
Submitted:
14 August 2024
Posted:
15 August 2024
You are already at the latest version
Abstract
Technology-based approaches for upper limb (UL) motor rehabilitation after stroke are designed mostly for severely affected patients to increase their recovery chances. However, the available randomised controlled trials (RCTs) focused on efficacy of technology-based interventions often include patients with a wide range of motor impairment. This scoping review aims at overviewing the actual severity of stroke patients enrolled in RCTs which claim to specifically address UL severe motor impairment. The literature search was conducted on Scopus and PubMed databases and included articles from 2008 to May 2024, specifically RCTs investigating the impact of technology-based interventions on UL motor functional recovery after stroke. Forty-eight studies were selected. They showed that upon patients’ enrolment the values of the UL Fugl-Meyer Assessment and Action Research Arm Test covered the whole range of both scales, thus revealing the non-selective inclusion of severe impaired patients. Heterogeneity in terms of numerosity, characteristics of enrolled patients, trial design, implementation, and reporting were present across studies. No clear difference in the severity of the included patients according to the intervention type was found. Patient stratification upon enrolment is crucial to best direct resources to those patients who will benefit the most from a given technology-assisted approach (personalised rehabilitation).
Keywords:
technological interventions
; motor rehabilitation
; upper limb
; stroke
; severe impairment
; Exoskeleton
; Neuroplasticity
; Rehabilitation
; Robotic training
; Brain Computer Interfaces
; Virtual Reality
1. Introduction
Most technology-based approaches for motor rehabilitation after stroke have been originally designed and developed with severely affected patients in mind [1,2]. As a matter of facts, plegic patients have little or no access to traditional approaches targeting upper limb function, which often rely on the presence of residual motor capabilities. Furthermore, technology can provide treatment with increased intensity, which is established as a crucial determinant of rehabilitation outcome [3]. An example of how technology can impact motor recovery of the upper limb can be found in Constraint-Induced Movement Therapy (CIMT), still one of the most effective approaches [4] that requires residual motor function on the affected limb. The lack or scarceness of such residual motor function can be at least partially overcome with technology, such as neuromuscular stimulation combined with CIMT [5]. Thus, technology can not only enhance the intensity of the treatment but also increase the number of patients that can access a given therapy, increasing the chances for all patients (including the more severely affected) to regain independence.
However, randomized controlled trials (RCT) testing these technology-based rehabilitation approaches often include patients with a wide range of motor impairment, and sometimes a small proportion of patients actually falls in the severe range as defined by clinical scales. Indeed, patients’ recruitment in rehabilitation is influenced by numerous factors and is still one of the most challenging steps for researchers aiming to bring technological devices to clinical practice [6]. Severity of motor deficit often comes with concomitant conditions, such as bed-confinement status (especially in the acute and subacute phases), cognitive impairment, pain, depression which altogether limit the ability of patients to participate in such trials. However, as the motor status at baseline is probably the most consistent prognostic factor of rehabilitation outcome [7], we believe that this aspect can be accounted for the hesitating translational success of many of these technological approaches, for several reasons. On one hand, success of clinical trials may be facilitated by the participation of less severe patients, who increase trial feasibility especially in the subacute phase, but are naturally destined to a more favorable outcome. As a consequence, the actual application of a given technology in severe patients may turn out disappointing in terms of outcome, regardless of the successful trial. On the other hand, some of these technological aids may provide little added benefit for less severe patients, who can take advantage of other, more traditional and less expensive rehabilitative exercises [4].
In this scoping review, we provide an overview on the actual severity of patients recruited in RCTs carried out to analyze the efficacy of technology-based rehabilitation approaches targeting severe upper limb impairment (explicitly mentioning patients severity in the title and/or abstract). These interventions are based on robotics, electrical or magnetic stimulation of the central nervous system (non-invasive brain stimulation, NIBS) or of peripheral structures (peripheral stimulation, PS), brain-computer interfaces (BCIs), virtual reality (VR) and, in general, advanced technological devices purposely developed for post-stroke motor rehabilitation. The identification of the most effective approaches is out of the scope of this review [8], where we intend to verify
- i)
- the actual severity of patients included in trials that explicitly declare to enroll severe subjects, to confirm or refute the anecdotal notion of extreme variability in baseline motor impairment which might be responsible for the hesitating translational success of such interventions [9]
- ii)
- whether some of these technological approaches have been more consistently tested on severe patients than others and eventually speculate on why they have.
Furthermore, we check whether the severity of patients was considered as an inclusion criterion and/or employed for stratification for primary or secondary analyses. We take into account whether each considered study achieved to confirm the efficacy of a given intervention or not, that is the superiority/not superiority of the target intervention vs the control condition (positive/negative results) also highlighting possible secondary analyses that were carried out by the authors to support their hypotheses.
The ultimate goal would be to provide useful hints to improve patients’ inclusion in RCTs, in order to favor the optimization of resources and efforts towards tailored, highly technological rehabilitation interventions that is instrumental to foster technology transfer into clinical practice.
2. Methods
2.1. Protocol and Eligibility Criteria
This scoping review was conducted according to the PRISMA standards. Our protocol was drafted using the Preferred Reporting Items for Systematic Reviews and Meta-analysis extension for Scoping Reviews (PRISMA—ScR, [10]) and revised by the research team. To be included in the review, papers needed to describe technology-based rehabilitative interventions targeting the recovery of motor function of the upper limb in stroke population.
Peer-reviewed journal papers were included if they were:
- published between the period of 2008–2024,
- written in English,
- involved human participants in the framework of a Randomised Controlled Trial.
- Papers were excluded if they
- did not fit into the conceptual framework of the study,
- were reviews, study protocols, and meta-analyses.
2.2. Information Sources and Search Strategy
Studies eligible for review were identified through electronic databases such as Scopus and PubMed from 2008 to 23 May 2024. Grey literature was excluded from the search process. The search strategies consisted of free text terms in the topic: “stroke” AND “severe” AND “rehabilitation” AND “Action Research Arm Test” OR “Fugl-Meyer Assessment” AND “randomised controlled trial” AND “upper limb” OR “hand”. The complete search terms and strategy are provided in the Supplementary materials (Table S1). The search strategies were developed and executed by a biomedical engineer (EC) and further refined through team discussion. The search was peer-reviewed by other expert researchers, i.e., a neurologist (FP) and a physiatrist (GM), using the Peer Review of Electronic Search Strategies checklist and modified as required [11]. The final search results were imported into the online systematic review software Rayyan [12]. Duplicates were identified by means of the Rayyan duplicates search algorithm and removed by a researcher.
2.3. Selection of Sources of Evidence
Two reviewers (EC, FP) screened titles and abstracts for inclusion, independently. For full-text screening, two reviewers (EC, FP) subsequently screened the full-text of potentially relevant articles to determine inclusion using similar inclusion and exclusion criteria. We resolved disagreements on study selection by consensus and discussion with other reviewers if needed or by a single arbitrator (GM). To ensure reliability between reviewers, a series of training exercises was conducted prior to commencing screening. Inter-rater agreement for study inclusion was calculated using percent agreement; when it reached > 80% across the team, we proceeded to the next stage. If lower agreement was observed, the inclusion and exclusion criteria were clarified, and another pilot test occurred.
2.4. Data Charting Process and Data Items
Data-charting form was jointly developed by three reviewers to determine which variables to extract. Three reviewers (EC, FP, GM) independently charted the data, discussed the results, and continuously updated the data-charting form in an iterative process.
For each article, data on the following characteristics were extracted:
- First Author Name
- Year of publication
- Source
- Population sample size (participants per group)
- Inclusion Criteria in the RCT related to the upper limb impairment
- Availability of the dataset used (Yes/No)
-
Time since injury (TSI), i.e., stroke event, classified as
- ◦
- ≤ 1 month (acute)
- ◦
- ≤ 3 months (early subacute)
- ◦
- ≤ 6 months (subacute)
- ◦
- > 6 months (chronic)
-
Intervention type, classified as
- ◦
- Brain-Computer Interface (BCI)
- ◦
- Non-Invasive Brain Stimulation (NIBS)
- ◦
- Peripheral Stimulation (PS)
- ◦
- Robotic
- ◦
- Virtual Reality (VR) and Visual
- Comparator, i.e., control interventions and/or comparison conditions
-
Active Motor Action required (Yes/Yes whenever possible/No):
- ◦
- Yes, if the intervention type requires participant’s residual motor ability (active motor exercise from the participant)
- ◦
- Yes whenever possible refers to conditions foreseeing active motor exercise when feasible, with the technology providing assistance as needed (e.g., robotics)
- ◦
- No otherwise
- Combination of technological interventions (Yes/No)
- Dose, expressed as minutes x number of sessions
- Primary and Secondary Outcomes
-
Key Findings, classified as Positive, Positive on secondary analyses, Negative. We define Key Findings as
- ◦
- Positive if between-group statistical analyses evaluated for the primary outcomes statistically confirm the hypothesis investigated in the study.
- ◦
- Positive on secondary analyses if between-group statistical analyses evaluated for sub-items of the primary/secondary outcomes or considering sub-groups of the population under investigation confirm the hypothesis investigated in the study or if within-group statistical analyses evaluated for the primary/secondary outcomes reveal a statistical improvement only for the experimental group.
- ◦
- Negative if between- and within-group analyses do not reveal statistically significant differences among groups.
Threshold for statistical significance was set to 0.05.
- Stratification for secondary analyses according to an upper limb impairment criterium
- Follow-up (Yes/No), i.e., if Yes, we reported the number of months after the end of the intervention
- Setting: Inpatient/Outpatient.
The extracted data were collected in a table in which rows represent the included articles, columns represent variables (data items). The spreadsheet software, Microsoft Excel, was used to create our custom extraction form. The choice was based on its ease of use, high customizability and worldwide diffusion. Before extracting the data from all papers included in the scoping review, the extraction form was tested for further refinements and underwent a calibration phase. This entailed three reviewers independently extracting data from 5 papers each and meeting afterward to discuss any discrepancies, with further refinement of the form if a high level of agreement between reviewers was not obtained.
2.5. Synthesis of Results
To analyse the database the following explanatory approaches are used: descriptive and frequency analysis and association analysis.
2.5.1. Descriptive and Frequency Analysis
Descriptive statistics concern the population of participants that are overall included in the selected studies in terms of: number of participants, sample size of intervention and control groups, dose of intervention, severity of upper limb motor impairment upon enrolment, as described by FMA and/or ARAT. Data have been summarized, according to their distribution (modality and dispersion), by means of mean and standard deviation (SD) or median and interquartile range (IQR), presented as difference between the first quartile (Q1) and the third quartile (Q3), i.e., Q1-Q3.
Frequency analyses concern the following variables: time since injury (at least 4 classes, i.e., acute, early subacute, subacute, chronic participants), setting (at least 3 classes, i.e., inpatient/outpatient/ inpatient and outpatient), availability of the dataset used (2 classes, i.e., Yes or No), technological rehabilitative intervention type (at least 5 classes, i.e., BCI, NIBS, PS, Robotic, VR and Visual) and whether it did or did not require an active motor exercise from the participants (3 classes, i.e., Yes/Yes whenever possible/No), comparison conditions, primary and secondary outcome measures, presence/absence of follow-up evaluations (2 classes, i.e., Yes or No), Key findings (3 classes, i.e., positive, negative and positive on secondary analyses), severity of upper limb deficit employed as inclusion criteria for participant enrolment and/or stratification for secondary statistical analyses. In frequency analysis, the counts and percentages of articles in each cluster are calculated. Studies that share a similar approach towards a specific variable are clustered together and those following different approaches are assigned to different groups. Clustering can be carried out based on values of a single variable on the entire data set or on a subset of articles which already belong to a cluster on a higher level.
All results are presented both narratively and by means of plot and pie charts when relevant.
2.5.2. Association Analysis
Association analysis explores the relationships between the variables. Since the number of possible combinations of variables are relatively large, the results are focused on those regarding the research questions. We hypothesize that the characteristics of the technological rehabilitation interventions would determine a difficulty in recruiting severely affected participants. Therefore, we have separately analyzed the severity upper limb motor impairment at baseline (as assessed via FMA) according to the
- type of intervention (e.g., Robotic, BCI, PS, …)
- required active upper limb motor actions from the participant by the intervention itself.
For each analysis, studies that share a similar approach, i.e., type of intervention or required active motor action, are clustered together. For each level of the analyzed variable, i.e., 5 levels for the variable TYPE OF INTERVENTION and 3 levels for the variable MOTOR ACTION, FMA data are pooled together. If needed, mean and SD data are estimated from data reported in the paper as median and IQR by means of the formula in [15].
All results are expressed as mean ± SD and presented both narratively and by means of plot charts.
3. Results
3.1. Selection of Sources of Evidence
The search returned a total of 189 papers. After the duplicate removal (96), 93 articles were screened. After screening of titles and abstracts, 41 papers were excluded, due to the following reasons:
- the rehabilitative intervention under investigation does not include a technology-based approach; videos/instruction displayed on screens or other devices of everyday use (personal computers, tablet, smartphones) were not included
- the design of the study does not follow the Randomised Controlled Trial design (wrong study design)
- the effectiveness of the rehabilitative intervention under investigation was not assessed in term of motor function improvement (wrong outcome)
- the paper presents a study protocol, a review or meta-analysis.
A total of 52 full-text papers have been examined. Four studies have been excluded during full-text search and check; thus 48 articles have been included in the scoping review.
Flow-chart in Figure 1 presents the detailed search and selection process.
3.2. Results of Individual Sources of Evidence
Results of individual sources of evidence are shown in Table 1. Table 1 reports the following subset of the items among those described in the section Data charting process and data items:
- First Author Name and Year of Publication
- Population sample size (participants per group)
- Severity of the impairment (FMA and ARAT per group, whenever available)
- Inclusion Criteria for the RCT related to the upper limb impairment
- Time since Injury
- Intervention Type
- Active Motor Action required
- Comparator
- Primary Outcome
- Key Findings
3.3. Synthesis of Results
3.3.1. Descriptive and Frequency Results
The included articles report data from 3000 adult participants. Three articles [18,23,52] include participants with a diagnosis of stroke and traumatic brain injury (TBI), respectively 5 and 3 TBI participants in [18] and [23], for a total of 8 participants. No detailed information on stroke/TBI ratio is reported in [52].
The average sample size of the groups (target intervention and control groups) is 29 ± 39 (mean ± SD). The RCT in [39] is the only study in which a very large number of participants, i.e., 770 participants, was enrolled. Conversely, there is more than one study in which a very small number of participants, i.e., less than 10 per group, is analysed [21,27,34,44,45,49,58]. Therefore, median and quartiles values, i.e., 20 (median) and 11-32 (Q1-Q3), provide more accurate estimates on the target intervention and control group sample size.
Enrolled participants include stroke in acute, early subacute, subacute and chronic phase. Most studies (62.53%) consider a homogeneous group of participants: 6.25% acute stroke participants, 16.70% early subacute stroke participants, 2.08% subacute stroke participants, 37.50% chronic stroke participants. The remaining studies (37.47%) include more than one group of stroke participants who differ in terms of time from the cerebral lesion to enrolment, e.g., early subacute and subacute. The distribution of studies across TSI classes is reported in Figure 2.
Most participants enrolled in the studies are inpatient (60.40%). Outpatient studies and those considering both inpatient and outpatient participation are 20.85% and 6.25%, respectively. For the remaining 12.5% there are no clear indications referring to the setting.
As for the severity of upper limb motor impairment upon enrolment, as described by FMA and/or ARAT, Figure 3 reports respectively the FMA (panel a) and ARAT (panel b) score at baseline of participants enrolled. Forty-two studies assess motor impairment at baseline in stroke participants by means of the FMA score; fifteen studies by means of the ARAT score. As shown in Figure 3, both FMA and ARAT scores at baseline extend throughout the whole range, i.e., FMA: 21.71 ± 11.41 (mean ± SD across 42 studies) and ARAT: 12.28 ± 10.85 (mean ± SD across 15 studies).
The complete dataset about characteristics of each participant enrolled in the study (e.g., individual FMA or ARAT scores) is available in 15% of studies.
As for the type of technological rehabilitative intervention, the pie chart in Figure 4 shows the distributions of studies across intervention types. Rehabilitative interventions administered by means of robotic devices and peripheral stimulation and their combination cover more than half of the tested interventions: 27.08%, 29.17% and 6.25% respectively. Fewer studies focus on BCI-based and NIBS interventions, both combined with other intervention types, and Virtual Reality and Visual rehabilitative interventions: 16.66% (8 articles), 14.58% (7 articles) and 6.25% (3 articles) respectively.
Most rehabilitative intervention approaches require participant’s residual motor ability (active motor exercise from the participant, 52.10%), 10.40% are categorised as “Yes whenever possible” referring to conditions foreseeing active motor exercise when feasible, with the technology providing assistance as needed (e.g., robotics), and 37.50% do not require any active motor action from the participants.
As for the dose of rehabilitative intervention, studies differ among them in terms of both minutes of each training session, 40 minutes (median) and 30-60 minutes (Q1-Q3), and number of training sessions (21.78 ± 14.39, mean ± SD) ranging from 12 sessions (Q1) to 28 sessions (Q3). The overall dose of intervention, resulting from the multiplication of minutes per session and number of sessions, is 13h (median) and 8-27h (Q1-Q3).
Table 2 shows for each surveyed primary and secondary outcome, the number of studies in which each outcome is used as primary or secondary. As for the primary outcome, the Upper Extremity Fugl-Meyer Assessment results the most frequent scale administered for the assessment of the efficacy of the rehabilitative interventions (38 on 48 studies, 79.17%). Conversely, as for the secondary outcomes, several evaluations, clinical/functional as well as instrumental, are considered. Among them the most frequent are the Stroke Impact Scale [64] (22.92%), the Barthel Index [65] (22.92%), the Wolf Motor Function Test [66] (18.75%), the Action Research Arm Test [14] (16.67%), and even also transcranial magnetic stimulation, electroencephalographic, electromyographic, kinematic and kinetic parameters (brain outcome and motor outcome 31.25%).
In 37.50% studies, participants are followed-up from 2 weeks to 9 months after the end of the rehabilitation, i.e., 3 months (median) and 3-5 months (Q1-Q3). For the other studies (62.50%) no follow-up evaluations are reported.
As for the comparison conditions, most studies (81.25%) are 2-arm RCTs. The remaining 18.75% compare more than 2 groups, up to 4 groups in [53]. For the 2-arm studies, the control conditions that are most commonly observed can be categorised as follows:
- Sham Stimulation/Control (applies to NIBS/PS and BCI studies, referring to conditions where the participants are induced to believe they are receiving stimulation or controlling a BCI system while they are not): 28.20%
- Similar intervention “without technology” (e.g., mirror therapy in contrast to VR-based mirror therapy): 17.95%
- Usual care: 17.95%
- Dose equivalent upper limb training (dose equivalent therapy session focused on the upper limb, considered in add-on to usual care): 10.26%
- Different combinations of technology-based approaches: 10.26%
- Different technology: 7.69%
- Different parameters of the same technology (e.g., different robotic assistance, anodal vs cathodal transcranial direct-current stimulation): 7.69%.
For studies comparing more than 2 groups, different interventions, e.g., as for technology or parameters, are mostly compared to the usual care control condition.
As shown in Table 1, most studies (89.58%) employ inclusion criteria related to the upper limb impairment for the participant enrolment. Figure 5 shows the inclusion criteria and their frequency across studies (43 studies include inclusion criteria). More than half of the studies define inclusion criteria by means of a FMA score (53.50%) or ARAT (9.30%). Nevertheless, evaluation based on motor outcome, i.e., range of motion or ability/inability to perform a specific task, such as that involved in the study protocol, are taken into account in 16.3% studies, as well as spasticity-related scales, i.e., Brunnstrom stages and Tardieu scale, in 11.63% studies. Specifically, for the FMA inclusion criteria, Figure 6 shows the reduction gained by defining inclusion criteria for the participant enrolment. That reduction, expressed as percentage, is computed as the one’s complement of the ratio between the FMA range defined as in the inclusion criteria and the whole FMA range (66-0), according to the following formula:
Seven studies make a reduction between 70% and 80%; among them, the study by Schrader et al. [52] in which inclusion criteria have been defined on the basis of the hand section of the FMA scale (maximum value 14). Most of the studies achieve a 50% reduction, thus including in the same analyses participants who differ in FMA score by 33, i.e., 50% of (66-0), for example in the range [8 38] in [61].
As for the severity of the upper limb impairment at baseline for the stratification of participants in secondary analyses, 25.00% studies exploit such evaluation, defining two or more levels of the variable: FMA (9 studies on 12) and ARAT, motor evoked potentials and range of motion (one per study).
As for the key findings of the trials, i) 41.67% report positive results, i.e., the studies confirm the hypothesis of efficacy of a given intervention via between group analysis, ii) 31.25% report positive results on secondary analyses, i.e., between-group statistical analyses evaluated for sub-items of the primary/secondary outcomes or considering sub-groups of the population under investigation confirm the original hypothesis or if within-group statistical analyses evaluated for the primary/secondary outcomes reveal a statistical improvement only for the experimental group. Negative results are reported from 25.00% of studies, i.e., the target intervention is not superior to the control condition.
3.3.2. Association Results
Figure 7 shows for each type of intervention (top panel in the figure) and motor action required to the participant by the intervention itself (bottom panel in the figure), the upper limb impairment severity (UE-FMA) of participants recruited in that group. Each study has been categorised both according to the intervention type (analysis presented in the top panel) and motor action required (analysis presented in the bottom panel). Data from studies belonging to the same category, e.g., intervention type PS, are pooled together and summarised by means of box charts.
As for the intervention type, most seem to cover almost half of the UE-FMA scale. On average PS-based interventions concern participants with a slightly lower UE-FMA value (18.46 ± 11.55) than other interventions (BCI: 19.52 ± 9.72, NIBS: 25.47 ± 10.67, Robotic: 23.46 ± 10.74; VR and Visual: 29.05 ± 10.36). However, robotic interventions, as shown from the distribution outliers, include studies with UE-FMA values both lower than 5 and higher than 40. As for the motor action required to the participant, studies in which experimental protocol does not require action to participant result to enrol participants with UE-FMA on average lower (19.44 ± 10.62) than studies requiring active motor action (22.41 ± 9.94), even whenever possible (25.14 ± 14.09). However, studies that require active motor actions enrol participants with reduced motor action ability (FMA < 5) as well as participants with moderate motor impairment (FMA=43).
4. Discussion
In this scoping review we provide a portrait of the current evidence derived from RCTs investigating the efficacy of technology-based interventions targeting upper limb motor recovery in patients with severe impairment after stroke. Our main aim is to verify the actual severity of the included patients enrolled in such trials, to confirm or refute the anecdotal notion of extreme variability in baseline motor impairment which might be responsible for the lack of strong evidence supporting efficacy of such interventions [9].
We included papers reporting at least one between FMA and ARAT to assess upper limb motor impairment (Table S1, Supplementary Materials), as they are commonly employed to investigate efficacy rehabilitative treatment [67]. Our results (Table 2) show that FMA is by far the most commonly employed as primary outcome measure, followed by ARAT; other measures that are specific for upper limb function are more commonly employed as secondary outcome, such as BBT, WMFT, MAL.
According to our descriptive analyses on FMA and ARAT values upon enrolment, we verified that the included patients altogether virtually cover the whole range of both scales (Figure 3a,b). That is, these RCTs that were originally implemented to investigate the efficacy of rehabilitative interventions designed for severe patients often include patients with mild to moderate deficits as well. This occurs despite the fact that almost 90% of the studies actually defined inclusion criteria based on severity. As a matter of facts, there is no unique definition of severity, even for the same assessment scale. Again, among those studies in which the inclusion criteria were based on severity, about 50% employed FMA for such a definition. However, the references for the proposed stratification did not converge on a unique subdivision. For example, several papers refer to Fugl-Meyer et al. [13] or Gladstone et al., [68] to justify the use of cut-off values for their inclusion criteria or stratification analyses, but no subdivision is provided in neither of these papers. Woodbury et al., [69] suggest a cut-off below 19 for severe patients and of 47 for moderately impaired patients, which is applied as an inclusion criterion by Carrico et al., [36]. Ding et al. [37] apply the clustering suggested in Woytowicz et al. [70] to define severity in patients with FMA < 35. Conroy et al., [38] apply a cut-off of 25 as suggested by Luft et al., [71]. As a possible explanation for such a wide range of severity among the enrolled patients, we hypothesized that the technology in study could play a role. For example, some robotic devices cannot be proposed to patients with severe spasticity, or an electromyographically triggered orthosis cannot be activated if patients have no residual movement in the target muscles. Thus, we categorized the papers according to the proposed technology. Electrical or magnetic stimulation of peripheral structures (PS) are the most represented technology in our review, followed by robotics. These two or their combinations represent approximately 63% of the studies. The BCI and NIBS (often in combination with other devices) are the topic of about 31% of the studies, while the less represented technology is VR, with just about 6% of the papers. In an attempt to further characterize the interventions according to the fact that they required (or not) active motor actions from the patients, we found out that more than 50% of the interventions required some residual motor ability from the patients. This could be an explanation for the trend to include “not-so-severe” patients in order to increase trial feasibility. Nevertheless, we did not observe a clear difference in the severity of the included patients when we divided the studies according to the technology or to the presence/absence of an active motor exercise. The distributions of patients’ severity (Figure 7) qualitatively show a tendency towards the more severe range for the interventions based on PS and for interventions not requiring active motor tasks. We also highlighted the heterogeneity of included patients in terms of time since injury. While the majority of studies targeted chronic patients exclusively (37.5%), the studies including mixed groups altogether reached a similar percentage (37.47%). It is well known that brain plasticity that underlies motor recovery is time dependent and the recovery potential is different according to the post-stroke phase [72].
Regarding the study design we also pointed out extreme variability in terms of dose/intensity of treatment, type of comparator and sample size. In almost 20% of the two-arm studies “usual care” is the only control condition, while an active comparator would be most desirable. Different dosage and very different sample sizes (ranging from 10 to almost 800 participants) limit the potential impact of our attempt to interpret the results of this scoping review that takes into account such a wide scenario of clinical studies. An indirect result of our scoping review derives from the papers that we excluded for reporting study protocols (n=13). These papers were all published between 2017 and 2023 [73,74,75,76,77,78,79,80,81,82,83,84,85], with ten of them being subsequent to 2020 testifying a progressive increase in the efforts dedicated to rigorous clinical trial design in this field of clinical research.
The ultimate goal of our review work is to improve the design of RCTs to boost the translation of rehabilitative technologies into clinical practice. Indeed, the majority of the selected studies report positive results, indicating efficacy of the proposed technology. However, about 30% of the studies required secondary analyses to support the benefit derived from the intervention in study. Some of them report positive results on secondary outcomes e.g., SIS and WMFT [17,38] and/or outcome sub-items, e.g., ARAT, FMA, MAS items [21,41]. Some required subgroup analyses e.g., proving efficacy only in severe patients [32,41,43,50]. The remaining 25% of openly negative studies (showing non-superiority of the proposed intervention) is likely underestimated, as it is known that publishing a negative result is harder and often occur only in the case of very well designed and well conducted, large clinical trials.
A further observation derived from our work is that along with established clinical and functional scales employed as primary or secondary outcomes (Table 2), 16 papers applied objective measurements of brain and motor activity as means to verify the effects of the intervention on the motor system performance. Advanced analyses on electroencephalographic [26,49] and transcranial magnetic stimulation recordings [43,49,58,60], electromyographic, kinematic and kinetic data [20,24,40,45,49,51,56,57,60,61,62] were performed in these studies to identify modifications in the motor system performance subserving a favorable motor outcome derived from the intervention in study. This suggests that technology is not only employed for the design of rehabilitative interventions but may play a crucial role in improving the outcome assessment with more objective, measurable and reproducible parameters that may serve as biomarkers of motor recovery.
This scoping review has several limitations, mostly related to the heterogeneity of the included studies in terms of numerosity, characteristics of enrolled patients, trial design, implementation, and reporting. We considered papers published between 2008 and 2024 observing a progressive improvement in all of these aspects which will hopefully be fruitful in the upcoming years to properly address some of the issues that we raised here and that remain unanswered. Only 7 studies provide a complete dataset documenting the individual severity of enrolled patients, that would allow a statistical analysis on how effective the interventions were according to a homogeneous stratification of patients based on severity. The policies for data availability are also progressively pointing towards safe data sharing according to internationally agreed General Data Protection Regulations.
5. Conclusions
We represented the current evidence derived from RCTs investigating the efficacy of technology-based interventions targeting upper limb motor recovery in patients with severe impairment after stroke. Our aim was to shed light on the problems of the current research in rehabilitation technologies, to ultimately boost the translational success of such approaches. There is undoubtedly a need for patient stratification upon enrolment, in order to direct resources to patients who will benefit the most from a given approach. The correct taxonomy of patient severity and the related correct reporting in clinical trials could significantly improve the transnationality and contextualization of the results obtained, avoiding biases that could affect potential effectiveness. Only severe patients should be recruited for the clinical validation of devices that are designed specifically for them, while design and development of technologies with adequate sensorimotor and cognitive stimulation would probably increase their salience (and effectiveness) for less affected subjects. As clinical trial design, implementation and reporting improves in this research field, subsequent systematic reviews will probably help in identifying strong evidence and thus clear indications for clinicians.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1. Database Search Strategies.
Author Contributions
Conceptualization, FP, GM.; methodology, EC, GM; formal analysis, EC, FP, GM; data curation, EC, FP; writing—original draft preparation, EC, FP, GM; writing—review and editing, DM, FC, JT, AR; supervision, DM, FC; funding acquisition, DM, FC, JT. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analysed during this study. Data sharing is not applicable to this article.
Acknowledgments
This work was partially funded by the Italian Ministry of Health (Ricerca Corrente 2024) and by Sapienza University of Rome—Progetti di Ateneo 2023.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Iosa, M.; Morone, G.; Fusco, A.; Bragoni, M.; Coiro, P.; Multari, M.; Venturiero, V.; De Angelis, D.; Pratesi, L.; Paolucci, S. Seven Capital Devices for the Future of Stroke Rehabilitation. Stroke Res Treat 2012, 2012, 187965. [Google Scholar] [CrossRef] [PubMed]
- Coscia, M.; Wessel, M.J.; Chaudary, U.; Millán, J.D.R.; Micera, S.; Guggisberg, A.; Vuadens, P.; Donoghue, J.; Birbaumer, N.; Hummel, F.C. Neurotechnology-Aided Interventions for Upper Limb Motor Rehabilitation in Severe Chronic Stroke. Brain 2019, 142, 2182–2197. [Google Scholar] [CrossRef] [PubMed]
- Ward, N.S.; Brander, F.; Kelly, K. Intensive Upper Limb Neurorehabilitation in Chronic Stroke: Outcomes from the Queen Square Programme. J Neurol Neurosurg Psychiatry 2019, 90, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Tenberg, S.; Mueller, S.; Vogt, L.; Roth, C.; Happ, K.; Scherer, M.; Behringer, M.; Niederer, D. Comparative Effectiveness of Upper Limb Exercise Interventions in Individuals With Stroke: A Network Meta-Analysis. Stroke 2023, 54, 1839–1853. [Google Scholar] [CrossRef] [PubMed]
- Dboba, M.M.; Mohd Nordin, N.A.; Manaf, H.; Mohd Rasdi, H.F. Effect of Constraint-Induced Movement Therapy Combined with Neuromuscular Electrical Stimulation on Upper Extremity Function in Stroke Survivors: A Protocol for Systematic Review. Medicine 2023, 102, e34249. [Google Scholar] [CrossRef] [PubMed]
- Morone, G.; Paolucci, S.; Mattia, D.; Pichiorri, F.; Tramontano, M.; Iosa, M. The 3Ts of the New Millennium Neurorehabilitation Gym: Therapy, Technology, Translationality. Expert Rev Med Devices 2016, 13, 785–787. [Google Scholar] [CrossRef]
- Coupar, F.; Pollock, A.; Rowe, P.; Weir, C.; Langhorne, P. Predictors of Upper Limb Recovery after Stroke: A Systematic Review and Meta-Analysis. Clin Rehabil 2012, 26, 291–313. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic Review or Scoping Review? Guidance for Authors When Choosing between a Systematic or Scoping Review Approach. BMC Medical Research Methodology 2018, 18, 143. [Google Scholar] [CrossRef]
- Morone, G.; Pichiorri, F. Post-Stroke Rehabilitation: Challenges and New Perspectives. J Clin Med 2023, 12, 550. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med 2018, 169, 467–473. [Google Scholar] [CrossRef]
- McGowan, J.; Sampson, M.; Salzwedel, D.M.; Cogo, E.; Foerster, V.; Lefebvre, C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. Journal of Clinical Epidemiology 2016, 75, 40–46. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—a Web and Mobile App for Systematic Reviews. Systematic Reviews 2016, 5, 210. [Google Scholar] [CrossRef]
- Fugl-Meyer, A.R.; Jääskö, L.; Leyman, I.; Olsson, S.; Steglind, S. The Post-Stroke Hemiplegic Patient. 1. a Method for Evaluation of Physical Performance. Scand J Rehabil Med 1975, 7, 13–31. [Google Scholar] [CrossRef] [PubMed]
- Platz, T.; Pinkowski, C.; van Wijck, F.; Kim, I.-H.; di Bella, P.; Johnson, G. Reliability and Validity of Arm Function Assessment with Standardized Guidelines for the Fugl-Meyer Test, Action Research Arm Test and Box and Block Test: A Multicentre Study. Clin Rehabil 2005, 19, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the Sample Mean and Standard Deviation from the Sample Size, Median, Range and/or Interquartile Range. BMC Medical Research Methodology 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed]
- Hesse, S.; Werner, C.; Pohl, M.; Mehrholz, J.; Puzich, U.; Krebs, H.I. Mechanical Arm Trainer for the Treatment of the Severely Affected Arm after a Stroke: A Single-Blinded Randomized Trial in Two Centers. American Journal of Physical Medicine and Rehabilitation 2008, 87, 779–788. [Google Scholar] [CrossRef]
- Lo, A.C.; Guarino, P.D.; Richards, L.G.; Haselkorn, J.K.; Wittenberg, G.F.; Federman, D.G.; Ringer, R.J.; Wagner, T.H.; Krebs, H.I.; Volpe, B.T.; et al. Robot-Assisted Therapy for Long-Term Upper-Limb Impairment after Stroke. N. Engl. J. Med. 2010, 362, 1772–1783. [Google Scholar] [CrossRef]
- Weber, D.J.; Skidmore, E.R.; Niyonkuru, C.; Chang, C.-L.; Huber, L.M.; Munin, M.C. Cyclic Functional Electrical Stimulation Does Not Enhance Gains in Hand Grasp Function When Used as an Adjunct to onabotulinumtoxinA and Task Practice Therapy: A Single-Blind, Randomized Controlled Pilot Study. Arch Phys Med Rehabil 2010, 91, 679–686. [Google Scholar] [CrossRef]
- Shindo, K.; Fujiwara, T.; Hara, J.; Oba, H.; Hotta, F.; Tsuji, T.; Hase, K.; Liu, M. Effectiveness of Hybrid Assistive Neuromuscular Dynamic Stimulation Therapy in Patients with Subacute Stroke: A Randomized Controlled Pilot Trial. Neurorehabilitation and Neural Repair 2011, 25, 830–837. [Google Scholar] [CrossRef]
- Rosewilliam, S.; Malhotra, S.; Roffe, C.; Jones, P.; Pandyan, A.D. Can Surface Neuromuscular Electrical Stimulation of the Wrist and Hand Combined with Routine Therapy Facilitate Recovery of Arm Function in Patients with Stroke? Archives of Physical Medicine and Rehabilitation 2012, 93, 1715–1721.e1. [Google Scholar] [CrossRef] [PubMed]
- Ochi, M.; Saeki, S.; Oda, T.; Matsushima, Y.; Hachisuka, K. Effects of Anodal and Cathodal Transcranial Direct Current Stimulation Combined with Robotic Therapy on Severely Affected Arms in Chronic Stroke Patients. Journal of Rehabilitation Medicine 2013, 45, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Cordo, P.; Wolf, S.; Lou, J.-S.; Bogey, R.; Stevenson, M.; Hayes, J.; Roth, E. Treatment of Severe Hand Impairment Following Stroke by Combining Assisted Movement, Muscle Vibration, and Biofeedback. Journal of Neurologic Physical Therapy 2013, 37, 194–203. [Google Scholar] [CrossRef] [PubMed]
- Krewer, C.; Hartl, S.; Müller, F.; Koenig, E. Effects of Repetitive Peripheral Magnetic Stimulation on Upper-Limb Spasticity and Impairment in Patients with Spastic Hemiparesis: A Randomized, Double-Blind, Sham-Controlled Study. Archives of Physical Medicine and Rehabilitation 2014, 95, 1039–1047. [Google Scholar] [CrossRef] [PubMed]
- Au-Yeung, S.S.Y.; Hui-Chan, C.W.Y. Electrical Acupoint Stimulation of the Affected Arm in Acute Stroke: A Placebo-Controlled Randomized Clinical Trial. Clinical Rehabilitation 2014, 28, 149–158. [Google Scholar] [CrossRef]
- Ang, K.K.; Chua, K.S.G.; Phua, K.S.; Wang, C.; Chin, Z.Y.; Kuah, C.W.K.; Low, W.; Guan, C. A Randomized Controlled Trial of EEG-Based Motor Imagery Brain-Computer Interface Robotic Rehabilitation for Stroke. Clinical EEG and Neuroscience 2015, 46, 310–320. [Google Scholar] [CrossRef] [PubMed]
- Pichiorri, F.; Morone, G.; Petti, M.; Toppi, J.; Pisotta, I.; Molinari, M.; Paolucci, S.; Inghilleri, M.; Astolfi, L.; Cincotti, F.; et al. Brain-Computer Interface Boosts Motor Imagery Practice during Stroke Recovery. Ann. Neurol. 2015, 77, 851–865. [Google Scholar] [CrossRef] [PubMed]
- Pennati, G.V.; Da Re, C.; Messineo, I.; Bonzaiuti, D. How Could Robotic Training and Botolinum Toxin Be Combined in Chronic Post Stroke Upper Limb Spasticity? A Pilot Study. European Journal of Physical and Rehabilitation Medicine 2015, 51, 381–387. [Google Scholar]
- Carrico, C.; Chelette, K.C.; Westgate, P.M.; Powell, E.; Nichols, L.; Fleischer, A.; Sawaki, L. Nerve Stimulation Enhances Task-Oriented Training in Chronic, Severe Motor Deficit after Stroke: A Randomized Trial. Stroke 2016, 47, 1879–1884. [Google Scholar] [CrossRef]
- Wu, X.; Guarino, P.; Lo, A.C.; Peduzzi, P.; Wininger, M. Long-Term Effectiveness of Intensive Therapy in Chronic Stroke. Neurorehabilitation and Neural Repair 2016, 30, 583–590. [Google Scholar] [CrossRef]
- Frolov, A.A.; Mokienko, O.; Lyukmanov, R.; Biryukova, E.; Kotov, S.; Turbina, L.; Nadareyshvily, G.; Bushkova, Y. Post-Stroke Rehabilitation Training with a Motor-Imagery-Based Brain-Computer Interface (BCI)-Controlled Hand Exoskeleton: A Randomized Controlled Multicenter Trial. Front Neurosci 2017, 11. [Google Scholar] [CrossRef]
- Tomić, T.J.D.; Savić, A.M.; Vidaković, A.S.; Rodić, S.Z.; Isaković, M.S.; Rodríguez-De-Pablo, C.; Keller, T.; Konstantinović, L.M. ArmAssist Robotic System versus Matched Conventional Therapy for Poststroke Upper Limb Rehabilitation: A Randomized Clinical Trial. BioMed Research International 2017, 2017. [Google Scholar] [CrossRef] [PubMed]
- Schick, T.; Schlake, H.-P.; Kallusky, J.; Hohlfeld, G.; Steinmetz, M.; Tripp, F.; Krakow, K.; Pinter, M.; Dohle, C. Synergy Effects of Combined Multichannel EMG-Triggered Electrical Stimulation and Mirror Therapy in Subacute Stroke Patients with Severe or Very Severe Arm/Hand Paresis. Restorative Neurology and Neuroscience 2017, 35, 319–332. [Google Scholar] [CrossRef] [PubMed]
- Brunner, I.; Skouen, J.S.; Hofstad, H.; Aßmus, J.; Becker, F.; Sanders, A.-M.; Pallesen, H.; Kristensen, L.Q.; Michielsen, M.; Thijs, L.; et al. Virtual Reality Training for Upper Extremity in Subacute Stroke (VIRTUES): A Multicenter RCT. Neurology 2017, 89, 2413–2421. [Google Scholar] [CrossRef]
- Rabadi, M.H.; Aston, C.E. Effect of Transcranial Direct Current Stimulation on Severely Affected Arm-Hand Motor Function in Patients After an Acute Ischemic Stroke: A Pilot Randomized Control Trial. American journal of physical medicine & rehabilitation 2017, 96, S178–S184. [Google Scholar] [CrossRef]
- Marquez-Chin, C.; Bagher, S.; Zivanovic, V.; Popovic, M.R. Functional Electrical Stimulation Therapy for Severe Hemiplegia: Randomized Control Trial Revisited. Canadian Journal of Occupational Therapy 2017, 84, 87–97. [Google Scholar] [CrossRef]
- Carrico, C.; Westgate, P.M.; Salmon Powell, E.; Chelette, K.C.; Nichols, L.; Pettigrew, L.C.; Sawaki, L. Nerve Stimulation Enhances Task-Oriented Training for Moderate-to-Severe Hemiparesis 3-12 Months After Stroke: A Randomized Trial. Am J Phys Med Rehabil 2018, 97, 808–815. [Google Scholar] [CrossRef] [PubMed]
- Ding, L.; Wang, X.; Guo, X.; Chen, S.; Wang, H.; Jiang, N.; Jia, J. Camera-Based Mirror Visual Feedback: Potential to Improve Motor Preparation in Stroke Patients. IEEE Transactions on Neural Systems and Rehabilitation Engineering 2018, 26, 1897–1905. [Google Scholar] [CrossRef] [PubMed]
- Conroy, S.S.; Wittenberg, G.F.; Krebs, H.I.; Zhan, M.; Bever, C.T.; Whitall, J. Robot-Assisted Arm Training in Chronic Stroke: Addition of Transition-to-Task Practice. Neurorehabilitation and Neural Repair 2019, 33, 751–761. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, H.; Bosomworth, H.; Krebs, H.I.; van Wijck, F.; Howel, D.; Wilson, N.; Aird, L.; Alvarado, N.; Andole, S.; Cohen, D.L.; et al. Robot Assisted Training for the Upper Limb after Stroke (RATULS): A Multicentre Randomised Controlled Trial. The Lancet 2019, 394, 51–62. [Google Scholar] [CrossRef]
- Ramos-Murguialday, A.; Curado, M.R.; Broetz, D.; Yilmaz, Ö.; Brasil, F.L.; Liberati, G.; Garcia-Cossio, E.; Cho, W.; Caria, A.; Cohen, L.G.; et al. Brain-Machine Interface in Chronic Stroke: Randomized Trial Long-Term Follow-Up. Neurorehabil Neural Repair 2019, 33, 188–198. [Google Scholar] [CrossRef]
- Takebayashi, T.; Takahashi, K.; Domen, K.; Hachisuka, K. Impact of Initial Flexor Synergy Pattern Scores on Improving Upper Extremity Function in Stroke Patients Treated with Adjunct Robotic Rehabilitation: A Randomized Clinical Trial. Topics in Stroke Rehabilitation 2020, 27, 516–524. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Park, G.; Cho, D.Y.; Kim, H.Y.; Lee, J.-Y.; Kim, S.; Park, S.-B.; Shin, J.-H. Comparisons between End-Effector and Exoskeleton Rehabilitation Robots Regarding Upper Extremity Function among Chronic Stroke Patients with Moderate-to-Severe Upper Limb Impairment. Scientific Reports 2020, 10. [Google Scholar] [CrossRef] [PubMed]
- Chew, E.; Teo, W.-P.; Tang, N.; Ang, K.K.; Ng, Y.S.; Zhou, J.H.; Teh, I.; Phua, K.S.; Zhao, L.; Guan, C. Using Transcranial Direct Current Stimulation to Augment the Effect of Motor Imagery-Assisted Brain-Computer Interface Training in Chronic Stroke Patients—Cortical Reorganization Considerations. Frontiers in Neurology 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-W.; Kuo, L.-C.; Lin, Y.-C.; Su, F.-C.; Lin, Y.-A.; Hsu, H.-Y. Development and Testing of a Virtual Reality Mirror Therapy System for the Sensorimotor Performance of Upper Extremity: A Pilot Randomized Controlled Trial. IEEE Access 2021, 9, 14725–14734. [Google Scholar] [CrossRef]
- Hu, Y.-Q.; Gao, T.-H.; Li, J.; Tao, J.-C.; Bai, Y.-L.; Lu, R.-R. Motor Imagery-Based Brain-Computer Interface Combined with Multimodal Feedback to Promote Upper Limb Motor Function after Stroke: A Preliminary Study. Evidence-based Complementary and Alternative Medicine 2021, 2021. [Google Scholar] [CrossRef] [PubMed]
- Boasquevisque, D.D.S.; Servinsckins, L.; De Paiva, J.P.Q.; Dos Santos, D.G.; Soares, P.; Pires, D.S.; Meltzer, J.A.; Plow, E.B.; De Freitas, P.F.; Speciali, D.S.; et al. Contralesional Cathodal Transcranial Direct Current Stimulation Does Not Enhance Upper Limb Function in Subacute Stroke: A Pilot Randomized Clinical Trial. Neural Plasticity 2021, 2021. [Google Scholar] [CrossRef] [PubMed]
- Dawson, J.; Liu, C.Y.; Francisco, G.E.; Cramer, S.C.; Wolf, S.L.; Dixit, A.; Alexander, J.; Ali, R.; Brown, B.L.; Feng, W.; et al. Vagus Nerve Stimulation Paired with Rehabilitation for Upper Limb Motor Function after Ischaemic Stroke (VNS-REHAB): A Randomised, Blinded, Pivotal, Device Trial. The Lancet 2021, 397, 1545–1553. [Google Scholar] [CrossRef] [PubMed]
- Llorens, R.; Fuentes, M.A.; Borrego, A.; Latorre, J.; Alcañiz, M.; Colomer, C.; Noé, E. Effectiveness of a Combined Transcranial Direct Current Stimulation and Virtual Reality-Based Intervention on Upper Limb Function in Chronic Individuals Post-Stroke with Persistent Severe Hemiparesis: A Randomized Controlled Trial. Journal of NeuroEngineering and Rehabilitation 2021, 18. [Google Scholar] [CrossRef]
- Cantillo-Negrete, J.; Carino-Escobar, R.I.; Carrillo-Mora, P.; Rodriguez-Barragan, M.A.; Hernandez-Arenas, C.; Quinzaños-Fresnedo, J.; Hernandez-Sanchez, I.R.; Galicia-Alvarado, M.A.; Miguel-Puga, A.; Arias-Carrion, O. Brain-Computer Interface Coupled to a Robotic Hand Orthosis for Stroke Patients’ Neurorehabilitation: A Crossover Feasibility Study. Frontiers in Human Neuroscience 2021, 15. [Google Scholar] [CrossRef]
- Takebayashi, T.; Takahashi, K.; Okita, Y.; Kubo, H.; Hachisuka, K.; Domen, K. Impact of the Robotic-Assistance Level on Upper Extremity Function in Stroke Patients Receiving Adjunct Robotic Rehabilitation: Sub-Analysis of a Randomized Clinical Trial. Journal of NeuroEngineering and Rehabilitation 2022, 19. [Google Scholar] [CrossRef]
- Jiang, Y.-F.; Zhang, D.; Zhang, J.; Hai, H.; Zhao, Y.-Y.; Ma, Y.-W. A Randomized Controlled Trial of Repetitive Peripheral Magnetic Stimulation Applied in Early Subacute Stroke: Effects on Severe Upper-Limb Impairment. Clinical Rehabilitation 2022, 36, 693–702. [Google Scholar] [CrossRef] [PubMed]
- Schrader, M.; Sterr, A.; Kettlitz, R.; Wohlmeiner, A.; Buschfort, R.; Dohle, C.; Bamborschke, S. The Effect of Mirror Therapy Can Be Improved by Simultaneous Robotic Assistance. Restor Neurol Neurosci 2022, 40, 185–194. [Google Scholar] [CrossRef]
- Ohnishi, H.; Miyasaka, H.; Shindo, N.; Ito, K.; Tsuji, S.; Sonoda, S. Effectiveness of Repetitive Facilitative Exercise Combined with Electrical Stimulation Therapy to Improve Very Severe Paretic Upper Limbs in with Stroke Patients: A Randomized Controlled Trial. Occup Ther Int 2022, 2022, 4847363. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-J.; Wang, S.-M.; Chen, C.; Chen, C.-A.; Wu, C.-W.; Chen, J.-J.; Peng, C.-W.; Lin, C.-W.; Huang, S.-W.; Chen, S.-C. High-Definition Transcranial Direct Current with Electrical Theta Burst on Post-Stroke Motor Rehabilitation: A Pilot Randomized Controlled Trial. Neurorehabilitation and Neural Repair 2022, 36, 645–654. [Google Scholar] [CrossRef]
- Wong, Y.; Li, C.-J.-Z.; Ada, L.; Zhang, T.; Månum, G.; Langhammer, B. UPPER LIMB TRAINING A WITH HAND ORTHOSIS IN EARLY SUBACUTE STROKE: A PILOT RANDOMIZED TRIAL. Journal of Rehabilitation Medicine 2022, 54. [Google Scholar] [CrossRef] [PubMed]
- Cordo, P.; Wolf, S.; Rymer, W.Z.; Byl, N.; Stanek, K.; Hayes, J.R. Assisted Movement With Proprioceptive Stimulation Augments Recovery From Moderate-To-Severe Upper Limb Impairment During Subacute Stroke Period: A Randomized Clinical Trial. Neurorehabilitation and Neural Repair 2022, 36, 239–250. [Google Scholar] [CrossRef]
- Takebayashi, T.; Takahashi, K.; Amano, S.; Gosho, M.; Sakai, M.; Hashimoto, K.; Hachisuka, K.; Uchiyama, Y.; Domen, K. Robot-Assisted Training as Self-Training for Upper-Limb Hemiplegia in Chronic Stroke: A Randomized Controlled Trial. Stroke 2022, 53, 2182–2191. [Google Scholar] [CrossRef]
- Williamson, J.N.; James, S.A.; He, D.; Li, S.; Sidorov, E.V.; Yang, Y. High-Definition Transcranial Direct Current Stimulation for Upper Extremity Rehabilitation in Moderate-to-Severe Ischemic Stroke: A Pilot Study. Frontiers in Human Neuroscience 2023, 17. [Google Scholar] [CrossRef]
- Dawson, J.; Engineer, N.D.; Cramer, S.C.; Wolf, S.L.; Ali, R.; O’Dell, M.W.; Pierce, D.; Prudente, C.N.; Redgrave, J.; Feng, W.; et al. Vagus Nerve Stimulation Paired With Rehabilitation for Upper Limb Motor Impairment and Function After Chronic Ischemic Stroke: Subgroup Analysis of the Randomized, Blinded, Pivotal, VNS-REHAB Device Trial. Neurorehabilitation and Neural Repair 2023, 37, 367–373. [Google Scholar] [CrossRef]
- Wang, T.; Liu, Z.; Gu, J.; Tan, J.; Hu, T. Effectiveness of Soft Robotic Glove versus Repetitive Transcranial Magnetic Stimulation in Post-Stroke Patients with Severe Upper Limb Dysfunction: A Randomised Controlled Trial. Frontiers in Neurology 2023, 13. [Google Scholar] [CrossRef]
- Chen, Z.-J.; He, C.; Xu, J.; Zheng, C.-J.; Wu, J.; Xia, N.; Hua, Q.; Xia, W.-G.; Xiong, C.-H.; Huang, X.-L. Exoskeleton-Assisted Anthropomorphic Movement Training for the Upper Limb After Stroke: The EAMT Randomized Trial. Stroke 2023, 54, 1464–1473. [Google Scholar] [CrossRef] [PubMed]
- Feingold-Polak, R.; Barzel, O.; Levy-Tzedek, S. Socially Assistive Robot for Stroke Rehabilitation: A Long-Term in-the-Wild Pilot Randomized Controlled Trial. IEEE Trans Neural Syst Rehabil Eng 2024, 32, 1616–1626. [Google Scholar] [CrossRef] [PubMed]
- Brunner, I.; Lundquist, C.B.; Pedersen, A.R.; Spaich, E.G.; Dosen, S.; Savic, A. Brain Computer Interface Training with Motor Imagery and Functional Electrical Stimulation for Patients with Severe Upper Limb Paresis after Stroke: A Randomized Controlled Pilot Trial. Journal of NeuroEngineering and Rehabilitation 2024, 21, 10. [Google Scholar] [CrossRef] [PubMed]
- Duncan, P.W.; Wallace, D.; Lai, S.M.; Johnson, D.; Embretson, S.; Laster, L.J. The Stroke Impact Scale Version 2.0. Evaluation of Reliability, Validity, and Sensitivity to Change. Stroke 1999, 30, 2131–2140. [Google Scholar] [CrossRef]
- Sulter, G.; Steen, C.; De Keyser, J. Use of the Barthel Index and Modified Rankin Scale in Acute Stroke Trials. Stroke 1999, 30, 1538–1541. [Google Scholar] [CrossRef]
- Morris, D.M.; Uswatte, G.; Crago, J.E.; Cook III, E.W.; Taub, E. The Reliability of the Wolf Motor Function Test for Assessing Upper Extremity Function after Stroke. Archives of Physical Medicine and Rehabilitation 2001, 82, 750–755. [Google Scholar] [CrossRef] [PubMed]
- Sivan, M.; O’Connor, R.J.; Makower, S.; Levesley, M.; Bhakta, B. Systematic Review of Outcome Measures Used in the Evaluation of Robot-Assisted Upper Limb Exercise in Stroke. J Rehabil Med 2011, 43, 181–189. [Google Scholar] [CrossRef]
- Gladstone, D.J.; Danells, C.J.; Black, S.E. The Fugl-Meyer Assessment of Motor Recovery after Stroke: A Critical Review of Its Measurement Properties. Neurorehabil Neural Repair 2002, 16, 232–240. [Google Scholar] [CrossRef]
- Woodbury, M.L.; Velozo, C.A.; Richards, L.G.; Duncan, P.W. Rasch Analysis Staging Methodology to Classify Upper Extremity Movement Impairment after Stroke. Arch Phys Med Rehabil 2013, 94, 1527–1533. [Google Scholar] [CrossRef]
- Woytowicz, E.J.; Rietschel, J.C.; Goodman, R.N.; Conroy, S.S.; Sorkin, J.D.; Whitall, J.; McCombe Waller, S. Determining Levels of Upper Extremity Movement Impairment by Applying a Cluster Analysis to the Fugl-Meyer Assessment of the Upper Extremity in Chronic Stroke. Arch Phys Med Rehabil 2017, 98, 456–462. [Google Scholar] [CrossRef]
- Luft, A.R.; McCombe-Waller, S.; Whitall, J.; Forrester, L.W.; Macko, R.; Sorkin, J.D.; Schulz, J.B.; Goldberg, A.P.; Hanley, D.F. Repetitive Bilateral Arm Training and Motor Cortex Activation in Chronic Stroke: A Randomized Controlled Trial. JAMA 2004, 292, 1853–1861. [Google Scholar] [CrossRef]
- Zeiler, S.R.; Krakauer, J.W. The Interaction between Training and Plasticity in the Poststroke Brain. Curr Opin Neurol 2013, 26, 609–616. [Google Scholar] [CrossRef] [PubMed]
- Alexander, J.; Langhorne, P.; Kidd, L.; Wu, O.; McConnachie, A.; van Wijck, F.; Dawson, J. SaeboGlove Therapy for Upper Limb Disability and Severe Hand Impairment after Stroke (SUSHI): Study Protocol for a Randomised Controlled Trial. Eur Stroke J 2021, 6, 302–310. [Google Scholar] [CrossRef]
- Dai, W.; Yang, X.; Liu, C.; Ding, H.; Guo, C.; Zhu, Y.; Dong, M.; Qian, Y.; Fang, L.; Wang, T.; et al. Effects of Repetitive Transcranial Magnetic Stimulation over the Contralesional Dorsal Premotor Cortex on Upper Limb Function in Severe Ischaemic Stroke: Study Protocol for a Randomised Controlled Trial. BMJ Open 2023, 13, e074037. [Google Scholar] [CrossRef]
- Gonzalez-Santos, J.; Soto-Camara, R.; Rodriguez-Fernández, P.; Jimenez-Barrios, M.; Gonzalez-Bernal, J.; Collazo-Riobo, C.; Jahouh, M.; Bravo-Anguiano, Y.; Trejo-Gabriel-Galan, J.M. Effects of Home-Based Mirror Therapy and Cognitive Therapeutic Exercise on the Improvement of the Upper Extremity Functions in Patients with Severe Hemiparesis after a Stroke: A Protocol for a Pilot Randomised Clinical Trial. BMJ Open 2020, 10, e035768. [Google Scholar] [CrossRef]
- Kinoshita, S.; Ikeda, K.; Yasuno, S.; Takahashi, S.; Yamada, N.; Okuyama, Y.; Sasaki, N.; Hada, T.; Kuriyama, C.; Suzuki, S.; et al. Dose-Response of rPMS for Upper Limb Hemiparesis after Stroke. Medicine (Baltimore) 2020, 99, e20752. [Google Scholar] [CrossRef]
- Lee, S.H.; Kim, W.-S.; Park, J.; Kim, J.; Paik, N.-J. Effects of Anodal Transcranial Direct Current Stimulation over the Contralesional Hemisphere on Motor Recovery in Subacute Stroke Patients with Severe Upper Extremity Hemiparesis: Study Protocol for a Randomized Controlled Trial. Medicine (Baltimore) 2020, 99, e19495. [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, L.; Wang, S.; Long, L.; Zang, Q.; Jia, G. Efficacy and Safety of Electroacupuncture at Auricular Concha Region in Promoting of Rehabilitation of Ischemic Stroke Patients with Upper Limb Motor Dysfunction: A Study Protocol for a Randomized Pilot Trial. Medicine (Baltimore) 2022, 101, e28047. [Google Scholar] [CrossRef]
- Mizuno, K.; Abe, T.; Ushiba, J.; Kawakami, M.; Ohwa, T.; Hagimura, K.; Ogura, M.; Okuyama, K.; Fujiwara, T.; Liu, M. Evaluating the Effectiveness and Safety of the Electroencephalogram-Based Brain-Machine Interface Rehabilitation System for Patients With Severe Hemiparetic Stroke: Protocol for a Randomized Controlled Trial (BEST-BRAIN Trial). JMIR Res Protoc 2018, 7, e12339. [Google Scholar] [CrossRef]
- Mohan, A.; Knutson, J.S.; Cunningham, D.A.; Widina, M.; O’Laughlin, K.; Arora, T.; Li, X.; Sakaie, K.; Wang, X.; Uchino, K.; et al. Contralaterally Controlled Functional Electrical Stimulation Combined With Brain Stimulation for Severe Upper Limb Hemiplegia-Study Protocol for a Randomized Controlled Trial. Front Neurol 2022, 13, 869733. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, H.; Shaw, L.; Bosomworth, H.; Aird, L.; Alvarado, N.; Andole, S.; Cohen, D.L.; Dawson, J.; Eyre, J.; Finch, T.; et al. Robot Assisted Training for the Upper Limb after Stroke (RATULS): Study Protocol for a Randomised Controlled Trial. Trials 2017, 18, 340. [Google Scholar] [CrossRef] [PubMed]
- Stoykov, M.E.; Biller, O.M.; Wax, A.; King, E.; Schauer, J.M.; Fogg, L.F.; Corcos, D.M. Bilateral Upper Extremity Motor Priming (BUMP) plus Task-Specific Training for Severe, Chronic Upper Limb Hemiparesis: Study Protocol for a Randomized Clinical Trial. Trials 2022, 23, 523. [Google Scholar] [CrossRef] [PubMed]
- van Lieshout, E.C.C.; Visser-Meily, J.M.A.; Neggers, S.F.W.; van der Worp, H.B.; Dijkhuizen, R.M. Brain Stimulation for Arm Recovery after Stroke (B-STARS): Protocol for a Randomised Controlled Trial in Subacute Stroke Patients. BMJ Open 2017, 7, e016566. [Google Scholar] [CrossRef]
- Wei, D.; Hua, X.-Y.; Zheng, M.-X.; Wu, J.-J.; Xu, J.-G. Effectiveness of Robot-Assisted Virtual Reality Mirror Therapy for Upper Limb Motor Dysfunction after Stroke: Study Protocol for a Single-Center Randomized Controlled Clinical Trial. BMC Neurol 2022, 22, 307. [Google Scholar] [CrossRef]
- Wei, X.; Xia, N.; Li, Y.-A.; Gu, M.; Zhang, T.; Gao, W.; Liu, Y. Immediate and Short-Term Effects of Continuous Theta Burst Transcranial Magnetic Stimulation over Contralesional Premotor Area on Post-Stroke Spasticity in Patients with Severe Hemiplegia: Study Protocol for a Randomized Controlled Trial. Front Neurol 2022, 13, 895580. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flow chart of search and selection process.
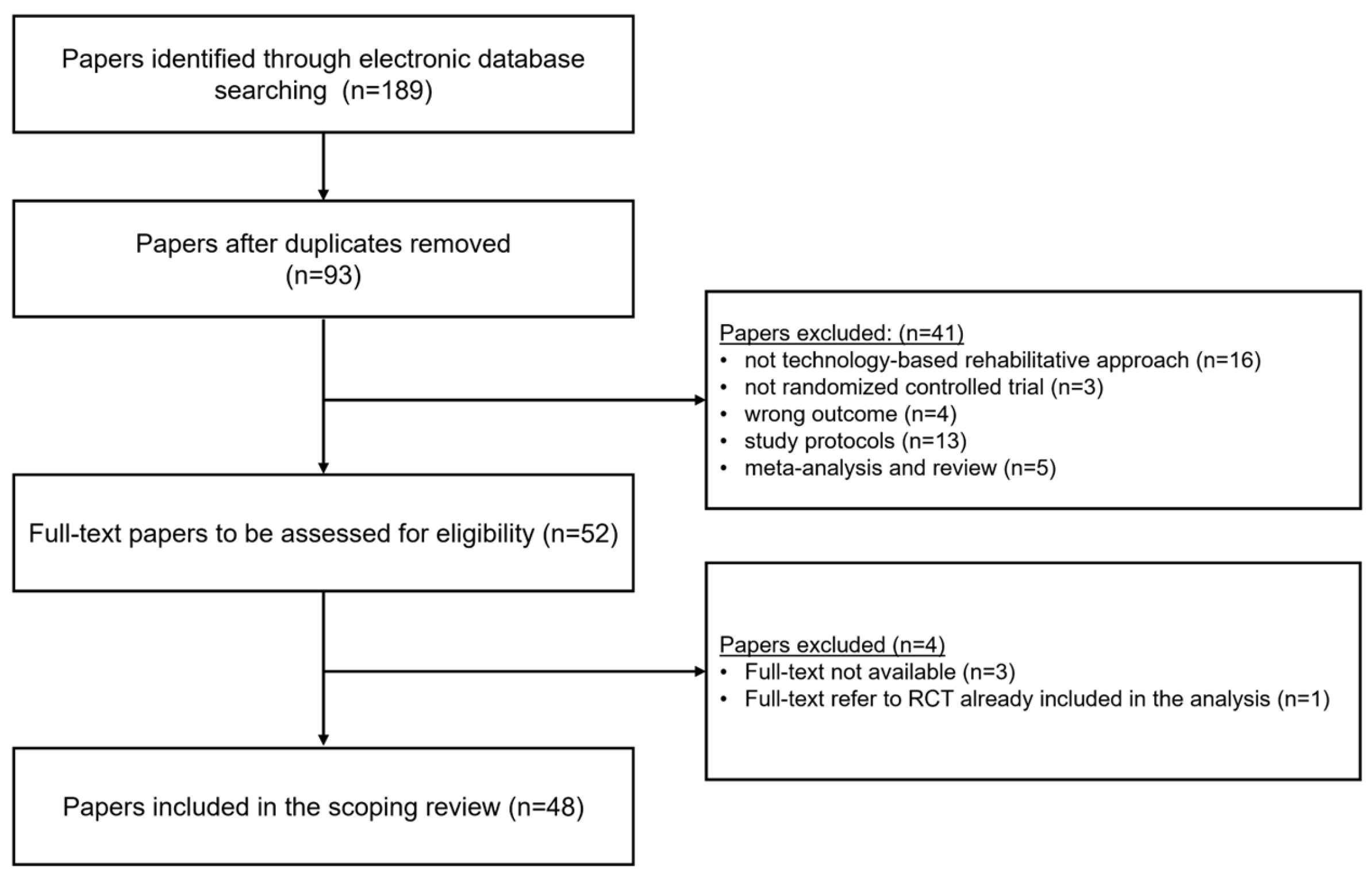
Figure 2.
Distribution across studies (n=48) of the stroke population enrolled and classified, in terms of time from the cerebral lesion to enrolment in the study, as follows: ≤ 1 month (acute), ≤ 3 months (early subacute), ≤ 6 months (subacute), > 6 months (chronic).
Figure 2.
Distribution across studies (n=48) of the stroke population enrolled and classified, in terms of time from the cerebral lesion to enrolment in the study, as follows: ≤ 1 month (acute), ≤ 3 months (early subacute), ≤ 6 months (subacute), > 6 months (chronic).
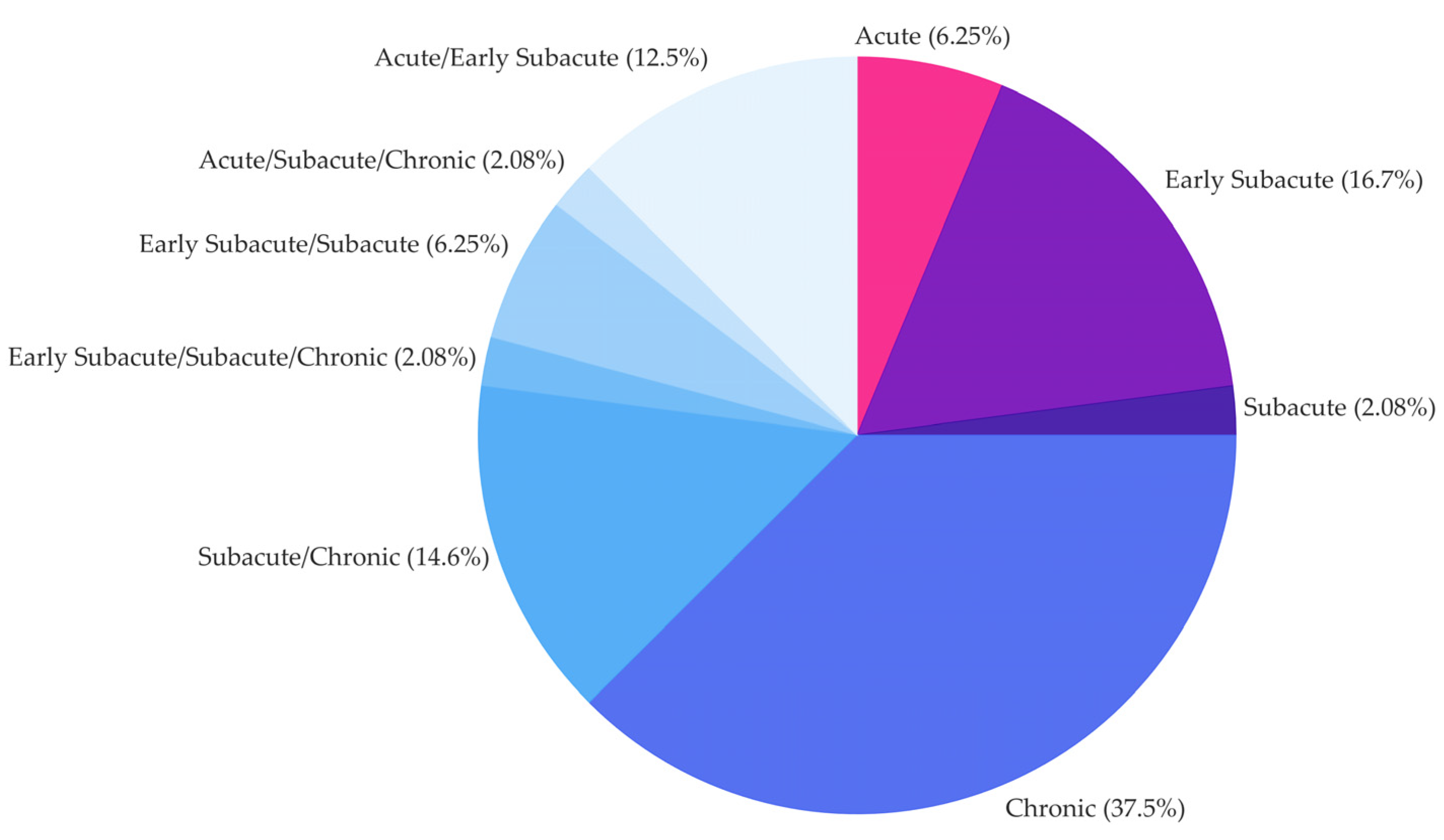
Figure 3.
(a)—Upper Extremity Fugl-Meyer Assessment (FMA) score: minimum score 0, maximum score 66 equal to normal. (b) Action Research Arm Test score: minimum score 0, maximum score 57 equal to normal. Red circle and grey line code for studies presenting FMA or ARAT score expressed as mean (red circle) ± standard deviation (grey line). Blue square marker and black line code for studies presenting FMA or ARAT score expressed as median (blue square) and first/third quartile (black line running from the first to the third quartile). (*) marker codes for two studies [52,62] that assess FMA out of a maximum of 60 scores and codes for one study [40] that assess FMA out of maximum of 54 score.
Figure 3.
(a)—Upper Extremity Fugl-Meyer Assessment (FMA) score: minimum score 0, maximum score 66 equal to normal. (b) Action Research Arm Test score: minimum score 0, maximum score 57 equal to normal. Red circle and grey line code for studies presenting FMA or ARAT score expressed as mean (red circle) ± standard deviation (grey line). Blue square marker and black line code for studies presenting FMA or ARAT score expressed as median (blue square) and first/third quartile (black line running from the first to the third quartile). (*) marker codes for two studies [52,62] that assess FMA out of a maximum of 60 scores and codes for one study [40] that assess FMA out of maximum of 54 score.
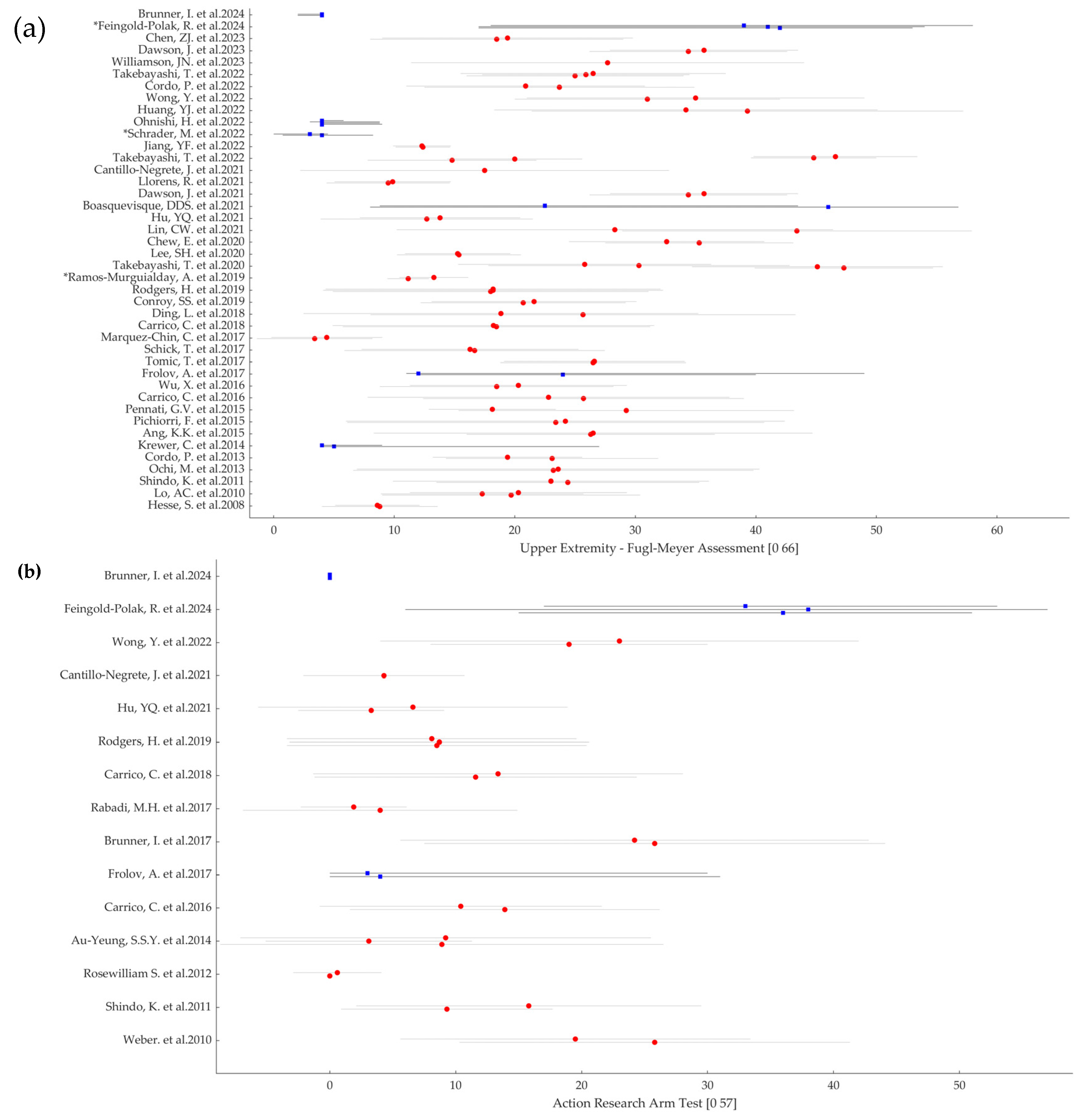
Figure 4.
Distribution across studies (n=48) of the technology-based rehabilitative intervention types, grouped as: Brain-Computer Interface (BCI), Non-Invasive Brain Stimulation (NIBS), Peripheral Stimulation (PS), Robotic, Virtual Reality (VR) and Visual and their combination.
Figure 4.
Distribution across studies (n=48) of the technology-based rehabilitative intervention types, grouped as: Brain-Computer Interface (BCI), Non-Invasive Brain Stimulation (NIBS), Peripheral Stimulation (PS), Robotic, Virtual Reality (VR) and Visual and their combination.
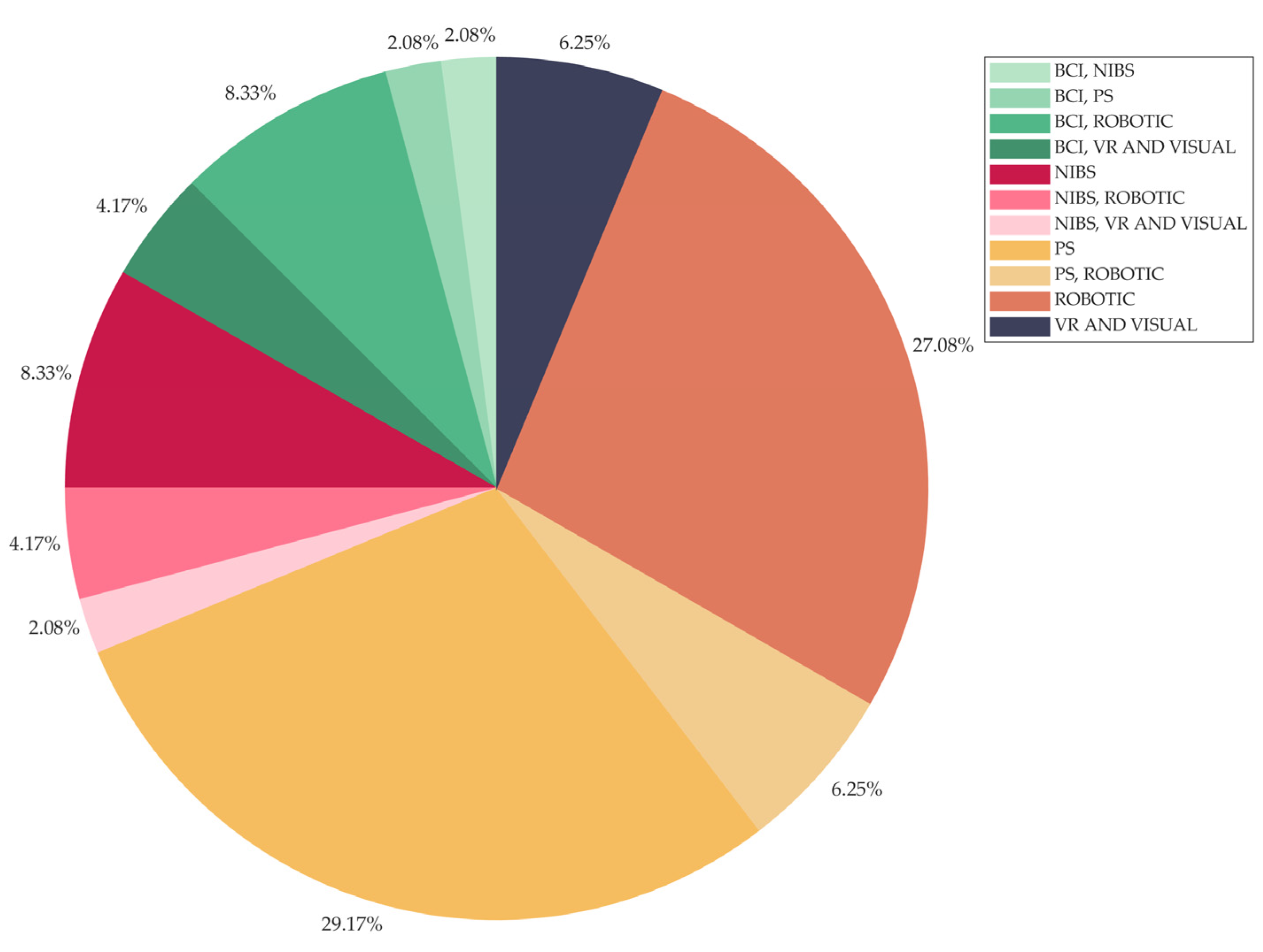
Figure 5.
Distribution across studies (n=43) of the parameters (clinical/functional scale or motor-related evaluation) used for the enrolment inclusion criteria definition and grouped as: UE-FMA: Upper Extremity Fugl-Meyer Assessment; ARAT: Action Research Arm Test; MRC: Medical Research Council Scale; MI: Motricity Index; SIAS: Stroke Impairment Assessment Set; Motor outcome concerns range of motion evaluation and evaluation of ability/inability to perform a specific task.
Figure 5.
Distribution across studies (n=43) of the parameters (clinical/functional scale or motor-related evaluation) used for the enrolment inclusion criteria definition and grouped as: UE-FMA: Upper Extremity Fugl-Meyer Assessment; ARAT: Action Research Arm Test; MRC: Medical Research Council Scale; MI: Motricity Index; SIAS: Stroke Impairment Assessment Set; Motor outcome concerns range of motion evaluation and evaluation of ability/inability to perform a specific task.
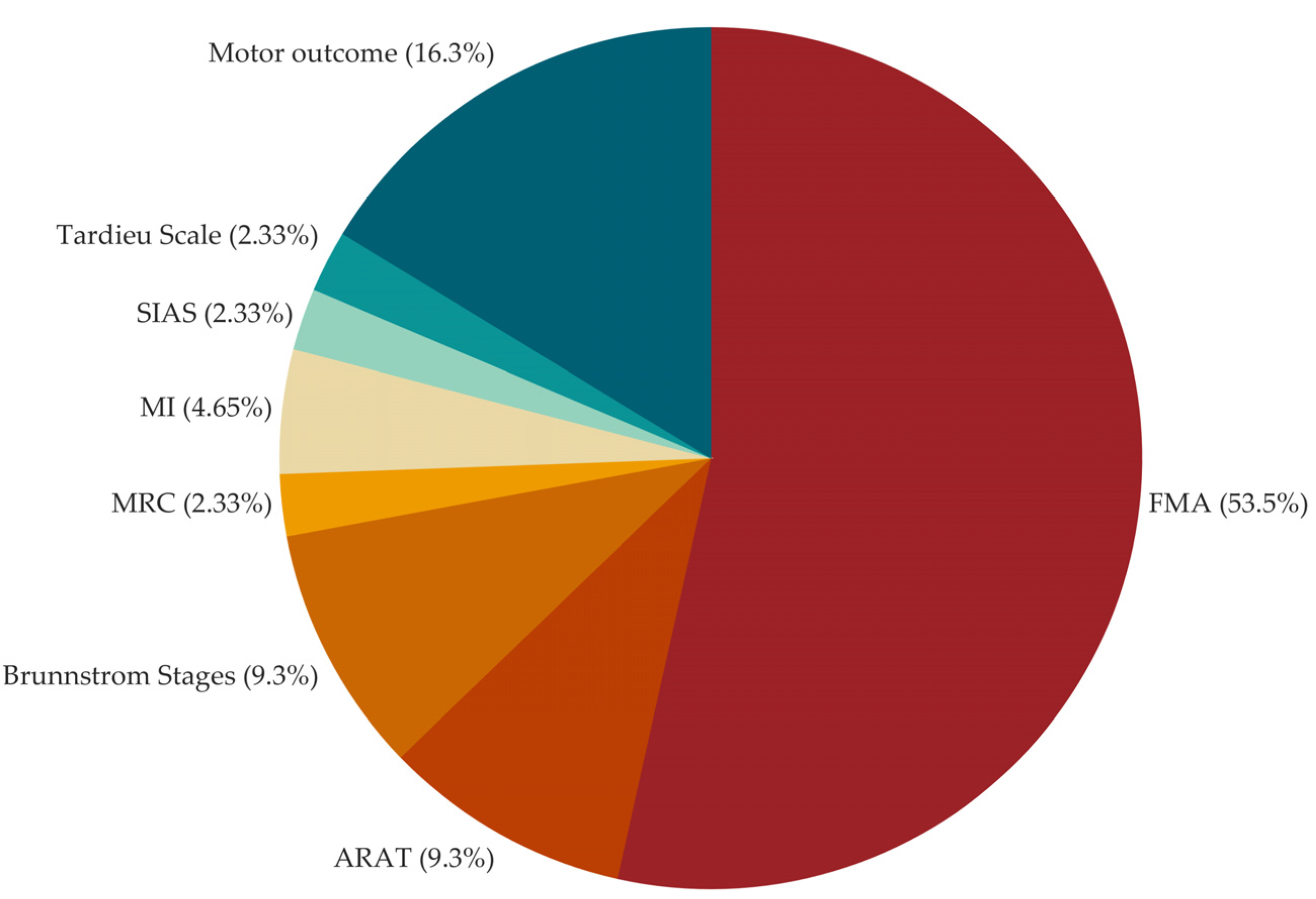
Figure 6.
Histogram of number of studies which define inclusion criteria by means of Upper Extremity Fugl-Meyer Assessment (UE-FMA) score, reported as function of the UE-FMA range reduction achieved by defining inclusion criteria for the participant enrollment.
Figure 6.
Histogram of number of studies which define inclusion criteria by means of Upper Extremity Fugl-Meyer Assessment (UE-FMA) score, reported as function of the UE-FMA range reduction achieved by defining inclusion criteria for the participant enrollment.
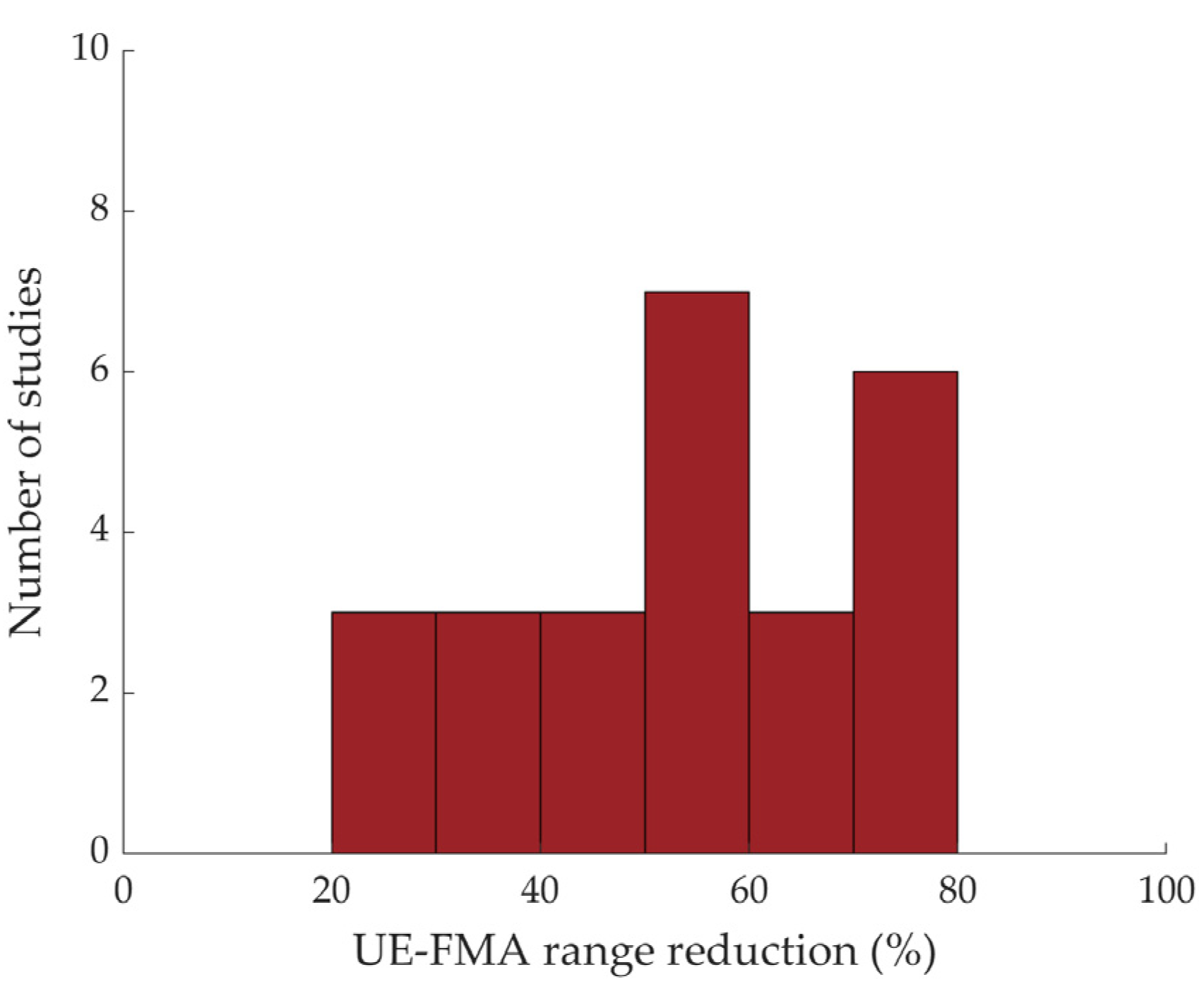
Figure 7.
Distribution across studies (n=42) of UE-FMA at baseline, grouped by intervention type (top panel) and motor action required to participant (bottom panel). The triangle-up marker codes for the average of each distribution. Intervention types were categorized as: BCI (Brain-Computer Interface), NIBS (Non-Invasive Brain Stimulation), PS (peripheral stimulation, Robotic, VR (Virtual Reality) and Visual. Each study is assigned to a single category. Studies that investigate combinations of technology-based interventions, e.g., BCI and PS or BCI and Robotic have been assigned to the most significant intervention type according to the study design, e.g., BCI and PS have been assigned to the BCI category when PS was employed in the control condition as well, thus BCI control resulted to be the core of the rehabilitative intervention in study. Active motor actions are categorized as: no/yes/ yes wherever possible.
Figure 7.
Distribution across studies (n=42) of UE-FMA at baseline, grouped by intervention type (top panel) and motor action required to participant (bottom panel). The triangle-up marker codes for the average of each distribution. Intervention types were categorized as: BCI (Brain-Computer Interface), NIBS (Non-Invasive Brain Stimulation), PS (peripheral stimulation, Robotic, VR (Virtual Reality) and Visual. Each study is assigned to a single category. Studies that investigate combinations of technology-based interventions, e.g., BCI and PS or BCI and Robotic have been assigned to the most significant intervention type according to the study design, e.g., BCI and PS have been assigned to the BCI category when PS was employed in the control condition as well, thus BCI control resulted to be the core of the rehabilitative intervention in study. Active motor actions are categorized as: no/yes/ yes wherever possible.
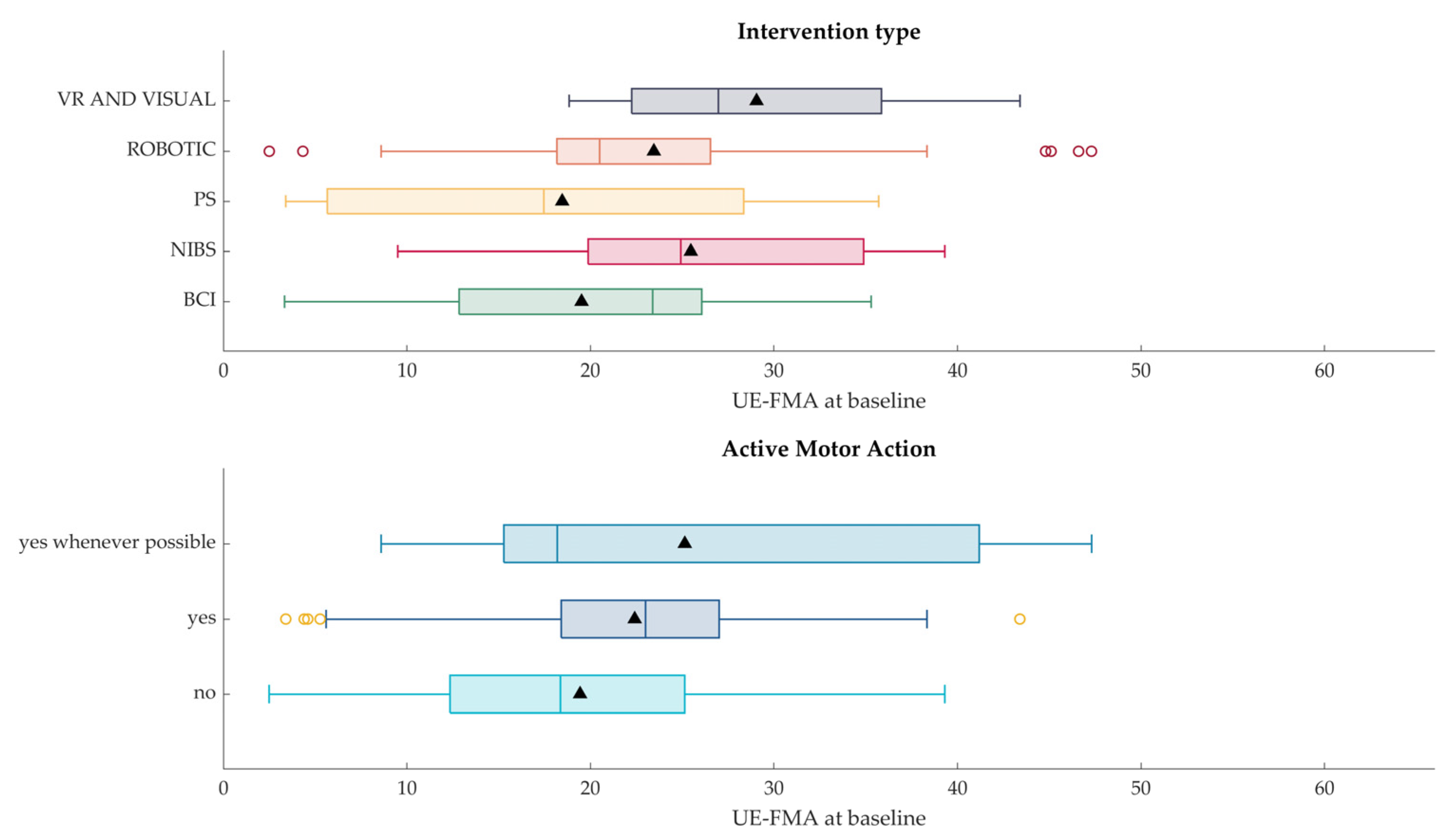

Table 1.
Studies included in the review. The following data are reported: name of first author and publication year, population sample size (number of participants per group, whenever available), severity of the impairment assessed via UE-FMA and ARAT (per group, whenever available), if inclusion criteria related to the upper limb impairment for the participant enrolment (IC) were defined, time since injury, intervention type, active motor action required, comparator, primary outcome measures, key findings. UE-FMA and ARAT values are reported as mean ± standard deviation or median and interquartile range (Q1-Q3).
Table 1.
Studies included in the review. The following data are reported: name of first author and publication year, population sample size (number of participants per group, whenever available), severity of the impairment assessed via UE-FMA and ARAT (per group, whenever available), if inclusion criteria related to the upper limb impairment for the participant enrolment (IC) were defined, time since injury, intervention type, active motor action required, comparator, primary outcome measures, key findings. UE-FMA and ARAT values are reported as mean ± standard deviation or median and interquartile range (Q1-Q3).
| First Author Name, Year of Publication | Population sample size (participants per group) | Severity of the impairment (UE-FMA and/or ARAT per group) | IC | Time since Injury | Intervention Type | Active Motor Action required | Comparator | Primary Outcome Measures | Key Findings |
|---|---|---|---|---|---|---|---|---|---|
| Hesse, 2008 [16] | EG: 27 CG: 27 |
UE-FMA EG: 8.8 ± 4.5 CG: 8.6 ± 3.5 |
Yes | ES | PS, Robotic | Yes, whenever possible | Different Technology | UE- FMA | Neg |
| Lo, 2010 [17] | EG: 47 CG1: 46 CG2: 27 |
UE-FMA EG: 19.7 ± 10.7 CG1: 17.3 ± 8.4 CG2: 20.3 ± 9.0 |
Yes | C | Robotic | Yes | Dose Equivalent UL training, Usual Care |
UE- FMA | Pos On Sec |
| Weber, 2010 [18] | EG: 10 CG: 13 |
ARAT EG: 19.5 ± 13.9 CG: 25.8 ± 15.5 |
Yes | C | PS | Yes | Without Technology | MAL | Neg |
| Shindo, 2011 [19] | EG: 10 CG: 10 |
UE-FMA EG: 24.4 ± 10.9 CG: 23.0 ± 13.1 ARAT EG: 9.3 ± 8.4 CG: 15.8 ± 13.7 |
Yes | ES | PS | Yes | Without technology | UE-FMA | Pos |
| Rosewilliam, 2012 [20] | EG: 31 CG: 36 |
ARAT EG: 0.0 ± 0.0 CG: 0.6 ± 3.5 |
Yes | A/ES | PS | No | Usual Care | ARAT | Neg |
| Ochi, 2013 [21] | EG: 9 CG: 9 |
UE-FMA EG: 23.2 ± 16.6 CG: 23.6 ± 16.7 |
Yes | C | NIBS, Robotic | No | Different Parameters | UE-FMA | Pos On Sec |
| Cordo, 2013 [22] | EG1: 22 EG2: 21 |
UE-FMA EG1: 23.1 ± 8.8 EG2: 19.4 ± 6.2 |
Yes | C | PS, Robotic | Yes | Different Technology | UE-FMA | Pos On Sec |
| Krewer, 2014 [23] | EG: 31 CG: 32 |
UE-FMA EG: 5 (4-27) CG: 4 (4-9) |
Yes | C | PS | No | Sham Stimulation | MTS UE-FMA |
Pos On Sec |
| Au-Yeung, 2014 [24] | EG: 29 CG1: 21 CG2: 23 |
ARAT EG: 8.9 ± 17.6 CG1: 3.1 ± 8.2 CG2: 9.2 ± 16.3 |
Yes | A | PS | No | Sham Stimulation, Usual Care | Force measures | Pos |
| Ang, 2015 [25] | EG: 11 CG: 14 |
UE-FMA EG: 26.3 ± 10.3 CG: 26.5 ± 18.2 |
Yes | C | BCI, Robotic | Yes | Different Combination | UE-FMA | Neg |
| Pichiorri, 2015 [26] | EG: 14 CG: 14 |
UE-FMA EG: 23.4 ± 17.3 CG: 24.2 ± 18.2 |
No | ES/S | BCI, VR and Visual | No | Without Technology | UE-FMA | Pos |
| Pennati, 2015 [27] | EG1: 8 EG2: 7 |
UE-FMA EG1: 29.25 ± 13.91 EG2: 18.14 ± 5.27 |
No | C | Robotic | Yes | Different Combination | UE-FMA BBT FIM MAS |
Neg |
| Carrico, 2016 [28] | EG: 18 CG: 18 |
UE-FMA EG: 25.7 ± 13.3 CG: 22.8 ± 15.0 ARAT EG: 13.9 ± 12.3 CG: 10.4 ± 11.2 |
Yes | C | PS | Yes | Sham Stimulation | UE-FMA |
Pos |
| Wu, 2016 [29] | EG: 99 CG: 28 |
UE-FMA EG: 18.5 ± 9.7 CG: 20.3 ± 9.0 |
Yes | C | Robotic | Yes | Usual Care | UE-FMA | Pos |
| Frolov, 2017 [30] | EG: 55 CG: 19 |
UE-FMA EG: 24.0 (12.0-40.0) CG: 12.0 (11.0-49.0) ARAT EG: 4.0 (0.0-31.0) CG: 3.0 (0.0-30.0) |
No | S/C | BCI, Robotic | No | Sham Control | UE-FMA ARAT |
Pos On Sec |
| Tomic, 2017 [31] | EG: 13 CG: 13 |
UE-FMA EG: 26.5 ± 7.7 CG: 26.6 ± 7.5 |
Yes | ES | Robotic | Yes | Dose Equivalent UL Training | UE-FMA | Pos |
| Schick, 2017 [32] | EG: 16 CG: 17 |
UE-FMA EG: 16.67 ± 10.80 CG: 16.29 ± 9.00 |
Yes | ES | PS | No | Different Combination | UE-FMA | Pos On Sec |
| Brunner, 2017 [33] | EG: 57 CG: 55 |
ARAT EG: 25.8 ± 18.3 CG: 24.2 ± 18.6 |
Yes | ES | VR and Visual | Yes | Dose Equivalent UL Training | ARAT | Neg |
| Rabadi, 2017 [34] | EG: 8 CG: 8 |
ARAT EG: 4.0 ± 10.9 CG: 1.9 ± 4.2 |
Yes | A | NIBS | No | Sham Stimulation | ARAT | Neg |
| Marquez-Chin, 2017 [35] | EG: 10 CG: 11C |
UE-FMA EG: 3.4 ± 4.8 CG: 4.4 ± 4.6 |
Yes | A/ES | PS | Yes | Usual Care | FIM UE-FMA |
Pos |
| Carrico, 2018 [36] | EG: 33 CG: 22 |
UE-FMA EG: 18.48 ± 12.75 CG: 18.23 ± 13.34 ARAT EG: 11.58 ± 12.80 CG: 13.36 ± 14.68 |
Yes | S/C | PS | No | Sham Stimulation | WMFT | Pos |
| Ding, 2018 [37] | EG: 38 CG: 41 |
UE-FMA EG: 25.66 ± 17.63 CG: 18.85 ± 16.38 |
No | S/C | VR and Visual | Yes | Dose Equivalent UL Training | UE-FMA | Pos |
| Conroy, 2019 [38] | EG: 22 CG: 19 |
UE-FMA EG: 20.7 ± 8.5 CG: 21.6 ± 8.5 |
Yes | C | Robotic | Yes | Different Combination | UE-FMA | Pos On Sec |
| Rodgers, 2019 [39] | EG: 239 CG1: 246 CG2: 223 |
UE-FMA EG: 18.0 ± 13.1 CG1: 18.2 ± 14.1 CG2: 18.2 ± 13.9 ARAT EG: 8.5 ± 11.9 CG1: 8.7 ± 11.9 CG2: 8.1 ± 11.5 |
Yes | S/C | Robotic | Yes, whenever possible | Dose Equivalent UL Training, Usual care | ARAT | Neg |
| Ramos-Murguialday, 2019 [40] | EG: 16 CG: 12 |
UE-FMA EG: 11.16 ± 1.73 CG: 13.29 ± 2.86 |
Yes | C | BCI, Robotic | Yes | Sham Control | UE-FMA (54) | Pos On Sec |
| Takebayashi, 2020 [41] | EG: 30 CG: 26 |
UE-FMA EG: 47.3 ± 7.4 (mild) CG: 45.1 ± 19.4 (mild) EG: 30.3 ± 12.5 (moderate) CG: 25.8 ± 10.5 (moderate) EG: 16.1 ± 10.5 (severe) CG: 14.8 ± 4.7 (severe) |
Yes | ES | Robotic | Yes, whenever possible | Dose Equivalent UL Training | UE-FMA | Pos On Sec |
| Lee, 2020 [42] | EG1: 19 EG2: 19 |
UE-FMA EG1: 15.37 ± 5.14 EG2: 15.26 ± 4.37 |
Yes | S/C | Robotic | Yes, whenever possible | Different Technology | UE-FMA WMFT |
(*) |
| Chew, 2020 [43] | EG: 10 CG: 9 |
UE-FMA EG: 35.3 ± 7.8 CG: 32.6 ± 8.1 |
Yes | C | BCI, NIBS | No | Sham Stimulation | UE-FMA |
Pos On Sec |
| Lin, 2021 [44] | EG: 9 CG: 9 |
UE-FMA EG: 43.4 ± 14.5 CG: 28.3 ± 18.1 |
Yes | C | VR and Visual | Yes | Without technology | UE-FMA | Pos |
| Hu, 2021 [45] | EG: 7 CG: 5 |
UE-FMA EG: 12.70 ± 8.80 CG: 13.80 ± 6.65 ARAT EG: 3.29 ± 5.79 CG: 6.60 ± 12.29 |
Yes | S/C | BCI, VR and Visual | No | Without technology | UE-FMA | Pos On Sec |
| Boasquevisque, 2021 [46] | EG: 15 CG: 15 |
UE-FMA EG: 46 (8-56.8) CG: 22.5 (8.8-43.5) |
No | A/ES | NIBS | No | Sham Stimulation | Safety (**) | Neg |
| Dawson, 2021 [47] | EG: 53 CG: 54 |
UE-FMA EG: 34.4 ± 8.2 CG: 35.7 ± 7.8 |
Yes | C | PS | Yes | Sham Stimulation | UE-FMA | Pos |
| Llorens, 2021 [48] | EG: 14 CG: 15 |
UE-FMA EG: 9.50 ± 5.11 CG: 9.87 ± 4.82 |
Yes | C | NIBS, VR and Visual | Yes | Usual Care | UE-FMA | Pos |
| Cantillo-Negrete, 2021 [49] | 10 cross-over study | UE-FMA 17.5 ± 15.3 ARAT 4.3 ± 6.4 |
Yes | S/C | BCI, Robotic | No | Usual Care | UE-FMA | Neg |
| Takebayashi, 2022 [50] | EG1: 17 EG2: 13 |
UE-FMA EG1: 14.8 ± 7.0 (severe) EG2: 20.0 ± 5.6 (severe) EG1: 44.8 ± 5.2 (moderate) EG2: 46.6 ± 6.8 (moderate) |
Yes | ES | Robotic | Yes, whenever possible | Different parameters | UE-FMA WMFT |
Pos On Sec |
| Jiang, 2022 [51] | EG: 24 CG: 20 |
UE-FMA EG: 12.38 ± 2.26 CG: 12.30 ± 2.39 |
Yes | A | PS | No | Usual Care | UE-FMA | Pos |
| Schrader, 2022 [52] | EG: 14 CG: 10 |
UE-FMA EG: 4.00 (0.75-8.25) CG: 3.00 (0.00-4.50) |
Yes | A/S/C | Robotic | No | Without technology | UE-FMA (60) | Pos |
| Ohnishi, 2022 [53] | EG1: 25 EG2: 22 EG3: 26 CG: 26 |
UE-FMA EG1: 4.0 (4.0-9.0) EG2: 4.0 (4.0-8.8) EG3: 4.0 (3.0-8.8) CG: 4.0 (4.0-5.8) |
Yes | EA | PS | Yes | Different parameters, Usual Care |
SIAS UE-FMA MAS FIM |
Pos |
| Huang, 2022 [54] | EG: 13 CG: 11 |
UE-FMA EG: 39.3 ± 17.9 CG: 34.2 ± 15.9 |
Yes | C | NIBS | No | Sham Stimulation | UE-FMA | Pos On Sec |
| Wong, 2022 [55] | EG: 15 CG: 15 |
UE-FMA EG: 31 ± 11 CG: 35 ± 14 ARAT EG: 19 ± 11 CG: 23 ± 19 |
Yes | A/ES | PS | Yes | Without technology | ARAT | Neg |
| Cordo, 2022 [56] | EG: 44 CG: 39 |
UE-FMA EG: 20.9 ± 9.9 CG: 23.7 ± 11.2 |
Yes | ES/S | PS, Robotic |
Yes | Different parameters | UE-FMA | Pos |
| Takebayashi, 2022 [57] | EG1: 42 EG2: 39 CG: 36 |
UE-FMA EG1: 25.9 ± 8.6 EG2: 26.5 ± 11.0 CG: 25.0 ± 0.9 |
Yes | C | Robotic | Yes | Without technology | UE-FMA | Pos On Sec |
| Williamson, 2023 [58] | 8 cross-over study | UE-FMA 27.7 ± 16.3 |
Yes | ES/S/C | NIBS | No | Different Parameters, Sham Stimulation | UE-FMA | Pos |
| Dawson, 2023 [59] | EG: 53 CG: 55 |
UE-FMA EG: 34.4 ± 8.2 CG: 35.7 ± 7.8 |
Yes | C | PS | Yes | Sham Stimulation | UE-FMA | Pos |
| Wang, 2023 [60] | EG1: 23 EG2: 23 CG: 23 |
UE-FMA EG1: 9 (IQR: 12) EG2: 11 (IQR: 8) CG: 14 (IQR: 16) |
Yes | ES/S | NIBS, Robotic | Yes | Different Technology, Usual care |
UE-FMA BI |
Pos |
| Chen, 2023 [61] | EG: 40 CG: 40 |
UE-FMA EG: 18.5 ± 10.5 CG: 19.4 ± 10.4 |
Yes | A/ES | Robotic | Yes | Usual Care | UE-FMA | Pos |
| Feingold-Polak, 2024 [62] | EG1: 10 EG2: 8 CG: 8 |
UE-FMA (60) EG1: 42 (17-53) EG2: 41 (17-54) CG: 39 (18-58) ARAT EG1: 36 (15-51) EG2: 38 (6-57) CG: 33(17-53) |
Yes | S | Robotic | Yes | Different Technology, Usual Care |
UE-FMA (60) ARAT MAL SIS |
Pos On Sec |
| Brunner, 2024 [63] | EG: 15 CG: 20 |
UE-FMA EG: 4 (2-4) CG: 4 (2-4) ARAT EG: 0 (0-0) CG: 0 (0-0) |
Yes | A/ES | BCI, PS | No | Usual Care | ARAT | Neg |
Legend: A: Acute phase (≤ 1 month); ARAT: Action Research Arm Test; BCI: Brain-Computer Interface; BBT: Box and Block Test; BI: Barthel Index; CG: Control Group; C: Chronic phase (> 6 months); EG: Experimental Group; ES: Early Subacute phase (≤ 3 months); FIM: Functional Independence Measure; IQR: inter-quartile range; MAL: Motor Activity Log; MAS: Modified Ashworth Scale; MTS: Modified Tardieu Scale; Neg: Negative key findings; NIBS: Non-Invasive Brain Stimulation; Pos: Positive key findings; Pos On Sec: Positive findings on secondary analyses; PS: Peripheral Stimulation; S: Subacute phase (≤ 6 months); SIAS: Stroke Impairment Assessment Set; SIS: Stroke Impact Scale; UL: upper limb; UE-FMA: Upper extremity Fugl-Meyer Assessment; VR: Virtual Reality; WMFT: Wolf Motor Function Test. (*) Lee et al. 2020 [42]: we did not define key findings because the hypothesis about the effectiveness of the intervention EG1 compared to the EG2 is not clear. (**) Boasquevisque et al. 2021 [46]: safety is defined as primary outcome, but authors stated the primary outcome results were published elsewhere. (60) or (54): the expression (60) and (54) codes for UE-FMA assessed on 60 or 54, respectively.
Table 2.
List of the primary and secondary outcomes and number of studies that consider each one as primary (column on the left side) or secondary (column on the right side) outcome.
Table 2.
List of the primary and secondary outcomes and number of studies that consider each one as primary (column on the left side) or secondary (column on the right side) outcome.
| Outcome | As Primary number of studies |
As Secondary number of studies |
|---|---|---|
| Upper Extremity Fugl-Meyer Assessment | 38 | 5 |
| Action Research Arm Test | 8 | 8 |
| Wolf Motor Function Test | 3 | 9 |
| Functional Independence Measure | 3 | 2 |
| Modified Ashworth Scale | 2 | 9 |
| Motor Activity Log | 2 | 6 |
| Stroke Impact Scale | 1 | 11 |
| Barthel Index | 1 | 11 |
| Box and Block Test | 1 | 4 |
| Stroke Impairment Assessment Set: knee-mouth and finger function test | 1 | |
| Modified Tardieu Scale | 1 | |
| Goal Attainment Scaling | 2 | |
| Motricity Index | 2 | |
| Medical Research Council Scale | 2 | |
| National Institutes of Health Stroke Scale | 2 | |
| Finger-Nose Test | 1 | |
| Jebsen-Taylor Hand Function Test | 1 | |
| Hamilton Depression Scale | 1 | |
| Mental Rotation Task | 1 | |
| Modified Rankin Scale | 1 | |
| Montreal Cognitive Assessment | 1 | |
| Nine-hole peg test | 1 | |
| Nottingham Sensory Assessment | 1 | |
| Numeric Rating Scale Pain | 1 | |
| Rancho Los Amigos Scale | 1 | |
| Rivermead Assessment of Somatosensory Performance | 1 | |
| Stroke specific Quality of Life Scale | 1 | |
| Motor outcome (kinematic, kinetic, electromyographic parameters) | 1 | 10 |
| Brain outcome (transcranial magnetic stimulation and electroencephalographic parameters) | 5 | |
| Safety (adverse events) | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



