
Submitted:
06 August 2024
Posted:
07 August 2024
You are already at the latest version
Abstract
With an aging population, the prevalence of geriatric diseases is increasing, especially among older individuals who live alone. This study investigates the potential of using TV viewing patterns to detect these diseases by analyzing variables such as daily average viewing time, peak viewing hours, and channel-switching behaviors. Significant correlations between TV viewing patterns and early indicators of geriatric diseases (depression, activities of daily living (ADL) performance, and cognitive function) were found. The correlations between the Korean form of the Geriatric Depression Scale (KGDS) and daily average viewing time and excessive channel switching were 0.320 and 0.308, respectively. The Korean version of the Modified Barthel Index (KMBI) showed correlations of -0.313 with daily average viewing time and -0.352 with excessive channel switching. Participants were divided into groups based on scores, and significant differences in peak viewing hours were observed among the different groups. The Korean version of the Mini-Mental State Examination (MMSE-K) groups showed significant differences at 3, 4, and 5 PM. The KGDS and KMBI groups showed significant differences at 8 PM and midnight and 1 AM and 2 AM, respectively. These findings suggest that TV viewing patterns can serve as effective early diagnostic indicators for geriatric diseases.
Keywords:
older adults
; television
; screen time
; cognition
; depression
; activities of daily living
1. Introduction
The 21st century is witnessing unprecedented changes in global demographic patterns, which are profoundly impacting healthcare systems worldwide. At the core of these changes is population aging, driven by increased life expectancy and decreased fertility rates. From 1950 to 2019, global life expectancy increased by 22.7 years, from 49.0 years to 71.7 years. Additionally, sustained economic growth and advancements in medical technology reduced infant mortality rates and extended the average human life expectancy. However, the increase in life expectancy was accompanied by the challenge of an aging population. Globally, as population aging has progressed, from 2000 to 2021, the proportion of individuals aged 65 and above has increased in 188 out of 204 countries (92.2%), compared to those aged 15 and below [1]. This trend in aging is likely to result in an increase in age-related diseases that will impose significant burdens on healthcare systems, manifesting in increased demand for long-term care services and financial pressures [2].
Geriatric diseases encompass a wide range of cognitive and physical conditions. Among them, cognitive decline, depression, and decreased activities of daily living (ADL) performance are particularly critical. Cognitive decline is closely related to neurodegenerative diseases such as Alzheimer's disease, vascular dementia, and Parkinson's disease, affecting memory, attention, and problem-solving abilities, thereby directly impacting the ability of older individuals to perform daily activities [3]. Depression is a common issue in geriatric diseases and is closely linked with cognitive decline [4]. Older individuals with depression experience more rapid cognitive deterioration, leading to a decrease in ADL function [5]. ADL function measures the ability of older individuals to perform tasks independently, including basic activities such as eating, bathing, dressing, and moving. A decline in ADL function makes independent living difficult, requiring additional care and support.
The early detection of geriatric diseases is crucial in slowing disease progression and preventing complications. Timely diagnosis and management can enhance the quality of life for older people, helping them maintain independence. Recently, innovative methods have been introduced for early detection. For instance, machine learning and artificial intelligence are actively used to predict and diagnose early signs of diseases by analyzing large datasets to assess the risk of conditions such as cardiovascular diseases, diabetes, and dementia [6]. Additionally, technologies like electronic noses that detect volatile organic compounds are used for early diagnosis. These noninvasive methods can identify chemical changes in the body before symptoms appear, making them effective in the early detection of neurodegenerative diseases [7]. However, despite advancements in early diagnostic technologies, the early detection of geriatric diseases through healthcare systems remains limited for older adults. In the case of older individuals living alone, the early diagnosis of geriatric diseases is particularly restricted due to factors such as lack of information, mobility issues, and communication difficulties [8]. Therefore, it is essential to develop friendlier methods for these individuals.
Older people spend approximately 37% of their waking hours watching television, averaging 6.4 hours per day [9]. This indicates that TV viewing occupies a relatively significant portion of older adults' lives. However, such viewing habits do not positively influence health. Prolonged TV watching is associated with an increased risk of dementia, a decline in cognitive functions such as language and memory, and various other negative outcomes for older individuals [10]. Moreover, it has been observed that limitations in physical function, mobility, and agility increase with TV viewing time regardless of physical activity level [11]. Thus, TV viewing and the health of older adults are closely linked, and this suggests the feasibility of analyzing the impact of TV viewing habits on the health statuses of older adults and predicting and responding to their physical and cognitive health conditions.
Older people’s high dependency on TV suggests that their health status can be predicted by analyzing their viewing patterns. Recent studies have explored new methods for managing the health of older people using TV viewing patterns, such as predicting levels of depression among older people using TV viewing time and program types [12] or developing health management algorithms for older adults using TV viewing patterns and motion sensors [13]. However, no research has directly examined the relationship between TV viewing variables and the health of older adults. If a broader range of variables related to TV viewing could be analyzed to reveal and systematize the correlations with the cognitive and psychological state of older individuals, detecting and diagnosing diseases early using only TV viewing patterns could be possible.
Therefore, this study aimed to collect data on detailed TV viewing variables from older individuals living alone, such as daily average viewing time, peak viewing hours, upper zapping threshold, lower zapping threshold, and average zapping per hour. The objective is to reveal the correlations between these variables and the risk factors of geriatric diseases, including cognitive decline, depression and decreased ADL performance. Overall, this study aimed to contribute toward developing an early diagnosis algorithm for geriatric diseases based on the TV viewing patterns of older adults.
2. Materials and Methods
2.1. Subjects
This study was conducted in collaboration with the Administrative Welfare Center in Paju City, Gyeonggi Province, and the real-time TV rating survey company ATAM Co., Ltd. Out of 56 individuals initially recruited, six were excluded due to missing data, resulting in 50 participants' data being utilized for the final statistics.
This research received approval from the Institutional Review Board (IRB) of Sunmoon University (SM-202401-002-3).
The selection criteria for the subjects were as follows:
1) Individuals aged 65 and above living alone;
2) Participants who agreed to participate in the study.
The exclusion criteria for the subjects were as follows:
1) Patients experiencing memory disorders due to neurological abnormalities;
2) Patients with a history of Axis I psychiatric disorders, including intellectual disabilities, schizophrenia, alcohol dependence, and bipolar disorder;
3) Patients who had undergone cerebrovascular surgery;
4) Patients with a history of substance abuse within the past 5 years;
5) Patients with a history of alcohol addiction treatment within the past 5 years;
6) Patients with vision impairment who were unable to read normal text even with the use of glasses;
7) Patients with hearing impairments who found it difficult to understand conversations even with the use of hearing aids;
8) Other patients deemed unsuitable for participation in the clinical trial by the examiner.
2.2. Experimental Procedures
In this study, the inclusion and exclusion criteria were meticulously reviewed to recruit participants, resulting in data being collected from 50 individuals. Based on the gathered data, an analysis was conducted on the correlations between participants' TV viewing patterns and early detection variables for dementia. The research was conducted according to the following procedure (Figure 1).
2.3. Data Collection
In this study, the correlations between variables related to TV viewing patterns and early detection of dementia were analyzed. Descriptions and collection methods for each variable are as follows:
To collect TV viewing pattern data, set-top boxes installed in the homes of older individuals living alone, managed by the Administrative Welfare Center and community centers in Paju City, Republic of Korea, were utilized. These set-top boxes, connected to the participants' TVs for care and welfare purposes, recorded the viewing information. The collected viewing data processed for statistical analysis in this study spanned 3 months, from October 1, 2023, to December 31, 2023, and included daily average viewing time, peak viewing hours, upper zapping threshold (cases where the number of zaps per hour exceeds the upper threshold), lower zapping threshold (cases where the number of zaps per hour is below the lower threshold), and average zapping per hour. The TV viewing variables were created by processing the available TV viewing data to facilitate correlation analysis. Specifically, daily average viewing time was calculated as the total viewing minutes; meanwhile, peak viewing hours were calculated by converting the 24 hours to a percentage and computing the viewing frequency for each time slot as a percentage.
Zapping is defined as entering (zap in) or exiting (zap out) a channel, using a remote control to switch from the currently watched channel to another, thereby avoiding unwanted programs or advertisements or exploring content broadcasted on different channels [14]. This study averaged the number of zapping instances during TV viewing at hourly intervals. According to the classification method of our collaborator, ATAM Co., Ltd., the upper zapping threshold was defined as instances where the current measured data exceeded the maximum value of each individual's past data measured over a specific period (4 weeks). Conversely, the lower zapping threshold was defined as instances where the current measured data fell below the minimum value of each individual's past data measured over the same period.
2.4. Measurements and Instrumentation
To assess the variables for the early detection of dementia, three validated assessment scales were employed: the Mini-Mental State Examination (MMSE) for cognitive assessment, the Geriatric Depression Scale (GDS) for evaluating the level of depression, and the Modified Barthel Index (MBI) for assessing ADL performance level.
2.4.1. MMSE
Developed by Folstein and McHugh in 1975, the MMSE is a cognitive assessment scale that is easier to administer than other cognitive scales and can be completed in 5–10 min. It has the advantage of minimal practice effects, allowing for repeated measurements throughout a disease to observe changes over time. It has demonstrated reliability and validity in screening for moderate to severe dementia patients, and the Korean version (MMSE-K) is the most widely used test in South Korea [15]. The scoring includes 10 points for temporal and spatial orientation (5 points each), 3 points for memory registration, 3 points for recall, 5 points for attention and calculation, 7 points for language function, and 2 points for comprehension and judgment, providing a total of 30 points. A score of 24 or above is considered “no cognitive impairment,” 20–23 is “mild cognitive impairment,” and 19 or below is “severe cognitive impairment.” For illiterate individuals, 1 point for temporal orientation, 2 points for attention and calculation, and 1 point for language function are added, ensuring that the total does not exceed the maximum score for each section [16]. The MMSE-K is widely used across various fields for its high reliability and validity as a simple cognitive function screening tool [17]. Since this study was conducted with Korean participants, the MMSE-K was used.
2.4.2. GDS
The GDS is a screening tool used to evaluate the severity of depressive symptoms in individuals aged 65 and above [18]. The original scale includes 30 items, while shorter versions contain 20, 15, 12, 10, 5, and 4 items. The scale is useful in distinguishing not only depressive disorders in older adults but also cognitive impairments, including dementia and physical illnesses that do not manifest as depressive symptoms. In this study, the scale consisted of 30 items, each scoring 1 point, allowing for a maximum score of 30. According to the score criteria, 0–9 points indicate a normal mood state, 10–19 points indicate mild depressive symptoms, and 20–30 points indicate severe depressive symptoms [19]. The scale is a useful screening and monitoring tool in primary care settings due to its high reliability, validity, sensitivity, and specificity [20]. Since this study was conducted with Korean participants, the Korean form of the GDS (KGDS) was used.
2.4.3. MBI
The MBI is a widely used scale for assessing ADL performance, and it is reported to have a high sensitivity, simplicity, ease of scoring, and high reliability and validity compared to other tools [21]. It consists of 11 items concerning the following ADLs: Personal hygiene, bathing, eating, toilet use, stair climbing, dressing, bowel control, bladder control, ambulation, wheelchair use, and transfers (chair/bed). The wheelchair item is measured only if the individual cannot walk; thus, the actual number of items measured is 10. Each item is scored on a 5–15-point scale, ranging from complete dependence to complete independence, where performing all items completely independently scores 100 points [22]. Since this study was conducted with Korean participants, the Korean version of the MBI (KMBI) was used.
2.5. Statistical Analysis
In this study, descriptive statistics were utilized to calculate general characteristics, including the mean and standard deviation of each variable. All statistical analyses were conducted using IBM SPSS 26.0 statistical software. The Kolmogorov–Smirnov test was performed to examine the normality distribution of the collected data. The correlations between variables were analyzed using Spearman's rank correlation coefficient (rs), which measures the strength of the linear relationship between two variables, where +1 indicates a positive linear relationship, -1 indicates a negative linear relationship, and 0 indicates no linear relationship. Values above 0.9 are considered very high, between 0.7 and 0.9 high, between 0.5 and 0.7 moderate, between 0.3 and 0.5 low, and below 0.3 indicates little, if any relationship, applicable to both positive and negative cases [23].
The Kruskal–Wallis test was also used to analyze peak viewing hours by MMSE-K, KGDS, and KMBI score groups. The following classification criteria for each assessment scale were applied:
2.5.1. MMSE-K
- Severe cognitive impairment group (n = 6): score≤19
- Moderate cognitive impairment group (n = 19): 20≤score≤23
- No cognitive impairment group (n = 25): score≥24
2.5.2. KGDS
- Severe depression group (n = 6): score≥22
- Moderate depression group (n = 2): 19≤score≤21
- Mild depression group (n = 14): 14≤score≤18
- No depression group (n = 28): score≤13
2.5.3. KMBI
- Normal ADL performance group (n = 35): score≥95
- Grade 6 group (n = 10): 85≤score≤94
- Grade 5 (n = 1): 70≤score≤84
- Grade 3 (n = 1): 40≤score≤54
- Grade 1 group (n = 3): score≤24
KMBI Grade 3 and Grade 5 each had only one case, so they were excluded from the statistics. All statistical significance levels were set at α=0.05.
3. Results
3.1. General Characteristics of Subjects
A total of 50 individuals aged 65 and above participated in the study, and the general characteristics are presented in Table 1.
3.2. Analysis of Correlations between TV Viewing Data and Cognitive Function, Depression, and ADL Performance
Normality tests were conducted using the pre- and post-measurement mean values of each variable. In this study, the data did not satisfy normality assumptions (p<0.05), meaning a nonparametric statistical analysis was conducted. According to Spearman's correlation results, no significant correlations were found between MMSE-K and the other variables. The correlation coefficient between KGDS and daily average viewing time was 0.320, indicating a low positive correlation, which was statistically significant (p<0.05). Similarly, the correlation coefficient between KGDS and the upper zapping threshold was 0.308, indicating a low positive correlation, and it was statistically significant (p<0.05). No significant correlation was found between KGDS and the other variables (p>0.05). The correlation coefficient between KMBI and daily average viewing time was -0.313, indicating a low negative correlation, which was statistically significant (p<0.05). Likewise, the correlation coefficient between KMBI and the upper zapping threshold was -0.352, indicating a low negative correlation, and it was statistically significant (p<0.05). No significant correlations were found between KMBI and the other variables (p>0.05). The correlation coefficient between daily average viewing time and the upper zapping threshold was 0.812, indicating a high positive correlation, which was statistically very significant (p<.01). The correlation coefficient between average zapping per hour and the upper zapping threshold was 0.495, indicating a moderate positive correlation, which was also statistically very significant (p<.01) (Table 2).
3.3. Analysis of Peak Viewing Hours by MMSE-K, KGDS, and KMBI Score Groups
As with the previous analyses, a normality test was conducted for this statistic. The statistic did not meet the normality assumption (p<0.05); therefore, nonparametric statistical analysis was performed. According to the results of the Kruskal–Wallis test, significant differences in peak viewing hours among MMSE-K groups were found at 3, 4, and 5 AM (p<0.05). At 3 AM, a significant difference was found between the severe cognitive impairment group and the no cognitive impairment group (p<0.05). At 4 and 5 AM, significant differences were observed between the severe cognitive impairment group and the moderate cognitive impairment group (p<0.05) and between the severe cognitive impairment group and the no cognitive impairment group (p<0.05). In the KGDS groups, a significant difference in peak viewing hours was found at 8 AM (p<0.05). Significant differences were found between the no depression group and the severe depression group (p<0.05) and between the no depression group and the mild depression group (p<0.05). In the KMBI groups, significant differences in peak viewing hours were found at 12, 1, and 2 AM (p<0.05). At 12, 1, and 2 AM, significant differences were found between the Grade 6 group and the normal group (p<0.05). No significant differences were found in the other statistical analyses (p>0.05). These results are presented in Table 3, Table 4 and Table 5.
4. Discussion
In this study, we analyzed the correlations between the TV viewing patterns of older people who live alone and their cognitive abilities, depression levels, and ADL performance levels. Statistical analyses revealed significant correlations between KGDS and KMBI and the daily average viewing time and upper zapping threshold. However, no significant correlations were found between peak viewing hours and MMSE-K.
As the starting point of media technology, TV has brought about significant changes in human culture since its introduction. These changes have influenced not only the realm of entertainment but also human daily life and health. As TV viewing has become an essential part of everyday life, the necessity for research on issues related to TV viewing and health status has emerged. Previous studies have illuminated the correlation between TV viewing and health status from various angles, including cognitive and physical aspects. For instance, according to the study by Neto et al., higher TV viewing times are associated with lower physical activity, leading to higher body mass index, waist circumference, body fat percentage, glucose, triglycerides, and HDL cholesterol levels, thus increasing the risk of obesity and various heart diseases [24]. Moreover, TV has a close association with mental health, as the study by McAnally et al. revealed that excessive TV viewing during childhood and adolescence increases the risk of developing anxiety disorders in older people [25]. These findings suggest that TV viewing, beyond a mere leisure activity, can significantly impact an individual's physical and mental health.
There is abundant research on the outcomes of TV viewing, such as decreased physical activity and increased psychological instability. However, few studies have been conducted on predicting users' health through easily collectible TV viewing variables. Some research studies have solely analyzed TV viewing time [12], while others have utilized applications [26] or employed wearable cameras simultaneously to gather information beyond TV viewing [27]. However, this study distinguishes itself from other studies by exclusively utilizing variables obtained from TV viewing to elucidate their relevance to health information. Assuming that zapping data, including total viewing time, viewing time slots, excessive zapping, and insufficient zapping, would vary according to the user's cognitive, depression, and ADL performance levels, we analyzed the correlations among these variables and derived several significant findings. Among these, the linkage between the degree of depression, the level of ADL performance, and zapping data is particularly meaningful.
The results of this study also include findings consistent with previous research. The correlation coefficient between KGDS and daily average viewing time was 0.320, indicating a low positive correlation and statistical significance. This suggests that higher TV viewing times are associated with higher levels of depression among users, considering that higher KGDS scores indicate increased levels of depression. Santos et al. investigated the associations among television viewing, physical activity, and depressive symptoms in European adults, finding that participants who watched TV for more than 2 h a day had higher depressive symptom scores, which could be mitigated through physical activity [28]. The study by Tolba et al. focused on “binge-watching” and analyzed its associations with depression and loneliness. The study found a relationship between binge-watching and both depression and loneliness, particularly noting that some viewing motives were also related to depression and loneliness, suggesting that binge-watching can negatively impact mental health [29]. Additionally, Yu et al. analyzed the associations between computer/mobile devices and TV viewing and depression, finding that longer TV viewing times were associated with a higher likelihood of depressive symptoms [30]. These results are consistent with the findings of this study.
Additionally, the statistical analysis results of this study showed a low negative correlation coefficient of -0.313 between KMBI and daily average viewing time, which was statistically significant. The KMBI score decreased with the decline in ADL performance, indicating that higher TV viewing times correspond to lower ADL levels. According to Fingerman et al., physical function limitations in older people lead to an increase in TV viewing time. This not only shows a link to decreased social, physical, and productive activities but also suggests the potential for further disabilities or loss of autonomy [31]. García-Esquinas et al. investigated the expected associations between TV viewing time and physical function, mobility, agility, and frailty indicators among older adults in a cohort study, revealing that longer TV viewing times in older adults, regardless of physical activity, are associated with a higher likelihood of physical function limitations [11]. Furthermore, Lin et al. examined the associations of physical activity, muscle-strengthening activities, and TV viewing, finding that excessive TV viewing negatively affects the physical activity of older adults, particularly showing low adherence to muscle-strengthening activities. This suggests a potential association between TV viewing and physical function decline in older adults [32]. Again, these research findings are consistent with the results of this study.
A point of interest in this study was the relationship between zapping and health variables. The statistical analysis of this study revealed a low positive correlation coefficient of 0.308 between the KGDS and upper zapping threshold, which was statistically significant. Similarly, the correlation coefficient between KMBI and the upper zapping threshold was -0.352, indicating a low, statistically significant negative correlation. This suggests that excessive zapping occurs among users with higher levels of depression or reduced physical function. Such findings could be attributed to the anxiety accompanying depression. Generally, higher levels of depression are associated with higher anxiety scores, and factors such as loss of pleasure, dependency, low self-confidence, isolation, medical conditions, poor financial status, memory problems, suffering, identity issues, physical limitations, fear of death, and loneliness contribute to increased depression and anxiety among older adults [33]. To reduce this anxiety, behavioral symptoms such as leg shaking and pacing may occur [34]. These behavioral symptoms are physical reactions commonly observed in states of anxiety and can include zapping as an expression of the physical tension experienced by individuals feeling anxious. Additionally, a decrease in physical activity due to physical function decline can increase anxiety levels. Khodabakhshi-Koolaee et al. investigated loneliness and anxiety according to physical activity among bedridden older individuals, finding higher loneliness and anxiety scores in the less active group [35]. These research findings further support the results of this study.
Interactions among various variables are also noteworthy. The correlation coefficient between daily average viewing time and the upper zapping threshold related to KGDS and KMBI variables was 0.812, indicating a strong positive correlation that was statistically significant. Additionally, the correlation coefficient between average zapping per hour and the upper zapping threshold was 0.495, reflecting a moderate, statistically significant positive correlation. Moreover, analyzing peak viewing hours according to each group of independent variables revealed several significant results. This suggests that, aside from the correlations mentioned above, correlations also exist among dependent variables.
When the independent variables were divided into groups based on classification criteria, differences in peak viewing hours were observed across groups. Significant differences were found in the MMSE-K group analysis at 3, 4, and 5 AM. Similarly, in the KGDS group analysis, significant differences were observed at 8 AM. Meanwhile, significant differences were noted in the KMBI group analysis at midnight, 1 AM, and 2 AM. Specifically, in the MMSE-K score-based classification, the severe cognitive impairment group showed significantly lower TV viewing rates during the early morning hours than other groups. Although not statistically significant, this group exhibited higher TV viewing rates during daytime hours, from 1 PM to 3 PM. The study by Hua et al. (2021) found that lower cognitive function is associated with very short or very long sleep durations, possibly explaining the TV viewing patterns in the severe cognitive impairment group [36].
Additionally, in the KGDS score-based classification, the no-depression group had a higher TV viewing rate between 8 AM and 9 AM than the other groups. According to the study by Xu et al. (2022), sleep disorders, including early morning awakening, difficulty falling asleep, difficulty maintaining sleep, and non-restorative sleep, are related to depressive disorders. This finding supports the notion that the no-depression group exhibited a more normal daily pattern than the others [37]. Since only the two groups with higher KGDS scores showed significant differences, identifying clear discussion points was challenging. However, a graphical representation indicated that all groups except the normal group tended to keep the TV on continuously. These statistical results demonstrate that TV viewing patterns can predict the user's health status, suggesting the potential for identifying significant correlations in future research after addressing the current study's limitations.
Despite its novel findings, this study has several limitations. Firstly, it considered the time the TV was used rather than the actual viewing time. That is, only data on the TV's ON and OFF status were collected, which did not account for situations where the viewer was engaged in other activities while watching TV or anomalies occurred. Secondly, the sample size was insufficient to identify relationships between TV viewing time, peak viewing periods, and overall cognitive abilities.
5. Conclusions
This study aimed to collect data on detailed variables related to TV viewing and analyze their correlations with cognitive function, depression levels, and ADL performance levels, which are early diagnostic factors for geriatric diseases. The statistically significant results were as follows: a low positive correlation was found between KGDS and daily average viewing time and the upper zapping threshold, while a low negative correlation was found between KMBI and daily average viewing time and the upper zapping threshold. Additionally, when the independent variables were divided into groups based on classification criteria, differences in peak viewing hours were observed across the groups. These findings suggest that developing an early diagnosis system for geriatric diseases using TV viewing patterns could be beneficial. This is expected to be particularly effective for older individuals living alone with limited healthcare access. Further research is needed to investigate the significance of zapping data, peak viewing hours, and health variables.
Author Contributions
Conceptualization, Y.-G.N.; formal analysis, Y.-G.N. and S.-Y.O.; investigation, Y.-G.N. and S.-Y.O.; writing—original draft preparation, S.-Y.O.; writing—review and editing, S.-Y.O.; supervision, Y.-G.N.; authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted according to the Declaration of Helsinki and was approved by the Institutional Review Board of Sun Moon University (ID: SM-202401-002-3, Approval date: 18 Apr 2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study and written informed consent has been obtained from the participants to publish this paper.
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to privacy restrictions. Please contact akk1263@naver.com for access.
Acknowledgments
This research was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No.2022R1C1C2007812).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Schumacher, A.E.; Kyu, H.H.; Aali, A.; Abbafati, C.; Abbas, J.; Abbasgholizadeh, R.; Abbasi, M.A.; Abbasian, M.; Abd ElHafeez, S.; Abdelmasseh, M. Global age-sex-specific mortality, life expectancy, and population estimates in 204 countries and territories and 811 subnational locations, 1950–2021, and the impact of the COVID-19 pandemic: A comprehensive demographic analysis for the Global Burden of Disease Study 2021. The Lancet 2024, 403, 1989–2056. [Google Scholar]
- Osareme, J.; Muonde, M.; Maduka, C.P.; Olorunsogo, T.O.; Omotayo, O. Demographic shifts and healthcare: A review of aging populations and systemic challenges. International Journal of Science and Research Archive 2024, 11, 383–395. [Google Scholar]
- Krellman, J.W.; Mercuri, G. Cognitive interventions for neurodegenerative disease. Current Neurology and Neuroscience Reports 2023, 23, 461–468. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Wu, W.; Zhou, J. Advances and challenges of non-invasive brain stimulation in age-related neurodegenerative diseases, volume II. Frontiers in Aging Neuroscience 2023, 15, 1275530. [Google Scholar] [CrossRef] [PubMed]
- Clemmensen, F.K.; Hoffmann, K.; Siersma, V.; Sobol, N.; Beyer, N.; Andersen, B.B.; Vogel, A.; Lolk, A.; Gottrup, H.; Høgh, P. The role of physical and cognitive function in performance of activities of daily living in patients with mild-to-moderate Alzheimer’s disease–A cross-sectional study. BMC Geriatrics 2020, 20, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Baghdadi, N.A.; Farghaly Abdelaliem, S.M.; Malki, A.; Gad, I.; Ewis, A.; Atlam, E. Advanced machine learning techniques for cardiovascular disease early detection and diagnosis. Journal of Big Data 2023, 10, 144. [Google Scholar] [CrossRef]
- Wilson, A.D. Developments of recent applications for early diagnosis of diseases using electronic-nose and other VOC-detection devices. Sensors 2023, 23, 7885. [Google Scholar] [CrossRef] [PubMed]
- Gong, N.; Meng, Y.; Hu, Q.; Du, Q.; Wu, X.; Zou, W.; Zhu, M.; Chen, J.; Luo, L.; Cheng, Y. Obstacles to access to community care in urban senior-only households: A qualitative study. BMC Geriatrics 2022, 22, 122. [Google Scholar] [CrossRef]
- Fingerman, K.L.; Kim, Y.K.; Ng, Y.T.; Zhang, S.; Huo, M.; Birditt, K.S. Television viewing, physical activity, and loneliness in late life. Gerontologist 2022, 62, 1006–1017. [Google Scholar] [CrossRef]
- Takeuchi, H.; Kawashima, R. Effects of television viewing on brain structures and risk of dementia in the elderly: Longitudinal analyses. Frontiers in Neuroscience 2023, 17, 984919. [Google Scholar] [CrossRef]
- García-Esquinas, E.; Andrade, E.; Martínez-Gómez, D.; Caballero, F.F.; López-García, E.; Rodríguez-Artalejo, F. Television viewing time as a risk factor for frailty and functional limitations in older adults: Results from 2 European prospective cohorts. International Journal of Behavioral Nutrition and Physical Activity 2017, 14, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Billis, A.S.; Batziakas, A.; Bratsas, C.; Tsatali, M.S.; Karagianni, M.; Bamidis, P.D. Enabling active and healthy ageing decision support systems with the smart collection of TV usage patterns. Healthcare Technology Letters 2016, 3, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Abreu, J.; Oliveira, R.; Garcia-Crespo, A.; Rodriguez-Goncalves, R. TV interaction as a non-invasive sensor for monitoring elderly well-being at home. Sensors 2021, 21, 6897. [Google Scholar] [CrossRef] [PubMed]
- Kyan, H.; Inoue, J. Agent-based modeling of zapping behavior of viewers, television commercial allocation, and advertisement markets. In Econophysics of Agent-Based Models; Springer: 2014; pp. 3–26.
- Shin, J.H. Diagnosis of dementia: Neuropsychological test. Korean Journal of Family Medicine 2010, 31, 253–266. [Google Scholar] [CrossRef]
- Kwon, Y.C. Korean version of Mini-Mental State Examination (MMSE-K) Part I: Development of the test for the elderly. Journal of the Korean Neuro-psychiatric Association 1989, 28, 125. [Google Scholar]
- Kim, D.; Kang, Y.; Yun, J.; Lee, K.; Han, K.; Chung, H. A correlation between the Mini Mental State Examination-Korean Version and the Neuro-behavioral Cognitive Status Examination in stroke patients. PNF and Movement 2012, 10, 45–52. [Google Scholar]
- Jamison, C.; Scogin, F. Development of an interview-based geriatric depression rating scale. The International Journal of Aging and Human Development 1992, 35, 193–204. [Google Scholar] [CrossRef] [PubMed]
- Albiński, R.; Kleszczewska-Albińska, A.; Bedyńska, S. Geriatric Depression Scale (GDS). Validity and reliability of different versions of the scale--Review. Psychiatr. Pol. 2011, 45, 555–562. [Google Scholar] [PubMed]
- Montorio, I.; Izal, M. The Geriatric Depression Scale: A review of its development and utility. International Psychogeriatrics 1996, 8, 103–112. [Google Scholar] [CrossRef]
- Leung, S.O.; Chan, C.C.; Shah, S. Development of a Chinese version of the Modified Barthel Index—Validity and reliability. Clin. Rehabil. 2007, 21, 912–922. [Google Scholar] [CrossRef]
- Choi, Y.; Kim, W.; Park, E.; Kim, E. The validity, reliability and discriminative index of the Korean version of Modified Barthel Index (K-MBI) in stroke patients. Journal of the Korea Academia-Industrial cooperation Society 2012, 13, 4119–4125. [Google Scholar] [CrossRef]
- Rovai, A.P.; Baker, J.D.; Ponton, M.K. Social Science Research Design and Statistics: A Practitioner's Guide to Research Methods and IBM SPSS; Watertree Press LLC: 2013.
- Maranhao Neto, G.A.; Pavlovska, I.; Polcrova, A.; Mechanick, J.I.; Infante-Garcia, M.M.; Medina-Inojosa, J.; Nieto-Martinez, R.; Lopez-Jimenez, F.; Gonzalez-Rivas, J.P. The combined effects of television viewing and physical activity on cardiometabolic risk factors: The Kardiovize Study. Journal of Clinical Medicine 2022, 11, 545. [Google Scholar] [CrossRef]
- McAnally, H.M.; Young, T.; Hancox, R.J. Childhood and adolescent television viewing and internalising disorders in adulthood. Preventive Medicine Reports 2019, 15, 100890. [Google Scholar] [CrossRef] [PubMed]
- Spinsante, S.; Gambi, E. Remote health monitoring for elderly through interactive television. Biomedical Engineering Online 2012, 11, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.C.; Rehg, J.M. Watching the TV watchers. Proceedings of the ACM on Interactive, Mobile, Wearable and Ubiquitous Technologies 2018, 2, 1–27.
- Santos, J.; Ihle, A.; Peralta, M.; Domingos, C.; Gouveia, É.R.; Ferrari, G.; Werneck, A.; Rodrigues, F.; Marques, A. Associations of physical activity and television viewing with depressive symptoms of the European adults. Frontiers in Public Health 2022, 9, 799870. [Google Scholar] [CrossRef] [PubMed]
- Tolba, A.A.; Zoghaib, S.Z. Understanding the binge-watching phenomenon on Netflix and its association with depression and loneliness in Egyptian adults. Media Watch 2022, 13, 264–279. [Google Scholar] [CrossRef]
- Yu, B.; Gu, Y.; Bao, X.; Meng, G.; Wu, H.; Zhang, Q.; Liu, L.; Sun, S.; Wang, X.; Zhou, M. Distinct associations of computer/mobile devices use and TV watching with depressive symptoms in adults: A large population study in China. Depress. Anxiety 2019, 36, 879–886. [Google Scholar] [CrossRef] [PubMed]
- Fingerman, K.L.; Ng, Y.T.; Huo, M.; Birditt, K.S.; Charles, S.T.; Zarit, S. Functional limitations, social integration, and daily activities in late life. The Journals of Gerontology: Series B 2021, 76, 1937–1947. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Park, J.; Hsueh, M.; Sun, W.; Liao, Y. Prevalence of total physical activity, muscle-strengthening activities, and excessive TV viewing among older adults; and their association with sociodemographic factors. International Journal of Environmental Research and Public Health 2018, 15, 2499. [Google Scholar] [CrossRef] [PubMed]
- Shree, M.K.R. An examination on causes for anxiety and depression among elderly people. The Journal of Contemporary Issues in Business and Government 2020, 26, 823–828. [Google Scholar]
- Kim, S.; Jeon, S.; Lee, M.Y.; Shin, D.; Lim, W.; Shin, Y.; Oh, K. The association between physical activity and anxiety symptoms for general adult populations: An analysis of the dose-response relationship. Psychiatry Investigation 2020, 17, 29. [Google Scholar] [CrossRef] [PubMed]
- Khodabakhshi-Koolaee, A.; Frouzan, F. Loneliness and death anxiety: Differences between active and bedridden older men. OMEGA-Journal of Death and Dying 2023, 00302228231153460. [Google Scholar] [CrossRef] [PubMed]
- Hua, J.; Zhuang, S.; Shen, Y.; Tang, X.; Sun, H.; Fang, Q. Exploring the bidirectional associations between short or long sleep duration and lower cognitive function: A 7-year cohort study in China. Frontiers in Aging Neuroscience 2021, 13, 727763. [Google Scholar] [CrossRef] [PubMed]
- Xu, G.; Yu, Y.; Tang, C.; Liu, Z.; Li, X.; Tan, Y.; Mai, X.; Li, R.; Xu, C.; Xie, G. Effect of early morning awakening in major depressive disorder. 2022.
Figure 1.
Flowchart of the experimental procedure.
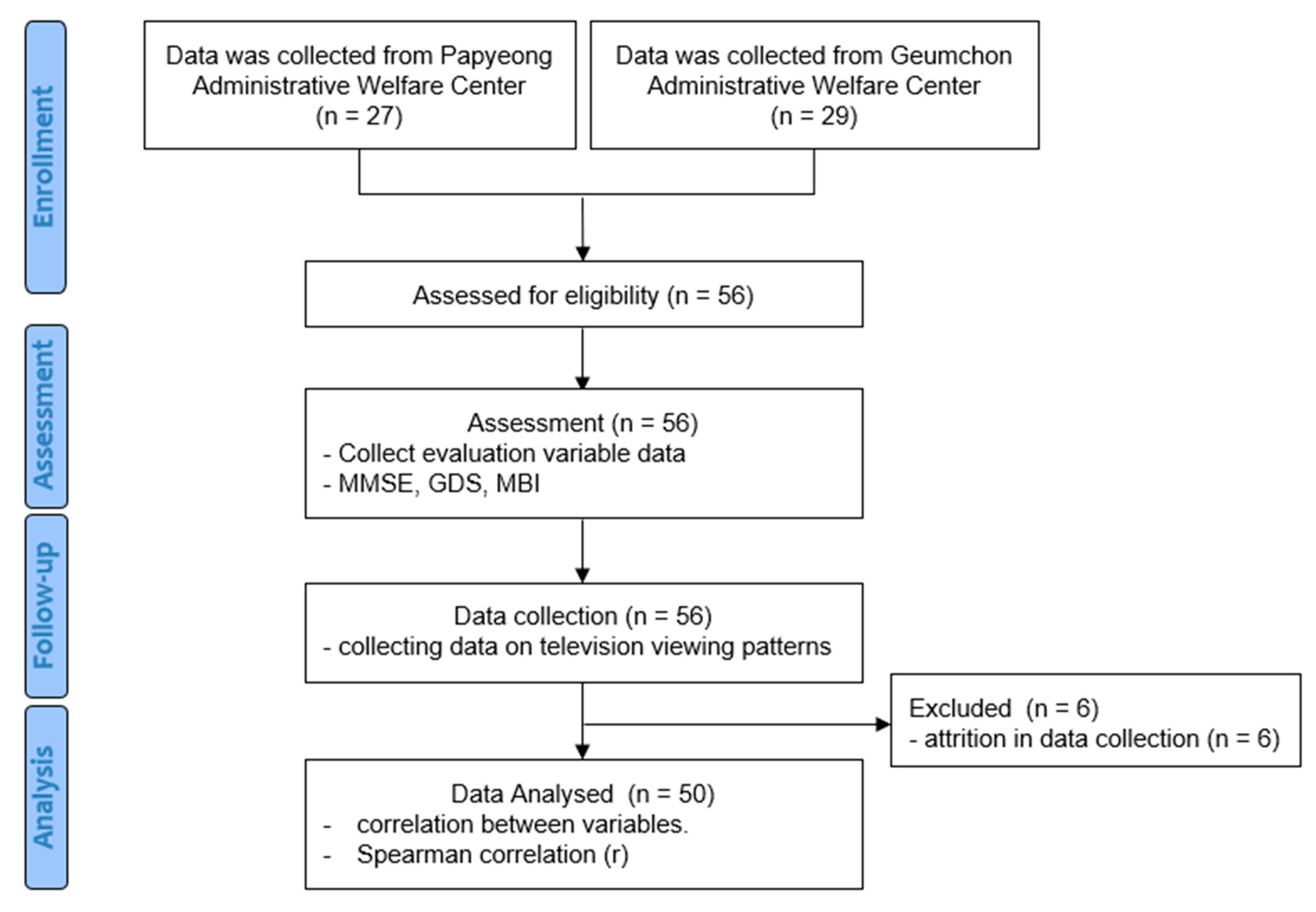

Table 1.
Participants’ general characteristics.
| Participants (n=50) | |
|---|---|
| Age (years) | 82.12 ± 4.32 |
| Height (cm) | 156.94 ± 6.59 |
| Weight (kg) | 56.76 ± 9.99 |
| MMSE-K (score: 0–30) | 23.72 ± 4.24 |
| KGDS (score: 0–30) | 12.60 ± 6.94 |
| KMBI (score: 0–100) | 90.02 ± 21.28 |
| Daily average viewing time (min) | 639.83 ± 297.21 |
| Upper zapping threshold (number of days) | 34.82 ± 27.79 |
| Lower zapping threshold (number of days) | 0.62 ± 1.39 |
| Average zapping per hour | 3.09 ± 1.65 |
Values are mean ± SD. MMSE-K, Korean version of the Mini-Mental State Examination; KGDS, Korean form of the Geriatric Depression Scale; KMBI, Korean version of the Modified Barthel Index.
Table 2.
Correlations between TV viewing data and cognitive function, depression, and ADL performance.
Table 2.
Correlations between TV viewing data and cognitive function, depression, and ADL performance.
| AGE | DAV | PVH | UZT | LZT | AZH | MMSE-K | KGDS | KMBI | |
|---|---|---|---|---|---|---|---|---|---|
| AGE | 1.000 | 0.102 | 0.070 | -0.001 | -0.063 | -0.192 | -0.208 | 0.012* | -0.245 |
| DAV | 0.102 | 1.000 | 0.161 | 0.812** | 0.150 | 0.495** | 0.264 | 0.320* | -0.313* |
| PVH | 0.070 | 0.161 | 1.000 | 0.091 | 0.129 | 0.230 | -0.216 | 0.088 | -0.022 |
| UZT | -0.001 | 0.812** | 0.091 | 1.000 | 0.046 | 0.590** | 0.145 | 0.308* | -0.352* |
| LZT | -0.063 | 0.150 | 0.129 | 0.046 | 1.000 | 0.324 | 0.033 | 0.098 | -0.127 |
| AZH | -0.192 | 0.495** | 0.230 | 0.590** | 0.324 | 1.000 | 0.087 | 0.218 | 0.088 |
| MMSE-K | -0.208 | 0.264 | -0.216 | 0.145 | 0.033 | 0.087 | 1.000 | -0.249 | -0.091 |
| KGDS | 0.012 | 0.320* | 0.088 | 0.308* | 0.098 | 0.218 | -0.249 | 1.000 | -0.153 |
| KMBI | -0.245 | -0.313* | -0.022 | -0.352* | -0.127 | 0.088 | -0.091 | -0.153 | 1.000 |
*p<.05, **p<.01. DAV, daily average viewing time (min); PVH, peak viewing hours; UZT. upper zapping threshold (number of days); LZT, lower zapping threshold (number of days); AZH, average zapping per hour.
Table 3.
Analysis of peak viewing hours by MMSE-K score groups.
| Hour of Day |
Mean ± SD | p | ||
| Severe (n=6) |
Moderate (n=19) |
None (n=25) |
||
| 0 | 2.83 ± 2.48 | 2.84 ± 1.95 | 2.92 ± 1.93 | 0.873 |
| 1 | 1.00 ± 1.55 | 2.26 ± 1.66 | 3.28 ± 2.36 | 0.226 |
| 2 | 0.50 ± 1.22 | 1.79 ± 1.44 | 1.92 ± 1.73 | 0.105 |
| 3 | 0.33 ± 0.82 | 1.51 ± 1.82 | 1.88 ± 1.83 | 0.048* |
| 4 | 0.33 ± 0.52 | 1.89 ± 1.76 | 2.00 ± 1.66 | 0.041* |
| 5 | 1.00 ± 2.00 | 2.63 ± 2.54 | 2.88 ± 1.64 | 0.049* |
| 6 | 2.17 ± 2.64 | 3.84 ± 2.67 | 3.37 ± 2.47 | 0.307 |
| 7 | 3.17 ± 2.79 | 4.84 ± 2.12 | 5.24 ± 1.29 | 0.152 |
| 8 | 5.17 ± 2.32 | 5.05 ± 2.59 | 5.48 ± 1.20 | 0.501 |
| 9 | 6.17 ± 2.64 | 6.05 ± 2.14 | 5.36 ± 1.25 | 0.786 |
| 10 | 5.83 ± 3.61 | 4.31 ± 2.06 | 4.08 ± 1.22 | 0.190 |
| 11 | 6.33 ± 4.36 | 4.60 ± 2.13 | 4.92 ± 1.15 | 0.268 |
| 12 | 6.50 ± 4.25 | 3.79 ± 2.27 | 3.84 ± 1.39 | 0.593 |
| 13 | 4.00 ± 2.45 | 3.58 ± 2.10 | 3.92 ± 1.33 | 0.291 |
| 14 | 5.33 ± 3.22 | 5.05 ± 2.47 | 4.08 ± 1.22 | 0.165 |
| 15 | 5.83 ± 3.61 | 5.89 ± 2.94 | 5.84 ± 1.20 | 0.645 |
| 16 | 4.00 ± 2.35 | 5.36 ± 2.74 | 5.92 ± 1.08 | 0.326 |
| 17 | 2.33 ± 2.74 | 4.37 ± 2.51 | 4.76 ± 1.23 | 0.623 |
| 18 | 3.50 ± 2.34 | 5.05 ± 2.04 | 5.44 ± 1.66 | 0.715 |
| 19 | 2.67 ± 3.25 | 4.37 ± 2.40 | 4.37 ± 1.74 | 0.657 |
| 20 | 4.00 ± 2.47 | 4.05 ± 2.19 | 3.76 ± 1.98 | 0.774 |
| 21 | 2.33 ± 2.94 | 4.77 ± 2.54 | 4.36 ± 1.35 | 0.540 |
| 22 | 3.67 ± 3.20 | 4.37 ± 2.44 | 4.72 ± 1.83 | 0.614 |
| 23 | 4.00 ± 2.37 | 3.74 ± 2.94 | 3.64 ± 1.99 | 0.913 |
*p<.05.
Table 4.
Analysis of peak viewing hours by KGDS score groups.
| Hour of Day |
Mean ± SD | p | |||
| None (n=28) |
Mild (n=14) |
Moderate (n=2) |
Severe (n=6) |
||
| 0 | 2.71 ± 2.24 | 2.93 ± 1.54 | 3.00 ± 1.41 | 3.50 ± 1.87 | 0.921 |
| 1 | 1.93 ± 1.90 | 2.29 ± 1.54 | 1.50 ± 0.71 | 3.17 ± 1.72 | 0.710 |
| 2 | 1.57 ± 1.64 | 1.64 ± 1.34 | 3.00 ± 1.41 | 2.67 ± 1.86 | 0.618 |
| 3 | 1.39 ± 1.62 | 1.57 ± 1.34 | 0.50 ± 0.71 | 2.67 ± 1.75 | 0.322 |
| 4 | 1.61 ± 1.75 | 1.79 ± 1.58 | 1.00 ± 0.00 | 3.67 ± 1.75 | 0.544 |
| 5 | 2.50 ± 2.25 | 2.64 ± 1.54 | 3.00 ± 2.83 | 2.83 ± 1.72 | 0.814 |
| 6 | 3.82 ± 2.89 | 3.14 ± 2.35 | 3.50 ± 2.12 | 3.17 ± 1.72 | 0.936 |
| 7 | 5.46 ± 2.25 | 4.14 ± 1.79 | 3.50 ± 2.12 | 4.00 ± 0.83 | 0.068 |
| 8 | 6.57 ± 3.89 | 5.21 ± 2.35 | 5.00 ± 0.00 | 5.00 ± 1.10 | 0.017* |
| 9 | 5.07 ± 2.89 | 5.07 ± 2.35 | 5.00 ± 0.00 | 3.33 ± 0.52 | 0.279 |
| 10 | 3.36 ± 2.15 | 4.21 ± 2.02 | 4.00 ± 1.41 | 4.67 ± 1.37 | 0.672 |
| 11 | 3.93 ± 2.15 | 4.14 ± 2.02 | 4.00 ± 1.41 | 3.67 ± 1.21 | 0.395 |
| 12 | 5.93 ± 4.15 | 5.21 ± 1.64 | 4.00 ± 0.00 | 5.50 ± 2.23 | 0.524 |
| 13 | 5.07 ± 2.45 | 5.50 ± 1.51 | 6.00 ± 1.41 | 5.67 ± 1.86 | 0.572 |
| 14 | 5.93 ± 4.29 | 4.21 ± 1.64 | 5.00 ± 2.12 | 5.50 ± 1.87 | 0.175 |
| 15 | 5.57 ± 2.49 | 4.64 ± 2.35 | 5.00 ± 1.41 | 5.33 ± 2.04 | 0.299 |
| 16 | 5.96 ± 2.40 | 5.07 ± 1.79 | 6.00 ± 1.41 | 5.67 ± 2.68 | 0.800 |
| 17 | 5.93 ± 2.45 | 4.71 ± 1.64 | 5.00 ± 2.12 | 5.33 ± 1.37 | 0.977 |
| 18 | 5.93 ± 2.89 | 4.57 ± 1.79 | 5.50 ± 2.12 | 4.83 ± 1.87 | 0.796 |
| 19 | 3.57 ± 2.89 | 4.71 ± 1.64 | 5.00 ± 2.12 | 3.83 ± 2.04 | 0.576 |
| 20 | 5.00 ± 2.25 | 5.07 ± 1.52 | 5.00 ± 1.41 | 3.83 ± 1.99 | 0.143 |
| 21 | 4.93 ± 2.40 | 4.50 ± 1.51 | 4.00 ± 1.41 | 3.67 ± 1.94 | 0.254 |
| 22 | 3.36 ± 1.52 | 4.71 ± 1.76 | 4.67 ± 2.87 | 3.83 ± 2.23 | 0.439 |
| 23 | 3.57 ± 2.45 | 4.00 ± 1.52 | 4.50 ± 1.87 | 3.64 ± 1.99 | 0.840 |
*p<.05.
Table 5.
Analysis of peak viewing hours by KMBI score groups.
| Hour of Day |
Mean ± SD | p | ||
| Grade 1 (n=3) |
Grade 6 (n=10) |
Normal (n=35) |
||
| 0 | 3.67 ± 1.53 | 4.20 ± 1.32 | 2.60 ± 1.96 | 0.036* |
| 1 | 2.67 ± 2.08 | 3.50 ± 1.18 | 1.86 ± 1.72 | 0.022* |
| 2 | 1.67 ± 2.08 | 2.80 ± 1.48 | 1.49 ± 1.52 | 0.029* |
| 3 | 1.67 ± 2.08 | 2.50 ± 1.51 | 1.37 ± 1.50 | 0.071 |
| 4 | 2.33 ± 2.52 | 2.80 ± 1.71 | 1.54 ± 1.58 | 0.118 |
| 5 | 3.67 ± 2.52 | 2.90 ± 1.66 | 2.31 ± 2.22 | 0.247 |
| 6 | 4.33 ± 2.08 | 3.60 ± 1.84 | 3.31 ± 2.00 | 0.614 |
| 7 | 5.33 ± 0.58 | 4.10 ± 1.66 | 4.89 ± 2.23 | 0.398 |
| 8 | 4.33 ± 1.15 | 5.00 ± 1.49 | 6.34 ± 3.52 | 0.083 |
| 9 | 4.33 ± 1.15 | 4.50 ± 1.49 | 5.14 ± 2.58 | 0.094 |
| 10 | 4.33 ± 2.08 | 4.50 ± 1.72 | 5.14 ± 2.58 | 0.332 |
| 11 | 4.33 ± 2.08 | 4.00 ± 1.97 | 4.23 ± 2.04 | 0.704 |
| 12 | 4.33 ± 2.08 | 3.70 ± 1.42 | 4.89 ± 4.17 | 0.608 |
| 13 | 4.67 ± 1.53 | 3.80 ± 1.14 | 4.40 ± 2.37 | 0.319 |
| 14 | 4.00 ± 2.65 | 3.20 ± 1.14 | 4.03 ± 2.27 | 0.416 |
| 15 | 3.33 ± 2.89 | 3.20 ± 1.23 | 4.20 ± 2.63 | 0.291 |
| 16 | 3.67 ± 2.31 | 4.00 ± 0.82 | 4.49 ± 1.95 | 0.058 |
| 17 | 4.67 ± 1.53 | 3.00 ± 0.85 | 5.29 ± 1.78 | 0.017 |
| 18 | 5.67 ± 0.58 | 5.50 ± 0.95 | 5.94 ± 2.46 | 0.214 |
| 19 | 5.67 ± 0.58 | 5.00 ± 1.25 | 5.86 ± 2.88 | 0.681 |
| 20 | 5.33 ± 0.58 | 4.20 ± 1.63 | 5.71 ± 2.30 | 0.985 |
| 21 | 5.67 ± 0.58 | 5.00 ± 1.10 | 5.31 ± 2.61 | 0.671 |
| 22 | 5.67 ± 0.58 | 5.70 ± 1.63 | 4.34 ± 2.31 | 0.356 |
| 23 | 5.00 ± 1.00 | 5.10 ± 1.10 | 3.49 ± 2.21 | 0.077 |
*p<.05.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



