
Submitted:
13 August 2024
Posted:
14 August 2024
You are already at the latest version
Abstract
Triple-negative breast cancer (TNBC) lacks the expression of estrogen receptors, human epidermal growth factor receptor 2, and progesterone receptors (PR). TNBC has the poorest prognosis among breast cancer subtypes and is more likely to respond to immunotherapy due to its higher expression of PD-L1 and a greater percentage of tumor-infiltrating lymphocytes. Immunotherapy has revolutionized TNBC treatment, especially with the FDA's approval of pembrolizumab (Keytruda) combined with chemotherapy for advanced cases, opening new avenues for treating this deadly disease. Although, immunotherapy can significantly improve patient outcomes in a subset of patients, achieving the desired response rate for all remains an unmet clinical goal. Strategies that improve responses to immune checkpoint blockade, including combining immunotherapy with chemotherapy, molecularly targeted therapy, or radiotherapy may improve response rates and clinical outcomes. In this review, we provide a short background on TNBC and immunotherapy and explore the different types of immunotherapy strategies that are currently being evaluated in TNBC. Additionally, we review why combination strategies may be beneficial, provide an overview of the combination strategies, and discuss the novel immunotherapeutic opportunities that may be approved in the near future for TNBC.
Keywords:
TNBC
; triple-negative breast cancer
; immunotherapy
; immune checkpoint inhibitors
; radiation therapy
; chemotherapy
1. Introduction
Triple-negative breast cancer (TNBC) represents 15-20% of breast cancers (BC) that are newly diagnosed and is a subtype with the fewest approved targeted therapies [1]. PARP inhibitors were approved by the FDA for patients with metastatic and early TNBC who have germline mutations in BRCA1/2 [2,3]. TNBC does not overexpress human epidermal growth factor receptor 2 (HER2) and lacks expression of either estrogen receptor (ER) or progesterone receptor (PR) [4]. Clinically, TNBC tumors are typically larger upon diagnosis and tend to develop nodal metastasis to the draining lymphatics [5]. This subtype is known for developing more lethal metastases which are more likely to originate in viscera, especially the brain and lungs, and less likely to spread to the bone [6]. TNBC patients have a higher chance of an early relapse than patients with other subtypes of BC and only a subset of TNBC patients respond better to chemotherapy [6,7]. TNBC recurrence often peaks between the first- and third year following diagnosis, then sharply declines in the years that follow. Relapses after eight or ten years are extremely rare [7]. Developments in treatment strategies remained limited for years and cytotoxic chemotherapy continues to be the primary systemic treatment for TNBC and is often used in the neoadjuvant setting [1]. This allows for a decrease in the tumor burden and an in vivo assessment of treatment response, such that pathological complete response (also known as pCR) is a useful prognostic marker for survival [8]. While there are several drugs targeting ER and HER2 in clinical subgroups, the paucity of progress in developing targeted therapies for TNBC is apparent [1].The understanding of the intricate molecular and genetic basis for TNBC has steadily improved over the last decade or so, with several classification schemas for TNBC proposed [5,9-11]. Using emerging technologies, such as next-generation sequencing (NGS), Lehmann et al. validated both intratumoral and intertumoral heterogeneity and simplified the molecular classification of TNBC into 6 different subtypes: basal-like 1 and 2 (BL1 and BL2), immunomodulatory (IM), luminal androgen receptor (LAR), mesenchymal (M), and mesenchymal stem-like (MSL) [12]. In 2016, Lehmann revised the classification into 4 distinct subtypes: BL1, BL2, M, and LAR. IM and MSL were left out due to their low cellularity and dependability on the tumor-infiltrating lymphocytes (TILs) and tumor-associated stromal cells [13]. Significant recent advancements have led to FDA approval of several drugs for TNBC and non-TNBC breast cancers (Table 1). Novel strategies such as immunotherapy [14], ionizing radiation therapy [15], platinum agents [16], and PARP inhibitors [17], have been explored to increase the pCR rates. TNBC is most likely to benefit from immunotherapy because several studies reported higher tumor mutational burden, increased expression of programmed cell death-ligand1 (PD-L1), and higher TILs in the tumor microenvironment (TME) compared to the other BC subtypes [18,19]. Based on several clinical trials, the immunotherapy and chemotherapy combination was approved in both, early and advanced TNBC settings [20]. In this review, we discuss the different types of immunotherapy strategies that are currently employed in TNBC, articulate why combination strategies may be beneficial, provide an overview of the combination strategies, review the current clinical challenges encountered, and provide insight into potential future clinical developments.

Table 1.
Updated list of FDA-approved drugs to treat TNBC and other breast cancers (accessed information from https://www.fda.gov/ on 7/26/2024).
Table 1.
Updated list of FDA-approved drugs to treat TNBC and other breast cancers (accessed information from https://www.fda.gov/ on 7/26/2024).
| Drug class | Subtype | Agents |
|---|---|---|
| Cytotoxic chemotherapy | All breast cancer subtypes | Carboplatin, Docetaxel, Doxorubicin, Epirubicin, Ixabepilone, Liposomal doxorubicin, Nab-paclitaxel, Paclitaxel, Vinorelbine |
| HR+ | No approved agents for only HR+ subtype | |
| HER2+ | Carboplatin | |
| HER2- | No approved agents for only HER2-subtype | |
| TNBC | Cisplatin | |
| Targeted therapy | All breast cancer subtypes | No approved agents targeting all subtypes |
| HR+ | Abemaciclib, Alpelisib, Anastrozole, Capivasertib, Elacestrant, Everolimus, Exemestane, Fulvestrant, Lapatinib, Letrozole, Palbociclib, Ribociclib, Tamoxifen, Toremifene | |
| HER2+ | Lapatinib, Margetuximab, Neratinib, Pertuzumab, Tucatinib, Trastuzumab | |
| HER2- | Abemaciclib, Alpelisib, Bevacizumab, Capivasertib, Elacestrant, Everolimus, Fulvestrant, Olaparib, Palbociclib, Ribociclib, Talazoparib | |
| TNBC | Atezolizumab, Pembrolizumab | |
| Antibody-Drug Conjugates | All breast cancer subtypes | Sacituzumab govitecan |
| HR+ | No approved agents for only HR+ subtype | |
| HER2+ | Ado-trastuzumab emtansine, Trastuzumab deruxtecan | |
| HER2- | No approved agents for only HER2- subtype | |
| TNBC | Trastuzumab deruxtecan (TNBC with low/ultra-low HER2 expression) |
2. Immune Microenvironment of TNBC
Despite the widely held notion that BC is not immunogenic, numerous studies demonstrated that TNBC can activate the immune system. Given that TNBC is associated with BRCA1/2 mutations that cause genomic instability and increased mutational burden, its immunogenicity is unsurprising. Numerous studies indicate that cancers associated with BRCA1/2 mutations are more highly immunogenic than tumors that are BRCA1/2 wild type [21]. Compared to other BC subtypes, TNBC displays lower clonal heterogeneity and higher immune gene expression [22]. The immune microenvironment of TNBC is a dynamic, intricate network of different immune cell populations, cytokines, and signaling pathways [23]. The immunological components of the TNBC tumor microenvironment are complex (Figure 1) as described below:
Figure 1.
Immunological components of TNBC tumor microenvironment. This illustration set forth the immunological components of TNBC tumor microenvironment which includes tumor-infiltrating lymphocytes (TILs), regulatory T cells (Tregs), tumor-associated macrophages (TAMs), cancer-associated fibroblasts (CAFs), tumor associated neutrophils (TANs), dendritic cells (DCs), natural killer (NK) cells, myeloid-derived suppressor cells (MDSCs), cancer-associated adipocytes (CAAs), and immune checkpoints.
Figure 1.
Immunological components of TNBC tumor microenvironment. This illustration set forth the immunological components of TNBC tumor microenvironment which includes tumor-infiltrating lymphocytes (TILs), regulatory T cells (Tregs), tumor-associated macrophages (TAMs), cancer-associated fibroblasts (CAFs), tumor associated neutrophils (TANs), dendritic cells (DCs), natural killer (NK) cells, myeloid-derived suppressor cells (MDSCs), cancer-associated adipocytes (CAAs), and immune checkpoints.
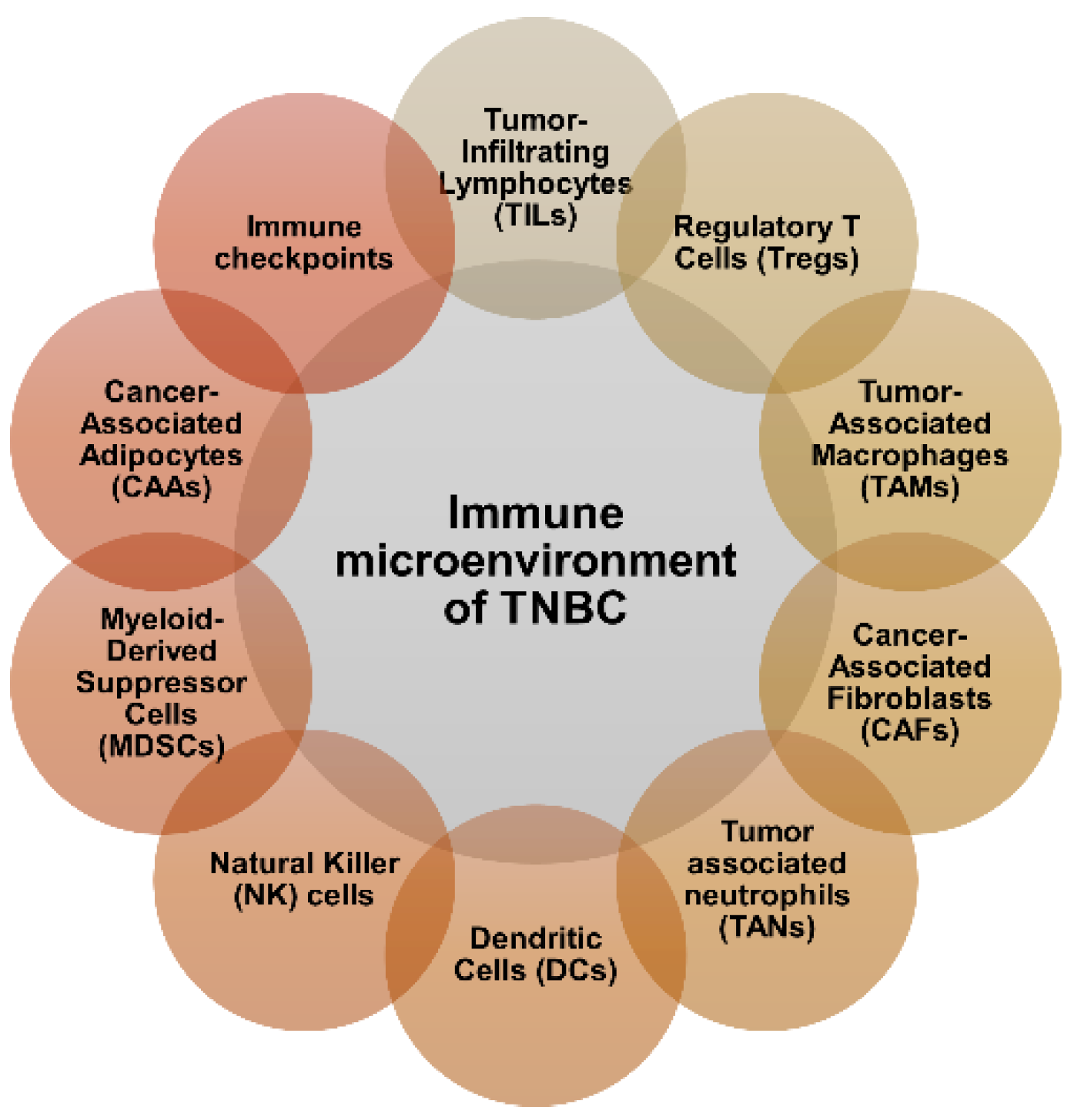
(a) Tumor-Infiltrating Lymphocytes (TILs): TNBC is defined by a high level of TIL infiltration, especially helper T cells (CD4+ T cells) and cytotoxic T cells (CD8+ T cells). TILs are associated with greater reactivity to immunotherapy and chemotherapy in TNBC patients [24]. Based on a meta-analysis evaluating TILs' prognostic value in TNBC, researchers found that TIL status should be considered as an effective prognostic factor for this subtype of BC as a high TIL level correlates with a better outcome [25,26].
(b) Regulatory T Cells (Tregs): A subpopulation of CD4+ T cells known as "Tregs" inhibits immunological responses, particularly those directed against malignancies. Tregs can suppress anti-tumor immune responses and encourage immune evasion in TNBC which may promote tumor growth and metastasis [27]. Presently, Treg infiltration is a predictive factor of TNBC, and treating and monitoring Treg infiltration in TNBC may benefit some patients [23].
(c) Tumor-Associated Macrophages (TAMs): TAMs are a diverse group of immune cells that infiltrate the TME and are derived from circulating monocytes [28]. TAMs are frequently polarized towards an M2-like pro-tumor phenotype in TNBC, which favors tumor development, invasion, and metastasis. They also play a role in immunological suppression and treatment resistance [29]. TAMs cooperate with Tregs in suppressing the anti-tumor immune activity [30].
(d) Cancer-Associated Fibroblasts (CAFs): CAFs represent a highly heterogeneous activated fibroblast subtype that exhibits dynamic modifications in the growth of tumors. CAFs modulate the extracellular matrix (ECM), boost tumor cell invasion and proliferation, induce neoangiogenesis in tumor cells, decrease anti-tumor immunity, and aid in the development of an immunosuppressive microenvironment [31]. CAFs may promote TNBC growth through inducing TGF-β [32].
(e) Tumor-associated neutrophils (TANs): TANs are a crucial part of the TME. Neutrophils can be activated in several ways, such as direct tumor cell lysing or cytotoxically inducing antitumor activity, thereby functioning as cells that suppress the immune system [33]. In TNBC TANs suppress anti-tumor immunity and promote tumor growth, migration, invasion, and metastasis. Furthermore, granulocyte-macrophage colony-stimulating factor (GM-CSF), which is secreted by TNBC cells, induces TANs to release tumor suppressor M, stimulates angiogenesis, and facilitates tumor cell infiltration [34].
(f) Dendritic Cells (DCs): DCs are essential for both triggering and controlling immune responses. T cells in TNBC may be exposed to tumor antigens by DCs which might trigger an immune response against the tumor [35]. Nonetheless, DC function within the TNBC milieu may be compromised, resulting in insufficient T cell priming and immunological evasion [36].
(g) Natural Killer (NK) cells: NK cells are innate immune cells that eliminate tumor cells directly without sensitization. Activated NK cells release perforin/granzyme upon encountering tumor cells. This causes cytokine secretion including TNF-α and IFN-γ which are involved in cytolysis. Using the MHC-I down-regulation mechanism—a common way for cancer cells to evade T cell recognition—NK cells can target and kill tumor cells with high efficacy [23]. Tumor development and immune evasion are facilitated by TNBC tumors, which frequently show reduced infiltration and compromised NK cell activity [37].
(h) Myeloid-Derived Suppressor Cells (MDSCs): MDSCs represent a multitude of immature myeloid cells possessing immunosuppressive characteristics [38,39]. In TNBC, MDSCs proliferate in the TME where they stifle T cell activation and encourage Treg proliferation, hence impeding anti-tumor immune responses [40].
(i) Cancer-Associated Adipocytes (CAAs): CAAs are adipose cells found within or around tumors that have been implicated in promoting cancer progression and metastasis. Adipocytes in the TME can release various signaling molecules and factors that support cancer cell growth, invasion, and resistance to therapy [41]. These interactions between tumor cells and adipocytes may contribute to TNBC aggressiveness.
(j) Immune checkpoints: Immune checkpoints are vital in regulating T cell activity and maintaining immunological homeostasis. Examples of these include cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) and PD-1 [42]. Immune checkpoint proteins are frequently overexpressed in TNBC tumors which cause T cell exhaustion and immune evasion. In TNBC, targeting immunological checkpoints has become a potentially effective therapeutic approach, especially when combined with chemotherapy or targeted therapy [43].
In general, tumor cell elimination usually calls for the onset of several events [19]. Initially, tumor cells release specific antigens which are processed by antigen-presenting cells (APCs) primarily DCs. To present antigenic signals to T cells, DCs migrate further to lymphoid tissues. Following that, T cells proliferate, get activated, migrate, and penetrate tumor tissues. At last, T lymphocytes can identify and destroy tumor cells. Tumor cell elimination also requires B cells and innate immune cells like NK cells [19]. A thorough understanding of the interactions between tumor cells and the immune environment is critical for refining potent immunotherapeutic strategies for TNBC.
3. Current Clinical Immunotherapy Approaches for TNBC
3.1. Cytokines
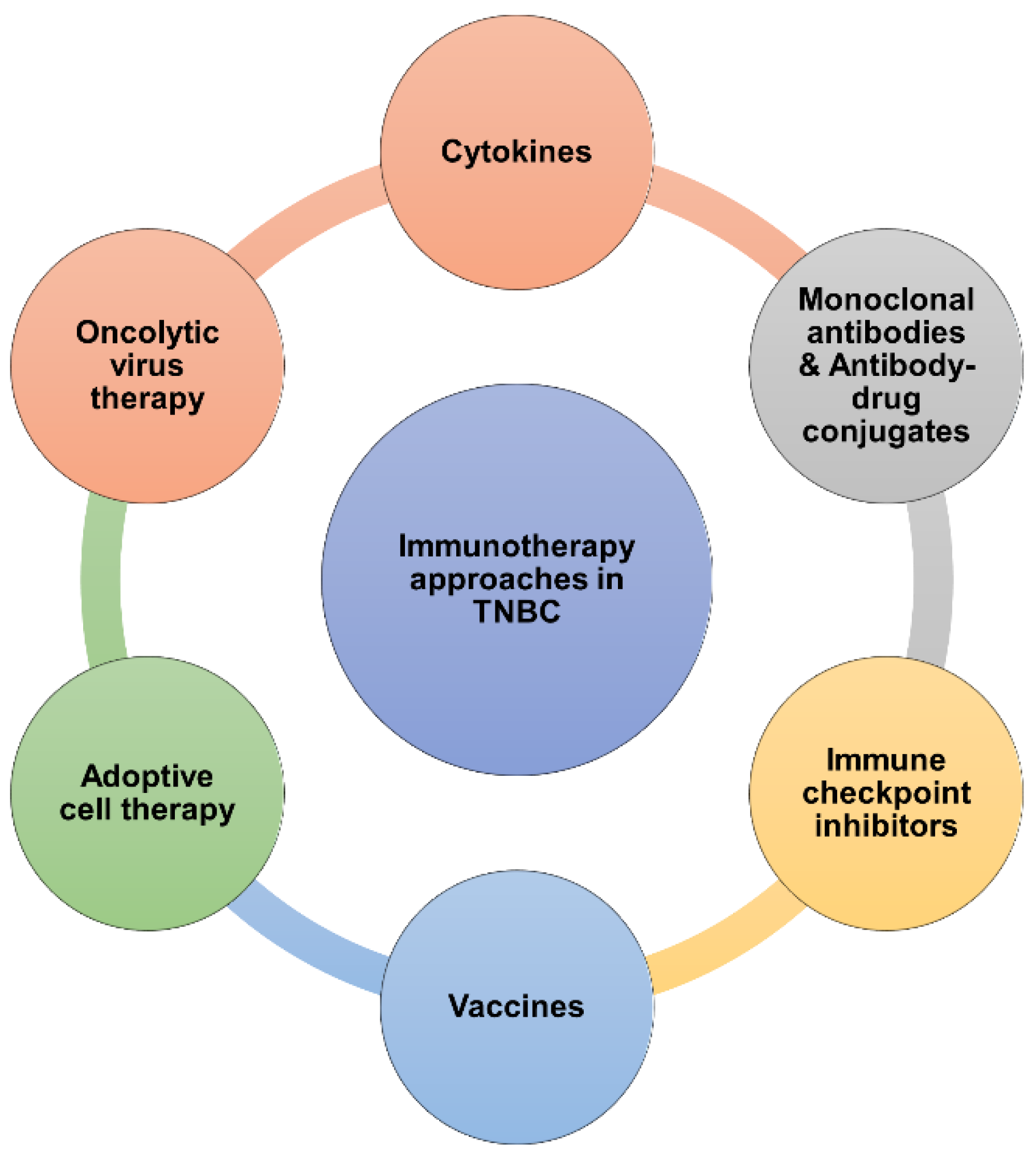
Cytokines are small proteins that are essential for immune response and cell signaling [44]. While cytokine-based therapies have been explored in several cancers including BC, their role in TNBC treatment is still actively explored. Cytokines regulate the host immune response to cancer cells and aid in prompting cancer cell death, making cytokine-based immunotherapy an intriguing possibility in cancer treatment [45]. The two cytokines approved by the FDA for the treatment of cancer, though not breast cancer, are IL-2 and IFN-α; nevertheless, their high toxicity profile has limited their use [44]. Several other cytokines including GM-CSF [46], IL-12, IL-15, and TNF are being tested in numerous clinical trials for their safety and effectiveness as cancer treatments [47]. Moreover, as single-agent immunotherapies, over 40 known cytokines have been approved for a restricted range of indications, including the treatment of cancer [48]. A recombinant adenovirus expressing IL-12 (AdIL-12) administered intratumorally has been demonstrated to cause substantial tumor regression in animal models of BC [48]. Patients with metastatic TNBC (mTNBC) demonstrated improved antigen presentation and a treatment-related spike in CD8+ TIL density following intratumoral administration of IL-12 (Phase-1 pilot study) [49]. An engineered cytokine called empegaldesleukin or NKTR-214 preferentially activates the IL-2 receptor with a focus on metastatic solid tumors, including TNBC (Phase-1 trial; NCT02869295) [50]. Cytokine activity facilitates both tumor-promoting and tumor-suppressive effects. Proinflammatory cytokines such as TNF-α and IL-6 for instance, regulate immunological interactions to promote anticancer effects. Cytokines present in the TME promote angiogenesis, epithelial-to-mesenchymal transition, invasion, and tumor growth—all processes linked to cancer development [51]. Several factors contribute to the poor efficacy of cytokine immune therapy including short half-life, increased toxicity, and low efficacy. High intratumoral cytokine dosages might cause systemic adverse effects including renal insufficiency, hypotension, neuropsychiatric symptoms, and respiratory failure [52]. Similarly, patients do not tolerate systemic treatment of recombinant IFN-α as well [53]. IRX-2, a novel therapy comprising numerous cytokines demonstrated activation of TME by elevating TIL numbers, PD-L1 expression, and lymphocyte activation in early TNBC patients in a phase I study. A phase II follow-up trial is underway (NCT04373031) [54]. Even though cytokines were thought to have several benefits when used as a monotherapy, most clinical trials that employed systemic cytokine monotherapy failed. This could be due to inadequate cytokine concentrations in the tumor upon parenteral administration, and major toxicities related to the activation of humoral or cellular checkpoints [55]. Figure 2 shows the current clinical immunotherapy approaches in TNBC.
Figure 2.
Current clinical immunotherapy approaches in TNBC. Clinical immunotherapy approaches for TNBC have been diversified in recent years and t his illustration summarizes those strategies which include cytokines, mAbs/ADCs, immune checkpoint inhibitors, vaccines, adoptive cell therapies, and oncolytic virus therapy.
Figure 2.
Current clinical immunotherapy approaches in TNBC. Clinical immunotherapy approaches for TNBC have been diversified in recent years and t his illustration summarizes those strategies which include cytokines, mAbs/ADCs, immune checkpoint inhibitors, vaccines, adoptive cell therapies, and oncolytic virus therapy.
3.2. Monoclonal Antibodies
The goal of using humanized monoclonal antibodies (mAbs) is to decrease immunotolerance and boost the immune response against tumors by blocking immunosuppressive checkpoints that the tumor uses to evade immune system control [56]. Trastuzumab was the first FDA-approved monoclonal antibody for the treatment of HER2-positive breast cancer [57]. TNBC tumors don’t express HER2 thus these patients can’t be treated with trastuzumab or other HER2-specific agents [58]. In 2009, the FDA authorized bevacizumab (Avastin), a humanized mAb that specifically targets VEGF-A. VEGF regulates tumor-induced immunosuppression in addition to blood vessel development [59]. Therefore, bevacizumab's immunomodulatory characteristics open possibilities for novel combination treatment approaches [59]. In 2010, the approval of bevacizumab for breast cancer was recommended for withdrawal by the Office of New Drugs (OND). Significant benefits were not confirmed by the required follow-up trials, and increased serious adverse events with a lack of survival benefit were revealed, leading to the conclusion that the risks outweigh the benefits of this indication [60]. Aspartic protease Cath-D is an extracellular target unique to TNBC. As a promising immunotherapy, an immunomodulatory antibody-based approach against Cath-D is presently in its developmental phase to treat TNBC patients [61].
3.3. Antibody-Drug Conjugates (ADCs)
ADCs can identify antigens that are tumor-specific or overexpressed in tumors and thus can kill cancer cells via antigen-dependent cell-mediated cytotoxicity (ADCC) [62]. ADCs utilize the specificity of mAbs on cellular-antigen identification to administer potent cytotoxic drugs in a tailored approach [63]. TNF receptor superfamily members such as CD40 can help DCs to stimulate anti-tumor T-cells and retrain macrophages to kill tumor stroma. The efficacy of anti-CD40 antibodies has been evaluated in several clinical trials [64].
ADC trastuzumab deruxtecan (DS-8201) is comprised of a cytotoxic topoisomerase I inhibitor and an anti-HER2 antibody connected by a cleavable tetrapeptide linker [65]. Its capacity to produce cytotoxic action against antigen-negative cells (bystander effect) may have led the FDA to approve it in BC patients who have been pretreated with trastuzumab emtansine (TDM1) [66]. The DESTINY-Breast04 and DESTINY-Breast06 trials have yielded critical data on the efficacy of trastuzumab deruxtecan in treating HER2-low breast cancer. DESTINY-Breast04 demonstrated that patients with HER2-low breast cancer (IHC 1+ or IHC 2+ without FISH amplification) had significantly superior progression-free survival (PFS) when treated with trastuzumab deruxtecan compared to those who received the physician’s choice of cytotoxic chemotherapy. This trial established trastuzumab deruxtecan as a viable treatment option for HER2-low breast cancer, highlighting its potential to change clinical practice [67].Similarly, the DESTINY-Breast06 trial expanded the understanding of trastuzumab deruxtecan efficacy by showing benefits for patients with IHC "ultra-low" breast cancer (IHC 0 but with subtle HER2 expression). This finding is particularly notable as it extends the applicability of trastuzumab deruxtecan to a broader patient population, including those previously not considered for HER2-targeted therapies (NCT04494425). These results are especially significant for TNBC patients, who traditionally have limited treatment options. Moreover, it is important to underscore the CNS activity of trastuzumab deruxtecan, as its ability to penetrate the central nervous system could provide substantial benefits for patients with brain metastases, a common and challenging complication in breast cancer. The TUXEDO-1 trial (NCT04752059) demonstrated that trastuzumab deruxtecan achieved a high intracranial response rate in patients with active brain metastases from HER2-positive breast cancer, establishing it as a viable treatment option for this condition [68]. Another ADC, Disitamab vedotin consists of a HER2 mAb conjugated to cytotoxic drug monomethyl auristatin E with a cleavable linker and is also being tested in clinical trials for several solid tumors including HER2+/low BCs [69].
Sacituzumab govitecan is the first ADC to receive FDA approval to treat TNBC which consists of a human trophoblast cell-surface antigen-2 (TROP2) antibody that is connected with a topoisomerase I inhibitor (SN-38) via a unique hydrolyzable linker [70]. Recently, a Phase III trial (ASCENT) demonstrated noticeably prolonged OS and PFS while using sacituzumab govitecan instead of single-agent chemotherapy [71]. Apart from HER2 and TROP2-based ADC, the activities of folate receptor alpha (FRα) and zinc transporter LIV-1-based ADC have been clinically evaluated for TNBC [61]. Ladiratuzumab vedotin is an ADC that targets Syndecan-1 on cancer cells. It binds to these cells, is internalized, and releases a cytotoxic agent that disrupts microtubules, leading to cell cycle arrest and apoptosis [72]. In early-phase clinical trials, ladiratuzumab vedotin is being explored as a monotherapy for patients with BC; some of these studies have already shown encouraging results [72]. In a phase I, multi-part, dose-escalation SGNLVA-001 trial mTNBC exhibited superior overall response rate (ORR) and disease control rate (DCR) with Ladiratuzumab vedotin [73]. Recently, Tsai and colleagues reported an ORR of 28% with Ladiratuzumab vedotin at 1.25 mg/kg indicating the favorable activity of the ADC [74].
Recently, a newly developed ADC (ESG401), which consists of a humanized anti-TROP2 IgG1 monoclonal antibody connected to the Topoisomerase I Inhibitor SN-38 through a stable cleavable linker, demonstrated promising effectiveness and tolerability in the Phase Ia trial [75]. Moreover, the effectiveness of ESG401 in treating brain metastases in first-line mTNBC patients corresponds with our prior findings in late-line mTNBC and HR+/HER2- BC patients (NCT04892342) [76]. Datopotamab deruxtecan (Dato-DXd) is another ADC where the antibody datopotamab, targeting TROP2 on breast cancer cells, is linked to the cytotoxic drug DXd. Once datopotamab binds to TROP2 and is internalized, the linker breaks down, releasing DXd to kill the cancer cell [77]. Dato-DXd's ability to recruit immune cells to cancer sites suggests that combining it with durvalumab, which blocks PD-L1 and enhances immune cell activity, may enhance its effectiveness. In the phase I study of Dato-DXd (NCT03401385), promising antitumor activity and a manageable safety profile were observed in patients with heavily pretreated advanced HR+/HER2– breast cancer and TNBC [78]. The ongoing TROPION-Breast03 trial (NCT05629585) will compare Dato-DXd alone or with durvalumab against standard care in patients with non-mTNBC with residual cancer cells post-surgery [77]. Thus, ADCs continue to play an ever-evolving and significant role in the management of mTNBC.
3.4. Immune Checkpoint Inhibitors
ICIs kill tumor cells by disabling the immune system's "braking" function on the immune cells that attack cancer. ICIs target the three best-characterized targets, PD-L1 (also called as B7 homolog 1) and PD-1 (also known as CD279) while blocking CTLA-4 (CD152) [79]. The mechanism of action of ICIs targeting PD-L1, PD-1, and CTLA-4 is shown in Figure 3. ICIs have the potential to be beneficial for both immunoinflammatory and immunological-suppressive types, potentially changing the TME from an "immune cold" to an "immune hot” phenotype [80]. The immunosuppressive PD-1 protein is mostly expressed on the cell surface (i.e., plasma membrane) of B, T, myeloid, and NK cells of the immune system [81]. The FDA-approved PD-1/PD-L1 inhibitors include atezolizumab, avelumab, cemiplimab, durvalumab, nivolumab, and pembrolizumab [82]. PD-L1 expression is directly correlated to histological grade and lymphocyte infiltration and is observed in 20–30% of TNBC cases [82].
Figure 3.
Mechanism of action of ICIs targeting PD-L1, PD-1, and CTLA-4. T cell inactivation and the prevention of tumor cell death are caused by their binding to the corresponding ligands on the surface of cancer cells. Immune checkpoint inhibition promotes anticancer activity and promotes T cell activation.
Figure 3.
Mechanism of action of ICIs targeting PD-L1, PD-1, and CTLA-4. T cell inactivation and the prevention of tumor cell death are caused by their binding to the corresponding ligands on the surface of cancer cells. Immune checkpoint inhibition promotes anticancer activity and promotes T cell activation.
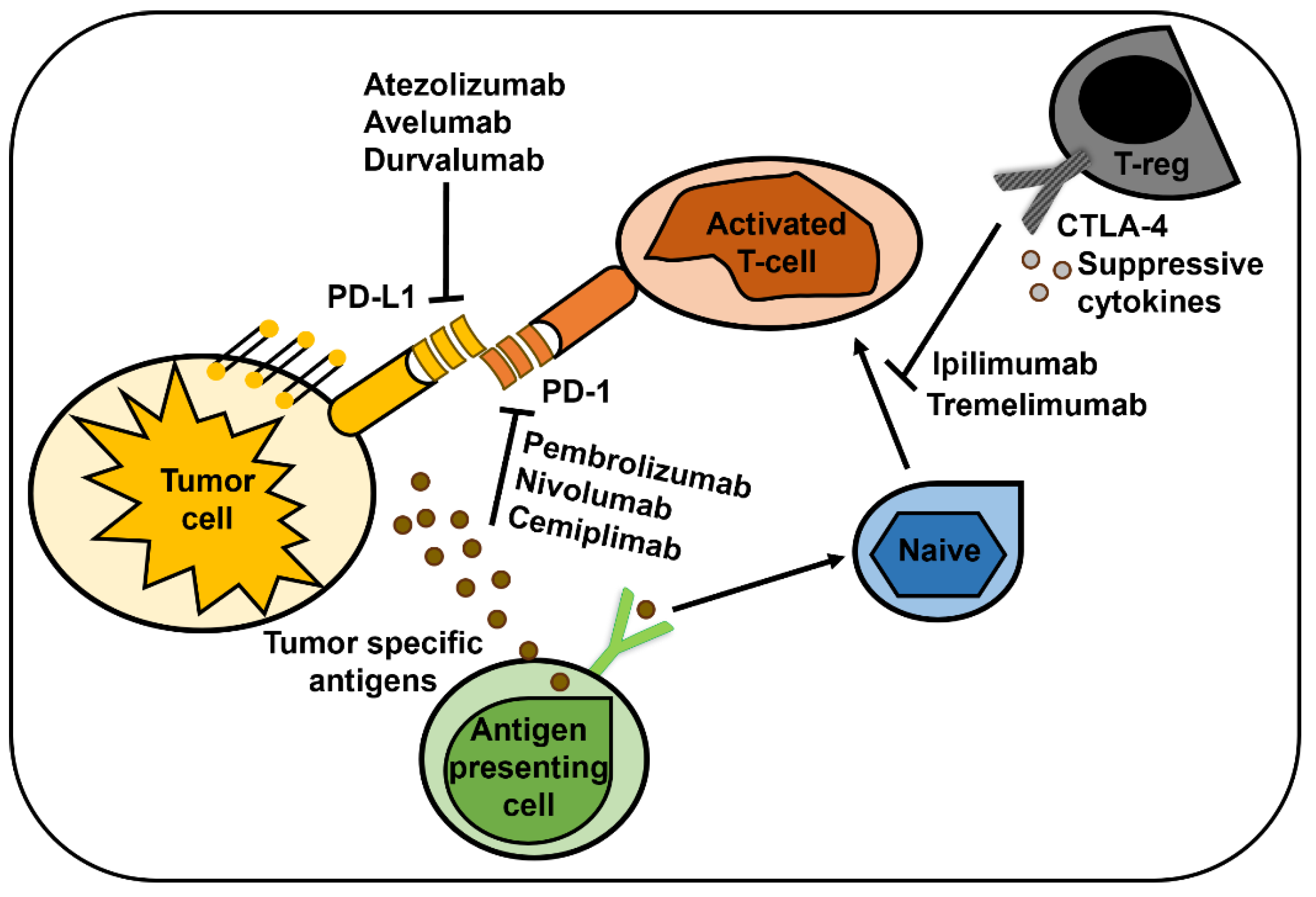
Pembrolizumab was found to be safe with good ORR in TNBC patients (KEYNOTE-012; [83]) and pembrolizumab monotherapy provided long-lasting antitumor efficacy in patients with both early and advanced PD-L1-positive TNBC with a combined positive score ≥ 1 [84,85]. PD-1 inhibitor JS001 demonstrated good safety and efficacy in mTNBC patients (NCT02838823) who failed prior multi-line treatments [86,87]. Pembrolizumab received approval based on the KEYNOTE-355 trial (NCT02819518), a multicenter, double-blind, randomized, placebo-controlled study involving patients with locally recurrent unresectable or metastatic TNBC who had not previously received chemotherapy for metastatic disease [88]. Similarly, atezolizumab monotherapy offered enduring clinical advantages for patients with mTNBC (NCT01375842; [89]) while avelumab provided an ORR of 44.4% (PD-L1≥10%) and 2.6% (PD-L1<10%) in TNBC patients (JAVELIN trial; [90]). The FDA initially approved atezolizumab in combination with nab-paclitaxel for first-line treatment of TNBC based on the IMpassion130 trial. However, this approval was later withdrawn following the negative results of the IMpassion131 trial [91].
T cells receive positive and negative feedback from the CD28 and CTLA-4 receptors, respectively [92]. CTLA-4 maintains T cell homeostasis since it specifically regulates CD4+ T cell responses [93]. Importantly, tissues from lymph node metastases show considerably higher CTLA-4 levels than tissue samples from the original breast tumor as seen in axial lymph node (ALN) metastasis [94]. There is presently no approved CTLA-4 inhibitor that can be used exclusively for TNBC, but ipilimumab is FDA-approved to treat several other cancers.
3.5. Vaccines
Known antigens associated with breast tumors are the main target of therapeutic vaccines, which work by actively immunizing against the tumor. Patient-specific tumor mutanome is used in cutting-edge settings to produce vaccines [95]. Vaccines can modify the TME through chemokines which can directly impact tumor growth as well as cytotoxic CD8+ T-cell (CTL) and NK responses. Several independent approaches have been used to develop therapeutic vaccines that use DC, DNA, RNA, peptides, carbohydrates, or all of the above [96]. CD4+ helper T lymphocytes can be stimulated by AE37 which is an Ii-Key hybrid of the MHC class II peptide. The randomized phase II trial comparing GM-CSF alone with the AE37 + GM-CSF vaccine to prevent BC recurrence revealed no statistically significant differences in the five-year DFS between the treatment arms [97,98]. Similarly, a phase 1 trial with FRα peptide vaccine was well tolerated and produced responses that lasted over a year in more than 90% of patients with BC [99]. Poxvirus used in the PANVAC vaccine encodes mucin-1 (MUC-1) and carcinoembryonic antigen (CEA) along with T-cell-stimulating proteins LFA-350, ICAM-1, and B7.1 [100]. Favorable clinical responses to this vaccine have been observed in a limited number of patients [101]. Similarly, mixed subtypes of BC subjects treated with autologous dendritic cell (DC) vaccine pulsed with various p53 peptides resulted in stable disease in ~ 30% of patients, and a small subgroup of these had an increased CD8+ T-cell responses [102]. Autologous DC vaccine increased PFS to over 3 years in a subgroup of ER/PR double negative [103] and PR negative stage IV BC subjects [104]. Early clinical investigations of the DC vaccine including hTERT [105] peptides and FRα [99] have demonstrated T-cell activation further supporting the role of the DC vaccine in BC management. These include a novel alpha-lactalbumin vaccine in patients with stage II-III TNBC (phase I) and in individuals at risk for TNBC who are planning to undergo preventative bilateral mastectomy (phase I) [106], STEMVAC, a DNA plasmid-based vaccine (phase II, NCT05455658) on patients with curatively treated stage I-III TNBC. STEMVAC targets proteins expressed on breast cancer stem cells, working to enhance the immune system's ability to detect and eliminate the cancer cells responsible for the disease [107].
3.6. Adoptive cell therapy (ACT)
T cells are crucial for cell-mediated immunity. Two forms of ACTs that can alter natural T cells ex vivo and reintroduce them into the body to make them more potent tumor-destroying agents are chimeric antigen receptor (CAR) T-cell and T-cell receptor (TCR)–engineered T-cell therapies [108]. CAR T-cells are designed to identify exclusively surface antigens by fusing antibody fragments on the T-cell's antigen-binding region. In contrast, MHC-expressed intracellular antigens are recognized by TCRs through the utilization of an alpha-beta chain heterodimer. Consequently, since TCRs may target a larger variety of antigens than CAR-T, they might be more advantageous in solid tumors [108]. Enhancing CAR-T cell infiltration in tumor tissues is a main obstacle for CAR-T therapy in BC. This obstacle may be addressed by combining the delivery of CAR-T cells with strong stimulation of APCs to produce chemotactic cytokines [109]. Receptor tyrosine kinase c-Met is overexpressed in approximately 50% of BCs. The intratumoral injections of c-Met-CAR-T cells were well tolerated and induced an inflammatory response in metastatic BC patients with c-Met-expression in a phase 0 trial (NCT01837602) [110]. Mesothelin is overexpressed in TNBC which is linked to a poorer prognosis [111]. This led to the development of mesothelin-specific CAR-T cells. Initial findings from a phase I/II trial (NCT02414269) in patients with advanced solid tumors demonstrated anti-tumor activity of mesothelin-targeted CAR-T cells without any significant toxicities [112]. Similarly, a combination of mesothelin-targeted CAR-T cells with pembrolizumab was found to be safe and well tolerated in patients with malignant pleural disease (NCT02792114) and demonstrated antitumor efficacy [113]. Over 90% of TNBC express high MUC1 protein which is linked to a poor prognosis [114]. An anti-MUC1 CAR-T cell-based phase I clinical trial is currently underway (NCT04020575) for patients with advanced MUC1-positive BC [115]. Another well-known marker for BC adverse prognostic is CEA [116]. A phase-I trial that aimed to analyze the safety and tolerability of anti-CEA T cell therapy (NCT00673829) in patients with metastatic BC has been suspended without any published results [117]. Luen et al. showcased how TILs could be a crucial factor in adapting clinical trial designs. Currently, TILs do not have clinical utility in any cancer type, and thus should not be utilized as a biomarker to tailor clinical therapies in daily practice. To fully investigate its clinical relevance, the next logical progression would be to consider using TILs as an adaptive factor in clinical trials [118]. Additional clinical testing of adoptive cell therapies in TNBC is warranted to improve the clinical outcome in subjects with TNBC, especially late-stage and mTNBC.
3.7. Oncolytic Virus Therapy
Natural or genetically engineered viruses that can proliferate selectively in cancer cells without harming healthy cells are known as oncolytic viruses (OVs) [119,120]. OV may lyse tumor cells by infecting them directly, multiplying within them, or stimulating the immune system [121]. OVs are designed to target several stages in the cancer-immunity cycle. Oncolytic viruses cause immunogenic cell death, which triggers the innate and adaptive immune systems by releasing danger signals and neo-antigens [122]. At present, the only type of OV authorized for cancer therapy is talimogene laherparepvec (T-VEC), a herpes simplex virus-1 (HSV) modified to express GM-CSF [123]. An additional phase II trial (NCT02658812) assessed the effectiveness of intratumoral T-VEC as monotherapy for locoregionally inoperable BC recurrence, irrespective of whether there was a distant recurrence. The results demonstrated that uncontrolled disease development made intratumoral T-VEC monotherapy less effective, and concurrent systemic treatment administration may be necessary [124]. The most researched OV for BC management is adenovirus. The ICOVIR-7 trial included patients with advanced and refractory solid cancer including BC. Although the OV was declared safe and a majority of subjects (16 out of 18) developed neutralizing antibodies, all BC subjects (n=3) failed to reach efficacy endpoints [125]. Conversely, Ad5/3-D24-GMCSF, an OV that codes for GM-CSF effectively immunized patients with advanced BCs including TNBC [126]. Currently, an OV MEM-288 that carries recombinant chimeric CD40 (MEM40) and human interferon beta (IFNβ) is being investigated (NCT05076760) in various solid cancers including TNBC [127]. In vivo and ex vivo testing of several different OVs, including Coxsackie, Maraba, Measles, Newcastle disease, Polio, and Vaccinia has cleared the path for human safety studies [128]. A phase I clinical trial (NCT01846091) using a measles virus that encodes human thyroidal sodium iodide symporter (MV-NIS) is presently being evaluated in a range of cancers including mTNBC [129].
4. Rationale of Combining Immunotherapy with Other Therapies
TNBC is an aggressive disease and often develops resistance to standard of care (SOC) treatment. Thus, immunotherapy in combination with SOC is expected to improve the outcome for several reasons: 1) Different therapies target cancer cells through distinct mechanisms. Combining immunotherapy with chemotherapy, targeted therapy or radiation therapy can attack cancer cells through multiple pathways simultaneously resulting in a robust response [130]; 2) Some therapies can increase the immune system's capacity to identify and target cancer cells. For example, chemotherapy can induce immunogenic cell death, releasing tumor antigens that activate the immune response thereby synergizing with immunotherapy [131]; 3) TNBC often develops resistance to single-agent therapies [132]. Combination therapies can target several pathways implicated in tumorigenesis and immune evasion, reducing the likelihood of developing resistance [133]; 4) Not all patients respond to immunotherapy alone. Combining immunotherapy with other therapies may broaden the spectrum of patients who benefit from treatment, improving overall outcomes [134]; 5) Combining lower doses of different therapies may reduce individual treatment-related toxicities while maintaining efficacy, improving patients' quality of life [133]; 6) Targeting TNBC with a combination of therapies can potentially decrease the risk of metastasis or recurrence by eradicating residual cancer cells that may metastasize to other tissues/organs [135]. Overall, combination strategies with immunotherapy represent a comprehensive approach to treating TNBC, addressing its heterogeneity and resistance mechanisms while maximizing therapeutic efficacy and minimizing toxicity. Several key TNBC clinical trials that include(d) immunotherapy in combination with other treatment modalities are listed in Table 2 (non-exhaustive list).
Table 2.
Combination of immunotherapy with other treatment modalities evaluated in clinical trials for TNBC (accessed information from https://www.clinicaltrials.gov/ on 6/17/2024).
Table 2.
Combination of immunotherapy with other treatment modalities evaluated in clinical trials for TNBC (accessed information from https://www.clinicaltrials.gov/ on 6/17/2024).
| Target | Interventions | Clinical status & Identifier | Status |
|---|---|---|---|
| PARP and PD-1 | Drug: Niraparib Biological: Pembrolizumab |
Phase I/II NCT02657889 |
Completed |
| PARP and PD-L1 | Drug: Avelumab Phase 1b Drug: Talazoparib Phase 1b Drug: Avelumab Phase 2 Drug: Talazoparib Phase 2 |
Phase Ib/II NCT03330405 |
Completed |
| PD-1 | Biological: Pembrolizumab Drug: Nab-paclitaxel Drug: Paclitaxel Drug: Gemcitabine Drug: Carboplatin Drug: Normal Saline Solution |
Phase III NCT02819518 |
Completed |
| PD-1 | Drug: Eribulin Mesylate Drug: Pembrolizumab |
Phase Ib/II NCT02513472 |
Completed |
| PD-L1 | Drug: Atezolizumab (MPDL3280A), an engineered anti-PDL1 antibody Drug: Nab-Paclitaxel Drug: Placebo |
Phase III NCT02425891 |
Completed |
| PD-L1 | Drug: Atezolizumab Drug: Nab-paclitaxel |
Phase Ib NCT01633970 |
Completed |
| PD-L1 | Drug: Atezolizumab (MPDL3280A), an engineered anti-PDL1 antibody Drug: Atezolizumab Placebo Drug: Paclitaxel |
Phase III NCT03125902 |
Completed |
| PD-1 | Drug: Nivolumab Radiation: Radiation therapy Drug: Low dose doxorubicin Drug: Cyclophosphamide Drug: Cisplatin |
Phase II NCT02499367 |
Ongoing |
| PD-1 | Biological: Pembrolizumab Drug: Nab-paclitaxel Drug: Anthracycline (doxorubicin) Drug: Cyclophosphamide Drug: Carboplatin Drug: Paclitaxel |
Phase I NCT02622074 |
Completed |
| PD-1 | Biological: Pembrolizumab Drug: Carboplatin Drug: Paclitaxel Drug: Doxorubicin Drug: Epirubicin Drug: Cyclophosphamide Drug: Placebo Biological: GM-CSF |
Phase III NCT03036488 |
Ongoing |
| PD-L1 | Drug: MEDI4736 (Durvalumab) Drug: Placebo Drug: Nab-Paclitaxel Drug: Epirubicin Drug: Cyclophosphamide |
Phase II NCT02685059 |
Completed |
| PD-L1 | Drug: Carboplatin Drug: Abraxane Drug: MPDL3280A (Atezolizumab) Procedure: Surgery Drug: Anthra |
Phase III NCT02620280 |
Ongoing |
| PD-L1 | Drug: Atezolizumab (MPDL3280A), an engineered anti-PDL1 antibody Drug: Placebo Drug: Nab-paclitaxel Drug: Doxorubicin Drug: Cyclophosphamide Drug: Filgrastim Drug: Pegfilgrastim |
Phase III NCT03197935 |
Completed |
| PD-1 | Drug: Pembrolizumab Radiation: Radiotherapy |
Phase II NCT02730130 |
Completed |
| PD-L1 | Radiation: SABR Drug: Atezolizumab |
Phase II NCT03464942 |
Completed |
| PD-1 and LIV-1 | Drug: Ladiratuzumab vedotin Drug: Pembrolizumab |
Phase Ib/II NCT03310957 |
Ongoing |
| PD-L1 and AKT | Drug: Atezolizumab Drug: Ipatasertib Drug: Paclitaxel Drug: Placebo for Atezolizumab Drug: Placebo for Ipatasertib |
Phase III NCT04177108 |
Completed |
| PD-1, PARP, and VEGFR-2 | Drug: SHR-1210 + Apatinib +Fluzoparib | Phase I NCT03945604 |
Completed |
| PD-1, VEGFR-2,c-KIT, and PDGFRb | Drug: Camrelizumab in combination with nab-paclitaxel and famitinib | Phase II NCT04129996 |
Completed |
| PD-L1 and CD73 | Drug: Paclitaxel Drug: Carboplatin Drug: MEDI4736 Drug: MEDI9447 |
Phase I/II NCT03616886 |
Ongoing |
| PD-L1 and modified oncolytic herpes virus | Biological: Talimogene Laherparepvec Biological: Atezolizumab |
Phase Ib NCT03256344 |
Ongoing |
| PD-L1 | Avelumab, SBRT, haNK and 15 other interventions/treatments | Phase I/II NCT03387085 |
Completed |
4.1. Combination of Immunotherapy with PARP Inhibitors
The combination of Poly ADP-ribose polymerase (PARP) inhibitors (PARPi) with immunotherapy is an active area of investigation for TNBC therapeutics. PARP plays an important role in the DNA repair process. Niraparib, olaparib, and talazoparib are key PARPi approved to treat BRCA1/2 mutant cancers [136]. However, recent studies have shown that PARPi may also have immunomodulatory effects that could enhance the efficacy of immunotherapy in TNBC [137]. TNBCs with BRCA mutations or other DNA repair deficiencies are significantly more sensitive to PARPi [138]. Several clinical trials are currently investigating the combination of PARPi with immunotherapy in TNBC.
Patients with germline BRCA1/2 mutation-associated HER2-negative BC undergoing treatment in the first- through third-line of therapy were randomized to receive either olaparib or chemotherapy in phase 3 OLYMPIAD trial [139]. Olaparib did not considerably increase OS in the study population as compared to chemotherapy, but the median PFS was 2.8 months longer. However, among patients receiving first-line treatment, olaparib increased OS by 7.9 months compared to chemotherapy alone [140]. This led to FDA approval for Olaparib therapy in women with TNBC with germline BRCA mutations. In the OlympiA trial (NCT02032823), adjuvant olaparib significantly enhanced invasive and distant disease-free survival in patients with high-risk, HER2-negative early breast cancer and germline BRCA1 or BRCA2 mutations, compared to placebo. However, olaparib had minimal impact on the overall patient-reported quality of life [141]. Likewise, patients receiving first- through fourth-line therapy for germline BRCA1/2 mutation-associated HER2-negative BC in the phase 3 EMBRACA trial were randomly assigned to receive talazoparib or chemotherapy [140]. In comparison to chemotherapy, talazoparib had a greater ORR and mPFS, but talazoparib did not considerably increase OS when compared to chemotherapy [140]. Based on these results PARPi monotherapy was suggested as SOC for metastatic HER2-negative BC patients with BRCA1/2 mutations [142]. Despite having strong response rates, PARPi-induced responses are generally less durable. Although checkpoint inhibitor monotherapy has a lower response rate than PARPi, it produces longer-lasting effects in mTNBC [143].
Comparing the results of the phase II KEYNOTE-162 trial [144] that combined PD-1 checkpoint inhibitor pembrolizumab with PARPi niraparib to trials with PARPi monotherapy, it became evident that patients with BRCA1 or BRCA2 pathogenic variants (PVs) displayed long-lasting responses with combination treatment [145]. In the phase I/II MEDIOLA basket trial combining olaparib and durvalumab the patients with metastatic HER-2-negative BC with a germline BRCA1/2 PVs were explicitly included in one of the four cohorts [146]. Overall, the combined regimen was well tolerated but it is unclear if the combined approach would be more effective in this group of patients with germline BRCA1/2 PVs than the PARP inhibitor alone, especially in terms of extending the duration of response [146]. Avelumab in combination with talazoparib has been assessed in two JAVELIN basket trials for patients with previously treated solid malignancies, including BC. The JAVELIN trials showed an acceptable level of safety [147]. While initial results from early-phase clinical trials have shown promising activity, larger randomized controlled trials are needed to establish the optimal combination regimen, patient selection criteria, and long-term outcomes. Combining PARP inhibitors with immunotherapy may also pose challenges, such as increased toxicity or the development of resistance. Therefore, careful monitoring and management of adverse events are essential moving forward.
4.2. Combination of Immunotherapy with Chemotherapy
Based on several preclinical and clinical studies it is clear that several chemotherapies kill tumor cells by promoting the recruitment and maturation of APCs, enhancing the antigen presentation, and encouraging T-cell activation [148]. Additionally, by releasing MHC molecules and cell surface antigens, chemotherapy drugs improve the immunogenicity of tumors [149]. Chemotherapy-induced transient immunosuppression results in an enormous release of cyto- and chemokines which boosts immune cell infiltration and activation. Therefore, the combination of PD-(L)1 inhibitor and chemotherapy is a viable strategy to improve immunotherapy efficacy and promote synergistic anti-tumor activity [19]. Numerous clinical trials combining immunotherapy and chemotherapy are being carried out based on this concept with significant clinical advantage attained.
Most clinical trials currently use immunotherapy and chemotherapy together in part because the response to ICIs is slower, whereas chemotherapeutic agents kill tumor cells and alter TME during the therapy period [19]. Previously untreated, advanced TNBC patients were treated with pembrolizumab plus chemotherapy or placebo plus chemotherapy as the first-line treatment in KEYNOTE-355. The chemotherapy regimens were chosen by the treating physicians and included gemcitabine/carboplatin, paclitaxel, and nab-paclitaxel [88]. Patients treated with pembrolizumab, and chemotherapy combination had a significant and clinically meaningful increase in PFS compared to the placebo-chemotherapy group with a combined positive score (CPS) ≥ 10. CPS is determined by the ratio of PD-L1 positive cells (tumor cells, lymphocytes, and macrophages) to the total number of tumor cells using the 22C3 assay [150]. The release of follow-up data showed that when pembrolizumab was added to chemotherapy, OS increased by about 7 months in the CPS ≥ 10 group and side effects were tolerable [150]. In the phase IB/II KEYNOTE-150 trial, patients with mTNBC who had undergone at least two lines of previous therapy were treated with pembrolizumab plus eribulin mesylate. Of the 167 patients recruited, 40% were categorized as stratum 1 since they had not previously received systemic therapy. In this group of patients, the survival was greatest for PD-L1-positive individuals [151]. The IMpassion130 phase III trial [87], further validated the efficacy of this immuno-chemotherapy combination for mTNBC patients who did not receive systemic therapy, following a phase Ib trial (NCT01633970) that showed the safety of atezolizumab plus nab-paclitaxel in patients with locally recurrent or mTNBC [152]. Based on preliminary findings, adding atezolizumab was associated with a benefit for PFS in both PD-L1-positive and intention-to-treat (ITT) populations. Atezolizumab was found to significantly enhance OS in the PD-L1-positive group from 18.0 months to 25.0 months in the second set of intermediate findings; however, in the ITT population, there was no significant difference [153]. As a result, the FDA approved atezolizumab in March 2019 for use as a first-line treatment for patients with late-stage TNBC in combination with nab-paclitaxel [154]. The combination of AKT inhibitor ipatasertib with atezolizumab + paclitaxel/nab-paclitaxel demonstrated excellent efficacy in treating advanced and mTNBC [155].
Nevertheless, these different results were noted in the phase III IMpassion131 trial which examined atezolizumab plus paclitaxel as first-line therapy for patients with advanced or mTNBC and compared the results to placebo plus paclitaxel. This study did not find any discernible differences in PFS between the two groups based on PD-L1 expression [156]. Based on recent single-cell sequencing (scSeq) data, paclitaxel may decrease critical anti-tumor immune cells in the TME while it may increase immunosuppressive macrophages which could impact the efficacy of atezolizumab [157]. However, additional investigations are warranted to validate these findings. In addition to concurrent chemotherapy, another novel approach for the immuno-chemotherapy combination is to induce low-dose chemotherapy before immunotherapy. Patients with mTNBC received no induction or 2 weeks of low-dose cyclophosphamide, cisplatin, doxorubicin, and hypo fractionated irradiation, followed by nivolumab in the phase II TONIC trial. The results suggested that doxorubicin or cisplatin induction, even for a short period, can shift the TIME toward an inflammatory state and enhance the response to nivolumab in TNBC [158]. Pembrolizumab and chemotherapy combination has consistently increased pCR in multiple clinical trials (I-SPY2 [159], KEYNOTE-173 [160], and KEYNOTE-522 [87]) in patients with early-stage TNBC. In July 2021, the FDA approved pembrolizumab as a neoadjuvant treatment for early-stage, high-risk TNBC alongside chemotherapy based on the improved pCR rates noted in these trials [161].
In the phase II GeparNuevo trial, durvalumab or placebo was administered every 4 weeks in addition to chemotherapy and their efficacy was assessed. Addition of durvalumab significantly increased the pCR rates in the window cohort but not in the overall study population [162]. In the NeoTRIP trial, a separate trial of the PD-L1 inhibitor atezolizumab, the efficacy of 8 cycles of carboplatin and nab-paclitaxel with or without atezolizumab was examined in high-risk TNBC. As an adjuvant treatment, 4 cycles of anthracycline regimen chemotherapy were given. The pCR rate in the ITT group was not significantly different with the addition of atezolizumab in a neoadjuvant setting [163]. Conversely, in the IMpassion031 study, atezolizumab given as a single drug with a standard chemotherapy regimen including doxorubicin and paclitaxel significantly increased pCR from 41% in the chemotherapy alone arm to 58% in the ateza-plus chemotherapy arm [164]. The IMpassion130 phase 3 trial, reported in 2018, showed that first-line treatment with atezolizumab plus nab-paclitaxel significantly improved PFS compared to placebo plus nab-paclitaxel in mTNBC. While the overall survival boundary was not crossed in this interim analysis and was not formally tested for statistical significance, numerical increases in median OS were observed in both the intention-to-treat and PD-L1-positive subgroups [165]. However, the FDA approval of atezolizumab was withdrawn due to the negative results from the IMpassion131 trial [166]. It should also be noted that the IMpassion130 and IMpassion131 trials used the SP142 assay for PD-L1 expression, which differs from other assays in detecting PD-L1 levels.
4.3. Combination of Immunotherapy with Radiotherapy
Radiotherapy (RT) is still a major treatment modality in TNBC even after recent advancements in endocrine therapy, chemotherapy, and targeted therapy for BC [134]. Numerous randomized trials have demonstrated that adjuvant radiation therapy decreases locoregional recurrence and improves survival in women with both early-stage and advanced-stage breast cancer. The impact of radiotherapy on immune signaling is still being elucidated [167,168]. Immune cells are attracted to the TME by radiation in several ways. It triggers the release of warning signals from dying tumor cells. DCs consume antigens from cancerous cells and deliver them to lymph nodes. The T cells are then exposed to them, which activates CD8 + and CD4 + T cells. Consequently, chemokines drive effector T-cell recruitment to tumors [169]. In BC patients, RT plus immunotherapy may produce systemic antitumor effects especially when RT is administered at higher doses using more advanced techniques. Potential explanations for these systemic effects include the growth and dissemination of effector immune cells to distant sites because of the local immune priming by RT [170].
The adaptive phase-2 TONIC study, however, demonstrated a limited increase (~10%) in ORR with low-dose radiation combination as compared to nivolumab alone [158]. The best ORRs were observed with nivolumab and chemotherapy combinations (doxorubicin 35%, cisplatin ORR 23%) in this trial as mentioned above. A multi-center phase 2 trial assessed the safety and efficacy of pembrolizumab plus RT in patients with mTNBC (NCT02730130) [171]. This study discovered that the unselected PD-L1 population's ORR in the ITT cohort was 17.6%, which was greater than the ORR of mTNBC patients who had previously received ICI monotherapy. Fifty patients who had received fewer than two lines of systemic therapy were included in a phase II AZTEC trial to receive atezolizumab plus RT (NCT03464942) [172]. Patients were randomized to receive either 24-Gy stereotactic ablative radiotherapy (SABR) in three fractions or 20 Gy SABR in one fraction. Five days following the last RT segment, atezolizumab was initiated. There was no discernible variation in median progression-free survival (mPFS) between the two cohorts. TIL levels of 5% and the PD-L1 expression had little impact on the efficacy [172]. It would be interesting to see the results of numerous trials that are currently investigating the clinical benefit of RT in combination with ICI in women with TNBC.
4.4. Dual Antibody Combinations and Dual Immunotherapies
ADCs can interact with anti-PD-(L)1 agents to improve tumor control [173]. Sacituzumab govitecan targets TROP2 and delivers topoisomerase I inhibitor SN38 to the tumor. The clinical efficiency of this agent with pembrolizumab as a first-line treatment for mTNBC is currently being assessing [19]. Similarly, the safety and efficacy of ladiratuzumab vedotin an ADC that targets LIV-1 [174] is being evaluated in combination with pembrolizumab in a phase Ib/II trial [175].
VEGF is a crucial factor in vascular endothelial cells that promotes angiogenesis, cell invasion, migration, proliferation, and survival, and enhances vascular permeability [176]. The combination of low-dose VEGFR inhibitor apatinib with anti-PD-1 agent camrelizumab and PARP1/2i fuzoloparib demonstrated a manageable safety profile and preliminary antitumor activity in patients with advanced TNBC [177]. FUTURE-C-Plus trial demonstrated that CD8+ and/or PD-L1 positive patients benefit more from the combination of famitinib (VEGFRi), camrelizumab (ICI), and chemotherapy (nab-paclitaxel) combinations [178]. The trial validated the safety, efficacy, and feasibility of triple therapy in TNBC and identified CD8+ positivity as a marker of favorable response with the triple therapy combination in the clinical setting [178].
Dual ICI therapies have been designed to overcome PD-(L)1 inhibitor resistance and reverse the tumor immunosuppressive microenvironment [179]. Durvalumab plus tremelimumab showed preliminary effectiveness and a manageable safety profile (NCT02536794) only in mTNBC patients (ORR 43%) while there was no response in ER+ BC [180]. Responders had higher expression of CD8, granzyme A, and perforin-1 post-therapy as compared to non-responders [180]. In the phase I/II SYNERGY (NCT03616886) trial locally advanced or mTNBC patients were treated with a combination of oleclumab (anti-CD73 antibody), durvalumab, and chemotherapy (carboplatin and paclitaxel). The phase II part of this trial was randomized 1:1 with/without oleclumab. However, this trial did not meet its primary endpoint (insignificant clinical benefit at 24 weeks) [181].
Similarly, in patients with mTNBC, a phase I trial (NCT03256344) assessed the safety of intrahepatic injection of T-VEC in combination with intravenous atezolizumab [182]. The five TNBC patients in their DLT cohorts did not have any dose-limiting toxicities (DLT), however, the majority of TNBC patients (90%) in this trial presented with grade 3 adverse events (AEs) with limited evidence of antitumor activity [182]. A first-in-human trial that included multimodality treatments including chemoradiation, NK cells therapy, typhoid conjugate vaccine (TCV), and a PD-L1 inhibitor as third-line therapy for mTNBC (NCT03387085) found the combination treatment to be safe, well tolerated, and achieved a 56% ORR in early efficacy results [183]. These encouraging results suggest that multimodal treatment will be the way forward for the management of recurrent and metastatic TNBC and may lead to the development of additional multimodality clinical trials.
5. Conclusion and Future Perspectives
The advancements in immunotherapy have brought renewed optimism for women battling local, recurrent, and metastatic triple-negative breast cancer (TNBC). Despite the success of integrating immunogenic chemotherapy with immune checkpoint inhibitors (ICI), particularly in late-stage and metastatic TNBC, trials evaluating adjuvant immune checkpoint inhibitors in operable TNBC like IMpassion030 (NCT03498716) have yielded unsatisfactory outcomes. These innovative treatments provide additional therapeutic options for patients who have undergone extensive prior therapies and developed resistance. Over the past few years a growing number of small molecule inhibitors including tyrosine kinase (EGFR and VEGFR), serine/threonine kinase (ATM, ATR, AKT, CDK1, CDK4/6, CHK1, DNA-PKcs, mTOR, PI3K, and WEE1), dual specific kinase inhibitors (TTK1, MEK), proteasome (PARP), and epigenetic (HDAC) have been tested in TNBC as monotherapy or in combination with other targeted agents or ICI [184,185]. While several of these therapeutic combinations are still in the experimental stage or undergoing clinical trials, they represent promising avenues for the treatment of TNBC (Table 3). Despite the clinical success of targeted small-molecule treatments for TNBC, drug resistance is still an ongoing challenge. Other possibilities include combination treatments, novel mutation inhibitors, and multi-targeted drugs. Novel therapeutic targets, such as BUB1, LIG4, Hh, and XPO1 are being investigated in preclinical or clinical studies for targeting TNBC [185-189]. It is anticipated that in the near future, these small-molecule inhibitors and immunotherapy will be able to work together to increase the anti-tumor activity of these drugs. Combination therapy may prove effective, but uncertainties still exist relating to method, sequence, dosage, and duration with a careful eye toward balancing toxicity and affordability.
Table 3.
List of non-immune therapies under clinical trials for TNBC treatment (accessed information from https://www.clinicaltrials.gov/ on 6/17/2024).
Table 3.
List of non-immune therapies under clinical trials for TNBC treatment (accessed information from https://www.clinicaltrials.gov/ on 6/17/2024).
| Target | Interventions | Clinical status & Identifier | Status |
|---|---|---|---|
| EGFR | Drug: Metformin Drug: Erlotinib |
Phase I NCT01650506 |
Completed |
| PI3K | Drug: BKM120 | Phase II NCT01790932 |
Completed |
| PI3K | Drug: BKM120 and Olaparib Drug: BYL719 and Olaparib |
Phase I NCT01623349 |
Completed |
| PI3K | Drug: BYl719 | Phase II NCT02506556 |
Completed |
| AKT | Drug: Ipatasertib Drug: Paclitaxel Drug: Placebo |
Phase II NCT02301988 |
Completed |
| AKT | Drug: Ipatasertib Drug: Paclitaxel Drug: Placebo |
Phase II NCT02162719 |
Completed |
| AKT | Drug: Paclitaxel Drug: AZD5363 Drug: Placebo |
Phase II NCT02423603 |
Unknown |
| AKT | Drug: Capivasertib Drug: Paclitaxel Drug: Placebo |
Phase III NCT03997123 |
On-going |
| AKT | Drug: Capivasertib Other: Laboratory Biomarker Analysis Drug: Olaparib Other: Pharmacological Study Drug: Vistusertib |
Phase Ib NCT02208375 |
On-going |
| AKT | Drug: GSK1120212 Drug: GSK2141795 |
Phase I NCT01138085 |
Completed |
| mTOR | Drug: Doxil Drug: Bevacizumab Drug: Temsirolimus |
Phase I NCT00761644 |
Completed |
| mTOR | Drug: Everolimus | Phase II NCT01931163 |
Completed |
| mTOR | Drug: Everolimus Drug: Eribulin mesylate Other: Pharmacological study Other: Laboratory biomarker analysis |
Phase I NCT02120469 |
Completed |
| mTOR | Drug: Everolimus Drug: Eribulin |
Phase I NCT02616848 |
Completed |
| CDK4/6 | Drug: Trilaciclib Drug: Gemcitabine Drug: Carboplatin |
Phase 2 NCT02978716 |
Completed |
| CDK4/6 | Drug: Trilaciclib Drug: Gemcitabine Drug: Carboplatin |
Phase 2 NCT02978716 |
Completed |
| ATR | Drug: M6620 Drug: Gemcitabine Drug: Cisplatin Drug: Etoposide Drug: Carboplatin Drug: Irinotecan |
Phase I NCT02157792 |
Completed |
| ATR | Drug: Olaparib Drug: Ceralasertib Drug: Adavosertib |
Phase 2 NCT03330847 |
On-going |
| ATR | Procedure: Biopsy Drug: Capivasertib Drug: Ceralasertib Biological: Durvalumab Drug: Olaparib Other: Quality-of-Life Assessment Drug: Selumetinib |
Phase II NCT03801369 |
On-going |
| CHK1 | Drug: LY2606368 | Phase II NCT02203513 |
Completed |
| WEE1 | Drug: Cisplatin Drug: AZD1775 |
Phase II NCT03012477 |
Completed |
| MEK | Drug: GSK1120212 Drug: GSK2141795 |
Phase I NCT01138085 |
Completed |
| MEK | Drug: Akt Inhibitor GSK2141795 Other: Laboratory Biomarker Analysis Drug: Trametinib |
Phase II NCT01964924 |
Completed |
| MEK | Drug: Ipatasertib Drug: Cobimetinib |
Phase I NCT01562275 |
Completed |
| MET, VEGFR2, RET, AXL, FTL3, etc. | Drug: Cabozantinib | Phase II NCT01738438 |
Completed |
| VEGF, PDGFR, HGF, etc. | Drug: Paclitaxel Drug: Carboplatin Drug: Sunitinib |
Phase I/II NCT00887575 |
Completed |
| VEGF, PDGFR, HGF, etc. | Drug: SU011248 Drug: Chemotherapy |
Phase II NCT00246571 |
Completed |
| Aurora-A, VEGFR, FGFR | Drug: ENMD-2076 | Phase II NCT01639248 |
Completed |
| EGFR, HER2 | Drug: Combination of Veliparib + Lapatinib | Phase: N/A NCT02158507 |
On-going |
| PI3K, mTOR | Drug: Prexasertib Drug: Cisplatin Drug: Cetuximab Drug: G-CSF Drug: Pemetrexed Drug: Fluorouracil Drug: LY3023414 Drug: Leucovorin |
Phase I NCT02124148 |
Completed |
| PARP | Drug: Pamiparib | Phase I/II NCT03333915 |
Completed |
| PARP | Drug: Talazoparib | Phase II NCT03499353 |
Completed |
| PARP | Drug: Olaparib | Phase II NCT02681562 |
Completed |
| PARP | Drug: Olaparib Radiation: Radiation therapy |
Phase I NCT03109080 |
Completed |
| PARP | Drug: Iniparib Drug: Gemcitabine Drug: Carboplatin |
Phase II NCT01045304 |
Completed |
| PARP | Drug: Cyclophosphamide Drug: Placebo Drug: Doxorubicin Drug: Paclitaxel Drug: Carboplatin Drug: Veliparib Drug: Placebo |
Phase III NCT02032277 |
Completed |
| HDAC | Drug: Chidamide combined with Cisplatin | Phase II NCT04192903 |
Completed |
| HDAC | Drug: Entinostat | Phase I NCT03361800 |
Terminated |
| HDAC | Drug: Romidepsin Drug: Cisplatin Drug: Nivolumab |
Phase I/II NCT02393794 |
On-going |
| SMO | Drug: LDE225 Drug: Docetaxel |
Phase I NCT02027376 |
Completed |
| XPO1 | Drug: Selinexor | Phase II NCT02402764 |
Completed |
Integrating artificial intelligence (AI) in treatment planning may revolutionize the prediction of therapeutic outcomes, enabling personalized precision medicine. High-throughput sequencing and AI can identify novel molecular markers and gene signatures, aiding clinicians in selecting the most effective patient-specific therapies. This may then assist the clinical care team in optimally selecting a “tailored patient-specific” therapy that is most likely to work thus opening new horizons in precision medicine [190]. This will require scientists, organizations, and medical professionals to work together to develop databases, remove technological obstacles, and support the creation of AI-assisted systems that can precisely identify the target populations/patients, predict the efficacy and prognosis, and strongly support the use of AI-assisted treatment. We anticipate that with the development of novel drug discovery/prediction datasets, large-scale genomic/genetic datasets, and immune signatures combined with large multicenter clinical trials will soon make significant strides in treating TNBC efficiently [191-195].
Author Contributions
S.N and S.S: Conceptualization; S.S: Writing – original draft; S.T, C.S, S.N: Writing – review & editing.
Funding
This work was supported by NCI R21 (1R21CA252010-01A1), HFHS Research Administration Start Up, HFHS Proposal Development Award, Game on Cancer Award and HFHS-Radiation Oncology Start Up to Shyam Nyati.
Acknowledgments
We thank HFCI for providing a Translational Oncology Postdoctoral Fellowship to Sushmitha Sriramulu.
Conflicts of Interest
SS, ST, SN: no COI; CS: Exact Sciences (paid consultant - no direct conflict).
References
- Zagami, P.; Carey, L.A. Triple negative breast cancer: Pitfalls and progress. NPJ Breast Cancer 2022, 8, 95. [Google Scholar] [CrossRef]
- Litton, J.K.; Rugo, H.S.; Ettl, J.; Hurvitz, S.A.; Gonçalves, A.; Lee, K.-H.; Fehrenbacher, L.; Yerushalmi, R.; Mina, L.A.; Martin, M. Talazoparib in patients with advanced breast cancer and a germline BRCA mutation. New England Journal of Medicine 2018, 379, 753–763. [Google Scholar] [CrossRef]
- Robson, M.; Im, S.-A.; Senkus, E.; Xu, B.; Domchek, S.M.; Masuda, N.; Delaloge, S.; Li, W.; Tung, N.; Armstrong, A. Olaparib for metastatic breast cancer in patients with a germline BRCA mutation. New England Journal of Medicine 2017, 377, 523–533. [Google Scholar] [CrossRef]
- Bauer, K.R.; Brown, M.; Cress, R.D.; Parise, C.A.; Caggiano, V. Descriptive analysis of estrogen receptor (ER)-negative, progesterone receptor (PR)-negative, and HER2-negative invasive breast cancer, the so-called triple-negative phenotype: a population-based study from the California cancer Registry. Cancer 2007, 109, 1721–1728. [Google Scholar] [CrossRef]
- Loizides, S.; Constantinidou, A. Triple negative breast cancer: Immunogenicity, tumor microenvironment, and immunotherapy. Front Genet 2022, 13, 1095839. [Google Scholar] [CrossRef]
- Liedtke, C.; Mazouni, C.; Hess, K.R.; Andre, F.; Tordai, A.; Mejia, J.A.; Symmans, W.F.; Gonzalez-Angulo, A.M.; Hennessy, B.; Green, M.; et al. Response to Neoadjuvant Therapy and Long-Term Survival in Patients With Triple-Negative Breast Cancer. J Clin Oncol 2023, 41, 1809–1815. [Google Scholar] [CrossRef]
- Blows, F.M.; Driver, K.E.; Schmidt, M.K.; Broeks, A.; van Leeuwen, F.E.; Wesseling, J.; Cheang, M.C.; Gelmon, K.; Nielsen, T.O.; Blomqvist, C.; et al. Subtyping of breast cancer by immunohistochemistry to investigate a relationship between subtype and short and long term survival: a collaborative analysis of data for 10,159 cases from 12 studies. PLoS Med 2010, 7, e1000279. [Google Scholar] [CrossRef]
- Cortazar, P.; Zhang, L.; Untch, M.; Mehta, K.; Costantino, J.P.; Wolmark, N.; Bonnefoi, H.; Cameron, D.; Gianni, L.; Valagussa, P.; et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet 2014, 384, 164–172. [Google Scholar] [CrossRef]
- Burstein, M.D.; Tsimelzon, A.; Poage, G.M.; Covington, K.R.; Contreras, A.; Fuqua, S.A.; Savage, M.I.; Osborne, C.K.; Hilsenbeck, S.G.; Chang, J.C.; et al. Comprehensive genomic analysis identifies novel subtypes and targets of triple-negative breast cancer. Clin Cancer Res 2015, 21, 1688–1698. [Google Scholar] [CrossRef]
- Yin, L.; Duan, J.J.; Bian, X.W.; Yu, S.C. Triple-negative breast cancer molecular subtyping and treatment progress. Breast Cancer Res 2020, 22, 61. [Google Scholar] [CrossRef]
- Speers, C.; Tsimelzon, A.; Sexton, K.; Herrick, A.M.; Gutierrez, C.; Culhane, A.; Quackenbush, J.; Hilsenbeck, S.; Chang, J.; Brown, P. Identification of novel kinase targets for the treatment of estrogen receptor-negative breast cancer. Clin Cancer Res 2009, 15, 6327–6340. [Google Scholar] [CrossRef]
- Lehmann, B.D.; Bauer, J.A.; Chen, X.; Sanders, M.E.; Chakravarthy, A.B.; Shyr, Y.; Pietenpol, J.A. Identification of human triple-negative breast cancer subtypes and preclinical models for selection of targeted therapies. J Clin Invest 2011, 121, 2750–2767. [Google Scholar] [CrossRef]
- Lehmann, B.D.; Jovanovic, B.; Chen, X.; Estrada, M.V.; Johnson, K.N.; Shyr, Y.; Moses, H.L.; Sanders, M.E.; Pietenpol, J.A. Refinement of Triple-Negative Breast Cancer Molecular Subtypes: Implications for Neoadjuvant Chemotherapy Selection. PLoS One 2016, 11, e0157368. [Google Scholar] [CrossRef]
- Schmid, P.; Adams, S.; Rugo, H.S.; Schneeweiss, A.; Barrios, C.H.; Iwata, H.; Dieras, V.; Hegg, R.; Im, S.A.; Shaw Wright, G.; et al. Atezolizumab and Nab-Paclitaxel in Advanced Triple-Negative Breast Cancer. N Engl J Med 2018, 379, 2108–2121. [Google Scholar] [CrossRef]
- Corradini, S.; Krug, D.; Meattini, I.; Matuschek, C.; Bolke, E.; Francolini, G.; Baumann, R.; Figlia, V.; Pazos, M.; Tonetto, F.; et al. Preoperative radiotherapy: A paradigm shift in the treatment of breast cancer? A review of literature. Crit Rev Oncol Hematol 2019, 141, 102–111. [Google Scholar] [CrossRef]
- Lin, Y.Y.; Gao, H.F.; Yang, X.; Zhu, T.; Zheng, X.X.; Ji, F.; Zhang, L.L.; Yang, C.Q.; Yang, M.; Li, J.Q.; et al. Neoadjuvant therapy in triple-negative breast cancer: A systematic review and network meta-analysis. Breast 2022, 66, 126–135. [Google Scholar] [CrossRef]
- Loibl, S.; O'Shaughnessy, J.; Untch, M.; Sikov, W.M.; Rugo, H.S.; McKee, M.D.; Huober, J.; Golshan, M.; von Minckwitz, G.; Maag, D.; et al. Addition of the PARP inhibitor veliparib plus carboplatin or carboplatin alone to standard neoadjuvant chemotherapy in triple-negative breast cancer (BrighTNess): a randomised, phase 3 trial. Lancet Oncol 2018, 19, 497–509. [Google Scholar] [CrossRef]
- Valencia, G.A.; Rioja, P.; Morante, Z.; Ruiz, R.; Fuentes, H.; Castaneda, C.A.; Vidaurre, T.; Neciosup, S.; Gomez, H.L. Immunotherapy in triple-negative breast cancer: A literature review and new advances. World J Clin Oncol 2022, 13, 219–236. [Google Scholar] [CrossRef]
- Li, L.; Zhang, F.; Liu, Z.; Fan, Z. Immunotherapy for Triple-Negative Breast Cancer: Combination Strategies to Improve Outcome. Cancers (Basel) 2023, 15. [Google Scholar] [CrossRef]
- Shah, M.; Osgood, C.L.; Amatya, A.K.; Fiero, M.H.; Pierce, W.F.; Nair, A.; Herz, J.; Robertson, K.J.; Mixter, B.D.; Tang, S.; et al. FDA Approval Summary: Pembrolizumab for Neoadjuvant and Adjuvant Treatment of Patients with High-Risk Early-Stage Triple-Negative Breast Cancer. Clin Cancer Res 2022, 28, 5249–5253. [Google Scholar] [CrossRef]
- Nolan, E.; Savas, P.; Policheni, A.N.; Darcy, P.K.; Vaillant, F.; Mintoff, C.P.; Dushyanthen, S.; Mansour, M.; Pang, J.B.; Fox, S.B.; et al. Combined immune checkpoint blockade as a therapeutic strategy for BRCA1-mutated breast cancer. Sci Transl Med 2017, 9. [Google Scholar] [CrossRef] [PubMed]
- Safonov, A.; Jiang, T.; Bianchini, G.; Gyorffy, B.; Karn, T.; Hatzis, C.; Pusztai, L. Immune Gene Expression Is Associated with Genomic Aberrations in Breast Cancer. Cancer Res 2017, 77, 3317–3324. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; He, S. The Characteristics of Tumor Microenvironment in Triple Negative Breast Cancer. Cancer Manag Res 2022, 14, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Ciarka, A.; Piatek, M.; Peksa, R.; Kunc, M.; Senkus, E. Tumor-Infiltrating Lymphocytes (TILs) in Breast Cancer: Prognostic and Predictive Significance across Molecular Subtypes. Biomedicines 2024, 12. [Google Scholar] [CrossRef]
- Mao, Y.; Qu, Q.; Chen, X.; Huang, O.; Wu, J.; Shen, K. The Prognostic Value of Tumor-Infiltrating Lymphocytes in Breast Cancer: A Systematic Review and Meta-Analysis. PLoS One 2016, 11, e0152500. [Google Scholar] [CrossRef] [PubMed]
- Denkert, C.; von Minckwitz, G.; Darb-Esfahani, S.; Lederer, B.; Heppner, B.I.; Weber, K.E.; Budczies, J.; Huober, J.; Klauschen, F.; Furlanetto, J.; et al. Tumour-infiltrating lymphocytes and prognosis in different subtypes of breast cancer: a pooled analysis of 3771 patients treated with neoadjuvant therapy. Lancet Oncol 2018, 19, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Tay, R.E.; Richardson, E.K.; Toh, H.C. Revisiting the role of CD4(+) T cells in cancer immunotherapy-new insights into old paradigms. Cancer Gene Ther 2021, 28, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Chanmee, T.; Ontong, P.; Konno, K.; Itano, N. Tumor-associated macrophages as major players in the tumor microenvironment. Cancers (Basel) 2014, 6, 1670–1690. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Wang, J.; Chen, Z.; Luo, J.; Guo, W.; Sun, L.; Lin, L. Targeting M2-like tumor-associated macrophages is a potential therapeutic approach to overcome antitumor drug resistance. NPJ Precis Oncol 2024, 8, 31. [Google Scholar] [CrossRef]
- Sami, E.; Paul, B.T.; Koziol, J.A.; ElShamy, W.M. The Immunosuppressive Microenvironment in BRCA1-IRIS-Overexpressing TNBC Tumors Is Induced by Bidirectional Interaction with Tumor-Associated Macrophages. Cancer Res 2020, 80, 1102–1117. [Google Scholar] [CrossRef]
- Gascard, P.; Tlsty, T.D. Carcinoma-associated fibroblasts: orchestrating the composition of malignancy. Genes Dev 2016, 30, 1002–1019. [Google Scholar] [CrossRef] [PubMed]
- Takai, K.; Le, A.; Weaver, V.M.; Werb, Z. Targeting the cancer-associated fibroblasts as a treatment in triple-negative breast cancer. Oncotarget 2016, 7, 82889–82901. [Google Scholar] [CrossRef] [PubMed]
- Nagaraj, S.; Schrum, A.G.; Cho, H.I.; Celis, E.; Gabrilovich, D.I. Mechanism of T cell tolerance induced by myeloid-derived suppressor cells. J Immunol 2010, 184, 3106–3116. [Google Scholar] [CrossRef] [PubMed]
- Queen, M.M.; Ryan, R.E.; Holzer, R.G.; Keller-Peck, C.R.; Jorcyk, C.L. Breast cancer cells stimulate neutrophils to produce oncostatin M: potential implications for tumor progression. Cancer Res 2005, 65, 8896–8904. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.W.; Kim, K.D.; Lee, H.K. The role of dendritic cells in tumor microenvironments and their uses as therapeutic targets. BMB Rep 2021, 54, 31–43. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Z.; Wang, R.; Wang, X.; Yang, H.; Dong, J.; He, X.; Yang, Y.; Guo, J.; Cui, J.; Zhou, Z. Impaired function of dendritic cells within the tumor microenvironment. Front Immunol 2023, 14, 1213629. [Google Scholar] [CrossRef] [PubMed]
- Domagala, J.; Lachota, M.; Klopotowska, M.; Graczyk-Jarzynka, A.; Domagala, A.; Zhylko, A.; Soroczynska, K.; Winiarska, M. The Tumor Microenvironment-A Metabolic Obstacle to NK Cells' Activity. Cancers (Basel) 2020, 12. [Google Scholar] [CrossRef]
- Youn, J.I.; Gabrilovich, D.I. The biology of myeloid-derived suppressor cells: the blessing and the curse of morphological and functional heterogeneity. Eur J Immunol 2010, 40, 2969–2975. [Google Scholar] [CrossRef]
- Udumula, M.P.; Sakr, S.; Dar, S.; Alvero, A.B.; Ali-Fehmi, R.; Abdulfatah, E.; Li, J.; Jiang, J.; Tang, A.; Buekers, T.; et al. Ovarian cancer modulates the immunosuppressive function of CD11b(+)Gr1(+) myeloid cells via glutamine metabolism. Mol Metab 2021, 53, 101272. [Google Scholar] [CrossRef] [PubMed]
- Ma, T.; Renz, B.W.; Ilmer, M.; Koch, D.; Yang, Y.; Werner, J.; Bazhin, A.V. Myeloid-Derived Suppressor Cells in Solid Tumors. Cells 2022, 11. [Google Scholar] [CrossRef]
- Bochet, L.; Meulle, A.; Imbert, S.; Salles, B.; Valet, P.; Muller, C. Cancer-associated adipocytes promotes breast tumor radioresistance. Biochem Biophys Res Commun 2011, 411, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Guo, Z.; Zhang, R.; Yang, A.G.; Zheng, G. Diversity of immune checkpoints in cancer immunotherapy. Front Immunol 2023, 14, 1121285. [Google Scholar] [CrossRef] [PubMed]
- Ye, F.; Dewanjee, S.; Li, Y.; Jha, N.K.; Chen, Z.-S.; Kumar, A.; Vishakha; Behl, T. ; Jha, S.K.; Tang, H. Advancements in clinical aspects of targeted therapy and immunotherapy in breast cancer. Molecular Cancer 2023, 22, 105. [Google Scholar] [CrossRef] [PubMed]
- Berraondo, P.; Sanmamed, M.F.; Ochoa, M.C.; Etxeberria, I.; Aznar, M.A.; Pérez-Gracia, J.L.; Rodríguez-Ruiz, M.E.; Ponz-Sarvise, M.; Castañón, E.; Melero, I. Cytokines in clinical cancer immunotherapy. British Journal of Cancer 2019, 120, 6–15. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Margolin, K. Cytokines in cancer immunotherapy. Cancers (Basel) 2011, 3, 3856–3893. [Google Scholar] [CrossRef] [PubMed]
- Petrina, M.; Martin, J.; Basta, S. Granulocyte macrophage colony-stimulating factor has come of age: From a vaccine adjuvant to antiviral immunotherapy. Cytokine Growth Factor Rev 2021, 59, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Deckers, J.; Anbergen, T.; Hokke, A.M.; de Dreu, A.; Schrijver, D.P.; de Bruin, K.; Toner, Y.C.; Beldman, T.J.; Spangler, J.B.; de Greef, T.F.A.; et al. Engineering cytokine therapeutics. Nature Reviews Bioengineering 2023, 1, 286–303. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, K.G.; Vrabel, M.R.; Mantooth, S.M.; Hopkins, J.J.; Wagner, E.S.; Gabaldon, T.A.; Zaharoff, D.A. Localized Interleukin-12 for Cancer Immunotherapy. Front Immunol 2020, 11, 575597. [Google Scholar] [CrossRef] [PubMed]
- Abdou, Y.; Goudarzi, A.; Yu, J.X.; Upadhaya, S.; Vincent, B.; Carey, L.A. Immunotherapy in triple negative breast cancer: beyond checkpoint inhibitors. npj Breast Cancer 2022, 8, 121. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.M.; Rolig, A.S.; Charych, D.H.; Hoch, U.; Kasiewicz, M.J.; Rose, D.C.; McNamara, M.J.; Hilgart-Martiszus, I.F.; Redmond, W.L. NKTR-214 immunotherapy synergizes with radiotherapy to stimulate systemic CD8(+) T cell responses capable of curing multi-focal cancer. J Immunother Cancer 2020, 8. [Google Scholar] [CrossRef] [PubMed]
- Cavazzoni, A.; Digiacomo, G. Role of Cytokines and Other Soluble Factors in Tumor Development: Rationale for New Therapeutic Strategies. Cells 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Conlon, K.C.; Miljkovic, M.D.; Waldmann, T.A. Cytokines in the Treatment of Cancer. J Interferon Cytokine Res 2019, 39, 6–21. [Google Scholar] [CrossRef] [PubMed]
- Dutcher, J.P.; Schwartzentruber, D.J.; Kaufman, H.L.; Agarwala, S.S.; Tarhini, A.A.; Lowder, J.N.; Atkins, M.B. High dose interleukin-2 (Aldesleukin) - expert consensus on best management practices-2014. Journal for ImmunoTherapy of Cancer 2014, 2, 26. [Google Scholar] [CrossRef] [PubMed]
- Page, D.B.; Pucilowska, J.; Sanchez, K.G.; Conrad, V.K.; Conlin, A.K.; Acheson, A.K.; Perlewitz, K.S.; Imatani, J.H.; Aliabadi-Wahle, S.; Moxon, N.; et al. A Phase Ib Study of Preoperative, Locoregional IRX-2 Cytokine Immunotherapy to Prime Immune Responses in Patients with Early-Stage Breast Cancer. Clin Cancer Res 2020, 26, 1595–1605. [Google Scholar] [CrossRef] [PubMed]
- Waldmann, T.A. Cytokines in Cancer Immunotherapy. Cold Spring Harb Perspect Biol 2018, 10. [Google Scholar] [CrossRef]
- Wesolowski, J.; Tankiewicz-Kwedlo, A.; Pawlak, D. Modern Immunotherapy in the Treatment of Triple-Negative Breast Cancer. Cancers (Basel) 2022, 14. [Google Scholar] [CrossRef]
- Gemmete, J.J.; Mukherji, S.K. Trastuzumab (herceptin). AJNR Am J Neuroradiol 2011, 32, 1373–1374. [Google Scholar] [CrossRef] [PubMed]
- Baez Navarro, X.; van den Ender, N.S.; Nguyen, A.; Sinke, R.; Westenend, P.; van Brakel, J.B.; Stobbe, C.; Westerga, J.; van Deurzen, C.H.M. HER2-low and tumor infiltrating lymphocytes in triple negative breast cancer: are they mutually connected? European Journal of Cancer 2024, 200. [Google Scholar] [CrossRef]
- Garcia, J.; Hurwitz, H.I.; Sandler, A.B.; Miles, D.; Coleman, R.L.; Deurloo, R.; Chinot, O.L. Bevacizumab (Avastin®) in cancer treatment: A review of 15 years of clinical experience and future outlook. Cancer Treatment Reviews 2020, 86, 102017. [Google Scholar] [CrossRef] [PubMed]
- Sasich, L.D.; Sukkari, S.R. The US FDAs withdrawal of the breast cancer indication for Avastin (bevacizumab). Saudi Pharm J 2012, 20, 381–385. [Google Scholar] [CrossRef] [PubMed]
- Luo, C.; Wang, P.; He, S.; Zhu, J.; Shi, Y.; Wang, J. Progress and Prospect of Immunotherapy for Triple-Negative Breast Cancer. Front Oncol 2022, 12, 919072. [Google Scholar] [CrossRef]
- Chang, H.L.; Schwettmann, B.; McArthur, H.L.; Chan, I.S. Antibody-drug conjugates in breast cancer: overcoming resistance and boosting immune response. The Journal of Clinical Investigation 2023, 133. [Google Scholar] [CrossRef] [PubMed]
- Panowski, S.; Bhakta, S.; Raab, H.; Polakis, P.; Junutula, J.R. Site-specific antibody drug conjugates for cancer therapy. MAbs 2014, 6, 34–45. [Google Scholar] [CrossRef]
- Vonderheide, R.H. CD40 Agonist Antibodies in Cancer Immunotherapy. Annu Rev Med 2020, 71, 47–58. [Google Scholar] [CrossRef]
- Azar, I.; Alkassis, S.; Fukui, J.; Alsawah, F.; Fedak, K.; Al Hallak, M.N.; Sukari, A.; Nagasaka, M. Spotlight on Trastuzumab Deruxtecan (DS-8201,T-DXd) for HER2 Mutation Positive Non-Small Cell Lung Cancer. Lung Cancer (Auckl) 2021, 12, 103–114. [Google Scholar] [CrossRef] [PubMed]
- Mark, C.; Lee, J.S.; Cui, X.; Yuan, Y. Antibody-Drug Conjugates in Breast Cancer: Current Status and Future Directions. Int J Mol Sci 2023, 24. [Google Scholar] [CrossRef]
- Modi, S.; Jacot, W.; Yamashita, T.; Sohn, J.; Vidal, M.; Tokunaga, E.; Tsurutani, J.; Ueno, N.T.; Prat, A.; Chae, Y.S.; et al. Trastuzumab Deruxtecan in Previously Treated HER2-Low Advanced Breast Cancer. New England Journal of Medicine 2022, 387, 9–20. [Google Scholar] [CrossRef]
- Bartsch, R.; Berghoff, A.S.; Furtner, J.; Marhold, M.; Bergen, E.S.; Roider-Schur, S.; Starzer, A.M.; Forstner, H.; Rottenmanner, B.; Dieckmann, K.; et al. Trastuzumab deruxtecan in HER2-positive breast cancer with brain metastases: a single-arm, phase 2 trial. Nature Medicine 2022, 28, 1840–1847. [Google Scholar] [CrossRef]
- Shi, F.; Liu, Y.; Zhou, X.; Shen, P.; Xue, R.; Zhang, M. Disitamab vedotin: a novel antibody-drug conjugates for cancer therapy. Drug Deliv 2022, 29, 1335–1344. [Google Scholar] [CrossRef]
- Fenn, K.M.; Kalinsky, K. Sacituzumab govitecan: antibody-drug conjugate in triple-negative breast cancer and other solid tumors. Drugs Today (Barc) 2019, 55, 575–585. [Google Scholar] [CrossRef] [PubMed]
- Bardia, A.; Rugo, H.S.; Tolaney, S.M.; Loirat, D.; Punie, K.; Oliveira, M.; Brufsky, A.; Kalinsky, K.; Cortés, J.; Shaughnessy, J.O.; et al. Final Results From the Randomized Phase III ASCENT Clinical Trial in Metastatic Triple-Negative Breast Cancer and Association of Outcomes by Human Epidermal Growth Factor Receptor 2 and Trophoblast Cell Surface Antigen 2 Expression. Journal of Clinical Oncology 2024, 42, 1738–1744. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, A.; Cusmai, A.; Acquafredda, S.; Rinaldi, L.; Palmiotti, G. Ladiratuzumab vedotin for metastatic triple negative cancer: preliminary results, key challenges, and clinical potential. Expert Opin Investig Drugs 2022, 31, 495–498. [Google Scholar] [CrossRef] [PubMed]
- Modi, S.; Pusztai, L.; Forero, A.; Mita, M.; Miller, K.; Weise, A.; Krop, I.; Burris, H., III; Kalinsky, K.; Tsai, M.; et al. Abstract PD3-14: Phase 1 study of the antibody-drug conjugate SGN-LIV1A in patients with heavily pretreated triple-negative metastatic breast cancer. Cancer Research 2018, 78, PD3–14. [Google Scholar] [CrossRef]
- Tsai, M.; Han, H.S.; Montero, A.J.; Tkaczuk, K.H.; Assad, H.; Pusztai, L.; Hurvitz, S.A.; Wilks, S.T.; Specht, J.M.; Nanda, R.; et al. 259P Weekly ladiratuzumab vedotin monotherapy for metastatic triple-negative breast cancer. Annals of Oncology 2021, 32, S474–S475. [Google Scholar] [CrossRef]
- Ma, F.; Qiu, F.; Tong, Z.; Wang, J.; Tan, Y.; Bai, R.; Zhou, Q.; Xing, X. Preliminary results from a first-in-human study of ESG401, a trophoblast cell-surface antigen 2 (TROP2) antibody drug conjugate (ADC), in patients with locally advanced/metastatic solid tumors. Journal of Clinical Oncology 2023, 41, 1100–1100. [Google Scholar] [CrossRef]
- Ma, F.; Qiu, F.; Tong, Z.; Shi, Y.; Yu, G.; Wu, X.; Wang, H.; Wang, J.; Yang, H.; Liu, A.; et al. ESG401, a trophoblast cell-surface antigen 2 (TROP2) antibody drug conjugate (ADC), for the treatment of first-line metastatic triple negative breast cancer (mTNBC). Journal of Clinical Oncology 2024, 42, e13132–e13132. [Google Scholar] [CrossRef]
- Bardia, A.; Pusztai, L.; Albain, K.; Ciruelos, E.M.; Im, S.A.; Hershman, D.; Kalinsky, K.; Isaacs, C.; Loirat, D.; Testa, L.; et al. TROPION-Breast03: a randomized phase III global trial of datopotamab deruxtecan ± durvalumab in patients with triple-negative breast cancer and residual invasive disease at surgical resection after neoadjuvant therapy. Ther Adv Med Oncol 2024, 16, 17588359241248336. [Google Scholar] [CrossRef] [PubMed]
- Bardia, A.; Krop, I.E.; Kogawa, T.; Juric, D.; Tolcher, A.W.; Hamilton, E.P.; Mukohara, T.; Lisberg, A.; Shimizu, T.; Spira, A.I.; et al. Datopotamab Deruxtecan in Advanced or Metastatic HR+/HER2– and Triple-Negative Breast Cancer: Results From the Phase I TROPION-PanTumor01 Study. Journal of Clinical Oncology 2024, 42, 2281–2294. [Google Scholar] [CrossRef] [PubMed]
- Byun, D.J.; Wolchok, J.D.; Rosenberg, L.M.; Girotra, M. Cancer immunotherapy - immune checkpoint blockade and associated endocrinopathies. Nat Rev Endocrinol 2017, 13, 195–207. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Hu, Y.; Xue, J.; Li, J.; Yi, J.; Bu, J.; Zhang, Z.; Qiu, P.; Gu, X. Correction: Advances in immunotherapy for triple-negative breast cancer. Molecular Cancer 2023, 22, 154. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, F.S.; Gaule, P.; McGuire, J.; Patel, K.; Blenman, K.; Pusztai, L.; Rimm, D.L. PD-L1 Protein Expression on Both Tumor Cells and Macrophages are Associated with Response to Neoadjuvant Durvalumab with Chemotherapy in Triple-negative Breast Cancer. Clin Cancer Res 2020, 26, 5456–5461. [Google Scholar] [CrossRef] [PubMed]
- Hargadon, K.M.; Johnson, C.E.; Williams, C.J. Immune checkpoint blockade therapy for cancer: An overview of FDA-approved immune checkpoint inhibitors. Int Immunopharmacol 2018, 62, 29–39. [Google Scholar] [CrossRef]
- Nanda, R.; Chow, L.Q.; Dees, E.C.; Berger, R.; Gupta, S.; Geva, R.; Pusztai, L.; Pathiraja, K.; Aktan, G.; Cheng, J.D.; et al. Pembrolizumab in Patients With Advanced Triple-Negative Breast Cancer: Phase Ib KEYNOTE-012 Study. J Clin Oncol 2016, 34, 2460–2467. [Google Scholar] [CrossRef] [PubMed]
- Adams, S.; Loi, S.; Toppmeyer, D.; Cescon, D.W.; De Laurentiis, M.; Nanda, R.; Winer, E.P.; Mukai, H.; Tamura, K.; Armstrong, A.; et al. Pembrolizumab monotherapy for previously untreated, PD-L1-positive, metastatic triple-negative breast cancer: cohort B of the phase II KEYNOTE-086 study. Ann Oncol 2019, 30, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Ganguly, S.; Gogia, A. Pembrolizumab monotherapy in advanced triple-negative breast cancer. The Lancet Oncology 2021, 22, e224. [Google Scholar] [CrossRef] [PubMed]
- Bian, L.; Zhang, H.; Wang, T.; Zhang, S.; Song, H.; Xu, M.; Yao, S.; Jiang, Z. JS001, an anti-PD-1 mAb for advanced triple negative breast cancer patients after multi-line systemic therapy in a phase I trial. Ann Transl Med 2019, 7, 435. [Google Scholar] [CrossRef] [PubMed]
- Schmid, P.; Cortes, J.; Pusztai, L.; McArthur, H.; Kümmel, S.; Bergh, J.; Denkert, C.; Park, Y.H.; Hui, R.; Harbeck, N.; et al. Pembrolizumab for Early Triple-Negative Breast Cancer. N Engl J Med 2020, 382, 810–821. [Google Scholar] [CrossRef] [PubMed]
- Cortes, J.; Cescon, D.W.; Rugo, H.S.; Nowecki, Z.; Im, S.A.; Yusof, M.M.; Gallardo, C.; Lipatov, O.; Barrios, C.H.; Holgado, E.; et al. Pembrolizumab plus chemotherapy versus placebo plus chemotherapy for previously untreated locally recurrent inoperable or metastatic triple-negative breast cancer (KEYNOTE-355): a randomised, placebo-controlled, double-blind, phase 3 clinical trial. Lancet 2020, 396, 1817–1828. [Google Scholar] [CrossRef]
- Emens, L.A.; Cruz, C.; Eder, J.P.; Braiteh, F.; Chung, C.; Tolaney, S.M.; Kuter, I.; Nanda, R.; Cassier, P.A.; Delord, J.P.; et al. Long-term Clinical Outcomes and Biomarker Analyses of Atezolizumab Therapy for Patients With Metastatic Triple-Negative Breast Cancer: A Phase 1 Study. JAMA Oncol 2019, 5, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Dirix, L.Y.; Takacs, I.; Jerusalem, G.; Nikolinakos, P.; Arkenau, H.T.; Forero-Torres, A.; Boccia, R.; Lippman, M.E.; Somer, R.; Smakal, M.; et al. Avelumab, an anti-PD-L1 antibody, in patients with locally advanced or metastatic breast cancer: a phase 1b JAVELIN Solid Tumor study. Breast Cancer Res Treat 2018, 167, 671–686. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, F.; Agostinetto, E.; Miggiano, C.; De Sanctis, R.; Zambelli, A.; Santoro, A. Hope and Hype around Immunotherapy in Triple-Negative Breast Cancer. Cancers (Basel) 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, A.; Gharibi, T.; Marofi, F.; Babaloo, Z.; Baradaran, B. CTLA-4: From mechanism to autoimmune therapy. Int Immunopharmacol 2020, 80, 106221. [Google Scholar] [CrossRef] [PubMed]
- Peng, Z.; Su, P.; Yang, Y.; Yao, X.; Zhang, Y.; Jin, F.; Yang, B. Identification of CTLA-4 associated with tumor microenvironment and competing interactions in triple negative breast cancer by co-expression network analysis. J Cancer 2020, 11, 6365–6375. [Google Scholar] [CrossRef] [PubMed]
- Kaewkangsadan, V.; Verma, C.; Eremin, J.M.; Cowley, G.; Ilyas, M.; Eremin, O. Tumour-draining axillary lymph nodes in patients with large and locally advanced breast cancers undergoing neoadjuvant chemotherapy (NAC): the crucial contribution of immune cells (effector, regulatory) and cytokines (Th1, Th2) to immune-mediated tumour cell death induced by NAC. BMC Cancer 2018, 18, 123. [Google Scholar] [CrossRef]
- Zhang, X.; Sharma, P.K.; Peter Goedegebuure, S.; Gillanders, W.E. Personalized cancer vaccines: Targeting the cancer mutanome. Vaccine 2017, 35, 1094–1100. [Google Scholar] [CrossRef] [PubMed]
- Burke, E.E.; Kodumudi, K.; Ramamoorthi, G.; Czerniecki, B.J. Vaccine Therapies for Breast Cancer. Surg Oncol Clin N Am 2019, 28, 353–367. [Google Scholar] [CrossRef] [PubMed]
- Mittendorf, E.A.; Ardavanis, A.; Litton, J.K.; Shumway, N.M.; Hale, D.F.; Murray, J.L.; Perez, S.A.; Ponniah, S.; Baxevanis, C.N.; Papamichail, M.; et al. Primary analysis of a prospective, randomized, single-blinded phase II trial evaluating the HER2 peptide GP2 vaccine in breast cancer patients to prevent recurrence. Oncotarget 2016, 7, 66192–66201. [Google Scholar] [CrossRef] [PubMed]
- Mittendorf, E.A.; Clifton, G.T.; Holmes, J.P.; Schneble, E.; van Echo, D.; Ponniah, S.; Peoples, G.E. Final report of the phase I/II clinical trial of the E75 (nelipepimut-S) vaccine with booster inoculations to prevent disease recurrence in high-risk breast cancer patients. Ann Oncol 2014, 25, 1735–1742. [Google Scholar] [CrossRef]
- Kalli, K.R.; Block, M.S.; Kasi, P.M.; Erskine, C.L.; Hobday, T.J.; Dietz, A.; Padley, D.; Gustafson, M.P.; Shreeder, B.; Puglisi-Knutson, D.; et al. Folate Receptor Alpha Peptide Vaccine Generates Immunity in Breast and Ovarian Cancer Patients. Clin Cancer Res 2018, 24, 3014–3025. [Google Scholar] [CrossRef]
- Heery, C.R.; Ibrahim, N.K.; Arlen, P.M.; Mohebtash, M.; Murray, J.L.; Koenig, K.; Madan, R.A.; McMahon, S.; Marté, J.L.; Steinberg, S.M.; et al. Docetaxel Alone or in Combination With a Therapeutic Cancer Vaccine (PANVAC) in Patients With Metastatic Breast Cancer: A Randomized Clinical Trial. JAMA Oncol 2015, 1, 1087–1095. [Google Scholar] [CrossRef]
- Mohebtash, M.; Tsang, K.Y.; Madan, R.A.; Huen, N.Y.; Poole, D.J.; Jochems, C.; Jones, J.; Ferrara, T.; Heery, C.R.; Arlen, P.M.; et al. A pilot study of MUC-1/CEA/TRICOM poxviral-based vaccine in patients with metastatic breast and ovarian cancer. Clin Cancer Res 2011, 17, 7164–7173. [Google Scholar] [CrossRef] [PubMed]
- Svane, I.M.; Pedersen, A.E.; Johansen, J.S.; Johnsen, H.E.; Nielsen, D.; Kamby, C.; Ottesen, S.; Balslev, E.; Gaarsdal, E.; Nikolajsen, K.; et al. Vaccination with p53 peptide-pulsed dendritic cells is associated with disease stabilization in patients with p53 expressing advanced breast cancer; monitoring of serum YKL-40 and IL-6 as response biomarkers. Cancer Immunol Immunother 2007, 56, 1485–1499. [Google Scholar] [CrossRef] [PubMed]
- Qi, C.J.; Ning, Y.L.; Han, Y.S.; Min, H.Y.; Ye, H.; Zhu, Y.L.; Qian, K.Q. Autologous dendritic cell vaccine for estrogen receptor (ER)/progestin receptor (PR) double-negative breast cancer. Cancer Immunol Immunother 2012, 61, 1415–1424. [Google Scholar] [CrossRef] [PubMed]
- Avigan, D.; Vasir, B.; Gong, J.; Borges, V.; Wu, Z.; Uhl, L.; Atkins, M.; Mier, J.; McDermott, D.; Smith, T.; et al. Fusion cell vaccination of patients with metastatic breast and renal cancer induces immunological and clinical responses. Clin Cancer Res 2004, 10, 4699–4708. [Google Scholar] [CrossRef] [PubMed]
- Vonderheide, R.H.; Glennie, M.J. Agonistic CD40 antibodies and cancer therapy. Clin Cancer Res 2013, 19, 1035–1043. [Google Scholar] [CrossRef] [PubMed]
- Budd, G.T.; Johnson, J.M.; Rhoades, E.E.; Moore, H.C.F.; Kruse, M.L.; Roesch, E.E.; Abraham, J.; Elliott, B.; Lach, D.; Tuohy, V.K. Phase I trial of an alpha-lactalbumin vaccine in patients with moderate- to high-risk operable triple-negative breast cancer (TNBC). Journal of Clinical Oncology 2022, 40, TPS1125–TPS1125. [Google Scholar] [CrossRef]
- Disis, M.; Liu, Y.; Stanton, S.; Gwin, W.; Coveler, A.; Liao, J.; Childs, J.; Cecil, D. 546 A phase I dose escalation study of STEMVAC, a multi-antigen, multi-epitope Th1 selective plasmid-based vaccine, targeting stem cell associated proteins in patients with advanced breast cancer. Journal for ImmunoTherapy of Cancer 2022, 10, A571–A571. [Google Scholar] [CrossRef]
- Zhao, L.; Cao, Y.J. Engineered T Cell Therapy for Cancer in the Clinic. Front Immunol 2019, 10, 2250. [Google Scholar] [CrossRef]
- Xu, N.; Palmer, D.C.; Robeson, A.C.; Shou, P.; Bommiasamy, H.; Laurie, S.J.; Willis, C.; Dotti, G.; Vincent, B.G.; Restifo, N.P.; et al. STING agonist promotes CAR T cell trafficking and persistence in breast cancer. J Exp Med 2021, 218. [Google Scholar] [CrossRef] [PubMed]
- Tchou, J.; Zhao, Y.; Levine, B.L.; Zhang, P.J.; Davis, M.M.; Melenhorst, J.J.; Kulikovskaya, I.; Brennan, A.L.; Liu, X.; Lacey, S.F.; et al. Safety and Efficacy of Intratumoral Injections of Chimeric Antigen Receptor (CAR) T Cells in Metastatic Breast Cancer. Cancer Immunol Res 2017, 5, 1152–1161. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.R.; Jiang, Y.Z.; Xu, X.E.; Yu, K.D.; Jin, X.; Hu, X.; Zuo, W.J.; Hao, S.; Wu, J.; Liu, G.Y.; et al. Comprehensive transcriptome analysis identifies novel molecular subtypes and subtype-specific RNAs of triple-negative breast cancer. Breast Cancer Res 2016, 18, 33. [Google Scholar] [CrossRef] [PubMed]
- Ghosn, M.; Cheema, W.; Zhu, A.; Livschitz, J.; Maybody, M.; Boas, F.E.; Santos, E.; Kim, D.; Beattie, J.A.; Offin, M.; et al. Image-guided interventional radiological delivery of chimeric antigen receptor (CAR) T cells for pleural malignancies in a phase I/II clinical trial. Lung Cancer 2022, 165, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Adusumilli, P.S.; Zauderer, M.G.; Rivière, I.; Solomon, S.B.; Rusch, V.W.; O'Cearbhaill, R.E.; Zhu, A.; Cheema, W.; Chintala, N.K.; Halton, E.; et al. A Phase I Trial of Regional Mesothelin-Targeted CAR T-cell Therapy in Patients with Malignant Pleural Disease, in Combination with the Anti-PD-1 Agent Pembrolizumab. Cancer Discov 2021, 11, 2748–2763. [Google Scholar] [CrossRef] [PubMed]
- Kufe, D.W. MUC1-C oncoprotein as a target in breast cancer: activation of signaling pathways and therapeutic approaches. Oncogene 2013, 32, 1073–1081. [Google Scholar] [CrossRef] [PubMed]
- Bamdad, C.C.; Yuan, Y.; Specht, J.M.; Stewart, A.K.; Smagghe, B.J.; Lin, S.C.-M.; Carter, M.G.; Synold, T.W.; Frankel, P.H.; Parekh, V.; et al. Phase I/II first-in-human CAR T–targeting MUC1 transmembrane cleavage product (MUC1*) in patients with metastatic breast cancer. Journal of Clinical Oncology 2022, 40, TPS1130–TPS1130. [Google Scholar] [CrossRef]
- Gaglia, P.; Caldarola, B.; Bussone, R.; Potente, F.; Lauro, D.; Jayme, A.; Caldarola, L. Prognostic value of CEA and ferritin assay in breast cancer: a multivariate analysis. Eur J Cancer Clin Oncol 1988, 24, 1151–1155. [Google Scholar] [CrossRef] [PubMed]
- Phase Ia/Ib Trial of 2nd Generation Anti-CEA Designer T Cells in Metastatic Breast Cancer. 2008.
- Luen, S.J.; Savas, P.; Fox, S.B.; Salgado, R.; Loi, S. Tumour-infiltrating lymphocytes and the emerging role of immunotherapy in breast cancer. Pathology 2017, 49, 141–155. [Google Scholar] [CrossRef] [PubMed]
- Fukuhara, H.; Ino, Y.; Todo, T. Oncolytic virus therapy: A new era of cancer treatment at dawn. Cancer Sci 2016, 107, 1373–1379. [Google Scholar] [CrossRef]
- Thoidingjam, S.; Sriramulu, S.; Freytag, S.; Brown, S.L.; Kim, J.H.; Chetty, I.J.; Siddiqui, F.; Movsas, B.; Nyati, S. Oncolytic virus-based suicide gene therapy for cancer treatment: a perspective of the clinical trials conducted at Henry Ford Health. Transl Med Commun 2023, 8, 11. [Google Scholar] [CrossRef] [PubMed]
- Zheng, M.; Huang, J.; Tong, A.; Yang, H. Oncolytic Viruses for Cancer Therapy: Barriers and Recent Advances. Mol Ther Oncolytics 2019, 15, 234–247. [Google Scholar] [CrossRef]
- Kaufman, H.L.; Kohlhapp, F.J.; Zloza, A. Oncolytic viruses: a new class of immunotherapy drugs. Nat Rev Drug Discov 2015, 14, 642–662. [Google Scholar] [CrossRef]
- Kaufman, H.L.; Shalhout, S.Z.; Iodice, G. Talimogene Laherparepvec: Moving From First-In-Class to Best-In-Class. Front Mol Biosci 2022, 9, 834841. [Google Scholar] [CrossRef]
- Kai, M.; Marx, A.N.; Liu, D.D.; Shen, Y.; Gao, H.; Reuben, J.M.; Whitman, G.; Krishnamurthy, S.; Ross, M.I.; Litton, J.K.; et al. A phase II study of talimogene laherparepvec for patients with inoperable locoregional recurrence of breast cancer. Sci Rep 2021, 11, 22242. [Google Scholar] [CrossRef]
- Nokisalmi, P.; Pesonen, S.; Escutenaire, S.; Särkioja, M.; Raki, M.; Cerullo, V.; Laasonen, L.; Alemany, R.; Rojas, J.; Cascallo, M.; et al. Oncolytic adenovirus ICOVIR-7 in patients with advanced and refractory solid tumors. Clin Cancer Res 2010, 16, 3035–3043. [Google Scholar] [CrossRef] [PubMed]
- Hemminki, O.; Parviainen, S.; Juhila, J.; Turkki, R.; Linder, N.; Lundin, J.; Kankainen, M.; Ristimäki, A.; Koski, A.; Liikanen, I.; et al. Immunological data from cancer patients treated with Ad5/3-E2F-Δ24-GMCSF suggests utility for tumor immunotherapy. Oncotarget 2015, 6, 4467–4481. [Google Scholar] [CrossRef]
- Monaco, M.L.; Idris, O.A.; Essani, K. Triple-Negative Breast Cancer: Basic Biology and Immuno-Oncolytic Viruses. Cancers (Basel) 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Lauer, U.M.; Beil, J. Oncolytic viruses: challenges and considerations in an evolving clinical landscape. Future Oncology 2022, 18, 2713–2732. [Google Scholar] [CrossRef]
- Liu, M.; Peng, K.-W.; Federspiel, M.; Russell, S.; Brunton, B.; Zhou, Y.; Packiriswamy, N.; Hubbard, J.; Loprinzi, C.; Peethambaram, P.; et al. Abstract P6-21-03: Phase I trial of intratumoral (IT) administration of a NIS-expressing derivative manufactured from a genetically engineered strain of measles virus (MV). Cancer Research 2019, 79, P6–21. [Google Scholar] [CrossRef]
- Vanneman, M.; Dranoff, G. Combining immunotherapy and targeted therapies in cancer treatment. Nat Rev Cancer 2012, 12, 237–251. [Google Scholar] [CrossRef] [PubMed]
- Fabian, K.P.; Wolfson, B.; Hodge, J.W. From Immunogenic Cell Death to Immunogenic Modulation: Select Chemotherapy Regimens Induce a Spectrum of Immune-Enhancing Activities in the Tumor Microenvironment. Front Oncol 2021, 11, 728018. [Google Scholar] [CrossRef]
- Nedeljković, M.; Damjanović, A. Mechanisms of Chemotherapy Resistance in Triple-Negative Breast Cancer-How We Can Rise to the Challenge. Cells 2019, 8. [Google Scholar] [CrossRef] [PubMed]
- Bayat Mokhtari, R.; Homayouni, T.S.; Baluch, N.; Morgatskaya, E.; Kumar, S.; Das, B.; Yeger, H. Combination therapy in combating cancer. Oncotarget 2017, 8, 38022–38043. [Google Scholar] [CrossRef]
- Jungles, K.M.; Holcomb, E.A.; Pearson, A.N.; Jungles, K.R.; Bishop, C.R.; Pierce, L.J.; Green, M.D.; Speers, C.W. Updates in combined approaches of radiotherapy and immune checkpoint inhibitors for the treatment of breast cancer. Front Oncol 2022, 12, 1022542. [Google Scholar] [CrossRef] [PubMed]
- Obidiro, O.; Battogtokh, G.; Akala, E.O. Triple Negative Breast Cancer Treatment Options and Limitations: Future Outlook. Pharmaceutics 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Ragupathi, A.; Singh, M.; Perez, A.M.; Zhang, D. Targeting the BRCA1/2 deficient cancer with PARP inhibitors: Clinical outcomes and mechanistic insights. Front Cell Dev Biol 2023, 11, 1133472. [Google Scholar] [CrossRef] [PubMed]
- Barchiesi, G.; Roberto, M.; Verrico, M.; Vici, P.; Tomao, S.; Tomao, F. Emerging Role of PARP Inhibitors in Metastatic Triple Negative Breast Cancer. Current Scenario and Future Perspectives. Front Oncol 2021, 11, 769280. [Google Scholar] [CrossRef] [PubMed]
- De Santis, P.; Perrone, M.; Guarini, C.; Santoro, A.N.; Laface, C.; Carrozzo, D.; Oliva, G.R.; Fedele, P. Early-stage triple negative breast cancer: the therapeutic role of immunotherapy and the prognostic value of pathological complete response. Explor Target Antitumor Ther 2024, 5, 232–250. [Google Scholar] [CrossRef] [PubMed]
- Robson, M.; Im, S.-A.; Senkus, E.; Xu, B.; Domchek, S.M.; Masuda, N.; Delaloge, S.; Li, W.; Tung, N.; Armstrong, A.; et al. Olaparib for Metastatic Breast Cancer in Patients with a Germline <i>BRCA</i> Mutation. New England Journal of Medicine 2017, 377, 523–533. [Google Scholar] [CrossRef] [PubMed]
- Litton, J.K.; Rugo, H.S.; Ettl, J.; Hurvitz, S.A.; Gonçalves, A.; Lee, K.H.; Fehrenbacher, L.; Yerushalmi, R.; Mina, L.A.; Martin, M.; et al. Talazoparib in Patients with Advanced Breast Cancer and a Germline BRCA Mutation. N Engl J Med 2018, 379, 753–763. [Google Scholar] [CrossRef] [PubMed]
- Tutt, A.N.J.; Garber, J.E.; Kaufman, B.; Viale, G.; Fumagalli, D.; Rastogi, P.; Gelber, R.D.; Azambuja, E.d.; Fielding, A.; Balmaña, J.; et al. Adjuvant Olaparib for Patients with <i>BRCA1</i>- or <i>BRCA2</i>-Mutated Breast Cancer. New England Journal of Medicine 2021, 384, 2394–2405. [Google Scholar] [CrossRef]
- Gupta, T.; Purington, N.; Liu, M.; Han, S.; Sledge, G.; Schapira, L.; Kurian, A.W. Incident comorbidities after tamoxifen or aromatase inhibitor therapy in a racially and ethnically diverse cohort of women with breast cancer. Breast Cancer Research and Treatment 2022, 196, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Miglietta, F.; Cinquini, M.; Dieci, M.V.; Cortesi, L.; Criscitiello, C.; Montemurro, F.; Del Mastro, L.; Zambelli, A.; Biganzoli, L.; Levaggi, A.; et al. PARP-inhibitors for BRCA1/2-related advanced HER2-negative breast cancer: A meta-analysis and GRADE recommendations by the Italian Association of Medical Oncology. Breast 2022, 66, 293–304. [Google Scholar] [CrossRef] [PubMed]
- Vinayak, S.; Tolaney, S.M.; Schwartzberg, L.S.; Mita, M.M.; McCann, G.A.-L.; Tan, A.R.; Hendrickson, A.E.W.; Forero-Torres, A.; Anders, C.K.; Wulf, G.M.; et al. TOPACIO/Keynote-162: Niraparib + pembrolizumab in patients (pts) with metastatic triple-negative breast cancer (TNBC), a phase 2 trial. Journal of Clinical Oncology 2018, 36, 1011–1011. [Google Scholar] [CrossRef]
- Vinayak, S.; Tolaney, S.M.; Schwartzberg, L.; Mita, M.; McCann, G.; Tan, A.R.; Wahner-Hendrickson, A.E.; Forero, A.; Anders, C.; Wulf, G.M.; et al. Open-label Clinical Trial of Niraparib Combined With Pembrolizumab for Treatment of Advanced or Metastatic Triple-Negative Breast Cancer. JAMA Oncology 2019, 5, 1132–1140. [Google Scholar] [CrossRef] [PubMed]
- Domchek, S.M.; Postel-Vinay, S.; Im, S.A.; Park, Y.H.; Delord, J.P.; Italiano, A.; Alexandre, J.; You, B.; Bastian, S.; Krebs, M.G.; et al. Olaparib and durvalumab in patients with germline BRCA-mutated metastatic breast cancer (MEDIOLA): an open-label, multicentre, phase 1/2, basket study. Lancet Oncol 2020, 21, 1155–1164. [Google Scholar] [CrossRef] [PubMed]
- Yap, T.A.; Bardia, A.; Dvorkin, M.; Galsky, M.D.; Beck, J.T.; Wise, D.R.; Karyakin, O.; Rubovszky, G.; Kislov, N.; Rohrberg, K.; et al. Avelumab Plus Talazoparib in Patients With Advanced Solid Tumors: The JAVELIN PARP Medley Nonrandomized Controlled Trial. JAMA Oncol 2023, 9, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Galluzzi, L.; Buqué, A.; Kepp, O.; Zitvogel, L.; Kroemer, G. Immunological Effects of Conventional Chemotherapy and Targeted Anticancer Agents. Cancer Cell 2015, 28, 690–714. [Google Scholar] [CrossRef] [PubMed]
- Zitvogel, L.; Tesniere, A.; Kroemer, G. Cancer despite immunosurveillance: immunoselection and immunosubversion. Nat Rev Immunol 2006, 6, 715–727. [Google Scholar] [CrossRef] [PubMed]
- Cortes, J.; Rugo, H.S.; Cescon, D.W.; Im, S.-A.; Yusof, M.M.; Gallardo, C.; Lipatov, O.; Barrios, C.H.; Perez-Garcia, J.; Iwata, H.; et al. Pembrolizumab plus Chemotherapy in Advanced Triple-Negative Breast Cancer. New England Journal of Medicine 2022, 387, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Tolaney, S.M.; Kalinsky, K.; Kaklamani, V.G.; D'Adamo, D.R.; Aktan, G.; Tsai, M.L.; O'Regan, R.M.; Kaufman, P.A.; Wilks, S.T.; Andreopoulou, E.; et al. Eribulin Plus Pembrolizumab in Patients with Metastatic Triple-Negative Breast Cancer (ENHANCE 1): A Phase Ib/II Study. Clin Cancer Res 2021, 27, 3061–3068. [Google Scholar] [CrossRef] [PubMed]
- Adams, S.; Gatti-Mays, M.E.; Kalinsky, K.; Korde, L.A.; Sharon, E.; Amiri-Kordestani, L.; Bear, H.; McArthur, H.L.; Frank, E.; Perlmutter, J.; et al. Current Landscape of Immunotherapy in Breast Cancer: A Review. JAMA Oncol 2019, 5, 1205–1214. [Google Scholar] [CrossRef]
- Schmid, P.; Rugo, H.S.; Adams, S.; Schneeweiss, A.; Barrios, C.H.; Iwata, H.; Diéras, V.; Henschel, V.; Molinero, L.; Chui, S.Y.; et al. Atezolizumab plus nab-paclitaxel as first-line treatment for unresectable, locally advanced or metastatic triple-negative breast cancer (IMpassion130): updated efficacy results from a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol 2020, 21, 44–59. [Google Scholar] [CrossRef] [PubMed]
- Emens, L.A.; Adams, S.; Barrios, C.H.; Diéras, V.; Iwata, H.; Loi, S.; Rugo, H.S.; Schneeweiss, A.; Winer, E.P.; Patel, S.; et al. First-line atezolizumab plus nab-paclitaxel for unresectable, locally advanced, or metastatic triple-negative breast cancer: IMpassion130 final overall survival analysis. Ann Oncol 2021, 32, 983–993. [Google Scholar] [CrossRef]
- Schmid, P.; Turner, N.C.; Barrios, C.H.; Isakoff, S.J.; Kim, S.B.; Sablin, M.P.; Saji, S.; Savas, P.; Vidal, G.A.; Oliveira, M.; et al. First-Line Ipatasertib, Atezolizumab, and Taxane Triplet for Metastatic Triple-Negative Breast Cancer: Clinical and Biomarker Results. Clin Cancer Res 2024, 30, 767–778. [Google Scholar] [CrossRef]
- Miles, D.; Gligorov, J.; André, F.; Cameron, D.; Schneeweiss, A.; Barrios, C.; Xu, B.; Wardley, A.; Kaen, D.; Andrade, L.; et al. Primary results from IMpassion131, a double-blind, placebo-controlled, randomised phase III trial of first-line paclitaxel with or without atezolizumab for unresectable locally advanced/metastatic triple-negative breast cancer. Ann Oncol 2021, 32, 994–1004. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, H.; Mo, H.; Hu, X.; Gao, R.; Zhao, Y.; Liu, B.; Niu, L.; Sun, X.; Yu, X.; et al. Single-cell analyses reveal key immune cell subsets associated with response to PD-L1 blockade in triple-negative breast cancer. Cancer Cell 2021, 39, 1578–1593. [Google Scholar] [CrossRef]
- Voorwerk, L.; Slagter, M.; Horlings, H.M.; Sikorska, K.; van de Vijver, K.K.; de Maaker, M.; Nederlof, I.; Kluin, R.J.C.; Warren, S.; Ong, S.; et al. Immune induction strategies in metastatic triple-negative breast cancer to enhance the sensitivity to PD-1 blockade: the TONIC trial. Nature Medicine 2019, 25, 920–928. [Google Scholar] [CrossRef] [PubMed]
- Nanda, R.; Liu, M.C.; Yau, C.; Shatsky, R.; Pusztai, L.; Wallace, A.; Chien, A.J.; Forero-Torres, A.; Ellis, E.; Han, H.; et al. Effect of Pembrolizumab Plus Neoadjuvant Chemotherapy on Pathologic Complete Response in Women With Early-Stage Breast Cancer: An Analysis of the Ongoing Phase 2 Adaptively Randomized I-SPY2 Trial. JAMA Oncol 2020, 6, 676–684. [Google Scholar] [CrossRef]
- Schmid, P.; Cortes, J.; Pusztai, L.; McArthur, H.; Kümmel, S.; Bergh, J.; Denkert, C.; Park, Y.H.; Hui, R.; Harbeck, N.; et al. Pembrolizumab for Early Triple-Negative Breast Cancer. New England Journal of Medicine 2020, 382, 810–821. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.M.; Rushton, T.; Nsiah, F.; Stone, R.L.; Beavis, A.L.; Gaillard, S.L.; Dobi, A.; Fader, A.N. Long-term disease-free survival with chemotherapy and pembrolizumab in a patient with unmeasurable, advanced stage dedifferentiated endometrial carcinoma. Gynecologic Oncology Reports 2024, 53, 101380. [Google Scholar] [CrossRef]
- Loibl, S.; Untch, M.; Burchardi, N.; Huober, J.; Sinn, B.V.; Blohmer, J.U.; Grischke, E.M.; Furlanetto, J.; Tesch, H.; Hanusch, C.; et al. A randomised phase II study investigating durvalumab in addition to an anthracycline taxane-based neoadjuvant therapy in early triple-negative breast cancer: clinical results and biomarker analysis of GeparNuevo study. Ann Oncol 2019, 30, 1279–1288. [Google Scholar] [CrossRef] [PubMed]
- Gianni, L.; Huang, C.S.; Egle, D.; Bermejo, B.; Zamagni, C.; Thill, M.; Anton, A.; Zambelli, S.; Bianchini, G.; Russo, S.; et al. Pathologic complete response (pCR) to neoadjuvant treatment with or without atezolizumab in triple-negative, early high-risk and locally advanced breast cancer: NeoTRIP Michelangelo randomized study. Ann Oncol 2022, 33, 534–543. [Google Scholar] [CrossRef]
- Mittendorf, E.A.; Zhang, H.; Barrios, C.H.; Saji, S.; Jung, K.H.; Hegg, R.; Koehler, A.; Sohn, J.; Iwata, H.; Telli, M.L.; et al. Neoadjuvant atezolizumab in combination with sequential nab-paclitaxel and anthracycline-based chemotherapy versus placebo and chemotherapy in patients with early-stage triple-negative breast cancer (IMpassion031): a randomised, double-blind, phase 3 trial. The Lancet 2020, 396, 1090–1100. [Google Scholar] [CrossRef]
- Schmid, P.; Adams, S.; Rugo, H.S.; Schneeweiss, A.; Barrios, C.H.; Iwata, H.; Diéras, V.; Hegg, R.; Im, S.-A.; Wright, G.S.; et al. Atezolizumab and Nab-Paclitaxel in Advanced Triple-Negative Breast Cancer. New England Journal of Medicine 2018, 379, 2108–2121. [Google Scholar] [CrossRef]
- Miles, D.; Gligorov, J.; André, F.; Cameron, D.; Schneeweiss, A.; Barrios, C.; Xu, B.; Wardley, A.; Kaen, D.; Andrade, L. Primary results from IMpassion131, a double-blind, placebo-controlled, randomised phase III trial of first-line paclitaxel with or without atezolizumab for unresectable locally advanced/metastatic triple-negative breast cancer. Annals of Oncology 2021, 32, 994–1004. [Google Scholar] [CrossRef]
- Radiotherapy to regional nodes in early breast cancer: an individual patient data meta-analysis of 14 324 women in 16 trials. Lancet 2023, 402, 1991–2003. [CrossRef] [PubMed]
- McGale, P.; Taylor, C.; Correa, C.; Cutter, D.; Duane, F.; Ewertz, M.; Gray, R.; Mannu, G.; Peto, R.; Whelan, T.; et al. Effect of radiotherapy after mastectomy and axillary surgery on 10-year recurrence and 20-year breast cancer mortality: meta-analysis of individual patient data for 8135 women in 22 randomised trials. Lancet 2014, 383, 2127–2135. [Google Scholar] [CrossRef]
- Charpentier, M.; Spada, S.; Van Nest, S.J.; Demaria, S. Radiation therapy-induced remodeling of the tumor immune microenvironment. Seminars in Cancer Biology 2022, 86, 737–747. [Google Scholar] [CrossRef]
- Ho, A.Y.; Wright, J.L.; Blitzblau, R.C.; Mutter, R.W.; Duda, D.G.; Norton, L.; Bardia, A.; Spring, L.; Isakoff, S.J.; Chen, J.H.; et al. Optimizing Radiation Therapy to Boost Systemic Immune Responses in Breast Cancer: A Critical Review for Breast Radiation Oncologists. Int J Radiat Oncol Biol Phys 2020, 108, 227–241. [Google Scholar] [CrossRef] [PubMed]
- McArthur, H.L.; Barker, C.A.; Gucalp, A.; Lebron-Zapata, L.; Wen, Y.H.; Phung, A.; Rodine, M.; Arnold, B.; Zhang, Z.; Ho, A. A single-arm, phase II study assessing the efficacy of pembrolizumab (pembro) plus radiotherapy (RT) in metastatic triple negative breast cancer (mTNBC). Journal of Clinical Oncology 2018, 36, 14–14. [Google Scholar] [CrossRef]
- David, S.; Savas, P.; Siva, S.; White, M.; Neeson, M.W.; White, S.; Marx, G.; Cheuk, R.; Grogan, M.; Farrell, M.; et al. Abstract PD10-02: A randomised phase II trial of single fraction or multi-fraction SABR (stereotactic ablative body radiotherapy) with atezolizumab in patients with advanced triple negative breast cancer (AZTEC trial). Cancer Research 2022, 82, PD10–02. [Google Scholar] [CrossRef]
- Sau, S.; Petrovici, A.; Alsaab, H.O.; Bhise, K.; Iyer, A.K. PDL-1 Antibody Drug Conjugate for Selective Chemo-Guided Immune Modulation of Cancer. Cancers (Basel) 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- de Nonneville, A.; Finetti, P.; Boudin, L.; Denicolaï, E.; Birnbaum, D.; Mamessier, E.; Bertucci, F. Prognostic and Predictive Value of LIV1 Expression in Early Breast Cancer and by Molecular Subtype. Pharmaceutics 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Meisel, J.L.; Pluard, T.J.; Vinayak, S.; Stringer-Reasor, E.M.; Brown-Glaberman, U.; Dillon, P.M.; Basho, R.K.; Varadarajan, R.; O'Shaughnessy, J.; Han, H.S.; et al. Phase 1b/2 study of ladiratuzumab vedotin (LV) in combination with pembrolizumab for first-line treatment of triple-negative breast cancer (SGNLVA-002, trial in progress). Journal of Clinical Oncology 2022, 40, TPS1127–TPS1127. [Google Scholar] [CrossRef]
- Niu, G.; Chen, X. Vascular endothelial growth factor as an anti-angiogenic target for cancer therapy. Curr Drug Targets 2010, 11, 1000–1017. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Shao, B.; Tong, Z.; Ouyang, Q.; Wang, Y.; Xu, G.; Li, S.; Li, H. A phase Ib study of camrelizumab in combination with apatinib and fuzuloparib in patients with recurrent or metastatic triple-negative breast cancer. BMC Med 2022, 20, 321. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.Y.; Xu, Y.; Chen, L.; Fan, L.; Ma, X.Y.; Zhao, S.; Song, X.Q.; Hu, X.; Yang, W.T.; Chai, W.J.; et al. Combined angiogenesis and PD-1 inhibition for immunomodulatory TNBC: concept exploration and biomarker analysis in the FUTURE-C-Plus trial. Mol Cancer 2022, 21, 84. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, Y.; Mittra, A.; Naqash, A.R.; Takebe, N. A review of mechanisms of resistance to immune checkpoint inhibitors and potential strategies for therapy. Cancer Drug Resist 2020, 3, 252–275. [Google Scholar] [CrossRef] [PubMed]
- Santa-Maria, C.A.; Kato, T.; Park, J.H.; Kiyotani, K.; Rademaker, A.; Shah, A.N.; Gross, L.; Blanco, L.Z.; Jain, S.; Flaum, L.; et al. A pilot study of durvalumab and tremelimumab and immunogenomic dynamics in metastatic breast cancer. Oncotarget 2018, 9, 18985–18996. [Google Scholar] [CrossRef] [PubMed]
- Buisseret, L.; Loirat, D.; Aftimos, P.; Maurer, C.; Punie, K.; Debien, V.; Kristanto, P.; Eiger, D.; Goncalves, A.; Ghiringhelli, F.; et al. Paclitaxel plus carboplatin and durvalumab with or without oleclumab for women with previously untreated locally advanced or metastatic triple-negative breast cancer: the randomized SYNERGY phase I/II trial. Nat Commun 2023, 14, 7018. [Google Scholar] [CrossRef] [PubMed]
- Hecht, J.R.; Raman, S.S.; Chan, A.; Kalinsky, K.; Baurain, J.F.; Jimenez, M.M.; Garcia, M.M.; Berger, M.D.; Lauer, U.M.; Khattak, A.; et al. Phase Ib study of talimogene laherparepvec in combination with atezolizumab in patients with triple negative breast cancer and colorectal cancer with liver metastases. ESMO Open 2023, 8, 100884. [Google Scholar] [CrossRef] [PubMed]
- Kistler, M.; Nangia, C.; To, C.; Sender, L.; Lee, J.; Jones, F.; Jafari, O.; Seery, T.; Rabizadeh, S.; Niazi, K.; et al. Abstract P5-04-02: Safety and efficacy from first-in-human immunotherapy combining NK and T cell activation with off-the-shelf high-affinity CD16 NK cell line (haNK) in patients with 2nd-line or greater metastatic triple-negative breast cancer (TNBC). Cancer Research 2020, 80, P5–04. [Google Scholar] [CrossRef]
- Sriramulu, S.; Thoidingjam, S.; Brown, S.L.; Siddiqui, F.; Movsas, B.; Nyati, S. Molecular targets that sensitize cancer to radiation killing: From the bench to the bedside. Biomed Pharmacother 2023, 158, 114126. [Google Scholar] [CrossRef] [PubMed]
- Ou, Y.; Wang, M.; Xu, Q.; Sun, B.; Jia, Y. Small molecule agents for triple negative breast cancer: Current status and future prospects. Translational Oncology 2024, 41, 101893. [Google Scholar] [CrossRef] [PubMed]
- Sriramulu, S.; Thoidingjam, S.; Chen, W.M.; Hassan, O.; Siddiqui, F.; Brown, S.L.; Movsas, B.; Green, M.D.; Davis, A.J.; Speers, C.; et al. BUB1 regulates non-homologous end joining pathway to mediate radioresistance in triple-negative breast cancer. J Exp Clin Cancer Res 2024, 43, 163. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Holloway, M.P.; Nguyen, K.; McCauley, D.; Landesman, Y.; Kauffman, M.G.; Shacham, S.; Altura, R.A. XPO1 (CRM1) inhibition represses STAT3 activation to drive a survivin-dependent oncogenic switch in triple-negative breast cancer. Molecular cancer therapeutics 2014, 13, 675–686. [Google Scholar] [CrossRef] [PubMed]
- Cicirò, Y.; Ragusa, D.; Sala, A. Expression of the checkpoint kinase BUB1 is a predictor of response to cancer therapies. Scientific Reports 2024, 14, 4461. [Google Scholar] [CrossRef] [PubMed]
- Sriramulu, S.; Thoidingjam, S.; Siddiqui, F.; Brown, S.L.; Movsas, B.; Walker, E.; Nyati, S. BUB1 Inhibition Sensitizes TNBC Cell Lines to Chemotherapy and Radiotherapy. Biomolecules 2024, 14, 625. [Google Scholar] [CrossRef] [PubMed]
- Xie, J.; Luo, X.; Deng, X.; Tang, Y.; Tian, W.; Cheng, H.; Zhang, J.; Zou, Y.; Guo, Z.; Xie, X. Advances in artificial intelligence to predict cancer immunotherapy efficacy. Front Immunol 2022, 13, 1076883. [Google Scholar] [CrossRef] [PubMed]
- Boniolo, F.; Dorigatti, E.; Ohnmacht, A.J.; Saur, D.; Schubert, B.; Menden, M.P. Artificial intelligence in early drug discovery enabling precision medicine. Expert Opin Drug Discov 2021, 16, 991–1007. [Google Scholar] [CrossRef] [PubMed]
- Garrone, O.; La Porta, C.A.M. Artificial Intelligence for Precision Oncology of Triple-Negative Breast Cancer: Learning from Melanoma. Cancers (Basel) 2024, 16. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Hu, J.; Zheng, Y.; Zhao, S.; Ma, J. Artificial intelligence: opportunities and challenges in the clinical applications of triple-negative breast cancer. Br J Cancer 2023, 128, 2141–2149. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Zhang, N.; Zhang, H.; Zhou, R.; Li, Z.; Yang, X.; Wu, W.; Li, H.; Luo, P.; Wang, Z.; et al. Artificial intelligence learning landscape of triple-negative breast cancer uncovers new opportunities for enhancing outcomes and immunotherapy responses. Journal of Big Data 2023, 10, 132. [Google Scholar] [CrossRef]
- Qureshi, R.; Irfan, M.; Gondal, T.M.; Khan, S.; Wu, J.; Hadi, M.U.; Heymach, J.; Le, X.; Yan, H.; Alam, T. AI in drug discovery and its clinical relevance. Heliyon 2023, 9, e17575. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



