
Submitted:
09 August 2024
Posted:
12 August 2024
You are already at the latest version
Abstract
Background: Strength assessment is one of the main fields in sports performance, physical rehabilitation, physical activity and health. Purpose: To compare maximal voluntary isometric contractions (MVIC) and paired voluntary isometric contractions (VIC) of knee extensors between an isokinetic dynamometer (BIODEX) and a portable and lightweight device (DINABANG). Methods: From 19 volunteers (age: 28.7±7 y; body mass: 72±10 kg and height: 173±7 cm) we obtained 114 paired MVIC measures and, from the force-time curves of these repetitions, 22507 paired VIC measures of knee extensors. Results: We observed “excellent” repeatability for MVIC (ICC:1.00; p<0.001) between BIODEX (247±79.5 Nm) and DINABANG (247±74.8 Nm), with “trivial” effect (mean difference: 0.12 Nm (0.02%); 95%CI: -0.13 to 0.23 Nm; p=0.606; d=0.048). Bland-Altman plots revealed high accuracy for MVIC (bias: 0.12 Nm) and consistent distribution (precision) inside the limits of agreement (-4.81 to 5.06 Nm) and respective 95%CI. “Excellent” repeatability was also observed for VIC (ICC:1.00; p<0.001) between BIODEX (219±84.1 Nm) and DINABANG (218±84.0 Nm), with “trivial” effect (0.24 Nm (0.11%); 0.08 to 0.11 Nm; p<0.001; d=0.100). Bland-Altman plots revealed high accuracy for VIC (bias: 0.24 Nm) and consistent distribution (precision) inside the limits of agreement (-4.5 to 4.9 Nm) and respective 95%CI. Conclusion: DINABANG is accurate, precise and reliable for torque measurement.
Keywords:
exercise
; health
; physical fitness
; rehabilitation
; physical therapy
; strength assessment
; exercise physiology
; sports biomechanics
; digital technology
1. Introduction
Muscle strength assessments are critical in rehabilitation, sports training, physical activity, and health centers (Ramírez-delaCruz et al. 2022; Rodrigues et al 2021). The crucial concern of the sport sciences professionals is achieving a reliable and reproducible measurement. Many different types of equipment have been used in such assessments (e.g. simple or isokinetic dynamometers), and the focus has been on different populations, such as athletes or patients (Baltzopoulos & Brodie 1989; Romero-Franco et al. 2017). In most of these studies, the measurement of maximal isometric strength has been associated with improved sports performance (Lum & Barbosa 2019), a reduction in the risk of falls in older people (Valenzuela et al. 2020), or a sign of progress during the rehabilitation process (Romero-Franco et al. 2017). Therefore, accurate and valid measurement systems are needed to reduce the degree of uncertainty to a minimum.
Isokinetic dynamometry represents the clinical “gold-standard” for strength assessment, but it is available in a limited number of specialized laboratories. In fact, isokinetic dynamometry has some limitations: it lacks portability, takes up a lot of physical space, requires a lot of training time for its use, and is expensive for some professionals. In response to these limitations, some authors have used their own dynamometers, which are cheaper, portable, and validated (Tuttle & Jacuinde 2011). Despite that, most of these devices only measure forces in the perpendicular direction, which limits their application to more realistic gestures (Hogrel et al. 2020). On this line, after a knee injury, measurements of maximal isometric strength of the hamstrings and quadriceps provide important information for clinicians to help make the decision on whether the athlete is fit to participate in physical activities (Lum & Barbosa 2019). Objective measurements of muscle strength become essential to know how the patient's treatment is progressing.
Typically, during a lower limb exercise program, the investigator/professional defines and controls the subject's effort based on subjective criteria until a quantitative assessment (e.g., isokinetic, or static strength assessment) is required (Krause et al. 2019). Specifically, when elastic bands are used to exercise the lower extremities, the question remains whether the force deployed is excessive or insufficient, both situations being suboptimal due to the risk of injury or lack of effectiveness (Hintermeister et al. 1998). Therefore, it would be necessary to use systems that accurately assess the torque performed by the athlete or patient, to optimize training. The DINABANG mobile application and its portable and lightweight device (Movi, https://www.movi-ing.com/ Montevideo, Uruguay) for isometric force–time curve assessment could address this problem by measuring, in real time, the torque of the involved limb to guide the decisions of the physiotherapist, the instructed patient, or the athlete during rehabilitation and training sessions. This system was already validated in some preliminary studies comparing different instruments (Santos et al. 2017; Simini et al. 2022).
A recent systematic review revealed that some current apps used in rehabilitation and exercise setups are valid and reliable for measuring bar movement velocity during lower and upper body resistance exercises; however, a significant systematic bias was detected with heavier loads (Silva et al. 2021). Although many low-cost dynamometers have recently been validated (Silva et al. 2021; Aramaki et al. 2016), strength devices coupled with angular position measurement are still lacking. DINABANG could address this problem by measuring, in real time, the lower limb torque to guide the physiotherapist’s decisions, the instructed patient or the athlete during rehabilitation or training sessions. DINABANG was designed with a strain gauge affixed between the elastic band and a brace just above the malleoli, an inertial measurement unit (IMU) and Bluetooth communication (Santos et al 2021). Thus, the aim of this study was to compare knee joint maximal isometric force–time curve related variables between the gold standard (isokinetic dynamometer) BIODEX (BIODEX System 4 Pro: BIODEX Medical Systems, https://biodexrehab.com/products/system-4-pro/, Shirley, NY, USA) and DINABANG by verifying its accuracy, precision, and repeatability. We hypothesized that the knee joint maximal isometric force–time curve between BIODEX and DINABANG are comparable.
2. Materials and Methods
We performed an experiment to simultaneously measure torque with DINABANG and BIODEX during standard exercise. The exercise protocol consisted of a maximum voluntary isometric contraction (MVIC) of knee extensors, with knee flexed at 60º. Twenty volunteers (age 28.7 ± 7 y, weight, 72 ± 10 kg, height: 173 ± 7 cm, BMI: 23.8 ± 2.4 kg/cm2) participated in the study. All subjects were healthy, with no prior history of cardiovascular, neuromuscular nor orthopedic disease. At the time of inclusion in the study, participants had not engaged into any systematic physical training program within the last year. The volunteers practiced some form of physical activity at least three times a week for at least half an hour per session (Tegner activity level ≥ 5) (Simini et al. 2022). Participants were encouraged to avoid extenuating exercise in the 48 hours before the study. All subjects agreed to participate voluntarily and signed a written informed consent prior to enrollment. The study protocol was approved by the Research Ethics Committee of the of Faculty of Sports—University of Porto (CEFADE 30_2022; Date of Approval: March 16th 2023).
2.1. Calibration
The maximum voluntary isometric contraction (MVIC) of knee extensors was performed using the BIODEX dynamometer (BIODEX System 4 Pro: BIODEX Medical Systems, Shirley, NY, USA) with a sampling frequency of 100 Hz. Simultaneous measurements were made using DINABANG with a sampling frequency of 200 Hz, decimated down to 100 Hz for compatibility with BIODEX. The calibration of the BIODEX was regularly checked according to the manufacturer's specifications. The DINABANG has a factory calibration, which is performed by establishing a calibration curve using standard reference masses.
2.2. Study Design and Protocol
The study design consisted of warm-up (5 min cycling at 1 Watt/kg), familiarization and practice with the equipment and the test protocol (Figure 1).
The subjects performed three repetitions of maximum voluntary isometric contraction (MVIC) of knee extensors. Records of Torque (BIODEX) and Force with Torque calculation (DINABANG) were simultaneously obtained with two devices: the isokinetic BIODEX (Figure 2a) and lightweight portable DINABANG (Figure 2b).
The measurements with subjects comfortably seated in BIODEX, with the trunk, hip and thigh stabilized (fixed by straps). To avoid compensatory movements the subjects were instructed to grasp on the stabilization handles during the test. One of the authors oriented the knee extension axis (identified as a horizontal line passing through the femoral condyles) to coincide with the BIODEX axis of rotation. The hip and ankle joints were positioned at 90º. The strap of DINABANG is also affixed at the ankle of the leg being evaluated by BIODEX. The DINABANG device calculates the instant torque from force and chain orientation. Subjects were instructed to perform three repetitions of maximum voluntary isometric contraction (MVIC) of knee extensors, trying to maximally pull the chain for 3-4 seconds. A rest time of 90 seconds was given between each MVIC. Torque-time data during each repetition was obtained, using a sampling frequency of 100Hz.
2.3. Synchronization and Data Extraction
DINABANG and BIODEX torque-time curve data were synchronized by the peak torque value in each repetition. To avoid differences between DINABANG and BIODEX measurements due to slack binding between the two systems, data from the first second and after the maximum value of each repetition were removed.
2.4. Statistical Analysis
Paired comparisons of 34 maximum voluntary isometric contraction (MVIC) of knee extensors were deemed sufficient. (software G * Power, version 3.1.9.6) assuming an error probability of 0.05 (Faul et al. 2007). Due to methodological reasons, one of the volunteers was excluded from the statistical analysis. From each of the 19 volunteers, 3 MVICs were obtained for each limb, resulting in 114 torque-time curves. A total of 114 paired MVIC and 22507 VIC (corresponding to torque-time curve data) of knee extensors were used for data analysis. A paired t-test was used to compare differences between the two instruments. Effect sizes (Cohen’s d) were interpreted with the following criteria: 0–0.19 trivial, 0.2–0.59 small, 0.6–1.19 moderate, 1.2–1.99 large, 2.0–3.99 very large and >4.0 nearly perfect (Hopkins et al., 2002). The Bland-Altman plot (Bland & Altman, 1986) was applied using open statistical software for the desktop and cloud (JAMOVI, www.jamovi.org) according to the guidelines (Giavarina, 2015) to quantify the agreement between two quantitative measurements by determining the bias (or mean of difference for normally distributed and median of the differences if non-normally distributed data) as a measure of accuracy, and limits of agreement as a measure of precision. The mean of the two measurements was plotted against the difference between them with 95% of the differences expected to lie within the limits of agreement (±1.96 standard deviations from the mean and respective 95% confidence interval. The confidence interval of the bias illustrates the magnitude of the systematic error, while the confidence intervals of the limits of agreements provide an estimation of the extent of the possible sampling error (Bland & Altman, 1986; Giavarina, 2015). Inspection of the slope of the linear regression (Bland–Altman plot) between both protocols (to check for proportional error) was performed. Intraclass correlation coefficients (ICC) (model: one-way random) were calculated using IBM SPSS Statistics V.29 to quantify the consistency (repeatability) between BIODEX and DINABANG each variable over a wide range of metabolic rates. Values less than 0.5, between 0.5 and 0.75, between 0.75 and 0.9, and greater than 0.90 were deemed indicative of poor, moderate, good, and excellent repeatability, respectively (Koo & Li, 2016). Statistical significance was established as p ≤ 0.05.
3. Results
We compared knee joint maximal isometric force–time curve related variables (MVIC and VIC) between the gold standard (isokinetic dynamometer) BIODEX and DINABANG by verifying its accuracy, precision, and repeatability.
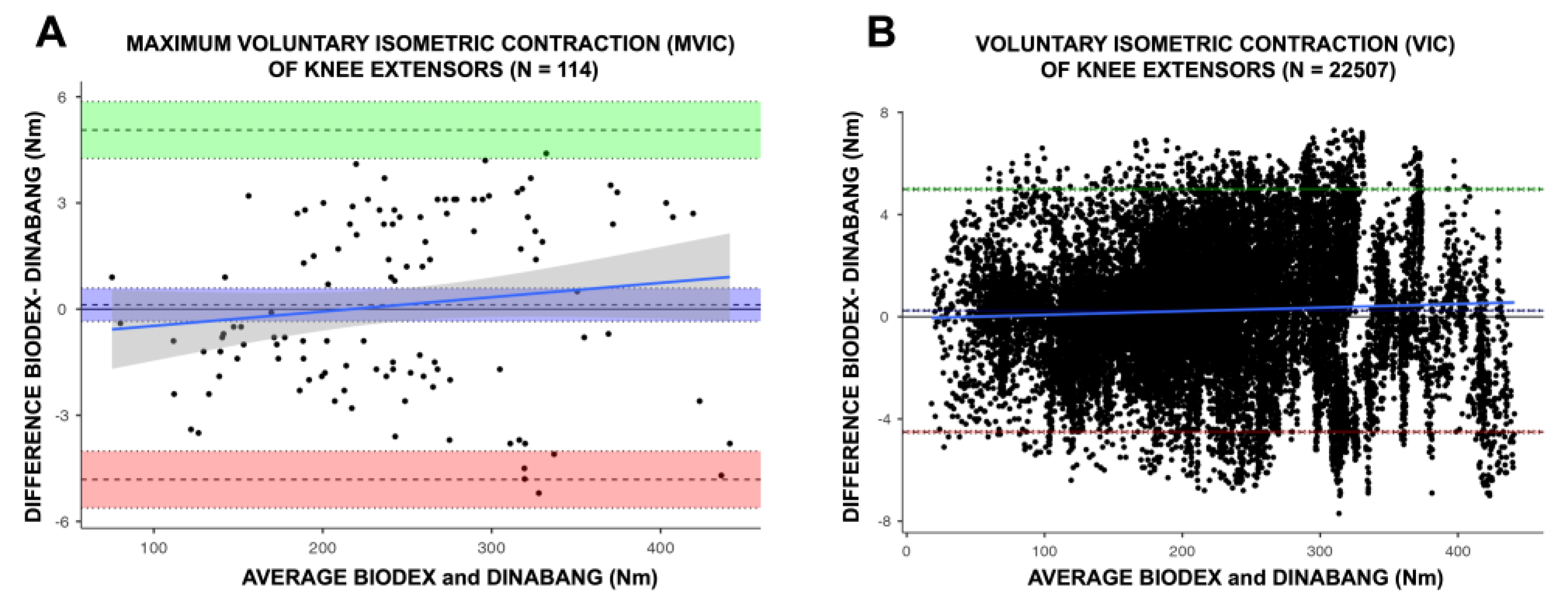
Regarding maximum voluntary isometric contractions (MVIC), we observed “excellent” repeatability (ICC: 1.00; 95%CI: 0.99 to 1.00; p < 0.001) between BIODEX (247.0 ± 79.5 Nm) and DINABANG (247.0 ± 74.8 Nm), and a “trivial” effect (mean diff.: 0.12 Nm (0.02%); 95%CI: -0.13 (-0.05) to 0.23 (0.09%) Nm; p = 0.606; d = 0.048). Bland-Altman plots revealed high accuracy for MVIC (bias: 0.12 Nm), with lines of equalities within the confidence interval of the mean differences. Besides, we observed a consistent distribution (precision) inside the limits of agreement (-4.81 to 5.06 Nm) and respective 95% confidence interval, with no proportional error (p = 0.17) (Figure 3 Panel A).
Regarding voluntary isometric contractions (VIC), we observed “excellent” repeatability (ICC: 1.00; 95%CI: 0.99 to 1.00; p < 0.001) between BIODEX (219.0 ± 84.1 Nm) and DINABANG (218.0 ± 84.0 Nm), and a “trivial” effect (mean diff.: 0.24 Nm (0.11%); 95%CI: 0.08 (0.03%) to 0.11 (0.05%) Nm; p < 0.001; d = 0.100). Bland-Altman plots revealed high accuracy for VIC (bias: 0.24 Nm), with lines of equalities within the confidence interval of the mean differences. Besides, we observed a consistent distribution (precision) inside the limits of agreement (-4.5 to 4.9 Nm) and respective 95% confidence interval, with proportional error (p < 0.001) (Figure 3 Panel B).
Thus, these results indicate that DINABANG is an accurate, precise, and reliable device for torque measurement, providing portability for on-field evaluations.
4. Discussion
The aim of this study was to compare maximum voluntary isometric contraction (MVIC) and paired voluntary isometric contractions (VIC) of knee extensors between the gold standard (isokinetic dynamometer) BIODEX and DINABANG, assessing their accuracy, precision, and repeatability. The main outcome suggests that DINABANG demonstrated excellent repeatability, consistent precision, and excellent accuracy for MVIC torque measurement compared to the BIODEX system, considered the gold standard. These results are particularly important and enhance credibility for professionals involved in strength and conditioning, as well as rehabilitation, especially in situations that require portability for on-field assessments and/or the evaluation of a large number of patients within a short period of time.
Quadriceps strength is particularly assessed in the realm of sports due to its significance as an isometric strength parameter for monitoring training progression and detecting strength imbalances as a predictor of injury risk (Noteboom et al., 2023). Older adults with knee osteoarthritis commonly exhibit quadriceps strength loss, which increases the risk of falls and serves as an indicator of sarcopenia (Claudino et al., 2021; Guirguis-Blake et al., 2018). Moreover, MVIC has been regarded in some studies as a fatigue and recovery criterion, facilitating the monitoring of training advancements (Jukic et al., 2023).
Unlike traditional muscular force sensors, the new system (DINABANG) allows the user to control the exact angle being tested due to the inclusion of an inertial movement unit. Although not fully validated, the system enables analysis of force, torque, and mechanical power as a function of motion. Future applications may expand upon these findings by exploring various conditions such as different training phases (competitive, pre-competitive, conditioning) or stages of rehabilitation, as well as different phases of intermittent games or medication regimens. The rationale behind this is that we anticipate fatigue, overreaching, or even overtraining profiles may reveal valuable diagnostic information about training and rehabilitation loads that surpasses the insights gained from a single maximum voluntary contraction (MVC) reading.
We acknowledge some limitations of the study. Firstly, the power measurement capabilities of both instruments were not considered in the present research, which focuses exclusively on the force and torque measurements of isometric contraction in normal volunteers. Secondly, studies involving individuals with movement disorders and aging populations may be valuable to expand the applicability of DINABANG, considering its varied force and coordination capabilities.
Nevertheless, the results from the current study suggest that sports medicine, training clubs, and rehabilitation facilities can assess neuromuscular function using a reliable device, enabling greater intervention control in real-life conditions. The minimum detectable difference typically reported for knee extensor torque is 25 to 28 Nm in the literature (Hartog et al., 2021), which is approximately 100 times greater than the average difference between BIODEX and DINABANG torque values. Consequently, DINABANG appears to be highly advantageous as a force recording tool in clinical trials within the health and performance field. The DINABANG device seems easily transportable for use in professionals' offices, gyms, sports fields, and even athletes' homes for remote follow-up. Since DINABANG is primarily a muscular power measurement system, we recommend that future studies compare force, torque, and mechanical power during movement.
5. Conclusions
DINABANG and BIODEX produced highly comparable maximum voluntary isometric contraction (MVIC) and voluntary isometric contraction (VIC) responses across a wide range of values. We also noted highly accurate data with minimal bias. The distribution within each dataset and their respective 95% confidence intervals were consistently aligned for MVIC and VIC. The repeatability, as measured by the Intraclass Correlation Coefficient (ICC), was excellent. Physiotherapists, support staff, exercise, and health professionals, as well as researchers, can now discern differences in strength capacities measured between the two devices.
Author Contributions
Conceptualization, D.S., F.S., A.B.S. and R.Z.; methodology, A.B.S. and R.Z.; validation, D.S., A.B.S. and R.Z.; formal analysis, A.B.S and R.Z.; investigation, D.S., A.B.S., F.S., L.A.P.T and R.Z ; resources, R.Z.; data curation, A.B.S. and R.Z; writing—original draft preparation, D.S., A.B.S. and R.Z.; writing—review and editing, D.S., A.B.S., L.A.P.T., F.S. and R.Z.; visualization, R.Z.; supervision, R.Z.; project administration, R.Z.; funding acquisition, D.S. and R.Z. All authors have read and agreed to the published version of the manuscript.
Funding
R.Z. was supported by The Research Center in Physical Activity, Health and Leisure (CIAFEL), Faculty of Sport, University of Porto (FADEUP), which is part of the Laboratory for Integrative and Translational Research in Population Health (ITR); both are funded by the Fundação Para a Ciência e Tecnologia (FCT; grants UIDB/00617/2020 https://doi.org/10.54499/UIDB/00617/2020; UIDP/00617/2020 https://doi.org/10.54499/UIDP/00617/2020 and LA/P/0064/2020, respectively).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of FACULTY OF SPORTS—UNIVERSITY OF PORTO (CEFADE 30_2022; Date of Approval: March 16th 2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are only available upon request from the corresponding author. The data are not publicly available due to their containing of information that could compromise the privacy of study participants.
Acknowledgments
In this section, you can acknowledge any support given which is not covered by the author contributions or funding sections. This may include administrative and technical support, or donations in kind (e.g., materials used for experiments).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Ramírez-delaCruz, M.; Bravo-Sánchez, A.; Esteban-García, P.; Jiménez, F.; Abián-Vicén, J. Effects of Plyometric Training on Lower Body Muscle Architecture, Tendon Structure, Stiffness and Physical Performance: A Systematic Review and Meta-analysis. Sports Med. Open 2022, 8, 40. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, J.A.L.; Santos, B.C.; Medeiros, L.H.; Gonçalves, T.C.P.; Júnior, C.R.B. Effects of Different Periodization Strategies of Combined Aerobic and Strength Training on Heart Rate Variability in Older Women. J. Strength Cond. Res. 2021, 35, 2033–2039. [Google Scholar] [CrossRef]
- Baltzopoulos, V.; Brodie, D.A. Isokinetic dynamometry. Applications and limitations. Sports Med. 1989, 8, 101–116. [Google Scholar] [CrossRef]
- Romero-Franco, N.; Jiménez-Reyes, P.; Montaño-Munuera, J.A. Validity and reliability of a low-cost digital dynamometer for measuring isometric strength of lower limb. J. Sports Sci. 2017, 35, 2179–2184. [Google Scholar] [CrossRef]
- Lum, D.; Barbosa, T.M. Brief Review: Effects of Isometric Strength Training on Strength and Dynamic Performance. Int. J. Sports Med. 2019, 40, 363–375. [Google Scholar] [CrossRef]
- Valenzuela, P.L.; Maffiuletti, N.A.; Saner, H.; et al. Isometric Strength Measures are Superior to the Timed Up and Go Test for Fall Prediction in Older Adults: Results from a Prospective Cohort Study. Clin. Interv. Aging 2020, 15, 2001–2008. [Google Scholar] [CrossRef] [PubMed]
- Tuttle, N.; Jacuinde, G. Design and construction of a novel low-cost device to provide feedback on manually applied forces. J. Orthop. Sports Phys. Ther. 2011, 41, 174–179. [Google Scholar] [CrossRef]
- Hogrel, J.Y.; Benveniste, O.; Bachasson, D. Routine monitoring of isometric knee extension strength in patients with muscle impairments using a new portable device: Cross-validation against a standard isokinetic dynamometer. Physiol. Meas. 2020, 41, 015003. [Google Scholar] [CrossRef] [PubMed]
- Krause, M.; Crognale, D.; Cogan, K.; et al. The effects of a combined bodyweight-based and elastic bands resistance training, with or without protein supplementation, on muscle mass, signaling and heat shock response in healthy older people. Exp. Gerontol. 2019, 115, 104–113. [Google Scholar] [CrossRef]
- Hintermeister, R.A.; Bey, M.J.; Lange, G.W.; Steadman, J.R.; Dillman, C.J. Quantification of elastic resistance knee rehabilitation exercises. J. Orthop. Sports Phys. Ther. 1998, 28, 40–50. [Google Scholar] [CrossRef]
- Santos, D.; Barboza, R.; Domínguez, J.; Fernández, A.; Veirano, F.; Pérez, P.; Motta, F.; Simini, F. DINABANG: Explosive Force Hamstring Rehabilitation Biomechanics Instrument», en 6th International Conference on Biotechnology and Bioengineering. Offenburg, Germany, 2017, pp. 26–28.
- Simini, F.; Santos, D.; Dominguez, J.; Barboza, R. DINABANG: A portable measurement device to monitor lower limb explosive torque and velocity with validation», in World Congress on Medical Physics and Biomedical Engineering, Marina Bay Sands; Singapore, 2022; pp. 1480–1482. Available online: https://wc2022.org/ (accessed on 4 August 2024).
- Silva, R.; Rico-González, M.; Lima, R.; Akyildiz, Z.; Pino-Ortega, J.; Clemente, F.M. Validity and Reliability of Mobile Applications for Assessing Strength, Power, Velocity, and Change-of-Direction: A Systematic Review. Sensors 2021, 21, 2623. [Google Scholar] [CrossRef] [PubMed]
- Aramaki, H.; Katoh, M.; Hiiragi, Y.; Kawasaki, T.; Kurihara, T.; Ohmi, Y. Validity and reliability of isometric muscle strength measurements of hip abduction and abduction with external hip rotation in a bent-hip position using a handheld dynamometer with a belt. J. Phys. Ther. Sci. 2016, 28, 2123–2127. [Google Scholar] [CrossRef] [PubMed]
- Santos, D.; Massa, F.; Dominguez, J.; Morales, I.; Del Castillo, J.; Mattiozzi, A.; Simini, F. Hamstring Torque, Velocity and Power Elastic Band Measurements during Hip Extension and Knee Flexion. Appl. Sci. 2021, 11, 10509. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, W.G.; A Scale of Magnitudes for Effect Statistics. A New View of Statistics. Available online: http://sportsci.org/resource/stats/effectmag.html (accessed on 4 August 2024).
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef] [PubMed]
- Giavarina, D. Understanding Bland Altman analysis. Biochem. Med. 2015, 25, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Noteboom, L.; Nijs, A.; Beek, P.J.; van der Helm, F.C.T.; Hoozemans, M.J.M. A Muscle Load Feedback Application for Strength Training: A Proof-of-Concept Study. Sports 2023, 11, 170. [Google Scholar] [CrossRef] [PubMed]
- Claudino, J.G.; Afonso, J.; Sarvestan, J.; et al. Strength Training to Prevent Falls in Older Adults: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2021, 10, 3184. [Google Scholar] [CrossRef]
- Guirguis-Blake, J.M.; Michael, Y.L.; Perdue, L.A.; Coppola, E.L.; Beil, T.L.; Thompson, J.H. Interventions to Prevent Falls in Community-Dwelling Older Adults: A Systematic Review for the U.S. Preventive Services Task Force; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2018. [Google Scholar]
- Jukic, I.; Prnjak, K.; McGuigan, M.R.; Helms, E.R. One Velocity Loss Threshold Does Not Fit All: Consideration of Sex, Training Status, History, and Personality Traits When Monitoring and Controlling Fatigue During Resistance Training. Sports Med. Open 2023, 9, 80. [Google Scholar] [CrossRef]
- Hartog, J.; Dijkstra, S.; Fleer, J.; van der Harst, P.; Mariani, M.A.; van der Woude, L.H.V. A portable isometric knee extensor strength testing device: Test-retest reliability and minimal detectable change scores of the Q-Force II in healthy adults. BMC Musculoskelet Disord. 2021, 22, 966. [Google Scholar] [CrossRef]
Figure 1.
DINABANG and Biodex set-up for simultaneous lower limb force measurements.
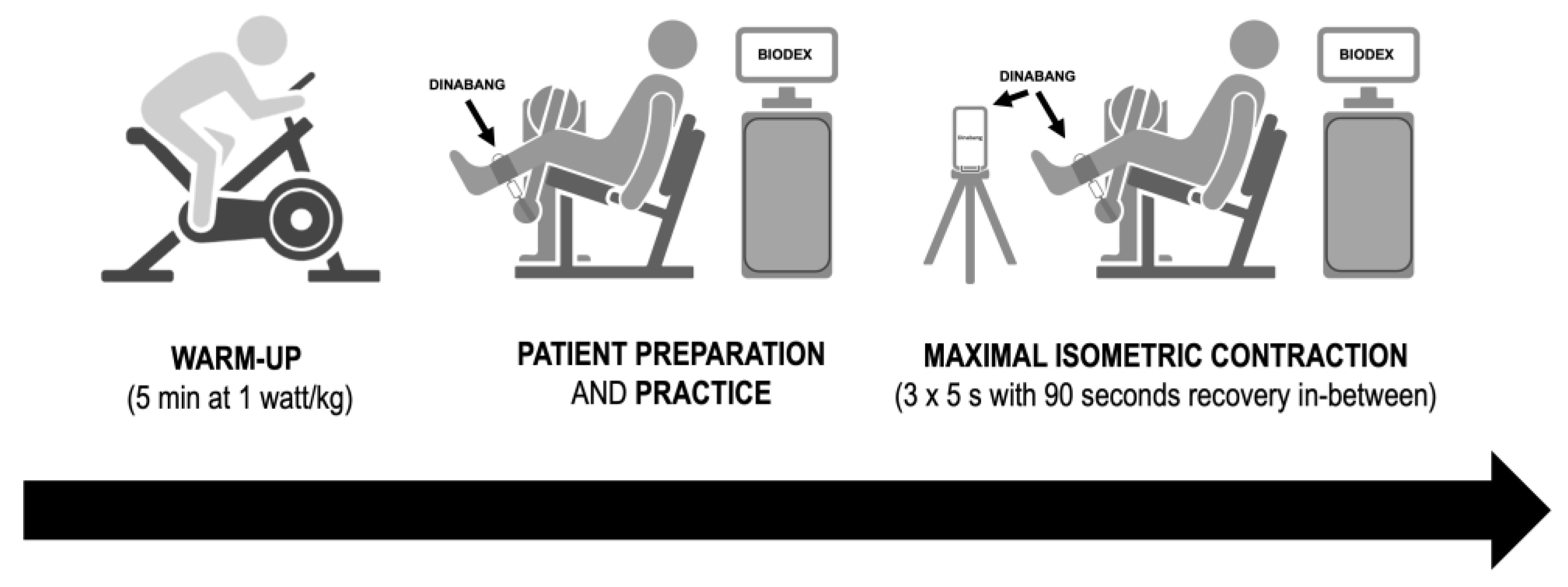
Figure 2.
Maximum voluntary isometric contraction (MVIC) of knee extensors set up and DINABANG connection. (A) Volunteer sitting in Biodex chair with DINABANG strap connected just above malleolus in lieu of usual Biodex cylinder, (B) Detail of DINABANG connected both to the ankle strap and to Biodex force connection at the back. Note DINABANG includes a carabine hook secured to the ankle strap.
Figure 2.
Maximum voluntary isometric contraction (MVIC) of knee extensors set up and DINABANG connection. (A) Volunteer sitting in Biodex chair with DINABANG strap connected just above malleolus in lieu of usual Biodex cylinder, (B) Detail of DINABANG connected both to the ankle strap and to Biodex force connection at the back. Note DINABANG includes a carabine hook secured to the ankle strap.
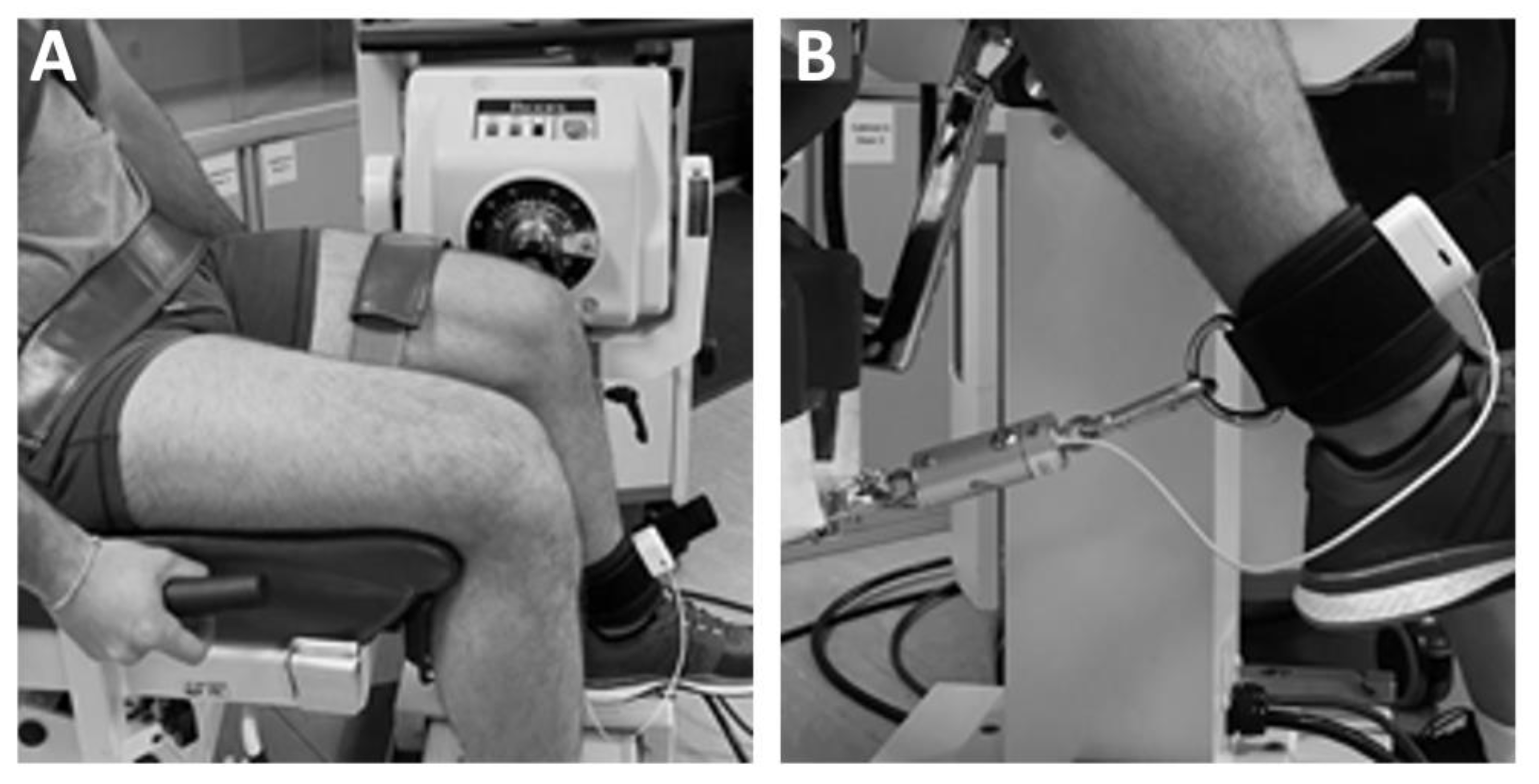
Figure 3.
Bland-Altman plots comparing DINABANG with BIODEX. Plot of differences of (A) the maximum voluntary isometric contraction (MVIC) of knee extensors (Nm) (B) voluntary isometric contraction (VIC) of knee extensors between BIODEX and DINABANG (Nm). Bias (dashed line), limits of agreement (dashed lines), and 95% CIs (shaded areas) between the BIODEX and DINABANG methods. Green, red and blue are upper limit, lower limit, bias and respective confidence bands. Blue line and respective 95% CI is the inspection of the slope of the linear regression between both conditions.
Figure 3.
Bland-Altman plots comparing DINABANG with BIODEX. Plot of differences of (A) the maximum voluntary isometric contraction (MVIC) of knee extensors (Nm) (B) voluntary isometric contraction (VIC) of knee extensors between BIODEX and DINABANG (Nm). Bias (dashed line), limits of agreement (dashed lines), and 95% CIs (shaded areas) between the BIODEX and DINABANG methods. Green, red and blue are upper limit, lower limit, bias and respective confidence bands. Blue line and respective 95% CI is the inspection of the slope of the linear regression between both conditions.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



