
Submitted:
12 August 2024
Posted:
14 August 2024
You are already at the latest version
Abstract
Background: Ovarian mesonephric-like adenocarcinoma (MLA) is a newly described histological type known for its aggressive behavior. This study aims to determine the frequency of ovarian MLA, review existing literature, and elucidate its clinicopathological characteristics, including potential therapeutic targets. Methods: We retrospectively reviewed the pathological diagnoses of 516 primary ovarian cancer surgical cases at our institution from 2010 to 2023. MLAs exhibiting typical morphological and immunohistochemical features were included. The frequency and clinicopathological characteristics of these cases were summarized. Additionally, we conducted a literature search using PubMed to collect and summarize previously reported cases of ovarian MLA. Results: Among the 516 primary ovarian cancer cases, we identified 3 cases (0.6%) of MLA. The patients were 52-76 years old, and the initial FIGO stages were IC1 (2 cases) and IIIB (1 case). All cases exhibited HRP, pMMR, PD-L1 negativity (CPS<1), and HER2-low expression. Two cases experienced metastatic recurrence. A literature review identified 97 cases of MLA. MLA frequently exhibited KRAS mutations (90%, 38/42), with a recurrence rate of 39% (26/67). Conclusion: MLA accounted for 0.6% of malignant ovarian tumors at our institution, all of which were advanced or recurrent cases. These cases showed HRP, pMMR, and PD-L1 negativity, indicating a lack of current therapeutic targets. Literature also reports a high incidence of advanced and recurrent cases, highlighting the need for accurate diagnosis and the development of new treatments. The frequent KRAS mutations suggest a potential therapeutic target for recurrent or metastatic MLA.
Keywords:
homologous recombination repair
; immunohistochemistry
; mesonephric-like adenocarcinoma
; ovary
; therapeutic target
1. Introduction
Mesonephric-like adenocarcinoma (MLA) of the ovary is a newly classified histological subtype added to the 2020 World Health Organization (WHO) classification of the female genital tumors. This tumor shares histopathological characteristics with mesonephric adenocarcinoma of the cervix, which originates from mesonephric duct remnants [1]. Most MLAs are reportedly associated with endometriosis, suggesting it is one of the tumors related to endometriosis [2,3].
Although MLA has similarities to low-grade endometrioid carcinoma, distinguishing features have been reported in morphological and immunohistochemical characteristics. Morphologically, the tumor cells, which are cuboidal to columnar, proliferate in various architectural patterns, including tubular, papillary, and solid structures, often containing eosinophilic material within glandular lumina [4]. Immunohistochemically, MLA is characterized by positive staining for TTF-1, GATA3, calretinin, and CD10 [1] and negative staining for estrogen receptor (ER), progesterone receptor (PR), and WT-1. Recognizing this histological type is crucial because, unlike low-grade endometrioid carcinoma, MLAs are reportedly associated with a poor prognosis and show a tendency for advanced stages and early recurrence [5].
Ovarian MLA is a rare tumor, expected to constitute less than 1% of ovarian tumors, similar to MLA in endometrial carcinoma, but its exact prevalence remains undetermined. Furthermore, reports indicate frequent cases of advanced stages and early recurrences, highlighting the need for therapeutic development. However, knowledge regarding molecular abnormalities that could serve as therapeutic targets in MLA is still insufficient.
This study aims to determine the prevalence of ovarian MLA and, by incorporating findings from the existing literature, elucidate its clinicopathological characteristics, focusing on potential therapeutic targets.
2. Materials and Methods
2.1. Patient Selection and Tissue Section Preparation
The present study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice and with the approval of the Institutional Review Board of the National Cancer Center, Tokyo, Japan (2020-111, 2010-077). Data from January 2010 to June 2023 were used, collecting a total of 683 consecutive patients with ovarian tumors. After the exclusion of 167 cases of borderline tumors or metastatic tumors, 516 cases of primary ovarian cancer were included in this study.
2.2. Pathological Diagnosis
At least two board-certified pathologists initially reviewed all the cases, and the pathological diagnoses in this study were subsequently confirmed by a gynecological pathologist (H.Y.) according to the 2020 WHO classification. Pathological diagnoses of MLA were confirmed based on the previously reported morphological features and immunohistochemical findings [4]. MLA should exhibit morphologic similarity to mesonephric adenocarcinoma of the uterine cervix. Different architectural patterns were observed, such as tubular, glandular (pseudo-endometrioid), papillary, cribriform, slit-like, retiform, glomeruloid, and solid, in various combinations. Intraluminal eosinophilic colloid-like material was frequently observed. Metaplastic changes such as squamous, ciliated, and mucinous differentiation are generally absent. Tumor cells are cuboidal or columnar cells with mild or moderately atypical angulated clear vesicular nuclei, often overlapping. The cytoplasm is usually scant to moderate, and mitotic activity is usually conspicuous. Immunohistochemically, the tumor cells show diffuse positivity of PAX8 and focal positivity of TTF-1, GATA3, CD10 (apical/luminal), and calretinin, whereas negativity of ER, PR, and WT-1. A p53 wild-type staining pattern and retained MMR proteins (MSH6 and PMS2) are also observed. One case of ovarian MLA was reported as a single case report [6]. The criteria for diagnosis of MLA were summarized in Supplementary Table S1, and the primary antibodies used for immunohistochemistry for IHC were listed in Supplementary Table S2.
2.3. Literature Review
The literature search was performed using publications indexed in PubMed (http://www.ncbi.nlm.nih.gov/pubmed) from February 1964 to December 2023. The following search terms were used in the PubMed database: “mesonephric-like adenocarcinoma AND ovary” or “ovarian mesonephric-like adenocarcinoma.” The reference lists of the included articles were manually checked for any undetected cases.
2.4. Statistical Analysis
Baseline characteristics were presented as frequencies and proportions for categorical variables. Continuous variables were presented as medians with ranges. All statistical analyses and graphic presentations were performed using SPSS (version 13.0J; SPSS Inc., Chicago, IL, USA).
3. Results
3.1. Clinical Characteristics
Of 516 cases of primary ovarian cancer, MLA was observed in 3 cases (0.6%). Each histological type and its prevalence are presented in Table 1.
The clinical features of these 3 cases are summarized in Table 2.
The ages ranged from 52 to 76 years, and all cases were postmenopausal. None of the cases were obese, and the initial symptoms included pelvic pain or the identification of an ovarian tumor due to a pelvic mass. All cases showed elevated CA125 levels, and CA19-9 was elevated in the two cases where it was measured. The maximum tumor diameter on imaging ranged from 13 to 16.5 cm. According to the International Federation of Gynecology and Obstetrics (FIGO, 2008), the initial stages were IC1 in two cases and IIIB in one case. Primary debulking surgery was performed in the two IC1 cases. The IIIB case underwent four courses of dose-dense Paclitaxel Carboplatin (ddTC) therapy as neoadjuvant chemotherapy, followed by interval debulking surgery and two additional courses of ddTC therapy. The initial pathological diagnosis was grade 1 endometrioid carcinoma in one case and mesonephric-like adenocarcinoma (MLA) in two cases. Recurrence was observed postoperatively in both IC1 cases at 1 and 16 months, respectively. The recurrence sites were the lung in one case and the lung and liver in the other, followed by chemotherapy. The postoperative follow-up period ranged from 8 to 42 months, with outcomes of dead of disease in one case, alive with disease in one case, and no evidence of disease in one case.
3.2. Pathological Findings
The pathological features of the three cases are summarized in Table 3 and representative histology is shown in Figure 1.
Macroscopically, all tumors had both solid and cystic components. Histologically, the tumors showed a mixed pattern of glandular and papillary structures, with eosinophilic colloid-like material inside the glands. The tumor cells ranged from cuboidal to columnar, with no nuclear pleomorphism, although some cells exhibited ground-glass nuclei and nuclear overlap. Endometriosis was observed in the background of all cases. Immunohistochemically, all cases were positive for GATA3, TTF-1, CD10, and calretinin but negative for estrogen and progesterone receptors and WT-1. All cases exhibited a wild-type p53 pattern and retained expression of MMR proteins. Additionally, programmed death-ligand 1 (PD-L1) was negative (combined positive score, CPS<1). The HER2 score for all tumors was 1+. The commercially available companion HRD test (MyChoice®) provided by Myriad Genetics was performed using the ovarian tumor tissue, revealing that homologous recombination repair was proficient in all the cases (genomic instability score was less than 5 in all the three cases and neither the BRCA1 nor the BRCA2 pathogenic variant was present).
3.3. Literature Review and Summary of Previously Reported Cases
A literature search on PubMed identified 97 cases of ovarian MLA with confirmed pathological diagnoses (Table 4 and Table 5) [1,2,5,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31].
The ages ranged from 29 to 84 years. According to FIGO, the initial stages were I in 33 cases, II in 12 cases, III in 15 cases, and IV in 7 cases. A significant proportion (84%, 21/25 cases) were associated with endometriosis. Recurrence was reported in 39% (26/67 cases). Three patients died among the 23 patients with available follow-up data. Notably, KRAS mutations were observed in 90% (38/42 cases). There has been minimal investigation into therapeutic target molecules, and no cases of HRD or MMRd have been identified to date. PD-L1 positivity has also not been reported.
4. Discussion
We identified three cases (0.6%) of MLA out of 516 primary ovarian cancer cases based on morphological and immunohistochemical staining results. Two cases showed metastatic recurrence, for which chemotherapy was initiated. All cases were HRP, pMMR, negative for PD-L1 (CPS < 1) and had a HER2 score 1+. A literature review identified 97 previously reported cases, confirming that advanced cases are common and have a high recurrence rate (39%). The molecular features associated with therapeutic targets in these cases were similar to our three cases, but a high frequency of KRAS mutations was observed, suggesting potential targets for therapy.
Ovarian MLA is predicted to be a rare tumor among ovarian neoplasms, similar to MLA in endometrial cancer, but there have been no reports on the frequency of ovarian MLA. In contrast, endometrial MLA has been reported to occur at a frequency of approximately 0.7% of all endometrial cancers [8,32]. In a combined morphological and molecular analysis of 570 endometrial carcinomas, only four cases (0.7%) were diagnosed as MLA [32]. Pors et al. (2018) also reported a similar frequency based on an analysis of 585 endometrial carcinomas between 1986 and 2017 [8]. Our investigation revealed that ovarian MLA, similar to endometrial MLA, occurs at a frequency of 0.6% (3/516, 95% CI 0.11%~ 1.8%) in a Japanese cohort.
Additionally, one of our three cases had been diagnosed as grade 1 endometrioid carcinoma. Before the establishment of the MLA concept, some MLA cases might have been diagnosed as low-grade endometrioid carcinoma. In cases of low-grade endometrioid carcinoma that show unusual clinical courses, such as early recurrence or distant metastasis, reconsideration of the diagnosis to MLA might be warranted.
Our three cases, along with the 97 cases identified through a literature review, suggest that MLA has more aggressive clinicopathological features compared to low-grade endometrioid carcinoma. Clinically notable, our literature review results show that approximately 12% of low-grade endometrioid carcinomas are reportedly stage III/IV [33], and 33% of MLAs are at stage III/IV. Additionally, while the recurrence rate of low-grade endometrioid carcinoma is around 9% [34], 39% of ovarian MLAs are reported to recur based on our literature review results. Furthermore, distant metastasis occurs in 33-56% of MLA cases [5,14]. Among our three cases, one was detected at an advanced stage, and two experienced distant metastatic recurrence. Histopathologically, compared to low-grade endometrioid carcinoma, MLAs typically have fewer solid components and more prominent gland formation. They lack the metaplastic changes such as squamous and mucinous metaplasia often seen in endometrioid carcinoma and exhibit cellular morphology that is more cuboidal than tall columnar. If immunostaining shows negative hormone receptor status, additional stains such as GATA3, TTF-1, calretinin, and CD10 can aid in diagnosing MLA [4]. Consistently, in the molecular classification of endometrial carcinoma (POLEmut, dMMR, p53abn, and NSMP), MLAs display an NSMP profile characterized by POLE wild-type, pMMR, and TP53 wild-type, which can further support the diagnosis.
Mismatch repair deficiency (dMMR) and PD-L1 expression in tumor cells or surrounding immune cells are known predictors of the efficacy of immune checkpoint inhibitors across various tumors [35]. Multiple studies have reported that ovarian MLA exhibits proficient mismatch repair (pMMR) [14,19]. Our literature review also found that all cases with evaluated MMR status were pMMR (100%, 35/35 cases). In contrast, approximately 8-19% of ovarian endometrioid carcinomas show dMMR [36], suggesting that pMMR might be a distinguishing feature of MLA from endometrioid carcinoma. However, the lack of increased tumor neoantigen production and immunogenicity in pMMR tumors indicates a lower likelihood of response to immune checkpoint inhibitors. Regarding PD-L1 expression in MLA, only one case has been reported as negative [11], and similarly, in our cases, PD-L1 expression was minimal in both tumor and surrounding immune cells. Although further studies with larger sample sizes are needed, the current evidence suggests that immune checkpoint inhibitors might be ineffective for advanced or recurrent MLA.
In our study, we reported HR status for the first time in multiple MLA cases. Previously, only one case had been reported as HRP [16], and our three cases were also HRP. While approximately half of high-grade serous carcinoma (HGSC) cases show homologous recombination deficiency (HRD) (Cancer Discovery, 2015), endometriosis-associated ovarian cancers are reported to have lower HRD rates compared to HGSC [37]. This suggests that ovarian MLA, like other endometriosis-associated ovarian cancers, may predominantly exhibit HRP. Since HRD is a predictive factor for the efficacy of PARP inhibitors, the effectiveness of PARP inhibitors for advanced or recurrent MLA may be limited, given the HRP status.
On the other hand, KRAS mutations might be a promising therapeutic target in MLA. Although we did not test for KRAS mutations in our cases, our literature review found that KRAS mutations were identified in 90% (38/42 cases) of tested cases, including specific mutations like G12V (42%, 16/38 cases), G12D (39%, 15/38 cases), and G12A (8%, 3/38 cases). Recent developments in targeted therapies for KRAS mutations in lung and other major cancers suggest potential cross-organ applicability. For example, the KRAS inhibitor sotorasib showed a 37% objective response rate in advanced or recurrent non-small cell lung cancer with KRAS p.G12C mutation [38]. Although most KRAS mutations in MLA are not p.G12C, ongoing research targeting other KRAS mutations might eventually benefit MLA treatment.
Additionally, although our analysis is limited to three cases, all exhibited weak HER2 protein expression (Score 1+). Recent studies have shown the clinical efficacy of HER2-ADC in low-HER2/HER2-expressing cancers, such as breast cancer [39], indicating that recurrent or metastatic MLA might also be a candidate for such therapies. Beyond HER2, the development of various ADCs is ongoing, and identifying target molecules in MLA is a crucial future research direction.
This study is a retrospective analysis conducted at a single high-volume cancer center, and the disease frequency distribution may differ from that in general hospitals. Therefore, this selection bias may influence the frequency of MLA identified in our study. Furthermore, our institution had only three cases to investigate therapeutic target molecules. Hence, the findings need to be validated through multicenter studies with larger cohorts of MLA cases. Additionally, this study did not investigate KRAS gene mutations. Although KRAS mutation testing is not mandatory for diagnosing MLA [4], identifying KRAS mutations could provide additional support.
In summary, an analysis of 516 primary ovarian cancer cases revealed that the frequency of ovarian MLA is 0.6%. Ovarian MLA exhibits HRP, pMMR, PD-L1 negativity, and low-HER2 expression, suggesting that the effectiveness of PARP inhibitors and immune checkpoint inhibitors may be limited. However, the high prevalence of KRAS mutations indicates that KRAS mutation could be a potential therapeutic target for recurrent or metastatic MLA. Given the high incidence of advanced, recurrent, and metastatic cases in MLA, it is essential to validate these therapeutic target findings in larger cohorts.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Morphological and immunohistochemical features of mesonephric-like adenocarcinoma; Table S2: Primary antibodies used for immunohistochemistry in this study.
Author Contributions
AO: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Visualization, Writing—original draft; HY: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing—original draft, Writing—review & editing; SK: Data curation, Resources, Visualization, Writing—review & editing; NK: Formal analysis, Investigation, Supervision, Writing—review & editing; MKK: Data curation, Resources, Supervision, Writing—review & editing; YT: Data curation, Resources, Supervision, Writing—review & editing; MU: Data curation, Resources, Supervision, Writing—review & editing; MI: Data curation, Resources, Supervision, Writing—review & editing.
Funding
This research received no external funding.
Institutional Review Board Statement
The present study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice and with the approval of the Institutional Review Board of the National Cancer Center, Tokyo, Japan (2020-111, 2010-077).
Informed Consent Statement
Informed consent was waived because of the retrospective nature of the study and the analysis used anonymous clinical data.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
We thank Sachiko Miura, M.T., and Toshiko Sakaguchi, M.T., for their technical assistance.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- McFarland, M.; Quick, C.M.; McCluggage, W.G. Hormone receptor-negative, thyroid transcription factor 1-positive uterine and ovarian adenocarcinomas: report of a series of mesonephric-like adenocarcinomas. Histopathology 2016, 68, 1013–1020. [Google Scholar] [CrossRef] [PubMed]
- McCluggage, W.G. Endometriosis-related pathology: a discussion of selected uncommon benign, premalignant and malignant lesions. Histopathology 2020, 76, 76–92. [Google Scholar] [CrossRef] [PubMed]
- Yano, M.; Shintani, D.; Katoh, T.; Hamada, M.; Ito, K.; Kozawa, E.; Hasegawa, K.; Yasuda, M. Coexistence of endometrial mesonephric-like adenocarcinoma and endometrioid carcinoma suggests a Müllerian duct lineage: a case report. Diagn Pathol 2019, 14, 54. [Google Scholar] [CrossRef] [PubMed]
- McCluggage, W.G. Mesonephric-like Adenocarcinoma of the Female Genital Tract: From Morphologic Observations to a Well-characterized Carcinoma With Aggressive Clinical Behavior. Adv Anat Pathol 2022, 29, 208–216. [Google Scholar] [CrossRef] [PubMed]
- Pors, J.; Segura, S.; Chiu, D.S.; Almadani, N.; Ren, H.; Fix, D.J.; Howitt, B.E.; Kolin, D.; McCluggage, W.G.; Mirkovic, J.; et al. Clinicopathologic Characteristics of Mesonephric Adenocarcinomas and Mesonephric-like Adenocarcinomas in the Gynecologic Tract: A Multi-institutional Study. Am J Surg Pathol 2021, 45, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Sugitani, A.; Ogawa, A.; Yoshida, H.; Kobayashi-Kato, M.; Kikkawa, N.; Tanase, Y.; Uno, M.; Ishikawa, M.; Kato, T. Ovarian Mesonephric-Like Adenocarcinoma With Recurrent Liver Metastases: A Case Report with Analysis of Therapeutic Molecular Targets. Int J Surg Pathol 2024, 32, 578–585. [Google Scholar] [CrossRef] [PubMed]
- Mirkovic, J.; McFarland, M.; Garcia, E.; Sholl, L.M.; Lindeman, N.; MacConaill, L.; Dong, F.; Hirsch, M.; Nucci, M.R.; Quick, C.M.; et al. Targeted Genomic Profiling Reveals Recurrent KRAS Mutations in Mesonephric-like Adenocarcinomas of the Female Genital Tract. Am J Surg Pathol 2018, 42, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Pors, J.; Cheng, A.; Leo, J.M.; Kinloch, M.A.; Gilks, B.; Hoang, L. A Comparison of GATA3, TTF1, CD10, and Calretinin in Identifying Mesonephric and Mesonephric-like Carcinomas of the Gynecologic Tract. Am J Surg Pathol 2018, 42, 1596–1606. [Google Scholar] [CrossRef] [PubMed]
- Chapel, D.B.; Joseph, N.M.; Krausz, T.; Lastra, R.R. An Ovarian Adenocarcinoma With Combined Low-grade Serous and Mesonephric Morphologies Suggests a Müllerian Origin for Some Mesonephric Carcinomas. Int J Gynecol Pathol 2018, 37, 448–459. [Google Scholar] [CrossRef] [PubMed]
- Dundr, P.; Gregová, M.; Němejcová, K.; Bártů, M.; Hájková, N.; Hojný, J.; Stružinská, I.; Fischerová, D. Ovarian mesonephric-like adenocarcinoma arising in serous borderline tumor: a case report with complex morphological and molecular analysis. Diagn Pathol 2020, 15, 91. [Google Scholar] [CrossRef]
- Seay, K.; Akanbi, T.; Bustamante, B.; Chaudhary, S.; Goldberg, G.L. Mesonephric-like adenocarcinoma of the ovary with co-existent endometriosis: A case report and review of the literature. Gynecol Oncol Rep 2020, 34, 100657. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Shen, Y.; Xie, C. Mesonephric-like adenocarcinoma of the ovary: A case report and a review of the literature. Medicine (Baltimore) 2020, 99, e23450. [Google Scholar] [CrossRef] [PubMed]
- Qazi, M.; Movahedi-Lankarani, S.; Wang, B.G. Cytohistopathologic correlation of ovarian mesonephric-like carcinoma and female adnexal tumor of probable Wolffian origin. Diagn Cytopathol 2021, 49, E207–E213. [Google Scholar] [CrossRef] [PubMed]
- da Silva, E.M.; Fix, D.J.; Sebastiao, A.P.M.; Selenica, P.; Ferrando, L.; Kim, S.H.; Stylianou, A.; Da Cruz Paula, A.; Pareja, F.; Smith, E.S.; et al. Mesonephric and mesonephric-like carcinomas of the female genital tract: molecular characterization including cases with mixed histology and matched metastases. Mod Pathol 2021, 34, 1570–1587. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Bae, G.E.; Jung, Y.Y.; Kim, H.S. Ovarian Mesonephric-like Adenocarcinoma With Multifocal Microscopic Involvement of the Fimbrial Surface: Potential for Misdiagnosis of Tubal Intraepithelial Metastasis as Serous Tubal Intraepithelial Carcinoma Associated With Ovarian High-grade Serous Carcinoma. In Vivo 2021, 35, 3613–3622. [Google Scholar] [CrossRef] [PubMed]
- Karpathiou, G.; Chauleur, C.; Picot, T.; Achour, S.; Corsini, T.; Devouassoux-Shisheboran, M.; Peoc’h, M. Ovarian mesonephric-like adenocarcinoma: morphological diversity and histogenetic considerations of an unusual tumour. Pathology 2022, 54, 647–650. [Google Scholar] [CrossRef] [PubMed]
- Ujita, M.; Abiko, K.; Kuwahara, R.; Emoto, I.; Amano, Y.; Konishi, I. Mesonephric-like adenocarcinoma of the ovary in an elderly woman: A case report and a review of the literature. J Obstet Gynaecol Res 2021, 47, 4490–4495. [Google Scholar] [CrossRef] [PubMed]
- Deolet, E.; Arora, I.; Van Dorpe, J.; Van der Meulen, J.; Desai, S.; Van Roy, N.; Kaur, B.; Van de Vijver, K.; McCluggage, W.G. Extrauterine Mesonephric-like Neoplasms: Expanding the Morphologic Spectrum. Am J Surg Pathol 2022, 46, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Koh, H.H.; Park, E.; Kim, H.S. Mesonephric-like Adenocarcinoma of the Ovary: Clinicopathological and Molecular Characteristics. Diagnostics (Basel) 2022, 12. [Google Scholar] [CrossRef] [PubMed]
- Ishida, K.; Ashihara, T.; So, M.; Minamiguchi, S.; Matsumura, N.; Nonogaki, T. Synchronous ovarian and uterine mesonephric-like carcinoma that potentially arose from endometrioid adenofibroma: A case report. J Obstet Gynaecol Res 2023, 49, 1052–1056. [Google Scholar] [CrossRef] [PubMed]
- Arslanian, E.; Singh, K.; James Sung, C.; Quddus, M.R. Somatic mutation analysis of Mesonephric-Like adenocarcinoma and associated putative precursor Lesions: Insight into pathogenesis and potential molecular treatment targets. Gynecol Oncol Rep 2022, 42, 101049. [Google Scholar] [CrossRef] [PubMed]
- Nilforoushan, N.; Liu, L.; Cheang, G.; Sui, A.C.; Andersen, J.; Finkelman, B.S.; Liu, Y.; Nasseri-Nik, N.; Vang, R.; Ronnett, B.M.; et al. Mucinous Tumor Coexisting With Mesonephric-like Proliferation/Tumor in the Ovary: A Novel Association. Am J Surg Pathol 2022, 46, 1095–1105. [Google Scholar] [CrossRef] [PubMed]
- Mirkovic, J.; Olkhov-Mitsel, E.; Amemiya, Y.; Al-Hussaini, M.; Nofech-Mozes, S.; Djordjevic, B.; Kupets, R.; Seth, A.; McCluggage, W.G. Mesonephric-like adenocarcinoma of the female genital tract: novel observations and detailed molecular characterisation of mixed tumours and mesonephric-like carcinosarcomas. Histopathology 2023, 82, 978–990. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Park, K.J.; Rehrauer, W.M.; Weisman, P.S. Mesonephric-like adenocarcinoma of the ovary with squamoid morular metaplasia, aberrant β-catenin expression, and concurrent FGFR2 and CTNNB1 mutations: a case report. Virchows Arch 2024, 484, 147–150. [Google Scholar] [CrossRef] [PubMed]
- Nilforoushan, N.; Liu, L.; Finkelman, B.S.; Andersen, J.; Liu, Y.; James, J.; Hung, C.F.; Wu, T.C.; Vang, R.; Xing, D. Ovarian Combined Serous Borderline Tumor/Low-grade Serous Carcinoma and Mesonephric-like Lesion: Report of 2 Cases With New Observations. Int J Gynecol Pathol 2023, 42, 182–191. [Google Scholar] [CrossRef] [PubMed]
- Stolnicu, S.; Bartalis, R.J.; Ye, Q.; Da Cruz Paula, A.; Weigelt, B.; Soslow, R.A. Ovarian RASoma With Mesonephric-like Adenocarcinoma and Mixed Mullerian Components: A Case Report With Molecular Analysis Demonstrating Multidirectional Mullerian Differentiation. Int J Gynecol Pathol 2023, 42, 620–626. [Google Scholar] [CrossRef] [PubMed]
- Kommoss, F.K.; Lee, C.H.; Tessier-Cloutier, B.; Gilks, C.B.; Stewart, C.J.; von Deimling, A.; Köbel, M. Mesonephric-like adenocarcinoma harbours characteristic copy number variations and a distinct DNA methylation signature closely related to mesonephric adenocarcinoma of the cervix. J Pathol 2024, 262, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Nadarajah, R.; Busmanis, I. Synchronous Bilateral Ovarian Mesonephric-like Adenocarcinomas with Separate Origins from High-Grade Mullerian Adenosarcoma and Endometriosis: Report of a Rare Case. Int J Gynecol Pathol 2024, 43, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.S.; Carney, M.E.; Killeen, J.L. Two Cases of Mesonephric-like Carcinoma Arising From Endometriosis: Case Report and Review of the Literature. Int J Gynecol Pathol 2023, 42, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Linck, J.; Torres, W. Mesonephric-like adenocarcinoma arising from endometrioid adenofibroma in a patient with in-utero exposure to diethylstilbestrol: A case report. Case Rep Womens Health 2023, 39, e00531. [Google Scholar] [CrossRef] [PubMed]
- Nagase, S.; Saeki, H.; Ura, A.; Terao, Y.; Matsumoto, T.; Yao, T. Mixed Mesonephric-like Adenocarcinoma, Clear Cell Carcinoma, and Endometrioid Carcinoma Arising from an Endometriotic Cyst. Int J Surg Pathol 2023, 10668969231213390. [Google Scholar] [CrossRef] [PubMed]
- Kolin, D.L.; Costigan, D.C.; Dong, F.; Nucci, M.R.; Howitt, B.E. A Combined Morphologic and Molecular Approach to Retrospectively Identify KRAS-Mutated Mesonephric-like Adenocarcinomas of the Endometrium. Am J Surg Pathol 2019, 43, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Peres, L.C.; Cushing-Haugen, K.L.; Köbel, M.; Harris, H.R.; Berchuck, A.; Rossing, M.A.; Schildkraut, J.M.; Doherty, J.A. Invasive Epithelial Ovarian Cancer Survival by Histotype and Disease Stage. J Natl Cancer Inst 2019, 111, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Swift, B.E.; Covens, A.; Mintsopoulos, V.; Parra-Herran, C.; Bernardini, M.Q.; Nofech-Mozes, S.; Hogen, L. The effect of complete surgical staging and adjuvant chemotherapy on survival in stage I, grade 1 and 2 endometrioid ovarian carcinoma. Int J Gynecol Cancer 2022, 32, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Paver, E.C.; Cooper, W.A.; Colebatch, A.J.; Ferguson, P.M.; Hill, S.K.; Lum, T.; Shin, J.S.; O’Toole, S.; Anderson, L.; Scolyer, R.A.; et al. Programmed death ligand-1 (PD-L1) as a predictive marker for immunotherapy in solid tumours: a guide to immunohistochemistry implementation and interpretation. Pathology 2021, 53, 141–156. [Google Scholar] [CrossRef] [PubMed]
- Soovares, P.; Pasanen, A.; Similä-Maarala, J.; Bützow, R.; Lassus, H. Clinical factors and biomarker profiles associated with patient outcome in endometrioid ovarian carcinoma - Emphasis on tumor grade. Gynecol Oncol 2022, 164, 187–194. [Google Scholar] [CrossRef] [PubMed]
- da Cunha Colombo Bonadio, R.R.; Fogace, R.N.; Miranda, V.C.; Diz, M.D.P.E. Homologous recombination deficiency in ovarian cancer: a review of its epidemiology and management. Clinics (Sao Paulo) 2018, 73, e450s. [Google Scholar] [CrossRef] [PubMed]
- Skoulidis, F.; Li, B.T.; Dy, G.K.; Price, T.J.; Falchook, G.S.; Wolf, J.; Italiano, A.; Schuler, M.; Borghaei, H.; Barlesi, F.; et al. Sotorasib for Lung Cancers with. N Engl J Med 2021, 384, 2371–2381. [Google Scholar] [CrossRef] [PubMed]
- Modi, S.; Jacot, W.; Yamashita, T.; Sohn, J.; Vidal, M.; Tokunaga, E.; Tsurutani, J.; Ueno, N.T.; Prat, A.; Chae, Y.S.; et al. Trastuzumab Deruxtecan in Previously Treated HER2-Low Advanced Breast Cancer. N Engl J Med 2022, 387, 9–20. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Morphological and immunohistochemical findings of a mesonephric-like adenocarcinoma of the ovary. The tumor shows various histological patterns, including glandular and papillary patterns (A, ×100) and tubular structures containing eosinophilic material in the hyalinized stroma (B, ×100). The tumor cells are cuboidal to cylindrical with enlarged nuclei (C, ×100). Immunohistochemically, the tumor cells are positive for PAX8, GATA3 (focal), TTF1 (focal), and CD10 (luminal) but negative for estrogen receptor and progesterone receptor (D-I, ×200). In addition, The tumor cells show intact expression of PMS2 and MSH6 (J and K, ×200), weakly positive for HER2 (focal; score 1+, ×200) (L), and PD-L1 negative (combined positive score < 1) (M, ×200).
Figure 1.
Morphological and immunohistochemical findings of a mesonephric-like adenocarcinoma of the ovary. The tumor shows various histological patterns, including glandular and papillary patterns (A, ×100) and tubular structures containing eosinophilic material in the hyalinized stroma (B, ×100). The tumor cells are cuboidal to cylindrical with enlarged nuclei (C, ×100). Immunohistochemically, the tumor cells are positive for PAX8, GATA3 (focal), TTF1 (focal), and CD10 (luminal) but negative for estrogen receptor and progesterone receptor (D-I, ×200). In addition, The tumor cells show intact expression of PMS2 and MSH6 (J and K, ×200), weakly positive for HER2 (focal; score 1+, ×200) (L), and PD-L1 negative (combined positive score < 1) (M, ×200).
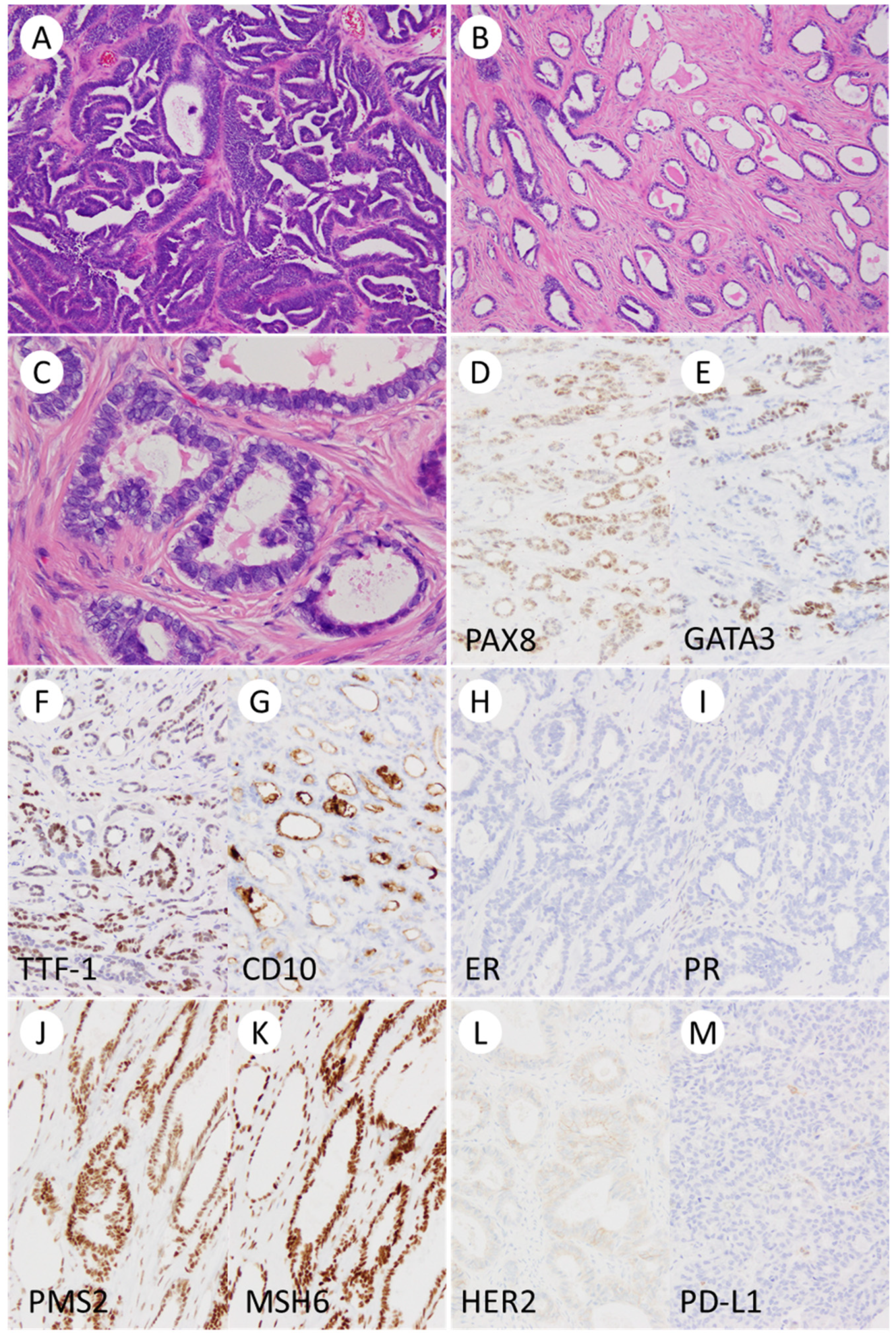

Table 1.
Histological type of 516 primary ovarian cancers.
| Histological type | n (%) |
|---|---|
| Total n = 516 | |
| High-grade serous carcinoma | 239 (46.3) |
| Clear cell carcinoma | 116 (22.5) |
| Endometrioid carcinoma | 57 (11.0) |
| Mucinous carcinoma | 30 (5.8) |
| Adenocarcinoma, unclassifiable* | 17 (3.3) |
| Low-grade serous carcinoma | 16 (3.1) |
| Mixed cell carcinoma | 11 (2.1) |
| Carcinosarcoma | 8 (1.6) |
| Immature teratoma | 4 (0.8) |
| Yolk sac tumor | 4 (0.8) |
| Mature teratoma with malignant transformation | 3 (0.6) |
| Mesonephric-like adenocarcinoma | 3 (0.6) |
| Undifferentiated carcinoma | 2 (0.4) |
| Malignant Brenner tumor | 1 (0.2) |
| Malignant struma ovarii | 1 (0.2) |
| Squamous cell carcinoma | 1 (0.2) |
| Others (unclassified) | 3 (0.6) |
* Small amounts of residual adenocarcinoma after chemotherapy.
Table 2.
Clinical characteristics of 3 cases of ovarian mesonephric-like adenocarcinoma.
| Case 1 | Case 2 | Case 3 | |
|---|---|---|---|
| Age [year] | 76 | 52 | 71 |
| Obstetric history | G3P3 | G0P0 | G0P0 |
| Menopause [year] | 58 | 50 | 51 |
| Previous medical history | rheumatoid arthritis | leiomyoma, lt shoulder fracture | breast cancer, dyslipidemia |
| Body mass index [kg/m2] | 18 | 22.9 | 22.5 |
| Symptom | pelvic pain, abdominal distension | adnexal mass | pelvic pain, pelvic mass |
| Tumor marker | CA19-9: 290 U/ml, CA125: 434 U/ml | CA19-9: 135 U/ml, CA125: 64 U/ml | CA125: 199 U/ml |
| Radiological diagnosis | rt ovarian cancer | lt ovarian cancer (s/o EM, CCC) | ovarian cancer |
| Clinical stage (FIGO2008) | cT1N0M0 | cT1N0M0 | cT3bN0M0 |
| Surgical procedure | PDS, TAH+BSO+OMT+PLND | PDS, TAH+BSO+OMT+PLND | IDS, TAH+BSO+OMT+PLND+LAR |
| Pathological stage | pT1c1N0M0 | pT1c1N0M0 | ypT2N0M0 |
| Tumor size [cm] | 15.5 | 13 | 16.5 |
| Recurrence [month] | Yes, 16 month | Yes, 1 month | No |
| Metastatic site | liver, lung | liver | - |
| Follow-up time [month] | 42 | 9 | 8 |
| Prognosis | DOD | AWD | NED |
Abbreviations: PDS, primary debulking surgery; TAH, total abdominal hysterectomy; BSO, bilateral salpingo-oophorectomy; OMT, omentectomy; PLND, pelvic limph node dissection; LAR, low anterior resection of rectum; DOD, dead of disease; AWD, alive with disease; NED, no evidence of disease.
Table 3.
Pathological features of 3 cases of ovarian mesonephric-like adenocarcinoma.
| Case 1 | Case 2 | Case 3 | |
|---|---|---|---|
| Laterality | bilateral | left | bilateral |
| Tumor size [cm] | rt. 15×11.5×9; lt. 4×3×1.5 | 16×10×4 | rt. 3.5×2.5×1; lt. 11.5×7×2 |
| Macroscopic type | solid and cystic | solid and cystic | solid and cystic |
| Glandular and papillary pattern | + | + | + |
| Intraluminal eosinophilic secretion | + | + | + |
| Spindled tumor cells | + | + | + |
| Sex cord-like pattern | + | - | + |
| Hyalinized/Fibrous stroma | + | + | + |
| Tumor infiltrating lymphocytes | a few | a few | a few |
| Glassy nucleus | + | + | + |
| Mitotic counts | up to 14/10HPFs | up to 10/10HPFs | up to 11/10HPFs |
| Metaplasia | no | no | no |
| Endometriosis | + | + | + |
| Endometrium | atrophic | atrophic | atrophic |
| Adenomyosis/Leiomyoma | -/+ | +/+ | +/+ |
| Immunohistochemistry | |||
| ER/PR/WT-1 | -/-/- | -/-/- | -/-/- |
| GATA3/TTF-1 positivity | focal/focal | focal/focal | diffuse/focal |
| CD10/Calretinin positivity | focal/focal | focal/focal | focal/rare |
| p53 | wild-type pattern | wild-type pattern | wild-type pattern |
| MMR | pMMR | pMMR | pMMR |
| PD-L1 (22C3) | CPS < 1 | CPS < 1 | CPS < 1 |
| HER2 | score 1+ | score 1+ | score 1+ |
| HR (myChoice®) | HRP (GIS = 4) | HRP (GIS = 1) | HRP (GIS = 2) |
Abbreviations: pMMR, mismatch repair proficient; CPS, combined positive score; HRP, homologous recombination proficient; GIS, genomic instability score.
Table 4.
Clinicopathological summary of previously reported cases of mesonephric-like adenocarcinoma of the ovary.
Table 4.
Clinicopathological summary of previously reported cases of mesonephric-like adenocarcinoma of the ovary.
| Author/year | n | Age | Laterality | Size (cm) | Surgical treatment | FIGO stage | Recurrence | Survival | Follow-up time (month) |
|---|---|---|---|---|---|---|---|---|---|
| McFarland/2016; Mirkovic/2018 | 5 | 42–62 (4); N/A (1) |
B (2); L (2); N/A (1) | 4-32 | TH + BSO (2); BSO (1); N/A (2) | IA (1); IC (1); IIB (1); IIIC (1); N/A (1) | Yes (1); No (4) | Alive (5) | 7–37 (4); N/A (1) |
| Pors/2018 | 1 | 67 | N/A | N/A | N/A | IC | N/A | N/A | N/A |
| Chapel/2018 | 1 | 80 | R | 10.6 | TH+BSO+OMT+P | IIIC | No | Alive | 3 |
| McCluggage/2020 | 5 | 50-77 | R (1); L (3); N/A (1) | 6 (1); N/A (4) | TH+BSO+PLND+OMT+P (1); N/A (4) | IIIA (1); NA (4) | N/A | N/A | N/A |
| Dundr/2020 | 1 | 61 | L | 3.5 | TH+BSO+OMT+P+A | IVB | No | Alive | N/A |
| Seay/2020 | 1 | 67 | R | 11 | TH+RSO+PLND+OMT | IA | Yes, abdominopelvic | Alive | 18 |
| Chen/2020 | 1 | 29 | R | 10 | TH+BSO+PLND+PALND+OMT | IC2 | No | Alive | 13 |
| Qazi/2020 | 1 | 51 | N/A | 18 | N/A | N/A | N/A | N/A | N/A |
| Pors/2021 | 25 | 36-81 | N/A | N/A | N/A | I (11); II–IV (7); N/A (7) | Yes (10); No (14); N/A (1) | 5-yr OS 71% (23) | 101 (mean) |
| da Silva/2021 | 15 | 36-76 | B (1); R (2); N/A (12) | 3.5-18.5 (12); N/A (3) | N/A | IA (2); IC (3); IIB (2); IIIA (1); IIIC (2); IV (3); NA (2) | Yes (10: abdominopelvic, 6; distant metastasis, 4) |
N/A | N/A |
| Kim/2021 | 1 | 47 | L | 4.4 | PLND+PALND+OMT+P | IIIC | No | Alive | 11 |
| Karpathiou/2021 | 1 | 74 | L | 19 | TH+OMT+P+LND | IIIB | No | Alive | 6 |
| Ujita/2021 | 1 | 84 | L | 7 | TH+BSO+pOMT | IC3 | No | Alive | 4 |
| Deolet/2022 | 4 | 33-75 | R (1); L (2); N/A (1) | 7-15 (3); N/A (1) | LSO (1); TH+BSO+OMT (1); BSO (1); cyctectomy (1) | IA (1); IC (1); IIIC (1); IVB (1) | Yes, abdominopelvic (1); No (3) | Alive (4) | 8-46 |
| Koh/2022 | 5 | 42-61 | R (2); L (3) | 4.7-11.0 | TH+BSO+PLND+PALND+P+OMT (1); TH+BSO+PLND+P+OMT (1); BSO+PLNb+P+OMT (1); TH+BSO+PLND+PALND+Pb+OMT (1); TH+BSO+P (1) | IA (1); IC (3); IIB (1) | Yes, distant metastasis (1); No (3); N/A (1) | Dead (1); Alive (3); N/A (1) | 11-53 (4); N/A (1) |
| Ishida/2022 | 1 | 69 | B | 3.2, 2.0 | TH+BSO | IIB | Yes, lung | N/A | N/A |
| Arslanian/2022 | 2 | 66-67 | R (1); L (1) | 8, 18 | TH+BSO+infracolic omentectomy+rightPALND(1); TH+BSO+PLND+OMT (1) | IC (1); IIIA1 (1) |
- | Dead (1); Alive (1) | 15-32 |
| Nilforoushan/2022 | 2 | 55-58 | L (2) | 12, 13 | TH+BSO+OMT (1); TH+LSO+OMT+LND+pelvic staging biopsy (1) | N/A | N/A | N/A | N/A |
| Mirkovic/2023 | 2 | 61-62 | R (2) | 9, 27 | TH+BSO+OMT+LAR (1); BSO+OMT+rectosigmoid and posterior vaginal ressection (1) | IIB (2) | N/A | Alive (2) | 12, 6 |
| Xu/2023 | 1 | 78 | R | 4.3 | TH+BSO+OMT+PLND | IC2 | Yes, pelvic | N/A | 60 |
| Nilforoushan/2023 | 1 | 70 | B | 6.2, 2.9 | TH+BSO+OMT | IVB | N/A | N/A | N/A |
| Stolnicu/2023 | 1 | 63 | L | 12 | TH+BSO | IC | N/A | N/A | N/A |
| Kommoss/2023 | 14 | 50-83 | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| Zhao/2023 | 1 | 58 | B | 10, 24 | TH+BSO | IC, IIA | N/A | N/A | N/A |
| Chang/2023 | 2 | 51-57 | R (2) | 9.6, 5.7 | TH+BSO+OMT+rt PLND (1); RATH+BSO+PLND (1) | IIIA1, IA1 | N/A | N/A | N/A |
| Linck/2023 | 1 | 65 | L | 3.2 | RATH+BSO+OMT+P | IIB | - | Alive | N/A |
| Nagase/2023 | 1 | 48 | R | 20 | RSO+OMT+P+colostomy (post TH+LSO) | IVB | - | Dead | 15 |
| The present study | 3 | 52-76 | L (1); R (1); B (1) | 13, 15.5, 16.5 | TH+BSO+OMT+PLNb (2); TH+BSO+OMT+PLNb+LAR (1) | IC1 (2); ypIIB (1) | Yes (2: liver, 2; lung, 1), No (1) | Alive (2); Dead (1) | 7-44 |
Abbreviations: N/A, not available; B, bilateral; L, left; R, right; TH, total hysterectomy; BSO, bilateral salpingo-oophorectomy; OMT, omentectomy; P, peritoneal resection; PLND/b, pelvic lymph node dissection/biopsy; PALND, para-aortic lymph node dissection; LSO, left salpingo-oophorectomy.
Table 5.
Genetic analysis and therapeutic targets in previously reported cases of mesonephric-like adenocarcinoma of the ovary.
Table 5.
Genetic analysis and therapeutic targets in previously reported cases of mesonephric-like adenocarcinoma of the ovary.
| Author/year | n | HRD | MMR | PD-L1 | HER2 | Genetic analysis | KRAS mutation | Other gene alterations |
|---|---|---|---|---|---|---|---|---|
| McFarland/2016; Mirkovic/2018 | 5 | N/A | N/A | N/A | N/A | TS (4); N/A (1) | 4/4 | PIK3CA |
| Pors/2018 | 1 | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| Chapel/2018 | 1 | N/A | N/A | N/A | N/A | TS | - | NRAS, BCOR |
| McCluggage/2020 | 5 | N/A | N/A | N/A | N/A | TS (1); N/A (4) | 1/1 | - |
| Dundr/2020 | 1 | N/A | N/A | N/A | N/A | TS | 1/1 | PIK3CA, CHEK2 |
| Seay/2020 | 1 | N/A | N/A | score 0 | N/A | TS | - | - |
| Chen/2020 | 1 | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| Qazi/2020 | 1 | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| Pors/2021 | 25 | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| da Silva/2021 | 15 | N/A | Intact (8); N/A (7) | N/A | N/A | TS | 13/15 | PIK3CA, SPOP, NRAS, SETD8, CTNNB1, CREBBP, NOTCH3, ARID1A, FBXW7, FANCA, AKT1, ASXL1, RAD54L |
| Kim/2021 | 1 | N/A | Intact | N/A | N/A | TS | 1/1 | - |
| Karpathiou/2021 | 1 | HRP | Intact | N/A | N/A | TS | 1/1 | CTNNB1 |
| Ujita/2021 | 1 | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| Deolet/2022 | 4 | N/A | N/A | N/A | N/A | TS | 3/4 | PIK3CA, PTEN amplification, 12p isochromosome |
| Koh/2022 | 5 | N/A | Intact (4); N/A (1) | N/A | N/A | TS (4); N/A (1) | 4/4 | - |
| Ishida/2022 | 1 | N/A | N/A | N/A | N/A | TS | 1/1 | SPOP, FANCA |
| Arslanian/2022 | 2 | N/A | Intact (2) | N/A | N/A | TS | 2/2 | PIK3CA |
| Nilforoushan/2022 | 2 | N/A | N/A | N/A | N/A | TS (1); N/A (1) | 1/2; N/A (1) | CTNNB1, FGFR2 amplification, CDKN2A/ p16 deletion |
| Mirkovic/2023 | 2 | N/A | Intact | N/A | N/A | TS | 2/2 | FANCA(1/2), CREBBP(2/2), POLE(1/2), PTEN(1/2) |
| Xu/2023 | 1 | N/A | Intact | N/A | N/A | TS | - | FGFR2, CTNNB1 |
| Nilforoushan/2023 | 1 | N/A | Intact | Negative | N/A | TS | 1/1 | NOTCH1 |
| Stolnicu/2023 | 1 | N/A | N/A | N/A | N/A | TS | 1/1 | RRR2R1A, ARHGAP35, IRS1 |
| Kommoss/2023 | 14 | N/A | Intact (14) | N/A | N/A | N/A | N/A | N/A |
| Zhao/2023 | 1 | N/A | Intact | N/A | N/A | N/A | N/A | N/A |
| Chang/2023 | 2 | N/A | N/A | N/A | N/A | TS (1); N/A (1) | 1/1 | TP53, PPP2R1A, SPEN |
| Linck/2023 | 1 | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| Nagase/2023 | 1 | N/A | N/A | N/A | N/A | TS | 1/1 | PIK3CA, FBXW7, RAD21 |
| The present case | 3 | HRP (3) | Intact (3) | CPS < 1 (3) | Score 1+ (3) | N/A | N/A | N/A |
Abbreviations: HRD, homologous recombination repair deficiency; MMR, mismatch repair; PD-L1, Programmed cell Death ligand 1; HER2, human epidermal growth factor receptor 2; TS, target sequencing; HRP, homologous recombination repair proficient.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



