
Submitted:
09 August 2024
Posted:
12 August 2024
You are already at the latest version
Abstract
Background: Hairy cell leukemia (HCL) is a rare indolent B-cell lymphoid malignancy. The majority of patients are asymptomatic and HCL is usually diagnosed incidentally during a routine blood cell counts. In symptomatic patients, typical symptoms are related to pancytope-nia and splenomegaly. In this review we present, rare clinical symptoms in patients with HCL. Methods: A literature search was conducted of PubMed, Web of Science, and Google Scholar for articles concerning hairy cell leukemia, leukemia cutis, bone lesions, neurological manifesta-tions, pulmonary symptoms, ocular manifestations, cardiac manifestation, rare symptoms. Publications from January 1980 to August 2024 were scrutinized. Additional relevant publica-ions were obtained by reviewing the references from the chosen articles. Results: Extra medul-lary and extra nodal manifestations of classic HCL are rare. However, leukemic involvement in the skin, bone, central nervous system, gastrointestinal tract, heart, kidney, liver, lung, ocular and other organs have been reported.
Keywords:
hairy cell leukemia
; leukemia cutis
; pulmonary involvement
; bone lesions
; neurological manifestations
; pulmonary symptoms
; ocular manifestations
; cardiac manifestation
; rare symptoms
1. Introduction
Classic hairy cell leukemia (HCL) is a rare, indolent B-cell leukemia which makes up about 2% of all cases, with an annual incidence of about 0.3 cases per 100 000 [1,2]. Its typical clinical presentation involves pancytopenia, with a few circulating lymphoid cells with circumferential hair-like cytoplasmic projections, splenomegaly, constitutional symptoms and increased susceptibility to infection [3,4,5]. Lymphadenopathy is reported in 8.5% to 30% of patients. HCL occurs more predominantly in middle age, with median age of diagnosis of 56 years (range: 40–70 years) [1,2]. The disease is extremely rare in younger patients; however, a few cases of HCL have been reported in children [6]. A diagnosis of HCL can be achieved morphologically, based on the presence of hairy cells, and by the characteristic immunophenotype of the leukemic cells. Moreover, in classic HCL, most patients present with a BRAF V600E mutation as the causal genetic event. In symptomatic patients, typical symptoms are related to pancytopenia and splenomegaly. Extramedullary and extra nodal manifestations of classic HCL also occur, but rarely. However, leukemic involvement has been reported in the skin, bone, central nervous system, gastrointestinal tract, heart, kidney, liver, lung, ocular system and other organs [7,8,9,10]. HCL variant (HCLv) is a clinical-pathologic entity with intermediate features between classical HCL and B-cell prolymphocytic leukemia [11]. In the 5th edition of the WHO classification (WHO-HAEM5), classic HCL is classified as splenic lymphoma/ leukemia, together with splenic marginal zone lymphoma (SMZL) with circulating villous cells in the peripheral blood (PB), splenic lymphoma with prominent nucleolus (SLPN) and, splenic diffuse red pulp lymphoma (SDRPL) [12]. In this classification, HCLv is included as SLPN together with CD5 negative B-prolymphocytic leukemia (B-PLL). However, HCLv still exists in the clinical International Consensual Classification (ICC) [13,14]. Cladribine and pentostatin have been the drugs of choice for more than 30 years for newly-diagnosed HCL [1,2]. In relapsed patients, re-treatment with purine analogs, alone or in combination with rituximab, is still an acceptable option. However, re-treatment with single-agent purine analogs often results in shorter responses, with some patients becoming refractory to the drugs. For these patients, other treatment options can be considered, including interferon-α (IFN-α), rituximab, bendamustine, fludarabine or BRAF inhibitors, used alone or in combination [15,16]. This review presents some of the rare clinical symptoms reported in patients with classical HCL.
2. Common Clinical Presentation
The majority of patients with HCL are asymptomatic at diagnosis and the disease is usually found incidentally during routine blood cell counts [16]. The typical clinical presentation of classical HCL involves pancytopenia, monocytopenia, splenomegaly, constitutional symptoms and increased risk of infection [1,2]. In most patients, lymph nodes are not enlarged; however, an atypical presentation, such as absence of splenomegaly and presence of lymphadenopathy and leukocytosis, may also be observed in some patients. Diagnosis is based on peripheral blood (PB) and bone marrow (BM) morphology, flow cytometry, immunophenotyping, immunohistochemistry and molecular studies. Splenomegaly is a prominent feature of HCL and is present in 70 to 100% of cases. However, the absence of splenomegaly does not exclude a diagnosis of HCL [17].
The spleen is palpable in around 80% of cases, and in 60%, it is >5 cm below the left costal margin [16,18]. In one report, 33% of cases of HCL recorded over a 30-month observation presented without splenomegaly [19]. Lymphadenopathy is rare at diagnosis, being observed in 8.5% to 30% of cases in some reports [20,21], with significant lymphadenopathy being only occasionally reported in other studies [19].
A diagnosis of HCL is based on typical morphology, flow cytometry of the neoplastic cells in PB and bone marrow BM aspirate, immunohistochemistry and molecular studies [1,2]. Although bone marrow aspirate is often a dry tap due to extensive marrow fibrosis, bone marrow (trephine) biopsy may show interstitial or patchy infiltrate with a “fried egg” appearance of cells (due to abundant cytoplasm and prominent cell borders). Typical hairy cells are medium in size with moderately-abundant pale-blue cytoplasm with a characteristic serrated cytoplasmic border, reniform nuclei, open chromatin and absent nucleoli. The characteristic immunophenotype of classic HCL cells includes co-expression of CD19, CD20, CD11c, CD25, CD103, CD200, FMC7, and CD123. The unique criterion for diagnosis of HCL is co-expression of CD103, CD25 and CD11c. Also, HCL can be distinguished from other B-cell lymphomas, including HCLv, based on annexin A1 expression; indeed, it has been reported that Annexin A1 is a 100% specific immunohistochemical marker for classical HCL [22]. The BRAF V600E mutation is present in almost all HCL patients and it plays a key role in the pathogenesis of his disease [23]. Marked splenomegaly, high number of HCL cells in PB, elevated β2 microglobulin, and increased lactate dehydrogenase (LDH) can predict resistance to purine analogs. The absence of BRAF V600E mutation in HCL is rare and is associated with poorer prognosis.
3. Rare Clinical Symptoms
Extramedullary and extra nodal manifestations of classic HCL are rare events [9]. However, leukemic involvement in skin, bone, central nervous system, gastrointestinal tracts, heart, lungs and ocular involvement have been reported (Table 1) [7,8].
3.1. Skin Symptoms
Cutaneous manifestations of HCL have been reported in about 10-12% of patients [24]. Skin symptoms may be specific to HCL or mostly non-specific, due to autoimmune reactions, infections and secondary neoplastic or drug-induced reasons. Specific cutaneous manifestations known as leukemia cutis, are very rare and can be seen as maculopapular, or infiltrative eruptions [24,25,26,27]. Direct infiltration of the skin by leukemic cells is defined as infiltration of the epidermis, the dermis, and the subcutaneous tissue by leukemic cells. In HCL, leukemia cutis is manifested as disseminated, erythematous maculopapules or nodules ranging from violaceous to red-brown in color or flesh-colored nodules, with central ulceration in some patients (Figure 1A) [25]. Skin changes are localized in one region or are disseminated in several parts of the skin, and are characterized microscopically as a perivascular mononuclear leukemic cell infiltration. In patients with HCL, the diagnosis of leukemia cutis is performed based on the histopatology of skin biopsy and the immunophenotyping of neoplastic cells [27,28]. Skin biopsy and immunophenotyping must be performed in all patients with suspicion of leukemia cutis. Leukemia cutis should be differentiated with other cancers, vasculitis, infections and inflammation [29,30].

Table 1.
Rare symptoms in hairy cell leukemia.
| Involved organ/ frequency | Ethiology | Clinical characteristics | Diagnostic procedures | Prognosis | References |
|---|---|---|---|---|---|
| Skin/ 10-12% of HCL cases | Mostly due to autoimmune reactions, infections and secondary neoplastic or drug-induced. Very rare leukemia cutis | Vasculitis, neutrophilic dermatoses, periarteritis nodosa, leukemia cutis | Skin biopsy specimens with immunohistochemical staining | Not affected by HCL skin symptoms in most patients | [24,25,26,27,28,29,30,31,32,33,34,35,36,37,38] |
| Boone lesions/3% of HCL patients | Leukemic skeletal infiltrations | Localized pain, multifocal lytic changes, osteolytic and osteoblastic lesions, severe osteoporosis | Roentgenograms, MRI, CT, PET, core biopsy of involved bone | Prognosis is usually not affected, | [44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59] |
| Pulmonary changes/infections common, leukemic infiltrations very rare¶ | Infections, leukemic pulmonary infiltration, mediastinal infiltrations | Pulmonary symptoms- cough, dyspnea, chest pain, hemoptysis | Chest X-rey, CT, lung biopsy if antibiotics and antifungal treatment not effective. | Treatment with cladribine and/or rituximab induced regression of pulmonary involvement in most patients.¶ | [62,63,64,65,66,67,68] |
| Neurologic manifestations/5% of HCL patients | Infections, invasion of HCL cells to CNS (rare) | Confusion, aphasia, headache, meningeal syndrome, motor ataxia, dizziness, weakness, slurred speech, frequent falls, facial droop, fatigue, blurry vision | Imaging studies (NMR, CT, PET) and lumbar puncture | PNA +/- CD20 antibodies or BRAF inhibitors are usually effective in controlling CNS symptoms | [74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90] |
| Ocular symptoms/ few (12) cases reported¶ | Leukemic infiltration, bleeding, infections | Ocular or orbital manifestations in most cases, panuveitis, conjunctivitis, lekemic corneal infiltrate, retinopathy, visual disturbance | Ophthalmological examination (Visual acuity, funduscopic examination), CT, biopsy of ocular mass | Cladribine induced improvement of the ocular complications | [91,92,93,94,95,96,97,98,99,100,101,102,103,104] |
| Rheumatological symptoms¶ | Immune-mediated or direct, nonimmune mechanism | Athritis, joint pain and swelling, erythema, and tenderness | Serologic tests, X-ray of joints, cytologic evaluation of synovial fluid¶ | Prognosis usually good, antileukemic and immunosuppressive treatment effective | [123,124,125,126,127,128,129,130,131,132] |
Abbreviations: BM – bone marrow, CNS – central nervous system, CR – complete response, CT – computed tomography,HCL – hairy cell leukemia, MRI – magnetic resonance imaging, PET – positron emission tomography, PNA – purine nucleos.
In most presented cases, specific treatment for HCL resulted in the disappearance of cutaneous infiltrates. Vasculitis is one of the more common nonspecific skin changes in HCL patients [31,32,33] and vasculitis syndromes such as cutaneous leukocytoclastic vasculitis (CLCV) (Figure 1B), polyarteritis nodosa (PAN), pyoderma gangrenosum and paraneoplastic vasculitis have been noted in HCL and other lymphoid malignancies. Vasculitis can present as the initial manifestation of HCL or can be diagnosed in the course of disease [31,32,33,34]. Moreover, vasculitis may be a reaction to infection or a paraneoplastic syndrome related to HCL itself [35]. In one report of 42 HCL patients, CLCV was identified in 21 and PAN in 17 [36]. Neutrophilic dermatoses like Sweet’s syndrome, pyoderma gangrenosum or neutrophilic eccrine hidradenitis are rarely observed in HCL.
Sweet’s syndrome (acute febrile neutrophilic dermatosis), characterized by erythematous painful lesions, sometime in form of plaques, has been reported as a presenting symptom at diagnosis or at the relapse of HCL [37,38]. Pyoderma gangrenosum is a neutrophilic, reactive, non-infectious, inflammatory dermatosis involving the skin and mucosal tssue (Figure 1C). It has been reported in few cases with HCL. Pyoderma gangrenosum was successfully treated with cladribine, without other immunosuppressive drugs as cyclosporine or corticosteroids [39,40,41]. Elsewhere, Elkon et al describe four patients with HCL and systemic vasculitis similar to polyarteritis nodosa that developed within two years of the onset of HCL [42], while Zervas et al. present a case of leukaemia-associated polyarthritis [43].
The most common skin symptoms in HCL patients are bacterial or viral infections, with the most commonly seen being herpetic infections, including herpes simplex, zoster and generalized varicella (Figure 1C). However, verrucae, dermatophyte, candidal infections, and pyogenic infections (i.e., abscesses, cellulitis, folliculitis, and pyoderma) were also observed in some patients. Opportunistic skin infections, including atypical mycobacterial skin infections, fungal infections and Ecthyma gangrenosum have also been reported in HCL patients [24].
3.2. Bone Lesions
Bone symptoms in HCL include osteolytic and osteoblastic lesions, severe osteoporosis, aseptic necrosis of the femoral head and multifocal lytic changes [44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59]. Pathological femoral fractures and asymptomatic or painful diffuse osteosclerosis with extensive thickening of bone were also reported in some patients [50,51,52].
Skeletal infiltrations are observed in approximately 3% of HCL patients [53,54,55,56], and some patients present with skeletal infiltration at diagnosis [47,57]. However, in most patients, bone involvement is recognized between a few weeks and several years after diagnosis of HCL [53]. The median time from diagnosis of HCL to the skeletal symptoms was 20 months (range, 0 to 93), although some patients have developed skeletal symptoms in complete hematological remission, and skeletal involvement has been found to develop 22 years after HCL diagnosis [46]. Some HCL patients with lytic bony lesions did not demonstrate splenomegaly [58,59]. In HCL patients with localized pain, skeletal roentgenograms can be normal or non-specific [50,55].
Diagnosis and treatment evaluation of bone lesions is based on computed tomography (CT) and positron emission tomography (PET) (Figure 2.) [53]. Before the age of 18F-FDG PET/CT imaging, skeletal lesions were most commonly diagnosed by CT and magnetic resonance imaging (MRI), which were also used to evaluate the response to treatment. MRI is indicated in patients who have no roentgenographic or bone scan alterations, or they are non-specific [54]. [54,60]. More recently 18F-FDG PET/CT imaging is recommended for diagnosis, staging and treatment assessment (Figure 2.) [46,61]. PET is more specific and sensitive than other imaging methods, including CT and MRI, and is more useful in the differentiation of HCL lesions and malignant bone tumors.
3.3. Pulmonary Symptoms
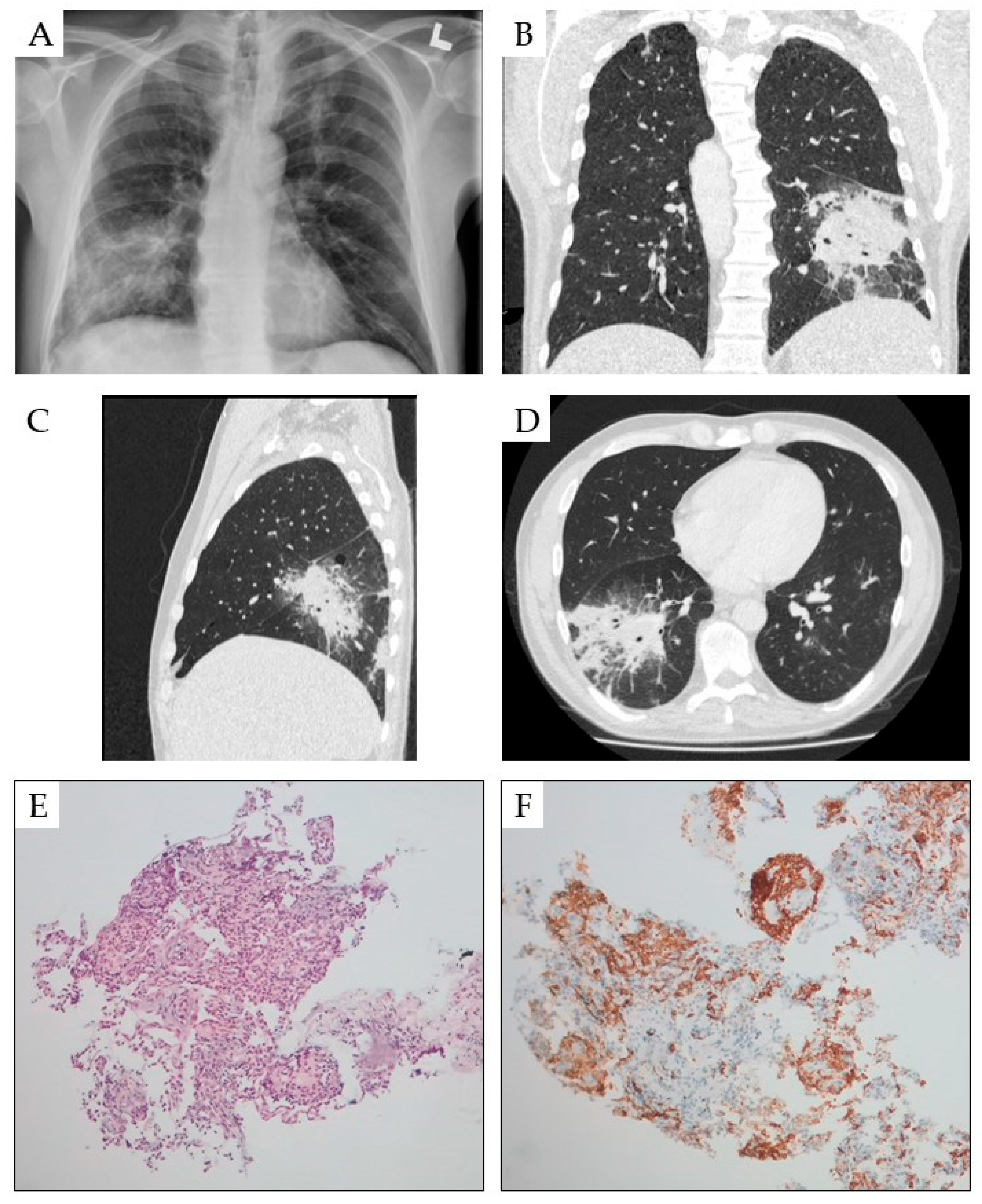
The most common cause of pulmonary symptoms in HCL are infections [62]. Disseminated atypical mycobacterial infections were reported in several patients with HCL [63,64,65,66,67]. Clinically, pulmonary infiltrations were usually observed on chest radiography in addition to fever and chills. Invasive diagnostic studies, including thoracotomy can be required for confirmation of the diagnosis of atypical mycobacteria infection infections with Mycobacterium kansasii, Mycobacterium avium-intracellulare, and Mycobacterium chelone. Mediastinal lymphadenopathy, and secondary pulmonary amyloidosis was also observed in some patients with HCL [10,68]. Pulmonary involvement by HCL cells is a very rare condition (Figure 3), with only few cases with leukemic lung infiltration being apparent in the literature [69,70,71,72,73]. A lung biopsy for histological examination is indicated in patients with pulmonary symptoms if antibiotics and antifungal treatment are not effective. However, a pulmonary biopsy is connected with a risk of bleeding, traumatic lung
3.4. Neurological Manifestations
Neurological complications were reported in approximately 5% of HCL patients [74], with the most common cause being infection. However, direct invasion of leukemic cells to the central nervous system (CNS) is rare in HCL [74,75,76,77,78,79,80,81,82,83,84,85]. In HCL patients, CNS involvement is typically indicated by confusion, aphasia, headache, meningeal syndrome, motor ataxia, dizziness, weakness, confusion, slurred speech, frequent falls, facial droop, fatigue, blurry vision and acute delusional symptoms [75,76,77,78,79,80,81,82,83,84]. Studies have also reported have also reported HCL localization in brain parenchyma and/or meninges [75,79,80,84,85,86,87,88,89,90]. In most HCL patients, CNS involvement is not related to large cell lymphoma disease transformation unlike CLL [81,85,86,87]. Systemic therapy with purine analogs and CD20 antibodies or, more recently with BRAF inhibitors are usually effective in controlling HCL demonstrating CNS involvement [75,82,85,88].
3.5. Ocular Symptoms
Ocular involvement of HCL is extremely rare and only few cases have been reported [91,92,93,94,95,96,97]. Of the nine reported cases, most involved the globe, with only two affecting the orbital mass [96,98]. In three-fourths of the patients, ocular or orbital manifestations were identified at the diagnosis of HCL. Therapy with cladribine induced an improvement of the ocular complications in most patients [93].
Panuveitis and retinal vasculitis coincident with HCL related to leukemic infiltration or bleeding have been noted in case reports [93,95,99], as was leukemic severe left-sided panuveitis with conjunctival and ciliary involvement in an HCL patient [99]. Local and systemic antibiotic therapy was ineffective, but rapid improvement was observed following treatment with cladribine.
Spontaneous subperiosteal orbital hematoma was also reported in an HCL patient with a history of orbital floor reconstruction due orbital fracture [100]. The patient received cladribine monotherapy. Four months later, the clinical symptoms (proptosis and diplopiahad) had resolved and near-complete resolution of the subperiosteal collection was seen in neuroimaging.
Retinopathy and visual disturbance due to intraretinal hemorrhage was reported as the initial symptom of HCL in a few patients [101,102]. In two cases, leukemic infiltration of the cornea was presented [103,104]. Also, orbital infections can develop, as HCL itself and antileukemic treatments are highly immunosuppressive.
3.6. Hearing Loss
Sudden hearing loss in patients with leukemia can be related to leukemic infiltration, hemorrhage and infection. El Enazi et al reported a patient with acute sensorineural hearing loss as an initial manifestation of HCL [105]. The morphology, immunohistochemistry and flow cytometry of the BM confirmed the diagnosis of HCL. This is the only case of sudden hearing loss in HCL noted to date, although a few cases with chronic myeloid leukemia and CLL have been reported [106,107,108,109,110]. Most of them had unilateral hearing loss, as in the HCL patient. Such sudden hearing loss in patients with leukemia can be attributed to leukemic infiltration, hemorrhage, blood hyperviscosity and infection.
3.7. Liver and Gastrointestinal Tract Symptoms
Hepatomegaly can be seen in up to 30% of HCL patients [7,111]. However, liver and gastrointestinal tract involvement has only been rarely reported in HCL patients. Dhanesar et al. describe a patient diagnosed with HCL involving the hepatic portal system during post splenectomy evaluation approximately four years after initial HCL ddiagnosis [112]. Computed tomography scan of the abdomen showed a tumor in the hepatic portal and peri-portal regions with bile duct obstruction. Following biopsy of the liver mass, a diagnosis of HCL was established [113,114].
Sen et al describe the first case report of an HCL patient manifesting clinically with duodenal involvement [115]. At HCL diagnosis, the patient had typical symptoms with pancytopenia and massive splenomegaly. A CT scan of the abdomen revealed thickening of the duodenum. Subsequent esophago-gastro-duodenoscopy (EGD) showed duodenal ulcerative inflammation. The duodenal biopsy demonstrated infiltration with HCL cells. The treatment with cladribine leaded to complete response including disappearance of duodenum involvement. In another report, Tariq et al present the case of a patient with gastric cancer developed during treatment of hairy cell leukemia with moxetumomab pasudotox [116]. In upper gastrointestinal endoscopy, a gastric mass with irregular margins was observed and histopathological evaluation showed well differentiated adenocarcinoma of the intestinal type.
3.8. Cardiac Manifestation
Progressive pericarditis and pleuritis in HCL patient at diagnosis was reported recently [117]. Symptoms completely resolved after treatment with purine analogs, with no recurrence observed during a five-year observation. In another report, Koczwara et al present the case of a 42-year-old HCL patient who developed transient cardiac failure following treatment with cladribine [118]. Cladribine interferes with the cardiac adenylate cyclase pathway and can induce cardiac dysfunction in some patients [119].
At diagnosis, hairy cell leukemia can ocassionally mimic infective endokarditis [120]. Ramasamy et al reported a case of HCL with fever of unknown origin, splinter haemorrhages with vasculitis and moderate splenomegaly splenomegaly and cytopenia at diagnosis, suggesting infective endocarditis; however, PB cultures and transthoracic echocardiogram were normal, and BM infiltration by CD19, CD25, CD11c, CD45 and CD103-positive lymphoid cells indicated a diagnosis of HCL [120]. Severe congestive heart failure was diagnosed in a patient with HCL treated with recombinant IFN-α2b [121]. Echocardiography showed severe global hypokinesis with second degree mitral and aortic valve insufficiency and reduced ejection fraction of 24%. The patient gradually improved after interferon was discontinued.
3.9. Rheumatological Manifestations
Rheumatological symptoms related either to the hematological malignancy or the immune system have been rarely reported in HCL patients [122,123,124]. The first patient with HCL and rheumatoid arthritis (RA) was reported in 1979 by Crofts et al; in this case, rheumatoid arthritis had developed two years before HCL diagnosis [125]. Westbrook and Golde analyzed 37 HCL patients and identified six patients with joint symptoms, usually associated with nodular skin lesions; all patients responded promptly to antileukemic therapy [126]. Facchini et al reported another patient who developed HCL eight years after RA diagnosis and suggested association between autoimmune disease and HCL [127]. In another patient, immune RA developed five years after a diagnosis of HCL [122]. More recently, Anil et al reported bilateral knee swelling, erythema, and tenderness, and mild bilateral pedal edema before HCL diagnosis; the author reported spontaneous resolution of the rheumatism symptoms before anti-leukemic treatment, which indicated that they were immune-mediated. [128]. In another case, a patient with HCL developed seropositive RA following treatment with IFN-α. In this case, the RA resolved over the next five months when interferon was administered for the HCL with no exacerbation of RA [129].
Zervas et al. presented a patient with HCL who developed seropositive RA [122]. In this patient, RA resolved when interferon-a treatment was implemented, suggesting that RA with an autoimmune mechanism was directly related to HCL; however, HCL-associated arthritis with a non-immune mechanism has been documented in several patients [123,124,129,130,131,132]. Sattar et al report the case of a patient with intermittent asymmetrical oligoarthritis, who subsequently developed HCL [123]. Importantly, HCL cells were also detected in the synovial fluid, suggesting an association between arthritis and HCL. Raimbourg at al observed another patient with osteoarticular symptoms among 27 patients with HCL [131]. This patient presented with polyarthritis involving the wrists, ankles, and knees, which responded to non-steroidal anti-inflammatory drugs. Hairy cells were identified in the joint fluid, thus establishing a diagnosis of HCL-related arthritis. The presented cases suggest that arthritis can have an immune basis in some patients, but not in others.
3.10. Soft Tissue Involvement
Pilichowska et al present the case of a patient with primary HCL of the breast, diagnosed incidentally during an elective reduction mammoplasty; the patient was asymptomatic without treatment one year following the HCL diagnosis [133]. In another patient, a pancreatic mass was observed under MRI nine years after HCL diagnosis and treatment with cladribine. An infiltrative lesion was reported along the pancreatic tail; it presented as a pancreatic mass partially encasing the pancreatic body, tail and splenic vessels, with an extension to the splenic hilum [134]. Fine-needle biopsy confirmed HCL infiltration.
4. Conclusions
In most patients, HCL is characterized by pancytopenia, splenomegaly, and bone marrow infiltration. However, several other unusual symptoms of HCL are reported in the literature. These include extramedullary and extra nodal manifestations of classic HCL in various organs including the skin, bones, central nervous system, gastrointestinal tract, heart, kidney, liver, lung and ocular symptoms.
Author Contributions
Conceptualization, T.R. and E.R.; writing—original draft preparation, T.R. and E.R..; writing—review and editing, T.R. E.R., M.B. A.J.;A.G. and E.R.; visualization, T.R., M.B. A.G. and E.R.; supervision, T.R.; funding acquisition, E.R. and T.R. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by grants from the Medical University of Lodz, Poland (No. 503/1-093-01/503-11-004 and 503/1093-1/503-11-003).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the Medical University of Lodz (No RNN/227/23/KE and No RNN/103/16/KE) for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study.
Data Availability Statement
The data presented in this study are available in this article.
Acknowledgments
We thank Edward Lowczowski from the Medical University of Lodz for editorial assistance and Aleksandra Samulska for technical assistance. We are grateful to the medical, nursing, and laboratory staff of the participating departments for their contributions to this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Grever, M.R.; Abdel-Wahab, O.; Andritsos, L.A.; Banerji, V.; Barrientos, J.; Blachly, J.S.; Call, T.G.; Catovsky, D.; Dearden, C.; Demeter, J.; et al. Consensus guidelines for the diagnosis and management of patients with classic hairy cell leukemia. Blood. 2017, 129, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Robak, T.; Matutes, E.; Catovsky, D.; Zinzani, P.L.; Buske, C. ESMO Guidelines Committee. Hairy cell leukaemia: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2015, 26, v100–v107. [Google Scholar] [CrossRef]
- Troussard, X.; Maitre, E. Untangling hairy cell leukaemia (HCL) variant and other HCL-like disorders: Diagnosis and treatment. J Cell Mol Med. 2024, 28, e18060. [Google Scholar] [CrossRef] [PubMed]
- Puła, A.; Robak, T. Hairy cell leukemia: a brief update on current knowledge and treatment prospects. Curr Opin Oncol. 2021, 33, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.; Yadav, S.; Mittal, N.; Rahman, K.; Sharma, A.; Gupta, A.; Nityan, S. Clinicopathological spectrum of hairy-cell leukemia: A single-center study with brief review of Indian literature. J Cancer Res Ther. 2020, 16, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Bosma, M.; Bartels, M. Hairy cell leukemia in a child? ! Blood. 2018, 132, 1216. [Google Scholar] [CrossRef] [PubMed]
- Polliack, A. Hairy cell leukemia: biology, clinical diagnosis, unusual manifestations and associated disorders. Rev Clin Exp Hematol. 2002, 6, 366–388 101046/j1468. [Google Scholar] [PubMed]
- Tadmor, T.; Polliack, A. Hairy cell leukemia: Uncommon clinical features, unusual sites of involvement and some rare associations. Best Pract Res Clin Haematol. 2015, 28, 193–9. [Google Scholar] [CrossRef] [PubMed]
- Troussard, X. Unusual clinical presentations of hairy cell leukemia. Acta Haematol. 2024, 147, 465–466. [Google Scholar] [CrossRef]
- Pattnaik, S.A.; Padhi, S.; Chhabra, G.; Panigrahi, M.K.; Das, P.K.; Bhola, R.K.; Mishra, S. Atypical presentation of hairy cell leukemia: a report and comprehensive review. Blood Res. 2020, 55, 123–127. [Google Scholar] [CrossRef]
- Robak, T. Hairy-cell leukemia variant: recent view on diagnosis, biology and treatment. Cancer Treat Rev. 2011, 37, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Alaggio, R.; Amador, C.; Anagnostopoulos, I.; Attygalle, A.D.; Araujo, I.B.O.; Berti, E.; Bhagat, G.; Borges, A.M.; Boyer, D.; Calaminici, M.; et al. The 5th edition of the World Health Organization classification of haematolymphoid tumours: lymphoid neoplasms. Leukemia. 2022, 36, 1720–1748. [Google Scholar] [CrossRef] [PubMed]
- Campo, E.; Jaffe, E.S.; Cook, J.R.; Leticia Quintanilla-Martinez, L.; Swerdlow, S.H.; Anderson, K.C.; Brousset, P.; Cerroni, L.; de Leval, L.; Dirnhofer, S.; et al. The International Consensus Classification of Mature Lymphoid Neoplasms: a report from the Clinical Advisory Committee. Blood. 2022, 140, 1229–1253. [Google Scholar] [CrossRef] [PubMed]
- Grever, M.; Andritsos, L.; Anghelina, M.; Arons, E.; Banerji, V.; Barrientos, J.; Bhat, S.A.; Blachly, J.; Broccoli, A.; Call, T.; et al. Hairy cell leukemia variant and WHO classification correspondence Re: 5th edition WHO classification haematolymphoid tumors: lymphoid neoplasms. Leukemia. 2024, 38, 1642–1644. [Google Scholar] [CrossRef] [PubMed]
- Robak, T.; Robak, P. Refractory and relapsed hairy-cell leukemia (HCL): casting light on promising experimental drugs in clinical trials. Expert Opin Investig Drugs. 2023, 32, 311–324. [Google Scholar] [CrossRef] [PubMed]
- Janus, A.; Robak, T. Hairy Cell Leukemia. In: Li W, editor. Leukemia [Internet]. Exon Publications, Brisbane, Australia; 2022 Oct 16. Chapter 3. pp. 33–52. PMID: 36395312. [CrossRef]
- Venkatesan, S.; Purohit, A.; Aggarwal, M.; Manivannan, P.; Tyagi, S.; Mahapatra, M.; Pati, H.P.; Saxena, R. Unusual presentation of hairy cell leukemia: a case series of four clinically unsuspected cases. Indian J Hematol Blood Transfus. 2014, 30, 413–417. [Google Scholar] [CrossRef]
- Zakarija, A.; Peterson, L.C.; Tallman, M.S. Hematology: Basic Principles and Practice. Philadelphia: Churchill Livingstone/Elsevier, 5th ed.; 2009. Chapter 84- Hairy cell leukaemia. In: Hoffman R, Benz EJ, Shatil SJ, Furie B, Silberstein LE, McGlave P, Heslop H (eds.) pp. 1349–1358. [Google Scholar]
- Rahman, K.; Kumari, S.; Singh, M.K.; Gupta, R.; Yadav, G.; Kumari, N.; Nityan, S. Atypical presentation of hairy cell leukemia: Significance of CD200 on flow cytometry. J Cancer Res Ther. 2018, 14, 1130–1134. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.; Yadav, S.; Mittal, N.; Rahman, K.; Sharma, A.; Gupta, A.; Nityan, S. Clinicopathological spectrum of hairy-cell leukemia: A single-center study with brief review of Indian literature. J Cancer Res Ther. 2020, 16, 120–126. [Google Scholar] [CrossRef]
- Galani, K.S.; Subramanian, P.G.; Gadage, V.S.; Rahman, K.; Ashok Kumar, M.S.; Shinde, S.; Mahadik, S.; Ansari, R.; Sengar, M.; Menon, H.; Nair, R.; Gujral, S. Clinico-pathological profile of Hairy cell leukemia: critical insights gained at a tertiary care cancer hospital. Indian J Pathol Microbiol. 2012, 55, 61–5. [Google Scholar] [CrossRef]
- Falini, B.; Tiacci, E.; Liso, A.; Basso, K.; Sabattini, E.; Pacini, R.; Foa, R.; Pulsoni, A.; Dalla Favera, R.; Pileri, S. Simple diagnostic assay for hairy cell leukaemia by immunocytochemical detection of annexin A1 (ANXA1). Lancet. 2004, 363, 1869–70. [Google Scholar] [CrossRef]
- Tiacci, E.; Trifonov, V.; Schiavoni, G.; Holmes, A.; Kern, W.; Martelli, M.P.; Pucciarini, A.; Bigerna, B.; Pacini, R.; Wells, V.A.; et al. BRAF mutations in hairy-cell leukemia. N Engl J Med. 2011, 364, 2305–2315. [Google Scholar] [CrossRef] [PubMed]
- Robak, E.; Jesionek-Kupnicka, D.; Robak, T. Skin changes in hairy cell leukemia. Ann Hematol. 2021, 100, 615–625. [Google Scholar] [CrossRef] [PubMed]
- Finan, M.C.; Su, W.P.; Li, C.Y. Cutaneous findings in hairy cell leukemia. J Am Acad Dermatol. 1984, 11, 788–97. [Google Scholar] [CrossRef] [PubMed]
- Robak, E.; Jesionek-Kupnicka, D.; Iskierka-Jazdzewska, E.; Janus, A.; Robak, T. Cutaneous leukocytoclastic vasculitis at diagnosis of hairy cell leukemia successfully treated with vemurafenib and rituximab. Leuk Res. 2021, 104, 106571. [Google Scholar] [CrossRef] [PubMed]
- Robak, E.; Braun, M.; Robak, T. Leukemia cutis-The current view on pathogenesis, diagnosis, and treatment. Cancers (Basel). 2023, 15, 5393. [Google Scholar] [CrossRef] [PubMed]
- Cho-Vega, J.H.; Medeiros, L.J.; Prieto, V.G.; Vega, F. Leukemia cutis. Am J Clin Pathol. 2008, 129, 130–142. [Google Scholar] [CrossRef] [PubMed]
- Parsi, M.; Go, M.S.; Ahmed, A. Leukemia Cutis. [Updated 2023 Jul 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK541136/[M1].
- Lawrence, D.M.; Sun, N.C.; Mena, R.; Moss, R. Cutaneous lesions in hairy-cell leukemia. Case report and review of the literature. Arch Dermatol. 1983, 119, 322–325 PMID: 6838238. [Google Scholar] [CrossRef] [PubMed]
- Grey, M.R.; Flanagan, N.G.; Kelsey, P.R. Severe skin rash in two consecutive patients treated with 2-chlorodeoxyadenosine for hairy cell leukaemia at a single institution. Clin Lab Haematol. 2000, 22, 111–113. [Google Scholar] [CrossRef]
- Broccoli, A.; Gandolfi, L.; Pellegrini, C.; Agostinelli, C.; Argnani, L.; Zinzani, P.L. Leukocytoclastic vasculitis associated with hairy cell leukemia at diagnosis: a case report and review of the literature. Tumori 2016, 102, S124–S127. [Google Scholar] [CrossRef]
- Gabriel, S.E.; Conn, D.L.; Phyliky, R.L.; Scott, R.E. Vasculitis in hairy cell leukaemia: review of literature and consideration of possible pathogenic mechanisms. J Rheumatol. 2016, 1986, 1167–1172 PMID: 3560105. [Google Scholar] [PubMed]
- Fain, O.; Hamidou, M.; Cacoub, P.; Godeau, B.; Wechsler, B.; Pariès, J.; Stirnemann, J.; Morin, A.S.; Gatfosse, M.; Hanslik, T.; et al. Vasculitides associated with malignancies: analysis of sixty patients. Arthritis Rheum 2007, 57, 1473–1480. [Google Scholar] [CrossRef] [PubMed]
- Moyers, J.T.; Liu, L.W.; Ossowski, S.; Goddard, L.; Kamal, M.O.; Cao, H. A rash in a hairy situation: Leukocytoclastic vasculitis at presentation of hairy cell Leukemia. Am J Hematol. 2019, 94, 1433–1434. [Google Scholar] [CrossRef] [PubMed]
- Hasler, P.; Kistler, H.; Gerber, H. Vasculitides in hairy cell leukemia. Semin Arthritis Rheum. 1995, 25, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Ventura, F.; Rocha, J.; Pereira, T.; Marques, H.; Pardal, F.; Brito, C. Sweet syndrome as the presenting symptom of hairy cell leukemia. Dermatol Online J. 2009, 15, 12 PMID: 19336029. [Google Scholar] [CrossRef] [PubMed]
- Levy, R.M.; Junkins-Hopkins, J.M.; Turchi, J.J.; James, W.D. Sweet syndrome as the presenting symptom of relapsed hairy cell leukemia. Arch Dermatol. 2002, 138, 1551–1554. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, R.P.; Newman, G.; Saperia, D. Pyoderma gangrenosum and hairy cell leukemia. J Dermatol Surg Oncol. 1987, 1, 1029–1031. [Google Scholar] [CrossRef]
- Jain, A.; Lad, D.; Prakash, G.; Khadwal, A.; Malhotra, P.; Bal, A.; Mallik, N.; Kumar, N.; Varma, S. Bullous pyoderma gangrenosum associated with hairy cell leukemia and its complete response to cladribine therapy. Indian J Hematol Blood Transfus. 2017, 33, 273–275. [Google Scholar] [CrossRef] [PubMed]
- Tombak, A.; Aygun, S.; Serinsoz, E.; Tiftik, E.N. Complete recovery of pyoderma gangrenosum after successful treatment of underlying hairy cell leukemia with cladribine. Korean J Intern Med. 2015, 30, 739–741. [Google Scholar] [CrossRef] [PubMed]
- Elkon, K.B.; Hughes, G.R.; Catovsky, D.; Clauvel, J.P.; Dumont, J.; Seligmann, M.; Tannenbaum, H.; Esdaile, J. Hairy-cell leukaemia with polyarteritis nodosa. Lancet. 1979, 2, 280–282. [Google Scholar] [CrossRef]
- Zervas, J.; Vayopoulos, G.; Kaklamanis, P.H.; Zerva, C.H.; Pfessas, P.H. Hairy-cell Leukaemia-associated polyarthritis: a report of two cases. Br J Rheumatol. 1991, 30, 157–158. [Google Scholar] [CrossRef]
- Cailly, L.; Gruchet, C.; Maitre, E.; Guidez, S.; Delwail, V.; Systchenko, T.; Moya, N.; Sabirou, F.; Levy, A.; Bobin, A.; et al. Hairy cell leukemia with isolated bone lesions. Clin Case Rep. 2023, 11, e7343. [Google Scholar] [CrossRef] [PubMed]
- Quesada, J.R.; Keating, M.J.; Libshitz, H.I.; Llamas, L. Bone involvement in hairy cell leukemia. Am J Med. 1983, 74, 228–231. [Google Scholar] [CrossRef]
- Robak, P.; Jesionek-Kupnicka, D.; Kupnicki, P.; Polliack, A.; Robak, T. Bone lesions in hairy cell leukemia: Diagnosis and treatment. Eur J Haematol. 2020, 105, 682–691. [Google Scholar] [CrossRef] [PubMed]
- Yonal-Hindilerden, I.; Hindilerden, F.; Bulut-Dereli, S.; Yıldız, E.; Dogan, I.O.; Nalcaci, M. Hairy cell leukemia presenting with isolated skeletal involvement successfully treated by radiation therapy and cladribine: a case report and review of the literature. Case Rep Hematol. 2015, 803921. [Google Scholar] [CrossRef]
- Fasulo, S.M.; Narvaneni, S.; Kumar, V.; Manje Gowda, A.; Sultana, Y. Lytic Bone Lesion: An Unusual presentation of hairy cell leukemia. Cureus. 2021, 13, e12959. [Google Scholar] [CrossRef] [PubMed]
- Notarfranchi, L.; Russo, F.; Re, F.; Mancini, C.; Martella, E.; Falini, B.; Aversa, F.; Tiacci, E. Hairy cell leukaemia mimicking multiple myeloma. Lancet Oncol. 2019, 20, e187. [Google Scholar] [CrossRef] [PubMed]
- VanderMolen, L.A.; Urba, W.J.; Longo, D.L.; Lawrence, J.; Gralnick, H.; Steis, R.G. Diffuse osteosclerosis in hairy cell leukemia. Blood. 1989, 74, 2066–9 PMID: 2804348. [Google Scholar] [CrossRef] [PubMed]
- Snell, K.S.; O'Brien, M.M.; Sendelbach, K.; Martino, R. Pathologic fracture occurring 22 years after diagnosis of hairy cell leukemia: case report and literature review. West J Med. 1999, 170, 172–174. [Google Scholar] [PubMed]
- Hudson, J.; Cobby, M.; Yates, P.; Watt, I. Extensive infiltration of bone with marrow necrosis in a case of hairy cell leukaemia. Skeletal Radiol. 1995, 24, 228–231. [Google Scholar] [CrossRef]
- Lembersky, B.C.; Ratain, M.J.; Golomb, H.M. Skeletal complications in hairy cell leukaemia: diagnosis and therapy. J Clin Oncol 1988, 6, 1280–1284 1284. [Google Scholar] [CrossRef]
- Filippi, A.R.; Franco, P.; Marinone, C.; Tarella, C.; Ricardi, U. Treatment options in skeletal localizations of hairy cell leukemia: a systematic review on the role of radiation therapy. Am J Hematol 2007, 82, 1017–1021. [Google Scholar] [CrossRef] [PubMed]
- Lal, A.; Tallman, M.S.; Soble, M.B.; Golubovich, I.; Peterson, L. Hairy cell leukemia presenting as localized skeletal involvement. Leuk Lymphoma 2002, 43, 2207–2211. [Google Scholar] [CrossRef] [PubMed]
- Karmali, R.; Farhat, M.; Leslie, W.; McIntire, M.G.; Gregory, S. Localized bone disease as a presentation of hairy cell leukemia. Clin Adv Hematol Oncol 2008, 6, 290–294 PMID: 18496495. [Google Scholar] [PubMed]
- Robak, P.; Jesionek-Kupnicka, D.; Kupnicki, P.; Polliack, A.; Robak, T. Multifocal osteolytic lesions in hairy cell leukemia-the importance of PET/CT in diagnosis and assessment. Ann Hematol. 2021, 100, 1641–1645. [Google Scholar] [CrossRef] [PubMed]
- Gray, M.T.; Rutherford, M.N.; Bonin, D.M.; Patterson, B.; Lopez, P.G. Hairy-cell leukemia presenting as lytic bone lesions. J Clin Oncol. 2013, 31, e410–e412. [Google Scholar] [CrossRef] [PubMed]
- Spedini, P.; Tajana, M.; Bergonzi, C. Unusual presentation of hairy cell leukemia. Haematologica. 2000, 85, 548 PMID: 10800175. [Google Scholar] [PubMed]
- Herold, C.J.; Wittich, G.R.; Schwarzinger, I.; Haller, J.; Chott, A.; Mostbeck, G.; Hajek, P.C. Skeletal involvement in hairy cell leukemia. Skeletal Radiol. 1988, 17, 171–5. [Google Scholar] [CrossRef] [PubMed]
- Doma, A.; Škerget, M.; Žagar, I. 18F-FDG PET/CT for staging and evaluation of therapy in a patient with unusual hairy cell leukemia presentation. Clin Nucl Med 2019, 44, e458–e460. [Google Scholar] [CrossRef] [PubMed]
- Vardiman, J.W.; Golomb, H.M. Autopsy findings in hairy cell leukemia. Semin Oncol 1984, 11, 370–380 PMID: 6505704. [Google Scholar] [PubMed]
- Bennett, C.; Vardiman, J.; Golomb, H. Disseminated atypical mycobacterial infection in patients with hairy cell leukemia. Am J Med. 1986, 80, 891–896. [Google Scholar] [CrossRef]
- Weinstein, R.A.; Golomb, H.M.; Grumet, G.; Gelmann, E.; Schechter, G.P. Hairy cell leukemia: association with disseminated atypical mycobacterial infection. Cancer. 1981, 48, 380–383. [Google Scholar] [CrossRef] [PubMed]
- Stanton, D.J.; Quadri, N.Z.; Tanabe, M.B. Concomitantly Diagnosed Disseminated M kansasii infection and hairy cell leukemia with review of pathophysiology. J Investig Med High Impact Case Rep. 2024, 12, 23247096241253343. [Google Scholar] [CrossRef] [PubMed]
- A0A0A0.
- Winter, S.M.; Bernard, E.M.; Gold, J.W.; Armstrong, D. Humoral response to disseminated infection by Mycobacterium avium-Mycobacterium intracellulare in acquired immunodeficiency syndrome and hairy cell leukemia. J Infect Dis. 1985, 151, 523–527. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.P., 3rd; Arcement, C.M.; Wong, R.; Robinson, A.E. Diffuse pulmonary disease associated with hairy cell leukemia. Acad Radiol. 1995, 2, 179–181. [Google Scholar] [CrossRef] [PubMed]
- Case 52-1982. A 50-year-old man with hairy cell leukemia, recurrent fever, and variable pulmonary infiltrates. N Engl J Med 1982, 307, 1693–700. [CrossRef]
- Hansen, T.; Constantin, C.; Weber, M.; Titze, U.; Hartmann, F. Bronchoalveolar lavage in hairy cell leukemia with pulmonary infiltration. Pathologe 2019, 40, 529–533. [Google Scholar] [CrossRef] [PubMed]
- Uzunhan, Y.; Cadranel, J.; Boissel, N.; Gardin, C.; Arnulf, B.; Bergeron, A. Lung involvement in lymphoid and lympho-plasmocytic proliferations (except lymphomas). Rev Mal Respir 2010, 27, 599–610. [Google Scholar] [CrossRef] [PubMed]
- Ecsiova, D.; Kamaradova, K.; Nova, M.; Hoffmann, P.; Rozsivalova, P.; Simkovic, M.; Zak, P. Pulmonary damage in a patient with hairy cell leukemia - infectious involvement or hematological disease activity? Case report. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2023, 167, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Lemiale, V.; Meignin, V.; Azoulay, É. (2011). Hairy cell leukemia with pulmonary infiltrates. In: Azoulay, E. (eds) Pulmonary Involvement in Patients with Hematological Malignancies. Springer, Berlin, Heidelberg. [CrossRef]
- Kimmel, D.W.; Hermann Jr, R.C.; O'Neill, B.P. Neurologic complications of hairy cell 176 leukemia. Arch Neurol. 1984, 41, 202–203. [Google Scholar] [CrossRef]
- Plenderleith, I.H. Hairy cell leukemia. Can Med Assoc J. 1970, 102, 1056–1060. [Google Scholar] [PubMed]
- Wolfe, D.W.; Scopelliti, J.A.; Boselli, B.D. Leukemic meningitis in a patient with hairy 180 cell leukemia. A case report. Cancer. 1984, 54, 1085–1087. [Google Scholar] [CrossRef] [PubMed]
- Knecht, H.; Budmiger, H.; Groscurth, P.; Streuli, R.A. Central nervous system involvement 182 in hairy cell leukemia. Klin Wochenschr. 1985, 63, 423–427. [Google Scholar] [CrossRef] [PubMed]
- Le Bezu, M.; Pinaudeau, Y.; Poirier, J.; Dreyfus, B. Involvement of the nervous system in 184 hairy cell leukemia. Arch Neurol. 1985, 42, 839. [Google Scholar] [CrossRef] [PubMed]
- Navarrete, D.; Bodega, E. Leukemic meningitis in a patient with hairy cell leukemia. A 186 case report. Nouv Rev Fr Hematol. 1987, 29, 247–9 PMID: 3697064. [Google Scholar] [PubMed]
- Chandana, S.R.; Kotecha, R.; Al-Janadi, A.; Chang, H.T.; Conley, B.A. Rare case of hairy cell leukemia with brain parenchymal involvement: a diagnostic dilemma. J Clin Oncol. 2013, 31, e186–e188. [Google Scholar] [CrossRef] [PubMed]
- McDowell, M.M.; Zhu, X.; Agarwal, N.; Nikiforova, M.N.; Lieberman, F.S.; Drappatz, J. Response of relapsed central nervous system hairy cell leukemia to vemurafenib. Leuk Lymphoma. 2016, 57, 2952–2954. [Google Scholar] [CrossRef]
- Perry, A.M.; Matsuda, K.; Wadhwa, V.; Hewitt, D.; Almiski, M.; Johnston, J.B.; Banerji, V. Multifocal brain involvement in a patient with hairy cell leukemia successfully treated with rituximab and cladribine. Blood Adv. 2017, 1, 899–902. [Google Scholar] [CrossRef] [PubMed]
- Rosen, D.S.; Smith, S.; Gurbuxani, S.; Yamini, B. Extranodal hairy cell leukemia presenting in the lumbar spine. J Neurosurg Spine 2008, 9, 374–376. [Google Scholar] [CrossRef] [PubMed]
- Claves, F.; Carras, S.; Burroni, B.; Maitre, E.; Boutonnat, J.; Troussard, X.; Molina, L. Atypical meningeal localization of classical hairy cell leukemia with an impressive response to rituximab and cladribine association. A case report and literature review. EJHaem. 2024, 5, 242–246. [Google Scholar] [CrossRef]
- Johnson, A.E.; Raju, A.R.; Jacob, A.; Hildebrandt, G.C. Case report: A case of classic hairy cell leukemia with CNS involvement treated with vemurafenib. Front Oncol. 2023, 12, 1100577. [Google Scholar] [CrossRef]
- Navarrete, D.; Bodega, E. Leukemic meningitis in a patient with hairy cell leukemia. A case report. Nouv Rev Fr Hematol. 1987, 29, 247–249 PMID: 3697064. [Google Scholar] [PubMed]
- Ito, K.; Harada, K.; Uchino, Y.; Hirano, K.; Sekiguchi, N. A rare clinical case of secondary central nervous system involvement without transformation in hairy cell leukemia: a case report and literature review. Acta Haematol. 2024, 147, 482–488. [Google Scholar] [CrossRef] [PubMed]
- Robak, T.; Dietrich, S. (2021). Hairy Cell Leukemia. In: Dreyling, M., Ladetto, M. (eds) Indolent Lymphomas. Hematologic Malignancies. Springer, Cham. [CrossRef]
- Ng, M.H.; Tsang, S.S.; Ng, H.K.; Sriskandavarman, V.; Feng, C.S. An unusual case of hairy cell leukemia: death due to leukostasis and intracerebral hemorrhage. Hum Pathol. 1991, 22, 1298–1302. [Google Scholar] [CrossRef]
- Dinçol, G.; Kahraman, R. Cryptococcus neoformans meningitis in a patient with hairy cell leukemia. Am J Hematol. 2006, 81, 387. [Google Scholar] [CrossRef] [PubMed]
- Jiang, K.; Punja, K.G.; Hyrcza, M.D.; Simpson, S.M. Beyond the norm: unusual orbital manifestation of hairy cell leukemia. Can J Ophthalmol. 2024, 59, e285–e287. [Google Scholar] [CrossRef] [PubMed]
- Deitch, R.D.; Wilson, F.M. Leukemic reticuloendotheliosis with presenting ocular complaints: report of acase. Arch Ophthalmol 1963, 69, 560–563. [Google Scholar] [CrossRef] [PubMed]
- Robinson, A.; Eting, E.; Zeidman, A.; Djaldetti, M.; Mittelman, M.; Savir, H. Ocular manifestation of hairy cell leukemia with dramatic response to 2-chlorodeoxyadenosine. Am J Ophthalmol 1996, 121, 97–99. [Google Scholar] [CrossRef]
- Charalel, R.; Jain, A.; Rachakonda, L.; Gaynon, M. Visualdis-turbance as initial presentation of hairy cell leukemia. Eur J Ophthalmol 2009, 19, 318–320. [Google Scholar] [CrossRef]
- Di Maria, A.; Redaelli, C.; Canevari, A.; Pagnucco, G.; Martinetti, M.; Bianchi, P.E. Unilateral retinal vasculitis associated with hairy cell leukaemia: immunogenetic study. Ophthalmologica. 1998, 212, 355–357. [Google Scholar] [CrossRef]
- Jiang, K.; Punja, K.G.; Hyrcza, M.D.; Simpson, S.M. Beyond the norm: unusual orbital manifestation of hairy cell leukemia. Can J Ophthalmol. 2024, 59, e285–e287. [Google Scholar] [CrossRef]
- Charalel, R.; Jain, A.; Rachakonda, L.; Gaynon, M. Visualdis-turbance as initial presentation of hairy cell leukemia. Eur J Ophthalmol 2009, 19, 318–320. [Google Scholar] [CrossRef] [PubMed]
- Coupland, S.E.; Krause, L.; Delecluse, H.J.; Anagnostopoulos, I.; Foss, H.D.; Hummel, M.; Bornfeld, N. ’ Lee, W. R.; Stein, H. Lymphoproliferative lesions of the ocular adnexa: analysis of 112 cases. Ophthalmology. 1998, 105, 1430–1441. [Google Scholar] [CrossRef]
- Zeidman, A.; Floru, S.; Robinson, A.; Polliack, A.; Djaldeti, M.; Savir, H.; Mittelman, M. Panuveitis responsive to 2-CdA: an unusual ocular presentation of hairy cell leukemia. Leuk Lymphoma. 1996, 20, 501–503. [Google Scholar] [CrossRef] [PubMed]
- North, V.S.; Jamerson, E.C.; Plum, W.; Tran, A.Q.; Kazim, M. Spontaneous subperiosteal orbital hematoma as a presenting sign of hairy cell leukemia in a patient with a long-standing orbital implant. Can J Ophthalmol. 2023, 58, e189–e191. [Google Scholar] [CrossRef] [PubMed]
- Bertram, B.; Schulte, K.; Wolf, S.; Glöckner, W.M.; Reim, M. Retinopathy as the first symptom of hairy cell leukemia. Klin Monatsbl Augenheilkd 1991, 199, 295–297 German PMID: 1762358. [Google Scholar] [CrossRef] [PubMed]
- Bertram, B.; Schulte, K.; Wolf, S.; Glöckner, W.M. A visual disorder as the initial symptom of hairy cell leukemia. Dtsch Med Wochenschr. 1991, 116, 157 German PMID: 1988279. [Google Scholar] [PubMed]
- Zák, P.; Chrobák, L.; Podzimek, K.; Hejcmanová, D.; Voglová, J.; Dulícek, P.; Mirová, S. An unusual course in hairy-cell leukemia with marked abdominal lymphadenopathy, leukemic infiltration of the cornea and skin changes. Vnitr Lek. 1996, 42, 463–6 Czech PMID: 8928422. [Google Scholar] [PubMed]
- Hejcmanová, D.; Abulgasim, H.A.; Jebavá, R.; Chrobák, L.; Podzimek, K.; Zák, P. Leukemické infiltráty rohovky u nemocné leukémiís "vlasatými bunkami" [Leukemic infiltration of the cornea in a patient with hairy-cell leukemia]. Cesk Slov Oftalmol. 1995, 51, 152–155 Czech PMID: 7656350. [Google Scholar] [PubMed]
- AlEnazi, A.; Alhedaithy, R.; Alfayez, A.; Alghonaim, Y. Acute profound sensorineural hearing loss as the initial manifestation of hairy cell leukemia, case report and literature review. Int J Surg Case Rep. 2019, 60, 200–203. [Google Scholar] [CrossRef]
- Nageris, B.; Or, R.; Hardan, I.; Polliack, A. Sudden onset deafness as a presenting manifestation of chronic lymphocytic leukemia. Leuk Lymphoma. 1993, 9, 269–271. [Google Scholar] [CrossRef]
- Genden, E.M.; Bahadori, R.S. Bilateral sensorineural hearing loss as a first symptom of chronic myelogenous leukemia. Otolaryngol Head Neck Surg. 1995, 113, 499–501. [Google Scholar] [CrossRef]
- Acar, G.O.; Acioğlu, E.; Enver, O.; Ar, C.; Sahin, S. Unilateral sudden hearing loss as the first sign of chronic myeloid leukemia. Eur Arch Otorhinolaryngol. 2007, 264, 1513–2516. [Google Scholar] [CrossRef] [PubMed]
- Nageris, B.; Or, R.; Hardan, I.; Polliack, A. Sudden onset deafness as a presenting manifestation of chronic lymphocytic leukemia. Leuk Lymphoma. 1993, 9, 269–271. [Google Scholar] [CrossRef] [PubMed]
- Naraev, B.G.; Linthicum, F.H., Jr. Rapid hearing loss in chronic lymphocytic leukemia. Otol Neurotol 2006, 27, 445–446. [Google Scholar] [CrossRef] [PubMed]
- Yam, L.T.; Janckila, A.J.; Chan, C.H.; Li, C.Y. Hepatic involvement in hairy cell leukemia. Cancer. 1983, 51, 1497–1504. [Google Scholar] [CrossRef]
- Dhanesar, G.K.; Livingston, J.; Maroules, M.; Lee, S.H. Hairy cell leukemia: hepatic affinity status post splenectomy. Cureus. 2023, 15, e39830. [Google Scholar] [CrossRef]
- Sahar, N.; Schiby, G.; Davidson, T.; Kneller, A.; Apter, S.; Farfel, Z. Hairy cell leukemia presenting as multiple discrete hepatic lesions. World J Gastroenterol. 2009, 15, 4453–4456. [Google Scholar] [CrossRef]
- Al-Saheli, Z.I.; Bazzi, T.; Barthel, B. Oncological management dilemma: a rare presentation of hairy cell leukaemia with hepatic involvement presenting concomitantly with pancreatic adenocarcinoma. BMJ Case Rep. 2022, 15, e252423. doi.org/ 10.1136/bcr–2022. [Google Scholar] [CrossRef]
- Sen, P.; Shaaban, H.; Modi, T.; Kumar, A.; Guron, G. Hairy cell leukemia presenting with duodenal involvement duodenum: a case report. N Am J Med Sci. 2015, 7, 288–290. [Google Scholar] [CrossRef]
- Tariq, S.; Bin Hamid, M.A.; Rahman, N.; Oleary, L.; Wong, K.; Sehbai, A. Unusual presentation of gastric cancer during treatment of hairy cell leukemia: Exploring the etiological basis of this rare phenomenon. Cancer Pathog Ther. 2023, 1, 146–148. [Google Scholar] [CrossRef]
- Iwashige, A.; Hirosawa, M.; Tsukada, J. Hairy cell leukemia presenting with progressive pericarditis and pleuritis. Ann Hematol. 2018, 97, 2527–2528. [Google Scholar] [CrossRef]
- Koczwara, B.; Spangenthal, E.; Bernstein, S.H. The development of congestive cardiac failure in a patient with hairy cell leukemia treated with 2-chlorodeoxyadenosine. Leuk Lymphoma. 1997, 26, 413–415. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, R.A.; Lowenstein, J.M. Inhibition of phosphorylation of troponin in rat heart by adenosine and 5-chloro-5-deoxyadenosine. Biochem Pharmacol 1991, 42, 685–692. [Google Scholar] [CrossRef]
- Ramasamy, C.; Dubashi, B.; Rekha, J.S.; Basu, D.; Jain, A.; Dutta, T.K. Hairy cell leukemia masquerading as infective endocarditis. Indian J Hematol Blood Transfus. 2013, 29, 84–86. [Google Scholar] [CrossRef] [PubMed]
- Sucak, G.T.; Haznedar, R.; Yalçin, R. Reversible cardiomyopathy in a patient with hairy cell leukaemia. Postgrad Med J. 1998, 74, 313–314. [Google Scholar] [CrossRef] [PubMed]
- Zervas, J.; Vayopoulos, G.; Kaklamanis, P.H.; Zerva, C.H.; Pfessas, P.H. Hairy-cell leukaemia-associated polyarthritis: a report of two cases. Br J Rheumatol. 1991, 30, 157–158. [Google Scholar] [CrossRef] [PubMed]
- Sattar, M.A.; Cawley, M.I.D. Arthritis associated with hairy cell leukaemia. Ann Rheum Dis 1982, 41, 289–391. [Google Scholar] [CrossRef] [PubMed]
- Harden, E.A.; Moore, J.O.; Haynes, R.F. Leukaemia associated arthritis: indentification of leukaemic cells in synovial fluid using monoclonal and polyclonal antibodies. Arthritis Rheum 1984, 27, 1306–1308. [Google Scholar] [CrossRef] [PubMed]
- Crofts, M.A.; Sharp, J.C.; Joyner, M.Y. Rheumatoid arthritis and hairy-cell leukaemia. Lancet. 1979, 314, 203–204. [Google Scholar] [CrossRef]
- Westbrook, C.A.; Golde, D.W. Autoimmune disease in hairy-cell leukaemia: clinical syndromes and treatment. Br J Haematol. 1985, 61, 349–356. [Google Scholar] [CrossRef]
- Anil, V.; Ganipisetti, V.; Harisinghani, K.; Kanugula, A.K. Hairy cell leukemia (HCL) presenting with joint swelling: case report and literature review of a rare rheumatological manifestation of a hematological disease. Cureus. 2023, 15, e35912. [Google Scholar] [CrossRef] [PubMed]
- Anil, V.; Ganipisetti, V.; Harisinghani, K.; Kanugula, A.K. Hairy cell leukemia (HCL) presenting with joint swelling: case report and literature review of a rare rheumatological manifestation of a hematological disease. Cureus. 2023, 15, e35912. [Google Scholar] [CrossRef] [PubMed]
- Taylor, H.G.; Davis, M.J.; Hothersall, T.E. Hairy cell leukaemia and rheumatoid arthritis. Br J Rheumatol. 1991, 30, 391–392. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Cathey, M.A. ; HawleyDJ Recombinant gamma interferon in rheumatoid arthritis. Arthritis Rheum 1986, 30, S18. [Google Scholar]
- Raimbourg, J.; Cormier, G.; Stéphane Varin Tanguy, G.; Bleher, Y.; Maisonneuve, H. Hairy-cell leukemia with inaugural joint manifestations. Joint Bone Spine. 2009, 76, 416–420. [Google Scholar] [CrossRef] [PubMed]
- L'Hirondel, J.L.; Troussard, X.; Macro, M.; Courtheoux, F.; Guaydier-Souquières, G.; Mandard, J.C.; Loyau, G. Polyarthrite révélatrice d'une leucémie à tricholeucocytes [Polyarthritis revealing hairy cell leukemia]. Rev Rhum Mal Osteoartic. 1992, 59, 749–753 PMID: 130659. [Google Scholar] [PubMed]
- Pilichowska, M.; Shariftabrizi, A.; Mukand-Cerro, I.; Miller, K. Primary hairy cell leukemia/lymphoma of the breast: a case report and review of the literature. Case Rep Pathol. 2014, 2014, 497027. [Google Scholar] [CrossRef]
- Aggarwal, N.; Neupane, R.; Thorburn, C.; Chisti, M.; Jamil, L.H. Hairy cell leukemia: a rare differential for a pancreatic mass. Am J Gastroenterology 2023, 118, 1562–1563. [Google Scholar] [CrossRef]
Figure 1.
Skin lesions in HCL. Direct infiltration of the skin by leukemic cells. Multiple scattered reddish-colored nodules and tumors with a smooth surface and high cohesion, without tendency to disintegrate and without accompanying symptoms (A). Maculopapular skin rash due to paraneoplastic dermatitis with cutaneous leukocytoclastic vasculitis. On the skin of the lower limbs, maculopapular eruptions with a hemorrhagic component and hemorrhagic vesicles and blisters with a tendency to form necrotic crusts in the center are visible, with the greatest intensity on separate parts of the limbs. Symptoms include moderate itching and pain (B). Pyoderma gangrenosum on the skin in a patient with HCL at diagnosis. The skin of the lower leg shows circumferentially spreading ulcers with sterile secretion, fibrin, a granular bottom and a carved, active edge. Pimples are also visible, spreading peripherally and merging to form painful ulcers. The symptoms disappeared after after treatment with cladribine (C). Zoster in a patient with HCL after treatment with cladribine. On the skin of the upper left part of the chest, left shoulder and arm there is an extensive erythematous focus with herpetic-like grouped vesicles partially filled with bloody secretion, formation of necrotic crusts and great pain (D).
Figure 1.
Skin lesions in HCL. Direct infiltration of the skin by leukemic cells. Multiple scattered reddish-colored nodules and tumors with a smooth surface and high cohesion, without tendency to disintegrate and without accompanying symptoms (A). Maculopapular skin rash due to paraneoplastic dermatitis with cutaneous leukocytoclastic vasculitis. On the skin of the lower limbs, maculopapular eruptions with a hemorrhagic component and hemorrhagic vesicles and blisters with a tendency to form necrotic crusts in the center are visible, with the greatest intensity on separate parts of the limbs. Symptoms include moderate itching and pain (B). Pyoderma gangrenosum on the skin in a patient with HCL at diagnosis. The skin of the lower leg shows circumferentially spreading ulcers with sterile secretion, fibrin, a granular bottom and a carved, active edge. Pimples are also visible, spreading peripherally and merging to form painful ulcers. The symptoms disappeared after after treatment with cladribine (C). Zoster in a patient with HCL after treatment with cladribine. On the skin of the upper left part of the chest, left shoulder and arm there is an extensive erythematous focus with herpetic-like grouped vesicles partially filled with bloody secretion, formation of necrotic crusts and great pain (D).
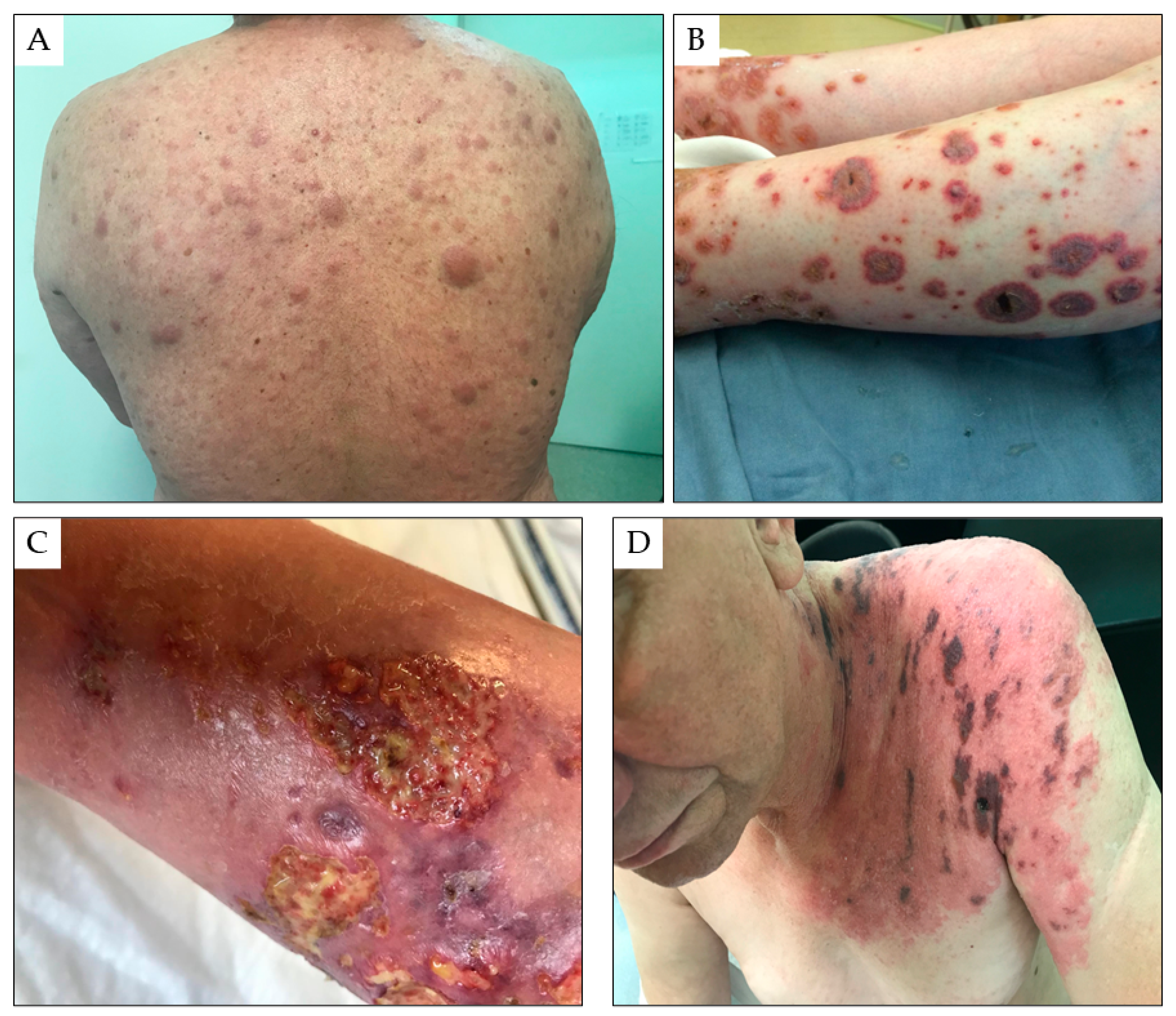
Figure 2.
Representative images of hairy cell leukemia bone lesions. Pathologic FDG uptake in the ribs, left humerus, vertebral body Th10, sacrum, right iliac, pubic bone, and ischium image in PET/CT imaging (A). Mixed osteolytic and osteoblastic lesions in the sacrum PET/CT imaging (B) and vertebrum PET/CT imaging (C). Bone marrow infiltrate of HCL in Haematoxyllin&Eosin staining, maginification of 100X (D) and in staining for CD20, magnification of 100X (E).
Figure 2.
Representative images of hairy cell leukemia bone lesions. Pathologic FDG uptake in the ribs, left humerus, vertebral body Th10, sacrum, right iliac, pubic bone, and ischium image in PET/CT imaging (A). Mixed osteolytic and osteoblastic lesions in the sacrum PET/CT imaging (B) and vertebrum PET/CT imaging (C). Bone marrow infiltrate of HCL in Haematoxyllin&Eosin staining, maginification of 100X (D) and in staining for CD20, magnification of 100X (E).
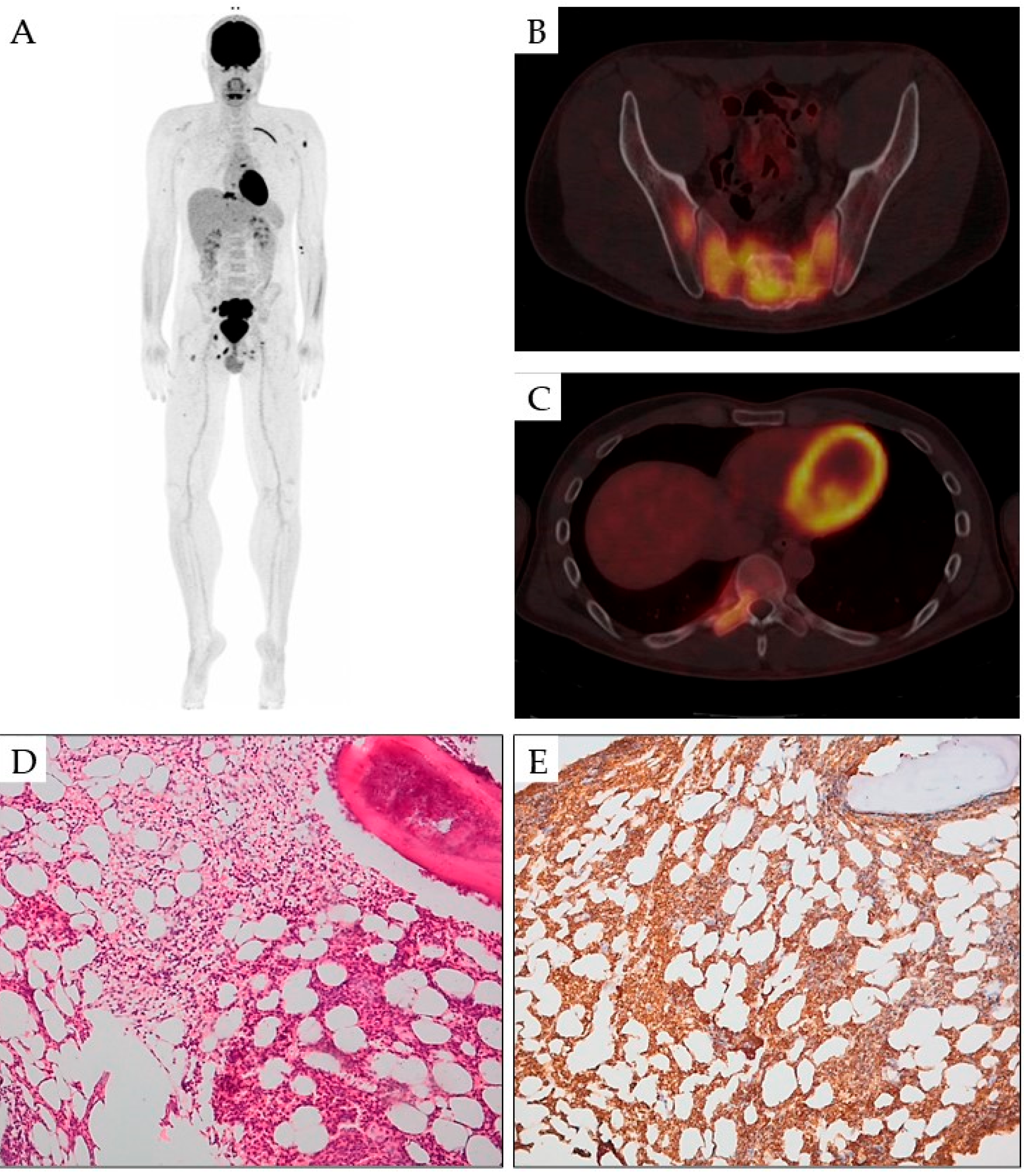
Figure 3.
Pulmonary involvement of HCL. X-ray chest PA view shows unilateral right diffuse pulmonary infiltrates (A). High-resolution computed tomography reveals septal thickening and multiple small and diffusely-merging focal consolidations with ground glass opacities in frontal (B), side (C) and transversal projection (D). Lung biopsy showing infiltrate of HCL in Haematoxyllin&Eosin staining, magnification of 100X (D) and in staining for CD20, magnification of 100X (F). damage or introduction of infection. Treatment with cladribine or rituximab induced regression of pulmonary involvement in most patients.
Figure 3.
Pulmonary involvement of HCL. X-ray chest PA view shows unilateral right diffuse pulmonary infiltrates (A). High-resolution computed tomography reveals septal thickening and multiple small and diffusely-merging focal consolidations with ground glass opacities in frontal (B), side (C) and transversal projection (D). Lung biopsy showing infiltrate of HCL in Haematoxyllin&Eosin staining, magnification of 100X (D) and in staining for CD20, magnification of 100X (F). damage or introduction of infection. Treatment with cladribine or rituximab induced regression of pulmonary involvement in most patients.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



