
Submitted:
10 August 2024
Posted:
12 August 2024
You are already at the latest version
Abstract
Reducing visceral fat is an important issue for obesity prevention. We previously reported a novel dietary intervention program using “Optimized Nutri-Dense Meals” based on the nutrients described in Dietary Reference Intakes in Japan. This open-label randomized controlled trial evaluated the visceral fat reducing effect of the program. In total, 100 Japanese obese/overweight male patients were recruited and divided into a control group that continued their usual diets and a test group that consumed test meals twice per weekday for four weeks. Visceral fat area, set as the primary outcome, was significantly decreased in the test group compared with the control group. Regarding other outcomes, the occupancy levels of some gut floras and presenteeism scores were significantly increased in the test group compared with the control group. These results indicate that dietary intervention based on the Dietary Reference Intakes can prevent visceral fat accumulation and contribute to the improvement of health, without the need for completely replacing the everyday diet.
Keywords:
visceral fat
; randomized control trial
; dietary reference intake
; Optimized Nutri-Dense Meals
1. Introduction
Excess visceral fat is associated with multiple diseases, such as type 2 diabetes mellitus (T2DM) and cardiovascular disease (CVD) [1]. It is also a well-known independent risk factor of CVD morbidity and mortality. According to a previous systematic review, Asians accumulate abdominal visceral fat more readily than Westerners [2]. Thus, the reduction of excess visceral fat is essential among the Asian population.
Nutritional education and dietary interventions are the simplest and most well-studied methods to reduce visceral fat. Nutritional education seems effective in raising awareness about dietary issues; however, its positive effects on biomarkers are limited [3,4]. Daily diet is as important as exercise for preventing obesity and reducing visceral fat. However, a dietary intervention that can be easily adopted by anyone has yet been discovered. Dietary interventions can be divided into calorie restriction and meal replacement. Calorie restriction has been reported to reduce lipid accumulation, oxidative stress, and inflammation in animal models [5] of obesity, and a visceral fat-reducing effect has been observed in human clinical studies [6]. Although calorie restriction has demonstrated strong potential, Hemmingsson reported difficulty in continuously implementing this method, especially in relatively young and non-obese individuals [7]. However, the effectiveness of meal replacement has been well-documented. In particular, traditional diets, such as the Mediterranean diet (MD) and traditional Japanese diet (washoku), have been researched. The MD has been reported to be more effective than limiting dietary calorie intake [8]. The MD is recognized as an intangible part of the cultural heritage of France, Italy, Greece, Spain, and Morocco by the United Nations Educational, Scientific, and Cultural Organization [9]. The MD is characterized by a high intake of vegetables, legumes, fresh fruits, non-refined cereals, nuts, and olive oil, especially extra virgin oil; moderate intake of red wine; and low consumption of red meat [10,11]. The MD and washoku have been reported to exert anti-obesity effects [12,13]. Although these local traditional diets have attracted attention because of their reliable effects, continuous consumption of specific traditional foods for a month is difficult owing of the limited availability of ingredients and differing areas of residence [14]. Furthermore, previous dietary interventions have required full meal replacements during the program period.
Recently, the concept of Optimized Nutri-Dense Meals has emerged in Japan. The details of this concept have been described in a previous article [14]; in brief, we adjusted the nutritional content of 33 types of nutrients, including energy-producing nutrients. The amounts of these nutrients were confirmed to be within the reference range. Their criteria were based on the Dietary Reference Intakes (DRIs) in Japan. In a previous randomized controlled trial (RCT), replacing two meals per weekday for four weeks with Optimized Nutri-Dense Meals showed hypotensive and Hemoglobin A1c (HbA1c)-reducing effects [15] (described as “COMB meals” in the reference). In previous single-arm studies, the potential effects of reducing visceral fat area, modifying lipid metabolism and gut flora, and enhancing work productivity have been observed [16]. In the present study, we evaluated the effects of Optimized Nutri-Dense Meals on visceral fat reduction. Furthermore, as supplementary data, we evaluated outcomes with potential for improvement, such as work productivity. This intervention study may provide insights into the impact of Japan’s DRIs on visceral fat.
2. Materials and Methods
This study was designed and conducted following the Consolidated Standards of Reporting Trials (CONSORT) 2010 guidelines. A complete copy of the checklist is provided in Supplemental Figure S1.
2.1. Study Design
This four-week, open-label RCT was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Medical Station Clinic Research Ethics Committee (approval no. 210114-3) following the ethical guidelines for research on humans (Ministry of Education, Culture, Sports, Science and Technology; Ministry of Health, Labor and Welfare, Japan). The trial was registered in the UMIN Clinical Trials Registry (registration no. UMIN000043180). Informed consent was obtained from all participants to publish the results as a treatise, under the condition that personal information would not be disclosed.
2.2. Study Population
Residents of Tokyo suburbs were recruited for this study through a website from January 15, 2021, to February 12, 2021. Those who wished to participate in the trial were invited to the Kouwa Clinic (Tokyo, Japan), where the details of the study and potential risks were explained, written informed consent was obtained, and the participants were screened. The inclusion criteria were as follows: (i) male individuals aged 30–64 years and (ii) body mass 2 index (BMI) of ≥23 kg/m2. The participants were selected in descending order of visceral fat area. The following participants were excluded:
- Those who could not continuously consume research foods because of business trips during the intake period (those who knew in advance that their eating rate would be <80%);
- Those who were judged to be inappropriate based on the answers to the lifestyle-related questionnaire and measurements of visceral fat area and abdominal circumference;
- Those who had abnormal laboratory test values or cardiopulmonary function and were judged to have problems participating in the study;
- Those with food allergies;
- Those who would face difficulty in treatment (including dietary guidance) by participating in the trial;
- Those who used implantable medical electrical equipment such as pacemakers;
- Those who used implantable metal medical equipment;
- Those undergoing dialysis;
- Those whose physical measurements, physical tests, and clinical test values before the start of ingestion showed significant deviations from the standard range;
- Those in other clinical studies at the start of the trial;
- Those who regularly consumed foods for specified health use, foods with functional claims, health foods, and supplements that may affect test results;
- Those who regularly consumed large amounts of alcohol;
- Those who smoked extremely often (≥21 cigarettes per day);
- Those with extremely irregular diets;
- Those with irregular life rhythms, such as shift and late-night workers;
- Those who underwent health examinations two weeks before the pre-intake examination;
- Those who planned to donate blood during the research period; and
- Those judged to be inappropriate by the principal investigator.
2.3. Randomization
Participants were randomly assigned to two groups according to the stratified block randomization method, stratified by visceral fat area, serum triglyceride (TG) level, and calorie intake calculated using the brief self-administered diet history questionnaire (BDHQ) measured at screening. The allocation manager created an allocation table, which was subsequently sealed in an envelope until the data were finalized, to ensure code breaking. The randomization process was executed by an allocation coordinator independent of the investigators.
2.4. Interventions
The trial was conducted in Tokyo, Japan, between February 1 and May 25, 2021. The test meals were provided in two forms: a breakfast meal set and a frozen lunch box. Participants in the test group were instructed to replace two meals, breakfast and lunch or dinner, with the test meals and to continue their usual diet for other meals. All test meals for the test groups were delivered to the participants' homes once every two weeks in a frozen state. Moreover, the participants were advised on the optimal timing for consuming the test meals. This regimen was instructed to be followed on weekdays for four weeks.
All test meals included 33 types of nutrients within the ranges listed in Table 1. Figure 1A shows an example of a lunch box instructed for lunch or dinner. Figure 1B shows the nutrient content. All remaining menus and nutritional contents are summarized in Supplemental Table S1. The meals could be consumed in any order from the delivered menu. Participants in the control group were instructed to consume their usual diet. No restrictions were placed on snack and alcohol consumption, but the latter was prohibited on the day before measurement in either group. Participants were asked to record the following information in a diary every day: meal record; amount of alcohol consumed; number of medicines or healthy foods, such as foods for specific health use; degree of exercise; lifestyle changes; confirmation of prohibited action; and any symptoms that were noticed. Moreover, the participants were required to wear an activity monitor (HJA-307IT; Omron Healthcare, Kyoto, Japan) that could record the total burned and active calories, and the results were recorded in a diary.
2.5. Outcomes
The primary outcome of this study was the change in visceral fat area. The secondary outcomes were changes in BMI and serum TG levels. Laboratory tests were conducted in addition to the secondary outcomes, gut flora analysis, and Japanese version of the Work Limitations Questionnaire (WLQ-J). Safety was evaluated based on the number of adverse events and abnormal test results.
2.6. Procedures
Visceral fat area and waist circumference measurement: Visceral fat area and waist circumference were measured using an EW-FA90 (Panasonic, Osaka, Japan). This equipment measures the visceral fat area using bioelectrical impedance [17]. Before undergoing measurement, the participants were asked to eat dinner at 21:00 on the day before the test, refrain from alcohol consumption, avoid eating and drinking after 21:00 on the day before the test (participants were allowed to drink water or a small amount of warm water), avoid excessive exercise beyond the daily range the day before the test, and refrain from smoking until after the measurement. The abdomen was exposed, and a belt was worn to measure intra-abdominal resistance at the navel level.
Blood pressure measurement: Systolic and diastolic blood pressures were measured at the same time using an HEM-705IT (Omron Healthcare, Kyoto, Japan) in the morning on the measurement day. Participants sat in a chair for at least 5 min at rest after measuring their blood pressures.
Laboratory tests: The following laboratory tests were performed: total protein, total albumin, total bilirubin, direct bilirubin, alkaline phosphatase, aspartate aminotransferase, alanine aminotransferase, lactate dehydrogenase, γ-glutamyl transferase, total cholesterol, TG, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), non-HDL-C, urea nitrogen, creatinine, uric acid, sodium, potassium, chloride, glucose, and hemoglobin a1c (HbA1c).
Fecal sampling, DNA extraction, and sequencing: Fecal samples were collected using Mykinso fecal collection kits containing a guanidine thiocyanate solution (Cykinso, Inc., Tokyo, Japan) and stored at 4 ℃. DNA was extracted from fecal samples using an automated DNA extraction machine (GENE PREP STAR PI-1200A; Kurabo Industries Ltd., Osaka, Japan) according to the manufacturer’s protocol. The V1–V2 region of the 16S rRNA gene was amplified using forward primers (16S_27Fmod: TCG TCG GCA GCG TCA GAT GTG TAT AAG AGA CAG AGR GTT TGA TYM TGG CTC AG) and reverse primers (16S_338R: GTC TCG TGG GCT CGG AGA TGT GTA TAA GAG ACA GTG CTG CCT CCC GTA GGA GT) with KAPA HiFi Hot Start Ready Mix (Roche). To sequence the 16S rRNA amplicons using the Illumina MiSeq platform, dual-index adapters were attached with the Nextera XT Index Kit. Each library was diluted to 5 ng/µL, and equal volumes of the libraries were mixed at 4 nM. The DNA concentration of the mixed libraries was quantified by quantitative polymerase chain reaction (qPCR) with the KAPA SYBR FAST qPCR Master Mix (KK4601, KAPA Biosystems), using primers 1 (AAT GAT ACG GCG ACC ACC) and 2 (CAA GCA GAA GAC GGC ATA CGA). Libraries were prepared according to the Illumina 16S library preparation protocol (Illumina, San Diego, CA, USA). Libraries were sequenced using the MiSeq Reagent Kit v2 (500 cycles) and 250 bp paired-ends.
Taxonomy assignment based on 16S rRNA gene sequences: The paired-end reads of the partial 16S rRNA gene sequences were analyzed using QIIME 2 (version 2020.8). The steps for data processing and assignment based on the QIIME 2 pipeline were as follows: (1) DADA2 for joining paired-end reads, filtering, and denoising and (2) assigning taxonomic information to each ASV using the naive Bayes classifier in the QIIME 2 classifier with the 16S gene of the V1-V2 region data of SILVA (version 138) to determine the identity and composition of the bacterial genera.
Assessment of presenteeism (WLQ-J): The WLQ-J was used to evaluate work-related productivity (presenteeism). The WLQ-J is a self-administered questionnaire that estimates the degree to which health problems affect job performance (work disability) and the impact of work productivity on work limitations in the previous two weeks [18].
2.7. Statistical Analysis
In our previous in-house study, 31 participants with a visceral fat area of >100 cm2 consumed the Optimized Nutri-Dense Meals for a duration of four weeks. The Hedges effect size for the reduction in the visceral fat area was calculated to be 0.62. Furthermore, with a set alpha level of 0.05 and 80% statistical power, the sample size was determined to be 50, accounting for dropout rates, as calculated by Bell Curve for Excel (ver. 3.23). The intervention duration in the present study was based on this previous research. The parameters analyzed in this study are presented as means ± standard deviations (SDs). The efficiency analysis was based on a per-protocol set. Safety analysis was based on a modified intent-to-treat principle (full analysis set).
To compare the numerical data between the control and test groups, the degree of change from week 0 was assessed using Student's t-test. For all two-sided tests, the significance level was set at 5%. Statistical analyses were performed using IBM SPSS Statistics version 27 (IBM Corporation, NY, US).
3. Results
3.1. Participants
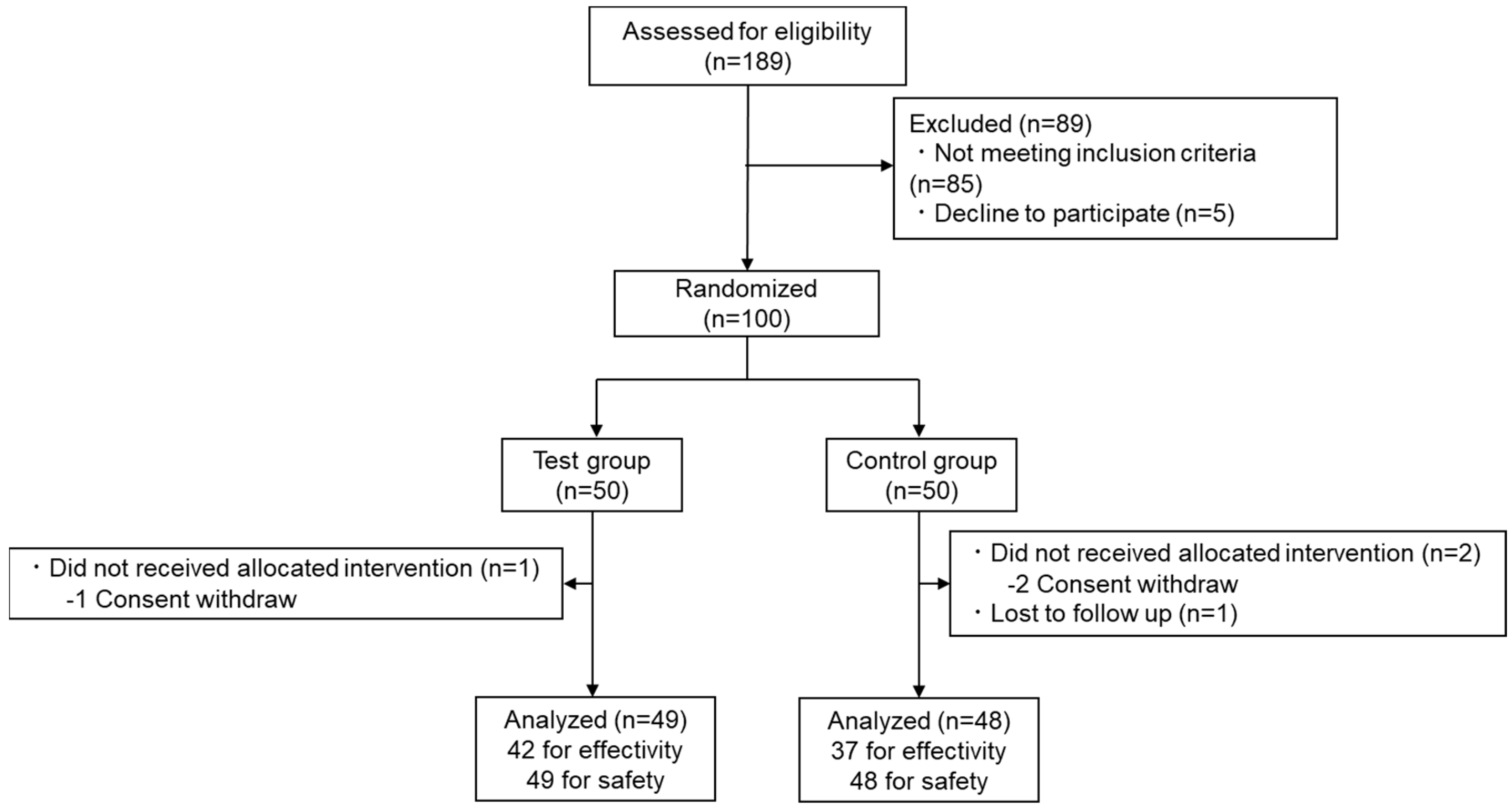
In total, 189 participants were recruited and screened, 100 of whom were enrolled and randomly allocated to the test or control groups (Figure 2). Three participants (one from the test group and two from the control group) withdrew from the study before further assessment for personal reasons unrelated to the trial. One additional participant withdrew from the study because of reasons unrelated to the trial. The overall dropout rate was 4%. Data from participants whose nutritional surveys and changes in exercise habits and lifestyles, based on interviews with the principal investigator and their diaries, were judged by the principal investigator as having the potential to interfere with the interpretation of the results and were excluded before statistical analysis. Significant differences in calorie intake and BDHQ test results between the groups were not observed at four weeks (control, 1821±594 kcal; test, 1689±596 kcal; p = 0.330). The demographic characteristics of each group are presented in Table 2.
3.2. Efficiency
The differences in the mean visceral fat area from week 0 to week 4 are shown in Table 3. Visceral fat area in the test group was more significantly reduced in the test group than that in the control group (p = 0.033). Moreover, BMI was more significantly reduced in the test group than that in the control group (p = 0.038). However, changes in TG levels were not significantly different (p = 0.316). Furthermore, body weight (p = 0.044), waist circumference (p = 0.033), non-HDL-C levels (p = 0.026), and HbA1c levels (p = 0.036) were more significantly reduced in the test group than those in the control group. Conversely, the occupancies of Bifidobacterium (p = 0.016) and the family Christensenellaceae (p = 0.046), as well as the WLQ-J total score (p = 0.020), were more significantly increased in the test group than those in the control group.
3.3. Safety
Eleven adverse events (four in the control group and seven in the test group) were reported (Supplementary Table S2A). The principal investigator determined that none of the adverse events were related to the test food. The values of all the parameters measured at weeks 0 and 4 to assess the safety of the intervention are shown in Supplementary Table S2B,C.
4. Discussion
This study showed that replacing patients’ usual diets with Optimized Nutri-Dense Meals on weekdays for four weeks reduced the visceral fat area and had additional positive effects. Visceral fat accumulation has a marked impact on CVD and metabolic syndrome [19]; thus, reducing visceral fat is important to prevent socially significant diseases. In this article, we discussed two types of interventions to combat visceral fat accumulation: nutritional education and dietary interventions. However, nutritional education is challenging in terms of exerting sufficient effects in everyday life [20]. Thus, the importance of dietary interventions, especially meal replacement, has been highlighted. The MD and washoku are potential candidates for intervention. The MD has been reported to reduce visceral fat in multiple RCTs with calorie restrictions [21,22]. In contrast, ad libitum intake of the MD did not reduce visceral fat in patients with coronary heart disease [23]. Other positive effects of the MD and washoku on visceral fat have also been reported [8,13]. However, food culture and distribution make widespread implementation of these diets difficult [14].
Here, we evaluated Optimized Nutri-Dense Meals, which is defined by nutrition content, rather than ingredients like the MD and washoku [14]. The total available energy of our intervention was relatively low (about 800 kcal/two meals on weekdays), but the diet was less strict than those in comparable studies, as other meals were not restricted in our study. Furthermore, the total calorie intake of the test group during the study period, tested using the BDHQ, was not significantly different from that of the control group, as shown in the Results section. Therefore, the advisable adjustment of nutritional balance, rather than calorie restriction, contributed to these results.
Our study also addressed micronutrient balance. A previous cohort study revealed that seven types of micronutrients–soluble dietary fiber, manganese, potassium, magnesium, vitamin K, folic acid, and pantothenic acid–are negatively associated with visceral fat accumulation [24]. Optimized Nutri-Dense Meals may address these deficiencies (Table 1) and potentially contribute to visceral fat reduction. Although dietary fiber was enriched in Optimized Nutri-Dense Meals, additional research is required to specify the ratio of soluble to insoluble fiber. Furthermore, it is unclear which nutrients primarily contribute to these observed effects.
The amount of dietary saturated fatty acids (SFAs) may also contribute to visceral fat outcomes. The amount of SFAs in Optimized Nutri-Dense Meals was limited to 6.2 g per two meal portions (Table 1). A previous RCT revealed that excessive SFA intake increased visceral fat [25]. However, an epidemiological study revealed that Japanese individuals consumed a relatively high amount of SFAs, ranging from 11.6 g/day to 14.1 g/day [26]. Considering these factors, reducing SFA intake may have contributed to decreased visceral fat.
In addition to the primary outcomes, significant improvements in health were observed across other areas, which have implications for future studies.
Our intervention increased the occupancies of Bifidobacterium and the family Christensenellaceae. Bifidobacterium is known for its anti-inflammatory effects, and its levels appear to be lower in obese people than those in lean people [27]. Bifidobacterium is a common target for prebiotic therapies against obesity, and prebiotic oligosaccharides, such as inulin, have been shown to stimulate their growth [28]. Additionally, a fiber-rich diet has been reported to enrich Bifidobacterium; for example, the MD improves Bifidobacterium occupancy in patients with human immunodeficiency virus (HIV)-1 [29]. Because water-soluble vitamins, such as vitamins B1 and B2, are considered to be important for Bifidobacterium growth [30], the richness of vitamins in the diet might further contribute to their growth. The family Christensenellaceae has been reported to be associated with reduced weight gain [31,32]. In a study in which participants followed an MD-modified ketogenic diet for six weeks and were encouraged to consume 60%–65% fats, reduce SFAs, and limit carbohydrates to 10%, the occupancy of the family Christensenellaceae improved [33]. Similar results were found in our study, although our novel program did not limit carbohydrate intake but had similar recommendations for fat intake. The limitations of SFAs and well-balanced micronutrients may contribute to the improvement of the gut flora. Further studies are required to confirm these hypotheses.
Presenteeism, defined as going to work despite feeling unhealthy, has recently emerged as a topic of significant interest [34]. While nutritional sufficiency is associated with workplace productivity, interventions such as nutrition education have only a minor impact on presenteeism [3,35]. In our previous single-arm study, we found that our program could potentially improve presenteeism. This potential was further substantiated through our RCT.
HbA1c, representing an average of several durations of blood sugar levels, also significantly improved in the test group, compared with that the control group (Table 3). The same result was observed in a previous RCT in patients with higher HbA1c levels [15]. Nutritional content, especially fiber and vitamin D, has also been discussed. Our results indicate the robustness of this positive effect on glucose metabolism.
As mentioned in the Introduction section, this trial provides insights into the impact of dietary intervention based on the DRIs. Experts’ critical reviews created the DRIs; however, to the best of our knowledge, its effectiveness in decreasing visceral fat has not been determined [14]. Few reports of intervention studies on government-published guidelines currently exist. The food-based guidelines reported by McCarthy (U.S.’s My Plate Guide) [36] and Fuller (Australian Guideline for Healthy Eating) [37] are examples, but they ar not DRIs. Since daily meals were not fully replaced in our trial, the impact of replacing all three daily meals with Optimized Nutri-Dense Meals should be determined in future studies.
This study has four limitations. First, the intervention period was short (four weeks). As the Cochrane review on the anti-obesity effect of catechin set 12 weeks as the minimum and 12–24 months as the medium term, our program should be evaluated for such lengths in the future [38]. Thus, another trial with a longer testing period is required. Second, the number of participants was limited to obese and overweight Japanese men. Notably, visceral fat tends to decrease more in men compared with women [39]. Further studies involving women should be conducted. According to a previous systematic review, Asians accumulate abdominal visceral fat more readily than Westerners [2]. Therefore, the effect on other ethnic groups should be determined in the future. While the nutrient content of the test meal in this study was based on the Japanese DRIs, whether the same effect could be expected under the same conditions in other populations must be verified. Third, serum TG level, one of the secondary outcomes, did not significantly improve, although the change was sufficient. We aim to evaluate the effectiveness of TG using an appropriate sample size in future studies. Finally, the key substances responsible for effectiveness were not isolated. Further research is required to identify the key substances and mechanisms involved. Comparisons between partially augmented dietary programs, such as vitamin- and mineral-only programs, could help solve this problem.
5. Conclusions
Our findings indicate that Optimized Nutri-Dense Meals based on the Japanese DRIs, replacing two meals per weekday for four weeks, might have a visceral fat-reducing effect in obese and overweight men. Furthermore, BMI, waist circumference, non-HDL-C level, HbA1c level, gut flora, and presenteeism significantly improved. This study highlights the importance of continuing a dietary intervention that includes multiple nutrients to prevent visceral fat accumulation, without completely replacing the daily diet. Our results also highlight the impact of dietary patterns based on DRIs.
6. Patents
None.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org: Figure S1, CONSORT2010 checklist; Table S1, Complete menu and nutrition content of test meals; Table S2A, All adverse events reported throughout the study; Table S2B, Blood test results; Table S2C, Urinalysis results.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following contributions were made: conceptualization, N.S., T.N., Y.H. and F.N.; methodology, N.S.; formal analysis, H.S.; writing—original draft preparation, N.S. .; writing, review, and editing, T.N., Y.H., and F.N.; visualization, N.S.; supervision, K.H.; project administration, T.Y. All authors have read and agreed to the published version of the manuscript.
Funding
Nissin Foods Holdings Co., Ltd. funded this research and provided the test food.
Institutional Review Board Statement
This study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Medical Station Clinic Research Ethics Committee (approval no. 210114-3), following ethical guidelines for research on humans (Ministry of Education, Culture, Sports, Science and Technology; Ministry of Health, Labor and Welfare, Japan). The trial was registered in the UMIN Clinical Trials Registry (registration no. UMIN000043180).
Informed Consent Statement
Informed consent was obtained from all participants to publish the results as a treatise under the condition that their personal information would not be disclosed.
Data Availability Statement
Data would be provided to the researchers who presented plans with appropriate methodologies and obtained consent from all co-authors.
Acknowledgments
We thank the participants of this study and the staff of Kouwa Clinic and EP Mediate.
Conflicts of Interest
N.S., T.N., Y.H., and F.N. are employed by Nissin Foods Holdings. H.S. is employed by EP Mediate Co., Ltd. T.Y. and K.H. have no relevant financial interests to declare.
References
- Neeland, I.J.; Ross, R.; Després, J.P.; Matsuzawa, Y.; Yamashita, S.; Shai, I.; Seidell, J.; Magni, P.; Santos, R.D.; Arsenault, B.; et al. Visceral and Ectopic Fat, Atherosclerosis, and Cardiometabolic Disease: A Position Statement. Lancet Diabetes Endocrinol 2019, 7, 715–725. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, S.; Horimai, C.; Katsukawa, F. Ethnic Differences in Abdominal Visceral Fat Accumulation between Japanese, African-Americans, and Caucasians: A Meta-Analysis. In Proceedings of the Acta Diabetologica; October 2003; Vol. 40. [Google Scholar]
- Drewnowski, A. Impact of Nutrition Interventions and Dietary Nutrient Density on Productivity in the Workplace. Nutr Rev 2020, 78, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Geaney, F.; Kelly, C.; Greiner, B.A.; Harrington, J.M.; Perry, I.J.; Beirne, P. The Effectiveness of Workplace Dietary Modification Interventions: A Systematic Review. Prev Med (Baltim) 2013, 57, 438–447. [Google Scholar] [CrossRef] [PubMed]
- Wilson, K.A.; Chamoli, M.; Hilsabeck, T.A.; Pandey, M.; Bansal, S.; Chawla, G.; Kapahi, P. Evaluating the Beneficial Effects of Dietary Restrictions: A Framework for Precision Nutrigeroscience. Cell Metab 2021, 33, 2142–2173. [Google Scholar] [CrossRef]
- Shen, W.; Chen, J.; Zhou, J.; Martin, C.K.; Ravussin, E.; Redman, L.M. Effect of 2-Year Caloric Restriction on Organ and Tissue Size in Nonobese 21- To 50-Year-Old Adults in a Randomized Clinical Trial- To CALERIE Study. American Journal of Clinical Nutrition 2021, 114, 1295–1303. [Google Scholar] [CrossRef]
- Hemmingsson, E.; Johansson, K.; Eriksson, J.; Sundström, J.; Neovius, M.; Marcus, C. Weight Loss and Dropout during a Commercial Weight-Loss Program Including a Very-Low-Calorie Diet, a Low-Calorie Diet, or Restricted Normal Food: Observational Cohort Study. Am J Clin Nutr 2012, 96, 953–961. [Google Scholar] [CrossRef] [PubMed]
- Roberts, C.K.; Barnard, R.J.; Croymans, D.M. Weight Loss with a Low-Carbohydrate, Mediterranean, or Low-Fat Diet. New England Journal of Medicine 2008, 359, 2169–2172. [Google Scholar] [CrossRef] [PubMed]
- Di Renzo, L.; Cioccoloni, G.; Falco, S.; Abenavoli, L.; Moia, A.; Sinibaldi Salimei, P.; De Lorenzo, A. Influence of FTO Rs9939609 and Mediterranean Diet on Body Composition and Weight Loss: A Randomized Clinical Trial NCT01890070 NCT. J Transl Med 2018, 16, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Mentella, M.C.; Scaldaferri, F.; Ricci, C.; Gasbarrini, A.; Miggiano, G.A.D. Cancer and Mediterranean Diet: A Review. Nutrients 2019, 11, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Esposito, K.; Giugliano, D. Mediterranean Diet and Type 2 Diabetes. Diabetes Metab Res Rev 2014, 30, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Asano, M.; Kushida, M.; Yamamoto, K.; Tomata, Y.; Tsuji, I.; Tsuduki, T. Abdominal Fat in Individuals with Overweight Reduced by Consumption of a 1975 Japanese Diet: A Randomized Controlled Trial. Obesity 2019, 27, 899–907. [Google Scholar] [CrossRef] [PubMed]
- Sakane, N.; Osaki, N.; Takase, H.; Suzuki, J.; Suzukamo, C.; Nirengi, S.; Suganuma, A.; Shimotoyodome, A. The Study of Metabolic Improvement by Nutritional Intervention Controlling Endogenous GIP (Mini Egg Study): A Randomized, Cross-over Study. Nutr J 2019, 18, 52. [Google Scholar] [CrossRef] [PubMed]
- Shobako, N.; Itoh, H.; Honda, K. Typical Guidelines for Well-Balanced Diet and Science Communication in Japan and Worldwide. Nutrients 2024, 16, 2112. [Google Scholar] [CrossRef] [PubMed]
- Shobako, N.; Goto, C.; Nakagawa, T.; Yamato, T.; Kondo, S.; Nakamura, F.; Nakazeko, T.; Hirano, Y.; Honda, K. Hypotensive and HbA1c Reducing Effect of Novel Dietary Intervention Program “COMB Meal Program”: Two Randomized Clinical Trials. J Funct Foods 2022, 98. [Google Scholar] [CrossRef]
- Nakazeko, T.; Shobako, N.; Hirano, Y.; Nakamura, F.; Honda, K. Novel Dietary Intervention Program “COMB Meal Program” Approaching Health and Presenteeism: Two Pilot Studies. J Funct Foods 2022, 92, 105050. [Google Scholar] [CrossRef]
- Ryo, M.; Maeda, K.; Onda, T.; Katashima, M.; Okumiya, A.; Nishida, M.; Yamaguchi, T.; Funahashi, T.; Matsuzawa, Y.; Nakamura, T.; et al. 2005.
- Yokota, J.; Fukutani, N.; Nin, K.; Yamanaka, H.; Yasuda, M.; Tashiro, Y.; Matsushita, T.; Suzuki, Y.; Yokota, I.; Teramukai, S.; et al. Association of Low Back Pain with Presenteeism in Hospital Nursing Staff. J Occup Health 2019, 61, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Maeda, N.; Funahashi, T.; Matsuzawa, Y.; Shimomura, I. Adiponectin, a Unique Adipocyte-Derived Factor beyond Hormones. Atherosclerosis 2020, 292, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Michalczyk, M.M.; Zajac-Gawlak, I.; Zając, A.; Pelclová, J.; Roczniok, R.; Langfort, J. Influence of Nutritional Education on the Diet and Nutritional Behaviors of Elderly Women at the University of the Third Age. Int J Environ Res Public Health 2020, 17, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Bajerska, J.; Chmurzynska, A.; Muzsik, A.; Krzyżanowska, P.; Mądry, E.; Malinowska, A.M.; Walkowiak, J. Weight Loss and Metabolic Health Effects from Energy-Restricted Mediterranean and Central-European Diets in Postmenopausal Women: A Randomized Controlled Trial. Sci Rep 2018, 8, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Panizza, C.E.; Lim, U.; Yonemori, K.M.; Cassel, K.D.; Wilkens, L.R.; Harvie, M.N.; Maskarinec, G.; Delp, E.J.; Lampe, J.W.; Shepherd, J.A.; et al. Effects of Intermittent Energy Restriction Combined with a Mediterranean Diet on Reducing Visceral Adiposity: A Randomized Active Comparator Pilot Study. Nutrients 2019, 11, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Mayr, H.L.; Itsiopoulos, C.; Tierney, A.C.; Kucianski, T.; Radcliffe, J.; Garg, M.; Willcox, J.; Thomas, C.J. Ad Libitum Mediterranean Diet Reduces Subcutaneous but Not Visceral Fat in Patients with Coronary Heart Disease: A Randomised Controlled Pilot Study. Clin Nutr ESPEN 2019, 32, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Ozato, N.; Saito, S.; Yamaguchi, T.; Katashima, M.; Tokuda, I.; Sawada, K.; Katsuragi, Y.; Imoto, S.; Ihara, K.; Nakaji, S. Association between Nutrients and Visceral Fat in Healthy Japanese Adults: A 2-Year Longitudinal Study Brief Title: Micronutrients Associated with Visceral Fat Accumulation. Nutrients 2019, 11, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Rosqvist, F.; Iggman, D.; Kullberg, J.; Cedernaes, J.; Johansson, H.E.; Larsson, A.; Johansson, L.; Ahlström, H.; Arner, P.; Dahlman, I.; et al. Overfeeding Polyunsaturated and Saturated Fat Causes Distinct Effects on Liver and Visceral Fat Accumulation in Humans. Diabetes 2014, 63, 2356–2368. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, M.; Harada, S.; Tsubota, K.; Yasukawa, T.; Takebayashi, T.; Nishiwaki, Y.; Kawasaki, R. Dietary Saturated Fatty Acid Intake and Early Age-Related Macular Degeneration in a Japanese Population. Invest Ophthalmol Vis Sci 2020, 61, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Gasteyger, C.; Larsen, T.M.; Vercruysse, F.; Pedersen, D.; Toubro, S.; Astrup, A. Visceral Fat Loss Induced by a Low-Calorie Diet: A Direct Comparison between Women and Men. Diabetes Obes Metab 2009, 11, 596–602. [Google Scholar] [CrossRef] [PubMed]
- Million, M.; Maraninchi, M.; Henry, M.; Armougom, F.; Richet, H.; Carrieri, P.; Valero, R.; Raccah, D.; Vialettes, B.; Raoult, D. Obesity-Associated Gut Microbiota Is Enriched in Lactobacillus Reuteri and Depleted in Bifidobacterium Animalis and Methanobrevibacter Smithii. Int J Obes 2012, 36, 817–825. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, A.K.; Brunius, C.; Mazidi, M.; Hellström, P.M.; Risérus, U.; Iversen, K.N.; Fristedt, R.; Sun, L.; Huang, Y.; Nørskov, N.P.; et al. Effects of Whole-Grain Wheat, Rye, and Lignan Supplementation on Cardiometabolic Risk Factors in Men with Metabolic Syndrome: A Randomized Crossover Trial. American Journal of Clinical Nutrition 2020, 111, 864–876. [Google Scholar] [CrossRef] [PubMed]
- Pastor-Ibáñez, R.; Blanco-Heredia, J.; Etcheverry, F.; Sánchez-Palomino, S.; Díez-Fuertes, F.; Casas, R.; Navarrete-Muñoz, M.Á.; Castro-Barquero, S.; Lucero, C.; Fernández, I.; et al. Adherence to a Supplemented Mediterranean Diet Drives Changes in the Gut Microbiota of Hiv-1-Infected Individuals. Nutrients 2021, 13, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Yoshii, K.; Hosomi, K.; Sawane, K.; Kunisawa, J. Metabolism of Dietary and Microbial Vitamin b Family in the Regulation of Host Immunity. Front Nutr 2019, 6, 1–12. [Google Scholar] [CrossRef]
- Goodrich, J.K.; Waters, J.L.; Poole, A.C.; Sutter, J.L.; Koren, O.; Blekhman, R.; Beaumont, M.; Van Treuren, W.; Knight, R.; Bell, J.T.; et al. Human Genetics Shape the Gut Microbiome. Cell 2014, 159, 789–799. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Mantrana, I.; Selma-Royo, M.; Alcantara, C.; Collado, M.C. Shifts on Gut Microbiota Associated to Mediterranean Diet Adherence and Specific Dietary Intakes on General Adult Population. Front Microbiol 2018, 9, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Nagpal, R.; Neth, B.J.; Wang, S.; Craft, S.; Yadav, H. Modified Mediterranean-Ketogenic Diet Modulates Gut Microbiome and Short-Chain Fatty Acids in Association with Alzheimer’s Disease Markers in Subjects with Mild Cognitive Impairment. EBioMedicine 2019, 47, 529–542. [Google Scholar] [CrossRef]
- Johns, G. Presenteeism in the Workplace: A Review and Research Agenda. J Organ Behav 2010, 31, 519–542. [Google Scholar] [CrossRef]
- Jensen, J.D. Can Worksite Nutritional Interventions Improve Productivity and Firm Profitability? A Literature Review. Perspect Public Health 2011, 131, 184–192. [Google Scholar] [CrossRef]
- McCarthy, W.J.; Rico, M.; Chandler, M.; Herman, D.R.; Chang, C.; Belin, T.R.; Love, S.; Ramirez, E.; Gelberg, L. Randomized Comparative Effectiveness Trial of 2 Federally Recommended Strategies to Reduce Excess Body Fat in Overweight, Low-Income Patients: Myplate.Gov vs Calorie Counting. Ann Fam Med 2023, 21, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Fuller, N.R.; Fong, M.; Gerofi, J.; Leung, L.; Leung, C.; Denyer, G.; Caterson, I.D. A Randomized Controlled Trial to Determine the Efficacy of a High Carbohydrate and High Protein Ready-to-Eat Food Product for Weight Loss. Clin Obes 2016, 6, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Jurgens, T.M.; Whelan, A.M.; Killian, L.; Doucette, S.; Kirk, S.; Foy, E. Green Tea for Weight Loss and Weight Maintenance in Overweight or Obese Adults. Cochrane Database of Systematic Reviews 2012, 2012. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Example lunch box. (A) Photograph of the overall lunch box. (B) Nutritional components of the meal. *K: Potassium, Ca: Calcium, Mg: Magnesium, P: Phosphorus, Ir: Iron, Zn: Zinc, Cu: Copper, Mn: Manganese, I: Iodine, Se: Selenium, Cr: Chromium, Mo: Molybdenum, RAE: Retinol Active Equivalent, VD: Vitamin D, αTOC: α-Tocopherol, VK: Vitamin K, VB1: Vitamin B1, VB2: Vitamin B2, Nia: Niacin, VB6: Vitamin B6, VB12: Vitamin B12, FA: Folic Acid, PA: Pantothenic Acid, VC: Vitamin C, n6FA: n6 Fatty Acid, n3FA: n3 Fatty Acid. Ile: Isoleucine, Leu: Leucine, Lys: Lysine, Thr: Threonine, Trp: Tryptophan, Val: Valine, His: Histidine.
Figure 1.
Example lunch box. (A) Photograph of the overall lunch box. (B) Nutritional components of the meal. *K: Potassium, Ca: Calcium, Mg: Magnesium, P: Phosphorus, Ir: Iron, Zn: Zinc, Cu: Copper, Mn: Manganese, I: Iodine, Se: Selenium, Cr: Chromium, Mo: Molybdenum, RAE: Retinol Active Equivalent, VD: Vitamin D, αTOC: α-Tocopherol, VK: Vitamin K, VB1: Vitamin B1, VB2: Vitamin B2, Nia: Niacin, VB6: Vitamin B6, VB12: Vitamin B12, FA: Folic Acid, PA: Pantothenic Acid, VC: Vitamin C, n6FA: n6 Fatty Acid, n3FA: n3 Fatty Acid. Ile: Isoleucine, Leu: Leucine, Lys: Lysine, Thr: Threonine, Trp: Tryptophan, Val: Valine, His: Histidine.
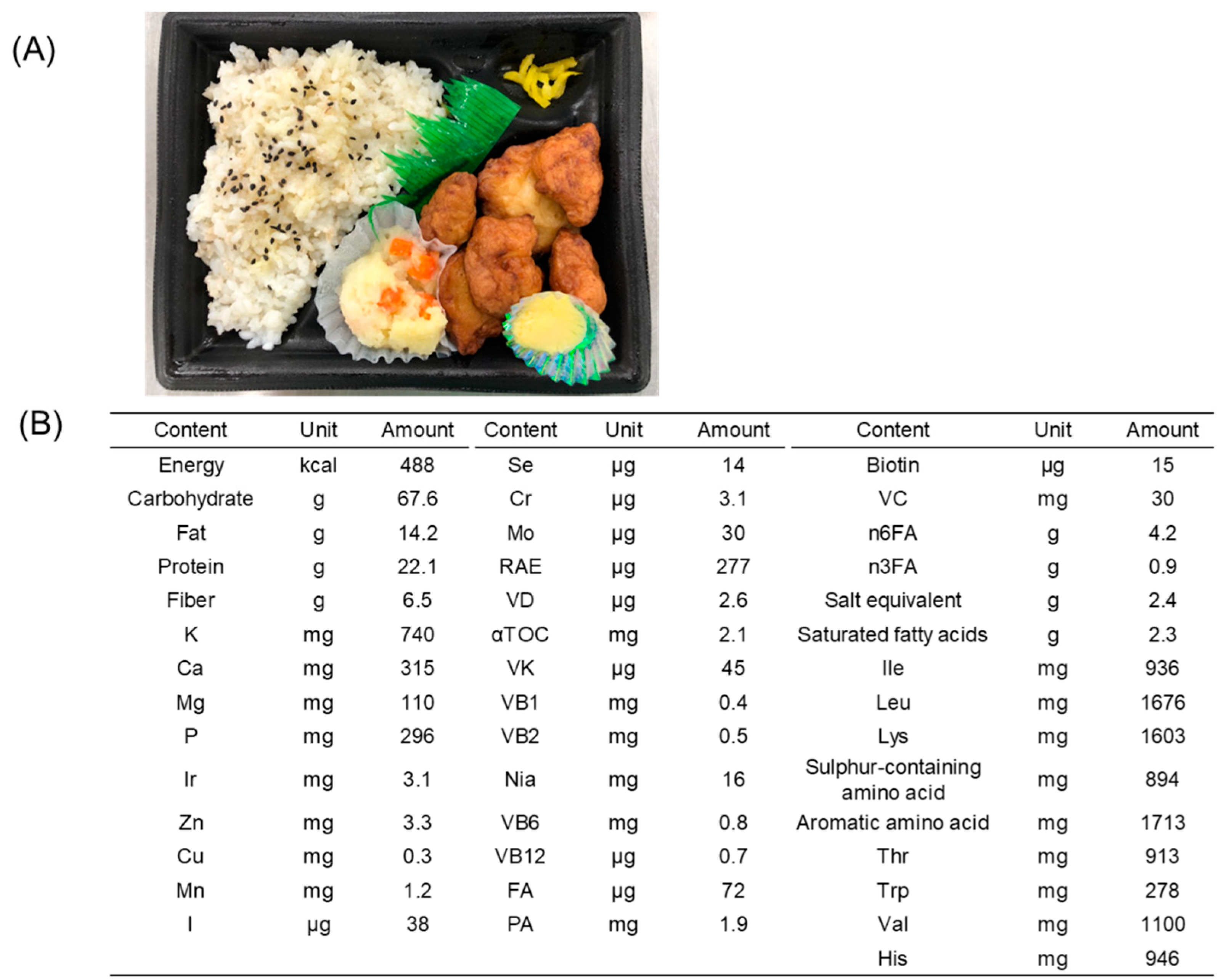
Figure 2.
CONSORT 2010 Flow Diagram for Study Participants.
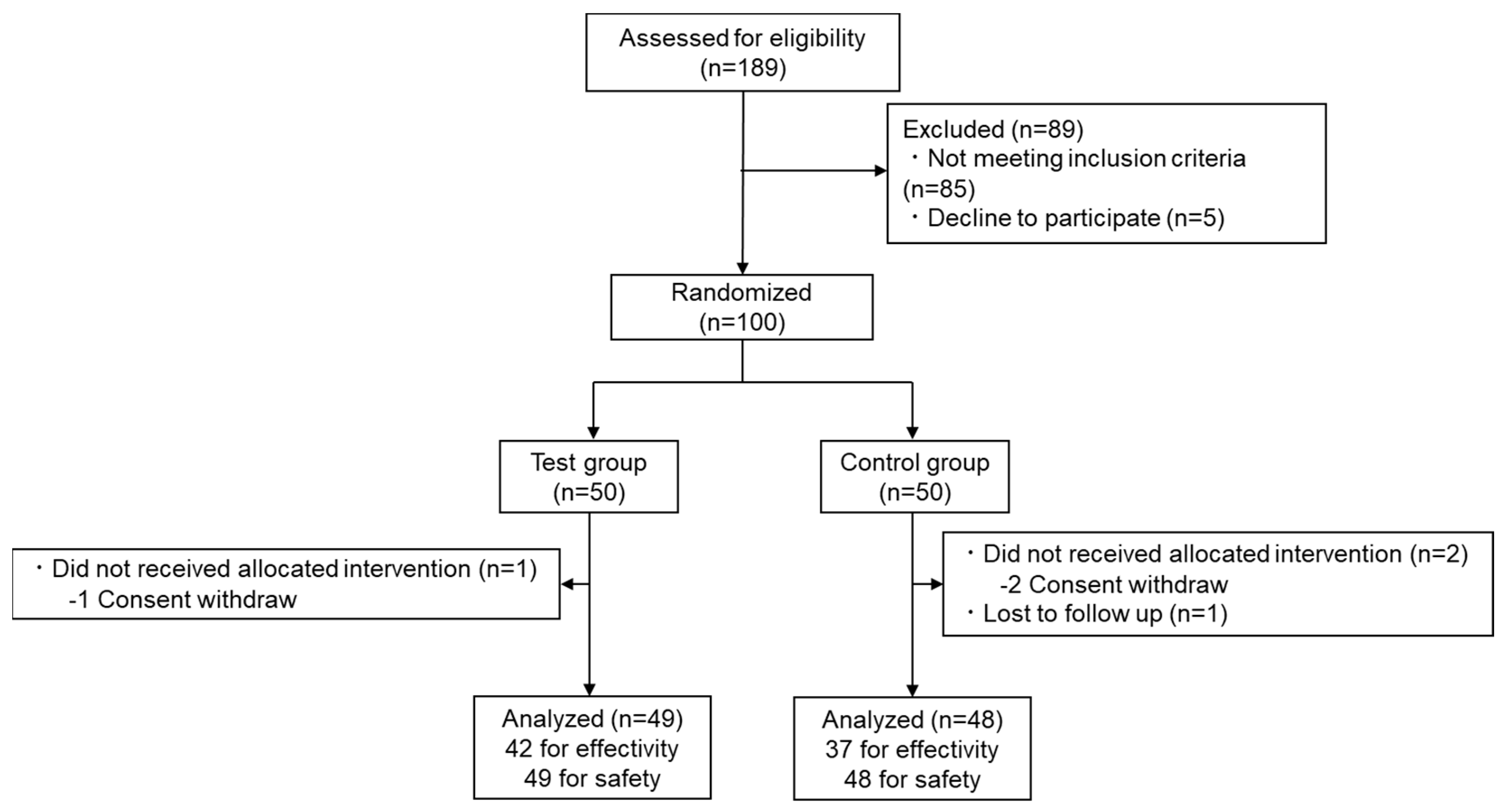

Table 1.
Limit of each nutritional component per portion of tested meals.
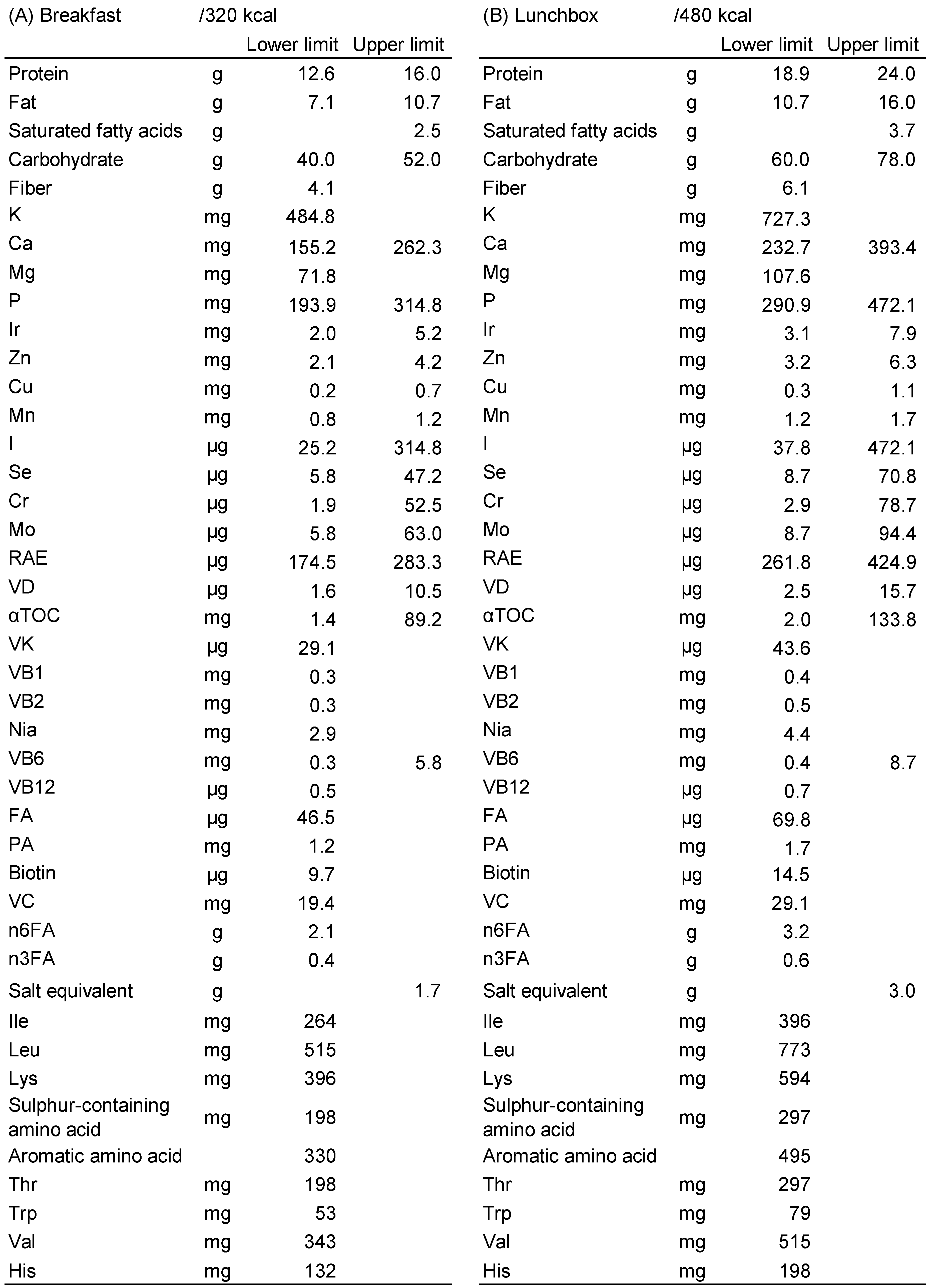 |
K: Potassium, Ca: Calcium, Mg: Magnesium, P: Phosphorus, Ir Iron, Zn: Zinc, Cu: Cupper, Mn: Manganese, I: Iodine, Se: Selenium, Cr: Chromium, Mo: Molybdenum, RAE: Retinol active equivalent, VD: Vitamin D, αTOC: α-tocopherol, VK: Vitamin K, VB1: Vitamin B1, VB2: Vitamin B2, Nia: Niacin, VB6: Vitamin B6, VB12: Vitamin B12, FA: Folic acid, PA: Pantothenic acid, VC: Vitamin C, n6FA: n6 Fatty acid, n3FA: n3 Fatty acid, Ile: Isoleucine, Leu: Leucine, Lys: Lysine, Thr: Threonine, Trp: Tryptophan, Val: Valine, His: Histidine.
Table 2.
Participant Characteristics.
 |
Each value is expressed as the mean ± SD. BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; TG, triglyceride; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; Glu, fasting blood glucose; HbA1c, hemoglobin A1c; SD, standard deviation.
Table 3.
Evaluation of the effectiveness of the trial.
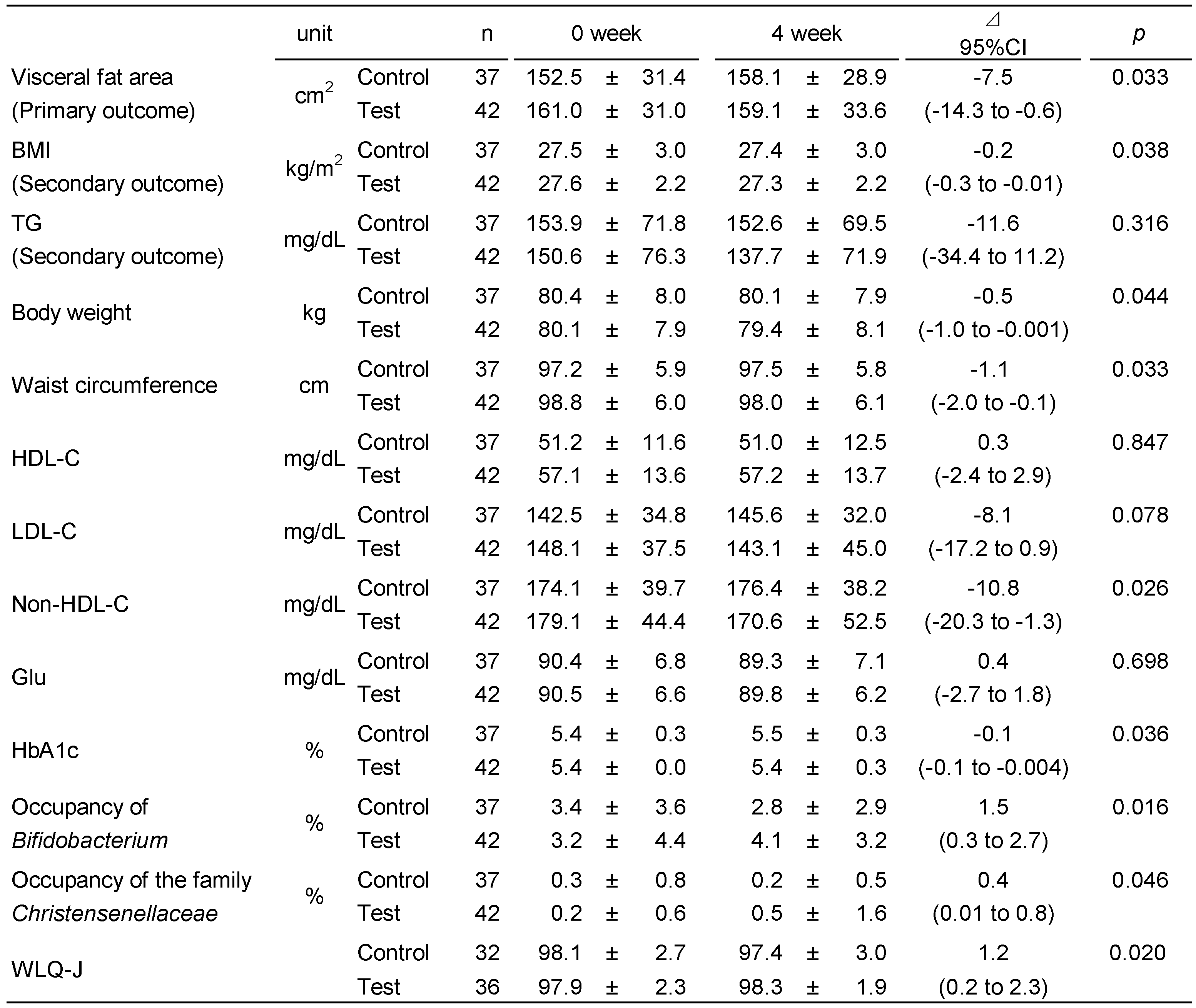 |
Each value is expressed as the mean ± SD. BMI, body mass index; TG, triglyceride; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; Glu, fasting blood glucose; HbA1c, hemoglobin A1c; WLQ-J, Work Limitation Questionnaire-Japanese; SD, standard deviation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



