
Submitted:
13 August 2024
Posted:
15 August 2024
You are already at the latest version
Abstract
Background and Aims: Sustained virologic response (SVR) lead to the decrease of portal hypertension, the regression of fibrosis, the improvement of the hepatic synthesis of procoagulant and anticoagulant factors. We aimed to assess the influence of SVR on coagulation parameters in HCV cirrhotic patients treated with DAAs. Methods: We performed a prospective study in the Institute of Gastroenterology and Hepatology Iasi, Romania, between January 2022 and February 2024. We included patients diagnosed with compensated and decompensated HCV-related liver cirrhosis, treated with direct antivirals (PrOD ± RBV or SOF/LED ± RBV) for 12/24 weeks. Blood samples for biochemical, immunological and coagulation tests were collected at baseline, EOT and SVR12/24. Results: We analyzed a group of 52 patients with HCV-related liver cirrhosis, predominantly female (68.0%), the degree of severity of cirrhosis placed the patients mainly in Child-Pugh classes B (40%) and C (36%). All patients achieved SVR. The MELD score decrease at EOT (13.48 ± 4.273; p =0.001), and SVR (9.88 ± 2.774; p = 0.000), compared to baseline (14.92 ± 4.707). Fibroscan values decreased at SVR (17.596 ± 3.7276; p = 0.000) compared to baseline (26.068 ± 7.0954). For all common coagulation parameters (platelets, INR, PT, fibrinogen, aPTT) there was a trend towards improvement during treatment, changes that were statistically significant for the majority of patients. Factor II low at baseline (75.40 ± 7.506), increases at EOT (87.40 ± 9.587), and later at SVR (99.12 ± 11.695; p = 0.000). FVIII values increased at baseline (175.52 ± 16.414) decrease at EOT (151.48 ± 13.703) and SVR (143.40 ± 13.937). FvW values decreased during treatment (146.84 ± 9.428 – baseline, 141.32 ± 9.690; p =0.000 – EOT, 126.68 ± 17.960 – SVR). In regards to the anticoagulant factors (PC, PS, ATIII), a significant improvement was brought on by SVR. Advanced stages of liver disease showed the most diminished FII activity, while at baseline and in Child-Pugh C patients we recorded the highest values of FVIII and FvW. Conclusions: Our study proved that the “reset” of the coagulopathy might be due to the improving of the liver function due to viral eradication secondary to AAD therapy.
Keywords:
coagulation parameters
; procoagulant factors
; anticoagulant factors
; chronic hepatitis C infection
; direct-acting antivirals therapy
; sustained virological response
; liver cirrhosis
1. Introduction
Achieving sustained virological response (SVR) has a significant impact on the natural course of liver disease related to chronic viral C infection. In numerous clinical studies, SVR has been shown to induce the regression of liver fibrosis, the improvement of liver synthesis and, implicitly, the reduction of portal hypertension, which are favorable outcomes in the disease’s progression, changes highlighted primarily in patients with mild or moderate fibrosis [1,2,3].
Another beneficial effect of the eradication of the C virus is brought on by the “reset” of the coagulopathy, an indirect effect that reveres the hypercoagulability status, associated with the cirrhotic patient, by modifying both the procoagulant and anticoagulant factors within close quarters of the normal parameters, thus significantly lowering the hemorrhagic or thrombotic complications [4,5].
It is already known that hemostasis in the cirrhotic patient presents some features of coagulation compared to physiological hemostasis, changes that result with the status of advanced liver disease [6]. Recent studies report that the hepatitis C virus (HCV) additionally influences coagulation status and may cause thrombotic or hemorrhagic complications to occur more frequently in patients with chronic HCV infection [7]. Inflammation at the vascular level together with altered coagulation secondary to HCV infection are elements that contribute to the increased risk of thromboembolic diseases [8]. On the other hand, thrombocytopenia and lower levels of clotting factors contribute to an increased risk of bleeding [9]. Thus, HCV infection is responsible for manifestations of both hypercoagulability and hypocoagulability [10].
Nielsen et al. are among the few researchers who have specifically investigated, in a prospective study, the hemostatic function of whole blood in patients with chronic HCV infection with varying degrees of liver fibrosis (absent, mild, advanced) treated and without antiviral treatment and the possible effects of viral replication on coagulation [11].
The effect of HCV viral replication on coagulation parameters was evaluated in the same prospective study involving patients treated with direct antivirals and SVR [11]. Minor changes in standard post-treatment coagulation parameters were found. Post antiviral treatment, the platelet count and fibrinogen parameters showed a partial “restoration” but at lower values than the control group. The same effect was noticed for the concentration of coagulation factors II – VII – X. Thus, the question arises as to whether the change in coagulation parameters in chronic HCV infection is only a result of viral replication or whether these changes are secondary to liver fibrosis that persists in patients even after SVR is obtained.
The impact of DAAs on coagulation parameters in patients with HCV-related liver cirrhosis is a controversial and intensely studied topic, the realm of which is still not fully explored. Among the first studies to evaluate coagulation parameters during DAAs treatment in patients with HCV infection was the one conducted by Tripodi et al. in 2017 [4], which investigated coagulation status in HCV-infected patients before, during, and after treatment using traditional global and individual coagulation tests, as well as using state-of-the-art methods, including thrombin generation with and without thrombomodulin, and thromboelastometry as a global method of coagulation status analysis. The authors of the study demonstrated in a prospective study the beneficial effect of DAAs on pro- and anticoagulant factors, by improving pro- and anticoagulant status; DAAs do not substantially alter their balance, but make them more stable and less likely to be disrupted as assumed before treatment [4].
Data from the literature show that obtaining SVR leads to improved hepatic synthesis of both procoagulant and anticoagulant factors and, implicitly, to a slow recovery of HCV-induced coagulopathy [4,5,12]. At the same time, recent studies have shown that obtaining SVR in patients with HCV-related liver cirrhosis was associated with improved MELD and Child-Pugh scores, which reflect improved hepatic synthesis function and implicitly, synthesis of coagulation factors [13,14,15,16,17,18,19,20,21].
The main objective of this study was to evaluate how coagulation parameters are influenced by the SVR obtained in patients with HCV cirrhosis, treated with AAD therapy and the correlation between the coagulation factors and liver cirrhosis severity.
2. Materials and Methods
2.1. Patients
We included patients diagnosed with compensated and decompensated HCV-related liver cirrhosis, randomly selected, who were eligible in accordance to the Ministry of Health criteria to be treated with with direct antivirals (Ombitasvir / Paritaprevir / Ritonavir + Dasabuvir ± Ribavirin or Sofosbuvir / Ledipasvir ± Ribavirin) for 12 / 24 weeks. The diagnosis of cirrhosis was based on clinical, biological and imaging data according to international guidelines.
The diagnosis of viral C infection was suspected by anti-HCV Ab positivity and confirmed by HCV-RNA, the detection limit being 15 IU/mL. Sustained virologic response was defined as an undetectable HCV-RNA level 12/24 weeks after completion of direct antiviral treatment. The study excluded patients with age less than 18 years, pregnant or breastfeeding women, patients with the human immunodeficiency virus defined by positive an-ti-HIV antibodies, liver cancer that does not have an indication for transplantation or that treated by ablation or resection at less than of 6 months after the procedure, or if there are CT/MRI signs of post-procedure tumor recurrence, patients with other extra-digestive neoplasms, with thrombophilia, with anticoagulant treatment, with chronic ethanol consumption or with drug contraindications for DAA therapy.
2.2. Study Protocol
We performed a prospective study in the Institute of Gastroenterology and Hepatology Iasi, Romania, between January 2022 and February 2024. We collected blood samples at 3 moments in time: at the initiation of antiviral treatment (baseline), at the end of antiviral treatment (EOT) and 12 weeks after completion of antiviral treatment (SVR12/24).
2.2.1. Laboratory Assessment
Blood samples for coagulation tests were collected from the antecubital vein. Two vacutainers of whole blood containing 1/10 volume of sodium citrate as anticoagulant were taken, each vacutainer having a capacity of 2.7 ml. Blood samples were centrifuged for 15 minutes at 2500xg/min, plasma was collected and stored in 0.5 ml devices and subsequently frozen at -80°C until examination. Processing of biological samples was performed after thawing the plasma at 37°C for 5 minutes. Biochemical measurements were performed from blood obtained on the same day of blood collection at the time of the medical visit.
2.2.2. Coagulation Profile Evaluation Tests
Prothrombin time, AP, INR, aPTT and fibrinogen were determined by the coagulometric method using an automatic analyzer according to the instructions (Sysmex CA – CA - 600). The activity of factors II and VIII was determined by the coagulometric method, with the help of an automatic analyzer (ACL TOP 750). The von Willebrand factor activity was performed by the immunoturbidimetric method, using the same analyzer (ACL TOP 750). Anticoagulant and chromogenic activity of AT III and protein C was determined using the automatic analyzer ACL TOP 750, and protein S was determined using the coagulometric method. Activity of all factors determined was performed using Bedford, MA 01730 - 2443 (USA) and Monza 338 - 20128 Milano (Italy) kits.
2.2. Evaluation of Liver Fibrosis
To asses liver fibrosis as part of our inquiry, we utilized the FibroScan® 520 compact model (Echosens, Paris, France) that comes with an M (normal) probe with a 3.5 MHz transducer frequency or XL (obese) probe with a 2.5 MHz transducer frequency. Patients were instructed to maintain a supine position with the right arm fully extended, after no less than 4 hours of fasting. At first, the M-probe was used for the investigation. However, if the distance between the liver capsule and the skin exceeded 25 mm, the XL probe was used. Reliable measurement was defined by 10 acquisitions within the cut off 30% for the interquartile interval. We defined mild fibrosis (F1) at a liver stiffness measurement over 5.6 kPa, significant fibrosis over 7.1 kPa (F2), advanced fibrosis over 9.5 kPa (F3) and cirrhosis over 12.5 kPa (F4).
2.4. Statistical Analysis
For the statistical analysis, Microsoft Excel and SPPS (Inc., Chicago, IL, version 28) were the programs used. There were 2 kinds of variables that occurred: categorical variables, which were identified in the form of absolute values and percentages, while continuous variables with normal distributions in the form of mean SD. The statistical equations and tests used were as follow: Chi-square for categorical data comparison, t-Student test for the arithmetic means of a parameter analyzed in two samples comparison, the Mann-Whitney U test for non-parametric tests and the Kolmogorov-Smirnov test in order to asses data distributions. The statistical significance of the results was illustrated by a p-value of 0.05.
2.5. Ethical Considerations
The ethical principles of the declaration of Helsinki were respected, with the study protocol being signed and explained in detail to all patients. Informed consent for study inclusion was obtained from all patients, thus agreeing to additional monitoring and blood sampling during antiviral treatment.
3. Results
3.1. General characteristics of the study population
We analyzed a group of 52 patients with HCV-related liver cirrhosis, predominantly female (68%), with an average age of 63.88 ± 9.387 years; the degree of severity of cirrhosis placed the patients mainly in Child-Pugh classes B (40%) and C (36%). All patients achieved SVR. None of the patients developed complications during the study period.
On average, the MELD score had the value of 14.92 ± 4.707, more than half of the patients (60%) having a MELD ≥ 15 compared to the others (40%). Most patients included in the study (76%) received treatment with LED/SOF, 15 patients (28%) also associated RBV and most patients – 37 (72%) were naïve to antiviral treatment (Table 1).
3.2. Evolution of virological parameters, liver function and the degree of liver fibrosis in the studied group
Undetectable HCV-RNA at EOT and SVR was achieved by all patients. The MELD score registered a statistically significant decrease at the EOT (13.48 ± 4.273; p = 0.001), and at the SVR an even more pronounced decrease is observed (9.88 ± 2.774; p = 0.000), compared to the initiation of antiviral treatment (14.92 ± 4.707). Fibroscan values were recorded only at the initiation of antiviral treatment and at the time of SVR where a statistically significant decrease was observed (17.596 ± 3.7276; p = 0.000) compared to the baseline value (26.068 ± 7.0954).
3.3. Evaluation of routine coagulation parameters in patients with HCV-related liver cirrhosis treated with DAAs and SVR
For all common coagulation parameters there was a trend towards improvement during antiviral treatment, changes that were statistically significant for the majority of patients included in the study.
In the studied group it was observed that the initial average value of platelets (103852.00 ± 62837.138) registered a statistically significant increase both at EOT (127125.00 ± 58090.868, p = 0.005) and at SVR (138160.00 ± 49819.407). The initial mean INR value (1.7220 ± 0.51522) decreased statistically significantly at EOT (1.4762 ± 0.40713; p = 0.001), and at the time of SVR the decreasing trend was maintained (1.3386 ± 0, 34864; p = 0.001). The initial mean value of PT (15.336 ± 3.3041) decreased statistically significantly both at EOT (14.505 ± 1.7142; p = 0.026) and at SVR (13.033 ± 1.8529; p = 0.001). Fibrinogen values also registered a statistically significant increase, constant over time, at baseline being 224.30 ± 96.803, at EOT - 297.35 ± 48.295 and at SVR reaching the average value of 328.68 ± 60.178. A similar trend of variation was also observed in the case of aPTT where a statistically significant decrease (p = 0.004) was found in the values at EOT (33.9519 ± 4.51637) and at SVR (31.1290 ± 5 .09690; p = 0.000) compared to the baseline value (36.760) (Figure 1).
Tr, platelets; INR, international normalized ratio; PT, prothrombin time; aPTT, activated partial thromboplastin time
3.4. Evaluation of procoagulant factors in patients with HCV-related liver cirrhosis treated with DAAs and SVR
When the AAD treatment was first started, blood tests showed that the activity for factor II was decreased and those of factor VIII and vW were increased. Characteristically of patients with liver cirrhosis, an increase in factor VIII is reported, which is also prevalent in the case of portal vein thrombosis.
In our study, at the initial time, the mean value of FII was low (75.40 ± 7.506), increasing with a statistically significance (p =0.000). At EOT, it reached the mean of 87.40 ± 9.587, followed by a maintained improvement at SVR, still remaining statistically significant, with a final mean FII of 99.12 ± 11.695 (p = 0.000).
At the same time, the FVIII values increased at the initiation of antiviral treatment (175.52 ± 16.414) decrease statistically significantly at the time of EOT (151.48 ± 13.703) and at SVR (143.40 ± 13.937).
A similar trend follows FvW, where a constant decrease in values is observed during antiviral treatment; at baseline a mean FvW value of 146.84 ± 9.428 was measured, which at EOT decreases statistically significantly (141.32 ± 9.690; p =0.000). At SVR, the final mean value of FvW (126.68 ± 17.960) further decreased statistically significantly (p =0.000) compared to the initial assessment (Figure 2).
3.5. Evaluation of anticoagulant factors in patients with HCV-related liver cirrhosis treated with DAAs and SVR
In our study all anticoagulant factors such as protein C, protein S and antithrombin III had low values at the initiation of antiviral therapy. This certifies the hemostatic imbalance, with the predisposition towards the occurrence of thrombotic accidents in the case of the cirrhotic patient. A significant improvement in values regarding the anticoagulant factors in patients with SVR was noted, similarly to the evolution of procoagulant factors.
The PC values increased statistically significantly (p = 0.000), from the initial evaluation (68.92 ± 8.411), to the EOT (86.24 ± 12.879), a phenomenon that is also observed at the SVR evaluation (95.84 ± 11,898).
PS values evolve in the same way, having a low mean value at the initiation of treatment (68.44 ± 3.163), increasing significantly statistically (p =0.000) at EOT (88.48 ± 15.951), accentuating its increase at the time of SVR, with the average value of PS reaching 95.64 ± 15.327 (p =0.000).
ATIII values increased steadily over time, in a manner also statistically significant (p =0.000). At the initial assessment the low mean value (77.64 ± 4.999) registered an increase at the EOT (90.00 ± 11.969), reaching a significant value at SVR (96.28 ± 11.778) (p = 0.000) (Figure 3).
3.6. Evaluation of the Relationship between the Severity of Liver Cirrhosis and Changes in Coagulation Factors
During the time allotted for the study, the evolution of coagulation factors in correlation to the liver damage severity from baseline, to EOT and finally SVR was investigated. The most advanced stages of liver disease showed the most diminished FII activity with no statistically significant differences between the three Child-Pugh classes during the follow-up period (Figure 4A). At the baseline of Child-Pugh class C patients we recorded the highest FVIII (Figure 4B) and FvW (Figure 4C) values.
Throughout the study, PC differences between Child classes showed statistical significance (p =0.001). Therefore, PC values were increased statistically significantly at the time of SVR compared to the initial assessment for all three severity classes; patients in Child-Pugh class C had the least increase in PC compared to patients in Child-Pugh classes A and B (Table 2A).
Similarly, protein S values showed the lowest values at the initial evaluation with statistical significance between the three classes in patients with Child-Pugh C (p =0.002). afterwards, PS values increased at the EOT assessment, by comparison to the initial values and showed no statistical significant difference between the three Child classes (p =0.665). At the SVR evaluation time, PS values continued to increase, again without statistical significance (p =0.781) between the three Child classes, with Child-Pugh C class patients having slightly lower mean PS values compared to the other patients (Table 2B).
Finally, the lowest ATIII values were observed at baseline, where a significant statistical difference between the patients in the Child classes was found (p =0.001). Thus, ATIII values were slightly higher in class A patients, whereas patients from class B and class C had statistically significantly lower ATIII values. At EOT the ATIII values increased slightly and became uniform between the three Child classes, the differences recorded being without statistical significance (p =0.438). The highest values were observed in patients of Child A, while patients of Child B and C had close values. ATIII values continued to increase also at the SVR assessment, where no statistically significant differences were recorded between the three Child classes (p =0.449). The highest values of ATIII were observed in patients of Child A class, the lowest values of ATIII were observed in patients of Child B class, patients of Child C class recording intermediate values, close to those of the Child A class patients (Figure 5).
4. Discussion
The natural course of HCV-related liver disease is significantly impacted by achieving sustained liver disease, due to the improvement in liver function that results from the direct antiviral therapy, effectively bringing the levels of coagulation factors within the normal range, causing a “reset” [5].
The present study showed that the viral eradication due to the AAD therapy improved liver function by bringing some of the coagulation factors within the normal range, thus bringing a resolution to the hypercoagulable state.
Among the first studies to evaluate coagulation parameters during DAA treatment in C virus-infected patients was that by Tripodi et al. in 2017, who demonstrated in a prospective study the beneficial effect of AAD on pro- and anticoagulant factors [4]. The authors investigated the coagulation status of HCV-infected patients before, during, and after treatment using traditional global and individual coagulation tests as well as state-of-the-art methods, including thrombin generation with and without thrombomodulin, whose role was previously shown to depict coagulation much more realistically than conventional tests. In addition, thromboelastometry was also used as a global method for analyzing the coagulation status, which graphically translates the entire process of clot formation and continues even after its formation with the evaluation of clot lysis and retraction - the fibrinolytic phase. Thus it was possible to analyze the viscoelastic characteristics of blood, properties already shown to be abnormal in cirrhotic patients. Prothrombin time, thrombin generation with or without thrombomodulin, thromboelastometry, as well as procoagulant (II, VIII, XIII, von Willebrand) and anticoagulant (antithrombin III and protein C) factors were analyzed.
In the present study, the investigated group consisted of patients with viral liver cirrhosis C, the majority being female (68%); the degree of severity of cirrhosis placed the patients mainly in Child-Pugh classes B and C, a fact that attests to the heterogeneity of the study group, which consisted of both compensated and decompensated cirrhotic, with an advanced degree of liver fibrosis.
Most of the patients included in the study, i.e., more than three quarters of them (76%), received treatment with LED/SOF, being the only one recommended and available at that time in our country for the treatment of patients with decompensated HCV or at the limit of hepatic decompensation.
MELD score values decreased significantly in EOT and SVR, data that are consistent with the results obtained in other studies that also demonstrated a significant decrease in liver parameters in patients with SVR [22]. On the other hand, Krassenburg LAP et al. showed that patients with Child-Pugh B/C cirrhosis had a moderate decrease in MELD score after AAD therapy [23]. In almost 20% of patients the decrease in MELD score was at least 2 points 12 weeks after the end of therapy. One of the largest studies including 409 patients with decompensated cirrhosis treated with AAD showed a mean ΔMELD 12 of - 0.85 compared with + 0.75 in untreated patients [24]. However, data from these studies showed no association between ΔMELD 12 and virologic response.
All patients included in the study had undetectable HCV RNA at EOT and SVR. The dramatic decrease in viremia after antiviral treatment also observed in this study is consistent with literature data [25] and demonstrates that we have included a cohort of patients that can be adapted to any population of cirrhotic patients with HCV infection candidates for antiviral treatment direct.
In this study, we inquired the dynamic changes over time of a wide range of coagulation parameters from the first presentation, at the EOT to the achievement of SVR. Traditional coagulation tests such as platelets, INR, PT, aPTT and individual coagulation factors such as procoagulant factors which include FII, FVIII, FvW (which are known to illustrate important changes in cirrhotic patients) and anticoagulant factors (antithrombin III, protein C, protein S) were monitored during this time period.
Studies in recent years have supported the idea that coagulopathy reflected in particular by prolongation of aPTT, INR and prothrombin type is associated with decreased liver synthesis function. Prothrombin time is a prognostic factor for survival, being an important marker of liver failure [26].
In the studied group, cirrhotic patients at the time of initiating AAD therapy, presented with a hypocoagulant status, diagnosed by an increased INR, prothrombin time and aPTT, associated with a fibrinogen within the normal range. The normal value of fibrinogen shows that the basic substrate for the thrombin to act exists and so, all coagulation parameters showed a a statistically significant trend towards improvement during the antiviral therapy for most of the patients included in the study.
There was a statistically significant increase in baseline mean platelet count at the end of treatment, a trend that was maintained in both direction and statistical significance (p = 0.000) and at SVR, when the highest platelet counts were achieved. The results of our study are consistent with those reported by Koh et al., who demonstrated in a prospective study of 100 patients followed for 23 months post-SVR that platelet counts improved markedly in patients who achieved SVR [27]. At the post-treatment evaluation, it was observed that no patient enrolled in the study had an altered prothrombin time. Platelet counts were low (< 160.000/mm3) in 80% of cirrhotic patients before therapy. At SVR assessment the mean platelet count in the 100 patients increased (from 209.000 to 239.000/mm3) and was within normal limits in approximately 90% of SVR patients. Before initiation of DAA, platelet counts were normal in patients with no or mild fibrosis, but even in these individuals the mean platelet count increased after SVR was achieved. A significant increase in platelets was observed in patients with moderate to advanced fibrosis. Last but not least, the authors showed that the number of platelets at the time of evaluation of liver elastography by fibroscan is inversely proportional to the degree of liver stiffness [27].
In the first study on the impact of SVR on coagulation parameters, proposed by Tripodi et al., platelet counts showed no significant improvement at EOT or SVR, while all other coagulation parameters showed an improvement in most patients, with no significant differences between pre- and post-antiviral treatment values, which contrasted the data we obtained [4]. Additionally, Tripodi et al. showed a decrease in prothrombin time at EOT and 12 weeks from achieving SVR, without statistical significance, which contradicts the data we obtained, where during the follow-up period the PT value registered significant changes.
Moreover, minor changes in standard coagulation parameters post-treatment were reported by another recent study, where platelet count and fibrinogen were partially “restored” post treatment, but below the values expressed in the control group. Furthermore, the concentration of factors II, VII, X was improved after antiviral treatment but to lower values than those of the control group despite obtaining SVR. These data differ from what our study illustrated, where the value of FII reached normal limits by increasing significantly at the time of SVR compared to the initial one.
In this study, it was observed that the average value of the usual parameters of coagulation, at all 3 moments, varied differently according to the Child-Pugh score, their number being inversely proportional to the severity of liver damage. Nielsen et al. are among the few researchers who specifically investigated, in a prospective study, the hemostatic function of whole blood in patients with chronic HCV infection with different degrees of liver fibrosis (absent, mild, advanced), with and without antiviral treatment, and the possible effects of viral replication on coagulation [11]. Compared with the control group of healthy patients, patients with chronic HCV infection with both mild and advanced fibrosis had thrombocytopenia and low antithrombin III concentration, which predisposes to thrombosis. At the same time, an increase in platelet aggregation was observed in patients with advanced fibrosis compared to those without or with mild liver fibrosis, a phenomenon that explains the occurrence of thrombotic events in patients with chronic HCV infection and increased fibrosis. At the same time, fibrinogen and aPTT values were decreased in the case of HCV infection, but their values did not differ according to the degree of liver fibrosis [11].
At the same time, recent studies that demonstrated an improvement in the number of platelets after AAD treatment raise an alarm signal in the case of these patients, this phenomenon being considered a predictive factor for triggering a thrombotic event [28,29,30,31]. Campello E et al., in a prospective study that included 58 patients with HCV cirrhosis treated with DAAs, mention that an increase in the number of platelets post-SVR is at the same time a risk factor for the occurrence of thrombotic complications in patients with more severe liver disease and portal hypertension [32]. In the studied group the authors reported 3 patients with Child B who developed non-malignant PVT one year after the end of antiviral treatment [32]. During our study, none of the patients developed thrombotic or hemorrhagic complications, but the follow-up period was short.
In the studied group, it was noted that the activity of all procoagulant factors was modified at the initiation of antiviral treatment. The activity for factor II was decreased while increased values of the activity of factor VIII and factor von Willebrand were recorded, the picture that defines the hypercoagulable status in cirrhotic patients at risk of thrombotic accidents. But over the course of the study, a statistically significant improvement in SVR was observed in these factors with increasing FII and decreasing factor VIII, as well as factor von Willebrand which followed a similar trend.
Similar to the evolution of procoagulant factors, in the case of anticoagulant factors (PC, PS, ATIII) a significant improvement in values was noted in patients with a sustained virological response. PC, PS and AT III values systematically increased over time, from the initial assessment (characteristic of a hypocoagulant status) to the other two determinations, reaching a significant value at the time of SVR. The exact reasons for the reduction in procoagulant imbalance are not definitely known, but the reduction in factor VIII concomitant with the increase in protein C following AAD treatment may be a likely explanation. Moreover, the simultaneous increase in AT III after treatment may contribute to the reduction of this procoagulant imbalance.
The results of clinical trials have shown that high levels of factor vW are a distinct feature of patients with liver cirrhosis. In this study we demonstrated that factor vW decreased in patients treated with antivirals, a fact that can be considered secondary to the beneficial effect of this therapy.
The results of our study are confirmed by those obtained by Tripodi (130), who demonstrated that FII, PC, and AT III increased significantly at EOT and persisted at SVR. Factor VIII concentration registered a statistically significant (p < 0.005) progressive decrease from EOT to SVR. The factor vW level decreased at the end of treatment, reaching statistical significance at SVR.
Russo et al. obtained the same results [5], showing that a decrease in FVIII and an increase towards normal values of protein C levels were the most significant changes in coagulation parameters. Moreover, an increase in FII, AT III and PS that highlights the improvement of pro- and anticoagulant factors liver synthesis in SVR patients was demonstrated. On the other hand, Nielsen et al. [11] observed that patients with chronic HCV infection treated with AAD and SVR had partial normalization of coagulation factors II, VII, and X.
The exact reasons why direct antivirals are effective in ameliorating pro- and anticoagulant factors in patients with HCV infection and SVR are not fully understood. It is known for certain that the synthesis of coagulation factors is impaired in cirrhotic patients, but the hypothesis that coagulation factors in SVR patients may also be low due to accelerated viral clearance cannot be excluded. Viral C infection activates coagulation through the mediation of proinflammatory cytokines, which leads to an acceleration of the clearance of coagulation factors from the bloodstream (110). Therefore, it can be assumed that HCV may act directly (decreased liver synthesis capacity) and/or indirectly (accelerated clearance of coagulation factors) on patients with HCV infection. In a recent study Meissner et al. (326) showed that there is a normalization of cytokines in patients with HCV infection treated with SOF/RBV, but their effect on coagulation factors was not studied.
5. Conclusions
The modification of coagulation parameters in patients with chronic HCV infection treated with the recently emerged AAD is still a matter of hypotheses, due to the relatively new medical therapy and the absence of an adequately long time for follow-up after the treatment. The reason why we see an improvement in the coagulation status is still under question, whether is due to the beneficial effect of the antiviral treatment caused by mechanisms not yet explained or due to improvement in liver function, proved by most clinical trails in which viral eradication was obtained.
Author Contributions
Concept and design, A.T. and L.H.; study coordination, C.S. and L.H.; methodology, C.-M.M., S.Z., R.I.A., I.D., R.N., A.R. and L.H.; software, S.Z, H.M., R.S., and A.R.; formal analysis, S.Z., R.N. and S.C.; investigation, R.N., R.S., R.I.A., and A.-M.S.; data curation, I.G., H.M., E.S, I.D., and S.C.; writing—original draft preparation, C.-M.M., R.N., E.S., and L.H.; writing—review and editing, A.T., A.-M.S.; visualization L.H.; supervision, A.T. and C.S. The published version of the manuscript has been read and approved by all authors.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of St. Spiridon Emergency Hospital Iasi, Romania, by Decision no. 29, dated 26 October 2018.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available because they are the property of the Institute of Gastroenterology and Hepatology, Iasi, Romania.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Masetti, C.; Lleo, A.; Colombo, M.; Colombo, M.; Aghemo, A. Postsustained Virological Response Management in Hepatitis C Patients. Semin Liver Dis 2020, 40, 233–239. [Google Scholar] [CrossRef]
- Reiberger, T.; Lens, S.; Cabibbo, G.; Nahon, P.; Zignego, A.L.; Deterding, K.; Elsharkawy, A.M.; Forns, X. EASL position paper on clinical follow-up after HCV cure. J Hepatol. 2024, 81, 326–344. [Google Scholar] [CrossRef]
- Cheng, C.H.; Chu, C.Y.; Chen, H.L.; et al. Direct-acting antiviral therapy of chronic hepatitis C improves liver fibrosis, assessed by histological examination and laboratory markers. J Formos Med Assoc. 2021, 120, 1259–1268. [Google Scholar] [CrossRef]
- Tripodi, A.; D’Ambrosio, R.; Padovan, L.; et al. Evaluation of coagulation during treatment with directly acting antivirals in patients with hepatitis C virus related cirrhosis. Liver Int. 2017, 37, 1295–1303. [Google Scholar] [CrossRef] [PubMed]
- Russo, F.P.; Zanetto, A.; Campello, E.; et al. Reversal of hypercoagulability in patients with HCV-related cirrhosis after treatment with direct-acting antivirals. Liver Int. 2018, 38, 2210–2218. [Google Scholar] [CrossRef] [PubMed]
- Azer, A.; Kong, K.; Basta, D.; Modica, S.F.; Gore, A.; Gorman, E.; Sutherland, A.; Tafesh, Z.; Horng, H.; Glass, N.E. Evaluation of coagulopathy in cirrhotic patients: A scoping review of the utility of viscoelastic testing. Am J Surg 2024, 227, 34–43. [Google Scholar] [CrossRef]
- González-Reimers, E.; Quintero-Platt, G.; Martín-González, C.; et al. Thrombin activation and liver inflammation in advanced hepatitis C virus infection. World J Gastroenterol 2016, 22, 4427–4437. [Google Scholar] [CrossRef]
- Zanetto, A.; Campello, E.; Senzolo, M.; Simioni, P. The evolving knowledge on primary hemostasis in patients with cirrhosis: A comprehensive review. Hepatology 2024, 79, 460–481. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Racila, A.; Muir, A.; et al. Long-term Patient-Centered Outcomes in Cirrhotic Patients With Chronic Hepatitis C After Achieving Sustained Virologic Response. Clin Gastroenterol Hepatol. 2022, 20, 438–446. [Google Scholar] [CrossRef] [PubMed]
- Northup, P.G.; Caldwell, S.H. Coagulation in liver disease: a guide for the clinician. Clin Gastroenterol Hepatol 2013, 11, 1064–1074. [Google Scholar] [CrossRef]
- Nielsen, N.S.; Jespersen, S.; Gaardbo, J.C.; et al. Impaired Platelet Aggregation and Rebalanced Hemostasis in Patients with Chronic Hepatitis C Virus Infection. Int J Mol Sci 2017, 18, 1016. [Google Scholar] [CrossRef]
- Ioannou, G.N.; Feld, J.J. What Are the Benefits of a Sustained Virologic Response to Direct-Acting Antiviral Therapy for Hepatitis C Virus Infection? Gastroenterology 2019, 156, 446–460. [Google Scholar] [CrossRef] [PubMed]
- Pearlman, B.L. Direct-Acting Antiviral Therapy for Patients with Chronic Hepatitis C Infection and Decompensated Cirrhosis. Dig Dis Sci 2024, 69, 1551–1561. [Google Scholar] [CrossRef]
- Young, K.; Liu, B.; Bhuket, T.; et al. Improved liver transplant waitlist mortality and lower risk of disease progression among chronic hepatitis C patients awaiting liver transplantation after the introduction of direct-acting antiviral therapies in the United States. J Viral Hepat. 2019, 26, 350–361. [Google Scholar] [CrossRef]
- Pol, S.; Parlati, L. Treatment of hepatitis C: the use of the new pangenotypic direct-acting antivirals in “special populations”. Liver Int. 2018, 38, 28–33. [Google Scholar] [CrossRef]
- Bachofner, J.A.; Valli, P.V.; Kroger, A.; et al. Direct antiviral agent treatment of chronic hepatitis C results in rapid regression of transient elastography and fibrosis markers fibrosis-4 score and aspartate aminotransferase-platelet ratio index. Liver Int. 2017, 37, 369–376. [Google Scholar] [CrossRef]
- Elsharkawy, A.; Samir, R.; El-Kassas, M. Fibrosis regression following hepatitis C antiviral therapy. World J Hepatol 2022, 14, 1120–1130. [Google Scholar] [CrossRef]
- Bethea, E.D.; Gaj, K.; Gustafson, J.L.; et al. Pre-emptive pangenotypic direct acting antiviral therapy in donor HCV-positive to recipient HCV-negative heart transplantation: an open-label study. Lancet Gastroenterol Hepatol 2019, 4, 771–780. [Google Scholar] [CrossRef]
- Hutchinson, S.J.; Valerio, H.; McDonald, S.A.; et al. Population impact of direct-acting antiviral treatment on new presentations of hepatitis C-related decompensated cirrhosis: a national record-linkage study. Gut. 2020, 69, 2223–2231. [Google Scholar] [CrossRef]
- Tosetti, G.; Degasperi, E.; Farina, E.; et al. Decompensation in Direct-Acting Antiviral Cured Hepatitis C Virus Compensated Patients With Clinically Significant Portal Hypertension: Too Rare to Warrant Universal Β-Blocker Therapy. Am J Gastroenterol 2021, 116, 1342–1344. [Google Scholar] [CrossRef]
- Calvaruso, V.; Craxi, A. Hepatic benefits of HCV cure. J Hepatol 2020, 73, 1548–1556. [Google Scholar] [CrossRef]
- Trifan, A.; Stanciu, C.; Gheorghe, L.; et al. Efficacy and safety of paritaprevir/ritonavir, ombitasvir, and dasabuvir with ribavirin for the treatment of HCV genotype 1b compensated cirrhosis in patients aged 70 years or older. Medicine 2017, 96, e9271. [Google Scholar] [CrossRef]
- Krassenburg, L.A.P.; Maan, R.; Ramji, A.; et al. Clinical outcomes following DAA therapy in patients with HCV-related cirrhosis depend on disease severity. J Hepatol. 2021, 74, 1053–1063. [Google Scholar] [CrossRef]
- Foster, G.R.; Irving, W.L.; Cheung, M.C.; et al. Impact of direct acting antiviral therapy in patients with chronic hepatitis C and decompensated cirrhosis. J Hepatol 2016, 64, 1224–31. [Google Scholar] [CrossRef]
- Pons, M.; Rodríguez-Tajes, S.; Esteban, J.I.; et al. Non-invasive prediction of liver-related events in patients with HCV-associated compensated advanced chronic liver disease after oral antivirals. J Hepatol. 2020, 72, 472–480. [Google Scholar] [CrossRef] [PubMed]
- Maynard, S.; Marrinan, E.; Roberts, L.; Stanworth, S. Does the Use of Viscoelastic Hemostatic Assays for Periprocedural Hemostasis Management in Liver Disease Improve Clinical Outcomes? Transfus Med Rev. 2024, 38, 150823. [Google Scholar] [CrossRef]
- Koh, C.; Heller, T.; Haynes-Williams, V.; et al. Long-term outcome of chronic hepatitis C after sustained virological response to interferon-based therapy. Aliment Pharmacol Ther. 2018, 37, 887–894. [Google Scholar] [CrossRef] [PubMed]
- Quaranta, M.G.; Ferrigno, L.; Tata, X.; D’Angelo, F.; Coppola, C.; et al. Liver function following hepatitis C virus eradication by direct acting antivirals in patients with liver cirrhosis: data from the PITER cohort. BMC Infect Dis 2021, 21, 413. [Google Scholar] [CrossRef]
- Poordad, F.; Castro, R.E.; Asatryan, A.; Aguilar, H.; Cacoub, P.; et al. Long-term safety and efficacy results in hepatitis C virus genotype 1-infected patients receiving ombitasvir/paritaprevir/ritonavir + dasabuvir ± ribavirin in the TOPAZ-I and TOPAZ-II trials. J Viral Hepat. 2020, 27, 497–504. [Google Scholar] [CrossRef]
- Airola, C.; Pallozzi, M.; Cerrito, L.; Santopaolo, F.; Stella, L.; Gasbarrini, A.; Ponziani, F.R. Microvascular Thrombosis and Liver Fibrosis Progression: Mechanisms and Clinical Applications. Cells. 2023, 12, 1712. [Google Scholar] [CrossRef]
- Wilson, S.; Joseph, J.; Danta, M.; Rabbolini, D.J. Viscoelastometry to Manage Bleeding in Liver Disease. Cureus. 2023, 15, e41401. [Google Scholar] [CrossRef] [PubMed]
- Campello, E.; Radu, C.M.; Zanetto, A.; et al. Changes in plasma circulating microvesicles in patients with HCV-related cirrhosis after treatment with direct-acting antivirals. Liver Int. 2020, 40, 913–920. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Usual coagulation parameters (platelet, INR, PT, fibrinogen, aPTT) - evolution during antiviral treatment (baseline, EOT, SVR).
Figure 1.
Usual coagulation parameters (platelet, INR, PT, fibrinogen, aPTT) - evolution during antiviral treatment (baseline, EOT, SVR).
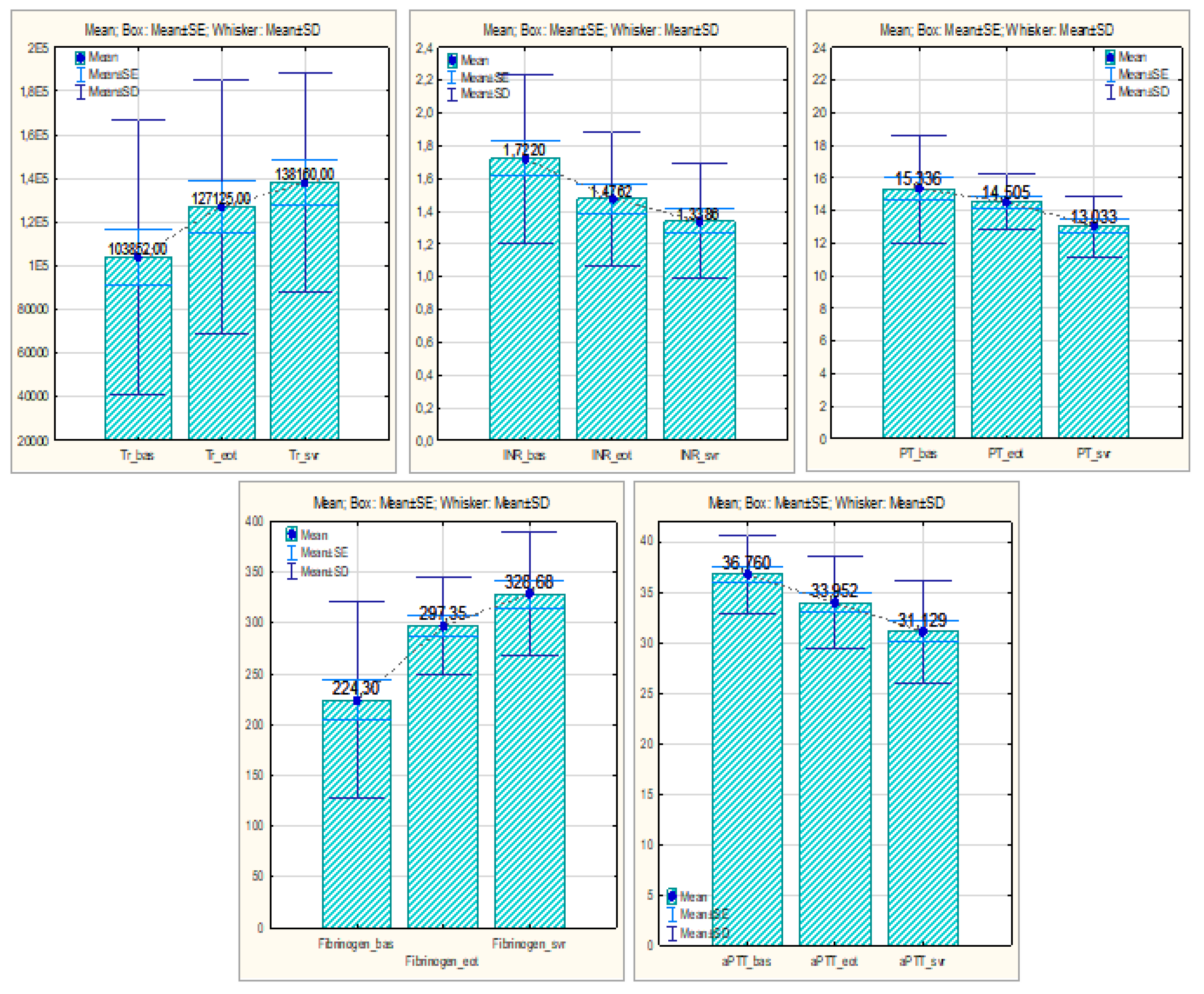
Figure 2.
Procoagulant factors (FII, F VIII, FvW) - evolution during antiviral treatment (baseline, EOT, SVR). FII, factor II; F VIII, factor VIII; FvW, factor von Willebrand
Figure 2.
Procoagulant factors (FII, F VIII, FvW) - evolution during antiviral treatment (baseline, EOT, SVR). FII, factor II; F VIII, factor VIII; FvW, factor von Willebrand
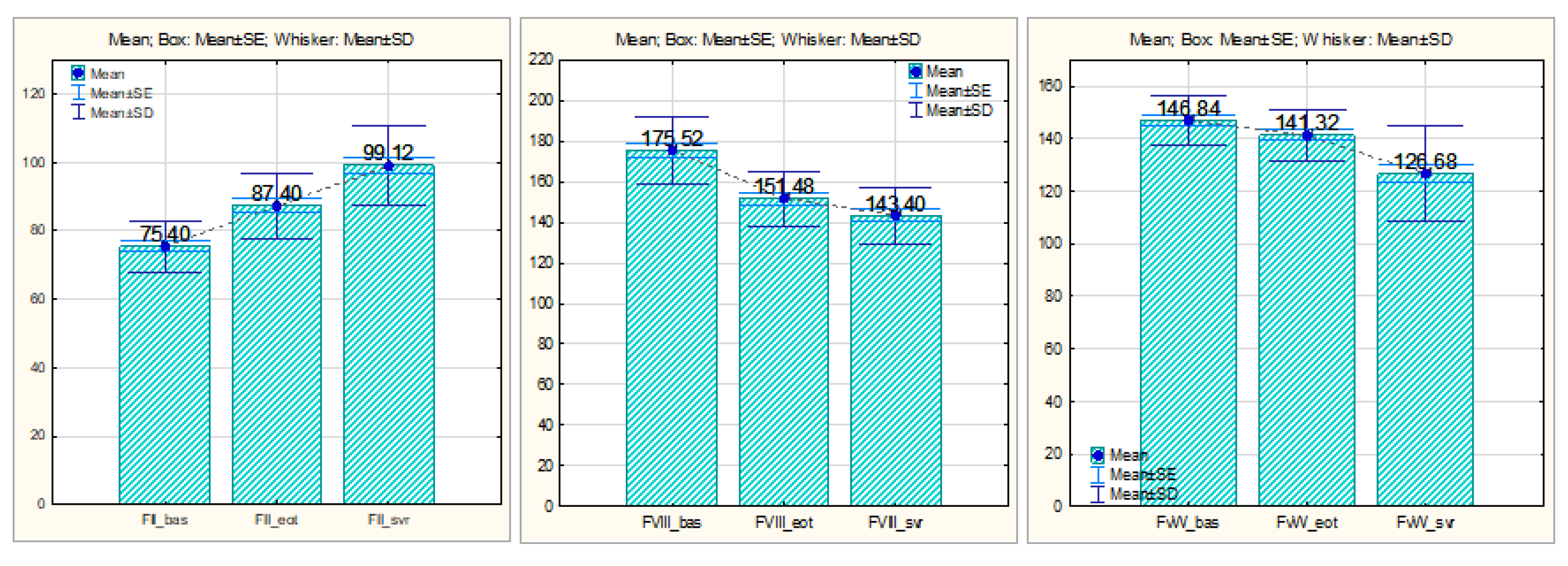
Figure 3.
Anticoagulant factors (PC, PS, AT III) - evolution during antiviral treatment (baseline, EOT, SVR). PC, protein C; PS, protein S; AT III, antithrombin III
Figure 3.
Anticoagulant factors (PC, PS, AT III) - evolution during antiviral treatment (baseline, EOT, SVR). PC, protein C; PS, protein S; AT III, antithrombin III
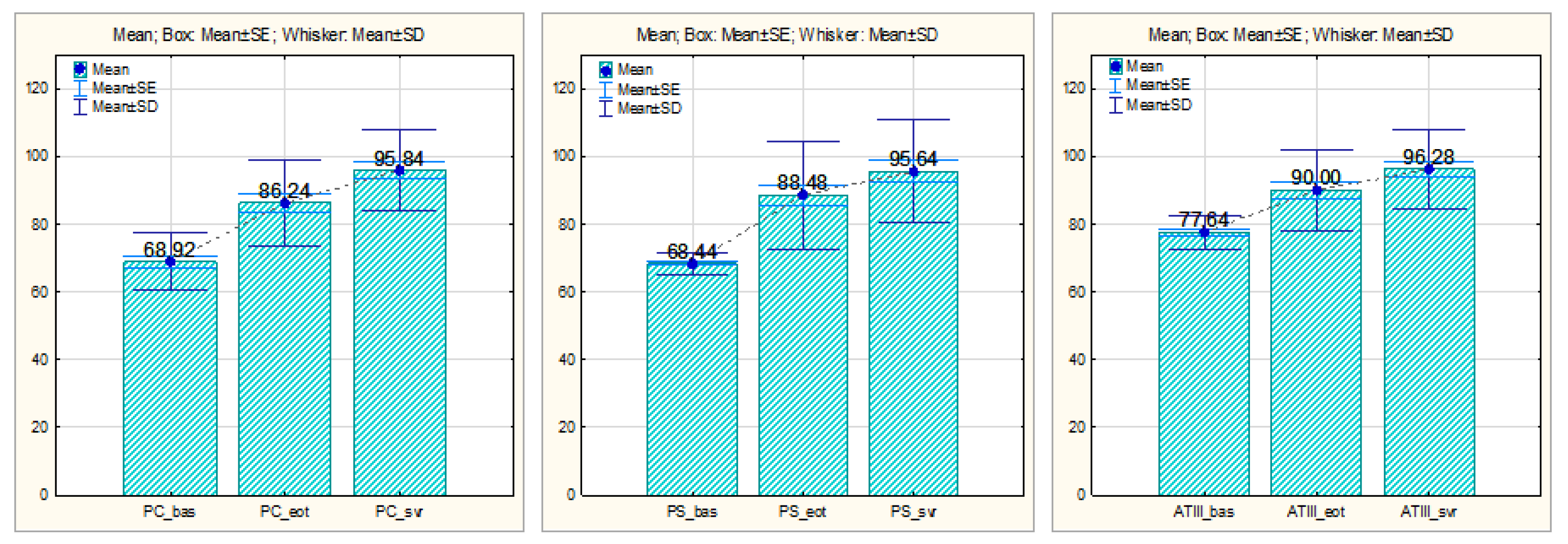
Figure 4.
Procoagulant factors (FII, F VIII, FvW) - initial value and evolution of values over time, compared by Child-Pugh classes.
Figure 4.
Procoagulant factors (FII, F VIII, FvW) - initial value and evolution of values over time, compared by Child-Pugh classes.
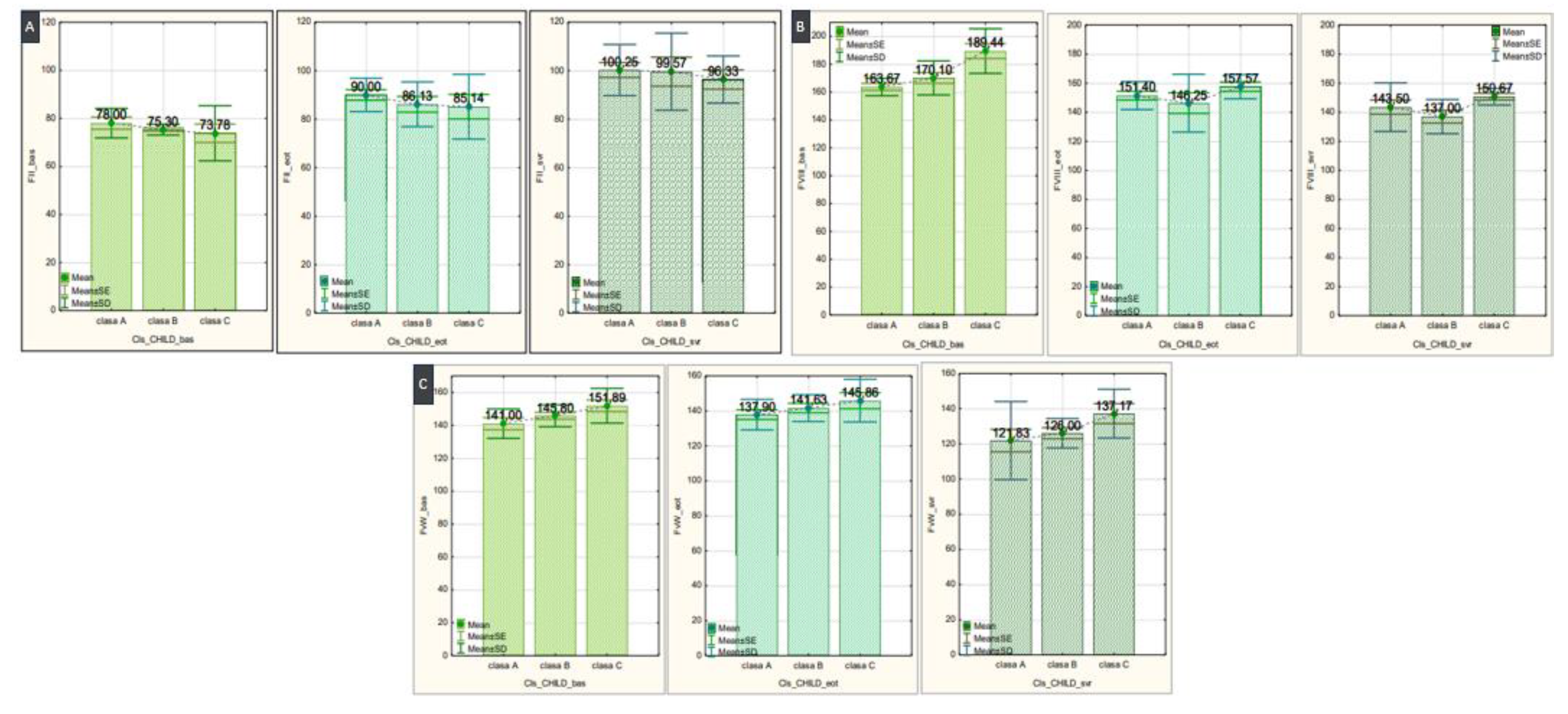
Figure 5.
Antithrombin III - initial value and evolution of values over time, compared by Child-Pugh classes.
Figure 5.
Antithrombin III - initial value and evolution of values over time, compared by Child-Pugh classes.
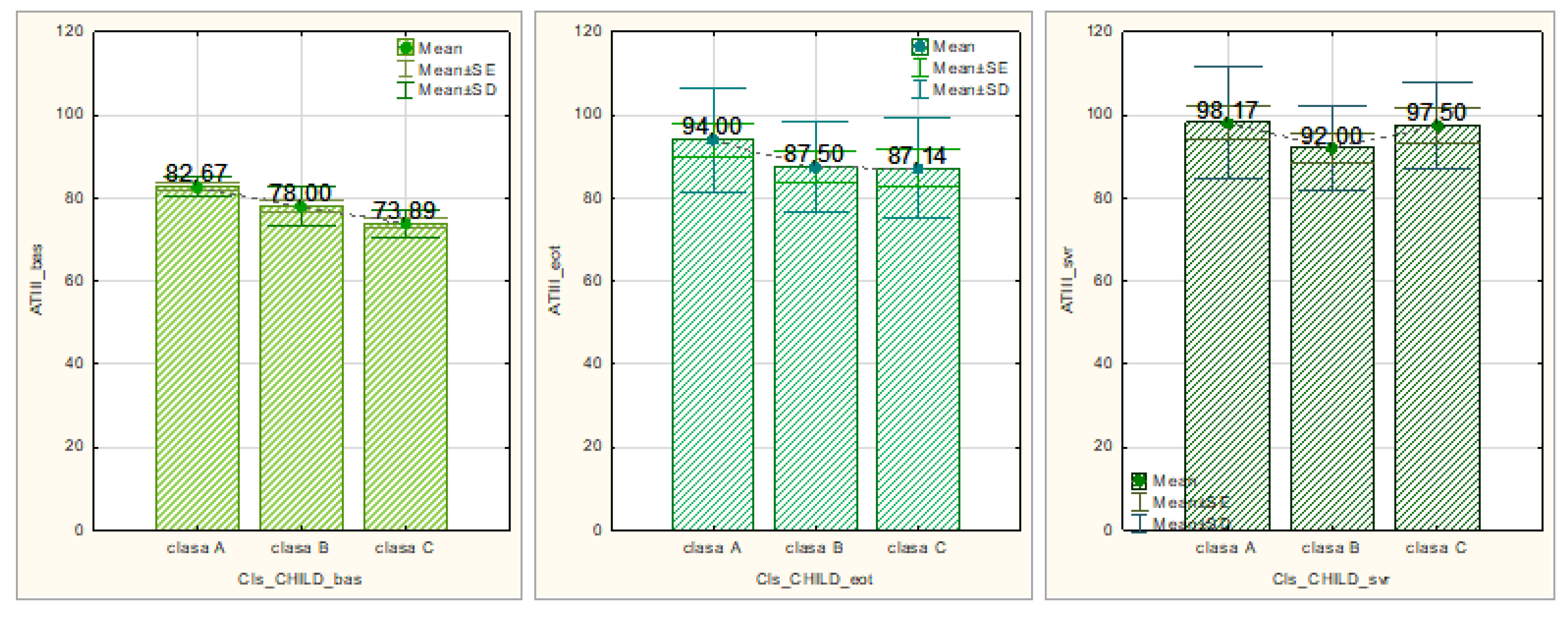

Table 1.
Baseline characteristics of the study patients.
| Parameters | Patients, N=52 |
|---|---|
|
Sex male, n (%) female, n (%) |
17 (32%) 35 (68%) |
| Age (years) | 63,88 ± 9,387 |
|
Child-Pugh class class A, n (%) class B, n (%) class C, n (%) |
12 (24%) 21 (40%) 19 (36%) |
|
MELD score < 15 ≥ 15 |
21 (40%) 31 (60%) |
|
Treatment DAA PrOD, n (%) LED / SOF, n (%) |
12 (24%) 40 (76%) |
| Experienced / naïve to IFN, n (%) | 15 (28%) / 37 (72%) |
| Ribavirin, n (%) | 15 (28%) |
| Antecedents of decompensation, n (%) | 29 (56%) |
| History of esophageal varices, n (%) | 35 (68%) |
| Fibroscan, kPa | 26 |
| SVR, n (%) | 52 (100%) |
n, number of subjects; SVR, sustained virologic response; DAA, direct acting antivirals; PrOD, Ombitasvir/Paritaprevir/Ritonavir, Dasabuvir; LED, ledipasvir; SOF, sofosbuvir; IFN, interferon; kPa, kilopascali.
Table 2.
Table 2A. Protein C – the initial value and the evolution of values over time, comparatively, by Child-Pugh classes.
Table 2.
Table 2A. Protein C – the initial value and the evolution of values over time, comparatively, by Child-Pugh classes.
| Protein C | |||
|---|---|---|---|
| CHILD class | N | Media ±SD | p |
| Baseline | 0,001** | ||
| class A | 14 | 75,50 ± 3,146 | |
| class B | 20 | 71,30 ± 3,129 | 0,075 |
| class C | 18 | 61,89 ± 9,993 | 0,010* |
| EOT | 0,002** | ||
| class A | 22 | 87,30 ± 10,253 | |
| class B | 17 | 95,50 ± 10,433 | 0,102 |
| class C | 13 | 74,14 ± 9,582 | 0,015* |
| SVR | 0,164 | ||
| class A | 24 | 96,75 ± 11,395 | |
| class B | 16 | 100,71 ± 12,392 | 0,474 |
| class C | 12 | 88,33 ± 10,328 | 0,156 |
Table 2.
Protein S – the initial value and the evolution of values over time, comparatively, by Child-Pugh classes.
Table 2.
Protein S – the initial value and the evolution of values over time, comparatively, by Child-Pugh classes.
| Protein S | |||
|---|---|---|---|
| CHILD class | N | Media ±SD | p |
| Baseline | 0,005** | ||
| class A | 13 | 71,83 ± 2,787 | |
| class B | 21 | 67,60 ± 2,011 | 0,005** |
| class C | 18 | 67,11 ± 3,018 | 0,002** |
| EOT | 0,665 | ||
| class A | 20 | 90,10 ± 3,018 | |
| class B | 19 | 90,63 ± 19,835 | 0,947 |
| class C | 13 | 83,71 ± 10,484 | 0,437 |
| SVR | 0,781 | ||
| class A | 25 | 96,75 ± 15,184 | |
| class B | 15 | 97,14 ± 18,898 | 0,959 |
| class C | 12 | 91,67 ± 12,910 | 0,527 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



