
Submitted:
05 August 2024
Posted:
06 August 2024
You are already at the latest version
Abstract
It is challenging to differentiate central nervous system (CNS) virus infections and neurological autoimmune diseases in the emergency department. Considering their different pathogenesis, we assume they differ in neuropsychiatric symptoms and laboratory results. 80 patients were included, 50 with CNS virus infections and 30 with CNS autoimmune diseases, confirmed by polymerase chain reaction (PCR) of cerebrospinal fluid (CSF). A binary logistic regression model and receiver operating characteristic (ROC) curve were conducted to examine the discrimination between the two diseases based on neuropsychiatric symptoms and laboratory results. Compared to patients with neurological autoimmune diseases, patients with CNS virus infections had higher incidence of abnormal behavior (p=0.026) and abnormal sensation/thought (p=0.029), higher total (p = 0.005), direct (p = 0.004), and indirect bilirubin (p = 0.004), increased CSF cell (p = 0.01) and CSF white cell counts (p = 0.01). ROC analysis showed that patients with disturbance of consciousness and abnormal sensation/thought were 7.79-fold and 5.07-fold more likely to be diagnosed with CNS virus infections (OR = 7.79, p = 0.008; OR = 5.07, p = 0.032). Each unit increase in blood indirect bilirubin concentration and CSF white cell counts increased risk of developing CNS virus infections by 1.25-fold and 1.01-fold (OR = 1.25, p = 0.016; OR = 1.01, p = 0.011). Our study found that patients with CNS viral infections tend to have higher blood indirect bilirubin concentration, CSF leukocyte count, frequency of disorders of consciousness, and abnormal sensation and thought, which may help differentiate them from neurological autoimmune diseases.
Keywords:
central nervous system
; virus infections
; neurological autoimmune diseases
; differentiation
1. Introduction
Neuropsychiatric symptoms in an emergency setting, which mainly include abnormal behavior, negative and positive symptoms, disturbance of consciousness, memory deficits, etc. [1], can manifest in both central nervous system (CNS) virus infections and neurological autoimmune diseases, which are diagnosed based on the presence or absence of a clear etiology [1,2,3,4]. Clinically, only based on the initial neuropsychiatric symptoms, without any other obvious physical signs, it is hard to differentiate CNS infections, such as Herpes simplex virus type 1 (HSV-1) encephalitis [5] from neurological autoimmune diseases, such as autoimmune encephalitis [6,7]. In some cases, those patients who had neuropsychiatric symptoms may even be treated with only antipsychotics without controlling the actual etiology, which would aggravate the symptoms of patients and even cause adverse outcomes [8]. Due to their different causes and clinical interventions, early accurate identification is the key for those with shared neuropsychiatric symptoms [2,4].
Studies have identified that infections and autoimmune diseases, the former, such as HSV [9], and the latter, such as anti-NMDA receptor encephalitis [4], play indispensable roles in inducing neuropsychiatric symptoms in different ways [10,11,12,13,14]. Infections can affect the permeability of the blood-brain barrier (BBB) through a series of inflammatory reactions and further trigger neuropsychiatric symptoms [15], which is consistent with the findings of studies exploring biomarkers in the blood and cerebrospinal fluid associated with mental disorders [16]. These studies have found changes in antibodies, albumin ratios, total protein, immunoglobulins, and cytokines, suggesting that BBB leakage or dysfunction may exist in patients with psychiatric disorders and induce neuropsychiatric symptoms [17]. Unlike infections, autoimmune diseases may cause brain dysfunction through autoantibodies [1,2]. Antibodies against neuronal cell-surface proteins, ion channels, or receptors have been found in patients with autoimmune encephalitis. The effects of brain-reactive antibodies are also confirmed by experimental animal studies, which have found that brain-reactive antibodies can induce psychotic-like symptoms [18]. The risk factors of autoimmune diseases include genetic susceptibility and infections [19]. Therefore, these existing results suggest that the combination of blood biomarkers, cerebrospinal fluid (CSF), and mental symptoms helps establish early clinical composite indicators that can distinguish these two types of diseases in the early stage.
However, few studies on the changes in CSF in Chinese patients with neuropsychiatric symptoms have been reported. Additionally, the hypothesis there are differential incidences of neuropsychiatric symptoms and differences in internal molecular biomarkers in Chinese patients with CNS virus infections and neurological autoimmune diseases have not been investigated. Therefore, we utilized the data of neuropsychiatric symptoms and laboratory inspection results of patients with the two types of conditions to explore the differences in the incidence of neuropsychiatric symptoms and internal molecular biomarkers between these two groups. Also, we expected to prove that initial neuropsychiatric symptoms and changes in internal molecular biomarkers could jointly differentiate CNS virus infections and neurological autoimmune diseases.
2. Methods
2.1. Participants and Data Acquisition
Patients included in this study were recruited through the emergency neurology department at Capital Medical University. Recruitment and data collection were conducted between 2020 and 2021. Patients diagnosed with CNS virus infections and CNS autoimmune diseases were included. Patients with a history of epilepsy or substance dependence were excluded. The data collection was fully anonymized and was approved by the ethics committee of Xuanwu Hospital of Capital Medical University.
2.2. Subgroup Definition
Diseases included CNS virus infections and neurological autoimmune diseases, diagnosed by the N2.3. ational Center for Neurological Disorders of China and confirmed with a PCR of CSF positive for virus or antibodies. The details of the patients included in this study are available in the Supplementary Material (Table 1). Neuropsychiatric symptoms are evaluated by clinicians and divided into the following categories based on psychopathology: abnormal behavior, impaired memory, abnormal sensation and thought (including illusions, delusions, and aphasia), and disturbance of consciousness [1].
2.3. Statistical Analyses
Statistical analyses were conducted in IBM SPSS Statistics 25 and RStudio. Categorical variables were compared using Chi-square tests between CNS virus infections and CNS autoimmune diseases, and continuous variables were compared using Wilcoxon rank-sum tests. Associations among diagnosis, neuropsychiatric symptoms, and laboratory inspection results were analyzed using binary logistic regression. Sex and age were included as covariates owing to their putative effects. A p-value < 0.05 was considered significant. The significant area under the curve (AUC) was used as an effective model to the discrimination of CNS virus infections from neurological autoimmune diseases. An area under the curve of at least 0.7 was considered satisfactory, and the null hypothesis value was set at 0.5.
3. Results
3.1. Demographics and Incidence of Neuropsychiatric Symptoms
Eighty patients were included in this study (Table 1), of whom 50 had CNS virus infections and 30 had CNS autoimmune diseases. No significant differences in age (p = 0.988) between the two groups, and the age composition ratio of the patients with different diseases Figure 1 was also failed to reach statistical significance (p = 0.602). There was a slightly higher proportion of males in all patients, with no significant group difference (p = 0.684).
Abnormal behavior is more frequent in patients with CNS virus infections (22.0%) than in those with neurological autoimmune diseases (3.3%), with a significant group difference (p = 0.026); abnormal sensation and thought is more frequent in patients with CNS virus infections (44.0%) than with neurological autoimmune diseases (20.0%), with a significant group difference (p = 0.029). Besides that, the differences of other incidence of neuropsychiatric symptoms in the two groups failed to reach statistical significance.
3.2. Association between Laboratory Inspection Results and Diseases
For blood biochemistry, the median of the concentrations of total bilirubin (p = 0.005), direct bilirubin (p = 0.004), and indirect bilirubin (p = 0.004) were higher in patients with CNS virus infections than in those with neuro-logical autoimmune diseases. However, the differences in other blood biochemistry items between the two types of conditions did not reach statistical significance (Table 2).
For CSF test results, the median of CSF cell counts (p = 0.01) and CSF white cell counts (p = 0.01) were higher in patients with CNS virus infections compared to patients with neurological autoimmune diseases. Apart from these, the differences in other CSF tests between the two types of conditions did not reach statistical significance (Table 3). Further mediation analysis revealed that CSF white cells did not mediate the effect of CSF cells on disease with the 97.5% confidence interval of Za*Zb containing zero (97.5% CI, -1.40e-05 to 3.87e-04).
3.3. Multivariable Analysis
Sex, age, CSF cell counts, CSF white cell counts, blood direct bilirubin concentration, blood indirect bilirubin concentration, and neuropsychiatric symptoms (abnormal behavior, impaired memory, abnormal sensation and thought, and disturbance of consciousness) were put in the model of binary logistic regression with forward LR. Ultimately, CSF white cell counts, blood indirect bilirubin concentration, abnormal sensation and thought, and disturbance of consciousness were selected to be associated with different diagnoses (Table 4). Patients with disturbance of consciousness were 7.79-fold more likely to be diagnosed with CNS virus infections than those without this symptom (OR = 7.79; p = 0.008); patients with abnormal sensation and thought were 5.07-fold more likely to be diagnosed with CNS virus infections than those without this symptom (OR = 5.07; p = 0.032); each unit increase in blood indirect bilirubin concentration was associated with a 1.25-fold increase in the risk of developing CNS virus infections rather than neurological autoimmune diseases (OR = 1.25; p = 0.016); and each unit increase in CSF white cell counts was associated with a 1.01-fold increase in the risk of developing CNS virus infections rather than neurological autoimmune diseases (OR = 1.01; p = 0.011). Receiver operating characteristic (ROC) analysis Figure 1 suggested that the area under the curve was 88.0% (AUC = 0.880, SE = 0.045, 95% CI = 0.792–0.967, p < 0.001).
4. Discussion
The main finding of this study is the confirmation that patients with CNS virus infections tend to have higher blood indirect bilirubin concentration and CSF white cell counts, and higher frequency of disturbance of consciousness and abnormal sensation and thought than patients with neurological autoimmune diseases. In addition, the present study demonstrates that the diagnostic accuracy is relatively sufficient to differentiate CNS virus infections with the four aspects mentioned above.
4.1. Neuropsychiatric Symptoms
Pathophysiology of neuropsychiatric symptoms has been explored in quantity [20,21]. Age has previously been shown to be a risk factor for disturbance of consciousness, which is more likely to occur with increasing age [22,23]. However, further comparison showed the difference in the age composition ratio between the two types of diseases included in this study was failed to reach statistical significance, which supports that the incidence of disturbance of consciousness is significantly different in the two conditions.
Studies have explored the associations between CNS virus infections and mental disorders. HSV-1 infections have been identified to affect the permeability of the blood-brain barrier and gray matter volume, which are the foundation of developing mental disorders; cognitive impairment has also been proven to be associated with herpes virus infections [24,25,26,27].
The mechanisms by which brain-reactive antibodies triggering neuropsychiatric symptoms have been increasingly explored. Previous studies showed that brain-reactive antibodies may target NMDARs in the brain, leading to their removal from the synapse and causing mental symptoms, which is in line with the glutamatergic model of schizophrenia [28]. However, the finding that brain-reactive antibodies can also be found in healthy people afford much food for thought. Recent reports revealed that the seroprevalence, immunoglobulin class, or titers of humoral autoimmunity against brain antigens do not predict disease [29]. That is, the effects of brain-reactive antibodies need more exploration.
4.2. Internal Molecular Biomarkers
The association of patients with CNS virus infections with increased CSF white cell counts is in accordance with previous studies. Increased CSF white cell counts are a signal of an inflammatory response in the central nervous system, and chemoattractant cytokines are thought to play a crucial role in controlling white cells into the subarachnoid space [30,31]. Therefore, increased CSF white cell counts further verified the effects of CNS virus infections on the blood-brain barrier.
As an antioxygen, blood indirect bilirubin is crucial to reactive oxygen species (ROS), which is thought to be the mediator of trans-endothelial migration of monocytes and affect the permeability of the blood-brain barrier [32]. Blood indirect bilirubin is also found to have potential immunomodulatory properties. Our finding that the concentration of blood indirect bilirubin in patients with CNS virus infections is slightly higher than that of patients with neurological autoimmune diseases is in line with previous studies, which have found that the concentration of blood indirect bilirubin is lower in patients with neurological autoimmune diseases like Guillain-Barré syndrome and multiple sclerosis [33,34]. However, absolute blood indirect bilirubin concentrations in the two disease groups in this study differ widely with previous studies. These differences may be attributable to the severity of diseases and sample size, and further studies are needed.
4.3. Strengths and Limitations
This study has several strengths. To our knowledge, it was the first study to investigate whether the differences in the internal molecular biomarkers and the incidence of neuropsychiatric symptoms can help to distinguish Chinese patients with CNS virus infections from those with neurological autoimmune diseases early and precisely. The study included CSF biochemistry results, which can reveal the changes in the brain more directly. Neuropsychiatric symptoms were classified into specific categories rather than sweeping generalizations, which will not only help clinicians to diagnose these diseases more efficiently, but also further research into the mechanisms of different neuropsychiatric symptoms.
The limitations of this study should also be noted. In our cross-sectional study, the status of CNS virus infections of patients with neurological autoimmune diseases hasn’t been learned. For example, one study showed that the prognosis of patients with autoimmune encephalitis after herpes simplex encephalitis was substantially worse than that reported in patients with classical anti-NMDAR encephalitis [9]. Besides, this study lacked comparisons with healthy controls and patients with functional mental disorders. A small sample size and lack of quantitative scores for mental symptoms may also lead to bias in the results.
5. Conclusions
The findings of this study suggest that the ROC curve based on the disturbance of consciousness, abnormal sensation and thought, CSF white cell counts, and indirect blood bilirubin can contribute to differentiating CNS virus infections from neurological autoimmune diseases, which may help make appropriate decisions about further treatment and controlling disease progression at an earlier stage.
Author Contributions
HW: XL, and DG designed the study. XL, LY, and HW contributed to data analysis, data interpretation, and the manuscript draft. DG, HCW, WZ, HW, XJ, LT, ZS and HW contributed to the data collection, clinical project management, medical monitoring, and manuscript preparation. WY and HW supervised the data analyses. WY, HCW, LY, and HW contributed to revising the manuscript.
Funding
This work was partly supported by STI2030-Major Projects+2021ZD0204300, the Beijing Health System Leading Talent Grant (2022-02-10), National Key R&D Program of China (2022YFC2503901), the Postgraduate Education Reform and Quality Improvement Project of Henan Province (YJS2021JD12, YJSCX202113Z).
Ethics approval
This study has been approved by the local ethics review board of Xuanwu Hospital and has been performed per the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. All patients gave their written informed consent before joining the study.
Consent to participate
All patients gave their written informed consent before joining the study.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Acknowledgments
The authors thank all participants and their caregivers for supporting this study. We confirm that we have read the journal’s guidelines on ethical publication issues and affirm that this report is consistent with those guidelines.
Conflicts of Interest
The authors declare that they have no conflict of interest.
References
- Dalmau J, Armangué T, Planagumà J, et al. An update on anti-NMDA receptor encephalitis for neurologists and psychiatrists: mechanisms and models. Lancet Neurol. 2019;18(11):1045-1057. [CrossRef]
- Dalmau J, Graus F. Antibody-Mediated Encephalitis. N Engl J Med. 2018;378(9):840-851. [CrossRef]
- Geis C, Planagumà J, Carreño M, et al. Autoimmune seizures and epilepsy. J Clin Invest. 2019;129(3):926-940. [CrossRef]
- Kayser MS, Dalmau J. Anti-NMDA receptor encephalitis, autoimmunity, and psychosis. Schizophr Res. 2016;176(1):36-40. [CrossRef]
- Asogwa K, Buabeng K, Kaur A. Psychosis in a 15-Year-Old Female with Herpes Simplex Encephalitis in a Background of Mannose-Binding Lecithin Deficiency. Case Rep Psychiatry. 2017;2017:1429847. [CrossRef]
- Deng S, Qiu K, Liu H, et al. Clinical Characteristics and Short-Term Prognosis of Autoimmune Encephalitis: A Single-Center Cohort Study in Changsha, China. Front Neurol. 2019;10:539. [CrossRef]
- Cochen V, Arnulf I, Demeret S, et al. Vivid dreams, hallucinations, psychosis and REM sleep in Guillain-Barré syndrome. Brain. 2005;128(Pt 11):2535-2545. [CrossRef]
- Jang Y, Lee ST, Lim JA, et al. Psychiatric symptoms delay the diagnosis of anti-LGI1 encephalitis. J Neuroimmunol. 2018;317:8-14. [CrossRef]
- Armangue T, Spatola M, Vlagea A, et al. Frequency, symptoms, risk factors, and outcomes of autoimmune encephalitis after herpes simplex encephalitis: a prospective observational study and retrospective analysis. Lancet Neurol. 2018;17(9):760-772. [CrossRef]
- Radhakrishnan R, Kaser M, Guloksuz S. The Link Between the Immune System, Environment, and Psychosis. Schizophr Bull. 2017;43(4):693-697. [CrossRef]
- Pillinger T, D’Ambrosio E, McCutcheon R, et al. Correction to: Is psychosis a multisystem disorder? A meta-review of central nervous system, immune, cardiometabolic, and endocrine alterations in first-episode psychosis and perspective on potential models. Mol Psychiatry. 2019;24(6):928. [CrossRef]
- Noto MN, Maes M, Vargas Nunes SO, et al. BDNF in antipsychotic naive first episode psychosis: Effects of risperidone and the immune-inflammatory response system. J Psychiatr Res. 2021;141:206-213. [CrossRef]
- Misiak B, Bartoli F, Carrà G, et al. Immune-inflammatory markers and psychosis risk: A systematic review and meta-analysis. Psychoneuroendocrinology. 2021;127:105200. [CrossRef]
- Kuchenbecker LA, Tipton PW, Martens Y, et al. Diagnostic Utility of Cerebrospinal Fluid Biomarkers in Patients with Rapidly Progressive Dementia. Ann Neurol. 2024;95(2):299-313. [CrossRef]
- Benros ME, Mortensen PB. Role of Infection, Autoimmunity, Atopic Disorders, and the Immune System in Schizophrenia: Evidence from Epidemiological and Genetic Studies. Curr Top Behav Neurosci. 2020;44:141-159. [CrossRef]
- Orlovska-Waast S, Köhler-Forsberg O, Brix SW, et al. Correction: Cerebrospinal fluid markers of inflammation and infections in schizophrenia and affective disorders: a systematic review and meta-analysis. Mol Psychiatry. 2019;24(6):929-934. [CrossRef]
- Pollak TA, Drndarski S, Stone JM, et al. The blood-brain barrier in psychosis. Lancet Psychiatry. 2018;5(1):79-92. [CrossRef]
- Brimberg L, Mader S, Jeganathan V, et al. Caspr2-reactive antibody cloned from a mother of an ASD child mediates an ASD-like phenotype in mice. Mol Psychiatry. 2016;21(12):1663-1671. [CrossRef]
- Esposito S, Autore G, Argentiero A, et al. Autoimmune encephalitis after herpes simplex encephalitis: A still undefined condition. Autoimmun Rev. 2022;21(12):103187. [CrossRef]
- Peters KR, Rockwood K, Black SE, et al. Neuropsychiatric symptom clusters and functional disability in cognitively-impaired-not-demented individuals. Am J Geriatr Psychiatry. 2008;16(2):136-144. [CrossRef]
- Nestler EJ, Hyman SE. Animal models of neuropsychiatric disorders. Nat Neurosci. 2010;13(10):1161-1169. [CrossRef]
- Inouye SK, Westendorp RG, Saczynski JS. Delirium in elderly people. Lancet. 2014;383(9920):911-922. [CrossRef]
- Hipp DM, Ely EW. Pharmacological and nonpharmacological management of delirium in critically ill patients. Neurotherapeutics. 2012;9(1):158-175. [CrossRef]
- Prasad KM, Eack SM, Goradia D, et al. Progressive gray matter loss and changes in cognitive functioning associated with exposure to herpes simplex virus 1 in schizophrenia: a longitudinal study. Am J Psychiatry. 2011;168(8):822-830. [CrossRef]
- Watson AM, Prasad KM, Klei L, et al. Persistent infection with neurotropic herpes viruses and cognitive impairment. Psychol Med. 2013;43(5):1023-1031. [CrossRef]
- Andreou D, Jørgensen KN, Nerland S, et al. Herpes simplex virus 1 infection on grey matter and general intelligence in severe mental illness. Transl Psychiatry. 2022;12(1):276. [CrossRef]
- Whitford TJ, Wood SJ, Yung A, et al. Structural abnormalities in the cuneus associated with Herpes Simplex Virus (type 1) infection in people at ultra high risk of developing psychosis. Schizophr Res. 2012;135(1-3):175-180. [CrossRef]
- Mikasova L, De Rossi P, Bouchet D, et al. Disrupted surface cross-talk between NMDA and Ephrin-B2 receptors in anti-NMDA encephalitis. Brain. 2012;135(Pt 5):1606-1621. [CrossRef]
- Daguano Gastaldi V, Bh Wilke J, Weidinger CA, et al. Factors predisposing to humoral autoimmunity against brain-antigens in health and disease: Analysis of 49 autoantibodies in over 7000 subjects. Brain Behav Immun. 2023;108:135-147. [CrossRef]
- Rösler A, Pohl M, Braune HJ, et al. Time course of chemokines in the cerebrospinal fluid and serum during herpes simplex type 1 encephalitis. J Neurol Sci. 1998;157(1):82-89. [CrossRef]
- Mahad D, Callahan MK, Williams KA, et al. Modulating CCR2 and CCL2 at the blood-brain barrier: relevance for multiple sclerosis pathogenesis. Brain. 2006;129(Pt 1):212-223. [CrossRef]
- Deng J, Liang XM, Zhang XL, et al. Relationship between serum bilirubin levels and optic neuritis. Chin Med J (Engl). 2013;126(17):3307-3310. [CrossRef]
- Peng F, Deng X, Yu Y, et al. Serum bilirubin concentrations and multiple sclerosis. J Clin Neurosci. 2011;18(10):1355-1359. [CrossRef]
- Li X, Li W, Shi X, et al. Is serum bilirubin associated with the severity of Guillain-Barré syndrome? Int J Neurosci. 2018;128(7):595-599. [CrossRef]
Figure 1.
ROC curve of the model to differentiate CNS virus infections with neurological autoimmune diseases based on abnormal sensation and thought, disturbance of consciousness, blood direct bilirubin concentration and CSF white cell counts. AUC, the area under the ROC curve; CNS, central nervous system; ROC curve, receiver operating characteristic curve.
Figure 1.
ROC curve of the model to differentiate CNS virus infections with neurological autoimmune diseases based on abnormal sensation and thought, disturbance of consciousness, blood direct bilirubin concentration and CSF white cell counts. AUC, the area under the ROC curve; CNS, central nervous system; ROC curve, receiver operating characteristic curve.
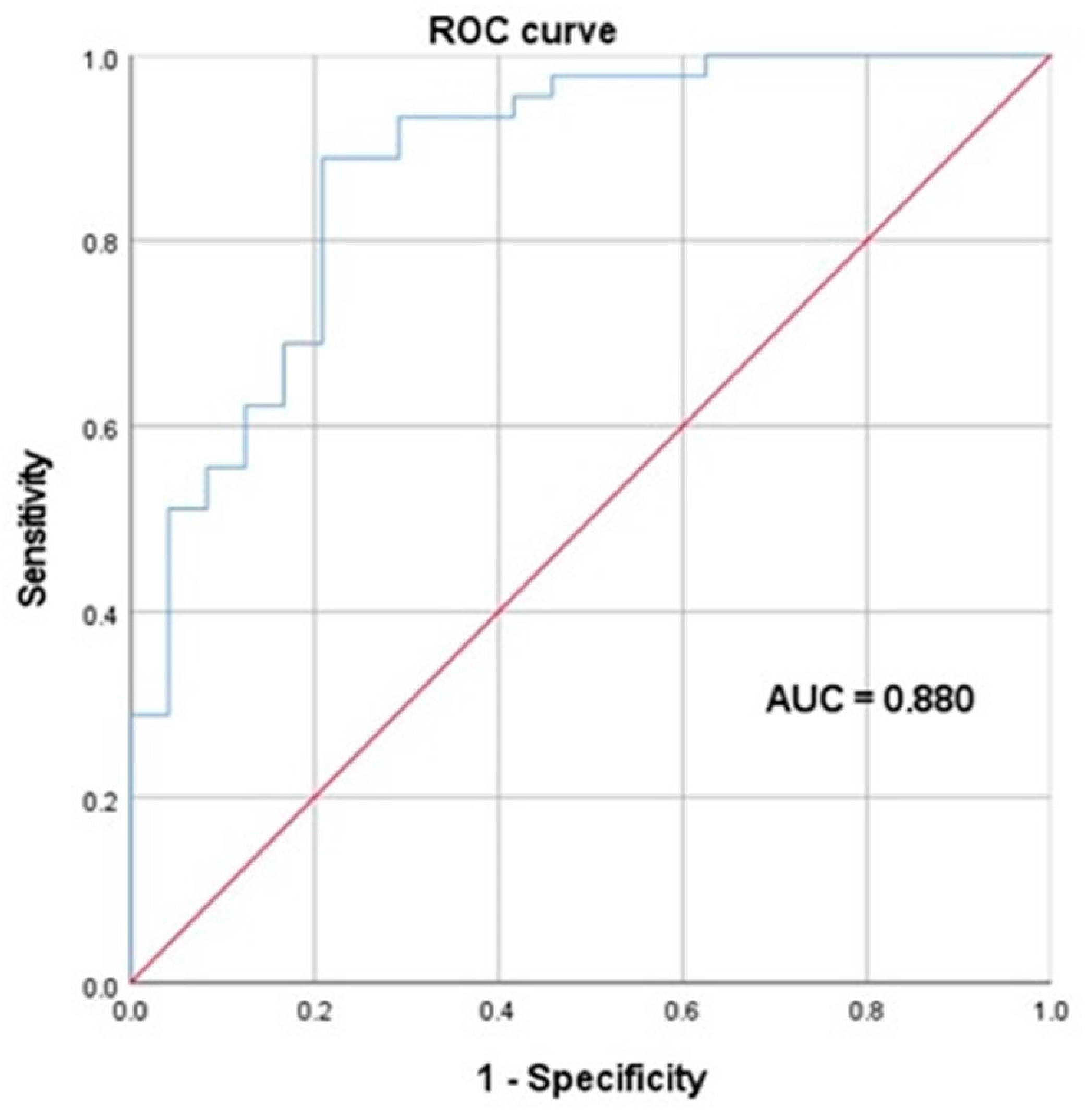

Table 1.
Demographics and incidences of neuropsychiatric symptoms of the studied patients.
| CNS virus infections (N=50) | Neurological autoimmune diseases (N=30) | p | |
|---|---|---|---|
| Sex | |||
| Male | 29 (58.0 %) | 16 (53.3 %) | 0.684 |
| Female | 21 (42.0 %) | 14 (46.7 %) | |
| Age (years) | |||
| Mean (SD) | 48.7 (17.6) | 48.6 (16.9) | 0.988 |
| Abnormal behavior | |||
| without | 39 (78.0 %) | 29 (96.7 %) | 0.026 |
| with | 11 (22.0 %) | 1 (3.3 %) | |
| Impaired memory | |||
| without | 48 (96.0 %) | 27 (90.0 %) | 0.358 |
| with | 2 (4.0 %) | 3 (10.0 %) | |
| Disturbance of consciousness | |||
| without | 30 (60.0 %) | 24 (80.0 %) | 0.064 |
| with | 20 (40.0 %) | 6 (20.0 %) | |
| Abnormal sensation and thought | |||
| without | 28 (56.0 %) | 24 (80.0 %) | 0.029 |
| with | 22 (44.0 %) | 6 (20.0 %) |
The p-value was obtained by chi-square test and t-test. CNS, central nervous system; SD, standard deviation.
Table 2.
Blood biochemistry results details of patients with different diagnosis.
| CNS virus infections | Neurological autoimmune diseases | p-value | |||
|---|---|---|---|---|---|
| Median | [Q1, Q3] | Median | [Q1, Q3] | ||
| Uric acid (μmol/L) | 269 | [178,391] | 252 | [220,331] | 0.833 |
| Creatinine (μmol/L) | 61 | [46.3,71.8] | 52 | [43.0,65.8] | 0.278 |
| Lactate dehydrogenase (IU/L) | 227 | [189,301] | 189 | [168,246] | 0.063 |
| Creatine kinase (IU/L) | 122 | [60.0,457] | 91 | [48.0,140] | 0.074 |
| Urea (mmol/L) | 4.7 | [3.47,5.68] | 4.7 | [4.32,6.50] | 0.611 |
| Total bile acids (μmol/L) | 2.5 | [1.73,4.13] | 4.8 | [2.40,6.20] | 0.060 |
| Indirect bilirubin (μmol/L) | 9.07 | [7.24,13.1] | 6.19 | [5.23,9.24] | 0.005 |
| Direct bilirubin (μmol/L) | 4.56 | [3.49,6.28] | 2.86 | [1.98,4.87] | 0.004 |
| Total bilirubin (μmol/L) | 14.3 | [10.8,19.5] | 9.32 | [6.73,13.4] | 0.004 |
| LDL (mmol/L) | 2.42 | [1.91,3.02] | 2.56 | [2.27,3.06] | 0.447 |
| HDL (mmol/L) | 0.975 | [0.793,1.43] | 1.21 | [0.905,1.44] | 0.278 |
| Triglycerides (mmol/L) | 0.97 | [0.668,1.27] | 0.92 | [0.705,1.36] | 0.656 |
| Albumin (g/L) | 40.6 | [36.3,43.3] | 41.4 | [38.2,43.6] | 0.379 |
The p-value was obtained by rank-sum test. CNS, central nervous system; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Table 3.
CSF test results details of patients with different diagnosis.
| CNS virus infections (N=50) | Neurological autoimmune diseases (N=30) | p-value | |||
|---|---|---|---|---|---|
| Median | [Q1, Q3] | Median | [Q1, Q3] | ||
| CSF cell counts (×106/L) | 263.00 | [40.0,1000] | 11.50 | [2.00,291] | 0.01 |
| CSF white cell counts (×106/L) | 16.50 | [2.75,140] | 2.00 | [1.00,9.00] | 0.01 |
| CSF glucose (mg/dL) | 61.40 | [55.3,73.4] | 66.80 | [57.8,75.1] | 0.53 |
| CSF chloride (mmol/L) | 125.00 | [121,128] | 126.00 | [123,130] | 0.12 |
| CSF protein (mg/dL) | 42.80 | [25.4,89.9] | 44.60 | [29.7,54.5] | 0.77 |
| CSF Lactic-acid (mmol/L) | 1.95 | [1.63,2.68] | 1.80 | [1.60,2.00] | 0.12 |
| CSF IgG (mg/dL) | 5.46 | [3.04,10.3] | 4.61 | [2.44,7.04] | 0.55 |
| CSF IgM (mg/dL) | 0.21 | [0.04,0.45] | 0.09 | [0.06,0.17] | 0.14 |
| CSF IgA (mg/dL) | 0.78 | [0.37,1.46] | 0.46 | [0.33,1.31] | 0.40 |
| IgG intrathecal synthesis rate | 3.18 | [1.52,9.09] | 6.29 | [2.35,9.22] | 0.54 |
The p-value was obtained by rank-sum test. CNS, central nervous system; CSF, cerebrospinal fluid.
Table 4.
Details of the model for differentiating CNS virus infections with neurological autoimmune diseases.
Table 4.
Details of the model for differentiating CNS virus infections with neurological autoimmune diseases.
| Degree of Freedom | P-value | OR | |
|---|---|---|---|
| Disturbance of consciousness | 1 | 0.008 | 7.79 |
| Abnormal sensation and thought | 1 | 0.032 | 5.07 |
| Blood indirect bilirubin | 1 | 0.016 | 1.25 |
| CSF white cell counts | 1 | 0.011 | 1.01 |
The p-value was obtained by Binary Logistic Regression. CSF, cerebrospinal fluid; OR, odds risk.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



