
Submitted:
07 August 2024
Posted:
08 August 2024
You are already at the latest version
Abstract
This in vitro study aimed to analyze the surface roughness (Ra) and color stability (ΔEab, ΔE00) following simulated mechanical brushing, and to evaluate the microtensile (μTBS) to dentin of Self Adhering Resin Flowable (SARF). The selected materials were Constic, Yflow AS, and Tetric N flow (TNF/control). Thirty composite resin cylinders were fabricated for surface property evaluation. Ra and color were assessed both before and after simulated brushing. The thresholds of 50:50% perceptibility and acceptability of color difference of the evaluated resins were assessed. For μTBS analysis, fifteen molars were selected, sectioned to expose flat dentin surfaces, and restored according to manufacturers' instructions. Subsequently, they were sectioned into sticks for microtensile testing. Statistically significant differences in Ra among the groups, with Constic exhibiting the highest Ra value (p < 0.05), while Yflow AS showed the lowest Ra value. No statistically significant difference in color was observed among the groups (p > 0.05). The 50:50% perceptibility and acceptability thresholds set at 1.2 and 2.7 for ΔEab and 0.8 and 1.8 for ΔE 00. All the results fell within the acceptable limits. The mean μTBS values of Constic, Yflow AS, and TNF were 10.649 MPa, 8.170 MPa, and 33.669 MPa, respectively. The study revealed increased Ra and comparable color stability among all tested composite resins after abrasion. However, SARF exhibited lower μTBS compared to conventional using an adhesive system.
Keywords:
self adhesive flowable composite
; toothbrushing
; microtensile bond strength
; surface properties
1. Introduction
Resin composites have undergone significant advancements since their inception, evolving to meet the demands of modern dentistry by enhancing their physical and optical properties. These materials have become the preferred choice for aesthetic restorations and areas subjected to significant chewing stresses, offering a versatile solution for replacing lost dental tissue resulting from caries and restoring long-term harmony, function, and stability of the dentition [1,2,3]. Despite their widespread use, composite resin restorations are susceptible to various types of failures, including restoration fracture, discoloration, adhesive failure to the tooth, and secondary caries [4,5]. Many of these failures are correlated with the sensitivity of the adhesive technique to moisture [6]. In response to these challenges, self-adhesive flowable resins (SAFRs) have emerged as promising alternatives aimed at simplifying restoration techniques [7].
SAFRs have similar indications to conventional flowable resins (CFRs), such as class I, class III and class V restorations, sealants, and repairs [7,8,9,10]. The self-adhesiveness of this new class of composite resin is conferred by the addition of the glycerol-phosphate molecule, which conditions the dental structure while also having an affinity for dental element calcium and methacrylate groups that copolymerize with other methacrylate monomers [11]. However, it is important to note that tissue demineralization is partial, meaning there is no complete removal of the smear layer, incorporating it into the adhesive interface, unlike the usually applied technique of total acid conditioning, where the smear layer is entirely removed [12]. The success of restorative treatment depends on the interaction between the restorative material and dental tissue, commonly evaluated through bond strength tests [10].
The microtensile μTBS (μTBS) of SAFR remains a subject of investigation, with conflicting findings compared to traditional bonding techniques [13,14,15]. While some studies suggest lower μTBS values for SAFR [14,14, others found that SARFs presented similar μTBS values in enamel and dentin [15]. Hayashi et al. [10] found that the adhesion values of SARFs are higher when prior acid etching is performed. Study highlight the need for further investigation into specific resin formulations, such as Constic resin (SAFR), to assess their clinical viability [16]. Studies evaluating the μTBS of restorative materials are crucial for subsequent clinical research, as stated by Brueckner et al. [13] and Elraggal et al. [17]. In vitro studies reflect the clinical performance of resins, and we can only use them in vivo after promising laboratory results. Additionally, no studies evaluating the μTBS of the Yflow SA (SAFR) were found.
The wear of a dental restoration can be influenced by factors such as occlusal contact, food bolus friction, and tooth brushing [18]. The abrasive challenge generated by tooth brushing can increase the roughness (Ra) of composite resins. Consequently, the literature highlights that simulated abrasion is a well-established model capable of simulating clinical conditions [19]. SARFs demonstrated high luster and a smooth surface after polishing. However, these characteristics were altered after simulated brushing, resulting in surface filler dislodgement [20]. After the abrasive challenge, SARFs exhibited higher surface roughness values compared to the conventional resin used as a control [19]. Increased roughness of restorative materials makes the surface more susceptible to plaque accumulation, staining, and deterioration of the material's aesthetic properties [21]. Color represents an important aspect of the aesthetic success of restorations. A previous study [20] highlighted that simulated brushing influenced the color stability of SARFs.
A previous study suggested further exploration of the physical and mechanical properties of SARFs to gain a deeper understanding of their polymerization process [22]. In vitro studies are crucial for the development of new materials, such as self-adhesive flowable resins (SAFRs), as they can provide essential information for further testing and ensure safety for future clinical trials [23]. The findings of this study can provide scientific evidence on the performance of SARFs, contributing to a better understanding of their characteristics and limitations. Thus, this study aimed to identify the behavior of SAFR in terms of Ra, color stability after simulated brushing, and μTBS to dentin. The null hypotheses are as follows: (a) there is no significant difference in the Ra of the composite resins after simulated brushing, (b) there is no significant difference in the color of the composite resins after simulated brushing, and (c) there is no significant difference in the μTBS between the SAFR and CFR.
2. Materials and Methods
An in vitro study was conducted to assess the Ra, color, and μTBS to dentin of the SAFRs Constic (DMG, Hambug, Germany) and Yflow SA (Yller Biomateriais, Pelotas, RS, Brazil) in comparison with the CFR Tetric N-flow (TNF) (Ivoclar Vivadent, Barueri, SP, Brazil). The study was carried out in two stages; initially, tests for Ra and color analysis were performed before and after simulated brushing. Subsequently, a μTBS test was conducted to evaluate the bonding resistance of the investigated resins to dentin (CAAE: 48791621.1.0000.5188). The entire description of the materials used in this study and the manufacturer’s instructions for use are presented in Table 1.
2.1. Initial Analysis of Surface Roughness and Color
The analyses of Ra and color stability were conducted with a sample size of 10 specimens per group. The number of specimens was determined based on a previous study [20] that evaluated the roughness and color stability of SARF resin compared to conventional flow resin. The study adopted a power of 80% and a significance level of 0.05, finding minimum differences of 0.04 in roughness and 0.96 in color. Although the required number of specimens was 5, a sample size of 10 specimens per group was adopted to achieve greater precision, in accordance with the recommendations outlined in the RoB assessment tool for laboratory studies on dental materials [24]. The samples were divided according to the type of restorative composite resin into three groups, each containing 10 specimens: Group 1A (TNF), Group 2A (Constic), and Group 3A (Yflow SA).
The specimens were prepared using a cylindrical Teflon matrix measuring approximately 2 mm thick and 6 mm in diameter. The matrix was filled with the restorative material in a single increment. After material insertion, a polyester strip was pressed onto the surface using a glass plate to ensure that the surface was flat and free from bubbles. Polymerization was carried out using Emitter C equipment (SCHUSTER, Santa Maria, RS, Brazil), with the light intensity measured above 800 mw/cm2 using an RD-7 radiometer (ECEL, Ribeirão Preto, SP, Brazil). Subsequently, the specimens were subjected to finishing and polishing using the Sof-Lex system (3 M, Oral Care, St. Paul, MN, USA) and felt discs (FGM, Joinville, SC, Brazil), followed by immersion in distilled water for 24 hours.
The initial analysis of Ra of the specimens was performed using a profilometer (Surftest SJ-301, Mitutoyo, Japan). The samples were individually placed on a glass plate with utility wax using a press with a load of 0.5 kgf for 3 seconds. Three random readings per specimen were taken (horizontal, transverse, and vertical), with the specimen rotated during each reading. The readings were taken through the center of the surface of each sample. The recorded Ra value was the average of the readings. Tooth colors were assessed using a spectrophotometer (Easyshade Advance 4.0, VITA Zahnfabrick, Bad Säckingen, Germany) against a black background. Calibration of the device was conducted after every three measurements. The CIELab color coordinates, including L*, a*, and b*, as defined by the International Commission on Illumination (CIE), were recorded. These coordinates are extensively utilized in the dental literature. The L* value signifies the psychometric brightness ranging from black to white (achromatic coordinate), while the a* (green‒red coordinate) and b* (blue‒yellow coordinate) values represent the psychometric chroma coordinates, indicating hue and chroma, respectively [25]. Measurements were conducted thrice for each specimen, and the resulting data were averaged. To enhance correlation with visual perception, the International Standard Organization (ISO) and the International Commission on Illumination (CIE) jointly recommend employing the CIEDE2000 color difference formula for determining total color difference, which is based on the CIELAB color space [26]. Recent studies have further corroborated that the CIEDE 2000 formula better represents color differences perceived by the human eye than does the CIELAB [26] formula. Thus, in this study, color differences were assessed using two parameters: CIEDE 2000 (ΔE 00) and CIELAB (ΔE ab). The CIELAB color difference (ΔE ab) was calculated using the following equation:
The CIEDE2000 color difference (∆E 00) was computed utilizing an Excel spreadsheet implementation of the CIEDE2000 color difference formula developed by Sharma [27]. ΔE00 (CIEDE 2000) was calculated using the following equation:
ΔL', ΔC', and ΔH' represent variations in brightness, color intensity, and hue among the specimens being compared. RT serves as a rotation function for elucidating how chroma and hue differences interact, particularly within the blue spectrum. S L, S C, and SH denote weighting functions, while K L, K C, and K H refer to terms that need adjustment based on experimental conditions [28]. The parametric factors kL, kC, and kH function as correction terms for experimental variations and will all be standardized to 1.0 under reference conditions as determined by the CIE technical report.
The color adaptability was assessed based on the color disparities observed between the teeth and the composite materials, considering thresholds of 50%:50% perceptibility and 50%:50% acceptability. Under these thresholds, the 50%:50% color difference (PT) perceptibility threshold denotes the degree of color variation that can be perceived by 50% of observers in controlled conditions, while the remaining 50% of observers perceive no discernible difference in color between the compared objects. Similarly, the 50%:50% color difference (AT) acceptability threshold signifies the level of color difference deemed acceptable by 50% of observers under controlled conditions, with the remaining 50% of observers opting to either replace or correct the restoration [28]. The ΔEab - CIELAB values were assessed based on 50%:50% perceptibility and 50%:50% acceptability criteria, with thresholds set at 1.2 and 2.7 according to the specifications outlined in ISO/TR 28642:2016. Additionally, the ΔE 00-CIEDE 2000 values were examined using the same perceptibility and acceptability standards, with corresponding thresholds established at 0.8 and 1.8, respectively, as indicated by prior research [28].
2.2. Simulated Toothbrushing
Simulated toothbrushing was conducted using a specific device (Biopdi, São Carlos, SP, Brazil) capable of performing back-and-forth movements across ten articulated arms via pulleys with dental brushes attached. Each complete movement was considered one cycle. The toothpaste Colgate Cavity protection (Colgate-Palmolive Company, New York, USA) was applied as a suspension and diluted in distilled water at a ratio of 2:1 using a mechanical agitator. The specimens underwent 20,000 cycles of brushing. The product was paired with Oral-B Indicator 40 Soft toothbrushes (Gillette do Brasil Ltda., São Paulo, SP, Brazil), featuring nylon bristles with the handles cut at the midpoint to fit into the machine. Following the brushing cycles, the specimens were removed from the machine and rinsed under running water. Given that individuals brush their teeth three times a day, a total of 5,465 brushing cycles occur over a year. Therefore, the chosen brushing period in this study is equivalent to approximately 3 years and 6 months in vivo [28].
2.3. Analysis of Roughness and Color after Simulated Brushing
The Ra and color measurements were conducted following the same criteria as those used for the initial assessment. The mean Ra values were recorded, and color differences between the coordinates were calculated using a specific formula.
2.4. Microtensile Test
For the μTBS evaluation, 15 human molars extracted upon the recommendation of a dentist were obtained following the guidelines of Resolution 466/12 of the National Health Council/MS after approval from the Research Ethics Committee - CCS/UFPB. The molars were divided into 3 groups according to the restorative material used, namely, Group 1B (TNF), Group 2B (Constic), and Group 3B (Yflow SA). The selected teeth were cleaned and embedded in acrylic resin cylinders to facilitate handling during preparation. The occlusal enamel was removed using a diamond disc (Extec, Enfield, CT, USA) mounted on a precision cutter (Labcut 1010, Extec Corp., Enfield, CT, USA) under water cooling to expose the dentin surface, resulting in a flat dentin surface. Subsequently, the specimens were ground with 600-grit silicon carbide paper (Saint-Gobain Abrasivos, Guarulhos, SP, Brazil) on a water-cooled polisher (ERIOS Polisher - 27000, ERIOS, São Paulo, SP, Brazil) for 60 seconds to provide a homogeneous layer of dentin slurry [30].
The adhesive system Adper Single Bond Plus (3 M ESPE) was applied following the manufacturer's recommended technique, only with TNF resin. A metal matrix band was placed, and each specimen received two increments, each 2.0 mm thick, of resin. Photoactivation was performed using an Optlux Plus light-curing unit (GNATUS) with a light intensity of 800 mW/cm2, as determined by a Demetron radiometer (Model 100, Demetron, USA), resulting in the formation of a block approximately 4.0 mm in height. The technique used adhered to the manufacturer's instructions (Table 1).
With a diamond disc (Extec, Enfield, CT, USA) mounted on a precision cutter (Labcut 1010, Extec, Enfield, CT, USA) under water cooling, the samples were longitudinally cut in the mesio-distal and vestibulo-lingual directions to obtain prism-shaped specimens measuring approximately 1 mm wide, 1 mm deep, and 10 mm high. These specimens consisted of two arms, one composed of the restorative material and the other composed of the dentin substrate, bonded together by an adhesive interface [30]. Seven sticks were obtained from each tooth, totaling 35 in the group where TNF resin was used. The sample size calculation was based on a previous study [31], adopting a power of 80% and a significance level of 0.05, resulting in 35 specimens, which was able to detect a difference of up to 5.3. The groups in which self-adhesive resins were used encountered problems in obtaining the required number of sticks, which will be discussed further.
Using a cyanoacrylate-based adhesive (Super Bond Gel – Loctite Brasil Ltd.) and an accelerator substance, the ends of each sample were fixed to the grips of the microtensile testing device, leaving the bond interface free. Subsequently, the grips attached to the specimen were positioned in a testing machine using a 500 N load cell, which was activated at a speed of 15 mm/min until reaching 10 N and then continued at a speed of 5 mm/min. The μTBS data, expressed in megapascals (MPa), were recorded by dividing the applied force at the time of rupture (peak load) by the bond area (mm²). Specimens that broke during transportation, handling, and/or assembly were excluded from the study.
After the test, the fractured specimens were examined under an optical microscope (HMV-2, Shimadzu, Kyoto, Japan) at a magnification of 200× by the same evaluator, and the fracture modes were classified as follows: A: Adhesive failure, which is a fracture within the adhesive layer. C: Cohesive failure, either within the resin composite or dentin. M: Mixed failure, where the fracture involves more than one material. P: Pretest failure, indicating that the fracture occurred before testing the specimen. G: Failure outside the testing area, where the specimen was attached to the device [32].
2.5. Data Analysis
The data were analyzed for normality using the Shapiro‒Wilk test. Since a normal distribution was not found in all groups, the nonparametric Kruskal‒Wallis test and Wilcoxon signed-rank test were used. A significance level of 5% (p < 0.05) was adopted for the analysis, and STATA version 14 was utilized. The μTBS data were analyzed using a descriptive approach.
3. Results
After the application of statistical tests, it was found that there were no statistically significant differences between the groups regarding initial Ra, as they maintained results between 0.1 and 0.13 µm. However, statistically significant differences were observed in relation to the final results, indicating that the Constic resin presented the highest superficial Ra. Differences were also observed in the analysis between the initial and final results (intragroup) for all tested resins (Table 2), showing an increase in Ra in all groups.
The color parameters of the groups are shown in Table 3 and Table 4. In the comparison according to the CIELAB formula (p=0.080) and CIEDE200 (p=0.144), there was no statistically significant difference (p>0.05) between the groups (G1A, G2A and G3A). The color variation values were analyzed based on 50%:50% perceptibility and 50%:50% acceptability criteria, with thresholds set at 1.2 and 2.7 for ΔEab and 0.8 and 1.8 for ΔE 00. All the results fell within the acceptable limits, as shown in Figure 1 and Figure 2.
Significant difficulty was observed in obtaining the required number of sticks for the microtensile test in the groups where the SARF restorations were performed. During the cutting process of the restored dental element, these materials exhibited fragility, resulting in detachment of the dentin in the first longitudinal cut or during the formation of the stick in the second cut. As a result, only 8 sticks were obtained in the Yflow SA resin group, and 11 sticks were obtained in the Constic resin group. This fragility indicates early failure in the restorations prior to the microtensile test. In contrast, obtaining the necessary sample size of sticks for the CFR was much easier, with no fractures occurring during cutting, resulting in a sample size of 50 sticks.
This fact complicated a statistical analysis of these data, which were then discussed through a descriptive comparison of the mean μTBS values. The analysis revealed that TNF had the highest mean μTBS (33.669 ± 6.453 MPa), followed by Constic (10.649 ± 4.406 MPa) and Yflow SA (8.170 ± 3.781 MPa) (Figure 3). The TNF group has a larger sample size (n = 35), which increases the reliability and precision of the mean estimates. This suggests that the mean μTBS of this group is more representative among the materials studied. The fracture patterns are shown in Figure 4.
4. Discussion
This in vitro study evaluated behavior of SARF in terms of Ra, color stability after simulated brushing, and μTBS to dentin. the Surface topography and color stability are critical factors for the clinical success of restorative dental treatments. An ideal restoration should have a smooth surface to prevent biofilm adhesion and maintain color stability over time [20,33]. Brushing is a common practice that significantly impacts the surface properties of restorative materials, affecting both their appearance and Ra [20].
The initial hypothesis that there would be no significant difference in Ra among the tested resin materials after simulated brushing was refuted. Specifically, the Constic resin demonstrated a notably greater Ra following the abrasive challenge, showing a significant increase in Ra (0.7 µm) compared to both the TNF (0.31 µm) and Yflow SA (0.18 µm) resins. This observed discrepancy can be attributed to variations in the composition of the organic matrix and the relatively low filler content present in the materials [19,34]. Past research has underscored the impact of organic matrix composition on material properties, particularly in relation to abrasion resistance. It has been noted that higher levels of Bis-GMA may contribute to a reduction in abrasion resistance, while increased amounts of UDMA and TEGDMA could enhance resistance to abrasion [19]. This suggests that differences in the resin composition among the tested materials likely played a pivotal role in the observed variations in Ra following simulated brushing.
This finding is supported by the data obtained by Lai et al. [20], who observed a significant increase in Ra values in the SAFR group (Vertise Flow) compared to two nanohybrid resins (GrandioSO Flow and G-aenial Universal Flow) after simulated brushing, with Ra values of 0.21 µm, 0.17 µm, and 0.11 µm, respectively. Similar results were reported by Malavasi et al. [20], who compared self-adhesive flowable resins (vertise flow and fusio liquid dentin) with a nanoparticulate resin (Filtek 350) after 20,000 cycles of simulated brushing. A greater increase in Ra was observed in the SAFR group, with values of 0.24 µm, 0.15 µm, and 0.13 µm, respectively. Notably, Costa et al. [35] emphasized in their study that Ra exceeding 0.2 µm could heighten susceptibility to biofilm accumulation and bacterial adhesion, potentially leading to the development of secondary caries and periodontal inflammation. However, they observed that Ra alterations ranging between 0.22 and 0.24 µm are considered clinically acceptable [35]. In this context, the Ra values of the Yflow SA self-adhesive resins were the only ones that met clinically acceptable standards.
The second null hypothesis, which posited no differences in color among the studied composite resins after simulated brushing, was accepted when applying the CIELAB (ΔE ab) and CIEDE2000 (ΔE 00) tools. These findings align with those of Malavasi et al. [19], where self-adhesive flowable resins (SAFRs) (vertise flow and fusio liquid dentin) showed no statistically significant changes compared to a nanoparticulate resin (Filtek 350) in terms of color variation. Similarly, the study by Sanal and Kilinc [36] comparing SAFR (Constic, Vertise Flow, and Fusio Liquid Dentin) with conventional resin (Filtek Supreme XTE) in ceramic repairs corroborates these results. It is important to note that in laboratory studies, intrinsic patient factors such as diet are not considered. The minor observed alterations, although statistically nonsignificant, may be attributed to the optical properties resulting from internal reactions of the restorative material [19] and simulated brushing.
The literature contains studies in which self-adhesive flowable resin (fusion liquid dentin) has been shown to demonstrate better color stability clinically for more than one year than conventional resin (TNF). In the TNF group, slight color mismatch, hue, or translucency was noted in 5 out of 30 restorations, albeit within the normal range of adjacent tooth structure [9]. Arregui et al. [37], on the other hand, examined two SARFs (vertise flow and experimental SAFRs) and one nanohybrid resin (premise flow) and noted statistically significant differences in color variation (ΔE) between the experimental SAFR group (12.25) and the Vertise Flow (6.57) and Premise Flow (3.47) groups. These variations could be attributed to the different methodologies employed, including immersion in high-temperature water for 30 days.
In this study, we assessed the total color difference (ΔE) using both the CIEDE 2000 (ΔE00) and CIELAB (ΔEab) formulas, considering acceptability (AT) and perceptibility (PT) (Figure 1 and Figure 2). A ΔEab value below 1.2 indicated that 50% of the observers could detect differences, while the other 50% could not [27]. For acceptability, a shade difference under 2.7 was deemed clinically acceptable [27]. The CIEDE 2000 formula thresholds for perceptibility and acceptability were set at 0.8 and 1.8, respectively [27]. Several studies have reported better agreement between the CIEDE2000 formula and visual findings (95% agreement) than between the CIEDE2000 formula and the CIELAB formula (75%), supporting its use in tooth color research [27]. Our results showed ΔE values below both the PT and AT thresholds for both formulas. Therefore, based on these interpretations, the results suggest that the color differences among the groups are clinically acceptable and do not pose a significant issue in terms of aesthetics for the studied composite resin restorations.
Upon interpreting our results, we observed the rejection of the third null hypothesis of this study, which suggested that self-adhesive resins would exhibit μTBS comparable to the CFR established in the market. This rejection was evidenced by two main factors: the occurrence of early restoration failure and the lower average μTBS in the groups restored with the SARF. The occurrence of restoration failure during the preexperimental period was reported in a previous study [13,17]. The fusio liquid dentin (FLD) group was the only group that did not exhibit failure, while the other self-adhesive resins showed failure frequencies of 3 out of 10 restorations and 5 out of 10 restorations, respectively [13]. The presence of this phenomenon may bias the results, leading to a possible overestimation of the values. Consequently, the authors chose to consider the μTBS value to be 0 MPa in cases of failure [13,17]. In the present study, we decided to exclude samples that fractured before the microtensile test from the analyses. This procedure was adopted to ensure the integrity and reliability of the results. The inferior performance of self-adhesive resins compared to CFR in terms of μTBS is supported by several previous studies [13,15,17,29,38].
Cengiz and Unal [40] conducted a microtensile μTBS test using Vertise Flow (VF) and Fusion Liquid Dentin (FLD) self-adhesive resins with and without the use of self-etch or total-etch dentin adhesives. The groups that did not receive dentin adhesive, as recommended by the manufacturers, had lower μTBS values. Notably, the use of universal adhesive with the total-etch technique improved the μTBS in all the evaluated groups. This study used a sample size of n=10 per group, similar to the values found in the Constic (n=11) and Yflow SA (n=8) groups in our research. The mean μTBS found without the use of the adhesive system was 8.06 for VF and 5.38 for FLD, values that are close to those found in our study: 11.027 for Constic and 8.17 for Yflow SA.
Peterson et al. [38] observed that the adhesive tags in self-adhesive resins were thin and spaced, in contrast to those in conventional resin, where they were partially branched. This study highlighted the poor interaction with dental tissue in the presence of a smear layer, raising doubts about the viability of self-adhesive resins as direct restorative materials [38,41]. It is important to highlight that these findings were revealed in a study that used flat dentin; under conditions closer to clinical reality, the failure rates may be even greater [42]. However, when applied to a dental surface without a smear layer, self-adhesive resin cements (with a mechanism similar to that of SARF) produce longer and more uniform resin tags [42]. This behavior raises doubts about the similarity of these materials to self-etch adhesives, as suggested by manufacturers [12]. A possible explanation for this recurring result is the high viscosity of self-adhesive resins, which may hinder deep penetration into dentinal tubules and between collagen fibers [13,39]. A systematic review addressing the μTBS of self-adhesive resins revealed that this inferior performance can be improved in dental enamel with the use of total acid conditioning [43].
This study, while informative, has some limitations worth noting. As a laboratory-based assay, it may not fully replicate the complex conditions encountered in the oral cavity, particularly those associated with more intricate cavities beyond the scope of our simulated flat dentin model. Additionally, the sample size in the SARF groups for the μTBS test could impact the generalizability of our findings to clinical settings. However, despite these limitations, our findings offer valuable insights. These findings provide a foundation for future in vitro investigations aimed at confirming the clinical safety and efficacy of SARF materials. By identifying potential areas of improvement and highlighting areas for further research, our study contributes to advancing the understanding and application of the SARF in clinical dentistry.
5. Conclusions
- -
- All the tested resin composites exhibited an increase in Ra following the abrasion protocol. The TNF and Constic SARFs had the highest Ra values;
- -
- The resin composites demonstrated similar color stability following simulated brushing;
- -
- SARFs exhibit weaker μTBS than CFR utilizing an adhesive system.
Author Contributions
Conceptualization, C. d. F. C. L., R.B.W.e.L. and B. B. V.; methodology, C. d. F. C. L., B. B. V., A.U.D.B. and S. B. M.; formal analysis, A. K. M. d. A., R.B.W.e.L. and R. B. E. L.; investigation, C. C. S. S., S. B. M.. and B. B. V.; data curation, C. d. F. C. L., R.B.W.e.L., A.U.D.B. and B. B. V ; writing—original draft preparation, C. d. F. C. L, B. B. V and C. C. S. S.; writing—review and editing, M. A. J. R. M., A. K. M. d. A and R. B. E. L..; visualization, C. d. F. C. L., S. B. M., and A.U.D.B..; supervision, M. A. J. R. M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of Federal University of Paraiba (Project identification code: 48791621.1.0000.5188 /Date 24 August 2021).
Data Availability Statement
All the data are available within the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Josic, U.; D'Alessandro, C.; Miletic, V.; Maravic, T.; Mazzitelli, C.; Jacimovic, J.; et al. Clinical longevity of direct and indirect posterior resin composite restorations: An updated systematic review and meta-analysis. Dent. Mater. 2023, 39, 1085–1094. [Google Scholar] [CrossRef]
- Pilcher, L.; Pahlke, S.; Urquhart, O.; O'Brien, K.K.; Dhar, V.; Fontana, M.; et al. Direct materials for restoring caries lesions: Systematic review and meta-analysis—a report of the American Dental Association Council on Scientific Affairs. J Am Dent Assoc (2023), 154, e1-e98. Erratum in: J. Am. Dent. Assoc 2023, 154.
- Perdigão, J.; Araujo, E.; Ramos, R.Q.; Gomes, G.; Pizzolotto, L. Adhesive dentistry: Current concepts and clinical considerations. J. Esthet. Restor. Dent. 2021, 33, 51–68. [Google Scholar] [CrossRef] [PubMed]
- Stewart, C.A.; Finer, Y. Biostable, antidegradative and antimicrobial restorative systems based on host-biomaterials and microbial interactions. Dent. Mater. 2019, 35, 36–52. [Google Scholar] [CrossRef]
- Zhou, X.; Huang, X.; Li, M.; Peng, X.; Wang, S.; Zhou, X.; et al. Development and status of resin composite as dental restorative materials. J. App Pol. Sci. 2019, 136, 48180. [Google Scholar] [CrossRef]
- Pinna, R.; Usai, P.; Filigheddu, E.; Garcia-Godoy, F.; Milia, E. The role of adhesive materials and oral biofilm in the failure of adhesive resin restorations. Am. J. Dent. 2017, 30, 285–292. [Google Scholar]
- Şişmanoğlu, S. Efficiency of self-adhering flowable resin composite and different surface treatments in composite repair using a universal adhesive. Niger. J. Clin. Pract. 2019, 22, 1675–1679. [Google Scholar] [CrossRef] [PubMed]
- Kalola, A.V.; Sreejith, S.U.; Kanodia, S.; Parmar, A.; Iyer, J.V.; Parmar, G.J. Comparative clinical evaluation of a self-adhering flowable composite with conventional flowable composite in Class I cavity: An in vivo study. J. Conserv. Dent. 2022, 25, 156–160. [Google Scholar]
- Wadhwa, S.; Nayak, U.A.; Kappadi, D.; Prajapati, D.; Sharma, R.; Pawar, A. Comparative Clinical Evaluation of Resin-based Pit and Fissure Sealant and Self-adhering Flowable Composite: An In Vivo Study. Int. J. Clin. Pediatr. Dent. 2018, 11, 430–434. [Google Scholar]
- Hayashi, K.; Ishii, R.; Takamizawa, T.; Aoki, R.; Muto, R.; Suda, S.; et al. Influence of etching mode on bonding performance of self-adhesive flowable resin composites to bovine teeth. Dent. Mater. J. 2024, 43, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Jordehi, A.Y.; Shahabi, M.S.; Akbari, A. Comparison of self-adhering flowable composite microleakage with several types of bonding agent in class V cavity restoration. Dent. Res. J. 2019, 16, 257–263. [Google Scholar] [PubMed] [PubMed Central]
- Sachdeva, P.; Goswami, M.; Singh, D. Comparative evaluation of shear bond strength and nanoleakage of conventional and self-adhering flowable composites to primary teeth dentin. Contemp. Clin. Dent. 2016, 7, 326–331. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Brueckner, C.; Schneider, H.; Haak, R. Shear Bond Strength and Tooth-Composite Interaction With Self-Adhering Flowable Composites. Oper. Dent. 2017, 42, 90–100. [Google Scholar] [CrossRef] [PubMed]
- Abdelraouf, R.M.; Mohammed, M.; Abdelgawad, F. Evaluation of Shear-Bond-Strength of Dental Self-Adhering Flowable Resin-Composite versus Total-Etch One to Enamel and Dentin Surfaces: An In-Vitro Study. Open Access Maced. J. Med. Sci. 2019, 7, 2162–2166. [Google Scholar] [CrossRef]
- Sibai, N.; El Mourad, A.; Al Suhaibani, N.; Al Ahmadi, R.; Al Dosary, S. Shear bond strength of self-adhesive flowable resin composite. Inter. J. Dent. 2022, v2022, 6280624. [Google Scholar] [CrossRef]
- Sachdeva, P.; Goswami, M.; Singh, D. Comparative evaluation of shear bond strength and nanoleakage of conventional and self-adhering flowable composites to primary teeth dentin. Contemp. Clin. Dent. 2016, 7, 326–331. [Google Scholar] [PubMed]
- Elraggal, A.; Raheem, I.A.; Holiel, A.; Alhotan, A.; Alshabib, A.; Silikas, N.; et al. Bond Strength, Microleakage, Microgaps, and Marginal Adaptation of Self-adhesive Resin Composites to Tooth Substrates with and without Preconditioning with Universal Adhesives. J. Adhes. Dent, 2024, 26, 53–64. [Google Scholar]
- Monteiro, B.; Spohr, A.M. Surface Roughness of Composite Resins after Simulated Toothbrushing with Different Dentifrices. J. Int. Oral. Health. 2015, 7, 1–5. [Google Scholar] [PubMed] [PubMed Central]
- Malavasi, C.V.; Macedo, E.M.; Souza, K.D.A.C.; Rego, G.F.; Schneider, L.F.; et al. Surface Texture and Optical Properties of Self-Adhering Composite Materials after Toothbrush Abrasion. J. Contemp. Dent. Pract. 2015, 16, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Lai, G.; Zhao, L.; Wang, J.; Kunzelmann, K.H. Surface properties and color stability of dental flowable composites influenced by simulated toothbrushing. Dent. Mater. J. 2018, 37, 717–724. [Google Scholar] [CrossRef]
- Jefferies, S.R. Abrasive finishing and polishing in restorative dentistry: a state-of-the-art review. Dent. Clin. North. Am. 2007, 51, 379–397. [Google Scholar] [CrossRef] [PubMed]
- Elraggal, A.; Raheem, I.A.; Holiel, A.; Alhotan, A.; Alshabib, A.; Silikas, N.; Watts, D.C.; Alharbi, N.; Afifi, R.R. Bond Strength, Microleakage, Microgaps, and Marginal Adaptation of Self-adhesive Resin Composites to Tooth Substrates with and without Preconditioning with Universal Adhesives. J. Adhes. Dent. 2024, 26, 53–64. [Google Scholar] [PubMed]
- Faggion, C.M., Jr. Guidelines for reporting pre-clinical in vitro studies on dental materials. J. Evid. Based Dent. Pract. 2012, 12, 182–189. [Google Scholar] [CrossRef]
- Delgado, A.H.; Sauro, S.; Lima, A.F.; Loguercio, A.D.; Della Bona, A.; Mazzoni, A. RoBDEMAT: A risk of bias tool and guideline to support reporting of preclinical dental materials research and assessment of systematic reviews. J. Dent. 2022, 127, 104350. [Google Scholar] [CrossRef] [PubMed]
- Arai, Y.; Kurokawa, H.; Takamizawa, T.; Tsujimoto, A.; Saegusa, M.; Yokoyama, M.; et al. Evaluation of structural coloration of experimental flowable resin composites. J. Esthet. Restor. Dent. 2021, 33, 284–293. [Google Scholar] [CrossRef] [PubMed]
- Durand, L.B.; Ruiz-López, J.; Perez, B.G.; Ionescu, A.M.; Carrillo-Pérez, F.; Ghinea, R.; et al. Color, lightness, chroma, hue, and translucency adjustment potential of resin composites using CIEDE2000 color difference formula. J. Esthet. Restor. Dent. 2021, 33, 836–843. [Google Scholar] [CrossRef]
- Sharma, G.; Wu, W.; Dalal, E.N. The CIEDE2000 color-difference formula: Implementation notes, supplementary test data, and mathematical observations. Color. Res. App. 2005, 30, 21–30. [Google Scholar] [CrossRef]
- Gómez-Polo, C.; Portillo Muñoz, M.; Lorenzo Luengo, M.C.; Vicente, P.; Galindo, P.; Martín Casado, A.M. Comparison of the CIELab and CIEDE2000 color difference formulas. J. Prosthet. Dent. 2016, 115, 65–70. [Google Scholar] [CrossRef]
- Turssi, C.P.; Binsaleh, F.; Lippert, F.; Bottino, M.C.; Eckert, G.J.; Moser, E.A.S.; et al. Interplay between toothbrush stiffness and dentifrice abrasivity on the development of noncarious cervical lesions. Clin. Oral. Investig. 2019, 23, 3551–3556. [Google Scholar] [CrossRef]
- Orellana, N.; Ramírez, R.; Roig, M.; Giner, L.; Mercade, M.; Durán, F.; et al. Comparative study of the microtensile bond strength of three different total etch adhesives with different solvents to wet and dry dentin (in vitro test). Acta Odontol. Latinoam. 2009, 22, 47–56. [Google Scholar]
- Yuan, H.; Li, M.; Guo, B.; Gao, Y.; Liu, H.; Li, J. Evaluation of Microtensile Bond Strength and Microleakage of a Self-adhering Flowable Composite. J. Adhes. Dent. 2015, 17, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Bolme, J.; Gjerdet, N.R.; Laegreid, T. Effect of saliva contamination on the bond strength of single-step and three-step adhesive systems. Eur. J. Oral. Sci. 2022, 130, e12838. [Google Scholar] [CrossRef]
- Guler, S.; Unal, M. The Evaluation of Color and Surface Roughness Changes in Resin based Restorative Materials with Different Contents After Waiting in Various Liquids: An SEM and AFM study. Microsc. Res. Tech. 2018, 81, 1422–1433. [Google Scholar] [CrossRef]
- AlHumaid, J.; Al Harbi, F.A.; ElEmbaby, A.E. Performance of Self-adhering Flowable Composite in Class V Restorations: 18 Months Clinical Study. J. Contemp. Dent. Pract. 2018, 19, 785–791. [Google Scholar] [PubMed]
- Costa, R.T.F.; Pellizzer, E.P.; Vasconcelos, B.C.D.E.; Gomes, J.M.L.; Lemos, C.A.A.; de Moraes, S.L.D. Surface roughness of acrylic resins used for denture base after chemical disinfection: A systematic review and meta-analysis. Gerodontology. 2021, 38, 242–251. [Google Scholar] [CrossRef] [PubMed]
- Sanal, F.A.; Kilinc, H. Evaluating Ceramic Repair Materials in Terms of Bond Strength and Color Stability. Int J Prosthodont. 2020, 33, 536–545. [Google Scholar] [CrossRef] [PubMed]
- David, C.; Cuevas-Suárez, C.E.; de Cardoso, G.C.; Isolan, C.P.; de Moraes, R.R.; da Rosa, W.; et al. Characterization of Contemporary Conventional, Bulk-fill, and Self-adhesive Resin Composite Materials. Oper. Dent. 2022, 47, 392–402. [Google Scholar] [CrossRef] [PubMed]
- Peterson, J.; Rizk, M.; Hoch, M.; Wiegand, A. Bonding performance of self-adhesive flowable composites to enamel, dentin and a nanohybrid composite. Odontology 2018, 106, 171–180. [Google Scholar] [CrossRef]
- Makishi, P.; Pacheco, R.R.; Sadr, A.; Shimada, Y.; Sumi, Y.; Tagami, J.; et al. Assessment of Self-Adhesive Resin Composites: Nondestructive Imaging of Resin-Dentin Interfacial Adaptation and Shear Bond Strength. Microsc. Microanal. 2015, 21, 1523–1529. [Google Scholar] [CrossRef]
- Cengiz, T.; Ünal, M. Comparison of microtensile bond strength and resin-dentin interfaces of two self-adhesive flowable composite resins by using different universal adhesives: Scanning electron microscope study. Microsc. Res. Tech. 2019, 82, 1032–1040. [Google Scholar] [CrossRef]
- Mine, A.; De Munck, J.; Van Ende, A.; Poitevin, A.; Matsumoto, M.; Yoshida, Y.; et al. Limited interaction of a self-adhesive flowable composite with dentin/enamel characterized by TEM. Dent. Mater. 2017, 33, 209–217. [Google Scholar] [CrossRef]
- Temel, U.B.; Van Ende, A.; Van Meerbeek, B.; Ermis, R.B. Bond strength and cement-tooth interfacial characterization of self-adhesive composite cements. Am. J. Dent. 2017, 30, 205–211. [Google Scholar] [PubMed]
- David, C.; Cardoso de Cardoso, G.; Isolan, C.P.; Piva, E.; Moraes, R.R.; Cuevas-Suarez, C.E. Bond strength of self-adhesive flowable composite resins to dental tissues: A systematic review and meta-analysis of in vitro studies. J. Prosthet. Dent. 2022, 128, 876–885. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
50%:50% perceptibility and 50%:50% acceptability criteria for ΔEab.
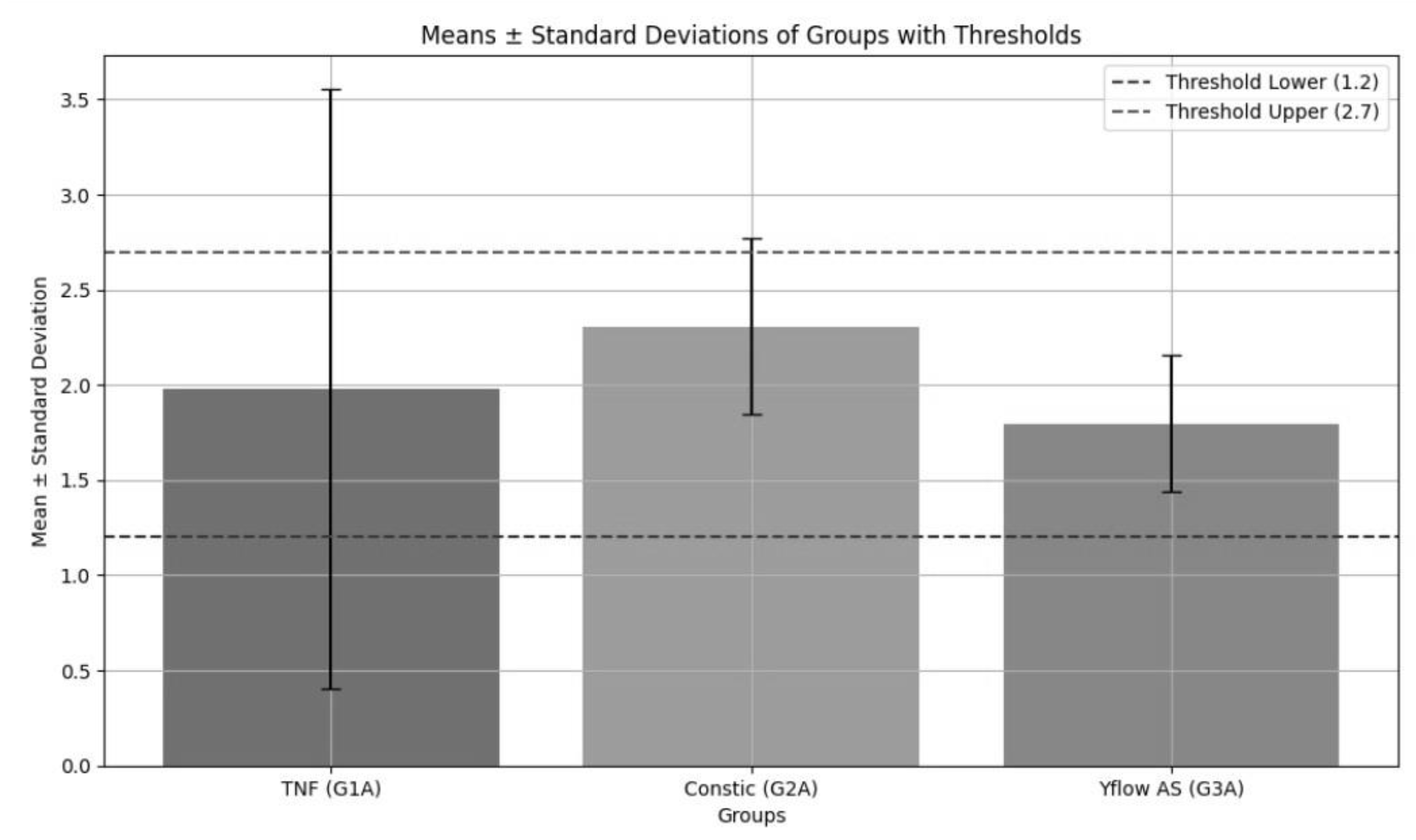
Figure 2.
50%:50% perceptibility and 50%:50% acceptability criteria for ΔE 00.
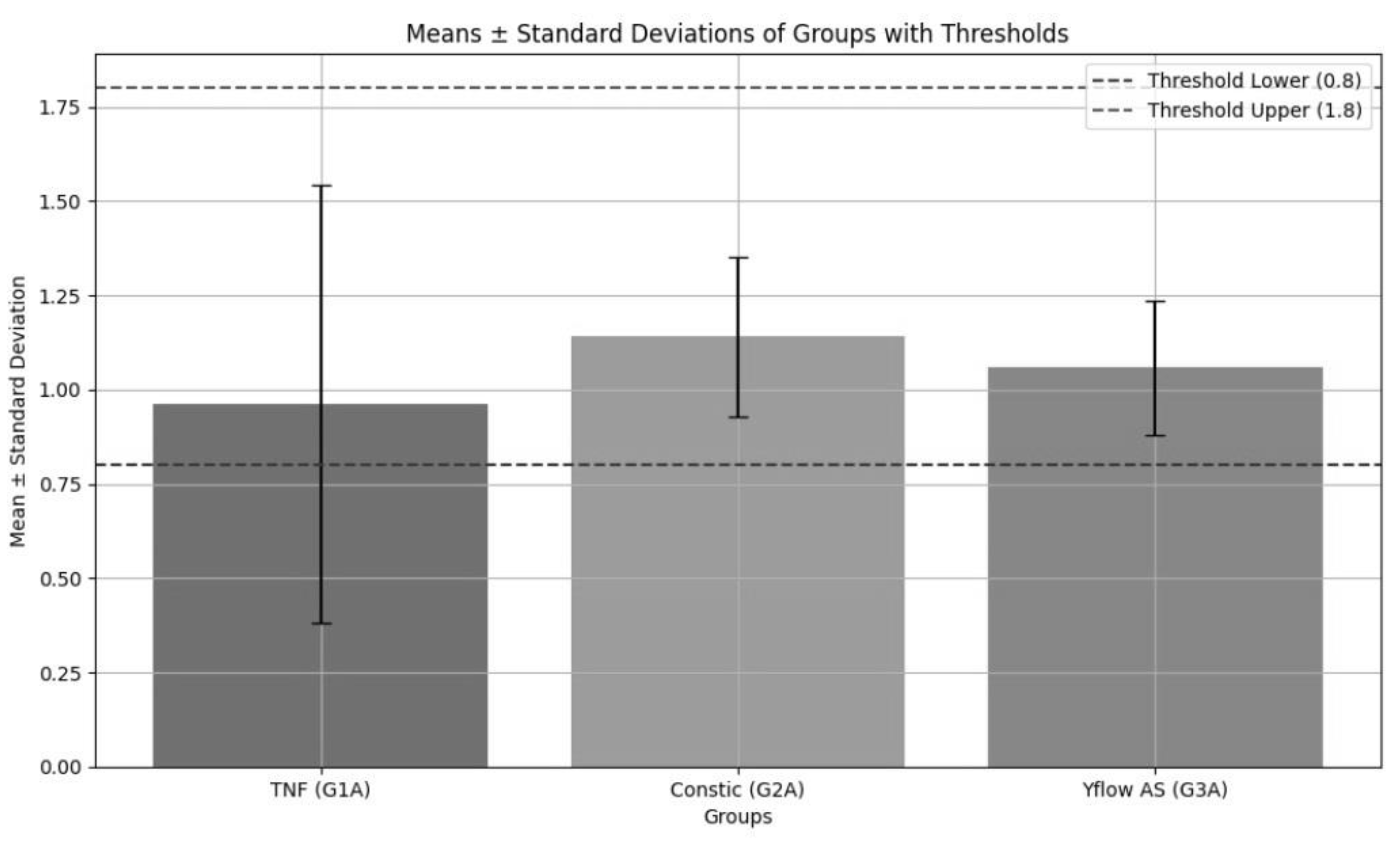
Figure 3.
Means and standard deviations of groups (μTBS).
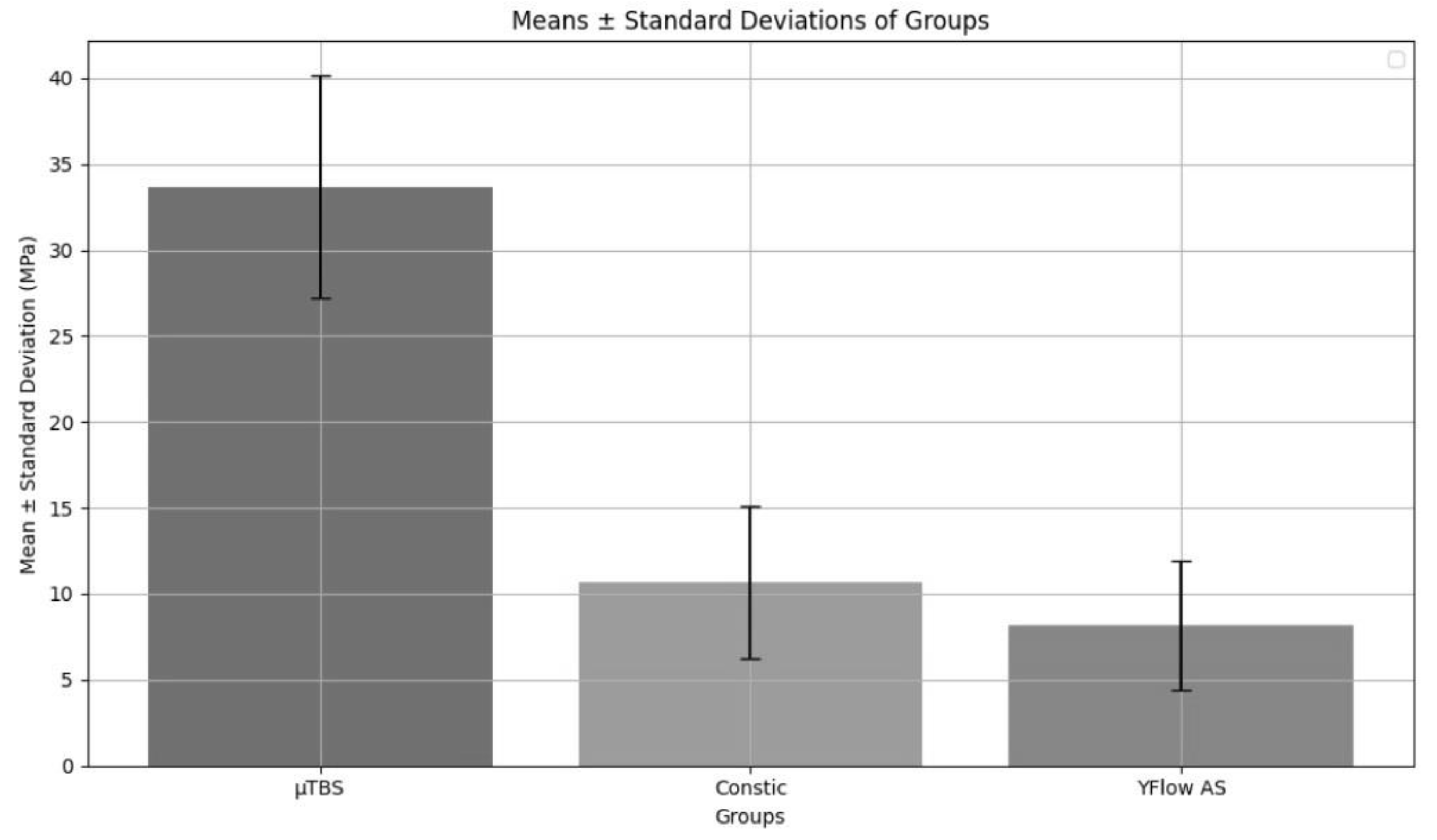
Figure 4.
Fracture patterns. A: Adhesive failure, which is a fracture within the adhesive layer. C: Cohesive failure, either within the resin composite or dentin. M: Mixed failure, where the fracture involves more than one material. P: Pretest failure, indicating that the fracture occurred before testing the specimen. G: Failure outside the testing area, where the specimen was attached to the device
Figure 4.
Fracture patterns. A: Adhesive failure, which is a fracture within the adhesive layer. C: Cohesive failure, either within the resin composite or dentin. M: Mixed failure, where the fracture involves more than one material. P: Pretest failure, indicating that the fracture occurred before testing the specimen. G: Failure outside the testing area, where the specimen was attached to the device


Table 1.
Product Composition.
| Product | Manufacturer | Lot No. | Chemical composition | Technique |
|---|---|---|---|---|
| Tetric N Flow (TNF) | Ivoclar Vivadent, Barueri, SP, Brazil | Z020DP Z019WR |
Dimethacrylates (including TEGDMA), barium oxide, ytterbium trifluoride, highly dispersed silica and mixed oxides, pigments, catalysts, and stabilizers. | Apply the adhesive to the enamel and dentin, then insert the resin into the cavity using the incremental technique. Use increments between 1.5 and 2 mm thick, polymerizing each one for 20 seconds. The halogen light should have a minimum intensity of 500 mW/cm² and be kept as close as possible to the restoration, ensuring that the entire surface is reached. |
| Constic | DMG, Hambug, Germany) | 232801 | Barium glass in a matrix of dental resins based on Bis-GMA. EBADMA, UDMA, HEMA, TEGDMA, HDMA, MDP. Pigments, additives, and catalyst. Filler volume: 66% by weight = 43% by volume. The range of variation of inorganic filler particles is from 0.02 to 2.3 µm. | After preparation, clean the tooth with water spray and then dry it with oil-free air spray. A superficially moist layer should remain. Apply the material to the cavity surface by pressing the syringe and rub for 25 seconds to form a thin layer (0.5 mm). Remove any excess if necessary and light-cure for 20 seconds. Then, apply increments of up to 2 mm and light-cure each one for 20 seconds. |
| Yflow SA | Yller Biomateriais, Pelotas, RS, Brazil | 00009968 | Methacrylate monomers, acid monomers, inorganic fillers, pigments, initiators, and stabilizers. | After dental cleaning, attach the applicator tip to the syringe and dispense the product directly into the preparation. Place the resin in increments of up to 2 mm and light-cure for 40 seconds. |
| Colgate Cavity Protection |
Colgate-Palmolive Industry and Commerce Ltd., New York, USA |
1500 ppm of Fluoride, Calcium Carbonate, Sodium Lauryl Sulfate, Sodium Saccharin, Tetrasodium Pyrophosphate, Sodium Silicate, Polyethylene Glycol, Sorbitol, Carboxymethyl Cellulose, Methylparaben, Propylparaben, Aromatic Composition, and Water. Contains Sodium Monofluorophosphate - MFP® |
Bis-GMA: Bisphenol A glycidyl methacrylate; EBADMA: Ethoxylated Bisphenol A Dimethacrylate; UDMA: Urethane Dimethacrylate; HEMA: 2-hydroxyethyl methacrylate. TEGDMA: Triethylene Glycol Dimethacrylate; HDMA: Hexamethylene Diacrylate; MDP: 10-methacryloyloxydecyl dihydrogen phosphate.
Table 2.
Mean and standard deviation of roughness (µm) before and after brushing.
| Groups | Before | After | p |
|---|---|---|---|
| TNF | 0,101 ± 0,019 | 0,316 ± 0,070 | 0,005* |
| Constic | 0,111 ± 0,019 | 0,702 ± 0,282 | 0,005* |
|
Yflow AS p |
0,131 ± 0,053 0.051 |
0,184 ± 0,065 <0,001* |
0,012* |
Table 3.
Comparison of color difference measures – ΔEab - CIELAB between groups.
| Groups | Mean ± dp |
|---|---|
| TNF | 1,977 ± 1,575 |
| Constic | 2,307 ± 0,464 |
| Yflow AS | 1,798 ± 0,356 |
| p | 0.080 |
Table 4.
Comparison of color difference measures - ΔE 00- CIEDE 200 between groups.
| Groups | Mean ± dp |
|---|---|
| TNF | 0,962 ± 0,580 |
| Constic | 1,140 ± 0,213 |
| Yflow AS | 1,058 ± 0,177 |
| p | 0.144 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



