
Submitted:
08 August 2024
Posted:
09 August 2024
You are already at the latest version
Abstract
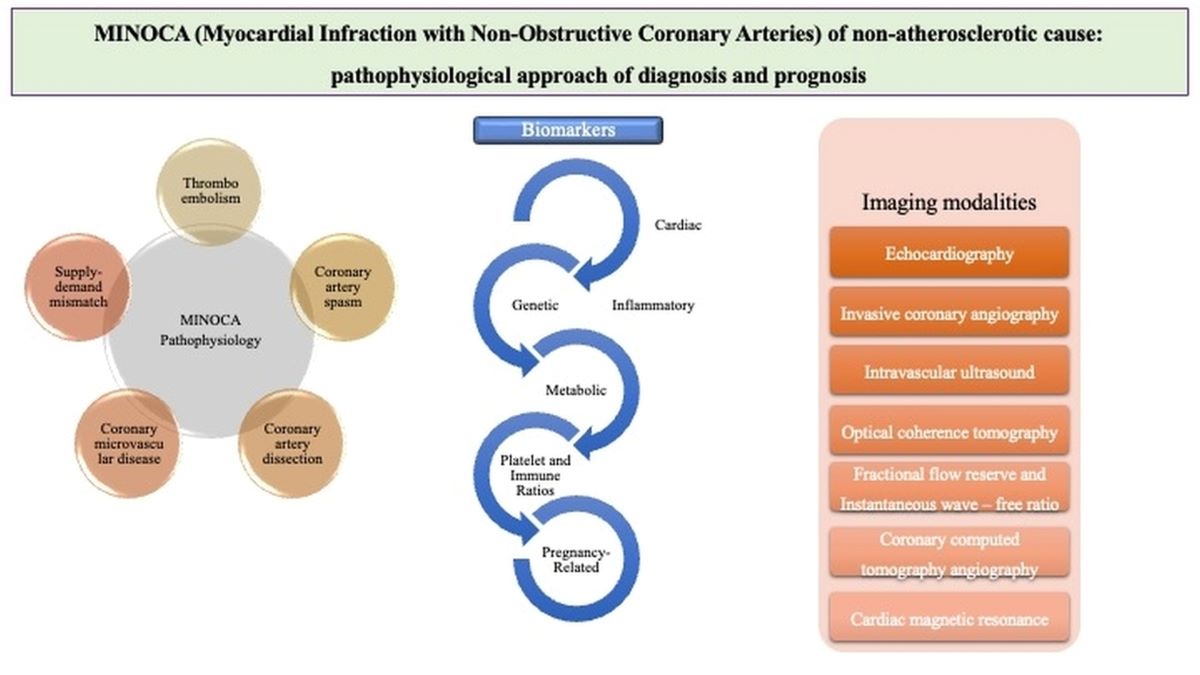
Myocardial Infarction with Non-Obstructive Coronary Arteries (MINOCA) is a clinical entity characterized by the absence of significant coronary artery obstruction in epicardial arteries (< 50%) on coronary angiography in the setting of acute myocardial infarction (AMI). This article aims to provide a narrative review of the pathophysiological mechanisms, diagnostic challenges, and prognosis associated with MINOCA focusing only on cases associated with myocardial ischemia but of non-atherosclerotic origin. Etiological factors, including thromboembolism, coronary artery spasm, spontaneous coronary artery dissection, coronary microvascular disease, and supply-demand mismatch are addressed. Imaging modalities such as echocardiography, advances in coronary angiography like intravascular ultrasound (IVUS) and optical coherence tomography (OCT), cardiac magnetic resonance (CMR), and coronary computed tomography angiography (CCTA) are also analyzed. MINOCA patients have a better short-term prognosis compared to those with obstructive coronary artery disease but face significant long-term risks, underscoring the need for precise diagnosis and management strategies. Elevated inflammatory markers and specific genetic predispositions are also associated with adverse outcomes in MINOCA. This review focused on MINOCA from the pathophysiological perspective on ischemic, non-atherosclerotic causes, the diverse underlying mechanisms, the challenges in achieving accurate diagnosis, the importance of a tailored therapeutic approach and the necessity for further investigation of clinical outcomes.
Keywords:
Myocardial Infarction with Non-Obstructive Coronary Arteries
; thromboembolism
; coronary artery spasm
; spontaneous coronary artery dissection
; coronary microvascular disease
; diagnosis
; prognosis
1. Introduction
Causes: Acute myocardial infarction (AMI) has been one of the most extensively studied cardiovascular diseases (CVDs). In the majority of AMI, a significant atherosclerotic stenosis or obstruction of any epicardial coronary artery is the leading cause[1]. The performance of coronary angiography worldwide in almost all patients with AMI has led to the increasing recognition of another entity; the myocardial infarction with non-obstructive coronary arteries (MINOCA). The definition of MINOCA includes all the criteria for AMI but requires non-significant stenosis in epicardial arteries (<50%) on coronary angiography [2]. The pathophysiologic mechanisms of MINOCA vary and can be divided into cardiac and extra-cardiac, while the former is further subdivided in ischemic and non-ischemic origin. Common ischemic mechanisms include thromboembolism, epicardial coronary artery spasm (CAS), spontaneous coronary artery dissection (SCAD), and coronary microvascular dysfunction (CMVD a mismatch between the oxygen needs and supply to the myocardium) [3]. While non-ischemic mechanisms typically involve situations where there is direct myocardial injury like myocarditis, cardiomyopathy Takotsubo [3]. The proposed mechanisms may be part of a systemic condition and sometimes are not fully understood.
Epidemiology and prognosis: The prevalence of MINOCA among patients presenting with AMI typically falls within a range of 3% to 15%[4,5,6,7]. Emerging evidence highlights notable disparities in MINOCA prevalence between different etiopathogenetic mechanisms and sexes, with women being more frequently diagnosed than men[8,9]. Systematic reviews indicate an annual mortality rate of approximately 2.0% for patients with MINOCA[8]. Compared to AMI with obstructive coronary artery disease (AMI-CAD), MINOCA patients are generally younger[10], with lower all-cause mortality, but higher than CAD-free population[9,11,12,13].
Diagnosis: Numerous challenges have been faced during MINOCA diagnosis due to its diverse etiologies, variable clinical presentations, and the absence of a gold-standard diagnostic modality. The coronary angiography and its advanced techniques like intravascular ultrasound (IVUS) and optical coherence tomography (OCT) is the basis of the diagnostic algorithm. Usually, the heterogeneity of the MINOCA causes prompts the utilization of multiple imaging techniques on the top of resting echocardiography, like cardiac magnetic resonance (CMR)[14], functional tests of myocardial ischemia and coronary flow reserve (CFR)[15,16]. Moreover, biomarkers (e.g., for myocardial injury or inflammation) may play a role in MINOCA investigation aiding in the comprehensive evaluation and management of patients with MINOCA[17]. In the era of genetics and artificial intelligence, precision medicine will play a pivotal role in the individualized management of MINOCA patients[18].
MINOCA is a rule-out diagnosis with lack of standardized protocols for diagnosis and therapeutic management. The present review aims to provide a more comprehensive insight of MINOCA with coronary vessels origin from the pathophysiological point of view, focusing on new diagnostic indices, prognosis and patient-tailored treatment.
2. Search Strategy
We searched MEDLINE and Embase databases from January 1990 to July 2024. Our search was confined in English language publications. We used the following search terms, including Medical Subject Headings: Myocardial Infarction with Non-Obstructive Coronary Arteries - MINOCA; thromboembolism; coronary artery spasm; spontaneous coronary artery dissection; coronary microvascular disease; pathophysiology; echocardiography; cardiac magnetic resonance (CMR); coronary flow reserve (CFR); intravascular ultrasound (IVUS); optical coherence tomography (OCT); biomarkers; prognosis; therapy. Except for case studies, and preclinical studies (in vitro and animal), all other types of clinical studies (observational, randomized, non-randomized, prospective, retrospective) were considered eligible. The articles’ reference list was checked to identify additional relevant papers for inclusion.
3. Pathophysiology
The pathophysiology of MINOCA is diverse and the causative factors associated with can be divided into cardiac (ischemic and non-ischemic) and extra-cardiac categories. For the purposes of this article, we will focus on coronary ischemic-driven causes such as thromboembolism (plaque disruption and coronary embolization), epicardial CAS, SCAD, CMVD and supply-demand imbalances (Figure 1).
Thromboembolism
Thromboembolism contributes to acute coronary syndrome (ACS) pathogenesis as a consequence of plaque disruption encompassing plaque rupture, erosion, and calcified nodules or it may be implicated as the sole intriguing factor per se in hypercoagulable states[19,20,21]. The use of high-resolution imaging modalities during coronary angiography like OCT or IVUS has revealed a high percentage of MINOCA cases linked with plaque disruption. Notably, plaque disruptions have been found in approximately one-third of MINOCA patients[22] and it is identified as a discontinuity of the fibrous cap overlying a lipid-rich core that typically occurs with superimposed thrombus formation. It is best visualized by OCT[10]. Plaque erosion is defined as a thrombus contiguous to the luminal surface of a plaque in the presence of an intact fibrous cap[23]. Calcific nodule defined on OCT imaging as a faint-signal region with blurry edges extending into the arterial lumen while a common feature in older patients with ACS but is rarely seen in MINOCA[24]. The above mentioned atherothrombotic phenomena are associated with distal embolization or occasionally, transient complete thrombotic lumen occlusion[25]. On the other hand, coronary embolic phenomena may arise from coronary or systemic arterial thrombi in the setting of thrombophilia disorders or other conditions associated with increased clotting tendency[12]. Hereditary thrombophilia like factor V Leiden mutation, protein S and C deficiencies or factor VIII/von Willebrand disease present with varying prevalence (14-25%) among MINOCA patients, especially in young women, but they are rarely investigated[12,26,27]. The antiphospholipid syndrome, myeloproliferative diseases, thrombotic thrombocytopenic purpura (TTP) and heparin-induced thrombocytopenia (HIT) may also play a role in MINOCA presentation in the context of acquired thrombophilia disorders, but they have not been investigated thoroughly yet[28,29]. In MINOCA patients, diagnostic testing including factor V Leiden levels, prothrombin 20210A, factor VIII, as well as activities of protein C and S, antithrombin, lupus anticoagulant, and a comprehensive analysis for antiphospholipid antibodies etc. should ideally be done when no other obvious reason for MINOCA is detected and thrombophilia is highly suspected (e.g., younger age, family history, without obvious cardiovascular risk factors etc) after the resolution of the acute phase to ensure diagnostic tests accuracy[30].
Coronary Artery Spasm (CAS)
CAS indicates diffuse or focal severe vasoconstriction (ie, >90%) of an epicardial coronary artery resulting in impaired myocardial blood supply[20]. Persistent CAS may lead to AMI and should also be considered in MINOCA patients. A systematic review and a prospective cohort study have demonstrated reproducibility of episodic ischemia and chest pain using provocative tests, with rates of 27% and 46%, respectively[12,31]. CAS tends to be more common in Asian populations and its pathopshysiology involves hyper-sensitivity of the vascular smooth muscle cells (VSMCs) triggered by exogenous factors like drugs or toxins (nicotine, amphetamines, cocaine) or spontaneously due to vasomotor disorders[32,33]. That hyper-reactivity is regulated by endothelium-derived signaling molecules like nitric oxide (NO) and vasoconstrictive factors released by the perivascular adipose tissue[34]. Increased Rho-kinase activity interfering with prolonged muscle contraction is also observed in patients with CAS, during active anginal episodes, and in smokers due to nicotine’s association with chronic low-grade inflammation[34]. CAS frequently occurs alongside myocardial bridging (MB), since 60% of patients with MB experienced significant vasoconstriction during provocative tests[35].
Spontaneous Coronary Artery Dissection (SCAD)
SCAD involves the formation of a false lumen within the coronary artery wall compressing the true lumen and typically leads to ACS[36]. Most cases of SCAD arise in the absence of traditional atherosclerotic plaque formation factors, are notably more prevalent in females, but its actual incidence is unknown. In coronary angiogram, SCAD typically results in substantial (>50%) stenosis of an epicardial coronary artery, but in the minority of cases coronary arteries might appear normal or nearly normal due to a gradual narrowing of the vessel, thereby constituting SCAD as a potential cause of MINOCA.
SCAD development is explained by two hypotheses. The “inside-out” hypothesis suggests that intimal disruption allows blood to seep into the vessel wall, forming a hematoma. On the other hand, the “outside-in” hypothesis favors the hematoma formation by bleeding from the vasa vasorum without endothelial-intimal layer injury. Both hypotheses lead to a common endpoint, growing hematoma, which compresses the true lumen causing myocardial ischemia[37]. Fibromuscular dysplasia has been proposed as an alternative mechanism[38,39]. Hormonal variations and physiological changes related to pregnancy and childbirth, have also been associated with alterations in the intima-media structure of the arterial wall[40]. Emotional stress, intense physical activities, and the use of sympathomimetic drugs may also play a key role in SCAD[38]. There is also a link between certain collagen vascular disorders, such as Marfan syndrome, Ehlers-Danlos syndrome, Alport syndrome, and nail-patella syndrome, as well as chronic inflammatory diseases like systemic lupus erythematosus, inflammatory bowel disease, and sarcoidosis[19]. Definitive SCAD diagnosis may require intravascaular imaging modalities. OCT is preferable, while IVUS offers deeper penetration for visualizing the entire intramural hematoma[41].
Coronary Microvascular Disease (CMVD)
CMVD has been long recognized as a frequent reason of ischemic symptoms and involves coronary microcirculation, like vessels smaller than 0.5 mm in diameter. Those vessels represent approximately 70% of the coronary artery network and their spasm resulting in high coronary vascular resistance may lead to significant myocardial ischemia when obstructive CAD is absent[42]. CMVD is quite common among patients with MINOCA. From the pathophysiological perspective, CMVD includes either functional abnormalities with increased propensity for vasoconstriction at the microvascular level and impaired endothelium-dependent and -independent coronary vasodilator capacities, and increased coronary microvascular resistance secondary to structural factors e.g., luminal narrowing, vascular remodeling, vascular obstruction, and extramural compression[43]. Among patients experiencing the coronary slow flow phenomenon during coronary angiogram the elevated basal microvascular resistance plays a predominant role[44]. A small study using stress CMR on 40 female patients after MINOCA found that two-thirds exhibited inducible perfusion abnormalities, suggesting CMVD. Yet, such perfusion issues were also observed in cases of myocardial edema accompanying conditions like myocarditis. Therefore, it was unclear whether CMVD is a cause or an effect of MINOCA[45]. The main obstacle to set the diagnosis of CMVD is the absence of easily performed techniques in routine clinical practice. Noninvasive tests like echocardiography CFR, stress CMR, or Positron Emission Tomography (PET) do not have widespread adoption due to time-constrains, limited expertise, availability issues, high costs, or radiation risks[46]. Consequently, the contribution of CMVD to MINOCA warrants further research.
Supply-Demand Mismatch and Type 2 Myocardial Infarction
Myocardial oxygen demand is regulated by key factors including cardiac systolic wall tension, contractility, and heart rate, while supply is mainly determined by coronary blood flow and oxygen content[47]. Type 2 AMI refers to cardiac events stemming from myocardial oxygen supply-demand mismatch. This can be seen in CAS and thrombosis or in severe systemic stresses like fast arrhythmias, anemia, severe aortic valve disease, hypotension, respiratory failure, shock (e.g., septic), heart failure or cardiomyopathy. It may also result from the adverse effects of toxins and pharmacological agents. Typically, non-obstructed coronary arteries are a common characteristic across all these conditions[48,49].
4. Diagnostic Approach Based on Pathophysiology
The AHA, ESC, and other scientific societies have outlined specific criteria and sequence for MINOCA diagnosis[20]. This is typically characterized by: 1) symptoms indicative of ACS, 2) troponin elevation, and 3) non-obstructive lesions (<50%) in coronary angiography leading to a provisional diagnosis of MINOCA[15,50]. Additionally, it’s a prerequisite to meticulously exclude any missed coronary obstruction and then to investigate the underlying mechanisms of myocardial injury[20], since MINOCA serves as a diagnostic puzzle, encompassing a diverse array of mechanisms with ischemic and non-ischemic origin[12,50,51]. Working diagnosis of MINOCA can indeed be challenging, and despite comprehensive evaluation, the underlying cause remains unidentified in up to 25% of patients[52,53]. Employing various advanced imaging modalities such as intravascular studies (OCT, IVUS), fractional flow reserve (FFR), as well as non-invasive techniques like CFR, cardiac computed tomography angiography (CCTA) and CMR, become imperative[54]. Moreover, biomarkers play a pivotal role in both diagnosis and prognosis. The emerging genetic factors and metabolomics may add depth to precision diagnosis and prognosis.
4.1. Imaging Modalities
4.1.2. Echocardiography
Echocardiography seldom contributes to reaching the final diagnosis in MINOCA patients associated with coronary vessels dysfunction. Nonetheless, it serves as an essential initial step for assessing AMI to identify wall motion abnormalities and exclude other reasons of myocardial injury such as pericarditis and aortic dissection[55]. In MINOCA patients suspected of having CMVD, non-invasive evaluation of reduced CFR (defined as a ratio of mean blood flow <2 between maximal hyperaemia and rest) can be achieved through transthoracic Doppler[15,56]. A reduced CFR signifies the vasculature’s inability to vasodilate and increase coronary blood flow adequately to meet metabolic demands during hyperaemic states. Nevertheless, its ability to discriminate CMVD from severe epicardial CAD may be sometimes limited.
4.1.3. Invasive Coronary Angiography
Coronary angiography remains the initial step to set MINOCA diagnostic work-up. Moreover, it is the gold standard in SCAD diagnosis, especially among young women presenting with AMI[15], while both type 2 and 3 of SCAD may necessitate better visualization with OCT or IVUS implementation for a definitive diagnosis. In case of undetermined cause of MINOCA “functional coronary angiography”, involving measurement of microvascular function/coronary reactivity, and intravascular imaging can be beneficial in pinpointing the underlying CMVD mechanism[50].
Provocative testing for coronary spasm should be considered during diagnostic angiography when CAS suspected[15,57]. This involves the administration of escalating doses of acetylcholine or ergonovine until induces an epicardial coronary vasospasm[58]. The test is considered diagnostic for epicardial CAS when shows: 1) a reduction in epicardial coronary diameter of ≥90% compared to the relaxed state after nitroglycerin administration, 2) reproduction of symptoms, and 3) ischemic ECG changes. However, patients with recent AMI (<6 weeks) are prone to experiencing inducible spasm during provocative testing[12].
Those, provocative tests may also elicit a vasoconstrictive response at microvascular levels, implicating coronary vasomotor disorders[59]. Microvascular spasm is diagnosed when typical ischemic ECG changes occur with angina but without significant narrowing of the epicardial coronary arteries[59]. Overall acetylcholine administration is a safe test with rare complications[60]. On the other hand, intracoronary administration of adenosine has limited diagnostic utility in CMVD-related MINOCA [15]. Because it may also indicate various reasons of myocardial injury and not exclusively MINOCA[15]. Intracoronary administration of vasodilators is crucial for diagnosing myocardial bridging, as it enhances the systolic ‘milking’ effect caused by the systolic compression of the intramural artery within the tunneled artery[59].
4.1.4. Intravascular Ultrasound (IVUS) and Optical Coherence Tomography (OCT)
Intracoronary vascular imaging, including OCT and IVUS, proves invaluable in assessing coronary lesions that may not be apparent on angiography, such as AMI resulting from plaque disruption, distal coronary artery embolization, and SCAD[59]. It allows both the lumen and plaque to be visualized[61]. Given the infrequent implementation of OCT or IVUS in routine practice, there is a likelihood of underdiagnosing the etiology of MINOCA cases[56]. Cost, local availability, and expertise represent potential limitations to the routine utilization of intravascular imaging[55].
IVUS is an ultrasound-based technology (~40 μm wavelength at 40 MHz) and offers a comprehensive 360-degree cross-sectional vessel image, allowing the detailed characterization of lesion morphology (e.g., ulcerations) and precise quantification of plaque burden[19,54,62]. OCT is an infrared light-based technology (1.3μm wavelength)[62,63] and it generates images with a resolution 10 times finer (10 um) than IVUS[62], accomplishing this in a mere 2.5 seconds[54]. OCT, with its exceptional resolution, allows visualization of luminal and superficial coronary artery lesions and enables assessment of morphologic features at the tissue level, especially SCAD and plaque disruption[15,64]. Hybrid IVUS-OCT imaging promise improved atherosclerotic plaque characterization by minimizing imaging artifacts in both datasets, but with increasing cost.
4.1.5. Fractional Flow Reserve (FFR) and Instantaneous Wave–Free Ratio (IFR)
FFR is an invasive hemodynamic functional measurement utilized to assess the significance of intermediate stenosis in epicardial coronary arteries[54]. This index is pressure-wire-based and is the gold standard invasive functional technique, since it determines whether a lesion is causative of inducing ischemia[54]. The role and reliability of FFR in the context of MINOCA are limited and warrant further study[65]. While FFR assesses the severity of epicardial stenosis, significant microvascular disease can elevate FFR values to the same degree as an epicardial stenosis[66]. These patients may show discordance between FFR and CFR, since CFR predominantly reflects the state of the microvascular system[66]. Consequently, CFR < 2.0 and an index of microcirculatory resistance (IMR) ≥ 25 units in patients with elevated FFR denote abnormal microvascular function[66].
4.1.6. Coronary Computed Tomography Angiography (CCTA)
Cardiac CT had emerged as a multi-potential diagnostic tool in the assessment of MINOCA, capable of identifying various aetiologies of the disease along with key prognostic factors. This imaging modality enables the assessment of extracardiac structures [54]. Most importantly, it can describe plaque characteristics like content, volume, distribution, and peri-coronary inflammation, in addition to maximal luminal stenosis[57,67]. However, it cannot identify culprit plaque rupture. Novel studies have utilized CCTA to characterize plaque and its inflammatory burden during the acute phase of MINOCA[54]. The peri-coronary fat inflammation, as detected by the Perivascular Fat Attenuation Index (pFAI), represents a novel imaging marker of inflammation[18,54]. Pergola et al. demonstrated that patients with MINOCA exhibited significantly elevated pFAI values compared to controls when assessed within eight days of the event, suggesting the potential utility of CCTA for identifying MINOCA cases of coronary origin[68]. Conversely, in cases of non-ischemic MINOCA, like myocarditis and takotsubo, the pFAI values remained unaltered for an extended duration. Up to now the current evidence is insufficient to support the routine use of pAFI in MINOCA[15].
4.1.7. Cardiac Magnetic Resonance (CMR)
CMR stands out as an essential test among others for MINOCA diagnosis and as a versatile imaging modality to delineate diverse pathophysiological effects of reversible (e.g., inflammation - edema) and irreversible (e.g., necrosis - fibrosis) acute myocardial injury[69,70]. As per the ESC guidelines (2023), CMR is designated as class I indication for all patients with MINOCA in the absence of an apparent underlying cause after invasive coronary angiography[50]. It constitutes a safe and non-invasive method for assessing myocardial perfusion, ventricular function, and the underlying mechanisms of myocardial injury[15]. Additionally, T2 and LGE sequences may uncover the size of myocardial infarct and abnormal diffusion patterns enabling the differentiation between ischemic and non-ischemic injuries[19,71]. Ischemic injuries typically exhibit myocardial edema or fibrosis along vascular territories, extended sub-endocardially or transmuraly. On the other hand, myocarditis usually shows a subepicardial or mid-wall pattern[19]. CMR enables quantification of myocardial damage due to microvascular dysfunction, using first-pass perfusion (FPP) and late gadolinium enhancement (LGE) techniques[71]. A recent study demonstrated that incorporating free-breathing LGE techniques into the standard imaging protocol enabled a definitive diagnosis in 48% of MINOCA patients who initially presented with normal scans[72].
A working diagnosis of MINOCA based on intracoronary OCT followed by early CMR within 1 week of AMI presentation, has a 85–100% sensitivity to identify ischemic causes of myocardial injury. In contrast, CMR alone had a diagnostic yield of approximately 74%[55,73]. In a recent prospective, multicenter study enrolling 170 patients with MINOCA, the majority of patients where OCT identified culprit lesion, had concomitantly an abnormal CMR imaging showing myocardial regional injury/infarction within the same coronary territory. Perhaps future management strategies for MINOCA of ischemic origin should combine direct intravascular imaging (e.g., OCT), and early utilization of CMR[53,74]. Finally, CMR-derived indices of myocardial perfusion like microcirculatory perfusion index (MPI), and perfusion resistance index (MPRI) may be associated with invasive measurements and hold prognostic significance in clinical outcomes[56]. All imaging modalities are summarized in Table 1.
4.2. Biomarkers
4.2.1. Troponin
Myocardial injury is characterized by elevated cardiac troponin (cTn) levels surpassing the 99th percentile [55]. Cardiac troponin either I (cTnI) or T (cTnT) and their high-sensitivity (hs)-cTn assays stand as the preferred biomarker of myocardial injury[49]. In cases of suspected MINOCA, a thorough diagnostic assessment should rule out other clinical causes of troponin elevation, such as noncardiac conditions (e.g., kidney impairment)[75]. cTn kinetics could serve as a distinguishing factor from AMI-CAD[17], since hs-cTn assay, does not demonstrate a remarkable and sharp rise in MINOCA populations compared to AMI-CAD populations[76]. Nevertheless, this observation cannot be expanded in the differential diagnosis of MINOCA[17].
4.2.2. Inflammatory Biomarkers
Evidence suggests that MINOCA shows higher initial inflammatory activity in the acute setting, more transient effects of myocardial injury, and faster recovery compared to patients with AMI-CAD[77]. Elevated C-reactive protein (CRP) levels, the most traditional inflammatory marker, are typically observed in MINOCA patients, and they are associated with increased risk of all-cause mortality and MACE[17,78]. However, studies have failed to find any difference in CRP and hs-CRP between MINOCA and AMI-CAD patients[17]. A long list of inflammatory factors such as P-selectin glycoprotein ligand-1 (PSGL-1), interleukin 6 (IL-6), and NF-κB essential modulator (NEMO) further have signified the exaggerated inflammatory activity in MINOCA patients[79,80,81].
MINOCA patients showed a greater increase in pro-inflammatory cytokines PlGF, oncostatin M, IL-20, and CCL-15 sVCAM-1 during the early post-infarction period and in CCL-21, sVCAM-1, oncostatin M, and PlGF after one year[82]. Notably, sVCAM-1 and CCL-21 were associated with atherosclerosis progression in MINOCA, possibly indicating complex mechanisms of microcirculatory changes. Among adipokines, visfatin, is an adipocytokine abundantly produced in visceral adipose tissue and expressed in various organs. Its potential role in endothelial dysfunction suggests its relevance to the pathogenesis of MINOCA[83]. An endless list of cytokines has been examined in MINOCA patients with potential association with MACE, but their validation is pending.
4.2.3. Natriuretic Peptides
4.2.4. Metabolic Profile
Studies involving MINOCA patients demonstrated that hyperuricemia, hyperglycemia[84], and hypercholesterolemia are related with adverse outcomes and MACE in this population[85,86]. Another study involving 1179 MINOCA patients revealed that elevated levels of Lp(a) are associated with a poorer prognosis in these individuals[87]. Elevated serum levels of Lp(a) have also been linked to microvascular injury and increased inflammatory markers, including CRP and IL-6[88,89]. All potential biomarkers in MINOCA are summarized in Table 2.
4.3. Genetic Factors/Metabolomics
Research into the genetic foundations of cardiovascular disease pathophysiology is growing, with a particular focus on how genetic susceptibility could be a primary driver of myocardial ischemia. Studies have shown that over 50% of the risk for CAD is linked to genetic factors, primarily single-nucleotide polymorphisms (SNPs) identified through genome-wide association studies (GWAS)[90]. The same recent genetic study has identified molecular pathways in the vascular endothelial growth factor A (VEGF-A) and CDKN2B-AS1 genes that are linked to alterations in CFR, emphasizing the importance of these genetic variants. Particularly, the CDKN2B-AS locus on chromosome 9p21, identified by GWAS, has been shown to significantly affect the proliferation and senescence of vascular smooth muscle and endothelial cells, impacting dysfunction in coronary microcirculation and interacts with inflammatory mediators[89]. Additionally, variations in the hemeoxygenase1 (HMOX1) gene, which encodes a stress-induced protective enzyme against myocardial ischemia, including SNPs with long promoter guanine-thymine repeats, have been associated with MINOCA. Genetic predisposition to microvascular dysfunction involves endothelin-1 (ET-1), a potent vasoconstrictor that modulates vascular tone and proliferation via endothelin-A (ET-A) and endothelin-B (ET-B) receptors[91]. The PHACTR1/EDN1 locus on chromosome 6p24 regulates ET-1 expression, with the rs9349379-G variant associated with elevated plasma ET-1 levels and increased risk of CAD and microvascular angina due to elevated coronary vascular resistance and impaired coronary blood flow. Further clinical trials are required [92,93].
The mechanism underlying SCAD might involve transforming growth factor-β (TGF-β) signaling, and hormonal function particularly prevalent in women[17]. Mutations in genes encoding TGFBR1/2 and SMAD3 are implicated in patients with SCAD and fibromuscular dysplasia (TGF-β), Ehlers-Danlos syndrome (TGF-β1, and TGF-β2 in type IV), Loeys-Dietz syndrome (SMAD2/3, TGFBR1/2), and Marfan syndrome[94,95,96,97]. Elevated circulating TGF-β pathway proteins are observed in SCAD, but a combination of miRNAs (including miR-let-7f-5p, miR-146a-5p, miR-151a-3p, and miR-223-5p) offers better predictive value warranting further investigation [17,98]. A study found that fibrillin-1 gene (FBN1) activates integrin αvβ6/TGF-β signaling, potentially leading to endothelial cell dysfunction and SCAD[17,99]. Recent histopathology studies suggest that fibrillin-1 deficiency affects arteriole integrity, increasing vascular permeability and SCAD propensity[100]. Targeting aberrant TGF signaling, along with genetic pathways involving FBN1 and ADAMTSL4, which interacts to fibrillin-1, may provide potential therapeutic strategies[96].
Rho kinase is a downstream effector of the RhoA small GTPase, and it mediates epicardial CAS and microvascular dysfunction[101]. Activation of Rho kinase plays a crucial role in the molecular mechanisms underlying CAS. Rho kinase enhances myosin light chain (MLC) phosphorylation, leading to vascular smooth muscle cell constriction and vasospasm[102,103]. Clinical studies have demonstrated elevated Rho kinase activity in CAS patients compared to non-CAS individuals, suggesting its potential as a biomarker for CAS diagnosis and prognosis[104]. Transcriptomics studies have elucidated the complex alterations in gene expression related to myocardial ischemia/reperfusion, encompassing pathways crucial for cardiac metabolism, inflammation, and extracellular matrix remodeling. Furthermore, the identification of key miRNA targets, termed ‘protectomiRs’, holds potential for therapeutic interventions aimed at cardioprotection and cardiac regeneration in conditions such as MINOCA. Transcriptomic studies have pinpointed specific miRNA clusters, such as miR15, miR17/92, and miR 302/367, alongside individual miRs like miR-99/Let-7c, miR-100/Let-7a, miR-199a, and miR-590. These regulatory molecules play a pivotal role in governing cardiomyocyte proliferation and hold promise for fostering robust cardiac regeneration in the adult myocardium. Epigenomic and transcriptomic profiling offer quantitative insights into epigenetic changes, gene expression, and splicing variants, vital for studying MINOCA progression and treatment responses.
5. Prognosis
The cardiovascular outcomes after MINOCA have been assessed in comparison to either AMI-free individuals or patients with AMI due to significant obstruction of epidardial coronary arteries (AMI-CAD). Comparison of prognosis between MINOCA and Ami-CAD patients is challenging due to the variations in the underlying pathophysiological mechanisms and the risk profile. Unfortunately, most studies have included in their analysis patients with highly variable causes of MINOCA meaning syndromes of ischemic (e.g., SCAD) and non-ischemic origin (e.g., stress cardiomyopathy). Hence, the prognosis of MINOCA and its associated factors are broadly concerned and should follow a causative stratification.
5.1. Comparison with Myocardial Infarction and Obstructed CAD
A systematic review has shown lower all-cause mortality at 12 months in MINOCA patients compared with AMI-CAD (4.7 % vs. 6.7 %)[12]. Patients with MINOCA have a significantly reduced all-cause mortality compared with those with AMI-CAD, including a 63% lower in-hospital mortality and 41% lower 12-month mortality. Although these findings may be reassuring, the 4.7% (95% CI, 2.6%–6.9%) of 12-month all-cause mortality for patients with MINOCA is of concern when compared with other published prognostic studies[12]. On the other hand, the KAMIR-NIH registry demonstrated similar 2-year all-cause death comparing MINOCA and AMI-CAD (9.1 % versus 8.8 %)[4]. This is a very high mortality rate after AMI for patients with non-obstructive CAD and highlights the importance of recognizing and treating MINOCA based on its etiology. However, a recent retrospective analysis of patients from the ACUITY study, involving 13,800 patients with moderate-to-high-risk ACS who underwent coronary angiography within 72 h, showed that compared to NSTEMI patients, MINOCA patients had a higher risk of one-year mortality (4.7 % vs. 3.6 %), although associated with an increase in non-cardiac deaths (2.1 % vs. 1.2 %), against a higher rate of recurrent AMI and repeated revascularizations in NSTEMI patients at one year[105]. It is well known that mortality increases along CAD severity, however, the prognosis of MINOCA patients may be equivalent to those without multi-vessel disease. Firstly, the Korean MI Registry [106] evaluated 12-month all-cause mortality in 8510 consecutive AMI patients, reporting a 3.1% annual mortality in those with MINOCA, 3.2% in those with single or double vessel coronary artery disease, and 6.5% in those with triple vessel disease or a significant left main coronary artery stenosis. Secondly, Ciliberti et al. [107] hypothesized that the worse prognosis in AMI-CAD patients than MINOCA counterparts is mainly affected by the presence of multi-vessel or left main disease.
In addition to mortality, the history of MINOCA is associated with higher cardiovascular morbidity. The GENESIS-PRAXIS study revealed that, despite the absence of obstructive CAD, MINOCA patients may have high risk characteristics and approximately 14% of MACE occur within 1 year of follow-up[108]. More notably, the results from the SWEDEHEART registry showed that 23.9% of MINOCA patients experienced MACE over a 4-year follow-up [109].
5.2. Comparison with General Population
The prognosis of MINOCA patients should be considered somewhat guarded despite being better than those with AMI-CAD, because it remains poorer than AMI-free subjects. Notably, both short- and long-term survival rates of MINOCA patients are lower than in the general population [109]. Patients with no previous AMI, but stable chest pain and normal/smooth coronaries on angiography have a 0.2% annual all-cause mortality, whereas those with only minor luminal irregularities have a 0.3% annual all-cause mortality, which are by far lower than MINOCA patients [4].
In the largest study to date Andersson et al. [110] compared long-term survival and causes of death in STE-ACS patients with and without obstructive CAD, the main findings were that STE-ACS patients without obstructive CAD (i) had a better short-term survival but similar or worse long-term survival compared with patients with obstructive CAD, (ii) had a worse short- and long-term survival compared with people in the general population, and (iii) mainly died of non-cardiovascular causes of death. Perhaps, the degree of cardiac injury during MINOCA may still increase the risk for adverse events.
5.3. Determinants of MINOCA Prognosis
Iteral, there is a limited number of studies on MINOCA’s prognostic risk factors, and it is not clear if they differ from the relative factors in AMI-CAD patients. A previous systematic review has shown that reduced LV ejection fraction, nonobstructive CAD, β-blockers during follow-up, and ST depression on ECG at admission are independent predictors of worse long-term prognosis of MINOCA patients[8]. The KAMIR-NIH study[2] concluded that, in MINOCA patients, old age, classical symptoms, ST interval elevation on ECG, Killip Class IV, and diabetes were independent predictors of all-cause death at the 2-year follow-up. Older age, higher creatinine concentration, low LV ejection fraction and ST elevation have also been linked to increased mortality [6,8]. Number of observational studies have added a plethora of potential independent predictors of MACE in the MINOCA population: history of hypertension, diabetes, smoking, female gender, atrial fibrillation, elevated creatinine levels and history of any of the following: stroke, AMI, peripheral vascular disease, heart failure, chronic obstructive pulmonary disease[111,112,113].
Intriguingly, some angiographic findings may be associated with worse prognosis. For instance, non-obstructive coronary atherosclerosis appears to be associated with poorer outcomes in MINOCA compared to patients devoid of evident atherosclerotic plaques [57,114]. In parallel, individuals with coronary slow flow demonstrate a heightened incidence of MACE than those with normal coronary flow rates. Patients with positive acetylcholine testing exhibited significantly worse long-term prognoses compared to those with negative results, suggesting that MINOCA patients with abnormal vasoreactivity face a heightened risk of future cardiovascular events[74].
Regarding the prognostic value of biomarkers, elevated hs-cTn levels constitute an independent risk factor for MACE events [115] and increased mortality (ACUITY trial) [105] in MINOCA patients. Moreover, elevated plasma levels of IL-6 have been associated with adverse cardiovascular outcomes[79,80], or atherothrombotic events in MINOCA, due to CMVD or coronary artery spasm[116].
6. Current Management of MINOCA
Since MINOCA has many plausible pathological mechanisms, it is still uncertain whether the classical treatment strategy for secondary prevention for type 1 AMI is suitable for MINOCA patients. On March 27, 2019, the American Heart Association (AHA) released guidelines for the diagnosis and management of MINOCA[20]; according to those recommendations, risk stratification and the most appropriate treatment scheme should be selected on the basis of etiology. However, most data derived from observational studies and require further investigation. For instance, a previous, large-scale observational study in Sweden[109] found significant proportions of patients after MINOCA on statins, angiotensin-converting enzyme inhibitors/angiotensin receptor blockers (ACEI/ARB), β-blockers, and dual antiplatelet therapy (DAPT): 84.5%, 64.1%, 83.4%, and 66.4%, respectively. Notably, in the same study 23.9% of patients experienced a MACE during an average follow-up of 4.1 years.
6.1. ACEI/ARB and Statins:
The risk of experiencing a MACE was 18% lower (HR, 0.82; 95% CI, 0.73–0.93) in patients with ACEI/ARB in comparison with no ACEI/ARB; 23% lower (HR, 0.77; 95% CI, 0.68–0.87) in patients with statins versus statins-free patients; and 14% lower after β-blocker usage (HR, 0.86; 95% CI, 0.74–1.01) than in patients without β-blockers. Hence, that study[109] showed that after MINOCA both statins and ACEI/ARB had a long-term beneficial effect on the outcome, while β-blocker showed a positive trend. In agreement, the KAMIR-NIH study[4] showed that long-term treatment of MINOCA patients with ACEI and statins was associated with reduced mortality after a 2-year follow-up. Similar results from the EMMACE-2 study showed the association of ACEI with reduced 6-month mortality (HR 0.31, 95% CI 0.03–0.78, p < 0.004) after MINOCA[117]. On the other hand, in the statins did not reduce MACE in MINOCA patients[118].
6.2. Anti-Platelet Therapy:
SWEDEHEART registry documented non-significant benefit after 1-year of DAPT therapy (HR,0.90 95% CI, 0.74–1.08). Other studies have shown neutral or even harmful effects of antiplatelet treatment to MINOCA patients, implicating its suspension in daily practice [119]. Ishii et al.[120] found that long-term use of aspirin after discharge due to MINOCA could not reduce adverse CV events. Other studies have shown that intensive clopidogrel therapy tends to be associated with an increased risk of CV mortality, AMI, and stroke in MINOCA patients[119]. In particular, a subgroup analysis of a randomized trial of antiplatelet strategies (with MINOCA being 6.7% of patients enrolled) compared high- vs low-dose clopidogrel, and high- vs low-dose aspirin. Such study demonstrated that higher-dose of clopidogrel was associated with poorer outcomes than standard dose among MINOCA patients [121]. Because of the diverse etiology and prognosis, perhaps the most proper MINOCA candidates for anti-platelet treatment should be selected according to the underlying etiology. Thereby, when plaque rupture is suspected or diagnosed as a cause of MINOCA, DAPT is recommended for 1 year, and single antiplatelet therapy is recommended for lifelong[122].
6.3. Etiological Therapy:
In the case of thromboembolism, coronary thrombi or emboli can result from a variety of thromboembolic disorders, including (1) acquired thromboembolic causes (left ventricular thrombus, prosthetic heart valves, atrial fibrillation, etc.) and (2) hereditary thromboembolic causes [protein C/S and antithrombin deficiency, factor V Leiden, etc.] [21,123,124]. Once diagnosed, treatment schemes should be individualized depending on the identified MINOCA cause according to the international guidelines[125].
The etiological therapy for CAS-induced MINOCA includes calcium-channel blocker (CCB) and nitrates for secondary prevention [126]. The combination of pharmaceutical therapy along with smoking cessation in smokers yields to symptoms relief in a significant proportion of patients with frequent episodes of CAS. Montone et al. [31] found that MINOCA patients who had positive screening for CAS stimulation and received CCB had a better prognosis than control counterparts.
In the case of SCAD, this is usually accompanied by intraluminal complications. If there is no obvious blood flow obstruction, conservative treatment is generally recommended, because coronary intervention and stenting may exaggerate dissection and expand the original range of the lesion. For this purpose, pharmaceutical therapy is preferred over percutaneous revascularization, unless there is hemodynamic instability. The cornerstone of pharmaceutical therapy is aspirin and β-blockers[127]. The latter has been associated with lower risk of recurrent SCAD in a large cohort study (HR, 0.39; 95% CI, 0.19-0.78; p = 0.008) [128]. For those undergoing percutaneous coronary intervention and stenting DAPT is highly recommended [129]. Lifelong therapy with low dose of aspirin is also recommended. Since its inconspicuous appearance is easily missed, and is not associated with atherosclerotic disorders, some researchers have not suggested traditional statin therapy[39].
In the case of CMVD, first line anti-anginal therapy with β-blockers, calcium channel blockers (CCBs) and nitrates should be used for their vasodilatory effect [130]. Perhaps, the non-dihydropyridine members (diltiazem, verapamil) with heart rate lowering effect may be a more favorable choice for angina relief. Ivabradine may play a role as a second-line agent, particularly in patients unable to tolerate β-blockers/ non-dihydropyridine CCBs or those who do not achieve an adequately controlled heart rate on maximally tolerated treatment because of its ability to lower the heart rate[131].
Additional strategies may also play a role in chronic pain alleviation e.g., antidepressants. Alterations in lifestyle including weight loss, smoking cessation, a high-fiber diet, increased consumption of fruits and vegetables, and sport are also beneficial for the prognosis of MINOCA patients[132]. Smoking cessation has been recognized as the cornerstone therapy of CMVD[133]. An indicative pharmaceutical algorithm of MINOCA of ischemic but non-atherosclerotic cause is presented in Figure 2.
7. Future Perspectives of MINOCA Personalized Therapy
There is relatively little data regarding tailored therapies for MINOCA. It should be considered as a working diagnosis that prompts further evaluation regarding its underlying etiology. The observed benefit for CFR and angina symptoms produced by ACEi or ARB served as the rationale for the design of the ongoing Women’s Ischemia Syndrome Evaluation (WISE) project to reduces events in non-obstructive CAD Trial (NCT03417388) with results expected in 2024[134]. Τhe project will conduct six randomized pharmacologic probe trials to mechanistically test improvement in coronary flow reserve and angina symptoms using ACEi, hormone therapy, aldosterone blockade, sildenafil and ranolazine. Targeting angina and quality of life (QOL), the Coronary Microvascular Angina (CorMicA) trial showed improvement in angina symptoms and QOL in patients whose medical management was guided by their mechanism based on the diagnostic invasive coronary reactivity testing results [135]. Therapeutic studies investigating pharmaceutical or interventional therapies in MINOCA patients will shed more light on the underlying mechanisms and their impact on prognosis.
8. Conclusions
MINOCA with ischemic but non-atherosclerotic cause is an increasingly recognized clinical entity associated with increased risk of MACE. Prompt diagnosis including multimodality imaging and biomarkers is of utmost importance to uncover the underlying cause. Treatment, though often empirical, is paramount and can be effective for symptoms amelioration once the cause is established. Several prognostic factors of morbidity and mortality in AMI-CAD patients have been identified to correlate with MINOCA patients, especially inflammatory markers. However, more investigation will shed light on the clinical course of MINOCA. A significant knowledge gap persists regarding diagnostic methods and management of patients with MINOCA. Therefore, future research should focus on those two domains: a) a multimodality diagnostic approach should be employed for prompt recognition of MINOCA. b) targeted evidence-based treatment should be instituted in order to prevent MACE and improve survival. Overall, the multifaceted nature, the demanding diverse diagnostic tools and the yet not fully clarified therapeutic strategies, make MINOCA management a significant clinical challenge.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, NPEK, SS; methodology, EK, DK; validation, NPEK NP; formal analysis, CP; investigation, EK, DK, TP, PK; resources, TP.; data curation, EK, DK, TP, PK; writing—original draft preparation, EK, DK, TP, PK.; writing—review and editing, NPEK, NP, CP, SS visualization, CP, NP, SS.; supervision, NPEK.; project administration, NPEK; funding acquisition, NPEK. All authors have read and agreed to the published version of the manuscript.”
Funding
This research was funded by the University of Cyprus, as an internal Research project, grant number “128 IAT- 2020”
Data Availability Statement
Not applicable.
Conflicts of Interest
None
References
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; Group, E.S.C.S.D. Fourth universal definition of myocardial infarction (2018). Eur Heart J 2019, 40, 237–269. [Google Scholar] [CrossRef] [PubMed]
- Pasupathy, S.; Tavella, R.; McRae, S.; Beltrame, J.F. Myocardial Infarction With Non-obstructive Coronary Arteries - Diagnosis and Management. Eur Cardiol 2015, 10, 79–82. [Google Scholar] [CrossRef]
- Boivin-Proulx, L.A.; Haddad, K.; Lombardi, M.; Chong, A.Y.; Escaned, J.; Mukherjee, S.; Forcillo, J.; Potter, B.J.; Coutinho, T.; Pacheco, C. Pathophysiology of Myocardial Infarction With Nonobstructive Coronary Artery Disease: A Contemporary Systematic Review. CJC Open 2024, 6, 380–390. [Google Scholar] [CrossRef] [PubMed]
- Choo, E.H.; Chang, K.; Lee, K.Y.; Lee, D.; Kim, J.G.; Ahn, Y.; Kim, Y.J.; Chae, S.C.; Cho, M.C.; Kim, C.J.; et al. Prognosis and Predictors of Mortality in Patients Suffering Myocardial Infarction With Non-Obstructive Coronary Arteries. J Am Heart Assoc 2019, 8, e011990. [Google Scholar] [CrossRef] [PubMed]
- Dreyer, R.P.; Tavella, R.; Curtis, J.P.; Wang, Y.; Pauspathy, S.; Messenger, J.; Rumsfeld, J.S.; Maddox, T.M.; Krumholz, H.M.; Spertus, J.A.; et al. Myocardial infarction with non-obstructive coronary arteries as compared with myocardial infarction and obstructive coronary disease: outcomes in a Medicare population. Eur Heart J 2020, 41, 870–878. [Google Scholar] [CrossRef] [PubMed]
- Eggers, K.M.; Hjort, M.; Baron, T.; Jernberg, T.; Nordenskjold, A.M.; Tornvall, P.; Lindahl, B. Morbidity and cause-specific mortality in first-time myocardial infarction with nonobstructive coronary arteries. J Intern Med 2019, 285, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Ishii, M.; Kaikita, K.; Sakamoto, K.; Seki, T.; Kawakami, K.; Nakai, M.; Sumita, Y.; Nishimura, K.; Miyamoto, Y.; Noguchi, T.; et al. Characteristics and in-hospital mortality of patients with myocardial infarction in the absence of obstructive coronary artery disease in super-aging society. Int J Cardiol 2020, 301, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Pelliccia, F.; Pasceri, V.; Niccoli, G.; Tanzilli, G.; Speciale, G.; Gaudio, C.; Crea, F.; Camici, P.G. Predictors of Mortality in Myocardial Infarction and Nonobstructed Coronary Arteries: A Systematic Review and Meta-Regression. Am J Med 2020, 133, 73–83.e74. [Google Scholar] [CrossRef] [PubMed]
- Bainey, K.R.; Welsh, R.C.; Alemayehu, W.; Westerhout, C.M.; Traboulsi, D.; Anderson, T.; Brass, N.; Armstrong, P.W.; Kaul, P. Population-level incidence and outcomes of myocardial infarction with non-obstructive coronary arteries (MINOCA): Insights from the Alberta contemporary acute coronary syndrome patients invasive treatment strategies (COAPT) study. Int J Cardiol 2018, 264, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Barr, P.R.; Harrison, W.; Smyth, D.; Flynn, C.; Lee, M.; Kerr, A.J. Myocardial Infarction Without Obstructive Coronary Artery Disease is Not a Benign Condition (ANZACS-QI 10). Heart Lung Circ 2018, 27, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Pasupathy, S.; Lindahl, B.; Litwin, P.; Tavella, R.; Williams, M.J.A.; Air, T.; Zeitz, C.; Smilowitz, N.R.; Reynolds, H.R.; Eggers, K.M.; et al. Survival in Patients With Suspected Myocardial Infarction With Nonobstructive Coronary Arteries: A Comprehensive Systematic Review and Meta-Analysis From the MINOCA Global Collaboration. Circ Cardiovasc Qual Outcomes 2021, 14, e007880. [Google Scholar] [CrossRef] [PubMed]
- Pasupathy, S.; Air, T.; Dreyer, R.P.; Tavella, R.; Beltrame, J.F. Systematic review of patients presenting with suspected myocardial infarction and nonobstructive coronary arteries. Circulation 2015, 131, 861–870. [Google Scholar] [CrossRef] [PubMed]
- Smilowitz, N.R.; Mahajan, A.M.; Roe, M.T.; Hellkamp, A.S.; Chiswell, K.; Gulati, M.; Reynolds, H.R. Mortality of Myocardial Infarction by Sex, Age, and Obstructive Coronary Artery Disease Status in the ACTION Registry-GWTG (Acute Coronary Treatment and Intervention Outcomes Network Registry-Get With the Guidelines). Circ Cardiovasc Qual Outcomes 2017, 10, e003443. [Google Scholar] [CrossRef] [PubMed]
- Mileva, N.; Paolisso, P.; Gallinoro, E.; Fabbricatore, D.; Munhoz, D.; Bergamaschi, L.; Belmonte, M.; Panayotov, P.; Pizzi, C.; Barbato, E.; et al. Diagnostic and Prognostic Role of Cardiac Magnetic Resonance in MINOCA: Systematic Review and Meta-Analysis. JACC Cardiovasc Imaging 2023, 16, 376–389. [Google Scholar] [CrossRef] [PubMed]
- Parwani, P.; Kang, N.; Safaeipour, M.; Mamas, M.A.; Wei, J.; Gulati, M.; Naidu, S.S.; Merz, N.B. Contemporary Diagnosis and Management of Patients with MINOCA. Curr Cardiol Rep 2023, 25, 561–570. [Google Scholar] [CrossRef] [PubMed]
- Gulati, M.; Levy, P.D.; Mukherjee, D.; Amsterdam, E.; Bhatt, D.L.; Birtcher, K.K.; Blankstein, R.; Boyd, J.; Bullock-Palmer, R.P.; Conejo, T.; et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 144, e368–e454. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Zhang, G.; Li, Z.; Li, D.; Chen, R.; Huang, C.; Li, Y.; Li, B.; Yu, H.; Chu, X.M. MINOCA biomarkers: Non-atherosclerotic aspects. Clin Chim Acta 2023, 551, 117613. [Google Scholar] [CrossRef] [PubMed]
- Fatima, L.; Goyal, A.; Yakkali, S.; Jain, H.; Raza, F.A.; Peer, T.; Kanagala, S.G.; Sohail, A.H.; Malik, J. Precision medicine in Myocardial Infarction With Non-obstructive Coronary Disease (MINOCA): A comprehensive review. Curr Probl Cardiol 2024, 49, 102185. [Google Scholar] [CrossRef] [PubMed]
- Lindahl, B.; Baron, T.; Albertucci, M.; Prati, F. Myocardial infarction with non-obstructive coronary artery disease. EuroIntervention 2021, 17, e875–e887. [Google Scholar] [CrossRef] [PubMed]
- Tamis-Holland, J.E.; Jneid, H.; Reynolds, H.R.; Agewall, S.; Brilakis, E.S.; Brown, T.M.; Lerman, A.; Cushman, M.; Kumbhani, D.J.; Arslanian-Engoren, C.; et al. Contemporary Diagnosis and Management of Patients With Myocardial Infarction in the Absence of Obstructive Coronary Artery Disease: A Scientific Statement From the American Heart Association. Circulation 2019, 139, e891–e908. [Google Scholar] [CrossRef] [PubMed]
- Agewall, S.; Beltrame, J.F.; Reynolds, H.R.; Niessner, A.; Rosano, G.; Caforio, A.L.; De Caterina, R.; Zimarino, M.; Roffi, M.; Kjeldsen, K.; et al. ESC working group position paper on myocardial infarction with non-obstructive coronary arteries. Eur Heart J 2017, 38, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, H.R.; Srichai, M.B.; Iqbal, S.N.; Slater, J.N.; Mancini, G.B.; Feit, F.; Pena-Sing, I.; Axel, L.; Attubato, M.J.; Yatskar, L.; et al. Mechanisms of myocardial infarction in women without angiographically obstructive coronary artery disease. Circulation 2011, 124, 1414–1425. [Google Scholar] [CrossRef] [PubMed]
- Vergallo, R.; Ren, X.; Yonetsu, T.; Kato, K.; Uemura, S.; Yu, B.; Jia, H.; Abtahian, F.; Aguirre, A.D.; Tian, J.; et al. Pancoronary plaque vulnerability in patients with acute coronary syndrome and ruptured culprit plaque: a 3-vessel optical coherence tomography study. Am Heart J 2014, 167, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Taruya, A.; Tanaka, A.; Nishiguchi, T.; Ozaki, Y.; Kashiwagi, M.; Yamano, T.; Matsuo, Y.; Ino, Y.; Kitabata, H.; Takemoto, K.; et al. Lesion characteristics and prognosis of acute coronary syndrome without angiographically significant coronary artery stenosis. Eur Heart J Cardiovasc Imaging 2020, 21, 202–209. [Google Scholar] [CrossRef]
- Johnson, T.W.; Raber, L.; di Mario, C.; Bourantas, C.; Jia, H.; Mattesini, A.; Gonzalo, N.; de la Torre Hernandez, J.M.; Prati, F.; Koskinas, K.; et al. Clinical use of intracoronary imaging. Part 2: acute coronary syndromes, ambiguous coronary angiography findings, and guiding interventional decision-making: an expert consensus document of the European Association of Percutaneous Cardiovascular Interventions. Eur Heart J 2019, 40, 2566–2584. [Google Scholar] [CrossRef] [PubMed]
- Zakai, N.A.; McClure, L.A. Racial differences in venous thromboembolism. J Thromb Haemost 2011, 9, 1877–1882. [Google Scholar] [CrossRef] [PubMed]
- Tomaiuolo, R.; Bellia, C.; Caruso, A.; Di Fiore, R.; Quaranta, S.; Noto, D.; Cefalu, A.B.; Di Micco, P.; Zarrilli, F.; Castaldo, G.; et al. Prothrombotic gene variants as risk factors of acute myocardial infarction in young women. J Transl Med 2012, 10, 235. [Google Scholar] [CrossRef] [PubMed]
- Stepien, K.; Nowak, K.; Wypasek, E.; Zalewski, J.; Undas, A. High prevalence of inherited thrombophilia and antiphospholipid syndrome in myocardial infarction with non-obstructive coronary arteries: Comparison with cryptogenic stroke. Int J Cardiol 2019, 290, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Mariotte, E.; Blet, A.; Galicier, L.; Darmon, M.; Parquet, N.; Lengline, E.; Boutboul, D.; Canet, E.; Traineau, R.; Schlemmer, B.; et al. Unresponsive thrombotic thrombocytopenic purpura in critically ill adults. Intensive Care Med 2013, 39, 1272–1281. [Google Scholar] [CrossRef] [PubMed]
- Cushman, M. Thrombophilia testing in women with venous thrombosis: the 4 P’s approach. Clin Chem 2014, 60, 134–137. [Google Scholar] [CrossRef] [PubMed]
- Montone, R.A.; Niccoli, G.; Fracassi, F.; Russo, M.; Gurgoglione, F.; Camma, G.; Lanza, G.A.; Crea, F. Patients with acute myocardial infarction and non-obstructive coronary arteries: safety and prognostic relevance of invasive coronary provocative tests. Eur Heart J 2018, 39, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Beltrame, J.F.; Sasayama, S.; Maseri, A. Racial heterogeneity in coronary artery vasomotor reactivity: differences between Japanese and Caucasian patients. J Am Coll Cardiol 1999, 33, 1442–1452. [Google Scholar] [CrossRef] [PubMed]
- Kaski, J.C.; Crea, F.; Meran, D.; Rodriguez, L.; Araujo, L.; Chierchia, S.; Davies, G.; Maseri, A. Local coronary supersensitivity to diverse vasoconstrictive stimuli in patients with variant angina. Circulation 1986, 74, 1255–1265. [Google Scholar] [CrossRef]
- Beltrame, J.F.; Psaltis, P.J. The Forgotten Vascular Layer in the Forgotten Coronary Disorder. J Am Coll Cardiol 2018, 71, 426–428. [Google Scholar] [CrossRef] [PubMed]
- Nam, P.; Choi, B.G.; Choi, S.Y.; Byun, J.K.; Mashaly, A.; Park, Y.; Jang, W.Y.; Kim, W.; Choi, J.Y.; Park, E.J.; et al. The impact of myocardial bridge on coronary artery spasm and long-term clinical outcomes in patients without significant atherosclerotic stenosis. Atherosclerosis 2018, 270, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.S.H. Spontaneous Coronary-Artery Dissection. N Engl J Med 2020, 383, 2358–2370. [Google Scholar] [CrossRef] [PubMed]
- Paulo, M.; Sandoval, J.; Lennie, V.; Dutary, J.; Medina, M.; Gonzalo, N.; Jimenez-Quevedo, P.; Escaned, J.; Banuelos, C.; Hernandez, R.; et al. Combined use of OCT and IVUS in spontaneous coronary artery dissection. JACC Cardiovasc Imaging 2013, 6, 830–832. [Google Scholar] [CrossRef] [PubMed]
- Saw, J.; Aymong, E.; Sedlak, T.; Buller, C.E.; Starovoytov, A.; Ricci, D.; Robinson, S.; Vuurmans, T.; Gao, M.; Humphries, K.; et al. Spontaneous coronary artery dissection: association with predisposing arteriopathies and precipitating stressors and cardiovascular outcomes. Circ Cardiovasc Interv 2014, 7, 645–655. [Google Scholar] [CrossRef] [PubMed]
- Tweet, M.S.; Hayes, S.N.; Pitta, S.R.; Simari, R.D.; Lerman, A.; Lennon, R.J.; Gersh, B.J.; Khambatta, S.; Best, P.J.; Rihal, C.S.; et al. Clinical features, management, and prognosis of spontaneous coronary artery dissection. Circulation 2012, 126, 579–588. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.N.; Tweet, M.S.; Adlam, D.; Kim, E.S.H.; Gulati, R.; Price, J.E.; Rose, C.H. Spontaneous Coronary Artery Dissection: JACC State-of-the-Art Review. J Am Coll Cardiol 2020, 76, 961–984. [Google Scholar] [CrossRef] [PubMed]
- Cerrato, E.; Giacobbe, F.; Rolfo, C.; Quadri, G.; Tomassini, F.; Ferrari, F.; Mariani, F.; Anselmino, M.; Bianco, M.; Belliggiano, D.; et al. Role of Invasive and Non-invasive Imaging Tools in the Diagnosis and Optimal Treatment of Patients with Spontaneous Coronary Artery Dissection. Curr Cardiol Rep 2019, 21, 122. [Google Scholar] [CrossRef]
- Beltrame, J.F.; Crea, F.; Camici, P. Advances in coronary microvascular dysfunction. Heart Lung Circ 2009, 18, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Godo, S.; Suda, A.; Takahashi, J.; Yasuda, S.; Shimokawa, H. Coronary Microvascular Dysfunction. Arterioscler Thromb Vasc Biol 2021, 41, 1625–1637. [Google Scholar] [CrossRef]
- Beltrame, J.F.; Limaye, S.B.; Horowitz, J.D. The coronary slow flow phenomenon--a new coronary microvascular disorder. Cardiology 2002, 97, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Mauricio, R.; Srichai, M.B.; Axel, L.; Hochman, J.S.; Reynolds, H.R. Stress Cardiac MRI in Women With Myocardial Infarction and Nonobstructive Coronary Artery Disease. Clin Cardiol 2016, 39, 596–602. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.H.; Ong, G.J.; Girolamo, O.C.; De Menezes Caceres, V.; Muminovic, A.; Chirkov, Y.Y.; Horowitz, J.D. Angina due to coronary artery spasm (variant angina): diagnosis and intervention strategies. Expert Rev Cardiovasc Ther 2021, 19, 917–927. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, J.I.; Buckberg, G.D. The myocardial oxygen supply:demand index revisited. J Am Heart Assoc 2014, 3, e000285. [Google Scholar] [CrossRef] [PubMed]
- Rafiudeen, R.; Barlis, P.; White, H.D.; van Gaal, W. Type 2 MI and Myocardial Injury in the Era of High-sensitivity Troponin. Eur Cardiol 2022, 17, e03. [Google Scholar] [CrossRef] [PubMed]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; Executive Group on behalf of the Joint European Society of Cardiology /American College of Cardiology /American Heart Association /World Heart Federation Task Force for the Universal Definition of Myocardial, I. Fourth Universal Definition of Myocardial Infarction (2018). Circulation 2018, 138, e618–e651. [Google Scholar] [CrossRef]
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.A.; Dweck, M.R.; Galbraith, M.; et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J 2023, 44, 3720–3826. [Google Scholar] [CrossRef] [PubMed]
- Rallidis, L.S.; Xenogiannis, I.; Brilakis, E.S.; Bhatt, D.L. Causes, Angiographic Characteristics, and Management of Premature Myocardial Infarction: JACC State-of-the-Art Review. J Am Coll Cardiol 2022, 79, 2431–2449. [Google Scholar] [CrossRef] [PubMed]
- Alves da Silva, P.; Bucciarelli-Ducci, C.; Sousa, A. Myocardial infarction with non-obstructive coronary arteries: Etiology, diagnosis, treatment and prognosis. Rev Port Cardiol 2023, 42, 655–666. [Google Scholar] [CrossRef] [PubMed]
- Pustjens, T.F.S.; Meerman, A.; Vranken, N.P.A.; Ruiters, A.W.; Gho, B.; Stein, M.; Ilhan, M.; Veenstra, L.; Winkler, P.; Lux, A.; et al. Importance of confirming the underlying diagnosis in patients with myocardial infarction and non-obstructive coronary arteries (MINOCA): a single-centre retrospective cohort study. BMC Cardiovasc Disord 2021, 21, 357. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, C., II; Perez-Aybar, A.E.; Roman-Ramos, J.A. MINOCA: A Working Diagnosis. Cureus 2023, 15, e49695. [Google Scholar] [CrossRef]
- Occhipinti, G.; Bucciarelli-Ducci, C.; Capodanno, D. Diagnostic pathways in myocardial infarction with non-obstructive coronary artery disease (MINOCA). Eur Heart J Acute Cardiovasc Care 2021, 10, 813–822. [Google Scholar] [CrossRef]
- Almeida, A.G. MINOCA and INOCA: Role in Heart Failure. Curr Heart Fail Rep 2023, 20, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Bakhshi, H.; Gibson, C.M. MINOCA: Myocardial infarction no obstructive coronary artery disease. Am Heart J Plus 2023, 33, 100312. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, H.R.; Smilowitz, N.R. Myocardial Infarction with Nonobstructive Coronary Arteries. Annu Rev Med 2023, 74, 171–188. [Google Scholar] [CrossRef] [PubMed]
- Rinaldi, R.; Princi, G.; La Vecchia, G.; Bonanni, A.; Chiariello, G.A.; Candreva, A.; Gragnano, F.; Calabro, P.; Crea, F.; Montone, R.A. MINOCA Associated with a Myocardial Bridge: Pathogenesis, Diagnosis and Treatment. J Clin Med 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Marrone, A.; Pavasini, R.; Scollo, E.; Gibiino, F.; Pompei, G.; Caglioni, S.; Biscaglia, S.; Campo, G.; Tebaldi, M. Acetylcholine Use in Modern Cardiac Catheterization Laboratories: A Systematic Review. J Clin Med 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Iwanczyk, S.; Wozniak, P.; Araszkiewicz, A.; Grygier, M.; Klotzka, A.; Lesiak, M. Optical coherence tomography in the diagnosis of myocardial infarction with non-obstructive coronary arteries. Postepy Kardiol Interwencyjnej 2022, 18, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Sucato, V.; Testa, G.; Puglisi, S.; Evola, S.; Galassi, A.R.; Novo, G. Myocardial infarction with non-obstructive coronary arteries (MINOCA): Intracoronary imaging-based diagnosis and management. J Cardiol 2021, 77, 444–451. [Google Scholar] [CrossRef] [PubMed]
- Borzillo, I.; De Filippo, O.; Manai, R.; Bruno, F.; Ravetti, E.; Galanti, A.A.; Vergallo, R.; Porto, I.; De Ferrari, G.M.; D’Ascenzo, F. Role of Intracoronary Imaging in Myocardial Infarction with Non-Obstructive Coronary Disease (MINOCA): A Review. J Clin Med 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Bryniarski, K.; Gasior, P.; Legutko, J.; Makowicz, D.; Kedziora, A.; Szolc, P.; Bryniarski, L.; Kleczynski, P.; Jang, I.K. OCT Findings in MINOCA. J Clin Med 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Del Buono, M.G.; Montone, R.A.; Iannaccone, G.; Meucci, M.C.; Rinaldi, R.; D’Amario, D.; Niccoli, G. Diagnostic work-up and therapeutic implications in MINOCA: need for a personalized approach. Future Cardiol 2021, 17, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Vancheri, F.; Longo, G.; Vancheri, S.; Henein, M. Coronary Microvascular Dysfunction. J Clin Med 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- Rampidis, G.P.; Kampaktsis, P.; Kouskouras, K.; Samaras, A.; Benetos, G.; Giannopoulos, A.; Karamitsos, T.; Kallifatidis, A.; Samaras, A.; Vogiatzis, I.; et al. Role of cardiac CT in the diagnostic evaluation and risk stratification of patients with myocardial infarction and non-obstructive coronary arteries (MINOCA): rationale and design of the MINOCA-GR study. BMJ Open 2022, 12, e054698. [Google Scholar] [CrossRef] [PubMed]
- Pergola, V.; Previtero, M.; Cecere, A.; Storer, V.; Castiello, T.; Baritussio, A.; Cabrelle, G.; Mele, D.; Motta, R.; Caforio, A.P.; et al. Clinical Value and Time Course of Pericoronary Fat Inflammation in Patients with Angiographically Nonobstructive Coronaries: A Preliminary Report. J Clin Med 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Daneshrad, J.A.; Ordovas, K.; Sierra-Galan, L.M.; Hays, A.G.; Mamas, M.A.; Bucciarelli-Ducci, C.; Parwani, P. Role of Cardiac Magnetic Resonance Imaging in the Evaluation of MINOCA. J Clin Med 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Gatti, M.; Carisio, A.; D’Angelo, T.; Darvizeh, F.; Dell’Aversana, S.; Tore, D.; Centonze, M.; Faletti, R. Cardiovascular magnetic resonance in myocardial infarction with non-obstructive coronary arteries patients: A review. World J Cardiol 2020, 12, 248–261. [Google Scholar] [CrossRef] [PubMed]
- Herling de Oliveira, L.L.; Correia, V.M.; Nicz, P.F.G.; Soares, P.R.; Scudeler, T.L. MINOCA: One Size Fits All? Probably Not-A Review of Etiology, Investigation, and Treatment. J Clin Med 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Lintingre, P.F.; Nivet, H.; Clement-Guinaudeau, S.; Camaioni, C.; Sridi, S.; Corneloup, O.; Gerbaud, E.; Coste, P.; Dournes, G.; Latrabe, V.; et al. High-Resolution Late Gadolinium Enhancement Magnetic Resonance for the Diagnosis of Myocardial Infarction With Nonobstructed Coronary Arteries. JACC Cardiovasc Imaging 2020, 13, 1135–1148. [Google Scholar] [CrossRef] [PubMed]
- Machanahalli Balakrishna, A.; Ismayl, M.; Thandra, A.; Walters, R.; Ganesan, V.; Anugula, D.; Shah, D.J.; Aboeata, A. Diagnostic Value of Cardiac Magnetic Resonance Imaging and Intracoronary Optical Coherence Tomography in Patients With a Working Diagnosis of Myocardial Infarction With Non-obstructive Coronary Arteries - A Systematic Review and Meta-analysis. Curr Probl Cardiol 2023, 48, 101126. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, J.; Onuma, S.; Hao, K.; Godo, S.; Shiroto, T.; Yasuda, S. Pathophysiology and diagnostic pathway of myocardial infarction with non-obstructive coronary arteries. J Cardiol 2024, 83, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Abdu, F.A.; Mohammed, A.Q.; Liu, L.; Xu, Y.; Che, W. Myocardial Infarction with Nonobstructive Coronary Arteries (MINOCA): A Review of the Current Position. Cardiology 2020, 145, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Rao, K.; De Silva, K.; Sood, A.; Denniss, A.R.; Hsu, C.J. Predicting Patients With Troponin Positive Chest Pain and Unobstructed Coronary Arteries With Electrocardiogram, Troponin Kinetics and GRACE Score. Heart Lung Circ 2022, 31, 1219–1227. [Google Scholar] [CrossRef] [PubMed]
- Mitsis, A.; Kadoglou, N.P.E.; Lambadiari, V.; Alexiou, S.; Theodoropoulos, K.C.; Avraamides, P.; Kassimis, G. Prognostic role of inflammatory cytokines and novel adipokines in acute myocardial infarction: An updated and comprehensive review. Cytokine 2022, 153, 155848. [Google Scholar] [CrossRef] [PubMed]
- Kadoglou, N.P.; Tahmatzidis, D.K.; Giannakoulas, C.; Kapelouzou, A.; Gkontopoulos, A.; Parissis, J.; Lampropoulos, S.; Kottas, G. Serum levels of novel adipokines, omentin-1 and chemerin, in patients with acute myocardial infarction: KOZANI STUDY. J Cardiovasc Med (Hagerstown) 2015, 16, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Hjort, M.; Eggers, K.M.; Lakic, T.G.; Lindback, J.; Budaj, A.; Cornel, J.H.; Giannitsis, E.; Katus, H.A.; Siegbahn, A.; Storey, R.F.; et al. Biomarker Concentrations and Their Temporal Changes in Patients With Myocardial Infarction and Nonobstructive Compared With Obstructive Coronary Arteries: Results From the PLATO Trial. J Am Heart Assoc 2023, 12, e027466. [Google Scholar] [CrossRef] [PubMed]
- Hjort, M.; Eggers, K.M.; Lindhagen, L.; Agewall, S.; Brolin, E.B.; Collste, O.; Daniel, M.; Ekenback, C.; Frick, M.; Henareh, L.; et al. Increased Inflammatory Activity in Patients 3 Months after Myocardial Infarction with Nonobstructive Coronary Arteries. Clin Chem 2019, 65, 1023–1030. [Google Scholar] [CrossRef] [PubMed]
- Daniel, M.; Ekenback, C.; Agewall, S.; Brolin, E.B.; Caidahl, K.; Cederlund, K.; Collste, O.; Eurenius, L.; Frick, M.; Younis-Hassan, S.; et al. Risk Factors and Markers for Acute Myocardial Infarction With Angiographically Normal Coronary Arteries. Am J Cardiol 2015, 116, 838–844. [Google Scholar] [CrossRef] [PubMed]
- Ryabov, V.V.; Vorobeva, D.A.; Kologrivova, I.V.; Suslova, T.E. Pro-Inflammatory Biomarkers and Progression of Atherosclerosis in Patients with Myocardial Infarction with Non-Obstructive Coronary Artery Disease: 1-Year Follow-Up. J Pers Med 2023, 13. [Google Scholar] [CrossRef] [PubMed]
- Stangret, A.; Dykacz, W.; Jablonski, K.; Wesolowska, A.; Klimczak-Tomaniak, D.; Kochman, J.; Tomaniak, M. The cytokine trio - visfatin, placental growth factor and fractalkine - and their role in myocardial infarction with non-obstructive coronary arteries (MINOCA). Cytokine Growth Factor Rev 2023, 74, 76–85. [Google Scholar] [CrossRef] [PubMed]
- Paolisso, P.; Foa, A.; Bergamaschi, L.; Donati, F.; Fabrizio, M.; Chiti, C.; Angeli, F.; Toniolo, S.; Stefanizzi, A.; Armillotta, M.; et al. Hyperglycemia, inflammatory response and infarct size in obstructive acute myocardial infarction and MINOCA. Cardiovasc Diabetol 2021, 20, 33. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.; Xu, H.; Ma, W.; Yuan, J.; Yu, M. Remnant Cholesterol Predicts Risk of Cardiovascular Events in Patients With Myocardial Infarction With Nonobstructive Coronary Arteries. J Am Heart Assoc 2022, 11, e024366. [Google Scholar] [CrossRef] [PubMed]
- Ma, W.; Gao, S.; Huang, S.; Yuan, J.; Yu, M. Hyperuricemia as a prognostic marker for long-term outcomes in patients with myocardial infarction with nonobstructive coronary arteries. Nutr Metab (Lond) 2021, 18, 107. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.; Ma, W.; Huang, S.; Lin, X.; Yu, M. Effect of Lipoprotein (a) Levels on Long-term Cardiovascular Outcomes in Patients with Myocardial Infarction with Nonobstructive Coronary Arteries. Am J Cardiol 2021, 152, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Guler, E.; Guler, G.B.; Kizilirmak, F.; Batgerel, U.; Demir, G.G.; Gunes, H.M.; Karaca, O.; Ozcan, O.; Barutcu, I.; Turkmen, M.M.; et al. Evaluation of adiponectin and lipoprotein(a) levels in cardiac syndrome X. Herz 2015, 40 Suppl 3, 291–297. [Google Scholar] [CrossRef]
- Lin, Y.K.; Yeh, C.T.; Kuo, K.T.; Fong, I.H.; Yadav, V.K.; Kounis, N.G.; Hu, P.; Hung, M.Y. Apolipoprotein (a)/Lipoprotein(a)-Induced Oxidative-Inflammatory alpha7-nAChR/p38 MAPK/IL-6/RhoA-GTP Signaling Axis and M1 Macrophage Polarization Modulate Inflammation-Associated Development of Coronary Artery Spasm. Oxid Med Cell Longev 2022, 2022, 9964689. [Google Scholar] [CrossRef] [PubMed]
- Severino, P.; D’Amato, A.; Prosperi, S.; Myftari, V.; Colombo, L.; Tomarelli, E.; Piccialuti, A.; Di Pietro, G.; Birtolo, L.I.; Maestrini, V.; et al. Myocardial Infarction with Non-Obstructive Coronary Arteries (MINOCA): Focus on Coronary Microvascular Dysfunction and Genetic Susceptibility. J Clin Med 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Halcox, J.P.; Nour, K.R.; Zalos, G.; Quyyumi, A.A. Endogenous endothelin in human coronary vascular function: differential contribution of endothelin receptor types A and B. Hypertension 2007, 49, 1134–1141. [Google Scholar] [CrossRef] [PubMed]
- Ford, T.J.; Corcoran, D.; Padmanabhan, S.; Aman, A.; Rocchiccioli, P.; Good, R.; McEntegart, M.; Maguire, J.J.; Watkins, S.; Eteiba, H.; et al. Genetic dysregulation of endothelin-1 is implicated in coronary microvascular dysfunction. Eur Heart J 2020, 41, 3239–3252. [Google Scholar] [CrossRef]
- Cox, I.D.; Botker, H.E.; Bagger, J.P.; Sonne, H.S.; Kristensen, B.O.; Kaski, J.C. Elevated endothelin concentrations are associated with reduced coronary vasomotor responses in patients with chest pain and normal coronary arteriograms. J Am Coll Cardiol 1999, 34, 455–460. [Google Scholar] [CrossRef]
- Verstraeten, A.; Perik, M.; Baranowska, A.A.; Meester, J.A.N.; Van Den Heuvel, L.; Bastianen, J.; Kempers, M.; Krapels, I.P.C.; Maas, A.; Rideout, A.; et al. Enrichment of Rare Variants in Loeys-Dietz Syndrome Genes in Spontaneous Coronary Artery Dissection but Not in Severe Fibromuscular Dysplasia. Circulation 2020, 142, 1021–1024. [Google Scholar] [CrossRef] [PubMed]
- Chung, A.W.; Au Yeung, K.; Sandor, G.G.; Judge, D.P.; Dietz, H.C.; van Breemen, C. Loss of elastic fiber integrity and reduction of vascular smooth muscle contraction resulting from the upregulated activities of matrix metalloproteinase-2 and -9 in the thoracic aortic aneurysm in Marfan syndrome. Circ Res 2007, 101, 512–522. [Google Scholar] [CrossRef] [PubMed]
- Saw, J.; Yang, M.-L.; Trinder, M.; Tcheandjieu, C.; Xu, C.; Starovoytov, A.; Birt, I.; Mathis, M.R.; Hunker, K.L.; Schmidt, E.M.; et al. Chromosome 1q21.2 and additional loci influence risk of spontaneous coronary artery dissection and myocardial infarction. Nature Communications 2020, 11, 4432. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Chen, Y.; Li, Y.; Li, Z.; Li, C.; Yu, T.; Xiao, L.; Yu, B.; Zhao, H.; Tao, M.; et al. Association of TSR1 Variants and Spontaneous Coronary Artery Dissection. J Am Coll Cardiol 2019, 74, 167–176. [Google Scholar] [CrossRef]
- Lozano-Prieto, M.; Adlam, D.; Garcia-Guimaraes, M.; Sanz-Garcia, A.; Vera-Tome, P.; Rivero, F.; Cuesta, J.; Bastante, T.; Baranowska-Clarke, A.A.; Vara, A.; et al. Differential miRNAs in acute spontaneous coronary artery dissection: Pathophysiological insights from a potential biomarker. EBioMedicine 2021, 66, 103338. [Google Scholar] [CrossRef]
- Li, L.; Liao, J.; Yuan, Q.; Hong, X.; Li, J.; Peng, Y.; He, M.; Zhu, H.; Zhu, M.; Hou, F.F.; et al. Fibrillin-1-enriched microenvironment drives endothelial injury and vascular rarefaction in chronic kidney disease. Sci Adv 2021, 7. [Google Scholar] [CrossRef]
- Margaritis, M.; Saini, F.; Baranowska-Clarke, A.A.; Parsons, S.; Vink, A.; Budgeon, C.; Allcock, N.; Wagner, B.E.; Samani, N.J.; von der Thusen, J.; et al. Vascular histopathology and connective tissue ultrastructure in spontaneous coronary artery dissection: pathophysiological and clinical implications. Cardiovasc Res 2022, 118, 1835–1848. [Google Scholar] [CrossRef]
- Mosaddeghzadeh, N.; Ahmadian, M.R. The RHO Family GTPases: Mechanisms of Regulation and Signaling. Cells 2021, 10. [Google Scholar] [CrossRef]
- Franczyk, B.; Dybiec, J.; Frak, W.; Krzeminska, J.; Kucmierz, J.; Mlynarska, E.; Szlagor, M.; Wronka, M.; Rysz, J. Cellular Mechanisms of Coronary Artery Spasm. Biomedicines 2022, 10. [Google Scholar] [CrossRef] [PubMed]
- Lanza, G.A.; Careri, G.; Crea, F. Mechanisms of coronary artery spasm. Circulation 2011, 124, 1774–1782. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, Y.; Yasuda, S.; Aizawa, K.; Tsuburaya, R.; Ito, Y.; Takeda, M.; Nakayama, M.; Ito, K.; Takahashi, J.; Shimokawa, H. Enhanced Rho-kinase activity in circulating neutrophils of patients with vasospastic angina: a possible biomarker for diagnosis and disease activity assessment. J Am Coll Cardiol 2011, 58, 1231–1237. [Google Scholar] [CrossRef] [PubMed]
- Planer, D.; Mehran, R.; Ohman, E.M.; White, H.D.; Newman, J.D.; Xu, K.; Stone, G.W. Prognosis of patients with non-ST-segment-elevation myocardial infarction and nonobstructive coronary artery disease: propensity-matched analysis from the Acute Catheterization and Urgent Intervention Triage Strategy trial. Circ Cardiovasc Interv 2014, 7, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Kang, W.Y.; Jeong, M.H.; Ahn, Y.K.; Kim, J.H.; Chae, S.C.; Kim, Y.J.; Hur, S.H.; Seong, I.W.; Hong, T.J.; Choi, D.H.; et al. Are patients with angiographically near-normal coronary arteries who present as acute myocardial infarction actually safe? Int J Cardiol 2011, 146, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Ciliberti, G.; Coiro, S.; Tritto, I.; Benedetti, M.; Guerra, F.; Del Pinto, M.; Finocchiaro, G.; Cavallini, C.; Capucci, A.; Kaski, J.C.; et al. Predictors of poor clinical outcomes in patients with acute myocardial infarction and non-obstructed coronary arteries (MINOCA). Int J Cardiol 2018, 267, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Raparelli, V.; Elharram, M.; Shimony, A.; Eisenberg, M.J.; Cheema, A.N.; Pilote, L. Myocardial Infarction With No Obstructive Coronary Artery Disease: Angiographic and Clinical Insights in Patients With Premature Presentation. Can J Cardiol 2018, 34, 468–476. [Google Scholar] [CrossRef] [PubMed]
- Lindahl, B.; Baron, T.; Erlinge, D.; Hadziosmanovic, N.; Nordenskjold, A.; Gard, A.; Jernberg, T. Medical Therapy for Secondary Prevention and Long-Term Outcome in Patients With Myocardial Infarction With Nonobstructive Coronary Artery Disease. Circulation 2017, 135, 1481–1489. [Google Scholar] [CrossRef]
- Andersson, H.B.; Pedersen, F.; Engstrom, T.; Helqvist, S.; Jensen, M.K.; Jorgensen, E.; Kelbaek, H.; Rader, S.; Saunamaki, K.; Bates, E.; et al. Long-term survival and causes of death in patients with ST-elevation acute coronary syndrome without obstructive coronary artery disease. Eur Heart J 2018, 39, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Montenegro Sa, F.; Ruivo, C.; Santos, L.G.; Antunes, A.; Saraiva, F.; Soares, F.; Morais, J. Myocardial infarction with nonobstructive coronary arteries: a single-center retrospective study. Coron Artery Dis 2018, 29, 511–515. [Google Scholar] [CrossRef] [PubMed]
- Nordenskjold, A.M.; Baron, T.; Eggers, K.M.; Jernberg, T.; Lindahl, B. Predictors of adverse outcome in patients with myocardial infarction with non-obstructive coronary artery (MINOCA) disease. Int J Cardiol 2018, 261, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Abdu, F.A.; Liu, L.; Mohammed, A.Q.; Luo, Y.; Xu, S.; Auckle, R.; Xu, Y.; Che, W. Myocardial infarction with non-obstructive coronary arteries (MINOCA) in Chinese patients: Clinical features, treatment and 1 year follow-up. Int J Cardiol 2019, 287, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Blankstein, R.; Shaw, L.J.; Chandrashekhar, Y. The Promise of Imaging in MINOCA. JACC Cardiovasc Imaging 2019, 12, 2100–2102. [Google Scholar] [CrossRef] [PubMed]
- Hjort, M.; Lindahl, B.; Baron, T.; Jernberg, T.; Tornvall, P.; Eggers, K.M. Prognosis in relation to high-sensitivity cardiac troponin T levels in patients with myocardial infarction and non-obstructive coronary arteries. Am Heart J 2018, 200, 60–66. [Google Scholar] [CrossRef]
- Gurzau, D.; Sitar-Taut, A.; Caloian, B.; Gusetu, G.; Comsa, H.; Fringu, F.; Zdrenghea, D.; Pop, D. The Role of IL-6 and ET-1 in the Diagnosis of Coronary MicroVascular Disease in Women. J Pers Med 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Cenko, E.; Manfrini, O.; Morell, C.; Das, R.; Barth, J.H.; Hall, A.S.; Gale, C.P.; Bugiardini, R.; Methods, o.b.o.E.o.; Events, M.o.A.C. Angiotensin-converting enzyme inhibitor therapy in patients non-obstructive coronary artery disease. European Heart Journal 2013, 34. [Google Scholar] [CrossRef]
- Cespon Fernandez, M.; Abu-Assi, E.; Raposeiras Roubin, S.; Munoz Pousa, I.; Dominguez Rodriguez, L.M.; Dominguez Erquicia, P.; Cobas Paz, R.; Caneiro Queija, B.; Jamhour Chelh, K.; Perez Casares, L.E.; et al. P880 Cardiovascular mortality in patients with MINOCA and prognostic effect of statin treatment. European Heart Journal 2019, 40. [Google Scholar] [CrossRef]
- Bossard, M.; Yusuf, S.; Tanguay, J.F.; Faxon, D.P.; Boden, W.E.; Steg, P.G.; Granger, C.; Kastrati, A.; Budaj, A.; Di Pasquale, G.; et al. 2387Recurrent cardiovascular events and mortality in relation to antiplatelet therapy in patients with myocardial infarction without obstructive coronary artery disease (MINOCA). European Heart Journal 2019, 40. [Google Scholar] [CrossRef]
- Ishii, M.; Kaikita, K.; Sato, K.; Yamanaga, K.; Miyazaki, T.; Akasaka, T.; Tabata, N.; Arima, Y.; Sueta, D.; Sakamoto, K.; et al. Impact of aspirin on the prognosis in patients with coronary spasm without significant atherosclerotic stenosis. Int J Cardiol 2016, 220, 328–332. [Google Scholar] [CrossRef] [PubMed]
- Bossard, M.; Gao, P.; Boden, W.; Steg, G.; Tanguay, J.F.; Joyner, C.; Granger, C.B.; Kastrati, A.; Faxon, D.; Budaj, A.; et al. Antiplatelet therapy in patients with myocardial infarction without obstructive coronary artery disease. Heart 2021, 107, 1739–1747. [Google Scholar] [CrossRef]
- Roffi, M.; Patrono, C.; Collet, J.P.; Mueller, C.; Valgimigli, M.; Andreotti, F.; Bax, J.J.; Borger, M.A.; Brotons, C.; Chew, D.P.; et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur Heart J 2016, 37, 267–315. [Google Scholar] [CrossRef] [PubMed]
- Pustjens, T.F.S.; Appelman, Y.; Damman, P.; Ten Berg, J.M.; Jukema, J.W.; de Winter, R.J.; Agema, W.R.P.; van der Wielen, M.L.J.; Arslan, F.; Rasoul, S.; et al. Guidelines for the management of myocardial infarction/injury with non-obstructive coronary arteries (MINOCA): a position paper from the Dutch ACS working group. Neth Heart J 2020, 28, 116–130. [Google Scholar] [CrossRef] [PubMed]
- Niccoli, G.; Scalone, G.; Crea, F. Acute myocardial infarction with no obstructive coronary atherosclerosis: mechanisms and management. Eur Heart J 2015, 36, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Ceasovschih, A.; Mantzouranis, E.; Dimitriadis, K.; Sorodoc, V.; Vlachakis, P.K.; Karanikola, A.E.; Theofilis, P.; Koutsopoulos, G.; Drogkaris, S.; Andrikou, I.; et al. Coronary artery thromboembolism as a cause of myocardial infarction with non-obstructive coronary arteries (MINOCA). Hellenic J Cardiol 2024. [Google Scholar] [CrossRef] [PubMed]
- Pirozzolo, G.; Seitz, A.; Athanasiadis, A.; Bekeredjian, R.; Sechtem, U.; Ong, P. Microvascular spasm in non-ST-segment elevation myocardial infarction without culprit lesion (MINOCA). Clin Res Cardiol 2020, 109, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Offen, S.; Yang, C.; Saw, J. Spontaneous coronary artery dissection (SCAD): A contemporary review. Clin Cardiol 2024, 47, e24236. [Google Scholar] [CrossRef] [PubMed]
- Saw, J.; Humphries, K.; Aymong, E.; Sedlak, T.; Prakash, R.; Starovoytov, A.; Mancini, G.B.J. Spontaneous Coronary Artery Dissection: Clinical Outcomes and Risk of Recurrence. J Am Coll Cardiol 2017, 70, 1148–1158. [Google Scholar] [CrossRef] [PubMed]
- Lawton, J.S.; Tamis-Holland, J.E.; Bangalore, S.; Bates, E.R.; Beckie, T.M.; Bischoff, J.M.; Bittl, J.A.; Cohen, M.G.; DiMaio, J.M.; Don, C.W.; et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Journal of the American College of Cardiology 2022, 79, e21–e129. [Google Scholar] [CrossRef] [PubMed]
- Corban, M.T.; Hung, O.Y.; Eshtehardi, P.; Rasoul-Arzrumly, E.; McDaniel, M.; Mekonnen, G.; Timmins, L.H.; Lutz, J.; Guyton, R.A.; Samady, H. Myocardial bridging: contemporary understanding of pathophysiology with implications for diagnostic and therapeutic strategies. J Am Coll Cardiol 2014, 63, 2346–2355. [Google Scholar] [CrossRef] [PubMed]
- Yin, Y.; Fang, C.; Jiang, S.; Wang, J.; Wang, Y.; Guo, J.; Lei, F.; Sun, S.; Pei, X.; Jia, R.; et al. Optical Coherence Tomographic Features of Pancoronary Plaques in Patients With Acute Myocardial Infarction Caused by Layered Plaque Rupture Versus Layered Plaque Erosion. Am J Cardiol 2022, 167, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Pacheco Claudio, C.; Quesada, O.; Pepine, C.J.; Noel Bairey Merz, C. Why names matter for women: MINOCA/INOCA (myocardial infarction/ischemia and no obstructive coronary artery disease). Clin Cardiol 2018, 41, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Teragawa, H.; Oshita, C.; Uchimura, Y.; Akazawa, R.; Orita, Y. Coronary Microvascular Vasodilatory Function: Related Clinical Features and Differences According to the Different Coronary Arteries and Types of Coronary Spasm. J Clin Med 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Handberg, E.M.; Merz, C.N.B.; Cooper-Dehoff, R.M.; Wei, J.; Conlon, M.; Lo, M.C.; Boden, W.; Frayne, S.M.; Villines, T.; Spertus, J.A.; et al. Rationale and design of the Women’s Ischemia Trial to Reduce Events in Nonobstructive CAD (WARRIOR) trial. Am Heart J 2021, 237, 90–103. [Google Scholar] [CrossRef] [PubMed]
- Ford, T.J.; Corcoran, D.; Oldroyd, K.G.; McEntegart, M.; Rocchiccioli, P.; Watkins, S.; Brooksbank, K.; Padmanabhan, S.; Sattar, N.; Briggs, A.; et al. Rationale and design of the British Heart Foundation (BHF) Coronary Microvascular Angina (CorMicA) stratified medicine clinical trial. Am Heart J 2018, 201, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, J.; Onuma, S.; Hao, K.; Godo, S.; Shiroto, T.; Yasuda, S. Pathophysiology and diagnostic pathway of myocardial infarction with non-obstructive coronary arteries. J Cardiol 2024, 83, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Hjort, M.; Eggers, K.M.; Lakic, T.G.; Lindback, J.; Budaj, A.; Cornel, J.H.; Giannitsis, E.; Katus, H.A.; Siegbahn, A.; Storey, R.F.; et al. Biomarker Concentrations and Their Temporal Changes in Patients With Myocardial Infarction and Nonobstructive Compared With Obstructive Coronary Arteries: Results From the PLATO Trial. J Am Heart Assoc 2023, 12, e027466. [Google Scholar] [CrossRef] [PubMed]
- Hjort, M.; Eggers, K.M.; Lindhagen, L.; Agewall, S.; Brolin, E.B.; Collste, O.; Daniel, M.; Ekenback, C.; Frick, M.; Henareh, L.; et al. Increased Inflammatory Activity in Patients 3 Months after Myocardial Infarction with Nonobstructive Coronary Arteries. Clin Chem 2019, 65, 1023–1030. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Main pathophysiological mechanisms of MINOCA of ischemic, non-atherosclerotic cause.
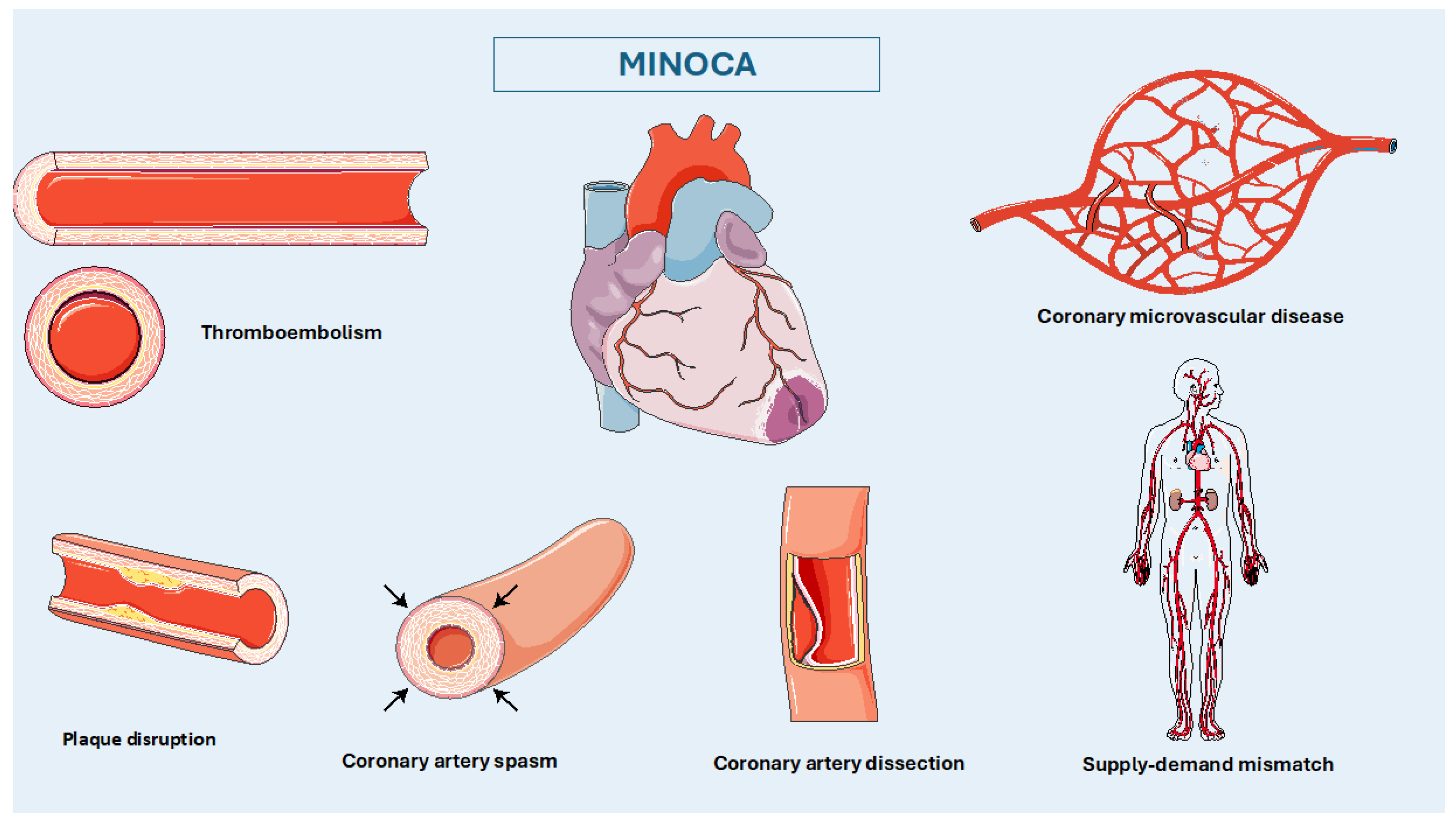
Figure 2.
Therapeutic algorithm of MINOCA of non-atherosclerotic cause.


Table 1.
Imaging modalities for MINOCA diagnosis.
| Imaging Modality | Parameters | Diagnosis | Prognosis |
|---|---|---|---|
| Echocardiography | - Myocardial function - Wall motion abnormalities - Coronary Flow Reserve (CFR) |
- Causes of myocardial injury - Differential diagnosis of other non-cardiac diseases - CMVD |
- Initial assessment tool |
| Invasive Coronary Angiography | - Coronary artery stenosis - Coronary flow rates - Epicardial coronary vasospasm |
- Coronary arteries visualization - SCAD - Vasospasm and microvascular dysfunction -Coronary artery bridging |
- Poorer outcomes in non-obstructive coronary atherosclerotic plaques - Worse prognosis in positive provocative testing for coronary spasm |
| Intravascular Ultrasound (IVUS) | - 360-deggree imaging of coronary arteries | - Detailed characterization of coronary lesions | - Poorer prognosis in complex lesions |
| Optical Coherence Tomography (OCT) | - Visualization of luminal and superficial lesions | - High-resolution imaging for precise lesion detection (plaque disruption, SCAD, and distal embolization) | - Poorer prognosis in disrupted lesions |
| Fractional Flow Reserve (FFR) and Instantaneous Wave-Free Ratio (IFR) | - Pressure measurements | - Functional significance of epicardial stenosis - Microvascular function with CFR and IMR |
- Risk stratification in specific cases |
| Coronary Computed Tomography Angiography (CCTA) | - Plaque characteristics -Perivascular Fat Attenuation Index (pFAI) |
- Identifies extracardiac structures - Lesion changes - Differentiation coronary vs non-coronary origin of MINOCA |
- Elevated pFAI values indicate load of inflammation |
| Cardiac Magnetic Resonance (CMR) | - Myocardial perfusion - Ventricular function - T2 and LGE sequences |
- Differentiation ischemic vs. non-ischemic injuries - Identification myocardial edema, fibrosis, and microvascular obstruction |
- Prognostic value of LGE, MPI and MPRI |
CMVD, coronary microvascular dysfunction; CFR, Coronary Flow Reserve; IMR, index of microcirculatory resistance; LGE, Late gadolinium enhancement; MINOCA, Myocardial Infarction with Non-Obstructive Coronary Arteries; MPI, Myocardial Perfusion Imaging; myocardial perfusion reserve index; pFAI, Perivascular Fat Attenuation Index; SCAD, Spontaneous Coronary Artery Dissection.
Table 2.
Biomarkers associated with MINOCA diagnosis and prognosis.
| Biomarkers | Mechanism | Changes in MINOCA | Prognostic value |
|---|---|---|---|
| Troponin (cTnI and cTnT) | Myocardiocytes destroy | ↑ cTn levels > 99th percentile: myocardial injury |
|
| C-reactive protein (CRP) | Inflammation | ↑ in MINOCA | ↑ risk of all-cause mortality and MACE |
| P-selectin glycoprotein ligand-1 (PSGL-1) | Inflammation | Discriminates between MINOCA, AMI-CAD and healthy controls | poorer prognosis in MINOCA patients |
| Interleukin 6 (IL-6) | Inflammation, CMVD, CAS | ↑ in CMVD and CAS | ↑ adverse cardiovascular outcomes |
| Soluble urokinase-type plasminogen activator receptor (suPAR) | Inflammation | ↑ in MINOCA vs healthy controls | ↑ adverse cardiovascular outcomes |
| N-terminal pro-B-type natriuretic peptide (NT-proBNP) | Endo-cardiac pressure | ↑ in MINOCA and AMI-CAD vs healthy controls | Unknown |
| Lipoprotein (a) (Lp(a)) | Lipid metabolism | ↑ in MINOCA | poorer prognosis in MINOCA patients |
| Visfatin | Inflammation, endothelial function | ↑ in MINOCA and type 2 diabetes mellitus | Unknown |
| Placental growth factor (PlGF) | Endothelial function, inflammation, angiogenesis | ↑ in MINOCA | Unknown |
| Fractalkine (CX3CL-1/FKN) | Plaque formation, inflammation, endothelial dysfunction | ↑ in MINOCA | Unknown |
| White blood cell count to mean platelet-volume ratio (WMR) | Inflammation | ↑ in MINOCA | ↑ risk of MACE |
| Neutrophil-to-platelet ratio (NPR) | Inflammation | ↑ in MINOCA | ↑ risk of MACE |
| Platelet-to-lymphocyte ratio (PLR) | Inflammation | ↑ in MINOCA | ↑ risk of MACE |
| Neutrophil-to-lymphocyte ratio (NLR) | Inflammation | ↑ in MINOCA | ↑ risk of MACE |
| Uric acid | - | ↑ in MINOCA | ↑ adverse outcomes and MACE |
| HMOX1 gene | stress-induced protective enzyme against myocardial ischemia | Long promoter guanine-thymine repeats | ↑ adverse outcomes and heart dysfunction |
| ET-1 (Endothelin-1) | Regulation vascular tone and proliferation | ↑ in MINOCA | Association with CMVD |
| TGF-β (Transforming Growth Factor-β) | endothelial cell dysfunction and vascular permeability | ↑ in MINOCA | Association with SCAD in women |
CMVD, coronary microvascular dysfunction; CAS, coronary artery spasm; HMOX1, Heme Oxygenase 1; MACE, Major Adverse Cardiovascular Events; AMI-CAD, Acute Myocardial Infarction with Coronary Artery Disease; MINOCA, Myocardial Infarction with Non-Obstructive Coronary Arteries; SCAD, Spontaneous Coronary Artery Dissection.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



