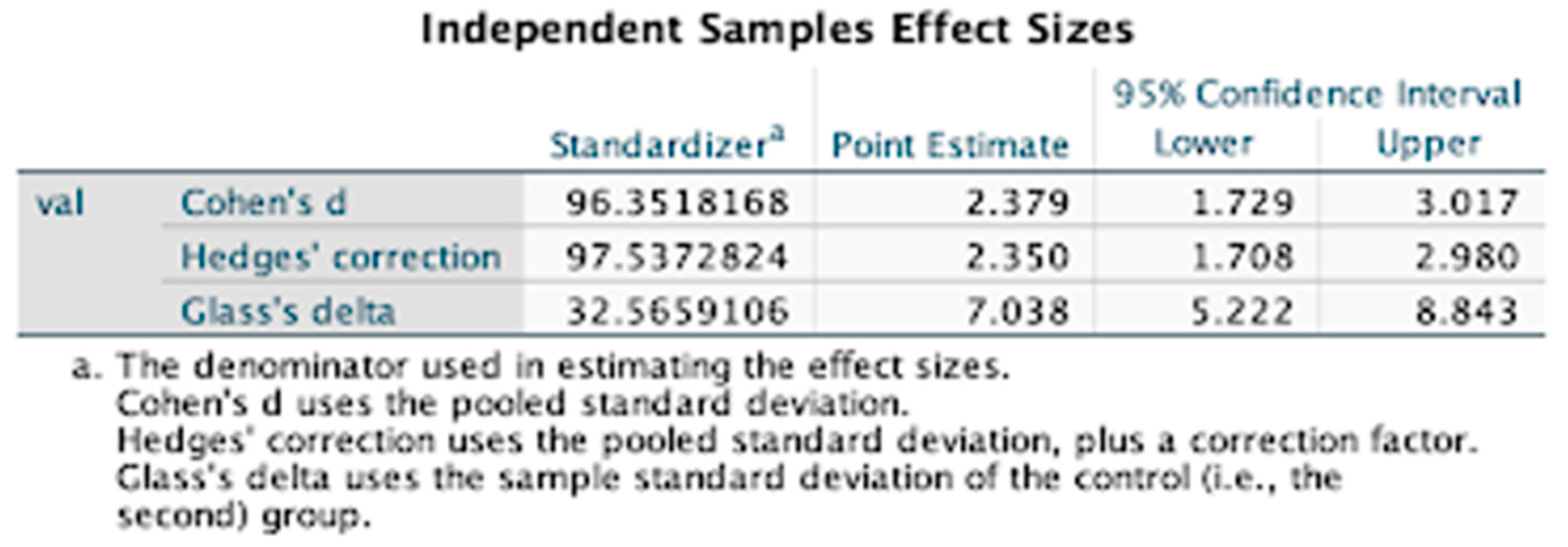
Table 11.
Descriptive samples effect sizes for age-standardized pedestrian road injury-related years of life lost for males compared to females in the Syrian Arab Republic, 1980–2021.
Table 11.
Descriptive samples effect sizes for age-standardized pedestrian road injury-related years of life lost for males compared to females in the Syrian Arab Republic, 1980–2021.
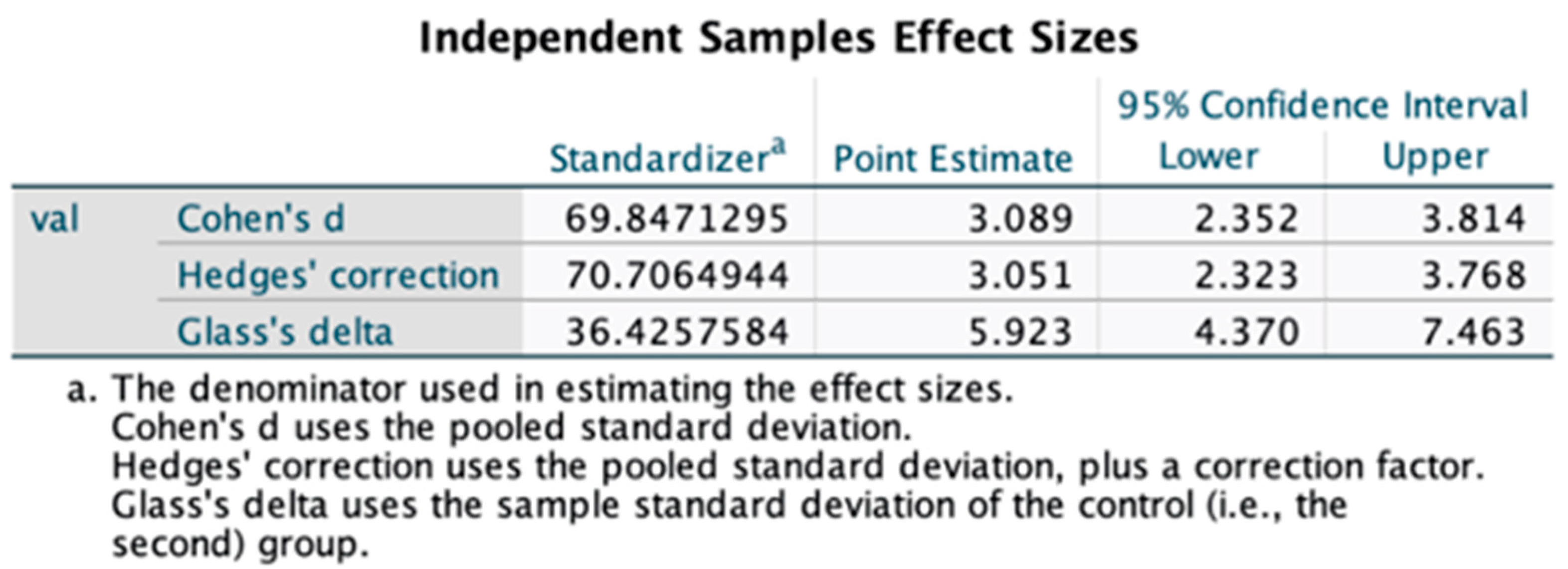
Table 12.
Descriptive statistics analysis for age-standardized pedestrian road injury incidence for males compared to females in the Republic of Georgia, 1990–2021.
Table 12.
Descriptive statistics analysis for age-standardized pedestrian road injury incidence for males compared to females in the Republic of Georgia, 1990–2021.
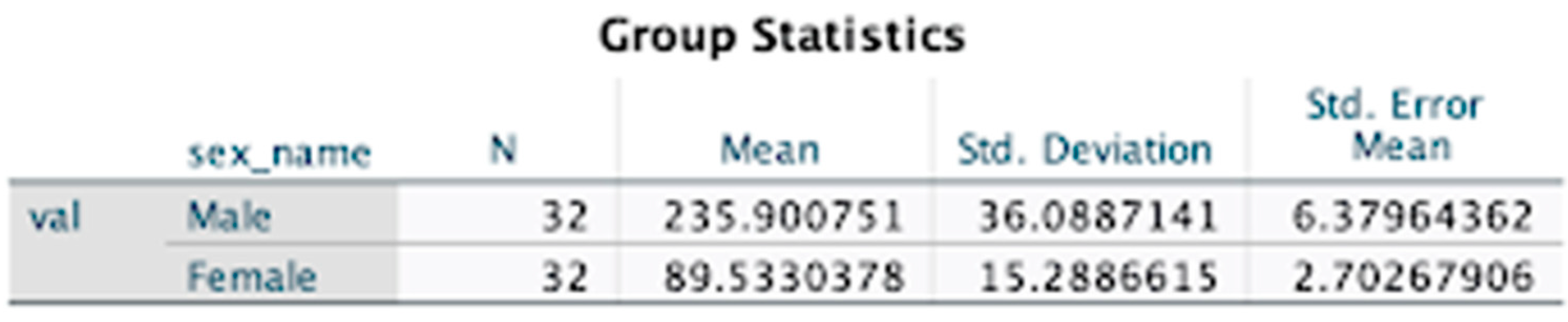
Table 13.
Descriptive statistics analysis for age-standardized pedestrian road injury incidence for males compared to females in the Syrian Arab Republic, 1990–2021.
Table 13.
Descriptive statistics analysis for age-standardized pedestrian road injury incidence for males compared to females in the Syrian Arab Republic, 1990–2021.
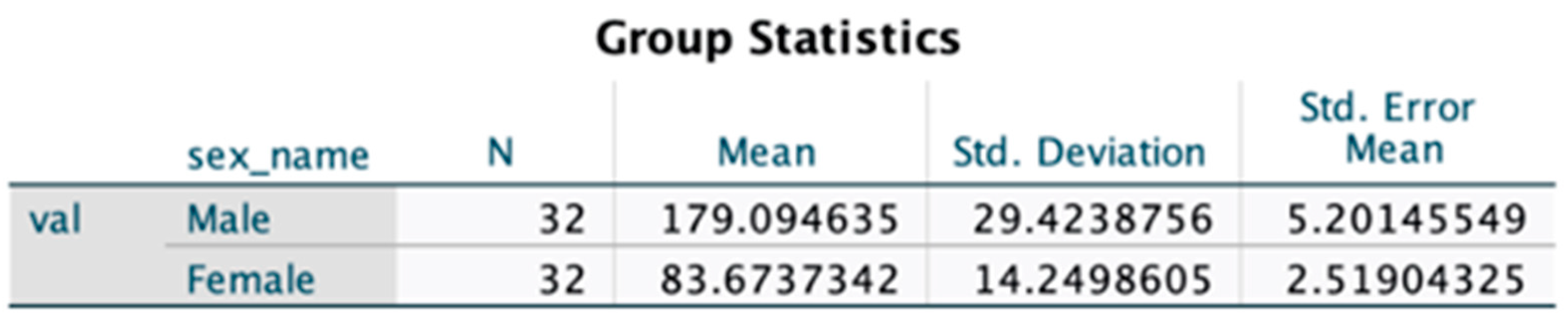
Table 14.
Descriptive independent samples test results for age-standardized pedestrian road injury incidence for males compared to females in the Republic of Georgia, 1990–2021.
Table 14.
Descriptive independent samples test results for age-standardized pedestrian road injury incidence for males compared to females in the Republic of Georgia, 1990–2021.

Table 15.
Descriptive independent samples test results for age-standardized pedestrian road injury incidence for males compared to females in the in the Syrian Arab Republic, 1990–2021.
Table 15.
Descriptive independent samples test results for age-standardized pedestrian road injury incidence for males compared to females in the in the Syrian Arab Republic, 1990–2021.

Table 16.
Descriptive samples effect sizes for age-standardized pedestrian road injury incidence for males compared to females in the Republic of Georgia, 1990–2021.
Table 16.
Descriptive samples effect sizes for age-standardized pedestrian road injury incidence for males compared to females in the Republic of Georgia, 1990–2021.
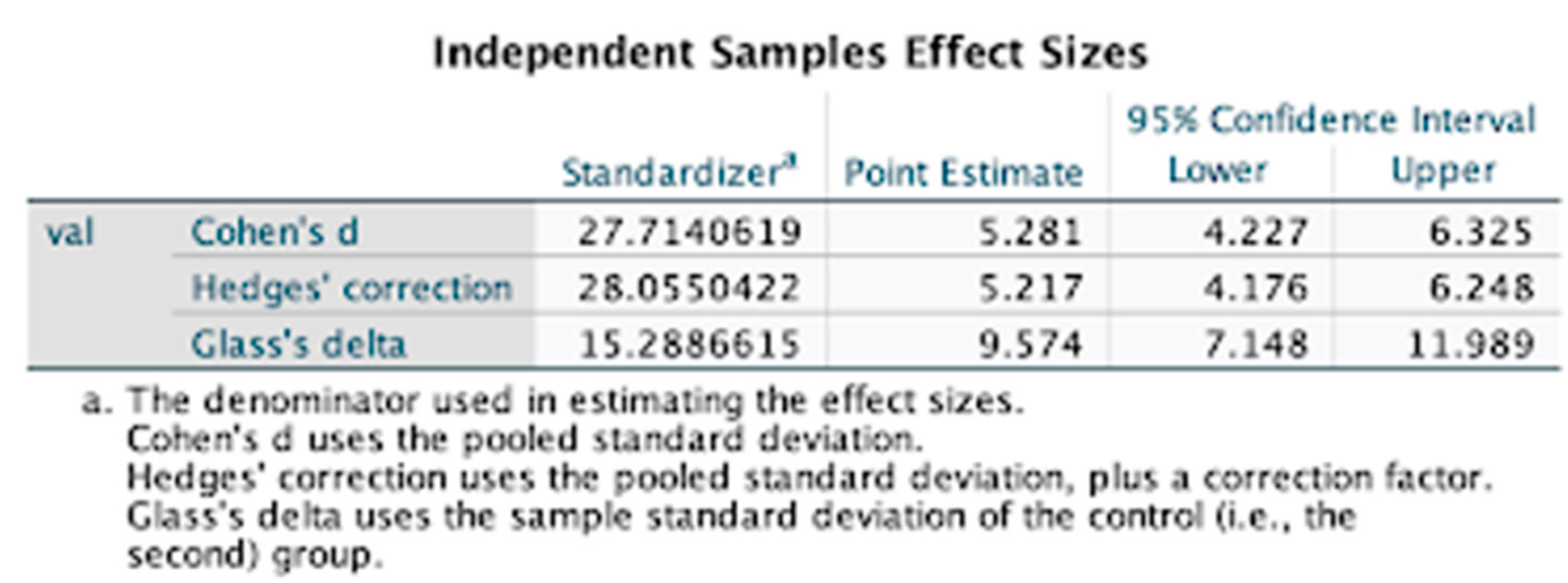
Table 17.
Descriptive samples effect sizes for age-standardized pedestrian road injury incidence for males compared to females in the Syrian Arab Republic, 1990–2021.
Table 17.
Descriptive samples effect sizes for age-standardized pedestrian road injury incidence for males compared to females in the Syrian Arab Republic, 1990–2021.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



