
Submitted:
07 August 2024
Posted:
08 August 2024
You are already at the latest version
Abstract
Lotions with or without 28% ascorbyl glucoside arginine complex (AGAC) were applied twice daily for 24 weeks in a double‐blind half‐face study of 27 Japanese females with solar lentigos (SLs). Pigmentation scores were evaluated using a photo‐scale and skin colors were assessed using a color difference meter and a Mexameter. Treatment with the test lotion elicited a significant decrease in pigment scores at 24 weeks compared to week 0; with a significant decrease in pigment scores at 24 weeks compared to the placebo lotion‐treated SLs. In the test lotion‐treated SLs; the L values and melanin index (MI) significantly (p<0.0001) increased and decreased; respectively; at 12 and 24 weeks of treatment compared to week 0. Comparisons of increased L (△L) values or decreased MI (△MI) values between test and placebo lotion‐treated SLs demonstrated that the test lotion‐treated SLs had significantly higher △L or △MI values than the placebo lotion‐treated SLs both at 12 and 24 weeks of treatment. The sum of our results strongly indicates that AGAC is distinctly effective in ameliorating the hyperpigmentation levels of SLs at a visibly recognizable level by the subjects without any hypo‐pigmenting effects or skin irritation.
Keywords:
Ascorbyl Glucoside Arginine Complex
; solar lentigo
; double‐blind half‐face study
; pigmentation
; L value
; melanin index
1. Introduction
Solar lentigos (SLs) are hyperpigmented lesions that frequently occur on sun-exposed skin, especially on the face and the dorsum of the hands of Asian subjects [1]. Based on the frequency of the final diagnosis of patients with various pigmentary disorders in Japan, SLs have the highest incidence, occurring in approximately 60% of all patients with hyperpigmentary disorders, while melasma and post-inflammatory hyperpigmentation (including ultraviolet B (UVB) melanosis) occur in as few as 5.2% and 3.3% of patients, respectively [1].
It is well known that UVB-induced hyperpigmentation develops a few days after exposure to UVB radiation and completely disappears within a few weeks to several months, depending on the ages of the subjects, after discontinuation of the UVB exposure [2]. The relatively rapid disappearance of UVB-pigmentation is mechanically associated with the UVB-hyperpigmentation mechanism involved whereby UVB radiation causes keratinocytes to transiently release IL-1α, which then stimulates the release of endothelin (EDN) and the cell membranous expression of stem cell factor (SCF) in an autocrine fashion, which in turn results in the transient activation of neighboring melanocytes [3,4,5,6,7,8,9,10,11,12]. That transient melanocyte activation ends immediately after the discontinuation of UVB irradiation. On the other hand, while SLs never develop within a few days after UVB exposure, they usually appear suddenly many years after repeated UVB exposures, and SLs never disappear thereafter [1]. These clinical characteristics of SLs have been speculated to be due to significant levels of cumulative DNA damage that occur in repeatedly UVB-exposed keratinocytes in the lesional epidermis [1]. Our studies of the biological factors that cause SLs already demonstrated that the lesional keratinocytes suffering from UV-induced DNA damage may begin to continuously secrete tumor necrosis factor (TNF)-α via an unknown mechanism, which in an autocrine fashion between keratinocytes triggers the secretion of EDNs and the cell membranous expression of SCF, resulting in turn in the continuous activation of neighboring melanocytes [13,14].
In general, hyperpigmentary disorders, including UVB-melanosis, SLs and melasma, are targeted by anti-pigmenting agents. However, an effective anti-pigmenting treatment for SLs is difficult especially for dark-skinned individuals because the treatment is required to reduce the hyperpigmentation without causing any undesirable hypopigmentation or contact irritation in the surrounding normally appearing pigmented skin. It is thought that hydroquinone (HQ) is one of the most effective drugs to treat hyperpigmentary disorders including SLs [15,16,17,18,19], but treatment with HQ often causes skin irritation [20,21,22,23,24,25,26]. Although many whitening agents are available [27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44] , some of which are targeted and approved especially to treat UVB-induced hyperpigmentation in Japan, little is known about the potential anti-pigmenting effects of those whitening agents on SLs because clinical evaluations of SLs are not required for approval as a whitening agent in Japan. Excluding kojic acid and rhododendrol, which have been reported to elicit hypopigmentation on the faces of dark-skinned individuals [45,46,47,48], other whitening agents approved in Japan are suitable candidates for investigating their potential anti-pigmenting effects on SLs because they have been proven to be substantially safe in terms of hypopigmentation and skin irritation since they have been commercially available for a long period of time. Among those whitening agents, ascorbic acid derivatives are thought to be invaluable agents especially from the skin safety point of view.
L-ascorbate-2-phosphate Mg (AMP), a whitening agent first approved in Japan, was reported to have a significant ameliorating effect on chloasma by acting as a tyrosinase inhibitor after it is enzymatically degraded by intrinsic epidermal phosphatases to release free ascorbic acid [49,50,51,52,53,54,55,56]. L-ascorbate-2-phosphate trisodium salt (APS) is another approved whitening agent in Japan [49,57,58]. APS is a modified derivative of AMP that improves its stability, namely its aggregation due to the Mg salt [59]. Ascorbyl glucoside (AG) is also a whitening agent approved in Japan that has been documented to have a depigmenting effect on UVB-hyperpigmentation by acting as a tyrosinase inhibitor itself or after it is converted by intrinsic epidermal glucosidase to free ascorbic acid [44].
Based on the requirement for approval of whitening agents in Japan, it is well established that topical application of AMP, APS or AG for 21 days on UVB (2MED)-exposed human skin significantly inhibits the UVB-increased pigmentation measured as L values at 21 days post-UVB irradiation. However, there had been no published data on the anti-pigmenting effect of topical treatment with APS, AMP or AG on SLs in a double-blind half-face study although a whole-face study using AMP on SLs for 3 months was reported to have some efficacy [50], although that study was flawed due to the lack of a placebo control. We have recently reported for the first time that in a double-blind half-face study of 27 Japanese female subjects with SLs using lotions with or without 6% APS (test lotion and placebo lotion, respectively) applied twice a day for 24 weeks, APS has a weak but significant anti-pigmenting effect on SLs and also a significant whitening effect even on normally pigmented non-lesional surrounding skin (NLS) [60]. However, that clinical study was not satisfactory for clinical evaluation because there was no significant difference in the pigment scores of SLs judged by a dermatologist between the test and placebo lotions. This prompted us to characterize the anti-pigmenting effects of ascorbyl glucoside arginine complex (AGAC) on SLs via the modification of AG by making a complex with arginine to reduce its acidity and to increase the concentration used to 28%. In this study, we conducted a double-blind half-face study of 27 Japanese female subjects with SLs using lotions with or without 28% AGAC (test lotion and placebo lotion, respectively) applied twice a day for 24 weeks. Here we show that repeated topical treatment with AGAC has a significant anti-pigmenting effect on SLs with a significant difference in pigment scores of SLs judged by a dermatologist between the test and the placebo lotions. Those results were corroborated by mechanical evaluations using a color difference meter and a Mexameter, and show that there was a significant whitening effect even on normally pigmented NLS without any hypo-pigmenting effects at a mechanical skin color level.
2. Results
2.1. Visible pigmentation level of SLs
Topical applications of lotions with or without 28% AGAC (test lotion and placebo lotion, respectively) were carried out twice daily for 24 weeks on the entire right and left sides of the subjects’ faces with SLs. The pigmentation levels of previously assigned SLs on the subjects’ faces were assessed at 0, 12 and 24 weeks using a photo-scale ranging from 1.0 to 5.0 by a dermatologist (KN) and these results are shown in Figure 1. The results indicated that whereas the placebo lotion-treated SLs did not have any significant decrease in pigment scores at 24 weeks of treatment, the test lotion-treated SLs had a significant (p<0.01) decrease in pigment scores at 24 weeks compared to week 0 (Figure 1A), with a significant (p=0.026) decrease in pigment scores at 24 weeks compared to the placebo lotion-treated SLs (Figure 1B). These results suggest that there was a distinct anti-pigmenting effect of the test lotion on SLs at a visible clinical level.
2.2. Clinical photographs of SLs and NLS
Representative photographs of the faces of subjects #7 and #12 before and after treatment for 24 weeks showed that the pigmentation level of the test lotion-treated SLs (red arrows) slightly decreased whereas the pigmentation level of the test lotion-treated NLS (blue arrows) did not have any distinct changes (Figure 2). In contrast, the pigmentation level of the placebo lotion-treated SLs (red arrows) and the NLS area (blue arrows) at 24 weeks remained unchanged compared to week 0 (Figure 2).
2.3. L and MI values of SLs
To evaluate anti-pigmenting effects on SLs, color difference (L) values and MI values of test lotion-treated SLs were measured using a color difference meter and a Mexameter MX18, respectively, at 0, 12 and 24 weeks of treatment and were compared with placebo lotion-treated SLs. In the test lotion-treated SLs, the L values significantly (p<0.0001) increased at 12 and 24 weeks of treatment compared to week 0 with a significant (p<0.0001) increase between 12 and 24 weeks (Figure 3A). In the placebo lotion-treated SLs, the L values also significantly (p<0.01) increased at 12 and 24 weeks of treatment compared to week 0 without any significant increase between 12 and 24 weeks (Figure 3A). Comparisons of increased (△) L values between test and placebo lotion-treated SLs demonstrated that the test lotion-treated SLs had significantly higher △L values than the placebo lotion-treated SLs both at 12 and 24 weeks of treatment (Figure 3B). While over a 2.0 △L and a 1.6 △L are distinctly or slightly, respectively, recognizable levels by the subjects [60], the ratio of subjects with over a 2.0 △L or 1.6 △L of SLs was 6 or 15 of 27 for the test lotion and 0 or 1, respectively, of 27 for the placebo lotion at 0~24 weeks (Figure 3B).
The MI values were significantly (p<0.0001) decreased at 12 and 24 weeks of treatment compared to week 0 in the test lotion-treated SLs with a significant (p<0.0001) decrease between 12 and 24 weeks (Figure 3C), while in the placebo lotion-treated SLs, the MI values also significantly (p<0.0001) decreased at 12 and 24 weeks of treatment compared to week 0 with a significant (p<0.01) decrease between 12 and 24 weeks (Figure 3C). Comparisons of decreased (△) MI values between the test and placebo lotion-treated SLs demonstrated that the test lotion-treated SLs had significantly (p<0.001 and p<0.0001) lower △ MI values than the placebo lotion-treated SLs at both 12 and 24 weeks, respectively, of treatment (Figure 3D). While over a 50 △MI is a distinctly recognizable level [60], the ratio of subjects with over a 50 △MI of SLs was 13 of 27 for the test lotion and 2 of 27 for the placebo lotion (Figure 3D). These findings suggest that the test lotion but not the placebo lotion has a distinct anti-pigmenting effect on SLs at both the color difference and MI levels.
2.4. L and MI values of NLS
To evaluate the whitening effects on NLS, L values and MI values of test lotion-treated NLS were measured using a color difference meter and a Mexameter MX18, respectively, at 0, 12 and 24 weeks of treatment and were compared with the placebo lotion-treated NLS. In the test lotion-treated NLS, L values significantly (p<0.05 and p<0.001) increased at 12 and 24 weeks, respectively, of treatment compared to week 0, whereas in the placebo lotion-treated NLS, L values did not increase at 12 and 24 weeks of treatment compared to week 0 (Figure 4A). Comparisons of △L values between the test and placebo lotion-treated NLS demonstrated that the test lotion-treated NLS had a significantly higher △L value than the placebo lotion-treated NLS at 24 weeks of treatment (Figure 4B). In the test lotion-treated NLS, MI values significantly (p<0.0001) decreased at 12 and 24 weeks of treatment compared to week 0 with a significant decrease between 12 and 24 weeks, while in the placebo lotion-treated NLS, MI values also significantly decreased at 12 and 24 weeks of treatment compared to week 0 without any significant decrease between 12 and 24 weeks (Figure 4C). Comparisons of △ MI values between test and placebo lotion-treated NLS demonstrated that the test lotion-treated NLS had a significantly lower △MI value than the placebo lotion-treated NLS at both 12 and 24 weeks of treatment (Figure 4D). While over a 30 △MI is a slightly recognizable level [60], the ratio of subjects with over a 30 △MI of NLS was 10 of 27 for the test lotion and 1 of 27 for the placebo lotion (Figure 4D). These findings suggest that the test lotion but not the placebo lotion has a distinct whitening effect on NLS at the color difference and MI levels.
2.5. Correlations between L and MI values in SLs and NLS
Correlation plots between L and MI values are shown in Figure 5 for SLs, NLS and SLs+NLS which indicated that L and MI values have a good correlation in SLs, NLS and SLs+NLS. Figure 6 shows correlation plots between L and MI values in test or placebo lotion-treated SLs and NLS. Those correlation plots demonstrated that in the test lotion-treated SLs, while the slopes of the correlation plots occur at a similar level at 0, 12 and 24 weeks of treatment, their intercepts distinctly decrease with a parallel shift through 0, 12 and 24 weeks of treatment. Those results indicate that the test lotion has a distinct potential to increase L values and decrease MI values, reflecting its distinct anti-pigmenting effects. In contrast, treatment with the placebo lotion did not have a tendency similar to the test lotion-treated SLs. In the test lotion-treated NLS, while the slopes of the correlation plots occur at a similar level at 0, 12 and 24 weeks of treatment, their intercepts distinctly decrease with a parallel shift through 0, 12 and 24 weeks of treatment. That indicates that the test lotion has a distinct potential capable of increasing L values and decreasing MI values, reflecting the whitening effects on NLS. In contrast, in the placebo lotion-treated NLS, the correlation plots did not have a such tendency.
2.6. General clinical evaluation
A general clinical evaluation was performed by a trained dermatologist (KN) at 0, 12 and 24 weeks of treatment. That evaluation demonstrated that treatments with the test lotion or the placebo lotion induced a significant decrease in the scores of scaling and stinging sensations at 24 weeks (Figure 7B, F), whereas the same treatments did not cause any changes in dryness, itchiness, erythema, or papules at 12 and 24 weeks (Figure 7A, C, D, E). Stinging sensations were significantly ameliorated after treatment with the test lotion or the placebo lotion for 12 and 24 weeks (p<0.001) compared with week 0 (Figure 7F). These findings indicate that both the test and the placebo lotions have a distinct ameliorating effect on scaling and stinging sensation without any skin irritations.
2.7. Clinical evaluation of skin redness based on erythema index values measured using a Mexameter MX18
Since erythema index values obtained using a Mexameter MX18 can serve as a measure of skin redness [61], erythema index values of test lotion-treated SLs were measured at 0, 12 and 24 weeks of treatment and were compared with those of placebo lotion-treated SLs. In the test lotion-treated SLs, erythema index values did not change at 12 and 24 weeks of treatment compared to week 0 (Figure 8A). In contrast, in the placebo lotion-treated SLs, erythema index values significantly (p<0.01) increased at 24 weeks of treatment compared to week 0 (Figure 8A). Comparisons of increased (△) erythema index values between the test and placebo lotion-treated SLs demonstrated that the test lotion-treated SLs had similar △erythema index values compared to the placebo lotion-treated SLs at both 12 and 24 weeks of treatment (Figure 8B). In the test lotion-treated NLS, erythema index values did not change at 12 and 24 weeks of treatment compared to week 0 (Figure 8A). However, in the placebo lotion-treated NLS, erythema index values significantly (p<0.0001) increased at 12 and 24 weeks of treatment compared to week 0 (Figure 8A). Comparisons of increased erythema index values between the test and placebo lotion-treated NLS demonstrated that the test lotion-treated NLS had lower △erythema index values than the placebo lotion-treated NLS at both 12 and 24 weeks of treatment (Figure 8B). These results indicate that the test lotion but not the placebo lotion has a distinct potential to ameliorate skin redness, which may reflect a weak anti-inflammatory effect of the test lotion.
2.8. Skin Safety
During the test period of 24 weeks, there were no skin problems including skin irritation or hypopigmentation in the test lotion or placebo lotion-treated skin. Therefore, the test lotion was considered by a dermatologist to be safe for long term use.
3. Discussion
Several epidermal hyperpigmentation mechanisms have been previously established [2,3,4,5,6,9,10,11,62] in which increased amounts of melanin granules in the hyperpigmented epidermis are mechanistically associated with either the up-regulated expression of tyrosinase in melanocytes and/or an increased level of melanocyte proliferation. The increased synthesis of tyrosinase and the stimulated melanocyte proliferation are substantially followed by melanocyte activation, which is triggered via activated intracellular signaling induced by melanogenic cytokines EDN and SCF that are highly secreted or produced by UV-exposed or mutated epidermal keratinocytes in SLs via an autocrine mechanism between keratinocytes with IL-1α or TNFα [3,5,6,11,13]. The activation of the SCF and/or EDN1-triggered intracellular signaling cascades mainly occurs in the MAPKK cascade, at the terminal point of which the cyclic AMP responsive element CREB is phosphorylated and activated by activated RSK or PKA [3,63]. The activation of CREB in turn stimulates expression of the melanocyte-specific master transcription factor MITF, which leads to the increased expression of many melanogenic components including tyrosinase, melanosomal proteins such as Pmel17 and EDN receptors [3,12,64]. In the lesional epidermis of SLs, SCF and EDN1 are significantly up-regulated at the mRNA and protein levels [13,14], which synergistically activates the MAPKK pathway [8]. Activation of the MAPKK pathway leads to the stimulated expression of almost all melanogenic components including tyrosinase, melanosomal proteins and their corresponding receptors, c-KIT and EDNRB at the gene, protein and immunostaining levels [1,13,14]. These melanogenic stimulation mechanisms involved in SLs could reasonably account for the intensive and persistent refractory hyperpigmentation of SLs. Thus, a reasonable therapeutic approach to ameliorate the epidermal hyperpigmentation in SLs would be to use specific inhibitors for EDN/SCF-activated melanogenic intracellular signaling pathways. In fact, we developed a signaling inhibitor isolated from a M. chamomilla extract (MCE) that can block the EDN-stimulated signaling pathway, which consists of EDN/endothelin receptor B/inositol tris phosphate/phospholipaseC/diacylglycerol/PKC/Raf-1/MET/ERK/RSK/cAMP/PKA/CREB/ MITF/tyrosinase [62,65,66]. We found that topical application of the MCE has a distinct potential to significantly reduce the hyperpigmentation levels of UVB-induced melanosis and SLs [66]. On the other hand, a challenge for the use of signaling inhibitors is that there is little expectation for the whitening effects on normally pigmented skin. That is a significant concern for Asian subjects with darkly-pigmented skin because of the lack of signaling activation mechanisms within melanocytes in normally pigmented skin. In this connection, tyrosinase inhibitors with high skin safety, such as ascorbic acid derivatives, would be good candidates as therapeutic agents that could ameliorate the hyperpigmented levels of SLs and also elicit a whitening effect on normally pigmented skin.
AGAC is thought to serve as a tyrosinase inhibitor following its conversion to ascorbic acid via its deglucosylation by epidermal α-glucosidases after it penetrates into the epidermis. α-glucosidases are known to exist in the epidermis as a protein glycosylation processing enzyme that can break the glucose of asparagine-linked carbohydrate moieties bound to proteins to release glucose in the Golgi area of keratinocytes [67]. In order for the action of tyrosinase inhibitors to be effective, it was essential to know whether the hyperpigmentation of SLs is accompanied by an accentuated expression of the key melanogenic enzyme tyrosinase in the lesional melanocytes. In this connection, it had already been reported that the hyperpigmentation in SLs occurs in concert with the up-regulated mRNA levels of tyrosinase in the increased numbers of tyrosinase-positive melanocytes in the SL lesional epidermis [14].
The present double-blind half-face study of subjects with SLs demonstrated that, whereas the placebo lotion did not cause any significant (p<0.01) decrease in pigment scores at 24 weeks of treatment, the test lotion containing AGAC elicited a significant (p<0.01) decrease in pigment scores at 24 weeks compared to week 0, with a significant (p=0.026) decrease in pigment scores at 24 weeks compared to the placebo lotion-treated SLs, which suggests that AGAC has a weak but distinct potential to ameliorate the clinical hyperpigmentation level of SLs. This clinical anti-pigmenting effect was corroborated by mechanical observations using a color difference meter and a Mexameter. In those mechanical evaluations, although both the test and the placebo lotions significantly increased L values or decreased MI values at 12 and 24 weeks of treatment, comparisons of the increased (△) L values or the decreased (△) MI values between the test and placebo lotion-treated SLs demonstrated that the test lotion-treated SLs had significantly higher △L and △MI values than the placebo lotion-treated SLs at both 12 and 24 weeks of treatment. Since the significant anti-pigmenting effects of the placebo lotion might reflect seasonal changes in skin color from September to February during this clinical study, the significant differences observed in both the △L and △MI values at 12 and 24 weeks compared to week 0 between the test and placebo lotions suggest that AGAC has a distinct anti-pigmenting effect on SLs at the color difference and MI levels. Further, our finding that the ratio of subjects with distinctly recognizable levels of over a 2.0 △L value or a 50 △MI value of SLs was 6 or 13 of 27 for the test lotion, and 0 or 2, respectively, of 27 for the placebo lotion at 0~24 weeks strongly supports the distinct and clinical ameliorating effects of AGAC on the hyperpigmentation levels of SLs. The sum of our results strongly indicates that AGAC is distinctly effective in diminishing the hyperpigmentation levels of SLs at a visibly recognizable level by the subjects themselves.
Of considerable interest is that in the test lotion-treated NLS, both the L and MI values significantly increased or decreased at 12 and 24 weeks of treatment compared to week 0. In contrast, in the placebo lotion-treated NLS, the L values did not increase at 12 and 24 weeks of treatment compared to week 0, while the MI values significantly decreased at 12 and 24 weeks of treatment. Although the significant decrease of the MI values in the placebo lotion-treated NLS seems to occur due to the seasonal variation from September to February during this clinical study, the significant whitening effects of the test lotion on NLS indicate that AGAC is to a certain extent effective in brightening the skin color levels of NLS. Comparisons of increased L (△L) values or decreased △MI values between the test and placebo lotion-treated SLs demonstrated that the test lotion-treated NLS have significantly higher △L and △MI values than the placebo lotion-treated NLS at 24 or both 12 and 24, respectively, weeks of treatment. Since the increased or decreased levels of L or MI values occur at lower levels than 2.0 △L or 50 △MI, respectively, it is probable that the subjects with SLs could not visibly recognize the skin color changes in NLS.
In the time course of the anti-pigmenting effects measured by a color difference meter and a Mexameter, the significant effects of the test lotion on SLs occurred in a step-by-step manner at 12 and 24 weeks of treatment with significant changes even between 12 and 24 weeks. In contrast, those significant effects of the placebo lotion occurred at 12 and 24 weeks of treatment without any significant changes between 12 and 24 weeks. These time course trends of the anti-pigmenting effects by the test lotion could provide an insight into predicting more distinct anti-pigmenting effects by further prolonged treatments with the test lotion. On the other hand, the test lotion-treated NLS had a significantly higher △L value than the placebo lotion-treated NLS at 24 weeks of treatment. In addition, the MI values of the test lotion-treated NLS significantly (p<0.001) decreased at 24 weeks of treatment compared to week 0 with a significantly lower △ MI value than the placebo lotion-treated NLS at both 12 and 24 weeks of treatment. The sum of these findings indicates that the test lotion has a significantly higher whitening effect on NLS than the placebo lotion and suggests that AGAC has a weak but significant whitening effect on NLS without any hypo-pigmenting effects.
It is of considerable interest to compare the anti-pigmenting effects on SLs and the whitening effects on NLS between AGAC and ASP, because the latter has been reported to have both anti-pigmenting and whitening effects in subjects with SLs [60]. Although both compounds have similar anti-pigmenting and whitening effects on SLs and NLS, respectively, as revealed by evaluation of L and MI values, a major difference occurs at the clinical scoring levels of pigmentation in SLs in which AGAC but not ASP exhibited a significant (p<0.01) decrease in pigment scores at 24 weeks compared to week 0, with a significant (p=0.026) decrease in pigment scores at 24 weeks compared to the placebo lotion-treated SLs. This indicates a slight superiority of AGAC to ASP from a clinical point of view although the production cost is much higher for AGAC than ASP. It is likely that the slight superiority of AGAC to ASP can be ascribed to the higher concentration used, i.e. 28% AGAC compared to 6% ASP, despite the fact that the rate of penetration into the epidermis is thought to be much higher for ASP than AGAC.
A major skin problem that occurs during the long term topical application of anti-pigmenting agents is skin irritation as is frequently observed for HQ [20,21,22]. Since such a long time of topical applications is required to attain a distinct anti-pigmenting effect in dark-skinned individuals with SLs, skin irritation that happens during the treatment is a major causative factor for not being able to continue the topical applications. Therefore, general clinical evaluations of skin symptoms, including skin irritation, are important and were carried out in this study by a trained dermatologist (KN). These clinical evaluations demonstrated that, while the test lotion rather significantly ameliorated scaling and stinging sensations at 24 weeks, there was no appearance of erythema, papules or itchiness during the 24 weeks of treatment. Further, based on the evidence that erythema index values measured using a Mexameter can serve as a reflection of skin redness due to hemoglobin levels in the blood flow [61], our evaluations revealed that the test lotion but not the placebo lotion has a distinct potential capable of diminishing skin redness. These findings strongly suggest that AGAC could act as an anti-pigmenting agent with a weak anti-inflammatory effect.
In conclusion, the sum of the above findings indicates that AGAC has a weak but significant anti-pigmenting effect on SLs and a significant whitening effect even on normally pigmented skin without the risk of eliciting hypopigmentation or skin irritation. This provides skin safety at a sufficient level to use for a long period time of topical applications, which is an essential requirement to achieve distinct anti-pigmenting effects on SLs.
4. Materials and Methods
4.1. Test materials
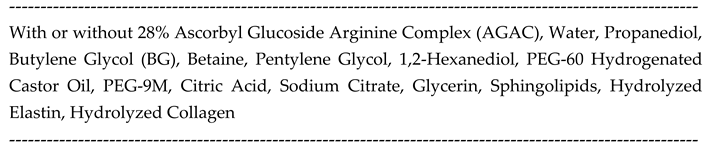
The chemical structure of AGAC is shown in Figure 9. The test and placebo lotions were provided by Doctor’s Choice Co., Ltd. The test lotion was comprised of 28% AGAC and other ingredients as listed in Table 1. The placebo lotion was comprised of the same components as the test lotion except it did not include AGAC.
4.2. Study design
This study was performed from September 2023 to March 2024, in the Ebisu Skin Research Center, Inforward Co. LTD, Tokyo, Japan. Lotions with or without 28% AGAC (test lotion and placebo lotion, respectively) were applied twice a day for 24 weeks. Thus, 27 Japanese female volunteers with SLs on the entire right and left sides of their faces were treated in a double-blind manner with the test lotion on one-half of their face and with the placebo lotion on the opposite side.
4.3. Compliance with ethical standards
Ethical approval
All procedures performed in this study involving human subjects were in accordance with the ethical standards of the Institutional and/or National Research Committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The present study adhered to the tenets of the Declaration of Helsinki and was reviewed and approved by the Japanese Ethics Committee, Clinical Research Review Center, General Incorporated Association (Approval No: CrrC23-020). A formal informed consent was obtained from each subject before the study. The UMIN study ID was assigned as UMIN000052115. Following screening by a dermatologist, 27 Japanese female volunteers with SLs on the entire right and left sides of their faces were enrolled in this study.
4.4. Evaluation of pigmentation level
Pigmentation levels in previously assigned SLs were evaluated using a photo-scale ranging from 1.0 to 5.0 of SLs on the face by a trained dermatologist (KN). The pigmentation levels in those previously assigned SLs and in non-lesional surrounding skin (NLS) were measured using a color difference meter CM-700 d (Konica Minolta Japan, Inc) to determine L values [60] and using a Mexameter MX18 (Courage+Khazaka Electronic GmbH)[61,68,69,70] to measure Melanin Index (MI) values at 0, 12 and 24 weeks of treatment.
4.5. General clinical evaluation
A general clinical evaluation was performed for dryness, scaling, erythema, papules, stinging sensations or itchiness with 1 to 5 scoring grades by a trained dermatologist (KN) at 0, 12 and 24 weeks of treatment.
4.6. Evaluation of skin redness level
For evaluation of skin irritation, skin redness levels in previously assigned SLs and NLS were evaluated using a Mexameter MX18 as erythema index values, which reflect hemoglobin levels related to skin blood flow [61].
4.7. Statistics
All data are expressed as means ± standard deviation (SD) unless noted otherwise. For pairwise comparisons, t test was used. Wilcoxon matched-pair test and Tukey’s comparison test were used to evaluate pigment scores and changes in L values and MI values, respectively. Friedman’s test and Dunn’s multiple comparisons test were used for skin scoring. p values < 0.05 are considered statistically significant.
Author Contributions
A.Y. and G.I. designed this study. M.T., K.N. and M.N. analyzed the data and M.T. and G.I. wrote the manuscript. M.N. and A.Y. financially supported this study. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Data Availability Statement
All relevant data are included in the manuscript.
Acknowledgments
Dr. Vincent Hearing has critically read this manuscript and made some kind and useful suggestions.
Conflicts of Interest
The authors state no conflict of interest.
Abbreviations:
SLs, solar lentigos; AGAC, Ascorbyl Glucoside Arginine Complex; EDN, endothelin; SCF, stem cell factor; NLS, non-lesional surrounding skin; AG, Ascorbyl Glucoside; AMP, L-ascorbate-2-phosphate Mg; APS, L-ascorbate-2-phosphate trisodium salt; HQ, hydroquinone; MI, melanin index; TNF, tumor necrosis factor; UVB, ultraviolet B.
References
- Imokawa, G. , Melanocyte Activation Mechanisms and Rational Therapeutic Treatments of Solar Lentigos. Int J Mol Sci 2019, 20. [Google Scholar] [CrossRef] [PubMed]
- Hachiya, A.; Kobayashi, A.; Yoshida, Y.; Kitahara, T.; Takema, Y.; Imokawa, G. , Biphasic expression of two paracrine melanogenic cytokines, stem cell factor and endothelin-1, in ultraviolet B-induced human melanogenesis. Am J Pathol 2004, 165, 2099–109. [Google Scholar] [CrossRef] [PubMed]
- Yada, Y.; Higuchi, K.; Imokawa, G. , Effects of endothelins on signal transduction and proliferation in human melanocytes. J Biol Chem 1991, 266, 18352–7. [Google Scholar] [CrossRef] [PubMed]
- Imokawa, G. , Autocrine and paracrine regulation of melanocytes in human skin and in pigmentary disorders. Pigment Cell Res 2004, 17, 96–110. [Google Scholar] [CrossRef] [PubMed]
- Imokawa, G.; Yada, Y.; Miyagishi, M. , Endothelins secreted from human keratinocytes are intrinsic mitogens for human melanocytes. J Biol Chem 1992, 267, 24675–80. [Google Scholar] [CrossRef] [PubMed]
- Imokawa, G.; Miyagishi, M.; Yada, Y. , Endothelin-1 as a new melanogen: coordinated expression of its gene and the tyrosinase gene in UVB-exposed human epidermis. J Invest Dermatol 1995, 105, 32–7. [Google Scholar] [CrossRef] [PubMed]
- Imokawa, G.; Kawai, M.; Mishima, Y.; Motegi, I. , Differential analysis of experimental hypermelanosis induced by UVB, PUVA, and allergic contact dermatitis using a brownish guinea pig model. Arch Dermatol Res 1986, 278, 352–62. [Google Scholar] [CrossRef] [PubMed]
- Imokawa, G.; Kobayasi, T.; Miyagishi, M. , Intracellular signaling mechanisms leading to synergistic effects of endothelin-1 and stem cell factor on proliferation of cultured human melanocytes. Cross-talk via trans-activation of the tyrosine kinase c-kit receptor. J Biol Chem 2000, 275, 33321–8. [Google Scholar] [CrossRef]
- Imokawa, G.; Yada, Y.; Kimura, M. , Signalling mechanisms of endothelin-induced mitogenesis and melanogenesis in human melanocytes. Biochem J 1996, 314 ( Pt 1) Pt 1, 305–312. [Google Scholar] [CrossRef]
- Hachiya, A.; Kobayashi, T.; Takema, Y.; Imokawa, G. , Biochemical characterization of endothelin-converting enzyme-1alpha in cultured skin-derived cells and its postulated role in the stimulation of melanogenesis in human epidermis. J Biol Chem 2002, 277, 5395–403. [Google Scholar] [CrossRef]
- Hachiya, A.; Kobayashi, A.; Ohuchi, A.; Takema, Y.; Imokawa, G. , The paracrine role of stem cell factor/c-kit signaling in the activation of human melanocytes in ultraviolet-B-induced pigmentation. J Invest Dermatol 2001, 116, 578–86. [Google Scholar] [CrossRef] [PubMed]
- Sato-Jin, K.; Nishimura, E. K.; Akasaka, E.; Huber, W.; Nakano, H.; Miller, A.; Du, J.; Wu, M.; Hanada, K.; Sawamura, D.; Fisher, D. E.; Imokawa, G. , Epistatic connections between microphthalmia-associated transcription factor and endothelin signaling in Waardenburg syndrome and other pigmentary disorders. FASEB J 2008, 22, 1155–68. [Google Scholar] [CrossRef] [PubMed]
- Hattori, H.; Kawashima, M.; Ichikawa, Y.; Imokawa, G. , The epidermal stem cell factor is over-expressed in lentigo senilis: implication for the mechanism of hyperpigmentation. J Invest Dermatol 2004, 122, 1256–65. [Google Scholar] [CrossRef] [PubMed]
- Kadono, S.; Manaka, I.; Kawashima, M.; Kobayashi, T.; Imokawa, G. , The role of the epidermal endothelin cascade in the hyperpigmentation mechanism of lentigo senilis. J Invest Dermatol 2001, 116, 571–7. [Google Scholar] [CrossRef] [PubMed]
- Rajaratnam, R.; Halpern, J.; Salim, A.; Emmett, C. , Interventions for melasma. Cochrane Database Syst Rev 2010, 7, Cd003583. [Google Scholar] [CrossRef] [PubMed]
- Arndt, K. A.; Fitzpatrick, T. B. , Topical use of hydroquinone as a depigmenting agent. Jama 1965, 194, 965–7. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, T. B.; Arndt, K. A.; el-Mofty, A. M.; Pathak, M. A. , Hydroquinone and psoralens in the therapy of hypermelanosis and vitiligo. Arch Dermatol 1966, 93, 589–600. [Google Scholar] [CrossRef] [PubMed]
- Kligman, A. M.; Willis, I. , A new formula for depigmenting human skin. Arch Dermatol 1975, 111, 40–8. [Google Scholar] [CrossRef] [PubMed]
- Heilgemeir, G. P.; Balda, B. R. , [Irreversible toxic depigmentation. Observations following use of hydroquinonemonobenzylether-containing skin bleaching preparations]. MMW Munch Med Wochenschr 1981, 123, 47–8. [Google Scholar]
- Halder, R. M.; Richards, G. M. , Topical agents used in the management of hyperpigmentation. Skin Therapy Lett 2004, 9, 1–3. [Google Scholar]
- Cheong, K. A.; Kim, H. J.; Kim, J. Y.; Kim, C. H.; Lim, W. S.; Noh, M.; Lee, A. Y. , Retinoic acid and hydroquinone induce inverse expression patterns on cornified envelope-associated proteins: implication in skin irritation. J Dermatol Sci 2014, 76, 112–9. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Du, X.; Zhang, L.; Jia, T.; Zhang, H.; Peng, B.; Hao, Y.; Tong, Z.; Che, D.; Geng, S. , Hydroquinone-induced skin irritant reaction could be achieved by activating mast cells via mas-related G protein-coupled receptor X2. Exp Dermatol 2023, 32, 436–446. [Google Scholar] [CrossRef] [PubMed]
- Kim, G. H.; Cheong, K. A.; Lee, A. Y. , Increased Skin Irritation by Hydroquinone and Rsetinoic Acid Used in Combination. Ann Dermatol 2017, 29, 715–721. [Google Scholar] [CrossRef] [PubMed]
- McKesey, J.; Tovar-Garza, A.; Pandya, A. G. , Melasma Treatment: An Evidence-Based Review. Am J Clin Dermatol 2020, 21, 173–225. [Google Scholar] [CrossRef] [PubMed]
- Tai, Y.; Wang, C.; Wang, Z.; Liang, Y.; Du, J.; He, D.; Fan, X.; Jordt, S. E.; Liu, B. , Involvement of Transient Receptor Potential Cation Channel Member A1 activation in the irritation and pain response elicited by skin-lightening reagent hydroquinone. Sci Rep 2017, 7, 7532. [Google Scholar] [CrossRef] [PubMed]
- Searle, T.; Al-Niaimi, F.; Ali, F. R. , Hydroquinone: myths and reality. Clin Exp Dermatol 2021, 46, 636–640. [Google Scholar] [CrossRef] [PubMed]
- Cabanes, J.; Chazarra, S.; Garcia-Carmona, F. , Kojic acid, a cosmetic skin whitening agent, is a slow-binding inhibitor of catecholase activity of tyrosinase. J Pharm Pharmacol 1994, 46, 982–5. [Google Scholar] [CrossRef] [PubMed]
- Kumar, K. J.; Vani, M. G.; Wang, S. Y.; Liao, J. W.; Hsu, L. S.; Yang, H. L.; Hseu, Y. C. , In vitro and in vivo studies disclosed the depigmenting effects of gallic acid: a novel skin lightening agent for hyperpigmentary skin diseases. Biofactors 2013, 39, 259–70. [Google Scholar] [CrossRef] [PubMed]
- Gonçalez, M. L.; Corrêa, M. A.; Chorilli, M. , Skin delivery of kojic acid-loaded nanotechnology-based drug delivery systems for the treatment of skin aging. Biomed Res Int 2013, 2013, 271276. [Google Scholar] [CrossRef] [PubMed]
- Ki, D. H.; Jung, H. C.; Noh, Y. W.; Thanigaimalai, P.; Kim, B. H.; Shin, S. C.; Jung, S. H.; Cho, C. W. , Preformulation and formulation of newly synthesized QNT3-18 for development of a skin whitening agent. Drug Dev Ind Pharm 2013, 39, 526–33. [Google Scholar] [CrossRef]
- Breathnach, A. C.; Nazzaro-Porro, M.; Passi, S.; Zina, G. , Azelaic acid therapy in disorders of pigmentation. Clin Dermatol 1989, 7, 106–19. [Google Scholar] [CrossRef] [PubMed]
- Verallo-Rowell, V. M.; Verallo, V.; Graupe, K.; Lopez-Villafuerte, L.; Garcia-Lopez, M. , Double-blind comparison of azelaic acid and hydroquinone in the treatment of melasma. Acta Derm Venereol Suppl (Stockh) 1989, 143, 58–61. [Google Scholar] [PubMed]
- Huang, C. H.; Sung, H. C.; Hsiao, C. Y.; Hu, S.; Ko, Y. S. , Transdermal delivery of three vitamin C derivatives by Er:YAG and carbon dioxide laser pretreatment. Lasers Med Sci 2013, 28, 807–14. [Google Scholar] [PubMed]
- Won, Y. K.; Loy, C. J.; Randhawa, M.; Southall, M. D. , Clinical efficacy and safety of 4-hexyl-1,3-phenylenediol for improving skin hyperpigmentation. Arch Dermatol Res 2014, 306, 455–65. [Google Scholar] [CrossRef] [PubMed]
- Son, K. H.; Heo, M. Y. , The evaluation of depigmenting efficacy in the skin for the development of new whitening agents in Korea. Int J Cosmet Sci 2013, 35, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y. S.; Lee, S. M.; Lin, C. C.; Liu, C. Y.; Wu, M. C.; Shi, W. L. , Kinetic study on the tyrosinase and melanin formation inhibitory activities of carthamus yellow isolated from Carthamus tinctorius L. J Biosci Bioeng 2013, 115, 242–5. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, P. W.; Chen, W. Y.; Aljuffali, I. A.; Chen, C. C.; Fang, J. Y. , Co-drug strategy for promoting skin targeting and minimizing the transdermal diffusion of hydroquinone and tranexamic acid. Curr Med Chem 2013, 20, 4080–92. [Google Scholar] [CrossRef] [PubMed]
- Tse, T. W.; Hui, E. , Tranexamic acid: an important adjuvant in the treatment of melasma. J Cosmet Dermatol 2013, 12, 57–66. [Google Scholar] [CrossRef]
- Eimpunth, S.; Wanitphadeedecha, R.; Manuskiatti, W. , A focused review on acne-induced and aesthetic procedure-related postinflammatory hyperpigmentation in Asians. J Eur Acad Dermatol Venereol 2013, 27 (Suppl. S1), 7–18. [Google Scholar] [CrossRef]
- Pillaiyar, T.; Manickam, M.; Namasivayam, V. , Skin whitening agents: medicinal chemistry perspective of tyrosinase inhibitors. J Enzyme Inhib Med Chem 2017, 32, 403–425. [Google Scholar] [CrossRef]
- Saeedi, M.; Eslamifar, M.; Khezri, K. , Kojic acid applications in cosmetic and pharmaceutical preparations. Biomed Pharmacother 2019, 110, 582–593. [Google Scholar] [CrossRef] [PubMed]
- Desai, S.; Ayres, E.; Bak, H.; Manco, M.; Lynch, S.; Raab, S.; Du, A.; Green, D.; Skobowiat, C.; Wangari-Talbot, J.; Zheng, Q. , Effect of a Tranexamic Acid, Kojic Acid, and Niacinamide Containing Serum on Facial Dyschromia: A Clinical Evaluation. J Drugs Dermatol 2019, 18, 454–459. [Google Scholar] [PubMed]
- Thawabteh, A. M.; Jibreen, A.; Karaman, D.; Thawabteh, A.; Karaman, R. , Skin Pigmentation Types, Causes and Treatment-A Review. Molecules 2023, 28. [Google Scholar] [CrossRef] [PubMed]
- Mota, S.; Rosa, G. P.; Barreto, M. C.; Garrido, J.; Sousa, E.; Cruz, M. T.; Almeida, I. F.; Quintas, C. , Comparative Studies on the Photoreactivity, Efficacy, and Safety of Depigmenting Agents. Pharmaceuticals (Basel) 2023, 17. [Google Scholar] [CrossRef] [PubMed]
- Matsunaga, K.; Suzuki, K.; Ito, A.; Tanemura, A.; Abe, Y.; Suzuki, T.; Yoshikawa, M.; Sumikawa, Y.; Yagami, A.; Masui, Y.; Inoue, S.; Ito, S.; Katayama, I. , Rhododendrol-induced leukoderma update I: Clinical findings and treatment. J Dermatol 2021, 48, 961–968. [Google Scholar] [CrossRef] [PubMed]
- Inoue, S.; Katayama, I.; Suzuki, T.; Tanemura, A.; Ito, S.; Abe, Y.; Sumikawa, Y.; Yoshikawa, M.; Suzuki, K.; Yagami, A.; Masui, Y.; Ito, A.; Matsunaga, K. , Rhododendrol-induced leukoderma update II: Pathophysiology, mechanisms, risk evaluation, and possible mechanism-based treatments in comparison with vitiligo. J Dermatol 2021, 48, 969–978. [Google Scholar] [CrossRef] [PubMed]
- Madhogaria, S.; Ahmed, I. , Leucoderma after use of a skin-lightening cream containing kojic dipalmitate, liquorice root extract and Mitracarpus scaber extract. Clin Exp Dermatol 2010, 35, e103–e105. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, M.; Kondo, M.; Sato, K.; Umeda, M.; Kawabata, K.; Takahashi, Y.; Suzuki, T.; Matsunaga, K.; Inoue, S. , Rhododendrol, a depigmentation-inducing phenolic compound, exerts melanocyte cytotoxicity via a tyrosinase-dependent mechanism. Pigment Cell Melanoma Res 2014, 27, 754–63. [Google Scholar] [CrossRef]
- Elmore, A. R. , Final report of the safety assessment of L-Ascorbic Acid, Calcium Ascorbate, Magnesium Ascorbate, Magnesium Ascorbyl Phosphate, Sodium Ascorbate, and Sodium Ascorbyl Phosphate as used in cosmetics. Int J Toxicol 2005, 24 (Suppl. S2), 51–111. [Google Scholar]
- Kameyama, K.; Sakai, C.; Kondoh, S.; Yonemoto, K.; Nishiyama, S.; Tagawa, M.; Murata, T.; Ohnuma, T.; Quigley, J.; Dorsky, A.; Bucks, D.; Blanock, K. , Inhibitory effect of magnesium L-ascorbyl-2-phosphate (VC-PMG) on melanogenesis in vitro and in vivo. J Am Acad Dermatol 1996, 34, 29–33. [Google Scholar] [CrossRef]
- Kobayashi, S.; Takehana, M.; Itoh, S.; Ogata, E. , Protective effect of magnesium-L-ascorbyl-2 phosphate against skin damage induced by UVB irradiation. Photochem Photobiol 1996, 64, 224–8. [Google Scholar] [CrossRef] [PubMed]
- Murtaza, F.; Bangash, A. R.; Khushdil, A.; Noor, S. M. , Efficacy of Trichloro-Acetic Acid Peel Alone Versus Combined Topical Magnesium Ascorbyl Phosphate for Epidermal Melasma. J Coll Physicians Surg Pak 2016, 26, 557–61. [Google Scholar]
- Shaikh, Z. I.; Mashood, A. A. , Treatment of refractory melasma with combination of topical 5% magnesium ascorbyl phosphate and fluorescent pulsed light in Asian patients. Int J Dermatol 2014, 53, 93–9. [Google Scholar] [CrossRef]
- Silva, G. M.; Maia Campos, P. M. , Histopathological, morphometric and stereological studies of ascorbic acid and magnesium ascorbyl phosphate in a skin care formulation. Int J Cosmet Sci 2000, 22, 169–79. [Google Scholar] [CrossRef]
- Wang, P. C.; Huang, Y. L.; Hou, S. S.; Chou, C. H.; Tsai, J. C. , Lauroyl/palmitoyl glycol chitosan gels enhance skin delivery of magnesium ascorbyl phosphate. J Cosmet Sci 2013, 64, 273–86. [Google Scholar] [PubMed]
- Yamamoto, K.; Shichiri, H.; Ishida, T.; Kaku, K.; Nishioka, T.; Kume, M.; Makimoto, H.; Nakagawa, T.; Hirano, T.; Bito, T.; Nishigori, C.; Yano, I.; Hirai, M. , Effects of Ascorbyl-2-phosphate Magnesium on Human Keratinocyte Toxicity and Pathological Changes by Sorafenib. Biol Pharm Bull 2017, 40, 1530–1536. [Google Scholar] [CrossRef] [PubMed]
- Foco, A.; Gasperlin, M.; Kristl, J. , Investigation of liposomes as carriers of sodium ascorbyl phosphate for cutaneous photoprotection. Int J Pharm 2005, 291, 21–9. [Google Scholar] [CrossRef]
- Nayama, S.; Takehana, M.; Kanke, M.; Itoh, S.; Ogata, E.; Kobayashi, S. , Protective effects of sodium-L-ascorbyl-2 phosphate on the development of UVB-induced damage in cultured mouse skin. Biol Pharm Bull 1999, 22, 1301–5. [Google Scholar] [CrossRef] [PubMed]
- Khan, H.; Akhtar, N.; Ali, A.; Khan, H. M. S.; Sohail, M.; Naeem, M.; Nawaz, Z. , PHYSICAL AND CHEMICAL STABILITY ANALYSIS OF COSMETIC MULTI- PLE EMULSIONS LOADED WITH ASCORBYL PALMITATE AND SODIUM ASCORBYL PHOSPHATE SALTS. Acta Pol Pharm 2016, 73, 1339–1349. [Google Scholar]
- Ishikawa, Y.; Niwano, T.; Hirano, S.; Numano, K.; Takasima, K.; Imokawa, G. , Whitening effect of L-ascorbate-2-phosphate trisodium salt on solar lentigos. Arch Dermatol Res 2019, 311, 183–191. [Google Scholar] [CrossRef]
- Feather, J. W.; Ellis, D. J.; Leslie, G. , A portable reflectometer for the rapid quantification of cutaneous haemoglobin and melanin. Phys Med Biol 1988, 33, 711–22. [Google Scholar] [CrossRef] [PubMed]
- Imokawa, G.; Kobayashi, T.; Miyagishi, M.; Higashi, K.; Yada, Y. , The role of endothelin-1 in epidermal hyperpigmentation and signaling mechanisms of mitogenesis and melanogenesis. Pigment Cell Res 1997, 10, 218–28. [Google Scholar] [CrossRef] [PubMed]
- Niwano, T.; Terazawa, S.; Nakajima, H.; Imokawa, G. , The stem cell factor-stimulated melanogenesis in human melanocytes can be abrogated by interrupting the phosphorylation of MSK1: evidence for involvement of the p38/MSK1/CREB/MITF axis. Arch Dermatol Res 2018, 310, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Niwano, T.; Terazawa, S.; Sato, Y.; Kato, T.; Nakajima, H.; Imokawa, G. , Glucosamine abrogates the stem cell factor + endothelin-1-induced stimulation of melanogenesis via a deficiency in MITF expression due to the proteolytic degradation of CREB in human melanocytes. Arch Dermatol Res 2018, 310, 625–637. [Google Scholar] [CrossRef] [PubMed]
- Imokawa, G.; Ishida, K. , Inhibitors of intracellular signaling pathways that lead to stimulated epidermal pigmentation: perspective of anti-pigmenting agents. Int J Mol Sci 2014, 15, 8293–315. [Google Scholar] [CrossRef] [PubMed]
- Kawashima, M.; Imokawa, G. , Hyperpigmentation mechanisms involved in UVB-melanosis and solar lentigo and clinical effects of Chamomira ET extract on the pigmentation. Mon. Book Derma. 2005, 98, 43–61. [Google Scholar]
- Imokawa, G. , Analysis of carbohydrate properties essential for melanogenesis in tyrosinases of cultured malignant melanoma cells by differential carbohydrate processing inhibition. J Invest Dermatol 1990, 95, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Dawson, J. B.; Barker, D. J.; Ellis, D. J.; Grassam, E.; Cotterill, J. A.; Fisher, G. W.; Feather, J. W. , A theoretical and experimental study of light absorption and scattering by in vivo skin. Phys Med Biol 1980, 25, 695–709. [Google Scholar] [CrossRef] [PubMed]
- Feather, J. W.; Hajizadeh-Saffar, M.; Leslie, G.; Dawson, J. B. , A portable scanning reflectance spectrophotometer using visible wavelengths for the rapid measurement of skin pigments. Phys Med Biol 1989, 34, 807–20. [Google Scholar] [CrossRef]
- Kollias, N.; Baqer, A. , Spectroscopic characteristics of human melanin in vivo. J Invest Dermatol 1985, 85, 38–42. [Google Scholar] [CrossRef]
Figure 1.
Evaluation of pigment scores of SLs at 0, 12 and 24 weeks of treatment.A: Time course of pigment scores of SLs, n=27, **; p<0.01 by Friedman test and Dunn’s multiple comparison test. B: Comparison of pigment scores of SLs between test- and placebo lotion-treated SLs at 24 weeks of treatment, n=27, *: p<0.05, by Wilcoxon matched-pair test.
Figure 1.
Evaluation of pigment scores of SLs at 0, 12 and 24 weeks of treatment.A: Time course of pigment scores of SLs, n=27, **; p<0.01 by Friedman test and Dunn’s multiple comparison test. B: Comparison of pigment scores of SLs between test- and placebo lotion-treated SLs at 24 weeks of treatment, n=27, *: p<0.05, by Wilcoxon matched-pair test.
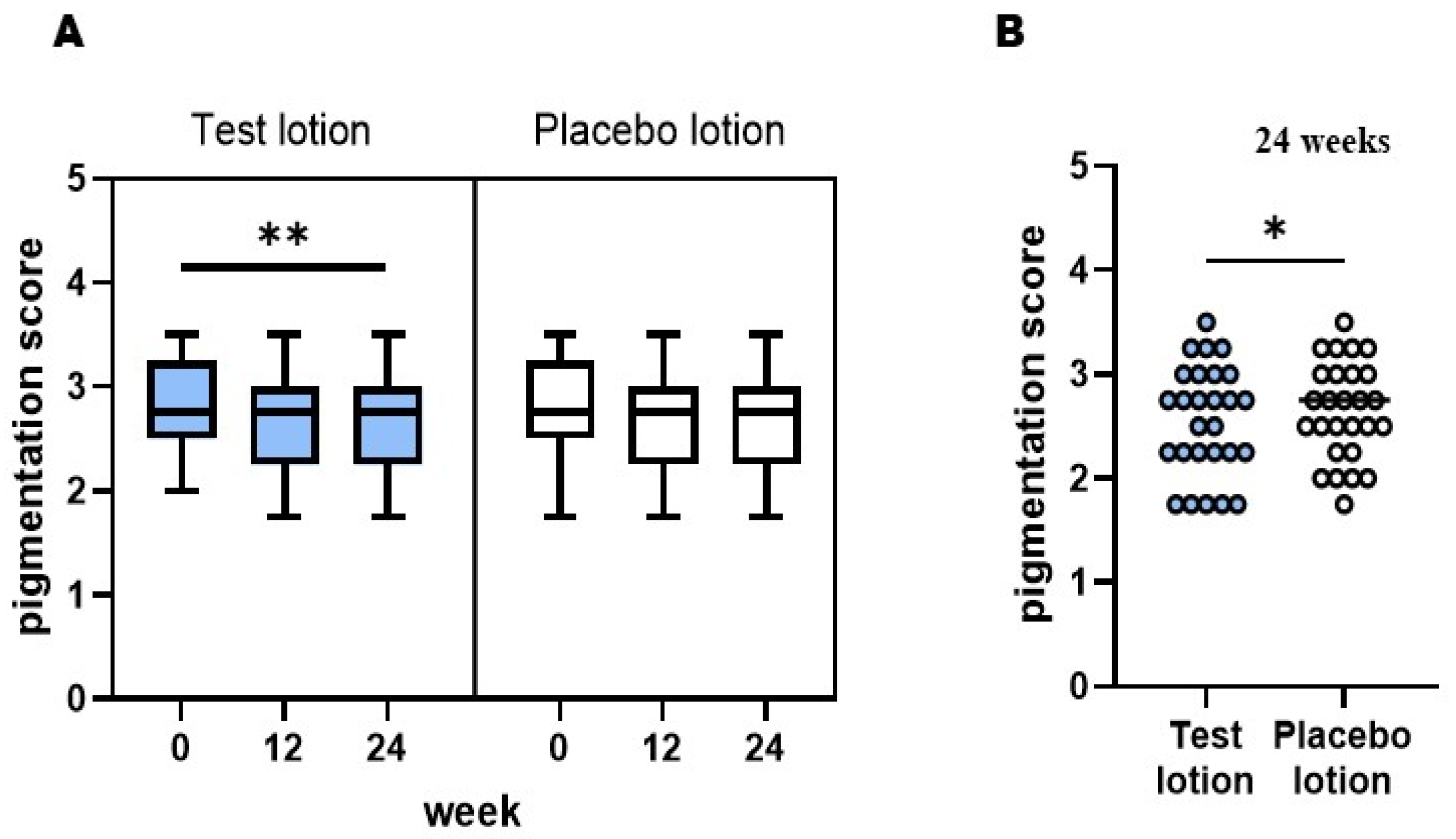
Figure 2.
Clinical photographs of SLs and NLS.A: Subject#7) Test Lotion/SLs (red arrows) at 0 and 24 weeks: ΔL value: 2.23, ΔMI value: 44.33. Test Lotion/NLS (blue arrows) at 0 and 24 weeks: ΔL value: 0.49, ΔMI value: 20.00. Placebo Lotion/SLs (red arrows) at 0 and 24 weeks: ΔL value: -0.24, ΔMI value: 40.00. Placebo Lotion/NLS (blue arrows) at 0 and 24 weeks: ΔL value: 0.21, ΔMI value: 3.67. B: Subject#12) Test Lotion/SLs (red arrows) at 0 and 24 weeks: ΔL value: 2.57, ΔMI value: 76.00. Test Lotion/NLS (blue arrows) at 0 and 24 weeks: ΔL value: 0.22, ΔMI value: 49.00, Placebo Lotion/SLs (red arrows) at 0 and 24 weeks: ΔL value: 1.27, ΔMI value: 44.00. Placebo Lotion/NLS (blue arrows) at 0 and 24 weeks: ΔL value: 1.20, ΔMI value: 21.0.
Figure 2.
Clinical photographs of SLs and NLS.A: Subject#7) Test Lotion/SLs (red arrows) at 0 and 24 weeks: ΔL value: 2.23, ΔMI value: 44.33. Test Lotion/NLS (blue arrows) at 0 and 24 weeks: ΔL value: 0.49, ΔMI value: 20.00. Placebo Lotion/SLs (red arrows) at 0 and 24 weeks: ΔL value: -0.24, ΔMI value: 40.00. Placebo Lotion/NLS (blue arrows) at 0 and 24 weeks: ΔL value: 0.21, ΔMI value: 3.67. B: Subject#12) Test Lotion/SLs (red arrows) at 0 and 24 weeks: ΔL value: 2.57, ΔMI value: 76.00. Test Lotion/NLS (blue arrows) at 0 and 24 weeks: ΔL value: 0.22, ΔMI value: 49.00, Placebo Lotion/SLs (red arrows) at 0 and 24 weeks: ΔL value: 1.27, ΔMI value: 44.00. Placebo Lotion/NLS (blue arrows) at 0 and 24 weeks: ΔL value: 1.20, ΔMI value: 21.0.
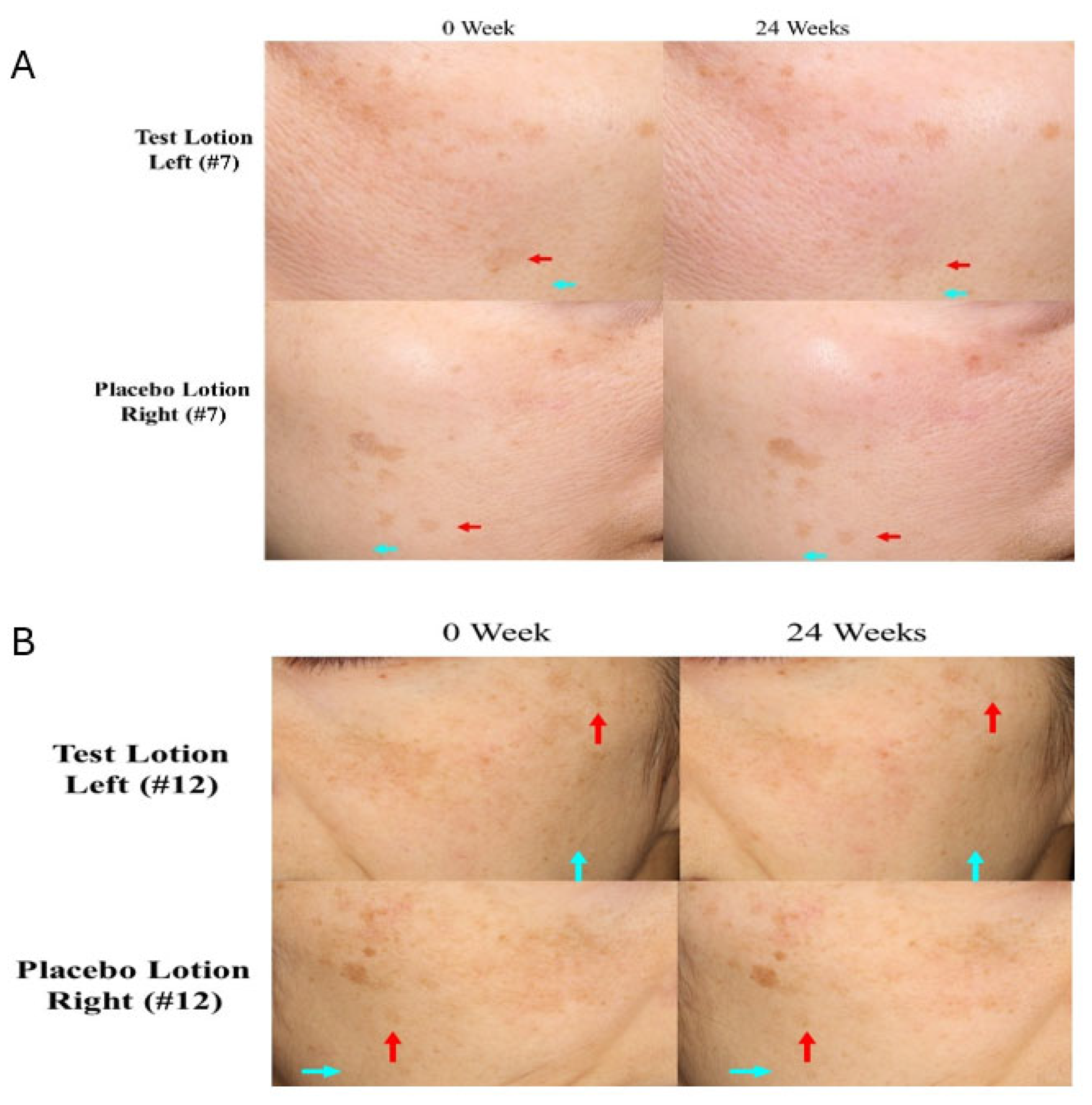
Figure 3.
Changes in L values and MI values of SLs after treatment for 24 weeks. N=27, A/C: Time course study, N=27, ****: p<0.0001, **: p<0.01 by Tukey’s comparison test, B/D: Increased L values and decreased MI values between 0 and 12, 0 and 24, and 12 and 24 weeks. ****: p<0.0001, ***: p<0.001, *: p<0.05 by paired t test.
Figure 3.
Changes in L values and MI values of SLs after treatment for 24 weeks. N=27, A/C: Time course study, N=27, ****: p<0.0001, **: p<0.01 by Tukey’s comparison test, B/D: Increased L values and decreased MI values between 0 and 12, 0 and 24, and 12 and 24 weeks. ****: p<0.0001, ***: p<0.001, *: p<0.05 by paired t test.
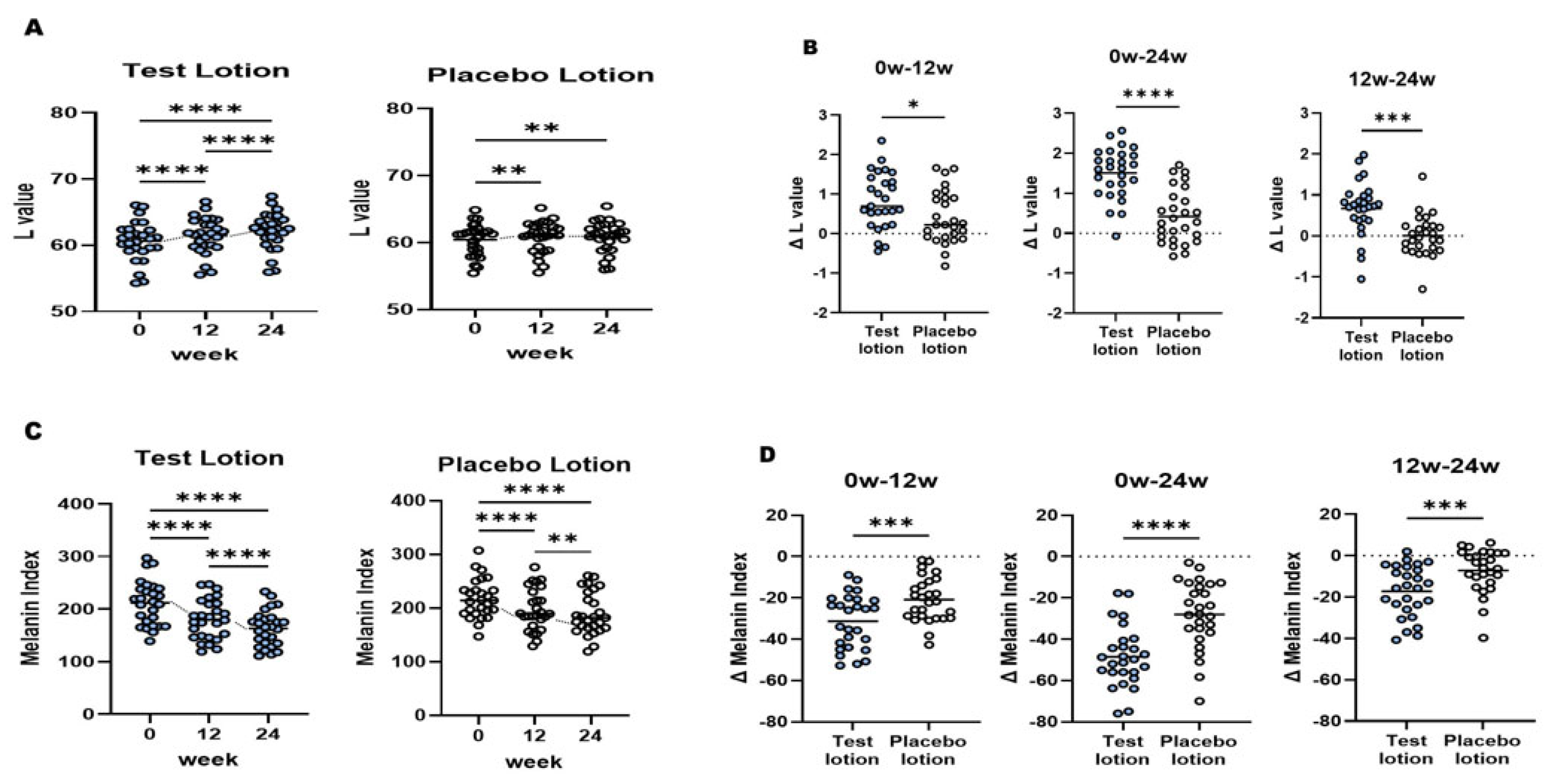
Figure 4.
Changes in L values and MI values of NLS after treatment for 24 weeks. N=27, A/C: Time course study, n=27, ****: p<0.0001; ***: p<0.0001, **: p<0.01 by Tukey’s comparison test, B/D: Increased L values and decreased MI values between 0 and 12. 0 and 24, and 12 and 24 weeks. ****: p<0.0001, ***: p<0.001 by paired t test.
Figure 4.
Changes in L values and MI values of NLS after treatment for 24 weeks. N=27, A/C: Time course study, n=27, ****: p<0.0001; ***: p<0.0001, **: p<0.01 by Tukey’s comparison test, B/D: Increased L values and decreased MI values between 0 and 12. 0 and 24, and 12 and 24 weeks. ****: p<0.0001, ***: p<0.001 by paired t test.
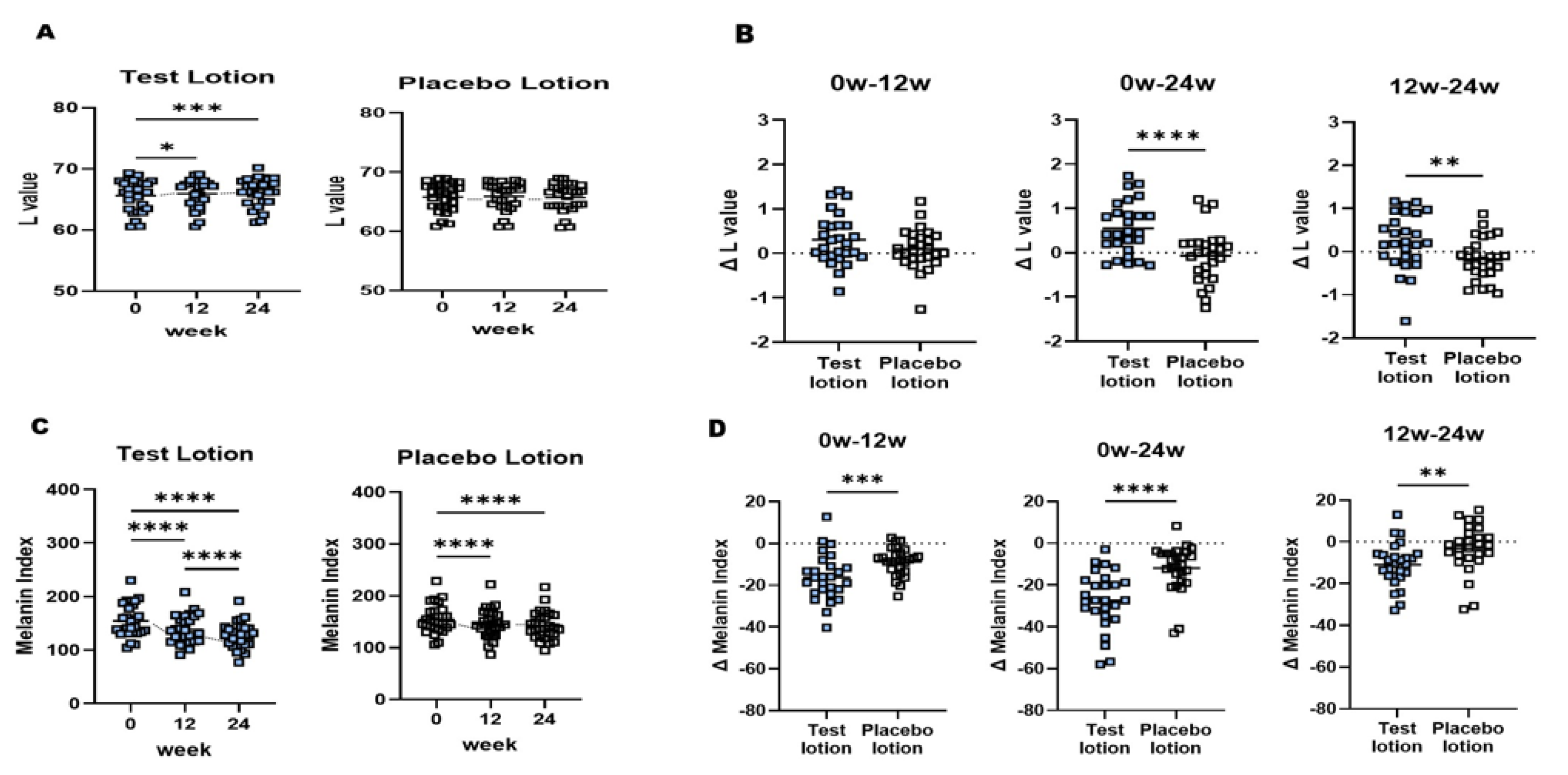
Figure 5.
Correlations between L and MI values in SLs, NLS and SLs+NLS during this clinical study.
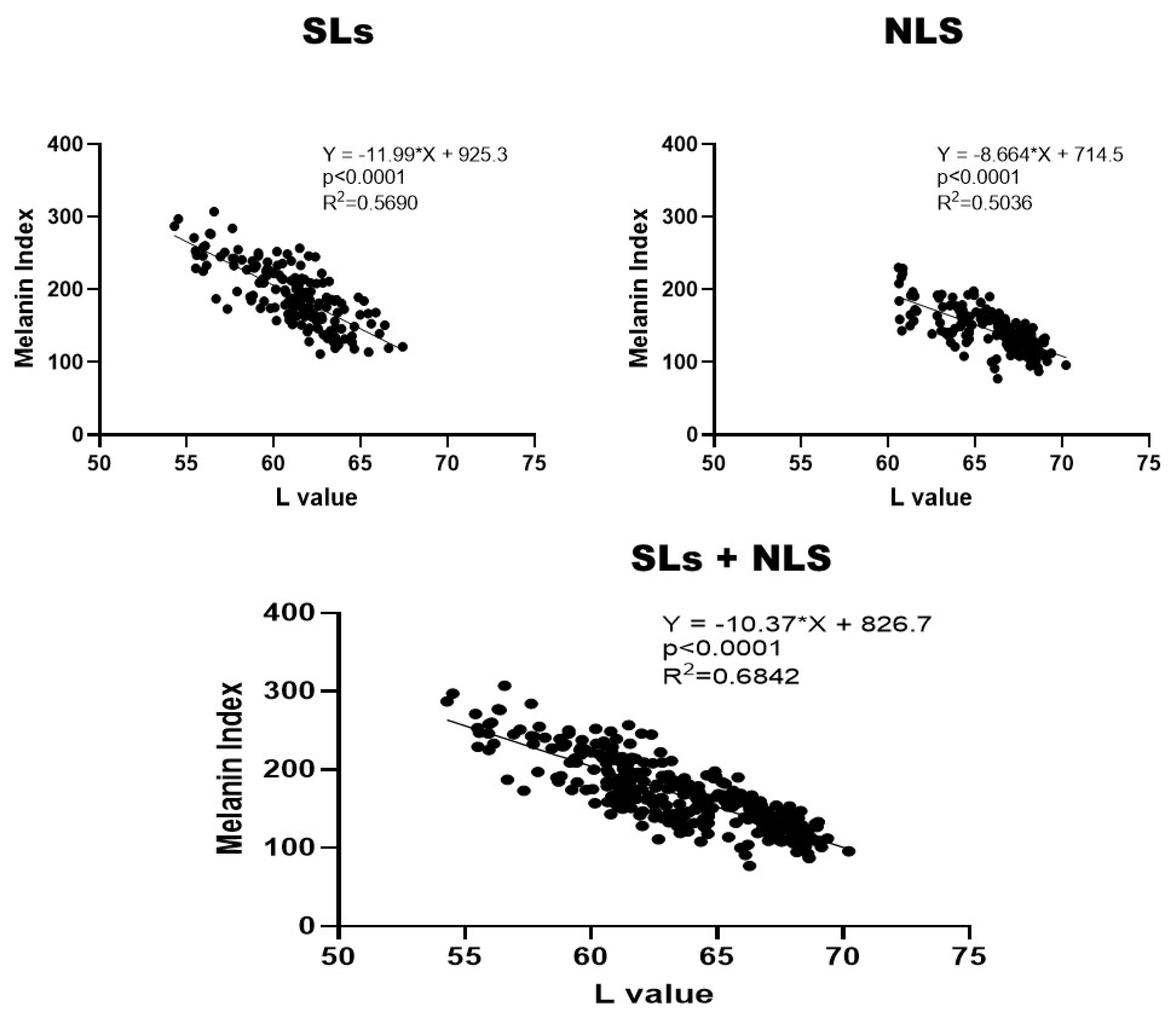
Figure 6.
Correlations between L and MI values in SLs and NLS at 0, 12 and 24 weeks of treatment with the test or the placebo lotion.
Figure 6.
Correlations between L and MI values in SLs and NLS at 0, 12 and 24 weeks of treatment with the test or the placebo lotion.
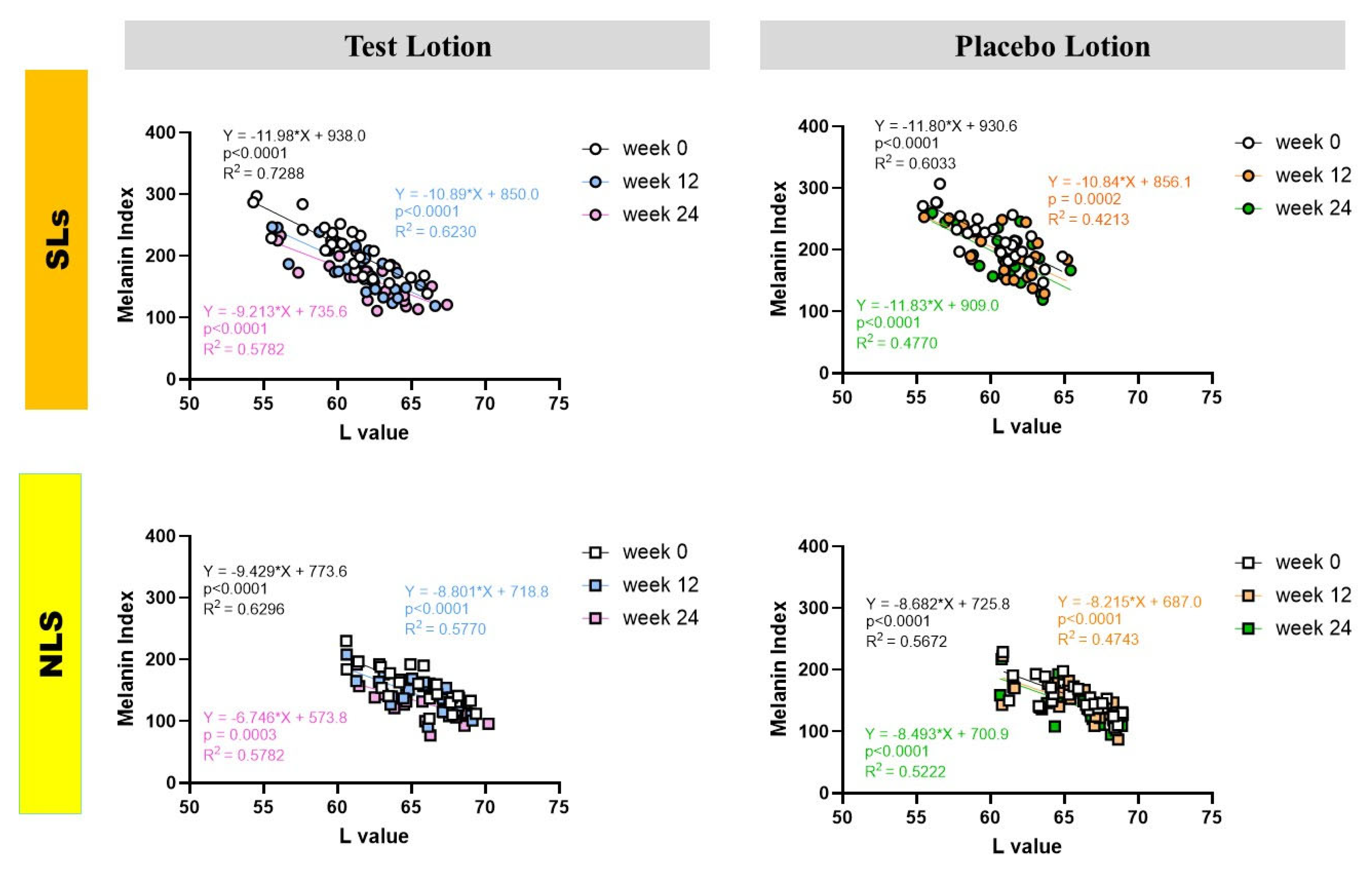
Figure 7.
Clinical effects of the test and placebo lotions on facial skin symptoms of SL patients. A: Dryness, B: Scaling, C: Itchy Sensation, D: Erythema, E: Papules, F: Stinging Sensation. Clinical scoring was performed at 0, 12 and 24 weeks according to the criteria described in the Materials and Methods section. n=27 *: p<0.05, ****: p<0.0001 compared to week 0; all data were analyzed by Friedman test and Dunn’s multiple comparisons test.
Figure 7.
Clinical effects of the test and placebo lotions on facial skin symptoms of SL patients. A: Dryness, B: Scaling, C: Itchy Sensation, D: Erythema, E: Papules, F: Stinging Sensation. Clinical scoring was performed at 0, 12 and 24 weeks according to the criteria described in the Materials and Methods section. n=27 *: p<0.05, ****: p<0.0001 compared to week 0; all data were analyzed by Friedman test and Dunn’s multiple comparisons test.
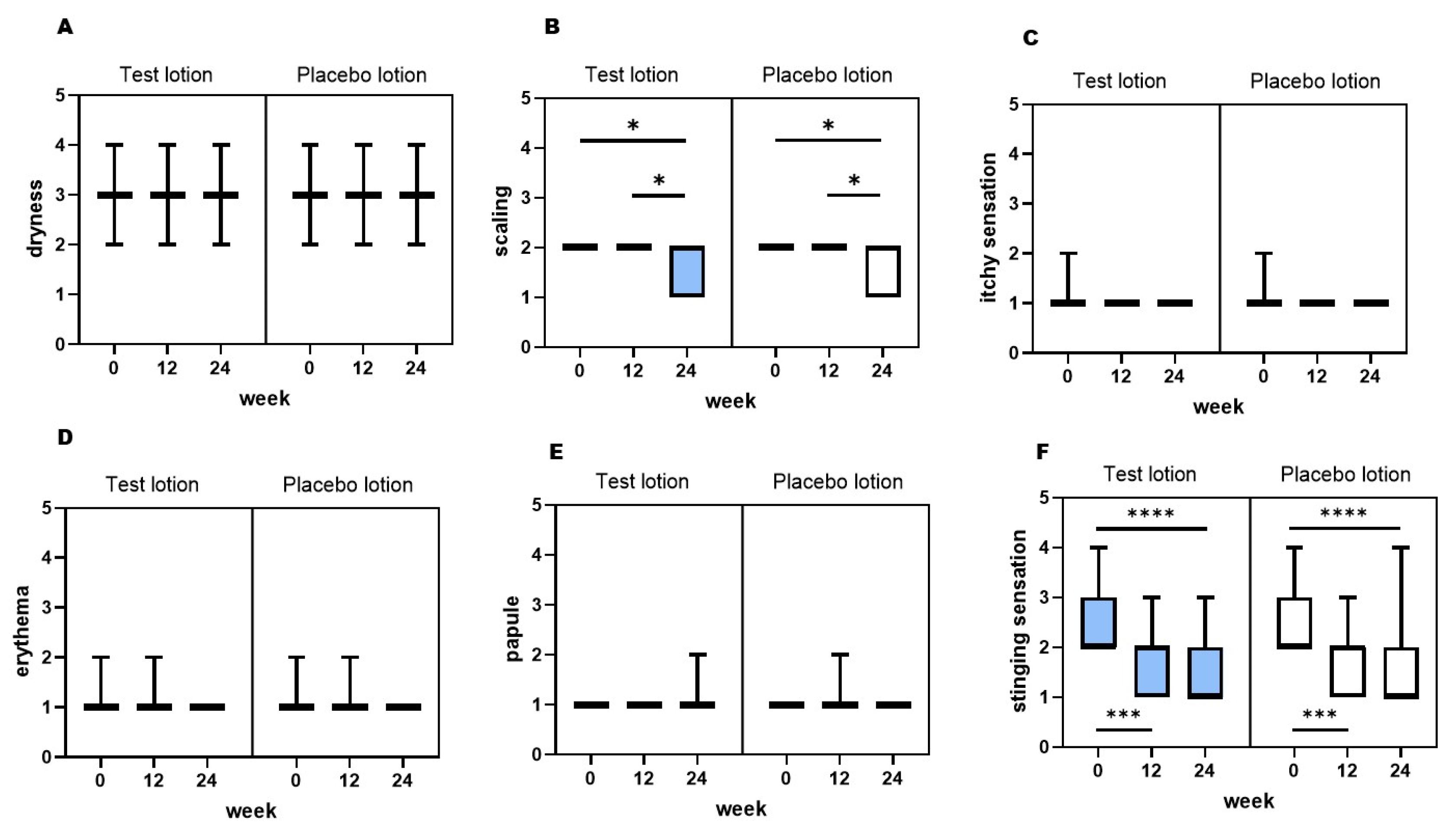
Figure 8.
Clinical effects of the test and placebo lotions on the intensity of skin redness measured as erythema index with a Mexameter MX18. .A: Time course study, N=27, ****: p<0.0001, *: p<0.05 by Tukey’s comparison test, B: Increased erythema index values between 0 and 12, 0 and 24, and 12 and 24 weeks. *: p<0.05 by paired t test.
Figure 8.
Clinical effects of the test and placebo lotions on the intensity of skin redness measured as erythema index with a Mexameter MX18. .A: Time course study, N=27, ****: p<0.0001, *: p<0.05 by Tukey’s comparison test, B: Increased erythema index values between 0 and 12, 0 and 24, and 12 and 24 weeks. *: p<0.05 by paired t test.
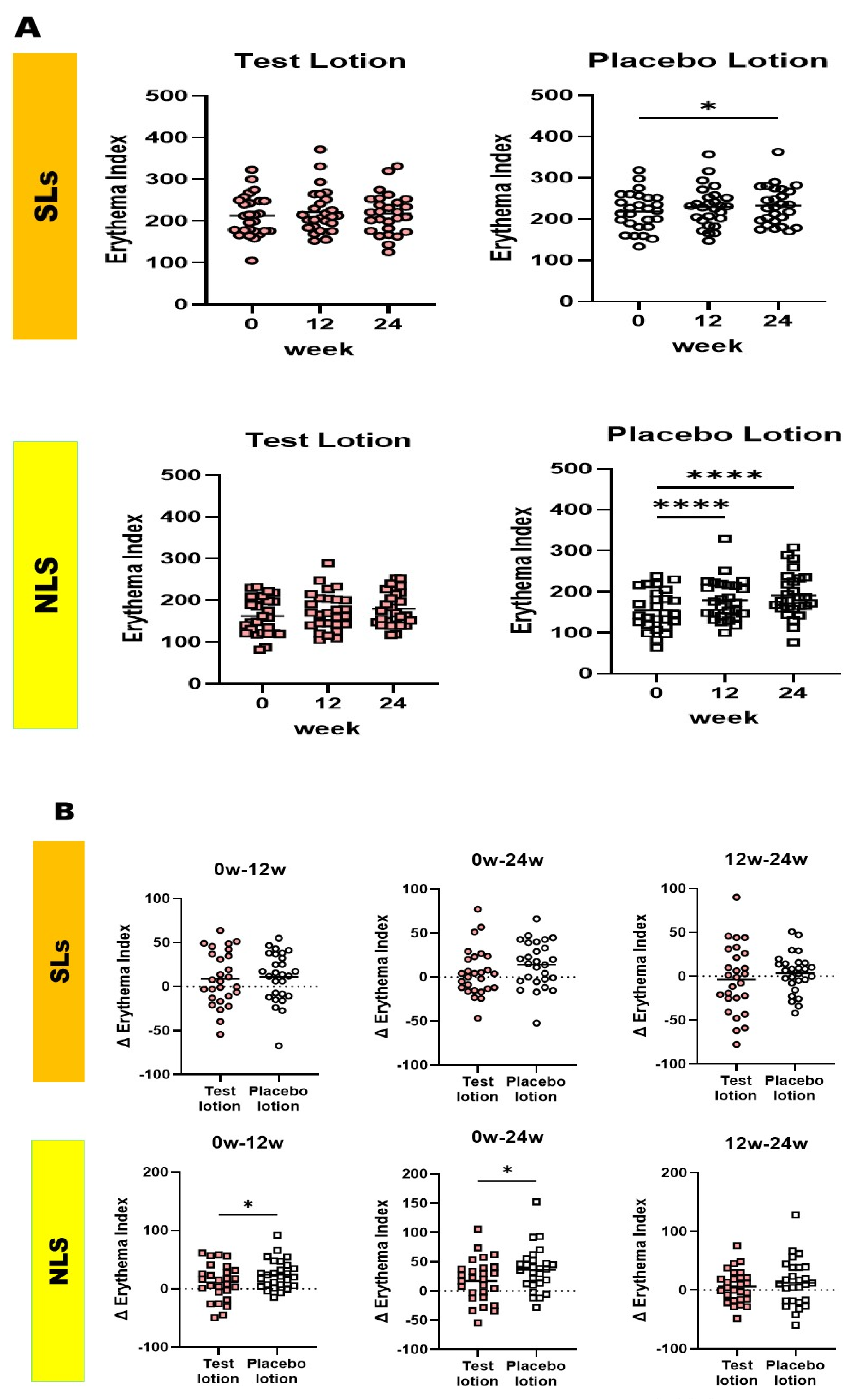
Figure 9.
Chemical structure of AGAC.
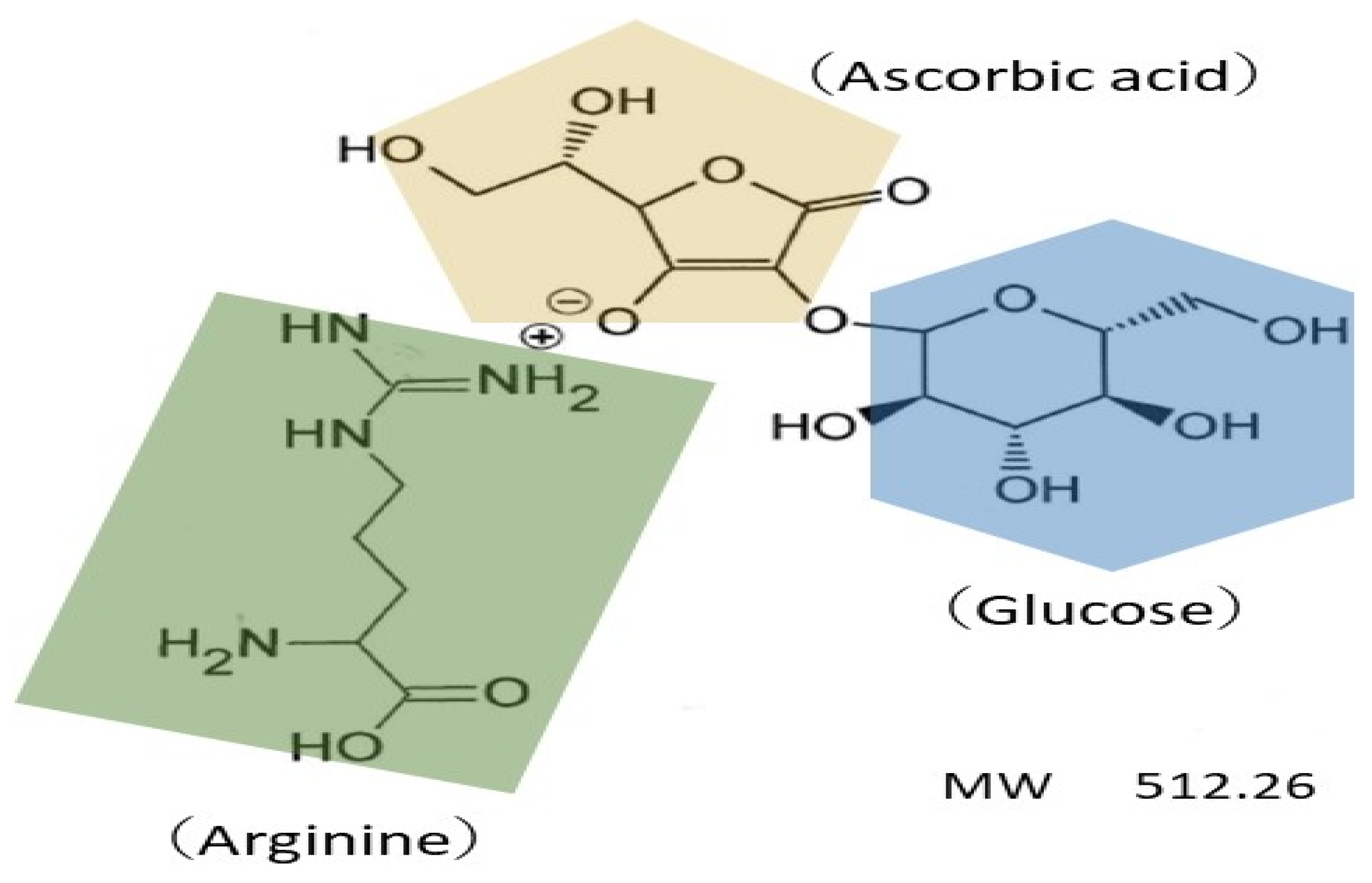

Table 1.
Full ingredients list of the test lotion (containing 28% AGAC) and the placebo lotion (without AGAC).
Table 1.
Full ingredients list of the test lotion (containing 28% AGAC) and the placebo lotion (without AGAC).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



