
Submitted:
08 August 2024
Posted:
08 August 2024
You are already at the latest version
Abstract
Reducing levels of low-density-lipoprotein-cholesterol (LDL-C) below recommended thresholds is a core component of cardiovascular prevention strategies. We hypothesized that the addition of bempedoic acid to patients already on statin-ezetimibe therapy was more effective than titrating the statin dose in reducing LDL-C. The study enrolled 120 patients at high cardiovascular risk, and with LDL-C above 70 mg/dl. They were randomly divided in two groups: bempedoic acid (BA) group, taking bempedoic acid in addition to statin plus ezitimibe, and the statin titration (ST) group including patients who doubled the dose of statin. At 12-weeks, BA group presented a greater significant decrease of LDL-C compared to ST group (-22.9% vs 7.5% p 0.002). Total-cholesterol decreased significantly in the BA group compared to ST (-14.8% vs-4.7% ; p 0.013) No significant between-groups changes in HDL and triglycerides occurred. At 12 weeks the number of patients who reached LDL-C lower than 70 mg/dl was 38 (63%) in the BA group versus 22 (37%) in the ST group (between group p 0.034). In the BA group the LDL lowering effect of bempedoic acid was similar between patients taking atorvastatin and rosuvastatin. No side effects occurred during the follow up period. In conclusion, the addition of Bempedoic acid to statin/ezetimibe combined treatment was more effective than doubling the dose of statin in reducing LDL-C. levels and increased the number of patients reaching the LDL-C goal.
Keywords:
bempedoic acid
; hypercolesterolemia
; primary prevention
; statins
; ezetimibe
1. Introduction
Cardiovascular (CV) diseases are the leading cause of death worldwide, being responsible for about 30% of total mortality. Atherosclerotic cardiovascular disease (ASCVD), through its main clinical manifestations that include ischemic heart disease, ischemic stroke and peripheral artery disease, accounts for most CV deaths [1,2]. The current clinical approach to the prevention of ASCVD includes the promotion of a healthy and physically active lifestyle as well as the administration of drugs for treating hypertension, hypercholesterolemia or diabetes whenever indicated [3]. Lowering blood levels of low-density lipoprotein-cholesterol (LDL-C) remains a primary target for counteracting the onset and progression of ASCVD: it has been estimated that 1 mmol/L reduction in LDL-C is associated with a 20–25% reduction in major adverse cardiovascular events and a 10% reduction in all-cause mortality over 5 years [4]. In the context of primary prevention, European guidelines recommend achieving the goal of LDL-C below 70 mg/dl for subjects considered at high CV risk [3]. The first and main option for lowering LDL-C are statins administered at a maximally tolerated dose since they have the most consistent demonstration of reducing CV risk [5,6,7]. American guidelines, recommend that clinicians prescribe a statin for the primary prevention of CVD for adults aged 40 to 75 years who have 1 or more CVD risk factors and an estimated 10-year CV risk of 10% or greater [8]. However, there are instances in which non-statin lipid-lowering therapies may be needed. These scenarios include patient unwillingness to take statins, intolerability of statin side effects, particularly when these drugs are taken at high doses, and failure to meet LDL-C goals with statin therapy alone. The association of statin with ezetimibe has showed to potentiate the LDL-C lowering effects of statins and partially filling this gap [9,10,11]. However, a significant proportion of patients considered at high risk remain with levels of LDL-C above the recommended threshold despite the combination therapy [12]. There is therefore a need for developing new drugs and pharmacological strategies for these patients. Bempedoic acid, is an inhibitor of the hepatic cholesterol biosynthetic pathway by modulating the activity of ATP citrate lyase, resulting in upregulation of LDL-receptors expression with improved clearance of LDL and reduction in blood LDL-C levels [13]. Several studies have reported significant reductions in LDL-C levels among patients treated with bempedoic acid alone, or as add-on to statin or to ezetimibe therapy [14,15,16]. The administration of bempedoic acid has showed to be capable of improving strong endpoints, by reducing major cardiovascular events in statin-intolerant patients [17]. Despite these encouraging results, the exact role of bempedoic acid in the prevention of ASCVD has not yet been established. In the present study we explored the potential role of bempedoic acid in patients at high-risk who were already on a comprehensive cholesterol-lowering therapy by taking a high-intensity statin and ezetimibe but who needed further therapeutic implementation not having reached the LDL-C goal. We compared the effects of adding bempedoic acid, for 12 weeks, to their background therapy with the alternative strategy of increasing the dose of statins. The primary endpoint was comparative change from baseline to week 12 in LDL-C. Secondary endpoint was comparing the number of patients reaching the target of LDL-C below 70 mg/dl at the end of the study.
2. Materials and Methods
2.1. Population
The study enrolled 120 patients who were attending the San Raffaele IRCCS cardiology outpatient service from June 2022 to January 2024. The following inclusion criteria were adopted: age over 18 years; stable clinical conditions; previous diagnosis of hypercholesterolemia; being already treated with a combined lipid lowering therapy including a high-intensity statin plus ezetimibe for at least three months; LDL-C levels persistently (at least in two previous determinations) above 70 mg/dl; no record of previous side effects to statin treatment; no history of cardiovascular and/or cerebrovascular diseases. The following exclusion criteria were adopted: significant renal failure (GFR < 30 ml/min); concomitant chronic liver diseases; recent diagnosis of cancer; patients who had total fasting triglycerides of 500 mg/dL or greater; patients taking other lipid-lowering drugs as niacin or nutraceutics products. The study complied with the Declaration of Helsinki and was approved by the local Ethics Committee of San Raffaele IRCCS (protocol number 04/2022). All patients gave written informed consent before entering the study. The Systematic COronary Risk Evaluation (SCORE2) algorithm [18] was used to estimate 10-year risk of fatal and non-fatal (myocardial infarction, stroke) cardiovascular diseases. According to the ESC guidelines we considered at high-risk patients of age between 50 and 69 years with an estimated CV risk of 5 to 10%; patients over 70 years with an estimated CV risk of 7.5 to 15%, and patient under 50 years with an estimated CV risk of 2.5 to <7.5% [3]
2.2. Study Design
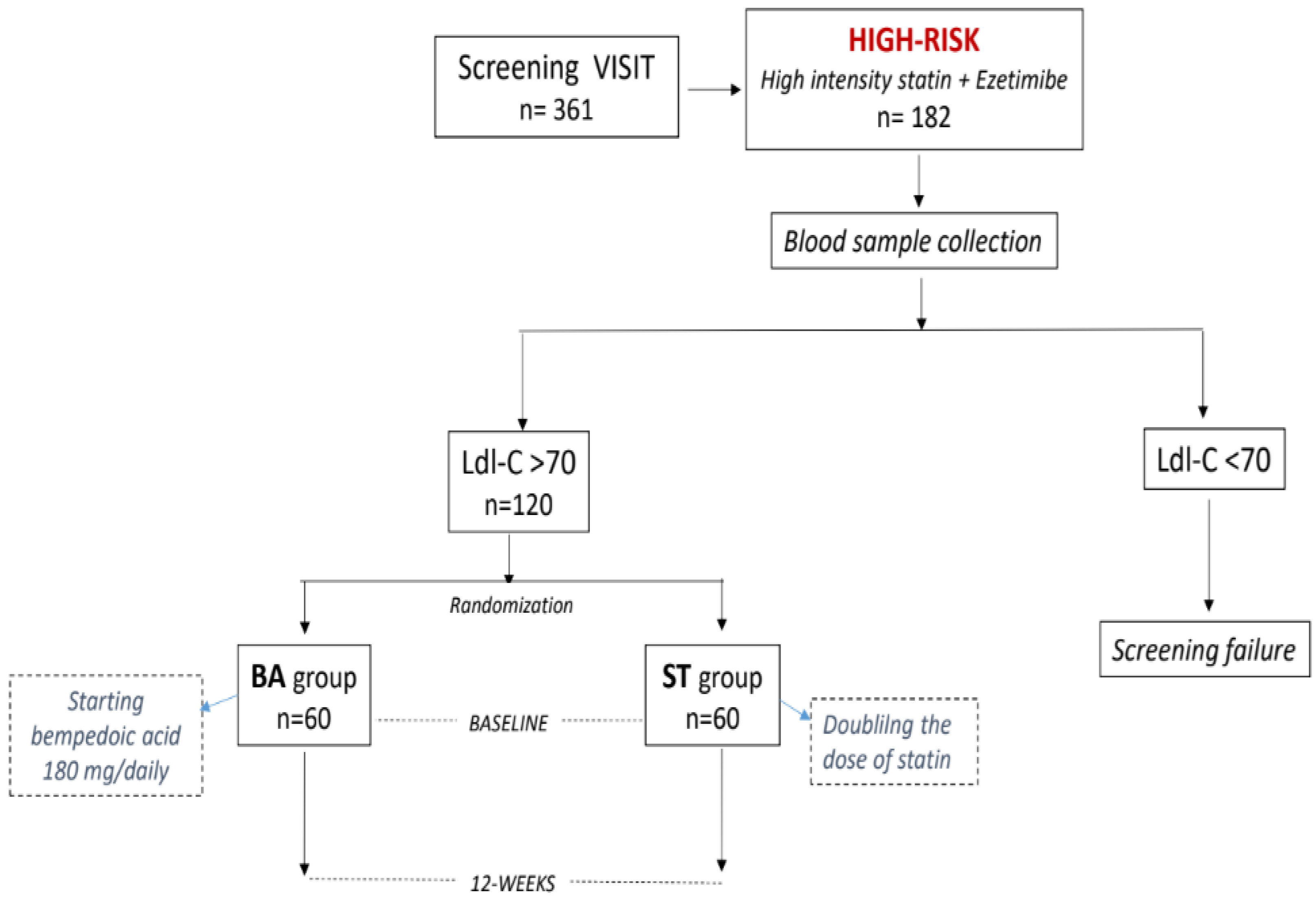
The study flow chart has been summarized in Figure 1. The study was conceived as an open randomized trial with two parallel arms. Patients were randomly assigned on 1:1 basis to one of the following groups: bempedoic acid (BA) or statin titration (ST). Each group was composed by 60 patients. The randomization code was developed by a computer random-number generator to select random permuted blocks. The protocol required that patients of the BA group would start bempedoic acid, 180 mg/daily, and would maintain unchanged their dose of statin through the study. Patients of the ST group would double the dose of their statin; no other changes in lipid lowering drugs were allowed during the entire study. At baseline patients performed a preliminary visit during which inclusion/exclusion criteria were evaluated; medical history previous blood cholesterol levels and anthropometric parameters were collected. Body mass index (BMI) was calculated through the following formula : BMI = kg/m2 where kg is a person’s weight in kilograms and m2 is their height in metres squared. During this visit, suitable patients were invited to participate to the study and those who agreed were then summoned for blood sample collection. Blood collections were performed during the morning between 7:30 and 9:30., within a week from the first visit. Patients were required to fast for 12 hours before the blood draw. The baseline assessment of LDL-C had a confirmatory value: those patients who had LDL-C above 70 mg/dl, were considered screening failure. For patients entering the study, blood collections were then repeated at 12-weksat the same time and in the same ways than at baseline. Clinical laboratory samples for the analysis of basic fasting lipids (total cholesterol (TC), calculated LDL-C, high density lipoprotein cholesterol (HDL-C), non-HDL-C and triglycerides). LDL-cholesterol concentration was calculated using the Friedewald formula: LDL-c (mg/dL) = TC (mg/dL) − HDL-c (mg/dL) − TG (mg/dL)/5 [19]. Patients were not asked to change their dietary habits and their lifestyle organization during the study.
2.3. Statistical Analysis
Since we did not find in the literature previous studies in which bempedoic acid was administered to patients already taking statin plus ezetimibe, we were unable to establish a proper size effect. Therefore, for the present research we based the sample size calculation on the data obtained by using bempedoic acid in the setting of primary prevention [17]. We estimated that a sample size of 55 subjects per group had 80% power to detect a difference in LDL-C decrease of 15 percentage points between the two groups, with a standard deviation of 10% using a two-sided significance level of 0.05. We estimated the drop-out rate to be 10% leading to an overall sample size of 60 patients per group. Data were expressed as median ± standard deviation. The Shapiro–Wilks hypothesis test was used to check the assumption of normality. For each parameter assessed delta (Δ) was defined as the difference between value at 12-weeks versus value at baseline. Between groups comparisons (Δs BA versus Δs ST) were made by using t test for unpaired groups. Categorical variables were compared by using the chi-square test. The level of significance was set at p < 0.05. Data were analysed by using SPSS software (version 20.0 IBM Corp, Amonk, New York, NY, USA).
3. Results
From an original population of 361 patients initially screened we selected 182 patients who resulted being at high CV risk and were taking high at the same time a high intensity statin and ezetimibe. One hundred and twenty out of 182 (66%) were then selected for participating to this study because they had LDL-C levels above the threshold of 70 mg/dl. Sixty-seven out of 120 had at 2 adjunctive CV risk factors beyond hypercholesterolemia. Seventy-five were taking at least two anti-hypertensive drugs. Eighty-six out of 120 (72%) were aged between 50 and 69; only 5 patients (4%) were under 50 years of age. More than 50% of the whole sample had diabetes. Baseline features of the population are reported in Table 1. At baseline the two groups were comparable regarding age, anthropometric data, laboratory parameters and pharmacological therapy. The average dose of atorvastatin taken by patients was 11.3 mg/daily that of rosuvatatin 8.2 mg/daily. Baseline LDL-C for the entire population was 88.7±21.7 mg/dl. All patients completed the study. At 12 weeks the reduction of LDL-C observed in the BA group was significantly greater than in the ST group (between-groups change: -13.8 mg/dl, [ 95%CI= -11.6-15.3] p 0.002). The reduction of TC in the BA group was significantly greater than in the ST (between-groups change: -9.5 mg/dl, [ 95% CI=-6.7-12.3], p 0.013) Figure 2). Changes in HDL and triglycerides were similar between the two groups. (Table 2). At 12 weeks the number of patients who reached LDL-C values lower than 70 mg/dl was 38 (63%) in the BA group versus 22 (37%) in the ST group (between group p 0.034). No changes of uric acid, glucose and creatine-kinase occurred in the two groups. Among patients of the BA group, 33 out of 60 (55%) were taking atorvastatin/ezetimibe and the average dose of atorvastatin was 10.6±2.2 mg. The average dose of rosuvastatin was 7.8±4.7. At 12 weeks, in the BA group the reduction of TC and LDL-C were similar between patients taking atorvastatin and rosuvastatin: TC: atorvastatin vs rosuvastatin = -20.8±3.6 vs-22.8±5; between-groups p 0.133. LDL-C: atorvastatin vs rosuvastatin = -20.3±5.7 vs 20.8±4.1; between-groups p 0.253. The number of patients reaching LDL-C values below the threshold of 70 mg/dl, was also similar among patients taking atorvastatin/ezetimibe and those taking rosuvastatin/ezetimibe: 20 (61%) versus 18 (66%) respectively: between-groups p 0.074.
Figure 1.
Study flow chart
4. Discussion
Lowering LDL-C below recommended thresholds is a key therapeutic target in the prevention of ASCVD [20]. However, many patients do not reach recommended values of LDL-C despite taking one or more lipids lowering drugs [12]. In high-risk patients, starting a statin therapy is strongly recommended but, in cases where statins fail to meet LDL-C goals, it is not clear what is the next best therapeutic option to further improve LDL-C control. In this scenario the new non-statin lipid lowering drugs can represent an alternative strategy for the physicians for optimizing LDL-C beyond statin titration till maximal tolerated dose. In the present study we found that the addition of bempedoic acid to patients already taking a combined therapy of high-intensity statin plus ezetimibe, was more effective than doubling the statin dose, in lowering LDL-C values. In particular, we observed a 22.9% reduction of LDL-C in the BA group versus a 7.5% reduction in the ST group. We believe that this is an original result for two reasons. Firstly, we did not find, in the literature, previous studies comparing bempedoic acid versus statin titration; secondly, to our knowledge, this is the first study in which bempedoic acid has been administered to patients already taking statin plus ezetimibe. The LDL-C lowering effect of bempedoic acid oscillates between 15 and 25% in relation to different clinical scenarios and background therapies. Our result completely agrees with previous studies in which bempedoic acid has been added to ezetimibe or used in monotherapy in patients with hypercholesterolemia and statin intolerance [21,22]. Conversely the LDL-C lowering effect that we observed in the BA group was greater when compared to the 15-18% reductions described in other studies performed in patients with already established ASCVD, or with multiple CV risk factors, and in which bempedoic acid has been added to statin therapy [23,24]. A possible explanation of the differences between our results and these two latter studies is that the doses of statins they used were higher than in our study. This is because in those studies bempedoic acid or placebo were added to maximally tolerated doses of statins; on the contrary the statin doses taken by our patients were low and still not optimized. Besides, other differences should be underlined: in the study of Goldberg et al. [24] for example, only a small proportion of patients were taking ezetimibe in association to statins and some patients were taking proprotein convertase subtilisin/kexin type 9 inhibitors. Regarding the 7.5% reduction of LDL-C that we observed in the ST group by doubling the dose of statin, this result appears to be also in line with previous literature: despite different statins have varying abilities to lower LDL-C, it has been estimated that, on average, doubling the dose of a statin results in an approximate 6% further decrease in LDL-C levels [25]. Interestingly, in this study, the greater reduction in LDL-C observed in the BA group resulted in a significantly higher percentage of patients of this group reaching the therapeutic target at 12 weeks in comparison to the ST group. This result suggests that starting bempedoic acid rather than titrating the statin dose would allow a quicker achievement of optimal values of LDL-C. Further studies are needed to clarify whether the observed differences persist over time and whether the triple strategy is associated with prognostic advantages in comparison to statin titration. Potential prognostic benefits of bempedoic acid in primary prevention have been suggested by a subgroup analysis of CLEAR Outcomes, in which a relative risk reduction of 39% and 27% for cardiovascular and all-cause mortality, respectively has been demonstrated [17]. Moreover, the prognostic impact of a triple therapy including of bempedoic acid, ezetimibe and maximally tolerated statins, have been recently explored: McQueen et al. [26], by using a simulation model, calculated that adding bempedoic acid plus ezetimibe in patients already on maximally tolerated statins and not at their LDL-C goal, would result in more major cardiovascular events avoided compared with the addition of ezetimibe alone. Overall, our results suggest that a “triple therapy” strategy, including bempedopic acid, statin and ezetimibe, could be the most effective for magnifying the LDL-C lowering effects in high-risk patients. A similar evidence emerges from the study of Ballantyne et al. [27], also conducted in a high risk population. In that study the addition of bempedoic acid to statin led to a 17.2% reduction of LDL-C, while the addition of bempedoic acid plus ezetimibe to statin obtained a 34% LDL-C reduction. In our study the addition of bempedoic acid was well tolerated when added to background of statin plus ezetimibe. These safety and tolerability findings were consistent with expectations based on previous bempedoic acid clinical trials [28,29]. However, this result should be taken with caution since the follow up period of the present study was very short and data regarding side effects, in the literature, are not univocal. For example, Ray et al. [23] observed that the incidence of adverse events leading to discontinuation of the drug was higher in the bempedoic acid group than in the placebo group. Further research including larger sample size, as well as the inclusion of a placebo group, are needed in order to confirm and expand our results. Limitations. The present study lacks a control group and this clearly weakens the robustness of our results. In this study we enrolled patients at high CV taking low doses of statins and ezetimibe; therefore, we cannot extend our results to patients at very high-risk taking high doses statins or to patient taking statins in combination with lipid lowering drugs other than ezetimibe. Despite this study was open to patients at high CV risk under 50 years, we encountered many difficulties in finding patients under 50 years who met the inclusion criterion of taking the combined treatment statin plus ezetimibe. Therefore. this group of age was underrepresented in this study and or results cannot be generalized to this group.
5. Conclusions
Our data suggest that the addition of bempedoic acid to statin-ezetimibe could be a reliable and effective strategy for reaching LDL-C target in high-risk patients. Further studies are needed to confirm our results and to clarify clinical implications of this new therapeutic strategy.
Author Contributions
G.M., M.V., and G.C., contributed to the conceptualization of the review; G.C, L.C., D.M.G. and P.S. prepared the initial draft after acquisition, analysis, and interpretation of the literature; G.R., M.P., and F.I. substantively revised it. All authors have read and agreed to the submitted version of the manuscript.
Funding
This work was supported by funding of the Italian Ministry of Health [Ricerca corrente]
Institutional Review Board Statement
In The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Ethics Committee of San Raffaele IRCCS of Rome (protocol code 04/2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been also obtained from the patients to publish this paper
Data Availability Statement
The data presented in this study are available on request from the corresponding authors.
Conflicts of Interest
The authors declare no conflicts of interest.ù.
References
- Herrington W, Lacey B, Sherliker P, Armitage J, Lewington S. Epidemiology of Atherosclerosis and the Potential to Reduce the Global Burden of Atherothrombotic Disease. Circ Res. 2016 Feb 19;118(4):535-46. [CrossRef]
- Parini P., Frikke-Schmidt R., Tselepis A.D., Moulin P., von Eckardstein A., Binder C.J., Catapano A.L., Ray K.K., Tokgözoğlu L. Taking action: European Atherosclerosis Society targets the United Nations Sustainable Development Goals 2030 agenda to fight atherosclerotic cardiovascular disease in Europe. Atherosclerosis. 2021;322:77–81. [CrossRef]
- Visseren FLJ, Mach F, Smulders YM, Carballo D, Koskinas KC, Bäck M, Benetos A, Biffi A, Boavida JM, Capodanno D, Cosyns B, Crawford C, Davos CH, Desormais I, Di Angelantonio E, Franco OH, Halvorsen S, Hobbs FDR, Hollander M, Jankowska EA, Michal M, Sacco S, Sattar N, Tokgozoglu L, Tonstad S, Tsioufis KP, van Dis I, van Gelder IC, Wanner C, Williams B; ESC National Cardiac Societies; ESC Scientific Document Group. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. 2021 Sep 7;42(34):3227-3337. [CrossRef]
- Baigent C. Cholesterol treatment trialists’ (CTT) collaborators: efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 2005; 366: 1267–1278. [CrossRef]
- LaRosa, JC, Grundy, SM, Waters, DD, et al. Intensive lipid lowering with atorvastatin in patients with stable coronary disease. N Engl J Med 2005;352:1425-1435. [CrossRef]
- Pedersen TR, Faergeman O, Kastelein JJ, Olsson AG, Tikkanen MJ, Holme I, Larsen ML, Bendiksen FS, Lindahl C, Szarek M, Tsai J; Incremental Decrease in End Points Through Aggressive Lipid Lowering (IDEAL) Study Group. High-dose atorvastatin vs usual-dose simvastatin for secondary prevention after myocardial infarction: the IDEAL study: a randomized controlled trial. JAMA. 2005 Nov 16;294(19):2437-45. [CrossRef]
- Ridker PM, Danielson E, Fonseca FA, Genest J, Gotto AM Jr, Kastelein JJ, Koenig W, Libby P, Lorenzatti AJ, MacFadyen JG, Nordestgaard BG, Shepherd J, Willerson JT, Glynn RJ; JUPITER Study Group. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med. 2008 Nov 20;359(21):2195-207. [CrossRef]
- US Preventive Services Task Force; Mangione CM, Barry MJ, Nicholson WK, Cabana M, Chelmow D, Coker TR, Davis EM, Donahue KE, Jaén CR, Kubik M, Li L, Ogedegbe G, Pbert L, Ruiz JM, Stevermer J, Wong JB. Statin Use for the Primary Prevention of Cardiovascular Disease in Adults: US Preventive Services Task Force Recommendation Statement. JAMA. 2022 Aug 23;328(8):746-753. [CrossRef]
- Cannon C.P., Blazing M.A., Giugliano R.P., McCagg A., White J.A., Théroux P., Darius H., Lewis B.S., Ophuis T.O., Jukema J.W., et al. Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes. N. Engl. J. Med. 2015;372:2387–2397. [CrossRef]
- Ezhov MV, Sergienko IV, Kryzhanovskiy SM, Manko KS, Timoshina EV. Comparative Efficacy and Safety of Statin Monotherapy and Statin plus Ezetimibe Combination in a Real-World Setting. Diseases. 2023 Nov 13;11(4):168. [CrossRef]
- Lee J, Lee SH, Kim H, Lee SH, Cho JH, Lee H, Yim HW, Yoon KH, Kim HS, Kim JH. Low-density lipoprotein cholesterol reduction and target achievement after switching from statin monotherapy to statin/ezetimibe combination therapy: Real-world evidence. J Clin Pharm Ther. 2021 Feb;46(1):134-142. [CrossRef]
- Daskalopoulou SS, Mikhailidis DP. Reaching goal in hypercholesterolaemia: dual inhibition of cholesterol synthesis and absorption with simvastatin plus ezetimibe. Curr Med Res Opin. 2006 Mar;22(3):511-28. [CrossRef]
- Biolo G, Vinci P, Mangogna A, Landolfo M, Schincariol P, Fiotti N, Mearelli F, Di Girolamo FG. Mechanism of action and therapeutic use of bempedoic acid in atherosclerosis and metabolic syndrome. Front Cardiovasc Med. 2022 Oct 28;9:1028355. [CrossRef]
- Thompson PD, Rubino J, Janik MJ, et al. Use of ETC-1002 to treat hypercholesterolemia in patients with statin intolerance. J ClinLipidol 2015; 9:295–304.
- Rubino J, MacDougall DE, Sterling LR, Hanselman JC, Nicholls SJ. Combination of bempedoic acid, ezetimibe, and atorvastatin in patients with hypercholesterolemia: a randomized clinical trial. Atherosclerosis. (2021) 320:122–8. 10.1016/j.atherosclerosis.2020.12.023.
- Lalwani ND, Hanselman JC, MacDougall DE, Sterling LR, Cramer CT. Complementary low-density lipoprotein-cholesterol lowering and pharmacokinetics of adding bempedoic acid (ETC-1002) to high-dose atorvastatin background therapy in hypercholesterolemic patients: a randomized placebo-controlled trial. J ClinLipidol. (2019) 13:568–79. 10.1016/j.jacl.2019.05.003.
- Nissen SE, Menon V, Nicholls SJ, Brennan D, Laffin L, Ridker P, Ray KK, Mason D, Kastelein JJP, Cho L, Libby P, Li N, Foody J, Louie MJ, Lincoff AM. Bempedoic Acid for Primary Prevention of Cardiovascular Events in Statin-Intolerant Patients. JAMA. 2023 Jul 11;330(2):131-140. [CrossRef]
- SCORE2 working group and ESC Cardiovascular risk collaboration. SCORE2 risk prediction algorithms: new models to estimate 10-year risk of cardiovascular disease in Europe. EurHeart J. 2021 Jul 1;42(25):2439-2454. [CrossRef]
- Tremblay AJ, Morrissette H, Gagné J-M, Bergeron J, Gagné C, Couture P. Validation of the Friedewald formula for the determination of low-density lipoprotein cholesterol compared with β-quantification in a large population. Clinical Biochemistry. 2004;37(9):785–790.
- Mhaimeed O, Burney ZA, Schott SL, Kohli P, Marvel FA, Martin SS. The importance of LDL-C lowering in atherosclerotic cardiovascular disease prevention: Lower for longer is better. Am J Prev Cardiol. 2024 Mar 18;18:100649. [CrossRef]
- Laufs U, Banach M, Mancini GBJ, Gaudet D, Bloedon LT, Sterling LR, Kelly S, Stroes ESG. Efficacy and safety of bempedoic acid in patients with hypercholesterolemia and statin intolerance. J Am Heart Assoc. 2019 Apr 2;8(7):e011662. [CrossRef]
- Ballantyne CM, Banach M, Mancini GBJ, Lepor NE, Hanselman JC, Zhao X, Leiter LA. Efficacy and safety of bempedoic acid added to ezetimibe in statin-intolerant patients with hypercholesterolemia: A randomized, placebo-controlled study. Atherosclerosis. 2018 Oct;277:195-203. [CrossRef]
- Ray KK, Bays HE, Catapano AL, Lalwani ND, Bloedon LT, Sterling LR, Robinson PL, Ballantyne CM; CLEAR Harmony Trial. Safety and Efficacy of Bempedoic Acid to Reduce LDL Cholesterol. N Engl J Med. 2019 Mar 14;380(11):1022-1032. [CrossRef]
- Goldberg AC, Leiter LA, Stroes ESG, Baum SJ, Hanselman JC, Bloedon LT, Lalwani ND, Patel PM, Zhao X, Duell PB. Effect of Bempedoic Acid vs Placebo Added to Maximally Tolerated Statins on Low-Density Lipoprotein Cholesterol in Patients at High Risk for Cardiovascular Disease: The CLEAR Wisdom Randomized Clinical Trial. JAMA. 2019 Nov 12;322(18):1780-1788. [CrossRef]
- Jones PH, Davidson MH, Stein EA, Bays HE, McKenney JM, Miller E, Cain VA, Blasetto JW; STELLAR Study Group. Comparison of the efficacy and safety of rosuvastatin versus atorvastatin, simvastatin, and pravastatin across doses (STELLAR* Trial). Am J Cardiol. 2003 Jul 15;92(2):152-60. [CrossRef]
- McQueen RB, Baum SJ, Louie MJ, Sasiela WJ, Bilitou A, Shah H, Nash B, Gillard KK, Ray KK. Potential Cardiovascular Events Avoided with Bempedoic Acid Plus Ezetimibe Fixed-Dose Combination Compared with Ezetimibe Alone in Patients with Atherosclerotic Cardiovascular Disease Taking Maximally Tolerated Statins. Am J Cardiovasc Drugs. 2023 Jan;23(1):67-76. [CrossRef]
- Ballantyne CM, Laufs U, Ray KK, Leiter LA, Bays HE, Goldberg AC, et al. Bempedoic acid plus ezetimibe fixed-dose combination in patients with hypercholesterolemia and high CVD risk treated with maximally tolerated statin therapy. Eur J PrevCardiol. 2020;27:593–603. [CrossRef]
- Thompson PD, MacDougall DE, Newton RS, et al. Treatment with ETC-1002 alone and in combination with ezetimibe lowers LDL cholesterol in hypercholesterolemic patients with or without statin intolerance. J ClinLipidol 2016; 10:556–567.
- Bays HE, Banach M, Catapano AL, Duell PB, Gotto AM Jr, Laufs U, Leiter LA, Mancini GBJ, Ray KK, Bloedon LT, Sasiela WJ, Ye Z, Ballantyne CM. Bempedoic acid safety analysis: Pooled data from four phase 3 clinical trials. J ClinLipidol. 2020 Sep-Oct;14(5):649-659.e6. [CrossRef]
Figure 2.
Percentage changes (12-weeks versus baseline) on lipids in the BA group (dark bars) and ST group (light bars) .
Figure 2.
Percentage changes (12-weeks versus baseline) on lipids in the BA group (dark bars) and ST group (light bars) .
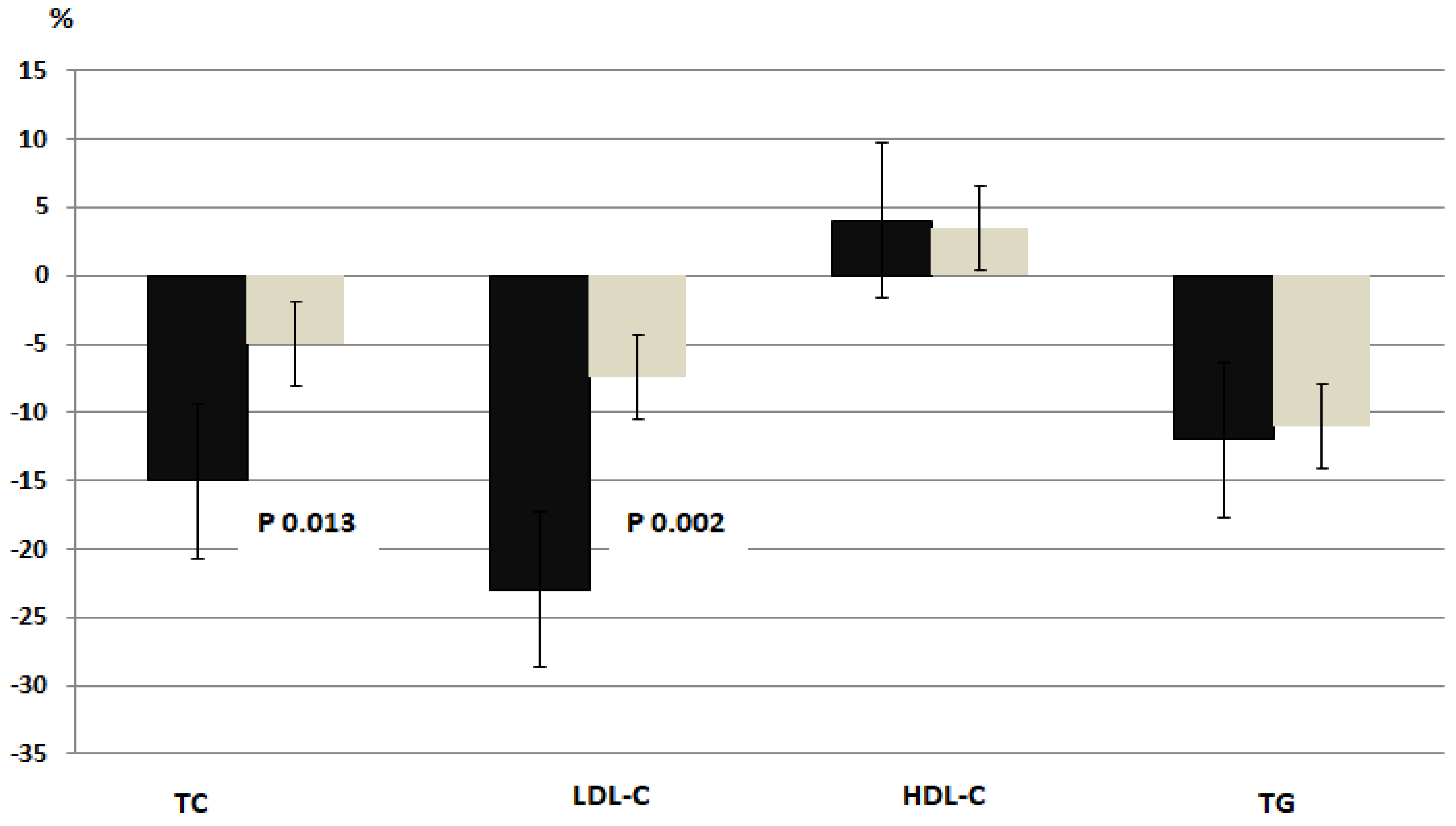

Table 1.
Baseline features of recruited patients according to the two groups allocation.
| BA group (n=60) | ST group (n=60) | |
| Clinical profile | ||
| Age, y | 61.7.4±11.2 | 61.9±7.4 |
| BMI, kg/m2 | 27.7±6.4 | 28.0±7.2 |
| Males, n (%) | 32 (53) | 34 (56) |
| Hypertension, n (%) | 39 (65) | 41 (68) |
| Diabetes, n (%) | 33 (55) | 32 (53) |
| Active smokers, n(%) | 18 (30) | 17 (28) |
| Laboratory | ||
| eGFR, ml/min per 1.73 m2 | 89.3±11.6 | 79.8±14.1 |
| ALT, U/l | 30.7±5.3 | 31.0±7.9 |
| AST, U/l | 30.2±8.2 | 29.8±8.6 |
| Creatinine, mg/dl | 0.91±0.7 | 0.87±0.3 |
| Uric acid, mg/dl | 6.2±1.5 | 5.8±2.1 |
| CK, U/l | 68.3±13.4 | 75.2±18.1 |
| Glucose, mg/dl | 101.2±26.7 | 97.8±21.84 |
| Treatments | ||
| Atorvastatin ,n (%) | 33 (55) | 31 (54) |
| Betablockers, n (%) | 14 (93.3) | 14 (93.3) |
| ACE-Is /ARBs, n (%) | 23 (38) | 21 (35) |
| CCAs, n (%) | 16 (27) | 19 (32) |
| Acetylsalicylic acid, n (%) | 7 (12) | 9 (15) |
| Clopidogrel, n (%) | 3 (5) | 4 (6) |
| Metformin, n (%) | 22 (37) | 23 (38) |
| SGLT2-Is, n (%) | 18 (30) | 17 (28) |
| Sitagliptin, n (%) | 6 (10) | 8 (13) |
BMI= body mass index; AST= aspartate aminotransferase; ALT= alenineaminotransferase, CK = creatine Kinase; ACE-Is= angiotensin converting enzyme inhibitors; ARBs= angiotensin receptor blockers; MRAs= mineralcorticoid receptor antagonists; CCAs= Calcium-channel antagonists; SGLT2-I= sodium-glucose transport protein 2 (SGLT2) inhibitors.
Table 2.
Changes on lipids in the two study groups (12-weeeks versus baseline). .
| BA group (n=60) | Δ | ST group (n=60) | Δ | |||
| Baseline | 12 weeks | Baseline | 12 weeks | |||
| Total-Chol, mg/dl | 148.8±44.5 | 126.9±52.1 | -21.9±6.2* | 146.0±48.6 | 139.5±55.2 | -6.5±2.4 |
| LDL-Chol, mg/dl | 89.9±7.9 | 69.4±6.5* | - 20.5±7.3* | 87.5±8.8 | 80.8±8.5 | -6.7±2.5 |
| HDL-Chol, mg/dl | 37.2±4.6 | 39.0±3.8 | 1.8±0.6 | 36.9±4.2 | 38.3±5.7 | 1.4±0.7 |
| TG, mg/dl | 108.4±32.4 | 95.9±39.1 | -12.5±3.7 | 109.2±33.7 | 99.1±26.4 | -10.2±3.1 |
LDL-C= low density lipoprotein cholesterol; HDL = high density lipoprotein cholesterol; TG= triglycerides. *Between-groups p <0.05
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



