
Submitted:
14 August 2024
Posted:
15 August 2024
You are already at the latest version
Abstract
The mosquito-borne zoonotic nematode parasites, Dirofilaria immitis and Dirofilaria repens, primarily affect dogs. In recent years, their distribution has expanded due to various factors influencing vector-borne pathogens. This study aimed to investigate the comparative prevalence of infection in dogs and humans within a hyperenzootic region of Europe and to estimate the proportional relationship between infection prevalence in dogs and humans, in the concept of “One Health”. To this end, 604 blood samples from dogs and 625 serum samples from humans living in the Thrace region of northeastern Greece were collected. Dog samples were examined using Kott’s test for Dirofilaria spp. microfilariae and a commercial serological test for D. immitis antigen. Human sera were analysed by western blot for both parasites. The overall prevalence of infection in dogs was 177 (29.3%), with 173 (28.6%) testing positive for D. immitis and 7 (1.3%) for D. repens, including 6 (1%) cases of mixed infection. Specific IgG antibodies were detected in 42 (6.7%) human samples, with 24 (3.8%) positive for D. immitis and 18 (2.9%) for D. repens. The infection proportion in humans was 23.4% of the corresponding canine infection, indicating a high risk of human infection in this hyperenzootic region.
Keywords:
comparative epidemiology
; dog
; Greece
; heartworm
; human dirofilariosis
; human
; one health
; prevalence
; pulmonary dirofilariosis
; subcutaneous dirofilariosis
; zoonosis
1. Introduction
Dirofilaria immitis and Dirofilaria repens (Rhabditida: Onchocercidae) are nematode parasites transmitted by the bites of infected culicid mosquitoes. While both primarily affect domestic dogs, other animals, particularly cats and wild carnivores, can also be infected [1]. Dirofilaria immitis, which has a worldwide distribution, parasitises the pulmonary artery and the right chambers of the heart, leading to canine cardiopulmonary dirofilariosis, commonly known as heartworm disease. In contrast, Dirofilaria repens is found in subcutaneous tissues, causing subcutaneous dirofilariosis, and is endemic in Europe, Asia, and Africa, but not in the Americas [2]. Regardless of the adult parasites' location, their offspring, the microfilariae, circulate in the bloodstream of competent hosts and can be transmitted to mosquito vectors, where they develop to the infective stage [2].
Both parasites have important zoonotic implications as they may infect humans, especially in hyperenzootic areas, causing pulmonary, subcutaneous or ocular dirofilariosis [3]. Although humans are accidental and in principle dead-end hosts for these parasites, the infections are considered emerging, as cases have increased in numbers in the last few decades [1].
The distribution of Dirofilaria species in Europe is expanding from the southern endemic areas to central and northern countries that were, until recently, considered free of infection [4]. In Greece, the prevalence of infection in dogs is higher in northern regions and appears to be increasing in the south, where it was, until a few years ago, very low [5,6,7,8,9]. It has been documented that the prevalence of infection in dogs in a given area may predict the rate of infection of other permissive hosts, e.g. cats [6,10,11]. Furthermore, seroepidemiological studies in humans living in endemic areas reveal seroprevalence rates similar to those recorded in dogs from the same regions [1].
As expected, most human cases in Europe have been recorded in Mediterranean regions, nonetheless, a few cases originated from central and northern countries [2]. Several human cases have been reported in Greece, involving pulmonary, ocular, and subcutaneous parasite localisations [12,13]. Other than the occasionally reported cases, no epidemiological study (e.g. serological surveys) in the population has been ever conducted to elucidate the epidemiology of human dirofilariosis in Greece. In this context, the present study aimed to record for the first time the prevalence of dirofilariosis in dogs and humans living in Thrace, a hyperenzootic region of north-eastern Greece [8,14].
2. Materials and Methods
2.1. Study Area
The geographical region of Thrace in north-eastern Greece (Figure 1) was selected for the comparative study of Dirofilaria spp. infection in dogs and humans, based on previous data recording the highest prevalence of heartworm infection in dogs in the country [8,14]. Thrace (41°74´N – 40° 73´, 26°63´E – 24°46´E), is distinguished into three regional units, i.e. Xanthi, Rodopi, and Evros (Figure 1), and is characterized by extensive mountain ranges to the north, lowlands to the coastal zone and the flow of two large rivers, Nestos, and Evros. Approximately, 31.3% of Thrace is covered by forests while its main geological characteristic is the wide wetland complexes of freshwater lakes and coastal lagoons, most of which are protected at National and European levels as they are included in the Ramsar Convention on Wetlands [15,16]. In the lowlands and coastal areas, the climate is Mediterranean and temperate, with milder weather than in the mountains, and with high humidity due to the frequent rainfall. The average temperature in the region is 14-16 °C [16].
2.2. Dog Samples
Dog blood samples were collected in the frame of their routine clinical examination. The animals included in the study fulfilled the following criteria: i) they were living in one of the regional units of Thrace for at least 12 months prior to the sampling, ii) they did not receive regular preventative treatment with macrocyclic lactones against dirofilariosis, iii) they lived at least one mosquito activity period (May to October), iv) they were older than 9 months. Written informed consent of the dog owner or the licensing of the municipal authorities in the case of stray dogs living in shelters was a prerequisite.
Overall, 604 dogs were examined, specifically 258, 249, and 97, from the regional units of Xanthi, Rodopi, and Evros, respectively (Figure 1). A questionnaire was filled out for each dog, including information regarding the region of residency, the lifestyle (outdoor/indoor/indoor-allowed outdoor), sex, age, and hair length. For each subject of the study, 2 ml of blood was collected in an EDTA tube from a peripheral vein (cephalic or jugular) and kept refrigerated (4 °C) until examination.
2.3. Human Samples
A total of 625 human samples were collected from residents of the three regional units of Thrace, i.e. 215, 200, and 210 samples from Xanthi, Rodopi, and Evros, respectively (Figure 1). Human sera were obtained from blood samples collected with the individual’s written consent, from subjects living in one of the three regional units of Thrace. Humans of all ages and genders, clinically healthy, who came to the General University Hospital of Alexandroupolis for a regular health check or as blood donors were included in the survey. After collection, the sera were stored in an Eppendorf tube at -20oC until examination. Every study participant filled a questionnaire including information regarding their age, gender and residency area. The collected human data were coded and stored anonymously, according to data protection legislation.
2.4. Sample Analysis
Each dog blood sample was examined by the modified Knott’s method for the detection of microfilariae [17]. Identification of the microfilariae was performed under the light microscope at 100× και 400× magnification, on the basis of morphometric and morphological features [17,18]. The detection of D. immitis antigen was performed by the commercial serological test DiroCheck® (Zoetis, Parsippany, New Jersey, U.S.).
Serological examination of human blood samples was performed by western blot analysis, separately for D. immitis and D. repens antigens, using parasites collected from canine cases of cardiopulmonary and subcutaneous dirofilariosis, respectively. For the development and standardisation of the method positive human sera from confirmed cases and negative control sera were used.
The parasites were homogenised per species in PBS supplemented with protease inhibitors (PMSF 100 μg/mL, Leupeptin 0.5 μg/mL, Aprotonin 0.5 μg/mL, Pepstatin 1 μg/mL, Sigma Aldrich, St Louis, MI, USA). Following homogenisation, Triton X-100 at 1 % final concentration was added and samples were rapidly frozen at -80oC, thawed, centrifuged at 10000×g for five minutes and the supernatant was collected and kept at -80oC. The protein concentration of the lysates was calculated with the BCA assay kit (23225, Thermo Scientific, Waltham, MA, USA). The quality and quantity of the isolated proteins were estimated by loading 5 μg, 10 μg and 20 μg from each species sample in a 10% Tris-glycine gel (Figure 2). For the detection of Dirofilaria-specific antibodies, the quantity of 20 μg of protein from each parasite was selected, separated in 12% gels. Proteins were transferred onto polyvinylidene difluoride (PVDF) membranes (Immobilon, Darmstadt, Germany) and 5% non-fat dry milk was used to block non-specific binding. Sera were diluted 1:50 in blocking buffer and incubated overnight at 4oC. Following three washing steps, membranes were incubated with an anti-human IgG HRP-conjugated secondary antibody (1:5000, 32935S, Cell Signaling, Danvers, MA, USA) and once again washed three times. Protein bands were detected using ECL chemiluminescent substrate (34577, Thermo Scientific, Waltham, MA, USA) and a ChemiDoc MP Imaging System (BioRad, Hercules, CA, USA). Sera were considered positive for each parasite species when specific bands were detected at 17-22 kDa for D. immitis and at 43-70 kDa for D. repens respectively [19,20].
2.5. Statistical Analysis
The sample sizes for both dog and human samples met the recommended threshold, indicating that to detect a difference in proportions with 95% confidence and 80% power, 91 samples were required [21]. Statistical analysis was performed using the Chi-square test of independence between the infection status for Dirofilaria spp. (positive or negative result for any of the Dirofilaria species examined) and a variety of variables [22]. Specifically, for dogs, the variables examined were breed, gender, age, hair length, lifestyle, and area of residency and for humans, the variables examined were sex, age, and area of residency. The level of significance was set at p= 0.05.
2.6. Institutional Review Board Statement
The study protocol and all the procedures were approved by the Ethical Committee of the University General Hospital of Alexandroupoli (no.: ΕΣ6/15-05-2020).
3. Results
3.1. Dog Samples
Overall, 177 (29.3%) dogs were found infected with at least one species of Dirofilaria. Of the 604 dogs examined, 173 (28.6%) were positive for D. immitis by at least one of the examination methods (serology and Knott’s test). More specifically, 87 (50.3%) samples were positive in both methods, while 84 (48.6%) were positive in serology only, and 2 (1.2%) samples in the Knott’s test only. Moreover, in 7 (1.3%) samples D. repens microfilariae were found in the Knott’s test. Mixed infection (D. immitis antigen or/and microfilariae and D. repens microfilariae) was found in 6 dogs. The results of the Knott’s test and the serological examination of dog samples are presented in detail in Table 1.
At the regional unit level, the number of dogs found positive for D. immitis by serology and/or the Knott’s test were 81 (31.4%), 57 (22.9%), and 35 (36.1%) in Xanthi, Rodopi, and Evros respectively. Furthermore, D. repens microfilariae were detected in 1 (0.4%) dog in Xanthi and in 6 (6.2%) in Evros (Table 1).
3.2. Human Samples
Based on results from method standardization using positive and negative control samples, and in accordance with the literature, human sera were considered positive for D. immitis when bands between 17 and 22 kDa were detected and positive for D. repens when bands between 43 and 70 kDa were observed (Figure 3) [19,20,23].
Overall, 42 (6.7%) samples were positive in western blot analysis for Dirofilaria spp. specific IgG antibodies, i.e. 24 (3.8%) for D. immitis and 18 (2.9%) for D. repens. In detail, 5 (2.3%) samples for D. immitis and 10 (4.7%) samples for D. repens were positive in Xanthi, 9 (4.5%) and 6 (3%) in Rodopi, and 10 (4.7%) and 2 (1%) in Evros, respectively (Table 2).
3.3. Statistical Analysis
The statistical analysis for the dogs’ results were applied in 546 of the total 604 animals due to insufficient data for 58 of them. Factors such as the gender [X2 (1, N = 546) = 5.21, p = 0.0022], lifestyle [X2 (2, N = 546) = 18.23, p < 0.001], and area of residency [X2 (2, N = 546) = 10.57, p = 0.005], were associated with Dirofilaria spp. infection, while hair length and age were not (p-value > 0,05) (Table 3). Male dogs were more likely (OR = 1.55) to be infected than female dogs and dogs living in the prefecture of Evros were more likely to be infected than dogs living in Rodopi (OR=2.03) or Xanthi (OR=1.15). Finally, dogs living outdoors had an increased risk of infection compared to dogs living indoors (OR = 2.4) or indoors-allowed outdoors (OR = 2.27) (Table 3).
Statistical analysis of the human samples revealed no significant statistical correlation between demographic factors (sex, age, and area of residency) and risk of infection (p-value > 0.05).
4. Discussion
This study is the first to comparatively investigate the prevalence of Dirofilaria spp. infection in both dogs and humans in a hyperenzootic area of Greece. Additionally, it represents the first serological screening for Dirofilaria spp. infection in the human population of Greece.
The study area was selected based on available epidemiological data, indicating that Thrace region has the highest infection rates in dogs in the country [8,14]. Indeed, the hyperenzootic profile of the area was confirmed by the present results, with an overall infection rate in dogs of 28.6% and the highest prevalence percentage of 36.1% recorded in the regional unit of Evros. On this basis, the results of the present study provide evidence regarding the rate of human contact with parasites of the genus Dirofilaria in an area of high infection pressure.
The hyperenzootic character of northern Greece for D. immitis has been repeatedly demonstrated by surveys on dog populations. The percentage of infection in dogs varies from 6.1% up to the extreme of 68% which was found in dogs from the easternmost town Didimoticho, in Evros [5,14,24,25,26,27]. This epizootiological status is associated with the geomorphology of northern Greece and the agricultural profile of the area. Indeed, northern Greece holds most of the wetlands of the country, 91% of the total rice fields, and 68.5% of the farm cattle population on a national level [5,28,29]. These conditions may favour mosquito development and populations’ abundance and stability [30,31]. This hypothesis is confirmed by entomological surveys which demonstrated that Aedes spp. population in eastern Macedonia and Thrace is 10 times larger than the corresponding in southern or in western Greece [32]. Furthermore, the mosquito species Culex pipiens and Aedes caspius, proven vectors of canine dirofilariosis, are the dominant mosquito species in northern Greece [32,33,34,35].
None of the dogs examined herein presented clinical evidence of heartworm disease or subcutaneous dirofilariosis at the routine clinical examination. However, heartworm disease is one of the most severe parasitic diseases in dogs and can be fatal. The pathogenesis of D. immitis is mainly related to pulmonary hypertension that leads to congestive heart failure [2]. Common clinical signs include chronic cough, respiratory distress, weakness, ascites, abnormal cardiac sounds, and sudden death [2,36,37]. Dirofilaria repens infection is de facto less severe. When clinical sings occur, they usually manifest as skin nodules that may develop in various sites, ranging from 0.5-3 cm in diameter [36].
Among the factors examined herein, sex, lifestyle, and area of residency were found to be associated with a higher risk of infection in dogs. Although it has been observed that in hyperenzootic areas the sex and activity of the dogs do not play a role in the risk of infection [2], male dogs are used more often as guards than female dogs, increasing the time spent outdoors under the pressure of mosquito bites. Indeed, dogs living exclusively outdoors were found with an increased risk of infection compared to dogs living indoors or indoors with outdoor access. Dogs living in the regional unit of Evros had the highest probability of infection compared to the other two regional units of the study. This is in accordance with previous data, as Evros is the area of the highest prevalence of infection recorded in dogs in Greece, i.e. 68% [14]. Although age was not found a statistically significant factor in the risk of infection, dogs over 7 years of age showed a higher percentage of infection. This observation is common in canine dirofilariosis which is a chronic condition, thus occurring more prevalently in older dogs as they accumulate exposure to infection over the years.
Human dirofilariosis is considered a sporadic zoonotic disease. However, in the last decades, the number of reported human cases have increased [1]. This may be attributed to a factual increase in incidences of human infection, due to various factors that promote the spreading of vector-borne diseases (VBD), but also to an enhancement of awareness in the medical community. The factors that are linked to the expansion and increase of VBD, [38] primarily to natural hosts and subsequently to accidental hosts, in this case, dogs and humans, respectively, are climate change, especially global warming and extreme meteorological phenomena (e.g. floods), the land use change, influencing vector and reservoir hosts biology and behaviour, and the intensified movement of humans, animals, and goods that promote vector and hosts spreading [39,40].
In Europe, most human cases are reported from Italy, followed by France and then Greece [1]. However, cases from central and northern European counties have also seen the light of publicity in the recent years [3,4]. Dirofilaria repens is the primary agent of human dirofilariosis in Europe and has been found in various sites of the human body, with predominant the region of the head and particularly the subcutaneous tissues and the eye (eyelid, periorbital region, and subconjunctiva [1,3]. Although humans are not the preferred host for D. repens, there are several cases where the parasites fully matured and produced microfilariae within the human host. To date, there are at least 24 cases of D. repens microfilaraemia in humans [41,42,43].
On the other hand, D. immitis infections in humans are less common in Europe [1,3]. Dirofilaria immitis typically migrates to the pulmonary arteries, where it is usually destroyed by the host’s immune system, generating a granulomatous nodular lesion in the lung parenchyma, known as a "coin lesion." This condition is usually asymptomatic and often discovered incidentally during imaging examinations. However, in some cases, the presence of the parasite can cause thoracic pain, cough, haemoptysis, low fever, and malaise [44]. Although the condition is generally self-limiting, surgical removal of the lesion is the standard treatment, as malignancy is considered in the differential diagnosis [3]. Dirofilaria immitis has never been reported to fully develop in humans and there is no case of recorded microfilaraemia.
The higher frequency of human D. repens infections compared to D. immitis infections may reflect the parasite’s better adaptation to human host, evidenced by the occasional reproductive maturity that the parasites reach in humans resulting in microfilaraemia. In addition, the subcutaneous and ocular localisation commonly associated with D. repens infections facilitate diagnosis compared to the parenchymal and most often pulmonary localization of D. immitis [3].
Despite the notion that in humans D. repens is related to subcutaneous nodules and ocular locations while D. immitis causes pulmonary nodules, both parasites have been found in many different locations of the human body, thus location of the parasite cannot by any means imply its species [1]. Furthermore, although the morphology of the cuticle of Dirofilaria may indicate the species, as D. repens displays a longitudinally striated cuticle while D. immitis does not, the fact that the parasites when extracted from the organ of parasitism are often already dead and to an extend destroyed and morphologically altered, in many cases the only safe identification is via molecular techniques (PCR) [3,45]. In fact, as reviewed by Pampiglione et al. [46], morphological misidentification of the parasites to the species level is rather common in the literature.
Human dirofilariosis, due to both D. immitis and D. repens, has been documented in Greece on several occasions [45,47]. However, in only a few instances of ocular and one case of subcutaneous dirofilariosis were the parasites unequivocally characterized by molecular means as D. repens [48] and D. immitis [49], respectively. A seroepidemiological survey in humans has never been carried out in the past and the prevalence of human infection in a selected, hyperenzootic area of Greece is reported herein for the first time.
In contrast to the relatively straightforward diagnosis of Dirofilaria infections in dogs, diagnosis in humans is more complex. Indeed, in dogs, D. immitis infection is diagnosed by the combination of the Knott’s method and a serological test. This is the proposed laboratory diagnostic procedure, providing very high diagnostic accuracy, as it covers cases of occult infection (infection in the absence of circulating microfilariae) and false negative serological results (low levels of circulating antigens) [36,37]. Notably, both scenarios were encountered in the present study, as occult infection was detected in 84 out of the 173 infected animals, and two animals had circulating D. immitis microfilariae with a negative serological test. For D. repens, although there is no serological test developed, again, the Knott’s method can reveal most of the infections in dogs [36]. On the other hand, diagnosis in humans, other than surgical removal and identification of the parasite when detected, is not easy, as microfilaraemia is very rare and has only been observed in some cases of D. repens infection. Similarly, due to the rarity of infections, there is no commercial serological test available for humans. Therefore, in-house ELISA and western blot assays have been developed and are applied in seroepidemiological surveys. In fact, serology is the only method to identify individuals who had recently been exposed to the parasites.
ELISAs developed for the detection of specific anti-Dirofilaria spp. antibodies, have employed somatic and excretory/secretory proteins of the parasites, as well as proteins of their bacterial endosymbiont Wolbachia, as antigens [50,51,52,53]. The crude somatic or excretory/secretory antigens used in ELISA have the drawback of cross-reactions with other parasites that may infect humans, especially Toxocara canis, a canine nematode causing “visceral larva migrans”, one of the most common zoonotic infections in the world [3,54]. Western blot analysis on the other hand, provides a reliable serological tool, with specific molecular weight bands indicating seropositivity for D. immitis and D. repens separately [3].
The seroprevalence in humans in Europe has been investigated in a few cases. In western Spain and in the Canary Islands, 9.3% and 6.4% of the population examined by ELISA (somatic antigen) were D. immitis positive, respectively [51,55]. In Portugal, a serosurvey by ELISA using somatic antigen and Wolbachia surface protein as antigen showed a prevalence of 6.1% [56]. In Romania, Moldova, and in Serbia, an ELISA with somatic antigen was used coupled with the detection of anti-Wolbachia surface protein and western blot. Taking into account the mixed infections, 7.4%, 14.8%, and 2.6% for D. immitis and 0.5%, 1.5%, and 2.3% for D. repens seropositivity were found in the three countries, respectively [19,20]. These percentages are close to the prevalence found in the present study, i.e., 3.8% for D. immitis and 2.9% for D. repens. Age, sex and area of residency of the individuals included in the present study were not associated with a higher risk for human dirofilariosis. Age in humans, as in dogs, is associated with a higher infection rate, due to repeated exposure to the parasite in an enzootic area [57]. However, the short lifespan of the parasites in a non-natural host clears the infections much sooner than in dogs, preventing chronic infections and thus, restricting the time during which antibodies can be detected.
5. Conclusions
Dirofilaria spp. infection in dogs living in the geographic region of Thrace remains highly prevalent. The detected proportion of infection in humans was 23.4% of the respective canine infection in the same area. Knowing the rate of human contact with the parasites in areas of high infection pressure is essential for implementing preventive measures, raising awareness among the medical community, and providing available data to promote and support prompt and accurate diagnosis of human infections. By incorporating the "One Health" concept, the present study emphasizes the interconnectedness of human, animal, and environmental health.
Timely diagnosis, and more importantly, effective prevention in dogs are crucial for protecting the health of both animals and humans. This is especially vital given the anticipated rise in cases and the spread of parasites due to climate change, increased animal travel, and the presence of invasive mosquito species. Monitoring and control of Dirofilaria infections have acquired additional significance recently, due to the development of resistant strains of D. immitis against macrocyclic lactones, i.e. the only drug molecules used for heartworm prevention [58,59]. Furthermore, medical doctors should be adequately informed about Dirofilaria infections in humans for accurate and prompt diagnosis that in some cases may prevent unnecessary medical procedures (e.g. surgeries) in patients. In this context, sensitive and easy-to-perform routine level serological methods should be developed for diagnosis in humans. Furthermore, these infections should become notifiable diseases in all enzootic/endemic countries, as is currently the practice in some eastern European countries, such as Ukraine, Belarus, and Russia, where a high number of cases have been reported in recent years [60]. This measure, in combination with regular epizootiological/epidemiological screening of the dog and human populations for Dirofilaria spp., is imperative for the surveillance of these important zoonotic infections.
Author Contributions
Conceptualization, A.D.; methodology, D.D., G.A., A.T., S.C. and A.D.; software, D.D., G.A., A.T., S.C. and A.D.; validation, K.C., M.P., and A.D.; formal analysis, A.T.; investigation, D.D., G.A. and A.D.; resources, S.C., K.C., M.P. and A.D.; data curation, D.D., and A.T.; writing—original draft preparation, D.D.; writing—review and editing, A.D.; visualization, A.D.; supervision, K.C., M.P., and A.D.; project administration, D.D. and A.D; funding acquisition, K.C. and M.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the University General Hospital of Alexandroupoli (no.: ΕΣ6/15-05-2020). Ethical review and approval were waived for sampling the animals in this study, as this was performed in the frame of routine veterinary checks already needed by each animal involved in the present study and coordinated by local veterinarians. No procedures have been performed on the animal solely for the purposes of the present study.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study and from the owners or authorized agents of the animals.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Acknowledgments
The authors would like to thank the following veterinary practitioners for their valuable help in sample collection: Julia Grammenidou, Thanos Karagiorgis, Thanasis Karkanis, Ioannis Konstantelis, Maria Barda, Aydin Mumin, and Eirini Sergkelidou.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Simón, F.; Siles-Lucas, M.; Morchón, R.; González-Miguel, J.; Mellado, I.; Carretón, E.; Montoya-Alonso, J. A. Human and animal dirofilariasis: The emergence of a zoonotic mosaic. Clin Microbiol Rev 2012, 25, 507–544. [Google Scholar] [CrossRef]
- McCall, J.W.; Genchi, C.; Kramer, L.H.; Guerrero, J.; Venco, L. Heartworm disease in animals and humans. Adv Parasitol 2008, 66, 193–285. [Google Scholar] [CrossRef]
- Simón, F.; Diosdado, A.; Siles-Lucas, M.; Kartashev, V.; González-Miguel, J. Human dirofilariosis in the 21st century: A scoping review of clinical cases reported in the literature. Transbound Emerg Dis 2022 69, 2424–2439. [CrossRef]
- Fuehrer, H.P.; Morelli, S.; Unterköfler, M.S.; Bajer, A.; Bakran-Lebl, K.; Dwużnik-Szarek, D.; et al. Dirofilaria spp. and Angiostrongylus vasorum: current risk of spreading in Central and Northern Europe. Pathogens 2021, 10, 1268. [Google Scholar] [CrossRef]
- Diakou, A.; Kapantaidakis, E.; Tamvakis, A.; Giannakis, V.; Strus, N. Dirofilaria infections in dogs in different areas of Greece. Parasit Vectors 2016, 9, 1–7. [Google Scholar] [CrossRef]
- Diakou, A.; Soubasis, N.; Chochlios, T.; Oikonomidis, I.L.; Tselekis, D.; Koutinas, C.; Karaiosif, R.; Psaralexi, E.; Tsouloufi, T.K.; Brellou, G.; Kritsepi-Konstantinou, M.; Rallis, T. Canine and feline dirofilariosis in a highly enzootic area: first report of feline dirofilariosis in Greece. Parasitol Res 2019, 118, 677–682. [Google Scholar] [CrossRef] [PubMed]
- Diakou, A. The prevalence of canine dirofilariosis in the region of Attiki. J Hel Vet Med Soc 2001, 52, 152–156. [Google Scholar] [CrossRef]
- Angelou, A.; Gelasakis, A.I.; Verde, N.; Pantchev, N.; Schaper, R.; Chandrashekar, R.; Papadopoulos, E. Prevalence and risk factors for selected canine vector-borne diseases in Greece. Parasit Vectors, 2019; 12, 1–11. [Google Scholar] [CrossRef]
- Symeonidou, I.; Sioutas, G.; Gelasakis, A.I.; Bitchava, D.; Kanaki, E.; Papadopoulos, E. Beyond borders: Dirofilaria immitis infection in dogs spreads to previously non-enzootic areas in Greece—a serological survey. Vet Sc. 2024, 11, 255. [Google Scholar] [CrossRef] [PubMed]
- Ryan, W.; Newcomb, K. Prevalence of feline heartworm disease-a global review. In Proceedings of the Heartworm Symposium ‘95, American Heartworm Society. Auburn, Alabama, USA, 31 March-2nd April 1995; pp. 79–86. [Google Scholar]
- Venco, L.; Genchi, M.; Genchi, C.; Gatti, D.; Kramer, L. Can heartworm prevalence in dogs be used as provisional data for assessing the prevalence of the infection in cats? Vet Parasitol 2011, 176, 300–303. [Google Scholar] [CrossRef]
- Rodis, N.; Kalouda Tsapadikou, V.; Zacharis, G.; Zacharis, N.; Potsios, Ch.; Krikoni, E.; Xaplanteri, P. Dirofilariasis and related traumas in Greek patients: Mini Review. J SurgTrauma 2021, 9, 4–7. [Google Scholar]
- Pampiglione, S.; Canestri Trotti, G.; Rivasi, F.; Vakalis, N. Human dirofilariasis in Greece: A review of reported cases and a description of a new, subcutaneous case. An Trop Med Parasitol 1996, 90, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Morelli, S.; Diakou, A.; Frangipane di Regalbono, A.; Colombo, M.; Simonato, G.; Di Cesare, A.; Passarelli, A.; Pezzuto, C.; Tzitzoudi, Z.; Barlaam, A.; et al. Use of in-clinic diagnostic kits for the detection of seropositivity to Leishmania infantum and other major vector-borne pathogens in healthy dogs. Pathogens 2023, 12, 696. [Google Scholar] [CrossRef]
- Ramsar Sites Information Service. Available online: https://rsis.ramsar.org/ (accessed on 20 July 2024).
- Eco Thraki. Available online: https://www.ecothraki.gr/ (accessed on 20 July 2024).
- Boch, J.; Supperer, R. Veterinärmedizinische Parasitologie Verlag Paul Parey, Berlin, Germany. 1992. [Google Scholar]
- Lindsey, L.R. Identification of canine microfilariae. J Am Vet Med Assoc 1965, 146, 1106–1114. [Google Scholar]
- Ciuca, L.; Simòn, F.; Rinaldi, L.; Kramer, L.; Genchi, M.; Cringoli, G.; Acatrinei, D.; Miron, L.; Morchon, R. Seroepidemiological survey of human exposure to Dirofilaria spp. in Romania and Moldova. Acta Trop 2018, 187, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Savić, S.; Stosic, M.Z.; Marcic, D.; Hernández, I.; Potkonjak, A.; Otasevic, S.; Ruzic, M.; Morchón, R. Seroepidemiological study of canine and human dirofilariasis in the endemic region of Northern Serbia. Front Vet Sci 2020, 7, 571. [Google Scholar] [CrossRef] [PubMed]
- Eng, J. Sample size estimation: how many individuals should be studied? Radiol 2003, 227, 309–313. [Google Scholar] [CrossRef] [PubMed]
- Zar, J.H. Biostatistical analysis, 4th ed.; New Jersey: Prentice-Hall US. 1998. [Google Scholar]
- Torres-Chable, O.M.; Brito-Argaez, L.G.; Islas-Flores, I.R.; Zaragoza-Vera, C.V.; Zaragoza-Vera, M.; Arjona-Jimenez, G.; Baak-Baak, C.M.; Cigarroa-Toledo, N.; Gonzalez-Garduño, R.; Machain-Williams, C.I.; Garcia-Rejon, J.E. Dirofilaria immitis proteins recognized by antibodies from individuals living with microfilaremic dogs. Infect Dev Ctries 2020, 14, 1442–1447. [Google Scholar] [CrossRef]
- Papazahariadou, M.G.; Koutinas, A.F.; Rallis, T.S.; Haralabidis, S.T. Prevalence of microfilaraemia in episodic weakness and clinically normal dogs belonging to hunting breeds. J Helminthol 1994, 68, 243–245. [Google Scholar] [CrossRef]
- Founta, A.; Theodoridis, Y.; Frydas, S.; Chliounakis, S. The presence of filarial parasites of dogs in Serrae Province. J Hell Vet Med Soc 1999, 50, 315–320. [Google Scholar] [CrossRef]
- Lefkaditis, M.; Koukeri, S.; Cozma, V. An endemic area of Dirofilaria immitis seropositive dogs at the eastern foothills of Mt Olympus, Northern Greece. Helminthol 2010, 47, 3–7. [Google Scholar] [CrossRef]
- Athanasiou, L.V. , Kontos, V.I., Kritsepi Konstantinou, M., Polizopoulou, Z.S., Rousou, X.A., Christodoulopoulos, G. Cross-sectional serosurvey and factors associated with exposure of dogs to vector-borne pathogens in Greece. Vector Borne Zoonotic Dis, 2019; 19, 923–928. [Google Scholar] [CrossRef]
- Tsochatzis, D.E. Development of analytical methods for the determination of residues of pesticides used in rice cultures: application for the assessment of their environmental implications, PhD Thesis, School of Chemical Engineering, Department of Chemistry. Thessaloniki: Aristotle University of Thessaloniki; 2012. p. 201.
- Geotechnical Chamber of Greece. Greek cattle milk production. 2011. Available online: chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://www.geotee.gr/lnkfiles/20120101_OLH_H_MELETH_GALA_13122011.pdf (accessed on 20.07.2024).
- Mwalugelo, Y.A.; Mponzi, W.P.; Muyaga, L.L.; Mahenge, H.H.; Katusi, G.C.; Muhonja, F.; Omondi, D.; Ochieng, A.O.; Kaindoa, E.W.; Amimo, F.A. Livestock keeping, mosquitoes and community viewpoints: a mixed methods assessment of relationships between livestock management, malaria vector biting risk and community perspectives in rural Tanzania. Malar J 2024, 23, 213. [Google Scholar] [CrossRef] [PubMed]
- Alho, A.M.; Landum, M.; Ferreira, C.; Meireles, J.; Goncalves, L.; de Carvalho, L.M.; Belo, S. Prevalence and seasonal variations of canine dirofilariosis in Portugal. Vet Parasitol 2014, 206, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Diakou, A.; Gewehr, S.; Kapantaidakis, E.; Mourelatos, S. Can mosquito population dynamics predict Dirofilaria hyperendemic foci? In Proceeding of 19th E-SOVE, Thessaloniki, Greece, 13-17 October 2014 p. 76.
- Shcherbakov, O.V.; Aghayan, S.A.; Gevorgyan, H.S.; Burlak, V.A.; Fedorova, V.S.; Artemov, G.N. An updated list of mosquito species in Armenia and Transcaucasian region responsible for Dirofilaria transmission: A review. J Vector Borne Dis 2023, 60, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Fotakis, E.A.; Chaskopoulou, A.; Grigoraki, L.; Tsiamantas, A.; Kounadi, S.; Georgiou, L.; Vontas, J. Analysis of population structure and insecticide resistance in mosquitoes of the genus Culex, Anopheles and Aedes from different environments of Greece with a history of mosquito borne disease transmission. Acta Trop 2017, 174, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Spanoudis, C.G.; Pappas, C.S.; Savopoulou-Soultani, M.; Andreadis, S.S. Composition, seasonal abundance, and public health importance of mosquito species in the regional unit of Thessaloniki, Northern Greece. Parasitol Res 2021, 120, 3083–3090. [Google Scholar] [CrossRef] [PubMed]
- ESDA, European Society of Dirofilariosis and Angiostrongylosis. Guidelines for clinical management of canine heartworm disease. Available online: https://www.esda.vet/wp-content/up loads/2017/11/GUIDELINES-FOR-CLINICAL-MANAGEMENT-OFCANINE-HEARTWORM-DISEASE.pdf (accessed on 20 July 2024).
- AHS, American Heartworm Society. Current canine guidelines for the prevention, diagnosis, and management of heartworm (Dirofilaria immitis) infection in dogs. Available online: https://d3ft8sckhnqim2.cloudfront.net/images/pdf/AHS_Canine _Guidelines_11_13_20.pdf?1605556516 (accessed on 20 July 2024).
- Morchón, R.; Montoya-Alonso, J.A.; Rodríguez-Escolar, I.; Carretón, E. What has happened to heartworm disease in Europe in the last 10 years? Pathogens 2022, 11, 1042. [Google Scholar] [CrossRef] [PubMed]
- Petrić, D., Bellini, R., Scholte, E. J., Rakotoarivony, L. M., & Schaffner, F. (2014). Monitoring population and environmental parameters of invasive mosquito species in Europe. Parasites & vectors, 7, 187. [CrossRef]
- Veronesi, F.; Deak, G.; Diakou, A. Wild Mesocarnivoresas reservoirs of endoparasites causing important zoonoses and emerging bridging infections cross Europe. Pathogens 2023, 12, 178. [Google Scholar] [CrossRef] [PubMed]
- Tasić-Otasevic, S.; Golubović, M.; Trichei, S.; Zdravkovic, D.; Jordan, R.; Gabrielli, S. Microfilaremic Dirofilaria repens infection in patient from Serbia. Emerg Infect Dis 2023, 29, 2548–2550. [Google Scholar] [CrossRef] [PubMed]
- Pupić-Bakrač, A.; Pupić-Bakrač, J.; Beck, A.; Jurković, D.; Polkinghorne, A.; Beck, R. Dirofilaria repens microfilaremia in humans: Case description and literature review. One health 2021, 13, 100306. [Google Scholar] [CrossRef]
- Huebl, L.; Tappe, D.; Giese, M.; Mempel, S.; Tannich, E.; Kreuels, B.; Ramharter, M.; Veletzky, L.; Jochum, J. Recurrent swelling and microfilaremia caused by Dirofilaria repens infection after travel to India. Emerg Infect Dis 2021, 27(6), 1701–1704. [Google Scholar] [CrossRef]
- Jacob, S.; Parameswaran, A.; Santosham, R.; Santosham, R. Human pulmonary dirofilariasis masquerading as a mass. Asian Cardiovasc Thorac Ann 2016, 24, 722–725. [Google Scholar] [CrossRef] [PubMed]
- Pampiglione, S.; Canestri Trotti, G.; Rivasi, F.; Vakalis, N. Human dirofilariasis in Greece: a review of reported cases and a description of a new, subcutaneous case. Ann Trop Med Parasitol 1996, 90, 319–328. [Google Scholar] [CrossRef]
- Pampiglione, S.; Rivasi, F.; Gustinelli, A. Dirofilarial human cases in the Old World, attributed to Dirofilaria immitis: a critical analysis. Histopathol 2009, 54, 192–204. [Google Scholar] [CrossRef]
- Rodis, N.; Kalouda Tsapadikou, V.; Zacharis, G.; Zacharis, N.; Potsios, Ch.; Krikoni, E.; Xaplanteri, P. Dirofilariasis and related traumas in Greek patients: Mini Review. J Surg Trauma 2021, 9, 4–7. [Google Scholar]
- Bozidis, P.; Sakkas, H.; Pertsalis, A.; Christodoulou, A. ; Kalogeropoulo,s C.D., Papadopoulou, C. Molecular analysis of Dirofilaria repens isolates from eye-care patients in Greece. Acta Parasitol 2021, 66, 271–276. [Google Scholar] [CrossRef]
- Falidas, E.; Gourgiotis, S.; Ivopoulou, O.; Koutsogiannis, I.; Oikonomou, C.; Vlachos, K.; Villias, C. Human subcutaneous dirofilariasis caused by Dirofilaria immitis in a Greek adult. J Infect Public Health 2016, 9, 102–104. [Google Scholar] [CrossRef]
- Simón, F.; Prieto, G.; Morchón, R.; Bazzocchi, C.; Bandi, C.; Genchi, C. Immunoglobulin G antibodies against the endosymbionts of filarial nematodes (Wolbachia) in patients with pulmonary dirofilariasis. Clin Diagn Lab Immunol 2003, 10, 180–181. [Google Scholar] [CrossRef]
- Simón, F.; Muro, A.; Cordero, M.; Martin, J. A seroepidemiologic survey of human dirofilariosis in Western Spain. Trop Med Parasitol 1991, 2, 106–108. [Google Scholar]
- Simón, F.; Prieto, G.; Muro, A.; Cancrini, G.; Cordero, M.; Genchi, C. Human humoral immune response to Dirofilaria species. Parassitologia 1997, 39, 397–400. [Google Scholar]
- Perera, L.; Muro, A.; Cordero, M.; Villar, E.; Simón, F. ; Evaluation of a 22 kDa Dirofilaria immitis antigen for the immunodiagnosis of human pulmonary dirofilariosis. Trop Med Parasitol 1994, 45, 249–252. [Google Scholar]
- Henke, K.; Ntovas, S.; Xourgia, E.; Exadaktylos, A.K.; Klukowska-Rötzler, J.; Ziaka, M. Who let the dogs out? unmasking the neglected: a semi-systematic review on the enduring impact of toxocariasis, a prevalent zoonotic infection. Int J Environ Res Public Health 2023, 20, 6972. [Google Scholar] [CrossRef] [PubMed]
- Cabrera, E.D.; Carretón, E.; Morchón, R.; Falcón-Cordón, Y.; Falcón-Cordón, S.; Simón, F.; Montoya-Alonso, J.A. The Canary Islands as a model of risk of pulmonary dirofilariasis in a hyperendemic area. Parasitol Res 2018, 117, 933–936. [Google Scholar] [CrossRef] [PubMed]
- Fontes-Sousa, A.P.; Silvestre-Ferreira, A.C.; Carretón, E.; Esteves-Guimarães, J.; Maia-Rocha, C.; Oliveira, P.; Lobo, L.; Morchón, R.; Araújo, F.; Simón, F.; Montoya-Alonso, J.A. Exposure of humans to the zoonotic nematode Dirofilaria immitis in Northern Portugal. Epidemiol Infect 2019, 147, e282. [Google Scholar] [CrossRef] [PubMed]
- Muro, A.; Cordero, M.; Ramos, A.; Simón, F. Seasonal changes in the levels of anti-Dirofilaria immitis antibodies in an exposed human population. Trop Med Parasitol 1991, 42, 371–374. [Google Scholar] [PubMed]
- Diakou, A.; Prichard, R.K. Concern for Dirofilaria immitis and macrocyclic lactone loss of efficacy: current situation in the USA and Europe, and future scenarios. Pathogens 2021, 10, 1323. [Google Scholar] [CrossRef] [PubMed]
- Traversa, D.; Diakou, A.; Colombo, M.; Kumar, S.; Long, T.; Chaintoutis, S.C.; Venco, L.; Betti Miller, G.; Prichard, R. First case of macrocyclic lactone-resistant Dirofilaria immitis in Europe - Cause for concern. Int J Parasitol Drugs Drug Resist. 2024, 25, 100549. [Google Scholar] [CrossRef]
- Kartashev, V.; Afonin, A.; Gonzalez-Miguel, J.; Sepulveda, R.; Simon, L.; Morchon, R.; Simon, F. Regional warming and emerging vector borne zoonotic dirofilariosis in the Russian Federation, Ukraine, and other post-Soviet states from 1981 to 2011 and projection by 2030. BioMed Res Int 2014, 858936. [Google Scholar] [CrossRef]
Figure 1.
The geographic area of Thrace and the number of dog and human samples examined for Dirofilaria infection from the regional units, i.e. Xanthi, Rodopi, and Evros.
Figure 1.
The geographic area of Thrace and the number of dog and human samples examined for Dirofilaria infection from the regional units, i.e. Xanthi, Rodopi, and Evros.
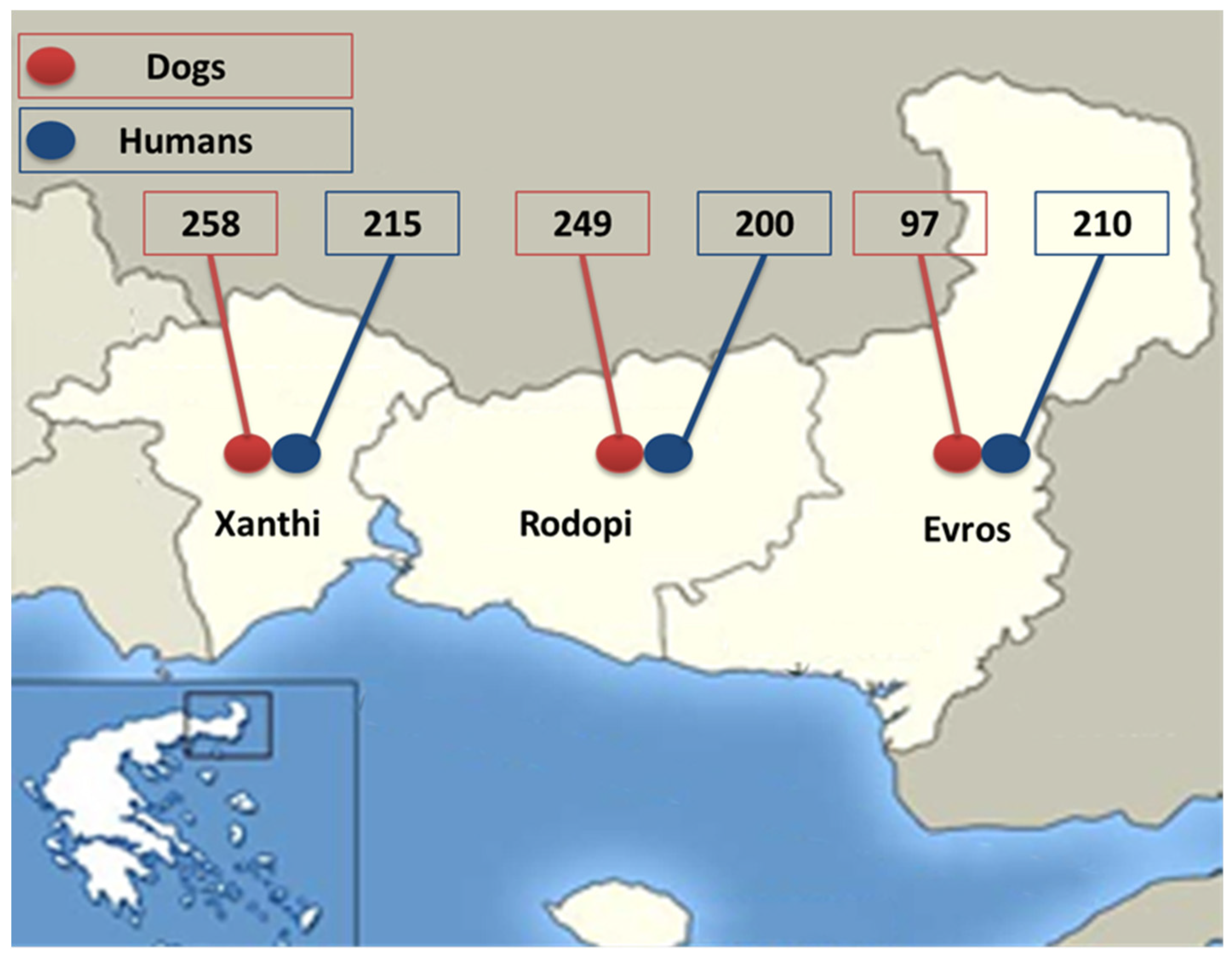
Figure 2.
Dirofilaria immitis and Dirofilaria repens proteins quality and quantity estimation by analysis of 5 μg, 10 μg, and 20 μg in 10% Tris-glycine gel.
Figure 2.
Dirofilaria immitis and Dirofilaria repens proteins quality and quantity estimation by analysis of 5 μg, 10 μg, and 20 μg in 10% Tris-glycine gel.
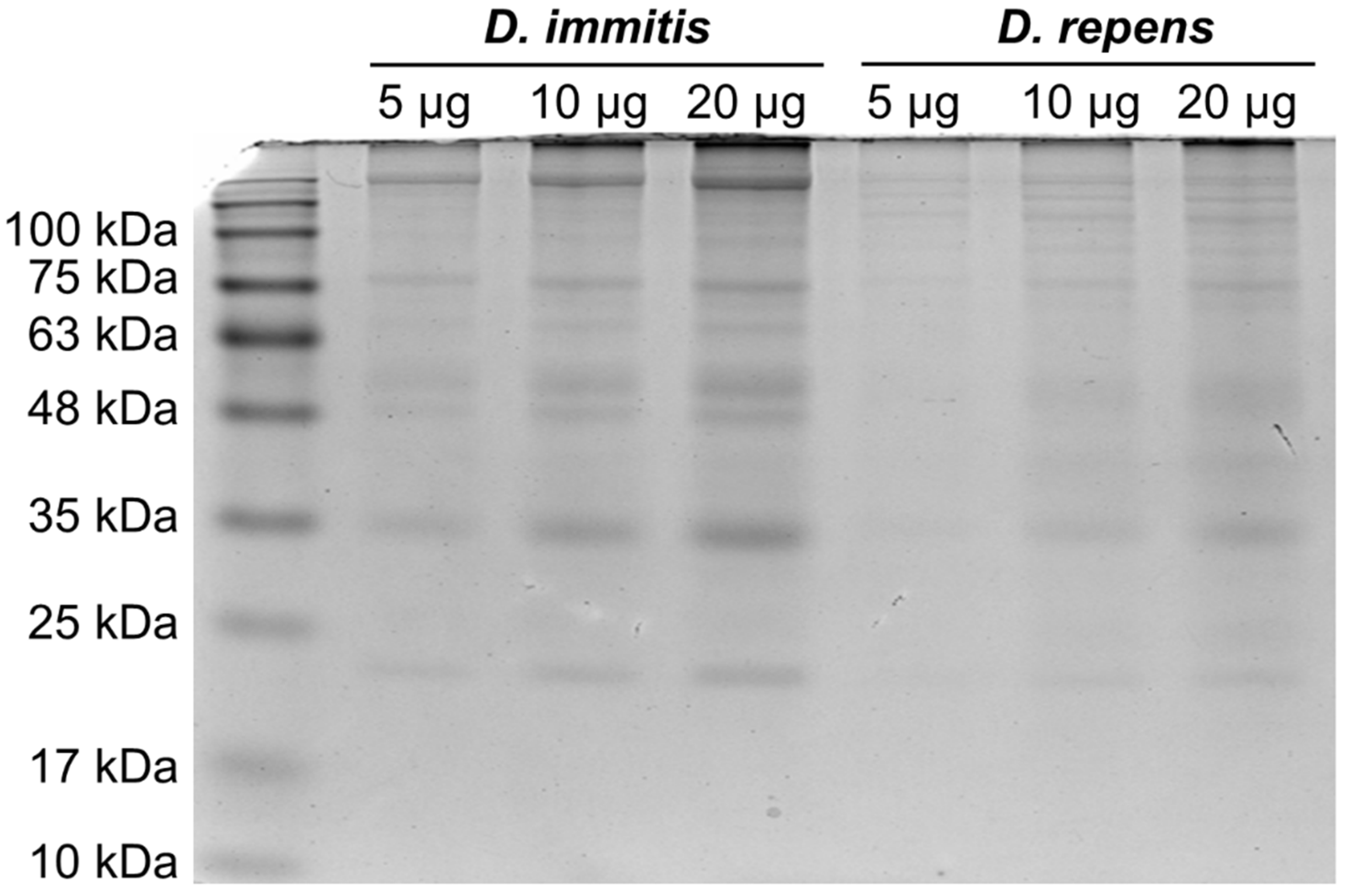
Figure 3.
Western blot analysis of human sera showing bands between 17 and 22 KDa (indicative of Dirofilaria immitis, panel A) and between 43 and 70 kDa (indicative of Dirofilaria repens, panel B). The respective bands are indicated by arrows.
Figure 3.
Western blot analysis of human sera showing bands between 17 and 22 KDa (indicative of Dirofilaria immitis, panel A) and between 43 and 70 kDa (indicative of Dirofilaria repens, panel B). The respective bands are indicated by arrows.
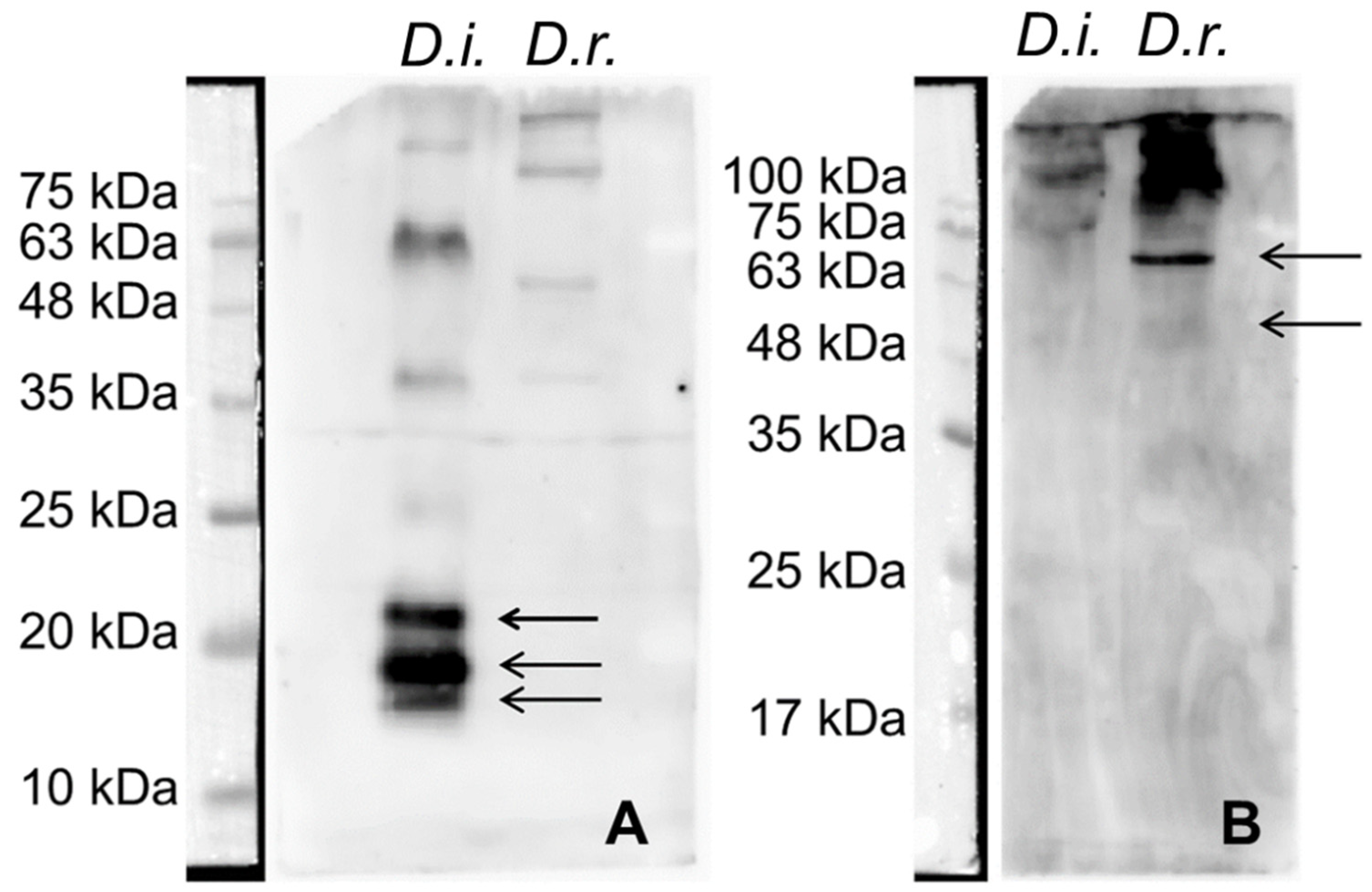

Table 1.
Dogs found positive by different examination methods for Dirofilaria immitis and Dirofilaria repens in the geographical region of Thrace and in each separate regional unit within Thrace.
Table 1.
Dogs found positive by different examination methods for Dirofilaria immitis and Dirofilaria repens in the geographical region of Thrace and in each separate regional unit within Thrace.
| Thrace (n = 604) | Xanthi (n = 258) | Rodopi (n = 249) | Evros (n = 97) | |||||
| Examination method | D. i. | D. r. | D. i. | D. r. | D. i. | D. r. | D. i. | D. r. |
| Knott | 86 (14.2%)* | 7 (1.3%)* | 45 (17.4%) | 1 (0.4%) | 20 (8%) | 0 | 21 (21.6%)* | 6 (6.2%)* |
| Serology | 171 (28.3%) | - | 80 (31%) | - | 56 (22.5%) | - | 35 (36.1%) | - |
| Knott or/and Serology | 173 (28.6%)* | 7 (1,3%)* | 81 (31.4%) | 1 (0,4%) | 57 (22.9%) | 0 | 35 (36.1%)* | 6 (6.2%)* |
D.i.= Dirofilaria immitis; D.r.= Dirofilaria repens * Mixed infection in 3 animals.
Table 2.
Seropositive (IgG) human samples by western blot analysis for Dirofilaria spp.
| Seropositive samples per parasite | |||
|---|---|---|---|
| Regional unit | Dirofilaria spp. | D. immitis | D. repens |
| Thrace (n = 625) | 42 (6.7%) | 24 (3.8%) | 18 (2.9%) |
| Xanthi (n = 215) | 15 (7%) | 5 (2.3%) | 10 (4.7%) |
| Rodopi (n = 200) | 15 (7.5%) | 9 (4.5%) | 6 (3%) |
| Evros (n = 210) | 12 (5.7%) | 10 (4.7%) | 2 (1%) |
Table 3.
Statistical analysis of the variables recorded for dogs examined for Dirofilaria spp. in the hyperenzootic area of Thrace, Greece.
Table 3.
Statistical analysis of the variables recorded for dogs examined for Dirofilaria spp. in the hyperenzootic area of Thrace, Greece.
| Variable | Dirofilaria positive | Dirofilaria negative | χ2 test / Fisher test (p-value) Odds ratio |
|---|---|---|---|
| Sex | |||
| Male | 70 (35.2%) | 129 (64.8%) | 5.21 (0.022) |
| Female | 90 (25.9%) | 257 (74.1%) | Odds ratio=1.55 |
| Age* | |||
| ≤ 3 | 67 (26.3%) | 188 (73.7%) | 4.92 (0.089) |
| 3−7 | 63 (29.3%) | 152 (70.7%) | |
| >7 | 30 (39.5%) | 46 (60.5%) | |
| R.U.** | |||
| Evros | 36 (37.1%) | 61 (62.9%) | 10.57 (0.005) |
| Rodopi | 56 (22.5%) | 193 (77.5%) | Odds ratio=2.03 |
| Xanthi | 68 (34.0%) | 132 (66.0%) | Odds ratio=1.15 |
| Lifestyle | |||
| Outside | 102 (37.5%) | 170 (62.5%) | 18.23 (<0.001) |
| Inside | 2 (20.0%) | 8 (80.0%) | Odds ratio=2.40 |
| In and out | 56 (21.2%) | 208 (78.8%) | Odds ratio=2.27 |
| Hair length | |||
| Short | 79 (32.5%) | 79 (32.5%) | 3.00 (0.223) |
| Medium | 57 (25.3%) | 57 (25.3%) | |
| Long | 24 (30.8%) | 24 (30.8%) |
*Age group (age in years)v**R.U.= Regional unit; p-value in bolt: statistical significant.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



