
Submitted:
05 August 2024
Posted:
06 August 2024
You are already at the latest version
Abstract
The management of vision-threatening retinal diseases remains challenging due to the lack of an effective drug delivery system. Encapsulated cell therapy (ECT) offers a promising approach for the continuous delivery of therapeutic agents without the need for immunosuppressants. In this context, an injectable and terminable collagen-alginate composite (CAC) ECT gel, designed with a Tet-on pro-caspase-8 system, was developed as a safe intraocular drug delivery platform for the sustained release of glial cell line-derived neurotrophic factor (GDNF) to treat retinal degenerative diseases (RDDs). This study examined the potential clinical application of the CAC ECT gel, focusing on its safety, performance, and termination through doxycycline (Dox) administration in the eyes of healthy New Zealand White rabbits, as well as its therapeutic efficacy in rabbits with sodium iodate (SI)-induced retinal degeneration. The findings indicated that CAC ECT gel can be safely implanted without harming the retina or lens, displaying resistance to degradation, facilitating cell attachment, and secreting bioactive GDNF. Furthermore, the GDNF levels could be modulated by the number of implants. Moreover, Dox administration was effective in terminating gel function without causing retinal damage. Notably, rabbits with retinal degeneration treated with the gels exhibited significant functional recovery in both a-wave and b-wave amplitudes and showed remarkable efficacy in reducing photoreceptor apoptosis. Given its biocompatibility, mechanical stability, controlled drug release, terminability, and therapeutic effectiveness, our CAC ECT gel presents a promising therapeutic strategy for various retinal diseases in a clinical setting, eliminating the need for immunosuppressants.
Keywords:
Composite hydrogel
; encapsulated cell therapy
; neuroprotection
; sustained drug delivery
; retina
1. Introduction
A number of diseases affecting the posterior segment of the eye, such as age-related macular degeneration (AMD), and retinitis pigmentosa (RP), pose a chronic threat to vision and demand extended treatment periods, among which photoreceptor cells are most affected. It presents a significant financial and labor-intensive challenge to both patients and physicians due to the extensive costs and efforts required for its treatment and management [1]. Current treatment options primarily involve administering medication through eye drops or intravitreal injections [2]. While applying eye drops is non-invasive and can be easily achieved by patients themselves, the necessity for frequent application often results in poor compliance [3,4]. Intravitreal injection is the current method for delivering drugs to the posterior segment of the eye [5]. However, to maintain effective drug levels, this invasive procedure must be performed regularly, which can lead to various cumulative risks and complications, including inflammation, endophthalmitis, retinal detachment, and cataracts [6]. As chronic retinal diseases necessitate multiple and repeated intravitreal injections for attaining effective local drug levels, there has been a growing interest in intraocular drug delivery systems [7].
Encapsulated cell therapy (ECT) is a promising strategy to provide continuous and freshly synthesized drug delivery to the targeted site by encapsulating drug-producing cells into a semipermeable membrane. The porous membrane enables oxygen and nutrients exchange to support cell survival and drug diffusion, while preventing immune cell access into the capsule without the requirement for immunosuppressants [8]. ECT, first introduced in the 1960s, has been explored for various diseases [9,10,11,12,13,14]. Despite notable progress in this field, its clinical application is still somewhat challenging to achieve. Long-term implantation of ECT systems often leads to device failure, attributed to issues with biocompatibility, system stability, cell viability, and drug production. In the realm of eye care, two ECT devices, NT-501 (Renexus®) and NT-503-3, developed by Neurotech Pharmaceuticals are designed to administer ciliary neurotrophic factor (CNTF) and a soluble anti-vascular endothelial growth factor receptor, respectively [15]. These devices, which anchor to the sclera, consist of synthetic polymers (polyethylene terephthalate and polyethersulfone) along with genetically engineered human retinal pigment epithelium cells (ARPE-19) [15]. Although NT-501 has shown to be safe and is capable of local drug release without the need for immunosuppression, it failed to achieve the primary goals in clinical trials for dry AMD and RP, leading to the discontinuation of its development for these conditions [16]. Similarly, a Phase II study for wet AMD using NT-503-3 was halted prematurely due to a high incidence of rescue interventions and insufficient patient responses [17]. While CNTF treatment may enhance photoreceptor cells survival, potential adverse effects, such as diminished electroretinogram (ERG) responses and miosis, could impact other aspects of a patient’s visual function [18]. Therefore, there is a significant demand for innovative and improved treatment options for retinal degenerative diseases (RDDs), particularly aimed at safeguarding retinal photoreceptor cells through neuroprotection. Numerous potential therapeutic candidates have been suggested, with the glial cell-derived neurotrophic factor (GDNF) emerging as a promising option to rescue photoreceptor cells [19].
In our previous work, we fabricated an injectable and terminable collagen alginate composite encapsulated cell therapy (CAC ECT) gel encapsulating GDNF-producing human embryonic kidney (HEK) cells (Figure 1A). Although the presence of cell attachment ligands in collagen promotes cell-matrix interaction, it displays a limited matrix stiffness. Therefore, alginate being a widely utilized material for cell encapsulation [20,21,22] with good biocompatibility, limited cytotoxicity, and ensured quality [21,22,23] was added to form semipermeable membrane and/or matrix. Alginate itself does not contain cell-binding motifs, which can potentially compromise cell viability over an extended period of time [24]. The combination of collagen with alginate allows the collagen-alginate composite (CAC) gel to better mimic the in vivo environment, providing mechanical protection to enclosed cells and enhancing mechanical stiffness [25,26]. Our earlier studies demonstrated that CAC ECT gel had shown promising therapeutic potential in rescuing photoreceptor cells in dystrophic Royal College of Surgeons rats, a rat model of photoreceptor degeneration. In addition, a biosafety switch, utilizing Tet-on pro-Casp8, was established into the CAC ECT gel to enable gel functionality termination through oral Dox administration for a safe intraocular drug delivery (Figure 1B). However, the translation of the ECT system from the laboratory to clinical application remains elusive. The rodent eye has been criticized for its small eye size compared to that of humans, the anatomical difference and species difference in drug pharmacokinetics, and limited vitreous capacity [27]. The rabbit is a commonly used animal model in ophthalmic studies due to its eye size being similar to that of humans, ease of handling, availability, and low cost [28,29]. Moreover, compared to rodents, rabbit eyes have enough space to accommodate multiple ocular implants, making it possible to evaluate the multiple gel performance and therapeutic efficacy in clinical situation. With the aim in translating CAC ECT gel to clinical application, this study investigated (1) in vivo safety of CAC ECT gel, (2) in vivo performance of CAC ECT gel, and (3) in vivo termination of CAC ECT gels by oral administration of doxycycline (Dox) in healthy New Zealand White (NZW) rabbits, and (4) in vivo therapeutic potential of CAC ECT gel in NZW rabbits with retinal degeneration induced by intravenous injection of sodium iodate (SI) (Figure 1C).
2. Results and discussion
2.1. In vivo Evaluation of the Effects of CAC ECT Gels on Retinal Structure and Function and Glial Cells Reactivity
Intravitreal implantation can induce toxicity, attributable primarily to the presence of a material itself. Additionally, the pharmacological agents and their metabolites, especially in scenarios involving biodegradable implants for drug administration, can further exacerbate this toxicity due to their concentration and interaction within the ocular environment. Prior to applying CAC ECT gels as an intraocular drug delivery platform for clinical application, it is crucial for us to determine the safety of intravitreal surgery and the effect of prolonged presence of CAC gel inside the vitreous on the eye. CAC ECT gels were injected into the vitreous of NZW rabbit eyes and left for 2 weeks. Operated control rabbit eyes that received medium only were also evaluated to determine if the surgical procedure could induce any changes in the retina. During the study, the weight and IOP of the rabbits were examined. It was noted that there was no significant difference in the body weight of the rabbit. In contrast, IOP in rabbits with gel injection revealed a short-term decrease when compared to unoperated and operated control over 2-week monitoring (Table 1). There are many causes that can lead to ocular hypotension, including intraocular inflammation, trauma, ophthalmic surgery, and the topical or systemic administration of medication [30]. Moreover, the leakage of intraocular fluid from the surgical wounds and the decrease in aqueous humour generation can lead to ocular hypotony as well [30]. In our study, two holes were made on the cornea using a 27-guage needle to release the IOP, ensuring a successful implantation. The observation of the short-term decrease in IOP may be attributed to the leakage of aqueous humour from the wound.
The potential for ocular surgery to induce cataract formation and retinal detachment was documented when the lens and retina were disturbed. Furthermore, medication-induced cataract is also common. BIO was employed to monitor corneal and lens opacities, the presence of cataract formation and retinal detachment following gel implantation. Over a 2-week monitoring period, no corneal and lens opacification, cataract formation, or retinal detachment was observed (data not shown), suggesting that the surgical procedure did not disturb the cornea, lens, or retina.
The effect of CAC ECT gel on retinal function over the two-week periods was evaluated using ERG (Figure 2A), which is a clinical method valued for its non-invasive measurement of the electrical activity of retinal neurons in response to light. a-wave indicates the function of photoreceptor cells, and the b-wave corresponds to the collective function of ON-bipolar and Müller cells. Both a- and b-wave amplitudes were obtained from the photopic and scotopic ERG data at different light intensity settings. The a-wave and b-wave amplitude, observed in the gel-treated rabbits (3-gel and 6-gel) after 2 weeks, showed no significant difference when compared with the unoperated control, highlighting that the surgical procedure and presence of CAC ECT gel in the vitreous did not affect the retinal function.
We next asked whether intravitreal implantation of CAC ECT gel has any toxic effect on retinal cytoarchitecture. H&E-stained retinal sections of rabbit eyes at 2 weeks after intravitreal gel injection were examined. All retinal layers were present and retinal architecture was found to be well-organized and distinct layers, including ONL, OPL, INL, and IPL and GCL, in all operated eyes including the operated control, 3-gel group, and 6-gel group when compared to the unoperated eyes (Figure 2B). Comparison of various retinal layer thickness revealed no significant differences among the operated eyes and unoperated eyes (Figure 2C). The results demonstrated that rabbits could endure multiple intravitreal administrations of CAC ECT gels without adverse effects as well as without eliciting detectable toxicity within the retinal environment. Additionally, the procedure associated with intravitreal implantation, as well as the CAC gels themselves, did not cause retinal edema or neuron atrophy. Overall, the CAC gels demonstrated excellent biocompatibility and were well tolerated when applied intraocularly, results that are consistent with the findings of other studies [31,32].
In response to foreign body biomaterials, various retinal glial cells, namely microglia, astrocytes, and Müller cells, can exhibit reactivity [33]. Sustained activation of these cells is potentially harmful to the retina, leading to dysfunction and degeneration of cells [34]. Therefore, we next investigated the effects of surgical procedures and the presence of CAC ECT gel on these cells. Immunohistochemistry was performed on the retinal sections. Iba-1 was used to mark microglial cells, while GFAP detected in the visualization of astrocytes and Müller cell end feet.
Microglial cells play a crucial role in preserving the stability of the retinal environment. They become active in response to changes in the parenchyma, altering their shape [35]. In all examined conditions, no significant alterations were observed in the number, distribution, or shape of the microglia (Figure 3A). There was minimal staining, no mention of Iba-1, need to describe Iba-1 signal first. Iba-1 immunoreactivity is primarily observed within the inner regions of the retina, such as in the Ganglion Cell Layer (GCL), Inner Plexiform Layer (IPL), and Inner Nuclear Layer (INL), where inactive microglia can be seen. Once microglial cell become active, their cell bodies become larger, and the cell processes become thicker. Operated rabbit group all exhibited thin and slender projections under iba-1 immunostaining, suggesting that intravitreal implantation of CAC ECT gel and surgical procedure did not trigger the transformation of microglia from a dormant to an active state
We next investigated whether intravitreal surgery and prolonged gel treatment could induce retinal stress. The expression of GFAP, a glial protein that is up regulated during gliosis, was assessed in unoperated eyes and operated eyes (Figure 3B). In the unoperated control eyes, GFAP immunoreactivity was predominantly localized to astrocytes in the GCL. In contrast, retinas from operated control, 3-gel and 6-gel rabbits exhibited GFAP expression in astrocytes in GCL as well as Müller cells that traverse various retinal layers. Yet, no significant difference was observed among these groups. Collectively, these results demonstrated that intravitreal surgery imposed a minimal increase in glial activation.
In the unoperated eye, GFAP immunoreactivity was predominantly detected in GCL. GFAP immunoreactivity was also found in Müller cells in some of retinas of operated control rabbits and gel-injected rabbits. Reactive gliosis of Müller glia is considered retinal responses to the injury [36,37]. Once retina undergoes injury or stress, Müller glial cell is found to be reactive, characterized by the increase in GFAP levels [38]. Studies have indicated that the upregulation of GFAP expression could serve as a biomarker for disrupted retinal homeostasis [39]. Enhanced GFAP fluorescence in Müller cells was detected at 2 and 4 weeks after injection of poly(lactic-co-glycolic acid) (PLGA) microspheres, with a return to baseline levels following 12 and 24 months post injection [40]. Similar observations have been reported, indicating that poly(ε-caprolactone) (PCL) implants could cause retinal stress, which can be inferred from the elevated levels of GFAP [41]. The controversy revolves around whether gliosis is detrimental or advantageous to the retinal tissue. Müller cell gliosis and chronic gliosis were found to accelerate disease progression and neurodegeneration. One the other hand, gliosis of Müller cells can stimulate the release of neurotrophic factors, thereby preserving retina neurons [42]. Our results demonstrated Müller cells were reactive with minimal increase in GFAP expression following intravitreal surgery. This may be a response to disrupted retinal homeostasis caused by the invasive surgical procedure, as a similar increase in GFAP was noted in the operated control as well.
2.2. In Vivo Performance of CAC ECT Gel
Having ascertained the safety of intravitreal implantation of CAC ECT gel in rabbit eyes, we next elucidate the in vivo performance of these CAC ECT gels, which is crucial for the success of ECT system. Healthy NZW rabbits were injected three or six units of gels intravitreally. The gels were then retrieved 2 weeks after for the assessment of gel morphology, system stability, resistance to degradation, encapsulated cell viability and GDNF release kinetics.
2.2.1. Gel Morphology, Encapsulation Power, Mechanical Stability, Material Degradation and Internal Structure
Morphology of retrieved gels after 2-week implantation was compared with those on the fabrication day. Following fabrication, the gels displayed a distinct cell core region predominantly occupied by HEK cells, surrounded by an acellular outer region (Figure 4A). After 2-week implantation, a similar cell core area as well as acellular outer region were identified in the retrieved gel (Figure 4A). It is worth noting there was no host tissue ingrowth and the absence of pericapsular fibrotic overgrowth (PFO) on the gel surface. It is reported that some ECT systems had uncontrollable cell growth kinetics that led to the formation of cell protrusion, which can induce immune response, encapsulated cell necrosis, and even device failure [43]. Yet, no cell protrusion was identified on retrieved gels, suggesting that CAC ECT gel display great encapsulation power. Meanwhile, retrieved gels were found to have intact gel integrity. Since alginate-based hydrogel can undergo slow degradation or dissolution in the presence of calcium chelating compounds and non-gelling cation [44] . The immune cells from the host attempt to degrade the foreign biomaterial as well [45] We next investigated the ability of CAC ECT gels to resist degradation by evaluating the change in gel diameter before and after implantation. Retrieved gels in the 3-gel and 6-gel groups showed no significant change in gel diameter when compared to pre-implantation level, highlighting that CAC system exhibited good resistance to degradation over 2 weeks (Figure 4B). Analysis of the thickness of acellular outer region before and after implantation demonstrated no significant difference, which is consistent with previous morphological finding that no cell protrusion was spotted after 2-week implantation (Figure 4C). The microstructure of the retrieved CAC ECT gels was then studied using SEM. SEM examination of the gel surfaces revealed a highly compact network where collagen fibrils and alginate were intertwined, creating a complex and three-dimensional porous structure, with no cells detected on the gel surface (Figure 4D). This finding aligns with previous observations that demonstrated the presence of an acellular outer region following a 2-week implantation in morphological examinations (Figure 4A). Further SEM analysis of the core region of the retrieved gel at 2 weeks showed that cells were attached to the CAC scaffold, and colonies of round cells were encapsulated within an interpenetrating network (IPN) of collagen and alginate, suggesting that composite hydrogel provide the network for cell attachment and proliferation.
Mechanical stability of the scaffold is in direct relation to the immunoprotective role of ECT device and viability of encapsulated cells [46]. ECT device has to be mechanical stable to resist the shear forces encountered during surgical procedure and the dynamic changes of microenvironment in the targeted site following implantation. Without good mechanical stability, a fractured device is likely to expose enveloped cells to the host, therefore causing device failure. Since no gel breakage and intact gel morphology were observed in all retrieved gel, it was clear that CAC scaffold can tolerate the shear forces during intravitreal surgery procedure and the changes in vitreous microenvironment. These results collectively suggested that our CAC scaffold carries good mechanical stability, which is in line with previous studies [31,32]. A well-designed ECT device should display good resistance to undesirable degradation so that unnecessary contact between encapsulated cell and host tissue is avoided. Therefore, biomaterials in a slow degrading rate or non-biodegradable biomaterials are required for ECT system. Previous studies showed that CAC gel can be degraded due to collagen degradation or alginate dissociation [47]. Matrix metalloproteinase (MMPs) are a group of zinc-dependent endopeptidases that are responsible for ECM remodeling [48] and type I collagen can be degraded in the presence of MMP2 [49]. Various MMPs such as MMP1, MMP2, and MMP9 are found in human vitreous [50]. Meanwhile, alginate-based hydrogel undergoes dissolution or degradation in the presence of calcium chelating compounds such as phosphate, citrate, and lactate and cations (Na+, Mg2+), and the process occurs in a slow and uncontrollable way [44]. Inorganic ions such as Na+, K+, Cl-, Ca2+, and Mg2+, are present in human vitreous [51]. The dissolution of CAC gel can be reflected by the gradual decrease in gel diameter. Yet, our results showed that over the 2-week monitoring, there was no visible change in gel diameter, which indicated that CAC scaffold had good resistance to degradation. These results were consistent with those observed in earlier studies demonstrating that CAC gel remained good resistant to degradation [31,32]. There are several possible explanations for long-term resistance ability to degradation in ocular tissue. Firstly, the concentration of Na+ and Ca2+ is relatively low in ocular tissue [52]. Moreover, increased MMP2 level is found to mediate vitreous liquefication, which is generally expressed in the elderly people or in some pathological states such as diabetic retinopathy [53]. In fact, during vitreous sample collection, we found that the majority of collected vitreous is gel-like, which may be an indication of low MMP2 level. However, this warrants further investigation.
One of the major restrictions to the clinical use of alginate in ECT system is the occurrence of foreign body reaction (FBR), which causes the dysfunction of encapsulated cells [54]. After the implantation of a biomaterial onto the host tissue, ECM can be deposited and adhered to the implant. This process is followed by the deposition of a variety of immune cells, such as neutrophils, monocytes, macrophages, and lymphocytes, on the surface of the implant, eventually leading to the formation of fibrotic tissue. The presence of PFO around the devices or implants can restrict the diffusion of oxygen, and nutrients as well as therapeutic drug, which can lead to a drop in viability of encapsulated cells, and device dysfunctionality [55]. The morphological examination on gels retrieved at 2 weeks showed no presence of PFO. These data indicated that CAC gels do not elicit FBR after an extended period of implantation, which is in agreement with Wang’s findings showing that alginate microspheres loaded with retinoic acid also revealed the absence of PFO following intravitreal implantation [56]. A possible explanation for this might be that eye is an immune-privilege organ [57].
Moreover, a good biomaterial for ECT system should enable encapsulated cells to proliferate inside the matrix so that cells can remain good viability and functionality. When cells are entrapped into collagen-based hydrogel, cells can adhere to collagen via integrin. Consequently, the interaction between cells and matrix can be enhanced, thereby improving cell viability. Our SEM results at 2 weeks demonstrated that HEK cells attached to CAC scaffold in which thick and concentrated collagen bundles were identified and colonies of cells were entrapped in the IPN network. These findings suggested that CAC scaffold provided a compact structure for cell to proliferate, which are in line with those of previous studies [47] demonstrating that the CAC gel exhibited rough surface and a complicated network that facilitating cell adhesion and proliferation.
2.2.2. Encapsulated Cell Viability and GDNF Secretion
Viability of encapsulated cell is considered a critical factor affecting the application of the ECT system. After 2 weeks of implantation, CAC ECT gels were retrieved from 3-gel and 6-gel rabbits to study their viability. Images of the Live-Dead assay of the retrieved gels from the 3-gel and 6-gel groups showed the distribution of viable cells and dying cells (Figure 5A). These results suggested that encapsulated cells were mostly viable after 2 weeks of implantation. Further analysis of cell viability revealed no significant difference between the 3-gel and 6-gel groups in terms of cell viability (Figure 5B). These results suggest that multiple gel injections do not cause a significant reduction in cell viability and the potential for the utilization of multiple gel administrations in personalized therapeutic strategies. The vitreous GDNF level of the unoperated control, operated control, 3-gel, and 6-gel group was assessed by GDNF ELISA at 2 weeks of implantation (Figure 5C). The GDNF level in the unoperated control and operated control was almost undetectable, and no significant difference was detected. For rabbits receiving 3-gel and 6-gel implants, accumulated GDNF levels of 2342.7625 pg/ml and 4321.9235 pg/ml were detected respectively, after 2 weeks of implantation, which were significantly higher than that of operated control. By doubling the amount of CAC ECT gel injected into the vitreous body, we observed a corresponding two-fold positive increase in GDNF levels. These results suggested that CAC ECT gels with permeability were able to secrete GDNF into vitreous in a dose-dependent manner. These results collectively suggested that CAC gel was selectively permeable to allow GDNF diffusion from the gel to rabbit vitreous while host immune cell cannot enter the gel matrix.
Permeability is another factor to be considered when designing ECT technology. ECT device should be designed with selective permeability to allow gas, nutrients in and out of the device and to enable the release of drugs from the device to the targeted site. SEM examination on gel surface suggested the formation of porous structure. Moreover, accumulated GDNF level was detected in rabbit vitreous. These results collectively suggested that CAC gel was selectively permeable to allow GDNF diffusion from the gel to rabbit vitreous while host immune cell cannot enter the gel matrix. The viability of encapsulated cells and their proliferation inside the gel matrix is critical for the application of ECT device. By comparing the cell viability between the 3-gel and 6-gel groups, we found that the number of hydrogels implanted into the vitreous does not significantly affect the viability of the encapsulated cells, and that the levels of GDNF are closely associated with the quantity of implants, which suggested that encapsulated cells were functional and secreted GDNF into vitreous owing to gel permeability. As discussed before, an individual may require different dosages to meet therapeutic efficacy and it can be achieved by tuning the number of implants. Together with previous findings, we envision the feasibility of employing CAC ECT gel for personalized medicine, which can be tuned by the number of gel implants.
2.3. In Vivo Termination of CAC ECT Gel
One major challenge is that when undesirable adverse effects are noted by physician or final goal is achieved, removal of implants is problematic but necessary [58]. The development of a biosafety switch that enables termination of device functionality without the requirement of invasive surgical removal is essential. Nevertheless, limited ECT systems have been designed with this “biosafety switch”. In order to tackle this problem, previous work by our team proposed Tet-on pro-Casp8 system as a promising alternative for ECT system termination. GDNF-secreting HEK cells, equipped with the Tet-on pro-Casp8 system, are capable of undergoing apoptosis upon administration of Doxycycline, regardless of whether the cells are in a non-proliferative phase [32].
The morphology of gels retrieved from Dox-treated rabbits was compared with those retrieved from rabbits without Dox treatment. All retrieved gels were found to have intact gel integrity, no gel breakage, and good encapsulation power in morphological studies (Figure 6A). No cell leakage was observed in both groups (Figure 6A). When gel surface was examined, there was absence of PFO and no host tissue ingrowth or adherence were detected (Figure 6A). However, cell shrinkage and massive fragmented cell debris that homogenously distributed in the cell core were spotted in Dox-treated gel while enclosed cells in non-Dox group had normal features such as spheroid shape, smooth appearance, and larger size (Figure 6A). Live-Dead assay demonstrated that the majority of encapsulated cells in the Dox-treated group were dead, as indicated by the red fluorescence. Only a small number of cells were identified as “living” with green fluorescence, but these cells appeared to be smaller and had broken morphology compared to those in non-Dox-treated gels (Figure 6B). Up to 95% decrease in cell viability was detected in the Dox-treated gels determined by MTS assay, which was consistent with Live-Dead analysis (Figure 6C). The secreted GDNF level in vitreous of non-Dox and Dox group was assessed by GDNF ELISA at 1 week after Dox administration. Compared with non-Dox treatment group, rabbits receiving Dox treatment showed a significant decrease in the accumulated GDNF level (Figure 6D), which further confirms that Dox could effectively terminate gel functionality.
Recent studies first showed retinal toxicities of Dox via intravitreal route using NZW rabbits [59]. To determine whether Dox administration imposed toxicity on retinal function, in vivo retinal function was assessed using ERG after 1-week Dox administration in healthy NZW rabbit eyes. Both Dox-treated and non-Dox-treated groups experienced minor alterations in photopic and scotopic a-wave and b-wave responses, with no statistically significant differences observed (Figure 6G). These results suggested that the function of both cone and rod photoreceptors, as well as inner retinal cells, was not significantly affected by Dox administration. To assess whether 1 week of oral administration of Dox had any effect on retinal architecture, retinal cytoarchitecture was assessed by H&E histology. Under the gross examination, retinal cytoarchitecture of unoperated control, Dox, and non-Dox treated groups were all well preserved (Figure 6E). Analysis of the thickness of various retinal layers revealed no significant differences among unoperated control, non-Dox treated group, and Dox treated group (Figure 6F), suggesting that oral Dox administration imposed no detrimental damage to retinal architecture.
Dox can be administrated to the eye through many routes, such as oral [60], topical [61], intravitreal [59], intravenous [62], intraperitoneal [63], subretinal [64] and subcutaneous [65] administration. We have chosen to use the oral route in our studies as it can mimic the clinical situations with human subjects. In this study, 0.1 mg/ml Dox in drinking water was applied to trigger the termination of CAC gel. Indeed, our results showed that Dox crossed blood-retinal barrier and significantly decreased the viability of encapsulated cells. Only a small number of cells were identified as “living” with green fluorescence, but these cells appeared to be smaller and had broken morphology compared to those in the non-Dox treated gels, suggesting that these cells may not be viable, which was consistent with MTS assay. These data were also consistent with the GDNF analysis on vitreous level demonstrating that gel functionality was almost terminated with undetectable GDNF level. Ejstrup et al. assessed the half-life of GDNF, which is around 37 hours in the porcine eye [66]. Due to the smaller volume of rabbit vitreous, it is expected that drug clearance would be more rapid in rabbits. These results were in accordance with our previous in vitro studies indicating that 1-day treatment of Dox could effectively induce cell apoptosis and 3-day treatment can inactivate gel functionality in rat eyes [32]. The dosage of Dox required to inactive gel functionality in rabbits was comparable to the results from earlier studies in the rats, where 1 mg/ml Dox in drinking water could terminate gel functionality, this indicated that Tet-on pro-Casp8 was highly sensitive to Dox. Further work is required to identify the lowest concentration via oral administration that can trigger the inactivation of gel functionality.
Retinal function and architecture were not affected by oral administration of Dox, as evidenced by ERG examination and H&E histology. Meanwhile, no fundus abnormalities or cataract formation (data not shown) were detected in rabbits with terminated gels. These data were in agreement with previous findings, which demonstrated that lower dosage of Dox via intravitreal administration has no toxicity to retina [59]. Recent studies have reported that similar to many tetracyclines, Dox is known to have anti-inflammatory effect, which is achieved through inhibition of tumor necrosis factor-alpha (TNF-α) and MMPs. Dox has exhibited neuroprotective effect in many animal models with neurodegeneration [67]. Dox was also found to have beneficial effects for diabetic retinopathy through its anti-inflammatory effect [68]. These findings, together with our results, confirmed that the safety of oral administration of low dosage of Dox on eye tissue to terminate gel functionality.
2.4. Therapeutic Efficacy of CAC ECT Gel in Rabbits with Retinal Degeneration
To demonstrate the ability of CAC ECT gels to secrete GDNF to treat retinal degenerative disease state, sodium iodate (SI)-induced model of retinal degeneration in a rabbit eye was employed. SI first directly damages RPE cells, causing secondary photoreceptor cell death, which serve as a good model for studying the novel treatments for photoreceptor cell rescue [69]. Intravenous injection of SI was performed on rabbit to establish retinal degeneration model, followed 2 weeks later by intravitreal injection of three or six unit of CAC ECT gel into rabbit vitreous to assess its therapeutical potential. Rabbits without SI injection served as baseline, a- and b-wave amplitudes of rabbits with retinal degeneration receiving no gel, 3-gel and 6-gel treatment were measured by ERG at 2 weeks after intravitreal gel injection. The amplitude of the a-wave in SI-induced rabbits without gel injection was significantly lower than the baseline level (Figure 7A), which can be alleviated by 3-gel and 6-gel treatment. Similarly, both the 3-gel and 6-gel groups exhibited significant recovery in scotopic b-wave amplitude compared to the group treated with SI only (Figure 7B).
After ascertaining the beneficial effects of CAC gel on retinal function, we proceeded to evaluate whether CAC ECT gel could rescue photoreceptor cells by H&E staining assessment (Figure 7B). Compared to the baseline level, rabbits that received SI injection without gel implantation exhibited a marked reduction in ONL thickness (Figure 7C) and the number of ONL nuclei per mm retina (Figure 7D). However, gel treatment groups including 3-gel and 6 gel group displayed a remarkable increase in ONL thickness (Figure 7C) and the number of ONL nuclei per mm (Figure 7D) when compared to no gel-treated rabbits. These findings suggested that CAC ECT gel was effective in rescuing photoreceptors in a rabbit model of SI-induced retinal degeneration.
To assess whether CAC ECT gel had potential in protecting photoreceptor cells from apoptosis, retinal sections from healthy rabbits and SI-injected rabbits with or without gel treatment were stained with TUNEL (Figure 7E). A notable increase in the number of TUNEL-positive apoptotic cells in the ONL was observed in the SI-treated group that did not receive gel treatment compared to baseline. However, the number of TUNEL-positive cells in the ONL significantly decreased in both the 3-gel and 6-gel treatment groups compared to non-gel treated rabbit retinas (Figure 7F). These data suggested that three units of CAC ECT gel treatment was highly effective in mitigating photoreceptor apoptosis in the retina. To explore whether functional and morphological rescue was attributed to GDNF secreted from CAC ECT gel, gels were retrieved from rabbit vitreous for the examination of their overall structure and cell viability. Live-Dead assay demonstrated that encapsulated cells were mostly viable after 2-week implantation with intact gel boundary and no cell leakage (Figure 7G). As for GDNF level, a similar GDNF release pattern was observed in rabbits with retinal degeneration compared to healthy rabbit eye (Figure 7H). These findings indicated that CAC ECT gels released GDNF into vitreous in a dose-dependent manner, leading to photoreceptor rescue in rabbits with retinal degeneration.
Neuroprotection of photoreceptor cells against degeneration is a promising alternative strategy to treat RRDs characterized by photoreceptor loss and degeneration. Our results showed that 3-and 6-gel treatment confer neuroprotection to photoreceptor against retinal degeneration induced by SI. Beneficial effects in retinal function were found in rabbits with 3-gel and 6-gel treatment compared to no gel-treated rabbits. We then evaluated the ONL thickness and ONL nuclei per mm, since a thinner ONL layer reflects photoreceptor loss [70,71]. Our results demonstrated thinning of ONL and a decrease in the ONL nuclei number after SI injection, as previously reported [72]. Rabbits treated with 3-gel and 6-gel injection showed thicker ONL and an increase in the number of nuclei in ONL than no gel-treated rabbits, which suggested that CAC ECT gel can rescue photoreceptor. To further confirm whether functional and morphological rescue was attributed to CAC ECT gel, we retrieved our gel and collected vitreous from SI-induced rabbits to assess encapsulated cell viability and vitreous GDNF levels. These data demonstrated that encapsulated cells were mostly viable and released GDNF in a dose-dependent fashion. These data collectively demonstrated that CAC ECT gel can secrete bioactive GDNF to improve retinal function and rescue photoreceptor cells, which corroborates the findings of our and other studies that employing ECT system to deliver GDNF is a promising strategy in the management of chronic degenerative or neurologic disorders [32,73,74]. Compared to the normal eye condition, the environment of degenerative retinas may be less favorable for ECT system performance. Yet, CAC ECT gels remained viable in the degenerative eyes, suggesting that CAC ECT gels have the potential to treat retinal degeneration. SI was found to induce photoreceptor death by apoptosis in animals [75], which is a hallmark pathological feature in most RDDs, like AMD and RP [76]. Our observations revealed a significant increase in the number of TUNEL-positive cells in the ONL following SI treatment, consistent with previous findings in mice [77] and rabbits [78], indicating that SI-induced retinal degeneration could serve as a reliable model for studying RDDs. Most importantly, gel treated rabbits showed a significant decrease in the number of TUNEL-positive nuclei in ONL. Together with the findings on cell viability in retrieved gels and increased accumulated vitreous GDNF levels, it is apparent that GDNF released from CAC ECT gels was able to reduce the number of TUNEL-positive cells in ONL. These results indicated that GDNF released from CAC ECT gel was able to prevent the photoreceptor from apoptosis. Our data also demonstrated that three units of CAC gels were able to have promising therapeutic potential in improving retinal function and morphological rescue. As discussed previously, individual patients may require different dosages to achieve therapeutic outcome; this may be achieved by tuning the number of implants. However, the number of CAC ECT implants required to meet the need of patients in different disease stages has not been properly studied and will require further investigation.
3. Materials and Methods
3.1. Cell Culture of HEK/293/GDNF/Tet-on Pro-Casp8
HEK 293 cells, engineered to overexpress GDNF and equipped with a Tet-on pro-Casp8 biosafety switch, were cultured as previously described [32]. The cell line was maintained in Dulbecco’s Modified Eagle Medium with high glucose (DMEM-HG, Life Technologies) supplemented with 10% Tet-on™-approved fetal bovine serum (FBS, Clontech) and 1% penicillin/streptomycin (Life Technologies). To sustain the overexpression of GDNF and the functionality of the Tet-on pro-Casp8 system, the culture medium was further supplemented with 7.5 μg/mL blasticidin (Invitrogen), 300 μg/mL zeocin (Invitrogen), and 500 μg/mL G418 sulfate (Gibco). The supplemented medium was refreshed every three days.
3.2. Preparation of CAC ECT Gel
CAC ECT gel was fabricated as previously described [32]. HEK/293/GDNF/Tet-on pro-Casp8 cells were trypsinized with 0.25% Trypsin-EDTA (Thermo Fisher Scientific). The HEK cell pellet was collected, then mixed with rat-tail neutralized collagen type I (BD Bioscience) solution in the presence of 1N NaOH and a sterilized 1.5% w/v alginate solution (Sigma-Aldrich) to form a cell-CAC mixture. A 2-stage protocol was applied to fabricate the CAC gel in this study. In brief, 2 μL aliquots of the cell-CAC mixture were injected into glass molds (Sigma-Aldrich, Cat. P0674) and then incubated at 37°C to initiate collagen gelation for 75 min, followed by immersion in 100 mM CaCl2 in 0.9% NaCl bath for alginate gelation. After 75 min, the CAC ECT gels were collected from the glass molds and rinsed with 0.9% NaCl (Figure 8). The CAC ECT gels were cultured using 24-well plates before conducting intravitreal gel injection in rabbits. In general, each gel is in a cylindrical shape with approximately 7 mm in length and 480 μm in diameter and contains 5x104 GDNF-secreting HEK cells.
3.3. Animal Care and Use
Female NZW rabbits, aged three to four months and weighing 2.8 to 3.1 kg, were housed in a room with controlled temperature and subjected to a 12-hour light/dark cycle. All animal handling procedures and experiments were conducted in line with the Association for Research in Vision and Ophthalmology (ARVO) Statement for the Use of Animals in Ophthalmic and Vision Research. The use of live animals for research and teaching purposes was approved by the Faculty Committee at The University of Hong Kong (CULATR No.4927-19 and CULATR No.5835-21).
3.4. Intravitreal Gel Injection
Rabbits were anaesthetized by an intramuscular injection of a mixture of xylazine (5 mg/kg) and ketamine (45 mg/kg) (Alfasan lab). To ensure sterility, the right eyelid and surrounding ocular tissue were cleaned with a diluted betadine solution (Mundipharma A.G.). Topical analgesia was achieved by applying 0.5% Alcaine (Alcon) onto the cornea. Afterwards, 1% Mydriacyl (Alcon) was applied onto the cornea to dilate the pupil. The conjunctiva was then separated from the sclera with the help of Vaness scissors curved. One incision (less than 2 mm from the limbus) was then carefully made into the vitreous with a 20-gauge blade (Alcon) under a surgical operating microscope (Zeiss) (Figure 3). Retinal and lens damage was avoided. To release enhanced intraocular pressure (IOP) during intravitreal gel injection, two holes were made near the corneal limbus using a 27-gauge needle. Three or six units of CAC ECT gels, suspended in DMEM-HG 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid (HEPES) medium (Gibco), were injected into the vitreous through sterilized round 0.5 mm thick gel-loading pipette tips (Corning). Upon completion of intravitreal gel injection, the wound was closed using 8-0 nylon suture. Finally, a subconjunctival injection of 2 mg/kg gentamicin (Vetone) was given. Topical administration of antibiotic ointment (Tobrex) was applied onto rabbit cornea for seven consecutive days to prevent post-operative infection. For rabbits serving as operated control, one incision into vitreous was made with intravitreal injection of the same volume of DMEM-HG HEPES medium.
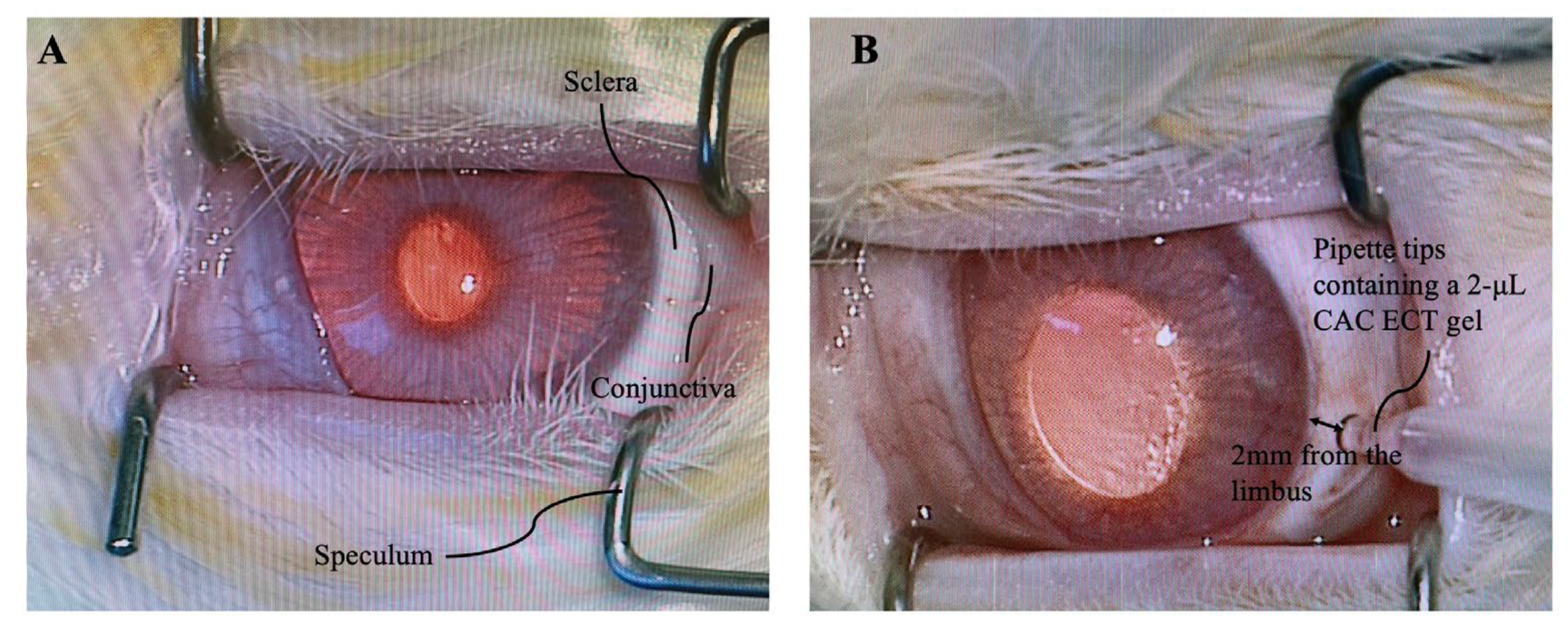
Figure 9.
Intravitreal injection of CAC ECT gels on healthy NZW rabbits. (A) The surrounding ocular tissue was first sterilized by diluted betadine. Then, eyelids were spread apart using a speculum. (B) One incision (2 mm from the limbus) into the vitreous was made using a 20-gauge blade followed by an insertion of a pipette tip containing a 2-μL CAC ECT gel into vitreous.
Figure 9.
Intravitreal injection of CAC ECT gels on healthy NZW rabbits. (A) The surrounding ocular tissue was first sterilized by diluted betadine. Then, eyelids were spread apart using a speculum. (B) One incision (2 mm from the limbus) into the vitreous was made using a 20-gauge blade followed by an insertion of a pipette tip containing a 2-μL CAC ECT gel into vitreous.
3.5. Intraocular Pressure (IOP), Binocular Ophthalmoscope (BIO) Examination and Body Weight Measurement
Prior to any surgical intervention, animals underwent a 2-week training period to acclimatize them to the IOP measurement process. The assessment of IOP was conducted utilizing Tonovet Plus (iCare), with an average of six readings taken for each measurement. To minimize the effect of circadian rhythm on IOP, the measurement of IOP was assessed at 5 pm [79]. IOP measurements were performed before surgery, and at 2 weeks post-injection. After IOP Measurement, BIO (All Pupil Indirect; Keeler) was used to monitor corneal and lens opacities as well as presence of cataract formation and retinal detachment. For body weight measurement, the rabbit was kept calm and was gently placed on the weighing pan. Its weight is recorded to two decimal places using a digital electronic balance.
3.6. ERG Recording
Rabbits were anaesthetized by an intramuscular injection of a mixture of xylazine (5 mg/kg) and ketamine (45 mg/kg) (Alfasan lab). For assessment of retinal function after operation, ERG measurements were conducted at around 2:00 pm to mitigate the impact of possible circadian variations. Rabbits were given 0.5% proparacaine hydrochloride ophthalmic drops (Alcon) for topical anesthesia. 1% tropicamide (Alcon) was applied onto rabbit cornea to dilate the pupil. Artificial tears (Tears Naturale II) were applied onto the cornea to moisturize the cornea for better signal conduction. Before photopic ERG studies, rabbits underwent 20 min of light adaptation. The photopic ERG responses were assessed using Espion E2 Electrophysiology System at 5.0 cd.s/m2. The final photopic ERG responses were averaged from fifteen consecutive measurements. Rabbits then underwent dark adaptation in total darkness for at least 10 min. ERG responses to a flash light stimulus at 0.01 and 10.0 cd.s/m2 were recorded. The amplitudes of a-wave and b-wave were collected for each photopic and scotopic stimulus.
3.7. Retinal Morphological Examination and Analysis
Rabbits were euthanized via intravenous injection of sodium pentobarbital (100 mg/kg; Alfasan). Their eyeballs were enucleated and fixed with 4% paraformaldehyde (PFA) (Sigma-Aldrich) in phosphate buffered saline (PBS) overnight. The superior and inferior portions of the fixed eyeballs were then removed, leaving a 10-mm-wide central section with the optic nerve attached for paraffin wax embedding (TissuePrepTM Embedding Media, Thermo Fisher Scientific) at 60°C. The paraffin embedded eye samples were horizontally cut into 5-μm thick sections using a microtome (Microm HM 315R). The sections containing optical nerve were stained with hematoxylin and eosin (H&E) stain and photographed with an upright microscope (Eclipse 80i, Nikon). The thickness of various retinal layers was measured using ImageJ software.
3.8. Immunohistostaining
After de-paraffinization and rehydration, retinal sections were, subjected to a 10-minute room temperature incubation with proteinase K in PBS (1:500) for antigen retrieval and followed by a 1-hour incubation with 10% goat serum (Vector Laboratories, CA, USA) in primary diluent to prevent unspecific binding. The sections were then incubated with anti-glial fibrillary acidic protein (GFAP) antibody (1:500; Cat# 14-9892-82, ThermoFisher) and anti-ionized calcium-binding adaptor molecule 1 (Iba-1) antibody (1:500, catalog # 019-19741, Wako) overnight at 4°C, and later with Alexa Fluor 568 goat anti-mouse IgG (Invitrogen) and Alexa Fluor 488 goat anti-rabbit IgG (Invitrogen) for 1 hour at room temperature. Negative controls involved substituting the primary antibody with a blocking buffer (10% goat serum). All images were captured with a fluorescence microscope (Eclipse 80i; Nikon) equipped with a digital camera (Diagnostic Instruments, Inc., Sterling Heights) using a 20x objective. GFAP fluorescence intensity was quantified using Image J software as previously described [80]. Briefly, rectangles were drawn from the apical surface of the ganglion cell layer to the retinal pigment epithelium, and the average GFAP fluorescent intensity in these rectangular areas was measured.
3.9. In Vivo Gel Performance Study
Healthy NZW rabbits receiving three or six units of gels were sacrificed 2 weeks post-injection. Gels were collected from the rabbit vitreous for their morphological examination, gel thickness analysis, assessment of cell viability and proliferation, and examination of internal microstructure. In addition, vitreous fluid was extracted and preserved at -80 °C for subsequent measurements of the accumulated GDNF levels (see below).
3.10. In Vivo Gel Termination Study
Healthy NZW rabbits receiving three units of gels were given drinking water containing 0.1 mg/mL Dox (Vetafram) supplemented with 3% sucrose (protected from light) for up to 1 week, starting from 1-week post-injection. Rabbits were sacrificed at 2 weeks after intravitreal gel injection, and CAC ECT gels were retrieved from rabbit vitreous for examination of cell viability and morphology (see below).
3.11. in Vivo Therapeutic Potential of CAC ECT Gel
Sodium iodate (SI)-induced retinal degeneration model was established as previously described [81]. SI powder (Sigma) was dissolved in 0.9% NaCl, which was then sterilized using a syringe filter (Millex-GP). Upon induction of general anesthesia by an intramuscular injection of a mixture of xylazine (5 mg/kg) and ketamine (45 mg/kg) (Alfasan lab), SI solution was injected intravenously into the marginal ear vein of the rabbit ear. At 2 weeks post-SI-injection, three or six units of CAC ECT gel that were fabricated one day earlier were intravitreally injected into their right eyes for assessment of therapeutic potential of gels.
3.12. Assessment of Cell Viability and Proliferation
The viability of encapsulated cells in the retrieved gels was evaluated by a tetrazolium-based Cell Titer 96 Aqueous Non-radioactive Cell Proliferation assay (3-(4,5-dimethylthiazol-2-yl)-5-(3-carboxymethoxyphenyl)-2-(4-sulfophenyl)-2H-tetrazolium, inner salt (MTS) assay, Promega) according to the manufacturer’s instructions. The gels were collected from the rabbit vitreous, placed into the wells of 48-well culture plates, and rinsed with 0.9% NaCl. Then, a mixture of 40 μL MTS, 4 μL phenazine methosulfate (PMS), and 200 μL serum free medium (SFM) was added. After an incubation at 37°C for 2 hours. Absorbance at 490 nm was measured with a microplate reader (Elx800, Biotek) . For background control, a mixture of 40 μL MTS, 4 μL PMS, and 200 μL SFM was added into the well without the gel. The absorbance of the retrieved gel from each experimental group was normalized with that on the day of gel fabrication. For Live-Dead assay, the retrieved gels in the 48-well plate were rinsed with 0.9% NaCl and supplemented with 2 μM Calcein AM and 4 μM Ethidium homodimer-1 (Molecular probes) in SFM. Subsequently, plates were incubated for 40 min at room temperature to allow homogenous staining of viable and dying cells. Images of gels stained with Live-Dead assay were acquired under a confocal microscope (LSM980, Zeiss) or a fluorescence microscope (Eclipse 80i; Nikon). The assessment of cell viability within the gels was conducted in accordance with the method previously described [32]. In brief, the quantification of viable and non-viable cells was performed by enumerating the pixels corresponding to live (green) and dead (red) cells in confocal microscopy images, utilizing the ImageJ software for analysis. Subsequently, cell viability was computed using the following formula:
Cell viability (%) = Living cells/ (Living cells + Dead cells) *100%
3.13. GDNF Quantification
Rabbit vitreous was collected, immediately frozen in liquid nitrogen and stored at -80°C prior to ELISA. Each vitreous sample in the form of gel-like structure was processed to a completely liquid-like structure by sonication (Sonics&Materials, USA Thermo Fisher, USA Eppendorf). GDNF level in rabbit vitreous was determined using the human GDNF ELISA Kit (#EHGDNF, TermoFisher Scientific) according to manufacturer’s instructions. The absorbance was read at 450 nm within 30 min using a multiplate reader (Elx800, Biotek).
3.14. Scanning Electron Microscope (SEM)
The retrieved gels were carefully washed with a 0.9% saline solution and then fix with 4% PFA, Sigma-Aldrich) at 4°C overnight. Subsequently, the gels underwent dehydration using a graded series of ethanol solutions. After further processing at the Electron Microscope Unit (Queen Mary Hospital), critical point drying (CPD 030, Bal-tec) was carried out, and samples were then sputtered with gold (SCD 005, Bal-tec). Finally, the samples were loaded on aluminum specimen holders for SEM imaging (LEO 1530 FEG SEM, Zeiss).
3.15. Terminal Deoxynucleotidyl Transferase (TdT)-Mediated dUTP Nick end Labelling (TUNEL) Assay
Retinal sections were subjected to TUNEL assay (DeadEndTM Fluorometric TUNEL System, Promega) to detect cell apoptosis, following the manufacturer’s instructions [82]. In brief, 5 µm retinal sections containing optical nerve heads were deparaffinized by xylene, followed by rehydration using descending series of ethanol. Proteinase K in PBS (1:500) was used for antigen retrieval. Retinal sections were then permeabilized with equilibration buffer for 5 min and stained with TUNEL reagents at room temperature for 1 hour. Subsequently, retinal sections were counterstained with 4′,6-diamidino-2-phenylindole (DAPI) to label the nuclei. The images were captured under the x20 objective using a fluorescence microscope (Eclipse 80i, Nikon). The number of TUNEL positive cell in ONL was quantified as previously described [32]. TUNEL-stained retinal sections with 900 pixels × 900 pixels were chosen for manual TUNEL positive cell counting with the help of ImageJ. The number of TUNEL positive cell per mm was defined as the number of TUNEL positive cell by the retina length in the selected area.
3.16. Statistical Analysis
Data were expressed as mean ± standard error of the mean (SEM) or standard deviation (SD). The graphs and statistical analysis were generated and evaluated using GraphPad Prism 10 (GraphPad). The significance level was set at 0.05. Data were compared using an unpaired t-test for studies with two experimental groups. One-way analysis of variance (ANOVA) followed by Bonferroni or Dunnett’s post-test and was used to analyse three or more experimental groups.
4. Conclusions
It is still a great challenge to treat chronic retinal eye diseases due to the difficulties in delivering drugs to the posterior segment of the eye. ECT has the potential to deliver freshly synthesized drugs in a sustained and controlled manner. However, the translation of the ECT system into clinical use remains elusive. In this work, the safety of intravitreal implantation of CAC ECT gel was evaluated. The presence of CAC ECT gels in rabbit vitreous and intravitreal surgery did not cause a detrimental effect on retinal function and architecture. Minimal glial activation was detected in the operated group owing to invasive intravitreal surgery. CAC ECT gels in rabbit eyes exhibited suitable encapsulation power without cell leakage from the device to surrounding tissue, shear-stable mechanical property, resistance to degradation and molecule permeability. Encapsulated cells were viable with the ability to secrete freshly synthesized GDNF into the rabbit vitreous in a controlled and sustained manner. CAC gel was also equipped with a biosafety switch in the event where the final goal is achieved, or side effects are noted by the physician. Gel functionality can be inactivated by Dox, an FDA-approved antibiotic, without eliciting damage to rabbit retinal function and architecture. The therapeutic outcomes of CAC ECT gel were examined in rabbits with retinal degeneration. Gel treatment showed a significant increase in retinal function and preserved photoreceptor cells through mitigating photoreceptor apoptosis. GDNF release can be tuned by multiplexing CAC gels into the eye, which can meet different drug requirements for personalized medicine.
Taking into consideration of the minimally invasive surgery procedure, lack of toxicity of CAC gels inside vitreous, good biocompatibility, mechanical stability, required resistance to degradation, controlled GDNF level, and therapeutic efficacy of CAC ECT gel, we envisage that CAC gel has the potential to deliver therapeutic drug to the posterior segment of the eye for the management of RDDs in clinical application without the requirement of immunosuppressants.
5. Limitation of this Study and Prospective Directions.
Our study had several limitations. Firstly, we did not investigate the chronic effect of gel implantation on retinal homeostasis over an extended period. Future studies are warranted to evaluate the long-term effects of terminated gels after Dox administration on the retina. In our current study, we demonstrated the therapeutic efficacy of CAC ECT gel in rabbits with retinal degeneration induced by SI. However, the higher GDNF levels after 6 gel injections when compared to 3 gel injections did not yield more protection; this may be due to the retinal degeneration model used. Compared to SI-induced rabbits, transgenic Pro347 Leu rabbits exhibited a slower and more progressive degeneration of photoreceptors, which is highly similar to the clinical situation in patients with RDDs [83]. This model may help better understand the association between therapeutic outcomes and the number of CAC ECT gels. Additionally, the fabrication of CAC ECT gels is labor-intensive and time-consuming (at least 5 hours) with a success rate of 30-40%, requiring highly trained technicians. Therefore, improving our fabrication skills is crucial for translating these findings into clinical use.
Author Contributions
Tingyu Hu: Conceptualisation; Data curation; Formal analysis; Investigation; Methodology; Validation; Visualisation; Roles/Writing-original manuscript draft. Ting Zhou: Curation data, Investigation. Ka Cheung Tam: Data curation, Investigation. Rajesh Kumar Goit: Data curatio, Investigation. Yau Kei Chan: Conceptualisation; Supervision; Writing –review & editing. Wai-Ching Lam: Conceptualisation; Supervision; Writing –review & editing. Amy Cheuk Yin Lo: Conceptualisation; Funding acquisition; Investigation; Resources; Supervision; Validation; Visualisation; Writing– review & editing.
Funding
This research was funded by the Health and Medical Research Fund, the Food and Health Bureau, The Government of the Hong Kong Special Administrative Region (06171516) and Seed Fund for Translational and Applied Research, The University of Hong Kong University Research Committee (202111160025).
Institutional Review Board Statement
The study was conducted in accordance with the Association for Research in Vision and Ophthalmology (ARVO) Statement for the Use of Animals in Ophthalmic and Vision Research and approved by the Faculty Committee at The University of Hong Kong (CULATR No.4927-19 and CULATR No.5835-21).
Data Availability Statement
The data that support the findings of this study are provided in the paper.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Schwartz, S.G.; Scott, I.U.; Flynn Jr, H.W.; Stewart, M.W. Drug delivery techniques for treating age-related macular degeneration. Expert Opin. Drug Deliv. 2014, 11, 61–68. [Google Scholar] [CrossRef]
- Bourne, R.R.A.; Flaxman, S.R.; Braithwaite, T.; Cicinelli, M.V.; Das, A.; Jonas, J.B.; Keeffe, J.; Kempen, J.H.; Leasher, J.; Limburg, H.; et al. Magnitude, temporal trends, and projections of the global prevalence of blindness and distance and near vision impairment: A systematic review and meta-analysis. Lancet Glob Health 2017, 5, e888–e897. [Google Scholar] [CrossRef]
- Yellepeddi, V.K.; Palakurthi, S. Recent Advances in Topical Ocular Drug Delivery. J Ocul Pharmacol Ther 2016, 32, 67–82. [Google Scholar] [CrossRef]
- Reardon, G.; Kotak, S.; Schwartz, G.F. Objective assessment of compliance and persistence among patients treated for glaucoma and ocular hypertension: A systematic review. Patient Prefer Adherence 2011, 5, 441–463. [Google Scholar] [CrossRef]
- Kim, Y.C.; Chiang, B.; Wu, X.; Prausnitz, M.R. Ocular delivery of macromolecules. J Control Release 2014, 190, 172–181. [Google Scholar] [CrossRef]
- Sampat, K.M.; Garg, S.J. Complications of intravitreal injections. Curr Opin Ophthalmol 2010, 21, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Yasukawa, T.; Tabata, Y.; Kimura, H.; Ogura, Y. Recent advances in intraocular drug delivery systems. Recent Pat Drug Deliv Formul 2011, 5, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Orive, G.; Hernández, R.M.; Gascón, A.R.; Calafiore, R.; Chang, T.M.; De Vos, P.; Hortelano, G.; Hunkeler, D.; Lacík, I.; Shapiro, A.M.; et al. Cell encapsulation: Promise and progress. Nat Med 2003, 9, 104–107. [Google Scholar] [CrossRef] [PubMed]
- Kuramoto, S.; Yasuhara, T.; Agari, T.; Kondo, A.; Jing, M.; Kikuchi, Y.; Shinko, A.; Wakamori, T.; Kameda, M.; Wang, F. BDNF-secreting capsule exerts neuroprotective effects on epilepsy model of rats. Brain Res. 2011, 1368, 281–289. [Google Scholar] [CrossRef]
- Aebischer, P.; Pochon, N.; Heyd, B.; Deglon, N.; Joseph, J.; Zurn, A.; Baetge, E.; Hammang, J.; Goddard, M.; Lysaght, M. Gene therapy for amyotrophic lateral sclerosis (ALS) using a polymer encapsulated xenogenic cell line engineered to secrete hCNTF. Hum. Gene Ther. 1996, 7, 851–860. [Google Scholar]
- Orive, G.; Hernández, R.M.; Gascón, A.R.; Calafiore, R.; Chang, T.M.; Vos, P.D.; Hortelano, G.; Hunkeler, D.; Lacík, I.; Shapiro, A.J. Cell encapsulation: Promise and progress. Nat. Med. 2003, 9, 104–107. [Google Scholar] [CrossRef]
- Goldberg, J.L.; Beykin, G.; Satterfield, K.R.; Nuñez, M.; Lam, B.L.; Albini, T.A. Phase I NT-501 Ciliary Neurotrophic Factor Implant Trial for Primary Open-Angle Glaucoma: Safety, Neuroprotection, and Neuroenhancement. Ophthalmol. Sci. 2023, 3. [Google Scholar] [CrossRef] [PubMed]
- Piller Puicher, E.; Tomanin, R.; Salvalaio, M.; Friso, A.; Hortelano, G.; Marin, O.; Scarpa, M. Encapsulated engineered myoblasts can cure Hurler syndrome: Preclinical experiments in the mouse model. Gene Ther. 2012, 19, 355–364. [Google Scholar] [CrossRef]
- Dubrot, J.; Portero, A.; Orive, G.; Hernández, R.M.; Palazón, A.; Rouzaut, A.; Perez-Gracia, J.L.; Hervás-Stubbs, S.; Pedraz, J.L.; Melero, I. Delivery of immunostimulatory monoclonal antibodies by encapsulated hybridoma cells. Cancer Immunol. Immunother. 2010, 59, 1621–1631. [Google Scholar] [CrossRef] [PubMed]
- Tao, W.; Wen, R.; Goddard, M.B.; Sherman, S.D.; O’Rourke, P.J.; Stabila, P.F.; Bell, W.J.; Dean, B.J.; Kauper, K.A.; Budz, V.A.; et al. Encapsulated cell-based delivery of CNTF reduces photoreceptor degeneration in animal models of retinitis pigmentosa. Invest Ophthalmol Vis Sci 2002, 43, 3292–3298. [Google Scholar] [PubMed]
- Kang-Mieler, J.J.; Rudeen, K.M.; Liu, W.; Mieler, W.F. Advances in ocular drug delivery systems. Eye 2020, 34, 1371–1379. [Google Scholar] [CrossRef] [PubMed]
- Kiss, S. Interim Results and Key Learnings from an Ongoing Phase 2 Study of Encapsulated Cell Therapy Compared to Aflibercept in Patients With Wet AMD. In Proceedings of the American Society of Retina Specialists annual meeting, San Francisco, CA, USA, 9–14 August 2016. [Google Scholar]
- Lin, J.B.; Murakami, Y.; Miller, J.W.; Vavvas, D.G. Neuroprotection for Age-Related Macular Degeneration. Ophthalmol Sci 2022, 2, 100192. [Google Scholar] [CrossRef] [PubMed]
- Frasson, M.; Picaud, S.; Léveillard, T.; Simonutti, M.; Mohand–Said, S.; Dreyfus, H.; Hicks, D.; Sahel, J. Glial Cell Line–Derived Neurotrophic Factor Induces Histologic and Functional Protection of Rod Photoreceptors in the rd/rd Mouse. Investig. Ophthalmol. Vis. Sci. 1999, 40, 2724–2734. [Google Scholar]
- Orive, G.; Santos, E.; Poncelet, D.; Hernández, R.M.; Pedraz, J.L.; Wahlberg, L.U.; De Vos, P.; Emerich, D. Cell encapsulation: Technical and clinical advances. Trends Pharmacol. Sci. 2015, 36, 537–546. [Google Scholar] [CrossRef]
- An, D.; Chiu, A.; Flanders, J.A.; Song, W.; Shou, D.; Lu, Y.-C.; Grunnet, L.G.; Winkel, L.; Ingvorsen, C.; Christophersen, N.S. Designing a retrievable and scalable cell encapsulation device for potential treatment of type 1 diabetes. Proc. Natl. Acad. Sci. USA 2018, 115, E263–E272. [Google Scholar] [CrossRef]
- Lee, K.Y.; Mooney, D.J. Alginate: Properties and biomedical applications. Prog Polym Sci 2012, 37, 106–126. [Google Scholar] [CrossRef] [PubMed]
- Ghidoni, I.; Chlapanidas, T.; Bucco, M.; Crovato, F.; Marazzi, M.; Vigo, D.; Torre, M.L.; Faustini, M. Alginate cell encapsulation: New advances in reproduction and cartilage regenerative medicine. Cytotechnology 2008, 58, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Andersen, T.; Auk-Emblem, P.; Dornish, M. 3D Cell Culture in Alginate Hydrogels. Microarrays 2015, 4, 133–161. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Xiao, W.; Tang, Y.; Li, K.; Fan, H. Biomimetic interpenetrating polymer network hydrogels based on methacrylated alginate and collagen for 3D pre-osteoblast spreading and osteogenic differentiation. Soft Matter 2012, 8, 2398–2404. [Google Scholar] [CrossRef]
- Sang, L.; Luo, D.; Xu, S.; Wang, X.; Li, X. Fabrication and evaluation of biomimetic scaffolds by using collagen–alginate fibrillar gels for potential tissue engineering applications. Mater. Sci. Eng. C 2011, 31, 262–271. [Google Scholar] [CrossRef]
- Thackaberry, E.A.; Lorget, F.; Farman, C.; Bantseev, V. The safety evaluation of long-acting ocular delivery systems. Drug Discov Today 2019, 24, 1539–1550. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.J.; Hong, H.K.; Na, Y.M.; Park, S.J.; Ahn, J.; Oh, J.; Chung, J.Y.; Park, K.H.; Woo, S.J. Use of Rabbit Eyes in Pharmacokinetic Studies of Intraocular Drugs. J Vis Exp 2016. [Google Scholar] [CrossRef]
- del Amo, E.M.; Urtti, A. Rabbit as an animal model for intravitreal pharmacokinetics: Clinical predictability and quality of the published data. Exp. Eye Res. 2015, 137, 111–124. [Google Scholar] [CrossRef]
- Okonkwo, O.N.; Tripathy, K. Ocular Hypotony. In StatPearls; Copyright © 2023, StatPearls Publishing LLC.: Treasure Island, FL, USA, 2023. [Google Scholar]
- Lee, B.R.; Hwang, J.W.; Choi, Y.Y.; Wong, S.F.; Hwang, Y.H.; Lee, D.Y.; Lee, S.-H. In situ formation and collagen-alginate composite encapsulation of pancreatic islet spheroids. Biomaterials 2012, 33, 837–845. [Google Scholar] [CrossRef]
- Wong, F.S.Y.; Tsang, K.K.; Chu, A.M.W.; Chan, B.P.; Yao, K.M.; Lo, A.C.Y. Injectable cell-encapsulating composite alginate-collagen platform with inducible termination switch for safer ocular drug delivery. Biomaterials 2019, 201, 53–67. [Google Scholar] [CrossRef]
- Anderson, J.M.; Rodriguez, A.; Chang, D.T. Foreign body reaction to biomaterials. Semin Immunol 2008, 20, 86–100. [Google Scholar] [CrossRef] [PubMed]
- Madeira, M.H.; Elvas, F.; Boia, R.; Gonçalves, F.Q.; Cunha, R.A.; Ambrósio, A.F.; Santiago, A.R. Adenosine A2AR blockade prevents neuroinflammation-induced death of retinal ganglion cells caused by elevated pressure. J Neuroinflammation 2015, 12, 115. [Google Scholar] [CrossRef] [PubMed]
- Wolf, S.A.; Boddeke, H.W.; Kettenmann, H. Microglia in Physiology and Disease. Annu Rev Physiol 2017, 79, 619–643. [Google Scholar] [CrossRef]
- Mizutani, M.; Gerhardinger, C.; Lorenzi, M. Müller cell changes in human diabetic retinopathy. Diabetes 1998, 47, 445–449. [Google Scholar] [CrossRef]
- Burkersroda, F.v.; Schedl, L.; Göpferich, A. Why degradable polymers undergo surface erosion or bulk erosion. Biomaterials 2002, 23, 4221–4231. [Google Scholar] [CrossRef]
- Lewis, G.P.; Fisher, S.K. Up-regulation of glial fibrillary acidic protein in response to retinal injury: Its potential role in glial remodeling and a comparison to vimentin expression. Int Rev Cytol 2003, 230, 263–290. [Google Scholar] [CrossRef] [PubMed]
- Kimble, T.D.; Fitzgerald, M.E.; Reiner, A. Sustained upregulation of glial fibrillary acidic protein in Müller cells in pigeon retina following disruption of the parasympathetic control of choroidal blood flow. Exp Eye Res 2006, 83, 1017–1030. [Google Scholar] [CrossRef]
- Giordano, G.G.; Chevez-Barrios, P.; Refojo, M.F.; Garcia, C.A. Biodegradation and tissue reaction to intravitreous biodegradable poly(D,L-lactic-co-glycolic)acid microspheres. Curr Eye Res 1995, 14, 761–768. [Google Scholar] [CrossRef]
- Boia, R.; Dias, P.A.N.; Martins, J.M.; Galindo-Romero, C.; Aires, I.D.; Vidal-Sanz, M.; Agudo-Barriuso, M.; de Sousa, H.C.; Ambrósio, A.F.; Braga, M.E.M.; et al. Porous poly(ε-caprolactone) implants: A novel strategy for efficient intraocular drug delivery. J Control Release 2019, 316, 331–348. [Google Scholar] [CrossRef]
- Bringmann, A.; Pannicke, T.; Grosche, J.; Francke, M.; Wiedemann, P.; Skatchkov, S.N.; Osborne, N.N.; Reichenbach, A. Müller cells in the healthy and diseased retina. Prog Retin Eye Res 2006, 25, 397–424. [Google Scholar] [CrossRef]
- Orive, G.; Santos, E.; Poncelet, D.; Hernández, R.M.; Pedraz, J.L.; Wahlberg, L.U.; De Vos, P.; Emerich, D. Cell encapsulation: Technical and clinical advances. Trends Pharmacol Sci 2015, 36, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Smidsrød, O.; Skjåk-Braek, G. Alginate as immobilization matrix for cells. Trends Biotechnol 1990, 8, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Ashimova, A.; Yegorov, S.; Negmetzhanov, B.; Hortelano, G. Cell Encapsulation Within Alginate Microcapsules: Immunological Challenges and Outlook. Front. Bioeng. Biotechnol. 2019, 7. [Google Scholar] [CrossRef] [PubMed]
- Arifin, D.R.; Kulkarni, M.; Kadayakkara, D.; Bulte, J.W.M. Fluorocapsules allow in vivo monitoring of the mechanical stability of encapsulated islet cell transplants. Biomaterials 2019, 221, 119410. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Lu, Z.; Wu, H.; Li, W.; Zheng, L.; Zhao, J. Collagen-alginate as bioink for three-dimensional (3D) cell printing based cartilage tissue engineering. Mater. Sci. Eng. C 2018, 83, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Birkedal-Hansen, H.; Moore, W.G.; Bodden, M.K.; Windsor, L.J.; Birkedal-Hansen, B.; DeCarlo, A.; Engler, J.A. Matrix metalloproteinases: A review. Crit Rev Oral Biol Med 1993, 4, 197–250. [Google Scholar] [CrossRef] [PubMed]
- Aimes, R.T.; Quigley, J.P. Matrix Metalloproteinase-2 Is an Interstitial Collagenase: INHIBITOR-FREE ENZYME CATALYZES THE CLEAVAGE OF COLLAGEN FIBRILS AND SOLUBLE NATIVE TYPE I COLLAGEN GENERATING THE SPECIFIC ¾- AND ¼-LENGTH FRAGMENTS (∗). J. Biol. Chem. 1995, 270, 5872–5876. [Google Scholar] [CrossRef] [PubMed]
- Jin, M.; Kashiwagi, K.; Iizuka, Y.; Tanaka, Y.; Imai, M.; Tsukahara, S. Matrix metalloproteinases in human diabetic and nondiabetic vitreous. Retina 2001, 21, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Kokavec, J.; Min, S.H.; Tan, M.H.; Gilhotra, J.S.; Newland, H.S.; Durkin, S.R.; Grigg, J.; Casson, R.J. Biochemical analysis of the living human vitreous. Clin. Exp. Ophthalmol. 2016, 44, 597–609. [Google Scholar] [CrossRef]
- Farmer, J.G.; Benomran, F.; Watson, A.A.; Harland, W.A. Magnesium, potassium, sodium and calcium in post-mortem vitreous humour from humans. Forensic Sci Int 1985, 27, 1–13. [Google Scholar] [CrossRef]
- Brown, D.J.; Bishop, P.; Hamdi, H.; Kenney, M.C. Cleavage of structural components of mammalian vitreous by endogenous matrix metalloproteinase-2. Curr Eye Res 1996, 15, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Bochenek, M.A.; Veiseh, O.; Vegas, A.J.; McGarrigle, J.J.; Qi, M.; Marchese, E.; Omami, M.; Doloff, J.C.; Mendoza-Elias, J.; Nourmohammadzadeh, M.; et al. Alginate encapsulation as long-term immune protection of allogeneic pancreatic islet cells transplanted into the omental bursa of macaques. Nat Biomed Eng 2018, 2, 810–821. [Google Scholar] [CrossRef] [PubMed]
- Strand, B.L.; Coron, A.E.; Skjak-Braek, G. Current and future perspectives on alginate encapsulated pancreatic islet. Stem Cells Transl. Med. 2017, 6, 1053–1058. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; He, S.; Chen, B. Retinoic acid-loaded alginate microspheres as a slow release drug delivery carrier for intravitreal treatment. Biomed. Pharmacother. 2018, 97, 722–728. [Google Scholar] [CrossRef] [PubMed]
- Medawar, P. Immunity to homologous grafted skin. III. The fate of skin homographs transplanted to the brain, to subcutaneous tissue, and to the anterior chamber of the eye. Br. J. Exp. Pathol. 1948, 29, 58. [Google Scholar] [PubMed]
- Ahn, Y.H.; Bensadoun, J.C.; Aebischer, P.; Zurn, A.D.; Seiger, A.; Björklund, A.; Lindvall, O.; Wahlberg, L.; Brundin, P.; Kaminski Schierle, G.S. Increased fiber outgrowth from xeno-transplanted human embryonic dopaminergic neurons with co-implants of polymer-encapsulated genetically modified cells releasing glial cell line-derived neurotrophic factor. Brain Res Bull 2005, 66, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Aydin, E.; Kazi, A.A.; Peyman, G.A.; Esfahani, M.R.; Muñoz-Morales, A.; Kivilcim, M.; Caro-Magdaleno, M. [Retinal toxicity of intravitreal doxycycline. A pilot study]. Arch Soc Esp Oftalmol 2007, 82, 223–228. [Google Scholar] [CrossRef]
- Mileva, R.; Rusenov, A.; Milanova, A. Population Pharmacokinetic Modelling of Orally Administered Doxycycline to Rabbits at Different Ages. Antibiotics 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Al-Maweri, S.A.; Halboub, E.; Ashraf, S.; Alqutaibi, A.Y.; Qaid, N.M.; Yahya, K.; Alhajj, M.N. Single application of topical doxycycline in management of recurrent aphthous stomatitis: A systematic review and meta-analysis of the available evidence. BMC Oral Health 2020, 20, 231. [Google Scholar] [CrossRef]
- RIOND, J.-L.; RIVIERE, J.E.; DUCKETT, W.M.; ATKINS, C.E.; JERNIGAN, A.D.; RIKIHISA, Y.; SPURLOCK, S.L. Cardiovascular effects and fatalities associated with intravenous administration of doxycycline to horses and ponies. Equine Vet. J. 1992, 24, 41–45. [Google Scholar] [CrossRef]
- Dogbevia, G.K.; Marticorena-Alvarez, R.; Bausen, M.; Sprengel, R.; Hasan, M.T. Inducible and combinatorial gene manipulation in mouse brain. Front Cell Neurosci 2015, 9, 142. [Google Scholar] [CrossRef] [PubMed]
- McGee Sanftner, L.H.; Rendahl, K.G.; Quiroz, D.; Coyne, M.; Ladner, M.; Manning, W.C.; Flannery, J.G. Recombinant AAV-Mediated Delivery of a Tet-Inducible Reporter Gene to the Rat Retina. Mol. Ther. 2001, 3, 688–696. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.J.; Gillett, A.; Booth, R.; Kimble, B.; Govendir, M. Pharmacokinetic Profile of Doxycycline in Koala Plasma after Weekly Subcutaneous Injections for the Treatment of Chlamydiosis. Animals 2022, 12. [Google Scholar] [CrossRef]
- Ejstrup, R.; Kiilgaard, J.F.; Tucker, B.A.; Klassen, H.J.; Young, M.J.; La Cour, M. Pharmacokinetics of intravitreal glial cell line-derived neurotrophic factor: Experimental studies in pigs. Exp Eye Res 2010, 91, 890–895. [Google Scholar] [CrossRef]
- Santa-Cecília, F.V.; Leite, C.A.; Del-Bel, E.; Raisman-Vozari, R. The Neuroprotective Effect of Doxycycline on Neurodegenerative Diseases. Neurotox. Res. 2019, 35, 981–986. [Google Scholar] [CrossRef] [PubMed]
- Scott, I.U.; Jackson, G.R.; Quillen, D.A.; Larsen, M.; Klein, R.; Liao, J.; Holfort, S.; Munch, I.C.; Gardner, T.W. Effect of doxycycline vs placebo on retinal function and diabetic retinopathy progression in patients with severe nonproliferative or non-high-risk proliferative diabetic retinopathy: A randomized clinical trial. JAMA Ophthalmol 2014, 132, 535–543. [Google Scholar] [CrossRef]
- Kiuchi, K.; Yoshizawa, K.; Shikata, N.; Moriguchi, K.; Tsubura, A. Morphologic characteristics of retinal degeneration induced by sodium iodate in mice. Curr Eye Res 2002, 25, 373–379. [Google Scholar] [CrossRef]
- Potic, J.; Bergin, C.; Giacuzzo, C.; Daruich, A.; Pournaras, J.-A.; Kowalczuk, L.; Behar-Cohen, F.; Konstantinidis, L.; Wolfensberger, T.J. Changes in visual acuity and photoreceptor density using adaptive optics after retinal detachment repair. Retina 2020, 40, 376–386. [Google Scholar] [CrossRef]
- Park, D.H.; Choi, K.S.; Sun, H.J.; Lee, S.J. Factors associated with visual outcome after macula-off rhegmatogenous retinal detachment surgery. Retina 2018, 38, 137–147. [Google Scholar] [CrossRef]
- Chowers, G.; Cohen, M.; Marks-Ohana, D.; Stika, S.; Eijzenberg, A.; Banin, E.; Obolensky, A. Course of Sodium Iodate–Induced Retinal Degeneration in Albino and Pigmented Mice. Investig. Ophthalmol. Vis. Sci. 2017, 58, 2239–2249. [Google Scholar] [CrossRef]
- Paolone, G.; Falcicchia, C.; Lovisari, F.; Kokaia, M.; Bell, W.J.; Fradet, T.; Barbieri, M.; Wahlberg, L.U.; Emerich, D.F.; Simonato, M. Long-Term, Targeted Delivery of GDNF from Encapsulated Cells Is Neuroprotective and Reduces Seizures in the Pilocarpine Model of Epilepsy. J Neurosci 2019, 39, 2144–2156. [Google Scholar] [CrossRef] [PubMed]
- Lindvall, O.; Wahlberg, L.U. Encapsulated cell biodelivery of GDNF: A novel clinical strategy for neuroprotection and neuroregeneration in Parkinson’s disease? Exp Neurol 2008, 209, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Balmer, J.; Zulliger, R.; Roberti, S.; Enzmann, V. Retinal Cell Death Caused by Sodium Iodate Involves Multiple Caspase-Dependent and Caspase-Independent Cell-Death Pathways. Int J Mol Sci 2015, 16, 15086–15103. [Google Scholar] [CrossRef] [PubMed]
- Dunaief, J.L.; Dentchev, T.; Ying, G.-S.; Milam, A.H. The Role of Apoptosis in Age-Related Macular Degeneration. Arch. Ophthalmol. 2002, 120, 1435–1442. [Google Scholar] [CrossRef] [PubMed]
- Enzbrenner, A.; Zulliger, R.; Biber, J.; Pousa, A.M.Q.; Schäfer, N.; Stucki, C.; Giroud, N.; Berrera, M.; Kortvely, E.; Schmucki, R.; et al. Sodium Iodate-Induced Degeneration Results in Local Complement Changes and Inflammatory Processes in Murine Retina. Int J Mol Sci 2021, 22. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.M.; Ahn, J.; Cha, S.; Yun, C.; Park, T.K.; Kim, Y.-J.; Goo, Y.S.; Kim, S.-W. The effects of intravitreal sodium iodate injection on retinal degeneration following vitrectomy in rabbits. Sci. Rep. 2019, 9, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ma, D.; Chen, C.-B.; Liang, J.; Lu, Z.; Chen, H.; Zhang, M. Repeatability, reproducibility and agreement of intraocular pressure measurement in rabbits by the TonoVet and Tono-Pen. Sci. Rep. 2016, 6, 35187. [Google Scholar] [CrossRef] [PubMed]
- Jiao, H.; Provis, J.M.; Natoli, R.; Rutar, M. Ablation of C3 modulates macrophage reactivity in the outer retina during photo-oxidative damage. Mol Vis 2020, 26, 679–690. [Google Scholar] [PubMed]
- Zhou, R.; Li, Y.; Qian, H.; Maminishkis, A.; Jha, B.; Campos, M.M.; Amaral, J.; Stanzel, B.; Bharti, K. Sodium iodate-induced retina and choroid damage model in rabbits to test efficacy of RPE auto-transplants. Investig. Ophthalmol. Vis. Sci. 2016, 57, 2253–2253. [Google Scholar]
- Zhang, X.; Cheng, M.; Chintala, S.K. Kainic acid-mediated upregulation of matrix metalloproteinase-9 promotes retinal degeneration. Investig. Ophthalmol. Vis. Sci. 2004, 45, 2374–2383. [Google Scholar] [CrossRef]
- Kondo, M.; Sakai, T.; Komeima, K.; Kurimoto, Y.; Ueno, S.; Nishizawa, Y.; Usukura, J.; Fujikado, T.; Tano, Y.; Terasaki, H. Generation of a Transgenic Rabbit Model of Retinal Degeneration. Investig. Ophthalmol. Vis. Sci. 2009, 50, 1371–1377. [Google Scholar] [CrossRef]
Figure 1.
Schematic diagrams illustrating a CAC ECT gel designed for drug delivery, equipped with a controllable biosafety switch and outlining the comprehensive experimental setup. (A), Gel safety and performance were assessed in the healthy New Zealand White Rabbit. (B), Gel termination can be achieved by Dox administration when necessary and its biosafety termination mechanism. (C), Therapeutic efficacy of gel was assessed in rabbits with retinal degeneration induced by sodium iodate. CAC ECT, collagen-alginate composite encapsulated cell therapy. HEK, human embryonic kidney. GDNF, glial cell-derived neurotrophic factor. Dox, doxycycline.
Figure 1.
Schematic diagrams illustrating a CAC ECT gel designed for drug delivery, equipped with a controllable biosafety switch and outlining the comprehensive experimental setup. (A), Gel safety and performance were assessed in the healthy New Zealand White Rabbit. (B), Gel termination can be achieved by Dox administration when necessary and its biosafety termination mechanism. (C), Therapeutic efficacy of gel was assessed in rabbits with retinal degeneration induced by sodium iodate. CAC ECT, collagen-alginate composite encapsulated cell therapy. HEK, human embryonic kidney. GDNF, glial cell-derived neurotrophic factor. Dox, doxycycline.
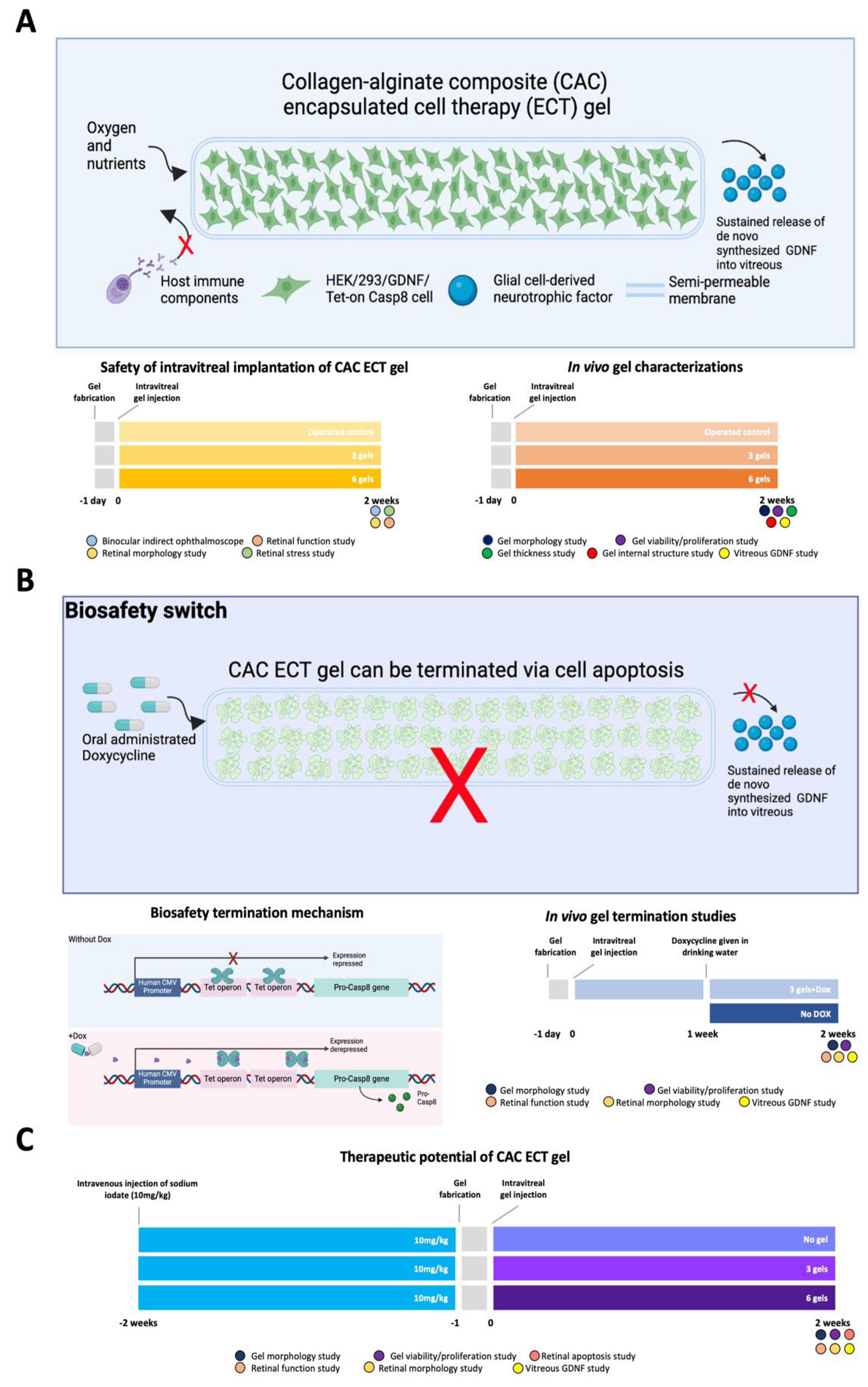
Figure 2.
Intravitreal injection of CAC ECT gels induced no changes in retinal function and retinal cytoarchitecture (A). The photopic and scotopic electroretinographic responses indicated retinal function of different groups, including the unoperated control, 3-gel, and 6-gel groups at 2 weeks. Photopic 5 a-wave and b-wave (mean ± SEM, n = 11, 4 and 3 animals for unoperated control, 3-gel and 6-gel groups, respectively), scotopic 0.01 a-wave and b-wave (mean ± SEM, n = 11, 4 and 6 animals for unoperated control, 3-gel and 6-gel groups, respectively) and scotopic 10 a-wave and b-wave (mean ± SEM, n = 12, 6 and 4 animals for unoperated control, 3-gel and 6-gel groups, respectively). (B) Representative images of H&E staining in rabbit retina: unoperated control, operated control, 3-gel and 6-gel. Scale bar, 50 μm. (C) The thickness of ONL, OPL, INL, and IPL in rabbits sacrificed at 2 weeks post operation. No significant changes in retinal thickness were obtained after One-way ANOVA followed by Bonferroni’s post-hoc comparisons tests. (mean ± SEM, n = 5, 3, 5, and 5 animals for unoperated control, operated control, 3-gels, and 6-gel respectively). OPL, outer plexiform layer. IPL, inner plexiform layer.
Figure 2.
Intravitreal injection of CAC ECT gels induced no changes in retinal function and retinal cytoarchitecture (A). The photopic and scotopic electroretinographic responses indicated retinal function of different groups, including the unoperated control, 3-gel, and 6-gel groups at 2 weeks. Photopic 5 a-wave and b-wave (mean ± SEM, n = 11, 4 and 3 animals for unoperated control, 3-gel and 6-gel groups, respectively), scotopic 0.01 a-wave and b-wave (mean ± SEM, n = 11, 4 and 6 animals for unoperated control, 3-gel and 6-gel groups, respectively) and scotopic 10 a-wave and b-wave (mean ± SEM, n = 12, 6 and 4 animals for unoperated control, 3-gel and 6-gel groups, respectively). (B) Representative images of H&E staining in rabbit retina: unoperated control, operated control, 3-gel and 6-gel. Scale bar, 50 μm. (C) The thickness of ONL, OPL, INL, and IPL in rabbits sacrificed at 2 weeks post operation. No significant changes in retinal thickness were obtained after One-way ANOVA followed by Bonferroni’s post-hoc comparisons tests. (mean ± SEM, n = 5, 3, 5, and 5 animals for unoperated control, operated control, 3-gels, and 6-gel respectively). OPL, outer plexiform layer. IPL, inner plexiform layer.
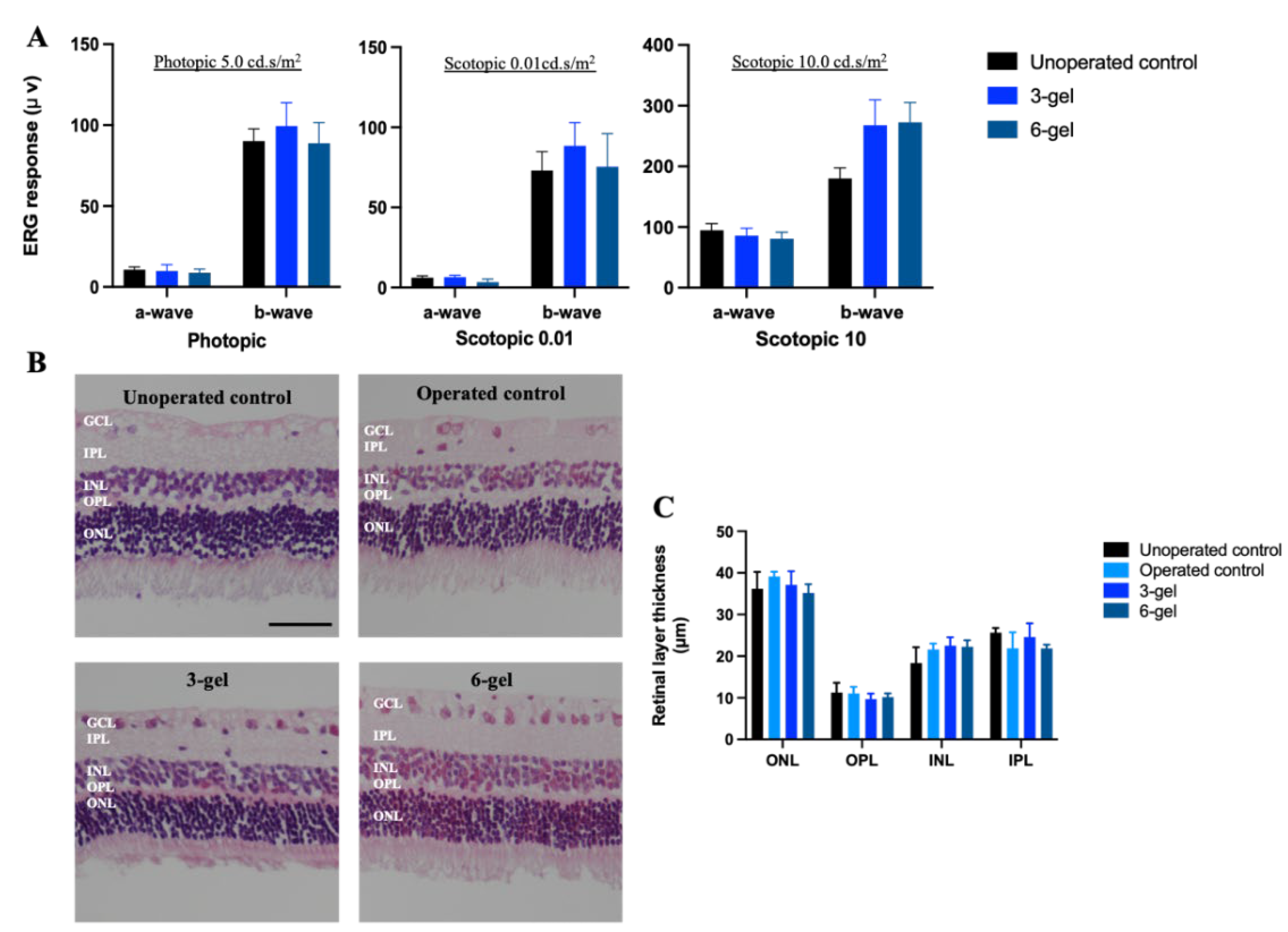
Figure 3.
CAC ECT gel may cause stress in the retina, as assessed by gliosis in Müller cells. (A-B) CAC ECT gels were injected into the vitreous cavity, and rabbits were euthanized 2 weeks later. Immunostaining of retinal paraffin was performed to detect microglial cells (Iba-1) (A), and astrocytes (GFAP) (B), with nuclear staining by DAPI (blue). Scale bar, 50 µm.
Figure 3.
CAC ECT gel may cause stress in the retina, as assessed by gliosis in Müller cells. (A-B) CAC ECT gels were injected into the vitreous cavity, and rabbits were euthanized 2 weeks later. Immunostaining of retinal paraffin was performed to detect microglial cells (Iba-1) (A), and astrocytes (GFAP) (B), with nuclear staining by DAPI (blue). Scale bar, 50 µm.
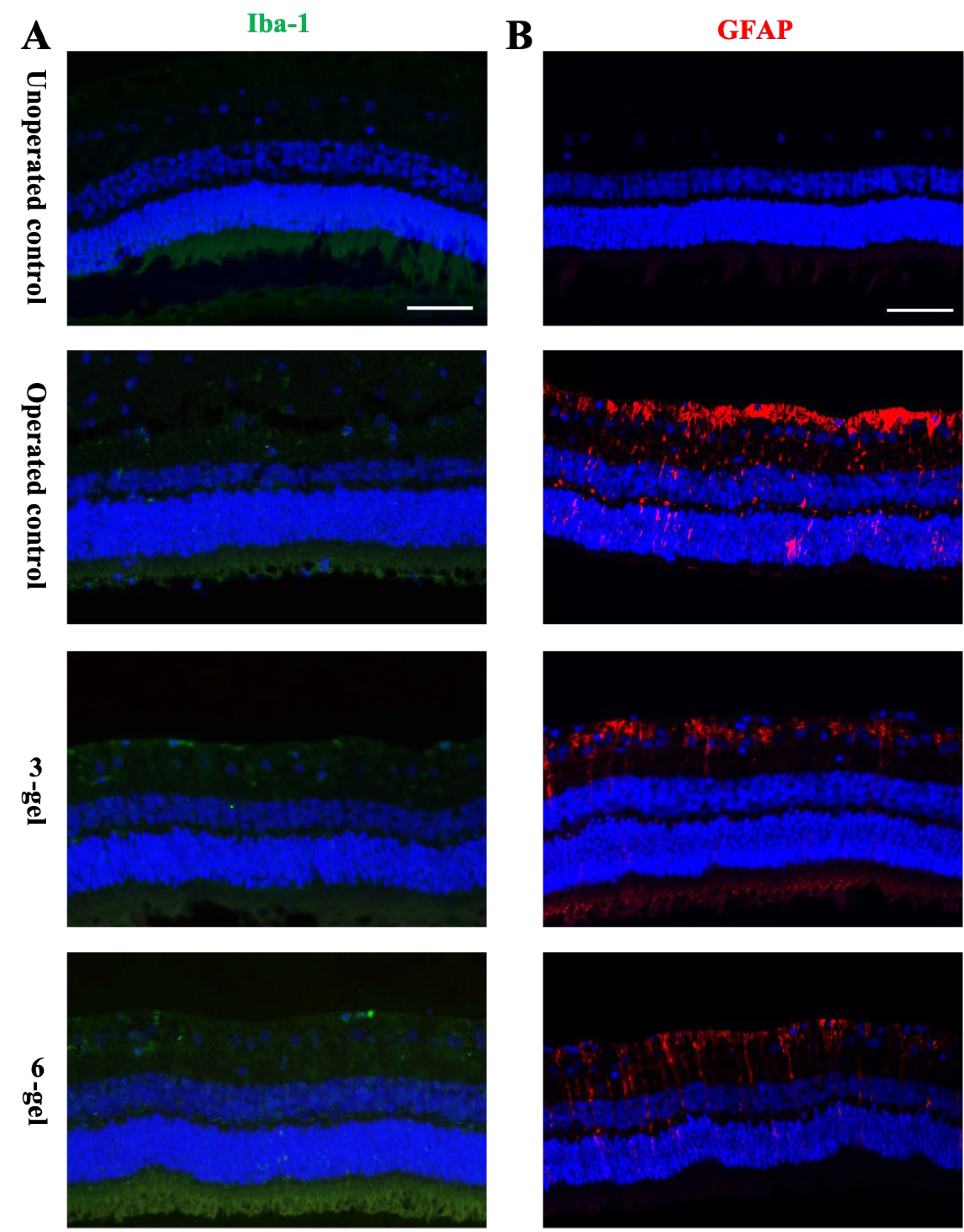
Figure 4.
In vivo performance of CAC ECT gel after 2-week implantation. (A) Morphology of gels on fabrication day and retrieved gels after 2-week implantation. Scale bar, 100 μm. (B) Diameter of gel before and after implantation (mean ± SEM, n = 6, 6, and 6 for pre-implantation level, 3 gels, and 6gels, respectively), One-way ANOVA with Dunnett’s post-hoc test demonstrated no significant difference. (C) Diameter of acellular outer region (mean ± SEM, n = 6, 6, and 6 for pre-implantation level, 3 gels, and 6 gels, respectively). One-way ANOVA with Dunnett’s post-hoc test demonstrated no significant difference. (D) SEM images showing the microstructure of CAC ECT gel, focusing on gel surface and core region after 2-week implantation. Top row: Porous IPN network consisting of collagen and alginate was assembled on the surface of CAC gel and a magnified view of porous network. Bottom row: cells were surrounded by collagen fibrils and CAC matrix and a magnified view of internal structure (*: alginate, +: collagen, #: cell).
Figure 4.
In vivo performance of CAC ECT gel after 2-week implantation. (A) Morphology of gels on fabrication day and retrieved gels after 2-week implantation. Scale bar, 100 μm. (B) Diameter of gel before and after implantation (mean ± SEM, n = 6, 6, and 6 for pre-implantation level, 3 gels, and 6gels, respectively), One-way ANOVA with Dunnett’s post-hoc test demonstrated no significant difference. (C) Diameter of acellular outer region (mean ± SEM, n = 6, 6, and 6 for pre-implantation level, 3 gels, and 6 gels, respectively). One-way ANOVA with Dunnett’s post-hoc test demonstrated no significant difference. (D) SEM images showing the microstructure of CAC ECT gel, focusing on gel surface and core region after 2-week implantation. Top row: Porous IPN network consisting of collagen and alginate was assembled on the surface of CAC gel and a magnified view of porous network. Bottom row: cells were surrounded by collagen fibrils and CAC matrix and a magnified view of internal structure (*: alginate, +: collagen, #: cell).
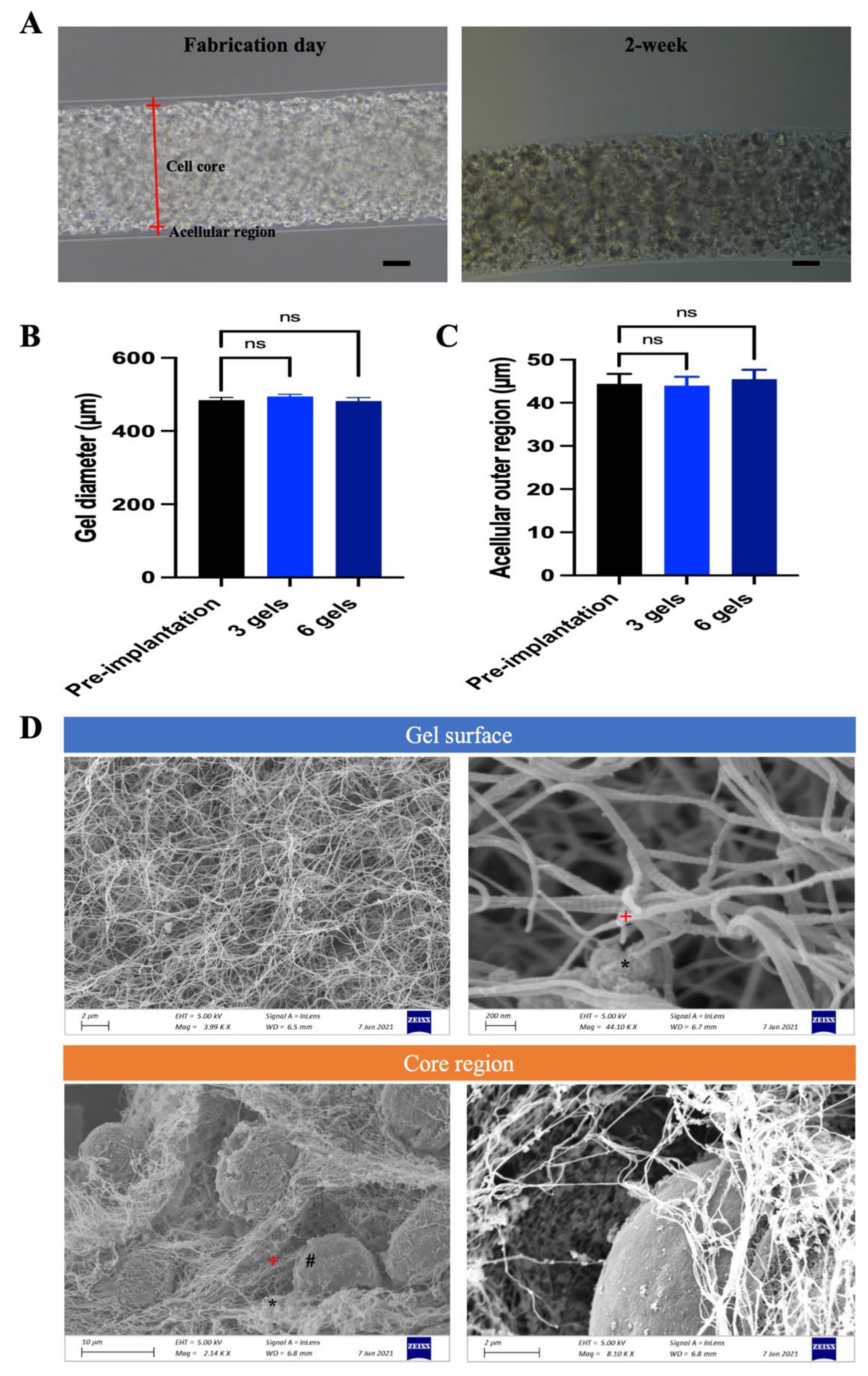
Figure 5.
Retrieved gels were mostly viable at 2 weeks and secreted GDNF in a dose-dependent manner. (A) Morphology (left column) and Live-Dead image (right column) of retrieved CAC ECT gels from 3-gel and 6-gel after 2 weeks of implantation. Scale bar, 100 μm. (B) Viability of retrieved gels from 3-gel and 6-gel group at 2 weeks assessed by Live-Dead assay (mean ± SD, n = 6, and 6 for 3-gel and 6-gel respectively). Unpaired t-test demonstrated no significant differences. ns, not significant. (C) Vitreous GDNF level measured by ELISA assay (mean ± SEM, n = 5, 3, 5, and 5 for unoperated control, operated control, 3-gel, and 6-gel respectively). ****p<0.0001 by One-way ANOVA followed by Bonferroni’s post-hoc comparisons tests.
Figure 5.
Retrieved gels were mostly viable at 2 weeks and secreted GDNF in a dose-dependent manner. (A) Morphology (left column) and Live-Dead image (right column) of retrieved CAC ECT gels from 3-gel and 6-gel after 2 weeks of implantation. Scale bar, 100 μm. (B) Viability of retrieved gels from 3-gel and 6-gel group at 2 weeks assessed by Live-Dead assay (mean ± SD, n = 6, and 6 for 3-gel and 6-gel respectively). Unpaired t-test demonstrated no significant differences. ns, not significant. (C) Vitreous GDNF level measured by ELISA assay (mean ± SEM, n = 5, 3, 5, and 5 for unoperated control, operated control, 3-gel, and 6-gel respectively). ****p<0.0001 by One-way ANOVA followed by Bonferroni’s post-hoc comparisons tests.

Figure 6.
One week of Dox administration can decrease encapsulated cell viability and terminate gel functionality, without affecting retinal morphology and causing changes in retinal function. (A) Phase contrast microscopic images of non-Dox treated gels and Dox treated gel. Scale bar, 100 μm. (B) Live-Dead image of retrieved gel from Dox treated group showing the distribution of viable cells and dying cells. Scale bar, 100 μm. (C) Relative cell viability of no Dox treated group and Dox treated group assessed by MTS assay. (mean ± SD, n = 11, and 6 for no Dox and +Dox group). ****p < 0.0001 by unpaired t-test. (D) Accumulated GDNF levels in rabbit vitreous by GDNF ELISA after 1 week of oral Dox administration. (mean ± SEM, n = 5, and 4 for non-Dox and Dox group respectively). ***p<0.001 unpaired t-test. (E) H&E-stained retinal sections demonstrated no major change in retinal cytoarchitecture. Scale bar, 50 μm. (F) The thickness of various retinal layers including ONL, OPL, INL, IPL, and GCL was measured. (mean ± SEM, n = 5, 4 and 4 for unoperated control, non-Dox and +Dox respectively). One-way ANOVA with Bonferroni post-hoc test demonstrated not significant differences. (G) The ERG response indicating the retinal functions of different groups including unoperated control, non-Dox and +Dox. Amplitudes of major wave components quantified included photopic 5 a- and b-wave (mean ± SEM, n = 6, 6 and 4 animals for unoperated control, non-Dox and +Dox respectively), scotopic 0.01 a-wave and b-wave (mean ± SEM, n = 6, 6 and 4 animals for unoperated control, non-Dox and +Dox respectively) and scotopic 10 a-wave and b-wave (mean ± SEM, n = 6, 6 and 4 animals for unoperated control, non-Dox and +Dox respectively). Statistical analysis using one-way ANOVA with Bonferroni post-hoc test demonstrated no significant differences. Dox, doxycycline.
Figure 6.
One week of Dox administration can decrease encapsulated cell viability and terminate gel functionality, without affecting retinal morphology and causing changes in retinal function. (A) Phase contrast microscopic images of non-Dox treated gels and Dox treated gel. Scale bar, 100 μm. (B) Live-Dead image of retrieved gel from Dox treated group showing the distribution of viable cells and dying cells. Scale bar, 100 μm. (C) Relative cell viability of no Dox treated group and Dox treated group assessed by MTS assay. (mean ± SD, n = 11, and 6 for no Dox and +Dox group). ****p < 0.0001 by unpaired t-test. (D) Accumulated GDNF levels in rabbit vitreous by GDNF ELISA after 1 week of oral Dox administration. (mean ± SEM, n = 5, and 4 for non-Dox and Dox group respectively). ***p<0.001 unpaired t-test. (E) H&E-stained retinal sections demonstrated no major change in retinal cytoarchitecture. Scale bar, 50 μm. (F) The thickness of various retinal layers including ONL, OPL, INL, IPL, and GCL was measured. (mean ± SEM, n = 5, 4 and 4 for unoperated control, non-Dox and +Dox respectively). One-way ANOVA with Bonferroni post-hoc test demonstrated not significant differences. (G) The ERG response indicating the retinal functions of different groups including unoperated control, non-Dox and +Dox. Amplitudes of major wave components quantified included photopic 5 a- and b-wave (mean ± SEM, n = 6, 6 and 4 animals for unoperated control, non-Dox and +Dox respectively), scotopic 0.01 a-wave and b-wave (mean ± SEM, n = 6, 6 and 4 animals for unoperated control, non-Dox and +Dox respectively) and scotopic 10 a-wave and b-wave (mean ± SEM, n = 6, 6 and 4 animals for unoperated control, non-Dox and +Dox respectively). Statistical analysis using one-way ANOVA with Bonferroni post-hoc test demonstrated no significant differences. Dox, doxycycline.
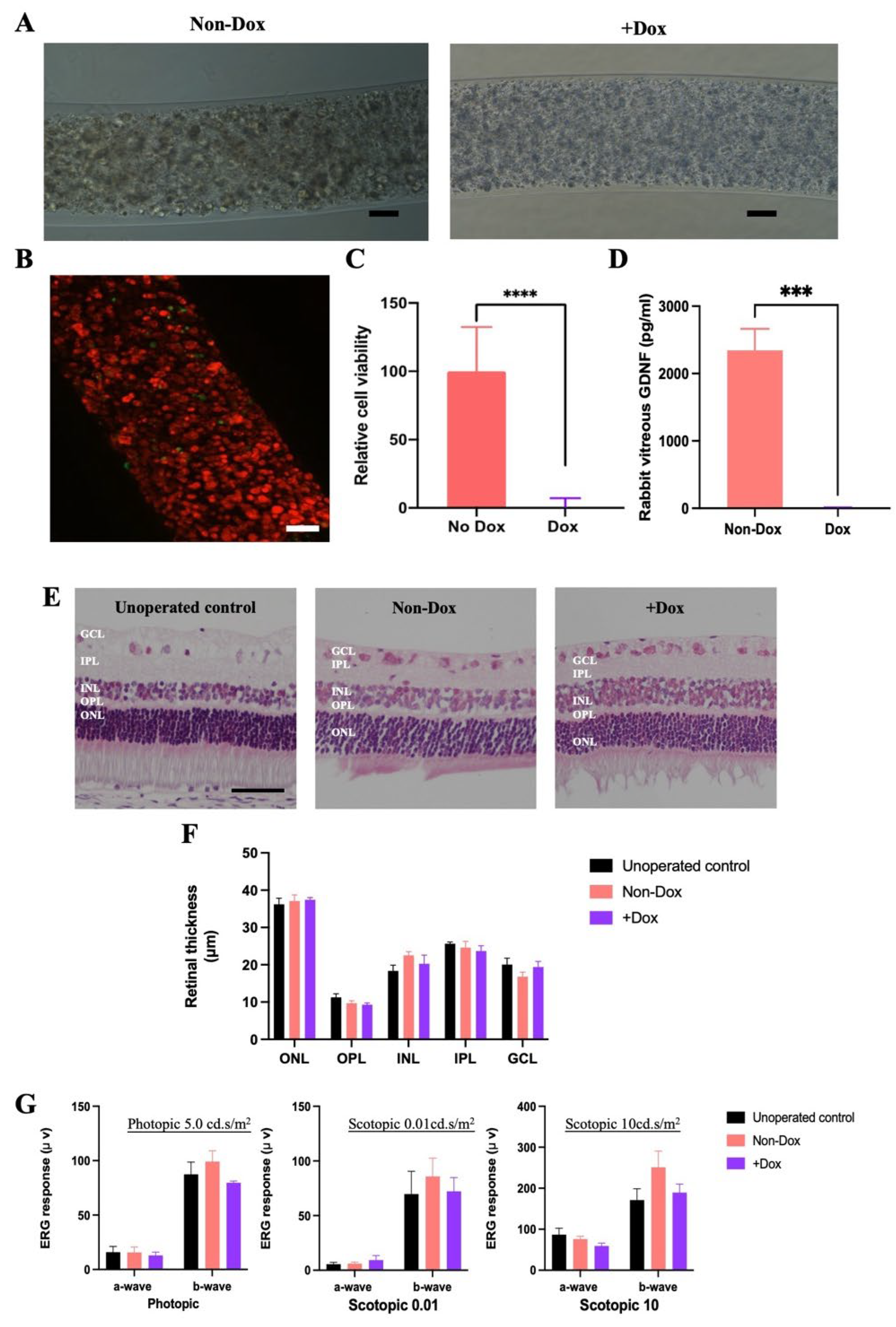
Figure 7.
The therapeutical efficacy of CAC ECT gels in rabbit with retinal degeneration induced by SI. (A) Scotopic a-wave and b-wave electroretinographic responses were measured at 10 cd.s/m2 indicating retinal functions in normal rabbit eyes (baseline) and SI-induced rabbit eyes including no gel-injected eyes, and eyes injected with 3 and 6 gels. (mean ± SEM, n = 11, 8, 7 and 6 independent animals for baseline, no gel, 3-gel and 6-gel). *p < 0.05, **p < 0.01, ***p < 0.001, ****p < 0.0001 by one-way ANOVA followed by Dunnett’s post-test. (B) Representative image of H&E-stained retinal sections from healthy rabbits (baseline), rabbits received with SI only, rabbits with 3-gel and 6g-gel treatment. Scale bar, 50 µm. (C) The thickness of ONL containing the photoreceptor nuclei was significantly higher in rabbits treated with CAC ECT gels when compared with no gel-treated rabbits after 2-week implantation. (mean ± SEM, n = 6, 8, 7, 6 for baseline, no gel, 3-gel and 6-gel group). *p < 0.05 by one-way ANOVA followed by Dunnett post t-test. (D) The number of ONL nuclei per mm was significantly higher in rabbits with 3-gel and 6-gel injection compared with no gel-treated rabbits after 2-week implantation. (mean ± SEM, n = 6, 8, 7 and 6 for baseline, no gel, 3-gel and 6-gel group). ****p < 0.0001 by one-way ANOVA followed by Dunnett post t-test. (E) Representative images showing the distribution of apoptotic cells in the retina detected by TUNEL assay and nuclei were stained by DAPI, TUNEL = terminal deoxynucleotidyl transferase dUTP nick end labeling DAPI = 4‘,6-diamidino-2-phenylindole. Scale bar, 50 µm. (F) The number of TUNEL positive apoptotic cell in ONL significantly decreased in SI-induced rabbits treated with 3-gel and 6-gel compared with no gel-treated rabbits after 2-week implantation. (G) Live/Dead assay showed that 3 gels-treated and 6 gels-treated animals contained mostly living cells (green). Scale bar, 100 μm. (H) Increased vitreous GDNF level only detected in rabbits with gel treatment. * p<0.05; **p<0.01; ***p<0.001; ****p<0.0001 by one-way ANOVA with Bonferroni post-hoc.
Figure 7.
The therapeutical efficacy of CAC ECT gels in rabbit with retinal degeneration induced by SI. (A) Scotopic a-wave and b-wave electroretinographic responses were measured at 10 cd.s/m2 indicating retinal functions in normal rabbit eyes (baseline) and SI-induced rabbit eyes including no gel-injected eyes, and eyes injected with 3 and 6 gels. (mean ± SEM, n = 11, 8, 7 and 6 independent animals for baseline, no gel, 3-gel and 6-gel). *p < 0.05, **p < 0.01, ***p < 0.001, ****p < 0.0001 by one-way ANOVA followed by Dunnett’s post-test. (B) Representative image of H&E-stained retinal sections from healthy rabbits (baseline), rabbits received with SI only, rabbits with 3-gel and 6g-gel treatment. Scale bar, 50 µm. (C) The thickness of ONL containing the photoreceptor nuclei was significantly higher in rabbits treated with CAC ECT gels when compared with no gel-treated rabbits after 2-week implantation. (mean ± SEM, n = 6, 8, 7, 6 for baseline, no gel, 3-gel and 6-gel group). *p < 0.05 by one-way ANOVA followed by Dunnett post t-test. (D) The number of ONL nuclei per mm was significantly higher in rabbits with 3-gel and 6-gel injection compared with no gel-treated rabbits after 2-week implantation. (mean ± SEM, n = 6, 8, 7 and 6 for baseline, no gel, 3-gel and 6-gel group). ****p < 0.0001 by one-way ANOVA followed by Dunnett post t-test. (E) Representative images showing the distribution of apoptotic cells in the retina detected by TUNEL assay and nuclei were stained by DAPI, TUNEL = terminal deoxynucleotidyl transferase dUTP nick end labeling DAPI = 4‘,6-diamidino-2-phenylindole. Scale bar, 50 µm. (F) The number of TUNEL positive apoptotic cell in ONL significantly decreased in SI-induced rabbits treated with 3-gel and 6-gel compared with no gel-treated rabbits after 2-week implantation. (G) Live/Dead assay showed that 3 gels-treated and 6 gels-treated animals contained mostly living cells (green). Scale bar, 100 μm. (H) Increased vitreous GDNF level only detected in rabbits with gel treatment. * p<0.05; **p<0.01; ***p<0.001; ****p<0.0001 by one-way ANOVA with Bonferroni post-hoc.
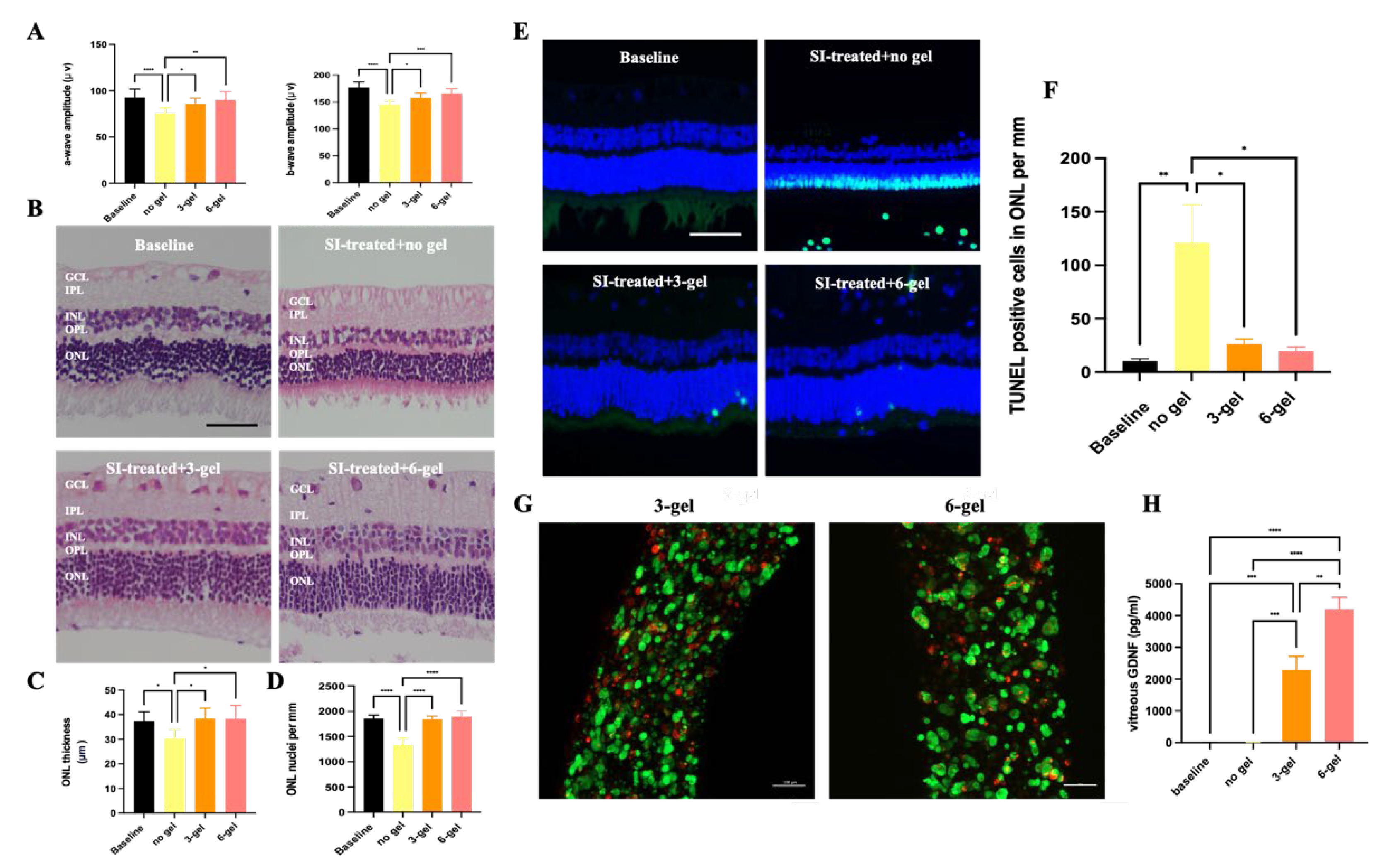
Figure 8.
Schematic diagram showing the detailed preparation of CAC ECT gels. (A) HEK/293/GDNF/Tet-on pro-Casp8 cells were trypsinized. (B) The HEK/293/GDNF/Tet-on pro-Casp8 cell pellet was mixed with collagen and alginate. (C) An aliquot of 2 μL of the gel mixture was prepared. (D) The 2 μL gel mixture was gently transferred to the glass molds. (E) The glass molds containing the 2 μL gel were collected into a 50 ml Falcon tube. (F) The glass molds were then placed in an incubator at 37°C for 75 min to initiate collagen gelation. (G) The glass molds were then introduced to a 100 mM CaCl2 solution followed by a CaCl2 bath to gelate the alginate. (H) The gels were collected from the molds and cultured in DMEM-HG medium before intravitreal gel injection.
Figure 8.
Schematic diagram showing the detailed preparation of CAC ECT gels. (A) HEK/293/GDNF/Tet-on pro-Casp8 cells were trypsinized. (B) The HEK/293/GDNF/Tet-on pro-Casp8 cell pellet was mixed with collagen and alginate. (C) An aliquot of 2 μL of the gel mixture was prepared. (D) The 2 μL gel mixture was gently transferred to the glass molds. (E) The glass molds containing the 2 μL gel were collected into a 50 ml Falcon tube. (F) The glass molds were then placed in an incubator at 37°C for 75 min to initiate collagen gelation. (G) The glass molds were then introduced to a 100 mM CaCl2 solution followed by a CaCl2 bath to gelate the alginate. (H) The gels were collected from the molds and cultured in DMEM-HG medium before intravitreal gel injection.
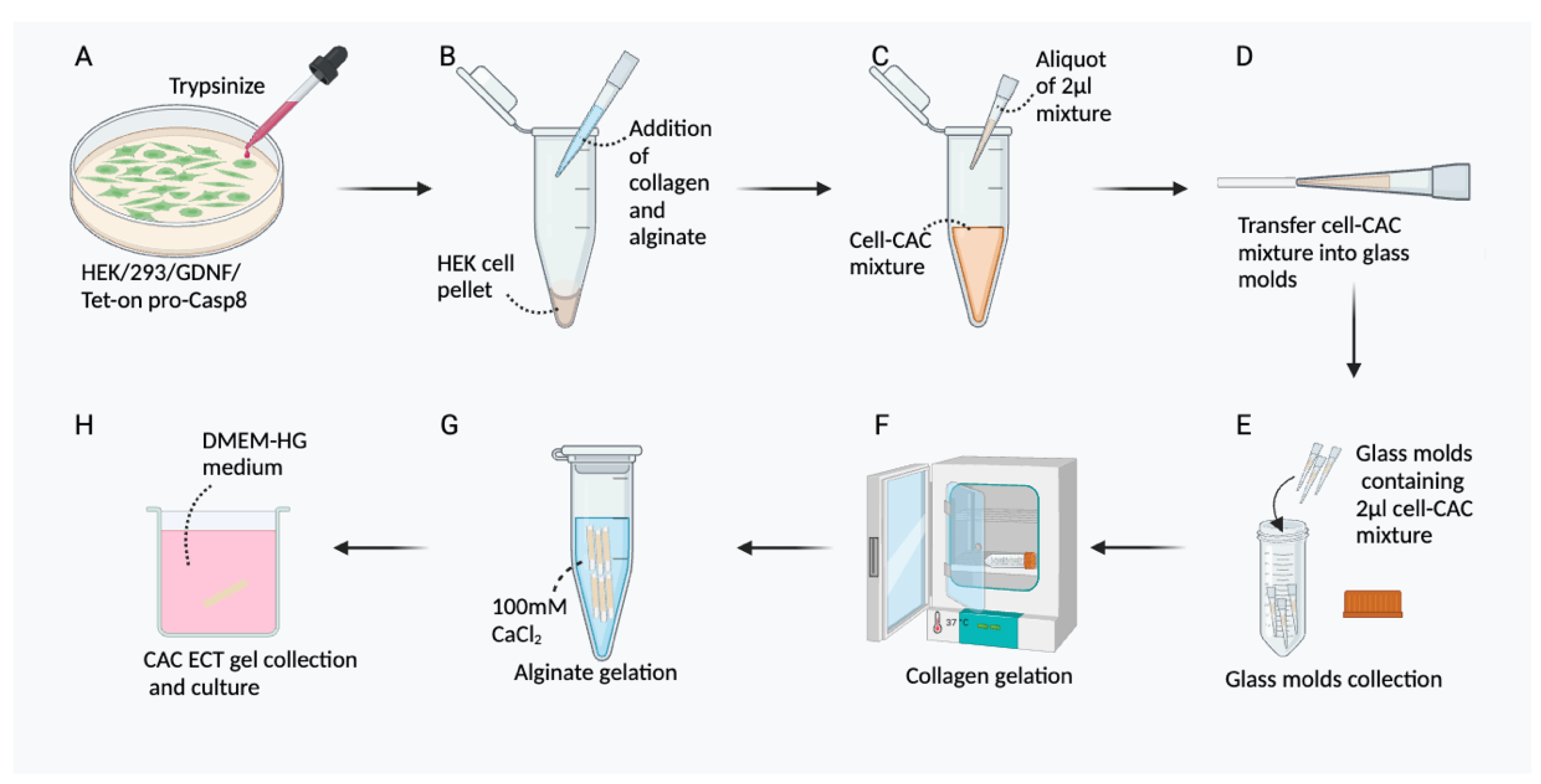

Table 1.
The CAC ECT gel did not cause any alterations in the body weight of the animals and induced a short-term decrease in IOP. The body weight and IOP of the rabbits were assessed post gel implantation 2 weeks. IOP was measured bilaterally in animals after operated control or gel implantation procedure at 2 weeks.
Table 1.
The CAC ECT gel did not cause any alterations in the body weight of the animals and induced a short-term decrease in IOP. The body weight and IOP of the rabbits were assessed post gel implantation 2 weeks. IOP was measured bilaterally in animals after operated control or gel implantation procedure at 2 weeks.
| Unoperated control | Operated control | 3-gel | 6-gel | |
|---|---|---|---|---|
| Body weight (kg) | 3.23±0.17 | 3.35±0.12 | 3.27±0.22 | 3.33±0.19 |
| IOP (mmHg) | 18.75±0.77 | 17.13±0.74 | 14.27±0.74 | 13.5±0.70 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



