
Submitted:
28 July 2024
Posted:
09 August 2024
You are already at the latest version
Abstract
Background: Vaccine hesitancy, identified by the World Health Organization as a top ten global health threat, presents a significant barrier to public health efforts, exacerbated by the politicization of vaccines during the COVID-19 pandemic.1 Motivational interviewing (MI) has been shown to be effective in addressing difficult topics, including vaccine hesitancy, emphasizing the need for its integration into medical education.2 Objective: This study explores ways to enhance the medical student curriculum on MI, specifically targeting the management of conversations with vaccine-hesitant patients. These authors seek to evaluate the impact of different teaching approaches on the efficacy of MI training within clinical education. Methods: A blinded study design was implemented, comparing two groups of medical students trained using distinct MI teaching methods: Learning Through Experience (LTE) and Traditional Teaching (TT). The LTE group engaged with a Vaccine Hesitant Standardized Patient (VHSP) before and after an instructional module on the use of MI to combat vaccine hesitancy. In contrast, the TT group interacted with a control Standardized Patient (SP) before the same module and then with the VHSP. Any medical student above the age of 18 was eligible for this study. All students in a vaccine elective at RVUCOM on the Colorado and Utah campuses were enrolled, as well as student volunteers. We excluded any students who opted out of the study. The effectiveness of each method was assessed through confidence and performance scores derived from participant self-evaluations and standardized patient feedback, respectively. Results: Participants in the TT group demonstrated superior mastery of MI skills as taught in the didactic session based on statistically significant findings across more tested variables. The LTE group exhibited enhanced ability in practical applications with standardized patients based on statistically significant findings. Both groups showed increased confidence in MI techniques, with the LTE group reporting greater confidence in vaccine knowledge and MI abilities. That said, the LTE method did not drastically outperform the TT approach in overall efficacy. Conclusions: The study indicates that while traditional TT training effectively imparts MI skills, the LTE approach may offer benefits in applying these skills in clinical scenarios. These findings suggest the potential for integrating multiple teaching methods into the medical curriculum to better prepare students for engaging with vaccine-hesitant patients. Further research is needed to explore the long-term effects of these teaching strategies on student performance and patient outcomes.
Keywords:
Vaccine hesitancy
; motivational interviewing
; medical education
; teaching methods
; clinical communication
Introduction
In the contemporary healthcare landscape, Vaccine Hesitancy (VH) has emerged as a critical challenge, undermining public health achievements and the global fight against infectious diseases. This phenomenon, characterized by a reluctance or refusal to vaccinate despite the availability of vaccines, affects millions globally, with the World Health Organization (WHO) identifying VH as one of the top ten threats to global health [1]. The resurgence of preventable diseases, evidenced by recent measles and whooping cough outbreaks, underscores the urgency of addressing VH [3]. In the past, there has been a period of vaccine enthusiasm followed by declination as herd immunity increases [4]. However, during the peak of the COVID-19 pandemic, nurses reported that less than two- thirds of individuals reported intent to receive the vaccine when it was released [5]. Such trends not only pose a direct threat to individual health but also jeopardize herd immunity, facilitating the spread of infections among unvaccinated and vulnerable populations.
Vaccine hesitancy is a complex topic influenced by many factors. Misinformation, distrust in healthcare systems, and cultural beliefs all contribute, necessitating a nuanced, empathetic approach to vaccine promotion [4]. While hesitancy is not novel, our approach to addressing it is. Motivational Interviewing (MI) is a patient-centered, dialogue-based method of enhancing intrinsic motivation to change attitudes by exploring and resolving ambivalence and resistance to change with empathy, reinforcing the patient’s ability to overcome their own barriers to change [6,7]. Although originally developed for substance use management in talk therapy, MI was quickly determined to be widely applicable across many fields [8]. The versatility of this method is demonstrated by the OARS acronym—Open questioning, Affirming, Reflective Listening, and Summarizing [6]. By fostering an
environment of empathy and mutual respect, this nuanced approach facilitates a collaborative partnership between care providers and patients, prioritizing patient autonomy and supportive guidance over directive interactions [9]. By exploring a patient’s desire for change with compassion, personal motivation is strengthened, increasing the likelihood that the patient will follow through [6]. Central to MI’s efficacy is its ability to bridge the gap between a patient’s current state and their preferred behavioral outcomes, presenting a promising strategy for addressing a complex topic such as VH [2,9].
MI offers a structured yet flexible methodology to navigate the complexities of vaccine deliberations effectively [2]. By strategically exploring a patient’s knowledge and concerns, MI positions itself as an indispensable tool within healthcare settings, demonstrating substantial success in mitigating vaccine hesitancy and enhancing patient engagement in health decisions. Additionally, MI can be accomplished briefly, making it ideal for healthcare settings [9]. Although this intervention takes little time away from a patient visit, it requires a well-trained practitioner to be most successful.
Teaching MI to emerging healthcare professionals presents a strategic approach to address VH by capitalizing on a critical period of skill acquisition [10]. Medical education provides an ideal setting for teaching MI techniques, as it aligns with the foundational goal of nurturing empathetic, patient-centered practitioners capable of navigating complex patient interactions [11]. By integrating MI into the curriculum, future healthcare providers would be equipped with a valuable communication toolkit designed to engage vaccine- hesitant individuals effectively. This educational strategy ensures that the next generation of medical professionals is adept at fostering trust and openness, which is essential for addressing VH and promoting public health initiatives [6]. Through hands-on training, simulations, and reflective practice, medical students can learn to apply MI principles in real-world contexts, preparing them to contribute positively to patient outcomes and vaccine uptake from the outset of their careers [10].
Incorporating MI for VH into the curricula of medical schools presents a multifaceted challenge, emblematic of the broader difficulties in adapting medical education to address emergent public health crises [12]. First, the nuanced skills required for effective MI, such as empathy, active listening, and fostering a nonjudgmental dialogue, are inherently difficult to teach using only traditional lecture-based formats [12]. These skills necessitate experiential learning opportunities, which can be resource-intensive to provide on a scale required for medical students. Furthermore, medical schools are already grappling with overcrowded curricula, making integrating comprehensive MI training a logistical puzzle [12]. Adding to the difficulty is the need for faculty development; educators must be proficient in MI to teach it effectively, requiring additional training and time that may be challenging to organize. Lastly, there is a pressing need for educational content to be evidence-based and dynamically updated to reflect the latest research and best practices, necessitating ongoing curriculum evaluation and revision [12]. While necessary to equip future physicians with the tools needed to combat VH effectively, an educational paradigm shift such as this one requires significant investment, innovation, and commitment at all levels of medical education.
In response to the challenge of vaccine hesitancy as well as need for enhanced communication skills among medical professionals, this study explores the efficacy of various instructional methods in teaching motivational interviewing (MI) within the medical curriculum. Medical education could be enriched by integrating more effective MI training and assessing how varied teaching approaches can influence the quality and effectiveness of future clinicians’ interactions with vaccine hesitant patients. These authors aim to discern which pedagogical methods most significantly impact students’ learning outcomes, confidence, and practical skills in MI to set a foundation for improving communication strategies that will enhance patient care and the success of public health initiatives.
Methods
Study Design and Participants
This blinded study was designed to evaluate the effectiveness of two instructional methods— Learning Through Experience (LTE) and Traditional Teaching (TT)—in teaching medical students motivational interviewing (MI) techniques in the context of vaccine hesitancy. Participants were first and second-year osteopathic medical students at Rocky Vista University College of Osteopathic Medicine, randomly assigned to one of the two groups.
Participants were first and second-year osteopathic medical students at Rocky Vista University College of Osteopathic Medicine (RVUCOM) on the Colorado and Utah campuses, randomly assigned to one of the two groups.
Inclusion and Exclusion Criteria
To design our project, we performed a literature review of around using key terms such as Motivational Interviewing (N = 13), Vaccine Hesitancy (N = 9), Education (N = 4), Vaccine Acceptance (N = 2), Vaccine Confidence (N = 2), COVID-19 (N = 6), Communication (N = 7) and Health Knowledge, Attitudes, Practice (N = 5). Most of the literature used to design this
project is from 2018-2024, except one referenced article from 2004. These key terms were searched as single terms and with the use of Boolean operators using PubMed, Google Scholar, and EBSCO.
Any medical student above the age of 18 was eligible for this study. Specifically, all students in a vaccine elective at RVUCOM on the Colorado and Utah campuses were enrolled as part of the course, as well as student volunteers. We excluded any students who opted out of the study.
Intervention
Participants in the LTE group first interacted with a Vaccine Hesitant Standardized Patient (VHSP) before participating in a didactic module on vaccine hesitancy and MI techniques. Following this module, they were re-exposed to the VHSP to apply learned skills. In contrast, the TT group engaged with a control standardized patient (SP) engaging in the module and performing an interaction with the VHSP (Figure 1).
Data Collection
Data Were Collected Using Two Primary Measures
Confidence Scores: A 22-item survey assessed participants’ confidence across seven themes, including vaccine hesitancy experience, vaccine knowledge, MI support, MI hinderance, vaccine hesitancy skills, and vaccine recommendation confidence.
Responses were quantified using a Likert scale ranging from 0 (not confident) to 4 (very confident) (Appendix A, Table A1).
Performance Scores: A 21-item checklist derived from the Interprofessional Simulation- Based Education rubric used by Rocky Vista University for grading Standardized Patient encounters was categorized into seven themes, including opening the discussion, gathering information, investigation, providing information, acknowledgement, providing closure, professionalism, and negative behaviors. Standardized Patients (SPs) rated participants on these items with scores of either 0 (not performed), 0.5 (partially performed) or 1 (performed effectively) (Appendix A, Table A2).
Statistical Analysis
Confidence and performance scores were analyzed to compare the effectiveness of the LTE and TT instructional methods. Comparisons were made using mean scores for each theme between groups. Confidence and performance scores were also analyzed to compare the LTE instructional group before and after the introduction of the vaccine hesitant module. Statistical significance was determined using paired and unpaired t-tests with a p-value < 0.05 considered statistically significant.
Ethical Considerations
This study was approved by the Institutional Review Board (IRB) of Rocky Vista University College of Osteopathic Medicine, with protocol number 2022-173. All participants provided informed consent before participation, with the assurance of confidentiality and the right to withdraw at any time without penalty.
Results
The study enrolled 36 participants randomly assigned to either the LTE group or the TT group. The demographic makeup of the population by academic year and program is shown in Figure 2.
In comparing these two different teaching methods using Performance Scores by themes, the TT group had significantly higher mean performance scores in Opening Discussion, and Providing Information, while the LTE group had significantly higher scores in Acknowledging Patient Concerns but exhibited a significantly higher number of Negative Behaviors (Table 1).
Comparing the students’ self-evaluations in their confidence of using MI in the context of vaccine hesitancy across teaching groups revealed the LTE group significantly reporting greater support in MI usage, but interestingly, they also revealed greater confidence in utilizing Vaccine Hesitancy Key Skills (Table 2).
When analyzing the SP performance scores during the timeline of the LTE intervention, it was found that the scores between the first and second SP were insignificantly different before completing the intervention compared to after completing the intervention with the exception of the LTE group having a significantly higher score in Providing Information to prior to completing the entire teaching intervention (Table 3).
Discussion
This study embarked on evaluating two pedagogical approaches—the TT method and the novel LTE method —within the context of motivational interviewing (MI) education in addressing vaccine hesitancy. Despite their conceptual differences, the study revealed that the LTE method did not outperform the established TT method unequivocally. Instead, each approach yielded distinct advantages in enhancing medical students’ competencies and confidence in engaging with vaccine-hesitant individuals.
The TT group demonstrated a robust acquisition of MI skills as imparted through didactic sessions, affirming the value of direct instruction followed by practice. Conversely, the LTE group excelled in applying these skills in practical settings, notably in standardized patient (SP) interactions. This suggests that initial exposure to a challenging scenario such as vaccine hesitancy may prime students for a deeper engagement with subsequent educational content, potentially due to heightened relevance and immediacy.
However, the LTE approach’s mixed results on subsequent MI skill application point to the complexity of learning and applying these nuanced communication techniques. While LTE participants showed greater confidence in MI abilities and vaccine knowledge, this did not consistently translate into superior skill execution compared to their TT counterparts. Such findings invite further discussion into the interplay between confidence, knowledge, and skill mastery in clinical education.
Several factors could account for the observed outcomes. Initial negative encounters in the LTE group, variations in baseline competency among SPs, and demographic differences within the groups might have influenced the results. Notably, the study’s design allowed for comparing each group’s performance over time, revealing nuanced improvements in SP navigation and MI technique application. Despite these insights, the study is not without limitations. The sample size, subjective nature of performance assessments, and variability in SP training across sites may affect the generalizability and interpretability of the findings. Future research endeavors could broaden the dataset, apply this study model across diverse MI applications, and assess the long-term retention and use of MI skills in clinical practice.
While the TT method sustained its efficacy in imparting MI skills, the LTE method offered valuable insights into the dynamics of learning and applying these skills in real-world scenarios. This study underscores the promise of diversified instructional strategies in medical education, especially as educators seek to equip students with the competencies needed for effective patient communication in an era marked by vaccine hesitancy and other public health challenges.
Moving forward, refining and expanding upon these educational models is imperative, ensuring that future healthcare professionals can navigate the complexities of patient interactions with empathy, skill, and confidence. Exploring additional innovative teaching methods and integrating longitudinal assessments into medical curricula could further enhance the effectiveness of MI training and its impact on patient care outcomes.
Conclusions
The comparative evaluation of the TT and LTE methods in the instructional domain of motivational interviewing (MI), particularly with a focus on vaccine hesitancy, has elucidated that each method brings valuable perspectives to the educational experience. While the TT method reaffirmed its efficacy in grounding students in MI theoretical frameworks and skills, the LTE method illuminated the importance of experiential learning, highlighting an enhanced capacity for students to apply MI techniques in patient interactions.
The nuanced differences between these approaches emphasize a broader pedagogical principle: integrating diverse teaching methodologies can enrich medical education, particularly in fields requiring complex interpersonal skills such as MI. This study suggests that a hybrid educational model, leveraging the strengths of both TT and LTE methods, could offer a more comprehensive learning experience, equipping students with the theoretical knowledge and practical expertise necessary for effective patient communication.
Furthermore, the divergence between self-assessed confidence and demonstrated competence in the LTE group points to an essential aspect of medical training—the need for educational strategies that build confidence and accurately reflect students’ abilities. This observation advocates for ongoing assessment and feedback mechanisms that help students calibrate their self-perceptions with objective performance metrics.
Looking forward, the findings from this study advocate for continued exploration and innovation in MI education. There is a clear indication to investigate how these teaching methodologies can be adapted and applied across various medical education contexts to address a range of public health challenges, including but not limited to vaccine hesitancy. Expanding upon the foundational insights provided by this investigation, subsequent studies could explore a more comprehensive array of instructional designs, engage larger and more diverse participant samples, and assess the long-term impact of different MI teaching methods on clinical practice and patient outcomes.
This study contributes to the ongoing dialogue on how best to prepare medical students for the complexities of modern healthcare. As vaccine hesitancy and other public health concerns continue to challenge the medical community, the role of effective communication—rooted in empathetic, patient-centered care—cannot be overstated. The journey to refine and enhance MI education is critical in this context, offering a pathway to improved patient engagement, trust, and health outcomes.
Appendix A

Table A1.
Questions posed to students before and after interacting with a vaccine-hesitant standardized patient. Responses to the questions included “not confident at all, somewhat confident, mostly confident, confident, and very confident.” Responses were converted to a numerical value on a Likert scale to determine quantitative differences between groups and across time.
Table A1.
Questions posed to students before and after interacting with a vaccine-hesitant standardized patient. Responses to the questions included “not confident at all, somewhat confident, mostly confident, confident, and very confident.” Responses were converted to a numerical value on a Likert scale to determine quantitative differences between groups and across time.
| Confidence Score Survey | |
| VH Experience | |
| Question 1 |
Have you recently encountered vaccine-hesitant individuals? |
| Question 2 |
Do you have experience counseling vaccine hesitant patients? |
| Vaccine Knowledge | |
| Question 1 |
Do you have knowledge about the benefits and side effects of the vaccine? * |
| Question 2 |
How confident are you in your ability to explain the benefits and side effects of the vaccine? |
| Question 3 |
How confident are you in your ability to answer your patient's questions about the vaccine? |
| Question 4 |
How confident are you in your ability to personally manage the patient's care based on their vaccine hesitancy status? |
| MI Support | |
| Question 1 |
I was confident in using MIT to inform the patient about relevant vaccine information |
| Question 2 |
I found the MIT helpful in structuring the conversation with the vaccine hesitant patient |
| MI Hinderance | |
| Question 1 |
I was confused on how to apply MIT to counsel the vaccine hesitant patient |
| Question 2 |
I did not find the MIT helpful in structuring the conversation with the vaccine hesitant patient |
| VH Hesitancy skills | |
| Question 1 |
How confident are you in your ability to work with your patient and their care team to encourage immunizations? |
| Question 2 |
How confident are you in your ability to work with the patient to set goals and create a plan for their health regarding immunizations? |
| Question 3 |
How confident are you in your ability to invent a solution to difficult problems? |
| Question 4 |
How confident are you in trying to solve problems or answer questions that have no single correct answer? |
| Question 5 |
How confident are you in your ability to analyze different arguments, perspectives, or solutions to a problem? |
| Question 6 |
How confident are you in your ability to use technology to communicate with the patient about future steps and the rest of their care team? |
| Question 7 |
Are you comfortable conversing with vaccine hesitant parents/patients? |
| Vaccine Recommendation Confidence | |
| Question 1 |
How confident are you in your ability to discuss vaccines with a patient during a physical? |
| Question 2 |
How confident are you in your ability to discuss vaccines with a patient during other office visits? |
| Question 3 |
How confident are you in your ability to discuss vaccines with a patient in multiple visits? |
| Question 4 |
How confident are you in your ability to discuss vaccines with vaccine-hesitant parents of pediatric patients during a regular office visit? |
| Question 5 |
How confident are you in your ability to discuss vaccines with vaccine-hesitant parents of pediatric patients during other office visits? |
| Question 6 |
How confident are you in your ability to discuss vaccines with vaccine-hesitant parents of pediatric patients in multiple visits? |
* Knowledge could be either about the COVID-19 vaccine or the MMR (Measles, Mumps, Rubella) vaccine.
Table A2.
Questions used to evaluate students on their interactions of the vaccine hesitant standardized patient interaction. Trained actors evaluated student performances as “student did not perform, partially performed, or performed effectively” for each action stated in the questionnaire. Responses were converted to numerical values of 0, 0.5, and 1 respectively to determine quantitative differences. Actions that were “partially performed” were given feedback by the standardized patient that has been removed from this study.
Table A2.
Questions used to evaluate students on their interactions of the vaccine hesitant standardized patient interaction. Trained actors evaluated student performances as “student did not perform, partially performed, or performed effectively” for each action stated in the questionnaire. Responses were converted to numerical values of 0, 0.5, and 1 respectively to determine quantitative differences. Actions that were “partially performed” were given feedback by the standardized patient that has been removed from this study.
| Performance Score Survey | |
| Opens Discussion | |
| Question 1 | Did the student ask why you are coming in today? |
| Gathers information | |
| Question 1 | Was the student organized with questioning following a logical thought process? |
| Question 2 | Did the student address vaccines not being up to date? |
| Question 3 | Did the student ask about current understanding of the vaccine? |
| Question 4 | Did the student demonstrate good listening skills? |
| Investigation | |
| Question 1 | Did the student determine where misinformation came from? |
| Question 2 | Did the student address emotions about the vaccine? |
| Question 3 | Did the student ask who vaccine decisions may affect in the household? |
| Provides Information | |
| Question 1 | Did the student provide accurate information about vaccine? |
| Question 2 | Did the student provide information about the risks and benefits of the vaccine? |
| Question 3 | Did the student avoid the use of jargon? |
| Acknowledges Patient | |
| Question 1 | Did the student demonstrate respect for the patient including appropriate cultural competence? |
| Question 2 | Did the student provide thanks for sharing information? |
| Closure | |
| Question 1 | Did the student make it clear that a decision about the vaccine did not have to be made right away? |
| Question 2 | Did the student encourage questions? |
| Professionalism | |
| Question 1 | Did the student appear professional? |
| Question 2 | Did the student appear confident? |
| Negative Behaviors | |
| Question 1 | Upon expressing vaccine hesitancy, did the student react negatively or judgmentally? |
| Question 2 | Upon expressing vaccine hesitancy, did the student initially respond by attempting to provide factual counterpoints? |
| Question 3 | Was the student at any point hostile, defensive, or dismissive? |
| Question 4 | Other than in the interest of time, did the student at any point interrupt the patient as they spoke? |
References
- Ten health issues WHO will tackle this year. Accessed July 16, 2024. https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019.
- Gagneur A, Lemaître T, Gosselin V, et al. A postpartum vaccination promotion intervention using motivational interviewing techniques improves short-term vaccine coverage: PromoVac study. BMC Public Health. 2018;18(1):811. [CrossRef]
- CDC. Measles Cases and Outbreaks. Measles (Rubeola). Published July 12, 2024. Accessed July 16, 2024. https://www.cdc.gov/measles/data-research/index.html.
- Schwartz JL. New Media, Old Messages: Themes in the History of Vaccine Hesitancy and Refusal. AMA J Ethics. 2012;14(1):50-55. [CrossRef]
- Kwok KO, Li KK, Wei WI, Tang A, Wong SYS, Lee SS. Editor’s Choice: Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int J Nurs Stud. 2021;114:103854. [CrossRef]
- Gagneur A. Motivational interviewing: A powerful tool to address vaccine hesitancy. Can Commun Dis Rep Releve Mal Transm Au Can. 2020;46(4):93-97. [CrossRef]
- Zolezzi M, Paravattil B, El-Gaili T. Using motivational interviewing techniques to inform decision-making for COVID-19 vaccination. Int J Clin Pharm. 2021;43(6):1728-1734. [CrossRef]
- Berger M. Motivational Interviewing: Preparing People for Change/Therapy with Difficult Clients: Using the Precursors Model to Awaken Change (Book). J Psychiatry Law. 2004;32(2):229-231. [CrossRef]
- Boness CL, Nelson M, Douaihy AB. Motivational Interviewing Strategies for Addressing COVID-19 Vaccine Hesitancy. J Am Board Fam Med JABFM. 2022;35(2):420-426. [CrossRef]
- Erschens R, Fahse B, Festl-Wietek T, et al. Training medical students in motivational interviewing using a blended learning approach: a proof-of-concept study. Front Psychol. 2023;14. [CrossRef]
- Hirsch EM. The Role of Empathy in Medicine: A Medical Student’s Perspective. Virtual Mentor VM. 2007;9(6):423-427. [CrossRef]
- Majumder MdAA, Haque M, Razzaque MS. Editorial: Trends and challenges of medical education in the changing academic and public health environment of the 21st century. Front Commun. 2023;8. [CrossRef]
Figure 1.
SP Exposure Design. All students were selected randomly to either be a part of the TT group (the upper portion of the graphic) or the LTE group (the lower portion of the graphic) to determine the effectiveness of each teaching method in the context of approaching vaccine hesitancy using MI.
Figure 1.
SP Exposure Design. All students were selected randomly to either be a part of the TT group (the upper portion of the graphic) or the LTE group (the lower portion of the graphic) to determine the effectiveness of each teaching method in the context of approaching vaccine hesitancy using MI.
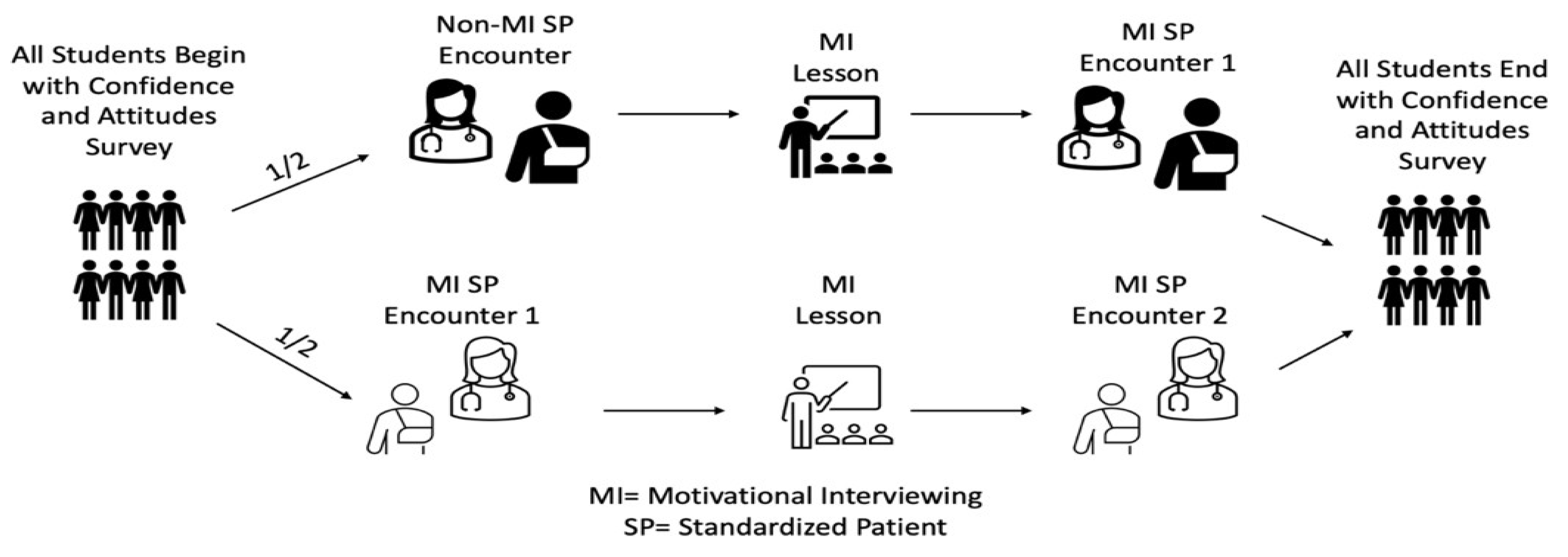
Figure 2.
Demographics of each population teaching intervention in teaching MI in the context of vaccine hesitancy. MSBS refers to students in the Master’s in Biomedical Sciences program while OMS-I and OMS-II refer to students in the Doctor of Osteopathic Medicine program Year 1 and Year 2.
Figure 2.
Demographics of each population teaching intervention in teaching MI in the context of vaccine hesitancy. MSBS refers to students in the Master’s in Biomedical Sciences program while OMS-I and OMS-II refer to students in the Doctor of Osteopathic Medicine program Year 1 and Year 2.
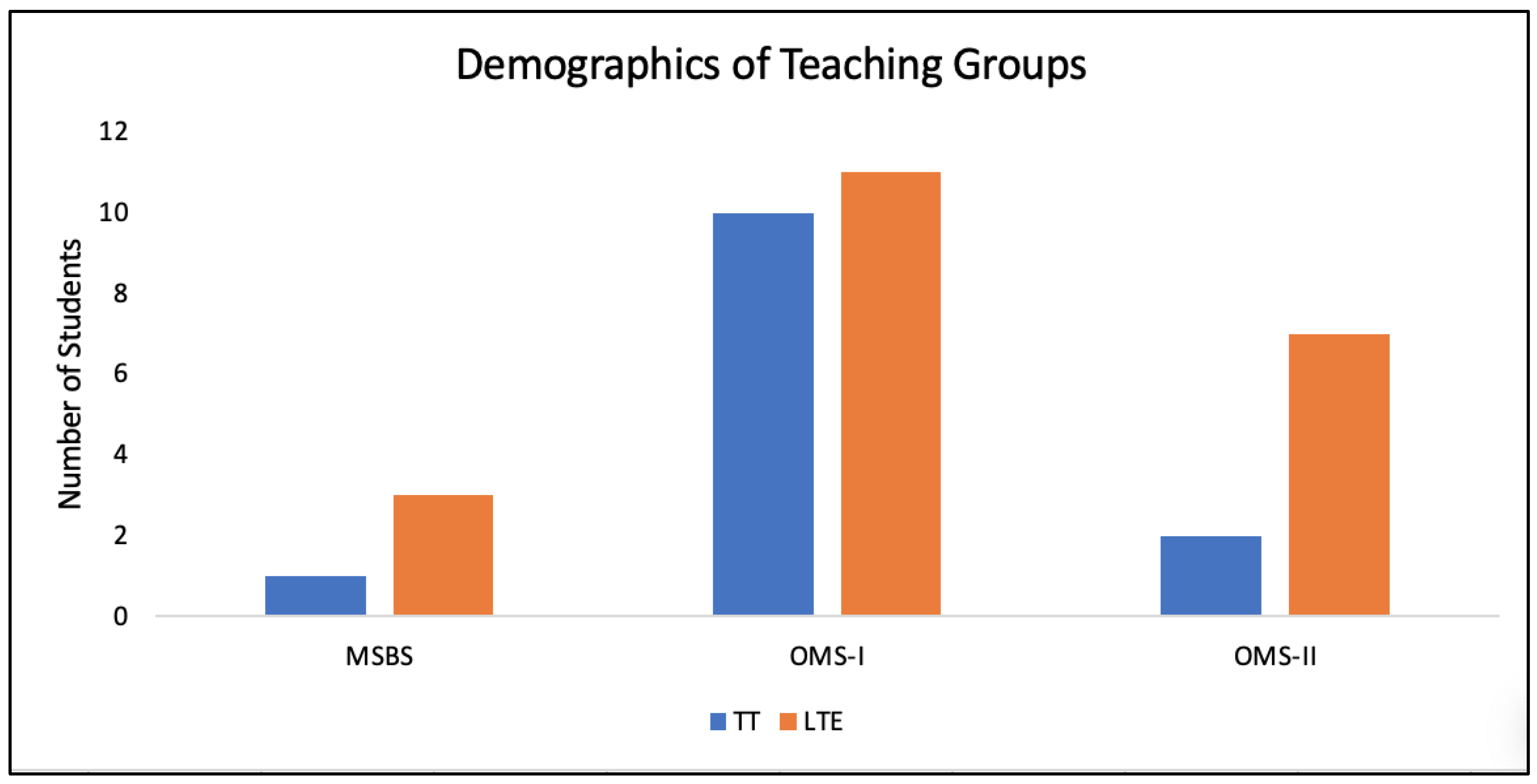
Table 1.
SP performance scores between TT and LTE teaching methods. All increased results are denoted with a “*” next to the higher value in comparing the two groups. All statistically significant increased values are denoted with a “**” along with their respected KWPV < 0.05.
Table 1.
SP performance scores between TT and LTE teaching methods. All increased results are denoted with a “*” next to the higher value in comparing the two groups. All statistically significant increased values are denoted with a “**” along with their respected KWPV < 0.05.
| TT SP Performance Score | LTE SP Performance Score | Kruskal-Wallis P- value | |||||
| Variable | N | Mean | Std Error | N | Mean | Std Error | |
| Opens Discussion | 13 | 1.88** | 0.08 | 22 | 1.55 | 0.10 | 0.0236** |
| Gathers Information | 13 | 3.58* | 0.12 | 22 | 3.41 | 0.19 | 0.9706 |
| Investigation | 13 | 1.73 | 0.29 | 22 | 1.86* | 0.14 | 0.6837 |
| Provides Information | 13 | 2.77** | 0.11 | 22 | 2.32 | 0.13 | 0.0213** |
| Acknowledging Patient Concerns |
13 | 1.38 | 0.14 | 22 | 1.73** | 0.10 | 0.0488** |
| Closure | 13 | 1.12 | 0.25 | 22 | 1.52* | 0.13 | 0.1865 |
| Professionalism | 13 | 1.85 | 0.09 | 22 | 1.93* | 0.04 | 0.4341 |
| Negative Behaviors |
13 | 0.34 | 0.16 | 22 | 0.77** | 0.23 | 0.0262** |
Table 2.
Confidence survey scores between TT and LTE teaching methods. All significantly increased results are denoted with a “*” next to the higher value in comparing the two groups. A “**” reflects statistically significant results in the values and the respected KWPV < 0.05.
Table 2.
Confidence survey scores between TT and LTE teaching methods. All significantly increased results are denoted with a “*” next to the higher value in comparing the two groups. A “**” reflects statistically significant results in the values and the respected KWPV < 0.05.
| TT Confidence Score | LTE Confidence Score | Kruskal-Wallis P-value | |||||
| Variable | N | Mean | Std Error | N | Mean | Std Error | |
| Vaccine Hesitancy Experience |
13 | 0.77* | 0.17 | 21 | 0.76 | 0.15 | 0.9058 |
| Vaccine Knowledge | 13 | 7.38 | 0.45 | 21 | 8.19* | 0.41 | 0.3356 |
| Support MI Usage | 13 | 5.54 | 0.27 | 21 | 6.33* | 0.27 | 0.0632 |
| Against MI Usage | 13 | 3.38* | 0.43 | 21 | 2.76 | 0.34 | 0.1573 |
| Vaccine Hesitancy Key Skills |
13 | 20.92 | 0.75 | 21 | 23.33* | 0.82 | 0.0612 |
| Confidence in Making a Vaccine Recommendation |
11 | 17.64 | 0.96 | 21 | 19.81* | 0.87 | 0.1004 |
Table 3.
SP performance scores of before completing the LTE teaching method and after completion of the LTE teaching method. All increased results are denoted with a “*” next to the higher value in comparing the two groups. All statistically significant results are denoted with a “**” along with their respected P-value < 0.05.
Table 3.
SP performance scores of before completing the LTE teaching method and after completion of the LTE teaching method. All increased results are denoted with a “*” next to the higher value in comparing the two groups. All statistically significant results are denoted with a “**” along with their respected P-value < 0.05.
| LTE Before Completion |
LTE Completed | ||||
|---|---|---|---|---|---|
| Variables | Mean | SD | Mean | SD | P-value |
| Opens Discussion | 0.955 | 0.045 | 0.955 | 0.045 | 1.0000 |
| Gathers Information | 3.523* | 0.174 | 3.409 | 0.174 | 0.6494 |
| Investigation | 1.864 | 0.165 | 1.864 | 0.165 | 1.0000 |
| Provides Information | 2.705** | 0.124 | 2.318 | 0.124 | 0.0382** |
| Acknowledges Patient Concerns | 1.682 | 0.107 | 1.727* | 0.107 | 0.7674 |
| Closure | 1.614* | 0.132 | 1.523 | 0.132 | 0.6324 |
| Professionalism | 1.841 | 0.072 | 1.932* | 0.072 | 0.3845 |
| Negative Behaviors | 0.659 | 0.216 | 0.772* | 0.216 | 0.7137 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



