
Submitted:
13 August 2024
Posted:
14 August 2024
You are already at the latest version
Abstract
Despite inclusive design focusing on improving environmental accessibility for mobility aid (MA) users, it often fails to ensure true inclusivity due to mismatches between interventions and user perceptions. Therefore, understanding mobility aids users' perceptions of inclusivity is essential for advancing disability studies and design, as it highlights key interventions for more effective practices. This study aims to explore perceived inclusivity in MAs usage and identifies gaps in users' needs, classifying their needs and offering recommendations to meet them. First, the DARE-Inclusive Design Framework was used to develop interview guidelines and interpret results. Next, semi-structured, in-depth interviews were conducted with 12 experienced physiotherapists in Iran, and finally, an inductive thematic analysis was used to identify and present themes. Four themes were identified: 1. Perceived Financial Value: Assessing Worth, 2. Objective Enhancements: Optimizing Environments and MAs, 3. Subjective Enhancements: Trustworthiness, Support, and Hope, and 4. Contextual Factors: Interpretations and Representations. The four interconnected themes provide guidelines for inclusivity-oriented interventions, emphasizing financial assessment, high-tech integration, and aesthetic and symbolic considerations in mobility aid design. Physiotherapists can also mediate emotional responses and enhance inclusion during rehabilitation. Additionally, social context and disability etiology impact users' acceptance and use of MAs.
Keywords:
Mobility aids
; Social inclusion
; Physiotherapy
; Inclusive design
; User experiences
1. Introduction
Users of mobility aids (MAs) (wheelchairs, walkers, orthosis, etc.), often experience various physical and social challenges in their daily lives, including incompatible environments [1,2], uneven distribution of accessibility to health services [3], public transport [4], and limited involvement in social interactions and activities [5,6,7,8]. Such challenges can potentially stimulate the perceived differences between MA users and individuals without mobility issues. This sense of separation, sometimes accompanied by negative feedback in their social experiences, triggers emotional reactions and may negatively impacts their self-perception [9,10,11]. This, in turn, leads to further social isolation [12,13] and can create a positive feedback loop [14] where increasing isolation and negative self-perception amplify each other. This loop may intensify negative responses regarding their environment, perpetuating a cycle of social and emotional challenges [9,15].
In response to the MA users’ challenges, the inclusive design approach tries to consider the aspects of equity, aging, disability, and technology-related skills to eliminate barriers—in environment and interactions with MAs—among individuals with diverse capabilities [16,17]. Using this approach enables designers to positively influence and shape users' experience in using MAs [18,19]. However, achieving true inclusivity cannot be limited to merely ensuring environmental accessibility and the effectiveness of MAs [20]. It is also essential to find out how MA users perceive, appraise, and experience inclusivity in practice. For instance, negative stereotypes toward disability in social interactions, can influence MA users' perceptions of disability [21,22,23]. Additionally, if the design of a wheelchair—both its appearance and operational aspects—does not align with the users' needs and preferences, users may still feel excluded. Therefore, other factors beyond accessibility can influence and shape their perceived inclusivity (PI) [24]. To this end, it is essential to explore whether MA users genuinely perceive the inclusivity-oriented interventions or if these efforts are seen as focusing solely on physical accessibility [25].
In this regard, UNICEF suggests the "5 A & Q" principles, which aim to consider the needs of users requiring assistive devices. These principles include Availability, Accessibility, Affordability, Adaptability, Acceptability, and Quality [26,27]. Previous studies have primarily focused on addressing the needs of individuals with mobility disabilities by implementing environmental adjustments [28,29,30], facilitating MA users' navigation [31], and optimizing ergonomics [29]. One of the few case studies in Iran evaluated the accessibility of library buildings and equipment. The results showed that accessibility was not rated as 'good' either by disabled users or architects [32]. These studies highlight the importance of wheelchair accessibility as a key determinant of independence, social participation, and overall inclusion in society [24].
Besides wheelchair accessibility, the perception of disability symbols affects attitudes toward inclusivity. The ambiguous design of the International Symbol of Access creates confusion among individuals with various impairments [33]. By primarily representing mobility impairment, it inadvertently contributes to a sense of exclusivity for those with other types of impairments. Furthermore, a lack of inclusivity is still perceived even in hospitality and customer services, where personalized support and accessibility are of great importance. Reports in Iran show that negative stereotypes and discrimination, even among state social workers and medical workers, impede people with disabilities from accessing essential services [23]. Also, while wheelchair tourists are eager to travel, existing barriers make them more selective about natural destinations, indicating that true inclusivity requires a cultural shift [25].
In this context, while studies have emphasized the importance of understanding the inclusivity across various aspects, including physical, psychological, and social considerations [20,34], no study to date has holistically examined the MA users’ PI and its classifications. Filling this gap provides valuable insights for enhancing mobility aids, environments, and related services, resulting from inclusivity-oriented interventions that are both relevant and effective. It also contributes to creating targeted policies and social programs that meet MA users' socioemotional needs [35], promoting inclusivity and support, thereby reducing stigma and enhancing social engagement. In this study, we aim to bridge this gap of knowledge by exploring the interconnected layers including emotional, social, and design aspects. We focus specifically on identifying the challenges users face when interacting with their MAs or engaging in social interactions in public and private settings. Additionally, due to the limited research on inclusivity in Iran and the underrepresentation of voices from Iranian MA users in global studies, we chose this setting for our study. To this end, we answer the following questions: What key themes represent the perceived mismatches among those with movement disabilities who use MAs? How can inclusivity-oriented interventions alleviate perceptions of exclusion? By addressing these questions, this study contributes to the multifaceted understanding of PI, aiding disability studies in creating a framework for co-design practices and policies that extend beyond accessibility.
This study begins with methodology, including a review of the DARE-Inclusive Design Framework, interview procedures, and data collection. In the results, we outline the themes of PI, which are analyzed in the discussion section to identify opportunities for enhancing the experiences of MA users. After discussing the future research directions, we provide a conclusion.
2. Materials and Methods
2.1. Establishment of the Study Procedure
Given that the phenomena of inclusivity and its properties are interconnected and subjective, a qualitative approach is adopted, which enables us in accessing tacit and taken-for-granted understanding of the PI [36]. To this end, the authors initially clarified key concepts in inclusive design, highlighting its differences from design for accessibility, design for all, and universal design [37]. Then, to examine and classify the experiences of MA users, we employed the DARE-Inclusive Design Framework [20]. In line with our research objectives, a number of experienced physiotherapists were selected for the in-depth interviews (IDIs) [38,39].
Subsequently, themes and sub-themes were identified, analyzed, and classified according to the DARE framework (Figure 1).
2.2. DARE-Inclusive Design Framework
This framework, outlined by Patrick and Hollenbeck categorizes overarching barriers in inclusive design into three levels: physical, social, and attitudinal [20]. DARE framework proposes that (a: Design) design signals a degree of social inclusion or exclusion, (b: Appraisal) users take note of these cues and evaluate the design based on its inclusivity, (c: Response) emotions are triggered by a mismatch between the individual (or aspects of their identity) and the design, and finally, (d: Experience) these emotions shape consumers' perception and overall experience. The three levels of DARE are as follows:
- Level 1 (L1) focuses on accessibility and is linked to industry regulations. L1 follows market-driven reform policies and neoliberalism principles, which suggest that market forces can self-regulate. Designs under L1 aim to meet minimum standards to remove barriers.
- Level 2 (L2) emphasizes increased engagement and positive emotions, promoting equitable access and fair relationships guided by social justice principles. Rooted in social justice, L2 seeks to validate users' experiences through empathy and understanding of how products impact their everyday lives.
- At Level 3 (L3), a minimal mismatch between users and design is ideal. L3 focuses on empowered success through positive design, emphasizing human flourishing and the complete inclusion of all individuals [40]. Users experience a state of flow, enjoying profound immersion in tasks with harmonious interaction between themselves and the environment, enabling fluid and creative interaction with their physical and social environment [20].
This framework allows us to comprehensively consider three levels of inclusivity, and the mismatches between users and their MAs, environment, and social context [20]. According to DARE, we categorize themes into three levels and explain how design optimization of environments and MAs influences the initial appraisal, prompts a response, and shapes the perception and experience of MA users.
2.3. Development of Interview Guidelines and Questions
For the initial draft of the interview guide, research team members reviewed literature review and highlighted the key relevant aspects of the DARE framework [20]. The authors discussed potential exclusion areas, such as engineering and ergonomics, which prioritize physical interactions. We integrated these considerations with insights from previous research. For study validity and rigor, a physiotherapist and an inclusive designer were invited to assemble a panel of design experts to refine the interview guidelines and questions further. Their insights and corrections were used only to refine the interview questions and were not incorporated into the final dataset. Following unanimous agreement among authors, the final interview guide was approved, outlining the sequence and content of questions under established guidelines.
2.4. Recruitment and Study Population
We considered physiotherapists as the participants due to their prolonged involvement in the rehabilitation processes [41]. This approach is ethically appropriate because MA users are considered a vulnerable group, and they may find it difficult to discuss their personal and emotional aspects with researchers they are meeting for the first time. Their close connection and holistic view of MA users' challenges offer valuable insights into users' perceptions, enabling discussion on how different inclusivity-oriented interventions impact PI. Accordingly, the inclusion criteria were: 1) qualification as a registered physiotherapist, 2) having work experience of over 5 years in either the private sector or hospital physiotherapy wards, and 3) willingness to participate voluntarily. Participants were excluded if they were involved in concurrent studies on the engineering and ergonomics of MA development, which focus on direct user-wheelchair interaction and could influence responses regarding inclusivity in using WUs. Employing a mix of purposive and snowball sampling, 12 physiotherapists with extensive experience in treating MA users agreed to participate in the interviews. The interviewers had no prior acquaintance with the participants. Table 1 outlines the characteristics of the participants.
2.5. Data Collection
The primary interviewer coordinated the time and location of the interviews with participants a day in advance. Subsequently, detailed interviews, lasting 50-90 minutes, took place between March 2022 and February 2023 in participants' private clinics and public hospitals (physiotherapy wards) in the cities of Kordkoy and Tehran, Iran. After obtaining written consent and signed confidentiality forms, interviews were recorded digitally, transcribed, and anonymized. The interviews followed a semi-structured IDIs outline, adjusted as necessary based on participants' responses. The IDIs included both general and specific questions about how individuals perceive inclusivity when using MAs. A calm environment was maintained to ensure participants felt at ease to respond to questions. Participants were given adequate time for responses, and discussions continued until data saturation was reached. The study followed the Consolidated Criteria for Reporting Qualitative Research checklists (COREQ) [42]. In English, some of the key semi-structured interview questions were:
- Broad questions (e.g., experiences, definition of disability, etc.).
- What is your thought on the adjustment of environments and MAs for clients’ needs? And how might they be improved?
- How do clients perceive their bodies and disability? How do they compare their body before and after disability challenge?
- How do clients see their MAs and environment? Are there any mismatches between their expectations and the existing situation?
- How can the technology influence the client's decision to accept or refuse a prescribed MA?
- How do clients feel about social activities and participation? How do culture and social context affect their perceptions?
- How do clients deal with potential social challenges? And what they do to improve their social participation?
2.6. Data Analysis
Within 48 hours post-interview, audio recordings were meticulously transcribed into text. All interviews, conducted in Persian, were translated into English and anonymously reviewed by two authors. Following transcription and initial verification, a structured analysis of the interview data was carried out using Braun and Clark's six-phased inductive thematic analysis framework [43]. This methodological approach involves sequential stages, including data familiarization, generation of preliminary codes, thematic identification, theme review, defining and naming the themes, and producing a report [44]. Transcripts were inputted into the Nvivo 12 software for coding the data, and the initial codebook was drafted. To enhance the credibility of the data analysis, the transcriptions were reviewed with participants to confirm the accuracy of their ideas and the responses. Two coders independently conducted parallel coding, followed by discussions to reconcile any differences in coding decisions. After coding was complete, the authors employed semantic and latent data interpretation strategies to identify broader themes [45]. This involved collating, sorting, and searching for repetitions, similarities, differences, and missing information within the coded excerpts. Finally, the relevant quotes were selected, and findings were reported in accordance with our research question. In this study "clients" reflects the participants' language, so "clients," " MA users," and "users" are used interchangeably.
2.7. Ethics
Ethical approval was granted by the Human Research Ethics Committee (Certification Number: 30016116). Participants were briefed on the study objectives, provided written consent, and had the option to withdraw at any time.
3. Results
Authors initially established and agreed upon 72 codes that clustered into 10 groups. In the next step, six themes and nine sub-themes were identified, which were later refined to four themes and six sub-themes through discussion. As this study represents the perspectives of MA users in Iran, more quotes are provided to illustrate their PI. After refining and reviewing codes and themes, the PI among MA users is reflected in four main themes:
- 1.
- Perceived Financial Value: Assessing Worth
- 8.
- Objective Enhancements: Optimizing Environments and MAs (Technological and ergonomics optimization in MAs; Enhancement of accessibility in private and public settings).
- 9.
- Subjective Enhancements: Trustworthiness, Support, and Hope (Fear and shyness in the usage of MAs in public settings; Desire for empathy from family and physiotherapists).
- 10.
- Contextual Factors: Interpretations and Representations (Causes of disability and inclusivity perceptions; Lack of aesthetic polish in MA design)
3.1. Theme 1: Perceived Financial Value: Assessing Worth
This theme primarily addresses the significance of valuing MAs. Participants noted that while standard MAs are generally not expensive, some users think that their quality does not justify the cost (Table 2; Q1, 2, and 3). Particularly, those clients desiring a high-quality wheelchair or customized orthosis find them unaffordable, thus settling for basic models lacking specialized features (Table 2; Q4). In this situation, MA users feel nobody understands their situation (Table 2; Q5). MA users here perceive exclusivity as a denial of their fundamental right to movement, exacerbated by the necessity to pay extra for their basic rights (Table 2; Q6). Three highly experienced participants noted that the economic context can influence the behavior of both MA users (Table 2; Q4) and producers as well. They highlighted that many companies prioritize financial gains over quality when producing MAs (Table 2; Q7). Alternatively, if users cannot afford commercially available MAs, they may opt to create their own solutions for mobility (e.g., handmade walkers or crutches) (Table 2; Q8).
3.2. Theme 2: Objective Enhancements: Optimizing Environments and Mas
This theme involves objective and tangible elements, which means that addressing these factors through engineering and technical considerations would impact their PI. Participants cited specific challenges where environmental adjustments, such as ramps or elevators, were lacking, thereby hindering accessibility (Table 3; Q13). This situation often led to feelings of anger, being overlooked and excluded in terms of ease of movement and maneuverability (Table 3; Q14, Q15). Moreover, participants highlighted the need for improved ergonomic quality in assistive products, as this would enhance comfort and reduce mismatches. This involves using higher quality materials, like softer pads for wheelchair seating, and incorporating relevant anthropometric data in product design to improve compatibility and comfort (Table 3; Q16-Q19). Ensuring the long-term functionality of the MAs was also highlighted, as participants reported instances of users expressing functional dissatisfaction. This situation often stemmed from mismatches in using the aids within indoor and outdoor spaces due to restricted movement, as well as discomfort from prolonged seating on the pad of the wheelchair or pressure on crutches (Table 3; Q20 and Q21). Participants also emphasized the significance of integrating new technologies into the design of MAs, which fosters acceptance and ongoing use of prescribed MAs (Table 3; Q22). Alongside the usability, the aesthetic of such mobility devices was highlighted which can affect the acceptance of MAs, specifically for youth (Table 3; Q22-Q24).
3.3. Theme 3: Subjective Enhancements: Trustworthiness, Support, and Hope
This theme involves the subjective and intangible elements, where MA users subconsciously and emotionally evaluate their environment and prescribed MAs. For instance, the trustworthiness factor encompasses aspects where users are dubious about the benefits, functionality, and even medical efficacy of MAs (Table 4; Q25). MA users may hesitate to fully rely on these aids due to concerns about stability and the probability of falling (Table 4; Q26). This uncertainty is highlighted, particularly when individuals fear the embarrassment of falling in public settings, leading to feelings of shame (Table 4; Q27). Participants stated that users perceive MAs as mere accessories rather than essential tools, further complicating their trust in these devices (Table 4; Q28). Participants noted that users typically adhere to physiotherapist instructions but may feel hopeless if they observe no progress in therapy sessions. In this situation, they seek continuous support from their families and physiotherapists as a reliable source of support and hope (Table 4; Q29, 30). Participants also conveyed MA users’ concerns about burdening their families, evoking feelings of guilt (Table 4; Q31). MA users sometimes feel they are not contributing to their community, which leads to disappointment about their future health prospects. (Table 4; Q32). Consequently, users may distance themselves from their physiotherapists or families, despite their persistent requests for progress updates on their recovery (Table 4; Q33). According to this theme, the perception of exclusion is reflected in their emotions and internal dialogue, shaping their overall perspective on disability.
3.4. Theme 4: Contextual Factors: Interpretations and Representations
This theme explores the symbolic significance and representation of MAs and users' bodies in public spaces. Within this theme, the social context and the cause of disability, influence how disability is perceived and depicted in society at large (Table 5; Q34, 35). For instance, mobility disability from war injuries, like those from the Holy Defense1 in Iran, is often seen as heroic. In contrast, disability resulting from theft-related incidents is frequently stigmatized and accompanied by guilt. (Table 5; Q36). Generally, users may resist using MAs due to stigma (Table 5; Q37). Dissatisfaction grows when they recognize the devices' limitations in functionality for health and mobility (Table 4; Q28). In response, physiotherapists play a pivotal role in promoting continued use by emphasizing the MAs' potential to enhance movement function (Table 3; Q15, Table 5; Q38). In social context, individuals with disabilities often face negative treatment, comments, and social pressures in public environments (Table 3; Q14, Table 4; Q27). Culturally, there is a tendency to underestimate individuals with physical disabilities (Table 7; Q39). Using MAs are often seen as a sign of failing to manage daily routines, which can label users as disabled. This perception exacerbates social pressure, especially when faced with public spatial challenges and accessibility issues, such as in public transport systems (Table 4; Q27). Under this social context, individuals experience fatigue and disinterest in social interactions (Table 5; Q40). According to this theme, the PI stems from their appraisal of social presumptions, and symbolic representation of disability, affecting their social interactions. In this regard, aesthetic consideration of MAs can remarkably affect their social symbolic representations (Table 4; Q24).
4. Discussion
In this section, each theme is interpreted, and the scope and connections with other themes or subthemes are discussed. Additionally, three levels of the DARE framework outline each theme's position. These four interconnected themes can serve as a guideline to enhance PI among MA users.
Theme 1 discusses the financial constraints related to the MAs, limiting access to basic assistive devices. This may prompt physiotherapists to seek alternatives or delay rehabilitation, potentially worsening the clients’ (patients) condition [47,48]. Consequently, more expensive treatments, like surgery, may be needed [49]. Financial limitations can even lead individuals to opt for second-hand MAs, which often lack proper anthropometric fit. This issue is exacerbated in the economic context of Iran, where inflation has significantly increased the prices of assistive devices, including imported ones, causing wheelchair prices to at least triple [50]. This concern extends globally, as international reports indicate that only 5–35% of the 80 million individuals worldwide in need of a wheelchair have access to one, mainly due to high costs that vary by country [51]. This issue is aligned with concerns raised by critics regarding commercialism in modern medicine [52,53].
While interviews imply conventional MAs are affordable (Table 1; Q1), from an inclusivity standpoint, the issue is not solely cost-related; it is about perceived dissatisfaction with the fundamental right of mobility. Users perceive MAs for mobility as an added financial burden, not just a cost issue. Thus, the dissatisfaction arises not from the cost but from having to pay for a right. This gap between their mobility rights and the financial hurdle in accessing MAs is perceived as inadequate inclusivity. Additionally, for those seeking advanced powered wheelchairs with features like stair climbing, costs can be higher, further enhancing feelings of exclusion. These costs can reduce individuals’ access to proper MAs and the opportunities to engage in social activities [54]. This highlights a gap in the first level of inclusivity according to the DARE framework, where MA users are still unsatisfied with the insufficiency of market-driven policies and efforts by the government and industry to meet their needs [20]. To this end, advocating increased governmental support for MA users and related services is recommended [32], aligning with recent proposals such as the Rehabilitation Policy Action Framework in Europe [54]. This framework outlines 48 options across six domains to translate political aspirations into actionable outcomes. This framework highlights reallocating healthcare funds for expanded rehabilitation resources, enhancing PI in theme 1.
Theme 2 shows that user objectively evaluate the design features of MAs and environmental accessibility, continuously thinking of optimization suggestions. According to the DARE framework's L1, users are aware of the efforts to include their needs but often notice mismatches between their needs and the design of MAs [20]. To this end, in cases of minor mismatches, they often try to find alternative solutions (e.g., using a padding to relieve pressure). But if mismatches escalate, it may lead to negative reactions and discontinued MA use, feeling their mobility needs cannot be met by MAs. According to previous studies, conventional wheelchairs inadequately address users’ needs both at home and in public spaces [55]. Also, the lack of anthropometric and ergonomic adjustments causes discomfort, affecting inclusivity [56]. In our study, participants also emphasized enhancing technology usability in MAs as a symbol of advancement. In other words, beyond enhancing usability, this aspect highlights the positive impact of technology on users’ psychological and social needs, as noted in previous studies [57]. However, in one of the recent studies, MA users noted that assistive technologies could simultaneously attract stigma from others [21]. Therefore, we must examine which features, either technological or appearance, of these MAs can evoke positive emotions and reduce stigma. The same pattern of dissatisfaction can occur in public environments or transportation when MA users experience disruptions to their routines. Elevated levels of environmental mismatch can contribute to negative stereotypes and condescending emotional responses [58] and even affect their social participation [1,59]. Disabled individuals, like all users, have the right to be considered in building and function planning [32]. To this end, Europe's Design for All (DfA) and Singapore's Barrier-Free Accessibility (BFA) program suggested promoting a social model of disability [33,60,61]. These initiatives advocate for barrier-free design in products, services, and environments to accommodate all abilities and socioeconomic situations.
According to DARE, Theme 2 initially addresses MA users’ tangible needs, corresponding to accessibility (L1). However, neglecting these needs may lead to impacting MA users psychologically, extending to L2 [20].
Theme 3 emphasizes the trustworthiness of MAs and space of usage, which may lead to caution and uncertainty for MA users in unfamiliar public settings. To overcome this hesitation, clients seek continuous confirmation of MA reliability, relying on physiotherapists' opinions and empathy to address mismatches between their internal needs and their environment. This affects MA users' feeling of having support and promotes their positive mental state [62]. This aligns with previous studies highlighting the significance of trust in patient care [63], which can also enhance treatment effectiveness [64]. Physiotherapists, in their role as trusted practitioners, can serve as catalysts in shaping users’ perceptions and persuading the acceptance of MAs. In addition, all design aspects of products and environments should promote a sense of trustworthiness for MA users, fostering their psychological comfort [65]. Research on trust in healthcare is expanding, encompassing empirical and conceptual investigations [65,66], as well as studies on communication [67] and service [48] in healthcare settings.
Emphasizing on trustworthiness in MA design is also important, as it directly influences users throughout the rehabilitation and affects their perception of the prescribed MA. If MAs are perceived as structurally fragile, users may hesitate to use them due to a lack of trust. Consequently, establishing trust, both from physiotherapists and within the environment, can alleviate doubts regarding disability. Accordingly, Theme 3 highlights the importance of validating users experiences across MAs—products, environment, and social support domains by empathizing with them [20], emphasizing the significance of enhancing interventions at L2 in DARE.
Theme 4 reveals how sociocultural context and disability etiology shape users’ perceptions of MAs inclusivity. This aligns with prior research, which show that social context influences how MAs are interpreted [21,22]. However, since the PI is considered a dynamic process [34], we expect perceptions and emotional responses to MAs to change over time for users [68].
On the other aspect, people's awareness of the etiology of disability within a social context can also influence the perception of disability and its representation with MAs in public settings. For instance, in war-related contexts, MA symbolizes heroism, with users embodying societal values, while, in theft incidents, those MAs can carry stigma and guilt, leading users to hide their disability or avoid using MAs. While prior studies have discussed the societal role [10,22,69], none have specifically addressed the etiology of disability, affecting the perceptions of and reactions toward MAs. In this context, regardless of how users of MAs perceive themselves (i.e., heroes or stigmatized), bystanders unaware of MA users' backstories may still view MAs through the lens of the prevailing discourse on disability [70]. For a bystander, here, the appearance of MAs is the only factor that serves as a primary medium for conveying stereotypes associated with mobility disability. Hence, MAs' aesthetics is a key factor that works as a language of the product [71], influencing the symbolic meaning of disability, evoking emotions in MA users, and impacting bystanders' impressions [72,73]. This creates a reciprocal relationship between the aesthetics of MAs and the social context, influencing both symbolic perceptions and real-world interactions [74]. We recommend incorporating elements of social refinement into the design of MAs by prioritizing power and agility concepts. This helps prevent the reinforcing positive feedback loop, where growing isolation and negative self-perception feed into each other. For instance, emphasizing external surfaces in wheelchairs with a futuristic style offers an opportunity to prioritize aesthetics over the traditional form-follows-function approach commonly seen in MAs [18]. We posit that addressing the symbolic and aesthetic aspects of MAs can indirectly but strongly influence users’ PI, as evidenced by prior research [75]. Future studies should explore how to translate emotional aspects into physical attributes of MAs.
At L2 of the DARE framework, we empathize with users' social experiences and understand how MAs’ appearance affects their interactions. By avoiding negative representations, we can foster enjoyment, enabling users to engage with their environment freely, without encountering negative perceptions (L3) [20]. Hence, Theme 4 aligns with the interventions of L2 and L3 in the DARE framework.
4.1. Limitations and Future Studies
Ethical constraints prevented us from interviewing individuals with disabilities during their recovery process. While our study focused on experiences of physiotherapists, their perspectives may not fully reflect MA users’ inner dialogues. Thus, future studies should involve both physiotherapists and active MA users for data collection. In this study, our access was limited to tracking the PI in MA use over time. Consequently, we suggest conducting longitudinal studies in future research to track the PI at each stage of rehabilitation. This study lacks practical inclusive design recommendations. Future research in design fields should focus on translating themes into actionable design interventions and soliciting patient feedback to refine these approaches. Additionally, a systematic review can compare our findings with existing literature, contributing to the development of an inclusive design toolkit for specialists in disability and design for care.
5. Conclusion
In this study, we identified four interconnected themes as a guideline for improving the PI: 1) Perceived Financial Value: Assessing Worth, 2) Objective Enhancements: Optimizing Environments and MAs, 3) Subjective Enhancements: Trustworthiness, Support, and Hope, and 4) Contextual Factors: Interpretations and Representations. These intertwined themes influence one another and ultimately shape the PI. Findings revealed that while the cost of MAs may not be a significant concern, users perceive it as exclusionary when they must pay for something considered a basic right for all. This aspect has been relatively overlooked in existing literature. Also, applying high-tech elements in MAs, beyond enhancing usability, can evoke positive emotions and relieve negative reactions like frustration, guilt, sadness, and shame. Theme 3 showed that fostering trustworthiness for MA users in physiotherapist interactions, environment, and design of MAs greatly enhances PI. We also justified how the context and cause of disability can indirectly influence users’ perception, utilization, and perpetuation of MAs. To this end, the aesthetic and symbolic representation of MAs in public spaces can influence the perception of social inclusion, a novel factor that has less been emphasized.
In terms of the DARE framework's inclusivity levels, Theme 1 revealed a gap in addressing accessibility, focusing on the L1. Theme 2 addressed the L1, but neglecting tangible aspects may extend a gap in the L2. Theme 3 highlighted trustworthiness and social support as catalysts, in enhancing PI, emphasizing the importance of interventions within L2. Furthermore, Theme 4 showed interventions in L2 and L3, where MA users' enjoyment is promoted by an empathetic understanding of their social experiences and avoidance of negative representations. In summary, our findings revealed substantial gaps across all three levels, with interconnected factors dynamically influencing PI. This shows that the DARE framework effectively justified and classified MA users' PI. We suggest that future studies incorporate the themes identified in this study into empirical research and offer feedback to optimize inclusivity for individuals using MAs.
Author Contributions
The authors confirm contribution to the paper as follows: Conceptualization, M.R.; methodology, M.R. and M.F.; software, M.R.; validation, M.R., C.C.; formal analysis, M.R. and M.F.; investigation, M.R. and M.F.; resources, M.R. and C.C.; data curation, M.R.; writing—original draft preparation, M.R. and C.C. and M.F.; writing—review and editing, M.R., C.C. and M.F.; visualization, M.R., and M.F.; supervision, C.C.; project administration, C.C.; funding acquisition, C.C. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Social Science and Humanities Research Council, grant numbers 100-001-824. May 2020-April 2024.
Institutional Review Board Statement
The study was conducted in accordance with the Concordia Research Ethics Committee and approved by the Concordia University's Ethical Review of Human Subject Research policy (protocol code 30016116, February 18, 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the authors.
Acknowledgments
We would like to thank the Mani Physiotherapy Center, Novin Physiotherapy Clinic, and all participants for their invaluable assistance during participant interviews.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Desai, R.H.; Hollingsworth, H.; Stark, S.; Putnam, M.; Eyler, A.; Wehmeier, A.; Morgan, K. Social Participation of Adults Aging with Long-Term Physical Disabilities: A Cross-Sectional Study Investigating the Role of Transportation Mode and Urban vs Rural Living. Disability and Health Journal 2023, 16, 101503. [Google Scholar] [CrossRef] [PubMed]
- Harris, F.; Yang, H.-Y.; Sanford, J. Physical Environmental Barriers to Community Mobility in Older and Younger Wheelchair Users. 2015. [CrossRef]
- Chen, K.; Zhao, P.; Qin, K.; Kwan, M.-P.; Wang, N. Towards Healthcare Access Equality: Understanding Spatial Accessibility to Healthcare Services for Wheelchair Users. Computers, Environment and Urban Systems 2024, 108, 102069. [Google Scholar] [CrossRef]
- Unsworth, C.A.; Rawat, V.; Sullivan, J.; Tay, R.; Naweed, A.; Gudimetla, P. “I’m Very Visible but Seldom Seen”: Consumer Choice and Use of Mobility Aids on Public Transport. Disability and Rehabilitation: Assistive Technology 2017, 14, 122–132. [Google Scholar] [CrossRef] [PubMed]
- Barker, D.J.; Reid, D.; Cott, C. The Experience of Senior Stroke Survivors: Factors in Community Participation among Wheelchair Users. Can J Occup Ther 2006, 73, 18–25. [Google Scholar] [CrossRef]
- Herrera-Saray, P.; Peláez-Ballestas, I.; Ramos-Lira, L.; Sánchez-Monroy, D.; Burgos-Vargas, R. Usage Problems and Social Barriers Faced by Persons with a Wheelchair and Other Aids. Qualitative Study from the Ergonomics Perspective in Persons Disabled by Rheumatoid Arthritis and Other Conditions. Reumatol Clin 2013, 9, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Park, G.-R.; Namkung, E.H. The Link between Disability and Social Participation Revisited: Heterogeneity by Type of Social Participation and by Socioeconomic Status. Disability and Health Journal 2024, 17, 101543. [Google Scholar] [CrossRef] [PubMed]
- Oishi, M.M.K.; Mitchell, I.M.; Loos, H.F.M.V. der Design and Use of Assistive Technology: Social, Technical, Ethical, and Economic Challenges; Springer New York, 2010; ISBN 978-1-4419-7030-5.
- Barlew, L.; Secrest, J.; Guo, Z.; Fell, N.; Haban, G. The Experience of Being Grounded: A Phenomenological Study of Living with a Wheelchair. Rehabilitation Nursing Journal 2013, 38, 193. [Google Scholar] [CrossRef] [PubMed]
- Costa, V. de S.P.; Melo, M.R.A.C.; Garanhani, M.L.; Fujisawa, D.S. Social Representations of the Wheelchair for People with Spinal Cord Injury. Rev. Latino-Am. Enfermagem 2010, 18, 755–762. [Google Scholar] [CrossRef] [PubMed]
- Edberg, A.-K.; Persson, D. The Experience of Active Wheelchair Provision and Aspects of Importance Concerning the Wheelchair Among Experienced Users in Sweden. 2011.
- Barker, D.J.; Reid, D.; Cott, C. Acceptance and Meanings of Wheelchair Use in Senior Stroke Survivors. The American Journal of Occupational Therapy 2004, 58, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Emerson, E.; Fortune, N.; Llewellyn, G.; Stancliffe, R. Loneliness, Social Support, Social Isolation and Wellbeing among Working Age Adults with and without Disability: Cross-Sectional Study. Disabil Health J 2021, 14, 100965. [Google Scholar] [CrossRef] [PubMed]
- Lidwell, W.; Holden, K.; Butler, J. Universal Principles of Design: 125 Ways to Enhance Usability, Influence Perception, Increase Appeal, Make Better Design Decisions, and Teach through Design; [25 Additional Design Principles]; rev. and updated.; Rockport Publ: Beverly, Mass, 2010; ISBN 978-1-59253-587-3.
- Rousseau-Harrison, K.; Rochette, A.; Routhier, F.; Dessureault, D.; Thibault, F.; Cote, O. Perceived Impacts of a First Wheelchair on Social Participation. Disability and Rehabilitation: Assistive Technology 2012, 7, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Newell, A. Inclusive Design or Assistive Technology. In Inclusive Design: Design for the Whole Population; Clarkson, J., Keates, S., Coleman, R., Lebbon, C., Eds.; Springer: London, 2003; pp. 172–181 ISBN 978-1-4471-0001-0.
- Yaldiz, N.; Agarwal, H.; Chakrabarti, A. Assessment of Inclusivity in a Product Life Cycle. In Proceedings of the Design in the Era of Industry 4.0, Volume 2; Chakrabarti, A., Singh, V., Eds.; Springer Nature: Singapore, 2023; pp. 747–760.
- Product Experience; Schifferstein, H.N.J., Hekkert, P., Eds.; 1st edition.; Elsevier Science: San Diego, CA, 2007; ISBN 978-0-08-045089-6.
- Heylighen, A.; Van der Linden, V.; Van Steenwinkel, I. Ten Questions Concerning Inclusive Design of the Built Environment. Building and Environment 2017, 114, 507–517. [Google Scholar] [CrossRef]
- Patrick, V.M.; Hollenbeck, C.R. Designing for All: Consumer Response to Inclusive Design. Journal of Consumer Psychology 2021, 31, 360–381. [Google Scholar] [CrossRef]
- Barbareschi, G.; Carew, M.T.; Johnson, E.A.; Kopi, N.; Holloway, C. “When They See a Wheelchair, They’ve Not Even Seen Me”—Factors Shaping the Experience of Disability Stigma and Discrimination in Kenya. Int J Environ Res Public Health 2021, 18, 4272. [Google Scholar] [CrossRef] [PubMed]
- Grue, J. The Social Meaning of Disability: A Reflection on Categorisation, Stigma and Identity. Sociology of Health & Illness 2016, 38, 957–964. [Google Scholar] [CrossRef]
- Human Right Watch “I Am Equally Human”. Available online: https://www.hrw.org/report/2018/06/27/i-am-equally-human/discrimination-and-lack-accessibility-people-disabilities-iran (accessed on 2 August 2024).
- Sahoo, S.K.; Choudhury, B.B. Wheelchair Accessibility: Bridging the Gap to Equality and Inclusion. Decision Making Advances 2023, 1, 63–85. [Google Scholar] [CrossRef]
- Perangin-Angin, R.; Tavakoli, R.; Kusumo, C. Inclusive Tourism: The Experiences and Expectations of Indonesian Wheelchair Tourists in Nature Tourism. Tourism Recreation Research 2023, 48, 955–968. [Google Scholar] [CrossRef]
- Physiopedia Assistive Devices. Available online: https://www.physio-pedia.com/Assistive_Devices (accessed on 9 February 2024).
- UNICEF, WHO. Assistive Technology for Children with Disabilities: Creating Opportunities for Education, Inclusion and Participation 2015 2018.
- Hossen Sajib, S. Identifying Barriers to the Public Transport Accessibility for Disabled People in Dhaka: A Qualitative Analysis. Transactions on Transport Sciences 2022, 13, 5–16. [Google Scholar] [CrossRef]
- Widehammar, C.; Lidström, H.; Hermansson, L. Environmental Barriers to Participation and Facilitators for Use of Three Types of Assistive Technology Devices. Assistive Technology 2019, 31, 68–76. [Google Scholar] [CrossRef]
- Basiri, A. Inclusivity and Diversity of Navigation Services. The Journal of Navigation 2021, 74, 269–272. [Google Scholar] [CrossRef]
- Basiri, A. Open Area Path Finding to Improve Wheelchair Navigation 2020.
- Bodaghi, N.B.; Zainab, A.N. Accessibility and Facilities for the Disabled in Public and University Library Buildings in Iran. Information Development 2013, 29, 241–250. [Google Scholar] [CrossRef]
- Vice, J.; Barstow, B.A.; Bowman, S.; Mehta, T.; Padalabalanarayanan, S. Effectiveness of the International Symbol of Access and Inclusivity of Other Disability Groups. Disability and Health Journal 2020, 13, 100836. [Google Scholar] [CrossRef] [PubMed]
- Holmes, K.; Maeda, J. Mismatch: How Inclusion Shapes Design; Reprint Edition.; The MIT Press: Cambridge, Massachusetts ; London, England, 2020; ISBN 978-0-262-53948-7.
- Turk, M.A.; Mitra, M. The Evolution of Disability and Health Research and Practice. Disability and Health Journal 2023, 16, 101450. [Google Scholar] [CrossRef] [PubMed]
- Tracy, S.J. Qualitative Research Methods: Collecting Evidence, Crafting Analysis, Communicating Impact; John Wiley & Sons, 2013; ISBN 978-1-4051-9202-6.
- Nussbaumer, L.L. Inclusive Design: A Universal Need; 1st edition.; Fairchild Books: New York : London, 2011; ISBN 978-1-56367-921-6. [Google Scholar]
- Jamshed, S. Qualitative Research Method-Interviewing and Observation. J Basic Clin Pharm 2014, 5, 87–88. [Google Scholar] [CrossRef] [PubMed]
- Longhurst, R. Interviews: In-Depth, Semi-Structured. In International Encyclopedia of Human Geography; Kitchin, R., Thrift, N., Eds.; Elsevier: Oxford, 2009; pp. 580–584. ISBN 978-0-08-044910-4. [Google Scholar]
- Pohlmeyer, A.E. How Design Can (Not) Support Human Flourishing. In Positive Psychology Interventions in Practice; Proctor, C., Ed.; Springer International Publishing: Cham, 2017; pp. 235–255. ISBN 978-3-319-51787-2. [Google Scholar]
- Chartered Society Of Physiotherapy Disabled, Not Defeated. Available online: https://www.csp.org.uk/frontline/article/disabled-not-defeated (accessed on 9 February 2024).
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated Criteria for Reporting Qualitative Research (COREQ): A 32-Item Checklist for Interviews and Focus Groups. International Journal for Quality in Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Thematic Analysis. In APA handbook of research methods in psychology, Vol 2: Research designs: Quantitative, qualitative, neuropsychological, and biological; APA handbooks in psychology®; American Psychological Association: Washington, DC, US, 2012; pp. 57–71. ISBN 978-1-4338-1005-3. [Google Scholar]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qualitative Research in Psychology 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Conceptual and Design Thinking for Thematic Analysis. Qualitative Psychology 2022, 9, 3–26. [Google Scholar] [CrossRef]
- UChicago Library The Holy Defense - The Graphics of Revolution and War - The University of Chicago Library. Available online: https://www.lib.uchicago.edu/collex/exhibits/graphics-revolution-and-war-iranian-poster-arts/holy-defense/ (accessed on 8 April 2024).
- Colizzi, M.; Lasalvia, A.; Ruggeri, M. Prevention and Early Intervention in Youth Mental Health: Is It Time for a Multidisciplinary and Trans-Diagnostic Model for Care? International Journal of Mental Health Systems 2020, 14, 23. [Google Scholar] [CrossRef] [PubMed]
- Rasoulivalajoozi, M.; Touir, G. Spinal Fusion Surgery for High-Risk Patients: A Review of Hospitals Information. Social Determinants of Health 2023, 9, 1–12. [Google Scholar] [CrossRef]
- Boden, I.; Robertson, I.K.; Neil, A.; Reeve, J.; Palmer, A.J.; Skinner, E.H.; Browning, L.; Anderson, L.; Hill, C.; Story, D.; et al. Preoperative Physiotherapy Is Cost-Effective for Preventing Pulmonary Complications after Major Abdominal Surgery: A Health Economic Analysis of a Multicentre Randomised Trial. Journal of Physiotherapy 2020, 66, 180–187. [Google Scholar] [CrossRef] [PubMed]
- EtemadOnline The price of a wheelchair has increased at least 3 times / 56% of disabled people in Tehran receive a pension. Available online: https://shorturl.at/coCXY (accessed on 5 May 2024).
- WHO-Asssitive Assistive Technology. Available online: https://www.who.int/news-room/fact-sheets/detail/assistive-technology (accessed on 4 January 2022).
- White, K. An Introduction to the Sociology of Health and Illness; SAGE Publications: London ; Thousand Oaks, Calif, 2002; ISBN 978-0-7619-6399-8.
- Matin, P. Introductionn of Medical Annthropology; 1st ed.; Farhameh: Tehran, 2021; ISBN 978-600-94057-1-8.
- Skempes, D.; Kiekens, C.; Malmivaara, A.; Michail, X.; Bickenbach, J.; Stucki, G. Supporting Government Policies to Embed and Expand Rehabilitation in Health Systems in Europe: A Framework for Action. Health Policy 2022, 126, 158–172. [Google Scholar] [CrossRef] [PubMed]
- Kapsalis, E.; Jaeger, N.; Hale, J. Disabled-by-Design: Effects of Inaccessible Urban Public Spaces on Users of Mobility Assistive Devices – a Systematic Review. Disability and Rehabilitation: Assistive Technology 2022, 0, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Mohebbi, V.; Dianat, I.; Castellucci, H.I. Psychometric Properties of the Iranian Version of the Wheelchair Seating Discomfort Assessment Tool (WcS-DAT) – Section II: A Revised Two-Dimensional Structure of Comfort and Discomfort to Improve Inclusive Design Practice. Disability and Rehabilitation: Assistive Technology 2023, 19, 1351–1357. [Google Scholar] [CrossRef]
- Domingues, I.; Pinheiro, J.; Silveira, J.; Francisco, P.; Jutai, J.; Correia Martins, A. Psychosocial Impact of Powered Wheelchair, Users’ Satisfaction and Their Relation to Social Participation. Technologies 2019, 7, 73. [Google Scholar] [CrossRef]
- Soetemans, J.K.; Jackson, L.M. The Influence of Accessibility on Perceptions of People with Disabilities. Canadian Journal of Disability Studies 2021, 10, 185–206. [Google Scholar] [CrossRef]
- Sadeghzadeh, C. Disabled Push for a Better Life in Iran. BBC News 2015.
- EIDD European Institute for Design and Disability in Stockholm, EIDD Stockholm Declaration Of. Available online: https://dfaeurope.eu/what-is-dfa/dfa-documents/the-eidd-stockholm-declaration-2004/ (accessed on 22 July 2024).
- BCA Code on Accessibility in the Built Environment 2019.
- Andrade, C.C.; Devlin, A.S. Stress Reduction in the Hospital Room: Applying Ulrich’s Theory of Supportive Design. Journal of Environmental Psychology 2015, 41, 125–134. [Google Scholar] [CrossRef]
- Wade, A. Q & A: Reality Check. The Engineer 2020, 300, 30–31. [Google Scholar] [CrossRef]
- Goold, S.D. Trust, Distrust and Trustworthiness. J Gen Intern Med 2002, 17, 79–81. [Google Scholar] [CrossRef] [PubMed]
- Cucuzzella, C.; Rasoulivalajoozi, M.; Farzamfar, G. Spatial Experience of Cancer Inpatients in the Oncology Wards: A Qualitative Study in Visual Design Aspects. European Journal of Oncology Nursing 2024, 102552. [Google Scholar] [CrossRef] [PubMed]
- Douglass, T.; Calnan, M. Trust Matters for Doctors? Towards an Agenda for Research. Soc Theory Health 2016, 14, 393–413. [Google Scholar] [CrossRef]
- Sousa-Duarte, F.; Brown, P.; Mendes, A.M. Healthcare Professionals’ Trust in Patients: A Review of the Empirical and Theoretical Literatures. Sociology Compass 2020, 14, e12828. [Google Scholar] [CrossRef]
- Mokdad, M.; Mebarki, B.; Bouabdellah, L.; Mokdad, I. Emotional Responses of the Disabled Towards Wheelchairs. In Proceedings of the Advances in Affective and Pleasurable Design; Chung, W., Shin, C.S., Eds.; Springer International Publishing: Cham, 2018; pp. 86–96. [Google Scholar]
- Jutai, J.; Day, H. Psychosocial Impact of Assistive Devices Scale (PIADS). Technology and Disability 2002, 14, 107–111. [Google Scholar] [CrossRef]
- Shinohara, K.; Wobbrock, J.O. Self-Conscious or Self-Confident? A Diary Study Conceptualizing the Social Accessibility of Assistive Technology. ACM Trans. Access. Comput. 2016, 8, 5:1–5:31. [Google Scholar] [CrossRef]
- Hernández, R.J.; Cooper, R.; Tether, B.; Murphy, E. Design, the Language of Innovation: A Review of the Design Studies Literature. She Ji: The Journal of Design, Economics, and Innovation 2018, 4, 249–274. [Google Scholar] [CrossRef]
- Norman, D.A. Emotional Design: Why We Love (or Hate) Everyday Things; Basic Books, 2004; ISBN 978-0-465-05135-9.
- Shi, A.; Huo, F.; Hou, G. Effects of Design Aesthetics on the Perceived Value of a Product. Front. Psychol. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Interaction Design Foundation What Is Aesthetics? Available online: https://www.interaction-design.org/literature/topics/aesthetics (accessed on 28 July 2023).
- dos Santos, A.D.P.; Ferrari, A.L.M.; Medola, F.O.; Sandnes, F.E. Aesthetics and the Perceived Stigma of Assistive Technology for Visual Impairment. Disability and Rehabilitation: Assistive Technology 2022, 17, 152–158. [Google Scholar] [CrossRef] [PubMed]
| 1 | The Iran-Iraq
War was referred to as the "Imposed War" and the "Holy
Defense" in Iran due to its perception as a defensive struggle against
aggression [46]. |
Figure 1.
Procedure of Research Design.
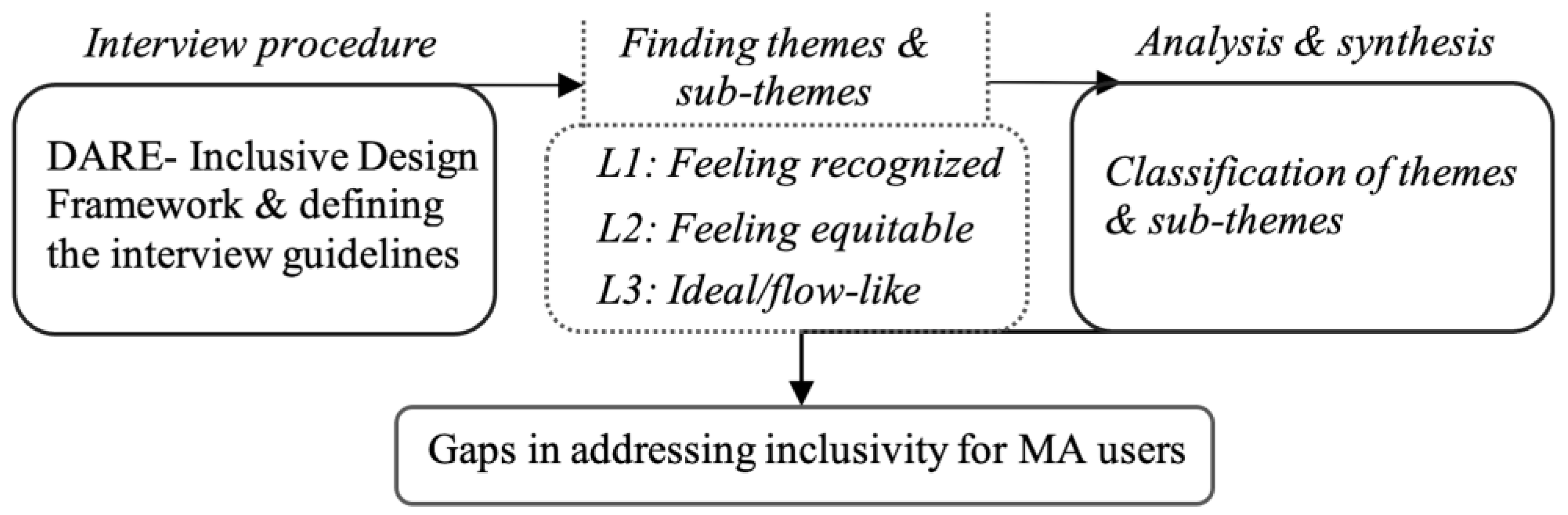

Table 1.
Background of participants and interview timing (N=12).
| Years of experiences | Interview time (Min) | Working experiences and profession category |
|---|---|---|
| *S=234, **A=18.14 (min-max:8-25) | S=840, A=70 (min-max:50-90) | Private clinic (N=4), health care centre (N=2), home visiting (N=1), state welfare organization (N=2) hospital (N=3), national medical committee of the Olympics (N=2). |
*S: Sum, **A: Average.
Table 2.
Participants supporting quotes on the theme 1.
| Quote (Q) # | Perceived Financial Value: Assessing Worth. |
|---|---|
| Q1 | Most assistive devices are affordable…However, if an orthosis were to be individually prepared by an orthotist during rehabilitation, it will certainly be more expensive for clients than mass-produced ones. |
| Q2 | …The economic factor is important in prescribing a solution [suggesting an MA].... It should not impose a financial burden on the individual…. A suitable price of MAs greatly influences the decision to accept or reject the product. |
| Q3 | The complaint was that the price we paid did not correspond to the period of use... I [user] paid a fee, but after a month of use, it is not washable, nor are the parts replaceable. This is a common complaint. |
| Q4 | …It is not fair for clients to endure fatigue or face potential tragedies just for not affording an orthosis…. Eventually, they have no choice but to accept the basic and inexpensive models of MAs. |
| Q5 | In developing societies where there is economic fluctuation, the clients often say: You've never been in my shoes to understand the financial strain it puts on me…. |
| Q6 | …It is difficult to pay for something that you didn't need to pay for before [mobility]. They [clients] often compare their current situation to their past. |
| Q7 | Producers' recommendations for user-friendliness are often related to their profit motives rather than focusing on research on users, development, and improving clients' health…. |
| Q8 | In a society like Afghanistan [A neighbouring country of Iran], or impoverished cities within Iran, despite a weak economy and poverty, people sometimes address their needs with minimal resources, such as wooden handmade canes, which are locally crafted. |
Table 3.
Participants supporting quotes on theme 2.
| Quote (Q) # | Objective Enhancements: Optimizing Environments and MAs |
|---|---|
| Q13 | The whole city can be a ground for constant complaints from disabled individuals…. Despite employing fanciest architectural style, like the fancy stairs, the slope is so steep that the wheelchair may overturn. |
| Q14 | …Being mindful of the environment for people with disabilities shows respect for their needs.... When users [MA users] see this effort, it boosts their self-confidence. But in places where nothing is set up for disabilities, everything seems to treat them (MA users) like a burden, leading to feelings of shame and helplessness that are seen on their faces. |
| Q15 | Their [clients] reaction is anger and finally yield and ask for help…. Our [physiotherapists] approach is moderating dissatisfaction or justifying shortcomings. |
| Q16 | In terms of anthropometry, there is limited variation in the sizing of these products [MAs] within our country [Iran]. Sizes are typically limited to small, medium, and large…. |
| Q17 | Ergonomics and environmental adaptation are important…. However, equipment from other countries may not always be suitable for the new environment [Iran]. |
| Q18 | It is very important to use a material that reduces the weight of the MAs. |
| Q19 | One of the factors is the lightness of the material…. The material used must be lightweight yet strong enough to carry the muscles and skeleton of the body. |
| Q20 | We need to have some devices [MAs] that show a sense of trust and functionality for a long time. …The feeling of relying on such device gives [to MA users] a peace of mind. |
| Q21 |
Sometimes the users complain about the long-time seating and lack of suitable structure of conventional wheelchairs with a sturdy material.…To reduce pressure, they add sponge foam padding. They complain so much that some refuse to use the product. They insist, asking if there's another way [for recovery]. |
| Q22 | Technology can have a significant impact, ranging from 20% to 40%. Especially for those who resist using MA [wheelchair]. |
| Q23 | The beauty of assistive products can influence MA users’ preference by 30-40%, which is significant for us [physiotherapists]. This is especially true for children and young people, where appearance matters a lot. |
| Q24 | Embellishments can motivate them to accept continued use over time. It may also affect their social interpretation…In my opinion, the best colors are vibrant and warm colors. There should be color variations and users' subconscious should like the color. The design of the work and clinic space should motivate people and do not remind them of their troubles. …We have to bring something into the clients' eyes that has a good effect on the patient's emotions. …The sense of touch is very important, for example, the roughness of the seat, and the coldness of the material should be taken into considerations. |
Table 4.
Participants supporting quotes on theme 3.
| Quote (Q) # | Subjective Aspects: Trustworthiness, Support, and Hope |
|---|---|
| Q25 | Sometimes they are unsure if relying on these devices will provide adequate support for movement. For example, they ask, "Is this device robust enough to carry me? |
| Q26 | …It [lack of trust to MAs] is rooted in their self-confidence. ...Timid individuals often try to hunch over and walk slowly and take great care. It is rooted in fear and anxiety. …Mental and psychological factors are very effective [in perception of the disability]. |
| Q27 | In an unsuitable environment, MAs can be perceived as an insult [for users], leading to feelings of shame and helplessness, like the sense of fear and shame after falling downstairs |
| Q28 | Once they are disappointed, they state it [MAs] is useless and consider it as a burden. That is why they may consider the MAs as an excessive gadget…. |
| Q29 | They are very open and receptive to the treatment process and respond: I will use whatever assistive device [MAs] you [physiotherapist] recommend. ...They continuously check their progressof rehabilitation. ...A trusting relationship with their doctor enhances clients' levels of hope. Sometimes clients trust their physiotherapists even more than their religious assumptions. |
| Q30 | Sometimes clients get nervous and depressed…they are upset with their own families and do not like to get help from them. They say: don't bother me. If the depression is severe and persistent, the patient may even contemplate suicide…. Without hope, they gradually face challenges and may engage in risky behaviors. |
| Q31 | Sometimes clients feel they have become a burden on their family. …For example, I have a client who feels embarrassed and ashamed when his wife and family bring him to physiotherapy. |
| Q32 | Regarding social participation, they feel shy and don't want to use assistive devices in public. |
| Q33 | Depression is a significant social challenge for them [clients]... If they believe they won't recover or regain a normal life, it leads to feelings of despair. ...When clients seem to have lost hope, they may refuse to cooperate with their physiotherapist. |
Table 5.
Participants supporting quotes on theme 4.
| Quote (Q) # | Contextual Factors: Interpretations and Representations |
|---|---|
| Q34 | They sigh. They believe that this [mobility disability] is a form of retribution and punishment for their past actions…. |
| Q35 | …Social, accessibility, and work environment issues, along with cultural differences, appearance [MAs] and clothing styles can affect the fit and perception of MAs, potentially exacerbating the patient's [clients] condition and reproducing the meaning of "I am a patient."… This interpretation [being dis/abled] may differ between rural areas, where disability is more associated with negative stereotypes, and the larger urban society. |
| Q36 |
Being socially perceived as a hero is different from being a fugitive or accused. Being [socially] accepted as someone whose fingers were cut off [according to religious law] for theft and someone whose finger is injured like Hans Brinker [Refers to Mary Mapes Dodge's novel about a boy who saves Amsterdam by plugging a dike leak with his finger] is very different. ...For instance, someone disabled due to an unsafe car or road often blames society and views themselves as a victim. …Owning a crutch or wheelchair from wartime, even if it's no longer necessary, serves as a heroic symbol for the individual–embodying qualities of courage, selflessness, and determination…. |
| Q37 | Products [MAs] should be designed to confer prestige rather than limitations…. |
| Q38 | …They [Clients] believe they're alone in their illness, unaware that others require assistance too…However, we can encourage them to persevere by offering support and empathy. |
| Q39 | [User] are most reluctant to use these devices due to societal negative attitudes and pity…. |
| Q40 | …The decline in individual independence, especially in social and financial areas, significantly affects clients' likelihood to use MAs. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



