
Submitted:
13 August 2024
Posted:
14 August 2024
You are already at the latest version
Abstract
Autism spectrum disorder (ASD) involves social communication difficulties and repetitive behaviors, with a growing prevalence worldwide. Symptoms include cognitive impairments, gastrointestinal (GI) issues, feeding difficulties, and psychological problems. A significant concern in ASD is food selectivity, leading to nutrient deficiencies. Common GI issues in ASD, such as constipation and irritable bowel syndrome, stem from abnormal gut flora and immune system dysregulation. Sensory sensitivities and behavioral challenges exacerbate these problems, correlating with neurological symptom severity. Children with ASD also exhibit higher oxidative stress due to low antioxidant levels like glutathione. Therapeutic diets, including ketogenic, high-antioxidant, gluten-free, and casein-free, show potential in managing ASD symptoms like behavior, communication, GI issues, and oxidative stress, though the evidence is limited. Various studies have focused on different populations, but there is increasing concern about the impact on children. This review examines the effect of food selectivity, GI problems, and antioxidant deficiencies in ASD and revises the effectiveness of various therapeutic diets, highlighting the need for further research to confirm their long-term benefits.
Keywords:
autism spectrum disorder
; nutrition
; vitamins
; oxidative stress
; diets
; food selectivity
; gastrointestinal disorders.
1. Introduction
Autism spectrum disorder (ASD), previously known as autism, is a complex developmental disability characterized by social communication difficulties and restrictive repetitive behaviors [1]. It is called "spectrum" because it includes a variety of manifestations and degrees of severity. ASD symptoms typically appear in the first years of life and persist into adulthood, including cognitive impairment, seizures, sleep disturbances, gastrointestinal (GI) issues, feeding difficulties, and mood disorders [2]. Additionally, psychological problems such as anxiety, depression, and behavioral challenges are also common [3].
In addition to autism, the Diagnostic and Statistical Manual of the Mental Disorders (DSM-V) considers Asperger syndrome as a part of the spectrum of ASD. Asperger syndrome is a condition where intellectual levels are average or above average in terms of communication skills but with difficulties understanding social situations [4]. The DSM also considers part of ASD a condition named childhood disintegrative disorder, which is a drastic loss of behavioral and developmental functioning after at least two years of normal development [5]. However, there are several classifications and levels of ASD severity.
The prevalence of ASD has increased significantly worldwide, with the World Health Organization estimating that approximately 1 in 100 children globally have autism [6]. In the United States, the Centers for Disease Control and Prevention (CDC) report that about 1 in 36 children are diagnosed with ASD [7], and in Mexico, the prevalence is approximately 1 in every 115 children [8]. This increase can be attributed to greater awareness, improved diagnostic methods, and changes in diagnostic criteria. However, prevalence varies considerably between regions and countries. Despite these variations, the global rise highlights the urgent need for resources and public health policies to support individuals with ASD and their families.
One of the main characteristics of ASD is an eating disorder frequently marked by strong food selectivity and pronounced dietary preferences [9]. This pattern is thought to be connected to physiological changes related to sensory perception that may be brought on by behavioral problems [10]. Autistic traits often manifest through sensory sensitivity, reluctance to try new foods, and food limitations. These limitations may include sensitivity to textures, preferences for specific brands, and difficulties with feeding [11]. Such preference or rejection of particular foods can significantly restrict the intake of essential nutrients necessary for appropriate physical and developmental growth [12, 13]. Previous reviews have indicated that neurodivergent individuals exhibit higher food selectivity than their neurotypical counterparts. This selectivity leads to nutrient insufficiency and an imbalanced body composition, with tendencies toward underweight and obesity [10]. A neurodivergent person is considered a person who has a neurological developmental disorder or disability, and a neurotypical person is a person who does not have it [14].
ASD is usually accompanied by GI issues that range from mild to severe symptoms, such as constipation, abdominal pain, diarrhea, and irritable bowel syndrome. The exact etiology of these issues is unknown; however, it is thought to be a mix of variables such as aberrant gut flora, immune system dysregulation, and increased intestinal permeability [15]. Furthermore, sensory sensitivities and behavioral challenges associated with ASD can increase feeding difficulties, worsening GI symptoms. GI problems correlate favorably with the severity of neurological symptoms in persons with ASD, highlighting the importance of focusing therapies on these patients' GI health [16]. In addition, children with ASD often exhibit higher oxidative stress caused by the lower levels of antioxidants, such as glutathione (GSH), the main intracellular antioxidant crucial for combating oxidative stress and maintaining cellular health, as well as by mitochondrial dysfunction, increased lipide peroxidation and other markers [17]. Oxidative stress has been linked to some neurological disorders, including ASD [18]. Antioxidant deficiencies in people with ASD may exacerbate symptoms such as behavioral disorders, cognitive impairments, and GI problems.
Treating these deficits with dietary modifications, supplements, and general nutritional support is becoming a more significant component of ASD management. Among the array of treatment options available, therapeutic diets have been somewhat under-researched despite their widespread adoption by families dealing with autism [19]. Several survey studies have highlighted positive outcomes associated with therapeutic diets, showing improvements in specific ASD symptoms such as behavior, communication, and overall health. Additionally, benefits have been reported in managing GI problems, attention issues, communication skills, and social interaction [20, 21]. Despite widespread interest in dietary interventions, there is no agreement on effective nutritional therapy.
A primary motivation for implementing therapeutic diets is the observation that children with ASD frequently have restricted diets, often consuming only a limited variety of foods. This tendency raises concerns about potential deficiencies in both macronutrients and micronutrients, underscoring dietary interventions' importance [10]. Therefore, this review aims to highlight the food preferences of the ASD population, analyze the impact of food selectivity, GI problems, and antioxidant deficiencies in individuals with ASD, and evaluate the effectiveness of therapeutic diets, including diets rich in antioxidants, gluten-free and casein-free, and ketogenic and essential fatty acids diets in managing these challenges.
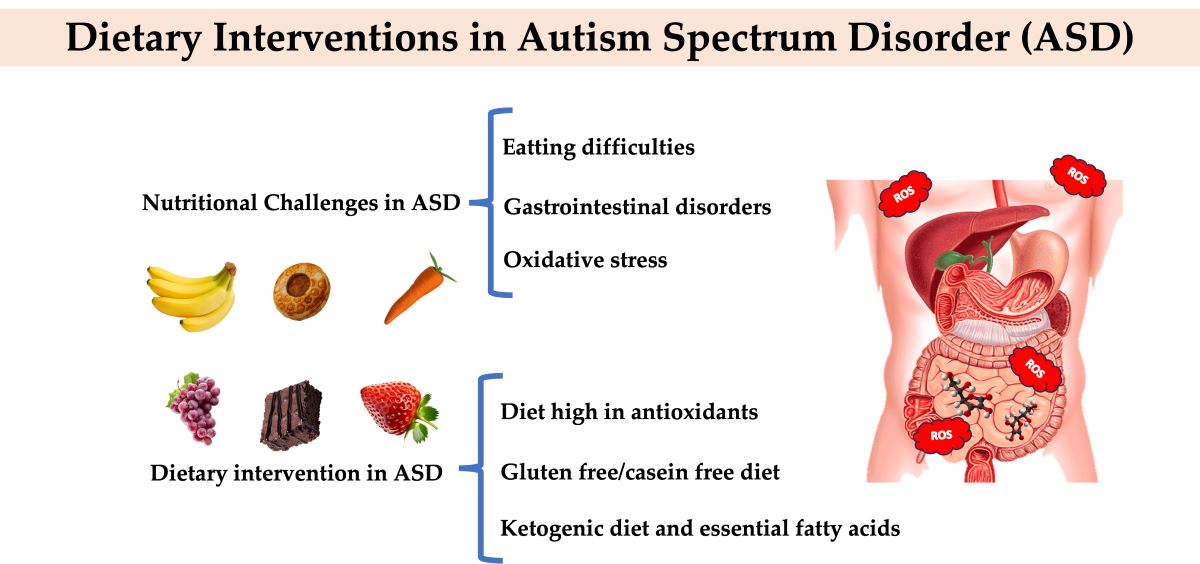
2. Nutritional Challenges in Autism Spectrum Disorder
Individuals with ASD encounter significant challenges in their nutrition, primarily stemming from their strict food preferences and difficulties in digesting and absorbing food [22]. Hence, several factors need to be taken into account before implementing any dietary intervention for managing ASD in individuals, including food selectivity, GI issues, and oxidative stress.
2.1. Eating Difficulties
Food selectivity is a developing health problem for children with ASD. Food selectivity can be defined as food rejection, food restriction, or intake of a particular food [23]. Food selectivity, considered an eating disorder affecting 70-80% of children with ASD for over two years, negatively impacts health, nutrient intake, and family relationships, especially during meals [24]. To a certain degree, food selectivity and feeding disorders are observed in neurotypical children, but they tend to be more severe in individuals with ASD [25, 26].
Sensory, behavioral, and biological factors influence food selectivity in individuals with ASD. Sensory sensitivities play a crucial role, as many children with ASD are susceptible to specific characteristics of foods, such as textures, tastes, colors, smells, appearance, and temperature of foods [27, 28]. These sensitivities can make certain foods intolerable, severely limiting the variety of accepted foods. Furthermore, behavioral factors, such as restrictive and repetitive interests and actions, contribute to dietary selectivity [25].
Another feeding difficulty (not disorder) commonly in ASD individuals is food neophobia, manifested as a consistent refusal of foods with particular characteristics or a reluctance to try new foods, which may occur with varying frequency across individuals. Refusing solid foods is common among individuals with ASD, and introducing foods with new textures, consistencies, and flavors often proves challenging [29]. As a result, they tend to consume the same foods repetitively. Children with ASD typically choose processed, sugary, and high-fat diets and reject fruits and vegetables [30]. Preferences for unhealthy foods can increase the risk of obesity and deficiencies in vitamins and minerals.
Sensory sensitivity, particularly oral sensitivity, can partially explain food selectivity and food neophobia in ASD [31, 32]. Studies have shown that children with ASD often exhibit atypical sensory processing, including heightened sensitivity to taste, touch, and other sensory inputs [33]. This can lead to food rejection based on their sensory characteristics and contribute to persistent food refusal behaviors. Neurological factors in ASD may reinforce these behaviors, making them difficult to change. Early evaluation and intervention for these sensory-related eating issues are crucial to prevent malnutrition and other health problems related to inadequate nutrient intake [24, 34, 35].
In the case of ASD, these behaviors can significantly disrupt the child's daily functioning and hinder their integration within peer groups [36]. Moreover, mealtime can be especially challenging for people with autism and their families. Each meal can become a source of stress and frustration for the parents as they try to balance the nutritional needs of the individual with autism with their sensory and behavioral limitations. This stress can affect family dynamics and make meals a tense and emotionally charged time. In addition to the understanding that introducing new foods may exacerbate food selectivity in individuals with ASD, it is recognized that inappropriate mealtime behaviors can contribute to restrictive eating habits and poor nutrition [37, 38].
Food selectivity has a direct and negative impact on the nutrition of individuals with ASD. By limiting the variety of foods consumed, children with ASD often have diets deficient in essential macronutrients and micronutrients, such as protein, vitamins, and minerals. This lack of nutrients can affect physical growth and development, leading to problems such as low weight, obesity, and deficiencies in the immune system. In the long term, these deficiencies can have serious health consequences, including the risk of chronic diseases and impaired cognitive and emotional development. For example, Molina-López, Leiva-García, Planells and Planells [10] conducted a cross-sectional case-control study in 144 children (N = 55 with ASD; N = 91 with neurotypical children) between 6 and 18 years of age to examine body composition, nutritional intake, food consumption frequency, and mealtime behavior. This study revealed that children with ASD showed lower weight (18.4% ASD vs. 3.20% comparison group) and higher obesity (16.3% ASD vs. 8.6% comparison group) than neurotypicals. In addition, ASD children had greater intake inadequacy (50% ASD vs. 22% comparison group), high food selectivity (60.6% ASD vs. 37.9% comparison group), and more eating problems (food rejection, limited variety, disruptive behavior) compared to neurotypical children. Children with ASD exhibit more altered mealtime behaviors, leading to higher food selectivity and nutritional deficiencies (moderate effect). Children with ASD reported a greater risk of nutritional insufficiency when exhibiting food selectivity [32]. According to Sharp, et al. [39], 78.5% of children with ASD had an inadequate diet in terms of five or more nutrients. Early diagnosis enables parents and caregivers to conduct nutritional interventions on time, with the assistance of specialists. Some nutritional inadequacies have been related to the disorder's pathophysiology; thus, addressing these concerns as soon as possible is critical to improving the health and well-being of those affected.
Table 1 shows different studies where various foods were evaluated by frequency of consumption. This information reveals that the level of acceptance of food for children with ASD varied significantly due to attributes such as texture, temperature, color, etc., and predominantly accepted smooth and easy-to-chew foods [9, 40, 41]. Additionally, these children prefer foods with high amounts of sugar and lower vegetables [42]. It also indicated that neurotypical children have a more diverse diet than neurodivergent children, noting that toddlers with ASD eat more snacks than neurotypical children [43]. However, a survey showed that children with ASD who were picky about foods had more GI affection than children without food selectivity [44]. Food selectivity, which leads to imbalances in diet composition, may indeed contribute to GI problems in at least some individuals with ASD [45]. It highlights the importance and urgency of parents to find new snacks look for snack options that are not only sensory appealing but also offer an adequate nutritional profile [46].
All these studies should be considered cautiously, as they present some limitations. For instance, many of them do not correlate the severity of ASD with the degree of food selectivity. Additionally, numerous studies compare children with ASD to independent neurotypical children, which means that the factors influencing differences in food selection could also be due to economic, familial, social, and other factors. Therefore, studies involving neurotypical siblings could be particularly insightful.
2.2. Gastrointestinal Disorders
Apart from the range of symptoms observed in the primary diagnostic criteria, individuals with ASD may exhibit non-neurological comorbidities, such as problems related to the GI tract [47, 48]. Children with autism have a high incidence of experiencing general symptoms related to their GI disorders and, consequently, might potentially influence food choices and contribute to instances of food refusal [49]. Esposito, et al. [50] performed a questionnaire interview in a case-control study and found that GI symptoms, parenting style, and sensory abnormalities were linked to children's food avoidance. In children with ASD, GI symptoms were related to heightened sensitivity to moving visual stimuli and smell. In another study, ASD participants with feeding problems had a higher rate of GI symptoms and challenging behavior and sensory issues [51].
The prevalence of GI symptoms in the ASD population can range from 20-80% [52]. The most common GI problems in individuals with autism are chronic constipation, diarrhea, and abdominal pain [53], with elevated occurrences of gastroesophageal reflux, bloody stools, vomiting, gaseousness, and signs of GI inflammation; increased intestinal permeability, food allergies, altered dietary nutrient intake, and metabolic disruptions have also been linked to ASD [47, 48]. In the systematic review carried out by Herrera-Mejía, Ramos-Jiménez, Jiménez-Vega, Campos-Vega, González-Córdova and Wall-Medrano [16], they found that the most prevalent GI symptoms were constipation (50-88.5%), flatulence (51-87.5%), abdominal distension (33-87.5%) and diarrhea (12.5-72.8%). In some studies, GI disorders were more prevalent and severe in ASD patients than in neurotypical volunteers.
The mechanisms of such disorders are not fully understood and appear to have a multifactorial basis, meaning they can arise from a combination of different factors [54]. In children and adolescents with ASD, GI problems are positively correlated with the severity of neurological manifestations [55]. For example, compared to children with less severe ASD, those with more severe ASD experienced diarrhea 10% more frequently. Children with ASD are more likely than neurotypicals to have GI symptoms at least occasionally [56]. Despite some discrepancies, most studies confirm a significant correlation between GI problems and ASD when compared to healthy, age-matched controls [54].
The pathophysiology of ASD may be influenced by gut microbiota and its metabolites. Studies have demonstrated that, compared to neurotypical children, individuals with ASD exhibit less diverse gut microbiota, a scarcity of beneficial bacteria, and a higher density of harmful bacteria [57]. Dysbiosis is widespread in ASD individuals, and particular abnormalities in the gut microbiota have been identified in patients with GI disorders [52]. The normal intestinal microbiota comprises beneficial bacteria such as Bifidobacterium, Lactobacillus, Bacteroidetes, and Firmicutes, which play crucial roles in digestion, producing short-chain fatty acids and immune system modulation. Maintaining a proper balance between these bacteria, particularly the Bacteroidetes/Firmicutes ratio and high microbial diversity, is essential for intestinal health. An imbalance, such as an increase in Firmicutes and a decrease in Bacteroidetes, has been associated with metabolic disorders and inflammatory bowel diseases, among other conditions.
The study by Shaaban, et al. [58] found that the bifidobacterium concentrations in children with ASD were lower than those in children without ASD. Similarly, Tomova, Husarova, Lakatosova, Bakos, Vlkova, Babinska and Ostatnikova [55] reported that patients with ASD had a lower Bacteroidetes/Firmicutes ratio and higher levels of lactobacilli species compared to neurotypical volunteers. In the same study, patients with more severe GI symptoms had lower Bacteroidetes/Firmicutes ratios and a greater abundance of bacteria Clostridium and Desulfovibrio than those with mild or moderate symptoms. The severity of the symptoms is correlated with the degree of GI microbial dysbiosis [53]. The systematic review by Nogay and Nahikian-Nelms [59] found among the analyzed studies, high growth rates of Clostridium histolyticum, C. perfringens, and Sutterella, a high ratio of Escherichia/Shigella, and a low ratio of Bacteroidetes/Firmicutes were generally related to GI problems. However, they concluded that published studies on the relationship between GI and behavioral issues with gut microbiota in autism are minimal and contradictory.
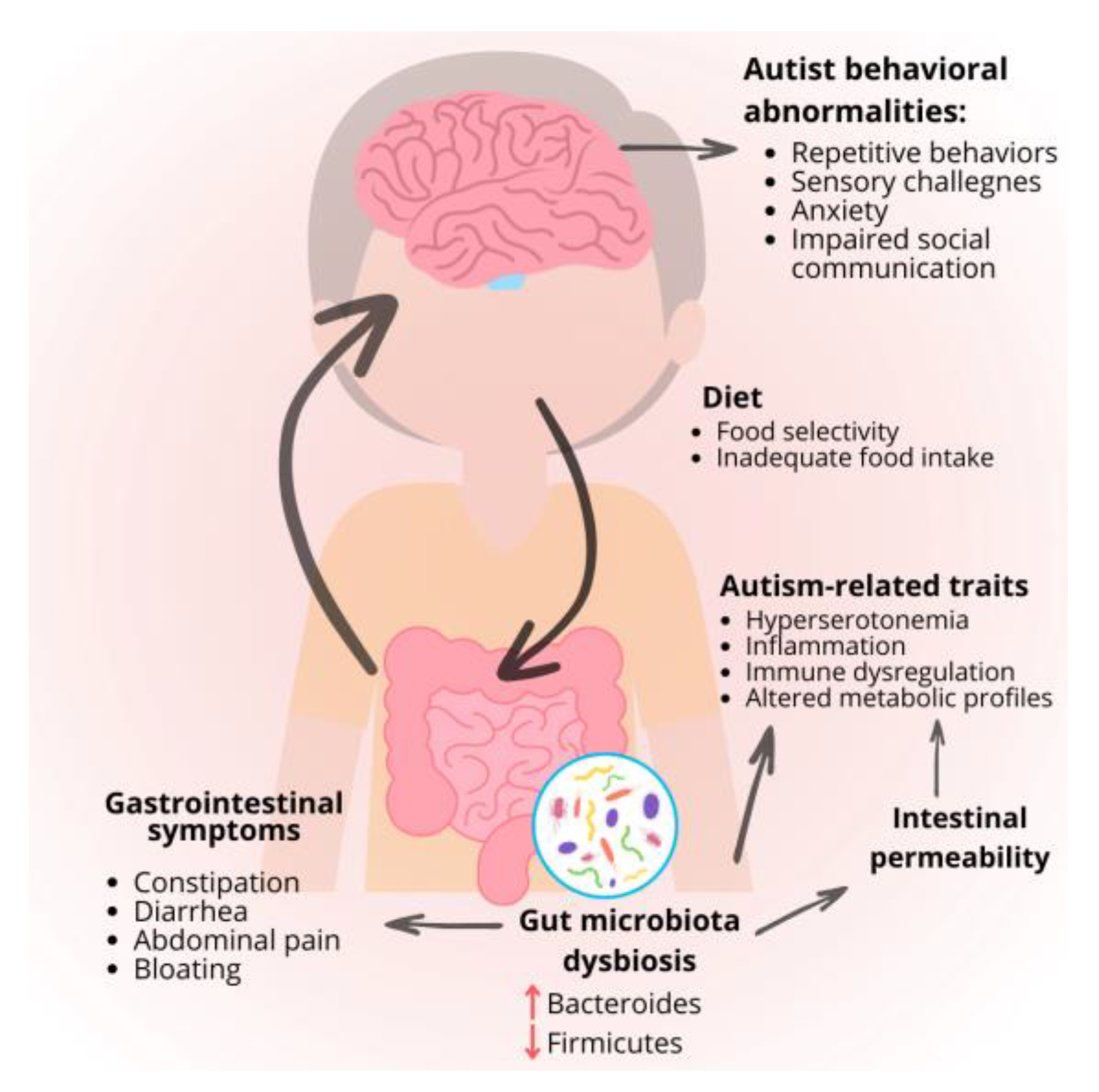
Changes in the microbiota accentuate neurological and digestive problems by stimulating responses to localized inflammatory processes that increase intestinal permeability [16]. There is existing interest in the morphology of the GI structure in children with ASD, which can present a high intestinal permeability (nearly 40% in comparison to the neurotypical public, presenting only <5%), high levels of pro-inflammatory lymphocytes, or even colonic lesions due to epithelial damage [60, 61]. GI problems in ASD patients, such as increased intestinal permeability, altered gut microbiota, and dysregulated GI motility and secretion, can influence the development of other autism-related traits. These disruptions can affect serotonin production, leading to the association of hyperserotonemia with ASD. The increased intestinal permeability leads to the entry of bacterial metabolites or partially digested nutrients into the bloodstream, accentuating the digestive, metabolome, and neurological disorders. These GI issues can also cause immune dysregulation, affecting behavior and brain function via the gut-brain axis through direct and indirect pathways involving the vagus nerve and immune system changes [47].
In a 2010 consensus report by Buie, et al. [62], 23 statements were provided regarding children with ASD and various aspects of diagnosing and treating GI disorders in this population. Among these statements, it was suggested that a combination of behavioral treatment and dietary manipulation (such as gluten-free and casein-free diets) could help reduce mealtime discomfort in some individuals. The report also emphasized the need for further research on nutritional interventions, with guidance from qualified nutritionists and pediatricians, while noting that dietary manipulation should not be used as the primary treatment for ASD.
Figure 1.
Impact of the gastrointestinal on autism spectrum disorder symptoms.
For food allergies, it has been reported it is 1.8 times more likely for this population to have some degree of asthma or food allergy. When put into comparison to the general pediatric population, around 5% of neurotypical children have food allergies, whereas in autistic children, this percentage is up to 20 to 25%. The systematic review and meta-analysis of Wang, et al. [63] found that the prevalence of food allergy was higher in participants with ASD than in controls, and participants with ASD were at risk of developing food allergy. Food refusal could often indicate selectiveness over food and reflect a food allergy that has not been well explored or diagnosed [64].
2.3. Oxidative Stress
Oxidative stress (OS) is a condition characterized by an imbalance between the production of reactive oxygen/nitrogen species (ROS/RNS) and the antioxidant defenses naturally found in organisms [65]. This is caused by excessive ROS/RNS, or decreased synthesis or functional antioxidant protection capacity [66]. Fundamentally, ROS and RNS include superoxide (O2−), hydroxyl, peroxyl, alkoxy, hydrogen peroxide, and peroxynitrite free radicals. These molecules in high amounts can cause significant cell membrane damage, alteration in membrane fluidity and permeability, and induce oxidative changes in proteins, lipids, and DNA [67]. It has been reported that oxidative damage caused by free radicals plays a substantial role in the development, occurrence, and severity of many pathogenic diseases, including autism, Alzheimer's, Parkinson's, amyotrophic lateral sclerosis, diabetes mellitus, cardiovascular and inflammatory diseases, cancer, among others [17]. Several factors contributing to the increase in OS are associated with contemporary lifestyle habits, such as an unhealthy diet, physical inactivity, smoking, and exposure to alcohol, pesticides, and food additives [68].
The cellular antioxidant defense mechanism serves two primary functions: inhibiting the production of free radicals and deactivating them if they are generated. To achieve this, several enzymatic and non-enzymatic defense molecules have evolved to mitigate oxidative damage by transferring excess electrons during the detoxification process. Key antioxidant enzymes, such as superoxide dismutase, catalase, and glutathione peroxidase, are crucial in neutralizing reactive oxygen species (ROS) and protecting cellular components from oxidative stress. Superoxide dismutase (SOD) catalyzes the conversion of superoxide radicals into hydrogen peroxide and oxygen, thereby preventing harmful reactions that superoxide might cause. Catalase (CAT) then converts hydrogen peroxide into water and oxygen, mitigating potential oxidative harm. Glutathione peroxidase (GPx) reduces hydrogen peroxide and organic hydroperoxides to water and corresponding alcohols, using GSH as a substrate, thus protecting cell membranes and lipids from peroxidation [69].
Non-enzymatic antioxidants are vital components of the cellular defense system against oxidative stress. These molecules, which include vitamins C and E, GSH, flavonoids, and carotenoids, directly scavenge ROS and RNS to prevent cellular damage. Vitamin C, a water-soluble antioxidant, neutralizes free radicals in the aqueous compartments of cells and tissues, while vitamin E, a lipid-soluble antioxidant, protects cell membranes from lipid peroxidation. GSH, a tripeptide, is critical in maintaining the redox balance within cells and regenerating other antioxidants. Flavonoids and carotenoids in various fruits and vegetables also contribute to antioxidant defense by inhibiting oxidative reactions and stabilizing free radicals [17]. These non-enzymatic antioxidants complement enzymatic antioxidants, ensuring comprehensive protection against oxidative damage and maintaining cellular health.
Increased OS and specific chemical stress are common features in ASD individuals [70, 71]. The former hypothesis, suggesting that ROS/RNS plays a significant role in ASD, is now widely accepted as factual [72]. The role of ROS/RNS in ASD is not yet fully understood; however, the redox imbalance and oxidative stress are essential components of ASD pathogenesis. Several studies have found elevated levels of oxidative stress markers in individuals with ASD, indicating that they experience more severe oxidative damage compared to neurotypical individuals [73]. Autism is associated with increased lipid peroxidation markers such as blood lipid peroxides and thiobarbituric acid reactive compounds compared to neurotypical controls [74, 75]. Some indirect markers, such as phospholipase A2 and loss of membrane lipoprotein asymmetry, have previously been documented in ASD individuals, as mentioned in the review of Bjørklund, Meguid, El-Bana, Tinkov, Saad, Dadar, Hemimi, Skalny, Hosnedlová and Kizek [73]. Furthermore, the ASD patients had elevated levels of pro-oxidants, such as perchlorethylene, hexane, and pentane, as well as heavy metals, such as mercury, lead, and arsenic. Autistic patients' blood circulation showed elevated amounts of cytokines and xanthine oxidase, which can produce free radicals [73].
Individuals with ASD present low plasma and cellular GHS (L-γ-glutamyl-L-cysteinyl-glycine) levels and lower GSH reserve capacity, increasing oxidative stress. A GSH redox imbalance is common in ASD children, as evidenced by lower quantities of reduced glutathione (GSH), higher oxidized glutathione (GSSG), and a lowered GSH/GSSG redox ratio [76]. Usui, Iwata, Miyachi, Takagai, Wakusawa, Nara, Tsuchiya, Matsumoto, Kurita and Kameno [71] found that a considerable reduction in cysteine glutathione disulfide in children with ASD is associated with impaired cysteine metabolism and increased oxidative stress. Major antioxidants such as GSH and cysteine are essential for fighting oxidative stress and sustaining cell health. GSH is vital in protecting cells against toxins, particularly in the brain. Antioxidant deficits, such as GSH, aggravate symptoms in people with ASD, including behavioral abnormalities, cognitive impairments, and GI problems [73]. Moreover, ASD exhibit reduced activities of key antioxidant enzymes, specifically SOD and CAT [17, 77]. Children with ASD have lower amounts of antioxidant serum proteins such as transferrin, which lowers free ferrous ion concentrations, and ceruloplasmin, which prevents the peroxidation of membrane lipids caused by metal ions like iron and copper [74].
Mitochondrial dysfunction is one of the leading causes of ASD pathology since there are abnormalities in the mitochondrial electron transport system that occur in the brains of patients with ASD [22, 78]. In addition, children with ASD present inactivation of mitochondrial aconitase, an enzyme that helps catalyze citrate to isocitrate [76]. Mitochondrial dysfunction can contribute to altered energy metabolism. Mitochondria are essential for producing adenosine triphosphate (ATP), the energy currency of the cell, and any impairment in their function can lead to reduced energy availability for cellular processes. It has been reported a reduced ATP synthesis in the brains of individuals with ASD by magnetic resonance spectroscopy and elevated levels of lactate and pyruvate indicating damaged energy and mitochondrial metabolism [79]. In addition, mitochondrial dysfunction can lead to increased production of ROS, further exacerbating oxidative stress
OS is recognized as a factor associated with the development of ASD, and impairments in the antioxidant system can impact the function of the brain [80]. The brain is particularly vulnerable to oxidative stress, especially during early development [81]. This vulnerability can lead to neurodevelopmental disorders, including ASD. The brain's high metabolic activity and oxygen consumption make it susceptible to damage from ROS. Individuals with ASD exhibit signs of oxidative stress in the brain [82]. This includes findings from studies that have reported physiological abnormalities such as increased lipid peroxidation and reduced antioxidant defenses in brain tissue derived from patients with ASD. Children with ASD often have reduced levels of key antioxidants and antioxidant enzymes in the brain, such as GSH, SOD, and CAT [83]. This reduced antioxidant capacity can impair the brain's ability to counteract oxidative stress, leading to increased oxidative damage and contributing to the pathophysiology of ASD. The oxidative stress observed in the brains of individuals with ASD is associated with dysfunction in brain regions involved in critical functions such as speech, auditory processing, social behavior, memory, and motor coordination [82]. This suggests that oxidative stress may play a role in the cognitive and behavioral symptoms associated with ASD.
Some studies state that OS in children with ASD may suggest an increase in this activity and a more complicated pattern involving different types of ROS and antioxidants [84]. Children with ASD have shown a decrease in hydroxyl radical scavenging activity and an increase in superoxide and alkoxyl radical scavenging activities. A study by Hirayama, et al. [85] suggests that redox changes in children with ASD represent a more complex antioxidative shift. They also revealed that the CoQ10 oxidation and serum 8-hydroxy-2′-deoxyguanosine (8-OHdG) values in their ASD group, consisting of >6 years old, were significantly increased than their control group, which translates into higher levels of oxidative stress and had substantially higher adiponectin values in children with ASD of the same ages as mentioned before. This study also suggests that OS in ASD patients is not simply increased but shows a complicated imbalance, including multiple types of ROS, subsequent ROS chain reactions, and comprehensive modifications in the antioxidant system. These affected factors are summarized in Figure 2.
Oxidative stress can also stimulate our immune response and cause allergic reactions, such as food allergies, which, as mentioned above, are sometimes present in ASD children. Thus, this suggests that the innate antioxidant protection mechanism of patients with allergic reactions is less effective than that of a healthy individual [86].
Targeting oxidative stress in ASD comprises strategies to reduce ROS generation and improve antioxidant defenses. Dietary therapies with antioxidant-rich foods and supplementing with vitamins and minerals, including vitamins E, C, and selenium, have shown promise in reducing oxidative damage. Furthermore, lifestyle changes, such as minimizing exposure to environmental pollutants and regulating inflammation, are essential components of a complete strategy for managing oxidative stress in people with ASD. Understanding and managing oxidative stress is critical for improving the health and well-being of people with ASD. Current research is investigating viable therapies and therapy techniques to combat oxidative stress and its effects on autism.
3. Dietary Intervention in ASD
It is recognized that many children with ASD are underweight due to insufficient intake of dietary fiber, vitamins, calcium, iron, and potassium [10]. Studies have also demonstrated that providing nutritional supplements to children with ASD in amounts exceeding their daily requirements for protein, carbohydrates, and fats can result in GI problems and obesity [10]. Also, there is evidence suggesting that individuals with ASD are more commonly affected by food allergies and intolerances, often necessitating dietary interventions as part of their medical treatment [87]. For this reason, it is necessary to implement diets that regulate food intake, as well as the minimum nutritional requirements for people with ASD.
3.1. Diet High in Antioxidants
Antioxidants play a critical role in the organism by protecting against ROS's harmful effects and preventing free radicals' formation [88]. The body naturally possesses antioxidant mechanisms that seek out and neutralize the damage caused by free radicals. Additionally, antioxidants can be consumed through the daily diet. While antioxidants effectively counter oxidative stress, it is essential to consume them in moderation, as excessive supplementation can increase the risk of allergic diseases [89].
Depending on their solubility, antioxidants can be divided into two categories: hydrosoluble and liposoluble. Water-soluble antioxidants are rapidly eliminated through urine, whereas fat-soluble antioxidants are absorbed in the presence of fats and can easily accumulate in the body [90]. Several antioxidants are available in different foods, including anthocyanins, carotenes, vitamins, flavonoids, etc. [91, 92]. Chemical structures of carotenoids, phenols, and major antioxidant vitamins are depicted in Figure 3.
Beta-carotene is a naturally abundant pigment that gives orange fruits and vegetables their characteristic color, such as sweet potatoes, carrots, mangos, and apricots. Beta-carotene is converted into vitamin A in the body, contributing to a lower risk of chronic diseases such as cardiovascular diseases, cancer, cataracts, and macular degeneration [93]. Numerous carotenoids exhibit antioxidant and anti-inflammatory properties [94].
Beta-cryptoxanthin, structurally similar to beta-carotene, is found in foods such as butternut squash, persimmons, pumpkin, hot chili peppers, papaya, and oranges. It is absorbed by intestinal cells and has higher bioavailability than beta-carotene or other carotenoids [95]. Like beta-carotene, beta-cryptoxanthin can be converted into retinol (vitamin A), although enzymes involved in this conversion prefer beta-carotene. Beta-cryptoxanthin has been shown to protect against DNA damage in some cases but may cause damage at high concentrations [96]. Additionally, it impacts genetic regulation, antioxidant activity, and inflammatory markers in vitro [96]. Lycopene, another carotenoid compound, is found in tomatoes, papaya, watermelon, among other fruits. Because of its anti-inflammatory and antioxidant qualities, this carotenoid can help with intestinal barrier diseases and promote intestinal health. However, more studies need to be done on these carotenoids to complement the existing information further.
Flavonoids are natural compounds extracted from plants, fruits, and vegetables known for their antioxidant effect. These compounds are particularly responsible for the color and aroma of flowers. Altered redox status and concurrent subclinical inflammation have been observed in individuals with ASD [76]. Specifically, quercetin and luteolin mainly exhibit potent antioxidant properties and possess a low redox potential, which may be beneficial in addressing autism-related issues [97]. In plants, flavonoids aid in developing seeds and fruits and act as a protective system against biotic and abiotic stresses [98]. Despite their excellent biological properties, flavonoids have very low bioavailability, challenging proper metabolism [99]. Flavonoids are divided into subgroups such as flavones, flavanols, isoflavones, and chalcones, depending on their attachment in their C and/or B ring, their degree of unsaturation and oxidation of their C ring [100].
Anthocyanins are polyphenols in berries, blue or red-colored vegetables, fruits, or flowers. Depending on their pH levels, these water soluble pigments exhibit vibrant blue or red hues. They are often used in the food industry for products like jam, candy, and beverages as natural alternatives to synthetic food dyes [101]. The high antioxidant activity of anthocyanins is primarily due to their glycosylated B-ring structure. Health benefits of antioxidants include a lower risk of cardiovascular disease, anticancer effect, reduced risk of diabetes, improved vision, and antimicrobial activity [102].
Flavones, secondary metabolites in vascular plants, are crucial in growth and development. Their antioxidant properties help scavenge free radicals, prevent lipid peroxidation, and modulate important enzyme activities [103]. Flavanols are commonly found in fruits, vegetables, cereals, and legumes; certain flavanols are considered functional components in dairy goods. Flavanols have been shown to reduce inflammation, participate in antioxidant activities, and act as a neuroprotective agent [104]. Flavonols, naturally found in broccoli and tomatoes, are well known for their ability to scavenge free radicals that can negatively impact the body. Quercetin, a model flavonol, demonstrates significant radical scavenging properties and helps protect the body from dangerous illnesses [105, 106]. Flavanones, minor chemical components in plants, are found mainly in citrus fruits and have gained considerable interest due to their antioxidant, antimicrobial, and other biological effects [107]. Isoflavonoids, found in soybeans, soybean products, and other legumes, are known for their role as phytoalexins, which are compounds that accumulate in plants during stress or microbial attacks. These compounds possess antibacterial, antioxidant, and antiviral properties [108].
As previously mentioned, vitamins also play an important role in antioxidant activity. Vitamin A plays a crucial role in regulating the development of the central nervous system through its active metabolite, retinoic acid [109]. Retinoic acid is instrumental in promoting intestinal immunity and preserving the integrity of mucosal epithelial cells [110]. Research has demonstrated that vitamin A can increase oxytocin levels through the CD38 pathway in individuals with autism. Oxytocin, in turn, can potentially enhance brain activity and significantly improve the social abilities of children with autism [111]. Vitamin A deficiency poses a significant public health concern due to its adverse effects, including anemia, a weakened immune system leading to susceptibility to infections, ocular symptoms, and an increased risk of mortality [112]. Studies have reported that therapy with vitamin A can help alleviate symptoms associated with ASD [113].
Vitamin C, or ascorbic acid, is a hydrosoluble antioxidant that neutralizes and removes oxidant agents and recycles other antioxidants while acting as a strong reducing agent [109]. Additionally, vitamin C serves as a cofactor in the biosynthesis of neurotransmitters such as serotonin [114] and has been found to have mood-improving properties [115]. Children with ASD were likely to have low vitamin C values due to their diet being poor in fruits and vegetables due to low intact or malabsorption [76]. The role of Vitamin C in health is closely tied to maintaining the internal microenvironment, which is determined by the redox balance. This balance is disrupted in various diseases, including obesity, cancer, neurodegenerative diseases, hypertension, and autoimmune diseases [116].
Vitamin E or α-tocopherol, is a liposoluble antioxidant known for its ability to scavenge free radicals. Reduced levels of vitamin E have been observed in the blood of individuals with ASD, and its supplementation is associated with attenuating ASD-like symptoms [117]. Vitamina E inhibits the peroxidation of membrane lipids by scavenging highly reactive peroxyl radicals [69].
Several studies suggest that supplementing vitamins and minerals can help reduce ASD symptoms [118, 119]. For example, Meguid, et al. [120] supplemented zinc to 30 children with ASD ages 3 to 8. The results of this study reduced Childhood Autism Rating Scale (CARS) scores, improved cognitive-motor performance, and lowered copper levels. In a study where vitamin A was supplemented in children with ASD, the symptoms of this disorder significantly enhanced, suggesting that supplementation can also be a viable option for this population [111]. Similarly, Adams, Audhya, McDonough-Means, Rubin, Quig, Geis, Gehn, Loresto, Mitchell and Atwood [118] compared children aged 5-16 (n = 55) to nonsibling, neurotypical controls (n = 44) of similar age, gender, and regional distribution. The results showed that oral vitamin and mineral supplementation helps children with autism improve their nutritional and metabolic state, including methylation, glutathione, oxidative stress, sulfation, ATP, NADH, and NADPH. In a clinical trial, a double-blind, placebo-controlled crossover study was conducted to evaluate the safety and efficacy of glutathione alone or in combination with vitamin C and N-acetylcysteine in children with autism who also have severe behavior problems [121] Participants received either a placebo or one of the two treatments for eight weeks. The study found that both glutathione alone and the combined therapy improved developmental skills and behavior compared to the placebo. This suggests that addressing the vitamin E/vitamin C/glutathione network can ameliorate ASD-like symptoms.
All of the antioxidants mentioned previously can be briefly summarized in Table 2. This topic has been extensively discussed. As previously reviewed by Önal, et al. [122], an excellent table displays the relevance of several studies where vitamin and mineral supplementation were given to children with ASD.
3.2. Gluten Free/Casein Free Diet
Individuals with ASD frequently suffer from casein and gluten allergies, which have a substantial influence on dietary management and general health [87, 127]. Casein, a protein found in milk and dairy products, and gluten, a protein found in wheat, barley, and rye, are frequent allergens that can cause severe responses in susceptible people. A gluten-free diet eliminates foods containing wheat, barley, rye, and any products made from these cereals, such as flour, bread, pasta, and bakery items [128]. On the other hand, a casein-free diet entails avoiding dairy products such as milk, yogurt, cheese, butter, cream, and ice cream, among others [129].
In children with ASD, the immune system's response to these proteins can aggravate both GI and behavioral symptoms [130]. Many studies indicate that people with ASD have a higher sensitivity or intolerance to casein and gluten [87, 127]. According to theories, the immunological and GI systems have a role in ASD development by modulating the gut-blood-brain barrier via bacterial byproducts such as lipopolysaccharides and short-chain fatty acids, which impact cytokine production. Furthermore, bacterial byproducts such as serotonin may influence neuropeptide production, whereas gluten and casein peptides are thought to promote opioid system activation. These neuropeptides may affect social behavior and communication, contributing to ASD etiology. This sensitivity can cause various GI disorders, including bloating, constipation, diarrhea, and abdominal pain. Furthermore, these dietary proteins have been linked to initiating inflammatory responses, which are thought to contribute to the overall symptomatology of autism [130]. Children with ASD have greater levels of pro-inflammatory cytokines following exposure to dietary proteins from gluten and casein compared to controls [131].
Case reports highlight the benefits of therapeutic diets for children with ASD, demonstrating improvements in eye contact and communication skills and the alleviation of symptoms like constipation and vomiting, mainly through the adoption of a GFCF diet [132]. The factors mentioned above, and other theories suggest that children with ASD must pay particular attention to their diet. Various studies have shown that parents often choose a GFCF diet for their children with ASD, as there appears to be a relation between the mechanisms of action of the immune system and the GI system [48, 133, 134]. Parents also report increased behavioral issues, such as hyperactivity, difficulty focusing and sleeping problems, and GI problems when not following a GFCF diet [135].
There are multiple double-blinded studies where a GFCF diet was not significantly beneficial. Most of these studies monitor very few sample sizes, some examples ranging from 12 to 74 children with ASD of different ages and follow-up periods from 1 to 24 weeks [136-141]. In a study, participants were evaluated three times: before the intervention, after six months, and after 12 months of adhering to a GFCF. However, post-intervention assessments did not reveal any significant changes in behaviors related to language, sociability, sensory speech communication, cognitive consciousness, autistic seclusion, or physical health disability [140].
Another study examined the impact of a gluten-free diet on a cohort of sixty-six children (aged 36–69 months) with ASD. The participants were divided into two groups: Group I followed a gluten-free diet, while Group II consumed at least one regular meal containing gluten per day for six months. Each child underwent a comprehensive behavioral and psychometric assessment at baseline and after the intervention period. After six months, both groups showed improvements on the tests, but no significant differences were observed between the two groups [142]. However, some detailed studies with up to four years of follow-up for a gluten-free, casein-free (GFCF) diet have reported significant benefits for children with gastrointestinal (GI) issues, primarily diarrhea and constipation. These studies found that the diet improved GI conditions and enhanced social behaviors and physiological symptoms compared to children with ASD who do not have GI issues [143, 144].
Nevertheless, systematic reviews on the GFCF suggest that the evidence is currently insufficient to either support or refute its effectiveness in alleviating ASD symptoms [145]. We can conclude that more studies with an increased sample size and prolonged follow-up periods are needed to conclude whether children with ASD benefit from this specific diet. However, this diet is the most commonly used in children with ASD (Matthews et al., 2023).
3.3. Ketogenic Diet and Essential Fatty Acids
At the moment, there is a growing interest in prospective dietary intervention as a viable treatment for ASD. The ketogenic diet (KD) is a promising treatment for neurological disorders; however, prospective controlled trials with high sample sizes are required to establish official recommendations. KD consists of consuming high amounts of fatty foods, low carbohydrates, and adequate protein [146]. By consuming low amounts of carbohydrates, our organism is forced to use ketone bodies as a fuel source, providing energy to the brain [147]. The ketogenic diet is beneficial and improves ASD symptoms [148].
This neuroprotective diet is often recommended for neurological disorders that are neurodegenerative or that have a metabolic defect, for instance, Alzheimer's disease, Parkinson's disease, migraines, etc., to lessen symptoms, and it has shown overall cognitive improvements[149]. For this reason, it also has been considered a complementary treatment to ASD due to its correlation with epilepsy [146]. Epilepsy is a common neurological comorbidity associated with ASD that affects the brain by exhibiting seizures. It is caused by different factors or categories such as genetics, structural, metabolic, infectious, immune, and others whose etiology remains vague [150]. Epilepsy affects about 1 out of 10 people with ASD [151].
In a pilot follow-up study, 30 children with ASD followed a ketogenic diet for six months. Seven subjects could not tolerate the diet, and five others adhered for only 1 or 2 months. The remaining subjects reported significant improvements in overall autistic behaviors [152]. In a similar study, 45 children with ASD, aged 3 to 8 years, participated in a controlled treatment divided into three groups: one group followed a ketogenic diet, another group followed a GFCF diet, and the control group followed a balanced diet. Results showed improved CARS scores for the ketogenic and GFCF diets compared to the control group. The ketogenic diet group also improved cognition and sociability compared to the GFCF and control groups, suggesting the potential benefits of these diets; however, more studies are needed to draw definitive conclusions [153]. Additionally, the ketogenic diet may act as an antioxidant, as ketone bodies are known to inhibit the production of ROS at a mitochondrial level by increasing NADH oxidation [154].
The pilot study of Mu, Corley, Lee, Wong, Pang, Arakaki, Miyamoto, Rho, Mickiewicz, Dowlatabadi, Vogel, Korchemagin and Shearer [147] investigated the relationship between behavioral parameters, blood metabolites, and trace elements in 10 typically developed controls and 17 children with ASD, both at baseline and after three months of treatment with a modified KD regimen. Key findings demonstrated that, at baseline, children with ASD had higher quantities of galactose intermediates, gut microbe-derived trimethylamine N-oxide, and N-acetylserotonin, but lower levels of 3-hydroxybutyrate and selenium than the control group. After three months on the KD regimen, the ASD group's circulating ketones and acetylcarnitine levels increased, while selenium levels returned to control values. The study also discovered a new unfavorable association between selenium levels and behavioral ratings. High responders to the KD intervention had higher concentrations of 3-hydroxybutyrate and ornithine and lower galactose levels, which improved our understanding of metabolic alterations in ASD and the potential benefits of KD intervention.
Supplementation for fatty acids, specifically omega 3 and 6, is also a popular treatment in children with ASD since these contribute to brain function, neurotransmission, and the composition of cell membranes and help decrease inflammation and oxidative stress. Omega 3 and omega 6 are dietary polyunsaturated fatty acids. Omega 3 is derived from alpha-linolenic acid (ALA) that turns into a 20-22 chain of carbon atoms that can convert to eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) once metabolized. Omega 6 derives from linoleic acid (LA) and turns into a longer chain; however, it converts to arachidonic acid instead [155].
Fatty acids have been used as a treatment in multiple neurological disorders, such as schizophrenia [156], depression [157], and bipolar disorder, amongst other disorders like ASD [158]. In children with ASD, DHA and EPA levels have been recognized to be significantly lower than the general population [159]. Therefore, supplementation for these fatty acids has shown benefits in decreasing ASD-like symptoms and helping with overall social behavior and repetitive behaviors [160, 161]. Moreover, according to a study by Matthews and Adams [2], this diet usually improves GI problems, attention issues, language/communication, and depression, among others.
4. Conclusions and Future Directions
ASD is a condition that requires increased attention due to its growing prevalence. Addressing ASD necessitates a multidisciplinary approach, considering the numerous factors involved. Children with ASD often experience metabolic and GI symptoms that can be derived from the condition itself. While many details remain to be discovered and understood, parents have turned to dietary interventions to alleviate behavioral and GI symptoms. Diets such as ketogenic, high antioxidant diets, and casein-gluten-free have garnered interest in managing ASD symptoms. Initial research suggests they may offer potential benefits. The exclusion of casein and gluten is based on the hypothesis that these components might trigger inflammatory or neurochemical responses in some individuals with ASD. These diets typically focus on reducing carbohydrate consumption and increasing the intake of healthy fats and lean proteins, potentially positively impacting brain function and energy metabolism. However, the evidence supporting the effectiveness of these dietary exclusions in children with ASD remains limited, necessitating further research to validate their widespread use. Ketogenic diets may increase the risk of deficiencies in essential vitamins such as A, D, and E. Therefore, children on such diets must receive appropriate medical supervision and, when necessary, supplements to ensure healthy growth and development. Regarding the supplementation of vitamins, minerals, and antioxidants, while beneficial, excessive intake can lead to pro-oxidant effects, potentially causing harm. Therefore, any supplementation should be discussed with the child’s physician to consider all aspects of their care.
In conclusion, while specific diets may offer benefits for some children with ASD, parents need to work closely with medical and nutritional professionals to ensure these diets are safe, balanced, and appropriate for the individual needs of each child. Dietary approaches in ASD children have shown improvements in attention span, cognition, and irritability, suggesting that following a specific diet improves behavioral aspects. However, given individual differences, not all diets will elicit the same response in every child, emphasizing the need for personalized assessment by a nutritionist or specialist. Further research is required to understand these treatments' long-term effectiveness and applicability in managing ASD in children.
Author Contributions
Conceptualization, C.L.D.-T.-S and A.L.P-D.; writing—original draft preparation, I.D.P.-C.; writing—review and editing, A.T.B.-M. and C.L.D.-T.-S.; supervision, A.R.I.-S., G.M.S.-J. and M.A.R.-G. All authors have read and agreed to the published version of the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Lord, C.; Elsabbagh, M.; Baird, G.; Veenstra-Vanderweele, J. Autism spectrum disorder. The Lancet 2018, 392, 508–520. [Google Scholar] [CrossRef] [PubMed]
- Matthews, J.S.; Adams, J.B. Ratings of the effectiveness of 13 therapeutic diets for Autism Spectrum Disorder: Results of a national survey. Journal of Personalized Medicine 2023, 13, 1448. [Google Scholar] [CrossRef] [PubMed]
- Masi, A.; DeMayo, M.M.; Glozier, N.; Guastella, A.J. An overview of Autism Spectrum Disorder, heterogeneity and treatment options. Neuroscience Bulletin 2017, 33, 183–193. [Google Scholar] [CrossRef] [PubMed]
- APA DSM-5: Manual diagnóstico y estadístico de los trastornos mentales. 2014.
- Mehra, C.; Sil, A.; Hedderly, T.; Kyriakopoulos, M.; Lim, M.; Turnbull, J.; Happe, F.; Baird, G.; Absoud, M. Childhood disintegrative disorder and autism spectrum disorder: a systematic review. Developmental Medicine and Child Neurology 2019, 61, 523–534. [Google Scholar] [CrossRef] [PubMed]
- WHO Autismo. https://www.who.int/es/news-room/fact-sheets/detail/autism-spectrum-disorders (November),.
- CDC Data and statistics on Autism Spectrum Disorder. https://www.cdc.gov/autism/data-research/index.html.
- Guizar, D. En México, uno de cada 115 niños padece autismo. https://www.dgcs.unam.mx/boletin/bdboletin/2020_291.html (November),.
- Byrska, A.; Błażejczyk, I.; Faruga, A.; Potaczek, M.; Wilczyński, K.M.; Janas-Kozik, M. Patterns of food selectivity among children with Autism Spectrum Disorder. Journal of Clinical Medicine 2023, 12, 5469. [Google Scholar] [CrossRef] [PubMed]
- Molina-López, J.; Leiva-García, B.; Planells, E.; Planells, P. Food selectivity, nutritional inadequacies, and mealtime behavioral problems in children with autism spectrum disorder compared to neurotypical children. International Journal of Eating Disorders 2021, 54, 2155–2166. [Google Scholar] [CrossRef] [PubMed]
- Baraskewich, J.; von Ranson, K.M.; McCrimmon, A.; McMorris, C.A. Feeding and eating problems in children and adolescents with autism: A scoping review. Autism: The International Journal of Research and Practice 2021, 25, 1505–1519. [Google Scholar] [CrossRef] [PubMed]
- Robea, M.-A.; Luca, A.-C.; Ciobica, A. Relationship between Vitamin Deficiencies and Co-Occurring Symptoms in Autism Spectrum Disorder. Medicina (Kaunas, Lithuania) 2020, 56, 245. [Google Scholar] [CrossRef]
- Monteiro, M.A.; Santos, A.A.A.D.; Gomes, L.M.M.; Rito, R.V.V.F. Autism Spectrum Disorder: A systematic review about nutritional interventions. Revista paulista de pediatria : orgao oficial da Sociedade de Pediatria de Sao Paulo 2020, 38, e2018262–e2018262. [Google Scholar] [CrossRef]
- Chapman, R.; Botha, M. Neurodivergence-informed therapy. Developmental Medicine and Child Neurology 2023, 65, 310–317. [Google Scholar] [CrossRef]
- Tye, C.; Runicles, A.K.; Whitehouse, A.J.; Alvares, G.A. Characterizing the interplay between autism spectrum disorder and comorbid medical conditions: An integrative review. Frontiers in Psychiatry 2019, 9, 751. [Google Scholar] [CrossRef] [PubMed]
- Herrera-Mejía, J.; Ramos-Jiménez, A.; Jiménez-Vega, F.; Campos-Vega, R.; González-Córdova, A.F.; Wall-Medrano, A. Alimentación funcional para corregir desórdenes gastrointestinales asociados a trastornos del espectro autista: una revisión sistemática. Nutrición Hospitalaria 2022, 39, 663–677. [Google Scholar]
- Manivasagam, T.; Arunadevi, S.; Essa, M.M.; SaravanaBabu, C.; Borah, A.; Thenmozhi, A.J.; Qoronfleh, M.W. Role of oxidative stress and antioxidants in autism. Personalized Food Intervention and Therapy for Autism Spectrum Disorder Management 2020, 193–206. [Google Scholar]
- Karhu, E.; Zukerman, R.; Eshraghi, R.S.; Mittal, J.; Deth, R.C.; Castejon, A.M.; Trivedi, M.; Mittal, R.; Eshraghi, A.A. Nutritional interventions for autism spectrum disorder. Nutrition Reviews 2020, 78, 515–531. [Google Scholar] [CrossRef]
- Hopf, K.P.; Madren, E.; Santianni, K.A. Use and perceived effectiveness of complementary and alternative medicine to treat and manage the symptoms of autism in children: A survey of parents in a community population. Journal of Alternative and Complementary Medicine 2016, 22, 25–32. [Google Scholar] [CrossRef]
- Winburn, E.; Charlton, J.; McConachie, H.; McColl, E.; Parr, J.; O’Hare, A.; Baird, G.; Gringras, P.; Wilson, D.C.; Adamson, A.; Adams, S.; Le Couteur, A. Parents’ and child health professionals’ attitudes towards dietary interventions for children with Autism Spectrum Disorders. Journal of Autism and Developmental Disorders 2013, 44, 747–757. [Google Scholar] [CrossRef]
- Şenel, H.G. Parents’ views and experiences about complementary and alternative medicine treatments for their children with Autistic Spectrum Disorder. Journal of Autism and Developmental Disorders 2009, 40, 494–503. [Google Scholar] [CrossRef]
- Sivamaruthi, B.S.; Suganthy, N.; Kesika, P.; Chaiyasut, C. The role of microbiome, dietary supplements, and probiotics in Autism Spectrum Disorder. International Journal of Environmental Research and Public Health 2020, 17, 2647. [Google Scholar] [CrossRef] [PubMed]
- Zulkifli, M.N.; Kadar, M.; Fenech, M.; Hamzaid, N.H. Interrelation of food selectivity, oral sensory sensitivity, and nutrient intake in children with autism spectrum disorder: A scoping review. Research in Autism Spectrum Disorders 2022, 93, 101928. [Google Scholar] [CrossRef]
- Rodrigues, J.V.S.; Poli, M.C.F.; Petrilli, P.H.; Dornelles, R.C.M.; Turcio, K.H.; Theodoro, L.H. Food selectivity and neophobia in children with autism spectrum disorder and neurotypical development: a systematic review. Nutrition Reviews 2023, 81, 1034–1050. [Google Scholar] [CrossRef]
- Marí-Bauset, S.; Zazpe, I.; Mari-Sanchis, A.; Llopis-González, A.; Morales-Suárez-Varela, M. Food selectivity in autism spectrum disorders. Journal of Child Neurology 2014, 29, 1554–1561. [Google Scholar] [CrossRef]
- Page, S.D.; Souders, M.C.; Kral, T.V.E.; Chao, A.M.; Pinto-Martin, J. Correlates of feeding difficulties among children with Autism Spectrum Disorder: A systematic review. Journal of Autism and Developmental Disorders 2022, 52, 255–274. [Google Scholar] [CrossRef]
- Gerhant, A.; Olajossy, M.; Olajossy-Hilkesberger, L. Neuroanatomical, genetic and neurochemical aspects of infantile autism. Psychiatria Polska 2013, 47, 1101–1111. [Google Scholar] [PubMed]
- Masgutova, S.; Masgutov, D. Reflex integration disorder as a ne w treatment paradigm for children with autism. Svetlana Masgutova Educational Institute for Neuro-Sensory-Motor and Reflex Integration, SMEI 2015, 171-180.
- Hubbard, K.L.; Anderson, S.E.; Curtin, C.; Must, A.; Bandini, L.G. A comparison of food refusal related to characteristics of food in children with autism spectrum disorder and typically developing children. Journal of the Academy of Nutrition and Dietetics 2014, 114, 1981–1987. [Google Scholar] [CrossRef] [PubMed]
- Kozioł-Kozakowska, A.; Piórecka, B.; Schlegel-Zawadzka, M. Prevalence of food neophobia in pre-school children from southern Poland and its association with eating habits, dietary intake and anthropometric parameters: a cross-sectional study. Public Health Nutrition 2018, 21, 1106–1114. [Google Scholar] [CrossRef]
- Cermak, S.A.; Curtin, C.; Bandini, L.G. Food selectivity and sensory sensitivity in children with autism spectrum disorders. Journal of the American Dietetic Association 2010, 110, 238–246. [Google Scholar] [CrossRef]
- Bandini, L.G.; Curtin, C.; Phillips, S.; Anderson, S.E.; Maslin, M.; Must, A. Changes in food selectivity in children with autism spectrum disorder. Journal of Autism and Developmental Disorders 2017, 47, 439–446. [Google Scholar] [CrossRef]
- Kral, T.V.; Souders, M.C.; Tompkins, V.H.; Remiker, A.M.; Eriksen, W.T.; Pinto-Martin, J.A. Child eating behaviors and caregiver feeding practices in children with autism spectrum disorders. Public Health Nursing 2015, 32, 488–497. [Google Scholar] [CrossRef] [PubMed]
- Malhi, P.; Saini, S.; Bharti, B.; Attri, S.; Sankhyan, N. Sensory processing dysfunction and mealtime behavior problems in children with autism. Indian Pediatrics 2021, 58, 842–845. [Google Scholar] [CrossRef]
- Riccio, M.P.; Franco, C.; Negri, R.; Ferrentino, R.I.; Maresca, R.; D'alterio, E.; Greco, L.; Bravaccio, C. Is food refusal in autistic children related to TAS2R38 genotype? Autism Research 2018, 11, 531–538. [Google Scholar] [CrossRef]
- Nadon, G.; Feldman, D.E.; Dunn, W.; Gisel, E. Association of sensory processing and eating problems in children with autism spectrum disorders. Autism Research and Treatment 2011, 2011, 541926–541926. [Google Scholar] [CrossRef]
- Lafraire, J.; Rioux, C.; Giboreau, A.; Picard, D. Food rejections in children: Cognitive and social/environmental factors involved in food neophobia and picky/fussy eating behavior. Appetite 2016, 96, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Torres, T.d.O.; Gomes, D.R.; Mattos, M.P. Factors associated with food neophobia in children: systematic review. Revista Paulista de Pediatria :Ogao Oficial da Sociedade de Pediatria de Sao Paulo 2021, 39, e2020089–e2020089. [Google Scholar] [CrossRef] [PubMed]
- Sharp, W.G.; Postorino, V.; McCracken, C.E.; Berry, R.C.; Criado, K.K.; Burrell, T.L.; Scahill, L. Dietary intake, nutrient status, and growth parameters in children with autism spectrum disorder and severe food selectivity: An electronic medical record review. Journal of the Academy of Nutrition and Dietetics 2018, 118, 1943–1950. [Google Scholar] [CrossRef]
- Huxham, L.; Marais, M.; van Niekerk, E. Idiosyncratic food preferences of children with autism spectrum disorder in England. South African Journal of Clinical Nutrition 2021, 34, 90–96. [Google Scholar] [CrossRef]
- Rashid, A.; Iftikhar, N.; Badar, S.A.; Masood, F.; Rehman, I. Factors influencing food selectivity and food preferences of children with autism spectrum disorder. Journal of Pharmaceutical Research International 2021, 33, 152–159. [Google Scholar] [CrossRef]
- Webber, A.; Robinson, C.; Gray, H.L. Diet quality in children with Autism Spectrum Disorder. Journal of Nutrition Education and Behavior 2018, 50, S125–S126. [Google Scholar] [CrossRef]
- Vissoker, R.; Latzer, Y.; Stolar, O.; Rabenbach, A.; Gal, E. Eating problems and patterns among toddlers and young boys with and without autism spectrum disorders. Research in Autism Spectrum Disorders 2019, 59, 1–9. [Google Scholar] [CrossRef]
- Tomova, A.; Soltys, K.; Kemenyova, P.; Karhanek, M.; Babinska, K. The influence of food intake specificity in children with autism on gut microbiota. International Journal of Molecular Sciences 2020, 21, 2797. [Google Scholar] [CrossRef]
- Gorrindo, P.; Williams, K.C.; Lee, E.B.; Walker, L.S.; McGrew, S.G.; Levitt, P. Gastrointestinal dysfunction in autism: parental report, clinical evaluation, and associated factors. Autism Research: Official Journal of the International Society for Autism Research 2012, 5, 101–108. [Google Scholar] [CrossRef]
- Park, H.J.; Choi, S.J.; Kim, Y.; Park, J.; Kim, Y.-R.; Lee, S.-H.; Jung, S.J.; Cho, M.S.; Oh, J.E. Dietary behavior and food preferences according to age and the parents' nutrition education needs of children with autism spectrum disorder. Journal of the Korean Society of Food Culture 2020, 35, 241–255. [Google Scholar]
- Hsiao, E.Y. Gastrointestinal issues in autism spectrum disorder. Harvard Review of Psychiatry 2014, 22, 104–111. [Google Scholar] [CrossRef]
- Leader, G.; Abberton, C.; Cunningham, S.; Gilmartin, K.; Grudzien, M.; Higgins, E.; Joshi, L.; Whelan, S.; Mannion, A. Gastrointestinal symptoms in Autism Spectrum Disorder: A systematic review. Nutrients 2022, 14, 1471. [Google Scholar] [CrossRef]
- Prosperi, M.; Santocchi, E.; Balboni, G.; Narzisi, A.; Bozza, M.; Fulceri, F.; Apicella, F.; Igliozzi, R.; Cosenza, A.; Tancredi, R.; Calderoni, S.; Muratori, F. Behavioral phenotype of ASD preschoolers with gastrointestinal symptoms or food selectivity. Journal of Autism and Developmental Disorders 2017, 47, 3574–3588. [Google Scholar] [CrossRef]
- Esposito, M.; Sloan, J.; Nappo, R.; Fadda, R.; Fotia, F.; Napoli, E.; Mazzone, L.; Valeri, G.; Vicari, S. Sensory processing, gastrointestinal symptoms and parental feeding practices in the explanation of food selectivity: Clustering children with and without autism. International Journal of Autism and Related Disabilities 2019, 2019, 1–12. [Google Scholar]
- Leader, G.; O’Reilly, M.; Gilroy, S.P.; Chen, J.L.; Ferrari, C.; Mannion, A. Comorbid feeding and gastrointestinal symptoms, challenging behavior, sensory issues, adaptive functioning and quality of life in children and adolescents with autism spectrum disorder. Developmental Neurorehabilitation 2021, 24, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Settanni, C.R.; Bibbò, S.; Ianiro, G.; Rinninella, E.; Cintoni, M.; Mele, M.C.; Cammarota, G.; Gasbarrini, A. Gastrointestinal involvement of autism spectrum disorder: focus on gut microbiota. Expert Review of Gastroenterology and Hepatology 2021, 15, 599–622. [Google Scholar] [CrossRef]
- Sanctuary, M.R.; Kain, J.N.; Chen, S.Y.; Kalanetra, K.; Lemay, D.G.; Rose, D.R.; Yang, H.T.; Tancredi, D.J.; German, J.B.; Slupsky, C.M. Pilot study of probiotic/colostrum supplementation on gut function in children with autism and gastrointestinal symptoms. PloS one 2019, 14, e0210064. [Google Scholar] [CrossRef]
- Bjørklund, G.; Pivina, L.; Dadar, M.; Meguid, N.A.; Semenova, Y.; Anwar, M.; Chirumbolo, S. Gastrointestinal alterations in autism spectrum disorder: What do we know? Neuroscience & Biobehavioral Reviews 2020, 118, 111–120. [Google Scholar]
- Tomova, A.; Husarova, V.; Lakatosova, S.; Bakos, J.; Vlkova, B.; Babinska, K.; Ostatnikova, D. Gastrointestinal microbiota in children with autism in Slovakia. Physiology & Behavior 2015, 138, 179–187. [Google Scholar]
- Chaidez, V.; Hansen, R.L.; Hertz-Picciotto, I. Gastrointestinal problems in children with autism, developmental delays or typical development. Journal of Autism and Developmental Disorders 2014, 44, 1117–1127. [Google Scholar] [CrossRef]
- Liu, J.; Wan, G.-b.; Huang, M.-s.; Agyapong, G.; Zou, T.-l.; Zhang, X.-y.; Liu, Y.-W.; Song, Y.-q.; Tsai, Y.-C.; Kong, X.-j. Probiotic therapy for treating behavioral and gastrointestinal symptoms in autism spectrum disorder: a systematic review of clinical trials. Current Medical Science 2019, 39, 173–184. [Google Scholar] [CrossRef]
- Shaaban, S.Y.; El Gendy, Y.G.; Mehanna, N.S.; El-Senousy, W.M.; El-Feki, H.S.; Saad, K.; El-Asheer, O.M. The role of probiotics in children with autism spectrum disorder: A prospective, open-label study. Nutritional Neuroscience 2018, 21, 676–681. [Google Scholar] [CrossRef]
- Nogay, N.H.; Nahikian-Nelms, M. Can we reduce autism-related gastrointestinal and behavior problems by gut microbiota based dietary modulation? A review. Nutritional Neuroscience 2021, 24, 327–338. [Google Scholar] [CrossRef]
- de Magistris, L.; Picardi, A.; Siniscalco, D.; Riccio, M.P.; Sapone, A.; Cariello, R.; Abbadessa, S.; Medici, N.; Lammers, K.M.; Schiraldi, C.; Iardino, P.; Marotta, R.; Tolone, C.; Fasano, A.; Pascotto, A.; Bravaccio, C. Antibodies against food antigens in patients with autistic spectrum disorders. BioMed Research International 2013, 2013, 729349–729349. [Google Scholar] [CrossRef] [PubMed]
- De Magistris, L.; Familiari, V.; Pascotto, A.; Sapone, A.; Frolli, A.; Iardino, P.; Carteni, M.; De Rosa, M.; Francavilla, R.; Riegler, G. Alterations of the intestinal barrier in patients with autism spectrum disorders and in their first-degree relatives. Journal of Pediatric Gastroenterology and Nutrition 2010, 51, 418–424. [Google Scholar] [CrossRef]
- Buie, T.; Campbell, D.B.; Fuchs III, G.J.; Furuta, G.T.; Levy, J.; VandeWater, J.; Whitaker, A.H.; Atkins, D.; Bauman, M.L.; Beaudet, A.L. Evaluation, diagnosis, and treatment of gastrointestinal disorders in individuals with ASDs: a consensus report. Pediatrics 2010, 125, S1–S18. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Shen, W.; Yao, H.; Zheng, R.; Chen, W.; Zhang, W. Association between Autism Spectrum Disorder and Food Allergy: A Systematic Review and Meta-analysis. Autism Research 2021, 14, 220–230. [Google Scholar]
- Al-Beltagi, M. Autism medical comorbidities. World Journal of Clinical Pediatrics 2021, 10, 15. [Google Scholar] [PubMed]
- Liu, X.; Lin, J.; Zhang, H.; Khan, N.U.; Zhang, J.; Tang, X.; Cao, X.; Shen, L. Oxidative stress in autism spectrum disorder—current progress of mechanisms and biomarkers. Frontiers in Psychiatry 2022, 13, 813304. [Google Scholar] [CrossRef]
- Membrino, V.; Di Paolo, A.; Alia, S.; Papiri, G.; Vignini, A. The Role of Oxidative Stress in Autism Spectrum Disorder: A Narrative Literature Review. Oxygen 2023, 3, 34–44. [Google Scholar] [CrossRef]
- Banerjee, J.; Das, A.; Sinha, M.; Saha, S. Biological efficacy of medicinal plant extracts in preventing oxidative damage. Oxidative Medicine and Cellular Longevity 2018, 2018. [Google Scholar] [CrossRef] [PubMed]
- Tsatsakis, A.; Docea, A.O.; Calina, D.; Tsarouhas, K.; Zamfira, L.-M.; Mitrut, R.; Sharifi-Rad, J.; Kovatsi, L.; Siokas, V.; Dardiotis, E. A mechanistic and pathophysiological approach for stroke associated with drugs of abuse. Journal of Clinical Medicine 2019, 8, 1295. [Google Scholar] [CrossRef] [PubMed]
- Pangrazzi, L.; Balasco, L.; Bozzi, Y. Oxidative stress and immune system dysfunction in autism spectrum disorders. International Journal of Molecular Sciences 2020, 21, 3293. [Google Scholar] [CrossRef] [PubMed]
- Morimoto, M.; Hashimoto, T.; Tsuda, Y.; Nakatsu, T.; Kitaoka, T.; Kyotani, S. Assessment of oxidative stress in autism spectrum disorder using reactive oxygen metabolites and biological antioxidant potential. PloS one 2020, 15, e0233550–e0233550. [Google Scholar] [CrossRef] [PubMed]
- Usui, N.; Iwata, K.; Miyachi, T.; Takagai, S.; Wakusawa, K.; Nara, T.; Tsuchiya, K.J.; Matsumoto, K.; Kurita, D.; Kameno, Y. VLDL-specific increases of fatty acids in autism spectrum disorder correlate with social interaction. EBioMedicine 2020, 58. [Google Scholar] [CrossRef] [PubMed]
- Burke, S.L.; Cobb, J.; Agarwal, R.; Maddux, M.; Cooke, M.S. How robust is the evidence for a role of oxidative stress in autism spectrum disorders and intellectual disabilities? Journal of Autism and Developmental Disorders 2021, 51, 1428–1445. [Google Scholar] [CrossRef] [PubMed]
- Bjørklund, G.; Meguid, N.A.; El-Bana, M.A.; Tinkov, A.A.; Saad, K.; Dadar, M.; Hemimi, M.; Skalny, A.V.; Hosnedlová, B.; Kizek, R. Oxidative stress in autism spectrum disorder. Molecular Neurobiology 2020, 57, 2314–2332. [Google Scholar] [CrossRef]
- Chauhan, A.; Chauhan, V.; Brown, W.T.; Cohen, I. Oxidative stress in autism: Increased lipid peroxidation and reduced serum levels of ceruloplasmin and transferrin-the antioxidant proteins. Life Sciences 2004, 75, 2539–2549. [Google Scholar] [CrossRef]
- Zoroglu, S.S.; Armutcu, F.; Ozen, S.; Gurel, A.; Sivasli, E.; Yetkin, O.; Meram, I. Increased oxidative stress and altered activities of erythrocyte free radical scavenging enzymes in autism. European Archives of Psychiatry and Clinical Neuroscience 2004, 254, 143–147. [Google Scholar] [CrossRef]
- Rose, S.; Melnyk, S.; Pavliv, O.; Bai, S.; Nick, T.; Frye, R.; James, S. Evidence of oxidative damage and inflammation associated with low glutathione redox status in the autism brain. Translational Psychiatry 2012, 2, e134–e134. [Google Scholar] [CrossRef] [PubMed]
- Söğüt, S.; Zoroğlu, S.S.; Özyurt, H.; Yılmaz, H.R.; Özuğurlu, F.; Sivaslı, E.; Yetkin, Ö.; Yanık, M.; Tutkun, H.; Savaş, H.A. Changes in nitric oxide levels and antioxidant enzyme activities may have a role in the pathophysiological mechanisms involved in autism. Clinica Chimica Acta 2003, 331, 111–117. [Google Scholar] [CrossRef]
- Chauhan, A.; Gu, F.; Essa, M.M.; Wegiel, J.; Kaur, K.; Brown, W.T.; Chauhan, V. Brain region-specific deficit in mitochondrial electron transport chain complexes in children with autism. Journal of Neurochemistry 2011, 117, 209–220. [Google Scholar] [CrossRef]
- Al-Mosalem, O.; El-Ansary, A.; Attas, O.; Al-Ayadhi, L. Metabolic biomarkers related to energy metabolism in Saudi autistic children. Clinical Biochemistry 2009, 42, 949–957. [Google Scholar] [CrossRef]
- Aranburu, E.; Matias, S.; Simón, E.; Larretxi, I.; Martínez, O.; Bustamante, M.Á.; Fernández-Gil, M.D.P.; Miranda, J. Gluten and FODMAPs relationship with mental disorders: Systematic review. Nutrients 2021, 13, 1894. [Google Scholar] [CrossRef]
- Wang, X.; Michaelis, E.K. Selective neuronal vulnerability to oxidative stress in the brain. Frontiers in Aging Neuroscience 2010, 2, 1224. [Google Scholar] [CrossRef]
- Rossignol, D.A.; Frye, R.E. Evidence linking oxidative stress, mitochondrial dysfunction, and inflammation in the brain of individuals with autism. Frontiers in Physiology 2014, 5, 150. [Google Scholar] [CrossRef] [PubMed]
- Morakotsriwan, N.; Wattanathorn, J.; Kirisattayakul, W.; Chaisiwamongkol, K. Autistic-like behaviors, oxidative stress status, and histopathological changes in cerebellum of valproic acid rat model of autism are improved by the combined extract of purple rice and silkworm pupae. Oxidative Medicine and Cellular Longevity 2016, 2016, 3206561. [Google Scholar] [CrossRef]
- Hirai, T.; Usui, N.; Iwata, K.; Miyachi, T.; Tsuchiya, K.J.; Xie, M.-J.; Nakamura, K.; Tsujii, M.; Sugiyama, T.; Matsuzaki, H. Increased plasma lipoprotein lipase activity in males with autism spectrum disorder. Research in Autism Spectrum Disorders 2020, 77, 101630. [Google Scholar] [CrossRef]
- Hirayama, A.; Wakusawa, K.; Fujioka, T.; Iwata, K.; Usui, N.; Kurita, D.; Kameno, Y.; Wakuda, T.; Takagai, S.; Hirai, T.; Nara, T.; Ito, H.; Nagano, Y.; Oowada, S.; Tsujii, M.; Tsuchiya, K.J.; Matsuzaki, H. Simultaneous evaluation of antioxidative serum profiles facilitates the diagnostic screening of autism spectrum disorder in under-6-year-old children. Scientific Reports 2020, 10, 20602–20602. [Google Scholar] [CrossRef] [PubMed]
- Sackesen, C.; Ercan, H.; Dizdar, E.; Soyer, O.; Gumus, P.; Tosun, B.N.; Büyüktuncer, Z.; Karabulut, E.; Besler, T.; Kalayci, O. A comprehensive evaluation of the enzymatic and nonenzymatic antioxidant systems in childhood asthma. Journal of Allergy and Clinical Immunology 2008, 122, 78–85. [Google Scholar] [CrossRef]
- Xu, G.; Snetselaar, L.G.; Jing, J.; Liu, B.; Strathearn, L.; Bao, W. Association of food allergy and other allergic conditions with autism spectrum disorder in children. JAMA Network Open 2018, 1, e180279–e180279. [Google Scholar] [CrossRef]
- Curieses Andrés, C.M.; Pérez de la Lastra, J.M.; Juan, C.A.; Plou, F.J.; Pérez-Lebeña, E. Antioxidant metabolism pathways in vitamins, polyphenols, and selenium: Parallels and divergences. International Journal of Molecular Sciences 2024, 25, 2600. [Google Scholar] [CrossRef] [PubMed]
- Sharifi-Rad, M.; Anil Kumar, N.V.; Zucca, P.; Varoni, E.M.; Dini, L.; Panzarini, E.; Rajkovic, J.; Tsouh Fokou, P.V.; Azzini, E.; Peluso, I. Lifestyle, oxidative stress, and antioxidants: back and forth in the pathophysiology of chronic diseases. Frontiers in Physiology 2020, 11, 694. [Google Scholar] [CrossRef]
- Lazzarino, G.; Listorti, I.; Bilotta, G.; Capozzolo, T.; Amorini, A.M.; Longo, S.; Caruso, G.; Lazzarino, G.; Tavazzi, B.; Bilotta, P. Water- and fat-soluble antioxidants in human seminal plasma and serum of fertile males. Antioxidants 2019, 8, 96. [Google Scholar] [CrossRef] [PubMed]
- Bjørklund, G.; Shanaida, M.; Lysiuk, R.; Butnariu, M.; Peana, M.; Sarac, I.; Strus, O.; Smetanina, K.; Chirumbolo, S. Natural compounds and products from an anti-aging perspective. Molecules 2022, 27, 7084. [Google Scholar] [CrossRef] [PubMed]
- Murdaca, G.; Gangemi, S. Vitamin D in health and disease. Biomedicines 2022, 11, 10. [Google Scholar] [CrossRef] [PubMed]
- Ebadi, M.; Mohammadi, M.; Pezeshki, A.; Jafari, S.M. , Health benefits of beta-carotene. In Handbook of food bioactive ingredients: properties and applications, Springer: 2023; pp 1-26.
- Puebla-Duarte, A.L.; Santos-Sauceda, I.; Rodríguez-Félix, F.; Iturralde-García, R.D.; Fernández-Quiroz, D.; Pérez-Cabral, I.D.; Del-Toro-Sánchez, C.L. Active and Intelligent Packaging: A Review of the Possible Application of Cyclodextrins in Food Storage and Safety Indicators. Polymers 2023, 15, 4317. [Google Scholar] [CrossRef] [PubMed]
- Burri, B.J.; Chang, J.S.T.; Neidlinger, T.R. β-Cryptoxanthin- and α-carotene-rich foods have greater apparent bioavailability than β-carotene-rich foods in Western diets. British Journal of Nutrition 2011, 105, 212–219. [Google Scholar] [CrossRef]
- Burri, B.J.; La Frano, M.R.; Zhu, C. Absorption, metabolism, and functions of β-cryptoxanthin. Nutrition Reviews 2016, 74, 69–82. [Google Scholar] [CrossRef]
- Kaviarasan, K.; Pugalendi, K.V. Influence of flavonoid-rich fraction from Spermacoce hispida seed on PPAR-alpha gene expression, antioxidant redox status, protein metabolism and marker enzymes in high-fat-diet fed STZ diabetic rats. Journal of Basic and Clinical Physiology and Pharmacology 2009, 20, 141–158. [Google Scholar] [CrossRef] [PubMed]
- Liga, S.; Paul, C.; Péter, F. Flavonoids: Overview of biosynthesis, biological activity, and current extraction techniques. Plants (Basel, Switzerland) 2023, 12, 2732. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Cao, H.; Huang, Q.; Xiao, J.; Teng, H. Absorption, metabolism and bioavailability of flavonoids: A review. Critical Reviews in Food Science and Nutrition 2022, 62, 7730–7742. [Google Scholar] [CrossRef]
- Panche, A.N.; Diwan, A.D.; Chandra, S.R. Flavonoids: an overview. Journal of Nutritional Science 2016, 5, e47. [Google Scholar] [CrossRef]
- Amogne, N.Y.; Ayele, D.W.; Tsigie, Y.A. Recent advances in anthocyanin dyes extracted from plants for dye sensitized solar cell. Materials for Renewable and Sustainable Energy 2020, 9, 23. [Google Scholar] [CrossRef]
- Khoo, H.E.; Azlan, A.; Tang, S.T.; Lim, S.M. Anthocyanidins and anthocyanins: colored pigments as food, pharmaceutical ingredients, and the potential health benefits. Food and Nutrition Research 2017, 61, 1361779–1361779. [Google Scholar] [CrossRef]
- Catarino, M.; Alves-Silva, J.; Pereira, O.; Cardoso, S. Antioxidant capacities of flavones and benefits in oxidative-stress related diseases. Current Topics in Medicinal Chemistry 2014, 15, 105–119. [Google Scholar] [CrossRef]
- Luo, Y.; Jian, Y.; Liu, Y.; Jiang, S.; Muhammad, D.; Wang, W. Flavanols from nature: A phytochemistry and biological activity review. Molecules 2022, 27, 719. [Google Scholar] [CrossRef]
- Deepika; Maurya, P. K. Health benefits of quercetin in age-related diseases. Molecules (Basel, Switzerland) 2022, 27, 2498. [Google Scholar] [CrossRef]
- Mahmud, A.R.; Ema, T.I.; Siddiquee, M.F.-R.; Shahriar, A.; Ahmed, H.; Mosfeq-Ul-Hasan, M.; Rahman, N.; Islam, R.; Uddin, M.R.; Mizan, M.F.R. Natural flavonols: actions, mechanisms, and potential therapeutic utility for various diseases. Beni-Suef University Journal of Basic and Applied Sciences 2023, 12, 47–47. [Google Scholar] [CrossRef]
- Brahmachari, G. Naturally occurring flavanones: An overview. Natural Product Communications 2008, 3, 1934578X0800300. [Google Scholar] [CrossRef]
- Křížová, L.; Dadáková, K.; Kašparovská, J.; Kašparovský, T. Isoflavones. Molecules (Basel, Switzerland) 2019, 24, 1076. [Google Scholar] [CrossRef]
- Indika, N.-L.R.; Frye, R.E.; Rossignol, D.A.; Owens, S.C.; Senarathne, U.D.; Grabrucker, A.M.; Perera, R.; Engelen, M.P.K.J.; Deutz, N.E.P. The rationale for vitamin, mineral, and cofactor treatment in the precision medical care of Autism Spectrum Disorder. Journal of Personalized Medicine 2023, 13, 252. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Liu, X.; Xiong, X.-Q.; Yang, T.; Cui, T.; Hou, N.-L.; Lai, X.; Liu, S.; Guo, M.; Liang, X.-H.; Cheng, Q.; Chen, J.; Li, T.-Y. Effect of vitamin A supplementation on gut microbiota in children with autism spectrum disorders - a pilot study. BMC Microbiology 2017, 17, 204–204. [Google Scholar] [CrossRef] [PubMed]
- Guo, M.; Zhu, J.; Yang, T.; Lai, X.; Lei, Y.; Chen, J.; Li, T. Vitamin A and vitamin D deficiencies exacerbate symptoms in children with autism spectrum disorders. Nutritional Neuroscience 2018, 22, 637–647. [Google Scholar] [CrossRef] [PubMed]
- Bastos Maia, S.; Costa Caminha, M.d.F.; Lins da Silva, S.; Rolland Souza, A.S.; Carvalho Dos Santos, C.; Batista Filho, M. The prevalence of vitamin A deficiency and associated factors in pregnant women receiving prenatal care at a reference maternity hospital in northeastern Brazil. Nutrients 2018, 10, 1271. [Google Scholar] [CrossRef]
- Liu, X.; Liu, J.; Xiong, X.; Yang, T.; Hou, N.; Liang, X.; Chen, J.; Cheng, Q.; Li, T. Correlation between nutrition and symptoms: Nutritional survey of children with Autism Spectrum Disorder in Chongqing, China. Nutrients 2016, 8, 294. [Google Scholar] [CrossRef] [PubMed]
- Berger, M.M.; Shenkin, A.; Schweinlin, A.; Amrein, K.; Augsburger, M.; Biesalski, H.-K.; Bischoff, S.C.; Casaer, M.P.; Gundogan, K.; Lepp, H.-L. ESPEN micronutrient guideline. Clinical Nutrition 2022, 41, 1357–1424. [Google Scholar] [CrossRef]
- Wang, Y.; Liu, X.J.; Robitaille, L.; Eintracht, S.; MacNamara, E.; Hoffer, L.J. Effects of vitamin C and vitamin D administration on mood and distress in acutely hospitalized patients. The American Journal of Clinical Nutrition 2013, 98, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Figueroa-Méndez, R.; Rivas-Arancibia, S. Vitamin C in health and disease: Its role in the metabolism of cells and redox state in the brain. Frontiers in Physiology 2015, 6, 397–397. [Google Scholar] [CrossRef]
- Krajcovicova-Kudlackova, M.; Valachovicova, M.; Mislanova, C.; Hudecova, Z.; Sustrova, M.; Ostatnikova, D. Plasma concentrations of selected antioxidants in autistic children and adolescents. Bratislavske Lekarske Listy 2009, 110, 247–250. [Google Scholar]
- Adams, J.B.; Audhya, T.; McDonough-Means, S.; Rubin, R.A.; Quig, D.; Geis, E.; Gehn, E.; Loresto, M.; Mitchell, J.; Atwood, S. Effect of a vitamin/mineral supplement on children and adults with autism. BMC Pediatrics 2011, 11, 1–30. [Google Scholar] [CrossRef] [PubMed]
- Bjørklund, G.; Waly, M.I.; Al-Farsi, Y.; Saad, K.; Dadar, M.; Rahman, M.M.; Elhoufey, A.; Chirumbolo, S.; Jóźwik-Pruska, J.; Kałużna-Czaplińska, J. The role of vitamins in autism spectrum disorder: what do we know? Journal of Molecular Neuroscience 2019, 67, 373–387. [Google Scholar] [CrossRef]
- Meguid, N.A.; Bjørklund, G.; Gebril, O.H.; Doşa, M.D.; Anwar, M.; Elsaeid, A.; Gaber, A.; Chirumbolo, S. The role of zinc supplementation on the metallothionein system in children with autism spectrum disorder. Acta Neurologica Belgica 2019, 119, 577–583. [Google Scholar] [CrossRef] [PubMed]
- ClinicalTrials.gov. https://clinicaltrials.gov/ct2/show/NCT00889538 (July),.
- Önal, S.; Sachadyn-Król, M.; Kostecka, M. A review of the nutritional approach and the role of dietary components in children with autism spectrum disorders in light of the latest scientific research. Nutrients 2023, 15, 4852. [Google Scholar] [CrossRef]
- Serra, D.; Henriques, J.F.; Sousa, F.J.; Laranjo, M.; Resende, R.; Ferreira-Marques, M.; de Freitas, V.; Silva, G.; Peça, J.; Dinis, T.C. Attenuation of autism-like behaviors by an anthocyanin-rich extract from portuguese blueberries via microbiota–gut–brain axis modulation in a valproic acid mouse model. International Journal of Molecular Sciences 2022, 23, 9259. [Google Scholar] [CrossRef]
- Wang, H.; Hu, L.; Peng, L.; Du, J.; Lan, M.; Cheng, Y.; Ma, L.; Zhang, Y. Dual encapsulation of β-carotene by β-cyclodextrin and chitosan for 3D printing application. Food Chemistry 2022, 378, 132088. [Google Scholar] [CrossRef] [PubMed]
- Cai, Z.; Chen, F.; Wang, Y.; Wang, X.; Yang, X.; Zhang, C. Lycopene maintains mitochondrial homeostasis to counteract the enterotoxicity of deoxynivalenol. Antioxidants 2023, 12, 1958. [Google Scholar] [CrossRef]
- Salehi, B.; Rescigno, A.; Dettori, T.; Calina, D.; Docea, A.O.; Singh, L.; Cebeci, F.; Özçelik, B.; Bhia, M.; Dowlati Beirami, A.; Sharifi-Rad, J.; Sharopov, F.; Cho, W.C.; Martins, N. Avocado-soybean unsaponifiables: A panoply of potentialities to be exploited. Biomolecules 2020, 10, 130. [Google Scholar] [CrossRef]
- Reissmann, A. Gluten-free and casein-free diets in the management of autism spectrum disorder: A systematic literature review. Movement and Nutrition in Health and Disease 2020, 4. [Google Scholar]
- González-Domenech, P.J.; Diaz-Atienza, F.; Gutiérrez-Rojas, L.; Fernández-Soto, M.L.; González-Domenech, C.M. A narrative review about autism spectrum disorders and exclusion of gluten and casein from the diet. Nutrients 2022, 14, 1797. [Google Scholar] [CrossRef] [PubMed]
- Quan, L.; Xu, X.; Cui, Y.; Han, H.; Hendren, R.L.; Zhao, L.; You, X. A systematic review and meta-analysis of the benefits of a gluten-free diet and/or casein-free diet for children with autism spectrum disorder. Nutrition Reviews 2022, 80, 1237–1246. [Google Scholar] [CrossRef] [PubMed]
- Fattorusso, A.; Di Genova, L.; Dell’Isola, G.B.; Mencaroni, E.; Esposito, S. Autism spectrum disorders and the gut microbiota. Nutrients 2019, 11, 521. [Google Scholar] [CrossRef]
- Jyonouchi, H.; Sun, S.; Itokazu, N. Innate immunity associated with inflammatory responses and cytokine production against common dietary proteins in patients with Autism Spectrum Disorder. Neuropsychobiology 2002, 46, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Herbert, M.R.; Buckley, J.A. Autism and Dietary Therapy. Journal of Child Neurology 2013, 28, 975–982. [Google Scholar] [CrossRef]
- Keller, A.; Rimestad, M.L.; Friis Rohde, J.; Holm Petersen, B.; Bruun Korfitsen, C.; Tarp, S.; Briciet Lauritsen, M.; Händel, M.N. The effect of a combined gluten- and casein-free diet on children and adolescents with autism spectrum disorders: A systematic review and meta-analysis. Nutrients 2021, 13, 470. [Google Scholar] [CrossRef]
- Saravia, L.; González-Zapata, L.I.; Rendo-Urteaga, T.; Ramos, J.; Collese, T.S.; Bove, I.; Delgado, C.; Tello, F.; Iglesia, I.; Gonçalves Sousa, E.D.; De Moraes, A.C.F.; Carvalho, H.B.; Moreno, L.A. Development of a food frequency questionnaire for assessing dietary intake in children and adolescents in South America. Obesity 2018, 26. [Google Scholar] [CrossRef] [PubMed]
- Whiteley, P.; Haracopos, D.; Knivsberg, A.-M.; Reichelt, K.L.; Parlar, S.; Jacobsen, J.; Seim, A.; Pedersen, L.; Schondel, M.; Shattock, P. The ScanBrit randomised, controlled, single-blind study of a gluten- and casein-free dietary intervention for children with autism spectrum disorders. Nutritional Neuroscience 2010, 13, 87–100. [Google Scholar] [CrossRef] [PubMed]
- Elder, J.H.; Shankar, M.; Shuster, J.; Theriaque, D.; Burns, S.; Sherrill, L. The gluten-free, casein-free diet in autism: results of a preliminary double blind clinical trial. Journal of Autism and Developmental Disorders 2006, 36, 413–420. [Google Scholar] [CrossRef]
- Johnson, C.R.; Handen, B.L.; Zimmer, M.; Sacco, K.; Turner, K. Effects of gluten free / casein free diet in young children with autism: A pilot study. Journal of Developmental and Physical Disabilities 2010, 23, 213–225. [Google Scholar] [CrossRef]
- Navarro, F.; Pearson, D.A.; Fatheree, N.; Mansour, R.; Hashmi, S.S.; Rhoads, J.M. Are ‘leaky gut’ and behavior associated with gluten and dairy containing diet in children with autism spectrum disorders? Nutritional Neuroscience 2015, 18, 177–185. [Google Scholar] [CrossRef]
- Pusponegoro, H.D.; Ismael, S.; Firmansyah, A.; Sastroasmoro, S.; Vandenplas, Y. Gluten and casein supplementation does not increase symptoms in children with autism spectrum disorder. Acta Paediatrica 2015, 104. [Google Scholar] [CrossRef]
- González-Domenech, P.J.; Díaz Atienza, F.; García Pablos, C.; Fernández Soto, M.L.; Martínez-Ortega, J.M.; Gutiérrez-Rojas, L. Influence of a combined gluten-free and casein-free diet on behavior disorders in children and adolescents diagnosed with autism spectrum disorder: a 12-month follow-up clinical trial. Journal of Autism and Developmental Disorders 2020, 50, 935–948. [Google Scholar] [CrossRef]
- Hyman, S.L.; Stewart, P.A.; Foley, J.; Cain, U.; Peck, R.; Morris, D.D.; Wang, H.; Smith, T. The gluten-free/casein-free diet: a double-blind challenge trial in children with autism. Journal of Autism and Developmental Disorders 2016, 46, 205–220. [Google Scholar] [CrossRef]
- Piwowarczyk, A.; Horvath, A.; Pisula, E.; Kawa, R.; Szajewska, H. Gluten-free diet in children with Autism Spectrum Disorders: A randomized, controlled, single-blinded trial. Journal of Autism and Developmental Disorders 2019, 50, 482–490. [Google Scholar] [CrossRef] [PubMed]
- Whiteley, P.; Rodgers, J.; Savery, D.; Shattock, P. A Gluten-free diet as an intervention for autism and associated spectrum disorders: Preliminary findings. Autism 1999, 3, 45–65. [Google Scholar] [CrossRef]
- Pennesi, C.M.; Klein, L.C. Effectiveness of the gluten-free, casein-free diet for children diagnosed with autism spectrum disorder: Based on parental report. Nutritional Neuroscience 2012, 15, 85–91. [Google Scholar] [CrossRef]
- Alamri, E.S. Efficacy of gluten- and casein-free diets on autism spectrum disorders in children. Saudi Medical Journal 2020, 41, 1041–1046. [Google Scholar] [CrossRef]
- Ruan, Y.; Chen, L.; She, D.; Chung, Y.; Ge, L.; Han, L. Ketogenic diet for epilepsy: an overview of systematic review and meta-analysis. European Journal of Clinical Nutrition 2022, 76, 1234–1244. [Google Scholar] [CrossRef]
- Mu, C.; Corley, M.J.; Lee, R.W.Y.; Wong, M.; Pang, A.; Arakaki, G.; Miyamoto, R.; Rho, J.M.; Mickiewicz, B.; Dowlatabadi, R.; Vogel, H.J.; Korchemagin, Y.; Shearer, J. Metabolic framework for the improvement of Autism Spectrum Disorders by a modified ketogenic diet: A pilot study. Journal of Proteome Research 2020, 19, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.W.Y.; Corley, M.J.; Pang, A.; Arakaki, G.; Abbott, L.; Nishimoto, M.; Miyamoto, R.; Lee, E.; Yamamoto, S.; Maunakea, A.K.; Lum-Jones, A.; Wong, M. A modified ketogenic gluten-free diet with MCT improves behavior in children with autism spectrum disorder. Physiology & Behavior 2018, 188, 205–211. [Google Scholar]
- Castro, K.; Faccioli, L.S.; Baronio, D.; Gottfried, C.; Perry, I.S.; dos Santos Riesgo, R. Effect of a ketogenic diet on autism spectrum disorder: A systematic review. Research in Autism Spectrum Disorders 2015, 20, 31–38. [Google Scholar] [CrossRef]
- Vera-González, A. , Pathophysiological mechanisms underlying the etiologies of seizures and epilepsy. In Epilepsy, Exon Publications: 2022.
- Liu, X.; Sun, X.; Sun, C.; Zou, M.; Chen, Y.; Huang, J.; Wu, L.; Chen, W.-X. Prevalence of epilepsy in autism spectrum disorders: A systematic review and meta-analysis. Autism 2021, 26, 33–50. [Google Scholar] [CrossRef] [PubMed]
- Evangeliou, A.; Vlachonikolis, I.; Mihailidou, H.; Spilioti, M.; Skarpalezou, A.; Makaronas, N.; Prokopiou, A.; Christodoulou, P.; Liapi-Adamidou, G.; Helidonis, E.; Sbyrakis, S.; Smeitink, J. Application of a Ketogenic Diet in Children With Autistic Behavior: Pilot Study. Journal of Child Neurology 2003, 18, 113–118. [Google Scholar] [CrossRef] [PubMed]
- El-Rashidy, O.; El-Baz, F.; El-Gendy, Y.; Khalaf, R.; Reda, D.; Saad, K. Ketogenic diet versus gluten free casein free diet in autistic children: a case-control study. Metabolic Brain Disease 2017, 32, 1935–1941. [Google Scholar] [CrossRef] [PubMed]
- Maalouf, M.; Sullivan, P.G.; Davis, L.; Kim, D.Y.; Rho, J.M. Ketones inhibit mitochondrial production of reactive oxygen species production following glutamate excitotoxicity by increasing NADH oxidation. Neuroscience 2007, 145, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Mori, T.A. Marine OMEGA-3 fatty acids in the prevention of cardiovascular disease. Fitoterapia 2017, 123, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Edemann-Callesen, H.; Bernhardt, N.; Hlusicka, E.B.; Hintz, F.; Habelt, B.; Winter, R.; Neubert, I.; Pelz, M.; Filla, A.; Soto-Montenegro, M.L.; Winter, C.; Hadar, R. Supplement treatment with NAC and omega-3 polyunsaturated fatty acids during pregnancy partially prevents schizophrenia-related outcomes in the poly i:c rat model. Antioxidants 2023, 12, 1068. [Google Scholar] [CrossRef] [PubMed]
- Mehdi, S.; Manohar, K.; Shariff, A.; Kinattingal, N.; Wani, S.U.D.; Alshehri, S.; Imam, M.T.; Shakeel, F.; Krishna, K.L. Omega-3 fatty acids supplementation in the treatment of depression: An observational study. Journal of Personalized Medicine 2023, 13, 224. [Google Scholar] [CrossRef]
- DiNicolantonio, J.J.; O'Keefe, J.H. The importance of marine omega-3s for brain development and the prevention and treatment of behavior, mood, and other brain disorders. Nutrients 2020, 12, 2333. [Google Scholar] [CrossRef]
- Amminger, G.P.; Berger, G.E.; Schäfer, M.R.; Klier, C.; Friedrich, M.H.; Feucht, M. Omega-3 fatty acids supplementation in children with autism: A double-blind randomized, placebo-controlled pilot study. Biological Psychiatry 2007, 61, 551–553. [Google Scholar] [CrossRef] [PubMed]
- Mazahery, H.; Stonehouse, W.; Delshad, M.; Kruger, M.C.; Conlon, C.A.; Beck, K.L.; von Hurst, P.R. Relationship between Long Chain n-3 Polyunsaturated Fatty Acids and Autism Spectrum Disorder: Systematic Review and Meta-Analysis of Case-Control and Randomised Controlled Trials. Nutrients 2017, 9, 155. [Google Scholar] [CrossRef] [PubMed]
- Siafis, S.; Çıray, O.; Wu, H.; Schneider-Thoma, J.; Bighelli, I.; Krause, M.; Rodolico, A.; Ceraso, A.; Deste, G.; Huhn, M.; Fraguas, D.; San José Cáceres, A.; Mavridis, D.; Charman, T.; Murphy, D.G.; Parellada, M.; Arango, C.; Leucht, S. Pharmacological and dietary-supplement treatments for autism spectrum disorder: a systematic review and network meta-analysis. Molecular autism 2022, 13, 10–10. [Google Scholar] [CrossRef] [PubMed]
Figure 2.
Diagram of affected activities in an increased oxidative stress in children with Autism Spectrum Disorder.
Figure 2.
Diagram of affected activities in an increased oxidative stress in children with Autism Spectrum Disorder.
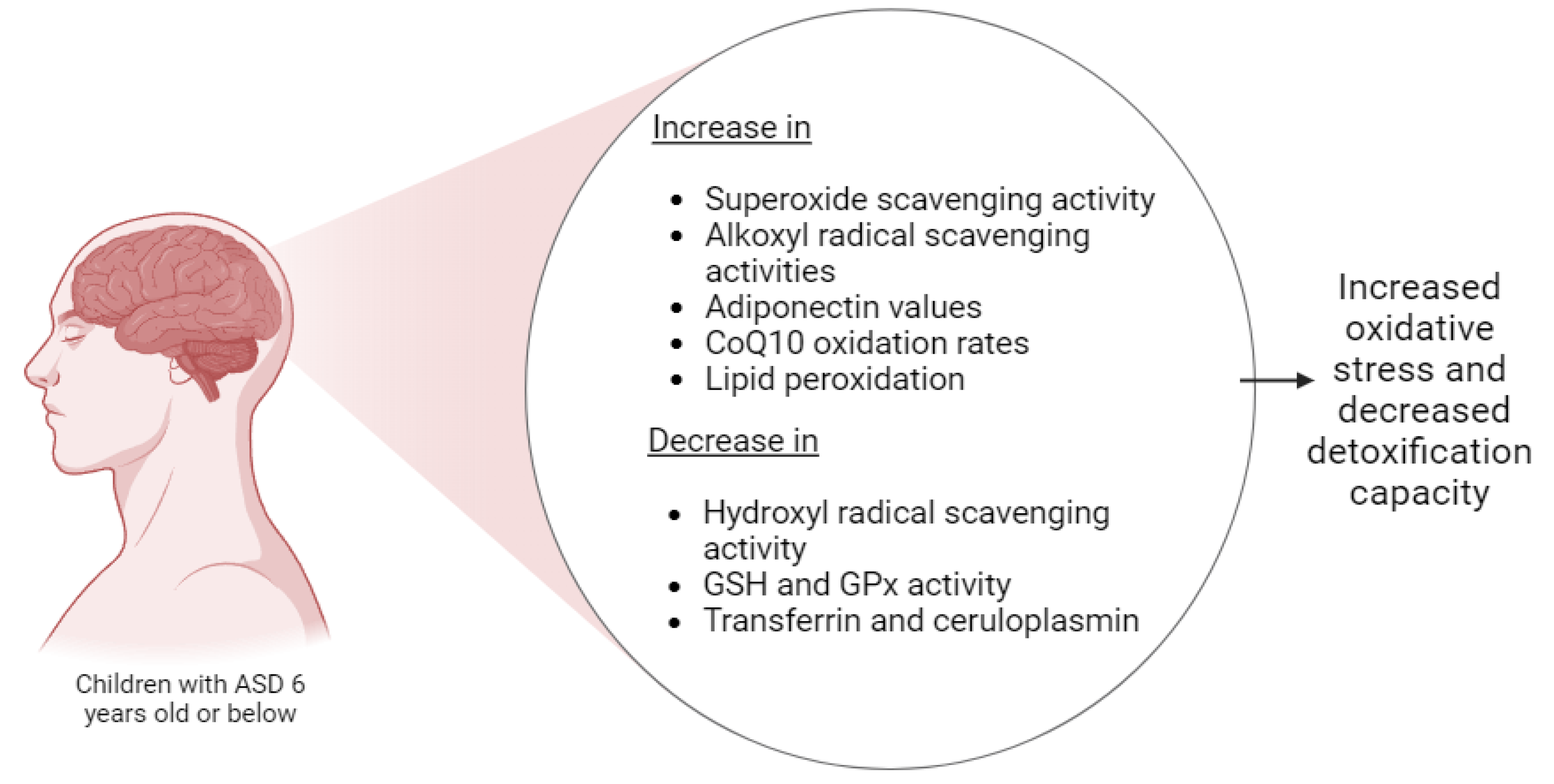
Figure 3.
Chemical structures of carotenoids, phenols, and main antioxidant vitamins.
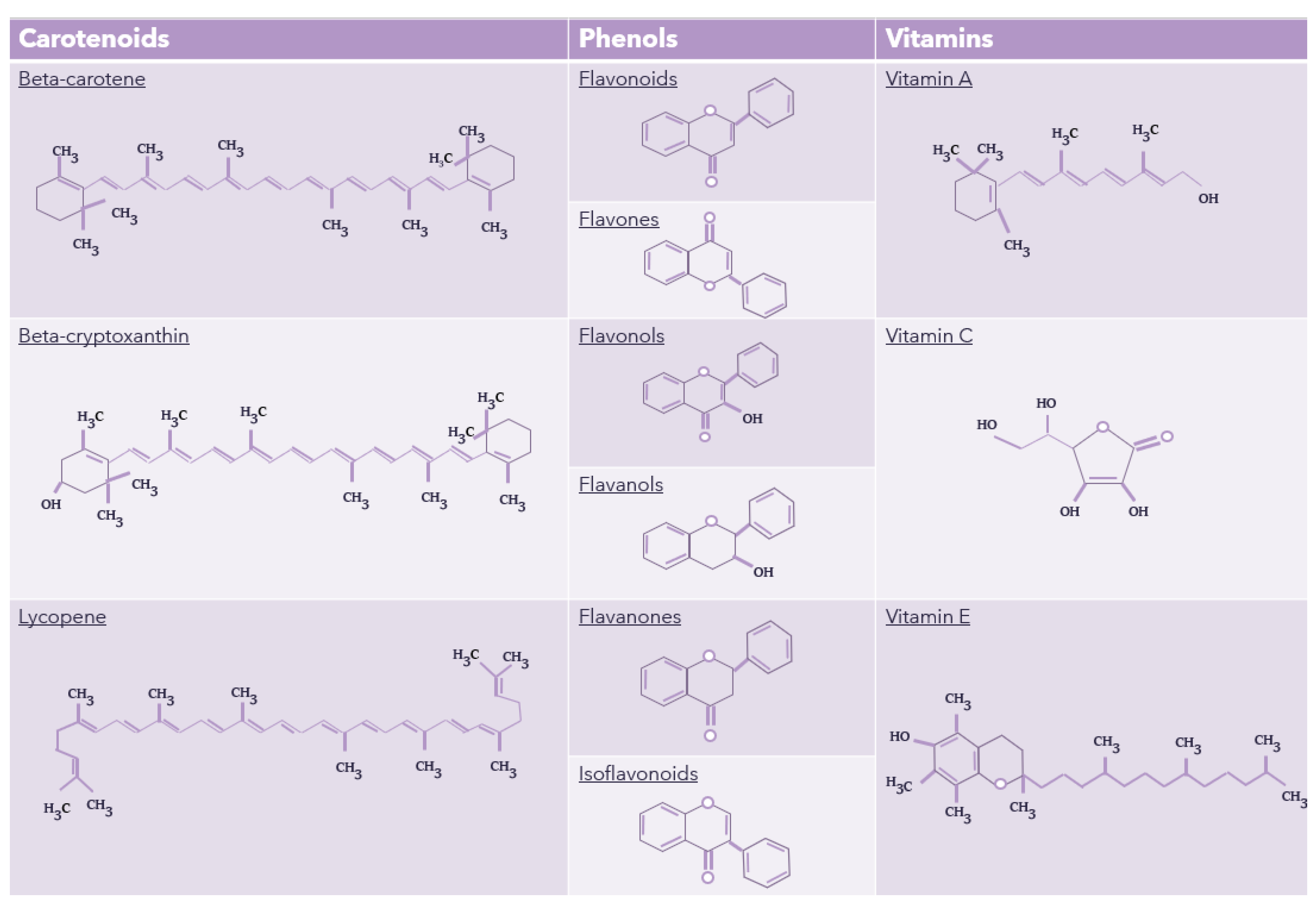

Table 1.
Studies related to food selectivity in children with ASD.
| Food/characteristic studied | Population number (n) | Methodology | Important results | Reference |
|---|---|---|---|---|
| Fruits, Vegetables, Dairy/milk, Flours, Fats, Legumes, Meats, Sweets, Snacks | 105 | An "Aut-Eat-questionnaire" survey was administered to parents of 105 children with ASD and 95 neurotypical children of 137 items or foods regularly consumed by their children. | Neurotypical children eat a significantly greater variety of food groups than children with ASD. Toddlers with ASD ate more snacks than neurotypical toddlers; Older children with ASD ate significantly fewer snacks than neurotypical children of the same age. |
[43] |
| Fruits, Fruit juice, Vegetables, Starchy vegetables, Unrefined carbohydrates, Refined carbohydrates, Eggs, Raw meats, Processed meats, Meat alternative, Dairy | 325 | Online surveys of parents and caregivers of children (ages 3 to 16) neurodivergent | The level of food acceptance varies in response to different food attributes, such as color, presentation, temperature, and texture. The food attributes preferred are crunchy, smooth, moist, and soft foods, with refined carbohydrates being the most accepted group. | [40] |
| Grains, Fruit, Vegetables, Dairy, Fats, Sugars | 39 | 24-hour reminder with parents of 39 children ages 2 to 17 with ASD | Compared to the diet of neurotypical children, the diet of children with ASD has fewer grains and vegetables and greater amounts of sugar in their diet. | [42] |
| Rice, Refined carbohydrates, Fruits, Vegetables | 68 | 68 surveys of parents of children with ASD aged 2 to 11 years and older | Children with ASD prefer easy chew foods, such as rice and bread. They also prefer junk food and some fruits and vegetables. Because they have sensory problems, they do not like crunchy or crunchy food and show an aversion to trying new food. | [41] |
| Grains and starches, Vegetables and marine food, Fruits, Meats, Foods rich in proteins, Dairy, Fat and sweets, Snacks | 130 | Survey of 130 parents who may have more than one neurodivergent child. | Children with ASD like foods that are high in sugar and fat. Children eat snacks more than once a day. Parents of children are interested in developing more nutritious snacks that are high in protein and low in calories with a minimum of additives. | [46] |
| Attributes of food such as texture, taste, color, and temperature | 173 | Questionnaire to parents about their child with ASD to determine consumption of a variety of foods according to different attributes (color, texture, etc.) and preferences | The average group of children with ASD preferred foods with a certain appearance, disliked sticky foods, preferred crispy foods, sweet foods, and refuses foods with mixed ingredients. | [9] |
| Animal products, plant products, bakery products, fats, milk, fruits, vegetables, and others | 62 | 46 children with ASD and 16 non-ASD children were included in this study to find a correlation between ASD children's diet and gut microbiota. Parents participated in mealtime questionnaires. | Children with ASD showed lower values of docosahexaenoic acid, docosapentanoic acid, iron, copper, iodine, and vitamins K, B6, and C. | [44] |
Table 2.
General research on antioxidants and their biological properties.
| Antioxidant | Nature (hydro/liposoluble) | Found in | Biological properties | References |
|---|---|---|---|---|
| Anthocyanins | Hydrosoluble | Berries, grapes, cherries, black beans, etc. | Reduce cellular lipid peroxidation. High ORAC value. Antithrombotic and antimicrobial activity. | [123] |
| Beta-carotene | Liposoluble | Carrots, sweet potatoes, apricots, mangos, etc. | Lower cardiovascular risk and eye disease. Antioxidant effects. | [124] |
| Beta-cryptoxanthin | Liposoluble | Tangerine, oranges, persimmon, papaya, paprika, carrot, etc. | Prevent progression of osteoarthritis in mice, cancer-preventive effects, anti-metabolic syndrome effects, etc. | [96] |
| Flavonoids | Hydrosoluble | Fruits, vegetables, fungi, etc. | Antioxidant, anti-inflammatory, anti-mutagenic effect. | [100] |
| Flavones | Hydrosoluble | Celery, red pepper, chamomile, mint, etc. | Anti-inflammatory, antimicrobial, and anticancer activities. | [103] |
| Flavanols | Hydrosoluble | Onion, tomatoes, kale, apples, grapes, etc. | Help reduce risk for cardiovascular diseases, anti-inflammatory, antioxidant, anticancer, antiviral, antimicrobial, etc. | [104] |
| Flavonols | Liposoluble | Cranberries, lettuce, broccoli, potatoes, tomatoes, etc. | Protect against oxidative stress, anti-inflammatory and antimicrobial effects, etc. | [105] |
| Flavanones | Hydrosoluble | Oranges, lemons, grapes, etc. | Free radical-scavenging properties, anti-inflammatory, blood lipid & cholesterol lowering properties, etc. | [107] |
| Isoflavonoids | Hydrosoluble | Soybeans and other legumes. | Antifungal, antibacterial, antiviral, and antioxidant activities. | [108] |
| Lycopene | Liposoluble | Tomato, watermelon, papaya, pink grapefruit, etc. | Help maintain mitochondrial homeostasis and intestinal health. Anti-inflammatory and antioxidant. | [125] |
| Vitamin A | Liposoluble | Carrots, etc. | Participant in cell reproduction and differentiation in the immune system. Play a role in vision. Contribute to reducing ASD symptoms, etc. | [109, 112] |
| Vitamin C | Hydrosoluble | Citrus fruit, strawberry, kiwi, broccoli, peppers, etc. | Neutralize oxidant agents, regulate the immune system, play a role in tissue growth and neurons. | [114, 116] |
| Vitamin E | Liposoluble | Nuts, broccoli, fish, vegetable oils, etc. | Inhibit lipid peroxidation, scavenges lipid peroxyl radicals, Immunity, Neuroprotective, Treating and preventing osteoarthritis | [69, 126] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



